Update on Perioperative Medicine Hugo Quinny Cheng, MD Division of Hospital Medicine University of California, San Francisco

Update on Perioperative Medicine Hugo Quinny Cheng, MD Division of Hospital Medicine University of California, San Francisco.
Mar 26, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Update on Perioperative Medicine
Hugo Quinny Cheng, MDDivision of Hospital Medicine
University of California, San Francisco

Update on Perioperative Medicine
1. Who needs a preoperative cardiac stress test?
2. What are the benefits and risks of -blockers?
3. Can statins prevent postoperative MI?
4. When can patients with stents go to the OR?
5. How should chronic anticoagulation be managed?
6. Should arthroscopy patients get DVT prophylaxis?
7. Is preoperative smoking cessation beneficial?

Preoperative Stress Testing
A 65 y.o. man with a history of coronary artery disease and long-standing diabetes will undergo radical prostatectomy. He had a myocardial infarction in 2003, but now has no cardiac symptoms.
Meds: lovastatin, atenolol, glyburide, benazepril, ASA
Exam: BP=115 / 70 HR=60; normal heart & lung exam
ECG: NSR, LVH, otherwise normal

65 y.o. man s/f radical prostatectomy. History of remote MI and long-standing diabetes. He is currently asymptomatic.
1. Stress test prior to surgery
2. No stress test is needed
3. Make him carry a copy of Harrison’s up a flight of stairs

“New Standard” Cardiac Risk Index
Predictors:– Higher risk operation*– Ischemic heart disease– Congestive heart failure– Diabetes requiring insulin– Creatinine > 2 mg/dL– Stroke or TIA
Predictors Complications**
0 0.5%
1 1.3%
2 4%
3 or more 9%
* Defined as intraperitoneal, intrathoracic, or suprainguinal vascular surgery
** Defined as MI, pulmonary edema, cardiac arrest, complete heart block
Lee, et al. Circulation, 1999

2007 ACC/AHA Guideline
Good Functional Capacity? Go to OR yes
≥ 3 predictors1 or 2 predictorsno predictors*
no or ?
Control HR & go to OR (IIa)
Vascular surgery?
Consider stress test if results will change management (IIa)
no
yes
or(IIb)
Go to OR
* CAD, CHF, DM, CKD, CVA/TIA

770 vascular patients with 1 or 2 of following:
Age > 70, MI, angina, CHF, DM, stroke / TIA, Cr > 1.8
Stress test (n = 386)No stress test (n = 384)
34 with extensive ischemia (9%); 12 had PCI or CABG
352 with no or limited ischemia
1.8% 30-day CV Death or MI
2.3%
1.1% 15%
Poldermans et al. JACC, 2006

0%
10%
20%
30%
40%
Revascularization +Medical Mgt
MedicalManagement
Dea
th o
r M
I
Poldermans, et al. JACC, 2007
Extensive Ischemia Predicts High Risk
101 patients undergoing vascular surgery, all with ≥ 3 risk predictors and stress test showing extensive ischemia

Reducing Risk with Medical Management
A 75 y.o. woman will undergo hemicolectomy next week. She has a history of diabetes and a remote stroke, but no current cardiovascular symptoms.
1. Start a -blocker
2. Start a statin
3. Start both -blocker & statin
4. No new medications needed

- 111 patients undergoing vascular surgery - All had ischemic potential on dobutamine echo- Randomized to beta-blocker or standard care
Poldermans, et al. NEJM, 1999
40
Cardiac
Mortality &
Nonfatal MI
(%)
7 14 21 28
10
20
30
Days after Surgery
Bisoprolol
Standard Care

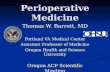
POISE: PeriOperative Ischemia Evaluation
8351 patients with s/f major noncardiac surgery• CAD, CHF, CVA/TIA, CKD, DM, or high-risk surgery• Not already taking -blocker
Metoprolol XL (immediately preop until 30 days postop)
Placebo
Patients followed for 30 days after surgery:
1° Endpoint: cardiac mortality & nonfatal arrest or MI
Poise Study Group. Lancet, 2008

POISE: Results
6.9%
2.3%
5.8%
3.1%
0%
1%
2%
3%
4%
5%
6%
7%
8%
CV Death, CardiacArrest, Nonfatal MI
Total Mortality
Placebo
Metoprolol XL
Metoprolol XL:Reduced cardiac events (mostly nonfatal MI)
but
Increased risk of stroke & total mortality
Poise Study Group. Lancet, 2008

POISE: Treatment Protocol
2-4 h
1st dose Metoprolol 100 mg XL*
2nd dose
Metoprolol 100 mg XL*
3rd & daily dose Metoprolol 200 mg XL*^
OR 0-6 h 12 h
* Study drug held for SBP < 100 or HR < 50^ Daily dose reduced to 100 mg if persistent bradycardia or hypotension

DECREASE III
497 statin naive patients s/f vascular surgery
Fluvastatin XL 80 mg/day• Started > 1 month preop• Continued > 1 mo postop
Placebo
Patients followed for 30 days after surgery:
Clinical Endpoint: cardiac death or nonfatal MI
Poldermans et al. Presented at ESC, 2008

DECREASE III: Results
10.1%
4.8%
0%
5%
10%
15%
20%
Cardiac Death or MI
Placebo
Fluvastatin XL
Fluvastatin XL:Reduced the composite outcome of cardiac death & nonfatal MI
No difference in rates of LFT or CPK elevation
Poldermans et al. Presented at ESC, 2008

DECREASE-IV
• 1066 patients with estimated 1-6% risk of postoperatived cardiac complications
• Randomized to: Bisoprolol
Fluvastatin XL
Bisoprolol + Fluvastatin
Double placebo• Drugs started average 34 days prior to surgery
• Primary endpoint: 30-day CV death or nonfatal MI

DECREASE-IV Results
Bisoprolol-treated patients had fewer complications
Trend towards benefit with statins
No safety issues
* *
* P < .002
Dunkelgrun et al. Ann Surg, 2009

Perioperative -blockers in 2009
Strong indications:• Already using -blocker to treat angina, HTN, arrhythmia• Patients with ischemic potential having vascular surgery
Possible indications:• Patients with ischemic potential having high-risk nonvascular
surgery (e.g., > 5 hours or > 500 cc blood loss)• Multiple risk predictors* in vascular or other high-risk surgery
(*Coronary disease, renal insufficiency, diabetes)
Titrate dose up gradually (rarely start immediately preop)

Statins: 2007 ACC/AHA Guideline
Definite indications (class I):• Continue statin if already taking prior to surgery
Probable indications (class IIa):• All vascular surgery patients
Possible indications (class IIb):• At least one risk predictor* in any intermediate risk surgery
*Coronary disease, renal insufficiency, diabetes, CVA/TIA

Delaying Surgery After Coronary Stent
A woman falls and suffers a cervical spine fracture. One month ago, she received a sirulimus-eluting stent for stable angina. The neurosurgeon won’t operate unless aspirin and clopidogrel are held for her surgery. Non-operative management in a halo for next 2 months is offered as an alternative.
What do you recommend to the patient & surgeon?

Patient with recently placed drug-eluting stent has a c-spine fracture. Surgeon won’t operate unless aspirin & clopidogrel are held perioperatively.
1. Hold ASA & clopidogrel
2. Hold ASA & clopidogrel but bridge with heparin
3. Keep her in a halo for next 2 months

Does Heparin Bridge Prevent Stent-related
Complications?
Prospective study of 103 patients with coronary stent placed within 12 months having noncardiac surgery• Antiplatelet drugs continued or held < 3 days• All patients received heparin drip or enoxaparin
14% of patient stented within 35 days of surgery suffered cardiac death or MI, or needed re-do PCI
Conclusion: High rate of cardiac complications even when bridging anticoagulants used
Vicenzi et al. Br J Anaesth, 2006

ACC/AHA Guidelines for PCI
• Avoid PCI unless patient has independent indications• Avoid PCI if patient may have upcoming surgery that
requires stopping dual antiplatelet therapy• Delay elective surgery in patients with recent PCI
– Balloon angioplasty: 2 - 4 weeks– Bare metal stent: 4 weeks– Drug eluting stent: 12 months
• If clopidogrel must be stopped, try to continue ASA• No evidence for bridging with other agents

Managing Perioperative Anticoagulation
Two patients who take coumadin underwent THA. One has atrial fibrillation due to HTN. The other has a mechanical AVR. Neither has a history of stroke or any other comorbidity.
1. Heparin bridge for AVR only
2. Heparin bridge for AF only
3. Heparin bridge for both
4. Heparin bridge for neither

Two patients who take coumadin underwent THA. One has AF due to HTN. The other has a mechanical AVR. Neither has a history of stroke any other comorbidity.
1. Heparin bridge for AVR only
2. Heparin bridge for AF only
3. Heparin bridge for both
4. Heparin bridge for neither

Thromboembolic Risks with Non-rheumatic Atrial Fibrillation
0%
1%
2%
3%
4%
5%
6%
7%
Without Coumadin With Coumadin
Ann
ual S
trok
e R
isk
Albers et al. Chest, 2001
CHADS-2 Score:
1 point for CHF, HTN, Age > 75, DM
2 points for Stroke/TIA
Score 0 - 2: < 5% annual stroke risk Score 3 - 4: 5-10%
Score 5 - 6: > 10%

Thromboembolic Risks with Mechanical Valves
0%
1%
2%
3%
4%
5%
6%
7%
Without Coumadin With Coumadin
Valve Thrombosis
Embolism
Ann
ual I
ncid
ence
Cannegieter, et al. Circulation, 1994

Effect of Mechanical Valve Location & Design on Thromboembolic Risk
Valve Location:
Aortic RR = 1.0
Mitral RR = 1.8
Valve Design:
Caged Ball RR = 1.0
Tilting Disk RR = 0.7
Bi-leaflet RR = 0.6
Cannegieter, et al. Circulation, 1994

Perioperative Anticoagulation: 2008 ACCP Guidelines
Atrial Fibrillation Mechanical Valve Recommend
CHADS2 = 5-6, recent CVA, or rheumatic AF
Any MVR; older (caged-ball or tilting disc) AVR; recent CVA
Full dose heparin bridge
CHADS2 = 3-4 Bileaflet AVR plus one additional stroke risk factor
Full or low dose heparin
CHADS2 = 0-2 Bileaflet AVR without AF or other stroke risk factor
Low dose or no heparin
Full dose = therapeutic dose of heparin IV or LMWH SC
Low dose = DVT prophylaxis dose of heparin SC or LMWH SC

DVT Prophylaxis
Which DVTs matter?• Symptomatic versus asymptomatic • Proximal versus distal
2008 American College of Chest Physicians:• Weights DVT risk greater than bleeding risk• Treats asymptomatic DVT as important

RCT of LMWH in Knee Arthroscopy
Background: 2008 ACCP guidelines recommend LMWH if additional risk factors for DVT are present.
Study Design: ~1300 patients randomized to compression hose or LMWH x 7 days after knee arthroscopy. All patients underwent screening ultrasound.
Results: Combined incidence of death or any clot reduced in patients receiving LMWH (0.9% vs 3.2%). Almost all clots were either asymptomatic or distal. Non-significant trend for increased bleeding.
Conclusions: LMWH superior to compression hose after knee arthroscopy (NNT = 43). Impact on symptomatic DVT small.
Camporese et al. Ann Intern Med, 2008.

Preoperative Smoking Cessation
A middle-aged man will undergo repair of a ventral hernia in 1 month. He currently smokes one pack of cigarettes per day. How do you counsel him?
1. Quit smoking now to prevent postoperative complications.
2. It’s always good to quit, but it’s too late to affect your risk of complications.
3. Don’t stop smoking! You will actually increase your surgical risk by quitting!

Effect of Smoking Cessation
0 10 20 30 40 50 60 70
Nonsmokers
8 or more weeks
4 - 8 weeks
2 - 4 weeks
Less than 2 weeks
Never quit
Complication Rate (%)
Time since quitting
p < .001
Warner, Anesthesiology 1984

Preoperative Smoking Cessation Counseling
RCTs of Preoperative Smoking Cessation Counseling:1. 120 patients undergoing arthroplasty in 6-8 weeks
2. 117 patients undergoing various operations in 4 weeks
3. 60 patients undergoing colorectal resection in 2-3 weeks
Intervention: Smoking cessation counseling at weekly meetings (or by telephone) & offer free nicotine replacement products
Outcomes: Postop complications, especically wound related (e.g., dehiscence, infection, hematoma)

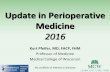
7%
31%
52%
83%
5%
18%
0%
20%
40%
60%
80%
100%
Quit or ReducedSmoking
WoundComplication
Any Complication
Control
Intervention
Smoking Cessation 6-8 Weeks Before TKA or THA
Moller et al. Lancet, 2002

26%
41%
13%
21%
0%
10%
20%
30%
40%
50%
Wound Complication Any Complication
Control
Intervention
Lindstrom et al. Ann Surg, 2008.
Smoking Cessation 4 Weeks Before Surgery

13%
27%
43%
89%
33%41%
0%
20%
40%
60%
80%
100%
Quit or ReducedSmoking
WoundComplication
Any Complication
Control
Intervention
Sorensen, et al. Colorectal Dis, 2003
Smoking Cessation 2-3 Weeks Before Colorectal Surgery

Take Home Points
• Reserve stress testing for higher risk patients
-- Limited ischemia ok, but extensive ischemia = high risk
• Start -blocker cautiously & only in high risk patients
• Delay surgery in patients with recent stent placement
• Individualize thrombotic risk assessment when managing perioperative anticoagulation
• Consider LMWH for knee arthroplasty patients
• Smoking cessation for ≥ 4 weeks may be beneficial
Related Documents