A COMPARATIVE STUDY OF 0.1% ROPIVACAINE WITH FENTANYL VERSUS 0.125% BUPIVACAINE WITH FENTANYL AS CONTINUOUS EPIDURAL INFUSION IN LABOUR ANALGESIA DISSERTATION SUBMITTED TO THE NATIONAL BOARD OF EXAMINATIONS NEW DELHI IN THE PARTIAL FULFILLMENT OF THE REQUIREMENT FOR THE DEGREE OF DIPLOMATE OF NATIONAL BOARD [ANAESTHESIOLOGY] SUBMITTED BY DR. JAYAPRAKASH . K Reg No. 101- 41132-111-100523 JANUARY 2011 – DECEMBER 2013 DEPARTMENT OF ANAESTHESIOLOGY G. KUPPUSWAMY NAIDU MEMORIAL HOSPITAL COIMBATORE – 641 037

Thesis full.pdf
Dec 01, 2015
0.1% ropivacaine vs 0.125% bupivacaine in labour epidural analgesia
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
A COMPARATIVE STUDY OF 0.1% ROPIVACAINE WITH FENTANYL
VERSUS 0.125% BUPIVACAINE WITH FENTANYL
AS CONTINUOUS EPIDURAL INFUSION IN LABOUR ANALGESIA
DISSERTATION SUBMITTED TO THE
NATIONAL BOARD OF EXAMINATIONS
NEW DELHI
IN THE PARTIAL FULFILLMENT OF THE REQUIREMENT FOR THE
DEGREE OF DIPLOMATE OF NATIONAL BOARD [ANAESTHESIOLOGY]
SUBMITTED BY
DR. JAYAPRAKASH . K
Reg No. 101- 41132-111-100523
JANUARY 2011 – DECEMBER 2013
DEPARTMENT OF ANAESTHESIOLOGY
G. KUPPUSWAMY NAIDU MEMORIAL HOSPITAL
COIMBATORE – 641 037
i
BONAFIDE CERTIFICATE
This is to certify that the dissertation “A COMPARATIVE STUDY OF 0.1%
ROPIVACAINE WITH FENTANYL VERSUS 0.125% BUPIVACAINE WITH
FENTANYL AS CONTINUOUS EPIDURAL INFUSION IN LABOUR ANALGESIA
” is a bonafide work of Dr. JAYAPRAKASH K (Reg No. 101-41132-111-100523), done
under direct guidance and supervision of Dr. RAJANI SUNDAR M.D., D.A during the
academic period 2011-2013 in partial fulfillment of National Board of Examination rules
and regulations for the award of Diplomate of National Board in Anaesthesiology.
DR. RAMKUMAR RAGUPATHY, M.S., MCH DR. RAJANI SUNDAR, M.D., D.A.,
DEAN CHIEF ANAESTHESIOLOGIST
GKNM HOSPITAL, COIMBATORE DEPARTMENT OF ANAESTHESIA
GKNM HOSPITAL, COIMBATORE.
ii
DECLARATION BY THE CANDIDATE
I hereby declare that this dissertation entitled “A COMPARATIVE STUDY OF
0.1% ROPIVACAINE WITH FENTANYL VERSUS 0.125% BUPIVACAINE WITH
FENTANYL AS CONTINUOUS EPIDURAL INFUSION IN LABOUR ANALGESIA”
is a bonafide and genuine research work carried out by me under the guidance of
Dr Rajani Sundar, M.D,D.A. Head of the department, Department of Anesthesiology,
G.Kuppusamy Naidu Memorial Hospital, Coimbatore.
Date:
Place:
Dr.Jayaprakash K
Postgraduate in Anaesthesiology
G.Kuppusamy Naidu Memorial Hospital
Coimbatore
iii
Acknowledgement:
I would like to thank Dr.Ramkumar Raghupathy M.S,MCH. Dean, G.K.N.M
hospital for permitting to do this study in our institution.
I would like to express my deep sense of gratitude to Dr.RAJANI
SUNDAR,M.D,D.A., Head of the Department, Anaesthesiology,for having suggested
this topic and providing constant guidance, encouragement and personal attention
during the study, without which this work would not hae been completed
successfully.
I am grateful to all our consultants Dr.Soundravalli M.D,D.A Dr.Palaniappan
M.D,D.A, Dr.Anandhi Arul M.D,D.A,DNB, Dr.Sai Gopalakrishnan D.A,DNB,
Dr.Sathyamurthy D.A,DNB and Dr.Muthukumar DNB for their valuable guidance
throughout the course of my study.
I would like to thank the Consultants and residents of the Department of Obststrics
and Gynaecology for their unwavering support for this study.
I am extremely thankful to the staff nurses of our labour theatre who helped me a lot
during this study.
I would like to thank my fellow post-graduates for their help during the course of this
study.
I thank Dr.Saleendran for his valuable help in completing the statistical analysis and
timely attention in compiling this manuscript.
I would finally thank my mother Mrs.Vasanthi and my wife Dr.Surya for supporting
me through all my endeavours.
Last but not the least, a special thanks to the patients who participated in this study.
Dr.Jayaprakash.K
iv
List of Abbreviations
ACOG - American Congress of Obstetricians and Gynecologists
ASA - American Society of Anesthesiologists
BP - Blood pressure
CaN - Cord around the neck
cm - Centimetre
CNS - Central nervous system
CVS - Cardio-Vascular syatem
EEG - Electroencephalogram
FD - Fetal distress
FP- Failure to progress
Ft-obs - Fetal tachypnea for observation
GDM - Gestational diabetes mellitus
h/hr - Hour
HR - Heart rate
IV - Intravenous
Kg - Kilogram
LOR - Loss of resistance
mcg/µg - Microgram
v
MF- Failure of maternal bearing down
mg - Milligram
ml - Millilitre
ML- Meconium stained liquor
mm - Millimetre
Numb - Numbness
PCEA - Patient controlled epidural analgesia
PIH - Pregnancy induced hypertension
RR - respiratory rate
Rx - Treatment
SpO2 - oxygen saturation
Temp - temperature
VAS - Visual Analog scale
VNRS - Verbal numerical rating scale
vi
Abstract:
Topic:
A comparative study of 0.1% ropivacaine with fentanyl versus 0.125%
bupivacaine with fentanyl as continuous epidural infusion in labour analgesia
Background and objectives:
Ropivacaine has been found to be equally efficacious as bupivacaine in
labour epidural analgesia. In our study we compared the analgesic efficacy, motor
blocking property and the effect on various labour outcomes of ropivacaine with
bupivacaine when used as a continuous epidural infusion during labour.
Methodology:
Seventy ASA I&II parturients with singleton pregnancies who presented in
active labour with cervical dilatation of 3-5cm were studied in a prospective,
randomized control manner. Patients were randomized into Group A(ropivacaine)-
35 patients and Group B(bupivacaine)- 35 patients.
Epidural analgesia was performed with a 18G Tuohy needle and a 20G
epidural catheter was placed in the best interlumbar space between L1 and L4.
Various parameters(heart rate, blood pressure, respiratory rate, oxygen saturation,
pain score) and complications if any were recorded every 15 minutes in the 1st hour,
every 30 minutes in the 2nd hour and every hour later on.
All data were collected and statistical analysis performed using SPSS
statistical package, version 17 for windows.
Results:
vii
There was no significant difference in the hemodynamics, pain relief, motor
block, mode of delivery, duration of labour and complications between ropivacaine
and bupivacaine.
Conclusion:
From this study it can be concluded that though ropivacaine is less potent
than bupivacaine, ropivacaine is as efficacaious as bupivacaine in the
concentrations used in our study.
viii
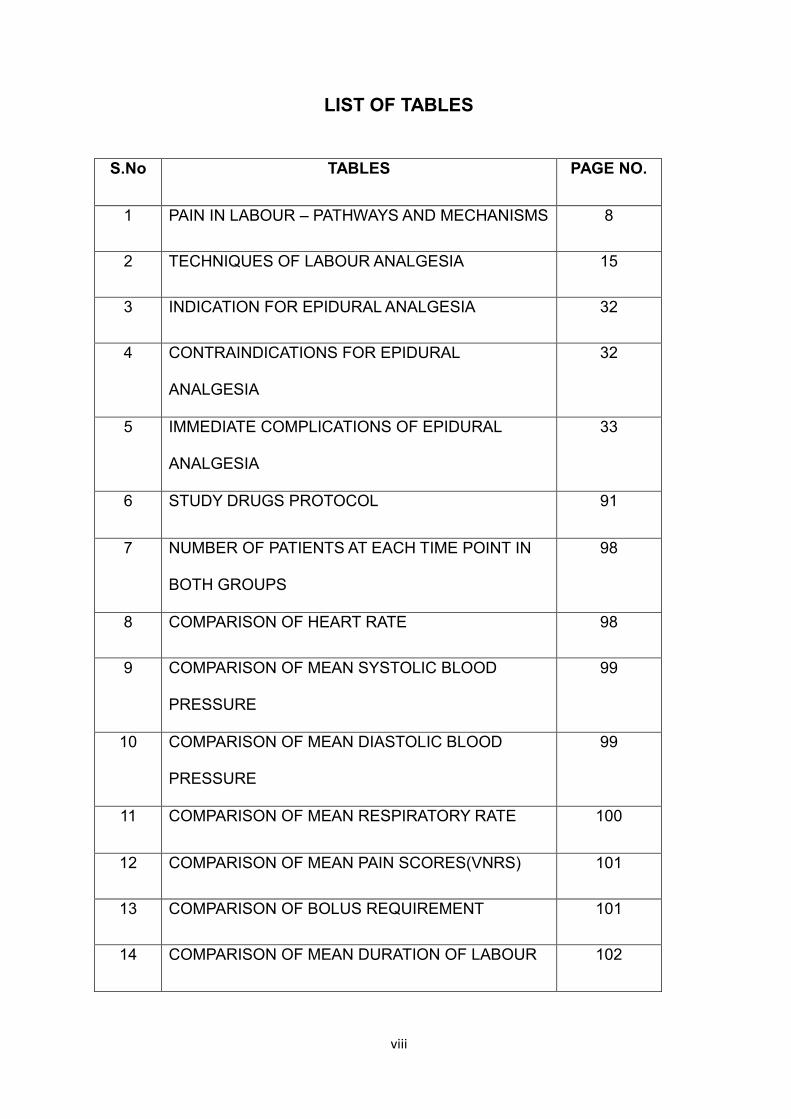
LIST OF TABLES
S.No TABLES PAGE NO.
1 PAIN IN LABOUR – PATHWAYS AND MECHANISMS 8
2 TECHNIQUES OF LABOUR ANALGESIA 15
3 INDICATION FOR EPIDURAL ANALGESIA 32
4 CONTRAINDICATIONS FOR EPIDURAL
ANALGESIA
32
5 IMMEDIATE COMPLICATIONS OF EPIDURAL
ANALGESIA
33
6 STUDY DRUGS PROTOCOL 91
7 NUMBER OF PATIENTS AT EACH TIME POINT IN
BOTH GROUPS
98
8 COMPARISON OF HEART RATE 98
9 COMPARISON OF MEAN SYSTOLIC BLOOD
PRESSURE
99
10 COMPARISON OF MEAN DIASTOLIC BLOOD
PRESSURE
99
11 COMPARISON OF MEAN RESPIRATORY RATE 100
12 COMPARISON OF MEAN PAIN SCORES(VNRS) 101
13 COMPARISON OF BOLUS REQUIREMENT 101
14 COMPARISON OF MEAN DURATION OF LABOUR 102
ix
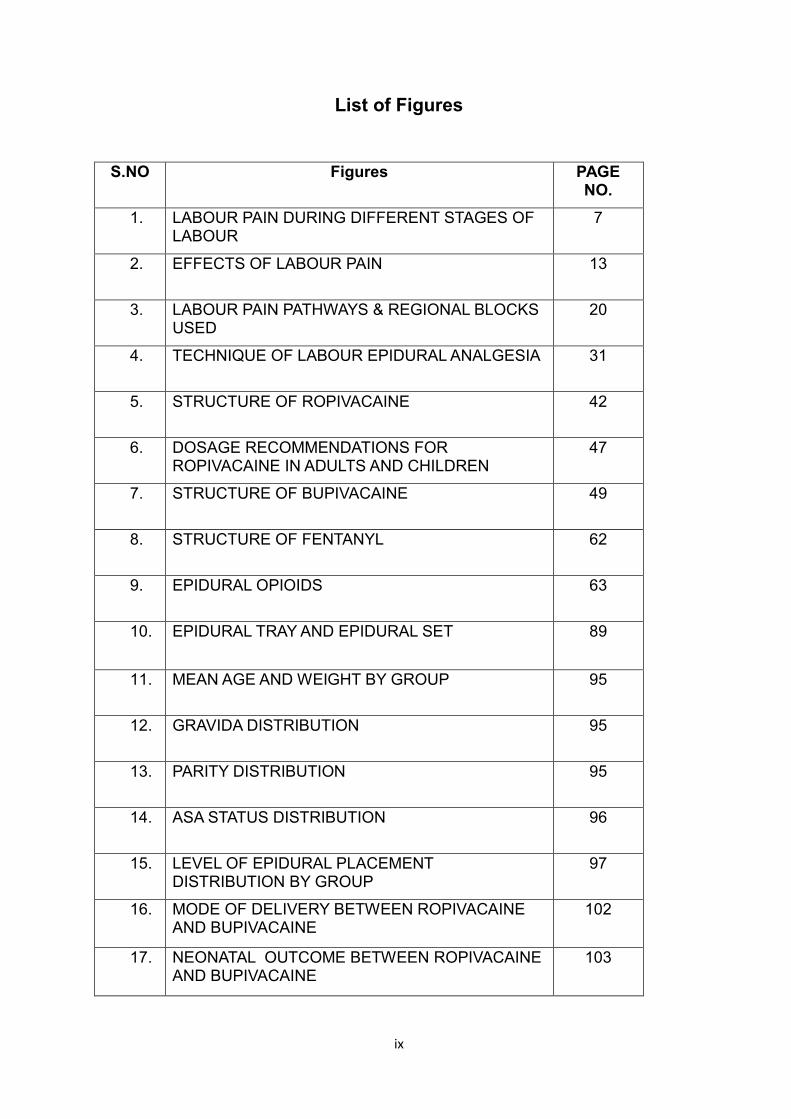
List of Figures
S.NO Figures PAGE NO.
1. LABOUR PAIN DURING DIFFERENT STAGES OF LABOUR
7
2. EFFECTS OF LABOUR PAIN 13
3. LABOUR PAIN PATHWAYS & REGIONAL BLOCKS USED
20
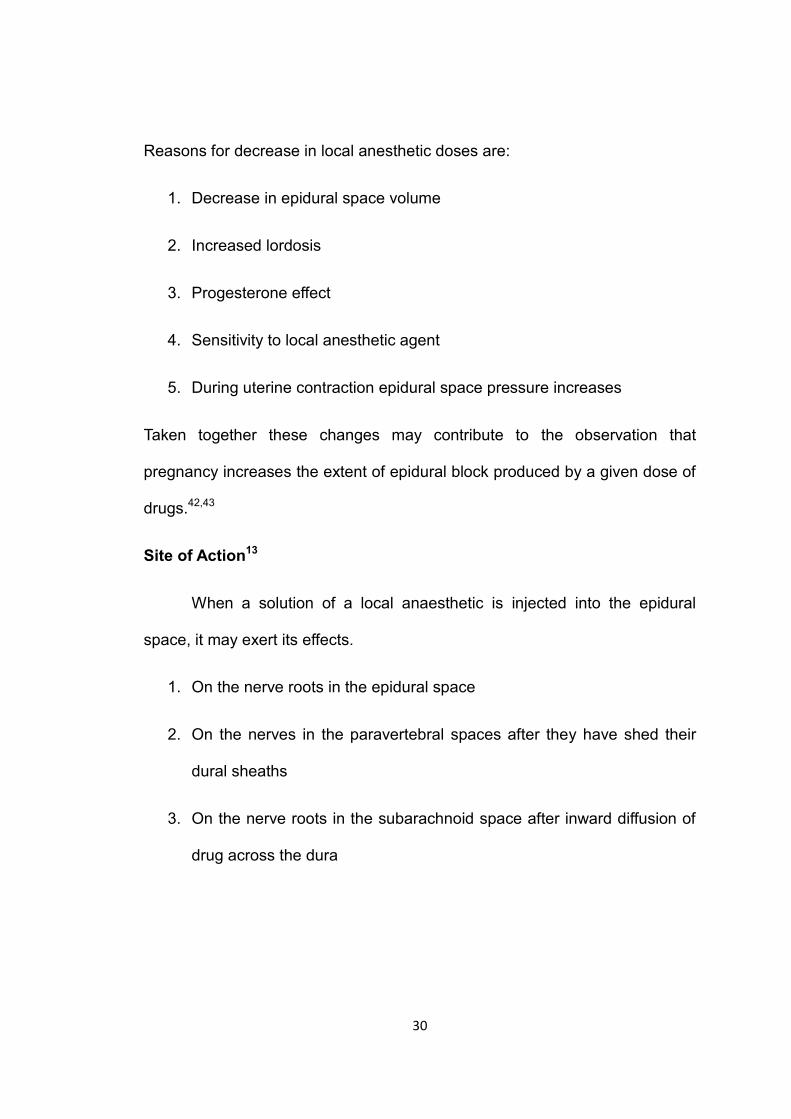
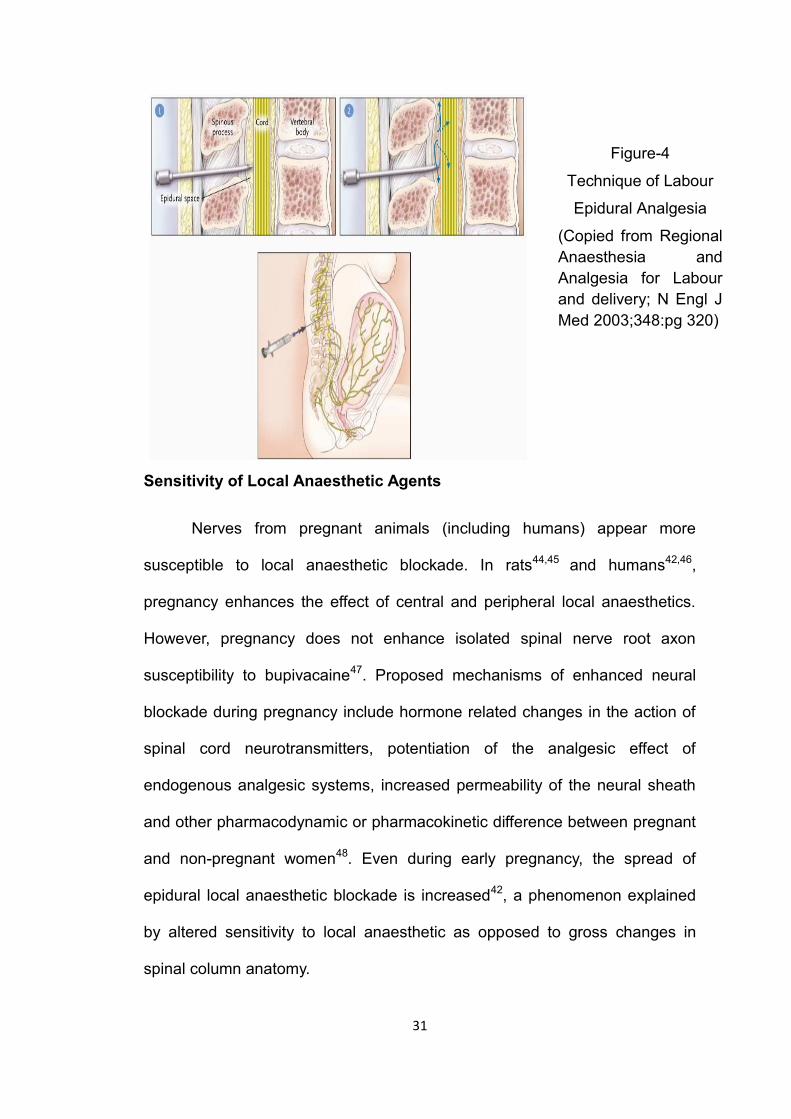
4. TECHNIQUE OF LABOUR EPIDURAL ANALGESIA 31
5. STRUCTURE OF ROPIVACAINE 42
6. DOSAGE RECOMMENDATIONS FOR ROPIVACAINE IN ADULTS AND CHILDREN
47
7. STRUCTURE OF BUPIVACAINE 49
8. STRUCTURE OF FENTANYL 62
9. EPIDURAL OPIOIDS 63
10. EPIDURAL TRAY AND EPIDURAL SET 89
11. MEAN AGE AND WEIGHT BY GROUP 95
12. GRAVIDA DISTRIBUTION 95
13. PARITY DISTRIBUTION 95
14. ASA STATUS DISTRIBUTION 96
15. LEVEL OF EPIDURAL PLACEMENT DISTRIBUTION BY GROUP
97
16. MODE OF DELIVERY BETWEEN ROPIVACAINE AND BUPIVACAINE
102
17. NEONATAL OUTCOME BETWEEN ROPIVACAINE AND BUPIVACAINE
103
x
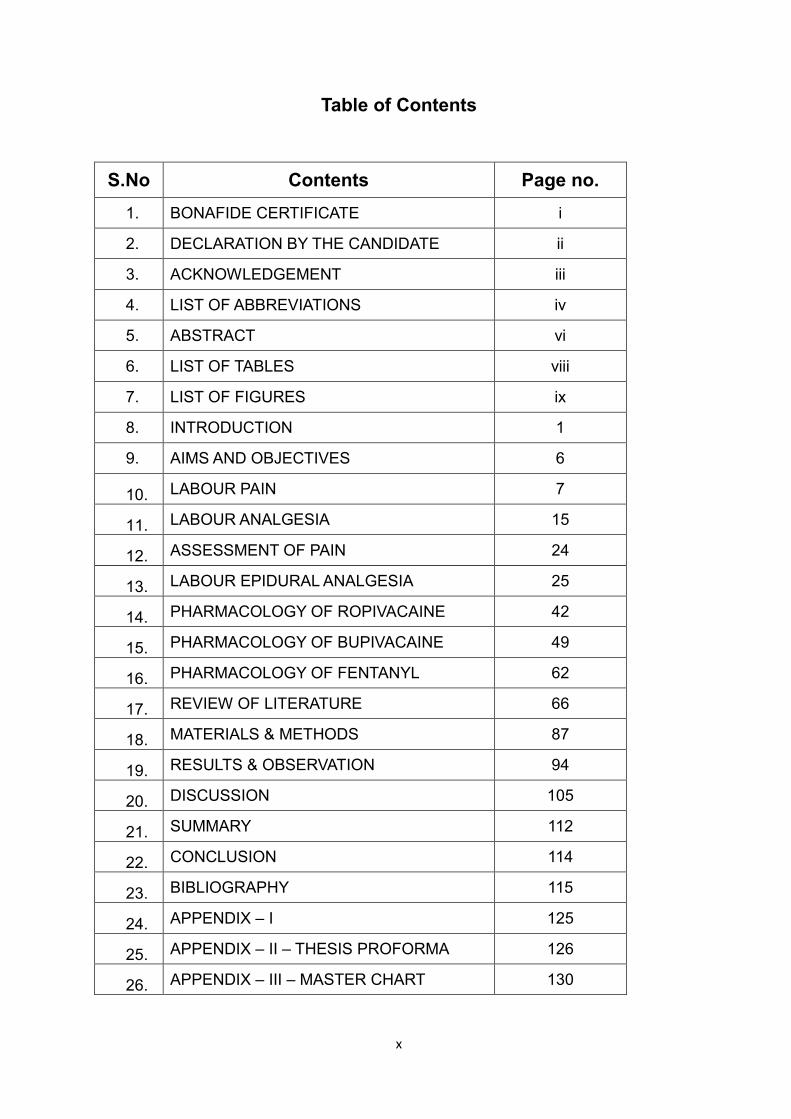
Table of Contents
S.No Contents Page no.
1. BONAFIDE CERTIFICATE i
2. DECLARATION BY THE CANDIDATE ii
3. ACKNOWLEDGEMENT iii
4. LIST OF ABBREVIATIONS iv
5. ABSTRACT vi
6. LIST OF TABLES viii
7. LIST OF FIGURES ix
8. INTRODUCTION 1
9. AIMS AND OBJECTIVES 6
10. LABOUR PAIN 7
11. LABOUR ANALGESIA 15
12. ASSESSMENT OF PAIN 24
13. LABOUR EPIDURAL ANALGESIA 25
14. PHARMACOLOGY OF ROPIVACAINE 42
15. PHARMACOLOGY OF BUPIVACAINE 49
16. PHARMACOLOGY OF FENTANYL 62
17. REVIEW OF LITERATURE 66
18. MATERIALS & METHODS 87
19. RESULTS & OBSERVATION 94
20. DISCUSSION 105
21. SUMMARY 112
22. CONCLUSION 114
23. BIBLIOGRAPHY 115
24. APPENDIX – I 125
25. APPENDIX – II – THESIS PROFORMA 126
26. APPENDIX – III – MASTER CHART 130
1
Introduction
Labour is a word that signifies one of the most happiest as well as one
of the most painful moments in a woman's life. If not dealt with properly, it can
lead to unpleasant experiences and mental agony. Labour is a highly complex
and personal process for every woman. Not every woman wants or needs
analgesic intervention for delivery. Every parturient should be educated
prenatally about labour and various modalities available for helping her. The
decision to receive any form of pain relief should be the patient's informed
decision.
The ASA & ACOG have said that
"Labor causes severe pain for many women. There is no other
circumstance where it is considered acceptable for an individual to
experience untreated severe pain, amenable to safe intervention, while
under a physician's care. In the absence of a medical contraindication,
maternal request is a sufficient medical indication for pain relief during
labor. Pain management should be provided whenever medically
indicated."1
Pain relief during labour has always been associated with religious &
cultural taboos, myths & controversies.
Pain free labour was denied to women because of the misinterpretation
of the biblical scripture
"In sorrow though shall bring forth children"
2
This lead clergymen of those bygone eras to insist that suffering in
labour was consistent with divine intent, since it was god's punishment to Eve
for disobeying his word.
This situation began to change in mid 1850's when few concerned
physicians became sympathetic to this agonising plight of women.
The first documented incident of pain relief during labour in USA was
for Fanny Longfellow in1847 with ether.2 The second woman to become
famous was Emma Darwin, wife of the eminent naturalist Charles Darwin who
was administered chloroform during labour. But the third incident influenced
the history of labour analgesia in a profound way. It was the administration of
chloroform to Queen Victoria by Dr.John Snow for her 8th confinement to
deliver Prince Leopold on April 7,1853.2 This made pain relief in labour
famous as well as more acceptable, since it had a royal patronage.
Advances in the field of labour analgesia have tread a long journey
from the days of ether and chloroform in 1847 to the present day practice of
comprehensive program of labour pain management using evidence based
medicine.
From 1840s to 1960s, different methods of pain relief were tried. This
included inhalational agents, systemic agents[opioids, ketamine, Twilight
sleep(morphine + scoploamine)], local blocks.
Most would agree that the ideal analgesic would be safe for the mother
and newborn, would have minimal effects on the progress of labor, and would
provide flexibility in changing conditions. Additionally, the ideal technique
would provide long-lasting, consistent analgesia titrated to individual
3
parturient’s needs, with minimal or no risk, no undesirable maternal or fetal
side effects, and with minimal physician input and cost.
There are various modalities available now commonly. It includes both
pharmacologic and non - pharmacological methods.
Non - pharmacological methods include psychoprohylaxis, hypnosis,
TENS( transcutaneous electrical nerve stimulation), biofeedback, and
acupuncture. Though they provide some form of pain relief, usually it is not
adequate and patients need additional form of pain relief. These methods
usually are unreliable and not consistent in the pain relief they provide.
Pharmacological methods include inhalational agents(entonox,
sevoflurane), systemic opioids (morphine, fentanyl, remifentanyl as PCEA).
Both these agents produce analgesia but not in a continuous and effective
manner. They also have systemic side effects on both the mother and fetus.
They may also interfere with the progress of labour.
Pharmacological methods also include regional anaesthesia. This in
turn comprises both regional blocks and central neuraxial blocks. Though
regional blocks give good pain relief they are associated with technical
difficulties as well. Paracervical plexus blocks are no longer used because of
their association with a relatively high fetal bradycardia. Pudendal nerve
blocks are mostly useful only in second stage of labour.
Central neuraxial blocks were introduced in labour in 1950. Pioneering
research in this field has lead to great development in the safe and effective
practice of neuraxial techniques. Modern neuraxial labour analgesia reflects a
4
shift in obstetrical anesthesia, thinking away from a simple focus on pain relief
and towards a focus on the overall quality of analgesia.3
Central neuraxial analgesia is the most versatile method of labour
analgesia and the gold standard technique for pain control in obstetrics that is
currently available. The satisfaction of birth experience is greater with
neuraxial techniques.4
Central neuraxial analgesia includes both subarachnoid as well as
epidural block
Among these epidural blockade comes close to being the ideal
analgesic technique in labour.4 It has the advantage of being able to provide
continuous analgesia for an unpredictable period of time and to convert
analgesia to anaesthesia if an operative intervention becomes necessary.
Epidural injection of a local anaesthetic combined with an opioid
provides a more rapid onset of analgesia with little motor blockade. The pain
relief starts sooner and also lasts longer than either drug alone. It allows both
the drugs to be used in lower concentration, thereby reducing the risk of local
anaesthetic systemic toxicity as well as opioid side effects.5,6,7
Bupivacaine and Ropivacaine are widely used to provide efficient
epidural analgesia in labour. The value of bupivacaine is limited by the risks of
motor blockade(associated with maternal dissatisfaction and increased
instrumental deliveries) and cardiac toxicity. Ropivacaine has the advantage
of more sensory motor differential blockade as well as decreased risk of
systemic toxicity. There have been conflicting comparisons of ropivacaine and
bupivacaine for labour analgesia.8,9,10 Some studies have suggested that
5
ropivacaine produces less motor block than bupivacaine while others found
the drugs to be indistinguishable. Dilute solutions of epidural local anesthetics
combined with opioids may be used to minimize unwanted motor block.
We undertook this study to see whether ropivacaine offers any
significant advantage over bupivacaine in our institutional practice in regards
to obstetrical outcome and whether a changeover from bupivacaine to
ropivacaine was warranted. This study compares the efficacy of Ropivacaine
and Bupivacaine in regards to pain relief, motor block, labour characteristics.
6
AIMS & OBJECTIVES:
Aim:
The aim of the study was to compare the efficacy of ropivacaine with
fentanyl and bupivacaine with fentanyl as continuous infusion in labour
epidural analgesia.
Objectives:
The current study was designed to compare the efficacy of ropivacaine
with fentanyl and bupivacaine with fentanyl as continuous infusion in labour
epidural analgesia with respect to
Pain relief
Motor block
Duration of labour
Mode of delivery
- Vaginal - Spontaneous / Assisted
- Cesarean section
Neonatal outcome - APGAR score, NICU admission
7
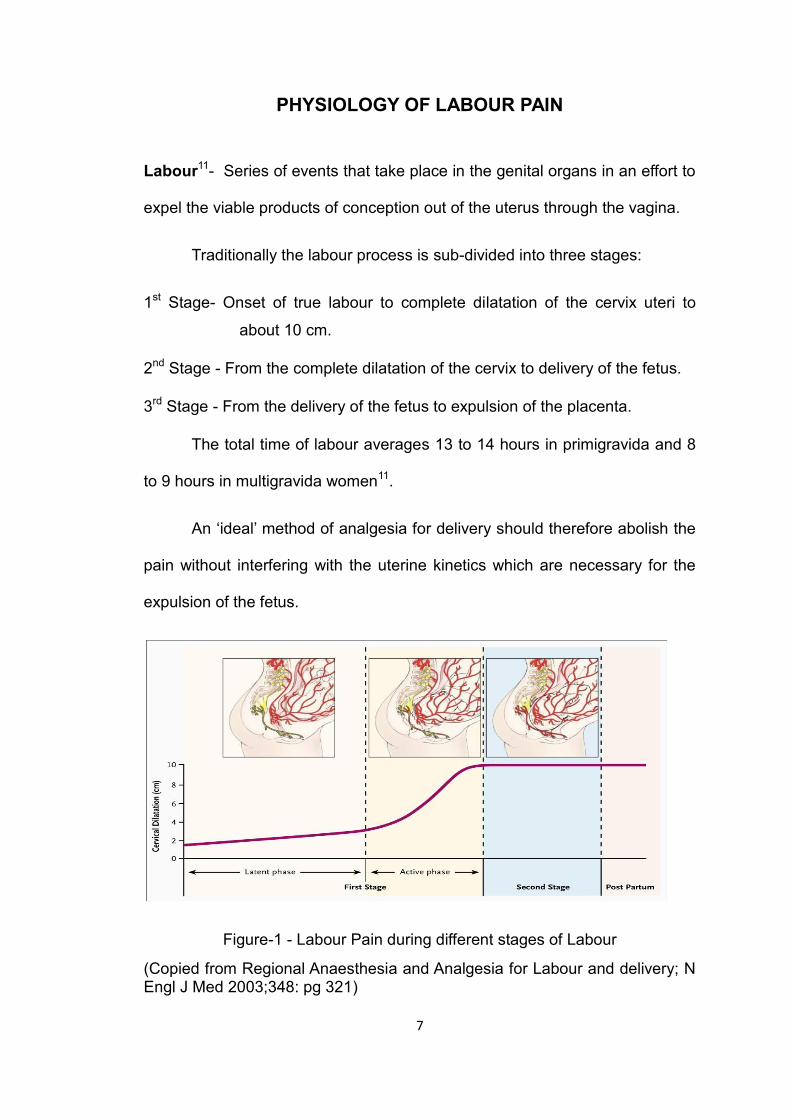
PHYSIOLOGY OF LABOUR PAIN
Labour11- Series of events that take place in the genital organs in an effort to
expel the viable products of conception out of the uterus through the vagina.
Traditionally the labour process is sub-divided into three stages:
1st Stage- Onset of true labour to complete dilatation of the cervix uteri to
about 10 cm.
2nd Stage - From the complete dilatation of the cervix to delivery of the fetus.
3rd Stage - From the delivery of the fetus to expulsion of the placenta.
The total time of labour averages 13 to 14 hours in primigravida and 8
to 9 hours in multigravida women11.
An ‘ideal’ method of analgesia for delivery should therefore abolish the
pain without interfering with the uterine kinetics which are necessary for the
expulsion of the fetus.
Figure-1 - Labour Pain during different stages of Labour
(Copied from Regional Anaesthesia and Analgesia for Labour and delivery; N Engl J Med 2003;348: pg 321)
8
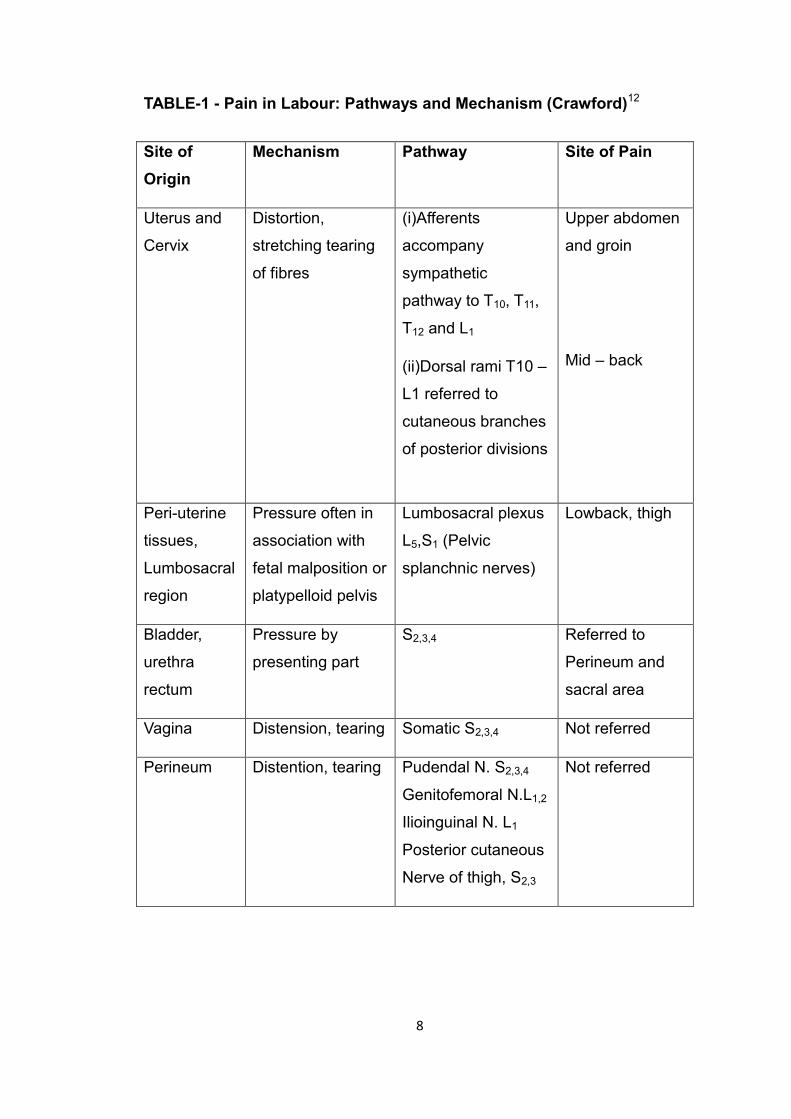
TABLE-1 - Pain in Labour: Pathways and Mechanism (Crawford)12
Site of
Origin
Mechanism Pathway Site of Pain
Uterus and
Cervix
Distortion,
stretching tearing
of fibres
(i)Afferents
accompany
sympathetic
pathway to T10, T11,
T12 and L1
(ii)Dorsal rami T10 –
L1 referred to
cutaneous branches
of posterior divisions
Upper abdomen
and groin
Mid – back
Peri-uterine
tissues,
Lumbosacral
region
Pressure often in
association with
fetal malposition or
platypelloid pelvis
Lumbosacral plexus
L5,S1 (Pelvic
splanchnic nerves)
Lowback, thigh
Bladder,
urethra
rectum
Pressure by
presenting part
S2,3,4 Referred to
Perineum and
sacral area
Vagina Distension, tearing Somatic S2,3,4 Not referred
Perineum Distention, tearing Pudendal N. S2,3,4
Genitofemoral N.L1,2
Ilioinguinal N. L1
Posterior cutaneous
Nerve of thigh, S2,3
Not referred
9
Pain pathways and mechanisms13,14
The description of peripheral pain pathway proposed by Cleland in
193315 was modified by Bonica14 and is fundamental to any consideration of
obstetric analgesia.
Pain in first stage of labour:
Intrinsic mechanism: During the first stage of labour, the pain is caused by:
1. Pressure on the nerve ending between the muscle fibres of the uterine
body and the fundus.
2. Contraction of the ischemic myometrium and the cervix, consequent to
the expulsion of blood from the uterus during contractions.
3. Inflammatory changes in the uterine muscle.
4. Contraction of the cervix and the lower uterine segment consequent to
the fear induced hyperactivity of the sympathetic nervous system.
Uterine contractions cause stretching, tearing and distortion and
possible ischemia of the uterine tissues, while simultaneous dilatation of the
cervix and stretching of the lower uterine segment is occurring. The pain
experienced by the mother is very variable and bears no constant relation with
the dilatation of cervix. These painful stimuli are transmitted by Aδ and C
fibres which accompany sympathetic pathways through the pelvic plexus,
inferior, middle and superior hypogastric plexus and the lumbar sympathetic
chain. The white rami of spinal nerves T11 and T12 are involved, but as labour
progresses T10 and L1 are recruited.
10
Pain pathways in second stage:
Intrinsic mechanism: Pain in the second stage of labour is mainly due to the
progressively increasing pressure of the presenting part causing:
1. Traction on the pelvic parietal peritoneum.
2. Stretching and tension of the bladder, urethra and rectum
3. Stretching and tension of ligaments and muscle of the pelvic cavity and
4. Abnormal pressure on one or more roots of the lumbosacral plexus.
Pain in the second stage is caused by distension of the pelvic
structures and peritoneum following the descent of the presenting part, in
addition to the pain of uterine contractions, although, once cervical dilatation
is complete, the pain induced by uterine contractions is much less intense.
The uterine pain produced by stretching or by pressure exerted in intra pelvic
structures including peritoneum, bladder, urethra and rectum is referred to
sacral segments. Pressure on the roots of lumbosacral plexus may manifest
itself as pain felt low in the back or in the thighs. Pain produced by stretching
of the peritoneum is transmitted by pudendal nerve (S2,3,4) and in part by the
posterior cutaneous nerve of thigh (S2,3), the genitofemoral nerve (L1,2) and
the ilioinguinal nerve (L1).
Central processing of pain:
The Aδ and C fibres conduct pain sensations from the uterus and the
spinal cord. The pain of parturition is mainly a visceral pain and therefore is
conducted in the Aδ and C fibres to the spinal cord. These fibres make
11
contact with lamina I, II and V. The convergence of cutaneous and visceral
fibres in lamina V is believed to form the basis of referred pain in labour.
From the spinal cord, the pain signals are transmitted to the brain via
the spinothalamic tract, which is divided into lateral and medical system. The
lateral system projects into the somatosensory cortex and brings about higher
responses such as fear, anxiety and also helps to initiate an appropriate
course of action. The medial system (slow conducting) project to the reticular
formation, periaqueductal grey matter, the hypothalamus and the limbic
system and is responsible for primitive responses to pain, which includes the
neuroendocrine response and hyperventilation.
Applied Clinical Aspects13:
During the latent phase of the first stage, the pain is felt as an ache or
a moderate cramp and is limited to the T11 and T12 dermatomes. As labour
progresses to the active phase, where the uterine contractions become more
intense, the pain in T11 and T12 dermatomes becomes sharp and cramping
and spreads to the adjacent T10 and L1 dermatomes.
The distribution of T10, T11, T12 and L1 dermatomes in the back overlies
the lower three lumbar vertebrae and the upper half of the sacrum. An
epidural block limited to these four segments produces relief of the low back
pain.
In the late 1st stage and in the early 2nd stage the pain is felt most
sharply in the perineum, in the lower part of the sacrum, anus and in the
thighs. Aching burning or cramping discomfort may appear. By blocking the
lower lumbar and upper sacral segments analgesia can be guaranteed.
12
Complete block of the sacral segments need only be performed when perineal
pain becomes worrisome and by this stage, the block of thoracolumbar
segments will hopefully be decaying to such an extent that abdominal muscle
strength will be adequate to permit voluntary expulsive efforts by the mother.
Effects of neural blockade on parturition13:
The effect of spinal innervation on uterine activity are complex and
depend on neural, hormonal and hemodynamic factor.
Previously it was believed that the motor activity of the uterus was
dependant on the sympathetic output through the lower seven thoracic
segments and that uterine activity would be impaired by blockade upto the
fifth thoracic segment. However subsequent work showed that the uterus is
independent of motor innervation and that uterine activity was more
dependant on humoral factors.
Normal progress in the 2nd stage of unstimulated labour is mainly
dependant on the strong expulsive efforts by the diaphragm on the abdominal
muscles, combined with tone of the pelvic diaphragm through which the
descending part of the fetus rotates. Premature loss of tone in the extrauterine
muscles will modify or delay the progress through poor expulsive efforts or
failure to rotate.
Labour may slow down further if the perineum is anaesthetized too
early in labour due to abolition of ‘Ferguson’s reflex’. The afferents of this
reflex come from receptors of the cervix and the vagina and pass centrally to
stimulate oxytocin secretion from posterior pituitary. However this deficit can
be readily overcome by exogenous oxytocin infusions.
13
In slow, incoordinate labour, analgesia relaxes the patient and the weak
irregular contractions of a high basal tone develop into low pressure, regular,
powerful uterine contractions.
In summary, the epidural blockade appears to have no direct
depressant effect on the uterine contractility besides inhibition of the oxytocin
release due to abolition of the Ferguson reflex. However indirectly, the neural
blockade may result in hypotension, reducing the myometrial perfusion
causing the contractility to fade. Besides, if early blockade of sacral segments
is prevented, the incidence of instrumental deliveries could be curtailed.
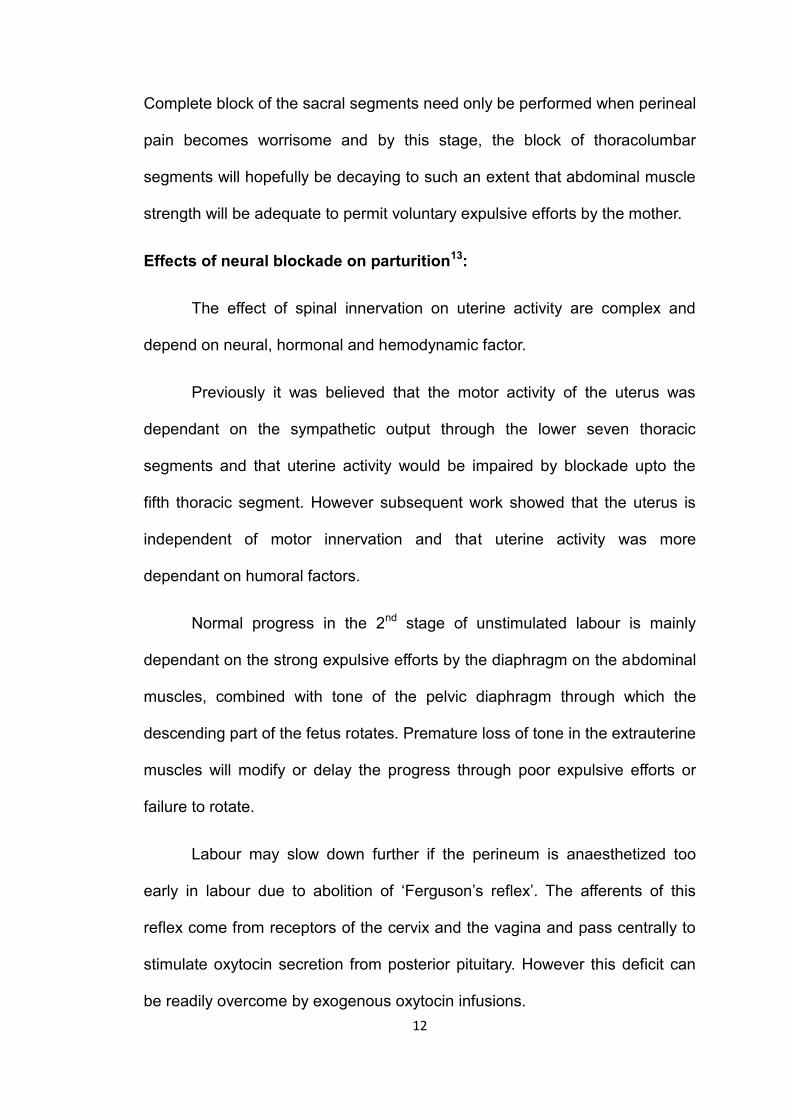
Figure – 2 - Effects of Labour pain
(Copied from Epidural Analgesia for Labor and Delivery; N Engl J Med
2010;362:1505)
14
Physiological effects of pain13
When pain of parturition is not adequately treated, several maternal
and fetal sequelae ensue because of the widespread maternal sympathetic
activation. This leads to various hormonal and metabolic disturbances in the
mother. These responses may be classified into cortical, suprasegmental and
segmental effects.
Cortical:
Pain will lead to fear, anxiety and increased skeletal muscle activity.
Suprasegmental:
Hyperventilation causes shift of maternal oxygen dissociation curve to
the left leading to foetal hypoxemia. Hyperventilation followed by
hypoventilation during the interval between uterine contractions leads to
transient apnea in mother. Maternal hypoventilation combined with a decrease
in uterine blood flow caused by catecholamines may lead to fetal hypoxemia.
Increased catecholamine production, hypertension, tachycardia,
increased lactic acid and free fatty acid production, hyperglycemia, increased
oxygen consumption, decreased uterine blood flow, impaired uterine
contractions, increased production of corticosteroids, beta-endorphins etc. are
the other suprasegmental effects.
Segmental:
Increased sympathetic tone produces decreased gastrointestinal
motility, delayed gastric emptying, ileus, nausea and vomiting.
15
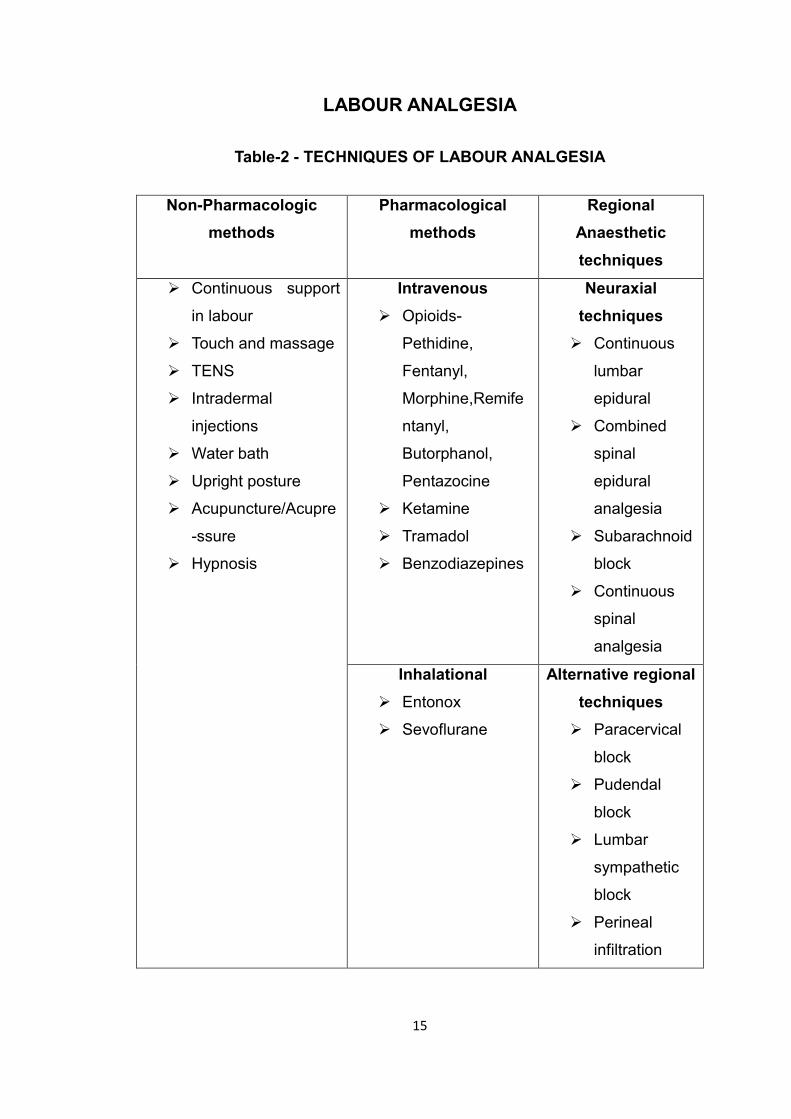
LABOUR ANALGESIA
Table-2 - TECHNIQUES OF LABOUR ANALGESIA
Non-Pharmacologic
methods
Pharmacological
methods
Regional
Anaesthetic
techniques
Continuous support
in labour
Touch and massage
TENS
Intradermal
injections
Water bath
Upright posture
Acupuncture/Acupre
-ssure
Hypnosis
Intravenous
Opioids-
Pethidine,
Fentanyl,
Morphine,Remife
ntanyl,
Butorphanol,
Pentazocine
Ketamine
Tramadol
Benzodiazepines
Neuraxial
techniques
Continuous
lumbar
epidural
Combined
spinal
epidural
analgesia
Subarachnoid
block
Continuous
spinal
analgesia
Inhalational
Entonox
Sevoflurane
Alternative regional
techniques
Paracervical
block
Pudendal
block
Lumbar
sympathetic
block
Perineal
infiltration
16
Attempts to minimize the pain of labour non-pharmacologically first
began in the early 20th century. Natural childbirth was pioneered by Grantly,
Dick, Read in 1932. He suggested that the pain of childbirth was brought
about by fear and tension and recommended passive muscle relaxation to
reduce the pain17.
Psychoprophylaxis is a technique which involves educating the
mother about the functioning of her body and the physiology of labour. It
originated in Russia and later popularized in France by Lamez18. Other
techniques involve simple emotional support from the patient’s partner or
another labour companion, touch and massage, the application of hot or cold
compresses and hydrotherapy.
Some techniques require fairly extensive preparation and antenatal
training. These include Biofeedback, Acupuncture, Hypnosis and
Transcutaneous electrical nerve stimulation (TENS). TENS involves the
application of a variable electrical stimulus to the skin at the site of pain and is
based upon the gate theory of pain control36. Studies have shown there to be
great or considerable relief of labour pain in 20-24% of mothers with about
60% having slight relief.
The advantages of all these techniques include quick discontinuation,
noninvasiveness and lack of any demonstrable ill effect on the fetus.
17
Systemic drugs13:
All drugs given systemically will cross the placenta to some extent.
Drugs which may reach the fetus in large amount are those with higher lipid
solubilities and low degrees of ionization20.
Pethidine is the most commonly used opiate in obstetric practice. It is
a synthetic opioid and the usual dose is 50 mg intramuscularly. Intramuscular
pethidine 100mg or 150mg was deemed satisfactory by only 22.4% of women
in first stage of labour and in 47.7% it gave no relief at all. Nausea and
vomiting occur in 50% of patients and exerts both immediate and long term
effects on fetus.
Morphine is a powerful opiate with a longer duration of analgesic
action compared to pethidine. It benefits from the ability to allay anxiety but
frequently causes nausea and vomiting and is apotent depressor of neonatal
respiration.
Benzodiazepines are used for maternal sedation. Diazepam has an
active metabolite, desmethyldiazepam which has a very long half life. Fetal
side effects include hypotonicity, decreased activity, respiratory depression
and decreased response to metabolic stress21. Lorazepam is relatively long
acting but has no active metabolites. It provides good anterograde amnesia,
which may not however be desirable during the birth experience.
Pentazocine is a partial agonist analgesic, and when used in multiple
doses, produces fewer low Apgar scores in babies as compared to
pethidine22. In addition the fetal heart rate is not so affected by pentazocine as
18
it is with pethidine. The chief drawback of pentazocine is unpleasant
hallucinogenic side effects and the limited pain relief that it can produce.
Ketamine has been used to produce analgesia during labour, doses in
the range of 0.25mg/kg reportedly produce effective analgesia without any
adverse effect on uterine blood flow, uterine activity or neonatal status23,24.
Remifentanil is a potent short-acting μ-opioid receptor agonist which is
rapidly metabolised in the mother and fetus. It has been used in PCA(patient
controlled analgesia) successfully with a setting of 20-40 µg bolus with a lock-
out interval of 2-3 minutes. The side effects associated are sedation,
respiratory depression and other opioid related effects. Remifentanil PCA for
labor analgesia is an important advance in the obstetric anesthesia
armamentarium, especially for parturients who do not want neuraxial
analgesia or when its use is contraindicated.25,26,27
Inhalational agents:
Until 1983 when the central midwives board withdrew approval for the
use of trichloroethylene by unsupervised midwives, there were 3 agents
available for use Nitrous oxide, trichloroethylene and methoxyflurance.
Trichloroethylene commonly causes nausea and vomiting and its
sweet smell may be unpleasant. Its use in labour is now uncommon.
Analgesia produced by Methoxyflurance persists into the period after
inhalation ceases. Nausea and vomiting are uncommon and although
inorganic fluoride concentrations are increased in both mother and infant, the
19
risk of renal damage seems negligible as long as inhalation is restricted to low
concentrations for limited periods.
Nitrous oxide was first used as an obstetric analgesic by Klikowitsch
in 1881. It became widely used with the introduction of the Minnitl apparatus
(1934) which delivered a mixture of nitrous oxide in air. In the early 1960’s the
currently available 50:50 prepared mixture of nitrous oxide and oxygen
(entonox) was described by Tunstall(1961). Entonox is employed as aself
administered intermittent inhalation which if used in the correct manner can
produce acceptable levels of analgesia. The effectiveness of entonox in
preventing the pain of labour is of approximately the same order as pethidine.
This has been stated by Beazley et al (1967) as 23% total success but 40%
total failure. It should be possible for 82% of mother to obtain substantial
benefit from inhalational analgesia when properly managed by the midwife.
Isoflurane, a volatile anesthetic agent has been used in a 0.75%
concentration in oxygen (Mc Leonetal 1985) where it produced good
analgesia but with a higher degree of drowsiness. More recently it has been
used in a 0.2% concentration in entonox (Wee et al 1993) where it produced
superior analgesia to entonox alone with no increase in drowsiness.
Sevoflurane, a volatile anaesthetic agent, because of its short onset
and offset of action, appears to be a best suited inhalational agent for labour
analgesia. It is used in the concentration of 0.8% with oxygen. It can provide
useful pain relief during the first stage of labour, and to a greater extent than
Entonox. Although greater sedative effects were experienced with
sevoflurane, it was preferred to Entonox(Yeo ST 2007).28.
20
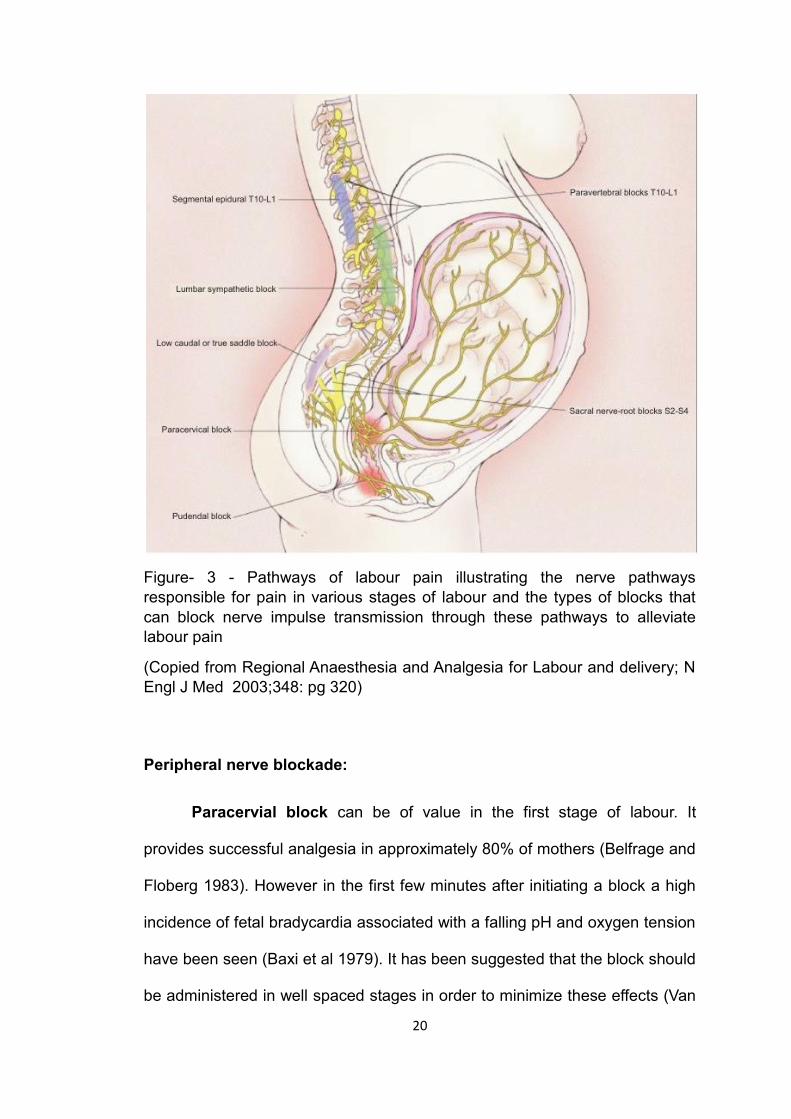
Figure- 3 - Pathways of labour pain illustrating the nerve pathways
responsible for pain in various stages of labour and the types of blocks that
can block nerve impulse transmission through these pathways to alleviate
labour pain
(Copied from Regional Anaesthesia and Analgesia for Labour and delivery; N
Engl J Med 2003;348: pg 320)
Peripheral nerve blockade:
Paracervial block can be of value in the first stage of labour. It
provides successful analgesia in approximately 80% of mothers (Belfrage and
Floberg 1983). However in the first few minutes after initiating a block a high
incidence of fetal bradycardia associated with a falling pH and oxygen tension
have been seen (Baxi et al 1979). It has been suggested that the block should
be administered in well spaced stages in order to minimize these effects (Van
21
Dorsten at al 1981). This complication has led to a marked diminution of its
use worldwide, although its success and simplicity might justify
reinvestigation.
Pudendal nerve block is almost always used to facilitate operative
vaginal delivery and is usually performed by the obstetrician. Local infiltration
of the perineum may be necessary as one study showed that bilateral
pudendal nerve block was not totally effective in nearly 50% of cases.
Central neuraxial blockade:
Lumbar epidural block
Lumbar epidural is currently the gold standard for pain relief in
obstetrics. Epidural analgesia provides the most effective form of pain relief
devised so far for labour and delivery3,29. The establishment of an epidural
service requires committed individuals and the precence of an anaethetist in
the labour ward, as well as equipment and staff education.
Corning has been credited with being the first to use epidural analgesia
in 1885. For many years caudal rather than lumbar epidural blockade was the
preferred method of obstetrics and postoperative pain relief. The use of
Tuohy’s needle in 1949 and the use of continuous catheter technique in both
caudal and lumbar epidural played a major part in enabling improvement in
epidural neural blockade.
Early 1970s saw an increased understanding of the segmental
blockade and its advantages with minimal local anesthetic dosage, thus
reducing the toxicity.
22
Caudal extradural block
Caudal extradural block is useful in the late first stage and second
stage of labour. It provides good relaxation of the perineal muscles. Problems
include a relatively high forceps rate, attributed to abnormalities of rotation of
the fetal head due to relaxation of the pelvic floor.
Intrathecal block
Single shot spinal have limited utility in early labour and are more
useful in the second stage of labour. It is an easier block than epidural
blockade and provides good relaxation for the pelvic musculature.
Disadvantages citied include post dural puncture headaches. However its
incidence is low with the use of fine pencil point (26 or 27G) needles.
Combined spinal epidural (CSE)
Since the introduction of this technique in the early 1980’s it has gained
increasing popularity for analgesia in labour and delivery. Because CSE has
a higher ambulatory potential it has been called the walking epidural. The
advantages are rapid and excellent pain relief, lower drug usage, and can be
used in advanced labour and in very demanding and uncooperative patients.
Requirements of a satisfactory analgesic technique in labour are as
follows (after Bromage)30
1) Safety
2) Effective analgesia throughout painful periods of labour.
3) No depressant effect on the maternal respiratory or cardiovascular
system.
23
4) No depressant effects on the progress of labour.
5) No depressant effects on the baby before or after delivery.
6) No unpleasant maternal side effects.
7) High technical success rate.
24
ASSESSEMENT OF ACUTE PAIN16
Pain is a uniquely personal symptom with no reliable objective signs,
so we have to accept an individual’s “self-report” of the severity of the pain
they are experiencing. A variety of “self-reporting” pain severity scoring
systems are used for adults; they correlate well and are generally reliable. It is
important that patients understand the method used, what us being assessed,
and why, and that the same method continues to be used to ensure reliability
and avoid confusion.
Categorical rating scales (CRS)
Frequently used to assess postoperative pain because it is a widely
applicable verbal method that can employ different descriptors of pain, e.g. No
pain, mild pain, moderate pain, severe pain.
Visual analog scale (VAS)
Employs a 10-cm draw line with the left anchor point descriptor labeled
“no pain’’ and the right-sided equivalent labeled “worst possible pain”. It
requires patients to mark their current pain severity on the continuum. The
VAS score is the measured distance from the “no pain” point to the pain
estimate.
Verbal numerical rating scale (VNRS)
Asks patient to estimate their pain severity as a number,”0” being no
pain and “10”being the worst possible pain. VNRS is easy to use, has better
responsiveness and better compliance.31Studies have shown NRS and VAS
have similar sensitivity.32 Beilin(2003)33 found NRS useful in the parturient
patients. Hence in this study we decided to use VNRS as the pain scoring
system.
25
Labour Epidural Analgesia
Of all the various modalities of pain relief available, Neuraxial labor
analgesia(most commonly epidural or combined spinal-epidural) is the most
effective method of pain relief during childbirth, and the only method that
provides complete analgesia without maternal or fetal sedation.3 Recent
Cochrane review on epidural analgesia has also come to the same
conclusion. Though CSEA is growing by leaps and bounds and offers effective
analgesia, we have limited our study to Continuous Epidural Analgesia.
26
ANATOMY OF EPIDURAL SPACE
Definition13
Epdidural Space is a potential space within the bony cavity of the
spinal canal outside the dural sac. It extends from foramen magnum to
coccyx communicating laterally with paravertebral space through the
intervertebral formina.
Boundaries35
Superiorly -The foramen magnum where the periosteal and spinal
layers of dura fuse together.
Inferiorly - The Sacrococygeal ligament.
Anteriorly - The posterior longitudinal ligament covering the posterior
aspect of the vertebral bodies and the intervertebral disc.
Posteriorly - Ligamentum flavum and the periosteum of the laminae.
Laterally - The pedicles of the spinal column and the intervertebral
foramina containing their neural elements.
Contents of the epidural space
The epidural space contains nerve roots that traverse it from foramina
to peripheral location, fat, areolar tissue, lymphatics and blood vessels, which
include the well organized Batson venous plexus.36
27
Epidural Veins
The epidural venous plexus is a valveless system, well known as
Batson venous plexus37. The veins form a network that run in four main trunks
along the space. They communicate with venous rings at each vertebral level,
with the basivertebral veins on the posterior aspect of each vertebral body
and with the ascending and deep cervical, intercostals, iliolumbar and lateral
sacral veins. They connect the pelvic veins below with the intracranial veins
above, so that air or other local anaesthetic solution injected into one of them
may ascend straight to the brain31.
Chronically increased intra-abdominal pressure or obstruction of the
inferior vena cava (as in late trimester of pregnancy or in the presence of
large intra abdominal tumour) can distend the epidural venous plexus, with
important implications for epidural anaesthesia.
Arterial Supply
Arteries enter the epidural space at each intervertebral foramen and
supply adjacent vertebra, ligaments and spinal cord. These arteries are from
the vertebral, deep cervical, ascending cervical, intercostal and lumbar and
iliolumbar arteries. They anastamose with their neighbors above and below,
cross the midline and lie chiefly in the lateral parts of the epidural space.
Fat and Areolar Tissue13
The epidural space is always said to contain fat, but since dural sac
virtually fills the bony spinal canal, this usually amounts to no more than a thin
transparent film of areolar tissue.
28
Nerve Roots13
31 pairs of spinal nerves with their dural cuffs traverse the space on
their way to the intervertebral foramina, the lower ones traveling at an
increasingly oblique angle.
Epidural Space in Pregnancy
The epidural space in parturients is at a distance of about 4-5cm from
the skin. The distance from the postero-medial border of ligamentum flavum
to the duramater is greatest in the second lumbar interspace ranging between
4mm to 8mm. Hence an epidural needle interested by the midline approach
should enter the space as close to the midline as possible to maximize the
distance between the ligamentum flavum and the dura38.
Hormonal changes affect vertebral ligamentous structure and may
make the ligamentum flavum feel softer39. Pregnant patients do not flex their
lumbar spine optimally, which may narrow the interspinous spaces and move
the line between interiliac crests [Tuffier’s line] more cephalad35.
Pregnancy induced widening of the pelvis may result in a head down
tilt of the spine in the lateral position potentially affecting the spread of
drugs40. Parturients may have presacral edema, making landmark
identification more difficult.
Epidural Volume13,36
The epidural veins are veins of the vertebral venous plexus, which form
an alternative pathway by which blood can reach the heart from the lower
extremity. This is of special Importance in pregnancy for compensating for the
obstruction to the inferior vena cava. In consequence, the epidural veins are
29
dilated and engorged. Since the total volume of the epidural space is fixed,
the engorged veins act as a space – occupying lesion to reduce the volume of
the extravascular portion of the space. Hence the local anaesthetic solution
injected in the epidural space will spread more extensively, reducing the dose
requirement of lumbar epidural analgesia in pregnancy. Also puncture of
engorged veins by an epidural catheter tip is more common during pregnancy.
Epidural Pressure13
In non-pregnant subjects the pressure in the lumbar epidural space is
normally 1 cm H2O. In early labour, between contractions, pressure in the
lateral position averages 1.63 cm H2O and rises to between 4-10 cm H2O by
the end of the first stage. Assuming the supine position will increase epidural
space pressure by upto 50% and this is proportional to the degree of inferior
vena caval obstruction. Uterine displacement will moderate the rise
prouduced in this position41.
Clinical Significance
The pressure in the epidural space is positive during labour. So
methods of identifying the space that depend on negative pressure should not
be used.
During uterine contraction the reflex increase in abdominal muscle tone
and the sudden efflux of blood from the contraction myometrium into the
venous system contribute to a further rise in epidural space pressure from 2-
8cm H2O, even in lateral position. Adequate epidural pain relief minimizes the
pressure rise produced during contraction13.
30
Reasons for decrease in local anesthetic doses are:
1. Decrease in epidural space volume
2. Increased lordosis
3. Progesterone effect
4. Sensitivity to local anesthetic agent
5. During uterine contraction epidural space pressure increases
Taken together these changes may contribute to the observation that
pregnancy increases the extent of epidural block produced by a given dose of
drugs.42,43
Site of Action13
When a solution of a local anaesthetic is injected into the epidural
space, it may exert its effects.
1. On the nerve roots in the epidural space
2. On the nerves in the paravertebral spaces after they have shed their
dural sheaths
3. On the nerve roots in the subarachnoid space after inward diffusion of
drug across the dura
31
Sensitivity of Local Anaesthetic Agents
Nerves from pregnant animals (including humans) appear more
susceptible to local anaesthetic blockade. In rats44,45 and humans42,46,
pregnancy enhances the effect of central and peripheral local anaesthetics.
However, pregnancy does not enhance isolated spinal nerve root axon
susceptibility to bupivacaine47. Proposed mechanisms of enhanced neural
blockade during pregnancy include hormone related changes in the action of
spinal cord neurotransmitters, potentiation of the analgesic effect of
endogenous analgesic systems, increased permeability of the neural sheath
and other pharmacodynamic or pharmacokinetic difference between pregnant
and non-pregnant women48. Even during early pregnancy, the spread of
epidural local anaesthetic blockade is increased42, a phenomenon explained
by altered sensitivity to local anaesthetic as opposed to gross changes in
spinal column anatomy.
Figure-4
Technique of Labour
Epidural Analgesia
(Copied from Regional
Anaesthesia and
Analgesia for Labour
and delivery; N Engl J
Med 2003;348:pg 320)
32
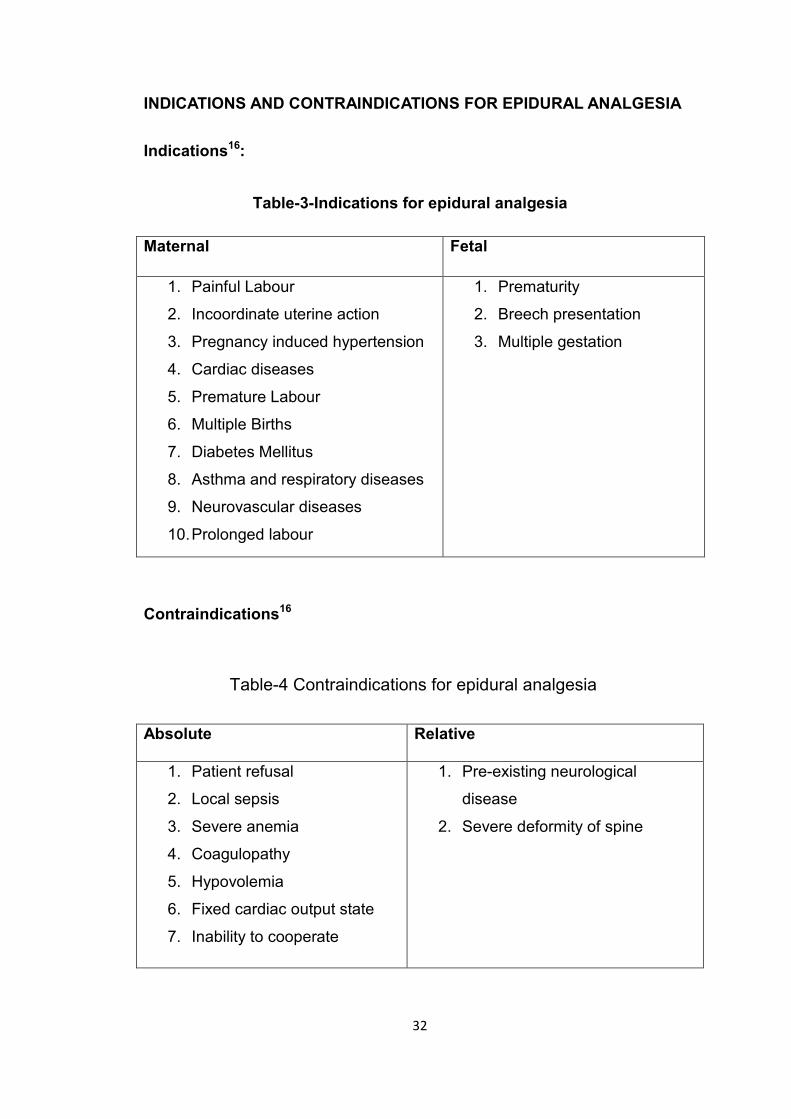
INDICATIONS AND CONTRAINDICATIONS FOR EPIDURAL ANALGESIA
Indications16:
Maternal Fetal
1. Painful Labour
2. Incoordinate uterine action
3. Pregnancy induced hypertension
4. Cardiac diseases
5. Premature Labour
6. Multiple Births
7. Diabetes Mellitus
8. Asthma and respiratory diseases
9. Neurovascular diseases
10. Prolonged labour
1. Prematurity
2. Breech presentation
3. Multiple gestation
Contraindications16
Absolute Relative
1. Patient refusal
2. Local sepsis
3. Severe anemia
4. Coagulopathy
5. Hypovolemia
6. Fixed cardiac output state
7. Inability to cooperate
1. Pre-existing neurological
disease
2. Severe deformity of spine
Table-4 Contraindications for epidural analgesia
Table-3-Indications for epidural analgesia
33
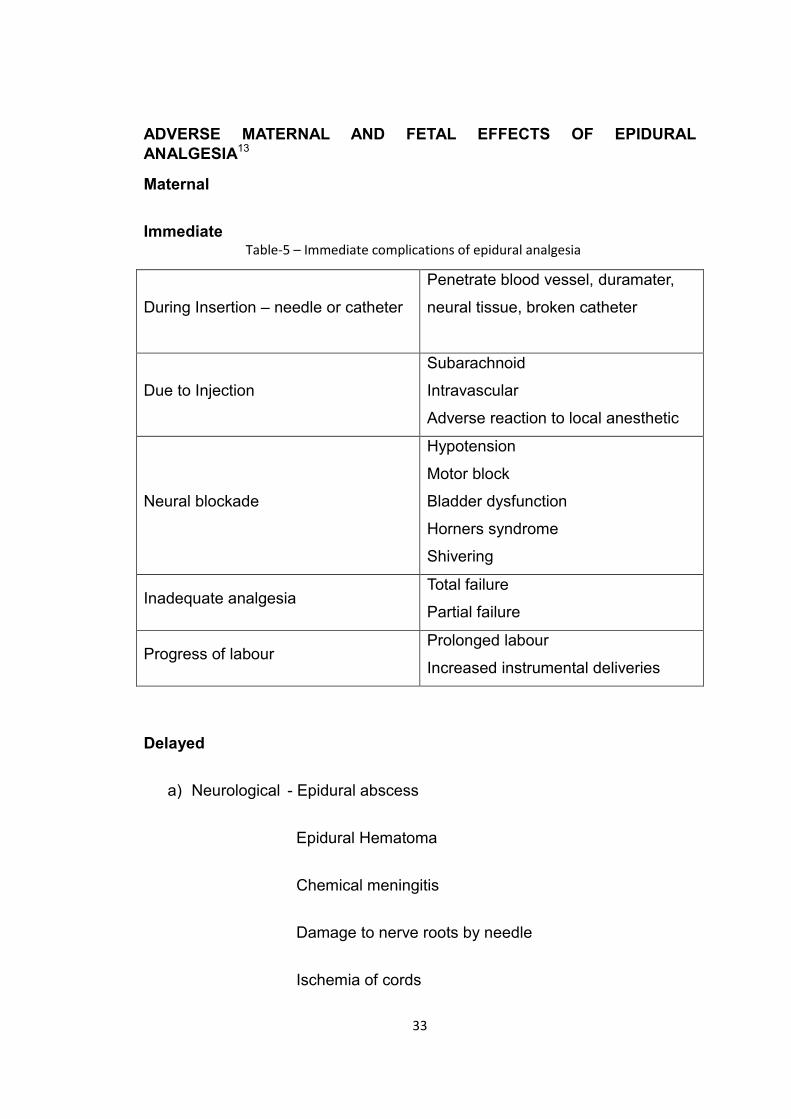
ADVERSE MATERNAL AND FETAL EFFECTS OF EPIDURAL
ANALGESIA13
Maternal
Immediate
During Insertion – needle or catheter
Penetrate blood vessel, duramater,
neural tissue, broken catheter
Due to Injection
Subarachnoid
Intravascular
Adverse reaction to local anesthetic
Neural blockade
Hypotension
Motor block
Bladder dysfunction
Horners syndrome
Shivering
Inadequate analgesia Total failure
Partial failure
Progress of labour Prolonged labour
Increased instrumental deliveries
Delayed
a) Neurological - Epidural abscess
Epidural Hematoma
Chemical meningitis
Damage to nerve roots by needle
Ischemia of cords
Table-5 – Immediate complications of epidural analgesia
34
b) Headache - Post dural puncture
c) Soreness at the site of needle entry
d) Broken cannula tip retention
Fetal
Immediate
a) Direct effect of local anesthetic
b) Indirect effect – Changes in uterine blood flow, Maternal hypoxia,
Changes in progress and outcome of labour
Delayed
a) Neurobehavioral Changes
PROBLEMS ASSOCIATED WITH EPIDURAL ANALGESIA
Hypotension:
It is a relatively common complication that can be easily prevented by
preloading the patient with ringer lactate solution (10-15ml/kg) and avoiding
aortocaval compression. Treatment includes more fluids, oxygen, and
ephedrine 3-6 mg IV in incremental doses49.
Dural puncture and post dural puncture headache:
The reported incidence of inadvertent dural puncture varies from 0.2-
7%49. Though a rare complication, it has disturbing sequelae of post dural
puncture headache. Its incidence in obstetrics remains about 1-5% even with
35
very small-bore spinal needle and optimized tip. PDPH has a major impact on
morbidity and on the patient’s satisfaction50.
The maintenance of high intake of fluids either orally or intravenously
has been suggested as a means of alleviating the symptoms of PDPH
(Kaikinen. S. Kaukinen 1981). Caffeine is commonly recommended for the
treatment of PDPH because of its cerebral vasoconstrictor properties.
Camann et al51 evaluated the use of caffeine for the treatment of PDPH and
found ab Improvement in 18 of the 20 patients. Epidural blood patch remains
the gold, standard treatment for PDPH with success rate of greater than 90%
and a low complication rate52.
Total spinal block
Total spinal block with rapidly developing hypotension,
unconsciousness, and respiratory paralysis may occur if the drug us
accidentally injected intrathecally. However this complication can be avoided
by a cautious approach and using test dose before the injection of the drug.
Since a smaller dose is used in selective epidural block, recovery will be more
rapid.
Blood tap:
The epidural venous plexus distortion present during pregnancy further
increases during uterine contractions. As a result, upto 10% of obstetric
epidural needle insertion amy involve a bloody tap and catheterization of
epidural vein may occur in upto 9% of cases (Verniquet 1980). Repositioning
the catheter in an adjacent space in the event of bloody tap can prevent
intravenous injection of the local anesthetic49.
36
Backache:
The incidence of backache after epidural anaesthesia has varied from
15-45%. However similar rates of 10.5 – 40% have been reported following
vaginal delivery without epidural block (Grovel L.H, Moir D.D, Mc Arthur) and
therefore other causes of backache need to the explored. Ronbuttler53 in his
study has found that back pain following epidural anaesthesia is common but
persistent back pain is much less common and a previous history of backache
increases the likelihood of postpartum backache following epidural
anaesthesia.
Shivering:
Incidence of shivering, in parturients receiving epidural analgesia
ranges from 20-50%(Webb 1981) with an incidence of 22% in parturients
without epidural analgesia. Thus an epidural vasodilatation cannot be wholly
responsible and other mechanisms such as maternal immunoglobulin
response to amniotic fluid or fetal cells has been suggested.
Urinary retention:
When the epidural block affects the sacral segments the mother may
not be aware of full bladder which may impede the progress of labour. Thus
the mother should be encouraged to void regularly and If required intermittent
catheterization should be done49.
Non fatal neurological complications:
Recent survey indicates that the incidence of non-fatal neurological
complication various from 1 in 7000 to 1 in 14,000(Scott D.B.) of which
37
commonest was single nerve neuropathy. In most cases the problem resolved
spontaneously but recovery may take several months49.
THE ADVANTAGES OF OBSTETRIC EPIDURAL ANALGESIA:
In obstetric units where successful epidural service is established,
almost any medical or obstetric complication may be regarded as an
indication for regional analgesia. This is largely because it may be desirable to
avoid both the stress of painful labour and the risk of general anaesthesia
should operative delivery be necessary.
Pain relief:
It is a single most important indication for epidural analgesia, which not
only provides physiological benefits to both mother and fetus but also makes
a parturient more comfortable, less fatigued and therefore more cooperative.
Hypertension:
Pregnancy induced hypertension is the commonest obstetric indication
for epidural analgesia. Epidural blockade is of little value in the absence of
pain,but in labour it has generally been found to control hypertension
successfully and better than hydralazine and magnesium sulphate (Neri et al
1986). Epidural analgesia prevents the sympathoadrenal over activity that is
characteristic of preeclampsia54, produces favorable hemodynamic changes
(Newsome et al 1986) and a consistent improvement in intervillous blood
flow55. Early work also showed how the complete analgesia could minimize
the chance of seizures (Moir et al 1972). Moreover, general anaesthesia that
is particularly risky in the presence of laryngeal edema can be avoided. There
38
can be little doubt however of its value in preeclampsia provided the catheter
is inserted before the onset of any coagulopathy.
Cardiac disease:
These patients have a propensity towards decompensation during
labour. Epidural pain relief can minimize the adverse effect of increased
cardiac output due to pain or anxiety.
Pulmonary disease:
Epidural analgesia is of benefit in pulmonary disease because it avoids
hyperventilation associated with painful contraction.
Trial of labour:
Review of labour in several 100 women with previous caesarean
sections suggest that epidural anaesthesia in no way masks the danger of
scar dehiscence or rupture (Carlsson et al 1980, Uppington 1983). The pain
from the scar and pain from the uterine contractions are felt at the same site
and the scar is most likely to be stressed during a contraction. Epidural local
anaesthetic more readily blocks the pain of uterine contraction (which is
conducted by AD fibres) than pathological pain, (predominantly C fibre
stimulation) so that it may aid in the diagnosis of scar dehiscence.
Rowbottom56 in his study found that the pain of uterine rupture was relieved
by bupivacaine 0.375% 6ml but not masked by the addition of fentanyl 25mcg
to bupivacaine 0.25% 6ml. The same phenomenon has been observed with
placental abruption in which epidural blockade does not abolish the pain
(Paterson 1979). Analgesia given early in these patients may reduce maternal
39
exhaustion and subsequently be converted to epidural anaesthesia in case a
caesarean section is warranted.
Conversion to obstetric anaesthesia:
If an epidural catheter is already insitu, in the event of fetal distress or
any need of caesarean section; it can easily be converted to anesthesia by
simply altering the dose of the drug, and the position of the patient, thus,
saving time and effort.
Preterm labour and twin pregnancy:
Osbourne et al suggested that the use of epidural analgesia in preterm
labour did improve the outcome for baby. Labour is less stressful and delivery
is less traumatic. Epidural analgesia was associated with reduced neonatal
mortality rate among low birth weight babies (David and Roren 1976).
Likewise the outlook in twin pregnancy particularly for the second twin is
improved (Crawford 1987).
Benefit in incoordinate uterine action:
By decreasing the catecholamine secretion associated with labour
pain, epidural block can improve uterine contractility and rhythmicity and is
especially indicated in cases of incoordinate uterine action.
Fetal indications:
Preterm fetus, Breech Presentation & Multiple pregnancy-
In these conditions an epidural block allows a more controlled delivery
because of relaxed pelvic floor muscles and a decreased urge to push.
40
Decreased blood loss:
It is evidenced following vaginal delivery under epidural block as
compared to delivery without epidural block (Bound A.G., Minor D.D). This
can be explained by the epidural induced peripheral vasodilatation that leads
to venous pooling and thus decreased cardiac output. Also, since the pelvic
viscera receive their vasomotor innervation (motor efferent) from T5 to T10,
which is above the level of epidural blockade (only T11 to L1 segment is
blocked in selective epidural) the baroreceptor response can produce
compensatory vasoconstriction of the pelvic viscera via the unblocked T5 to
T10 a segment and thus, lead to diminution of bleeding49.
Modes of epidural:
The epidural is usually initiated with a loading dose of either local
anaesthetic or local anaesthetic with opioids. Following this there are different
types of maintenance regimes. They are
1.Intermittent boluses – The patients are given intermittent boluses when
their pain increases. The maternal satisfaction is good & quality of analgesia
is good. But there may be peaks and valleys in pain relief. There is greater
chance of risk of hypotension, local anaesthetic toxicity and motor block.
2.Continuous infusion – The patients are on a background infusion of
local anaesthetic and opioids and breakthrough pain is treated with top-up
boluses. The maternal satisfaction, quality of analgesia is good. The analgesia
is also continuous without the peaks and troughs. The amount of drug
utilization may be high. The risk of hypotension, motor block is intermediate.
41
3.PCEA(patient controlled epidural analgesia) – Here the patient
controls her own medications. The PCEA can be given as demand only or
with continuous infusion The bolus, lock-out interval, maximum dose per hour
are set with or without a basal infusion. The maternal satisfaction is the
highest in this group, since it gives the pain control in the hands of patient
itself. The quality of analgesia is good, the drug utilization minimal. The risk of
local anaesthetic toxicity, hyotension and motor blockade is minimal. Demand
only PCEA has an increased incidence of breakthrough pain and higher pain
scores.
42
ROPIVACAINE
It is a new, long-acting local amide anesthetic with similarities in
structure, pharmacology and pharmacokinetics to that of bupivacaine.
Ropivacaine is a pure (S-isomer) enantiomer.
STRUCTURAL FORMULA
MECHANISM OF ACTION 57,58
Ropivacaine reversibly interferes with the entry of sodium into the
nerve cell membranes, leading to decreased membrane permeability to
sodium and raises the threshold for electrical excitability. It blocks the
generation and the conduction of nerve impulses, presumably by increasing
the threshold for electrical excitation in the nerve, by slowing the propagation
of the nerve impulse, and by reducing the rate of rise of the action potential.
The order of blockade affecting the nerve fibres is: autonomic, sensory and
motor; and the effect disappears in the reverse order. Clinically the order of
loss of sensation is: pain, temperature, touch, proprioception and skeletal
muscle tone. Repeated activation by a train of depolarizing pulses increases
the inhibitory effects of ropivacaine and produces a hyperpolarizing shift.
Figure – 5 - Structure of Ropivacaine
43
PHYSIOCHEMICAL PROPERTIES
It is chemically described as S-(-)-1-propyl-2',6'-pipecoloxylidide
hydrochloride monohydrate. The drug substance is a white crystalline powder,
with a molecular formula of C17H26N2O·HCl·H2O and molecular weight of
328.89. The pKa of ropivacaine is approximately the same as bupivacaine
(8.1) However, ropivacaine has an intermediate degree of lipid solubility
compared to bupivacaine and mepivacaine. The specific gravity of
ropivacaine solution ranges from 1.002 to 1.005 at 25°C.
PHARMACOKINETICS 58
ABSORPTION
The systemic concentration of ropivacaine is dependent on the total
dose and concentration of drug administered, the route of administration, the
patient's hemodynamic/circulatory condition, and the vascularity of the
administration site. From the epidural space, ropivacaine shows complete and
biphasic absorption. The half-lives of the 2 phases, (mean ± SD) are 14 ± 7
minutes and 4.2 ± 0.9 h, respectively. The slow absorption is the rate limiting
factor in the elimination of ropivacaine which explains why the terminal half-
life is longer after epidural than after intravenous administration. Ropivacaine
shows dose proportionality up to the highest intravenous dose studied, 80 mg,
corresponding to a mean ± SD peak plasma concentration of 1.9 ± 0.3 µg/mL
DISTRIBUTION
After intravascular infusion, ropivacaine has a steady state volume of
distribution of 41 ± 7 litres. Ropivacaine is 94% protein bound, mainly to α1-
44
acid glycoprotein. An increase in total plasma concentrations during
continuous epidural infusion has been observed, related to a postoperative
increase of α1-acid glycoprotein. Variations in unbound, i.e.,pharmacologically
active concentrations have been less than in total plasma concentration.
Ropivacaine readily crosses the placenta and equilibrium in regard to
unbound concentration will be rapidly reached.
METABOLISM
Ropivacaine is extensively metabolized in the liver, predominantly by
aromatic hydroxylation mediated by cytochrome P450 (CYP)1A2 to 3-hydroxy
Ropivacaine and by N-dealkylation by CYP3A4 to 2',6'-pipecoloxylidide
(PPX).After a single IV dose, approximately 37% of the total dose is excreted
in the urine as both free and conjugated 3-hydroxy ropivacaine. Low
concentrations of 3-hydroxy ropivacaine have been found in the plasma.
Urinary excretion of the 4-hydroxy ropivacaine, and both the 3-hydroxy N-de-
alkylated (3-OH-PPX) and 4-hydroxy N-de-alkylated (4-OH-PPX) metabolites
account for less than 3% of the dose. An additional metabolite, 2-hydroxy-
methyl-ropivacaine has been identified but not quantified in the urine.
The N-de-alkylated metabolite of ropivacaine (PPX) and 3-OH-
ropivacaine are the major metabolites excreted in the urine during epidural
infusion. Total PPX concentration in the plasma was about half as that of total
ropivacaine; however, mean unbound concentrations of PPX was about 7 to 9
times higher than that of unbound ropivacaine following continuous epidural
infusion up to 72 hours. Unbound PPX, 3-hydroxy and 4-hydroxy ropivacaine,
45
have a pharmacological activity in animal models less than that of
ropivacaine.
There is no evidence of in vivo racemization in urine of ropivacaine.
ELIMINATION
The kidney is the main excretory organ for most local anesthetic
metabolites. In total, 86% of the ropivacaine dose is excreted in the urine after
intravenous administration of which only 1% relates to unchanged drug.
Ropivacaine has a mean ± SD total plasma clearance of 387 ± 107 mL/min,
an unbound plasma clearance of 7.2 ± 1.6 L/min, and a renal clearance of 1
mL/min.
The mean ± SD terminal half-life is 1.8 ± 0.7 h after intravascular
administration and 4.2 ± 1.0 h after epidural administration.
DIFFERENTIAL CONDUCTION BLOCK
With low concentrations of local anaesthetic, selective blockade of pre -
ganglionic sympathetic nervous system B fibres occur. Slightly higher
concentrations interrupt conduction in small C fibres and small and medium
sized Aδ fibres with loss of pain and temperature sensation.
PHARMACODYNAMICS
Systemic absorption of ropivacaine can produce effects on the central
nervous and cardiovascular systems. At blood concentrations achieved with
therapeutic doses, changes in cardiac conduction, excitability, refractoriness,
contractility, and peripheral vascular resistance have been reported. Toxic
blood concentrations depress cardiac conduction and excitability, which may
46
lead to atrioventricular block, ventricular arrhythmias and to cardiac
arrest,sometimes resulting in fatalities. In addition, myocardial contractility is
depressed and peripheral vasodilation occurs, leading to decreased cardiac
output and arterial blood pressure. Animal studies have demonstrated that the
cardiac toxicity of ropivacaine is less than bupivacaine as ropivacaine causes
significantly less depression of cardiac contractility (QRS widening).59
Following systemic absorption, ropivacaine can produce central
nervous system stimulation, depression or both. Apparent central stimulation
is usually manifested as restlessness, tremors, shivering, progressing to
convulsions, followed by depression and coma, progressing ultimately to
respiratory arrest. However, ropivacaine may have a primary depressant
effect on the medulla and on higher centers. The depressed stage may occur
without a prior excited stage.
DOSAGE AND ADMINISTRATION
The rapid injection of a large volume of ropivacaine solution should be
avoided and fractional (incremental) doses should always be used. The
smallest dose and concentration required to produce the desired result should
be administered.
The dose of ropivacaine administered varies with the anesthetic
procedure, the area to be anesthetized, the vascularity of the tissues, the
number of neuronal segments to be blocked, the depth of anaesthesia and
degree of muscle relaxation required, the duration of anaesthesia desired,
individual tolerance, and the physical condition of the patient. Patients in poor
general condition due to aging or other compromising factors such as partial
47
or complete heart conduction block, advanced liver disease or severe renal
dysfunction require special attention although regional anaesthesia is
frequently indicated in these patients. To reduce the risk of potentially serious
adverse reactions, attempts should be made to optimize the patient's
condition before major blocks are performed, and the dosage should be
adjusted accordingly.
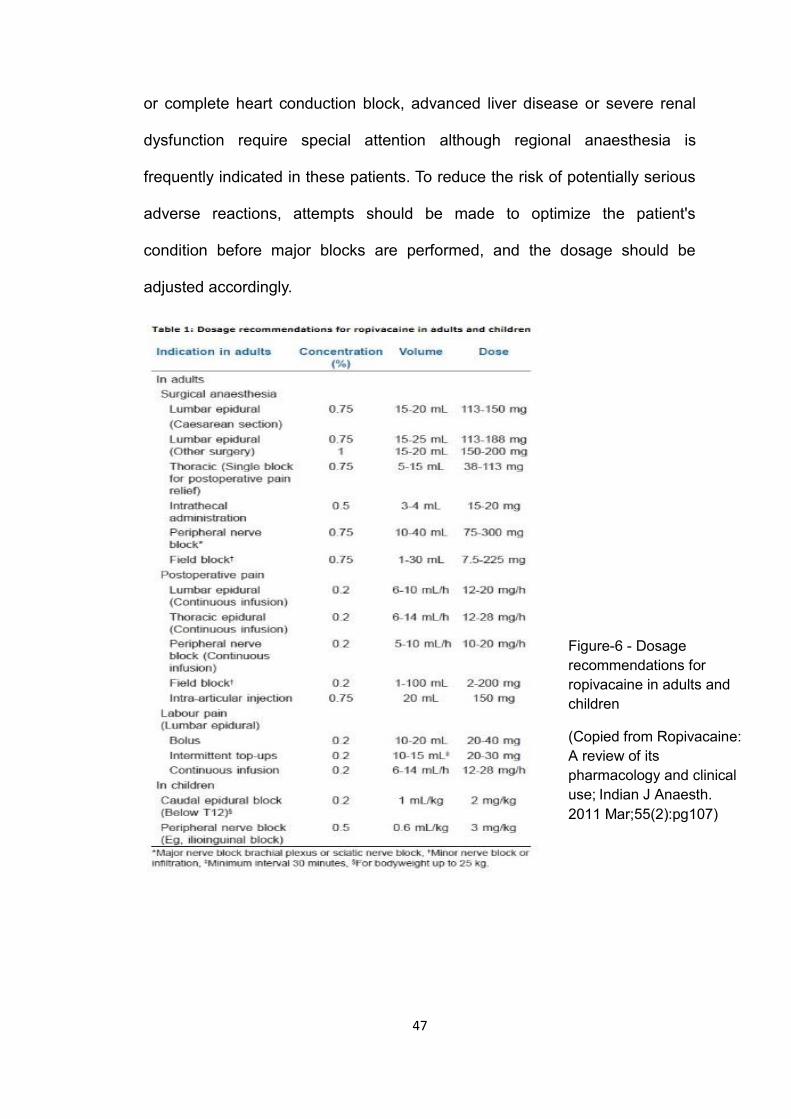
Figure-6 - Dosage
recommendations for
ropivacaine in adults and
children
(Copied from Ropivacaine:
A review of its
pharmacology and clinical
use; Indian J Anaesth.
2011 Mar;55(2):pg107)
48
SIDE EFFECTS:
INCIDENCE (≥5%)
For the indications of epidural administration in surgery, cesarean
section, postoperative pain management, peripheral nerve block, and local
infiltration,, the following treatment-emergent adverse events were reported
with an incidence of ≥5% in all clinical studies(N=3988):hypotension (37.0%),
nausea(24.8%), vomiting(11.6%), bradycardia(9.3%),fever(9.2%), pain(8.0%),
postoperative complications(7.1%), anemia(6.1%), paraesthesia(5.6%),
headache(5.1%), pruritus (5.1%), and back pain (5.0%).
INCIDENCE (1-5%)
Urinary retention, dizziness, rigors, hypertension, tachycardia, anxiety,
oliguria, hypoesthesia,chest pain, hypokalemia, dyspnea, cramps, and urinary
tract infection.
PRECAUTIONS:
Ropivacaine should be used in patients receiving CYP1A2(involved in
metabolizing Ropivacaine to 3-hydroxy Ropivacaine,a major metabolite)
inhibitors like fluvoxamine and enoxacin,since this may lead to an increased
plasma concentration of Ropivacaine.
49
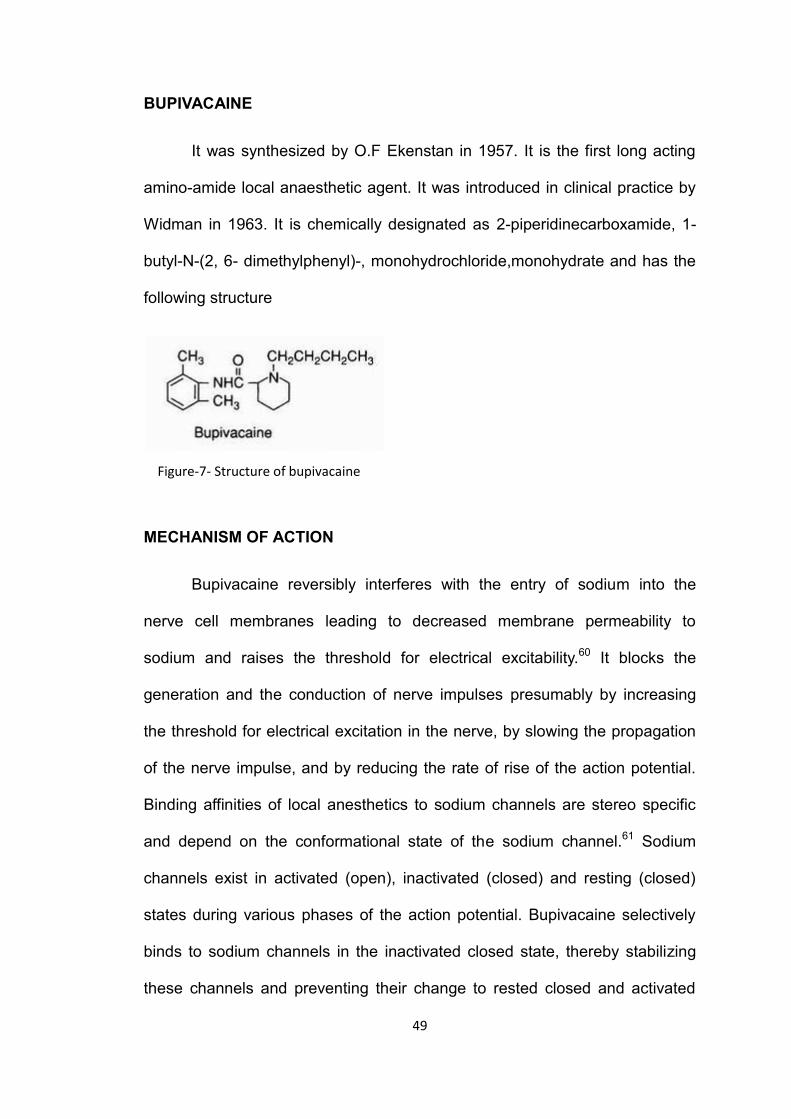
BUPIVACAINE
It was synthesized by O.F Ekenstan in 1957. It is the first long acting
amino-amide local anaesthetic agent. It was introduced in clinical practice by
Widman in 1963. It is chemically designated as 2-piperidinecarboxamide, 1-
butyl-N-(2, 6- dimethylphenyl)-, monohydrochloride,monohydrate and has the
following structure
MECHANISM OF ACTION
Bupivacaine reversibly interferes with the entry of sodium into the
nerve cell membranes leading to decreased membrane permeability to
sodium and raises the threshold for electrical excitability.60 It blocks the
generation and the conduction of nerve impulses presumably by increasing
the threshold for electrical excitation in the nerve, by slowing the propagation
of the nerve impulse, and by reducing the rate of rise of the action potential.
Binding affinities of local anesthetics to sodium channels are stereo specific
and depend on the conformational state of the sodium channel.61 Sodium
channels exist in activated (open), inactivated (closed) and resting (closed)
states during various phases of the action potential. Bupivacaine selectively
binds to sodium channels in the inactivated closed state, thereby stabilizing
these channels and preventing their change to rested closed and activated
Figure-7- Structure of bupivacaine
50
open states in response to nerve stimulus. It binds to specific sites located on
the inner position of the sodium channels and obstructs the external openings
and maintains them in the inactivated closed state, which is not permeable to
sodium, so that the conduction of nerve impulses does not occur. On repeated
application of depolarization, partially depressed sodium ion current (tonic
inhibition) is further reduced leading to phasic inhibition called use dependent
block. The sole use of local anesthetic is less common than the use of local
anesthetic-opioid combination because of a significant failure rate (regression
of sensory block and inadequate analgesia) and relatively high incidence of
hypotension. In general, the progression of Anaesthesia is related to the
diameter, myelination and conduction velocity of affected nerve fibers.
Clinically, the order of loss of nerve function is as follows: (1) pain, (2)
temperature, (3) touch, (4) proprioception, and (5) skeletal muscle tone.
PHYSIOCHEMICAL PROPERTIES
Bupivacaine Hydrochloride is 2-Piperidinecarboxamide, 1-butyl-N-(2,6-
dimethylphenyl)-,monohydrochloride, monohydrate, a white crystalline powder
that is freely soluble in 95 percent ethanol, soluble in water, and slightly
soluble in chloroform or acetone. The pKa of bupivacaine is 8.1. However,
bupivacaine possesses a greater degree of lipid solubility and is protein
bound to a greater extent than lidocaine.
It is 95% protein bound. It is a chiral drug having a left(S) or right (R)
configuration. It is available for clinical use as racemic mixtures of the
enantiomers. It is 4 times more potent than lidocaine.
51
The dural permeability and the movement of local anaesthetic through
the sodium channel of the nerve membrane is claimed to be more dependent
on the molecular weight. The molecular weight of bupivacaine is 288: most
other local anesthetics are of smaller molecular weights.
High lipid solubility promotes diffusion through membranes, thereby
speeding the onset of action and also increasing the potency and duration of
effect. Higher the aqueous lipid solubility coefficient (343 for bupivacaine),
more rapid is the entry into the lipid membrane and longer is the duration of
action.
DIFFERENTIAL CONDUCTION BLOCK
With low concentrations of local anaesthetic, selective blockade of pre-
ganglionic sympathetic nervous system B fibres occur. Slightly higher
concentrations interrupts conduction in small C fibres and small and medium
sized A fibres with loss of pain and temperature sensation.
PHARMACOKINETICS
ABSORPTION
The rate of systemic absorption of local anesthetics is dependent upon
the total dose and concentration of drug administered, the route of
administration, the vascularity of the administration site, and the presence or
absence of epinephrine in the anesthetic solution. A dilute concentration of
epinephrine (1:200,000 or 5 mg/mL) usually reduces the rate of absorption
and peak plasma concentration of bupivacaine, permitting the use of
52
moderately larger total doses and sometimes prolonging the duration of
action.
The onset of action with bupivacaine is rapid and anaesthesia is long-
lasting. The duration of Anaesthesia is significantly longer with bupivacaine
than with any other commonly used local anesthetic. It has also been noted
that there is a period of analgesia that persists after the return of sensation,
during which time the need for potent analgesics is reduced.
DISTRIBUTION
Local anesthetics are bound to plasma proteins in varying degrees.
Generally, the lower the plasma concentration of drug, the higher the
percentage of drug bound to plasma proteins. Local anesthetics appear to
cross the placenta by passive diffusion. The rate and degree of diffusion is
governed by: (1) the degree of plasma protein binding, (2) the degree of
ionization, and (3) the degree of lipid solubility. Fetal/maternal ratios of local
anesthetics appear to be inversely related to the degree of plasma protein
binding, because only the free, unbound drug is available for placental
transfer. Bupivacaine, with a high protein binding capacity (95%), has a low
fetal/maternal ratio (0.2-0.4). First pass pulmonary extraction is dose
dependent.62
The extent of placental transfer is also determined by the degree of
ionization and lipid solubility of the drug. Lipid soluble, non-ionized drugs
readily enter the fetal blood from the maternal circulation.
53
Depending upon the route of administration, local anesthetics are
distributed to some extent to all body tissues, with high concentrations found
in highly perfused organs such as the liver, lungs, heart and brain.
Pharmacokinetic studies on the plasma profile of bupivacaine after
direct intravenous injection suggest a three-compartment open model. The
first compartment is represented by the rapid intravascular distribution of the
drug. The second compartment represents the equilibration of the drug
throughout the highly perfused organs such as the brain, myocardium, lungs,
kidneys, and liver. The third compartment represents an equilibration of the
drug with poorly perfused tissues, such as muscle and fat. The elimination of
drug from tissue depends largely upon the ability of binding sites in the
circulation to carry it to the liver where it is metabolized.
After injection of bupivacaine for caudal, epidural or peripheral nerve
block in man, peak levels of bupivacaine in the blood are reached in 30 to 45
minutes, followed by a decline to insignificant levels during the next 3 to 6
hours.
Various pharmacokinetic parameters of the local anesthetics can be
significantly altered by the presence of hepatic or renal disease, addition of
epinephrine, factors affecting urinary pH, renal blood flow, the route of drug
administration, and the age of the patient. The half-life of bupivacaine in
adults is 2.7 hours and in neonates 8.1 hours.
In clinical studies, elderly patients reached the maximal spread of
analgesia and maximal motor blockade more rapidly than younger patients.
Elderly patients also exhibited higher peak plasma concentrations following
54
administration of this product. The total plasma clearance was decreased in
these patients.
METABOLISM
Amide-type local anesthetics such as bupivacaine are metabolized
primarily in the liver via conjugation with glucuronic acid. Patients with hepatic
disease, especially those with severe hepatic disease, may be more
susceptible to the potential toxicities of the amide-type local anesthetics. The
major metabolite of bupivacaine is N-desbutyl bupivacaine.63 The clearance
rate is 0.47 litres/min.
EXCRETION
The kidney is the main excretory organ for most local anesthetics
(bupivacaine) and their metabolites. Urinary excretion is affected by renal
perfusion and factors affecting urinary pH.
Only 5% of bupivacaine is excreted unchanged in the urine. The
elimination half-life is 210 minutes. In infants and elderly the half life is
prolonged.
When administered in recommended doses and concentrations,
bupivacaine does not ordinarily produce irritation or tissue damage and does
not cause methemoglobinemia.
PHARMACODYNAMICS
Systemic absorption of local anesthetics (bupivacaine) can produce
effects on the central nervous and cardiovascular systems. At blood
concentrations achieved with therapeutic doses, changes in cardiac
55
conduction, excitability, refractoriness, contractility, and peripheral vascular
resistance have been reported. Toxic blood concentrations depress cardiac
conduction and excitability, which may lead to atrioventricular block,
ventricular arrhythmias and to cardiac arrest, sometimes resulting in fatalities.
In addition, myocardial contractility is depressed and peripheral vasodilation
occurs, leading to decreased cardiac output and arterial blood pressure.
Following systemic absorption, local anesthetics (bupivacaine) can
produce central nervous system stimulation, depression or both. Apparent
central stimulation is usually manifested as restlessness, tremors, shivering,
progressing to convulsions followed by depression and coma ultimately
laeding to respiratory arrest. However, the local anesthetics have a primary
depressant effect on the medulla and on higher centers. The depressed stage
may occur without a prior excited stage.
DOSAGE AND ADMINISTRATION
The rapid injection of a large volume of bupivacaine solution should be
avoided and fractional (incremental) doses should always be used. The
smallest dose and concentration required to produce the desired result should
be administered.
The dose of any local anesthetic administered varies with the
anesthetic procedure, the area to be anesthetized, the vascularity of the
tissues, the number of neuronal segments to be blocked, the depth of
anaesthesia and degree of muscle relaxation required, the duration of
anaesthesia desired, individual tolerance, and the physical condition of the
patient. Patients in poor general condition due to aging or other compromising
56
factors such as partial or complete heart conduction block, advanced liver
disease or severe renal dysfunction require special attention although regional
anaesthesia is frequently indicated in these patients. To reduce the risk of
potentially serious adverse reactions, attempts should be made to optimize
the patient's condition before major blocks are performed, and the dosage
should be adjusted accordingly.
In recommended doses, bupivacaine hydrochloride produces complete
sensory block, but the effect on motor function differs among the three
concentrations.
0.25%—when used for caudal, epidural, or peripheral nerve block, produces
incomplete motor block. Should be used for operations in which muscle
relaxation is not important, or when another means of providing muscle
relaxation is used concurrently. Onset of action may be slower than with the
0.5% or 0.75% solutions.
0.5%—provides motor blockade for caudal, epidural, or nerve block, but
muscle relaxation may be inadequate for operations in which complete
muscle relaxation is essential.
0.75%—produces complete motor block. Most useful for epidural block in
abdominal operations requiring complete muscle relaxation, and for
retrobulbar anaesthesia. Not for obstetrical anaesthesia.
The duration of anaesthesia with bupivacaine is such that for most
indications, a single dose is sufficient.
57
Maximum dosage limit must be individualized in each case after
evaluating the size and physical status of the patient, as well as the usual rate
of systemic absorption from a particular injection site. Most experience to date
is with single doses of bupivacaine up to 225 mg with epinephrine 1:200,000
and 175 mg without epinephrine; more or less drug may be used depending
on individualization of each case.
These doses may be repeated up to once every three hours. In clinical
studies to date, total daily doses up to 400 mg have been reported. Until
further experience is gained, this dose should not be exceeded in 24 hours.
The duration of anesthetic effect may be prolonged by the addition of
epinephrine.
These dosages should be reduced for young, elderly or debilitated
patients.
Bupivacaine is contraindicated for obstetrical paracervical blocks, and
is not recommended for intravenous regional anaesthesia (Bier Block).
Use in Epidural Anaesthesia
During epidural administration of bupivacaine, 0.5% and 0.75%
solutions should be administered in incremental doses of 3 mL to 5 mL with
sufficient time between doses to detect toxic manifestations of unintentional
intravascular or intrathecal injection. In obstetrics, only the 0.5% and 0.25%
concentrations should be used; incremental doses of 3 mL to 5 mL of the
0.5% solution not exceeding 50 mg to 100 mg at any dosing interval are
recommended. Repeat doses should be preceded by a test dose containing
epinephrine if not contraindicated. Use only the single dose ampoules and
58
single dose vials for caudal or epidural Anaesthesia; the multiple dose vials
contain a preservative and therefore should not be used for these procedures
FACTORS INFLUENCING ANAESTHETIC ACTIVITY
ADDITION OF VASOCONSTRICTOR: The duration of action of bupivacaine
is proportional to the time the drug is in contact with the nerve fibres. The
addition of vasoconstrictor like epinephrine will prolong the duration of action
of drug. However the effect of prolonging the duration of action by adding
epinephrine is less than that observed with lidocaine which is attributed to its
high lipid solubility.
DOSAGE OF THE DRUG: Increase in dose of bupivacaine either by larger
volume or more concentrated solution results in more profound depth,
prolonged duration and faster onset of block.
SITE OF INJECTION: Rapid onset and shorter duration occur with intrathecal
or subcutaneous infiltration of bupivacaine.
CARBONATION AND pH ADJUSTMENT: An increase in the pH of the drug
increases the amount of drug in the unionized for resulting in faster onset of
conduction blockade. Carbon dioxide raises the threshold for impulse firing by
changing the extent of channel inactivation at rest.
LIPOSOMAL LOCAL ANAESTHETICS: Large unilamellar vesicles that
exhibit a pH gradient can efficiently encapsulate bupivacaine and
subsequently provide a sustained release system that greatly increases the
duration of neural blockade when compared with plain local anaesthetic
solutions.64
59
SIDE EFFECTS
1. Allergic reactions
2. Systemic toxicity
ALLERGIC REACTIONS: They are less than 1% and are immunologically
mediated.65 The occurrence of rash, utricaria and laryngeal edema with or
without hypotension and bronchospasm during intradermal testing is highly
suggestive of allergic reactions.
SYSTEMIC TOXICITY:
Bupivacaine toxicity occurs due to excess plasma concentration of the
drug. The magnitude of systemic absorption depends on the dose
administered into the tissue, vascularity at the injection site, presence of
epinephrine in the solution. CNS manifestations occur with plasma
concentrations of 4.5-5.5mcg/ml.66 The features are numbness of tongue and
circumoral tissues, restlessness, vertigo, tinnitus, difficulty in focusing, slurred
speech, skeletal muscle twitching of face and extremities and convulsions.
The treatment comprises oxygenation, ventilation and intravenous midazolam.
In the 1980’s reports indicated that bupivacaine possessed a relatively
high potency for cardiotoxicity. Accidental IV injection of bupivacaine results in
precipitious hypotension, cardiac dysrhythmias and atrioventricular heart
block.67 It is found that due to rapid saturation of the protein binding sites,
significant mass of unbound drug is available for diffusion into the conducting
system of heart. Cardio toxicity occurs at a plasma concentration of 8-
10mcg/ml.68
60
The threshold for cardiac toxicity produced by bupivacaine may be
decreased in patients on antidysrhythmic drugs and medications which
depress impulse propagation (beta blockers,digitalis and calcium channel
blockers).69 In the presence of propanolol, cardio toxic effects occur at 2-
3mcg/ml of plasma concentration. Epinephrine and Phenylephrine also
increases bupivacaine toxicity.
Dissociation of highly lipid soluble bupivacaine from sodium channel
receptor site is slow causing persistent depressant effect on Vmax and cardio
toxicity.70Patients with cardiac depression or cardiac arrest due to bupivacaine
toxicity will be difficult to resuscitate. R-enantiomer of bupivacaine is more
toxic than the S-enantiomer. Tachycardia can enhance frequency dependent
blockade of cardiac channels by bupivacaine leading to cardiac toxicity.71
Cardiac arrest caused by bupivacaine is very difficult to treat and
reverse.
Bretylium 20 mg/kg IV reverses bupivacaine induced cardiac
depression and increase the threshold for ventricular tachycardia but since
the world's natural supply of bretylium is nearly exhausted, and the drug is no
longer available it has been deleted from the Advanced Cardiovascular Life
Support (ACLS) algorithm.72 On intravascular infusion of encapsulated
bupivacaine in multilamellar liposome, the nervous and cardiac toxicity of
bupivacaine was found to be reduced.73 Intralipid or commonly available IV
lipid emulsion can be effective in treating severe cardiac toxicity secondary to
local anaesthetic over dosage. Human cases have been reported with
successful use of Intralipid in the treatment of cardiac toxicity.74,75
61
NEUROTOXICITY
Spinal anaesthesia with 0.5% bupivacaine is associated with a lower
incidence of transient radicular irritation compared to lidocaine.76
USES
Bupivacaine is used for local infiltration, epidural anaesthesia and
analgesia, spinal anaesthesia and all peripheral nerve blocks.
RECENT ADVANCES
Apart from sodium channel blockade, non-sodium channel action also
plays an important beneficial role by local anesthetics in subtle modulation on
neutrophil function. They selectively inhibit priming without affecting activation
of neutrophils and prevent hyper-sensitization causing tissue damage. This
effect occurs at much lower concentration than those required for sodium
channel blockade. This is mediated by local anaesthetic interactions with G
protein signaling.77
CONTRAINDICATIONS
Presence of hypersensitivity to local anesthetics of the amide type or
other components of bupivacaine solutions. Other conditions are presence of
inflammation and or sepsis near the proposed site of injection, severe shock,
heart block and for intravenous regional anaesthesia(IVRA).
62
FENTANYL
It is a phenyl piperidine derivative, synthetic opiod agonist which is 75-
125 times more potent than morphine.78
STRUCTURAL FORMULA
MECHANISM OF ACTION
Opioids act as agonists at stereo specific opioid receptors at
presynaptic and postsynaptic sites in the central nervous system (principally
brainstem and spinal cord) and outside the central nervous system in
peripheral tissues.79,80
Analgesia that follows epidural placement of opioid reflects diffusion of
the drug across the dura to gain access to mu opioid receptors in the
substantia gelatinosa of the spinal cord as well as systemic absorption to
produce effects similar to those that would follow IV administration of opioid.
The principal effect of opioid receptors activation is a decrease in
neurotransmission.81,82 This occurs largely by presynaptic inhibition of
neurotransmitter (acetylcholine, dopamine, nor epinephrine, substance P)
release, although postsynaptic inhibition of evoked activity might also occur.
Figure-8-Structure of Fentanyl
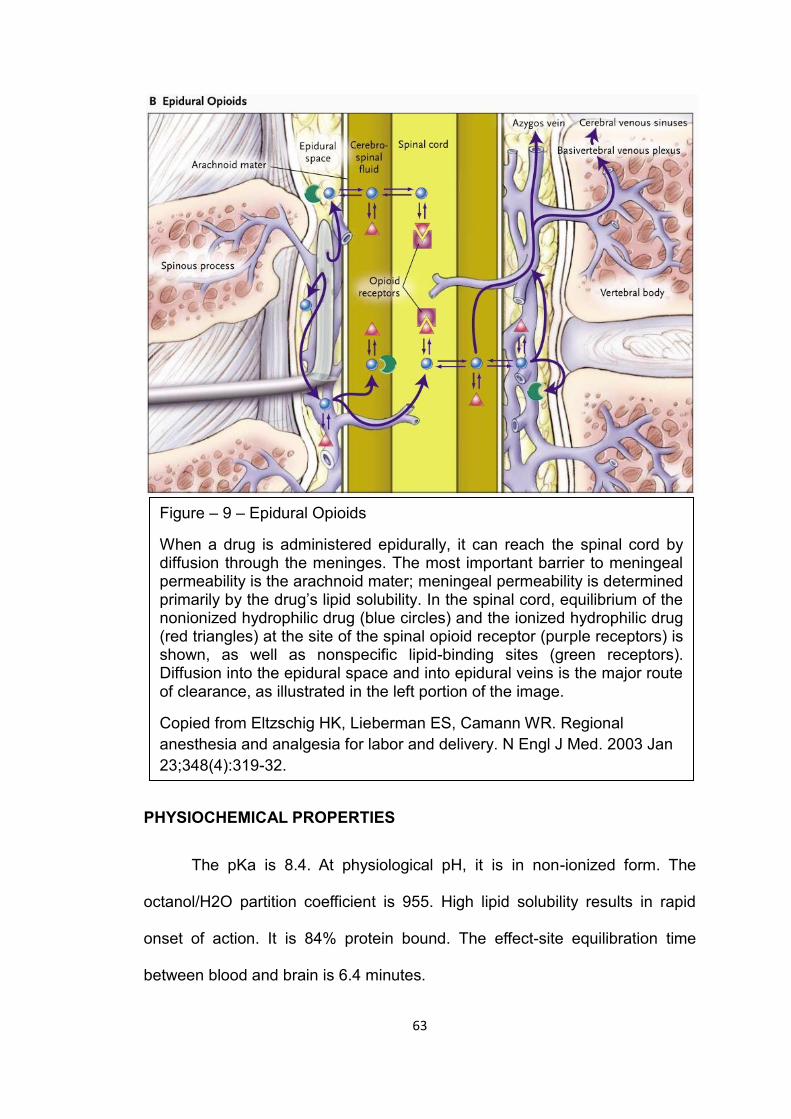
63
PHYSIOCHEMICAL PROPERTIES
The pKa is 8.4. At physiological pH, it is in non-ionized form. The
octanol/H2O partition coefficient is 955. High lipid solubility results in rapid
onset of action. It is 84% protein bound. The effect-site equilibration time
between blood and brain is 6.4 minutes.
Figure – 9 – Epidural Opioids
When a drug is administered epidurally, it can reach the spinal cord by diffusion through the meninges. The most important barrier to meningeal permeability is the arachnoid mater; meningeal permeability is determined primarily by the drug’s lipid solubility. In the spinal cord, equilibrium of the nonionized hydrophilic drug (blue circles) and the ionized hydrophilic drug (red triangles) at the site of the spinal opioid receptor (purple receptors) is shown, as well as nonspecific lipid-binding sites (green receptors). Diffusion into the epidural space and into epidural veins is the major route of clearance, as illustrated in the left portion of the image.
Copied from Eltzschig HK, Lieberman ES, Camann WR. Regional
anesthesia and analgesia for labor and delivery. N Engl J Med. 2003 Jan
23;348(4):319-32.
64
PHARMACOKINETICS
On administration, it undergoes rapid redistribution to inactive tissue
sites such as fat and skeletal muscles.83 The lungs exert a significant first
pass effect and transiently take up approximately 75% of the injected dose.84
The t1/2 α is 1-2.5 minutes and t1/2 β is 10-30 minutes. The volume of
distribution is 335 litres. It is primarily metabolized in liver by N-dealkylation
and hydroxylation providing nor-fentanyl. The metabolite is excreted by
kidneys and can be detected in urine upto 48 hours. Animal studies suggest
that nor-fentanyl has less analgesic potency than fentanyl.85 The elimination
half-life is 3.1-6.6 hours. The elimination half time is longer than morphine due
to greater lipid solubility and larger volume of distribution. The clearance rate
is 1530 ml / minute. Context sensitive half time after 4 hours of infusion is 260
minutes.
PHARMACODYNAMICS
Central nervous system: It reduces the MAC of isoflurane upto 80%86,
produces ceiling effect with increased dosage hence little effect on EEG. It
also decreases CMRO2 and intracranial pressure, increases muscle tone and
causes muscle rigidity.
Cardiovascular system: It reduces the heart rate due to stimulation of the
central vagal nucleus and reduction of sympathetic tone thus decreasing the
hemodynamic response to laryngoscopy and endotracheal intubation.
Respiratory system: It depresses the upper airway, tracheal and lower
respiratory tract reflexes,eliminates or blunts somatic and autonomic response
65
to tracheal intubation and causes dose dependent depression of ventilatory
response to CO2.
Endocrine effects: Modifies humoral response to surgery, prevents increase
in blood glucose, plasma catecholamine, antidiuretic hormone, renin,
aldosterone, cortisol and growth hormone concentrations.
Gastrointestinal system: It causes relaxation of the lower esophageal
sphincter and delays gastric emptying. It increases biliary duct pressure and
causes spasm of sphincter of Oddi. Stimulation of Chemoreceptor trigger
zone in area postrema of medulla leads to nausea and vomiting.
Renal system: There are no significant effects
DOSAGE AND ADMINISTRATION
INTRAVENOUS DRUG DELIVERY: Fentanyl 1-2 µg/kg provides analgesia. In
doses 2-20µg/kg, it blunts the pressor response to laryngoscopy and surgical
stimulation along with inhalational agents. Used in total intravenous
anaesthesia with loading dose 4-20µg/kg and maintainenance infusion rate of
2-10µg/kg/hr or additional boluses of 25-100µg.
EPIDURAL DELIVERY: Fentanyl is used in the dose of 50-100µg for
initiation of epidural analgesia. For maintenance a dose 1-4µg/ml is
used.87,From previous studies a dose of 2µg/ml is the commonly used dose
which provides the best pain relief with minimal side effects. The addition of
fentanyl decreases the MLAC(minimum local anaesthetic concentration) of
local anaesthetics. They act synergistically with the local anaesthetics in
epidural space.88
66
REVIEW OF LITERATURE:
Stienstra et al(1995)89 did a prospective randomized study in 76 full
term parturients to compare the effects of continuous epidural infusion of
ropivacaine 0.25% with bupivacaine 0.25% on pain relief and motor block
during labor, and on the neonate.Group I & group II received 10 ml of 0.25%
bupivacaine and 0.25% ropivacaine respectively. Then they were started on
an epidural infusion of the same drug at 6-12 ml/h. Top-up boluses of 6-10ml
were given as and when required. They found that the onset of pain relief
(verbal scale), contraction pain (visual analog scale), intensity of motor
block(modified Bromage scale), and duration of motor block were not
statistically different between the groups. However the ropivacaine group had
a higher proportion of neonates with neurologic and adaptive capacity
score(NACS) >35 than the bupivacaine group 2 hours after delivery. They
concluded that ropivacaine 0.25% and bupivacaine 0.25% are equally
effective for epidural pain relief during labor.
McCrae AF(1995)90 compared ropivacaine and bupivacaine in labor
epidural analgesia regarding pain relief in a prospective randomized
controlled trial. Epidural analgesia was initiated with 10ml of 0.5%
ropivacaine. When a top-up was requested, 0.25% ropivacaine or 0.25%
bupivacaine 10 ml was given (the same drug as the main dose). The study
ended when a second top-up was requested or delivery of the baby occurred.
The only significant difference between the groups was a shorter onset of pain
relief after the main dose of bupivacaine. There were no significant differences
n duration, onset of pain relief after top-up, quality of analgesia, spread of
67
sensory block and motor block between the groups. Cardiovascular changes
and neonatal outcome were also similar in the two groups.
Eddleston JM et al(1996)91 compared 0.25% ropivacaine and 0.25%
bupivacaine in a total of 104 parturients for extradural analgesia in labour. The
women in the bupivacaine group required more top-up doses to maintain
analgesia (median 3.0 vs 2.0) (P < 0.05). The onset of sensory block, quality
of analgesia, ultimate level of maximum sensory block and maternal
satisfaction were similar in both groups. The incidence, intensity and duration
of motor block were slightly but not significantly less in the ropivacaine group.
The ropivacaine group had a higher incidence of spontaneous vaginal delivery
(70.59% vs 52.00%). There was no significant difference in neonatal outcome
as assessed by Apgar scores, umbilical acid-base status and neurological and
adaptive capacity score at 2 and 24 h after delivery. They concluded that
ropivacaine and bupivacaine in a concentration of 0.25% produced
comparable analgesia for pain relief of labour with no detectable adverse
effect on the neonate.
Benhamou et al.(1997)92 did a prospective randomized on 133
parturients for identifying the optimum infusion rate of 0.2% ropivacaine as
continuous infusion. Four groups received a fixed rate 0.2% ropivacaine of
4/6/8/10 ml/h and additional bolus doses as and when necessary. Contraction
pain, quality of analgesia, sensory block, motor block and neonatal Apgar
scores were assessed. There were no significant differences between groups
in terms of analgesia, motor block, obstetrical or neonatal outcome. However
the 4 ml/h group required more boluses and the 10ml/h group received a
significantly higher dose of ropivacaine compared to 6ml/h. They concluded
68
that 0.2% ropivacaine was effective and well tolerated when given as a
continuous extradural infusion at 6-8 ml/h and may be used as the sole
analgesic during labour.
Cascio et al.(1997)93 compared four different rates of 0.2%
ropivacaine in continuous labour epidural analgesia in 128 parturients as a
prospective randomized study.After a bolus of 5 ml of 0.2% ropivacaine, a
continuous infusion was started at 4, 6, 8, or 10 mL/hour. Rescue analgesia
was provided with 5-mL "top-up" injections as and when necessary. Pain relief
was assessed by using a visual analog pain scale (VAPS) and motor block
was assessed by using a modified Bromage scale. They found that all
infusion regimens effectively decreased VAPS, and most patients in all groups
had minimal or no motor block at the end of the first stage of labor. Mean total
number of the top-up injections required per patient were 3, 2, 1.5, and 1.4,
respectively, in the 4, 6, 8, and 10-mL/hour groups (P < .05, 4 mL/hour vs. all
other groups). Despite receiving more total bolus dosages, the 4-mL/hour
group had less motor block in the lower extremities (P < .05). Apgar scores
and neurological adaptive capacity scores were similar for all groups.Thay
finally concluded that a rate of 6 mL/hour may be the lowest effective rate that
provides the best combination of pain relief, motor block, and rebolusing.
Owen et al.(1998)10 did a prospective double blind randomized
controlled trial on 51 labouring ASA I and II parturients.Their aim was to
compare the effects of 0.125% ropivacaine with 0.125% bupivacaine in
laboring patients using patient-controlled epidural analgesia (PCEA). Basal
infusion rates of 6 ml/h were supplemented with patient-controlled boluses of
5 ml, available every 10 min with a 30-ml/h limit. For inadequate analgesia,
69
10-ml boluses of study solution was administered until patient comfort was
achieved. There were no significant differences in verbal pain scores, amount
of local anesthetics used, sensory levels, motor blockade, labor duration,
mode of delivery, side effects, or patient satisfaction. They concluded that
0.125% ropivacaine and bupivacaine were clinically indistinguishable and are
both highly effective for labor analgesia using PCEA.
Yaakov Beilin et al(1999)94 did a prospective, randomized, double-
blinded study to determine the lowest concentration of ropivacaine that offers
pain relief for the initiation of labor epidural analgesia. Group I received 0.2%
ropivacaine, Group II received 0.15% ropivacaine, Group III received 0.1%
ropivacaine. Initially 13 ml was given in each group. Fifteen minutes later, the
adequacy of analgesia was assessed. If the patient reported that her degree
of analgesia was not adequate, an additional 5 mL of the study medication
was given, the degree of pain relief was reassessed 15 min later and the
study was concluded. They found that in Group I 26 of 28(93%),in Group II 18
of 28(64%),in Group III 4 of 12(33%) had adequate analgesia.They found that
0.2% ropivacaine offers significant analgesia more often than 0.15% or 0.1%
ropivacaine. They concluded that if ropivacaine is selected as the sole local
anaesthetic for the initiation of labor epidural analgesia, the minimal
concentration should be 0.2%.
Gautier et al.(1999)95 did a prospective randomized double blinded
study in 90 patients to evaluate the benefits of the administration of
intermittent bolus doses of 0.125% ropivacaine compared with 0.125%
bupivacaine after addition of sufentanil for analgesia during labor. The 90
patients were assigned randomly to receive 10 ml of 0.125% bupivacaine,
70
plus 7.5 µg sufentanil or 10ml of 0.125% ropivacaine, plus 7.5 µg sufentanil.
The duration of analgesia, visual analogue scores for pain, motor blockade
(using a six‐point modified Bromage scale), patient satisfaction scores,
nausea, pruritus, heart rate, and blood pressure were recorded. There were
no significant differences in analgesia onset time, number of patients requiring
reboluses, total infusion volume, VAS pain scores, duration of 2nd stage of
labour or mode of delivery. However the ropivacaine group had lower
incidence of motor block after the 3rd injection. They concluded that 0.125%
ropivacaine with sufentanil affords reliable analgesia with minimal motor
blockade.
Meister et al (2000)96 compared 0.125% Ropivacaine with 2µg/ml
Fentanyl and 0.125% Bupivacaine with 2µg/ml Fentanyl for epidural Labour
Analgesia. They chose 50 laboring women and randomized them to receive
either 0.125% Ropivacaine with Fentanyl 2µg/ml or 0.125% Bupivacaine with
Fentanyl 2µg/ml by using patient controlled epidural analgesia (PCEA)
technique. They found no differences in verbal pain scores; local anesthetic
used patient satisfaction or side effects between the groups. However the
Ropivacaine/Fentanyl group developed significantly less motor block than
Bupivacaine/Fentanyl group. They concluded that although
Ropivacaine/Fentanyl group developed less significantly less motor blockade
whether these results are applicable to anesthesia practices which do not use
PCEA remained to be determined.
Campbell et al (2000)97 conducted a prospective randomized double
blinded study to compare the efficacy of 0.08% Bupivacaine and 2µg/ml
Fentanyl or 0.08% Ropivacaine and 2µg/ml Fentanyl to initiate ambulatory
71
labour epidural analgesia. 40 nulliparous women in early labour <5cm cervical
dilation received either 20ml of 0.08% Bupivacaine and 2µg/ml Fentanyl (BF)
or 20ml of 0.08% Ropivacaine and 2µg/ml Fentanyl (RF) to initiate epidural
analgesia. They found that 0.08% Ropivacaine and 2µg/ml Fentanyl provided
consistent, effective labour analgesic without causing clinically significant
adverse maternal/fetal effects while concurrently preserving maternal ability to
void urine and ambulate.
Fettes et al (2000)98 conducted a randomized double blinded trial with
40 primigravid patients to compare intermittent bolus vs. continuous
administration of epidural Ropivacaine with Fentanyl for epidural analgesia.
Plain Ropivacaine 0.2%, 15-20 ml was titrated until analgesia and bilateral
sensory block to T10 was produced (Time Zero).Patients were then given
either an infusion of Ropivacaine 2mg/ml with 2µg/ml Fentanyl or hourly
boluses of 10ml of the same solution and on request additional 10ml were
given for analgesia. They found no differences between the two groups in
patient characteristics, obstetric/neonatal outcome, and sensory/motor block.
However the total drug dose used in the intermittent group was lower and
duration of uninterrupted analgesia (time to 1st rescue bolus) was longer. They
concluded that intermittent bolus is a more efficacious mode of analgesia.
Fischer et al(2000)99 conducted a prospective randomized double
blinded trial on 200 parturients to compare the administration of 0.1%
ropivacaine and 0.5 µg/ml sufentanil with that of 0.1% bupivacaine and 0.5
µg/ml sufentanil via patient controlled epidural analgesia route during labor. A
test dose of 5ml study solution was administered, followed by a loading dose
5 min later. PCEA regimen was of 5ml bolus,10 min lockout time.
72
Supplementary analgesia was of 5ml of study solution administered through
the PCEA pump by the nurse. The two groups did not differ in VAS, volume of
anesthetic solution used, mode of delivery, or side effects. The ropivacaine
group had significantly less motor block during first stage of labor and the
second stage of labour was shorter. The ropivacaine group patients also
requested more supplemental boluses to achieve analgesia during the second
stage of labor.Maternal satisfaction was greater in the bupivacaine group.
They concluded that 0.1% ropivacaine and 0.5 µg/ml sufentanil produce less
motor block but are clinically less potent than 0.1% bupivacaine and 0.5 µg/ml
sufentanil when given as PCEA infusion.
Helene Finegold et al(2000)100 did a double blind, randomized study
to compare analgesic efficacies of ropivacaine-fentanyl and bupivacaine-
fentanyl infusions for labour epidural analgesia in 100 term nulliparous
women. One group received a bolus of 10ml of 0.25% bupivacaine and
infusion of 0.125% bupivacaine with 2 µg/ml fentanyl. Another group received
10 ml of 0.2% ropivacaine bolus and infusion of 0.1% ropivacaine with 2 µg/ml
fentanyl. The median VAS scores were not different between the groups at
any of the evaluation periods. However, at least 80% of patients in the
ropivacaine group had no demonstrable motor block after the first hour
compared with only 55% of patients given bupivacaine. They concluded that
though bupivacaine and ropivacaine produced satisfactory labour analgesia,
ropivacaine infusion was associated with less motor block throughout the first
stage of labour and at 10 cm dilatation .
Ruban P et al(2000)101 did a prospective randomized controlled trial on
36 nulliparous parturients to study the effect of adding fentanyl 2 µg/ml on
73
demand-only PCEA using ropivacaine 0.125% for labour analgesia. All
patients were started on epidural analgesia with 10 ml 0.2% ropivacaine.
Then one group was started on 0.125% ropivacaine and another group on
0.125% ropivacaine with fentanyl 2 µg/ml. PCEA was was programmed to a
demand-only mode with bolus of 5 ml, lockout time of 10 minutes and
maximum volume per hour of 20 ml. Both groups were similar in the ratio of
successful PCEA demand to total number of demands, the satisfaction score
and the maternal-fetal outcome. However the total amount of ropivacaine
used per hour was lower in the group that received fentanyl. They concluded
that the addition of fentanyl had a dose-sparing effect on the requirement of
ropivacaine.
McClellan KJ, Faulds D(2000)102 updated the use of ropivacaine in
regional anaesthesia. Ropivacaine is a long-acting, enantiomerically pure (S-
enantiomer) amide local anaesthetic with a high pKa and low lipid solubility
which blocks nerve fibres involved in pain transmission (A delta and C fibres)
to a greater degree than those controlling motor function (A beta fibres). The
drug was less cardiotoxic than equal concentrations of racemic bupivacaine
but more so than lidocaine (lignocaine) in vitro and had a significantly higher
threshold for CNS toxicity than racemic bupivacaine in healthy volunteers
(mean maximum tolerated unbound arterial plasma concentrations were 0.56
and 0.3 mg/L, respectively). Extensive clinical data have shown that epidural
ropivacaine 0.2% is effective for the initiation and maintenance of labour
analgesia, and provides pain relief after abdominal or orthopedic surgery
especially when given in conjunction with opioids (co administration with
opioids may also allow for lower concentrations of ropivacaine to be used).
74
The drug had efficacy generally similar to that of the same dose of
bupivacaine with regard to pain relief but caused less motor blockade at low
concentrations. They concluded that ropivacaine is a well tolerated regional
anaesthetic with an efficacy broadly similar to that of bupivacaine. However, it
may be a preferred option because of its reduced CNS and cardiotoxic
potential and its lower propensity for motor block.
Dresner M, Freeman J, Calow C, Quinn A, Bamber J(2000)103
compared ropivacaine 0.2% with bupivacaine 0.1% with fentanyl for analgesia
during labour. In the bupivacaine group (BUPIV), 101 healthy parturients
received 0.1% bupivacaine with fentanyl 2 µg/ml and 102 women received
0.2% ropivacaine in the ropivacaine group (ROPIV). Both groups received an
initial loading dose of 15 ml, a continuous infusion of 8 ml/hr, and top-ups of
10 ml. Breakthrough pain not responding to a routine top-up was treated with
an 'escape' top-up of 10 ml 0.25% bupivacaine. The two groups were
compared for complete analgesia at 30 min, routine and 'escape' top-up
requirements, midwife assessment of analgesic efficacy, delivery mode,
patient VAS for first and second stage analgesia, overall satisfaction, and
patient assessment of motor blockade. Patients receiving ropivacaine
received fewer routine top-ups and fewer escape top-ups. The ropivacaine
group was more likely to be pain free in the first stage. There were no
significant differences in patients' assessment of motor block or mode of
delivery between the groups. Pain relief and satisfaction scores from
midwives and patients were consistently better in the ropivacaine group, but
did not reach statistical significance.
75
Merson N(2001)104 did a comparison of motor block between
ropivacaine and bupivacaine for continuous labor epidural analgesia. 68
healthy term primigravid parturients were randomized to receive an initial
bolus dose of 10 mL of 1 of the following: 0.25% bupivacaine (high
bupivacaine), 0.25% ropivacaine (high ropivacaine), 0.125% bupivacaine (low
bupivacaine), or 0.125% ropivacaine (low ropivacaine) along with 10 µg of
sufentanil added to it. A continuous infusion of a 0.1% study drug infusion with
0.6 µg/ml of sufentanil at a rate of 8 to 14 ml/h was then started .
Supplemental doses of 10 ml of a 0.125% study solution with 10 µg of
sufentanil were given as needed. He observed that a statistically significant
greater percentage of parturients receiving bupivacaine had motor block than
those who received ropivacaine, with a marked decrease in the occurrence of
motor block in the low ropivacaine group. Though the pain relief seemed to be
less satisfactory in the ropivacaine groups, the difference was not statistically
significant. Ropivacaine produced significantly less motor block than
bupivacaine in the 0.25% and the 0.125% loading doses, with the greatest
difference seen in the lower concentration loading dose of ropivacaine.
Chua NP, Sia AT, Ocampo CE(2001)105 compared hourly dose
requirement of ropivacaine 0.125% (group R, n = 16) with bupivacaine
0.125% (group B, n = 16) provided by demand-only (bolus 5 ml, lockout 10
min) in parturient-controlled epidural analgesia during labour. The hourly dose
requirement was comparable although group R had a lower successful to total
demands ratio (p < 0.05). They also found that both groups were clinically
indistinguishable in terms of pain relief and side effects. They concluded that,
76
at a concentration of 0.125%, ropivacaine and bupivacaine were equally
effective when self-administered using this patient-controlled regimen.
Fernández-Guisasola J et al.(2001)106 did a prospective randomized
double blinded study on 98 parturients to compare 0.0625% bupivacaine with
fentanyl and 0.1% ropivacaine with fentanyl which were thought to be
equipotent for continuous epidural labor analgesia. Epidural analgesia was
initiated with 8ml of 0.7% lignocaine and 50µg of fentanyl for both the groups.
Continuous epidural infusion of 0.0625% bupivacaine with fentanyl 2 µg/ml or
0.1% ropivacaine with fentanyl 2 µg/ml was started at 15ml/h depending upon
the study group. Top-up boluses of 5ml of study solution was used as and
when required. There were no statistically significant differences in pain
intensity, level of sensory block, degree of motor block, hemodynamic
variables, secondary effects, mode of delivery, neonatal outcome or patient
satisfaction. They concluded that both solutions were equally efficient in
providing highly effective epidural analgesia for labor with minimal motor
block, but the results suggest that bupivacaine may be more potent than
ropivacaine.
H.J.Clement et al (2002)107 did a double blind, randomized,
prospective trial on 140 parturients who requested epidural analgesia to
compare 0.15% ropivacaine plus sufentanil 0.5 µg/ml versus 0.10%
bupivacaine plus sufentanil 0.5 µg/ml. No differences was observed between
the two groups for pain scores, total volume of anaesthetic solution used,
duration of labour, mode of delivery, side‐effects or satisfaction score. They
concluded that 0.1% bupivacaine and 0.15% ropivacaine produce effective
and equivalent analgesia during labour, with similar incidences of motor block.
77
Lacassie HJ et al.(2002)108 conducted a study to determine the motor
block MLAC(minimum local anaesthetic concentration) of bupivacaine and
ropivacaine. 60 parturients were enrolled. Each received a 20-mL bolus of
epidural bupivacaine or ropivacaine. The first woman in each group received
0.35%. Up-down sequential allocation was used to determine subsequent
concentrations at a testing interval of 0.025%. Effective motor block was
defined as a Bromage score <4 within 30 min. The up-down sequences were
analyzed by using the Dixon and Massey method and probit regression to
quantify the motor block minimal local analgesic concentration. They found
that motor block MLAC for bupivacaine was 0.326% and for ropivacaine was
0.497%. The ropivacaine/bupivacaine potency ratio was 0.66 and was similar
to the sensory potency ratio for these two drugs.
Owen MD et al.(2000)109 designed this study to evaluate a
concentration near the reported 50% effective dose values for ropivacaine
and bupivacaine in an attempt to detect differences between the drugs during
routine clinical use in labor epidural. This was because studies had shown
that ED50 of Ropivacaine was 60% as potent as Bupivacaine. Fifty-nine
nulliparous women in labor were randomized to receive 0.075% ropivacaine
or bupivacaine, each with fentanyl 2 µg/mL. Epidural analgesia was initiated
with 20 ml of study dolution and PCEA was initiated with the following
settings: 6 mL/h basal rate, 5 mL bolus, 10 min lockout, and 30 mL/h limit.
Breakthrough pain was treated with 10-mL boluses of study solution. They
found that both 0.075% ropivacaine and bupivacaine, with fentanyl, were
equally effective for labor analgesia using the patient-controlled epidural
analgesia technique. There were no statistically significant differences in the
78
amount of local anesthetic used, verbal pain scores, sensory levels, motor
blockade, labor duration, mode of delivery, side effects or patient satisfaction.
Lee BB et al.(2002)110 formulated a study to compare 0.1%
ropivacaine with 0.2% ropivacaine and to examine the effect of addition of
fentanyl. 58 nulliparous laboring parturients were enrolled in a prospective
double-blind randomized control study. Epidural analgesia was established
with 0.2% ropivacaine and the patients were then randomized to receive one
of the following epidural infusions at 10 mL/h: 0.2% ropivacaine (group R2, n
= 19), 0.1% ropivacaine (group R1, n = 19), or 0.1% ropivacaine with 2 µg/mL
fentanyl (group RF, n = 20). Supplementary analgesia was provided on
request with 5-mL boluses of 0.2% ropivacaine. All solutions provided
effective analgesia during early labor, with all groups requiring similar
numbers of supplementary top-ups. Visual analog pain scores in groups R2
and RF were equivalent and lower than in group R1 (P =.006). Hypotension
was more frequent in group RF compared with groups R2 and R1 (P =.014).
Patient and midwife satisfaction and obstetric and neonatal outcomes were
similar among groups. Maternal venous plasma concentrations of ropivacaine
were greater in group R2 compared with groups R1 and RF (P =.008), but
umbilical venous concentrations were similar. They concluded that epidural
infusion of 0.1% ropivacaine alone at 10 mL/h provided adequate analgesia in
the first stage of labor. The addition of 2 µg/mL fentanyl to 0.1% ropivacaine
improved analgesia to a quality similar to 0.2% ropivacaine alone.
Asik I, Goktug A, Gulay I, Alkis N, Uysalel A(2002)111 compared
bupivacaine 0.2% and ropivacaine 0.2% combined with fentanyl for the
initiation and maintenance of analgesia during labour and delivery in sixty
79
labouring nulliparous women who were randomly allocated to receive either
bupivacaine 0.2% with fentanyl 2 µg/ml (B/F), or ropivacaine 0.2% with
fentanyl 2 µg/ml (R/F). For the initiation of epidural analgesia, 8 mL of the
study solution was administered. Supplemental analgesia was obtained with 4
ml of the study solution according to parturients' needs when their pain was >
or = 4 on a VAS. Analgesia, hourly local anaesthetic use, motor block, patient
satisfaction and side effects between groups were evaluated during labour
and at delivery. No differences in verbal pain scores, hourly local anaesthetic
use or patient satisfaction between groups was observed. However, motor
block was observed in 10 patients in the B/F group whereas only two patients
had motor block in the R/F group (P < 0.05). The incidence of instrumental
delivery was also higher in the B/F group than in the R/F group (P< 0.05).
They concluded that ropivacaine 0.2% combined with fentanyl 2 µg/ml
provided effective analgesia with significantly less motor block and need for
an instrumental delivery than a bupivacaine/fentanyl combination at the same
concentrations during labour and delivery.
Fernandez C et al.(2003)112 compared the analgesic efficacy and
extent of motor block when 0.125% ropivacaine or 0.125% bupivacaine were
given in continuous perfusion through an epidural catheter during labor in 60
ASA I-II women, each carrying a single fetus at full term and in spontaneous
labor. Women in the ropivacaine group (R) (n = 30) received 8 mL of 0.2%
ropivacaine for analgesic induction, followed by a continuous perfusion of 10
mL/h of 0.125%. The bupivacaine group (B) (n = 30) received the same
concentration and infusion rate as group (R).The objective of analgesia was to
achieve a score less than 3 on a visual analog painscale. If analgesia was
80
inadequate, a 5 mL bolus of 0.2% ropivacaine or bupivacaine, depending on
group, was administered. The motor block was evaluated on an abbreviated
Bromage scale and hemodynamic stability, fetal status, type of delivery and
the total dose of local anesthetic was also recorded. Analgesia and
haemodynamics were similar in both groups. Group R required a larger
number of additional boluses, although the difference was not statistically
significant. Motor block was observed in 8 patients in group B and 1 in group
R (p < 0.05). Fetal status was similar in both groups. Both drugs were equally
effective for controlling the pain accompanying labor, such that ropivacaine
offered no advantage over bupivacaine in that regard. Ropivacaine's reduced
motor block effect at the doses administered may offer an advantage in some
situations, such as when a walking epidural is provided.
Boselli et al.(2003)113 compared the PCEA administration of 0.15%
ropivacaine plus 0.5 µg/mL of sufentanil with that of 0.1% ropivacaine plus
0.5 µg/mL of sufentanil for labor analgesia. This was done to determine
whether a decreased concentration of ropivacaine could produce equally
effective analgesia. This was done in a prospective double blind randomized
controlled study on 130 parturients. They found that 0.1% Ropivacaine plus
0.5 µg/mL of sufentanil given via patient-controlled epidural anesthesia for
labor analgesia was equally as effective as ropivacaine 0.15% plus 0.5 µg/mL
of sufentanil, with a 30% local anesthetic-sparing effect and a 40% reduction
in cost. However this reduction in ropivacaine concentration was not
associated with a decrease in the incidence of motor block, side effects, or
instrumental deliveries.
81
Gogarten W et al.(2004)114 did a multicentric double-blinded
randomized study on 450 women to determine the optimal concentration of
ropivacaine for bolus-only patient-controlled epidural labour analgesia. The 4
groups received bupivacaine 0.125% with sufentanil 0.75 µg/ml, ropivacaine
0.125% or 0.175% with sufentanil 0.75 µg/ml or ropivacaine 0.2%. After an
initial bolus of 10 mL of the study solution, and once visual analogue scores
(VAS) were below 30 mm, patient-controlled epidural analgesia was initiated
with a bolus of 4 mL, a lockout interval of 15 min and without a background
infusion. They observed that Bupivacaine 0.125% and ropivacaine 0.125%
with sufentanil proved equally effective in providing labour analgesia without a
difference in local anaesthetic consumption, motor blockade or mode of
delivery. Ropivacaine 0.175% plus sufentanil enhanced the quality of
analgesia of the initial loading dose, whereas ropivacaine 0.2% without
sufentanil increased the consumption of local anaesthetics and the degree of
motor blockade. They concluded that despite recent studies indicating that
bupivacaine and ropivacaine may not be equipotent, both local anaesthetics
provided equi-effective analgesia at equal doses without a difference in side-
effects.
Atienzar MC et al.(2004)115 did a prospective randomized study on 80
nulliparous parturients in labour to evaluate the efficacy of 0.1% ropivacaine
with fentanyl 2µg/ml in labour epidural analgesia. All patients had epidural
analgesia initiated with 0.2% ropivacaine and fentanyl and were then
randomized to receive either 0.1% ropivacaine with fentanyl 2 µg/ml at 10ml/
h(Group R1, n = 38) or 0.2% ropivacaine with fentanyl 2 µg/ml at 8
ml/h(Group R2, n = 39) as epidural infusions. Supplementary analgesia was
82
provided on request with 5ml of 0.2% ropivacaine as an epidural bolus. They
found that there were no significant differences between the groups in visual
analogue pain scores, motor block or sensory block. Side effects, patient
satisfaction, labour outcome and neonatal outcomes were similar in both
groups. However the amount of local anaesthetic used was lower in the 0.1%
ropivacaine plus fentanyl group than in the 0.2% ropivacaine group. They
concluded that 0.1% ropivacaine plus fentanyl provided adequate analgesia
and the level of analgesia was comparable to that provided by 0.2%
ropivacaine with no differences with regard to motor or sensory block.
Neera Sah et al.(2007)116 conducted a prospective randomized double
blinded study in 162 ASA-I and II full term primiparous laboring women to
compare the efficacy of Ropivacaine, Bupivacaine and Levobupivacaine. All
patients received 8ml of local anesthetic + fentanyl (100µg) followed by
infusion of 12 ml/hr of local anesthetic with 2µg/ml of fentanyl. Patients were
allocated to one of the three groups, group 1 received bolus infusion of
Bupivacaine 0.125%, group 2 received bolus and infusion of Levobupivacaine
0.125%, and group 3 received bolus of ropivacaine 0.2% and infusion of
ropivacaine 0.1%. Vital signs, VAS score, sensory and motor block were
recorded every hour. They found no statistically significant difference in pain
(VAS) / motor (Bromage) score among the 3 groups.
Yaakov Beilin et al.(2007)117 studied the effects of mode of delivery of
bupivacaine, ropivacaine and levobupivacaine. They sought to determine if
there was a difference in mode of delivery among parturients who receive
epidural bupivacaine, ropivacaine, or levobupivacaine. Nulliparous women at
term requesting labor analgesia with a cervical dilation of 5 cm were
83
randomized to receive epidural bupivacaine, ropivacaine, or levobupivacaine.
Analgesia was initiated with a bolus of 15 mL of 0.0625% of the assigned LA
with fentanyl 2 µg/mL. Analgesia was maintained with an infusion of the same
solution at 10 mL/h. The primary endpoint was the operative delivery rate
(instrumental assisted vaginal delivery plus cesarean delivery). Ninety-eight
women received bupivacaine, 90 ropivacaine, and 34 levobupivacaine (before
it was removed from the US market). There was less motor block in the
levobupivacaine group when compared with the ropivacaine and bupivacaine
groups, P less than 0.05. There was no significant difference in the duration of
the first or second stage of labor, the total dose of LA received per hour of
labor, or neonatal outcome among groups. They concluded that bupivacaine,
ropivacaine, and levobupivacaine all confer adequate labor epidural
analgesia, with no significant influence on mode of delivery, duration of labor,
or neonatal outcome.
Wang Li Zhong et al.(2010)118 conducted a randomized clinical trial in
450 nulliparous parturients to compare Ropivacaine, Bupivacaine and
Levobupivacaine with Sufentanil for PCEA during labour. A concentration of
0.05%, 0.075%, 0.125% or 0.15% of either Ropivacaine (group R),
Bupivacaine (group B) and Levobupivacaine (group L) with Sufentanyl
0.5µg/ml was epidurally administered by PCEA mode. Effective analgesia was
defined as VAS score ≤30mm. The relative median potency for each local
anesthesia was calculated using a probit regression model. They found no
significant difference among groups in the numbers of effective analgesia,
pain scores, hourly local anesthesia concentration used and sensory/motor
blockade. They concluded that by using PCEA lower concentration of
84
Ropivacaine, Bupivacaine and Levobupivacaine with Sufentanil produced
similar analgesia and motor blockade. Analgesic efficacy mainly depends on
concentration rather than type of anesthetics.
Sumit Kalra et al.(2010)119 compared the efficacy of low concentration
of Bupivacaine with Fentanyl and Bupivacaine with Sufentanil for epidural
labour analgesia. 50 full term parturients received a initial bolus dose of a
10ml of 0.125% Bupivacaine. The patients were randomly divided into two
groups: Fentanyl group (F) received 0.0625% Bupivacaine + 2.5µg/ml
Fentanyl. Sufentanil group (S) received 0.625% Bupivacaine + 0.25µg/ml
Sufentanil. Verbal analogue pain scores, need of supplementary boluses,
mode of delivery and maternal satisfaction neonatal APGAR scores were
recorded. No significant difference was observed in the 2 groups. They
concluded that both Fentanyl and Sufentanil were equally effective in
providing labour analgesia with hemodynamic stability, maternal satisfaction
without serious maternal / fetal side effects
Ngan Kee WD et al.(2010)120 compared the complete dose response
curves of bupivacaine and ropivacaine through a random allocation-graded
dose-response study of these drugs given epidurally for labor analgesia.
Three hundred laboring nulliparous patients were randomly given epidural
bupivacaine (5, 10, 15, 20, 30, or 40 mg) or ropivacaine (7, 15, 20, 30, 45, or
60 mg) in 20 ml of saline. Visual Analog Scale pain scores were recorded for
30 min. Response was defined by the percentage decrease in pain score from
baseline at 30 min, and dose-response data were analyzed by using nonlinear
regression. The ED50 of ropivacaine was greater than that of bupivacaine
(15.3 mg vs. 11.3 mg, P = 0.0003), but ED90 was similar (40.6 mg vs. 33.4 mg,
85
P = 0.29). The potency ratio at ED50 for ropivacaine:bupivacaine was 0.75.
The curves had similar steepness .They concluded that ropivacaine is less
potent than bupivacaine, but otherwise they have similar dose–response
characteristics. The difference in potency was not statistically significant at
ED90 doses.
Lee HL, Lo LM, Chou CC, Chuah EC(2011)121 did a comparison
between 0.08% ropivacaine and 0.06% levobupivacaine for epidural
analgesia during nulliparous labor in a retrospective study in a single center.
The purpose of the retrospective study was to assess whether a combination
of 0.06% levobupivacaine and fentanyl 2 µg/ml had the same effects as
0.08% ropivacaine and fentanyl 2 µg/ml on the mode of delivery and other
obstetric outcomes when used for epidural analgesia of labor in nulliparous
women. Computer records of 392 Asian nulliparous parturients, who had
presented with spontaneous labor or spontaneous rupture of the membranes,
and had received epidural analgesia, were retrospectively reviewed. Of these,
193 received 0.08% ropivacaine and 199 received 0.06% levobupivacaine.
Fentanyl 2 µg/ml was used in both regimens. There were no significant
differences in the mode of delivery, duration of labor, or neonatal outcome
between the two groups. In the levobupivacaine group, the parturients
required top-up boluses of local anesthetics more frequently and the
incidence of temporary maternal fever and the cost of local anesthetic were
higher. However, the amount of local anesthetic administered during labor
was lower than for the ropivacaine group. 0.06 % levobupivacaine was as
effective as 0.08% ropivacaine,when both were used with fentanyl 2 µg/ml for
labor epidural analgesia of nulliparous women.
86
Materials & Methods
This was a prospective randomized control trial involving 70 parturients
(35 in each group) attending the Dept. of Obsetrics & Gynaecology,
G.Kuppusamy Naidu Memorial Hospital, Coimbatore over a period of 1
year(December 2011-December 2012).Institutional ethics committee and
scientific committee approval was obtained. All patients admitted to the labour
room were counseled regarding labour analgesia. The procedure was
explained to the patient. Informed consent was obtained. Detailed history of
the patient was collected. Routine investigations like blood grouping and
typing, hemoglobin and platelet count were done as per our hospital labour
protocol. Patients fulfilling the inclusion criteria and who gave consent were
then randomly allocated to one of the study groups on the basis of
computerized randomized list.
Inclusion Criteria:
1.Normal singleton pregnancies.
2.Age – 18-35 years
3.ASA status- I & II
4.Patients in active labour with cervical dilatation – 3-5 cm.
Exclusion Criteria:
1.Contraindications to epidural block
2.Pre-term pregnancy
3.Multiple pregnancy
4.Previous cesarean section.
87
Materials needed:
1. 18 G Tuohy needle
2. 20 G epidural catheter
3. 2 cc,5 cc,10 cc sterile syringes
4. Hypodermic needles – 18G & 26G
5. Bowl, Sponge holding forceps, Swabs, Chlorhexidine solution.
6. Sterile gown, Gloves, Cap & Mask
7. Tape for fixing catheter.
8. Local anaesthetic solution – 2% Lignocaine%
9. 2% lignocaine with adrenaline vial, 0.25% Bupivacaine vial, 0.2%
Ropivacaine ampoule, Fentanyl - 100µg.
10. Emergency kit with working laryngoscope, cuffed endotracheal tubes of
appropriate size, airway, suction apparatus with suction catheter,
Inj.Adrenaline, Inj.Atropine, Inj.Thiopentone, Inj.Succinyl choline,
Oxygen cylinder.
11. Monitor for continuous monitoring for Non-invasive blood pressure,
ECG, Respiratory rate, Oxygen saturation.
88
Figure-10 - Epidural tray and epidural set
89
Methodology:
An 18G IV cannula was inserted and patient was started on an infusion
Ringer lactate solution.
The patient was then positioned in Lt. lateral position or sitting position
based on the anaesthetist convenience and her back aligned with the edge of
the bed. Under strict aseptic precautions, the skin over the lower thoracic and
lumbar region was cleaned and area draped. The best interlumbar space
between L1 and L4 was identified and infiltrated with 2% lignocaine.
The skin was pierced with 18G needle in the interlumbar space. The
epidural needle was inserted with bevel facing upward and pushed till it
pierced the interspinous ligament. The stylet was then removed. A 10ml
LOR(Loss Of Resistance) syringe filled with either Air or saline was attached
to the hub of the epidural needle. The needle was then slowly advanced with
pressure exerted on the air/saline column through the plunger of the LOR
syringe. The epidural space was identified with LOR to injection of air or
saline. Careful aspiration was done to make sure that the duramater was not
punctured. If CSF was aspirated, the needle was withdrawn and reintroduced
in a different space. If no CSF was aspirated, the LOR syringe was removed.
The depth of the epidural space was noted. A 20G fine epidural catheter was
threaded through the needle into the epidural space. The epidural needle was
removed. The catheter was positioned so that a length of 5cm of catheter
remained in the epidural space. Careful aspiration of the cathter was again
done to check for CSF or blood.
90
Once the cathter was satisfactorily sited, the puncture site was cleaned
and an occlusion dressing applied over it. A bacterial filter was attached to the
hub of the cathter. A small test dose of local anaesthetic(3ml of 2% Lignocaine
with Adrenaline) was injected via the catheter to rule out intravascular or
intrathecal placement of catheter. If there were no signs of motor block
(intrathecal placement) or tachycardia(intravascular placement) after 5
minutes the patient was turned supine. A bolus dose of the test drug was
given followed by the infusion. The bolus and infusion protocol of each study
group were as follows :
Table-6-Study drugs protocol
Group Bolus Infusion
A 6ml of 0.2%
Ropivacaine
6-8ml/hr of 0.1% Ropivacaine with 2µg/ml
fentanyl
B 6ml of 0.25%
Bupivacaine
6-8ml/hr of 0.125% Bupivacaine with
2µg/ml fentanyl
Breakthrough pain was managed with 6ml of either 0.2% Ropivacaine
or 0.25% Bupivacaine depending on the study group they were involved.
Various maternal parameters were continuously monitored and noted
every 15 minutes in the first hour, every 30 minutes in the second hour and
every hourly thereafter. Continuous fetal heart monitoring was also done.
91
Parameters monitored:
1.Maternal Heart rate
2.Maternal Blood pressure
3.Maternal respiratory rate & oxygen saturation.
4.Pain relief by 11 point verbal numerical rating scale (VNRS)
5.Motor block by Bromage score(0-3)
Clinical outcome studied:
1.Pain relief
2.Motor block
3.Duration of labour
4.Mode of delivery - Vaginal - Spontaneous / Assisted
- Cesarean section
5.Neonatal outcome - APGAR score, NICU admission.
Sample size:
Sample size has been calculated to detect a 40% difference in the
occurrence of motor block between the two groups. The optimal sample size
required would be 25 in each group( 50 in total) with 80% power and 5% level
of significance. The incidence of significant motor block (2 or 3 on a 0–3
scale) was assumed to be 30%. (Owen 1998).
92
Statistical analysis:
All statistical analysis were performed using SPSS(Statistical package
for social sciences) version 17 for windows. The profile of the cases were
compared with the treatment allocation in order to check if there was any
significant imbalance. Descriptive statistics are presented as mean± 1SD.
Component bar and line diagrams were drawn as and when required. Chi-
square test for association was used to compare categorical variables
between treatment allocations.
93
Results and Observation
Our study included 70 pregnant women. They were randomly allocated
to either Group – A(0.1% ropivacaine with 2µg/ml fentanyl) or group-B(0.125%
bupivacaine with 2µg/ml fentanyl).
The initial patient and procedure characteristics were age, weight,
patient ASA grade, patient gravid and parity, vaginal dilatation, site od epidural
placement, comorbid conditions of the patients.
The outcomes measured were hemodynamics of the patient, pain
score, bolus requirement, motor block, mode of delivery, duration of labor,
neonatal outcome, and complications if any.
Profile of the preganant women:
Age :
The patients age ranged from 17-36 years. The average age did not
differ between the two groups. The mean age of women in Group-A was
25.37±3.85 years and that of group-B was 25.23±3.623.The difference was
not statistically significant.(P=0.874)
Weight :
The patients weight ranged from 46-89 kgs at the time of presentation.
The average weight of the women allocated to group-A was 68±8.86 kgs and
that of those in Group-B was 64.29±9.03 kgs. This difference in weight
between the two groups was statistically not significant.(P=0.087)
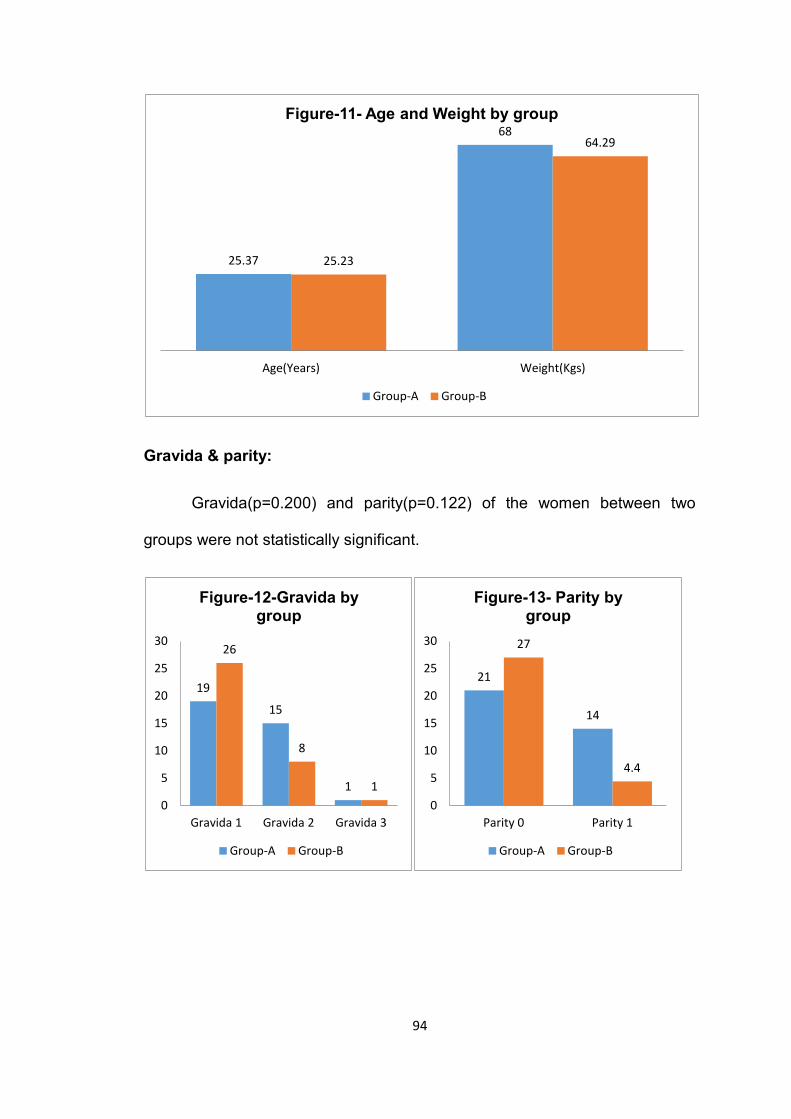
94
Gravida & parity:
Gravida(p=0.200) and parity(p=0.122) of the women between two
groups were not statistically significant.
25.37
68
25.23
64.29
Age(Years) Weight(Kgs)
Figure-11- Age and Weight by group
Group-A Group-B
19
15
1
26
8
1
0
5
10
15
20
25
30
Gravida 1 Gravida 2 Gravida 3
Figure-12-Gravida by group
Group-A Group-B
21
14
27
4.4
0
5
10
15
20
25
30
Parity 0 Parity 1
Figure-13- Parity by group
Group-A Group-B
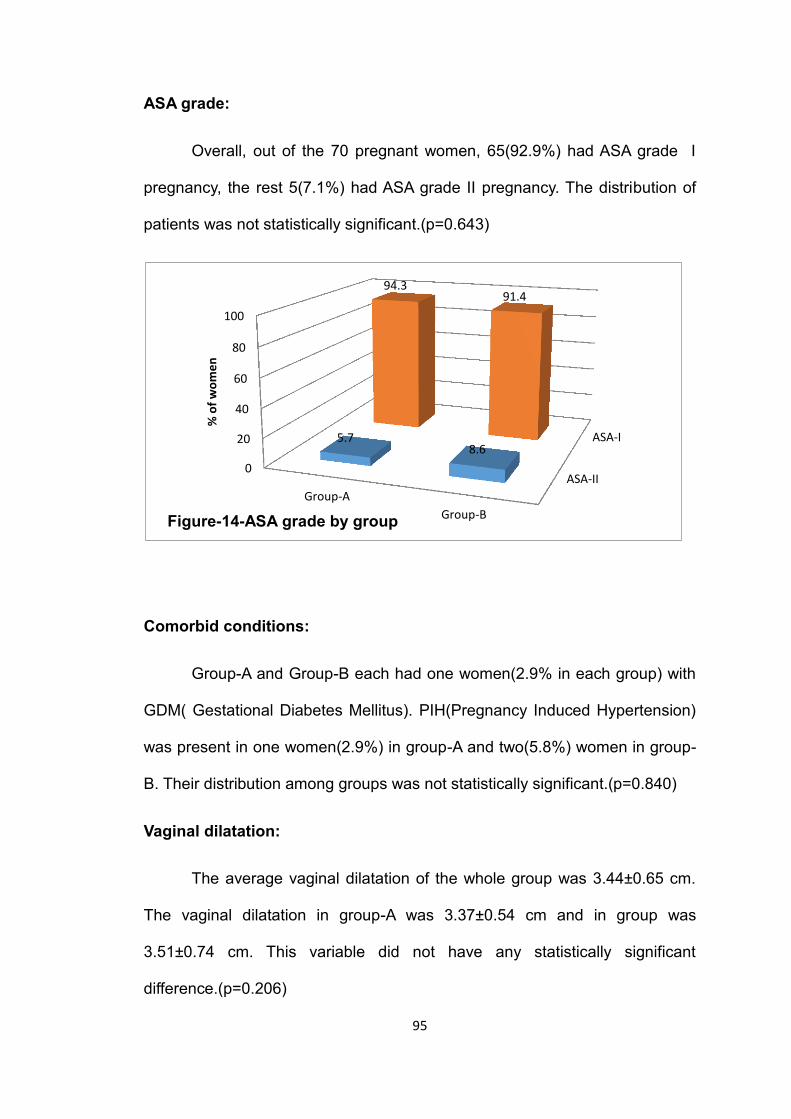
95
ASA grade:
Overall, out of the 70 pregnant women, 65(92.9%) had ASA grade I
pregnancy, the rest 5(7.1%) had ASA grade II pregnancy. The distribution of
patients was not statistically significant.(p=0.643)
Comorbid conditions:
Group-A and Group-B each had one women(2.9% in each group) with
GDM( Gestational Diabetes Mellitus). PIH(Pregnancy Induced Hypertension)
was present in one women(2.9%) in group-A and two(5.8%) women in group-
B. Their distribution among groups was not statistically significant.(p=0.840)
Vaginal dilatation:
The average vaginal dilatation of the whole group was 3.44±0.65 cm.
The vaginal dilatation in group-A was 3.37±0.54 cm and in group was
3.51±0.74 cm. This variable did not have any statistically significant
difference.(p=0.206)
ASA-II
ASA-I
0
20
40
60
80
100
Group-A
Group-B
5.7 8.6
94.3 91.4
% o
f w
om
en
Figure-14-ASA grade by group
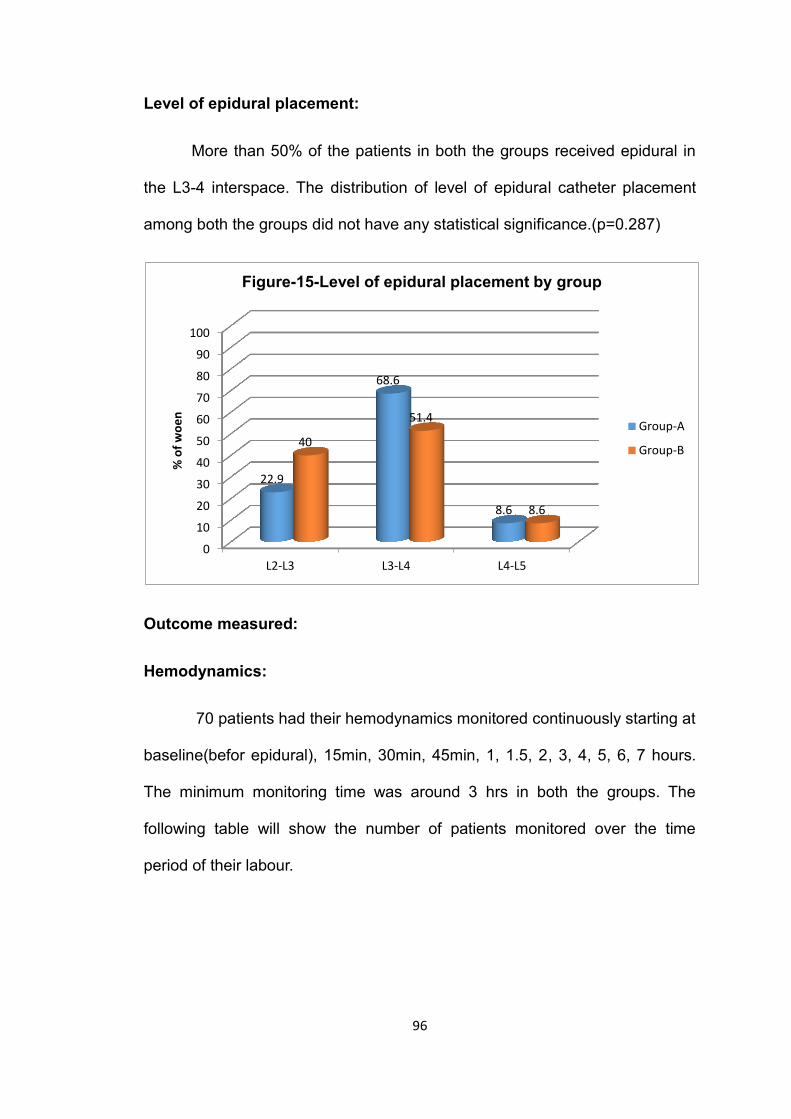
96
Level of epidural placement:
More than 50% of the patients in both the groups received epidural in
the L3-4 interspace. The distribution of level of epidural catheter placement
among both the groups did not have any statistical significance.(p=0.287)
Outcome measured:
Hemodynamics:
70 patients had their hemodynamics monitored continuously starting at
baseline(befor epidural), 15min, 30min, 45min, 1, 1.5, 2, 3, 4, 5, 6, 7 hours.
The minimum monitoring time was around 3 hrs in both the groups. The
following table will show the number of patients monitored over the time
period of their labour.
0
10
20
30
40
50
60
70
80
90
100
L2-L3 L3-L4 L4-L5
22.9
68.6
8.6
40
51.4
8.6
% o
f w
oe
n
Figure-15-Level of epidural placement by group
Group-A
Group-B
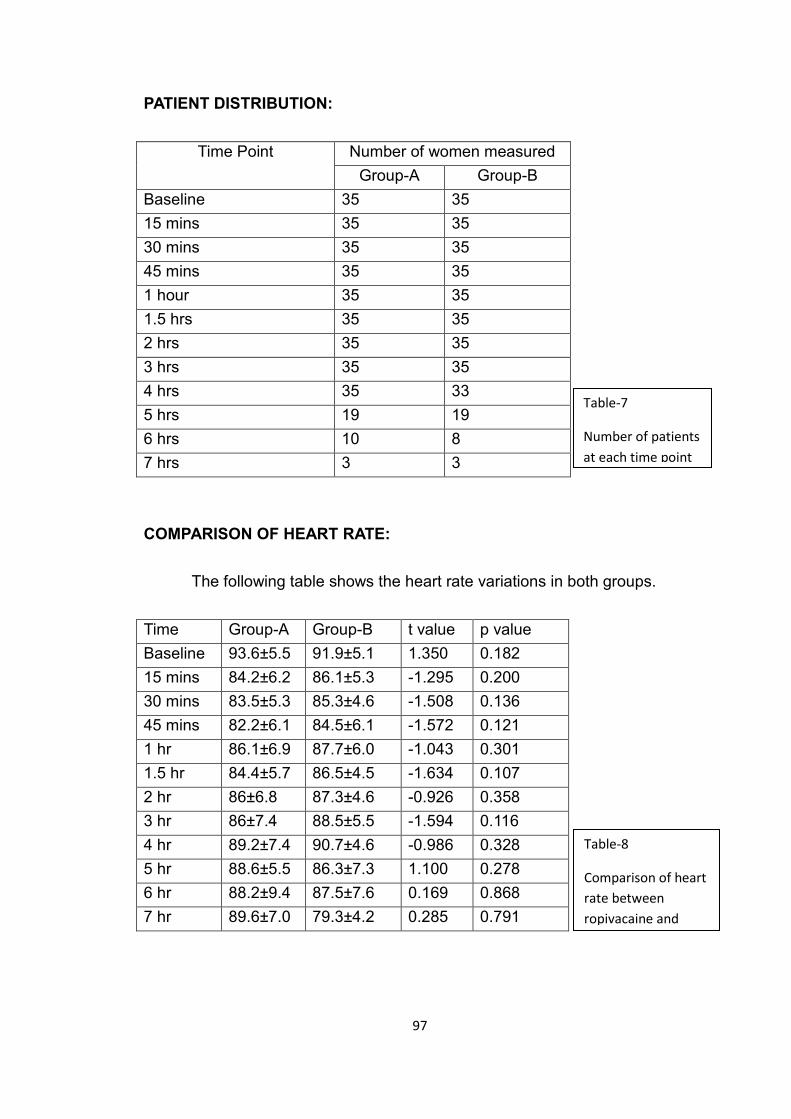
97
PATIENT DISTRIBUTION:
Time Point Number of women measured
Group-A Group-B
Baseline 35 35
15 mins 35 35
30 mins 35 35
45 mins 35 35
1 hour 35 35
1.5 hrs 35 35
2 hrs 35 35
3 hrs 35 35
4 hrs 35 33
5 hrs 19 19
6 hrs 10 8
7 hrs 3 3
COMPARISON OF HEART RATE:
The following table shows the heart rate variations in both groups.
Time Group-A Group-B t value p value
Baseline 93.6±5.5 91.9±5.1 1.350 0.182
15 mins 84.2±6.2 86.1±5.3 -1.295 0.200
30 mins 83.5±5.3 85.3±4.6 -1.508 0.136
45 mins 82.2±6.1 84.5±6.1 -1.572 0.121
1 hr 86.1±6.9 87.7±6.0 -1.043 0.301
1.5 hr 84.4±5.7 86.5±4.5 -1.634 0.107
2 hr 86±6.8 87.3±4.6 -0.926 0.358
3 hr 86±7.4 88.5±5.5 -1.594 0.116
4 hr 89.2±7.4 90.7±4.6 -0.986 0.328
5 hr 88.6±5.5 86.3±7.3 1.100 0.278
6 hr 88.2±9.4 87.5±7.6 0.169 0.868
7 hr 89.6±7.0 79.3±4.2 0.285 0.791
Table-8
Comparison of heart
rate between
ropivacaine and
bupivacaine groups
Table-7
Number of patients
at each time point
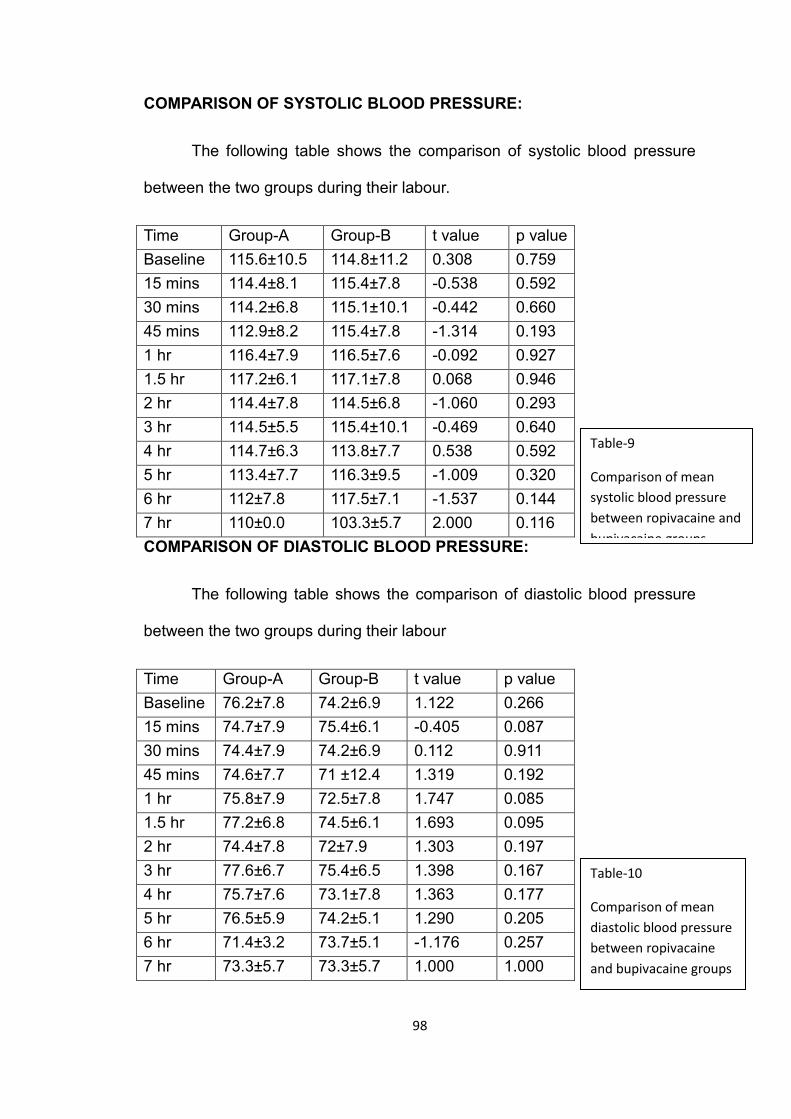
98
COMPARISON OF SYSTOLIC BLOOD PRESSURE:
The following table shows the comparison of systolic blood pressure
between the two groups during their labour.
Time Group-A Group-B t value p value
Baseline 115.6±10.5 114.8±11.2 0.308 0.759
15 mins 114.4±8.1 115.4±7.8 -0.538 0.592
30 mins 114.2±6.8 115.1±10.1 -0.442 0.660
45 mins 112.9±8.2 115.4±7.8 -1.314 0.193
1 hr 116.4±7.9 116.5±7.6 -0.092 0.927
1.5 hr 117.2±6.1 117.1±7.8 0.068 0.946
2 hr 114.4±7.8 114.5±6.8 -1.060 0.293
3 hr 114.5±5.5 115.4±10.1 -0.469 0.640
4 hr 114.7±6.3 113.8±7.7 0.538 0.592
5 hr 113.4±7.7 116.3±9.5 -1.009 0.320
6 hr 112±7.8 117.5±7.1 -1.537 0.144
7 hr 110±0.0 103.3±5.7 2.000 0.116
COMPARISON OF DIASTOLIC BLOOD PRESSURE:
The following table shows the comparison of diastolic blood pressure
between the two groups during their labour
Time Group-A Group-B t value p value
Baseline 76.2±7.8 74.2±6.9 1.122 0.266
15 mins 74.7±7.9 75.4±6.1 -0.405 0.087
30 mins 74.4±7.9 74.2±6.9 0.112 0.911
45 mins 74.6±7.7 71 ±12.4 1.319 0.192
1 hr 75.8±7.9 72.5±7.8 1.747 0.085
1.5 hr 77.2±6.8 74.5±6.1 1.693 0.095
2 hr 74.4±7.8 72±7.9 1.303 0.197
3 hr 77.6±6.7 75.4±6.5 1.398 0.167
4 hr 75.7±7.6 73.1±7.8 1.363 0.177
5 hr 76.5±5.9 74.2±5.1 1.290 0.205
6 hr 71.4±3.2 73.7±5.1 -1.176 0.257
7 hr 73.3±5.7 73.3±5.7 1.000 1.000
Table-9
Comparison of mean
systolic blood pressure
between ropivacaine and
bupivacaine groups
Table-10
Comparison of mean
diastolic blood pressure
between ropivacaine
and bupivacaine groups
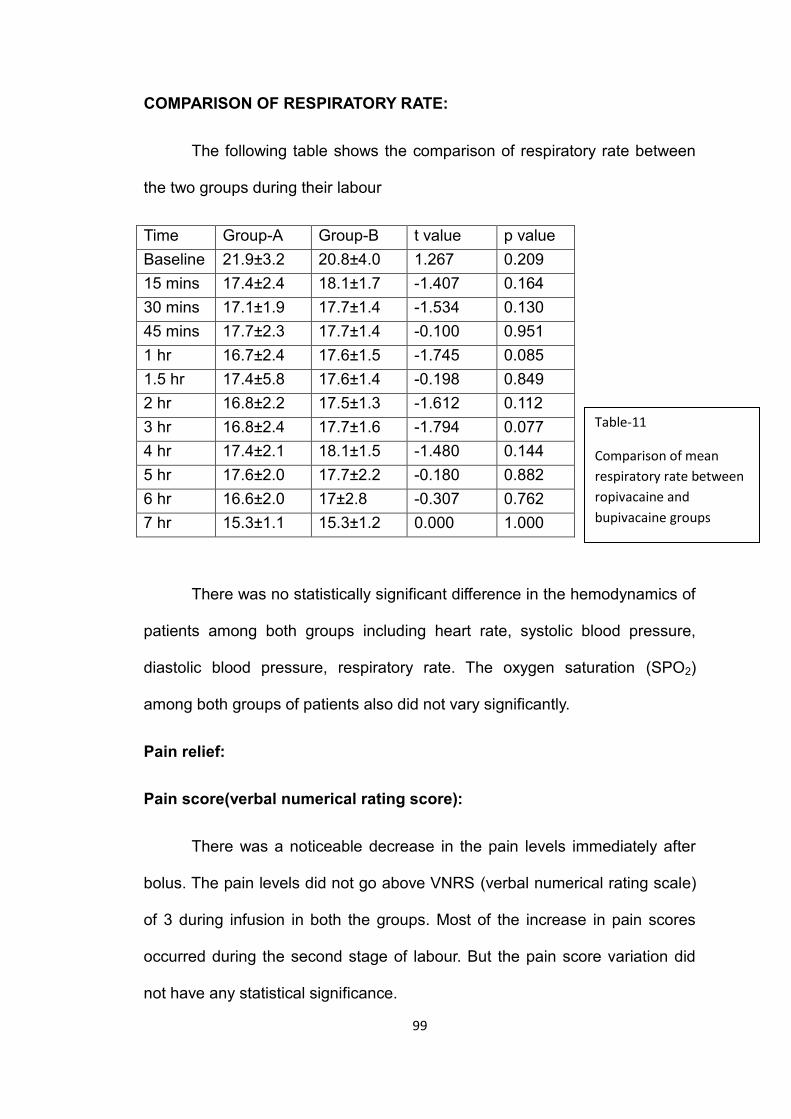
99
COMPARISON OF RESPIRATORY RATE:
The following table shows the comparison of respiratory rate between
the two groups during their labour
Time Group-A Group-B t value p value
Baseline 21.9±3.2 20.8±4.0 1.267 0.209
15 mins 17.4±2.4 18.1±1.7 -1.407 0.164
30 mins 17.1±1.9 17.7±1.4 -1.534 0.130
45 mins 17.7±2.3 17.7±1.4 -0.100 0.951
1 hr 16.7±2.4 17.6±1.5 -1.745 0.085
1.5 hr 17.4±5.8 17.6±1.4 -0.198 0.849
2 hr 16.8±2.2 17.5±1.3 -1.612 0.112
3 hr 16.8±2.4 17.7±1.6 -1.794 0.077
4 hr 17.4±2.1 18.1±1.5 -1.480 0.144
5 hr 17.6±2.0 17.7±2.2 -0.180 0.882
6 hr 16.6±2.0 17±2.8 -0.307 0.762
7 hr 15.3±1.1 15.3±1.2 0.000 1.000
There was no statistically significant difference in the hemodynamics of
patients among both groups including heart rate, systolic blood pressure,
diastolic blood pressure, respiratory rate. The oxygen saturation (SPO2)
among both groups of patients also did not vary significantly.
Pain relief:
Pain score(verbal numerical rating score):
There was a noticeable decrease in the pain levels immediately after
bolus. The pain levels did not go above VNRS (verbal numerical rating scale)
of 3 during infusion in both the groups. Most of the increase in pain scores
occurred during the second stage of labour. But the pain score variation did
not have any statistical significance.
Table-11
Comparison of mean
respiratory rate between
ropivacaine and
bupivacaine groups
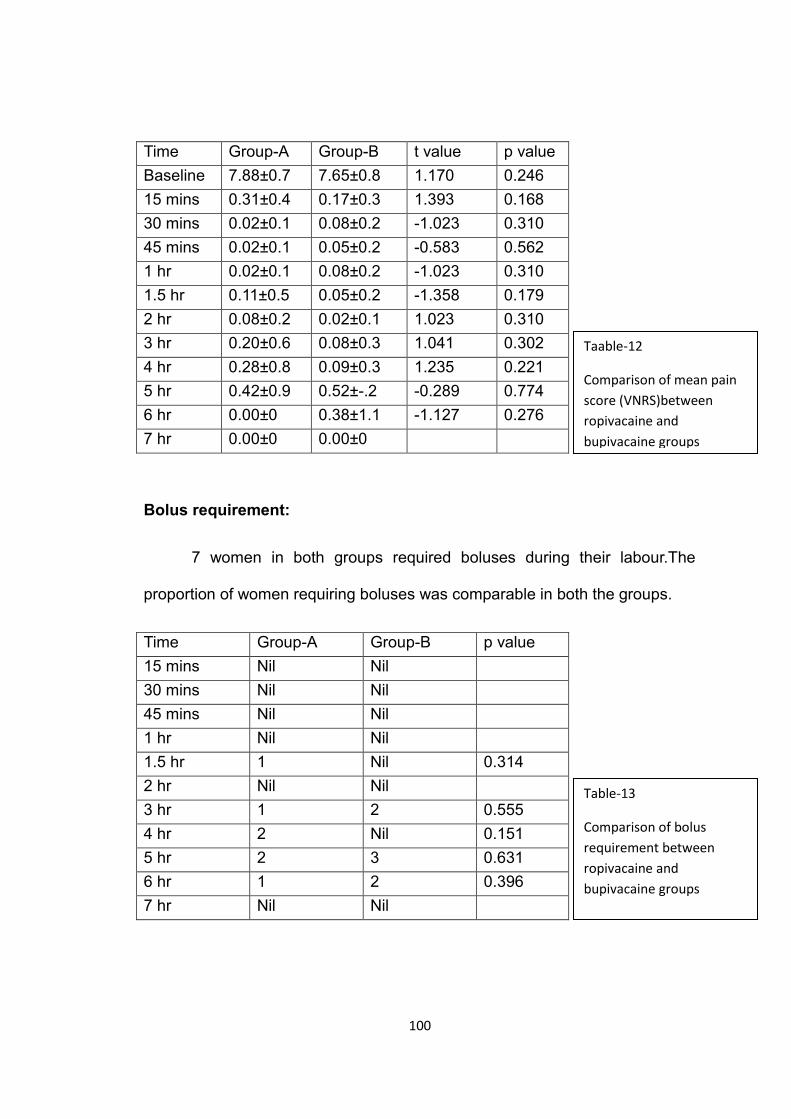
100
Time Group-A Group-B t value p value
Baseline 7.88±0.7 7.65±0.8 1.170 0.246
15 mins 0.31±0.4 0.17±0.3 1.393 0.168
30 mins 0.02±0.1 0.08±0.2 -1.023 0.310
45 mins 0.02±0.1 0.05±0.2 -0.583 0.562
1 hr 0.02±0.1 0.08±0.2 -1.023 0.310
1.5 hr 0.11±0.5 0.05±0.2 -1.358 0.179
2 hr 0.08±0.2 0.02±0.1 1.023 0.310
3 hr 0.20±0.6 0.08±0.3 1.041 0.302
4 hr 0.28±0.8 0.09±0.3 1.235 0.221
5 hr 0.42±0.9 0.52±-.2 -0.289 0.774
6 hr 0.00±0 0.38±1.1 -1.127 0.276
7 hr 0.00±0 0.00±0
Bolus requirement:
7 women in both groups required boluses during their labour.The
proportion of women requiring boluses was comparable in both the groups.
Time Group-A Group-B p value
15 mins Nil Nil
30 mins Nil Nil
45 mins Nil Nil
1 hr Nil Nil
1.5 hr 1 Nil 0.314
2 hr Nil Nil
3 hr 1 2 0.555
4 hr 2 Nil 0.151
5 hr 2 3 0.631
6 hr 1 2 0.396
7 hr Nil Nil
Taable-12
Comparison of mean pain
score (VNRS)between
ropivacaine and
bupivacaine groups
Table-13
Comparison of bolus
requirement between
ropivacaine and
bupivacaine groups
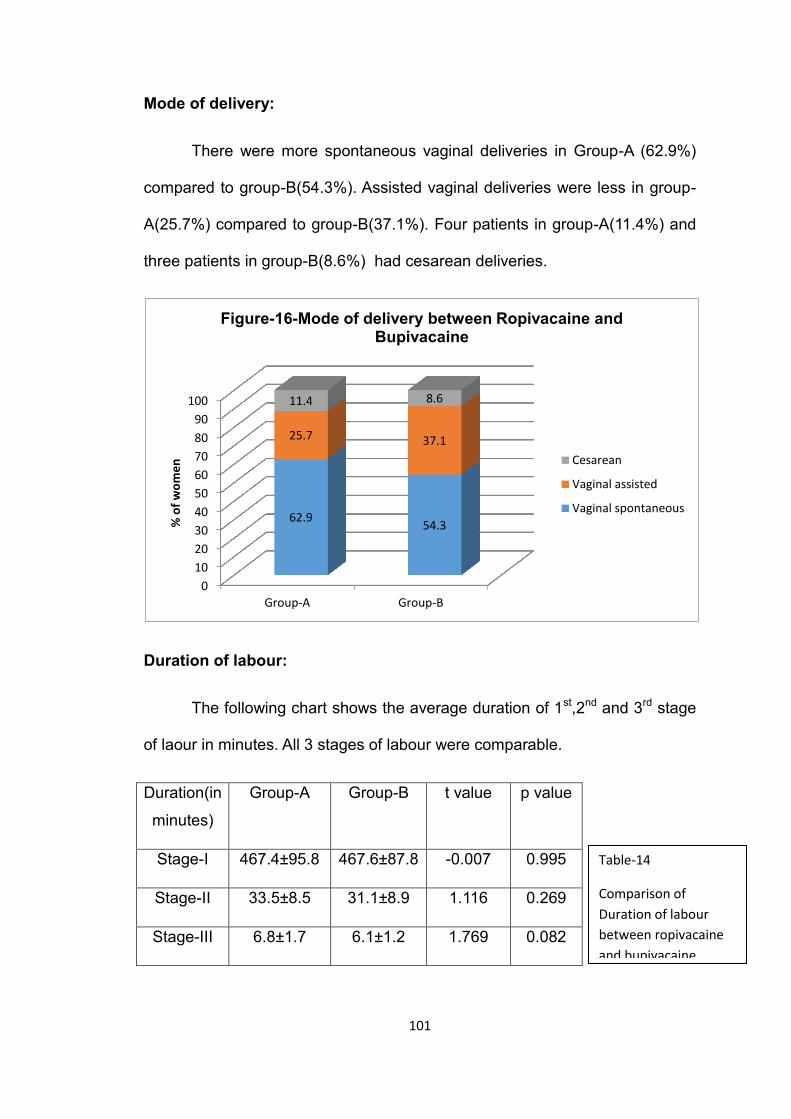
101
Mode of delivery:
There were more spontaneous vaginal deliveries in Group-A (62.9%)
compared to group-B(54.3%). Assisted vaginal deliveries were less in group-
A(25.7%) compared to group-B(37.1%). Four patients in group-A(11.4%) and
three patients in group-B(8.6%) had cesarean deliveries.
Duration of labour:
The following chart shows the average duration of 1st,2nd and 3rd stage
of laour in minutes. All 3 stages of labour were comparable.
Duration(in
minutes)
Group-A Group-B t value p value
Stage-I 467.4±95.8 467.6±87.8 -0.007 0.995
Stage-II 33.5±8.5 31.1±8.9 1.116 0.269
Stage-III 6.8±1.7 6.1±1.2 1.769 0.082
0
10
20
30
40
50
60
70
80
90
100
Group-A Group-B
62.9 54.3
25.7 37.1
11.4 8.6
% o
f w
om
en
Figure-16-Mode of delivery between Ropivacaine and Bupivacaine
Cesarean
Vaginal assisted
Vaginal spontaneous
Table-14
Comparison of
Duration of labour
between ropivacaine
and bupivacaine
groups
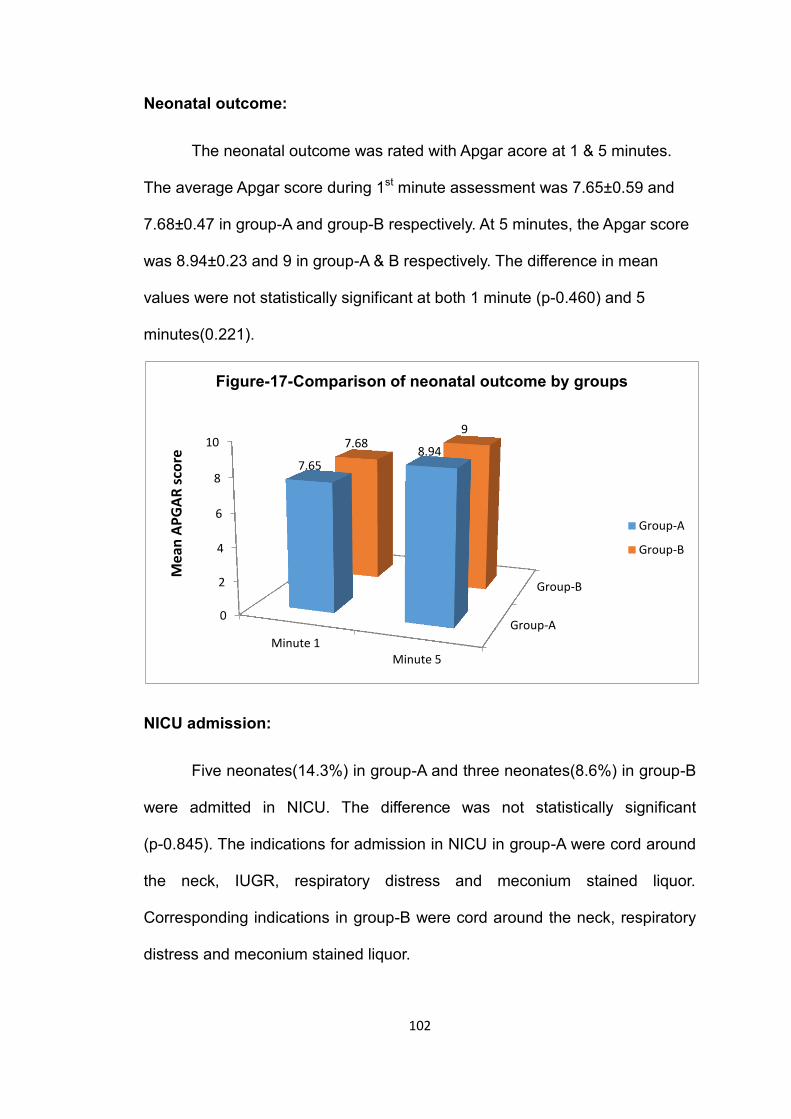
102
Neonatal outcome:
The neonatal outcome was rated with Apgar acore at 1 & 5 minutes.
The average Apgar score during 1st minute assessment was 7.65±0.59 and
7.68±0.47 in group-A and group-B respectively. At 5 minutes, the Apgar score
was 8.94±0.23 and 9 in group-A & B respectively. The difference in mean
values were not statistically significant at both 1 minute (p-0.460) and 5
minutes(0.221).
NICU admission:
Five neonates(14.3%) in group-A and three neonates(8.6%) in group-B
were admitted in NICU. The difference was not statistically significant
(p-0.845). The indications for admission in NICU in group-A were cord around
the neck, IUGR, respiratory distress and meconium stained liquor.
Corresponding indications in group-B were cord around the neck, respiratory
distress and meconium stained liquor.
Group-A
Group-B
0
2
4
6
8
10
Minute 1 Minute 5
7.65 8.94
7.68 9
Mea
n A
PG
AR
sco
re
Figure-17-Comparison of neonatal outcome by groups
Group-A
Group-B
103
Motor block:
Motor blockade of Bromage score-1 was observed in 3 persons
belonging to group-B. This was observed during the 5th hour in all 3 patients.
There was no clinically observable motor blockade in Group-A. However this
was not statistically significant(p-=0.071).
Numbness:
Numbness was seen in 2 patients in group-B and compared to none in
group-A. It was seen in 6th and 7th hour. The numbness rate was not
statistically significant.
Pruritis:
Pruritis was not seen in any patients in both the groups.
104
Discussion
The recently published cochrane review34 on epidural versus non-
epidural or no analgesia in labour has concluded that epidural offered better
pain relief, a reduction in the need for additional pain relief , a reduced risk of
acidosis and a reduced risk of naloxone administration.
In our study we have compared bupivacaine with ropivacaine for labor
epidural analgesia. Bupivacaine is a proven drug for effective labor analgesia.
We decided to compare bupivacaine with ropivacaine, which is marketed as a
levo-enantiomer because ropivacaine has a better sensory-motor
differentiation and less cardiotoxic potential compared to bupivacaine.
Many studies state that the potency of ropivacaine is 60% as that of
bupivacaine.8,9 There have been many studies which compare equal
concentrations of both drugs10,95,96,99 (i.e.0.125% bupivacaine vs 0.125%
ropivacaine). There have also been many studies which state to have
compared equi-potent concentrations of both drugs106,107.(i.e 0.1%
bupivacaine vs 0.15% ropivacaine). Most of the studies have found that both
drugs did not differ significantly except ropivacaine had less motor block on
prolonged infusion.
The recommended dose of bupivacaine in labor epidural analgesia is
0.0625%-0.125% and that of ropivacaine is 0.08%-0.2% at the rate of 8-
15ml/hour.16
105
We used 6ml of 0.2% ropivacaine for initiation(Beillin1999)94 and 6ml/hr
of 0.1% ropivacaine with 2µg/ml fentanyl(Benhamou 1997,Cascio 1997)92,93
for maintenance.
Neuraxial local anesthetics and opioids act synergistically to provide
neuraxial analgesia. This combination decreases the MLAC of local
anaesthetics used.88 We used fentanyl in a concentration of 2 µg/ml as it was
used most commonly in previous studies.
We decided to compare 0.1% ropivacaine with fentanyl and 0.125%
bupivacaine with fentanyl to see whether a less potent ropivacaine offers the
same pain relief and if it offers any significant advantage over bupivacaine at
this concentration.
The parturients were comparable in regards to age, weight, gravida,
parity, vaginal dilatation in both groups.
Pain relief:
Pain is a subjective phenomenon and it is difficult to measure. There
are many different scales to measure pain - verbal rating scale, numerical
rating scale (NRS), visual analog scale(VAS) etc. In our study we used NRS
as the pain scoring system because it was easy to use along with patients’
understanding and compliance being better.
In our study we found that the mean pain level was 7.8±0.7 in
ropivacaine group and 7.6±0.8 in bupivacaine group. After epidural it came
down to 0.31 in ropivacaine and 0.17 in bupivacaine group. The pain score
went upto 0.42 in ropivcaine and 0.52 in bupivacaine group at the end of 5
106
hours. There was no clinically demonstrable difference in the onset of pain
relief. This was consistent with the results obtained by Meister et al 200096.
They compared equal concentrations of 0.125% bupivacaine and 0.125%
ropivacaine along with fentanyl in both groups. They found that mean NRS
scores which were around 9 in bupivacaine and 8 in ropivacaine respectively,
came down to 0.4 & 0.3 post epidural. This study finding was echoed in the
study done by Fernandez et al 2001106 when they compared 0.0625%
bupivacaine with fentanyl and 0.1% ropivacaine and fentanyl.
There were no clinically demonstrable differences in the onset of pain
relief. Patient satisfaction was also comparable in both groups
Though our study used a less potent concentration of ropivacaine,
there was no statistically significant difference in the pain relief offered.
Motor blockade:
When Halpern et al 2003123 did a meta-analysis comparing ropivacaine
and bupivacaine he found that 19 out of 23 studies favoured ropivacaine to
have minimal motor block and 5 of those studies were statistically significant.
In our study, only 2 patients in bupivacaine group had demonstrable
Bromage score-I motor block. There was no clinically demonstrable motor
block in the ropivacaine group. This difference was not clinically significant.
The incidence of motor block in our study was low in ropivacaine and
also significantly lower than bupivacaine in many of the comparative
studies(Gautier 1999,Fischer 2000,Meister 2000,Campbell 2000)95,96,97,99
This may be because the volume of drug used in our study was low(6 ml
107
bolus and 6-8ml/hr infusion) thereby resulting in a lesser concentration of
drugs.
Duration of labour:
Duration of 1st stage of labour:
The duration of labour is determined by the intensity of uterine
contraction, the dilatation of cervix and the descent of the presenting part of
fetus.
A meta-analysis by Halpern et al(1988)122 concluded that epidural
analgesia prolonged 1st stage of labour by 42 minutes.
But other studies including the recent Cochrane review34 comparing
epidural and non-epidural methods of labour analgesia did not find any
difference in the length of 1st stage of labour.
In our study the duration of first stage of labour was 467.7±95.8
minutes in ropivacaine group and 467.6±87.8 minutes in the bupivacaine
group. There was no statistically significant difference in the mean duration.
Many studies compared varying concentrations of bupivacaine with
ropivacaine. They did not find any difference in the duration of 1st stage of
labour between bupivacaine and ropivacaine (Feranandez 2001,Owen 2002,
Boselli 2003).106,109,113
The results of our study correlate well with the above mentioned
studies.
108
In contrast Lee et al 2002110 in their study compared found that the
bupivacaine group had longer first stage of labour than ropivacaine group.
However they concluded that the difference may be of limited clinical
significance.
Duration of 2nd stage of labour:
According to ACOG guidelines, second stage of labour is said to be
prolonged when the duration was more than 3 hours for primipara and more
than 2 hours for multipara with regional anaesthesia.
A metanalysis done by Halpern et al122 on 2400 parturients who
received either epidural analgesia or parenteral opioid analgesia found that
the second stage of labour was prolonged by 14 minutes. A recent Cochrane
review34 on epidural versus non-epidural or no analgesia in labour found that
women who had epidural were more likely to have a longer second stage of
labour.
In our study there was no difference in the duration of second stage of
labour in both groups. The mean duration was 33.5 min in ropivacaine group
and 31.1 min in bupivacaine group. This difference was not statistically
significant. Our result coincides well with the meta-analysis done by Halpern
et al in 2003123 which took into account 23 studies comparing ropivacaine and
bupivacaine for labour epidural analgesia. They found that neither
bupivacaine nor ropivacaine group had any difference in the duration of
second stage of labour.
109
Mode of delivery:
Instrumental vaginal delivery:
Halpern et al 1988122 in their meta analysis found that women with
epidural were twice as likely to have an instrumental vaginal delivery as
compared to control groups. Cambic and Wong 2010124 in their review on
labour analgesia and obstetric outcomes concluded that effective second
stage analgesia might be associated with an increased rate of instrumental
vaginal delivery.
In our study we had an instrumental delivery rate of 25.7% in
ropivacaine group and 37.1% in bupivacaine group which was not statistically
significant. In majority of cases, maternal failure was the cause of instrumental
delivery. Our study results coincide with the study done by Finegold et al in
2000100, which used a similar concentration of drugs as our study. They had a
instrumental vaginal delivery rate of 18% in ropivacaine group and 28% in
bupivacaine. In both our studies though the instrumental delivery rates were
less in ropivacaine, the differences were not statistically significant.
The meta-analysis of 23 studies comparing ropivacaine and
bupivacaine in 2003 by Halpern et al123 also did not find any difference in
the mode of delivery between the two drugs.
However a meta-analysis of 6 studies comparing 0.25% ropivacaine
and 0.25% bupivacaine done by Writer et al125 in 1998 found that there were
fewer instrumental vaginal deliveries in the ropivacaine group. This may be
because of the higher concentration of bupivacaine used and difference in the
motor blocking potency of ropivacaine.
110
Caesarean delivery:
Epidural analgesia is not associated with an increased rate of cesarean
delivery. This has been the conclusion of a meta-analysis by Halpern et al
1988122 and the recent Cochrane review 201134 done on epidural vs non-
epidural and no analgesia in labour.
In our study,we had a cesarean delivery rate of 11.4% in ropivacaine
and 8.6% in bupivacaine group. The main reasons for the cesarean delivery
among both groups were failure to progress, fetal distress due to cord around
the neck and meconium stained liquor.
Beilin et al in 2007117 compared ropivacaine with bupivacaine and their
effect on outcome of delivery. Bupivacaine group had a cesarean rate of 33%
against a 30% rate in ropivacaine group.
The meta-analysis by Halpern et al 2003123 also found no difference in
cesarean delivery rates between ropivacaine and bupivacaine when used for
labor epidural.
Fetal and neonatal outcome:
The recent Cochrane review34 which compared epidural analgesia with
other forms of analgesia including inhaltional and intravenous(mainly opioids)
observed that there was less fetal acidosis and less naloxone administration
in babies born to mothers having labour epidural analgesia.
In our study the fetal heart rate during the process of labour analgesia
was within normal limits. There was no incidence of post epidural fetal
bradycardia. The mean APGAR score was 7.65 & 7.68 in ropivacaine and
111
bupivacaine groups respectively. At 5 minutes it averaged to 8.94 & 9
respectively. There was no significant difference in NICU admission in both
groups.
Beilin and Halpern in 2010126 did a focused review with various studies
that compared bupivacaine and ropivacaine and concluded that there was no
evidence that neonatal outcome is adversely affected when ropivacaine or
bupivacaine is used for labor analgesia.
Writer et al.125 found a difference in the neurologic and adaptive
capacity score, favoring ropivacaine, at 24 hours after birth, but not at 2 hours
after birth. But recent evidence suggests that the neurologic and adaptive
capacity score is unreliable.127
The incidence of low Apgar scores at 5 minutes is approximately 2%
for both drugs.123 In addition, the umbilical artery and vein pH are well
maintained regardless of which local anesthetic is used. 110Also, the incidence
of need for neonatal resuscitation is low and similar with both drugs.117
The incidence of complications were very minimal in both groups.
112
Summary
This study was undertaken to compare continuous epidural ropivacaine
with fentanyl and continuous epidural bupivacaine with fentanyl in labour
analgesia.
A total of 120 patients were randomly allocated into 2 groups. Group A
received 6ml of 0.2% ropivacaine as the initial bolus followed by 6ml/hr
infusion of 0.1% ropivacaine with 2µg/ml fentanyl. Group B received 6ml of
0.25% bupivacaine as initial bolus followed by 6ml/hr infusion of 0.125%
bupivacaine with 2µg/ml fentanyl. Various parameters and complications if
any were recorded every 15 minutes in the 1st hour, every 30 minutes in the
2nd hour and every hour later on.
The observations noted were as follows:
Pain relief as observed by verbal numerical rating scale was as low as
0.02 in both the groups till 2 hours. The mean score went upto 0.42 in
Group-A(ropivacaine) and 0.52 in Group-B(bupivacaine). The
fluctuations in pain were not clinically or statistically significant between
the two study groups.
The number of patients who required bolus were 7(20%) in both the
groups.
The spontaneous deliveries were more, 62.9% in Group-A as
compared to 54.3% in Group-B. The instrumental delivery rates were
less, 25.7% in Group-A as compared to 37.1% in Group-B.Cesarean
sections were performed in 4(11.4%) women in Group-A as compared
113
to 3(8.4%) patients in Group-B. These differences were not statistically
significant.
The duration of first stage of labour was 467 minutes in both the
groups. The mean duration of second stage of labour was 33 minutes
in Group-A as compared to 31 minutes in Group-B. The third stage of
labour was 6 minutes in both the groups.
No adverse neonatal outcome(because of the drugs used) in the form
of low Apgar scores or admission to NICU were noticed in both the
groups.
Motor block was observed in 3 patients (8.5%) in Group B(bupivacaine)
only. There was no clinically observable motor blockade in Group-
A(ropivacaine). This difference was not statistically significant.
The incidence of complications was minimal and comparable in both
groups.
Drawbacks of our study:
We did not double-blind this study.
We relied upon Apgar score for assessing the neurobehavioural
outcome of the baby.
We did not measure the umbilical cord pH to know the effect of drugs
on the acid base status of the newborn due to financial constraints.
114
Conclusion
Obstetric analgesia strives at making childbirth, a pleasurable and
painless event. As a means toward this end, we should ideally adopt the best
possible technique, something that would provide excellent analgesia with
minimal side effects and absolute safety to the mother and child.
The observations of this study show that pain relief offered by epidural
ropivacaine is as good and effective as epidural bupivacaine. Also the
duration of labour, mode of delivery, neonatal outcome and complications are
comparable between the two groups.
From this study it can be concluded that though ropivacaine is less
potent than bupivacaine, ropivacaine is as efficacaious as bupivacaine in the
concentrations used in our study.
115
Bibliography: 1. ACOG - Committee on Obstetric practice – Committee Opinion –
Number 295, July 2004.
2. ASA newsletter – September 1997, Volume 69,Number 9.
3. Wong CA. Advances in labour analgesia, Int J Womens Health 2009;1:139-54.
4. Hawkins JL. Epidural analgesia for Labour and delivery. N Engl J Med 2010;362: 1503-10.
5. Polley LS, Columb MO, Wagner DS, Naughton NN. Dose-dependent reduction of the minimum local analgesic concentration of bupivacaine by sufentanil for epidural analgesia in labor. Anesthesiology 1998;89(3):626–632.
6. Lyons G, Columb M, Hawthorne L, Dresner M. Extradural pain relief in labour: bupivacaine sparing by extradural fentanyl is dose dependent.Br J Anaesth. 1997;78(5):493–497.
7. Justins DM, Francis D, Houlton PG, Reynolds F. A controlled trial of extradural fentanyl in labour. Br J Anaesth. 1982;54(4):409–414.
8. Polley L S, Columb M O, Naughton N N, Wagner D S, van de Ven C J. Relative analgesic potencies of ropivacaine and Bupivacaine for epidural analgesia in labor: implications for therapeutic indexes. Anesthesiology 1999; 90: 944-50.
9. Capogna G, Celleno D, Fusco P, Lyons G, Columb M. Relative potencies of Bupivacaine and ropivacaine for analgesia in labour. Br J Anesth 1999; 82: 371-73.
10. Owen M D, D’ Angelo R, Gerancher J C. 0.125% ropivacaine is similar to 0.125% Bupivacaine for labor analgesia using patient controlled epidural infusion. Anesth Analg 1998; 86: 527-31.
11. D.C., Dutta, Normal Labour, Text book of Obstetrics
12. Crawford. J.S. (1982), Obstetric Analgesia and anaesthesia I Current reviews in obstetrics and Gynecology. Edinburgh:Churchill Livingstone.
13. Wylie and Churchill-Davidsons, A practice of Anaesthesia 5th Edition.
14. Bonica, J J (1979). Peripheral mechanisms and pathways of parturition pain. Brit. J. Anaesth 1979,51, 3S.
15. Cleland, J.G. P (1933). Paravertebral anaesthesia in obstetrics. Experimental and clinical basis. Surg, Gynecol, Obstet, 57, 51.
116
16. Obstetric anaesthesia, Wylie and Churchill-Davidsons, A practice of Anaesthesia, 7th Edition.
17. Dick Read G (1959). Childbirth without fear, 2nd edit. New York: Harper and Row.
18. Lamaze F 1958, painless childbirth (Celestin LR trans) London; Burke.
19. Melzack A R 1984, The myth of painless child birth. Pain 19: 321-327.
20. Ginsburg J, 1971 Am Rev Pharmacid 11:387.
21. McAllister CB 1980, Placental transfer and neonatal effects of diazepam when administered to women just before delivery Br J Anaesth 53:423-427.
22. RefStad SO, Lindback E 1980, Ventilatory depression of the new born of women receiving pethidine or pentazocine Br.J Anaesth 52: 265-271.
23. Gallon S (1976) Ketamine for obstetric deliviery, Anaesthesiology, 44, 522.
24. Hodgkinson R, Marx G, Kim S.S and Miclat, N.M (1977) Neonatal neurobehavioral tests following vaginal delivery under ketamine thiopental and extradural analgesia. Anesth Analg cum Res 56, 548.
25. Hinova A, Fernando R. Systemic remifentanil for labor analgesia. Anesth Analg.2009 Dec;109(6):1925-9.
26. Waring J, Mahboobi SK, Tyagaraj K, Eddi D. Use of remifentanil for labor analgesia: the good and the bad. Anesth Analg. 2007
27. Schnabel A, Hahn N, Broscheit J, Muellenbach RM, Rieger L, Roewer N, Kranke P.Remifentanil for labour analgesia: a meta-analysis of randomised controlled trials. Eur J Anaesthesiol. 2012 Apr;29(4):177-85.
28. Yeo ST, Holdcroft A, Yentis SM, Stewart A, Bassett P. Analgesia with sevoflurane during labour: ii. Sevoflurane compared with Entonox for labour analgesia. Br J Anaesth. 2007 Jan;98(1):110-5
29. Crawford JS 1979, Lumbar Epidural block in Labour, a clinical analysis Br. J. Anesth 44: 66-74.
30. Bromage P.R. (1978) Epidural Analgesia Philadelphia: W B.Saunders
31. Hjermstad MJ, Fayers PM, Haugen DF, Caraceni A, Hanks GW, Loge JH, Fainsinger R, Aass N, Kaasa S; European Palliative Care Research Collaborative (EPCRC).Studies comparing numerical Rating Scales, Verbal Rating Scales, and Visual Analogue Scales for
117
assessment of pain intensity in adults: a systematic literature review. J Pain Symptom Manage. 2011 Jun;41(6):1073-93.
32. Breivik EK, Björnsson GA, Skovlund E. A comparison of pain rating scales bysampling from clinical trial data. Clin J Pain. 2000 Mar;16(1):22-8.
33. Beilin Y, Hossain S, Bodian CA. The numeric rating scale and labor epidural analgesia. Anesth Analg. 2003 Jun;96(6):1794-8
34. Anim-Somuah M, Smyth R, Howell C. Epidural versus non-epidural or no analgesia in labour. Cochrane Database Syst Rev. 2005 Oct 9;(4):CD000331. Review. Update in: Cochrane Database Syst Rev. 2011;(12):CD000331
35. Spinal analgesia: intradural and extradural; Lee’ Synopsis of Anaesthesia.
36. Anaesthesia for Obstetrics; Anaesthesia , Ronald D.Miller.
37. Batson O.V. Ann.Surg. 1940, 112, 138,; Am. J. Roentgenol, 1942, 48, 715.
38. Epidural Space anatomy, depts.. Washington. Edu / aneth / regional / epidural space; www.google.com.
39. Brown D.L: Spinal, epidural and caudal anaesthesia: Anatomy, physiology and technique. In chestnut DH(ed): Obstetric Anaesthesia: Principles and practice, 2nd Ed. St. Louis, Mosby, 1999, p187.
40. Cynthia A.Wong, Mark C. Norris; Acute Situation: Obstetrics; Text book of Regional Anaesthesia P.Prithiviraj.
41. Galbert, M.W. and Marx.G.F.(1974), Extradural pressures in parturient patient Anaesthesiology, 40, 499.
42. Bromage PR: Spread of analgesic solution in the epidural space and their site of action; A statistical study Br.J anaesth 34: 161, 1962.
43. Abouleish E I : Post partum tubal ligation requires more bupivacaion for spinal anaesthesia than does caesarean section anaesth analg 65: 897, 1986.
44. Kaneko M, Kirhara V, Kosaka V: Pregnancy Enhances the antinociceptive effects of extradural lignocaine in the rat. Br. J. Anaesth 72:657y, 1994.
45. Popitz Bergez FA, Lesson S, Thalhammer J G et al: intraneural lidocaine uptake compared with analgesic difference between pregnant and non-pregnant rates eg Anesth 22; 363, 1997.
118
46. Butlerworth J F, Walker F O, Lysak S L: Pregnancy increase median nerve susceptibility of lidocaine Anaesthesioloy 72: 962, 1990.
47. Dietz F B, Jaffe R A: Pregnency does not increase susceptibility to bupivacaine in spinal root axons, Anaesthesiology 87:610,1997.
48. Lauretli GR: Mechanisms of labour pain, In norvis M C (ed): obstetric Anaesthesia 2nd ed Philadelphia, Lippincott, 1999, P235.
49. Dalt J.S., Taneja Bharti. Obstetric Analgesia – An Indian perspective Ons. And Gynae 2000; 3: 176-180.
50. Stamer U.M, Grond S, Schneck H, Wulf H. Surveys on the use of regional anaesthesia in obstetrics. Carr Opin Anaesth 1999; 12: 565-71.
51. Camann WR, Murray R.S., Mushlin P.S., Lambert DH. Effects of oral caffeine on postdural puncture headache; a double blind placebo controlled trial 1990; 70: 181-184.
52. Horlocker T.T. Complications of spinal and epidural anaesthesia. Anaesthesiology Clinic 2000; 18: 461-485.
53. Butler. R, Fuller J. Backpain following epidural anaessthesia in labour. Can J Anaesth 1998; 45:5 / 724-728.
54. Abboud TK, Afrasiabi A, Sarki F, Daftarian F, Nagappala S, Noverhid R, Kuhnert B, Miller F, Continuous infusion epidural analgesia in Parturients receiving bupivacaine, chloroprocaine or lidocaine – maternal fetal and neonatal effects. Anaesth Analg 63: 421 – 428 1984.
55. Jouppila P, Jouppila R, Hollmen A et al 1982. Lumbar epidural Analgesia to improve intervillous blood flow during labour in severe preeclamsia. Obstet Gynecol 1982; 59:158-161.
56. Rowbottom SJ, Critchley LA, Gin T. 1997. Uterine rupture and epidural analgesia during trial of labour. Anaesthesia 1997; 52:486-5.
57. Simpson D et al. Ropivacaine-A review of its use in regional anesthesia and acute pain management. Drugs 2005; 65 (18):2675-2717.
58. Liu BG, Zhuang XL, Li ST, Xu GH. The effects of ropivacaine on sodium currents in dorsal horn neurons of neonatal rats. Anesth Analg. 2000 May; 90(5): 1034-8.
59. Morrison SG, Dominguez JJ, Frascarolo P, Reiz S. A comparison of the electrocardiographic cardiotoxic effects of racemic bupivacaine, levobupivacaine and ropivacaine in anesthetized swine. Anesth Analg. 2000 Jun; 90(6):1308-14.
119
60. Butterworth JF, Strichartz GR. Molecular mechanism of local anesthesia-A review.Anesthesiology 1990; 72:722-34.
61. Lee-Son S, Nang GK, Concus A et al. Stereo selective inhibition of neuronal sodium channels by local anesthetics: Evidence for two sights for action? Anesthesiology 1992;77; 324-35.
62. Rothstein P, Cole J, Pih BR. Pulmonary extraction of bupivacaine is dose dependent. Anesthesiology 1984; 61;236.
63. Pihlajamaki K, Kantro J, Lindberg R et al. Extradural administration of bupivacaine: Pharmacokinetics and metabolism in pregnant and non pregnant women. Br J Anesth 1990; 64:556-62.
64. Duncan L, Wildsmith JAW. Liposomal local anesthetics. Br J Anesth 1995; 75:260-61.
65. Brown DT, Beamish D, Wildsmith JAW. Allergic reaction to an amide local anesthetic.Br J Anesth 1981; 53:435-37.
66. Covino BG, Vassallo HC. Local anesthesia, mechanism of action and clinical use. New York: Grune and Stratton, 1976.
67. Albright GA. Cardiac arrest following regional anesthesia with etidocaine or bupivacaine.Anesthesiology 1979; 51:285-87.
68. Timour Q, Fuys N, Coazon P et al. Possible role of drug interactions, bupivacaine induced problems related to intraventricular conduction disorder. Reg Anesth 1990; 15:180-85.
69. Roitman K, Sprung J, Wallace M et al. Enhancement of bupivacaine cardio toxicity with cardiac glycosides and beta adrenergic blockers-A case report. Anesth Analg 1993; 76: 658-61.
70. Atlee Jl, Bosnjak ZL. Mechanism of dysrhythmias during anesthesia. Anesthesiology 1990; 72:347-74.
71. Kendig JJ. Clinical implications of the modulated receptor hypothesis; local anesthetics and the heart. Anesthesiology 1985; 62:382-84.
72. Chestnut H. Obstetric Anesthesia -Principles and Practice, 3rd Edition,2004:pg – 813.
73. Boogaerts J, Decdercq A, Lafont N et al. Toxicity for bupivacaine encapsulated into liposomes and injected IV: comparison with plain solutions. Anesth Analg 1993; 76:553-55.
74. Picard j, Meek T. Lipid emulsion to treat overdose of local anesthetic, the gift of the globe. Anesthesia 2006; 61:107-09.
120
75. Rosenblatt MA, Abel M, Fischer GW et al. Successful use of a 20% lipid emulsion to resuscitate a patient after a presumed bupivacaine related cardiac arrest. Anesthesiology 2006; 105:217-18.
76. Hiller A, Rosenberg PH. Transient neurological symptoms after spinal anesthesia with 4% mepivacaine and 0.5% bupivacaine. Br J Anesth 1997; 79:301-05.
77. Akio J, Yoshitomi A, Kohji N et al. Local anesthetics inhibit priming of neutrophils by lipopolysaccharide for enhanced release of superoxides: suppression of cytochrome b 558 expression by disparate mechanism. Journal of leukocyte biology 2005; 78:1356-65.
78. Stoelting RK, Editors. Pharmacology and physiology in anesthetic practice 3rd ed.Philadelphia, Pennsylvania: Lippincott ravens publishers; 1999 p.93.
79. Pleuvry BJ. Opiod receptors and their relevance to anesthesia. Br J Anesth 1993; 71:119-26.
80. Stein C. The control of pain in peripheral tissues by opiods. N Engl J Med 1995; 332:1685-90.
81. Atcheson R, Lambert DG. Update on opiod receptors. Br J Anesth 1994; 73:132-34.
82. De Leon-Casasola OA, Lema MJ - post operative epidural opioid analgesia.What are their choices? Anesth Analg 1996; 83:867-75.
83. Hug CC, Murphy MR. Tissue redistribution of fentanyl and termination of its effects in rats. Anesthesiology 1991; 55:369-75.
84. Roerig DL, Kotrly KJ, Vucins EJ et al. First pass uptake of fentanyl, Meperidine and morphine in human being. Anesthesiology 1987; 67:466-72.
85. Schneider E, Brune K. Opiod activity and distribution of fentanyl metabolites. Naunyn Schmiedebergs Arch Pharmacle 1986; 334:267-74.
86. Mc Evan AI, Smith C, Dyar O et al. Isoflurane minimum alveolar concentration eduction by fentanyl. Anesthesiology 1993; 78:864-69.
87. Ronald. D Miller .Miller’s Anaesthesia 7th edition.
88. Lyons G, Columb M, Hawthorne L, Dresner M. Extradural pain relief in labour: bupivacaine sparing by extradural fentanyl is dose dependent.Br J Anaesth. 1997;78(5):493–497.
121
89. Stienstra R, Jonker T, Bourdrez P, Kuijpers J, van Kleef J, Lundberg U. Ropivacaine 0.25% Versus Bupivacaine 0.25% for Continuous Epidural Analgesia in Labor: A Double-Blind Comparison. Anesth Analg 1995;80(2):285-9.
90. McCrae AF, Jozwiak H, McClure JH. Comparison of ropivacaine and bupivacaine in extradural analgesia for the relief of pain in labour. Br J Anaesth. 1995 Mar;74(3):261-5.
91. Eddleston JM, Holland JJ, Griffin RP, Corbett A, Horsman EL, Reynolds F. A double-blind comparison of 0.25% ropivacaine and 0.25% bupivacaine for extradural analgesia in labour. Br J Anaesth. 1996 Jan;76(1):66-71.
92. Benhamou D, Hamza J, Eledjam JJ, Dailland P, Palot M, Seebacher J, Milon D,Heeroma K. Continuous extradural infusion of ropivacaine 2 mg ml-1 for pain relief during labour. Br J Anaesth. 1997 Jun;78(6):748-50.
93. Cascio MG, Gaiser RR, Camann WR, Venkateswaran P, Hawkins J, McCarthy D.Comparative evaluation of four different infusion rates of ropivacaine (2 mg/mL) for epidural labor analgesia. Reg Anesth Pain Med. 1998 Nov-Dec;23(6):548-53.
94. Beilin Y, Galea M, Zahn J, Bodian CA. Epidural ropivacaine for the initiation of labor epidural analgesia: a dose-finding study.Anesth Analg 1999;88:1340–5.
95. Gautier P, De Kock M, Van Steenberge A, Miclot D, Fanard L, Hody JL. A double-blind comparison of 0.125% ropivacaine with sufentanil and 0.125% bupivacaine with sufentanil for epidural labor analgesia. Anesthesiology. 1999 Mar;90(3):772-8
96. Meister G C, D’ Angelo R, Owen M, Nelson K E, Gaver R. A comparison of epidural analgesia with 0.125% Ropivacaine with Fentanyl versus 0.125% Bupivacaine with Fentanyl during labor. Anesth Analg 2000; 90: 632-37.
97. Campbell DC, Zwack RM, Crone LL, Yip RW. Ambulatory labor epidural analgesia: bupivacaine versus ropivacaine. Anesth Analg 2000; 90: 1384–9.
98. Fettes PDW, Moore CS, Whiteside JB, Mcleod GA, Wildsmith JAW. Intermittent vs continuous administration of epidural ropivacaine with fentanyl for analgesia during labour. Br J Anaesth 2000; 97: 359–64.
99. Fischer C, Blanie P, Jaouen E, Vayssiere C, Kaloul I, Coltat J. Ropivacaine, 0.1%, Plus Sufentanil, 0.5 µg/ml, versus Bupivacaine, 0.1%, Plus Sufentanil, 0.5 µg/ml, Using Patient-controlled Epidural
122
analgesia for Labor: A Double-blind Comparison.Anaesthesiology 2000;92(6):1588-1593.
100. Finegold H, Mandell G, Ramanathan S. Comparison of ropivacaine 0.1%-fentanyl and bupivacaine 0.125% -fentanyl infusions for epidural labour analgesia. Can J Anesth 2000 / 47: 8 / pp 740–745
101. Ruban P, Sia AT, Chong JL. The effect of adding fentanyl to ropivacaine 0.125% on patient-controlled epidural analgesia during labour. Anaesth Intensive Care. 2000 Oct;28(5):517-21.
102. McClellan KJ, Faulds D. Ropivacaine: an update of its use in regional anaesthesia. Drugs. 2000 Nov;60(5):1065-93.Dresner M, Freeman J, Calow C, Quinn A, Bamber J: Ropivacaine 0.2% versus bupivacaine 0.1% with fentanyl: a double blind comparison for analgesia during labour. Br J Anesth. 2000 Dec; 85(6):826-9.
103. Dresner M, Freeman J, Calow C, Quinn A, Bamber J: Ropivacaine 0.2% versus bupivacaine 0.1% with fentanyl: a double blind comparison for analgesia during labour. Br J Anesth. 2000 Dec; 85(6):826-9.
104. Merson N. A comparison of motor block between ropivacaine and bupivacaine for continuous labor epidural analgesia. AANA J. 2001 Feb;69(1):54-8.
105. Chua NP, Sia AT, Ocampo CE: Parturient-controlled epidural analgesia during labour: bupivacaine vs. ropivacaine. Anaesthesia. 2001 Dec; 56(12):1169-73.
106. Fernández-Guisasola J, Serrano ML, Cobo B, Muñoz L, Plaza A, Trigo C, Del Valle SG. A comparison of 0.0625% bupivacaine with fentanyl and 0.1% ropivacaine with fentanyl for continuous epidural labor analgesia. Anesth Analg. 2001 May;92(5):1261-5.
107. Clément HJ, Caruso L, Lopez F, Broisin F, Blanc-Jouvan M, Derré-Brunet E, Thomasson A, Leboucher G, Viale JP. Epidural analgesia with 0.15% ropivacaine plus sufentanil 0.5 microgram ml-1 versus 0.10% bupivacaine plus sufentanil 0.5 microgram ml-1: a double-blind comparison during labour. Br J Anaesth. 2002 Jun;88(6):809-13.
108. Lacassie HJ, Columb MO, Lacassie HP, Lantadilla RA. The relative motor blocking potencies of epidural bupivacaine and ropivacaine in labor. Anesth Analg. 2002 Jul;95(1):204-8
109. Owen MD, Thomas JA, Smith T, Harris LC, D’Angelo R. Ropivacaine 0.075% and Bupivacaine 0.075% with Fentanyl 2 µg/mL are Equivalent for Labor Epidural Analgesia. Anesth Analg 2002;94:179–83.
123
110. Lee BB, Ngan Kee WD, Lau WM, Wong AS. Epidural infusions for labor analgesia: a comparison of 0.2% ropivacaine, 0.1% ropivacaine, and 0.1% ropivacaine with fentanyl. Reg Anesth Pain Med. 2002 Jan-Feb;27(1):31-6.
111. Asik I, Goktug A, Gulay I, Alkis N, Uysalel A: Comparison of bupivacaine 0.2% and ropivacaine 0.2% combined with fentanyl for epidural analgesia during labour. Eur J Anaesthesiol. 2002 Apr; 19(4):263-70.
112. Fernandez C, Sala X, Plaza A, Lopez A, Celemin M, Gomar C: Epidural anesthesia with ropivacaine vs. bupivacaine in continuous perfusion for the treatment of labor pains. Rev Esp Anestesiol Reanim. 2003 Feb; 50(2):70-6.
113. Boselli E, Debon R, Duflo F, Bryssine B, Allaouchiche B, Chassard D.Ropivacaine 0.15% plus sufentanil 0.5 microg/mL and ropivacaine 0.10% plus sufentanil 0.5 microg/mL are equivalent for patient-controlled epidural analgesia during labor. Anesth Analg. 2003 Apr;96(4):1173-7.
114. Gogarten W, Van de Velde M, Soetens F, Van Aken H, Brodner G, Gramke HF, Soetens M, Marcus MA. A multicentre trial comparing different concentrations of ropivacaine plus sufentanil with bupivacaine plus sufentanil for patient-controlled epidural analgesia in labour. Eur J Anaesthesiol. 2004 Jan;21(1):38-45.
115. Atienzar MC, Palanca JM, Borras R, Esteve I, Fernandez M, Miranda A.Ropivacaine 0.1% with fentanyl 2 microg mL(-1) by epidural infusion for labour analgesia. Eur J Anaesthesiol. 2004 Oct;21(10):770-5.
116. Neera Sah, Vallejo M, Phelps A, Finegold H, Mandell G, Ramanathan. Efficacy of ropivacaine, bupivacaine, and levobupivacaine for labor epidural analgesia .S. Journal of Clinical Anesthesia 2007; 19: 214–17.
117. WANG Li-zhong, CHANG Xiang-yang, LIU Xia, HU Xiao-xia and TANG Bei-lei. Comparison of bupivacaine, ropivacaine and levobupivacaine with sufentanil for patient-controlled epidural analgesia during labor: a randomized clinical trial. Chin Med J 2010;123(2):178-83.
118. Beilin Y, Guinn NR, Bernstein HH, Zahn J, Hossain S, Bodian CA. Local anesthetics and mode of delivery: bupivacaine versus ropivacaine versus levobupivacaine. Anesth Analg. 2007 Sep;105(3):756-63.
124
119. Kalra S, Saraswat N, Agnihotri GS. Comparison of efficacy of bupivacaine and fentanyl with bupivacaine and sufentanil for epidural labor analgesia. Saudi J Anaesth. 2010 Sep;4(3):178-81.
120. Ngan Kee WD, Ng FF, Khaw KS, Lee A, Gin T. Determination and comparison of graded dose-response curves for epidural bupivacaine and ropivacaine for analgesia in laboring nulliparous women. Anesthesiology. 2010 Aug;113(2):445-53.
121. Lee HL, Lo LM, Chou CC, Chuah EC: Comparison between 0.08% ropivacaine and 0.06% levobupivacaine for epidural analgesia during nulliparous labor: a retrospective study in a single center. Chang Gung Med J. 2011 May-Jun;34(3):286-92.
122. Halpern SH, Leighton BL, Ohlsson A, Barrett JF, Rice A. Effect of epidural vs parenteral opioid analgesia on the progress of labor: a meta-analysis. JAMA. 1998 Dec 23-30;280(24):2105-10.
123. Halpern SH, Walsh V. Epidural ropivacaine versus bupivacaine for labor: a meta-analysis. Anesth Analg. 2003 May;96(5):1473-9
124. Cambic CR, Wong CA. Labour analgesia and obstetric outcomes. Br J Anaesth.2010 Dec;105 Suppl 1:i50-60.
125. Writer WD, Stienstra R, Eddleston JM, Gatt SP, Griffin R, Gutsche BB, Joyce TH, Hedlund C, Heeroma K, Selander D. Neonatal outcome and mode of delivery after epidural analgesia for labour with ropivacaine and bupivacaine: a prospective meta-analysis. Br J Anaesth. 1998 Nov;81(5):713-7.
126. Beilin Y, Halpern S. Focused review: ropivacaine versus bupivacaine for epidural labor analgesia. Anesth Analg. 2010 Aug;111(2):482-7.
127. Halpern SH, Littleford JA, Brockhurst NJ, et al. The neurologic and adaptive capacity score is not a reliable method of newborn evaluation. Anesthesiology 2001;94:958–62.
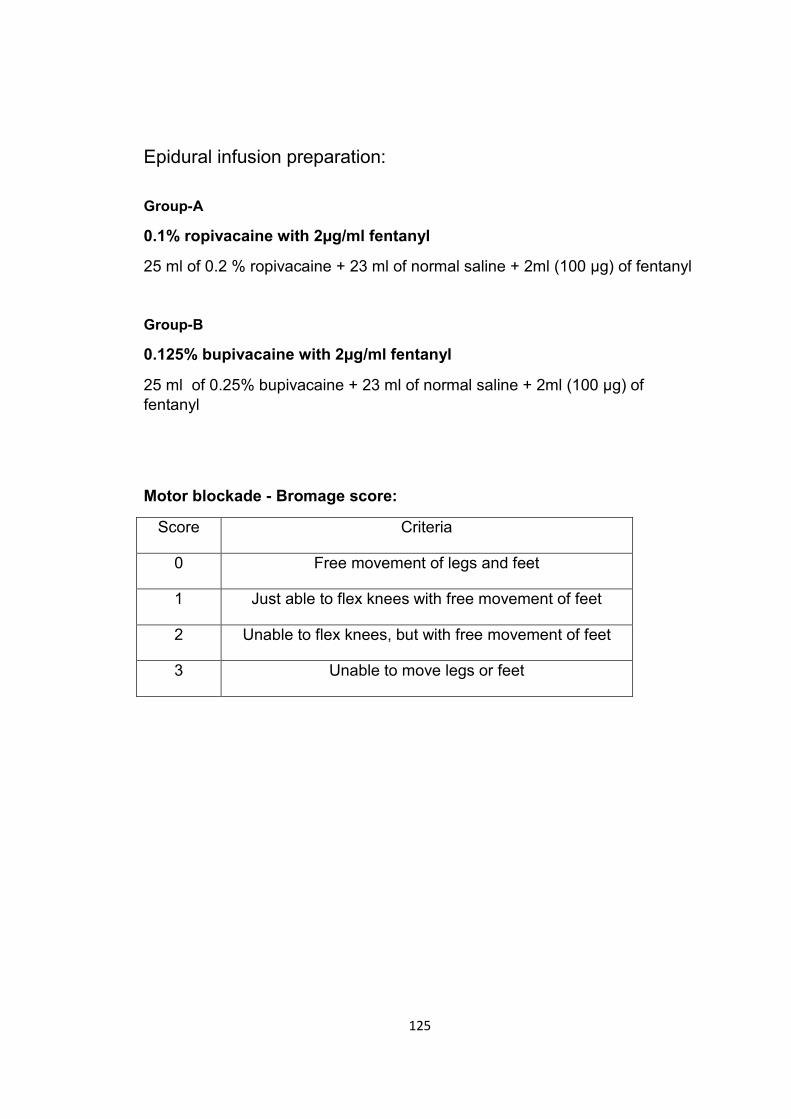
125
Epidural infusion preparation:
Group-A
0.1% ropivacaine with 2µg/ml fentanyl
25 ml of 0.2 % ropivacaine + 23 ml of normal saline + 2ml (100 µg) of fentanyl
Group-B
0.125% bupivacaine with 2µg/ml fentanyl
25 ml of 0.25% bupivacaine + 23 ml of normal saline + 2ml (100 µg) of
fentanyl
Motor blockade - Bromage score:
Score Criteria
0 Free movement of legs and feet
1 Just able to flex knees with free movement of feet
2 Unable to flex knees, but with free movement of feet
3 Unable to move legs or feet
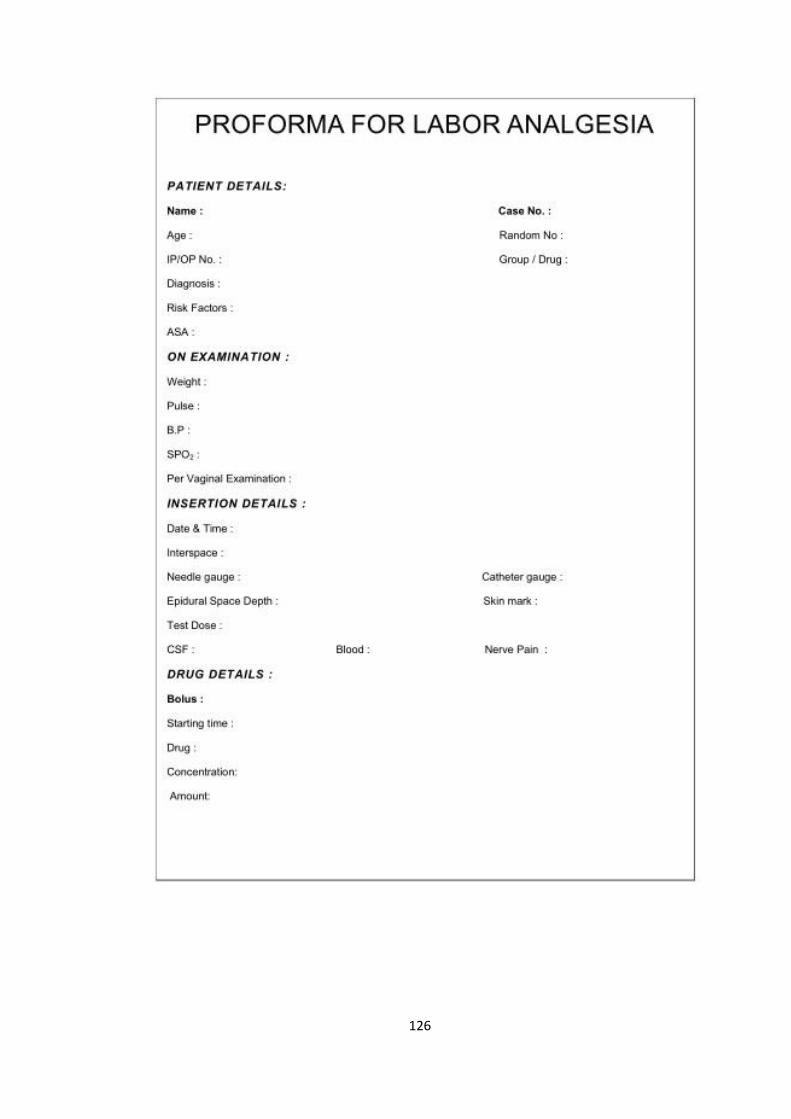
126
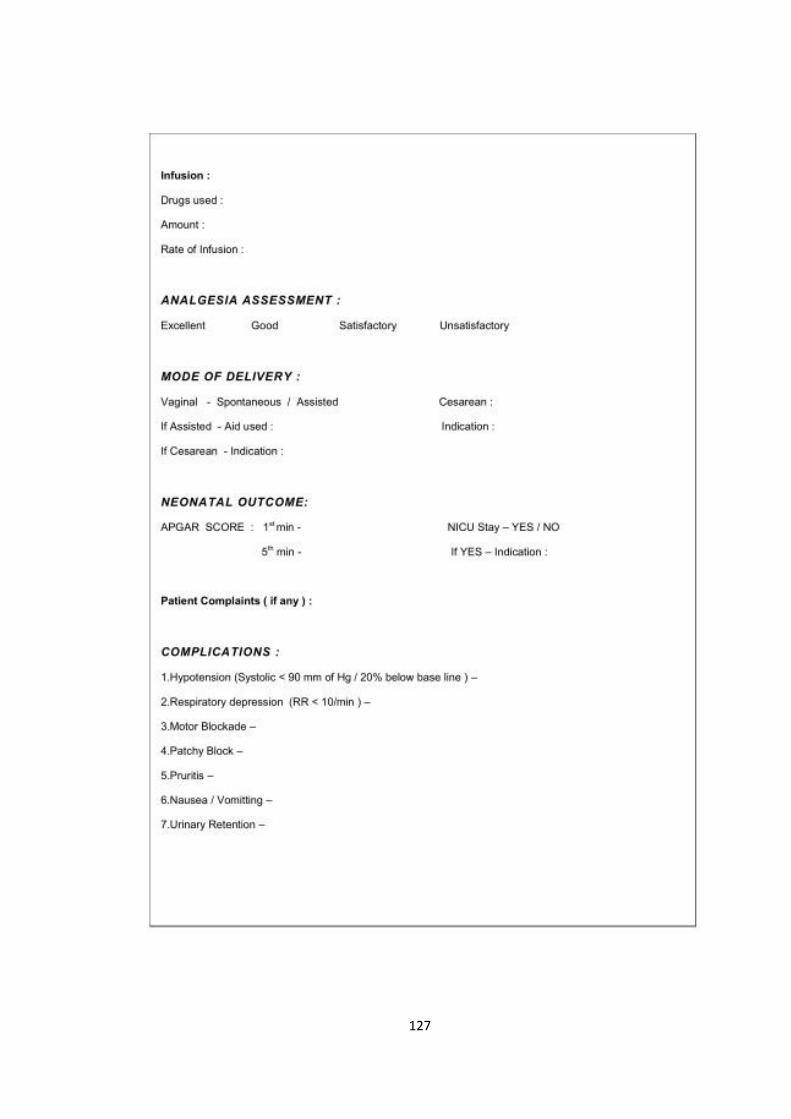
127
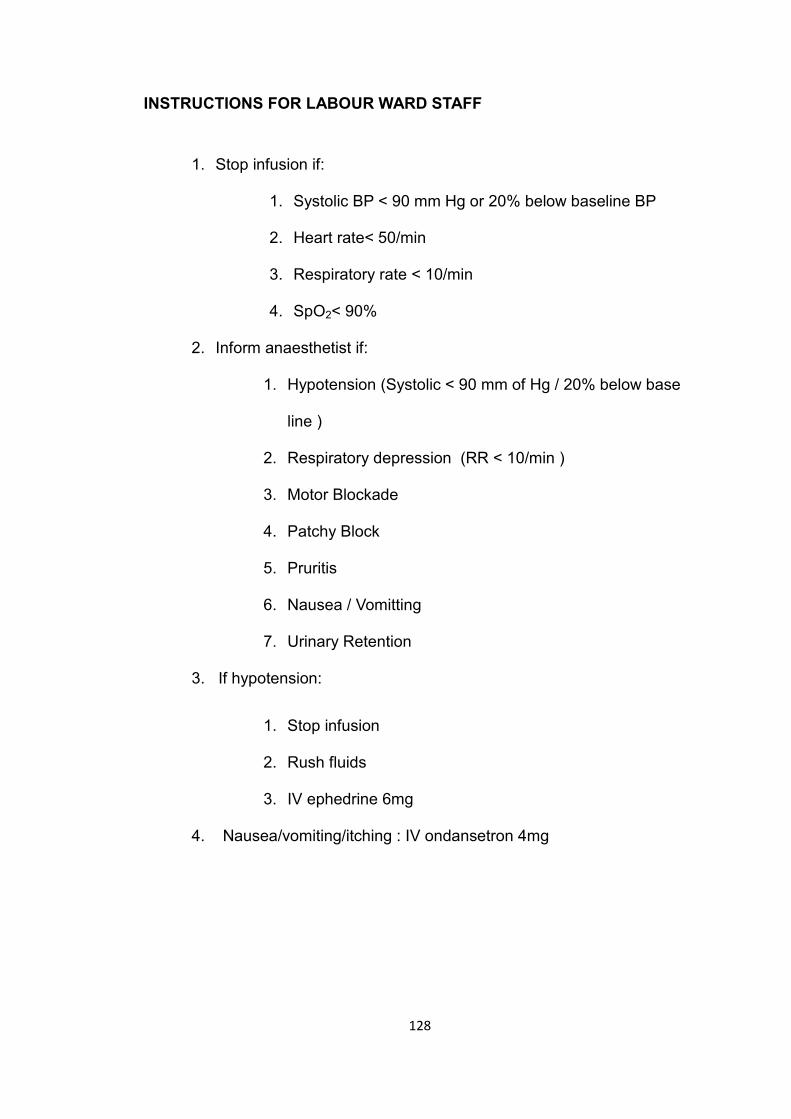
128
INSTRUCTIONS FOR LABOUR WARD STAFF
1. Stop infusion if:
1. Systolic BP < 90 mm Hg or 20% below baseline BP
2. Heart rate< 50/min
3. Respiratory rate < 10/min
4. SpO2< 90%
2. Inform anaesthetist if:
1. Hypotension (Systolic < 90 mm of Hg / 20% below base
line )
2. Respiratory depression (RR < 10/min )
3. Motor Blockade
4. Patchy Block
5. Pruritis
6. Nausea / Vomitting
7. Urinary Retention
3. If hypotension:
1. Stop infusion
2. Rush fluids
3. IV ephedrine 6mg
4. Nausea/vomiting/itching : IV ondansetron 4mg
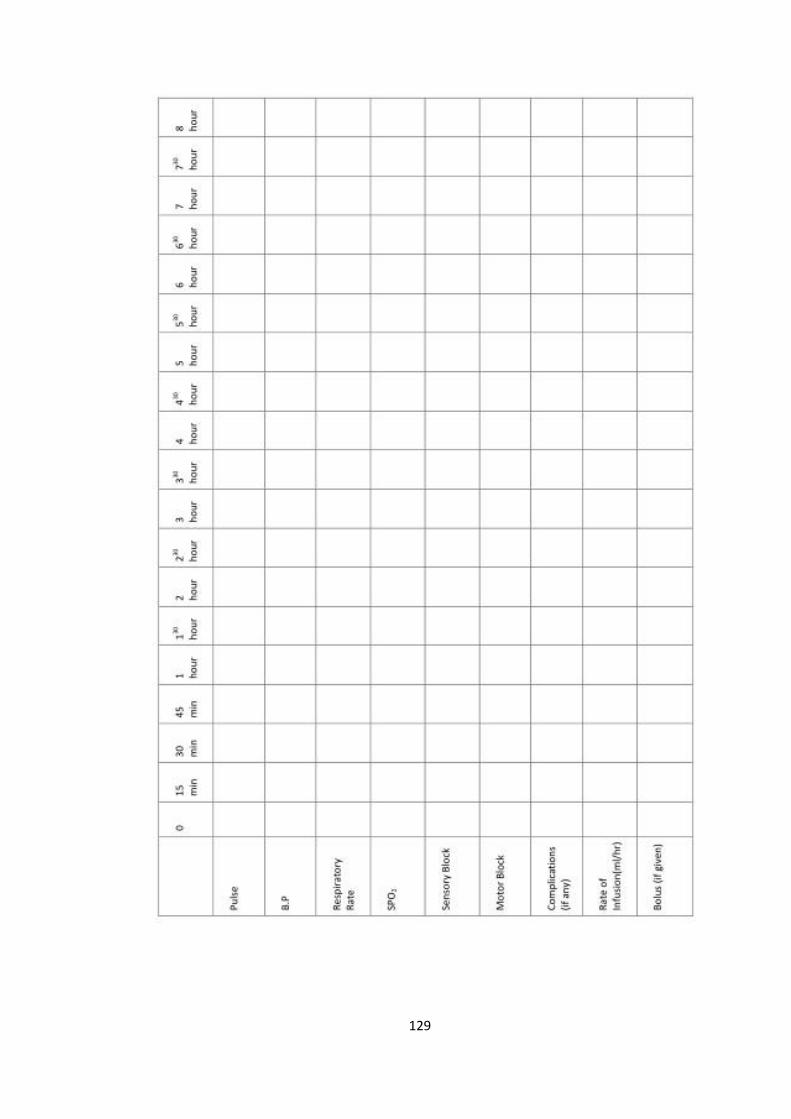
129
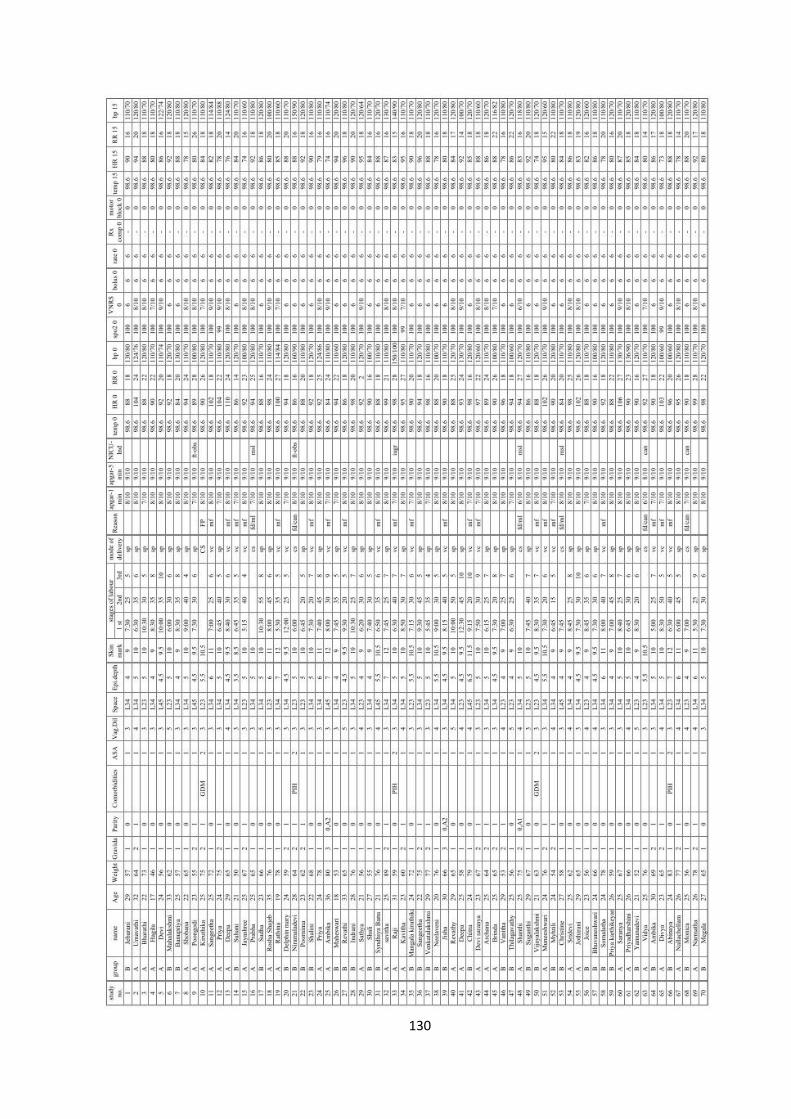
130
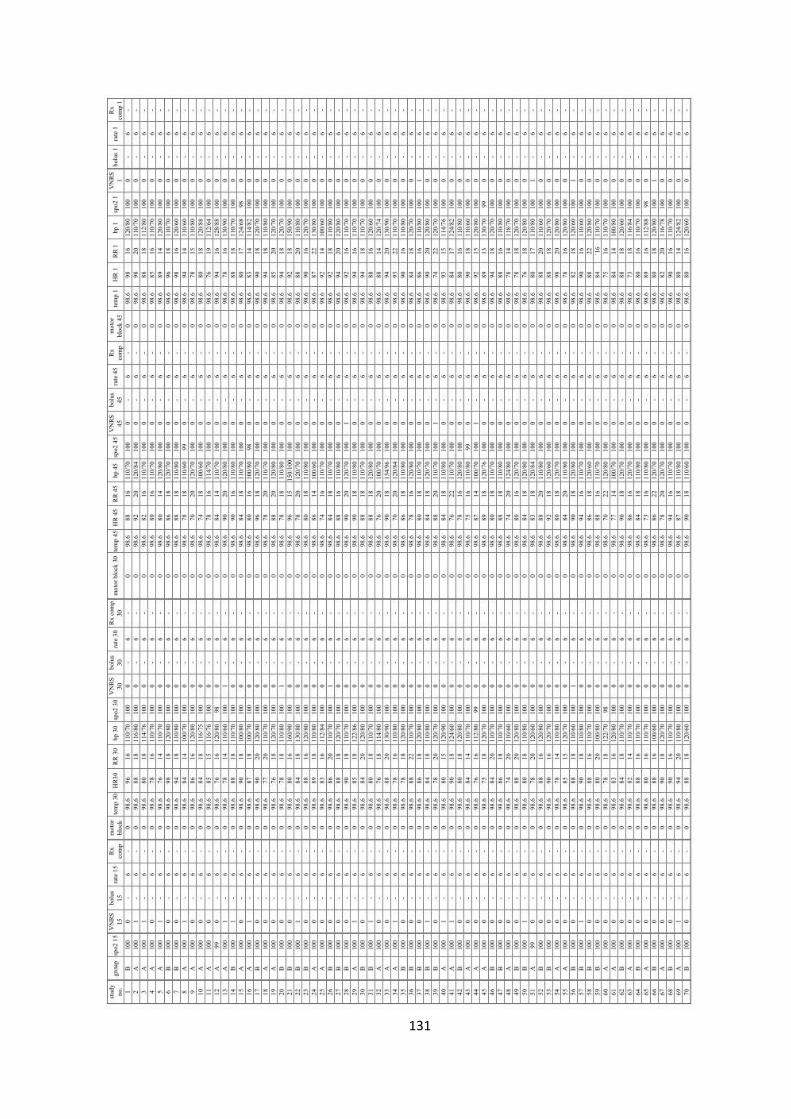
131
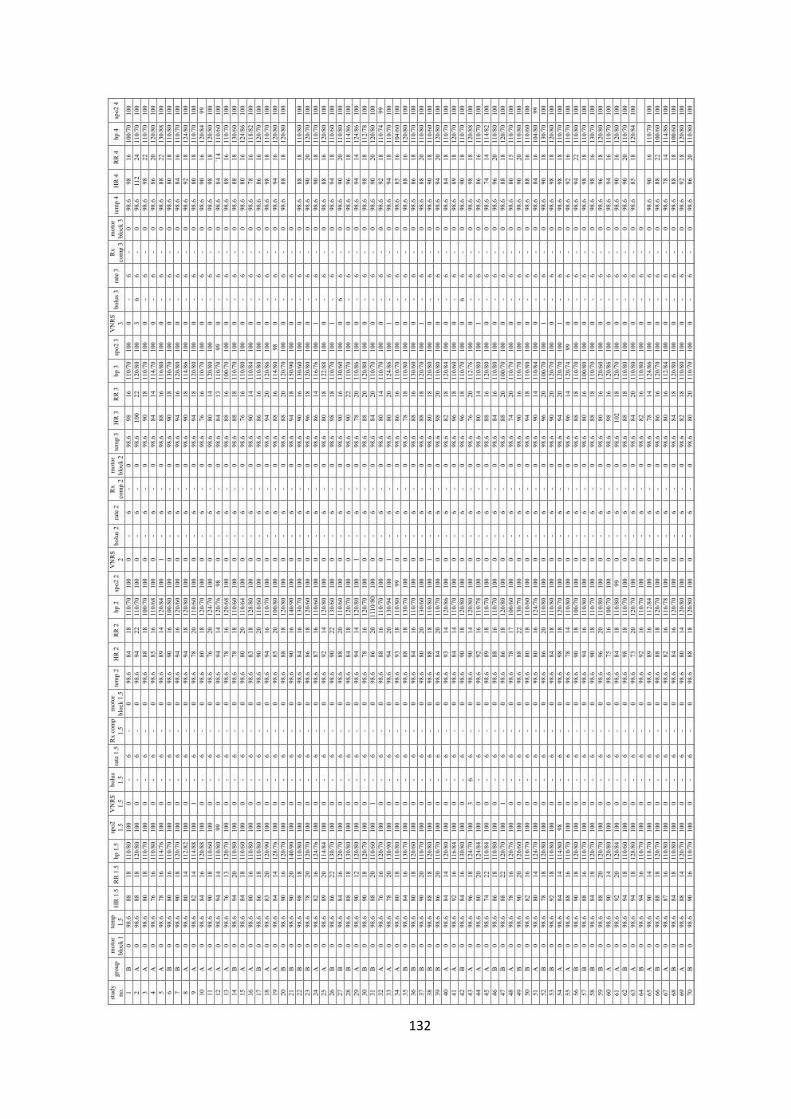
132
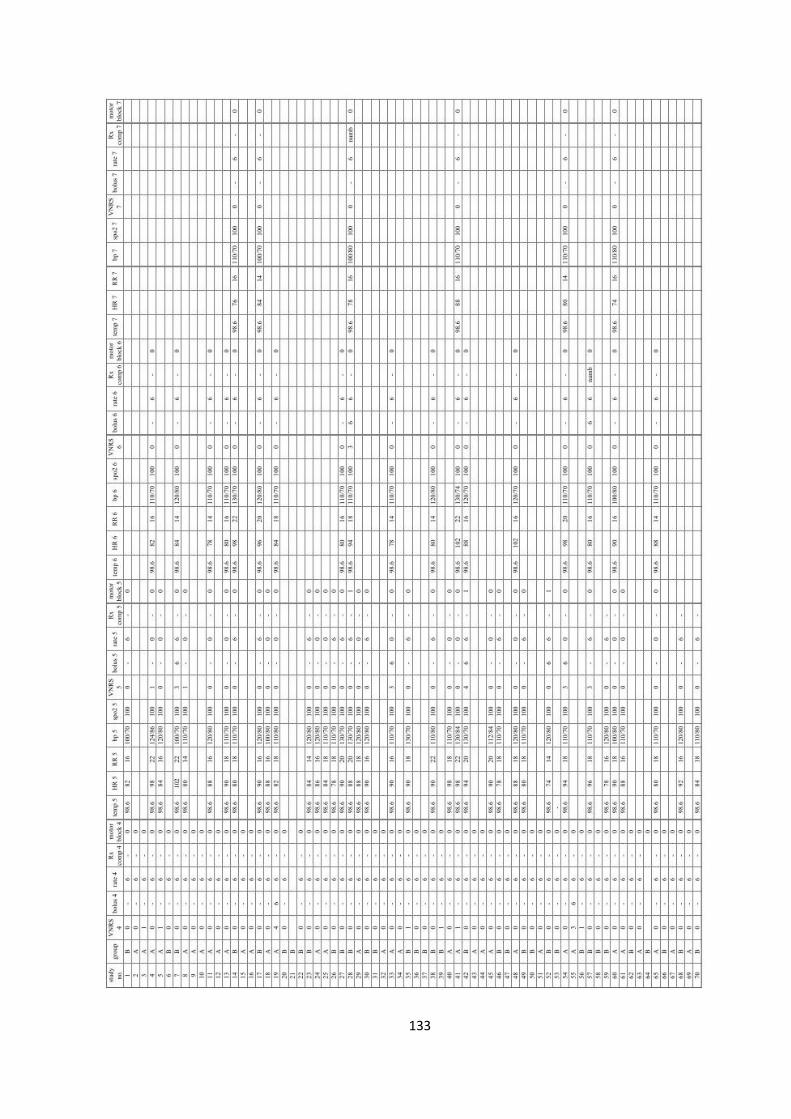
133
Related Documents











