The Posterior Pole and Papillomacular Fold in Posterior Microphthalmos Novel Spectral-Domain Optical Coherence Tomography Findings Sawsan R. Nowilaty, MD, 1 Ahmed Mousa, PhD, 2 Nicola G. Ghazi, MD 1 Purpose: To report and analyze the spectral-domain optical coherence tomography (SD-OCT) features of the posterior pole and papillomacular fold (PMF) in posterior microphthalmos (PM) in relation to axial length of the globe and corneal power. Design: Comparative case series. Participants: Forty eyes of 20 PM patients and 70 eyes of 35 age-matched controls. Methods: All PM and control eyes underwent a full biometric evaluation, including axial length and corneal power measurements, and macular SD-OCT. In addition, a novel SD-OCT marker of the posterior pole curvature, termed the posterior pole curvature index (PPCI), was measured along both the vertical and horizontal meridians. The OCT characteristics of the PMF were analyzed and the PPCIs were compared and correlated with the axial length and corneal power in both groups of eyes, and with the PMF severity in PM eyes. Main Outcome Measures: We considered the SD-OCT features of the PMF, the PPCI in PM eyes and controls, and the correlations between PPCI and PMF severity and axial length. Results: All PMFs were predominantly horizontal and partial thickness, sparing the outer retina except the outer plexiform layer. The PPCI in PM eyes (mean standard deviation, 14540.3 microns; median, 144) was significantly larger than that of controls (1412.8 microns; median, 14; P<0.0001). In addition, the vertical PPCI in PM eyes, but not in controls, was notably larger than the horizontal PPCI (mean difference, 5530.4 microns; P<0.0001). In PM eyes, the PPCI strongly correlated with PMF height (R ¼ 0.68; P<0.0001), inverse axial length (R ¼ e0.71; P<0.0001), and corneal power (R ¼ 0.49; P ¼ 0.002), and the PMF height correlated strongly and inversely with the axial length (R ¼ e0.62; P<0.0001). Conclusions: The PMF in PM eyes has characteristic morphologic SD-OCT features. The increased posterior pole curvature in PM and its significant correlation with the axial length, the PMF severity and keratometry established in this study suggest that PM eyes are not only shorter than normal, but seem to be abnormally shaped posteriorly, particularly along the vertical meridian. This factor may play a role in the pathogenesis and morphology of the PMF. Financial Disclosure(s): The authors have no proprietary or commercial interest in any of the materials discussed in this article. Ophthalmology 2013;-:-–- ª 2013 by the American Academy of Ophthalmology. Posterior microphthalmos (PM) is an ocular condition characterized by high hyperopia, a short axial length, posterior segment foreshortening, and a normal appearing anterior segment of normal or subnormal dimensions. 1-5 A retinal papillomacular fold (PMF) 1-4 or wrinkles 3,4 are characteristic findings in most eyes with the condition. These features are also present in nanophthalmos, but in the latter, the anterior segment is visibly small. 6-8 Previous reports have emphasized the posterior segment findings in PM and nanophthalmos, including the clinical appearance of the PMF. 1-4,7 It has been suggested that PMF formation may be the result of the disparity between the normal growth of the retina and the halted growth of the sclera, leading to redundancy of the retinal tissue. 1,9 However, the exact mechanism for the PMF formation remains speculative. Previous optical coherence tomography (OCT) studies have reported some of the morphologic features of the neural retina within the PMF and showed that the retinal pigment epithelium (RPE) and outer retina are intact and uninvolved by the PMF. 10-18 However, a detailed analysis of the internal structure of the PMF in a large sample of pa- tients is still lacking, especially with spectral-domain (SD)- OCT. Furthermore, although the axial (sagittal) biometric features of eyes with PM, namely a short axial length and vitreous compartment, a normal or slightly subnormal an- terior chamber depth and a relatively high lenseanterior chamber depth ratio have been reported, 1-5,9,13 information 1 Ó 2013 by the American Academy of Ophthalmology ISSN 0161-6420/13/$ - see front matter Published by Elsevier Inc. http://dx.doi.org/10.1016/j.ophtha.2013.01.026

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
The Posterior Pole and Papillomacular Fold inPosterior MicrophthalmosNovel Spectral-Domain Optical Coherence TomographyFindings
Sawsan R. Nowilaty, MD,1 Ahmed Mousa, PhD,2 Nicola G. Ghazi, MD1
Purpose: To report and analyze the spectral-domain optical coherence tomography (SD-OCT) features ofthe posterior pole and papillomacular fold (PMF) in posterior microphthalmos (PM) in relation to axial lengthof the globe and corneal power.
Design: Comparative case series.Participants: Forty eyes of 20 PM patients and 70 eyes of 35 age-matched controls.Methods: All PM and control eyes underwent a full biometric evaluation, including axial length and corneal
power measurements, and macular SD-OCT. In addition, a novel SD-OCT marker of the posterior pole curvature,termed the posterior pole curvature index (PPCI), was measured along both the vertical and horizontal meridians.The OCT characteristics of the PMF were analyzed and the PPCIs were compared and correlated with the axiallength and corneal power in both groups of eyes, and with the PMF severity in PM eyes.
Main Outcome Measures: We considered the SD-OCT features of the PMF, the PPCI in PM eyes andcontrols, and the correlations between PPCI and PMF severity and axial length.
Results: All PMFs were predominantly horizontal and partial thickness, sparing the outer retina except theouter plexiform layer. The PPCI in PM eyes (mean � standard deviation, 145�40.3 microns; median, 144) wassignificantly larger than that of controls (14�12.8 microns; median, 14; P<0.0001). In addition, the vertical PPCI inPM eyes, but not in controls, was notably larger than the horizontal PPCI (mean difference, 55�30.4 microns;P<0.0001). In PM eyes, the PPCI strongly correlated with PMF height (R ¼ 0.68; P<0.0001), inverse axial length(R ¼ e0.71; P<0.0001), and corneal power (R ¼ 0.49; P ¼ 0.002), and the PMF height correlated strongly andinversely with the axial length (R ¼ e0.62; P<0.0001).
Conclusions: The PMF in PM eyes has characteristic morphologic SD-OCT features. The increased posteriorpole curvature in PM and its significant correlation with the axial length, the PMF severity and keratometryestablished in this study suggest that PM eyes are not only shorter than normal, but seem to be abnormallyshaped posteriorly, particularly along the vertical meridian. This factor may play a role in the pathogenesis andmorphology of the PMF.
Financial Disclosure(s): The authors have no proprietary or commercial interest in any of the materialsdiscussed in this article. Ophthalmology 2013;-:-–- ª 2013 by the American Academy of Ophthalmology.
Posterior microphthalmos (PM) is an ocular conditioncharacterized by high hyperopia, a short axial length,posterior segment foreshortening, and a normal appearinganterior segment of normal or subnormal dimensions.1-5
A retinal papillomacular fold (PMF)1-4 or wrinkles3,4 arecharacteristic findings in most eyes with the condition.These features are also present in nanophthalmos, but inthe latter, the anterior segment is visibly small.6-8 Previousreports have emphasized the posterior segment findings inPM and nanophthalmos, including the clinical appearanceof the PMF.1-4,7 It has been suggested that PMF formationmay be the result of the disparity between the normalgrowth of the retina and the halted growth of the sclera,leading to redundancy of the retinal tissue.1,9 However,
� 2013 by the American Academy of OphthalmologyPublished by Elsevier Inc.
the exact mechanism for the PMF formation remainsspeculative.
Previous optical coherence tomography (OCT) studieshave reported some of the morphologic features of theneural retina within the PMF and showed that the retinalpigment epithelium (RPE) and outer retina are intact anduninvolved by the PMF.10-18 However, a detailed analysis ofthe internal structure of the PMF in a large sample of pa-tients is still lacking, especially with spectral-domain (SD)-OCT. Furthermore, although the axial (sagittal) biometricfeatures of eyes with PM, namely a short axial length andvitreous compartment, a normal or slightly subnormal an-terior chamber depth and a relatively high lenseanteriorchamber depth ratio have been reported,1-5,9,13 information
1ISSN 0161-6420/13/$ - see front matterhttp://dx.doi.org/10.1016/j.ophtha.2013.01.026

Ophthalmology Volume -, Number -, Month 2013
regarding the biometry of the posterior pole of the globe islimited. Also, to our knowledge, there are no reportedstudies that investigated a potential correlation between thebiometric characteristics of eyes with PM and the PMFfeatures, such as its height and morphology. Understandingthe biometry of the posterior pole in PM and its relationshipto the PMF characteristics and to other ocular biometricvariables may lead to a better understanding of the PMFfeatures and to clues regarding its pathogenesis.
In this study of a large cohort of PM eyes, we providea detailed analysis of the PMF features and investigate novelposterior pole biometric characteristics using SD-OCT. Inaddition, we study the relationship between these posteriorpole biometric characteristics and some of the fold features,such as its height and structure, as well as their relationshipto other ocular biometric variables, such as the axial lengthand the corneal curvature, in an effort to characterize thebiometric features of PM in a more comprehensive mannerand to elicit clues related to the pathogenesis of the PMF.
Subjects and Methods
The study was approved by the Institutional Review Board of theKing Khaled Eye Specialist Hospital and adhered to the tenets ofthe Declaration of Helsinki. The current study is a retrospective,case-control series. A total of 20 patients (40 eyes) were recruitedas cases, with 35 age-matched individuals (70 eyes) as controls.
PM Patients
All 20 patients enrolled in this retrospective OCT comparativeanalysis came from the clinical practice of one author (SRN) andwere part of a larger prospective clinical and genetic study of13 families with PM of which some genetic and biometric resultswere published.19,20 The diagnostic criteria of PM used in theprospective study included axial length <20 mm, hyperopia >8diopters (D), normal-appearing anterior segment of grossly normalsize, PMFs or wrinkles, normal intraocular pressure, and no ocularmalformations or associated syndromic disease. All identified PMpatients underwent a full clinical evaluation, including cycloplegicrefraction, a full biometric evaluation of the globe with measure-ments of the axial length, central anterior chamber depth, lensthickness, and vitreous depth (IOLMaster; Carl Zeiss Meditec AG,Jena, Germany); and measurement of the corneal diameter usinga caliper and measurement of the corneal power using manualkeratometry (Nidek ARK-700 Autorefractor-keratometer, Gama-gori, Japan or Topcon KR 8800 Autokerato-refractometer, Tokyo,Japan) and Orbscan IIz (Bausch and Lomb, Salt Lake City, UT),averaging the results of both methods for a final corneal power.Cooperative patients also underwent macular SD-OCT to study thePMF features. Of the 29 total patients recruited, 20 patients from11 families (40 eyes) had good quality SD-OCT and reliable ocularbiometry and these make up the cohort for this study.
SD-OCT Testing and Analysis
In all PM patients (40 eyes) a Spectralis SD-OCT (Spectralis,Heidelberg Engineering, Heidelberg, Germany) was used to studythe macular area. SD-OCT testing comprised at least 1 vertical and1 horizontal cut centered at the foveal area and passing through thePMF. In 19 eyes, additional vertical, horizontal, raster, and/orradial macular scans were obtained.
The initial intent of the study was to examine the morphologyand internal structure of the PMF, analyzing its shape, the integrity
2
of the neural retinal layers, the presence or absence of structuraldisorganization or cystic changes within the PMF, and the corre-lation of the PMF height with the axial length of the globe.However, after studying the SD-OCT of several PM eyes,a consistent feature became evident, suggesting an abnormallyincreased posterior pole curvature in the macular area that varied indegree among eyes and seemed to be grossly proportional to theheight of the PMF. To study this peculiar feature in a quantitativemanner, a novel parameter termed the posterior pole curvatureindex (PPCI) was calculated for all PM eyes as follows: Along thecurved RPE/Bruch membrane (RPE/BM) complex hyperreflectiveband, a point of maximum curvature was identified by the point oftangency between a horizontal line and the curvature of the RPE/BM complex (Fig 1A, B). At that point, the inner RPE surface wasidentified. To either side of this point, 2 other equidistant pointslocated 1500 microns from the point of maximum curvature werelocated and connected by a straight line. The vertical distancebetween this line and the inner RPE surface at the point ofmaximum curvature described represented the PPCI. This indexwas obtained using both the vertical (Fig 1A) and the horizontal(Fig 1B) OCT line scans yielding vertical and horizontal PPCIs,respectively, the values of which were then averaged to calculatean averaged PPCI. The 3 PPCIs (horizontal, vertical, andaveraged PPCI) were recorded for each eye.
In addition, the PMF severity was quantified by OCT. Using thevertical OCT line scan, 2 parameters were obtained for all PM eyesas follows. First, the “total PMF height” was estimated as thedistance between the BM hyperreflective band and the apex of thePMF. Second, the “PMF protrusion” beyond the inner surface ofthe retina was estimated by the distance between a hypothetical lineconnecting the inner surface of the retina on either side of the PMFprotrusion and the apex of the PMF (Fig 1A).
Controls
An age-matched control group was recruited and comprised 35individuals (aged 3e36 years; 70 eyes) with no prior history of eyesurgery, trauma, or disease and no significant refractive error (mean� standard deviation, 0.0�0.9 D; median, 0.1; range, e2.25to þ1.75). All control eyes underwent prospective autorefraction,axial length measurement (IOL Master, Carl Zeiss Meditec),manual keratometry (Nidek ARK-700, or Shin Nippon Autoref-K9003D, Japan) and Spectralis macular SD-OCT. The same meth-odology described was used to establish vertical, horizontal, andaveraged PPCIs in the control eyes for comparative analysis(Fig 1C, D).
Statistical Analysis
Collected data was stored using Microsoft Excel 2007. Data an-alysis was performed using SPSS version 19.0 (IBM Inc, Chicago,Illinois), MedCalc 11.6 (MedCalc Software bvba, Mariakerke,Belgium) and StatsDirect statistical software, version 2.7.2(StatsDirect Ltd, Cheshire, UK). A descriptive analysis was con-ducted for the continuous and categorical variables, and inferentialanalysis was performed to investigate potential differences, asso-ciations, and/or correlations among variables. The Pearson corre-lation test was applied to investigate the hypothesized correlationsbetween different indices, where the Pearson coefficient wascalculated as indicator for the correlation power. The Man-neWhitney U test was used to investigate the mean differencebetween groups. P<0.05 was considered significant withina confidence interval of 95%.
The vertical, horizontal, and averaged PPCIs in PM eyes werecompared with those of the age-matched control eyes. In addition,the vertical PPCI was compared with the horizontal one and the
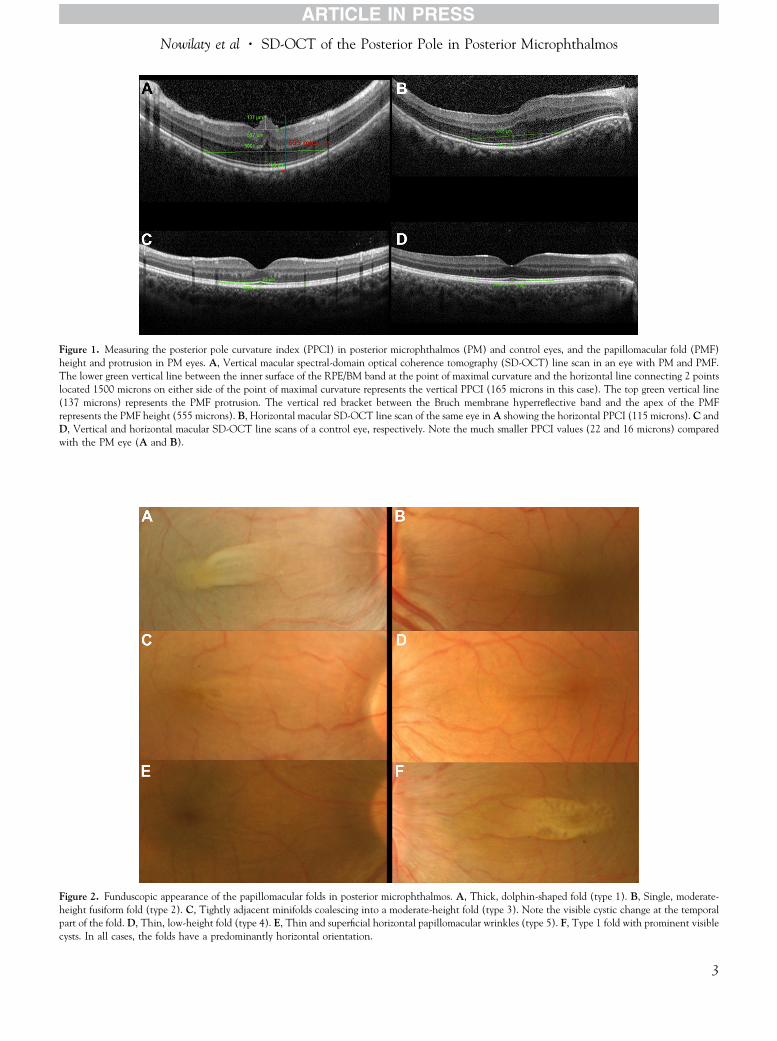
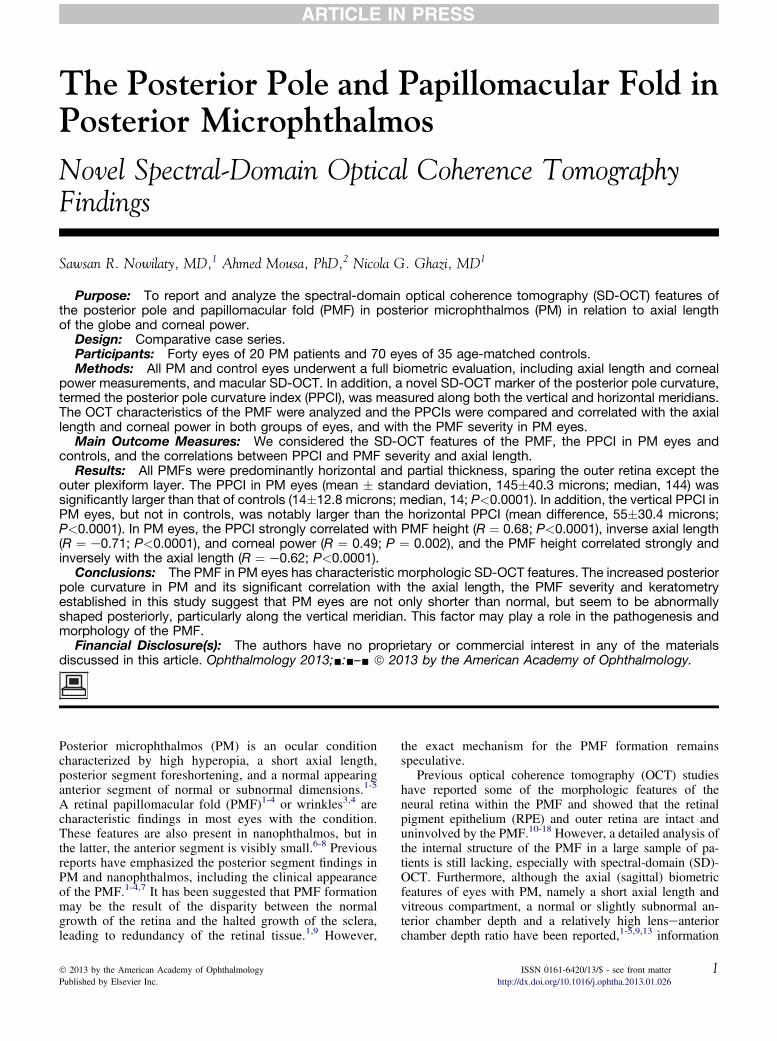
Figure 1. Measuring the posterior pole curvature index (PPCI) in posterior microphthalmos (PM) and control eyes, and the papillomacular fold (PMF)height and protrusion in PM eyes. A, Vertical macular spectral-domain optical coherence tomography (SD-OCT) line scan in an eye with PM and PMF.The lower green vertical line between the inner surface of the RPE/BM band at the point of maximal curvature and the horizontal line connecting 2 pointslocated 1500 microns on either side of the point of maximal curvature represents the vertical PPCI (165 microns in this case). The top green vertical line(137 microns) represents the PMF protrusion. The vertical red bracket between the Bruch membrane hyperreflective band and the apex of the PMFrepresents the PMF height (555 microns). B, Horizontal macular SD-OCT line scan of the same eye in A showing the horizontal PPCI (115 microns). C andD, Vertical and horizontal macular SD-OCT line scans of a control eye, respectively. Note the much smaller PPCI values (22 and 16 microns) comparedwith the PM eye (A and B).
Figure 2. Funduscopic appearance of the papillomacular folds in posterior microphthalmos. A, Thick, dolphin-shaped fold (type 1). B, Single, moderate-height fusiform fold (type 2). C, Tightly adjacent minifolds coalescing into a moderate-height fold (type 3). Note the visible cystic change at the temporalpart of the fold. D, Thin, low-height fold (type 4). E, Thin and superficial horizontal papillomacular wrinkles (type 5). F, Type 1 fold with prominent visiblecysts. In all cases, the folds have a predominantly horizontal orientation.
Nowilaty et al � SD-OCT of the Posterior Pole in Posterior Microphthalmos
3

Table 1. Baseline and Biometric Characteristics of Posterior Microphthalmos Cases Versus Controls (OU Data)
Variable
PM Cases (11 Male, 9 Female) Controls (15 Male, 20 Female)
P valueMean SD Median Range Mean SD Median Range
Age (yrs) 18.4 9.9 19.0 3.5 to 47 21.0 9.8 24.0 3.0 to 36 0.088Refractive error (D) þ15.1 2.3 þ15.5 þ9.1 to þ18.9 0.0 0.9 0.1 -2.3 to þ1.8 <0.0001Average keratometry (D) 48.7 2.3 49.4 41.9 to 52.4 43.0 1.1 43.0 40.5 to 46.3 <0.0001Globe axial length (mm) 16.4 1.2 16.1 15.2 to 19.9 23.4 1.9 23.4 21.5 to 25.0 <0.0001Vertical PPCI (mm) 173 43.1 172 66 to 252 12.9 16.4 14 -35 to 50 <0.0001Horizontal PPCI (mm) 118 43.1 123 10 to 198 14.7 12.1 17 -25 to 37 <0.0001Averaged PPCI (mm) 145 40.3 144 56 to 223 13.8 12.8 14 -26 to 37 <0.0001Verticalehorizontal PPCI (mm) 55 30.4 51 -15 to 122. -1.8 13.2 0.0 -35 to 28 <0.0001Papillomacular fold height (mm) 620 164.4 603 320 to 1022 NA NA NA NA NAPapillomacular fold protrusion (mm) 197 124.5 171 21.0 to 540 NA NA NA NA NA
D ¼ diopters; OU, both eyes; PM ¼ posterior microphthalmos; PPCI ¼ posterior pole curvature index; SD ¼ standard deviation; NA ¼ not applicable.
Ophthalmology Volume -, Number -, Month 2013
3 PPCIs were correlated with axial length and keratometry in bothgroups, and with the PMF height and protrusion in PM eyes. Theseanalyses were performed using data obtained from all eyes of eachgroup (data shown in the Results section). Furthermore, allanalyses were repeated for the right and left eyes’ data separately inan effort to eliminate potential errors owing to the correlationbetween measurements of the right and left eye from the samesubject.
Results
Patient Characteristics and PMF FunduscopicFeatures
We included 20 patients (11 male, 9 female; 40 eyes) with PMrecruited from 11 families (Table 1). All cases had unaffectedparents whose eyes had no or minor refractive error. Nineteenpatients from 10 families were Saudi Arabian and 1 patient wasIndian. Patients’ age ranged from 3.5 to 47 years (mean,18.4�9.9; median, 19), which was not different from that ofcontrols (mean, 21�9.8; median, 24; P ¼ 0.088). Best-correctedSnellen visual acuity ranged from 20/30 to 20/160. Hyperopiaranged from þ9.13 to þ18.88 D (mean, 15.08�2.4; median,15.50). All eyes had normal-appearing anterior segments withgrossly normal dimensions. Horizontal corneal diameters werewithin normal ranges, from 10 to 13.25 mm (mean, 11.4�0.8;median, 11.30). Corneal powers were generally high (range,41.90e52.37 D; mean 48.65�2.3; median, 49.42). Axial lengths ofthe globes ranged from 15.21 to 19.88 mm (mean, 16.37�1.2;median, 16.08).
On fundus examination and photography, all eyes had eithera retinal fold or shallower retinal wrinkles in the papillomaculararea. The fold or wrinkles were predominantly horizontal inorientation. A high degree of symmetry in the shape and height ofthe fold was observed among fellow eyes (36/40 eyes; 90%). Fivetypes of folds were seen. Type 1 is a single, thick, funnel- ordolphin-shaped neurosensory retinal fold noted in 16 eyes of 8patients (Fig 2A, F). It was either horizontal (9/16 eyes) or slantedslightly obliquely and inferiorly toward the fovea (7/16 eyes). Thelatter was identified by an increased yellow/brown color. Type 2 isa single fusiform fold of moderate height, tapering toward thefovea, noted in 7 eyes of 4 patients (Fig 2B). Type 3 presents asseveral tightly adjacent minifolds coalescing into a moderateheight fold seen in 10 eyes of 5 patients (Fig 2C). Type 4 isa thin, low-lying fold observed in 3 eyes of 2 patients (Fig 2D).Lastly, type 5 fold is reduced to thin and delicate horizontalpapillomacular wrinkles with almost no appreciable height, and
4
was noted in 4 eyes of 2 patients who also had the longest axiallengths in this series (Fig 2E).
Visible retinal cysts within the PMF were seen in 10 of 16 eyes(5 patients) with type 1 fold (Fig 2F) and in 4 eyes (2 patients) withtype 3 fold (Fig 2C). In another 6 eyes of 3 patients with type 1fold, no cysts were seen on clinical examination (Fig 2A),although they were detected with SD-OCT (see below).
OCT Features of the PMF
PMF Shape and Height. All patients had an SD-OCTeidentifi-able retinal PMF or wrinkles. Using the vertical OCT cuts, thefolds could be categorized into one of the following 5 configu-rations: an omega-shaped fold (4 eyes) defined as a high, invertedU-shaped fold containing �1 large, centrally located, inner nuclearlayer cyst(s) (Fig 3A); a high, inverted U-shaped fold (8 eyes;Fig 3B); an inverted V-shaped fold (4 eyes; Fig 3C); a low-height, dome-shaped fold (20 eyes; Fig 3D); or only retinalsurface wrinkles (4 eyes; Fig 3E). Crownlike surfacecorrugations at the apex of the formed PMF were detected in 25eyes (Fig 3BeD, F, G). The folds protruded vitread beyond theinner retinal surface to variable degrees. The total height of thePMF ranged from 320 to 1022 microns (mean, 620�164.4;median, 603), whereas the PMF protrusion ranged from 21 to540 microns (mean, 197�124.5; median, 171).
PMF Structure. A foveal depression with appropriate repre-sentation of the retinal layers could only be identified in the 4eyes of the 2 cases where the PMFs were reduced to wrinkles(Fig 4A, available at http://aaojournal.org). These eyes had thelongest axial length in the series (19.18e19.88 mm). In noneof the other 36 eyes could a foveal depression be identifiedand all the retinal layers were represented throughout themacular area (Figs 3AeD, FeH and 4BeF; available at http://aaojournal.org). In all eyes, the PMF, regardless of its height,invariably spared the RPE, photoreceptor outer segments, innersegment/outer segment junction, external limiting membrane,and outer nuclear layer. The inner and outer portions of theouter plexiform layer, however, were consistently includedwithin the structure of the PMF, and the normal stratification ofthe retinal layers was preserved within the PMF and beyond itin all 36 eyes (Figs 1A, 3BeD, FeH, and 4BeF; available athttp://aaojournal.org).
In 25 eyes (62.5%), the apical surface of the PMF was corru-gated and this feature was present independent of the shape orheight of the PMF (Fig 3BeD, F, G). Surface corrugations werepresent in all PMFs that seemed clinically as tight adjacentminifolds (type 3 fold; n ¼ 10 eyes), but also in several PMFswhere corrugations were clinically invisible (in 9 eyes with type
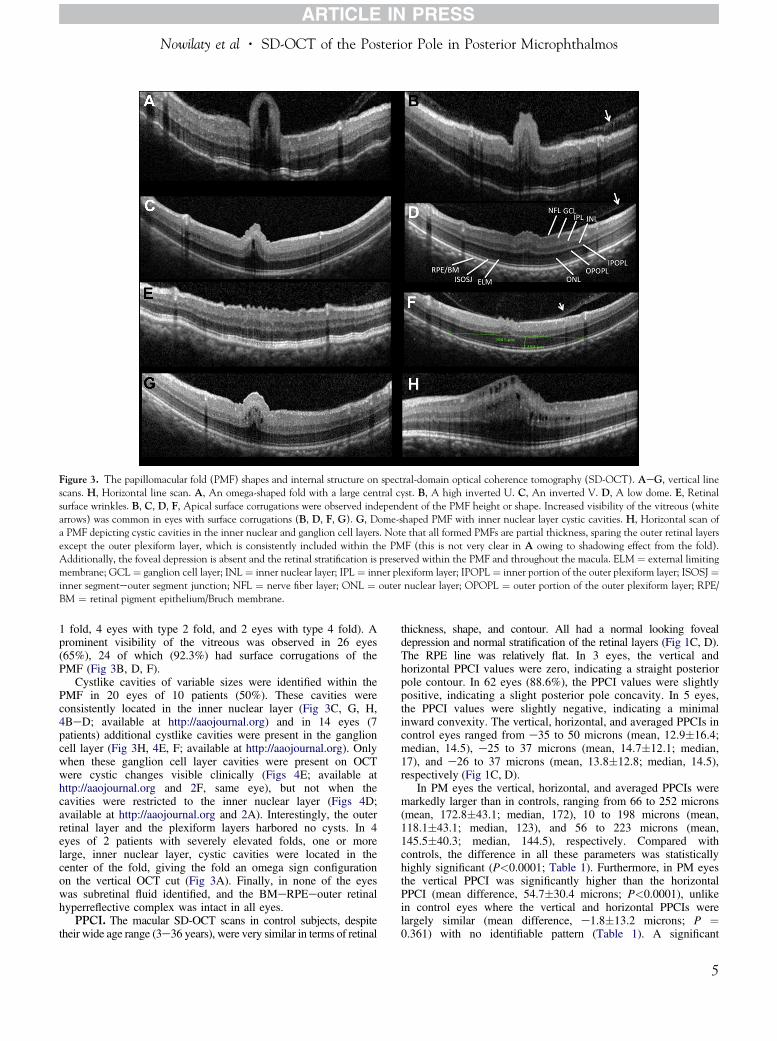
Figure 3. The papillomacular fold (PMF) shapes and internal structure on spectral-domain optical coherence tomography (SD-OCT). AeG, vertical linescans. H, Horizontal line scan. A, An omega-shaped fold with a large central cyst. B, A high inverted U. C, An inverted V. D, A low dome. E, Retinalsurface wrinkles. B, C, D, F, Apical surface corrugations were observed independent of the PMF height or shape. Increased visibility of the vitreous (whitearrows) was common in eyes with surface corrugations (B, D, F, G). G, Dome-shaped PMF with inner nuclear layer cystic cavities. H, Horizontal scan ofa PMF depicting cystic cavities in the inner nuclear and ganglion cell layers. Note that all formed PMFs are partial thickness, sparing the outer retinal layersexcept the outer plexiform layer, which is consistently included within the PMF (this is not very clear in A owing to shadowing effect from the fold).Additionally, the foveal depression is absent and the retinal stratification is preserved within the PMF and throughout the macula. ELM ¼ external limitingmembrane; GCL¼ ganglion cell layer; INL ¼ inner nuclear layer; IPL¼ inner plexiform layer; IPOPL¼ inner portion of the outer plexiform layer; ISOSJ¼inner segmenteouter segment junction; NFL ¼ nerve fiber layer; ONL ¼ outer nuclear layer; OPOPL ¼ outer portion of the outer plexiform layer; RPE/BM ¼ retinal pigment epithelium/Bruch membrane.
Nowilaty et al � SD-OCT of the Posterior Pole in Posterior Microphthalmos
1 fold, 4 eyes with type 2 fold, and 2 eyes with type 4 fold). Aprominent visibility of the vitreous was observed in 26 eyes(65%), 24 of which (92.3%) had surface corrugations of thePMF (Fig 3B, D, F).
Cystlike cavities of variable sizes were identified within thePMF in 20 eyes of 10 patients (50%). These cavities wereconsistently located in the inner nuclear layer (Fig 3C, G, H,4BeD; available at http://aaojournal.org) and in 14 eyes (7patients) additional cystlike cavities were present in the ganglioncell layer (Fig 3H, 4E, F; available at http://aaojournal.org). Onlywhen these ganglion cell layer cavities were present on OCTwere cystic changes visible clinically (Figs 4E; available athttp://aaojournal.org and 2F, same eye), but not when thecavities were restricted to the inner nuclear layer (Figs 4D;available at http://aaojournal.org and 2A). Interestingly, the outerretinal layer and the plexiform layers harbored no cysts. In 4eyes of 2 patients with severely elevated folds, one or morelarge, inner nuclear layer, cystic cavities were located in thecenter of the fold, giving the fold an omega sign configurationon the vertical OCT cut (Fig 3A). Finally, in none of the eyeswas subretinal fluid identified, and the BMeRPEeouter retinalhyperreflective complex was intact in all eyes.
PPCI. The macular SD-OCT scans in control subjects, despitetheir wide age range (3e36 years), were very similar in terms of retinal
thickness, shape, and contour. All had a normal looking fovealdepression and normal stratification of the retinal layers (Fig 1C, D).The RPE line was relatively flat. In 3 eyes, the vertical andhorizontal PPCI values were zero, indicating a straight posteriorpole contour. In 62 eyes (88.6%), the PPCI values were slightlypositive, indicating a slight posterior pole concavity. In 5 eyes,the PPCI values were slightly negative, indicating a minimalinward convexity. The vertical, horizontal, and averaged PPCIs incontrol eyes ranged from e35 to 50 microns (mean, 12.9�16.4;median, 14.5), e25 to 37 microns (mean, 14.7�12.1; median,17), and e26 to 37 microns (mean, 13.8�12.8; median, 14.5),respectively (Fig 1C, D).
In PM eyes the vertical, horizontal, and averaged PPCIs weremarkedly larger than in controls, ranging from 66 to 252 microns(mean, 172.8�43.1; median, 172), 10 to 198 microns (mean,118.1�43.1; median, 123), and 56 to 223 microns (mean,145.5�40.3; median, 144.5), respectively. Compared withcontrols, the difference in all these parameters was statisticallyhighly significant (P<0.0001; Table 1). Furthermore, in PM eyesthe vertical PPCI was significantly higher than the horizontalPPCI (mean difference, 54.7�30.4 microns; P<0.0001), unlikein control eyes where the vertical and horizontal PPCIs werelargely similar (mean difference, e1.8�13.2 microns; P ¼0.361) with no identifiable pattern (Table 1). A significant
5

Ophthalmology Volume -, Number -, Month 2013
correlation between the vertical and horizontal PPCIs in both PMeyes (R ¼ 0.84; P<0.0001) and controls (R ¼ 0.55; P<0.0001)was also seen.
Correlations of PPCI with Axial Length, PMFHeight and Protrusion, and Keratometry
In PM eyes, the axial length exhibited a strong and statisticallysignificant inverse correlation with the vertical, horizontal, andaveraged PPCIs (R ¼ e0.59, e0.73, and e0.71, respectively;P<0.0001 for all parameters; Table 2 and Fig 5A, both available athttp://aaojournal.org). In contrast, in control eyes, only thehorizontal but not the vertical PPCI demonstrated a statisticallysignificant correlation with axial length (R ¼ 0.41 [P<0.0001]and R ¼ 0.15 [P ¼ 0.216], respectively), whereas the averagedPPCI demonstrated a modest but statistically significantcorrelation with axial length (R ¼ 0.29; P ¼ 0.015; Table 2,available online at http://aaojournal.org).
The total PMF height correlated strongly with the vertical PPCI(R¼ 0.71; P<0.0001), horizontal PPCI (R¼ 0.56; P<0.0001), andaveraged PPCI (R ¼ 0.68; P<0.0001; Table 2, Fig 5B, availableonline at http://aaojournal.org). Likewise, the PMF protrusionstrongly correlated with the vertical PPCI (R ¼ 0.62; P<0.0001),horizontal PPCI (R ¼ 0.46; P ¼ 0.003), and averaged PPCI (R ¼0.58; P<0.0001; Table 2, Fig 5C, available online at http://aaojournal.org). Finally, the PMF height and protrusion correlatedstrongly and significantly with the inverse axial length (R ¼e0.62 [P<0.0001] and R ¼ e0.54 [P<0.0001], respectively;Table 2, Fig 5D, E, available online at http://aaojournal.org).
A statistically significant positive correlationwas also seen in PMeyes between the average corneal power and each of the vertical (R¼0.34; P ¼ 0.037), horizontal (R ¼ 0.57; P<0.0001), and averagedPPCI (R ¼ 0.49; P ¼ 0.002; Table 2 and Fig 5F; available online athttp://aaojournal.org). In control eyes, however, the correlationbetween average corneal power and the vertical PPCI (R ¼ 0.29;P ¼ 0.016) or averaged PPCI (R ¼ 0.27; P ¼ 0.025) were onlymodest but statistically significant, whereas the correlationbetween corneal power and horizontal PPCI was both weak andinsignificant (R ¼ 0.18; P ¼ 0.136). In addition, the corneal powerof PM eyes was significantly higher than that of controls, with anaverage of 48.7�2.3 and 43�1.12 D, respectively (P<0.0001).
Statistical analysis of the data from the right and left eyesseparately in both PM eyes and controls did not show notabledifferences compared with the pooled bilateral data analyses. Theresults for the right eye analysis are detailed in Table 2; available athttp://aaojournal.org and summarized as follows: (1) All PPCIsremained significantly larger in PM cases compared with controlsand the vertical PPCI was significantly larger than the horizontalone only in PM eyes; (2) In PM eyes, (a) all PPCIs continued tocorrelate significantly with the axial length, (b) all PPCIs,particularly the vertical PPCI, continued to correlate significantlywith PMF height and protrusion, and (c) the horizontal andaveraged PPCIs maintained a strong correlation withkeratometry; (3) In contrast, among controls, the horizontal, butnot the vertical, PPCI correlated strongly with the axial length,and none of the PPCIs correlated with keratometry.
Discussion
Our study reports novel findings in a large cohort of PM eyes.Based on SD-OCT findings, (1) the height, contour, andinternal structure of the PMF have relevant clinical correla-tions; (2) the neurosensory PMF is invariably partial thickness,sparing the photoreceptor outer segments, inner segment/outer
6
segment junction, external limiting membrane, and outernuclear layer; and (3) the posterior pole curvature is consis-tently and abnormally steep, particularly along its verticalmeridian, and strongly correlates with the macular foldseverity, inverse axial length and average corneal curvature.
The SD-OCT morphologic features of the PMF describedherein are unique. In addition to identifying 5 morphologicconfigurations of the PMF based on SD-OCT characteris-tics, some of the features of the PMF internal structure re-ported here seem to have clinical relevance. For example,the intraretinal cystlike cavities seen within the PMF in 50%of the cases were consistently located in the inner nuclearlayer, but in some cases additional ganglion cell layer cystswere depicted. Only when those ganglion cell layer cavitieswere present on OCT were cystic changes visible clinically,but not when the cavities were restricted to the inner nuclearlayer. Remarkably, these cystic cavities were observed re-gardless of the fold height, thickness, or shape and invari-ably spared all other retinal layers, including the plexiformlayers. This suggests that these cavities are different fromthe cystoid changes seen in diseases such as diabeticmacular edema or inflammatory conditions where a break-down in the blood retinal barrier results in intraretinal fluidaccumulation typically affecting the outer plexiformlayer.21,22 We believe that these cavities represent structuralabnormalities rather than cysts of extravascular fluid accu-mulation. Although fluorescein angiography was notroutinely performed in our patients, none of the eyes thatunderwent fluorescein angiography showed leakage in themacula, as has also been observed by others.3,4,9,10
The absence of a foveal depression in nanophthalmic eyeshas been previously described in time-domain-OCTstudies.23 It was also noted upon reviewing previouslypublished TD-OCT scans of PM cases.10-15 In our series,with the exception of the 4 eyes where the PMF was reducedto superficial wrinkles, none of the eyes with a formed PMFhad an identifiable foveal depression and all the retinal layerswere represented throughout the macular area (Fig 1A, B,3AeD, FeH, and 4BeF; available at http://aaojournal.org).This suggests that the fovea is poorly differentiated in PMeyes and may explain the previous observations that theseeyes rarely attain a visual acuity better than 20/40 despiterefractive correction.1,13,7,8,24,25 This was also the case inour series where only 1 patient had a visual acuity >20/40.The preservation of the retinal stratification noted throughoutthe foveal area in PM eyes is in contradistinction to thesuggestion of Bijlsma et al,23 who reported that the “absentfoveal depression seen on time-domain OCT images wasmore likely caused by crowding of the outer retinal layersfilling up the depression.” The use of SD-OCT permitsa superior visualization of the stratification of the inner retinallayers and a better understanding of the internal structure ofthe PMF than previous TD-OCT studies. The absent fovealdepression in themajority of our casesmay also correspond tothe previously described “absent or rudimentary fovealavascular zone” reported in PM3,4,10 and nanophthalmiceyes.25 Furthermore, the absence of a foveal depression mayat least in part explain the increased yellow/browndiscoloration observed in the folds, particularly the thickfolds seen in our series. The presence of inner retinal layers
Nowilaty et al � SD-OCT of the Posterior Pole in Posterior Microphthalmos
in the area of the expected fovea, where they should not benormally present, may account for the increased macularpigment, a component of which has been previouslylocalized to the inner plexiform layer.26
The novel findings of this study related to the increasedposterior pole curvature in PM and the partial thicknessnature of the PMF might offer new clues into the patho-genesis of the PMF. To our knowledge, there are no reportsof a vertical PMF in eyes with PM, nor has there been anexplanation to the consistent horizontal orientation of thePMF. The consistently steeper vertical posterior polecurvature compared with the horizontal curvature noted inall PM eyes, but not in controls in this study may at leastpartially explain the horizontal or slightly oblique yetpredominantly horizontal orientation of the PMF reportedboth here and in previous studies.1-4,7,9-16 Also, the strongercorrelation between the fold height and/or protrusion and thevertical PPCI compared with the horizontal PPCI furthersupports this hypothesis. Moreover, our study found that incontrol eyes only the horizontal PPCI correlated with axiallength as opposed to PM eyes, where both the vertical andhorizontal PPCIs strongly correlated with the inverse axiallength. This suggests that in PM eyes, not only the hori-zontal posterior pole curvature becomes steeper as the eyebecomes shorter, but also the vertical posterior pole curva-ture becomes even steeper than the horizontal one, as sug-gested by the significant difference between the vertical andhorizontal PPCIs in PM eyes (P<0.0001) unlike in controls(P ¼ 0.361). We hypothesize that, in the spectrum of eyeswith PM and nanophthalmos, the shorter the globe, the morecurved is the posterior pole, particularly along its verticalmeridian, leading to the appearance of a PMF with apredominantly horizontal orientation opposite to the me-ridian of steeper curvature. In addition, because the curva-ture of the posterior pole along its vertical meridianincreases, the PMF becomes more prominent, as suggestedby the strong and statistically significant correlation betweenthe vertical PPCI and fold height and protrusion found inthis study (R ¼ 0.71 and 0.62, respectively; P<0.0001 forboth correlations). Our hypothesis is also supported by thefinding that the 4 eyes in this study that had a PMF reducedto only surface papillomacular wrinkles were eyes witha longer axial length (range, 19.37e19.88 mm; mean,19.63) than the median for the study eyes (16.08 mm) anda much smaller vertical PPCI (range, 66e113 microns;mean, 99; median, 108) than those of the other PM eyes(range, 108e252 microns; mean, 181; median, 176) despitehigher vertical PPCI values than control eyes (range, -35 to50 microns; mean, 12.9; median, 14.5). Thus, these eyesmay represent the lower end of the PM spectrum.
Although this hypothesis may initially suggest that thePMF may represent a mere redundancy in retinal tissuealong the posterior pole vertical meridian in eyes that aregenetically programmed to be much shorter than normalowing to halted scleral growth, as has been previouslysuggested,1,9 our finding that the PMF is invariably partialthickness indicates that there may be more to explainthe PMF formation than just retinal tissue redundancy. Thepartial thickness nature of the PMF with sparing of theinner/outer segment junction on SD-OCT was first noted in
a case of nanophthalmos and bilateral PMFs (Hong A.Bilateral Papillomacular Folds in nanophthalmos: advancedretinal imaging. Invest Ophthalmol Vis Sci 2010;51:E-Abstract 4385). In addition, 2 recent case reports of PMpublished subsequent to our initial submission of thismanuscript to Ophthalmology also described this find-ing.17,18 One may postulate that the outer retina may bespared from folding by virtue of its direct proximity to theRPE pump that keeps it apposed and aligned. Anotherhypothesis may involve the vitreous, whereby vitreoustraction may lead to more folding of the more inner retinallayers versus the outer layers. This is supported by ourfinding of a prominent visibility of the vitreous in 26 eyes(65%), the majority of which (24 eyes; 92%) had surfacecorrugations of the PMF. A third hypothesis may be thatgenetic variables may impact the degree of retinal folding inPM eyes. However, in this study, 17 patients (34 eyes; 85%)had detectable mutations in either PRSS56 or MFRP,whereas the remaining 3 patients (6 eyes; 15%) had nodetectable mutations. Yet, the partial involvement of theretina by the PMF was consistent regardless of the presenceor absence of the mutation as well as the type of mutationdetected, suggesting a low likelihood that genetic factorsalone can explain the partial thickness nature of the PMF.Although it is likely that the etiology of the partial thicknesscharacteristic observed for the PMF may be multifactorial,with involvement of ocular environmental and geneticfactors, further studies are needed to elucidate this finding.
Another interesting finding in this study is that PM eyeshad average corneal curvatures that were significantly higherthan those of controls (48.7 vs 43 D; P<0.0001). Steepcorneas have been reported in isolated cases of PM.1,3-5,9,11,13,15 Furthermore, our group has shown that a stronginverse correlation exists between corneal power and axiallength in PM eyes.20 Interestingly, our current study alsoshows a strong correlation between the PPCIs and inverseaxial length, as well as with the averaged corneal curvaturein eyes with PM, as opposed to controls. This suggests thatPM eyes are not only shorter than normal, but areabnormally shaped both anteriorly with steep corneas, andposteriorly at the macula with a steep posterior polecurvature. Whether the high corneal and posterior polecurvature values represent a developmental compensatorymechanism for the short axial length and high hyperopia orare encoded by the same genetic factors that determine thesize and shape of the eye in PM remains to be determined.
Some of the SD-OCT findings described in this study areunique. The PPCI parameter in particular is novel. Itallowed for the first time to measure quantitatively some ofthe biometric features of the posterior pole in eyes with PM.The marked and robust differences between the PPCI in PMeyes and controls, as well as the absence of wide variationsamong control eyes with mild to no refractive error frompeople of different age groups (3e36 years) also supports itsvalidity as a worthwhile parameter to evaluate in PM eyes,and possibly in eyes with other forms of refractive errors.Although the PM and control groups included a few chil-dren as young as 3 years, it is unlikely that their biometricdata confounded our analyses because most postnatal oculargrowth occurs during the first 2 years of life.5,27,28
7
Ophthalmology Volume -, Number -, Month 2013
Although it can be argued that the PPCI may be affectedby the OCT acquisition protocol and acquisition anglethrough the pupil, or that scaling horizontal distance byOCT maybe affected by axial length or refractive error,also known as magnification effect, the dramatic andconsistent differences observed between the control eyesand PM eyes along both the vertical and horizontalmeridians as well as the robustness and consistency of thefindings in the 2 groups of eyes make the effects of suchpotential confounders less important. Specifically, the dataon the magnification effect on OCT measurements areconflicting29-31 and seem to be small, on the order of 2%.29
The difference in the PPCI measurements between PMand control eyes, however, was much more than whatcould be attributed to magnification effects alone. Also,the consistently higher vertical PPCI compared with thehorizontal PPCI in every PM eye tested cannot beexplained by the magnification effects since the refractiveerror and axial length parameters for a given eye shouldhave affected both PPCI measurements equally. Finally,because the PPCI is a vertical measurement from theRPE surface to the horizontal line, and because verticalmeasurements are not affected by magnification, thisfurther minimizes the impact of magnification on ournovel parameter. Studies comparing the PPCI by OCT tothose obtained with other imaging modalities, such asmagnetic resonance imaging or ultrasonography, may behelpful in further elucidating the posterior pole biometryin such eyes, although such imaging modalities also havetheir inherent limitations, such as reproducibility, motionand acquisition artifacts, and being operator dependent.Studies involving imaging software that can reconstructthe 3-dimensional shape of the posterior pole from OCT-derived variables such as the PPCI may also beworthwhile.
References
1. Boynton JR, Purnell EW. Bilateral microphthalmos withoutmicrocornea associated with unusual papillomacular retinalfolds and high hyperopia. Am J Ophthalmol 1975;79:820–6.
2. Fried M, Meyer-Schwickerath G, Koch A. Excessive hyper-metropia: review and case report documented by echography.Ann Ophthalmol 1982;14:15–9.
3. Spitznas M, Gerke E, Bateman JB. Hereditary posteriormicrophthalmos with papillomacular fold and high hyperopia.Arch Ophthalmol 1983;101:413–7.
4. Khairallah M, Messaoud R, Zaouali S, et al. Posterior segmentchanges associated with posterior microphthalmos. Ophthal-mology 2002;109:569–74.
5. Fledelius HC, Fuchs HJ, Rosenberg T. Oculometric charac-teristics of extreme hypermetropia in two Faroese families.Optom Vis Sci 2004;81:762–8.
6. Khan AO. Posterior microphthalmos versus nanophthalmos[letter]. Ophthalmic Genet 2008;29:189.
7. Serrano JC, Hodgkins PR, Taylor DS, et al. The nano-phthalmic macula. Br J Ophthalmol 1998;82:276–9.
8. Singh OS, Simmons RJ, Brockhurst RJ, Trempe CL. Nano-phthalmos: a perspective on identification and therapy.Ophthalmology 1982;89:1006–12.
8
9. Meire F, Leys M, Boghaert S, de Laey JJ. Posterior micro-phthalmos. Bull Soc Belge Ophthalmol 1989;231:101–6.
10. Kim JW, Boes DA, Kinyoun JL. Optical coherence tomog-raphy of bilateral posterior microphthalmos with papil-lomacular fold and novel features of retinoschisis and dialysis.Am J Ophthalmol 2004;138:480–1.
11. Aras C, Ozdamar A, Ustundag C, Ozkan S. Optical coherencetomographic features of papillomacular fold in posteriormicrophthalmos. Retina 2005;25:665–7.
12. Erdol H, Kola M, Turk A, Akyol N. Ultrasound bio-microscopy and OCT findings in posterior microphthalmos.Eur J Ophthalmol 2008;18:479–82.
13. Slotnick S, Fitzgerald DE, Sherman J, Krumholz DM. Perva-sive ocular anomalies in posterior microphthalmos. Optometry2007;78:71–7.
14. Buyukyildiz HZ, Demirci G, Gulkilik G. Optical coherencetomography in posterior microphthalmos with papillomacularfold and high hyperopia in two siblings. Ann Ophthalmol(Skokie) 2008;40:45–7.
15. Hooyberghs P, Foets B, Casteels I. Two siblings with smalleyes. Bull Soc Belge Ophtalmol 2008309–10. 11e7.
16. Ayala-Ramirez R, Graue-Wiechers F, Robredo V, et al. A newautosomal recessive syndrome consisting of posterior micro-phthalmos, retinitis pigmentosa, foveoschisis, and optic discdrusen is caused by a MFRP gene mutation. Mol Vis [serialonline] 2006;12:1483-9. Available at: http://www.molvis.org/molvis/v12/a168/. Accessed December 23, 2012.
17. Jackson TE, Yang YC, Shun-Shin GA. Spectral domainoptical coherence tomography findings in retinal folds asso-ciated with posterior microphthalmos. J AAPOS 2012;16:389–91.
18. Kumar M, Das T, Kesarwani S. Spectral domain opticalcoherence tomography finding in posterior microphthalmos.Clin Exp Optom 2012;95:651–2.
19. Aldahmesh MA, Nowilaty SR, Alzahrani F, et al. Posteriormicrophthalmos as a genetically heterogeneous condition thatcan be allelic to nanophthalmos [letter]. Arch Ophthalmol2011;129:805–7.
20. Nowilaty SR, Khan AO, Aldahmesh MA, et al. Biometricand molecular characterization of clinically diagnosedposterior microphthalmos. Am J Ophthalmol 2013;155:361–372.
21. Fine BS, Brucker AJ. Macular edema and cystoid macularedema. Am J Ophthalmol 1981;92:466–81.
22. Pelzek C, Lim JI. Diabetic macular edema: review and update.Ophthalmol Clin North Am 2002;15:555–63.
23. Bijlsma WR, van Schooneveld MJ, Van der Lelij A. Opticalcoherence tomography findings for nanophthalmic eyes.Retina 2008;28:1002–7.
24. Cross HE, Yoder F. Familial nanophthalmos. Am J Oph-thalmol 1976;81:300–6.
25. Walsh MK, Goldberg MF. Abnormal foveal avascular zone innanophthalmos. Am J Ophthalmol 2007;143:1067–8.
26. Snodderly DM, Auran JD, Delori FC. The macular pigment.II. Spatial distribution in primate retinas. Invest OphthalmolVis Sci 1984;25:674–85.
27. Larsen JS. The sagittal growth of the eye. IV. Ultrasonicmeasurement of the axial length of the eye from birth topuberty. Acta Ophthalmol (Copenh) 1971;49:873–86.
28. Gordon RA, Donzis PB. Refractive development of the humaneye. Arch Ophthalmol 1985;103:785–9.
29. Sanchez-Cano A, Baraibar B, Pablo LE, Honrubia FM.Magnification characteristics of the Optical CoherenceTomograph STRATUS OCT 3000. Ophthalmic Physiol Opt2008;28:21–8.

Nowilaty et al � SD-OCT of the Posterior Pole in Posterior Microphthalmos
30. Wang XY, Huynh SC, Burlutsky G, et al. Reproducibilityof and effect of magnification on optical coherence tomog-raphy measurements in children. Am J Ophthalmol 2007;143:484–8.
31. Samarawickrama C, Wang XY, Huynh SC, et al. Effects ofrefraction and axial length on childhood optic disk parametersmeasured by optical coherence tomography. Am J Ophthalmol2007;144:459–61.
Footnotes and Financial Disclosures
Originally received: July 6, 2012.Final revision: January 11, 2013.Accepted: January 11, 2013.Available online: ---. Manuscript no. 2012-1013.1 Vitreoretinal Division, King Khaled Eye Specialist Hospital, Riyadh,Saudi Arabia.2 Department of Ophthalmology, King Saud University, Riyadh, SaudiArabia.
Presented at: the Joint Meeting of the American Academy of Ophthal-mology (AAO) and the Asia-Pacific Academy of Ophthalmology (APAO)in Chicago, November 10e14, 2012.
Financial Disclosures:The authors have no proprietary or commercial interest in any of thematerials discussed in this article.
Correspondence:Sawsan R. Nowilaty, MD, Senior Consultant Ophthalmologist, Vitreor-etinal Division, King Khaled Eye Specialist Hospital, PO Box 7191,Riyadh, 11462, Saudi Arabia. E-mail: [email protected].
9
Related Documents