Dr. Abdulkareem Alsuwaida Associate Professor King Saud University Hemodialysis Symposium 08-09 February 2014 Al Madinah AlMunawwarah

The Management of Hypertension In Hemodialysis Patients
Jan 30, 2016
The Management of Hypertension In Hemodialysis Patients. Dr. Abdulkareem Alsuwaida Associate Professor King Saud University. Hemodialysis Symposium 08-09 February 2014 Al Madinah AlMunawwarah. - PowerPoint PPT Presentation
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Dr. Abdulkareem AlsuwaidaAssociate Professor King Saud University
Hemodialysis Symposium08-09 February 2014
Al Madinah AlMunawwarah

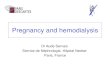
Iseki et al. Ther Apher Dial 2007;11:183-188

SYSTOLIC BLOOD PRESSURE mm HgSYSTOLIC BLOOD PRESSURE mm Hg
stro
ke d
eath
sst
roke
dea
ths
Hea
rt d
eath
sH
eart
dea
ths
StrokeStroke
168168<120<120 125125 135135 148148
22
44
88
1616
3232
HeartHeart
168 168
120120 125125 135135 148148
1616
88
44
22
11

Stidley et al. J Am Soc Nephrol 2006;17:513-520
Unadjusted survival by baseline predialysis systolic BP

“Reverse-epidemiology”Low BP is a consequence of other disease:
Major CVDMalnutrition-inflammation-atherosclerosis
complexLVD

Mechanism of HTNSodium and volume overload.Sympathetic nervous system activityInappropriate renin secretion.Alteration in endothelin and nitric oxide.Erythropoietin therapy.Hyperparathyroidism.Other:
Uremic toxins, Nocturnal hypoxemia and sleep disturbances
Nephrol Dial Transplant. 2004 May; 19(5):1058-68

Mechanism of HTNHypervolemia is the major factorPositive Sodium balance
Increases intake and decreased excretion Achieving DW will control 60% of cases of
HTNAssessment of DW
Am J Kidney Dis. 1996 Aug; 28(2):257-61

Mechanism of HTNRenin inappropriately high for ? etiology.
Increase vascular resistanceIncreased in sympathetic activity
Originate from kidneys Uremic metabolites that activate chemoreceptors
within the kidney Increase vascular resistance and systemic BP

When and How to measure the BP in dialysis patients?Dialysis Unit: During, Before, or AfterHome BPABPM

When and How to measure the BP in dialysis patients?Predialysis SBP overestimated mean SBP by
an average of 10 mm HgPostdialysis SBP underestimated mean SBP
by an average of 7 mm HgBP reasings over a period of 1 to 2 weeks
rather than isolated readings should be used

Alborzi et al. CJASN 2007;2:1228-1234

When and How to measure the BP in dialysis patients?Interdialytic ABP monitoring best represent
BP in dialysis patients.Only method that will show diurnal variation Difficult to repeat, Vascular access
Home BP

Relationship between BP and mortality in dialysis patients
Luther JM Kidn Int 2008;73:667-668

Target blood pressure?Scarcity of evidencePre-dialysis BP < 150/90
ABPM < 140/85 Avoid drop of SBP greater than 30 mm Hg or
post dialysis postural hypotension. Increase mortality and hospitalization
< 110/60 mm Hg correlates significantly with the risk of death within 5 years
Kidney Int 2007;71: 454–61. Kidney Int 2004;66:1212–20. Am J Kidn Dis. 2005;45

ABPM systolic BP and mortality.
Agarwal R Hypertension. 2010;55:762-768

Management of Hypertension Step 1: Lifestyle modifications and control of
volume status with lifestyle modifications.Step 2: Control of volume status with dialysis.Step 3: Administration of antihypertensive
drugs.

Life style modifications Body weight:
'obesity paradox‘ Mainly explained by mal-or undernutrition.
Low salt intake 1000 to 1500 mg of sodium/day
Exercise

Life style modifications Tobacco use
59% more CHF68% more PVDMortality 37%
Foley et al. Kidney Int 2003; 63: 1462-7.

Life style modifications

Management of Hypertension Control of volume status Limit interdialytic weight gain
a 2.5 kg is associated with a significant increase in BP
Achieve dry weightFrequent dialysis & Longer dialysis time
Agarwal R, et al. Hypertension. 2009 Mar; 53(3):500-7.

Dry WeightCriteria to determining DW:No marked fall in BP during dialysis.No hypertension (predialysis BP at the
beginning of the week <140/90 mm Hg).No peripheral edema.No pulmonary congestion on chest X-ray.Cardiothoracic ratio ≤50% (≤53% in
females).

Dry-weight reduction in hypertensive hemodialysis patients (DRIP): a randomized, controlled trial.
Agarwal R, et al. Hypertension. 2009 Mar; 53(3):500-7.

Antihypertensive drugs160/95 mmHg immediate before the next
dialysis session Campese VM TA. Hypertension in dialysis
patients. 2004.
All classes of antihypertensive can be used in dialysis patients (Except diuretics).
Compelling indications are similar

Treatment of Hypertension ARBs and ACE are the preferable first line of
antihypertensive drugsPrevent left ventricular hypertrophy
Cannella G etal.Am J Kidney Dis. 1997 Nov; 30(5):659-64.Suzuki H et al. Am J Kidney Dis. 2008 Sep; 52(3):501-6.

Pharmacokinetic properties of ACE Inhibitors in ESRDT1/2(h)
normal
T1/2(h)
ESRD
Initial dose in
HD
Maintenance dose in HD
Removal during HD
Captopril 2-3 20-30 12.5 q24h 25-50 q24h Yes
Enalapril 11 prolonged 2.5 q24h or q48h
2.5-10 q24h or q48h
Yes
Fosinopril 12 prolonged 10 q24h 10-20 q24h Yes
Lisinopril 13 54 2.5 q24h or q48h
2.5-10 q24h or q48h
Yes
Ramipril 11 prolonged 2.5-5q24h 2.5-10 q24h yes
Henrich W. Principles and Practice of Dialysis

Pharmacokinetic properties of ARB’s in ESRD
T1/2(h)
normal
T1/2(h)
ESRD
Initial dose in HD
Maintenance dose in HD
Removal during HD
Candesartan 9 ? 4 q24h 8-32 q24h No
Irbesartan 11-15 11-15 75-150 q24h 150-300 q24h No
Losartan 2 4 50 q24h 50-100 q24h No
Telmisartan 24 ? 40 q24h 20-80 q24h No
Valsartan 6 ? 80 q24h 80-160 q24h No
Henrich W. Principles and Practice of Dialysis

Pharmacologic properties of β-blockers in chronic dialysis patients
T1/2(h)
normal
T1/2(h)
ESRD
Initial dose in HD
Maintenance dose in HD
Removal during HD
Acebutolol 3.5 3.5 200 q24h 200-300 q24h yes
Atenolol 6-9 <120 25 q48h 25-50 q48h Yes
Carvedilol 4-7 4-7 5 q24h 5 q24h no
Metoprolol 3-4 3-4 50 b.i.d. 50-100 b.i.d. high
Propranolol 2-4 2-4 40 b.i.d. 40-80 b.i.d. yes
Henrich W. Principles and Practice of Dialysis

Hypertension in hemodialysis patients treated with atenolol or lisinopril: a randomized controlled trial. Agarwal R et al NDT 2014
ESRD with LVHlisinopril (n = 100) or atenolol (n = 100) each
administered three times per week after dialysis.
Results:Hospitalizations for heart failure were worse in
the lisinopril group (IRR 3.13, P = 0.021). All-cause hospitalizations were higher in the
lisinopril group [IRR 1.61 (95% CI 1.18-2.19, P = 0.002)].

• Blood pressure remaining above goal in spite of concurrent use of 3 antihypertensive agents of different classes.
Resistant Hypertension

Resistant HTN in ESRD Transdermal clonidine at weekly intervals.Minoxidil, a potent vasodilator,
used with beta blockers
Spironolactone in Hemodialysis Patients 25-50 mg post dialysis Risk of hyperkalemiaImprove EF and Improve BP control Large studies are done

Resistant HypertensionThe use of non steroidal anti-inflammatory
drugsRenovascular hypertensionIncreasing cysts in polysystic kidney diseaseCompliance

Resistant HTN in ESRD Renal sympathetic nerve ablation
Hyperactivation of the sympathetic nervous system
J Clin Hypertens (Greenwich). 2012 Nov;14
The Future?Device-Based Therapy for Resistant
Hypertension Baroreflex Activation Therapy Renal Denervation Therapy

Baroreflex Activation Therapy (BAT)Continuously Modulates the Autonomic Nervous System
HR Vasodilation Natriuresis Renin secretion

Anatomical Location of Renal Sympathetic Nerves
Arise from T10-L1Follow the renal
artery to the kidneyPrimarily lie within
the adventitia
The Journal of Clinical Hypertension. 14, pages 799–801,2012Circulation. 2002;106:1974–1979


Intradialytic hypertension 5-15%Mechanism
Extracellular volume overload Increased cardiac output Changes in sodium levels Activation of the renin–angiotensin–aldosterone
system Overactivity of the sympathetic nervous system Endothelial cell dysfunction. Removal of anti HTN during dialysis

Intradialytic Hypertension The most important treatment is adequate
sodium and water removal and reducing sympathetic hyperactivity.
Changing to non-dialyzable antihypertensive medications
Altering the dialysis prescription.

Summary Sodium excess and extracellular volume
expansion is the major factor in the development of hypertension.
Lifestyle modifications is critical.Control of volume status (Dietary salt and
fluid restriction).Correcting adequately volume expansion with
dialysis.All classes of antihypertensive drugs can be
used in dialysis patients

Thank YouThank You
Related Documents