8/4/2019 Global Burden of Tb
http://slidepdf.com/reader/full/global-burden-of-tb 1/79
1
A rapid appraisal of organisation , implementation
and utilization of DOTS in Jammu district
Supervisor : Dr S.Vivek Adish
BY –
DR Vinay Chib
National Institute of Health and Family Welfare
Munirka, New Delhi-110067
8/4/2019 Global Burden of Tb
http://slidepdf.com/reader/full/global-burden-of-tb 2/79
2
Table 1 Acronyms
AIDS Acquired Immunodeficiency Syndrome
CHC Community Health Centre
CTD Central TB Division
DANIDA Danish International Development Agency
DTC District TB Centres
DTO District Tuberculosis Centre
DMC Designated Microscopy Centre
GDP Gross Domestic Product
HDI Human Development Index
HIV Human Immunodeficiency Virus
MO Medical Officer
MOTC Medical Officer Tuberculosis Centre
MDR-TB Multi-drug Resistant TB
NTP National Treatment Program
PHC Primary Health Care Centre
RNTCP Revised National Tuberculosis Control Programme
SIDA Swedish International Development Agency
STC State TB Cells
8/4/2019 Global Burden of Tb
http://slidepdf.com/reader/full/global-burden-of-tb 3/79
3
STO State Tuberculosis Officer
STLS Senior Tuberculosis Laboratory Supervisor
STS Senior Treatment Supervisors
TB Tuberculosis
TBHV Tuberculosis Health Visiter
TU Tuberculosis Unit
USAID United States Agency for International Development
WHO World Health Organization.

8/4/2019 Global Burden of Tb
http://slidepdf.com/reader/full/global-burden-of-tb 4/79
4
8/4/2019 Global Burden of Tb
http://slidepdf.com/reader/full/global-burden-of-tb 5/79
5
INTRODUCTION :-
GLOBAL BURDEN OF TB
Tuberculosis is the leading cause of death from a curable infectiousdisease caused by Mycobacterium Tuberculosis. TB has affected
mankind for over 5000 years and is still continuing to be a leading
cause of morbidity and mortality. More than 1.3 million people die of
this disease every year. Nearly 1/3rd
of the world’s population is
infected with tuberculosis Bacilli and approximately 10% of them
have a lifetime risk of developing TB disease.
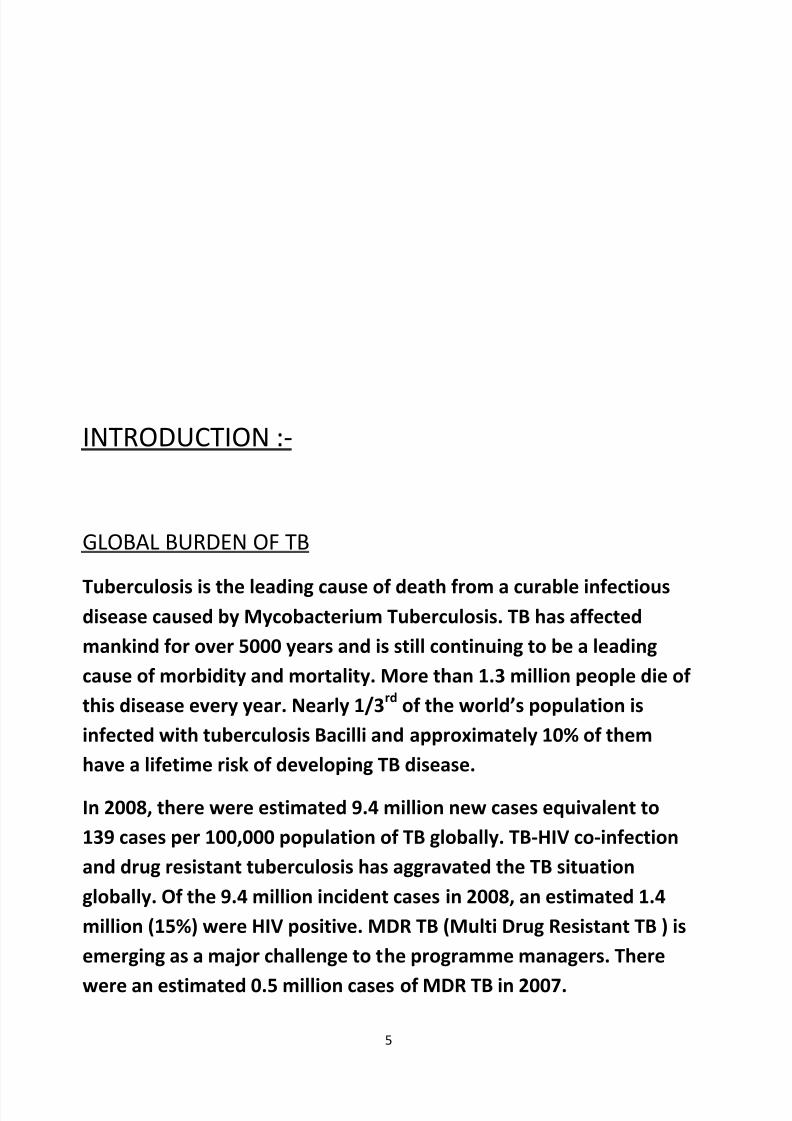
In 2008, there were estimated 9.4 million new cases equivalent to
139 cases per 100,000 population of TB globally. TB-HIV co-infection
and drug resistant tuberculosis has aggravated the TB situation
globally. Of the 9.4 million incident cases in 2008, an estimated 1.4
million (15%) were HIV positive. MDR TB (Multi Drug Resistant TB ) is
emerging as a major challenge to the programme managers. There
were an estimated 0.5 million cases of MDR TB in 2007.
8/4/2019 Global Burden of Tb
http://slidepdf.com/reader/full/global-burden-of-tb 6/79
6
TB DISEASE AND TREATMENT
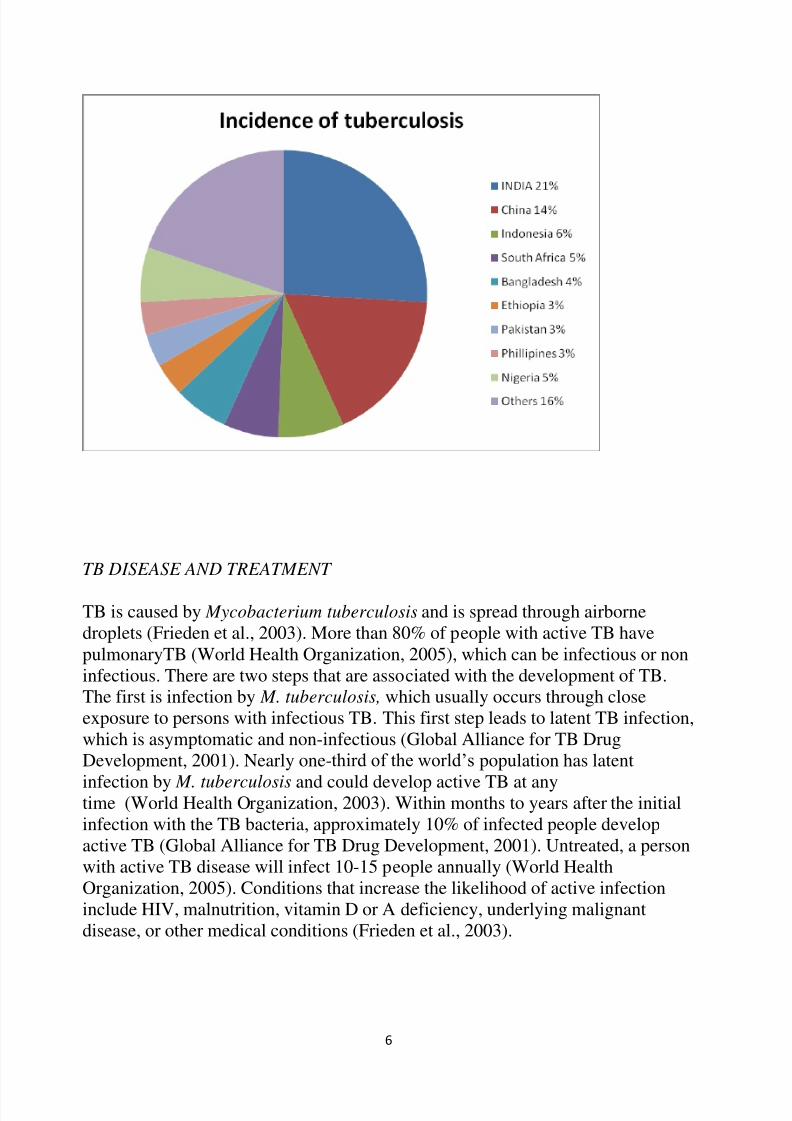
TB is caused by Mycobacterium tuberculosis and is spread through airbornedroplets (Frieden et al., 2003). More than 80% of people with active TB havepulmonaryTB (World Health Organization, 2005), which can be infectious or noninfectious. There are two steps that are associated with the development of TB.The first is infection by M. tuberculosis, which usually occurs through closeexposure to persons with infectious TB. This first step leads to latent TB infection,which is asymptomatic and non-infectious (Global Alliance for TB DrugDevelopment, 2001). Nearly one-third of the world‟s population has latent
infection by M. tuberculosis and could develop active TB at anytime (World Health Organization, 2003). Within months to years after the initialinfection with the TB bacteria, approximately 10% of infected people developactive TB (Global Alliance for TB Drug Development, 2001). Untreated, a personwith active TB disease will infect 10-15 people annually (World HealthOrganization, 2005). Conditions that increase the likelihood of active infectioninclude HIV, malnutrition, vitamin D or A deficiency, underlying malignantdisease, or other medical conditions (Frieden et al., 2003).

8/4/2019 Global Burden of Tb
http://slidepdf.com/reader/full/global-burden-of-tb 7/79
7
8/4/2019 Global Burden of Tb
http://slidepdf.com/reader/full/global-burden-of-tb 8/79
8
TUBERCULOSIS BURDEN IN INDIA
India is the highest TB burden country accounting for 1/5th
of globalincidence. Every year approx. 18 Lac people develop TB and about 4
Lakh die from it.
In India EVERY DAY:
More than 40,000 people become newly infected
with tuberculosis bacilli.
More than 5000 develop TB disease.
More than 1000 people die of TB(i.e. 1 death every
11/2
minutes.)
In 2008, out of estimated global incidence of 9.4 million cases, 1.98
million cases were from India.
ESTIMATED BURDEN OF TB IN INDIA
No of million (95%CI) Rate per lac
person(95%CI)
Incidence( WHO
estimate 2009)
All cases
AFB smear positive
1.982
0.885
168
75Period
Prevalence(2000-GOI
estimate)
AFB positive
Bacillary
1.7
3.8
165
369
Prevalence all
cases(2000 WHO est)
Prevalence All cases
4.968
3.304
443
283
8/4/2019 Global Burden of Tb
http://slidepdf.com/reader/full/global-burden-of-tb 9/79
9
(2007 WHO
estimate)
Prevalence all cases
(2009 WHOestimate)
2.186 185
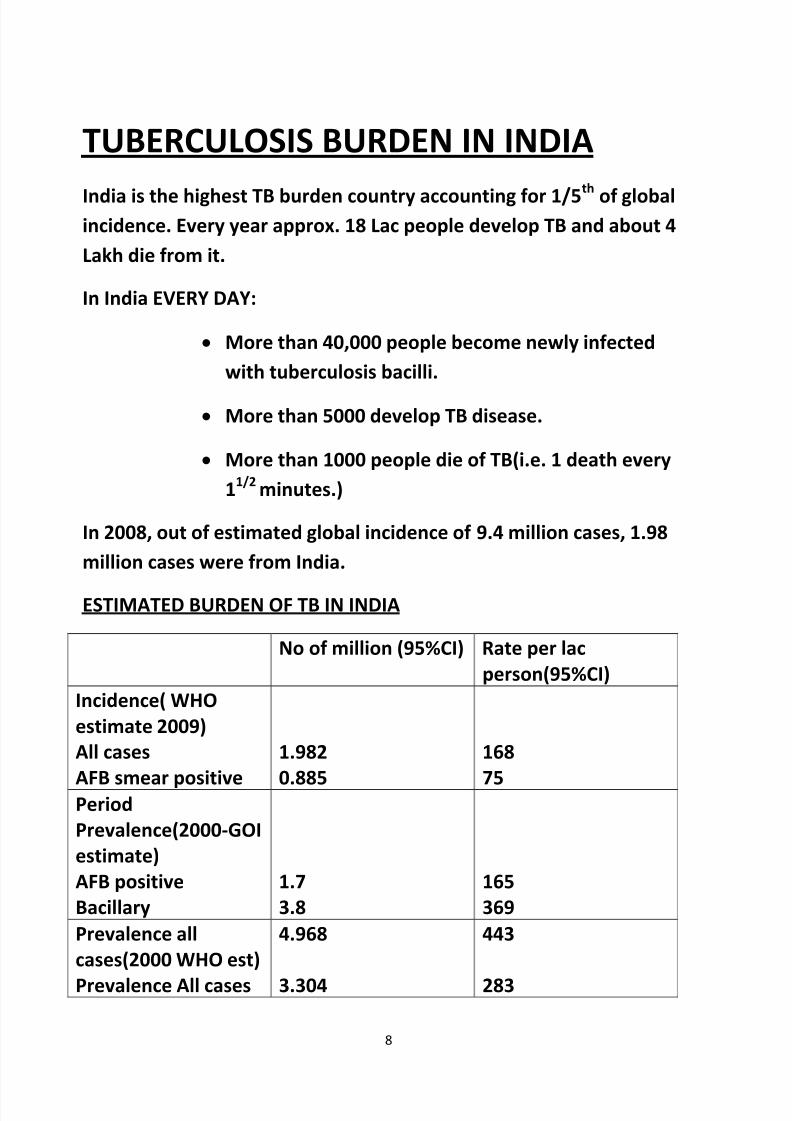
TB-related Millennium Development GoalGoal 6 – to combat HIV/AIDS, malaria and other diseasesTarget 8 – to have halted by 2015 and begun to reverse the
incidence of malaria and other major diseases, includingtuberculosis.Indicators for Target 8 to be used to evaluate the implementationand impact of TB control:Indicator 23: Between 1990 and 2015, to halve the prevalenceand death rates associated with tuberculosis; andIndicator 24: by 2005, to detect 70% of new smear positiveTB cases arising annually, and to successfully treat 85% of these cases.
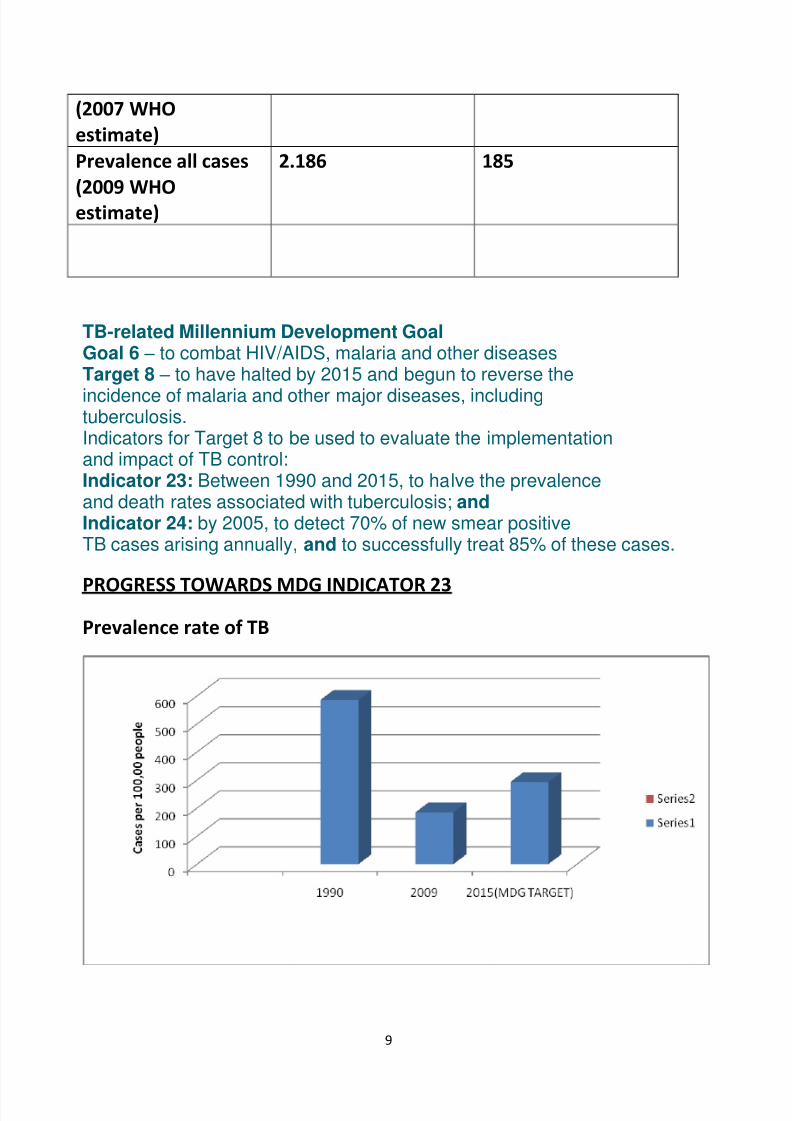
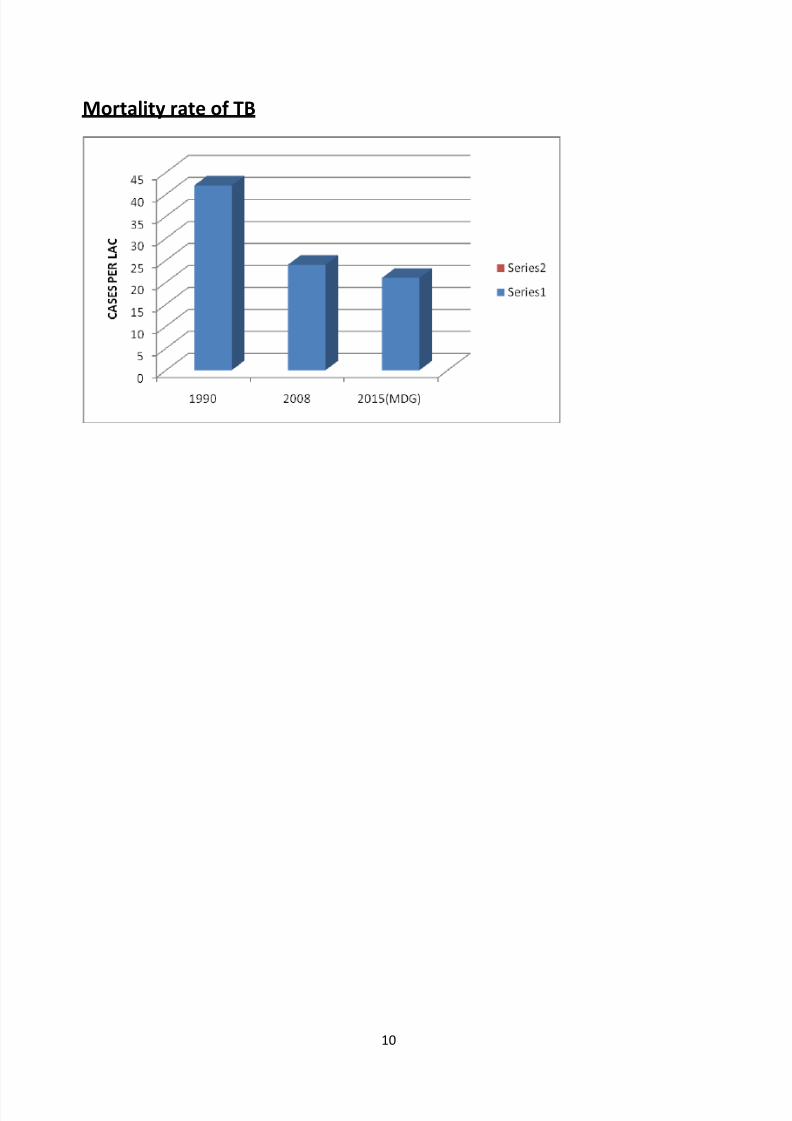
PROGRESS TOWARDS MDG INDICATOR 23
Prevalence rate of TB
8/4/2019 Global Burden of Tb
http://slidepdf.com/reader/full/global-burden-of-tb 10/79
10
Mortality rate of TB
8/4/2019 Global Burden of Tb
http://slidepdf.com/reader/full/global-burden-of-tb 11/79
11
The revised National TB control program (RNTCP) based oninternationally recommendations Directly Observed Treatment Short
Course (DOTS) Strategy was launched in 1997 and was expanded
across the country in a phased manner with support from the World
Bank and other development partners.
The objectives of the program are to :
a) To achieve and maintain cure rate of at least 85% among New
Sputum positive patients.
b) To achieve and maintain case detection at least 70% of the
estimated NSP cases in the community.
The only effective means by which 85% cure rate or more has been
shown to be achieved able on a programme basis is by application of
the DOTS strategy.
DOTS is a systematic strategy which has 5 components:-
1. Political and administrative commitment.
2. Good quality diagnoses by sputum smear microscopy.
3. Uninterrupted supply of good quality drugs.
4. Directly observed treatment.
5.Systematic accountability
8/4/2019 Global Burden of Tb
http://slidepdf.com/reader/full/global-burden-of-tb 12/79
12
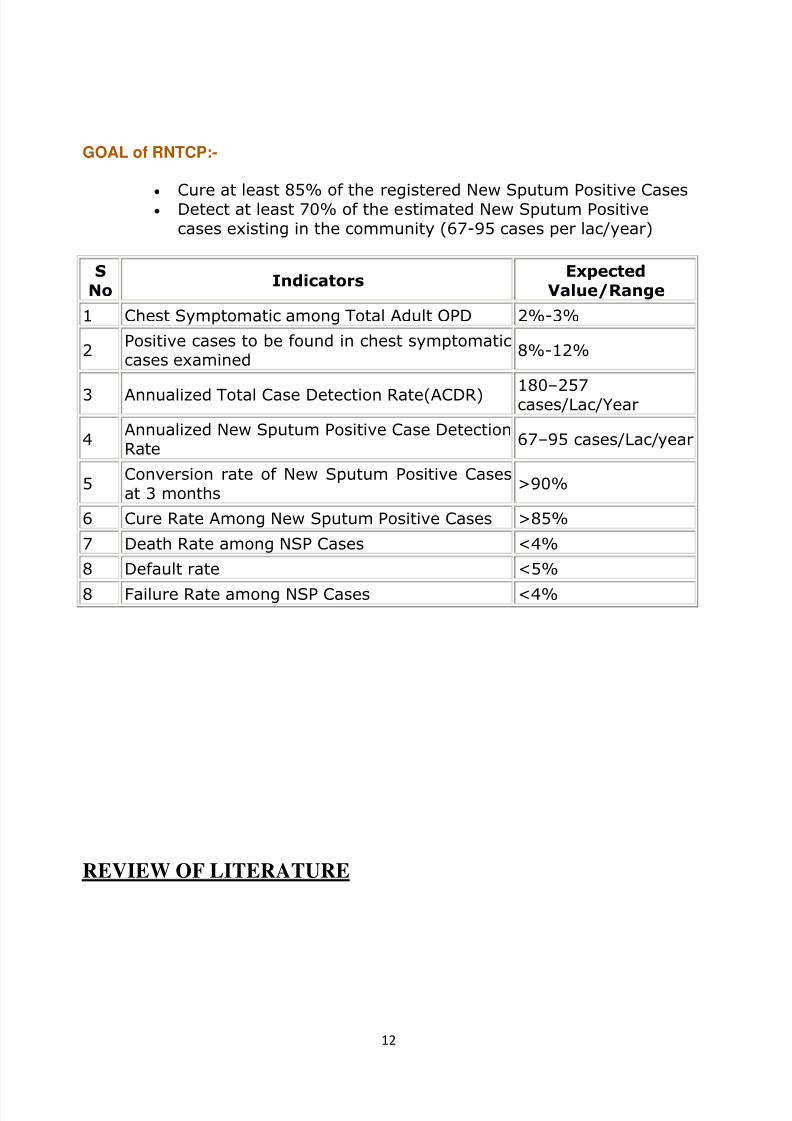
GOAL of RNTCP:-
Cure at least 85% of the registered New Sputum Positive Cases Detect at least 70% of the estimated New Sputum Positive
cases existing in the community (67-95 cases per lac/year)
S
NoIndicators
Expected
Value/Range
1 Chest Symptomatic among Total Adult OPD 2%-3%
2Positive cases to be found in chest symptomaticcases examined
8%-12%
3 Annualized Total Case Detection Rate(ACDR) 180–
257cases/Lac/Year
4Annualized New Sputum Positive Case DetectionRate
67–95 cases/Lac/year
5Conversion rate of New Sputum Positive Casesat 3 months
>90%
6 Cure Rate Among New Sputum Positive Cases >85%
7 Death Rate among NSP Cases <4%
8 Default rate <5%
8 Failure Rate among NSP Cases <4%
REVIEW OF LITERATURE
8/4/2019 Global Burden of Tb
http://slidepdf.com/reader/full/global-burden-of-tb 13/79
13
Tuberculosis (TB) is a serious global health threat, infecting more than 8 millionpeople with the active form of the disease and killing almost 2 million people eachyear. TB control and treatment has become a growing concern in developingcountries, particularly in India, where more than 20 percent of new TB cases
occur annually (World Health Organization, 2005). The public health sector of India is ill equipped to deal with this burden, having a shortage of functioningpublic health infrastructure (Bajpai and Goyal, 2004). This shortage leads tofurther economic and health consequences for those infected with TB as theyoften go into debt to seek treatment from the ill-regulated private sector; they usethe private sector as an alternative to seeking care from the public sector, which isoften perceived to be of poor quality (Bajpai and Goyal, 2004; Gupta,2005;Rajeswari et al., 1999).
Previous national TB control programs in place in India since the advent of drugsto treat the disease in the 1960s were proven inefficient and ineffective at properlydetecting and treating TB.Globally, national governments and international aidorganizations have joined forces to combat this epidemic by implementingfunctioning public health care programs using the Directly Observed Treatment,Short-Course (DOTS) strategy. In India, this effort has taken the form of theRevised National Tuberculosis Control Programme (RNTCP), one of the twolargest programs of its kind in the world both in terms of population coverage andnumber of patients treated (World Health Organization, 2005). The RNTCP, firsttested at a pilot level in 1993, was implemented in almost all districts of India
through the existing public health infrastructure by 2005 (Agarwal and Chauhan2005). Financed primarily as a centrally funded (with assistance from externalloans and grant aid) disease control program, the RNTCP also requires stateinitiative and inputs for its implementation. The program is implemented at thedistrict level, which is the lowest level of administrative division in India.
The need for increased TB control in India is apparent, as evidenced by the factthat there are almost 2 million new cases of active TB each year in India alone(World Health Organization, 2005). The potential economic benefits of
implementing a well functioning DOTS program in India have been estimated at$750 million (in 1993-1994 prices) annually (Dholakia and Almeida, 1996).
The primary mechanism currently in place under WHO guidelines for the globalcontrol of TB is the worldwide implementation of functioning DOTS programs.DOTS, originally an acronym for “directly observed therapy, short-course,” is
now used to describe a broader WHO public health strategy for TB control(Onyebujoh et al., 2005).
8/4/2019 Global Burden of Tb
http://slidepdf.com/reader/full/global-burden-of-tb 14/79
14
There are five aspects that comprise the DOTS strategy: “sustained political
commitment; access to quality assured TB sputum microscopy; standardizedshort-course chemotherapy for all cases of TB under proper case managementconditions, including direct observation of treatment; uninterrupted supply of
quality-assured drugs; [and a] recording and reporting system enabling outcomeassessment of all patients and assessment of overall programme performance”
(World Health Organization, 2003). The DOTS strategy requires the use of sputum smear microscopy for the diagnosis of pulmonary TB (Global Alliance forTB Drug Development, 2001). Treatment programs are given under intermittentconditions (preferably three times per week) and must be directly observed by ahealth care provider or trained community member (World Health Organization,2003).
The standard treatment regimen is for a duration of six months and costs as littleas $11-$17 in developing nations (World Health Organization, 2005a). DOTS hasbeen shown to be an extremely cost-effective treatment strategy; some studiesclaim that DOTS is the most cost-effective of all health interventions available.Others indicate that it costs as little as $1-$4 per discounted year of life saved(Ahlburg, 2000). In India, „conservative‟ estimates show that the potential
tangible benefits of DOTS implementation are on the order of US$750 million peryear (Dholakia and Almeida,1996).
Strict supervision and monitoring is very important component in RNTCP. A
study on effectiveness of DOTS on Tuberculosis patients treated underRNTCP(A.Mishra and S.Mishra NTI Bangalore 2007) showed that higher curerate and conversion rates were achieved due to concrete efforts in the form of strict supervision and monitoring along with motivation of cases health and non-health personnel.
An evaluation of bacteriological diagnosis of smear positive pulmonarytuberculosis under programme condition in three districts in the context of DOTSimplementation was done by Paranasivam, CN Narang(Indian journal of TB
2006) The study revealed an unacceptably high level of false positive in sputumsmear microscopy in Wardha district. This could be attributed to the absence of systematic and intensive trainings in smear examination consequent to the nonimplementation of the DOTS strategy in this district and a high standard of trainings offered in RNTCP.
Another study by Gopi PG and Chander sekaran (Indian journal 2006) showed that cure andconversion rates were linearly associated with initial sputum smear grading. High default anddeath rates were responsible for low cure and conversion. The proportion of patients who
required extension of treatment and those who had an unfavourable treatment outcome weresignificantly higher among patients with 3+ initial smear grading. This reiterates the need to
8/4/2019 Global Burden of Tb
http://slidepdf.com/reader/full/global-burden-of-tb 15/79
15
pay more attention in motivating these patients to return to regular treatment and sustainedcommitment in the control of Tuberculosis .
The economic burden of TB is especially high due to the number of people
infected and the fact that more than 75 percent of TB morbidity and mortalityoccurs in the most economically active segment of the population, those between15 and 54 years of age (Ahlburg, 2000). Additionally, there is a vicious cyclebetween poverty and TB disease. The poor are more likely to contract TB due tocrowded living conditions. The probability of infection as well as the probabilityof developing active TB from this infection is correlated with malnutrition,crowding, poor sanitation, and poor air circulation; these factors are all associatedwith poverty. Those who develop active TB are then more likely to fall into orremain in poverty due to the economic costs of the illness. There is inadequatediagnosis and treatment among the poor, which leads to more ill-health and death,which ultimately increases poverty. Although TB is not exclusively a disease of the poor, the poor are less likely to seek and receive quality care, and are two tothree times more likely to self-medicate than higher income groups. This lack of adequate treatment aggravates the health and economic effects of the disease(Ahlburg, 2000).The health status of the population is particularly important in India, where manypeople earn their living through physical power. Disease and poor health can pushpeople into extreme poverty, making it impossible for them to pull themselves outof this state1 (Bajpai and Goyal, 2004). Some studies indicate that a third of those who had to
borrow or sell assets to meet health care costs fell below the poverty line, andthese studies suggest that out of pocket medical costs may push as much as 2.2percent of the population below the poverty line each year (Gupta, 2005). Muchof India‟s disease burden is comprised of infant and maternal morbidity andmortality, infectious diseases, and nutritional deficiencies. Many of theseproblems could be severely reduced through the use of low cost interventions andprevention undertaken by the public health structure of the government (Bajpaiand Goyal, 2004).
In India, there is a large public health care system, which consists of the provision of carethrough a network of sub-centers, primary health care centers (PHC), community health centers(CHC), family welfare centers (FWC), and district hospitals. Coverage by government health
services varies widely across the states of India, although almost all states were still inadequateaccording to the specific guidelines set by the Indian government. In addition to the lack of physical infrastructure, there is a severe lack of qualified staff in the health centers. This is aproblem particularly in rural areas, where staff recruitment is a serious problem (Bajpai and
Goyal, 2004). This leads to health services being severely skewed towards urban areas(Seshadri, 2003). These shortages in
the public health care system disproportionately affect the poor, who are thepredominant users of primary health care services. The absence of adequate public
8/4/2019 Global Burden of Tb
http://slidepdf.com/reader/full/global-burden-of-tb 16/79
16
services means that many people either entirely do without medical care or seek expensive and unregulated care in the private sector. Spending in the private
sector accounts for almost eighty percent of expenditure on health (Bajpai andGoyal, 2004). Many of the problems with public health services are caused by
inadequate funding by the central and state governments, whose expenditure onhealth (combined) accounts for three percent of government spending, or less thanone percent of India‟s GDP (Mahal et al., 2002).
Governments of other developing nations spend about three percent of their GDPon 14 health, while governments of developed nations spend about five percent of their GDPs (Bajpai and Goyal, 2004). In India, government spending on health is
a responsibility of the state and national governments.
Rationale --
The purpose of the study is to assess the extent of the objectives of DOTS being
achieved. Since RNTCP is an integrated programme, the key challange is to
balance the urgent need for rapid expansion of the programme with the equally
important need to ensure quality of implementation.
There could be situation where RNTCP guidelines may get diluted at
some places as already observed in various studies, which may lead to problemsand negative influences on the outcome of the programme . Being such a large
8/4/2019 Global Burden of Tb
http://slidepdf.com/reader/full/global-burden-of-tb 17/79
17
scale programme, there is need for reliable information regarding strengths and
weeknesses in the implementation of DOTS both at micro and macro levels, so as
to identify areas requiring improvement. It is not enough to view the programme
from providers perspective only ,but it is equally important to consider views and
experiences of the patients under going treatment .taking into consideration the
facts above, a need is felt to review the implementation of RNTCP-DOTS strategy.
The present study is an attempt to undertake review of the programme of the
RNTCP at the micro level, so as to identify areas requiring strengthening and
make suitable recommendations in order to achieve the desired goals of the
programme.
General Objective –
To study the organisation, implementation and utilization of DOTS in Jammu
district.
Specific Objectives –
To describe infrastructure facilities and resources available for RNTCP-
DOTS in Jammu District. To study providers perception regarding DOTS.
To analyse the implementation and achievements of DOTS at various levels
in the district
To ascertain the extent of satisfaction with services provided and problems
if any among patients availing treatment under RNTCP.
To make necessary recommendations for the improvement of the
programme.
MATERIALS AND METHODS:
The details of the methodology adopted for the study is given below:
1. Study design- A descriptive study design was used in the study.
2. Study Area-
8/4/2019 Global Burden of Tb
http://slidepdf.com/reader/full/global-burden-of-tb 18/79
18
The study on RNTCP-DOTS Strategy was conducted in DTC Jammu and its
TUs, DMCs and DOT Centres.
3. Study population-
a. Service providers – For obtaining information on operational aspects of
the programme and problems faced in implementation , staff members
involved in diagnosis and treatment of TB patients at DTC, TUs, DMCs
and DOT Centres.
Among services providers at these centres the following staff were
included: DTO , MO , STS, STLS, TBHV, LTs.
b. Beneficiaries- To ascertain the extent of satisfaction and problemsfaced in availing treatment for TB,beneficiaries were included in the
study from DTC and DOT centres.
Sampling procedure and Sampling size:-
Jammu district has 4 Tuberculosis units and 18 DMCs. Selection of DMCs
was done as per the RNTCP guidelines for the internal evaluation of the
district. A total of 5 DMCs and 10 DOT Centres were selected.
A. Service providers- with regard to service providers all staff directly
involved in RNTCP at DTC,TU,DMC and DOT centres were included-
1. DTO -1
2. MO – 10
3. STS - 4
4. STLS -3
5. TBHV-4
6. LTs - 8
7. DOT Providers- 10
8. ASHA - 10
8/4/2019 Global Burden of Tb
http://slidepdf.com/reader/full/global-burden-of-tb 19/79
19
B. TB patients availing treatment – The DTC Jammu has four TUs from
which proportionate samples of patients was taken. Both pulmonary
and EP TB cases were included in the present studies. The reference
period from which the patient were selected for the study was 9 months
which equivalent to the longest period for which anti TB drugs can be
prescribed under RNTCP in any category.
C. Patients and their treatment cards- in order to ascertain treatment out
come, treatment cards of TB patients were included.
D. Observation- Observation was also made to see the selected activities
under the programme. For this all TUs , 5 DMCs out of 18 DMCs and 10
DOT centres were included. Activities like sputum examination fordiagnosis, DOTS administration , health education , waste management
,record maintenance etc being performed by health workers was
observed.
Data Collection technique – The following techniques for data collection were
used.
Secondary data – Study of Records and Registers-
TB register of each TU
Lab register of each DMC
Treatment cards
Primary data – 1. Interview of TB Patients – A total of 50 patients were
interviewed using semi structured interview schedule for collecting information
on various aspects like accessibility to DOT centres , experiences while availingtreatment , extend of satisfaction with treatment etc.
2. Interview of service providers – All the health providers who are working
under RNTCP i.e a total of 50 were interviewed using semi structured interview
schedule. Information collected included duties and responsibilities under RNTCP
, problem faced , suggestions for improvement of the programme.
3. Observation of infrastructure and facilities - Observation check list was used
to access the physical infrastructure , facilities and supplies at various DOT
8/4/2019 Global Burden of Tb
http://slidepdf.com/reader/full/global-burden-of-tb 20/79
20
centres and DMCs. This included waiting area for patients availability of
medicines , water , electricity , lab facilities , disinfection of bio medical waste
etc.
Tools for data collection –
Interview schedule to elicit the information from TB patients.
(Annexure......)
Interview schedule for staff (Annexure.....)
Observation check list for DMC (Annexure.....)
Observation check list for DOT centre (Annexure.....)
Observation check list for TU drug store (Annexure.....)
OBSERVATIONS AND FINDINGS-
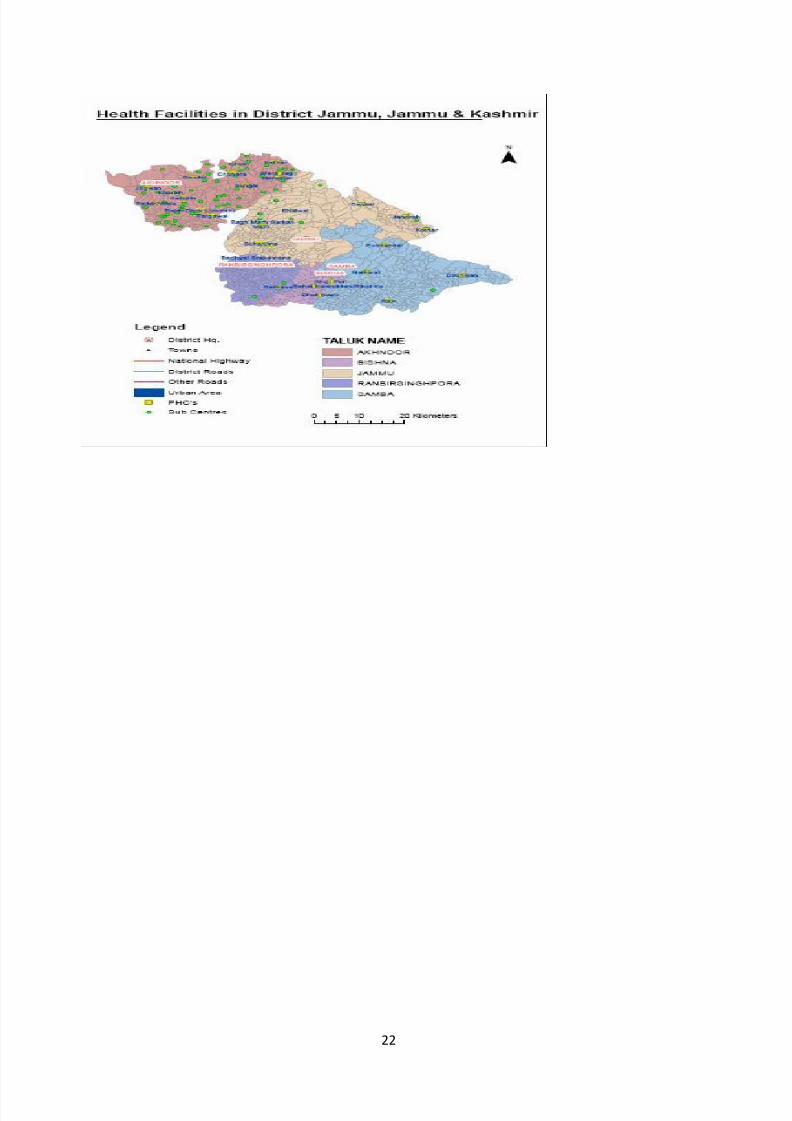
RNTCP in Jammu District-
Jammu District is one of the 22 districts of the state of Jammu &
Kashmir. In the north, Jammu and Udhampur district
bound the district; district Samba in the East, while international
8/4/2019 Global Burden of Tb
http://slidepdf.com/reader/full/global-burden-of-tb 21/79
21
borders are in south and west. Jammu city is situated on the banks of
river Tawi and is the winter capital of J&K state.
About 1/4th
part of the district is hilly. Most part of Dansal and
Purmandal Blocks are hilly while larger part of Akhnoor is hilly. Forest
covers about a third of the area of District. Consequently, Jammu
consists of difficult and inaccessible areas.
Samba is a newly formed district of Jammu province `but from RNTCP
point of view, it is still working as Tuberculosis Unit under DTC
Jammu.
RNTCP in Jammu District was implemented on 8th
April 2004.It is a truly
integrated programme, implemented through DTC, TUs, DMCs, DOT Centres.
DOTS is the most cost effective way to deal with TB problem through wide
spread network for an improved case finding activity coupled with the facility for
the treatment of cases found as near to their homes as possible.
The WHO’s Directly Observed Treatment – Short Course Strategy consists of
measures to ensure a complete cure and to prevent development and drugresistance. Health workers are trained to directly observe TB patients ingest the
anti TB drugs thrice in a week. DOTS also involves the establishment of case
detection and monitoring system.
8/4/2019 Global Burden of Tb
http://slidepdf.com/reader/full/global-burden-of-tb 22/79
22
8/4/2019 Global Burden of Tb
http://slidepdf.com/reader/full/global-burden-of-tb 23/79
23
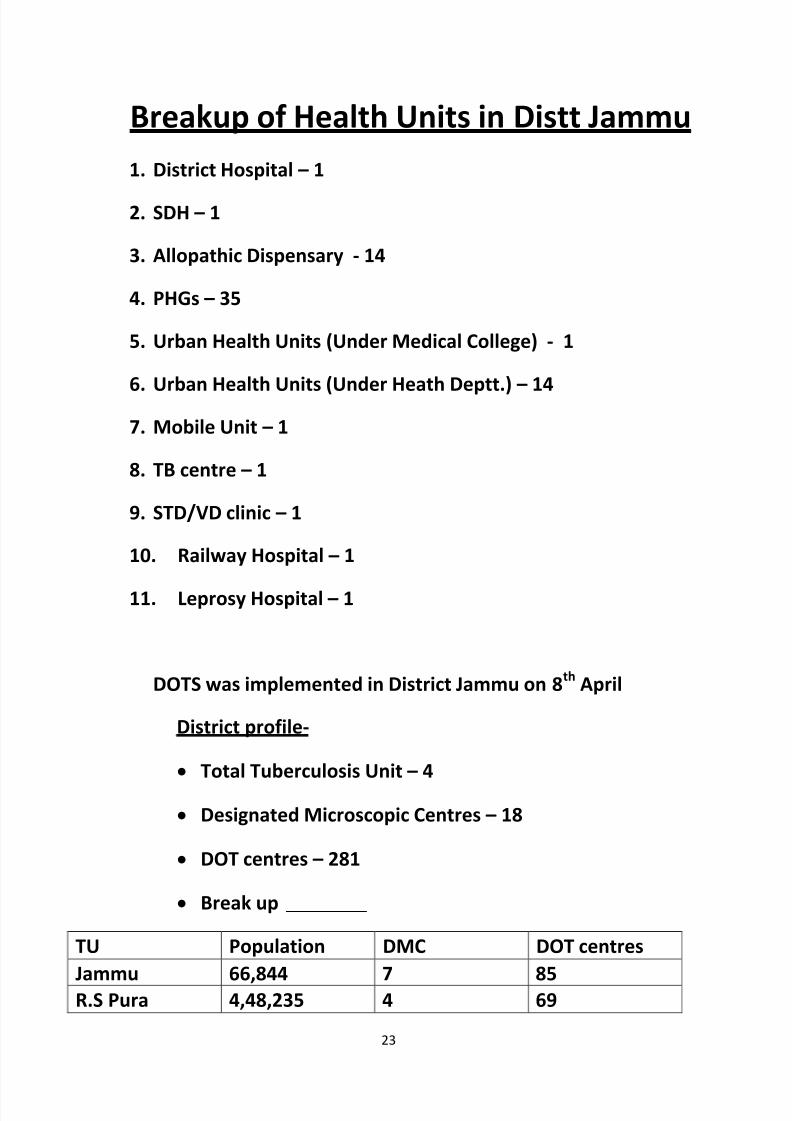
Breakup of Health Units in Distt Jammu
1. District Hospital – 1
2. SDH – 1
3. Allopathic Dispensary - 14
4. PHGs – 35
5. Urban Health Units (Under Medical College) - 1
6. Urban Health Units (Under Heath Deptt.) – 14
7. Mobile Unit – 1
8. TB centre – 1
9. STD/VD clinic – 1
10. Railway Hospital – 1
11. Leprosy Hospital – 1
DOTS was implemented in District Jammu on 8th
April
District profile-
Total Tuberculosis Unit – 4
Designated Microscopic Centres – 18
DOT centres – 281
Break up
TU Population DMC DOT centres
Jammu 66,844 7 85R.S Pura 4,48,235 4 69
8/4/2019 Global Burden of Tb
http://slidepdf.com/reader/full/global-burden-of-tb 24/79
24
Akhnoor 3,71,470 3 75
Samba 3,19,212 4 52
Total 18,05761 18 281
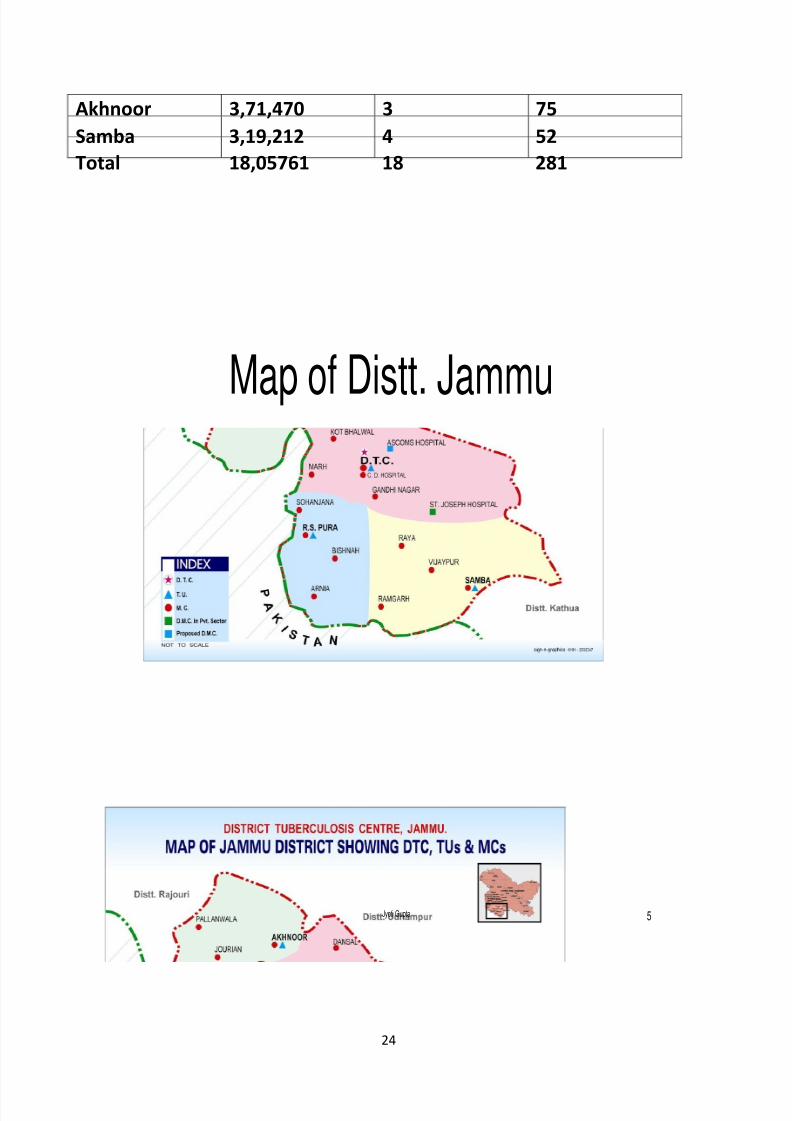
Jyoti Gupta 5
Map of Distt. Jammu
8/4/2019 Global Burden of Tb
http://slidepdf.com/reader/full/global-burden-of-tb 25/79
25
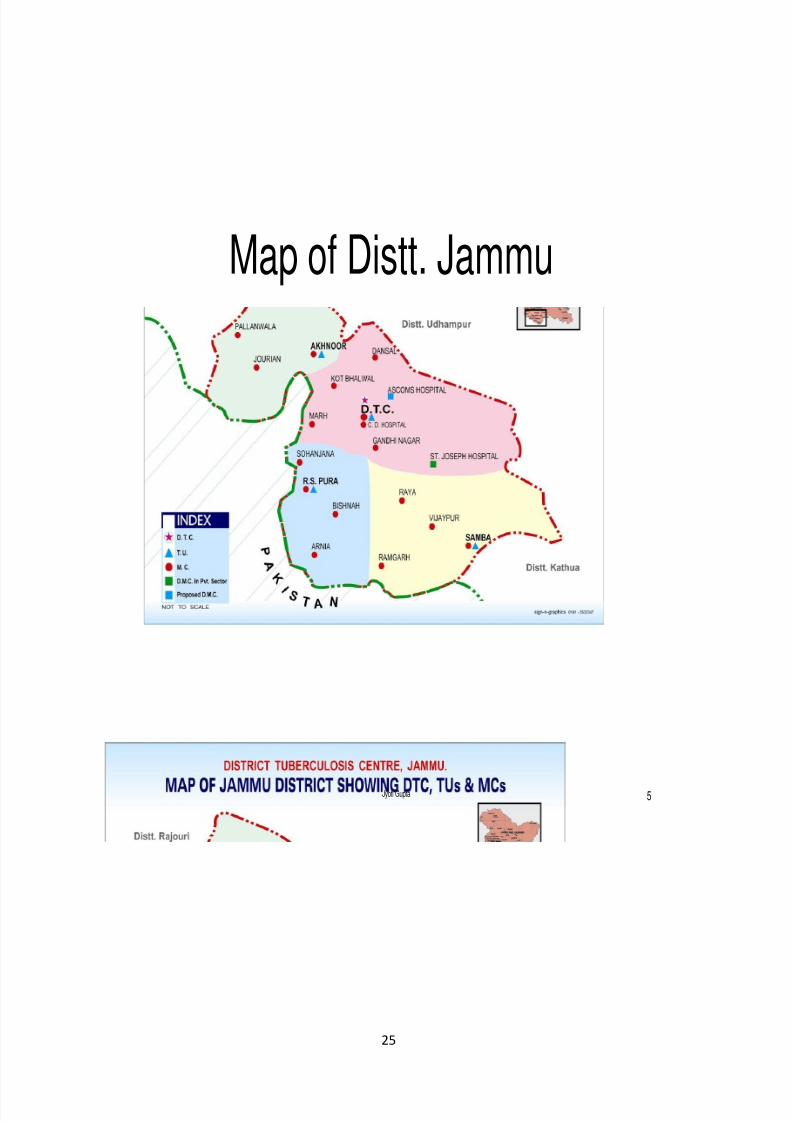
Jyoti Gupta 5
Map of Distt. Jammu
8/4/2019 Global Burden of Tb
http://slidepdf.com/reader/full/global-burden-of-tb 26/79
26
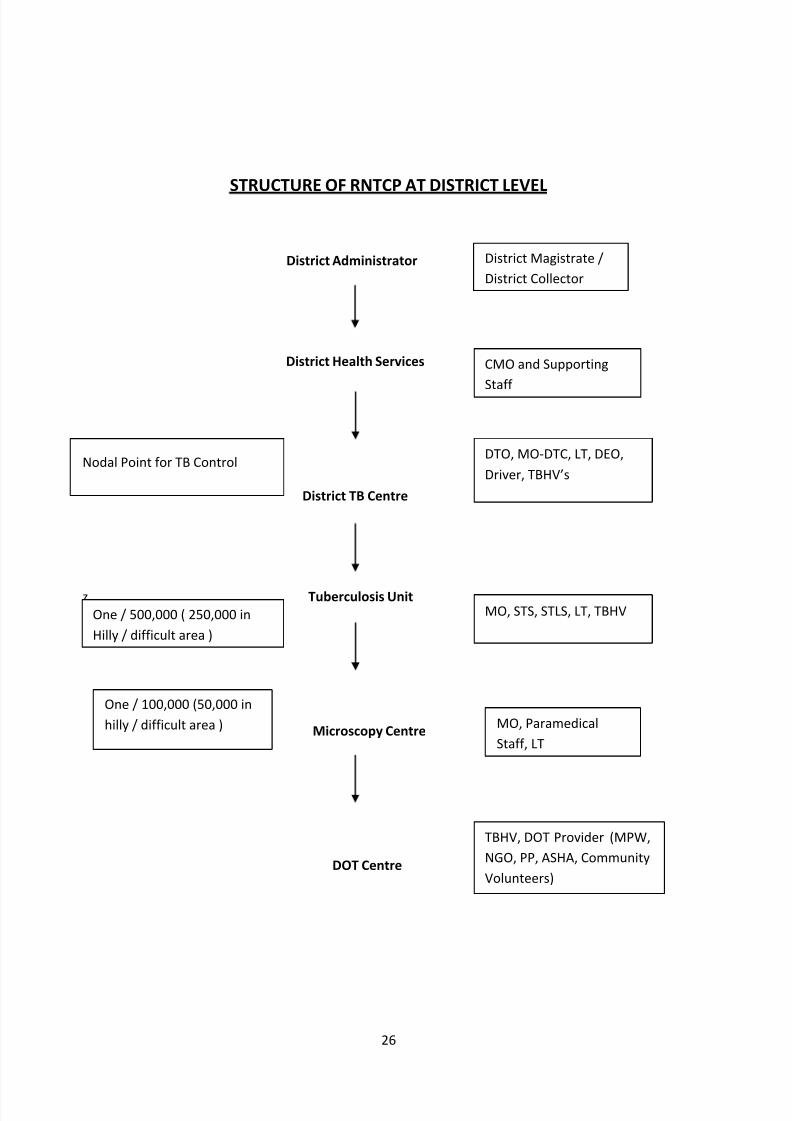
STRUCTURE OF RNTCP AT DISTRICT LEVEL
District Administrator
District Health Services
Nodal Point for TB Control
District TB Centre
z Tuberculosis Unit
Microscopy Centre
DOT Centre
One / 500,000 ( 250,000 in
Hilly / difficult area )
One / 100,000 (50,000 in
hilly / difficult area )
CMO and Supporting
Staff
DTO, MO-DTC, LT, DEO,
Driver, TBHV’s
MO, STS, STLS, LT, TBHV
MO, Paramedical
Staff, LT
TBHV, DOT Provider (MPW,
NGO, PP, ASHA, Community
Volunteers)
District Magistrate /
District Collector
8/4/2019 Global Burden of Tb
http://slidepdf.com/reader/full/global-burden-of-tb 27/79
27
ORGANISATION STRUCTURE
DISTRICT TUBERCULOSIS CENTRE JAMMU
District Tuberculosis Centre Jammu is the Nodal point for TB Control activities in
the district. The building of DTC is located in Chest Disease Hospital Complex,
near Govt. Medical College Jammu. The DTO has the overall responsibility of
physical and financial management of RNTCP at the district level. The DTO is also
responsible for involvement of other sectors in RNTCP and is assisted by one MO.
The post of the second MO is lying vacant in DTC.
MO in DTC is looking after the OPD. She is sending the Chest Symptomatics to
DMC which is a part of DTC only. DTC also has a DOT Centre where patients are
given medicines under direct supervisions by DOT Providers ( Jr. Staff Nurse and
FMPHW). Drug days for direct observation treatment are Monday, Wednesday
and Friday.
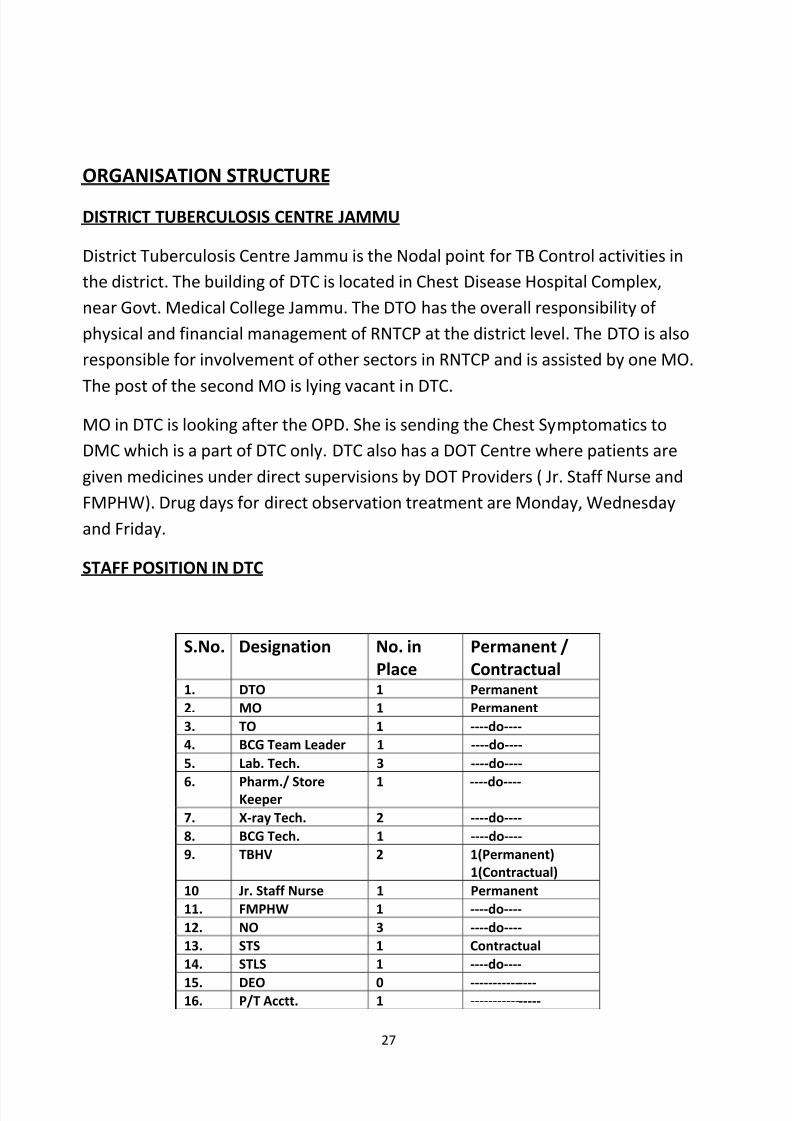
STAFF POSITION IN DTC
S.No. Designation No. in
Place
Permanent /
Contractual1. DTO 1 Permanent
2. MO 1 Permanent
3. TO 1 ----do----
4. BCG Team Leader 1 ----do----
5. Lab. Tech. 3 ----do----
6. Pharm./ StoreKeeper
1 ----do----
7. X-ray Tech. 2 ----do----
8. BCG Tech. 1 ----do----
9. TBHV 2 1(Permanent)
1(Contractual)
10 Jr. Staff Nurse 1 Permanent
11. FMPHW 1 ----do----
12. NO 3 ----do----
13. STS 1 Contractual
14. STLS 1 ----do----
15. DEO 0 ---------------16. P/T Acctt. 1 ----------------
8/4/2019 Global Burden of Tb
http://slidepdf.com/reader/full/global-burden-of-tb 28/79
28
17. SA 1 Permanent
18. Accountant 1 ----do----
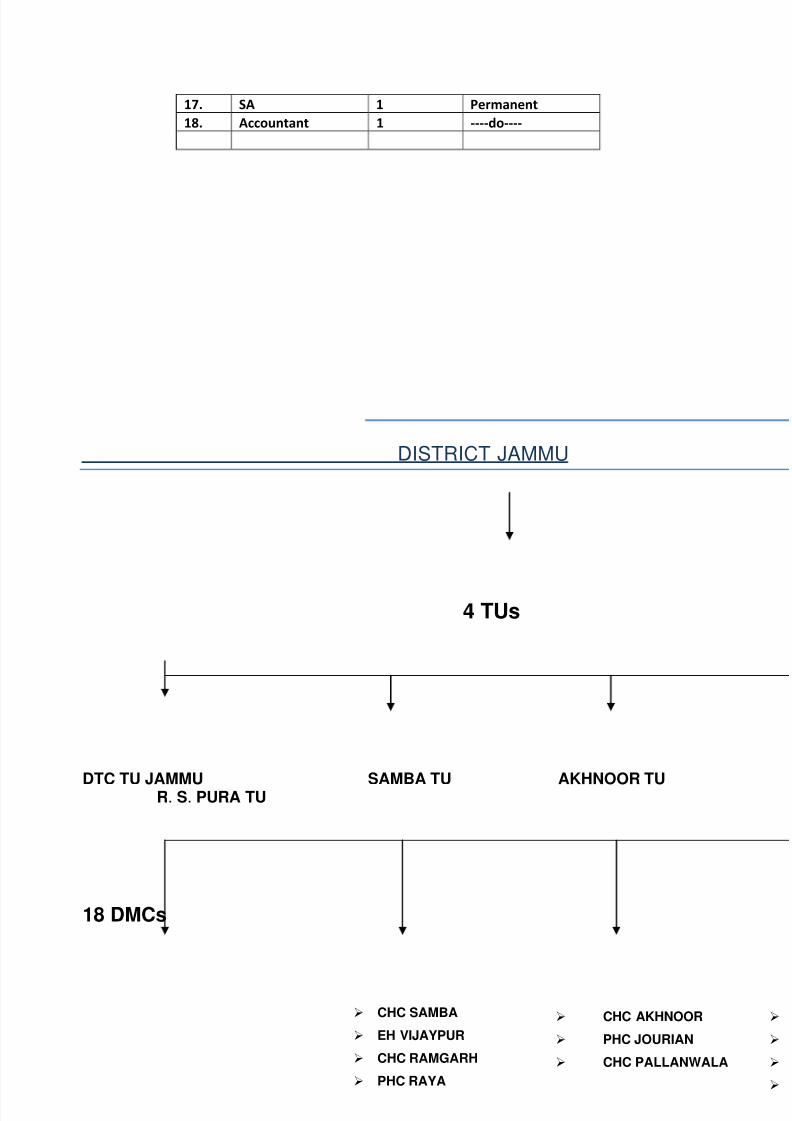
DISTRICT JAMMU
4 TUs
DTC TU JAMMU SAMBA TU AKHNOOR TU R. S. PURA TU
18 DMCs
CHC SAMBA
EH VIJAYPUR
CHC RAMGARH
PHC RAYA
CHC AKHNOOR
PHC JOURIAN
CHC PALLANWALA
8/4/2019 Global Burden of Tb
http://slidepdf.com/reader/full/global-burden-of-tb 29/79
29
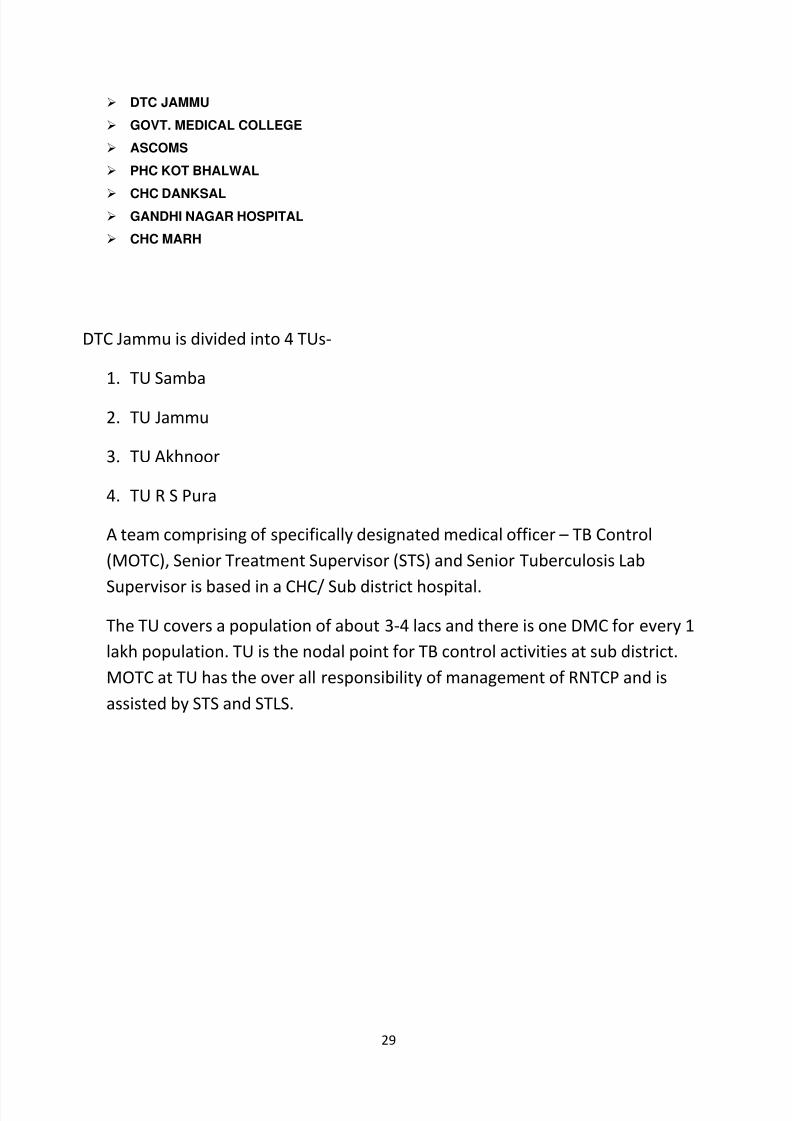
DTC JAMMU
GOVT. MEDICAL COLLEGE
ASCOMS
PHC KOT BHALWAL
CHC DANKSAL GANDHI NAGAR HOSPITAL
CHC MARH
DTC Jammu is divided into 4 TUs-
1. TU Samba
2. TU Jammu
3. TU Akhnoor
4. TU R S Pura
A team comprising of specifically designated medical officer – TB Control
(MOTC), Senior Treatment Supervisor (STS) and Senior Tuberculosis Lab
Supervisor is based in a CHC/ Sub district hospital.
The TU covers a population of about 3-4 lacs and there is one DMC for every 1
lakh population. TU is the nodal point for TB control activities at sub district.
MOTC at TU has the over all responsibility of management of RNTCP and is
assisted by STS and STLS.
8/4/2019 Global Burden of Tb
http://slidepdf.com/reader/full/global-burden-of-tb 30/79
30
OPERATIONAL ASPECTS OF RNTCP – DOTS
1. Case detection and diagnosis
Sputum microscopy is the primary tool for diagnosing and monitoring of TBpatients. Sputum microscopy is done only in Designated Microscopy Centres
(DMCs).
In district Jammu there are 18 DMCs. Persons with cough for
two weeks or more, with or without other symptoms suggested of TB are promptly
identified as pulmonary TB suspects and are subjected to sputum smear
microscopy for AFB By the medical officers.
In all the DMCs there is a full time trained lab technician who
fills up the lab forms and gives sputum containers to patients after instructing himhow to cough out the sputum. He collects on the spot specimen and gives another
container for early morning sample. After collection of sputum staining is done and
a report is prepared with proper grading. All the sputum positive results are
written in red ink in the lab register. In all the DMCs all the essential consumables
including binocular microscope is available. Facilities for running water for the
staining purpose are also present in all the DMCs. At the end of every month a
summary abstract is completed by every LT.
In health centres other than DMCs there is no provision for collection of sputum.Also no sputum slides are being made in PHIs. Patients from these centres are
referred to nearest DMC.
2. Categorisation , Registration and initiation of treatment –
If the sputum smear examination is positive for
AFB , the patients is referred to MO for categorisation of disease (into CAT-1,2 and 3) and
TBHV makes home visit to confirm the address of the patient. If the patient is resident of the
area he/she is started on anti TB treatment after assigning registration number in TB register
of that TU, otherwise patient is referred to respective DOT centre for further case
management.
The anti TB treatment started after proper health education and motivation. Sputum
negative patients are given a course of antibiotic and then sputum examination is repeated. If
he does not improve he is referred for chest x ray and other investigations for confirmation of
diagnosis.
8/4/2019 Global Burden of Tb
http://slidepdf.com/reader/full/global-burden-of-tb 31/79
31
3. Treatment regimen followed -
CAT- I : New sputum positive , seriously ill sputum negative and seriously ill extra
pulmonary.
2 months-RHZE , 4 months RH (thrice in a week).
CAT-II : Retreatment cases
2 months SRHZE , 1 month RHZE , 5 months RHE (thrice in a week)
CAT- III : Non seriously ill sputum negative and EP
2 months RHZ , 4 months RH (thrice in a week)
R- Rifampicin
H- Isoniazide
E-Ethambutol
S-Streptomycin
Z- Pyrazinamide
( GOI 1997 )
All drugs are administered trice weekly for a period of 2/3 months. Patient is asked to
swallow the medicines in front of the health worker in Intensive phase. After this repeat
sputum examination is done, if found negative continuation phases started. In this phase
drugs are provided on weekly basis, the first dose of which is directly supervised. All the
entries are made and patient’s record is maintained by TBHV/DOT provider at DOT centre
which is under supervision of STS. MOTC is responsible for managing the treatment unit.
Drug Administration
During intensive phase thrice in a week patient is given medicine under direct
supervision – Monday, Wednesday and Friday. If the patient misses taking drugs on a
specific day, he can take them next day. The patient must be contacted within one day
of missing dose in intensive phase. During continuation phase the first dose of weekly
blister should be directly observed. The patient must be contacted within a week of
missing weekly collection of drugs.
8/4/2019 Global Burden of Tb
http://slidepdf.com/reader/full/global-burden-of-tb 32/79
32
Follow up-
The follow up of each patient is to be done at 2-3 months and second at 4-5 months and last at
the end of the treatment. Two sputum smears are examined each time during follow up. For
the patients who need to be transferred from one TU to another, the transfer form is filled and
patient is referred to respective areas.
4. DRUGS FOR TB TREATMENT
An uninterrupted supply of good quality Anti-TB drugs is one of the five components of DOTS
strategy. A strong procurement & logistics management with respect to drugs is essential to
strengthen every link in the drug supply chain from manufacturer to patients. There is a unique
system of providing drugs in patient wise boxes ( PWB ) which contain drugs for entire
duration of Treatment for each category of Patient. Once a patient is started on anti- TB
treatment, a box is assigned to that patient, thus ensuring that entire course is available
uninterrupted.
DRUG MANAGEMENT :
a. Selection : The essential drugs used in RNTCP are Rifampicin , Isonized , Ethambutol ,
Pyrazinamide & Streptomycin.
b. Procurement of Drugs : Procurement of anti TB drugs is done both for PWBs as well as
loose drugs. In exceptional circumstances few patients may have to be put on Non-
DOTS regimen. For such patients loose drugs need to be procured. Loose drugs are also
required for pediatric patients , adult patients with low body weight & over weight
patients. Procurement of anti TB drugs is made through independent agency appointed
by the Ministry of Health & Family Welfare, Govt. of India .
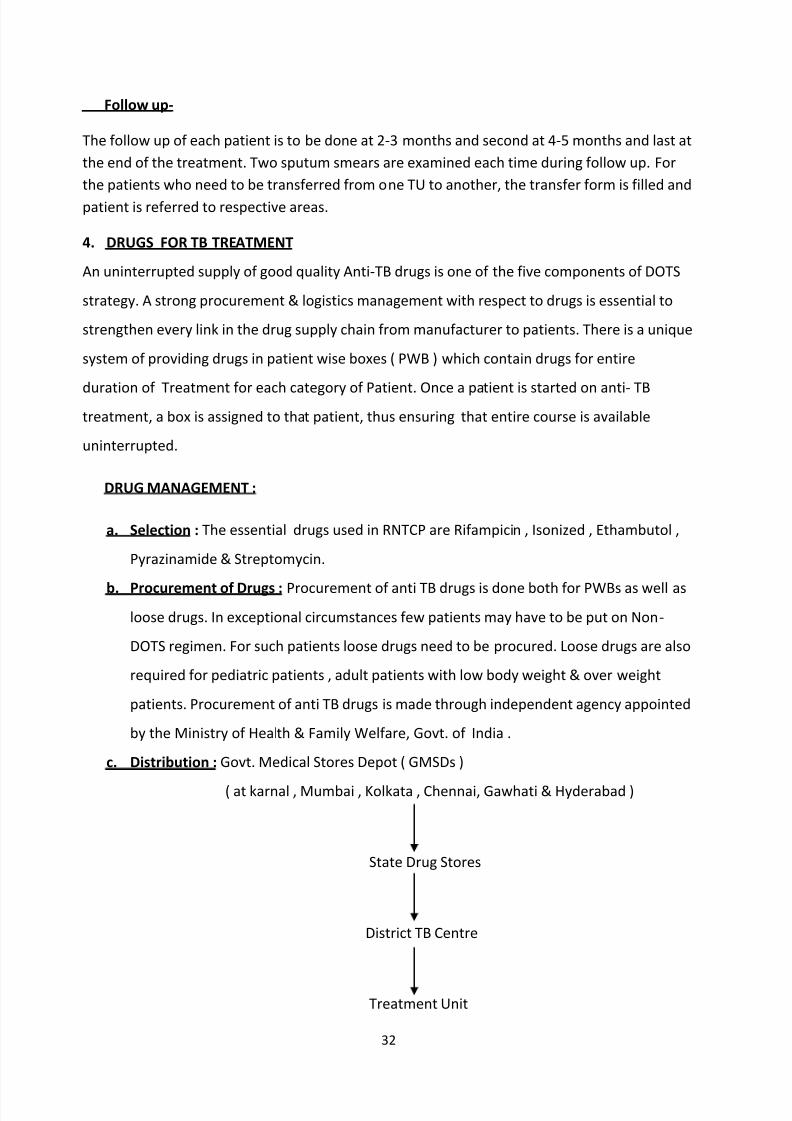
c. Distribution : Govt. Medical Stores Depot ( GMSDs )
( at karnal , Mumbai , Kolkata , Chennai, Gawhati & Hyderabad )
State Drug Stores
District TB Centre
Treatment Unit
8/4/2019 Global Burden of Tb
http://slidepdf.com/reader/full/global-burden-of-tb 33/79
33
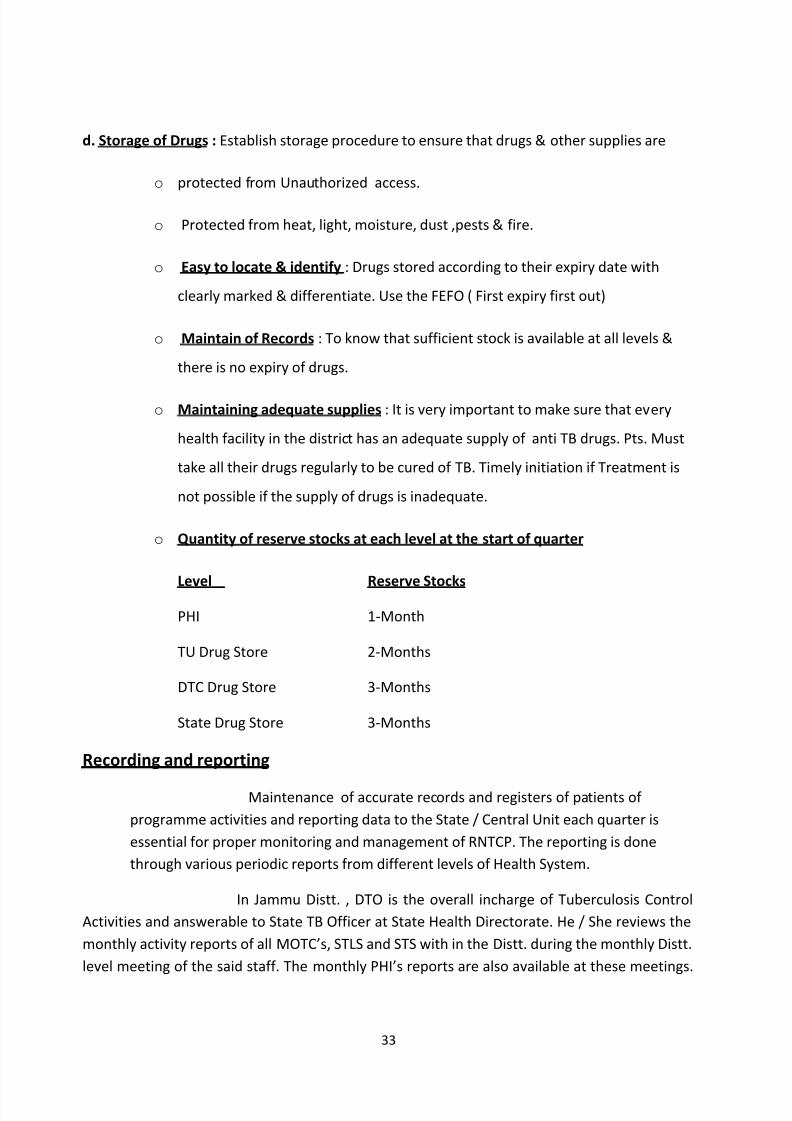
d. Storage of Drugs : Establish storage procedure to ensure that drugs & other supplies are
o protected from Unauthorized access.
o Protected from heat, light, moisture, dust ,pests & fire.
o Easy to locate & identify : Drugs stored according to their expiry date with
clearly marked & differentiate. Use the FEFO ( First expiry first out)
o Maintain of Records : To know that sufficient stock is available at all levels &
there is no expiry of drugs.
o Maintaining adequate supplies : It is very important to make sure that every
health facility in the district has an adequate supply of anti TB drugs. Pts. Must
take all their drugs regularly to be cured of TB. Timely initiation if Treatment is
not possible if the supply of drugs is inadequate.
o Quantity of reserve stocks at each level at the start of quarter
Level Reserve Stocks
PHI 1-Month
TU Drug Store 2-Months
DTC Drug Store 3-Months
State Drug Store 3-Months
Recording and reporting
Maintenance of accurate records and registers of patients of
programme activities and reporting data to the State / Central Unit each quarter is
essential for proper monitoring and management of RNTCP. The reporting is done
through various periodic reports from different levels of Health System.
In Jammu Distt. , DTO is the overall incharge of Tuberculosis Control
Activities and answerable to State TB Officer at State Health Directorate. He / She reviews the
monthly activity reports of all MOTC’s, STLS and STS with in the Distt. during the monthly Distt.
level meeting of the said staff. The monthly PHI’s reports are also available at these meetings.
8/4/2019 Global Burden of Tb
http://slidepdf.com/reader/full/global-burden-of-tb 34/79
34
The date of the review is fixed in advance. It is held on 1st
of every month. Minutes of these
meetings are also kept by DTO.
At TU level reporting and recording is done by MOTC, STS and STLS.
Tuberculosis register is kept at Sub-Distt. (TU) level in the Distt. TB treatment cards of the
patients are kept in all peripheral health units. A duplicate card is given to the peripheral
health functionaries who administer DOT. Patients keep identity card only. Monthly report is
prepared every month and submitted to DTC. Quarterly report on case finding, sputum
conversion rate of patients who are on treatment and all possible outcomes of smear positive
cases of pulmonary TB (Cured, Treatment completed, Failure, Defaulted, Died and Transferred
out) is prepared by STS. The STLS is primarily responsible for supervising all the lab. activities
including checking 100% of sputum positive slides and at least 10% of sputum negative slides.
It is the responsibility of TU to compile the DMC wise reports of sputum examination done,
sputum found positive, NSP, sputum negative, patients put on treatment, extra pulmonarycases and submit the report to DTO.
At DMC, the responsible staff are MO and LT. Tools at this level will be
referral for treatment register, patients treatment card, RNTCP lab. register and supervisor
register. MO should meet weekly all the staff involved in RNTCP. He is responsible for
compilation of monthly PHI reports and its submission to TU.DTO who compiles the report (4
copies) in respect to all TB units and sends three of them to the STO, The National Tuberculosis
Institute Bangalore and to Central TB Division, DGHS Nirman Bhawan New Delhi.
5. Supervision and monitoring –
Supervision is a systematic process for increasing the efficiency of health workers by
developing their knowledge, perfecting their skills, improving their attitude towards work
and increasing their motivationRNTCP has inherent ability to conduct regular supervision
and monitoring at all the levels- national, state, district and sub- district.
In Jammu District , District Tuberculosis Officer is the overall incharge of Tuberculosis
Control Activities and answerable to State Tuberculosis Officer at the State Health
Directorate. D.T.O. with the support of M.O. of DTC is responsible for ensuring the quality
diagnosis , treatment, logistics and reporting. She is undertaking supervisory visits to all
T.U’s and Medical Colleges in the Distt. every month and all CHC’s and PHC’s in the Distt.
every quarter. D.T.O. is provided with a govt. vehicle for purpose of supervision. She is
maintaining the Tour Diary for keeping the record of supervisory visits.
At T.U. Level , MOTC, STS, and STLS are responsible for undertaking supervisory visits to all
the PHI’s, NGO’s and PP’s. The MOTC is responsible for supervising the work of TU, STS and
STLS in addition to his / her other responsibilities. He has to submit Tour Programme at the
begining of the month to D.T.O. and maintains Tour Diary for keeping the record of his
8/4/2019 Global Burden of Tb
http://slidepdf.com/reader/full/global-burden-of-tb 35/79
35
supervisory visits. He can hire the vehicle for this activity and can claim charges as per
RNTCP guidelines from DTC.
STLS is responsible for the quality of sputum smear microscopy services provided by
DMC’s under TU. He is visiting all the DMC’s under the TU at least once in a month.
STS visits all the PHI’s at least once every month he checks whether all the sputum smear
positive patients recorded in the TB Lab. register are placed on treatment and register in
TB register. He also compares the date in the TB Lab. register with that in the TB register.
STS & STLS are provided with a motor bike under RNTCP guidelines for supervisory visits.
They also prepare Tour Programme and maintain Tour Diary every month. They also carry
supervisory checklist for this activity at DMC’s and DOT Centres.
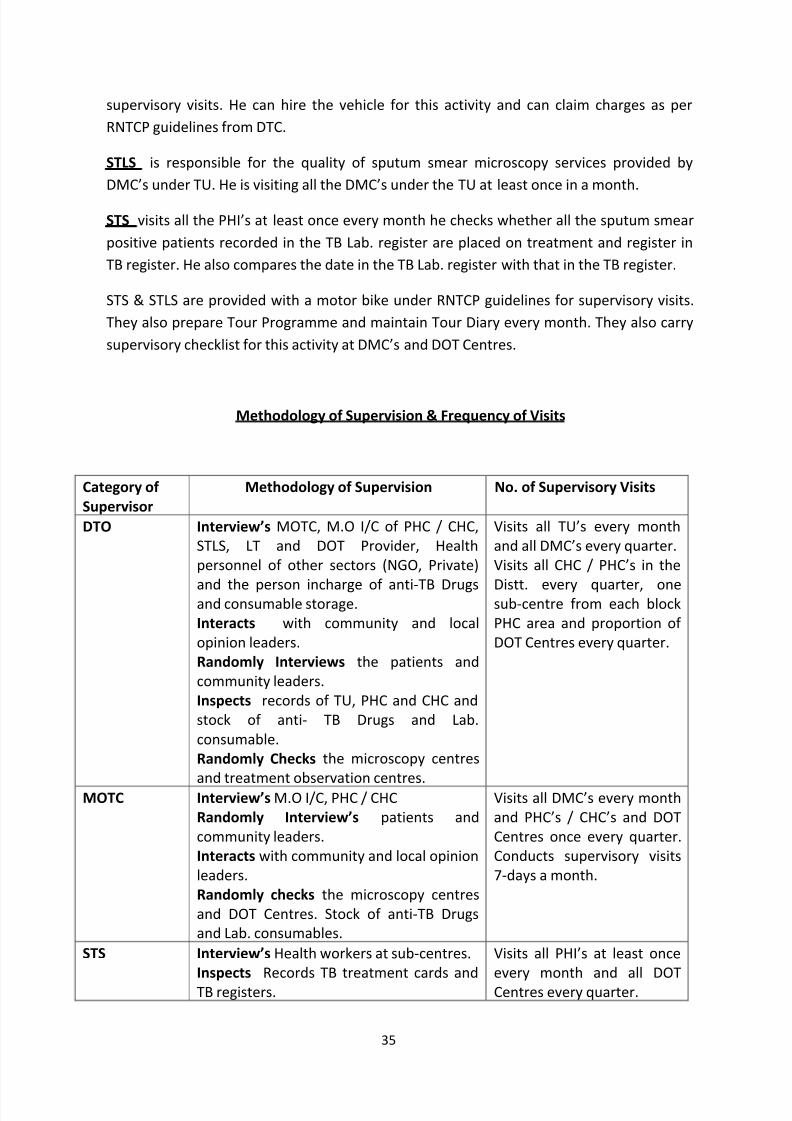
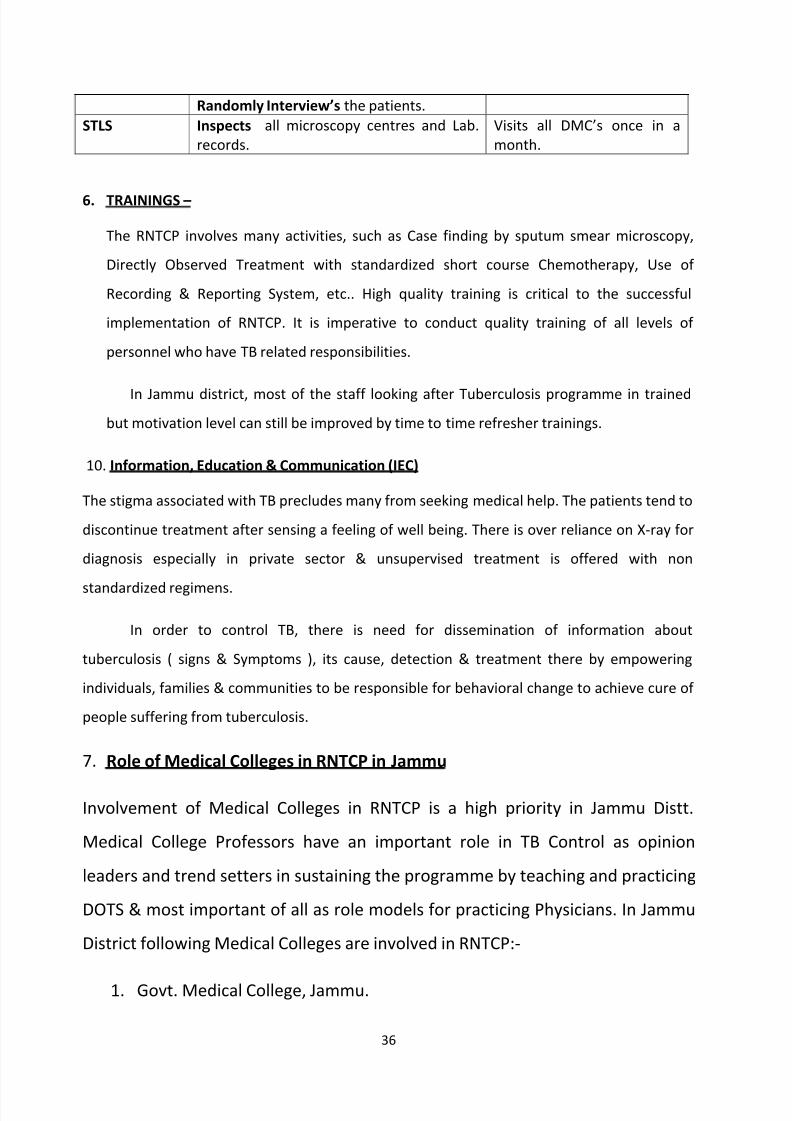
Methodology of Supervision & Frequency of Visits
Category of
Supervisor
Methodology of Supervision No. of Supervisory Visits
DTO Interview’s MOTC, M.O I/C of PHC / CHC,
STLS, LT and DOT Provider, Health
personnel of other sectors (NGO, Private)
and the person incharge of anti-TB Drugsand consumable storage.
Interacts with community and local
opinion leaders.
Randomly Interviews the patients and
community leaders.
Inspects records of TU, PHC and CHC and
stock of anti- TB Drugs and Lab.
consumable.
Randomly Checks the microscopy centres
and treatment observation centres.
Visits all TU’s every month
and all DMC’s every quarter.
Visits all CHC / PHC’s in the
Distt. every quarter, onesub-centre from each block
PHC area and proportion of
DOT Centres every quarter.
MOTC Interview’s M.O I/C, PHC / CHC
Randomly Interview’s patients and
community leaders.
Interacts with community and local opinion
leaders.
Randomly checks the microscopy centres
and DOT Centres. Stock of anti-TB Drugs
and Lab. consumables.
Visits all DMC’s every month
and PHC’s / CHC’s and DOT
Centres once every quarter.
Conducts supervisory visits
7-days a month.
STS Interview’s Health workers at sub-centres.
Inspects Records TB treatment cards and
TB registers.
Visits all PHI’s at least once
every month and all DOT
Centres every quarter.
8/4/2019 Global Burden of Tb
http://slidepdf.com/reader/full/global-burden-of-tb 36/79
36
Randomly Interview’s the patients.
STLS Inspects all microscopy centres and Lab.
records.
Visits all DMC’s once in a
month.
6. TRAININGS –
The RNTCP involves many activities, such as Case finding by sputum smear microscopy,
Directly Observed Treatment with standardized short course Chemotherapy, Use of
Recording & Reporting System, etc.. High quality training is critical to the successful
implementation of RNTCP. It is imperative to conduct quality training of all levels of
personnel who have TB related responsibilities.
In Jammu district, most of the staff looking after Tuberculosis programme in trained
but motivation level can still be improved by time to time refresher trainings.
10. Information, Education & Communication (IEC)
The stigma associated with TB precludes many from seeking medical help. The patients tend to
discontinue treatment after sensing a feeling of well being. There is over reliance on X-ray for
diagnosis especially in private sector & unsupervised treatment is offered with non
standardized regimens.
In order to control TB, there is need for dissemination of information about
tuberculosis ( signs & Symptoms ), its cause, detection & treatment there by empowering
individuals, families & communities to be responsible for behavioral change to achieve cure of
people suffering from tuberculosis.
7. Role of Medical Colleges in RNTCP in Jammu
Involvement of Medical Colleges in RNTCP is a high priority in Jammu Distt.
Medical College Professors have an important role in TB Control as opinion
leaders and trend setters in sustaining the programme by teaching and practicing
DOTS & most important of all as role models for practicing Physicians. In Jammu
District following Medical Colleges are involved in RNTCP:-
1. Govt. Medical College, Jammu.
8/4/2019 Global Burden of Tb
http://slidepdf.com/reader/full/global-burden-of-tb 37/79
37
2.Acharya Sri Chander College of Medical Sciences.
Govt. Medical College, Jammu
GMC, Jammu is playing a very important role in RNTCP. It is functioning as DMCas well as Dot centre. Since it is a tertiary level Hospital, people have lot of faith
in the medical facilities available here. It caters to both rural & urban population
in Jammu District. There is a separate Chest Diseases Hospital in Jammu city,
where all chest symptomatics prefer to come for diagnosis & treatment. Also
there are special wards for indoor patients. Patients in emergencies are referred
to CD hospital. They are admitted here & treated with prolongation pouches.
There is a well established Microscopy Centre which is performing very
well as far as sputum microscopy is concerned. A well trained team of Medical
Officer, Lab. tech., TBHV ( DOT provider ) is looking after RNTCP in CD Hospital.
Also the Chest Physician posted in CD Hospital are contributing a lot in this
programme. Above all Principal medical College who is a Chest physician. He is
running a evening chest clinic in the hospital premises to help the chest
symptomatics.
Acharya Sri Chander College Of Medical Sciences. ( ASCOMS )
ASCOMS is a private Medical college. It also has a DMC & a Treatment centre.
RNTCP team comprising of Medical Officer, Lab. Tech., Dot provider ( TBHV ) is
working there. Since the medical college is situated away from the city, the
patients generally avoid going there. Most of the Doctors in the hospital are
trained in RNTCP. Chest physicians working there are also trying their best to
improve the outputs / results.
8/4/2019 Global Burden of Tb
http://slidepdf.com/reader/full/global-burden-of-tb 38/79
38
DTO ( District Tuberculosis officer ) Jammu is overall incharge of the DMC,
ASCOMS. She is regularly supervising the DMC work & coordinating with the
Doctors of ASCOMS for better results.
No. of NGO's and Private Practioners in Jammu Distt.
Initial attempts were made to involve many NGO’s and private practioners.
1. St. Joseph’s Missionary Hospital at Barjani Smailpur–28 pts.
2. Mother Teresa Charitable Trust at New Plots–2 pts.
3. Shivgotra Medicos (Retd. Army Personal) Bahu fort–7 pts.
4. Shivam Medicos Talab Tillo–2 pts.
5. Catholic Social Service Society, Kunjwani–8 pts. (Sh.Nayamat Ali) (Coordinator)
6. (7-8) ASHA Workers.25-pts.have completed their treatment.Only 1 (one) ASHA Worker
is presently engaged-3 pts.
7. NGO’s and PVT. Practioners in other parts of TU Jammu.
8. Approx. 45-50 ASHA Workers in TU R.S. Pura.
9. ESI Hospital (DOT Centre).
10. Railway Hospital (DOT Centre).
8/4/2019 Global Burden of Tb
http://slidepdf.com/reader/full/global-burden-of-tb 39/79
39
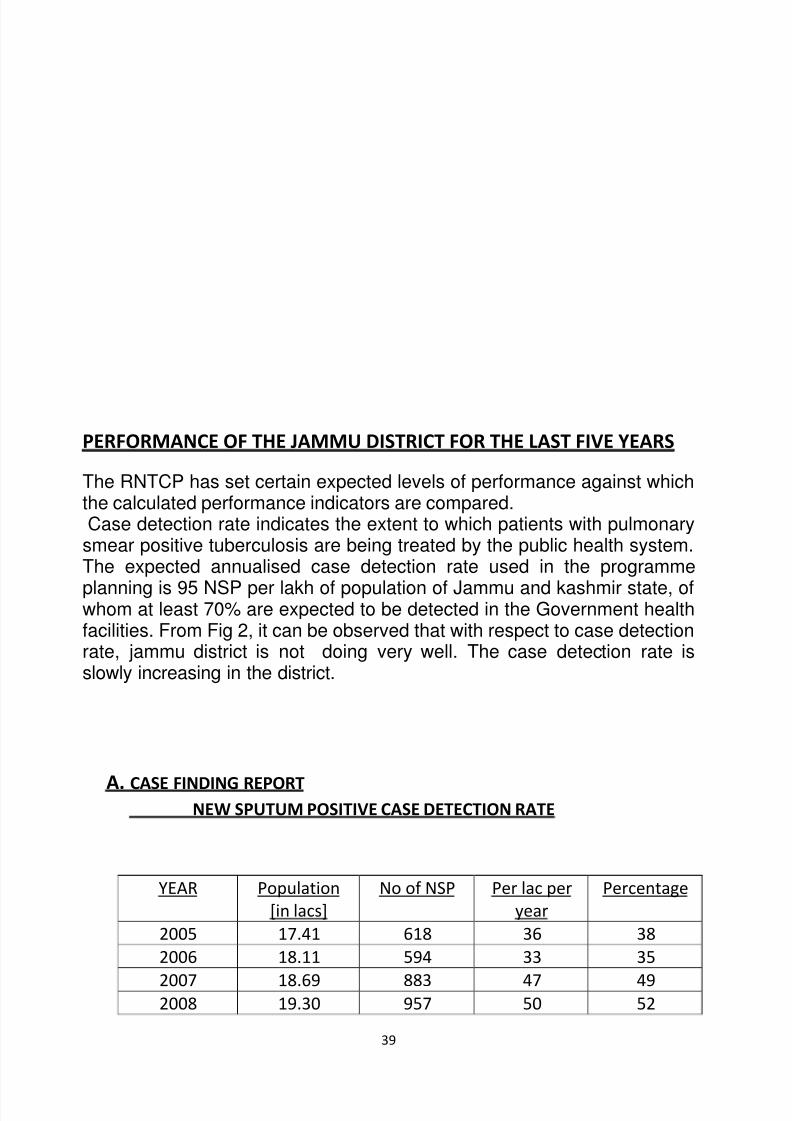
PERFORMANCE OF THE JAMMU DISTRICT FOR THE LAST FIVE YEARS
The RNTCP has set certain expected levels of performance against whichthe calculated performance indicators are compared.Case detection rate indicates the extent to which patients with pulmonary
smear positive tuberculosis are being treated by the public health system.The expected annualised case detection rate used in the programme
planning is 95 NSP per lakh of population of Jammu and kashmir state, ofwhom at least 70% are expected to be detected in the Government healthfacilities. From Fig 2, it can be observed that with respect to case detectionrate, jammu district is not doing very well. The case detection rate isslowly increasing in the district.
A. CASE FINDING REPORTNEW SPUTUM POSITIVE CASE DETECTION RATE
YEAR Population
[in lacs]
No of NSP Per lac per
year
Percentage
2005 17.41 618 36 38
2006 18.11 594 33 35
2007 18.69 883 47 492008 19.30 957 50 52
8/4/2019 Global Burden of Tb
http://slidepdf.com/reader/full/global-burden-of-tb 40/79
40
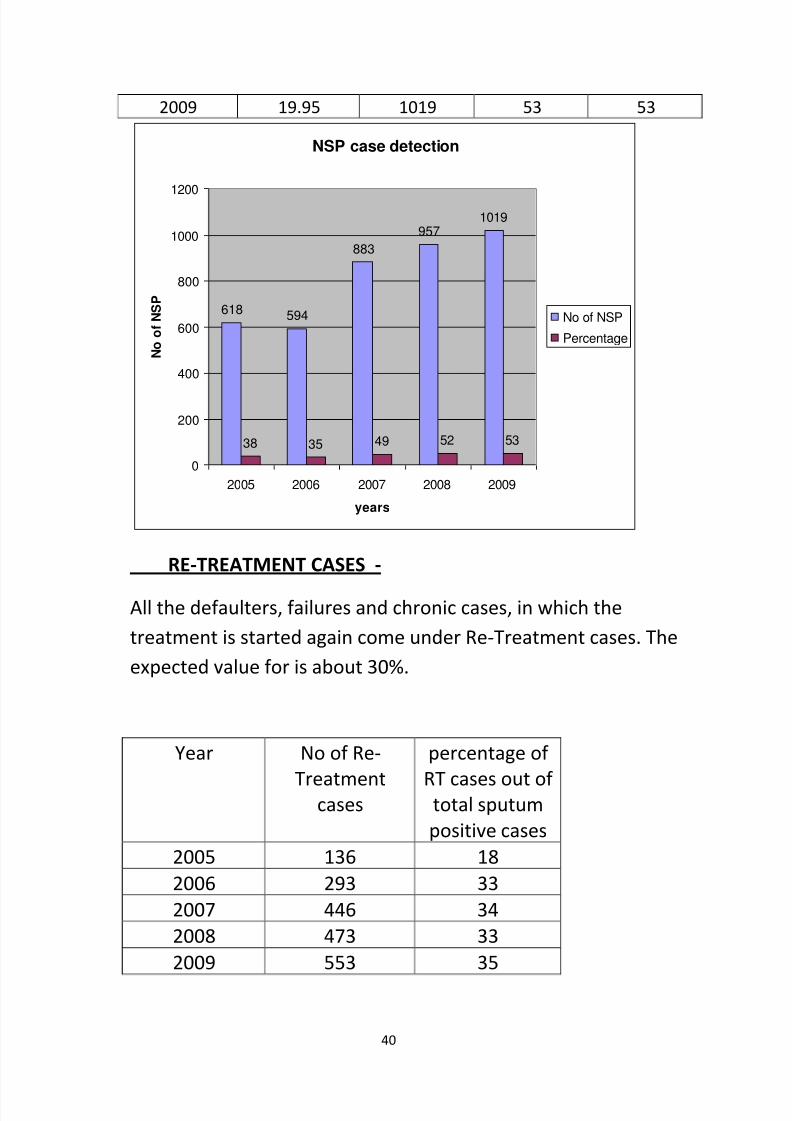
2009 19.95 1019 53 53
NSP case detection
618 594
883
9571019
38 35 49 52 53
0
200
400
600
800
1000
1200
2005 2006 2007 2008 2009
years
N o o f N S P
No of NSP
Percentage
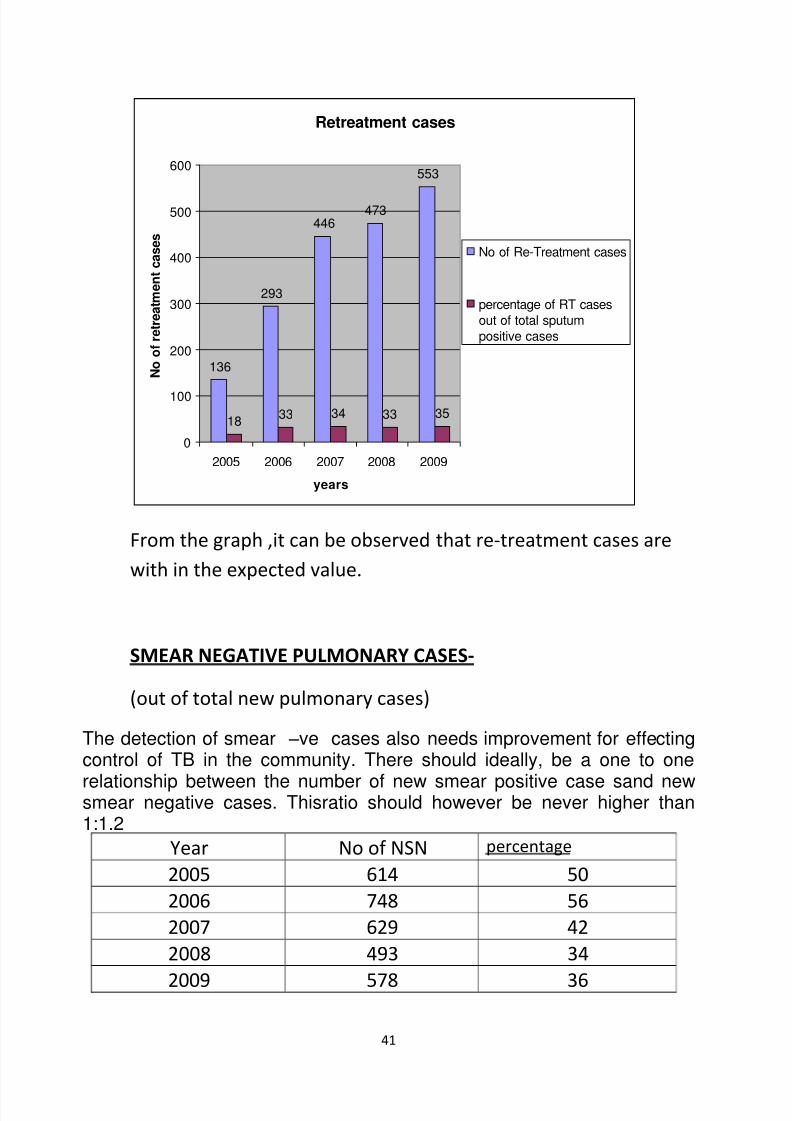
RE-TREATMENT CASES -
All the defaulters, failures and chronic cases, in which the
treatment is started again come under Re-Treatment cases. The
expected value for is about 30%.
Year No of Re-
Treatmentcases
percentage of
RT cases out of total sputum
positive cases
2005 136 18
2006 293 33
2007 446 34
2008 473 33
2009 553 35
8/4/2019 Global Burden of Tb
http://slidepdf.com/reader/full/global-burden-of-tb 41/79
41
Retreatment cases
136
293
446473
553
1833 34 33 35
0
100
200
300
400
500
600
2005 2006 2007 2008 2009
years
N o o f r e t r e a t m e n t c a s e s
No of Re-Treatment cases
percentage of RT cases
out of total sputum
positive cases
From the graph ,it can be observed that re-treatment cases are
with in the expected value.
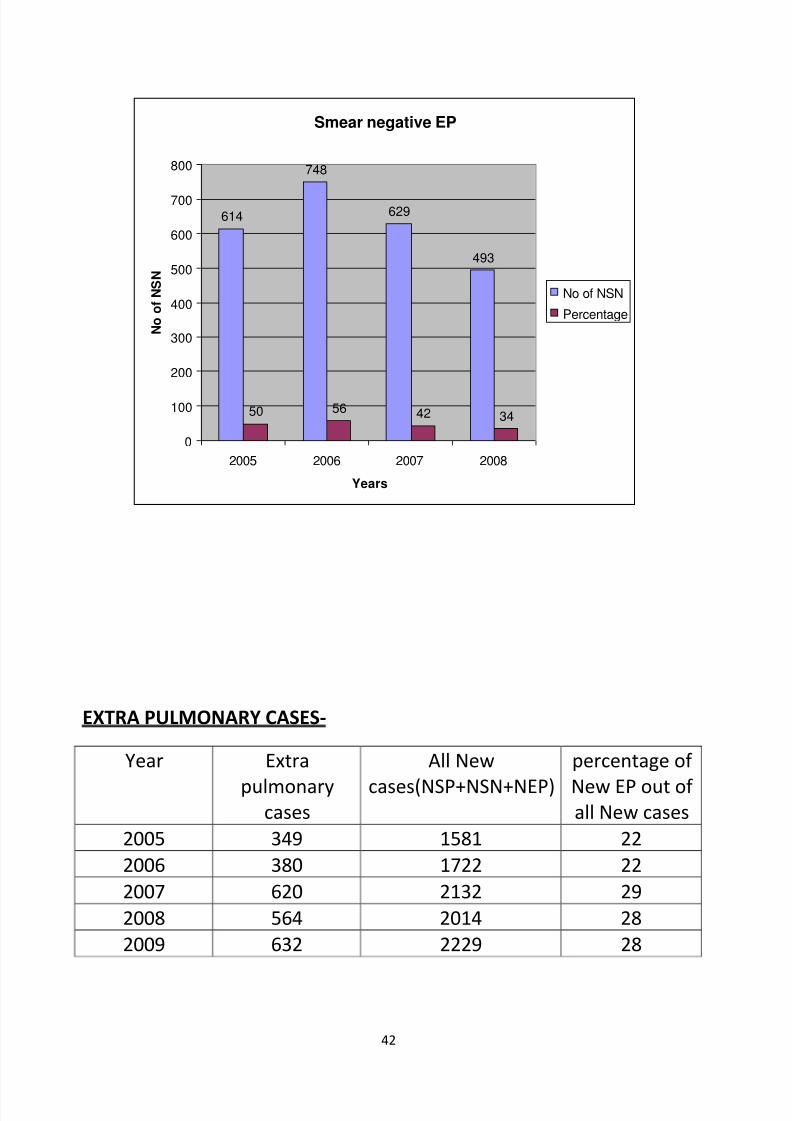
SMEAR NEGATIVE PULMONARY CASES-
(out of total new pulmonary cases)
The detection of smear –ve cases also needs improvement for effectingcontrol of TB in the community. There should ideally, be a one to one
relationship between the number of new smear positive case sand newsmear negative cases. Thisratio should however be never higher than1:1.2
Year No of NSN percentage
2005 614 50
2006 748 56
2007 629 42
2008 493 34
2009 578 36
8/4/2019 Global Burden of Tb
http://slidepdf.com/reader/full/global-burden-of-tb 42/79
42
Smear negative EP
614
748
629
493
50 56 42 34
0
100
200
300
400
500
600
700
800
2005 2006 2007 2008
Years
N o o f N S N
No of NSN
Percentage
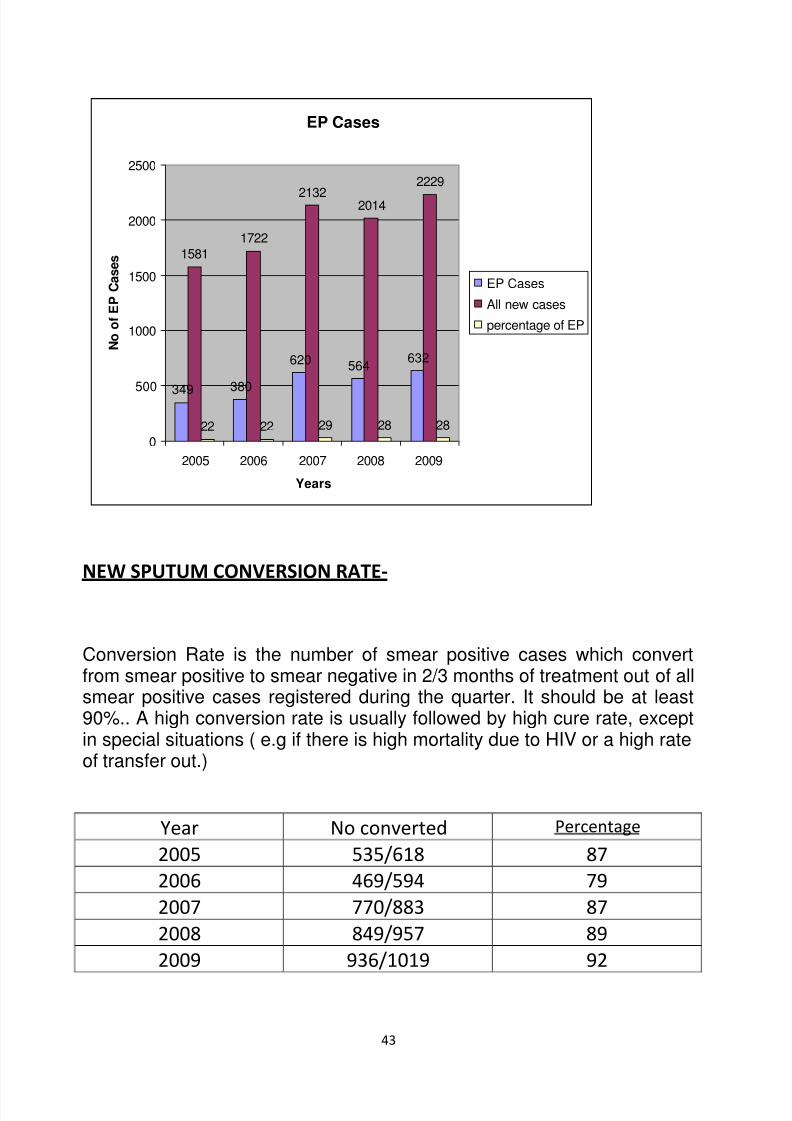
EXTRA PULMONARY CASES-
Year Extra
pulmonarycases
All New
cases(NSP+NSN+NEP)
percentage of
New EP out of all New cases
2005 349 1581 22
2006 380 1722 22
2007 620 2132 29
2008 564 2014 28
2009 632 2229 28
8/4/2019 Global Burden of Tb
http://slidepdf.com/reader/full/global-burden-of-tb 43/79
8/4/2019 Global Burden of Tb
http://slidepdf.com/reader/full/global-burden-of-tb 44/79
44
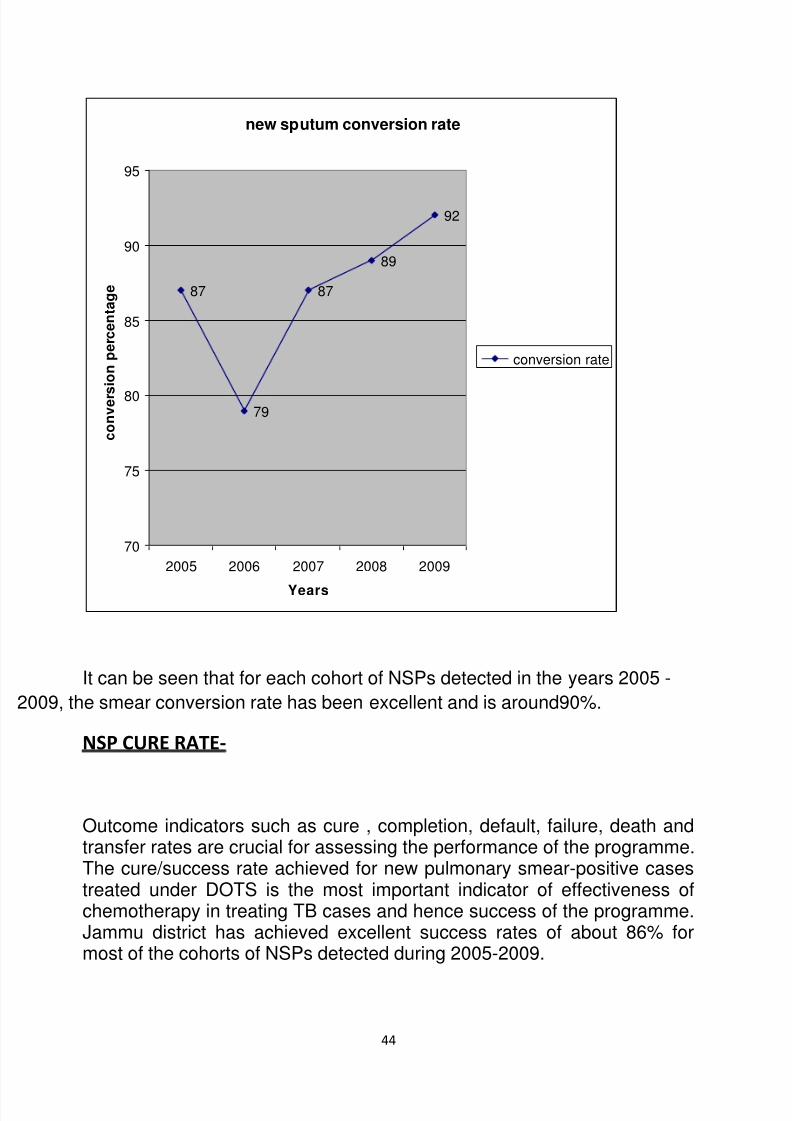
new sputum conversion rate
87
79
87
89
92
70
75
80
85
90
95
2005 2006 2007 2008 2009
Years
c o n v e r s
i o n p
e r c e n t a g e
conversion rate
It can be seen that for each cohort of NSPs detected in the years 2005 -
009, the smear conversion rate has been excellent and is around90%.
NSP CURE RATE-
Outcome indicators such as cure , completion, default, failure, death andtransfer rates are crucial for assessing the performance of the programme.The cure/success rate achieved for new pulmonary smear-positive casestreated under DOTS is the most important indicator of effectiveness ofchemotherapy in treating TB cases and hence success of the programme.Jammu district has achieved excellent success rates of about 86% formost of the cohorts of NSPs detected during 2005-2009.
8/4/2019 Global Burden of Tb
http://slidepdf.com/reader/full/global-burden-of-tb 45/79
45
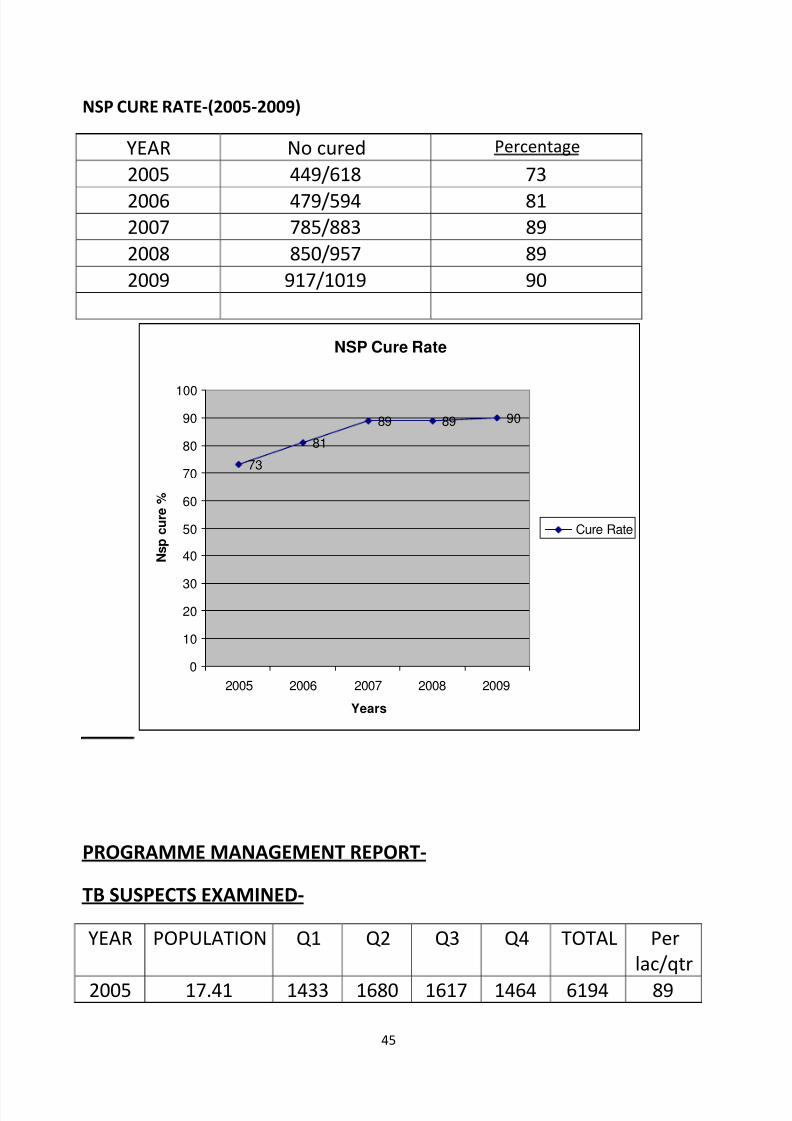
NSP CURE RATE-(2005-2009)
YEAR No cured Percentage
2005 449/618 73
2006 479/594 812007 785/883 89
2008 850/957 89
2009 917/1019 90
NSP Cure Rate
73
81
89 89 90
0
10
20
30
40
50
60
70
80
90
100
2005 2006 2007 2008 2009
Years
N s p c u r e %
Cure Rate
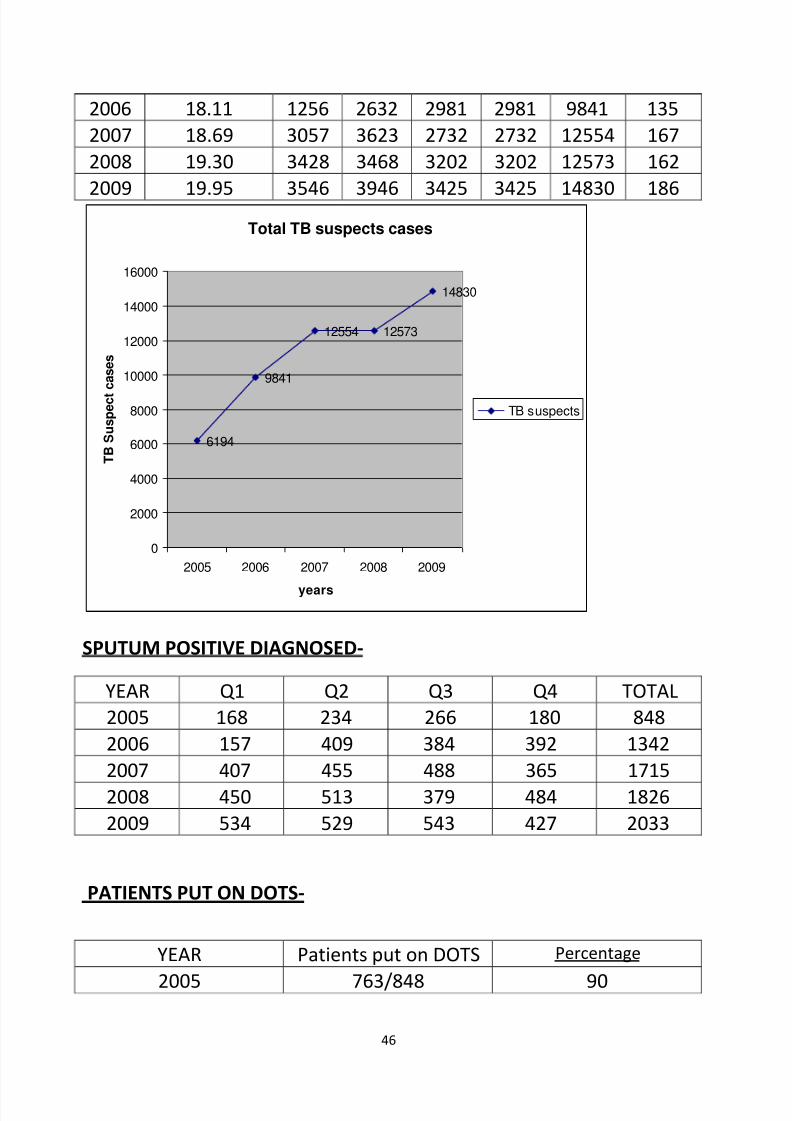
PROGRAMME MANAGEMENT REPORT-
TB SUSPECTS EXAMINED-
YEAR POPULATION Q1 Q2 Q3 Q4 TOTAL Per
lac/qtr
2005 17.41 1433 1680 1617 1464 6194 89
8/4/2019 Global Burden of Tb
http://slidepdf.com/reader/full/global-burden-of-tb 46/79
46
2006 18.11 1256 2632 2981 2981 9841 135
2007 18.69 3057 3623 2732 2732 12554 167
2008 19.30 3428 3468 3202 3202 12573 162
2009 19.95 3546 3946 3425 3425 14830 186Total TB suspects cases
6194
9841
12554 12573
14830
0
2000
4000
6000
8000
10000
12000
14000
16000
2005 2006 2007 2008 2009
years
T B S u s p e c t c a s e s
TB suspects
SPUTUM POSITIVE DIAGNOSED-
YEAR Q1 Q2 Q3 Q4 TOTAL
2005 168 234 266 180 848
2006 157 409 384 392 1342
2007 407 455 488 365 1715
2008 450 513 379 484 1826
2009 534 529 543 427 2033
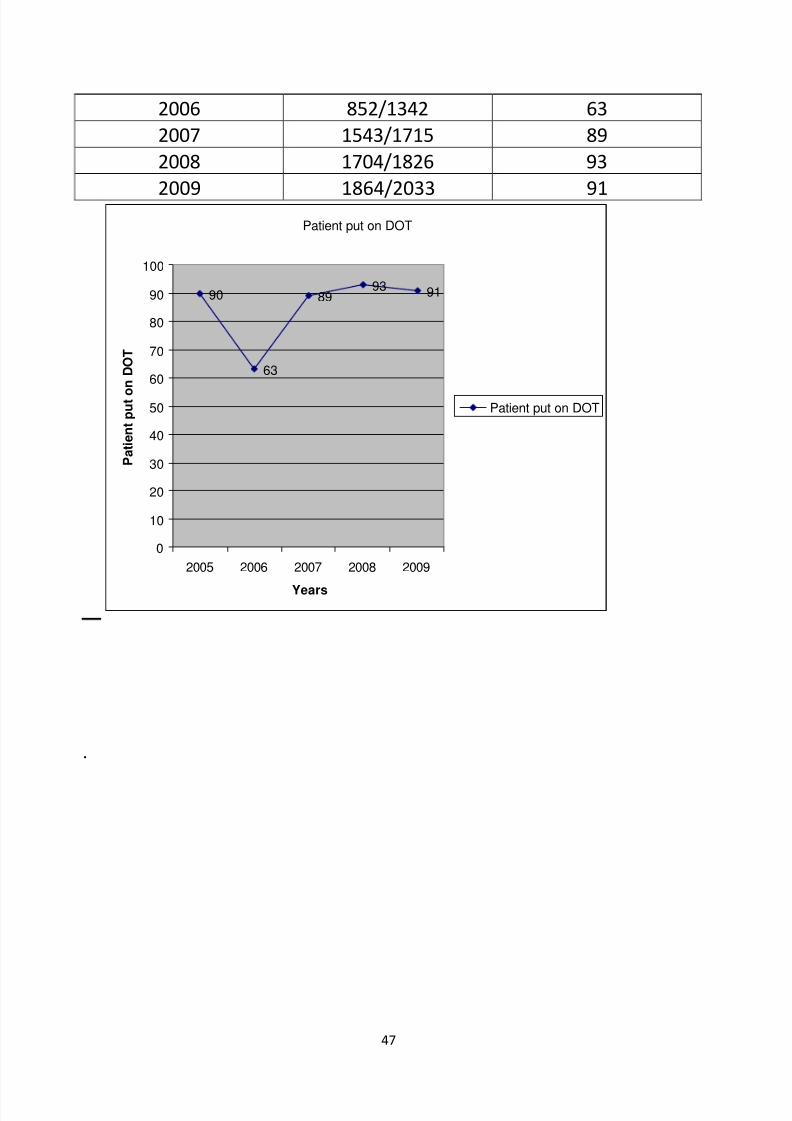
PATIENTS PUT ON DOTS-
YEAR Patients put on DOTS Percentage
2005 763/848 90
8/4/2019 Global Burden of Tb
http://slidepdf.com/reader/full/global-burden-of-tb 47/79
47
Patient put on DOT
90
63
8993 91
0
10
20
30
40
50
60
70
80
90
100
2005 2006 2007 2008 2009
Years
P a t i e n t p u t o
n D O T
Patient put on DOT
.
2006 852/1342 63
2007 1543/1715 89
2008 1704/1826 93
2009 1864/2033 91
8/4/2019 Global Burden of Tb
http://slidepdf.com/reader/full/global-burden-of-tb 48/79
48
Practices followed by programme personnel under RNTCP-To review the actual practices followed under RNTCP in terms of detailed
operational aspects , the various categories of staff were interviewed
using semi structured interview schedule.
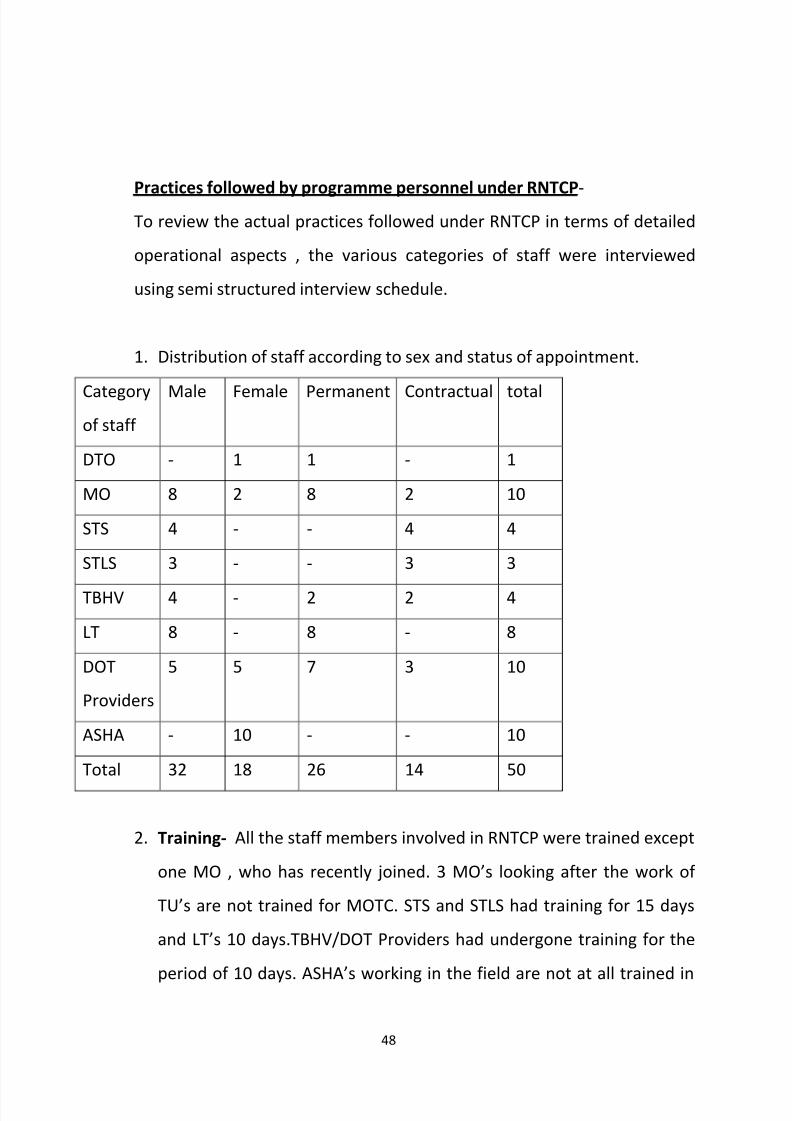
1. Distribution of staff according to sex and status of appointment.
Category
of staff
Male Female Permanent Contractual total
DTO - 1 1 - 1
MO 8 2 8 2 10
STS 4 - - 4 4
STLS 3 - - 3 3
TBHV 4 - 2 2 4
LT 8 - 8 - 8
DOT
Providers
5 5 7 3 10
ASHA - 10 - - 10
Total 32 18 26 14 50
2. Training- All the staff members involved in RNTCP were trained except
one MO , who has recently joined. 3 MO’s looking after the work of
TU’s are not trained for MOTC. STS and STLS had training for 15 days
and LT’s 10 days.TBHV/DOT Providers had undergone training for the
period of 10 days. ASHA’s working in the field are not at all trained in
8/4/2019 Global Burden of Tb
http://slidepdf.com/reader/full/global-burden-of-tb 49/79
49
RNTCP. Most of the staff is working for TB programme for more than 5
years.
3. Duties and responsibilities of the staff- It was started by all staff
members interviewed that none of them were provided with written
job responsibilities by the higher activities. They had come to know
about these from their training as well as day to day experience on job.
4. Address verification- All MO’s were asked as how to verify the address
of the patient, all of them answered that the address is verified,
through home visits by TBHV. As mentioned by TBHV’s after obtaining
report of the sputum examination of the patient, if found positive for
AFB , address is confirmed by home visits. The contact person of the
patient, who is any responsible person who knows the patient and can
take his responsibility is approached if address can not be verified.
5. Initiation of treatment – when asked how the treatment of the TB
patient started before confirmation of address, where as fourmentioned that treatment can be started if someone responsible
guaranties and address is verified later.
6. Drug administration - when asked how do they ensure that patient
really consume medicines , all of them said by direct observation.
Regarding help from the community volunteers or NGO’s , six out of
ten DOT Providers said they take the help of NGO’s and ASHA’s in
administering DOTS. For the purpose of home visits they stated for
address verification and for tracing the patients in case they default.
For the mode of transport, 8 of them replied by their own transport
and 2 said by bus.
7. Action taken for seriously ill patients – TBHV/DOT Providers were
asked as to what they do in case of seriously ill patients who fail to
8/4/2019 Global Burden of Tb
http://slidepdf.com/reader/full/global-burden-of-tb 50/79
50
report for drug collection on scheduled date. 2 TBHV;s and 6 DOT
Providers told that it is the family’s responsibility to take care of
seriously ill and medicines are given to family members for
unsupervised therapy.2 of them said that home visits are made and
sometimes of ASHA is taken.
8. Material management – Drugs and Supply - As per information
available from 9 out of 10 MO’s all ATT drugs are received as central
supply from central TB division. The drugs are available in adequate
quantity and in regular supply. Supply of the lab chemicals , reagents
and consumables were also reported to be regular and adequate. Only
1 MO reported that he faces problem of irregular supply of drugs and
lab consumables as he working in tertiary level health centre and
patient load is very high there. All STS , STLS and LT’s also reported
adequate and regular supply of drugs and lab chemicals but they
themselves have to go to the DTC and collect these consumables asthere is no provision from district to supply these medicines to their
centres.
9. Supervisory visits – MO’s , STS and STLS were asked about frequency
and the nature of supervisory activities perform by them. Only 1 MO
reported that he is making 3- 4 visits in his DOT centres per month. All
the 4 STS and 3 STLS reported to make 4-8 visits to their centres per
month. They are using motor bikes provided to them under RNTCP for
this purpose. They are making tour programme and maintaining tour
diary which they submit to DTO at the end of the month. They are
provided with supervisory checklist. STS said that they check all the
treatment cards and records of the patients and also supply of the
drugs. They make defaulter visits along with TBHV in case the patient is
8/4/2019 Global Burden of Tb
http://slidepdf.com/reader/full/global-burden-of-tb 51/79
51
not retrieved by TBHV alone. All STLS said that they cross check all the
positive slides and 10-20% of the negative slides, they also check
regularity of supply of lab consumables. They visits all the DMC’s at
least once in a month. MO’s visit DMC’s occasionally as reported by all
STLS. DTO Jammu is also playing important role in the supervision. She
is visiting all the DOT centres in the district regularly and putting
forward the reports of her findings to STO. She also mentioned that
she is provided with a vehicle for supervision.
Medical officer’s perception regarding satisfaction level in staff & patients.
Medical officers were asked about their perception regarding satisfaction
among the staff & patients with the implementation of the programme. All of
them replied that staff was only partially satisfied with the implementation of the
programme.
Regarding patients satisfaction, 6 out of four said that patients were
partially satisfied. All M.Os mentioned that they were fully aware of the
problems faced by patients. They all said that there is no difference in working of
regular & contractual staff.
Information, Education & Communication
All 10 LTs were asked as to what Instructions they give to patients for
sputum sample. All said cough deeply.
All the MOs, TBHVs & DOT providers mentioned that motivation & health
education is provided individually. The detailed health education is provided at
the beginning of treatment & is supported by all health workers.
8/4/2019 Global Burden of Tb
http://slidepdf.com/reader/full/global-burden-of-tb 52/79
52
When asked regarding IEC in there DOT centres, said that posters are used
for conveying messages, whereas MO mentioned about community meetings
and health talks.
Waste Management: All medical officers & LTs stated that sputum cups & slides
are kept in 5% phenol & then disposed off in the hospital bins.
Recording & Reporting: This information was collected during interview of
service provides as well as during observation of various DOT centres. The TB lab
register at all DOT centres in maintained by LT as well as lab forms for sputum
are entered by LT. The patient’s treatment cards & drug records are maintained
by DOT provides. All patients maintain their Identity cards but all entries are
made by DOT provider/TBHV. The indent register for lab chemicals, reagent &
consumables is maintained by all STLS & for drugs , disposal syringes & needles in
maintained by all STS. The TB register for each treatment units is maintained by
respective STS as well as all entries in it are made by him.
All LTs stated that performance reports are sent monthly to STS &
quarterly reports are also being submitted at the end of each quarter.
All the STS & STLS stated that monthly reports are submitted to DTO,
which are compiled into quarterly reports by Data Entry operator.All medical
officers also confirmed that reporting on performance of cases in done monthly
by LTS & TBHVs. 4 MOs stated that reports are sent to central TB Division –
MOHFW & state TB officer.
Monitoring of the programme:
All MOs mentioned that regular monthly meetings are held between DOTS
implementing staff i.e. LTs, TBHVs, STS, STLS & DTO. Regular monthly meetings
8/4/2019 Global Burden of Tb
http://slidepdf.com/reader/full/global-burden-of-tb 53/79
53
are also held between DTO & STO. As told by DTO teams from MOHFW & other
agencies also visit to review the programme.
Problems faced & suggestions given by staff :
Health workers were asked to enumerate the problem faced by them &
suggestion for improving the patient care services.
Out of 10 LTs, 5LTs said that they did not face any problem. 2 LTs remained
silent & rest 3 mentioned few problem:-
Lab was too small & working space was inadequate.
Patients do not give proper sputum samples so smear examination has to be
repeated.
They also mentioned about heavy work load be cause they also have to do all
the routine has lab in the health centres TBHVs told that they face problemduring have visits. It was difficult & hectic job to find a house in many
localities especially in case of slums.
One TBHV mentioned that area covered by him was to big. They also stated
that they had to walk a lot to trace a house. Some patients give wrong
address because of which patient can not be traced.
DOT providers stated that patients prefer taking medicines home rather
swallowing them in their presence. In DOT centres, patients bring some local
leaders/influential peoples of that area to take medicines at home.
Two DOT providers also stated that space provided for the centre is not
adequate for administration of DOTS.
STS, & STLS also stated problem because of absence of MOTC, in their TUS.
They also stated that few health worker do not co-operate with them during field
8/4/2019 Global Burden of Tb
http://slidepdf.com/reader/full/global-burden-of-tb 54/79
54
visits. AT few DOT centres there is no permanent DOT provider because of
scarcity of man power. They suggested that community volunteers/ASHAS should
be involved in activity.
Not much suggestion were given by them. MOs stated that refresher training
of staff should be done time to time. They also reported scarcity of man power in
the fields should be sorted out.
MOs also suggested that supervisory staff should act more activity for better
performance of the programme.
Problems faced & satisfaction with treatment among TB patients.
In order to obtain information regarding various problems faced by patients &
their satisfaction with services provided, a sample of 60 patients was selected
from various DOT centres of Distt.
General profile of patients interviewed
Category Male Female Total
No. No. No.
Cat. I 20 15 35
Cat II 12 3 15
Cat III 6 4 10
38 22 60
Category wise distribution = pie chart

8/4/2019 Global Burden of Tb
http://slidepdf.com/reader/full/global-burden-of-tb 55/79
55
8/4/2019 Global Burden of Tb
http://slidepdf.com/reader/full/global-burden-of-tb 56/79
56
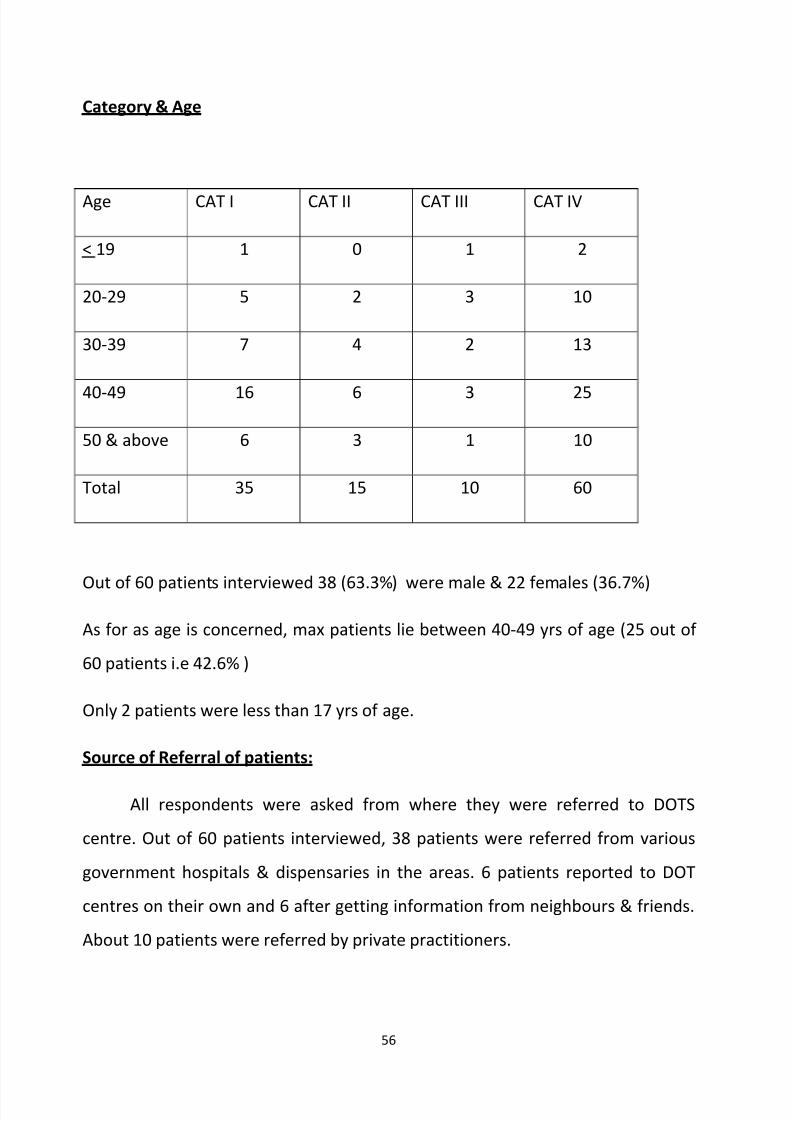
Category & Age
Age CAT I CAT II CAT III CAT IV
< 19 1 0 1 2
20-29 5 2 3 10
30-39 7 4 2 13
40-49 16 6 3 25
50 & above 6 3 1 10
Total 35 15 10 60
Out of 60 patients interviewed 38 (63.3%) were male & 22 females (36.7%)
As for as age is concerned, max patients lie between 40-49 yrs of age (25 out of
60 patients i.e 42.6% )
Only 2 patients were less than 17 yrs of age.
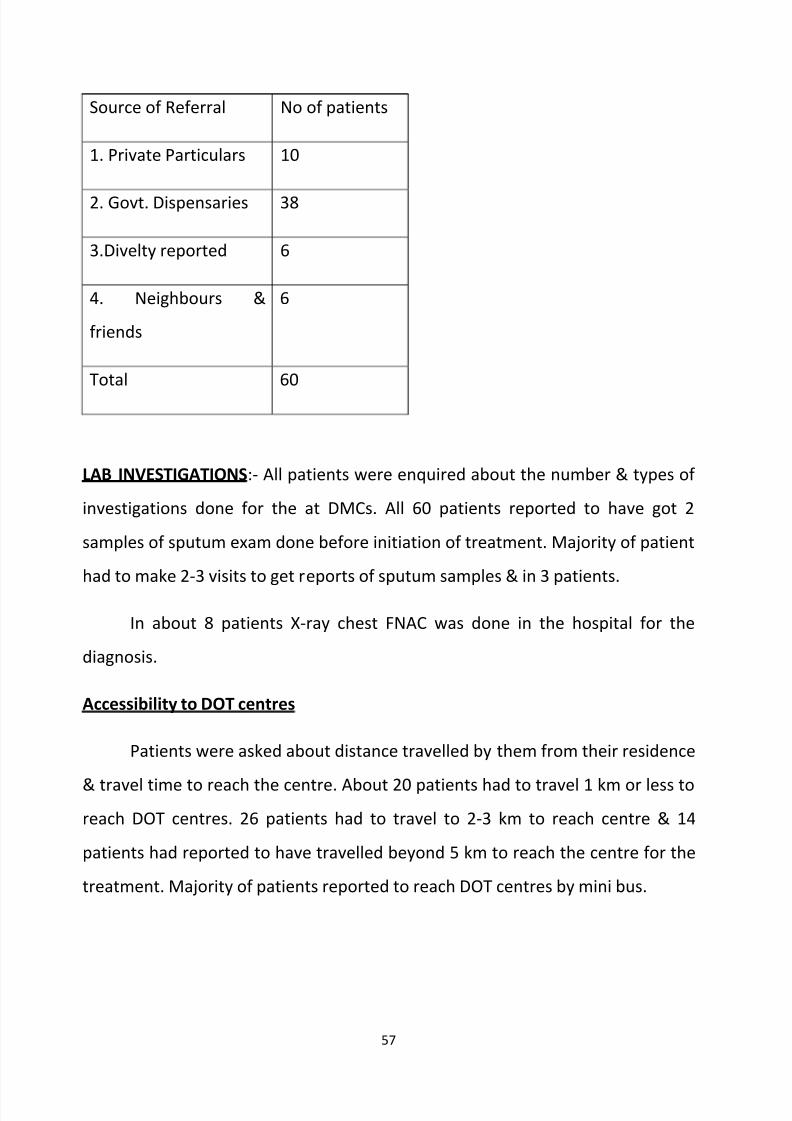
Source of Referral of patients:
All respondents were asked from where they were referred to DOTS
centre. Out of 60 patients interviewed, 38 patients were referred from various
government hospitals & dispensaries in the areas. 6 patients reported to DOT
centres on their own and 6 after getting information from neighbours & friends.
About 10 patients were referred by private practitioners.
8/4/2019 Global Burden of Tb
http://slidepdf.com/reader/full/global-burden-of-tb 57/79
57
Source of Referral No of patients
1. Private Particulars 10
2. Govt. Dispensaries 38
3.Divelty reported 6
4. Neighbours &
friends
6
Total 60
LAB INVESTIGATIONS:- All patients were enquired about the number & types of
investigations done for the at DMCs. All 60 patients reported to have got 2
samples of sputum exam done before initiation of treatment. Majority of patient
had to make 2-3 visits to get reports of sputum samples & in 3 patients.
In about 8 patients X-ray chest FNAC was done in the hospital for the
diagnosis.
Accessibility to DOT centres
Patients were asked about distance travelled by them from their residence
& travel time to reach the centre. About 20 patients had to travel 1 km or less to
reach DOT centres. 26 patients had to travel to 2-3 km to reach centre & 14
patients had reported to have travelled beyond 5 km to reach the centre for the
treatment. Majority of patients reported to reach DOT centres by mini bus.
8/4/2019 Global Burden of Tb
http://slidepdf.com/reader/full/global-burden-of-tb 58/79
58
Waiting time at DOTS centre
The average waiting time in getting treatment was reported to be 15 to 25 .
Patients at DOT centres at secondary & tertiary level hospitals reported thatthey have to wait for about half an hour.
Availability of Medicines
All patients were asked if they could obtain all medicines prescribed to the
to them. According to all, the anti TB medicines were available for every patient
put on DOTS treatment from the centre & were available free of cost in blister
packs.
Improvement in symptoms from in of Treatment
When patients were asked regarding of doses of treatment taken after
which there was improvement in their symptoms, majority of then (45 ie 75%)
reported improvement in symptoms with 10-12 doses of anti-tuberculosis drugs
ie 3-4 weeks of regular treatment.
Missed doses during treatment whenasked about number of doses of
treatment they have missed till date, only 4 patients said that they have missed
one dose. 2 patient reported too sick as the reason for missed doses, whereas 2
other reported “gone out”.
Attitude of health staff
As regards the attitude of DOTS centres health staff patients, 54 (90%)
stated it to be fully sympathetic & only 6 had different views of which 3 stated to
be rude/unsympathetic.
As regards the availability of staff of DOTS centre 59 respondents stated
that the staff was present.
8/4/2019 Global Burden of Tb
http://slidepdf.com/reader/full/global-burden-of-tb 59/79
59
Health Education:
54 patients said that they were provided. Information about TB and
related issues whereas 6 said no information was provided to them. They toldthat they were advised to cover their face while coughing & not to food &
utensils so that other don’t get disease from them.
Satisfaction in the services available.
56 patients (96.6%) said that they were satisfied with services. However, 3
patients responded by saying as some what satisfied & one even said that he is
not satisfied because he has to come from from far off place.
When asked about reason for satisfied they said lack of financial burden as
these medicine are available free of cost. Also sympathetic attitude of the
providers was enumerated as reason for their satisfaction.
Problems faced by patient
Out 60 patients interviewed, 18 patients (30%) reported to have faced one
or more problems. Some of the problems they maintained were:-
Difficult to come on alternate day
Symptoms not improving
Wastage of time
Owners don’t allow to go to centre
Long distance to be travelled to reach DOT centre
Too week to go to centre
Long distance to be travelled to reach DOT centre
8/4/2019 Global Burden of Tb
http://slidepdf.com/reader/full/global-burden-of-tb 60/79
60
Findings Based on observation of DOT centre
A check list was used in order to obtain information on operational
procedure & practices adopted under RNTCP at DOT centres.
A total of 10 DOT centres were selected for this purpose and following
observations were made:
All the patient wise boxes were being marked & maintained for each
patient. There was facilties for clean water in all DOT centres. A total of 50
patients were observed for direct observation of treatment & the findings were:
Patients physically reported to collect drugs – 48/60 = 80%
Drugs carried by relatives – 12/60 = 20%
Medicines swallowed under direct observation – 40/48 = 83.5%
Medicines carried have by patients = 8/48 = 16.5%
All entries were correctly entered & treatment cards were complete:
Home address verification was done in 45 patients.
Adequate stock of anti TB drugs was available for Cat I, Cat II & Cat III patients,
but not as per RNTCP guidelines. Boxes were stored in safe dry places not
exposed to sunlight. Adequate number of disposable syringes, needles & distilled
water ampoules for CAT II patients were available only in 2 centers. In Rest 8 DOT
centres patients were getting then own disposable syringes.
8/4/2019 Global Burden of Tb
http://slidepdf.com/reader/full/global-burden-of-tb 61/79
61
IEC material in from of banners& posters were displayed in all the DOT centres.
Health workers were also motivating & giving health education to TB patient so
that they adhere to treatment.
Observations at Designated Microscopic Centres-
A total of 5 DMCs were selected as per RNTCP guidelines for the internal
evaluation of the District. A Check list was made and following observations were
made –
All the chest symptomatic from OPD were referred to DMCs where RNTCP
trained LT was present who was filling up the lab forms and was giving
sputum containers to patients after instructing him how to cough out the
sputum. He was collecting on the spot specimen and was giving another
container for early morning sample. After collection of sputum staining
was done and a report was prepared with proper grading. All the sputumpositive results were written in red ink in the lab register. In all the DMCs
all the essential consumables including binocular microscope was
available. Facilities for running water for the staining purpose were also
present in all the DMCs. At the end of every month a summary abstract is
completed by every LT.
8/4/2019 Global Burden of Tb
http://slidepdf.com/reader/full/global-burden-of-tb 62/79
62
Discussion-
Appraisal of any programme is important both at macro land micro levels, the
present study has been conducted with the aim of a micro level performance
appraisal of the RNTCP in a District the important aspects of the programme like
organizational` and operational features, availability of resources, treatment
outcome among patients registered as well as experiences and problems among
service providers and beneficiaries of services.
Since initiation of RNTCP in this district about 6 years have passed and it is
assumed that the programme has overcome the likely problems in the initial
phase of implementation. For successful implementation of the programme it is
essential to have an effective organization with committed staff who are well
conversant with the programme objectives and their own role towards its
implementation. From the study of the organizational set up, it was evident that
the human resource available and their distribution in the different functional
units i.e. the Treatment Units and their attached DOTS centres had been quite
satisfactory as per the programme guidelines, trained in RNTCP and well
experienced in TB control activities. Another strength of the programme in terms
of human resource in this District was that on the whole the staffs were aware
about their job responsibilities towards the RNTCP even though they were not
provided with any written job chart.
One of the essential features of RNTCP is the commitment under the programme
to ensure a regular, adequate and uninterrupted supply of all anti TB drugs and
other supplies including equipment and consumable items for running the
programme.
One of the parameters for assessment of performance of the TB control
programme is its ability to detect maximum number of cases and to put them on
8/4/2019 Global Burden of Tb
http://slidepdf.com/reader/full/global-burden-of-tb 63/79
63
regular treatment and thereby achieve best cure rate of over 85% as per the
objective of the RNTCP.
In this study the different indicators of treatment outcome for the District werecalculated for five years i.e. from 2005 to 2009 and it was observed that case
detection had been very low in the past but slowly improving. The cure rate
achieved for new sputum positive cases treated under DOTS is the most
important indicater of effectiveness of chemotherapy in treating TB cases and
hence success of the programme. Jammu district has achieved excellent cure
rates of about 89%-90% in last 3 years. The Sputum conversion rates at the end
of 2/3 months were nearing 90% in last 2 years which is well in comparision with
expected levels.
With regard to the various qualitative aspects of treatment of patients, the
practice in this Distt. was reported to be to initiate treatment only after
verification of address of the diagnosed case as already described. Those who are
residing outside the area of jurisdiction of the TUs are referred after investigation
and diagnosis, to their respective TUs/DOTs centres near to their residential
areas. This practice will be useful for all patients registered for treatment at the
centre since it will ensure proper follow up of patient as well as default action
when required, provided the timely home visit and address verification is done
and treatment initiated by the staff. Problems like too large population and areato be covered by staff, inadequate work space for staff particularly for
laboratory, patients giving wrong addresses should be taken care of.
For the success of the DOTS strategy adopted under the RNTCP, one of the most
essential requirements is to ensure direct observation of treatment taken by the
8/4/2019 Global Burden of Tb
http://slidepdf.com/reader/full/global-burden-of-tb 64/79
8/4/2019 Global Burden of Tb
http://slidepdf.com/reader/full/global-burden-of-tb 65/79
65
and sustained efforts on the part of the staff during subsequent contacts with
the patients during the later part of treatment. Other media of communication
like hoardings and posters were seen to be displayed in most of the DOTS centres
but there is need for more emphasis on IEC through interpersonal
communication to ensure continued motivation of patients to complete the
treatment.
Being a highly infectious disease, infectious sputum samples are to be handled by
the laboratory staff, one of the essential requirements under the programme is
proper and hygienic disposal of all such infectious material for the safety of the
community and of the personnel handling such materials.
On the whole the infrastructural facilities under the programme at the Distt
centres were quite satisfactory. Accessibility and approachability of the
diagnostic and treatment facilities at convenient locations in easily identifiable
manner are the strong features that could be noticed in this study.
Few DMCs are working as DOTs centres due to shortage of space & also at few
centres LTs administrating the treatment to patient. Though there were few
problems related to the lay out and availability of space in some of the DOTS
centres, in general there was adequate space for staff as well as waiting space
for patients, availability of water and electricity, maintenance of general
cleanliness etc. Binocular microscopes were available in all the microscopy
centres. It was satisfying to note that generally patients did not have any
problem in getting the tests done or in getting the reports as seen from the
interview data from patients. There was no shortage of items like drugs or other
laboratory reagents reported by any staff, which is to be recognized as a very
strong feature of the programme.
8/4/2019 Global Burden of Tb
http://slidepdf.com/reader/full/global-burden-of-tb 66/79
66
Though DTO, STS and STLS are looking after supervision & monitoring of the
RNTCP. Medical officers at the TUs should be made responsible and accountable
for the activities so that case detection can be improved in the peripheral areas.
Patients were also by and large satisfied with the services from the centres.
However few patients had stated to have faced some kind of problem like
difficulty in coming on alternate days for treatment and long distance to travel,
financial loss etc. Patients who have to attend centres from their place of work
had express difficulty in getting permission could have contributed to the
increase default rate only a very small number among the interviewed patients
reported to have missed any dose during the treatment. However, those few
who missed gave reason like ‘urgent work’ or ‘gone out’ etc which gives an
impression that they have not clearly realized the significance of uninterrupted
treatment which needs to be stressed while motivating the patients.
Maintenance of records and submission of monthly and quarterly reported were
found to be reasonably good in the DTC, TUs and DOTS centre as per the
programme guidelines.
Some of the shortcomings observed at the implementation level in DOTS centre
could easily be overcome if proper and adequate supervision is being carried out
by the concerned staff, it seems that no regular schedule of visits are prepared or
followed. Need for special emphasis on more regular and effective supervision is
amply evident.
8/4/2019 Global Burden of Tb
http://slidepdf.com/reader/full/global-burden-of-tb 67/79
67
Conclusions and recommendations-
Conclusions-
A rapid appraisal of organisation , implementation and utilization of DOTS in
Jammu district of Jammu and Kashmir.
General Objective –
To study the organisation, implementation and utilization of DOTS in Jammu
district.
Specific Objectives –
To describe infrastructure facilities and resources available for RNTCP-
DOTS in Jammu District.
To study providers perception regarding DOTS.
To analyse the implementation and achievements of DOTS at various levels
in the district
To ascertain the extent of satisfaction with services provided and problemsif any among patients availing treatment under RNTCP.
To make necessary recommendations for the improvement of the
programme
Methodology-
The study was descriptive in nature and was conducted in DTC and DOT Centres
of Jammu.
The study population comprised of(1) service providers i.e DTO, MOs, STS, STLS,
TBHVs, LTs, DOT Providers and ASHAs.
(2) Beneficiaries included 60 patients.
Observation of selected activities and infrastructure facilities and resources was
done using an observation check list in 6 DMCs and 10 DOT Centres. All 50
service providers were interviewed using semi structured interview schedule for
collecting information on various aspects like accessibility to DOTS Centres
8/4/2019 Global Burden of Tb
http://slidepdf.com/reader/full/global-burden-of-tb 68/79
68
experiences while availing treatment ,extent of satisfaction with treatment etc.
The records studied were TB registers, TB Lab registers and treatment cards of
the patients. Thorough information was obtained on space available, availability
of water, electricity, medicines, lab facilities etc.
Study findings-
The present study focuses on some of the important aspects of RNTCP-DOTS in
Jammu District. RNTCP has been operational since 2004.
Profile of the district -
Total Tuberculosis Unit – 4
Designated Microscopic Centres – 18
DOT centres – 281
District Tuberculosis Centre Jammu is the Nodal point for TB Control activities in
the district.
DTC Jammu is divided into 4 TUs-
5. TU Samba
6. TU Jammu
7. TU Akhnoor
8. TU R S Pura
A team comprising of specifically designated medical officer – TB Control
(MOTC), Senior Treatment Supervisor (STS) and Senior Tuberculosis LabSupervisor is based in a CHC/ Sub district hospital.
OPERATIONAL ASPECTS OF RNTCP – DOTS
8. Diagnosis and Treatment - Sputum microscopy is the primary tool for diagnosing
and monitoring of TB patients. Sputum microscopy is done only in Designated
Microscopy Centres (DMCs). In all the DMCs there is a full time trained lab
technician who is looking after collection, staining and grading of the smears.
8/4/2019 Global Burden of Tb
http://slidepdf.com/reader/full/global-burden-of-tb 69/79
69
If the sputum smear examination is positive
for AFB , the patients is referred to MO for categorisation of disease (into CAT-1,2 and 3)
and TBHV makes home visit to confirm the address of the patient. The anti TB treatment
started after proper health education and motivation. During intensive phase thrice in a
week patient is given medicine under direct supervision – Monday, Wednesday and Friday.During continuation phase the first dose of weekly blister should be directly observed. All
the entries are made and patient’s record is maintained by TBHV/DOT provider at DOT
centre which is under supervision of STS. MOTC is responsible for managing the treatment
unit.
There is a unique system of providing drugs in patient wise boxes ( PWB ) which contain drugs
for entire duration of Treatment for each category of Patient.
Follow up-
The follow up of each patient is to be done at 2-3 months and second at 4-5 months and last at
the end of the treatment. Two sputum smears are examined each time during follow up
Waste Management: All medical officers & LTs stated that sputum cups & slides
are kept in 5% phenol & then disposed off in the hospital bins.
Recording and reporting
In Jammu Distt. , DTO is the overall incharge of Tuberculosis Control
Activities and answerable to State TB Officer at State Health Directorate. He / She reviews the
monthly activity reports of all MOTC’s, STLS and STS with in the Distt. during the monthly Distt.
level meeting of the said staff.
At TU level reporting and recording is done by MOTC, STS and STLS.
Tuberculosis register is kept at Sub-Distt. (TU) level in the Distt only. Monthly report is
prepared every month and submitted to DTC. Quarterly report on case finding, sputum
conversion rate of patients who are on treatment and all possible outcomes of smear positive
cases of pulmonary TB (Cured, Treatment completed, Failure, Defaulted, Died and Transferred
out) is prepared by STS. The STLS is primarily responsible for supervising all the lab activities. It
is the responsibility of TU to compile the DMC wise reports and submit it to DTO.
DTO compiles the report (4 copies) in respect to all TB units and sends three of them to the
STO, The National Tuberculosis Institute Bangalore and to Central TB Division, DGHS Nirman
Bhawan New Delhi.
9. Supervision and monitoring –
8/4/2019 Global Burden of Tb
http://slidepdf.com/reader/full/global-burden-of-tb 70/79
70
In Jammu District D.T.O. with the support of M.O. of DTC is responsible for ensuring the
quality diagnosis , treatment, logistics and reporting.
At T.U. Level , MOTC, STS, and STLS are responsible for undertaking supervisory visits to all
the PHI’s, NGO’s and PP’s STLS is responsible for the quality of sputum smear microscopy
services provided by DMC’s under TU. STS visits all the PHI’s at least once every month he
checks whether all the sputum smear positive patients recorded in the TB Lab. register are
placed on treatment and register in TB register.
10. TRAININGS –
In Jammu district, most of the staff looking after Tuberculosis programme in trained but
motivation level can still be improved by time to time refresher training.
IEC-
In order to control TB, there is need for dissemination of information about tuberculosis ( signs
& Symptoms ), its cause, detection & treatment there by empowering individuals, families &
communities to be responsible for behavioral change to achieve cure of people suffering from
tuberculosis.
As per health providers, motivation & health education is provided individually,
at the beginning of treatment. In DOT centres, posters are used for conveying
messages, whereas MO mentioned about community meetings and health talks.
11. Role of Medical Colleges in RNTCP in Jammu
In Jammu District following Medical Colleges are involved in RNTCP:-
1. Govt. Medical College, Jammu.2.Acharya Sri Chander College of Medical Sciences.
Govt. Medical College, Jammu
GMC, Jammu is playing a very important role in RNTCP. It is functioning as DMC
as well as DOT centre. Since it is a tertiary level Hospital, people have lot of faith
in the medical facilities available here. It caters to both rural & urban population
in Jammu District. There is a separate Chest Diseases Hospital in Jammu city,
8/4/2019 Global Burden of Tb
http://slidepdf.com/reader/full/global-burden-of-tb 71/79
71
where all chest symptomatics prefer to come for diagnosis & treatment. Also
there are special wards for indoor patients. Patients in emergencies are referred
to CD hospital. They are admitted here & treated with prolongation pouches.
ASCOMS is a private Medical college. It also has a DMC & a Treatment
centre. RNTCP team comprising of Medical Officer, Lab. Tech., Dot provider (
TBHV ) is working there. Since the medical college is situated away from the city,
the patients generally avoid going there.
Problems faced & suggestions given by staff :
Lab was too small & working space was inadequate heavy work load because
they also have to do all the routine has lab in the health centres.
TBHVs told that they face problem during have visits. It was difficult & hectic
job to find a house in many localities especially in case of slums, area covered
by him was to big.
DOT providers stated that patients prefer taking medicines home rather
swallowing them in their presence..
STS, & STLS also stated problem because of absence of MOTC, in their TUS. AT
few DOT centres there is no permanent DOT provider because of scarcity of man
power. They suggested that community volunteers/ASHAS should be involved in
activity.
Problems faced & satisfaction with treatment among TB patients.
In order to obtain information regarding various problems faced by patients &
their satisfaction with services provided, a sample of 60 patients was selected
from various DOT centres of Distt.
Out of 60 patients interviewed 38 (63.3%) were male & 22 females (36.7%)
8/4/2019 Global Burden of Tb
http://slidepdf.com/reader/full/global-burden-of-tb 72/79
72
As for as age is concerned, max patients lie between 40-49 yrs of age (25 out of
60 patients i.e 42.6% )
Source of Referral of patients: Maximum were referred from variousgovernment hospitals & dispensaries in the areas. Few patients reported to DOT
centres on their own or after getting information from neighbours & friends.
LAB INVESTIGATIONS:-. All patients reported to have got 2 samples of sputum
exam done before initiation of treatment. Majority of patient had to make 2-3
visits to get reports of sputum samples.
Accessibility to DOT centres Maximum patients had to travel to 2-3 km to reach
centre & few patients had reported to have travelled beyond 5 km to reach the
centre for the treatment.
Waiting time at DOTS centre-15 to 25 minutes.
Medicines
According to all, the anti TB medicines were available for every patient put
on DOTS treatment from the centre & were available free of cost in blister packs.
Improvement in symptoms from in of Treatment
There was improvement in their symptoms, after 10-12 doses of anti-
tuberculosis drugs i.e 3-4 weeks of regular treatment.
Missed doses during treatment only 4 out of 60 patients said that they have
missed one dose. 2 patient reported too sick as the reason for missed doses,
whereas 2 other reported “gone out”.
Attitude of health staff- sympathetic and available during working hours.
8/4/2019 Global Burden of Tb
http://slidepdf.com/reader/full/global-burden-of-tb 73/79
73
Health Education:
Patients said that they were provided information about TB and related
issues. They told that they were advised to cover their face while coughing & notto food & utensils so that other don’t get disease from them.
Satisfaction in the services available.
56 patients (96.6%) said that they were satisfied with services.
Problems faced by patient
Out 60 patients interviewed, 18 patients (30%) reported to have faced one
or more problems. Some of the problems they maintained were:-
Difficult to come on alternate day
Symptoms not improving
Wastage of time
Owners don’t allow to go to centre
Long distance to be travelled to reach DOT centre
Too week to go to centre
Long distance to be travelled to reach DOT centre
The high quality of care and strict adherence to the RNTCP guidelines should becontinued and maintained to sustain the smear conversion and success rates alreadyachieved by the State under the programme.
8/4/2019 Global Burden of Tb
http://slidepdf.com/reader/full/global-burden-of-tb 74/79
74
RECOMMENDATIONS-
Based on observations and findings made during the study on organisation,
implementation and utilisation of RNTCP-DOTS Strategy, it was foundthat overall performance of the district was satisfactory. But still there is
scope for improvement in various components of the programme.
PROBLEM RECOMMENDATIONS
1.Low case detection- The case
detection had been low in the district
since the implementation of RNTCP.
To improve the case detection,
supervision at DMCs and DOT Centres
should be intensified. MOs at the TUlevels should be trained for MOTC
training and should be held
accountable for supervision. All BMOs
and MOs at PHCs should stress upon
case detection in their monthly
meetings. Community volunteers,
NGOs, ASHAs and AWWs should also
be involved more for this purpose.
2. Trainings- Very few trainings were
conducted in the district in last two
years.
Training of the staff has to be
according to the guidelines. The health
professionals across all strata , have to
be sensitized to proper diagnosis and
treatment of all sputum positive cases.
Skill based training programme are part
of RNTCP strategy. Because of transfers
, promotions and retirements ,
trainings need to be a constant affair.
-3. Inadequate Space and Staff -
Problem of inadequate space was
observed in few centres. Medicines
The DOT centre for administering
treatment should be separate from the
lab so that patients are observed better
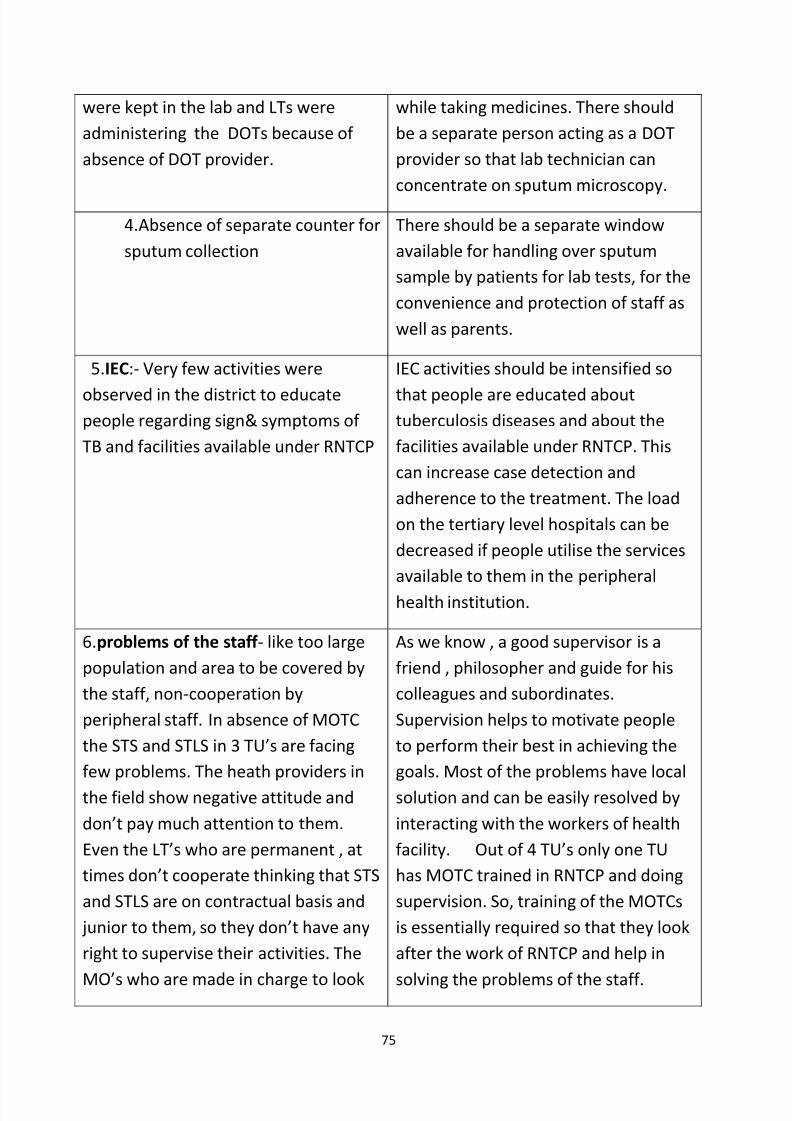
8/4/2019 Global Burden of Tb
http://slidepdf.com/reader/full/global-burden-of-tb 75/79
75
were kept in the lab and LTs were
administering the DOTs because of
absence of DOT provider.
while taking medicines. There should
be a separate person acting as a DOT
provider so that lab technician can
concentrate on sputum microscopy.
4.Absence of separate counter for
sputum collection
There should be a separate window
available for handling over sputum
sample by patients for lab tests, for the
convenience and protection of staff as
well as parents.
5.IEC:- Very few activities were
observed in the district to educatepeople regarding sign& symptoms of
TB and facilities available under RNTCP
IEC activities should be intensified so
that people are educated abouttuberculosis diseases and about the
facilities available under RNTCP. This
can increase case detection and
adherence to the treatment. The load
on the tertiary level hospitals can be
decreased if people utilise the services
available to them in the peripheral
health institution.
6.problems of the staff - like too large
population and area to be covered by
the staff, non-cooperation by
peripheral staff. In absence of MOTC
the STS and STLS in 3 TU’s are facing
few problems. The heath providers in
the field show negative attitude and
don’t pay much attention to them.
Even the LT’s who are permanent , at
times don’t cooperate thinking that STS
and STLS are on contractual basis and
junior to them, so they don’t have any
right to supervise their activities. The
MO’s who are made in charge to look
As we know , a good supervisor is a
friend , philosopher and guide for his
colleagues and subordinates.
Supervision helps to motivate people
to perform their best in achieving the
goals. Most of the problems have local
solution and can be easily resolved by
interacting with the workers of health
facility. Out of 4 TU’s only one TU
has MOTC trained in RNTCP and doing
supervision. So, training of the MOTCs
is essentially required so that they look
after the work of RNTCP and help in
solving the problems of the staff.
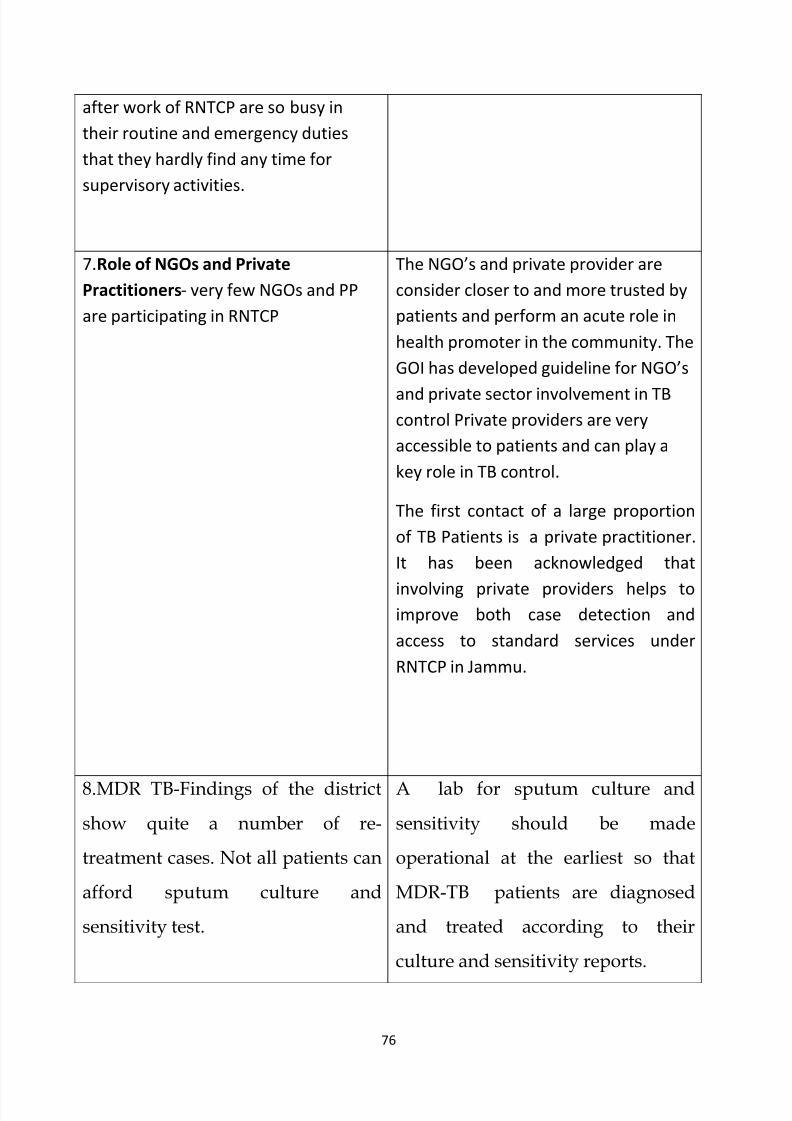
8/4/2019 Global Burden of Tb
http://slidepdf.com/reader/full/global-burden-of-tb 76/79
76
after work of RNTCP are so busy in
their routine and emergency duties
that they hardly find any time for
supervisory activities.
7.Role of NGOs and Private
Practitioners- very few NGOs and PP
are participating in RNTCP
The NGO’s and private provider are
consider closer to and more trusted by
patients and perform an acute role in
health promoter in the community. The
GOI has developed guideline for NGO’s
and private sector involvement in TBcontrol Private providers are very
accessible to patients and can play a
key role in TB control.
The first contact of a large proportion
of TB Patients is a private practitioner.
It has been acknowledged that
involving private providers helps toimprove both case detection and
access to standard services under
RNTCP in Jammu.
8.MDR TB-Findings of the district
show quite a number of re-
treatment cases. Not all patients can
afford sputum culture and
sensitivity test.
A lab for sputum culture and
sensitivity should be made
operational at the earliest so that
MDR-TB patients are diagnosed
and treated according to their
culture and sensitivity reports.
8/4/2019 Global Burden of Tb
http://slidepdf.com/reader/full/global-burden-of-tb 77/79
77
9.TB/HIV Collaboration
REFERENCES
Agarwal, S. P., and Chauhan, L. S. (2005). "Tuberculosis Control in India,"Directorate
General of Health Services, Ministry of Health and Family Welfare, New Delhi.
Ahlburg, D. A. (2000). The economic impacts of tuberculosis.Bajpai, N. (2003). "India: Towards the Millennium Development Goals." UnitedNationsDevelopment Programme.
Bajpai, N., and Goyal, S. (2004). Primary Health Care in India: Coverage andQualityIssues
CentralTB Division (2000). "Operational Guidelines for Tuberculosis Control."
CentralTB Division, Directorate General of Health Services, New Delhi.
Central TB Division (2001). "TB India 2001: RNTCP Status Report."
DirectorateGeneral of Health Services, Ministry of Health and Family Welfare,New Delhi.
Central TB Division (2002). "TB India 2002: RNTCP Status Report.".
Central TB Division (2003). "TB India 2003: RNTCP Status Report."
Central TB Division (2005). "RNTCP Performance Report, India: 2005."Directorate General of Health Services, Ministry of Health and FamilyWelfare, New Delhi.
8/4/2019 Global Burden of Tb
http://slidepdf.com/reader/full/global-burden-of-tb 78/79
78
Das Gupta, M., Khaleghian, P., and Sarwal, R. (2003). "Governance of CommunicableDisease Control Services," Rep. No. 3100. World Bank,Washington, DC.
Deogaonkar, M. (2004). Socio-economic inequality and its effect on healthcaredeliveryin India: Inequality and healthcare. Electronic Journal of Sociology.
Dholakia, R., and Almeida, J. (1996). "The potential economic benefits of theDOTSstrategy against TB in India." World Health Organization, Geneva.Frieden, T. R., Sterling, T. R., Munsiff, S. S., Watt, C. J., and Dye, C. (2003).Tuberculosis. The Lancet 362, 887-899.Global Alliance for TB Drug Development (2001). "The Economics of TB DrugDevelopment." Global Alliance for TB Drug Development, New York.
Gupta, D. (2005). "Covering a billion with DOTS: My Experience with India'sRevised TB Control Programme (1998-2004)," Delhi.Understanding Political Incentives for Providing Public Services. The World
BankResearch Observer 20, 1-27.
Khatri, G. R., and Frieden, T. R. (2002). Controlling Tuberculosis in India.
Rajeswari, R., Balasubramanian, R., Muniyandi, M., Geetharamani, S., Thresa,
X., andVenkatesan, P. (1999). Socio-economic impact of tuberculosis on patientsandfamily in India. International Journal of Tuberculosis and Lung Disease 3,869-Seshadri, S. R. (2003). Constraints to scaling-up health programmes: Acomparativestudy of two Indian states. Journal of International Development 15,101-114.Chandersekran, V.Gopi (2002) Indian journal of Tuberculosis.(2005)
Paramasivam and C.N Narang. (Indian journal of Tuberculosis)
A.Mishra and S.Mishra NTI Banaglore Bulletin 2007.
World Health Organization (2000). "Joint Tuberculosis Programme Review:India."
World Health Organization (2003). "Treatment of tuberculosis: guidelines fornationalprogrammes," 3rdWorld Health Organization (2005a).
"Global tuberculosis control: surveillance, planningfinancing." World HealthOrganization, Geneva.

8/4/2019 Global Burden of Tb
http://slidepdf.com/reader/full/global-burden-of-tb 79/79
World Health Organization (2005b). "Tuberculosis: Fact Sheet No. 104." WorldHealthOrganization, Geneva.