Teat Surgery Adarsh Kumar

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Teat Surgery
Adarsh Kumar
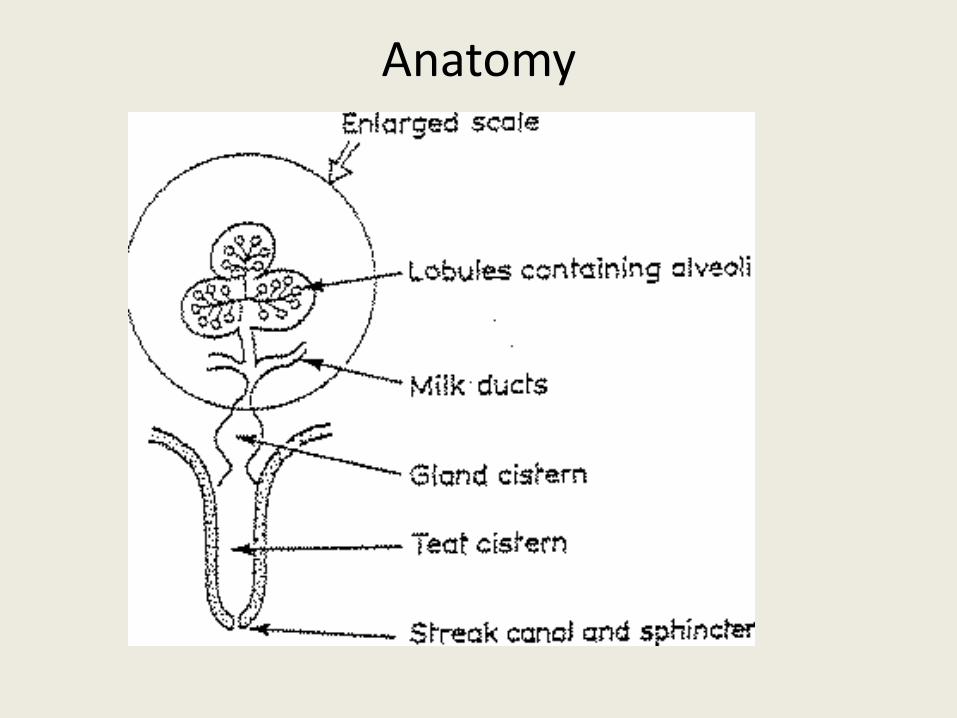
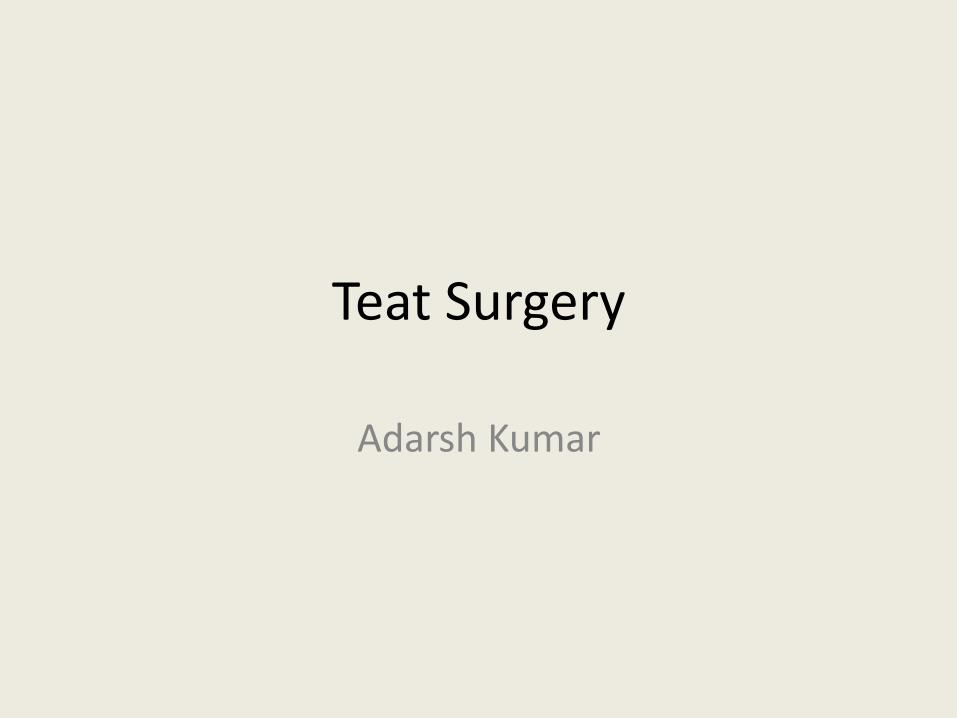
Anatomy

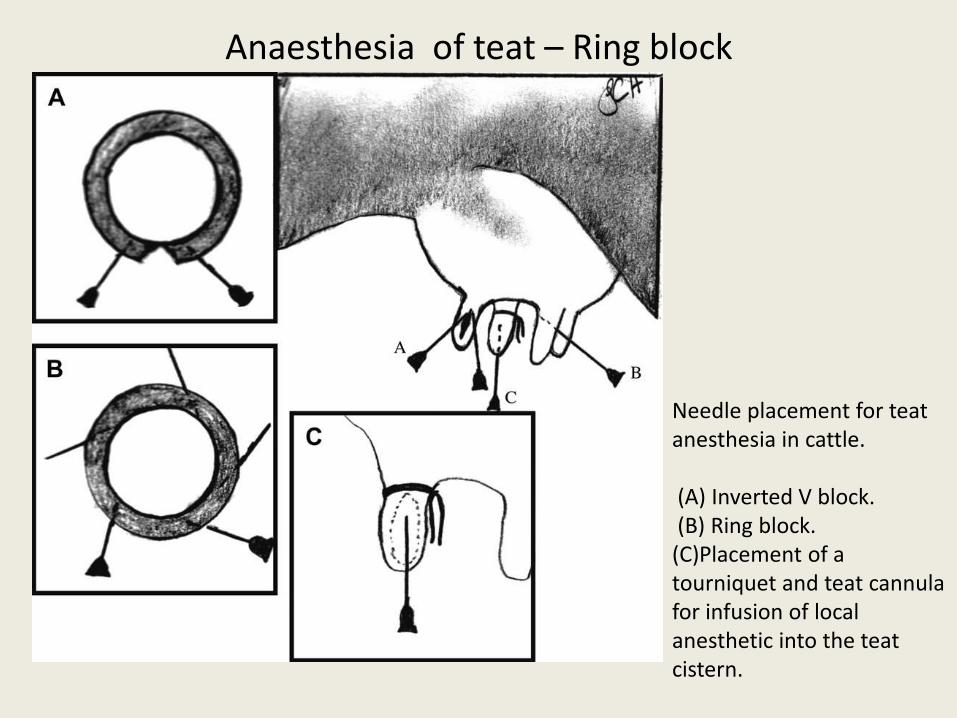
Anaesthesia of teat – Ring block
Needle placement for teat anesthesia in cattle.
(A) Inverted V block.(B) Ring block.
(C)Placement of a tourniquet and teat cannulafor infusion of local anesthetic into the teat cistern.
•Use plain Lignocainewithout adrenaline
Teat Lacerations
• Teat lacerations are categorized as
• Acute
• Chronic (more than 12 hours old).
• Surgical intervention on the teat is best performed during the first 12 hours following the injury.
• Teat lacerations are classified as simple or complex (inverted “Y” or “U”),
• Longitudinal or transverse, and proximal or distal.
• The orientation of the blood supply of the teat is longitudinal.
• A transverse laceration results in more damage to the blood supply resulting in more edema, avascular necrosis and dehiscence post-operatively compared with a longitudinal laceration.
• The more circumference is involved, the worse is the prognosis.
• Distal injuries involving the streak canal are also regarded as having a poor prognosis.
• Proximal and transverse lacerations are difficult to repair. At this location, the mucosa is difficult, the suture and the teat swell more post-operatively.
• Teat lacerations are classified as being partial thickness (skin to submucosa)
• Full thickness (skin to mucosa with milk leaking out of the incision).
• recommended to
• apply cold hydrotherapy on the injured teat while waiting for the veterinarian.
• The hydrotherapy helps decrease the inflammation and helps clean the teat for surgery.
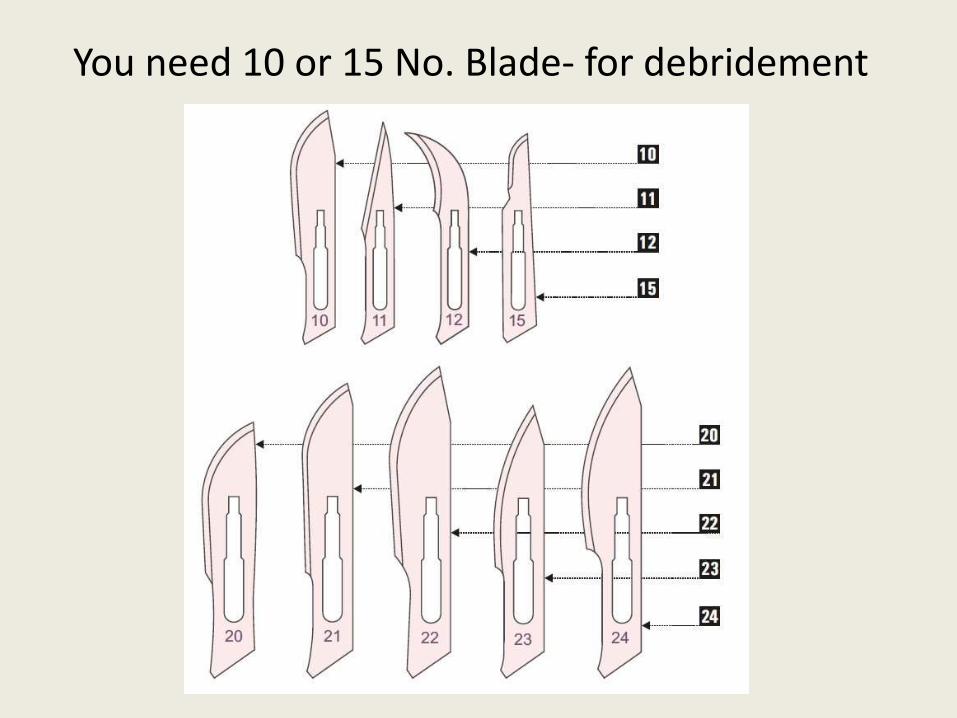
You need 10 or 15 No. Blade- for debridement
Laceration repair
• Mucosa and the submucosa are first reconstructed using a simple continuous pattern.
• The muscular and subcutaneous layers are closed with a simple continuous pattern
• The skin is carefully apposed using a simple interrupted.
• Care is taken to leave the skin sutures slightly loose because swelling is expected at the surgery site.
• Throughout the procedure, the surgery site is frequently lavaged with saline.
• Antibiotics can be added to the lavage solution.
• Hemostasis is performed to avoid formation of mural hematoma that may obstruct the teat cistern.
Post operative
• self-retaining plastic teat canula with a cap into the streak canal
• Antibiotic umbrella.• Severe post-operative edema can be treated by
applying ice around the teat for a few days.• Crushed ice in a rectal sleeve can be placed around the
teat. Daily Twenty minute application.• The skin sutures are removed no more then 9 days
after the surgery.• If the sutures are left in place longer, excessive
fibrosis and suture tract infection may occur.




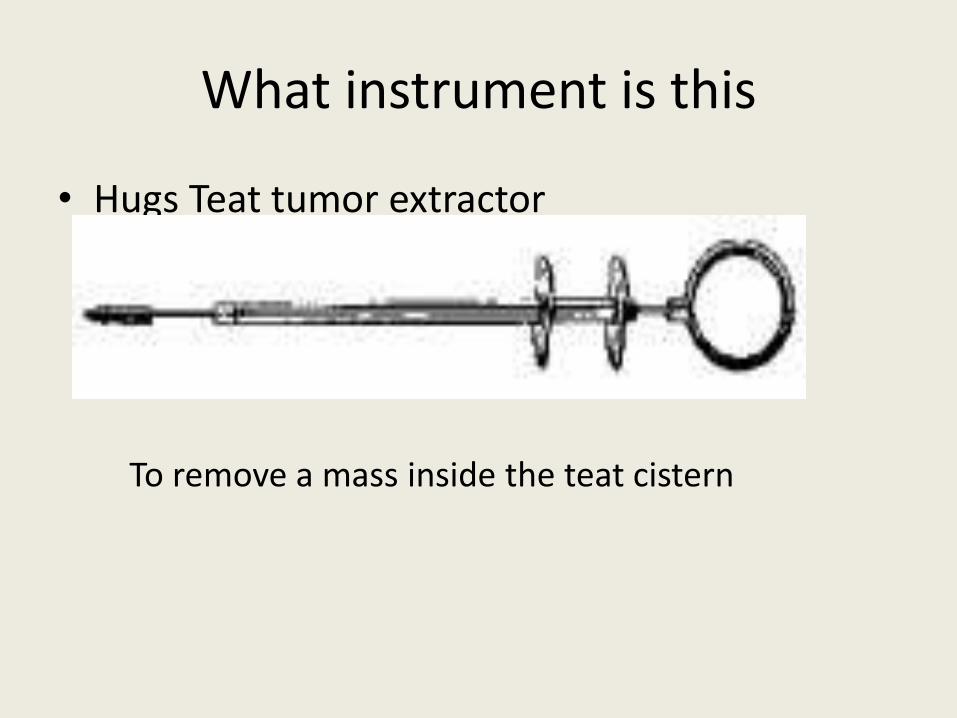
What instrument is this
• Hugs Teat tumor extractor
To remove a mass inside the teat cistern
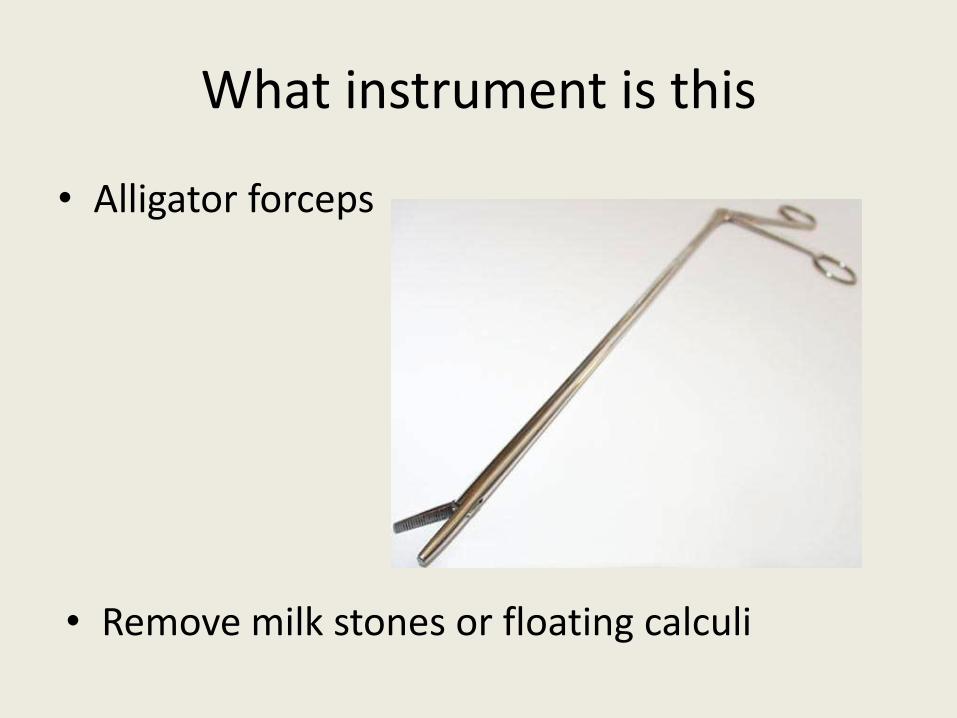
What instrument is this
• Alligator forceps
• Remove milk stones or floating calculi
What instrument is this
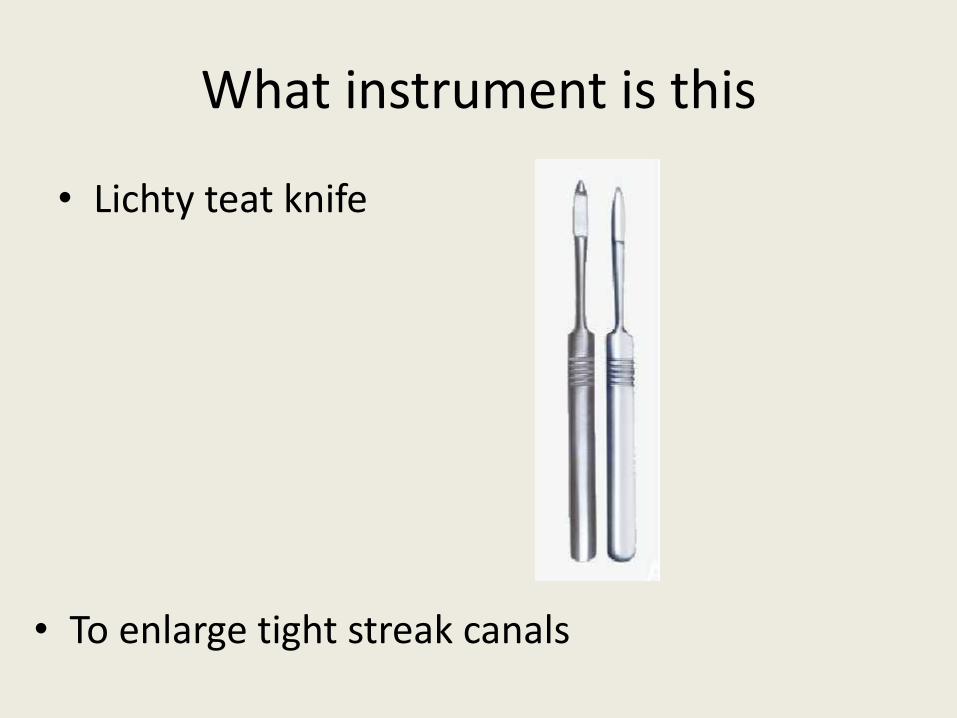
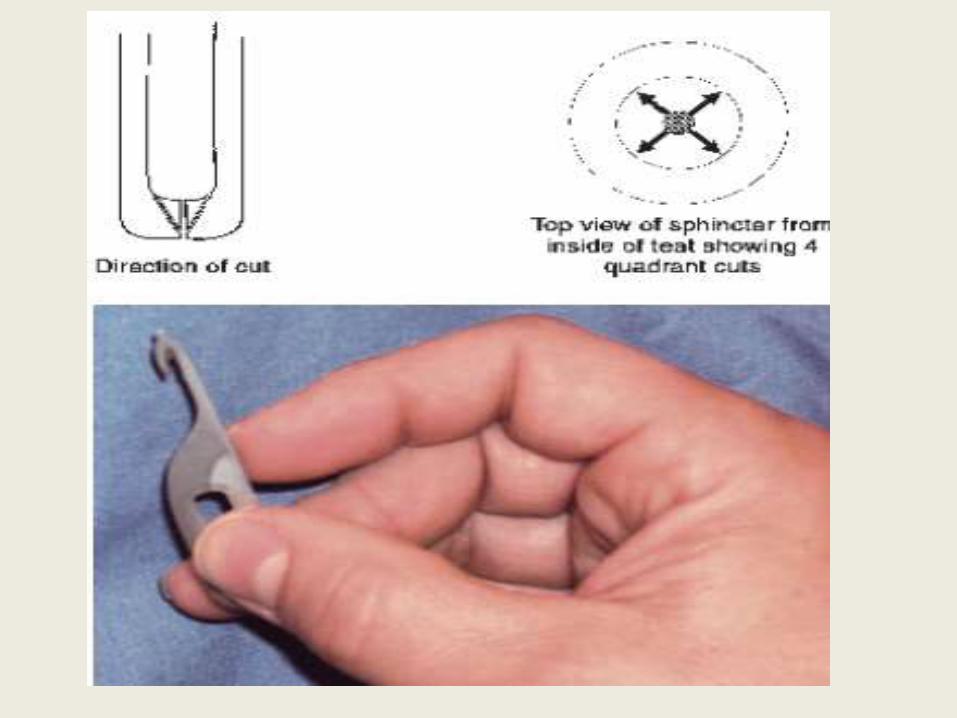
• Lichty teat knife
• To enlarge tight streak canals
What instrument is this
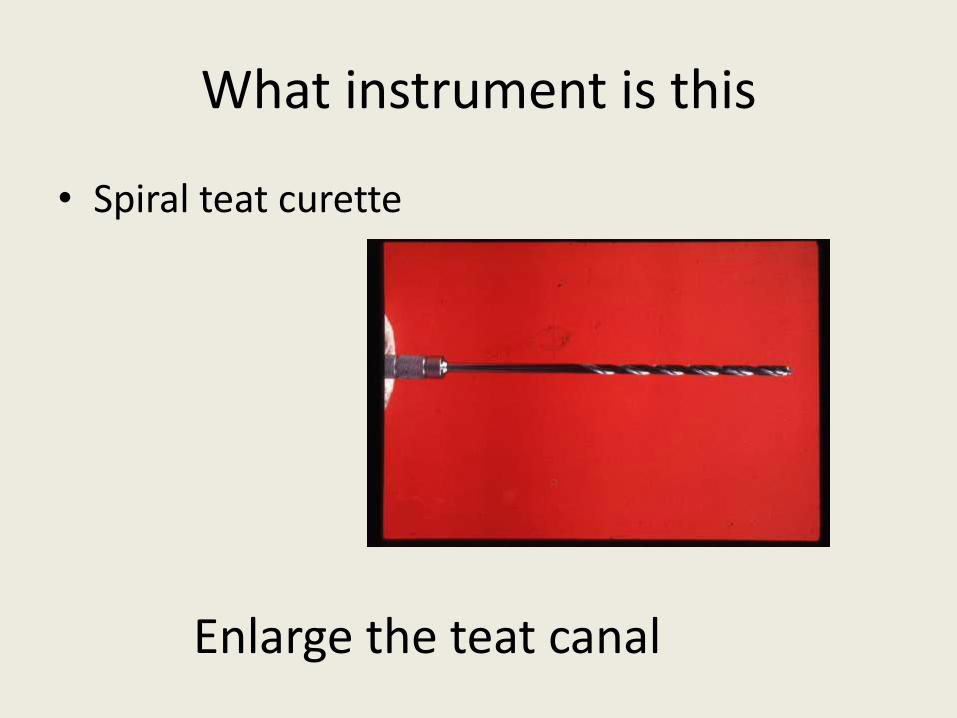
• Spiral teat curette
Enlarge the teat canal
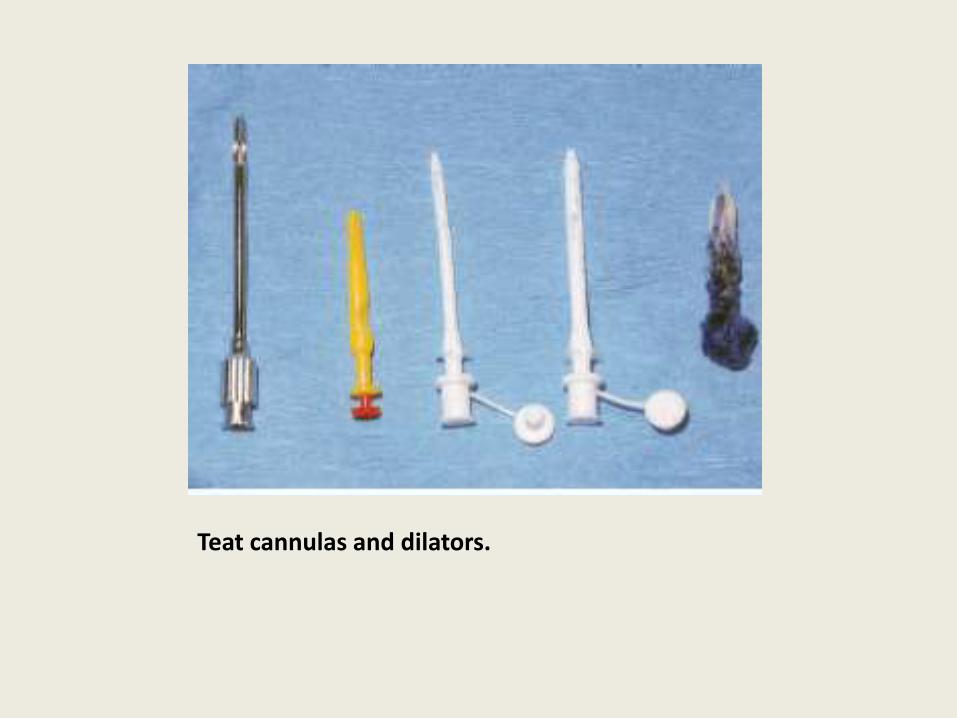
Teat cannulas and dilators.
NTI natural teat inserts.
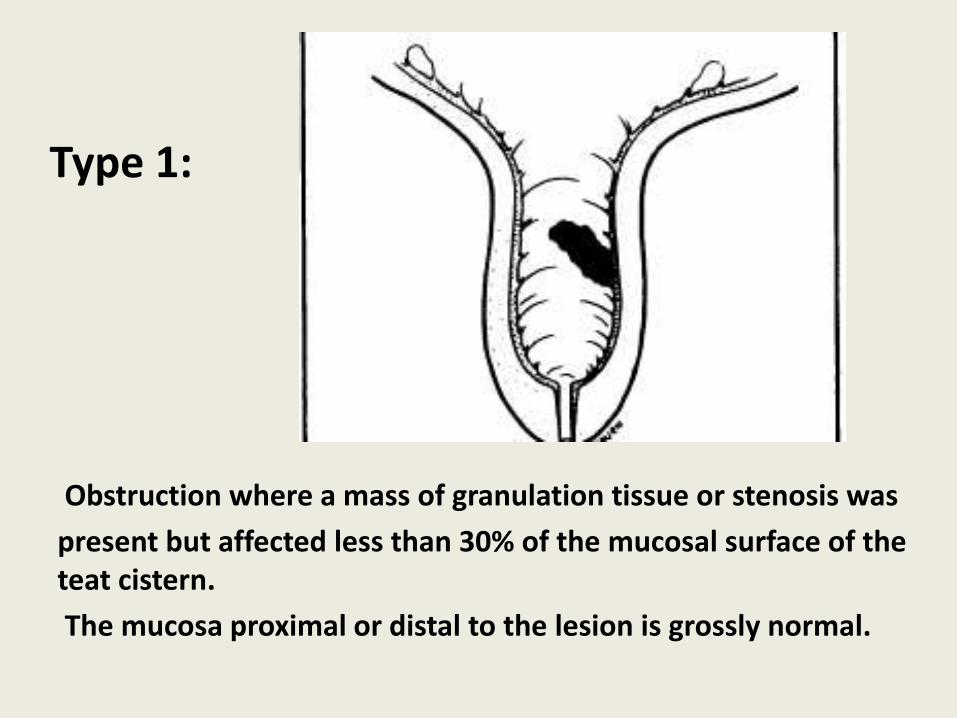
Obstruction where a mass of granulation tissue or stenosis was
present but affected less than 30% of the mucosal surface of the teat cistern.
The mucosa proximal or distal to the lesion is grossly normal.
Type 1:
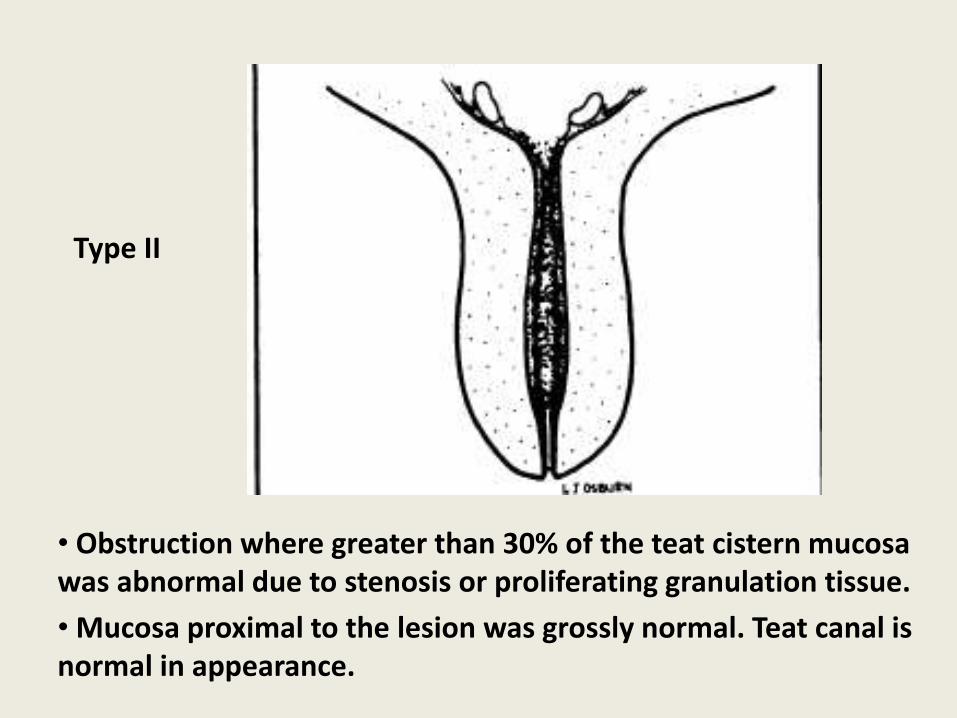
• Obstruction where greater than 30% of the teat cistern mucosa was abnormal due to stenosis or proliferating granulation tissue.
• Mucosa proximal to the lesion was grossly normal. Teat canal is normal in appearance.
Type II
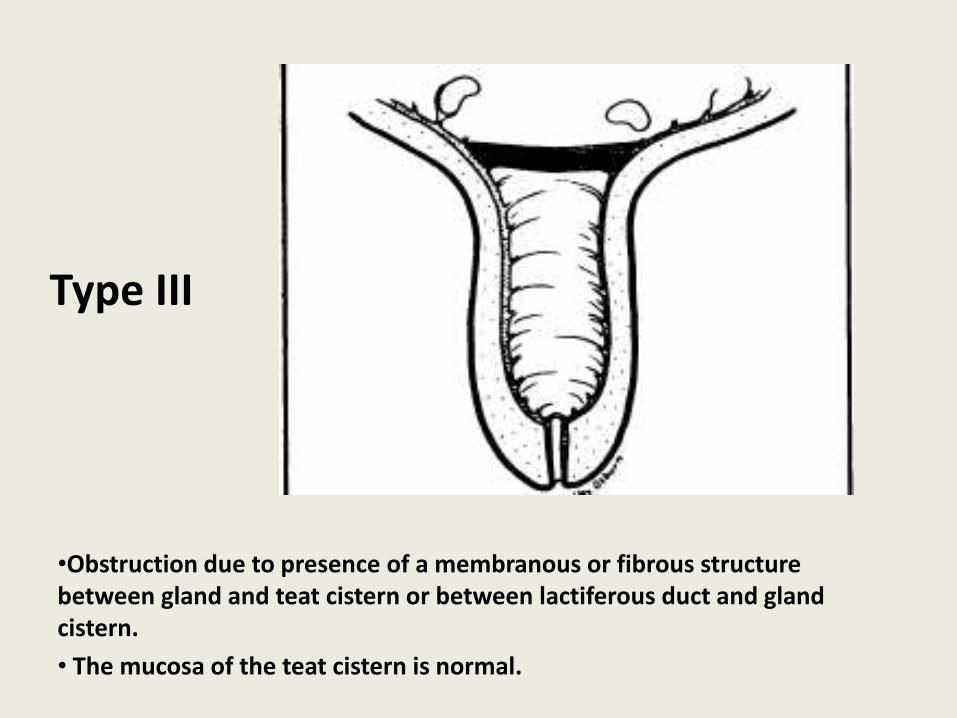
•Obstruction due to presence of a membranous or fibrous structure between gland and teat cistern or between lactiferous duct and gland cistern.
• The mucosa of the teat cistern is normal.
Type III
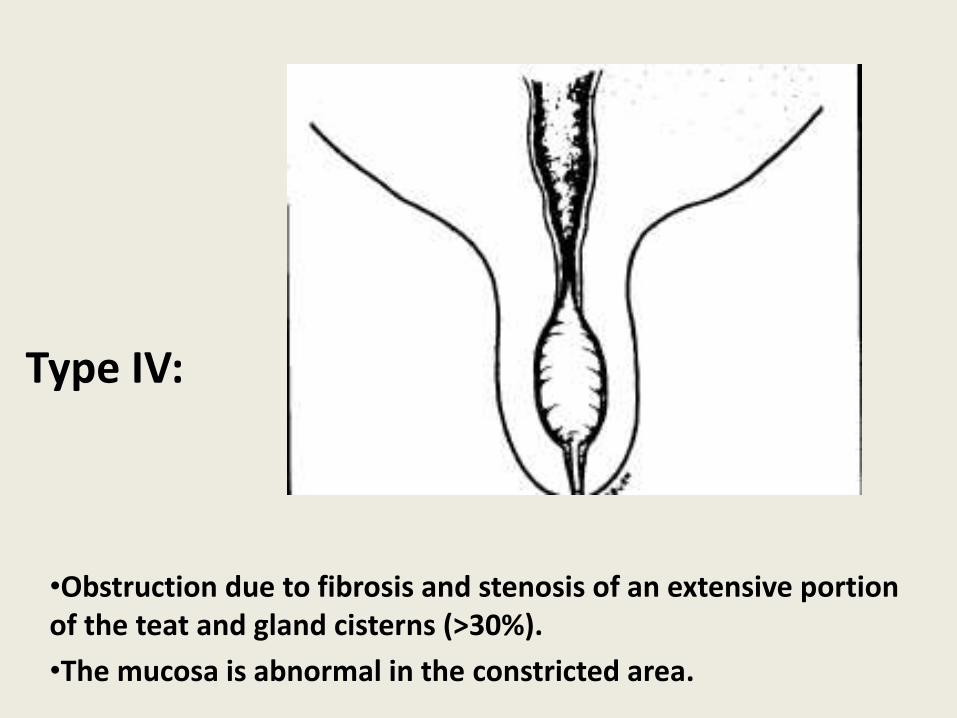
•Obstruction due to fibrosis and stenosis of an extensive portion of the teat and gland cisterns (>30%).
•The mucosa is abnormal in the constricted area.
Type IV:
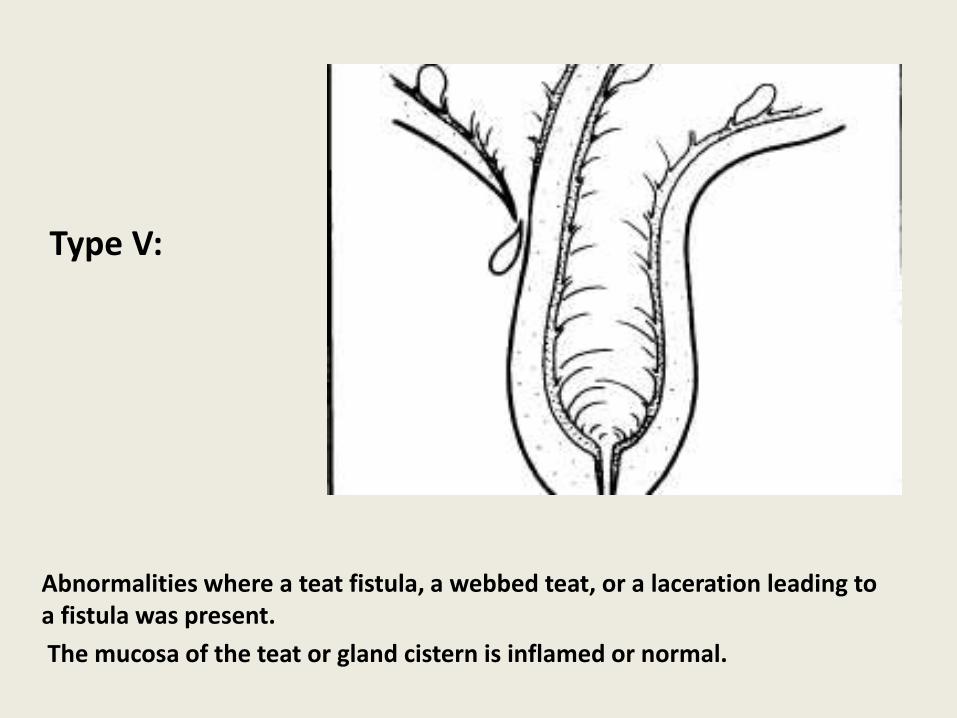
Abnormalities where a teat fistula, a webbed teat, or a laceration leading to a fistula was present.
The mucosa of the teat or gland cistern is inflamed or normal.
Type V:
What does chemical destruction of the teat involve
• 100 cc of (10% formalin diluted in 500 cc of saline)
• Or 100 cc of 3% silver nitrate solution
• 250 ml of acriflavine (1ml in 500 ml of NSS)
• 20 ml of 5% Copper sulfate
• 60 ml of chlorhexidine
• Pre-treat with Megludyne
Related Documents