1 The Effect of Dental Hygiene Regulation on Access to Care Tanya N. Wanchek Weldon Cooper Center for Public Service and Department of Public Health Sciences University of Virginia October 27, 2008 Working Paper Do not cite without author’s permission. Abstract By specializing in preventative oral healthcare, dental hygienists (DHs) have the potential to improve oral health in the United States. DHs decrease the cost and increase the availability of oral healthcare beyond what would be provided by dentists alone. Yet, laws and regulations in many U.S. states prevent DHs from fulfilling their potential. A prior study by Wing et al. (2005) found that states that impose more restrictions on the functions DHs are permitted to perform have lower wages and poorer oral health outcomes. This study adds entry restrictions, including educational and licensure requirements, to the analysis by developing a model in which a state’s entry and practice restrictions jointly affect the DH labor market and access to care. After evaluating anecdotal evidence from four case studies, we estimate the effect of variations in entry and practice restrictions across the U.S. using a three stage least squares (3SLS) estimation method. The results are consistent with the hypotheses that entry restrictions reduce employment rates, practice restrictions increase productivity and wage rates, and wage and employment rates are endogenous to each other and jointly influence access to care. The implication for states seeking to improve oral health is that both entry and practice laws and regulations must be considered jointly in order to significantly improve access to care.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

1
The Effect of Dental Hygiene Regulation on Access to Care
Tanya N. Wanchek
Weldon Cooper Center for Public Service and Department of Public Health Sciences
University of Virginia
October 27, 2008
Working Paper Do not cite without author’s permission.
Abstract By specializing in preventative oral healthcare, dental hygienists (DHs) have the potential to improve oral health in the United States. DHs decrease the cost and increase the availability of oral healthcare beyond what would be provided by dentists alone. Yet, laws and regulations in many U.S. states prevent DHs from fulfilling their potential. A prior study by Wing et al. (2005) found that states that impose more restrictions on the functions DHs are permitted to perform have lower wages and poorer oral health outcomes. This study adds entry restrictions, including educational and licensure requirements, to the analysis by developing a model in which a state’s entry and practice restrictions jointly affect the DH labor market and access to care. After evaluating anecdotal evidence from four case studies, we estimate the effect of variations in entry and practice restrictions across the U.S. using a three stage least squares (3SLS) estimation method. The results are consistent with the hypotheses that entry restrictions reduce employment rates, practice restrictions increase productivity and wage rates, and wage and employment rates are endogenous to each other and jointly influence access to care. The implication for states seeking to improve oral health is that both entry and practice laws and regulations must be considered jointly in order to significantly improve access to care.

2
In the United States, state legislatures and dental boards are typically responsible for promulgating dental hygiene laws and regulations. The laws and regulations create a set of restrictions on both the entry into the dental hygiene profession and the functions that can be performed by licensed dental hygienists (DHs). While scholars have analyzed the effect of entry and practice restriction separately, their simultaneous effect has not been fully explored. Using a basic demand and supply framework, we hypothesize that supply of DHs is a function of entry restrictions, which reduce the number of licensed DHs available. Demand for DHs by dental offices is a function of practice restrictions, which influence the productivity and, consequently, the wage of DHs. Entry and practice restrictions, operating through their affect on wage and employment, jointly influence access to care. This model is consistent with results from four case studies and with broader trends across the U.S. This study has important policy implications. Dental caries, or tooth decay, affect 59 percent of children aged 5 to 17 years, 27 percent of adults aged 35 to 44 years old, and 30 percent of adults 65 years and older in the United States (CDC 2008). Wide disparities exist across the U.S. Adults who had a dental visit in the past year ranged from 58 percent in Oklahoma to 80.5 percent in Connecticut (BRFSS 2006). Even within low-income income groups, Delaware had twice the rate of dentist visits, at 60.7 percent, than Oklahoma, at 30.6 percent (BRFSS 2006). In the U.S., 27 percent of the elderly have lost their teeth, but this ranges from 13 percent in California and Hawaii to 42 percent in Kentucky and West Virginia (Gooch 2003). While caries can be treated relatively easily during a regular dental visit, if left untreated they can result in pain, disability, and even death.1 DHs have the potential to expand the quantity of oral health care providers available and increase the productivity of dental offices. In order to understand how the regulatory environment affects the DH labor market and access to care, we first review relevant studies on dental hygiene and other occupational regulations. We then expand the literature by developing a simple supply and demand model that can predict the changes in wage and DH employment resulting from various changes in entry and practice restrictions. Finally, we test the model using variations that exist across the U.S. We use a three stage least squares (3SLS) estimation method to estimate the effect of restrictions on wages and employment rates. The predicted values from the 3SLS estimation, which capture the portion of employment and wage that is attributable to the regulatory environment, are used as explanatory variables for access to care. The results are presented for access to care among males and females and among different income groups and are compared with results using the actual values of employment and wage. Finally, this article concludes with a discussion of the policy implications for improving access to oral health care. Literature Scholars have long recognized that restrictions on entry into an occupation through licensure requirements may distort the labor market and allow for monopoly rents (Friedman 1962; Benham 1980). The general consensus is that licensing restrictions and lack of reciprocity between states limit in-migration and raise wages in a number of professions (Kleiner 1982; Boulier 1980). Dentistry has received a fair amount of attention within this literature. Among the findings are that licensing exam failure rates among dentists and physicians can restrict entry, causing wages to rise (Benham 1968). Dental fees are estimated to be on average 8.5 to 17.9 percent higher for a variety of procedures in states without reciprocity agreements (Shepard 1978; Kleiner and Kudrle 2000). More restrictive regulation of dentistry has not, however, improved quality of oral health care (Shepard 1978; Kleiner and Kudrle 2000).
1 The seriousness of failure to treat caries is demonstrated by the 2007 death of a 12-year-old Maryland boy from an abscessed tooth cause by decay, which could easily have been diagnosed and treated. (The Washington Post 2/28/07, accessed 714/08.)
3
Dental hygiene entry restrictions have received somewhat less attention in the occupational regulation literature, despite the considerable costs involved with education and licensure requirements. Entry into the DH profession is typically a four-step process. First, the individual must gain admission to an American Dental Association (ADA) accredited dental hygiene education program. In 2006, there were 329 dental hygiene programs in the U.S.2 Competition to enter one of these programs is often intense with many programs receiving more than twice the number of qualified applicants as positions.3 Second, the student must invest in at least two years of DH education.4 Third, graduates must successfully pass two examinations, a written national exam and a state or regional clinical exam.5 Finally, the graduate must obtain a license in the state where he/she wishes to practice. This final licensure requirement means that if a DH wishes to practice in a different state, he/she must obtain a license in the new state. To qualify for licensure by credentials, which allows the DHs to avoid retaking the clinical examination, the majority of states require the applicant to have worked previously for a specific number of years, often between two and five years, and to pay a fee ranging from $35 to $850.6 As of 2007, no state permitted reciprocity, or the automatic recognition of out-of-state licenses. The DH labor shortage in California provides an interesting opportunity to examine one aspect of entry, educational requirements. In 2000, California experienced a period of rapid growth in demand for oral health care. During this period, DH wages rose rapidly. In contrast, the number of dental assistants rose significantly, but their wage did not. Dental assistants are not required to be licensed and generally receive on the job training. They assist patients, but are more limited than DHs in the functions that they can perform. Thus, dental assistances are at least a partial substitute for DHs. Brown et al. (2007) argue that California’s DH educational requirements produced a short-term bottleneck that resulted in a rapid increase in DH wages. Dental assistants had fewer obstacles to entry, allowing the quantity of dental assistants to respond to the increased demand. Their study did not, however, consider an alternative method of entry—licensure by credentials—that could also have helped alleviate shortages by allowing DHs in lower wage states to move to high demand areas. Although there have been few studies of entry restrictions, dental hygiene practice restrictions have received relatively more attention. DH practice restrictions range from allowing DHs to perform only basic teeth cleaning and polishing to conducting more complex or potentially hazardous procedures, such as administering anesthesia and conducting restorative functions. Restrictions also dictate the level of supervision required by dentists, ranging from direct supervision to complete autonomy.7 Direct
2 The requirements to get into DH programs range from requiring a high school diploma (46 percent), some college courses (16 percent), one year of college (27 percent), two years of college (8 percent), to other requirements (3 percent) (ADA, 2003). In addition, some community colleges require that the applicant be a resident of the district in which the school is located. 3 Accurate assessment is difficult because there are no records of the number of students applying to multiple programs. Between 1994 and 1999 applications to DH programs have consistently exceeded 20,000 per year for a system capacity of 5,800 to 6,500 first-year spaces (ADA 2003). All of Virginia’s DH programs received over twice as many qualified applicants as there were spaces available. See Virginia Joint Subcommittee (1997). 4 Alabama, which permits licensure through on the job training, is an exception. 5 To become licensed in most states candidates must pass a written National Board Dental Hygiene Examination (NBDHE) administered by the ADA and a Clinical State or Regional Board Examination. 6 For example, Alabama, Arkansas, Maine, and California each require five years of practice in the state of origin before granting a licensure by credentials. Many states require letters of recommendation and fees ranging from $35 in Pennsylvania to $850 in Oregon. Four states—Kansas, Missouri, New Hampshire, and West Virginia—will accept any of the four regional exams or any state’s individual exam when licensing DHs, while ten states require individuals to take their state-specific exam. ADHA, “National and Regional Exam Boards,” ADHA, http://www.adha.org/careerinfo/exam_boards.htm (accessed 12/4/07). 7 Between 1993 and 2007, states allowing general supervision in most settings increased from 30 to 43; states allowing DHs to administer local anesthesia increased from 16 to 40; and those allowing DHs to provide nitrous

4
supervision requires the dentist to be present in the office, personally diagnose the condition, authorize the procedure, and evaluate the performance of the DH. General supervision requires the dentist to authorize the procedure, but does not require that the dentist be present in the treatment facility. Complete autonomy allows the DH to work without reporting to a dentist.8 Higher practice restrictions reduce the productivity of DHs, resulting in an underutilization of DHs and an increase in dental wages as dentists are needed to perform more services (DeVany 1982). The potentially anti-competitive effect of dental hygiene restrictions came under scrutiny by the Federal Trade Commission (FTC) in the late 1980s. A FTC study estimated that the price effects of states-imposed restrictions on the number of dental auxiliaries that dentists are permitted to employ or the functions DH can perform result in a seven to eleven percent increase in the average price of a dental visit (Liang and Ogur 1987). However, the FTC did not take any broad actions.9 Seeking to draw a link from practice restrictions to access to oral health care, Wing et al. (2005) constructed an index of practice restrictions, the dental hygiene professional practice index (DHPPI), covering all fifty states in 2001. They found that less restrictive regulations are positively correlated with DH salaries and number of dental visits. They did not, however, find a statistically significant relationship between DH regulation and the supply of DHs and dentists. The present study utilizes the DHPPI index to measure practice restrictions. Rather than looking at entry and practice restrictions as independent regulations, this study focuses on how the restrictions interact to influence the DH profession. Because both types of restrictions can influence the DH labor market and access to care, focusing on one restriction at a time runs the risk of biasing results. Rather, policymakers need to better understand the joint effect of their laws and regulations. Entry and Practice Restrictions in the States Most U.S. states promulgate DHs laws and regulations through dental boards composed largely of dentists, but with some consumer and DH representation. Each of these participants has an interest in seeing different types of laws and regulations implemented. Dentists, for example, may benefit from having more restrictive DH practice regulations, which can result in higher dental wages (DeVany 1982). Currently licensed DHs would likely benefit from fewer new DHs entering the profession, which would drive up their equilibrium wage. Consumers benefit from more liberal entry and practice restrictions that expand the availability of services and lower prices. These diverse interests have resulted in a mix of regulations. A casual glance at the correlation in entry and practice regulations reveals little relationship between the types of laws and regulations within a state. Practice restrictions, measured by DHPPI, have less than a .1 correlation with any entry restriction, where 0 is no correlation and 1 is perfect correlation. The highest correlation is between practice years and cost of credentials, with a correlation coefficient of .33. Although the institutional factors going into DH regulation is beyond the scope of this paper, the low correlation suggests that states have a range of interests beyond consumer welfare in mind when creating their regulatory environment.
oxide increased from 9 to 26 states. American Dental Hygiene Association (ADHA), http://www.adha.org/governmental_affairs/index.html (accessed 6/11/07). 8 Colorado is currently the only state that permits DHs complete autonomy. 9 In 2003, the FTC did charge the South Caroline Board of Dentistry of engaging in anticompetitive behavior for requiring children in public health setting must be seen by a dentist before treatment by a dental hygienist. The Board settled in 2007. See http://www.ftc.gov/os/adjpro/d9311/index.shtm (accessed 10/4/08).
5
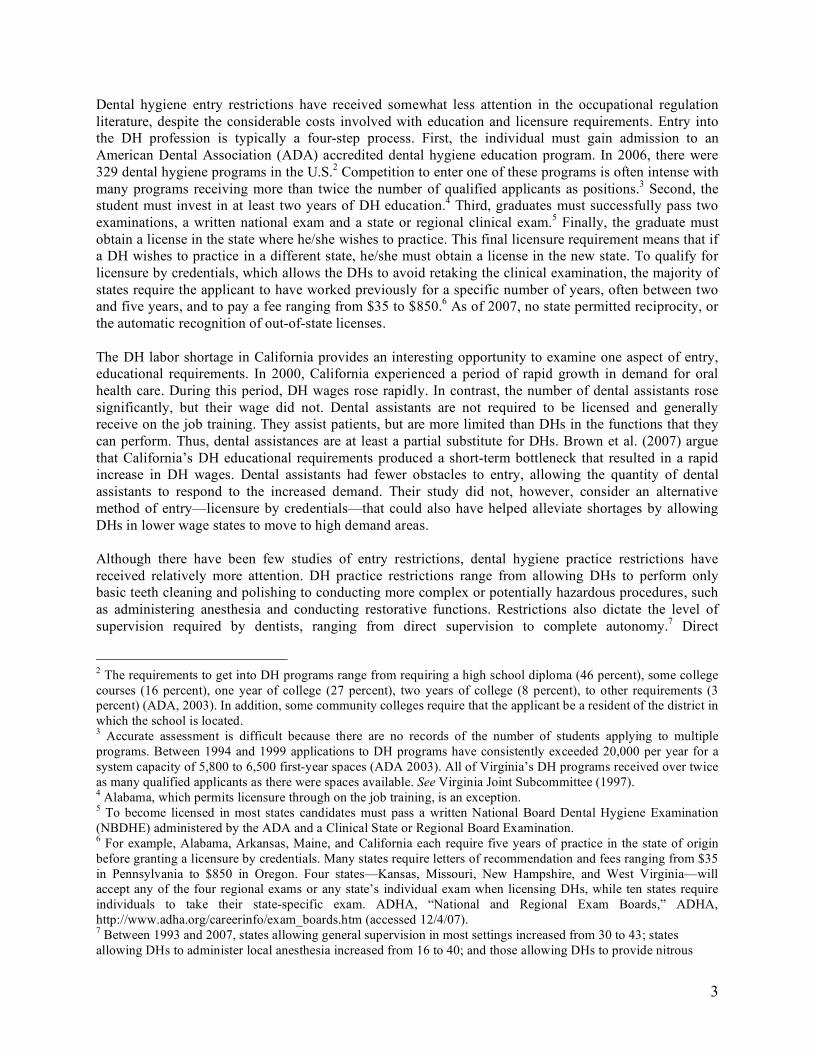
Table 1. Correlation between Entry and Practice Restrictions Practice
years Credentials Average
graduate Exams permitted
DHPPI Cost of credentials
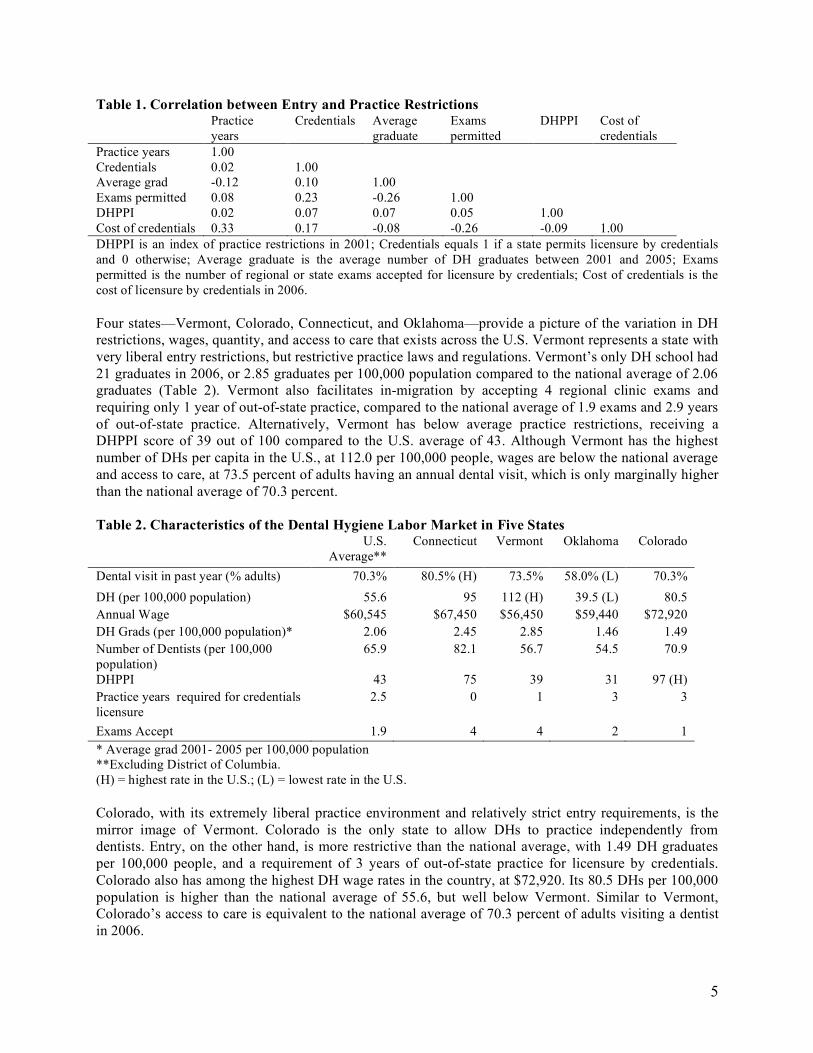
Practice years 1.00 Credentials 0.02 1.00 Average grad -0.12 0.10 1.00 Exams permitted 0.08 0.23 -0.26 1.00 DHPPI 0.02 0.07 0.07 0.05 1.00 Cost of credentials 0.33 0.17 -0.08 -0.26 -0.09 1.00 DHPPI is an index of practice restrictions in 2001; Credentials equals 1 if a state permits licensure by credentials and 0 otherwise; Average graduate is the average number of DH graduates between 2001 and 2005; Exams permitted is the number of regional or state exams accepted for licensure by credentials; Cost of credentials is the cost of licensure by credentials in 2006. Four states—Vermont, Colorado, Connecticut, and Oklahoma—provide a picture of the variation in DH restrictions, wages, quantity, and access to care that exists across the U.S. Vermont represents a state with very liberal entry restrictions, but restrictive practice laws and regulations. Vermont’s only DH school had 21 graduates in 2006, or 2.85 graduates per 100,000 population compared to the national average of 2.06 graduates (Table 2). Vermont also facilitates in-migration by accepting 4 regional clinic exams and requiring only 1 year of out-of-state practice, compared to the national average of 1.9 exams and 2.9 years of out-of-state practice. Alternatively, Vermont has below average practice restrictions, receiving a DHPPI score of 39 out of 100 compared to the U.S. average of 43. Although Vermont has the highest number of DHs per capita in the U.S., at 112.0 per 100,000 people, wages are below the national average and access to care, at 73.5 percent of adults having an annual dental visit, which is only marginally higher than the national average of 70.3 percent. Table 2. Characteristics of the Dental Hygiene Labor Market in Five States
U.S. Average**
Connecticut Vermont Oklahoma Colorado
Dental visit in past year (% adults) 70.3% 80.5% (H) 73.5% 58.0% (L) 70.3% DH (per 100,000 population) 55.6 95 112 (H) 39.5 (L) 80.5 Annual Wage $60,545 $67,450 $56,450 $59,440 $72,920 DH Grads (per 100,000 population)* 2.06 2.45 2.85 1.46 1.49 Number of Dentists (per 100,000 population)
65.9 82.1 56.7 54.5 70.9
DHPPI 43 75 39 31 97 (H) Practice years required for credentials licensure
2.5 0 1 3 3
Exams Accept 1.9 4 4 2 1 * Average grad 2001- 2005 per 100,000 population **Excluding District of Columbia. (H) = highest rate in the U.S.; (L) = lowest rate in the U.S. Colorado, with its extremely liberal practice environment and relatively strict entry requirements, is the mirror image of Vermont. Colorado is the only state to allow DHs to practice independently from dentists. Entry, on the other hand, is more restrictive than the national average, with 1.49 DH graduates per 100,000 people, and a requirement of 3 years of out-of-state practice for licensure by credentials. Colorado also has among the highest DH wage rates in the country, at $72,920. Its 80.5 DHs per 100,000 population is higher than the national average of 55.6, but well below Vermont. Similar to Vermont, Colorado’s access to care is equivalent to the national average of 70.3 percent of adults visiting a dentist in 2006.

6
Alternatively, Connecticut and Oklahoma fall on both ends of the regulatory and access to care spectrum. Connecticut has both liberal entry and practice restrictions and has been rewarded with the highest number of dental visits in the U.S., at 80.5 percent. Connecticut accepts licensure by credential applications from individuals who have taken any region exam and does not require prior practice in another state. Practice restrictions are relatively liberal at 75 on the DHPPI index. Wages, at $67,450, and employment, at 95 DHs per 100,000, are higher than the national average, but well below the highest-ranking states. At the other end of the spectrum, Oklahoma has relatively more restrictions on entry and practice than the average state and has the lowest access to care rate in the country. Oklahoma scored a 31 out of 100 on the DHPPI index and requires three years of experience for licensure by credentials. In 2006, only 58 percent of adults had a dental visit. The combinations of restrictions, wages, employment, and outcomes in Vermont, Colorado, Connecticut, and Oklahoma evidence a pattern. In Vermont and Colorado, the restrictions and wage move in opposite directions, with Colorado having high wages and Vermont having below average wages. Outcomes in both states were close to the U.S. average. Connecticut and Oklahoma represent states that have chosen complimentary restrictions. Connecticut has liberal entry and practice restrictions, high DH employment rates, and good access to care outcomes. Oklahoma chose restrictive laws and regulations and has had low employment rates and poor outcomes. If a state’s policy goal is to improve access to care, then Connecticut’s liberal entry and practice restrictions appear to be a good model. However, a more formal method is needed to analyze the broader patterns throughout the U.S. A Model We develop a simple model to capture the relationship between entry and practice restrictions, wages, employment, and access to care. In this model, supply of DHs is a function of entry restrictions, while demand for DHs is a function of practice restrictions. Access to care depends on the number of DHs, wages, dentists, and dental assistants per capita, income, and density. The basic model can be written as a system of interdependent equations: Supply: DHs = f(entry restrictions, wage)
(-) (+) Demand: Wage = f(practice restrictions, DHs)
(-) (-) Outcome: Access to Care = f(DHs, dentists, dental assistants, wage, income, density)
(+) (+) (+) (+/-) (+) (+) The first two equations represent a basic labor market demand and supply relationship. Entry restrictions shift the supply curve. Higher entry restrictions reduce supply by increasing the cost of entry. The relative scarcity of DHs then drives up wages. Other things equal, higher entry restriction result in higher wages and fewer DHs employed in equilibrium. An example of this situation is California’s DH labor shortage, where a scarcity of DHs drove up wage rates (Brown et al. 2007). Practice restrictions, alternatively, shift the demand curve for DHs. High practice restrictions reduce demand for DHs because dental offices are no longer able to utilize DHs in the most productive ways. Dentists must perform some tasks that would be performed by DHs if practice restrictions were relaxed. In other words, DHs make less of a contribution to the total production of oral health services. Because DHs are paid their marginal productivity in equilibrium, reducing productivity lowers the wage rate. The lower wage, in turn, reduces the number of DHs by discouraging entry. The observable result is lower wages and fewer DHs. A basic supply and demand model facilitates analysis of the case where restrictions vary simultaneously. If both entry and practice restrictions move in the same direction, then the result is an unambiguous
7
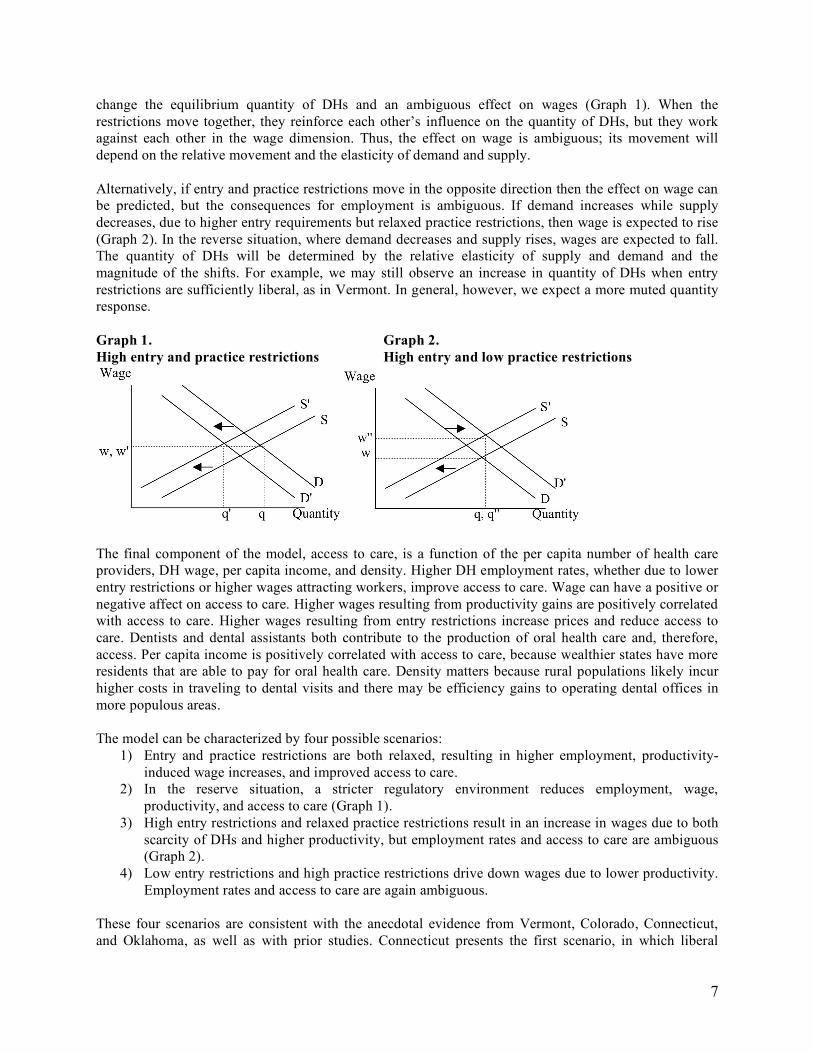
change the equilibrium quantity of DHs and an ambiguous effect on wages (Graph 1). When the restrictions move together, they reinforce each other’s influence on the quantity of DHs, but they work against each other in the wage dimension. Thus, the effect on wage is ambiguous; its movement will depend on the relative movement and the elasticity of demand and supply. Alternatively, if entry and practice restrictions move in the opposite direction then the effect on wage can be predicted, but the consequences for employment is ambiguous. If demand increases while supply decreases, due to higher entry requirements but relaxed practice restrictions, then wage is expected to rise (Graph 2). In the reverse situation, where demand decreases and supply rises, wages are expected to fall. The quantity of DHs will be determined by the relative elasticity of supply and demand and the magnitude of the shifts. For example, we may still observe an increase in quantity of DHs when entry restrictions are sufficiently liberal, as in Vermont. In general, however, we expect a more muted quantity response. Graph 1. Graph 2. High entry and practice restrictions High entry and low practice restrictions
The final component of the model, access to care, is a function of the per capita number of health care providers, DH wage, per capita income, and density. Higher DH employment rates, whether due to lower entry restrictions or higher wages attracting workers, improve access to care. Wage can have a positive or negative affect on access to care. Higher wages resulting from productivity gains are positively correlated with access to care. Higher wages resulting from entry restrictions increase prices and reduce access to care. Dentists and dental assistants both contribute to the production of oral health care and, therefore, access. Per capita income is positively correlated with access to care, because wealthier states have more residents that are able to pay for oral health care. Density matters because rural populations likely incur higher costs in traveling to dental visits and there may be efficiency gains to operating dental offices in more populous areas. The model can be characterized by four possible scenarios:
1) Entry and practice restrictions are both relaxed, resulting in higher employment, productivity-induced wage increases, and improved access to care.
2) In the reserve situation, a stricter regulatory environment reduces employment, wage, productivity, and access to care (Graph 1).
3) High entry restrictions and relaxed practice restrictions result in an increase in wages due to both scarcity of DHs and higher productivity, but employment rates and access to care are ambiguous (Graph 2).
4) Low entry restrictions and high practice restrictions drive down wages due to lower productivity. Employment rates and access to care are again ambiguous.
These four scenarios are consistent with the anecdotal evidence from Vermont, Colorado, Connecticut, and Oklahoma, as well as with prior studies. Connecticut presents the first scenario, in which liberal

8
restrictions resulted in high numbers of DHs and the best outcomes in the U.S. Oklahoma fits under the second scenario and Graph 1, where restrictive laws and regulations have produced low numbers of DHs (q'), average wages (w'), and poor access to care. The third scenario and Graph 2 represent Colorado, which has the most liberal practice restrictions in the country, inducing a high demand for DHs, but relatively strict entry, resulting in low employment rates. The shifts in supply and demand induce high wages (w''), but mediocre outcomes. Vermont represents the fourth scenario, in which an increased supply and decreased demand result in higher quantity, but lower wages and productivity and mediocre outcomes. This model is also consistent with the study by Wing et al. (2005), which found that high practice restrictions were correlated with low wages, but were not correlated with the number of DHs per capita. If strict practice restrictions combined with liberal entry restrictions represent the dominant pattern among states, then the proposed model predicts that demand will decrease while supply increased, as in Vermont. The observable outcome is low wages and an indeterminate number of DHs, which is precisely the effect observed by Wing et al. While anecdotal evidence is consistent with the model, a more systematic comparison is needed to identify the broader trends that exist across the U.S. Empirical Model To analyze the variations in U.S. states, we first employ a three stage least squares (3SLS) estimation technique to find the predicted values of DH employment and wage (Zellner and Theil 1962). The predicted values are then used as explanatory variables in an OLS regression on access to care. The OLS estimates measure how well a state’s predicted wage and employment rates, given their regulatory environment, explain access to care. The estimates are compared to OLS estimates using the actual values of employment and wage. The comparison between predicted and actual values allows us to isolate the marginal contribution of the regulatory environment in explaining access to care. Analysis of the DH labor market is complicated by the fact that wages and employment are endogenous to each other. This two-way causality means that OLS estimates of the structural model of supply and demand will be biased and inconsistent. Therefore, the relationship between wages and employment is modeled as a system of simultaneous equations. The 3SLS estimator accounts for contemporaneous correlation in the error terms across equations, allowing for a consistent covariance matrix across for the error terms of the model (Greene 2000). Consequently, 3SLS is the most efficient estimator of a system of equations in larger samples. One disadvantage of the 3SLS method, however, is if the system is not correctly specified, then the errors are compounded through all the estimates. Heteroscedasticity is also a concern. We test for heteroscedasticity using Pagan-Hall and scatter plot tests; both fail to reject homoscedasticity (see Appendix B). The first stage of the 3SLS estimation method solves for all endogenous variables in the system by rewriting the endogenous variables as a function of the exogenous variables. The fitted values of each endogenous variable from the OLS estimation of the reduced form equations are used as instruments in the structural equations. The second stage involves estimating the structural equations separately using the first stage fitted values. The final stage involves using the covariance matrix as a weighting matrix as well as the instruments derived in the first stage to jointly estimate the equations in the structural model. Using instruments to estimate endogenous variables ensures consistency, while joint estimation ensures asymptotic efficiency (Wacziarg 2001). We estimate the system of equations using a 3SLS procedure with a STATA software package. In predicting employment and wage rates in the 3SLS estimation, we control for the number of dentists and dental assistants. Dentists and dental assistants both influence the use of DHs by potentially providing either complimentary or substitute services. Higher practice restrictions, or a low DHPPI, are negatively correlated with wages. Wages and DH employment are endogenous to each other and, therefore, must be

9
included as an explanatory variable for each other. We separate access to care among males and females to determine if there is a differential effect based on sex. Per capita state income and density are included in all the regressions as control variables. Income captures general differences in wealth among states. Density controls for rural and urban populations, which may influence the ability of individuals to find nearby care providers. To increase the sample size, and therefore the efficiency of the estimator, we pool data from 2002, 2004, and 2006. After estimating the effect of the regulatory environment on wage and employment, the next step is to link them to access to care. The predicted values of wage and employment derived from the 3SLS estimation can be interpreted as the portion of wage and employment that is attributable to the state’s regulatory environment, number of dentists and dental hygienists, income, and density. We use the predicted wage and employment estimates as explanatory variables in an OLS regression on access to care. The 3SLS estimation of the labor market supply and demand is:
!
DHs ="1+ #
11DH Wage + #
12D Employment + #
13DA Employment + #
14DH Grads
!
+"15
Cost Credentials + "16
Credientials + "17
Income + "18
Density + #1
!
Wage ="2
+ #21
DH Employment + #22
DHPPI + #23
Income + #24
density + $2
The OLS estimation of access to care:
!
Dental Visits Male ="3
+ #31
Predicted DH Employment + #32
Predicted Wage
!
+ "33
D Employment + "34
DA Employment + "35
Income + "36
density + #3
!
Dental Visits Female ="4
+ #41
Predicted DH Employment + #42
Predicted Wage
!
+ "43
D Employment + "44
DA Employment + "45
Income + "46
density + #4
To be consistent with the model, we expect entry restrictions, including DH graduates, cost of credentials, and availability of credentials, to be negatively correlated with employment. Practice restrictions, measured by DHPPI, are expect to be negatively correlated with wages. Predicted employment and wage rates are expected to be positively correlated with dental visits. Because wage and employment are endogenous, this estimation method does not allow us to isolate the effects of entry and practice restrictions. This method can, however, identify whether the cumulative regulatory environment affects access to care. Data Description To increase our sample size we pool data from 2002, 2004, and 2006.10 The variables included are:
• ln(DH Employment), ln(D Employment), and ln(DA Employment), which represent the log of the rate of DHs, dentists, and dental assistances per 100,000 population, are obtained from the Bureau of Labor Static (BLS), Department of Labor’s Occupational Employment Statistics Survey and U.S. Census Bureau population estimates.
10 Data is missing for: Dental employment - IL, AK, ND, OR, RI in 2001; AK, ND, OR, UT, VT in 2002; AK, DC, OR, RI, UT in 2003; AK, CO, HI, MN, OR, RI, TN, UT in 2004; AK, OR in 2005; DH employment – MD, UT in 2001; DC, UT in 2002 and 2003; RI in 2007; DA employment - RI in 2004; DH wage – SC in 2004; DHIP – DE in all years; Dental visits – data only available for 2002, 2004, and 2006.

10
• ln(DH Wage) is the log inflation-adjusted state’s average wage rate obtained from (BLS), Department of Labor’s Occupational Employment Statistics Survey and U.S. Census Bureau population estimates.
• ln(DH Grads) is the log of the average number of DH school graduates per 100,000 population between 2001 and 2005. Data was obtained from the U.S. Department of Education, Integrated Postsecondary Education Data System (IPEDS).
• Credentials is a dummy variable equaling 1 if the state permits licensure by credentials and 0 if the state does not permit credentials. ln(Cost Credential) is the log of the inverse of the amount a state charges to obtain a licensure by credentials. We used an inverse of the costs in order to distinguish states that charge low costs, representing liberal entry restrictions, from states that have zero costs because they do not allow licensure by credentials. Information on state licensure by credentials requirements is obtained from the American Dental Hygiene Association, http://www.adha.org/careerinfo/licensure.htm (accessed 10/10/07).
• ln(per cap Income) is the log of each state’s inflation-adjusted per capita personal income, provided by the Bureau of Economic Analysis.
• ln(Density) is the log of the population density per square mile in 2000, estimated by the U.S. Census Bureau.
• DHHPI 2001 represents the index of practice restrictions, provided by Wing et al. (2004). The index incorporates four categories: legal and regulatory environment, supervision in different practice settings, tasks permitted under varying levels of supervision, and reimbursement. A higher score indicates that the state provides a less restrictive practice environment for DHs, with a maximum score of 100. The data covers 2001 laws and regulations.
• ln(visit female) and ln(visit male) are the log of the percent of female and male adults, 18 years and older, who had at least one dental office visit in the past year. The data is from the Centers for Disease Control and Prevention’s Behavioral Risk Factor Surveillance System (BRFSS) survey. The BRFSS survey only included oral health questions in 2002, 2004, and 2006.
• ln(visit $15k or less), ln(visit $15k -$25k), ln(visit $25k -$35k), ln(visit $35k -$50k), and ln(visit $50k+) are the log of the percent of adults visiting a dental office separated into five income categories: individuals earning less than $15,000, from $15,000 to 24,999, from $25,000 to 34,999, from $35,000 to 49,000, and over $50,000. The categories are provided by BRFSS.
Results The results of the 3SLS and OLS estimations are consistent with the model’s predictions. Entry restrictions are negatively correlated with the number of DHs per capita and practice restrictions are negatively correlated with DH wages. Furthermore, the predicted wage and employment rates are positively correlated with access to care. A comparison with OLS regressions using the predicted versus the actual values is consistent with the productivity-induced portion of the wage rate increasing access to care, while total wage rates decreases access to care. The 3SLS estimation addresses two hypotheses of the model. The first hypothesis—entry restrictions reduce the number of DHs employed—is consistent with the results of the pooled regression (Table 3). Entry restrictions reduce the number of DHs per capita. The dummy variable for whether a state permits licensure by credentials is correlated with employment rates at the 1 percent significance level. The cost of credentials, which is the inverse of the ln(Cost Credentials) variable, is also negatively correlated with DH employment per capita at the 1 percent significance level. Average per capita DH graduate significantly predicts DH employment at the 5 percent confidence level. The negative correlation between
11
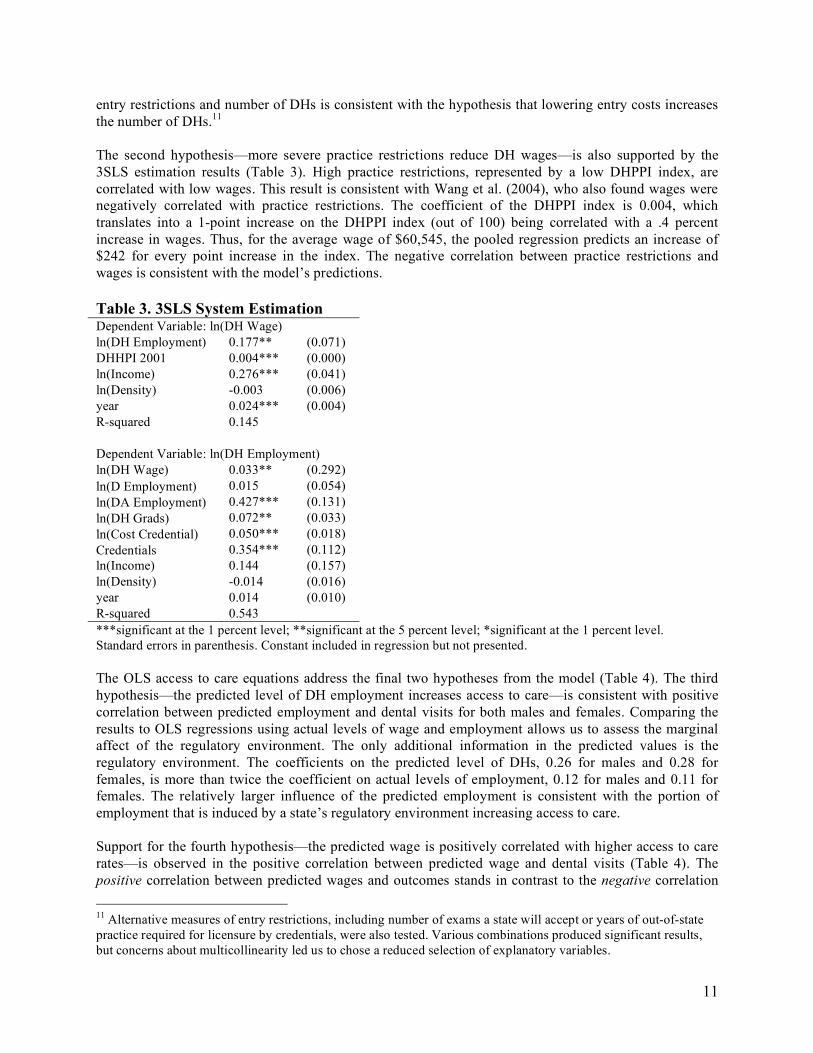
entry restrictions and number of DHs is consistent with the hypothesis that lowering entry costs increases the number of DHs.11 The second hypothesis—more severe practice restrictions reduce DH wages—is also supported by the 3SLS estimation results (Table 3). High practice restrictions, represented by a low DHPPI index, are correlated with low wages. This result is consistent with Wang et al. (2004), who also found wages were negatively correlated with practice restrictions. The coefficient of the DHPPI index is 0.004, which translates into a 1-point increase on the DHPPI index (out of 100) being correlated with a .4 percent increase in wages. Thus, for the average wage of $60,545, the pooled regression predicts an increase of $242 for every point increase in the index. The negative correlation between practice restrictions and wages is consistent with the model’s predictions. Table 3. 3SLS System Estimation Dependent Variable: ln(DH Wage) ln(DH Employment) 0.177** (0.071) DHHPI 2001 0.004*** (0.000) ln(Income) 0.276*** (0.041) ln(Density) -0.003 (0.006) year 0.024*** (0.004) R-squared 0.145 Dependent Variable: ln(DH Employment) ln(DH Wage) 0.033** (0.292) ln(D Employment) 0.015 (0.054) ln(DA Employment) 0.427*** (0.131) ln(DH Grads) 0.072** (0.033) ln(Cost Credential) 0.050*** (0.018) Credentials 0.354*** (0.112) ln(Income) 0.144 (0.157) ln(Density) -0.014 (0.016) year 0.014 (0.010) R-squared 0.543 ***significant at the 1 percent level; **significant at the 5 percent level; *significant at the 1 percent level. Standard errors in parenthesis. Constant included in regression but not presented. The OLS access to care equations address the final two hypotheses from the model (Table 4). The third hypothesis—the predicted level of DH employment increases access to care—is consistent with positive correlation between predicted employment and dental visits for both males and females. Comparing the results to OLS regressions using actual levels of wage and employment allows us to assess the marginal affect of the regulatory environment. The only additional information in the predicted values is the regulatory environment. The coefficients on the predicted level of DHs, 0.26 for males and 0.28 for females, is more than twice the coefficient on actual levels of employment, 0.12 for males and 0.11 for females. The relatively larger influence of the predicted employment is consistent with the portion of employment that is induced by a state’s regulatory environment increasing access to care. Support for the fourth hypothesis—the predicted wage is positively correlated with higher access to care rates—is observed in the positive correlation between predicted wage and dental visits (Table 4). The positive correlation between predicted wages and outcomes stands in contrast to the negative correlation 11 Alternative measures of entry restrictions, including number of exams a state will accept or years of out-of-state practice required for licensure by credentials, were also tested. Various combinations produced significant results, but concerns about multicollinearity led us to chose a reduced selection of explanatory variables.

12
between actual wages and outcomes. The best explanation for the difference in sign is that predicted wage is capturing productivity enhancements created by low practice restrictions, which drive up wages and access to care. Actual wages is capturing the additional influence of other factors, such as scarcity in DHs, which are driving up wages but decreasing access. In competitive markets, DHs will be paid their marginal product; higher productivity results in higher wages and more services. Alternative, when other variables drive up wages, the cost of providing oral health services increases. Some of the higher costs will be passed on to consumers in the form of higher prices, resulting in less access to care. Thus, the contrast between actual and predicted wages provides additional support for the hypothesis. Dentists, dental assistants, and income do not have independent explanatory power in the predicted values regressions, but they are significant when actual wages and employment rate are used. This suggests that predicted wages and employment rates adequately incorporate information about dentists, dental assistants, and income. Density, on the other hand, was not a significant predictor in explaining wages or employment (Table 3), but is significant in the predicted values OLS regressions. While density does not play a role in the DH labor market, but it does influence the rate at which adults visit the dentists. One possibility is that it is more costly to travel to seek oral health care in rural areas. Another explanation is that large western states with low population density have a different attitude toward oral health care. Table 4. Access to Care with Predicted and Actual DH Wage and Employment Predicted values Actual values Dependent Variable: ln(visit male) year -0.007* (0.004) 0.001 (0.003) Predicted DH employment 0.260*** (0.079) Predicted DH wage 0.115** (0.057) ln(DH Employment) 0.116*** (0.014) ln(DH wage) -0.109*** (0.034) ln(D Employment) 0.023 (0.020) 0.044*** (0.016) ln(DA Employment) -0.133 (0.045) 0.140*** (0.026) ln(income) -0.018 (0.038) 0.061** (0.027) ln(density) 0.022*** (0.005) 0.018*** (0.004) R-squared 0.465 0.618 Dependent Variable: ln(visit female) year -0.003*** (0.004) -0.001 (0.003) Predicted DH employment 0.276*** (0.072) Predicted DH wage 0.156*** (0.052) ln(DH Employment) 0.112*** (0.013) ln(DH wage) -0.077** (0.032) ln(D Employment) 0.023 (0.019) 0.045*** (0.016) ln(DA Employment) -0.032 (0.040) 0.128*** (0.025) ln(income) -0.021 (0.035) 0.062** (0.026) ln(density) 0.017*** (0.004) 0.013*** (0.004) R-squared 0.474 0.6125 Number of obs. 135 138 ***significant at the 1 percent level; **significant at the 5 percent level; *significant at the 1 percent level. Standard errors in parenthesis. Constant included in regression but not presented. Income and socio-economic status are thought be primary determinants of access to care in the U.S. In order to better understand access to care among different income groups, we repeat the pooled regression using five income groups (Table 5). Both the predicted and the actual number of DHs working in a state significantly influences the likelihood of visiting the dentist’s office for all income groups, although only at the 10 percent significance level for individuals with income between $25,000 and $35,000. Because

13
the regression is in log-linear form, the results can be interpreted as supply elasticities. The largest effect of DHs on access to care is among the lowest income groups, where the coefficient of 0.51 indicates that a 1 percent increase in per capita DH employment would result in a .51 percent increase in dental visits. The lowest income group likely relies more on lower-cost DHs and dental assistants dentists. This explanation is consistent with the lack of correlation between dentists and access to care in the OLS regression with actual wages and employment rates. Like in the previous access to care regressions, actual and predicted wage have different signs. Actual DH wage is negatively correlated with access to care and is significant for all but the poorest individuals. Alternatively, the predicted wage is positive, but it is only significant among the highest and the lowest income groups. Thus, the evidence is consistent with practice restrictions continuing to influence productivity, which increases wage, but here the effect is only felt by some income groups. Also like the previous regressions, dentists and dental assistants are not significant when the predicted levels of DH wage and employment are included. On exception is that, among the wealthiest income group, dental assistants are negatively correlated with access to care. One explanation is that states experiencing a shortage of DHs, as Brown et al. (2007) found in California, are substituting for dental assistants, which are not as efficient as DHs at producing services. However, it is not clear why this would only affect the wealthiest income group. In sum, the positive correlation between the predicted levels of DHs, wage and access to care establish a link from the regulatory environment to access to care, operating through the DH labor market. Lower entry and practice restrictions increase employment and wages. The portion of employment and wages that is attributable to the regulatory environment is positively correlated with access to care. Although this model cannot isolate the effect of either type of restriction, the significance of the joint effect on access sends a clear message: states can improve access to care by simultaneously lowering entry and practice restrictions.

14
Table 5. Access to Care by Income Group Predicted values Actual values Dependent Variable: ln(visit $15k or less) Predicted DH employment 0.513*** (0.156) Predicted DH wage 0.226*** (0.115) ln(DH Employment) 0.144*** (0.033) ln(DH wage) -0.165 (0.078) ln(D Employment) 0.014 (0.040) 0.055 (0.038) ln(DA Employment) -0.063 (0.090) 0.243*** (0.061) R-squared 0.424 0.443 Dependent Variable: ln(visit $15k -$25k) Predicted DH employment 0.311** (0.124) Predicted DH wage -0.049 (0.091) ln(DH Employment) 0.096*** (0.025) ln(DH wage) -0.242*** (0.062) ln(D Employment) 0.042 (0.031) 0.081*** (0.029) ln(DA Employment) -0.005 (0.072) 0.212*** (0.047) R-squared 0.309 0.378 Dependent Variable: ln(visit $25k -$35k) Predicted DH employment 0.152* (0.084) Predicted DH wage 0.046 (0.061) ln(DH Employment) 0.083*** (0.015) ln(DH wage) -0.194*** (0.036) ln(D Employment) 0.026 (0.021) 0.038** (0.018) ln(DA Employment) 0.006 (0.049) 0.137*** (0.028) R-squared 0.324 0.502 Dependent Variable: ln(visit $35k -$50k) Predicted DH employment 0.211*** (0.076) Predicted DH wage 0.090 (0.056) ln(DH Employment) 0.095*** (0.014) ln(DH wage) -0.147*** (0.033) ln(D Employment) 0.014 (0.020) 0.037** (0.016) ln(DA Employment) -0.050 (0.044) 0.101*** (0.026) R-squared 0.241 0.436 Dependent Variable: ln(visit $50k+) Predicted DH employment 0.153*** (0.032) Predicted DH wage 0.087** (0.048) ln(DH Employment) 0.071*** (0.009) ln(DH wage) -0.074*** (0.021) ln(D Employment) 0.007 (0.012) 0.019* (0.010) ln(DA Employment) -0.063** (0.028) 0.035** (0.016) R-squared 0.330 0.478 Standard errors in parenthesis. ***significant at the 1 percent level; **significant at the 5 percent level; *significant at the 1 percent level. Constant, income, and dummy variables for year and density were included in regression, but omitted from the table. The first two equations in the system, DH Employment and DH Wage, were also included in the estimates, but are omitted from the table.

15
Summary This study highlights the need to account for both DH entry and practice restrictions when analyzing the DH labor market and its effect on access to care. We develop a model that incorporates a basic labor market supply and demand framework. In this model, entry restrictions are a function of employment, practice restrictions are a function of wages, and DH employment and wages are functions of access to care. Four predictions from the model are: entry restrictions reduce the number of DHs employed, practice restrictions lower DH wages, the portions of the employment rate and wage that are explained by the regulatory environment are positively correlated with access to care. The model’s predictions are consistent with patterns observed throughout the U.S. Using a 3SLS estimation method, we find that entry requirements are negatively correlated with DH employment and practice restrictions are negatively correlated with wages. The predicted values from the 3SLS estimates are then used as explanatory variables in an OLS regression on access to care. The predicted values isolate the portion of wages and employment that is explained by the regulatory environment and other state characteristics. The OLS results reveal that predicted DH employment rate is positively correlated with the percent of adults who visited the dentist. Predicted employment had a larger effect on access than actual employment, suggesting that the regulatory environment in particular is influencing access to care. Predicted wage is positively correlation with access to care while actual wage is negatively correlated with access. This contrast suggests that the predicted value is capturing productivity enhancements resulting from lower practice restrictions. These results are consistent with a state’s regulatory environment influencing employment rates and productivity, which in turn increase access to care. This analysis has important policy implications. High caries rates and low dental visitation rates have prompted public health officials across the U.S. to proclaim a need to take action to improve oral health. This study suggests that a state’s regulatory environment can have a large effect on the rate at which adults visit dentists. First, state can expand the number of DHs working in a state both by providing more educational opportunities and by facilitating in-migration of DHs from other states. Second, states can increase the services available by expanding the functions DHs are permitted to perform and reducing the required dental oversight. Lowering restrictions has the effect of increasing DHs’ productivity, leading to higher wages for DHs without increasing the price of services for consumers. Finally, the fact that both wages and employment are significant explanatory variables for each other, suggests that entry and practice restrictions cannot be analyzed in isolation. The restrictions jointly determine wages and employment and, consequently, access to care. Therefore, the optimal way to increase access is to lower both entry and practice restrictions. States that focus on just one type of restriction run the risk of driving up wages or lowering productivity, without improving the oral health the population.

16
American Dental Association (ADA) (2003). Dental Education, Licensure and Regulation of
Dental Professionals. Centers for Disease Control and Prevention (CDC) (2008). Preventing Dental Caries, Preventing
Chronic Diseases: Investing Wisely in Health. U.S. Department of Health and Human Services.
Benham, Lee (1980). The Demand for Occupational Licensure. in Rottenberg, S. (ed.), Occupational Licensure and Regulation. American Enterprise Institute for Public Policy Research, Washington D.C.
Benham, L., A. Maurizi, M.W. Reder (1968). Migration, Location and Renumeration of Medical Personell: Physicians and Dentists, The Review of Economics and Statistics 50: 332-347.
Boulier, Bryan L. (1980). An Empirical Examination of the Influence of Licensure and Licensure Reform on the Geographic Distribution of Dentists. in Rottenberg, S. (ed.), Occupational Licensure and Regulation. American Enterprise Institute for Public Policy Research, Washington, D.C.
DeVany, Arthur S., Wendy L. Gramm, Thomas R. Saving, Charles W. Smithson (1982). The Impact of Input Regulation: The Case of the U.S. Dental Industry, J.L. & Econ. 367: 367-382.
Friedman, Milton (1962). Capitalism and Freedom. University of Chicago Press, Chicago. Gooch, B.F., P.F. Eke, and D.M. Malvitz (2003). Public Health and Aging: Retention of Natural
Teeth Among Older Adults --- United States, 2002, Morbidity and Mortality Weekly Report Centers for Disease Control and Prevention, Atlanta, GA.
Greene, William H. (2000). Econometric Analysis. Prentice-Hall, Englewood Cliffs, N.J. Kleiner, Morris, Robert Gay, and Karen Greene (1982). Barriers to Labor Migration: The Case
of Occupational Licensing, Industrial Relations 21: 383-393. Kleiner, Morris and Robert T. Kudrle (2000). Does Regulation Affect Economic Outcomes? The
Case of Dentistry, Journal of Law and Economics 43: 547-582. Liang, J.N. and Ogur, J.D. (1987). Restrictions on Dental Auxiliaries: An Economic Policy
Analysis, Bureau of Economic Staff Report Federal Trade Commission, Washington, D.C.
Ozbay, K., D. Ozmen, and J. Berechman, (2006). Modeling and analysis of the link between accessibility and employment growth, Journal of Transportation Engineering-Asce 132: 385-393.
Shepard, Lawrence (1978). Licensing Restrictions and the Cost of Dental Care, Journal of Law and Economics 21: 187-201.
Virginia Joint Subcommittee (1997). Availability of Dental Hygienists, House Document. Virginia House of Representatives.
Wacziarg, Roman T. (2001). Measuring the Dynamic Gains from Trade World Bank Econ. Review 15: 393-429.
Wing, Paul, Margaret H.Langelier, Tracey A. Continelli, and Ann Battrell (2005). A Dental Hygiene Professional Practice Index (DHPPI) and Access to Oral Health Status and Service Use in the United States, Journal of Dental Hygiene 79: 10-10.
Zellner, A. and Theil, H. (1962). Three-Stage Least Squares: Simultaneous Estimation of Simultaneous Equations, Econometrica 30: 54-78.

17
Table A. Summary of Variables Used in Analysis Number of
observations Mean value Standard
Deviation Minimum value
Maximum value
Wage 51 $60,546 $9,248 $38,580 $82,780 DH per capita 51 65.9 18.4 32.7 112 Dentists per capita 51 63.4 16.5 42.1 131.4 DH Grad per capita
51 0.25 0.12 0.05 0.72
Personal Income 51 $33,670 $5,521 $24,664 $52,811 DHPPI (PR) 51 43.6 20.4 10.0 97.0 Cost credentials 2006
51 $271.68 $356.86 $0 $2000
Exam (ER) 51 1.88 1.62 0.0 5.0 Credentials (ER) 51 0.9 0.3 0.0 1.0 Practice yrs (ER) 48 2.9 0.98 1.0 4.0 Visits 51 69.9 5.3 58.0 80.5 Visits less than HS 49 47.0 6.9 32.6 60.5 Visits HS 51 64.0 5.2 52.2 77.1 Visits HS plus 51 71.6 4.7 61.1 80.6 Visits BA 51 81.5 3.4 73.3 87.8 Visits 65 51 66.0 7.1 46.4 78.2 Appendix B. Heteroscedascitiy To address the potential that heteroscedasticity could bias the results, we test whether the residuals were randomly dispersed throughout the range of estimated dependent variables. We first estimate the Pagan-Hall test statistic for the predicted values from the first stage, instrumental variables estimates. The Pagan-Hall test statistic has a Chi-Squared(8) distribution and the null hypothesis is that the disturbances are homoscedastic. The Pagan-Hall test statistic for employment is 13.908, with a 0.130 p-value, and for wage is 9.466, with a 0.305 p-value, which fails to reject homoscedasticity for both wage and employment. The results suggest that at least in the first stage of the estimation, heteroscedasticity is not a major concern. Because the instrumental variables regressions do not capture the full 3SLS estimates, we also looked at the 3SLS estimator residuals plotted against the predicted dependent variables (Graphs 3 and 4). The scatter plots do not reveal a funnel-shaped patterns, as would be present under heteroscedasticity (Ozbay et al. 2006). Graph 3. Wage Residuals Graph 4. Employment Residuals
Related Documents