Tuberculosis, its epidemiology & current situation.
Jan 20, 2016
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript


Tuberculosis,Tuberculosis,its epidemiology & its epidemiology &
current situationcurrent situation
Tuberculosis,Tuberculosis,its epidemiology & its epidemiology &
current situationcurrent situation

Causal Causal AgentAgentCausal Causal AgentAgent
- - Mycobacterium tuberculosisMycobacterium tuberculosis ccomplexomplex
- - M. tuberculosisM. tuberculosis - M. bovis- M. bovis - M. africanum- M. africanum - M. microti- M. microti - M. caneti- M. caneti - M. pinnipedii- M. pinnipedii - M. caprae- M. caprae

- Slow and Little Alarmant- Slow and Little AlarmantClinical Clinical PresentationPresentation
- Excessive - Excessive Delay Delay to Consult the HCto Consult the HC
- Very Late Diagnosis- Very Late Diagnosis
LongLong time to be contagious when the Cases are Diagnosed time to be contagious when the Cases are Diagnosed
- M. tuberculosis delay - M. tuberculosis delay 16-24 h16-24 h. to be divided. to be divided (60 < Estafiloc.) (60 < Estafiloc.)
Very Slow Very Slow Division CapacityDivision CapacityVery Slow Very Slow Division CapacityDivision Capacity
provided by Caminero

Causal AgentCausal Agent
- Mycobacterium tuberculosis complex - Mycobacterium tuberculosis complex
Polyvalent Polyvalent behaviourbehaviour depending depending on medium.on medium.

■ In a tuberculosis patient, there are In a tuberculosis patient, there are different bacillary populationsdifferent bacillary populations formed of formed of bacilli in different situationsbacilli in different situations
- Location- Location
- pH- pH
- Replication rate, susceptibility to drugs, …- Replication rate, susceptibility to drugs, …
Bacillary populationsBacillary populations
provided by Caminero

Bacillary populationsBacillary populations1. 1. RapidlyRapidly multiplying bacilli multiplying bacilli
- Optimum medium: Extracellular. PH 6.5-7, maximum oxygenation (cavern wall)
- Large number of bacilli → High probability of spontaneous natural mutations
Many Millions
Natural Resistant Mutants
FailureFailure

RelapsesRelapses2. 2. SlowSlow multiplication Bacilli multiplication Bacilli
- Intramacrophagic location. Acid pH. Population<105
No Naturally Resistant MutantsNo Naturally Resistant Mutants
Bacillary populationsBacillary populations

Bacillary populationsBacillary populations3. 3. IntermittentlyIntermittently growing bacilli growing bacilli
- Unfavourable conditions. Solid caseum. Extracellular
- Population <105 - Relapse capacity
No Naturally Resistant MutantsNo Naturally Resistant Mutants
RelapsesRelapses

Bacillary Bacillary populationspopulations
1. Rapidly multiplying bacilli1. Rapidly multiplying bacilli → INHINH
- Optimum medium: Extracellular. PH 6.5-7, maximum oxygenation (cavern wall)
- Large number of bacilli → High probability of spontaneous mutations
2. Slowly multiplying bacilli2. Slowly multiplying bacilli → PZPZ
- Intramacrophagic location. Acid pH. Population<105
3. Intermittently growing bacilli3. Intermittently growing bacilli → RIFRIF
- Unfavourable conditions. Solid caseum. Extracellular- Population <105. Relapse capacity
4. Bacilli in latent state:4. Bacilli in latent state: Not susceptible to drugs
- Reactivations and relapses
provided by Caminero

2. 2. ReservoirReservoir. Source of Infection. Source of Infection2. 2. ReservoirReservoir. Source of Infection. Source of Infection
provided by Caminero

ReservoirReservoirReservoirReservoir
- MAN:- MAN: * Infected, healthy* Infected, healthy
World Population:World Population: 6.100 Millions 6.100 Millions
M. TB Infection:M. TB Infection: 2.000 Millions 2.000 Millions
¡¡ Possible Reservoir MDR-TB: ¡¡ Possible Reservoir MDR-TB: 50 Millions50 Millions !! !!
provided by Caminero

Source of InfectionSource of InfectionSource of InfectionSource of Infection
- MAN:- MAN:
* Active * Active diseasedisease
TB Cases: TB Cases: 16 million 16 million
MDR-TB Cases:MDR-TB Cases: + 500.000+ 500.000
provided by Caminero

Mechanism of Mechanism of TransmissionTransmissionMechanism of Mechanism of TransmissionTransmission
- Fundamentally AEROGEN- Fundamentally AEROGEN
- Very Uncommon:- Very Uncommon: - Cutaneous-Mucosal- Cutaneous-Mucosal
- Urogenital- Urogenital
- Inoculation- Inoculation
- Tran placental, etc- Tran placental, etc
provided by Caminero

TB Transmission. Contagious aerosol (droplets < 5 micras)

Greatest TB Greatest TB TransmittersTransmittersGreatest TB Greatest TB TransmittersTransmitters
1.- Persons with bad Coughs1.- Persons with bad Coughs
2.- Sputum Sm+ Patients2.- Sputum Sm+ Patients
3.- Untreated patients3.- Untreated patients4.- Patients who have just commenced treatment4.- Patients who have just commenced treatment
5.- Cases with poor response to treatment5.- Cases with poor response to treatment

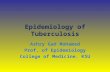
Pulmonary TB (85%)
Exposure toSource of disease
Sputum Smear+
Infection
Active TB
Extra Pulmonary(15%)
10-15 persons / year 5 – 10%
Sputum Smear Negative (35%)
50%
TB Epidemiologic TB Epidemiologic CycleCycle

TB TB RiskRisk Groups Groups Relative Risk of developing TBRelative Risk of developing TB
(compared with control population, regardless of (compared with control population, regardless of PPD)PPD)
TB TB RiskRisk Groups Groups Relative Risk of developing TBRelative Risk of developing TB
(compared with control population, regardless of (compared with control population, regardless of PPD)PPD)
- HIV/AIDS 150
- Silicosis 30
- Diabetes 2 – 4.1
- Chronic renal failure / Haemodial. 10 – 25.3
- Gastrectomy 2-5
- Jejunoileal by-pass 27 - 63
- Kidney transplant 37
- Heart “ 20 - 74
- Head or neck carcinoma 16
ATS/CDC. Am J Respir Crit Care Med 2000; 161 (part 2)

M. tuberculosis Resistance M. tuberculosis Resistance Natural Resistant Mutants according to Bacillary Natural Resistant Mutants according to Bacillary
PopulationPopulation
M. tuberculosis Resistance M. tuberculosis Resistance Natural Resistant Mutants according to Bacillary Natural Resistant Mutants according to Bacillary
PopulationPopulation
INH 1 x 105-106 Bacilli
RIF 1 x 107-108 Bacilli
SM 1 x 105-106 Bacilli
EMB 1 x 105-106 Bacilli
PZ 1 x 102-104 Bacilli ?
Quinolones 1 x 105-106 Bacilli ?
Others 1 x 105-106 Bacilli ?

M. tuberculosis Resistance M. tuberculosis Resistance Bacillary Population in different TB LesionsBacillary Population in different TB Lesions
M. tuberculosis Resistance M. tuberculosis Resistance Bacillary Population in different TB LesionsBacillary Population in different TB Lesions
TB Sm+ 107-109 Bacilli
Cavitary 107-109 Bacilli
Infiltrated 104-107 Bacilli
Nodules 104-106 Bacilli
Adenopathies 104-106 Bacilli
Renal TB 107-109 Bacilli
Extrapul. TB 104-106 Bacilli

Bacteriological Fundaments
of TB Treatment
1. Drug combinations
The combination of drugs prevents the
appearance of resistance,
because it avoids the selection of
naturally resistant mutants

Selection of Natural Resistance,Selection of Natural Resistance,
Acquired and Initial ResistanceAcquired and Initial Resistance
SUSCEPTIBLESUSCEPTIBLE
to Drugsto Drugs
RESISTANTRESISTANT
to Drugsto Drugs
LatentLatent
ContagiousContagious
LatentLatent
Contagious Contagious
Develop intoDevelop into
DR TBDR TB
transmissiontransmission
acquire DR-TBacquire DR-TB acquire (M)DR-TBacquire (M)DR-TB
transmissiontransmissionDevelop Develop
into TBinto TB

Basic Concepts in TB Resistance
M.D.R.M.D.R.

M. Tuberculosis Resistance M. Tuberculosis Resistance Multidrug-resistance (MDR)Multidrug-resistance (MDR)
M. Tuberculosis Resistance M. Tuberculosis Resistance Multidrug-resistance (MDR)Multidrug-resistance (MDR)
Defined as resistance at a minimum to “INH+RIF”
It is extremely dangerous, as this TB is very difficult to cure
MDR may be:– Primary or Initial– Acquired
Will it determine Will it determine
the the futurefuture of TB? of TB?

موارد مقاوم به چند دارو
موارد حساس به دارو
250 تا 25بین میلیون تومان
000,200کمتر از تومان هزينه
%95بیش از درصد60 تا 40 اميد بهبودي
ماه6 ماه24 تا 18طول دوره
درمان
موارد100% ماه6 تا 4
% 10کمتر از موارد
به مدت کوتاه
نیاز به بستری
غالبا نارسایی تنفسی برای تمام عمر ندارد معلوليت
حفظ يك منبع آلودگي از نوع مقاوم
حذف یک منبع انتشار
يدميولوژيپا
مقايسه هزينه ، طول مدت درمان و اثر بخشي رژيم هاي درماني موجود ميان يك
بيمار مبتال به سل حساس به دارو و يك بيمار به سل مقاوم به چند دارو

LOSS OF HEALTHY LIFE DUE TO TB
Rank Condition %DALYs1 Lower respiratory infections 6.12 HIV/AIDS 6.03 Unipolar depressive disorders 4.54 Diarrhoeal diseases 4.15 Ischaemic heart disease 4.06 Childhood diseases 3.37 Cerebrovascular disease 3.18 Malaria 2.99 Road traffic accidents 2.6
10 Tuberculosis 2.5

Estimated numbers of new cases, 2006Estimated numbers of new cases, 2006
No estimate
0–999
10 000–99 999
100 000–999 999
1 000 000 or more
1000–9999
Estimated number of new TB cases (all forms)
9m cases annually>1/3 in India and China

Estimated TB incidence rate, 2006Estimated TB incidence rate, 2006
Estimated new TB cases (all forms) per 100 000 population
No estimate
0-24
50-99
300 or more
25-49
100-299World : 139/100,000
Highest TB rates per capita are in Africalinked to HIV/AIDS

Tuberculosis notification rates, 2006Tuberculosis notification rates, 2006
No report
0–24
25–49
50–99
100 or more
Notified TB cases (new and relapse) per 100 000 population
World : 82/100,000
82*100/139 = 57%
Smear+ CDR= 61%

World Health
Assembly 1991
"…attain a global target of cure of 85% sputum-positive patients under treatment and detection
of 70% of cases by the year 2000"

MILLENNIUM DEVELOPMENT GOALS (2015)MILLENNIUM DEVELOPMENT GOALS (2015)
1. Eradicate poverty and hunger2. Universal primary education3. Empower women4. Reduce child mortality5. Improve maternal health6. Combat HIV/AIDS, malaria and other diseases7. Environmental sustainability8. Global partnership for development
Sto
p T
B D
epa
rtmen
tS
top
TB
Dep
artm
ent

Targets for global TB controlMILLENNIUM DEVELOPMENT GOALS
"to have halted and begun to reverse incidence... by 2015"
Targets for global TB controlMILLENNIUM DEVELOPMENT GOALS
"to have halted and begun to reverse incidence... by 2015"
Implementation (DOTS) Target YearCase detection 70% 2005
Treatment success 85% 2004/5
ImpactPrevalence 50% 2015
Death 50% 2015 Incidence <1 per million 2050

Estimated TB Burden I.R.IRAN – 2006
Estimated TB Burden I.R.IRAN – 2006
GlobalGlobal EMROEMRO IranIran
Prevalence RatePrevalence Rate 219/100,000219/100,000 152/100,000152/100,000 2828/100,000/100,000
Mortality RateMortality Rate 25/100,00025/100,000 20/100,00020/100,000 33/100,000/100,000
Incidence RateIncidence Rate
All formsAll forms 139/100,000139/100,000 105/100,000105/100,000 2222/100,000/100,000
SS+SS+ 62/100,00062/100,000 47/100,00047/100,000 1010/100,000/100,000
HIV prev. in new TB casesHIV prev. in new TB cases 7.7 %7.7 % 1.1 %1.1 % 1.71.7

Estimated HIV prevalence in new TB cases, 2006Estimated HIV prevalence in new TB cases, 2006
No estimate
0–4
20–49
50 or more
5–19
HIV prevalence in TB cases, (%)
World= 7.7%

MDR-TB Prevalence Rate among new cases2006
MDR-TB Prevalence Rate among new cases2006
World: 3.1%
EMRO: 2.9%

MDR-TB Prevalence Rate among Previously Treated Cases2006
MDR-TB Prevalence Rate among Previously Treated Cases2006
World: 19.3%
EMRO: 28.9%

XDR-TBXDR-TB
Extensively drug-resistant TB (XDR TB) defined as:
MDR TB with further resistance to:
•A fluoroquinolone
• One or more of the following injectable drugs:
kanamycin, amikacin, capreomycin
Source: Global XDR-TB Task Force, 7-8 October, 2006

Czech Republic
The b
oundarie
s and n
am
es sh
ow
n a
nd th
e d
esig
natio
ns u
sed o
n th
is map d
o n
ot im
ply
the e
xpre
ssion o
f any o
pin
ion
whatso
ever o
n th
e p
art o
f the W
HO
conce
rnin
g th
e le
gal sta
tus o
f any co
untry
, territo
ry, city
or a
rea o
r of its a
uth
oritie
s, or co
nce
rnin
g th
e d
elim
itatio
n o
f its frontie
rs or b
oundarie
s. Dotte
d lin
es o
n m
aps re
pre
sent a
ppro
xim
ate
bord
er lin
es fo
r w
hich
there
may n
ot y
et b
e fu
ll agre
em
ent.
WH
O 2
005. A
ll rights re
serv
ed
Ecuador
Georgia
Argentina
Bangladesh
Germany
Republic of Korea
Armenia
Russian Federation
South Africa
Portugal
Latvia
Mexico
Peru
USA
Brazil
UK
Sweden
Thailand
Chile
Spain
Islamic Republic of Iran
China, Hong Kong SAR
France
Japan
Norway
Canada
Countries with confirmed XDR-TB cases as of February 2007
Countries with confirmed XDR-TB cases as of February 2007

Estimated number of
cases
Estimated number of
deaths
1.6 million8.8 million
116,000*424,000
All forms of TB
Multidrug -resistant
TB )MDR-TB(Extensively drug-resistant TB )XDR-TB(
27,000* 16,000*
* Calculated based on several available estimates
Latest Global TB Estimates - 2005Latest Global TB Estimates - 2005

Drug susceptible TB*
*or limited resistance
Manageable with 4 drug regimen - DOTS
Resistance to H&R
Treatable with 2nd line drugs
MDR-TB
1990
XDR-TB
2006
Resistance to 2nd line drugs
Treatment options seriously restricted
Total DR ?
Resistance to all available drugs
No treatment options
Evolution of drug-resistant TBEvolution of drug-resistant TB

سلوضعيت فعلي بيماري در جمهوري اسالمي ايران
سلوضعيت فعلي بيماري در جمهوري اسالمي ايران

بيست و دو كشور داراي بيشترين بار بيماري

فراواني و ميزان بروز گزارش شده سل در كشور (1387)
فراواني و ميزان بروز گزارش شده سل در كشور (1387)
ميزان بروزگزارش شده
/ (100,000) تعداد
13.4 9742 كل اشكال سل
6.7 4885 اسمير خلط مثبت
سل ريوي
2.7 1936 اسمير خلط منفي
3.6 2606 سل خارج ريوي

وضعيت ميزان بيماريابي سل در كشور (1387)
وضعيت ميزان بيماريابي سل در كشور (1387)
CDR
) ميزان بروز/100,000)
تعدادمورد انتظار
گزارش شده
61 % 22 13.4 9742 كل اشكال سل
67% 10 6.7 4885 اسمير خلط مثبت سل
ريوي2.7 1936 اسمير خلط
منفي
3.6 2606 سل خارج ريوي

موارد 67%موجود
شناسايي و گزارش شده
.اند
موارد شناسايي نشده )گم شده(:
بيماران33%
اين موارد شناسايي نشده، كجا گم شده اند؟

روند فراواني موارد سل اسمير مثبت گزارش شده در كشور
1387 به تفكيك مليت
روند فراواني موارد سل اسمير مثبت گزارش شده در كشور
1387 به تفكيك مليت

ميزان بروز سل ريوي اسمير خلط مثبت برحسب دانشگاههاي علوم پزشكي كشور –
1387 سال

توزيع جنسي بروز سل ريوي اسمير مثبت در كشور 1387 در سال
توزيع جنسي بروز سل ريوي اسمير مثبت در كشور 1387 در سال
50%
50%
مرد زن

نتيجه درمان بيماران مبتال به سل ريوي اسمير مثبت
85 سال –جمهوری اسالمی ایران
نتيجه درمان بيماران مبتال به سل ريوي اسمير مثبت
85 سال –جمهوری اسالمی ایران
1385
83 ميزان موفقيت درمان

Related Documents