Address for correspondence:
J. RICHELME,25 boulevard Victor-Hugo,06000 [email protected]
DOI: 10.1051/odfen/2012207 J Dentofacial Anom Orthod 2012;15:307� RODF / EDP Sciences
1
C L I N I C A L C A S E S
Esthetics and pre-prostheticorthodontic treatment. Three clinicalcases.
Jean RICHELME
We have long considered pre-prosthetictreatment plans an integral part of ourtherapeutic arsenal. In fact, orthodonticsoffers many possible types of prosthesesto improve treatment and to help ensurelong-term results.
Esthetically speaking, the appearance ofthe gingiva plays an absolutely critical role inoverall esthetic perception, a fortiori forpatients whose smile line is average orhigh. In these cases, having healthy gingivadoes not in and of itself guarantee thatorthodontic rehabilitation will be successful.
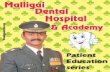
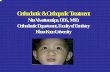
Ideally, when someone smiles, the line ofthe necks of the teeth is parallel to both theplane of occlusion and the horizontal refer-ence lines: the bi-commissural line and thebi-pupillary line (fig. 1 and 2).
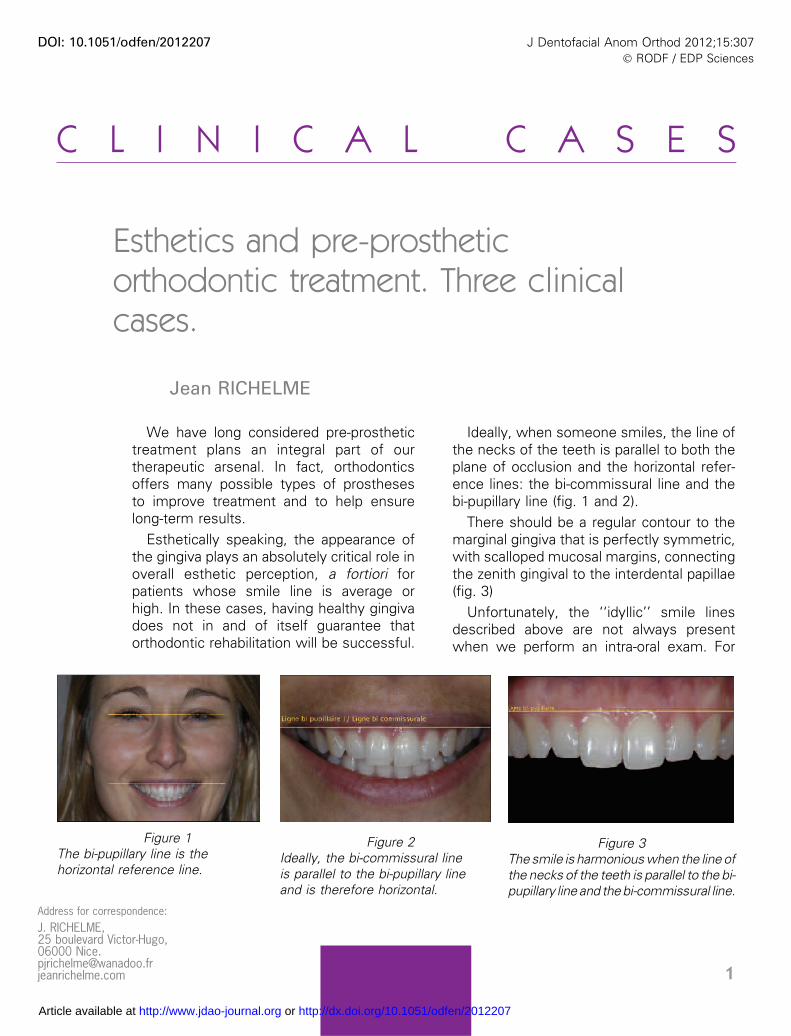
There should be a regular contour to themarginal gingiva that is perfectly symmetric,with scalloped mucosal margins, connectingthe zenith gingival to the interdental papillae(fig. 3)
Unfortunately, the ‘‘idyllic’’ smile linesdescribed above are not always presentwhen we perform an intra-oral exam. For
Figure 1The bi-pupillary line is thehorizontal reference line.
Figure 2Ideally, the bi-commissural lineis parallel to the bi-pupillary lineand is therefore horizontal.
Figure 3The smile is harmonious when the line ofthe necks of the teeth is parallel to the bi-pupillary line and the bi-commissural line.
Article available at http://www.jdao-journal.org or http://dx.doi.org/10.1051/odfen/2012207
patients with an average or high‘‘gummy’’ smile, any irregularity inthe alignment of the gingival marginsand/or the absence of interdentalpapillae may present a noticeablecosmetic imperfection.
When the above gingival defectspresent, we can often improve theesthetics of these patients in a mini-mally invasive and ‘‘elegant’’ mannerby performing a few judiciously cho-sen vertical movements of the mis-aligned teeth.
Patients can present several simplesituations:– the line of the necks of the teeth is
not harmonious because of theexcessively apical position of oneor two teeth, and, in this case,mucogingival surgery cannot cor-rect it or is insufficient to correct it;
– one of the incisive-canine groupoccasionally presents an absenceof papillae;
– the line of the necks of the teethhas an ideal gingival architecture,but one of the teeth (strategic) is
severely decayed and requiresa crown lengthening, that in thelong term, would modify thearchitecture.In these three situations, a general
practitioner, with some fairly simpleorthodontic traction, can for the mostpart find a solution to these estheticproblems that affect the gingiva.
In this article, we are going toillustrate treatment for these gingivaldefects by presenting three clinicalcases.
Orthodontic materials have evolvedand have simplified orthodontic prac-tice because of technical featuressuch as the Ni-Ti� orthodontic wirewith shape memory.
We can now avoid the drudgery ofwire bending that the general practi-tioner is not even trained to dobecause it takes just a single proce-dure to reposition a tooth by usingshape memory wire that contains allthe pre-programmed prescription forthe individual patient.
1 – METHOD
For these ‘‘mini orthodontic treat-ments’’, we use NiTi wire (16 mmdiameter), pre-programmed to beadapted to the shape of the arch. Wegenerally only use a part of the arch,i.e. about two to three teeth on eitherside of the misaligned tooth.
‘‘Homemade’’ attachments arebent and bonded to the labial facesof the placeholder teeth with a flow-able orthodontic composite.
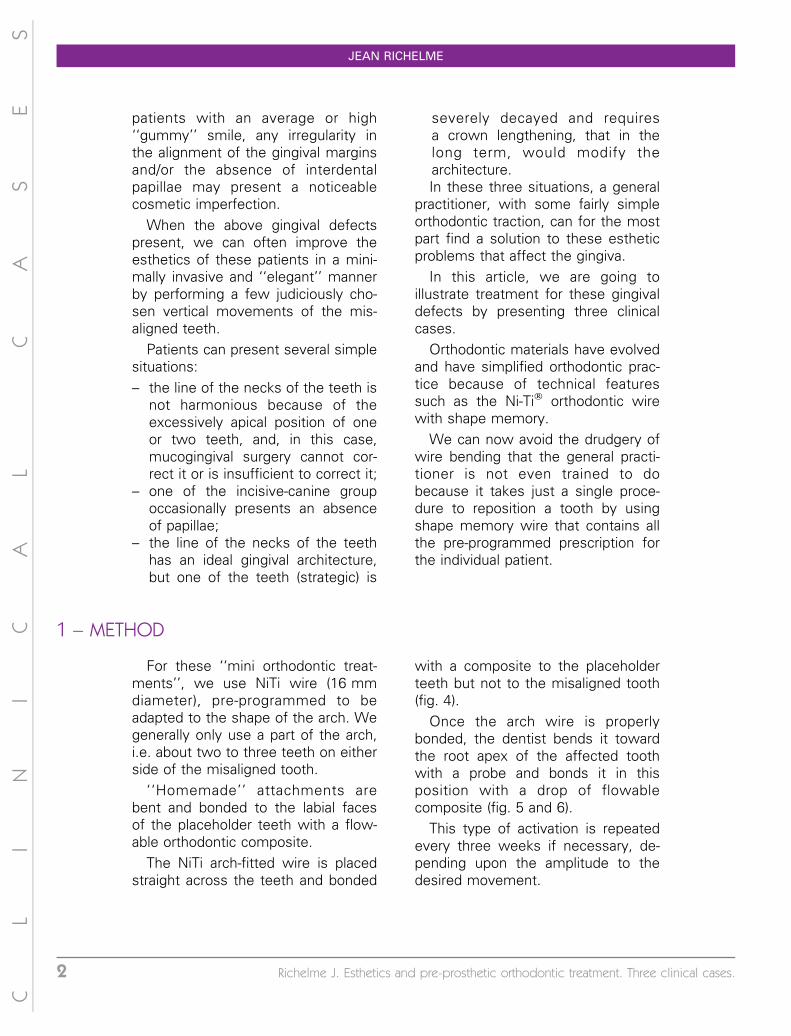
The NiTi arch-fitted wire is placedstraight across the teeth and bonded
with a composite to the placeholderteeth but not to the misaligned tooth(fig. 4).
Once the arch wire is properlybonded, the dentist bends it towardthe root apex of the affected toothwith a probe and bonds it in thisposition with a drop of flowablecomposite (fig. 5 and 6).
This type of activation is repeatedevery three weeks if necessary, de-pending upon the amplitude to thedesired movement.
CL
IN
IC
AL
CA
SE
S
JEAN RICHELME
2 Richelme J. Esthetics and pre-prosthetic orthodontic treatment. Three clinical cases.
These dental movements effect are-shaping of the osseous structureand therefore of the periodontal line,modifying the height and alignment ofthe critical gingival scallops.
In the particular case of restoringseverely decayed strategic teeth, we
do not always wish to modify thegingival structure.
In this situation, each activation isaccompanied by an intrasulcular inci-sion into the supracrestal fibers inorder to extrude the tooth withoutdisplacing the periodontal margin.
2 – CLINICAL CASES
2 – 1 – First clinical situation
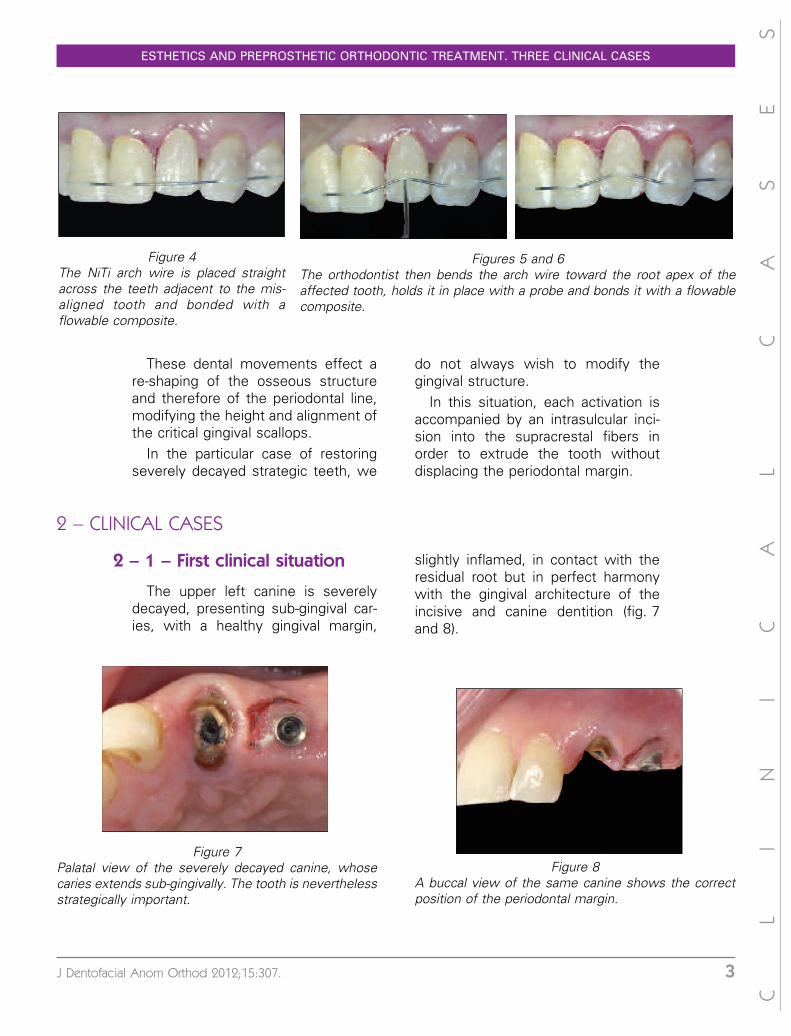
The upper left canine is severelydecayed, presenting sub-gingival car-ies, with a healthy gingival margin,
slightly inflamed, in contact with theresidual root but in perfect harmonywith the gingival architecture of theincisive and canine dentition (fig. 7and 8).
CL
IN
IC
AL
CA
SE
S
Figures 5 and 6The orthodontist then bends the arch wire toward the root apex of theaffected tooth, holds it in place with a probe and bonds it with a flowablecomposite.
Figure 4The NiTi arch wire is placed straightacross the teeth adjacent to the mis-aligned tooth and bonded with aflowable composite.
Figure 7Palatal view of the severely decayed canine, whosecaries extends sub-gingivally. The tooth is neverthelessstrategically important.
Figure 8A buccal view of the same canine shows the correctposition of the periodontal margin.
ESTHETICS AND PREPROSTHETIC ORTHODONTIC TREATMENT. THREE CLINICAL CASES
J Dentofacial Anom Orthod 2012;15:307. 3
Saving this canine is crucial, andfortunately, the relationship of thecrown to the root is very favorable. Asurgical elongation of the tooth crownmight save this vulnerable canine.
Unfortunately, it would entail anunsightly modification to the gingivalarchitecture. The surgical elongationtechnique could be applied to theentire anterior dentition to minimizethe negative impact on the canine butonce again the surgery is not appro-priate since it is aggressive andesthetically risky.
The dentist could also decide tointrude this tooth using orthodonticpressure: the periodontium will movewith the tooth. Then, the increase inperiodontal height that results fromthe movement will be reduced byusing surgical elongation that shouldrestore the initial harmony of the smileline.
The use of orthodontic pressure, alongtime part of our practice, can bemodified to avoid surgical interven-tion.
The strategy is specific to thiscondition: move the tooth not theperiodontium, thus creating a true
coronary elongation that is non-surgi-cal. To do this, we made a temporarycrown attached with an intra-radicularpost embedded in the residual rootand temporary crowns on the poster-ior implants. We placed a NiTi wirepassively between the crowns on theimplants and the incisors.
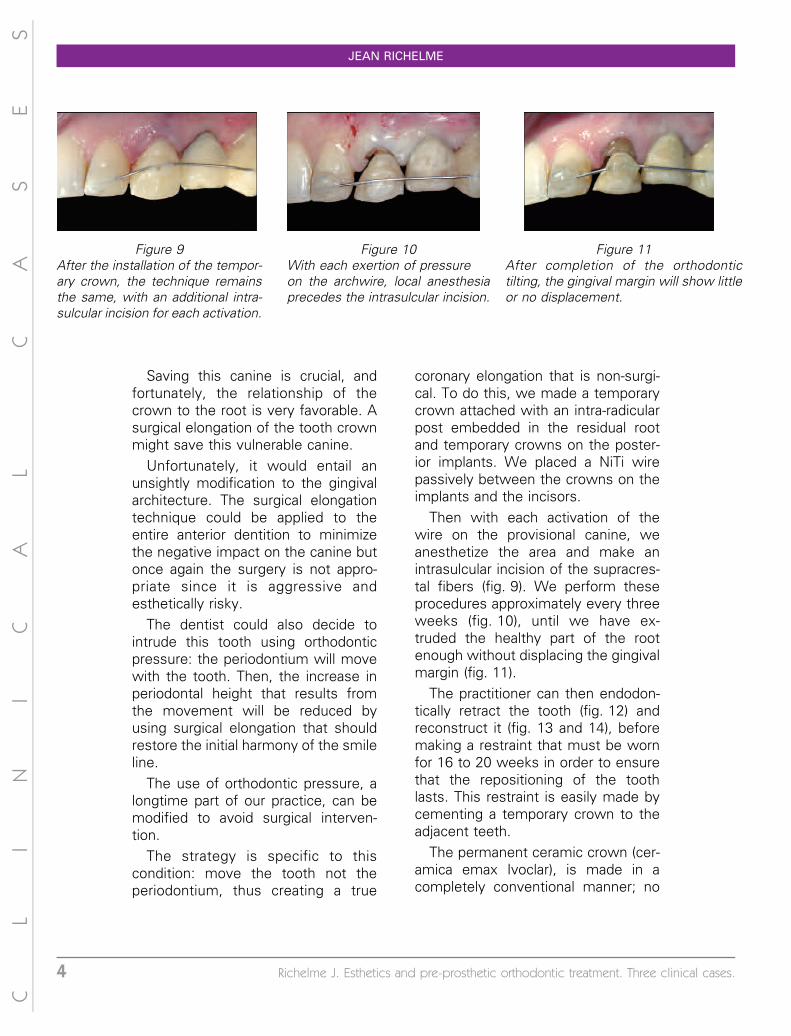
Then with each activation of thewire on the provisional canine, weanesthetize the area and make anintrasulcular incision of the supracres-tal fibers (fig. 9). We perform theseprocedures approximately every threeweeks (fig. 10), until we have ex-truded the healthy part of the rootenough without displacing the gingivalmargin (fig. 11).
The practitioner can then endodon-tically retract the tooth (fig. 12) andreconstruct it (fig. 13 and 14), beforemaking a restraint that must be wornfor 16 to 20 weeks in order to ensurethat the repositioning of the toothlasts. This restraint is easily made bycementing a temporary crown to theadjacent teeth.
The permanent ceramic crown (cer-amica emax Ivoclar), is made in acompletely conventional manner; no
CL
IN
IC
AL
CA
SE
S
Figure 11After completion of the orthodontictilting, the gingival margin will show littleor no displacement.
Figure 10With each exertion of pressureon the archwire, local anesthesiaprecedes the intrasulcular incision.
Figure 9After the installation of the tempor-ary crown, the technique remainsthe same, with an additional intra-sulcular incision for each activation.
JEAN RICHELME
4 Richelme J. Esthetics and pre-prosthetic orthodontic treatment. Three clinical cases.
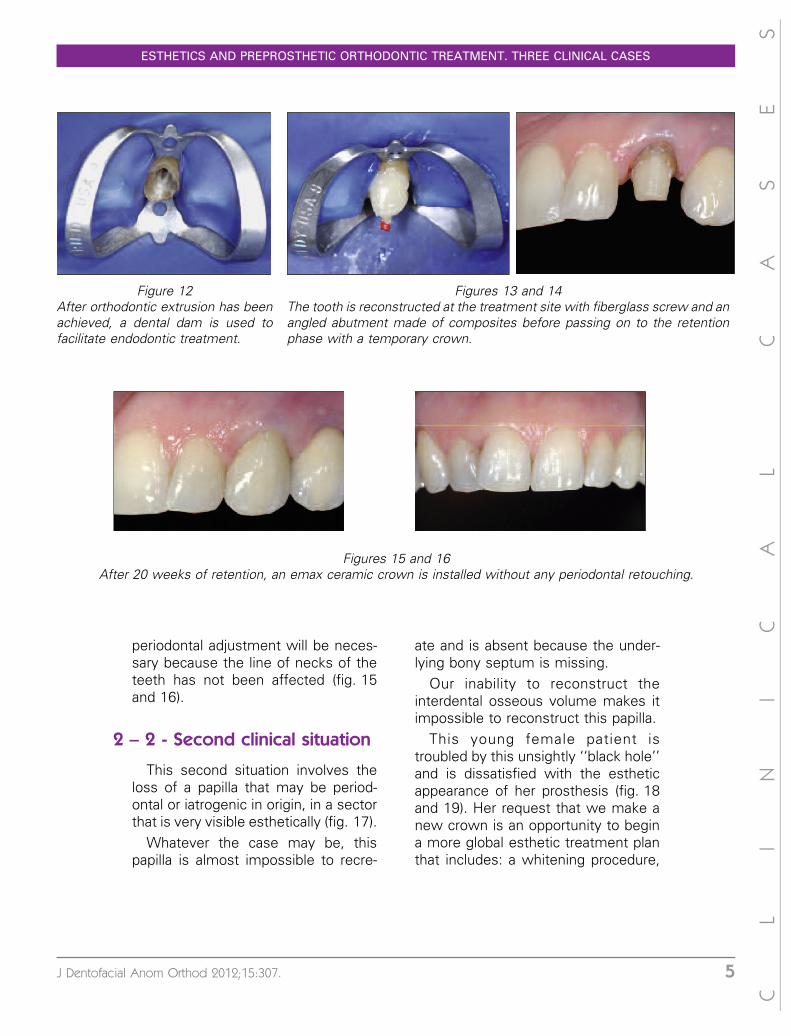
periodontal adjustment will be neces-sary because the line of necks of theteeth has not been affected (fig. 15and 16).
2 – 2 - Second clinical situation
This second situation involves theloss of a papilla that may be period-ontal or iatrogenic in origin, in a sectorthat is very visible esthetically (fig. 17).
Whatever the case may be, thispapilla is almost impossible to recre-
ate and is absent because the under-lying bony septum is missing.
Our inability to reconstruct theinterdental osseous volume makes itimpossible to reconstruct this papilla.
This young female patient istroubled by this unsightly ‘‘black hole’’and is dissatisfied with the estheticappearance of her prosthesis (fig. 18and 19). Her request that we make anew crown is an opportunity to begina more global esthetic treatment planthat includes: a whitening procedure,
CL
IN
IC
AL
CA
SE
S
Figure 12After orthodontic extrusion has beenachieved, a dental dam is used tofacilitate endodontic treatment.
Figures 13 and 14The tooth is reconstructed at the treatment site with fiberglass screw and anangled abutment made of composites before passing on to the retentionphase with a temporary crown.
Figures 15 and 16After 20 weeks of retention, an emax ceramic crown is installed without any periodontal retouching.
ESTHETICS AND PREPROSTHETIC ORTHODONTIC TREATMENT. THREE CLINICAL CASES
J Dentofacial Anom Orthod 2012;15:307. 5
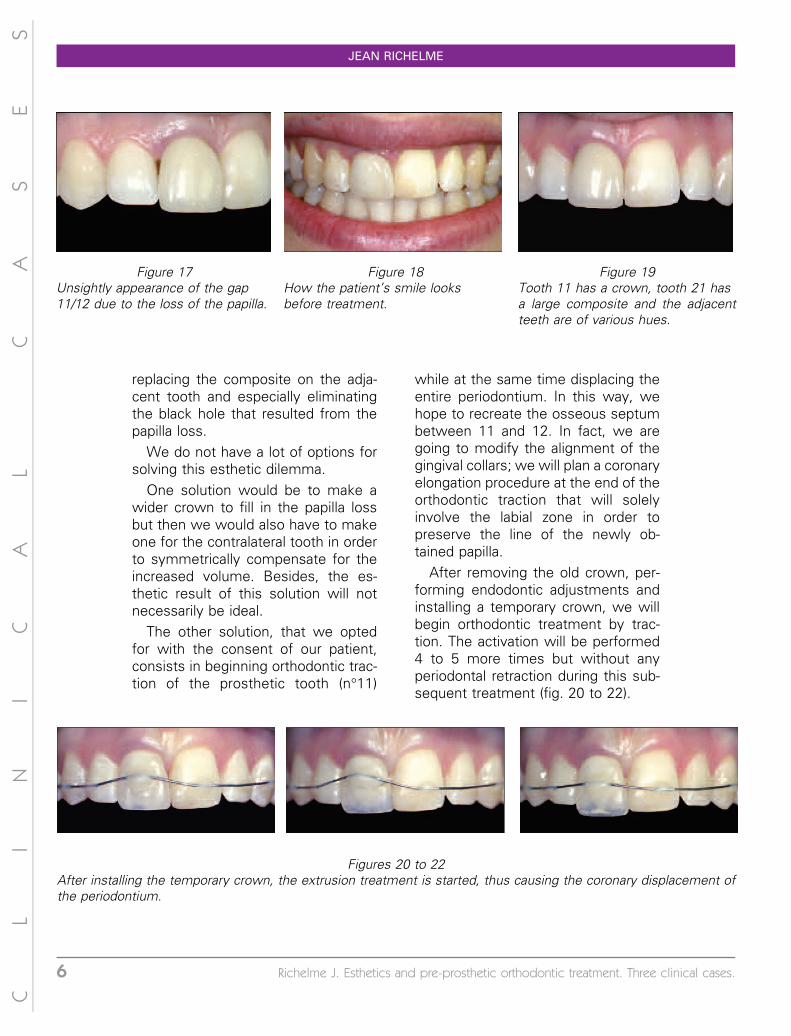
replacing the composite on the adja-cent tooth and especially eliminatingthe black hole that resulted from thepapilla loss.
We do not have a lot of options forsolving this esthetic dilemma.
One solution would be to make awider crown to fill in the papilla lossbut then we would also have to makeone for the contralateral tooth in orderto symmetrically compensate for theincreased volume. Besides, the es-thetic result of this solution will notnecessarily be ideal.
The other solution, that we optedfor with the consent of our patient,consists in beginning orthodontic trac-tion of the prosthetic tooth (n�11)
while at the same time displacing theentire periodontium. In this way, wehope to recreate the osseous septumbetween 11 and 12. In fact, we aregoing to modify the alignment of thegingival collars; we will plan a coronaryelongation procedure at the end of theorthodontic traction that will solelyinvolve the labial zone in order topreserve the line of the newly ob-tained papilla.
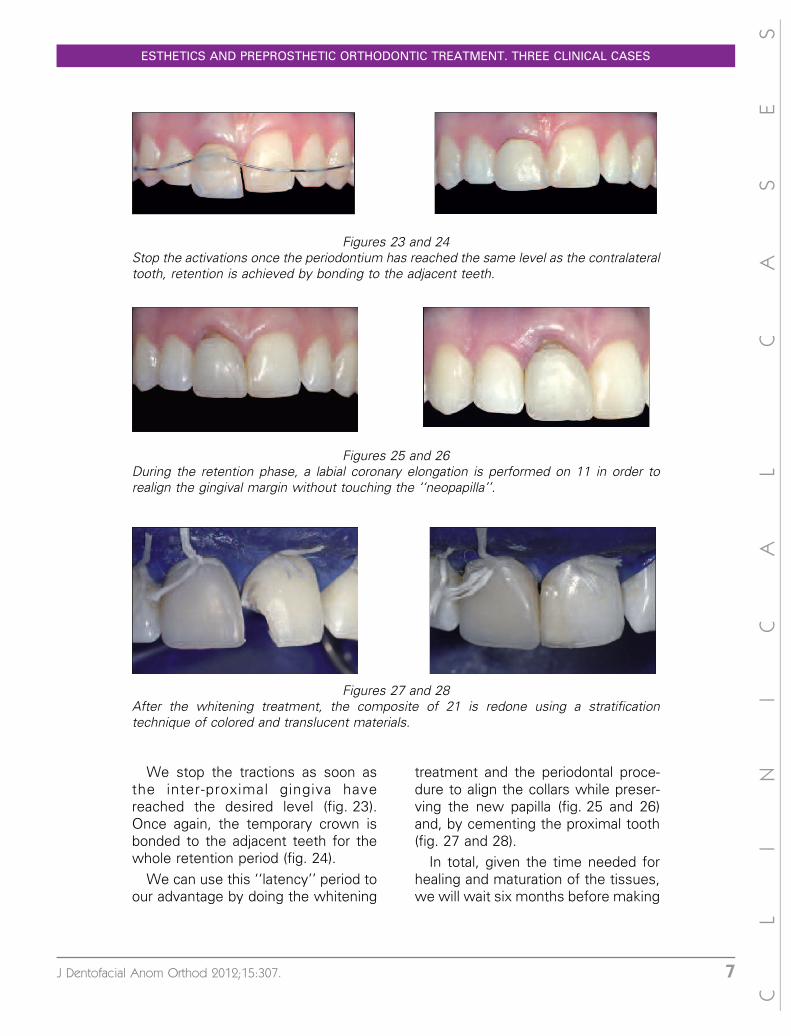
After removing the old crown, per-forming endodontic adjustments andinstalling a temporary crown, we willbegin orthodontic treatment by trac-tion. The activation will be performed4 to 5 more times but without anyperiodontal retraction during this sub-sequent treatment (fig. 20 to 22).
CL
IN
IC
AL
CA
SE
S
Figure 17Unsightly appearance of the gap11/12 due to the loss of the papilla.
Figure 18How the patient’s smile looksbefore treatment.
Figure 19Tooth 11 has a crown, tooth 21 hasa large composite and the adjacentteeth are of various hues.
Figures 20 to 22After installing the temporary crown, the extrusion treatment is started, thus causing the coronary displacement ofthe periodontium.
JEAN RICHELME
6 Richelme J. Esthetics and pre-prosthetic orthodontic treatment. Three clinical cases.
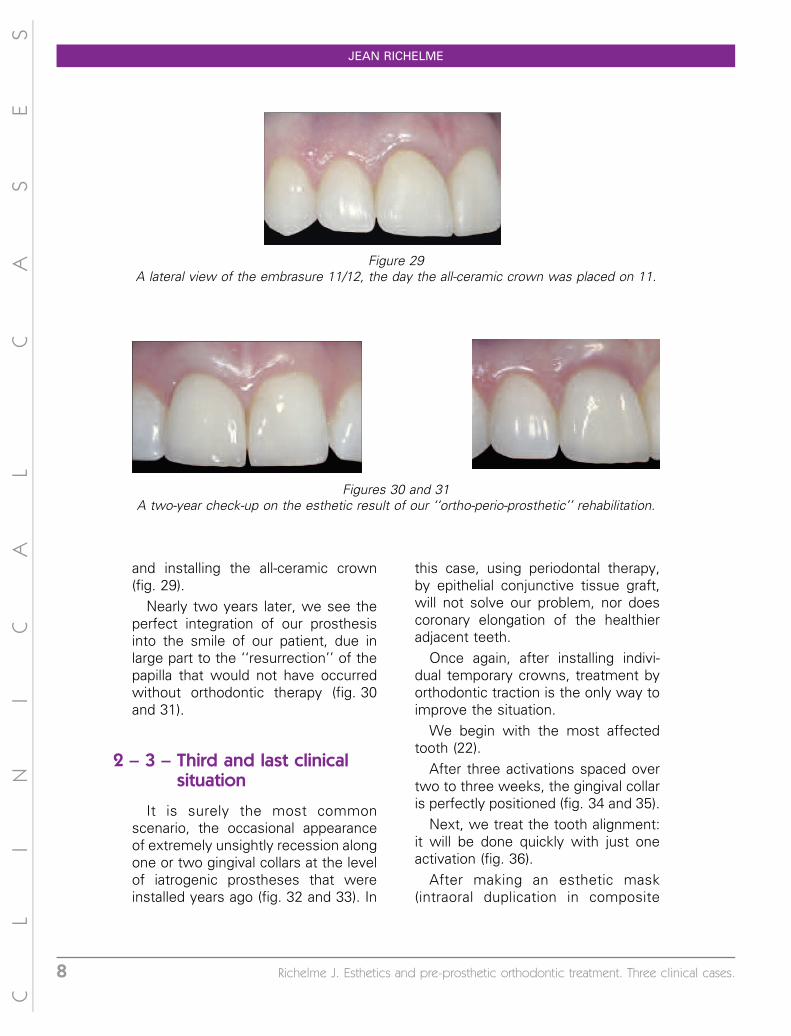
We stop the tractions as soon asthe inter-proximal gingiva havereached the desired level (fig. 23).Once again, the temporary crown isbonded to the adjacent teeth for thewhole retention period (fig. 24).
We can use this ‘‘latency’’ period toour advantage by doing the whitening
treatment and the periodontal proce-dure to align the collars while preser-ving the new papilla (fig. 25 and 26)and, by cementing the proximal tooth(fig. 27 and 28).
In total, given the time needed forhealing and maturation of the tissues,we will wait six months before making
CL
IN
IC
AL
CA
SE
S
Figures 23 and 24Stop the activations once the periodontium has reached the same level as the contralateraltooth, retention is achieved by bonding to the adjacent teeth.
Figures 25 and 26During the retention phase, a labial coronary elongation is performed on 11 in order torealign the gingival margin without touching the ‘‘neopapilla’’.
Figures 27 and 28After the whitening treatment, the composite of 21 is redone using a stratificationtechnique of colored and translucent materials.
ESTHETICS AND PREPROSTHETIC ORTHODONTIC TREATMENT. THREE CLINICAL CASES
J Dentofacial Anom Orthod 2012;15:307. 7
and installing the all-ceramic crown(fig. 29).
Nearly two years later, we see theperfect integration of our prosthesisinto the smile of our patient, due inlarge part to the ‘‘resurrection’’ of thepapilla that would not have occurredwithout orthodontic therapy (fig. 30and 31).
2 – 3 – Third and last clinicalsituation
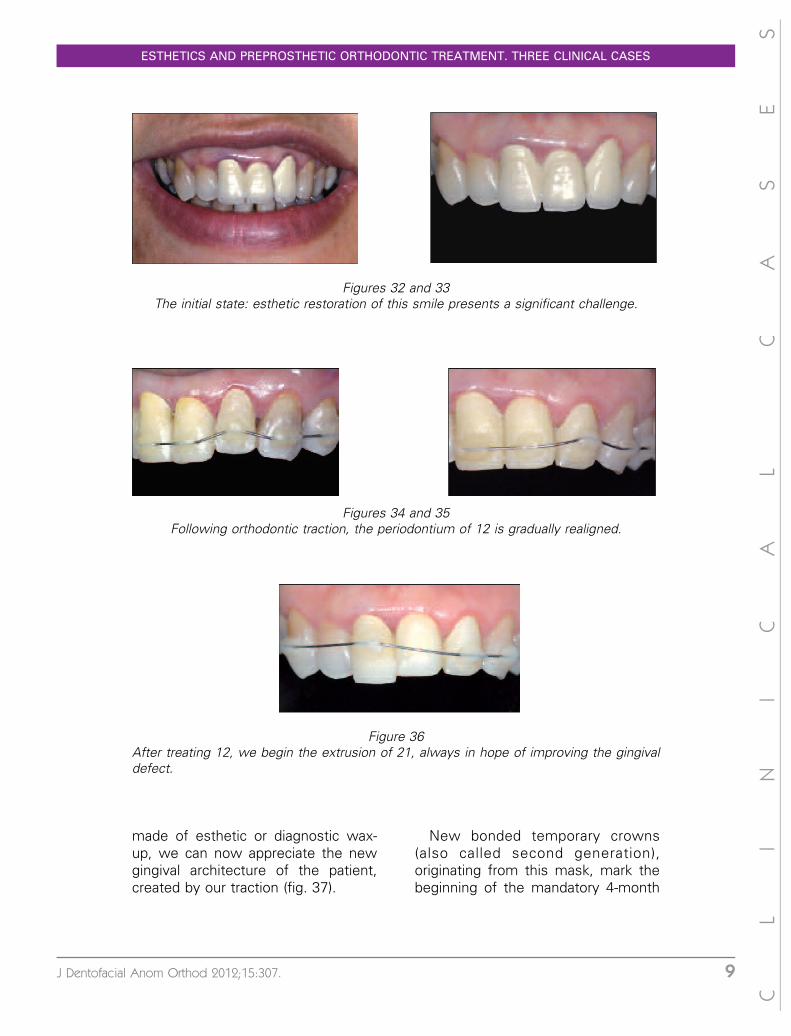
It is surely the most commonscenario, the occasional appearanceof extremely unsightly recession alongone or two gingival collars at the levelof iatrogenic prostheses that wereinstalled years ago (fig. 32 and 33). In
this case, using periodontal therapy,by epithelial conjunctive tissue graft,will not solve our problem, nor doescoronary elongation of the healthieradjacent teeth.
Once again, after installing indivi-dual temporary crowns, treatment byorthodontic traction is the only way toimprove the situation.
We begin with the most affectedtooth (22).
After three activations spaced overtwo to three weeks, the gingival collaris perfectly positioned (fig. 34 and 35).
Next, we treat the tooth alignment:it will be done quickly with just oneactivation (fig. 36).
After making an esthetic mask(intraoral duplication in composite
CL
IN
IC
AL
CA
SE
S
Figure 29A lateral view of the embrasure 11/12, the day the all-ceramic crown was placed on 11.
Figures 30 and 31A two-year check-up on the esthetic result of our ‘‘ortho-perio-prosthetic’’ rehabilitation.
JEAN RICHELME
8 Richelme J. Esthetics and pre-prosthetic orthodontic treatment. Three clinical cases.
made of esthetic or diagnostic wax-up, we can now appreciate the newgingival architecture of the patient,created by our traction (fig. 37).
New bonded temporary crowns(also called second generation),originating from this mask, mark thebeginning of the mandatory 4-month
CL
IN
IC
AL
CA
SE
S
Figures 32 and 33The initial state: esthetic restoration of this smile presents a significant challenge.
Figures 34 and 35Following orthodontic traction, the periodontium of 12 is gradually realigned.
Figure 36After treating 12, we begin the extrusion of 21, always in hope of improving the gingivaldefect.
ESTHETICS AND PREPROSTHETIC ORTHODONTIC TREATMENT. THREE CLINICAL CASES
J Dentofacial Anom Orthod 2012;15:307. 9
retention period, that allows us tovalidate in consultation with the pa-tient the new alignment of her teeth(fig. 38).
After attempting to whiten theadjacent teeth that improves only theocclusal first half, the defect will berehabilitated by installing three all-
CL
IN
IC
AL
CA
SE
S
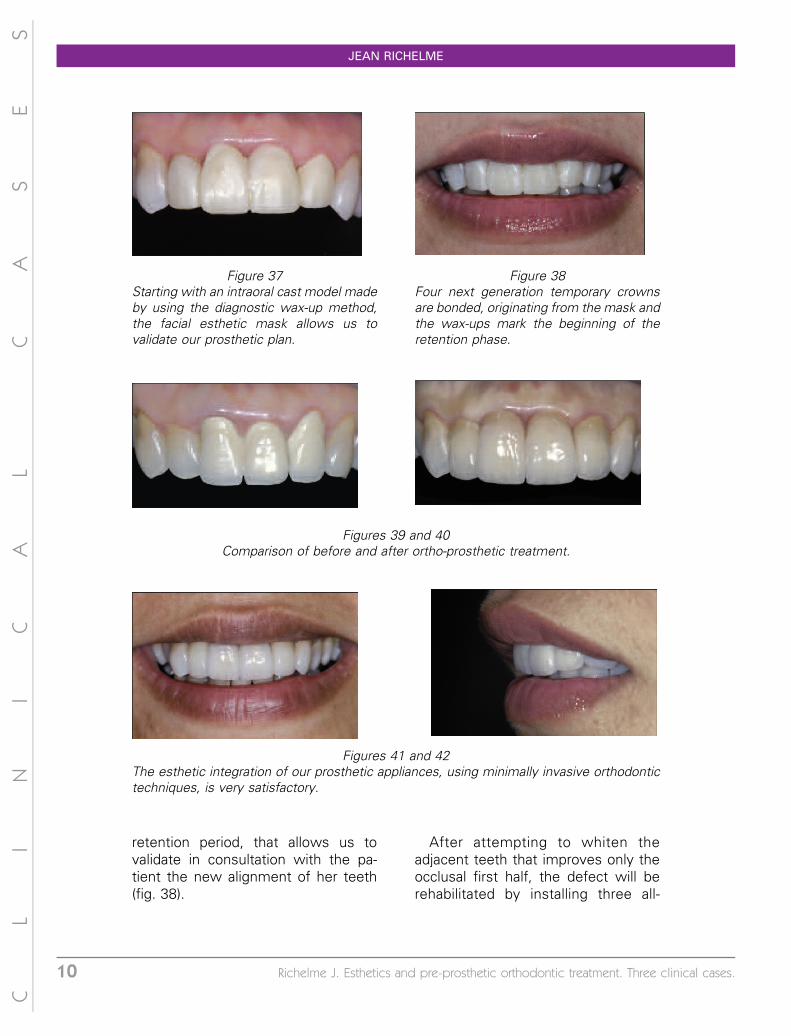
Figure 37Starting with an intraoral cast model madeby using the diagnostic wax-up method,the facial esthetic mask allows us tovalidate our prosthetic plan.
Figure 38Four next generation temporary crownsare bonded, originating from the mask andthe wax-ups mark the beginning of theretention phase.
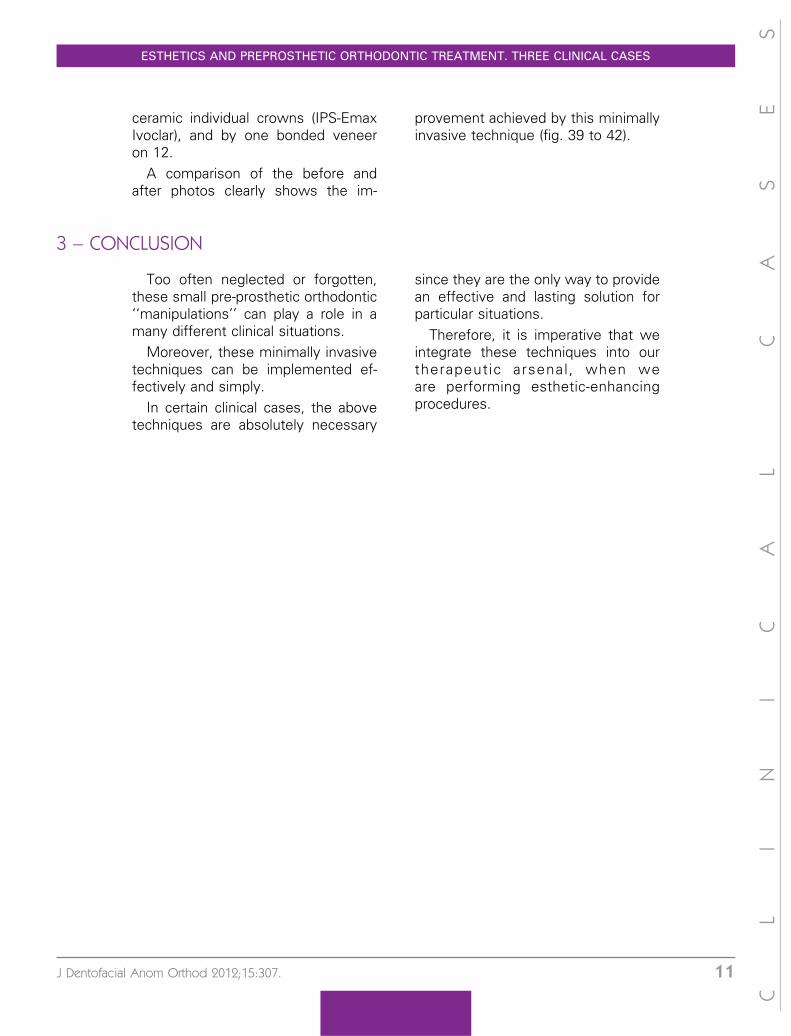
Figures 39 and 40Comparison of before and after ortho-prosthetic treatment.
Figures 41 and 42The esthetic integration of our prosthetic appliances, using minimally invasive orthodontictechniques, is very satisfactory.
JEAN RICHELME
10 Richelme J. Esthetics and pre-prosthetic orthodontic treatment. Three clinical cases.
ceramic individual crowns (IPS-EmaxIvoclar), and by one bonded veneeron 12.
A comparison of the before andafter photos clearly shows the im-
provement achieved by this minimallyinvasive technique (fig. 39 to 42).
3 – CONCLUSION
Too often neglected or forgotten,these small pre-prosthetic orthodontic‘‘manipulations’’ can play a role in amany different clinical situations.
Moreover, these minimally invasivetechniques can be implemented ef-fectively and simply.
In certain clinical cases, the abovetechniques are absolutely necessary
since they are the only way to providean effective and lasting solution forparticular situations.
Therefore, it is imperative that weintegrate these techniques into ourtherapeutic arsenal , when weare performing esthetic-enhancingprocedures.
CL
IN
IC
AL
CA
SE
S
ESTHETICS AND PREPROSTHETIC ORTHODONTIC TREATMENT. THREE CLINICAL CASES
J Dentofacial Anom Orthod 2012;15:307. 11