Teaching Competency in Family Medicine Maternity Care: a National Forum. Toronto, June 7 th , 2013 "Defining competence for the purposes of assessment in Maternity and Newborn Care in Family Medicine: Less is More! Tim Allen, William Ehman For the Working Group on the Assessment of Competence in Maternity and Newborn Care College of Family Physicians of Canada No conflicts

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Teaching Competency in Family Medicine Maternity Care: a National Forum. Toronto, June 7th , 2013
"Defining competence for the purposes of assessment in Maternity and Newborn Care in Family
Medicine: Less is More!
Tim Allen, William Ehman For the Working Group on the Assessment of Competence in Maternity and Newborn Care College of Family Physicians of Canada
No conflicts
“Key Features” – What are they?
n Observable, essential steps in the resolution of clinical situation/problem
n Where we tend to make mistakes n Predictors of competence eg.
n Diagnosis >treatment n Gathering>interpreting data n Undifferentiated>differentiated n Problem specific>routine actions n Using knowledge>regurgitating knowledge
Evaluation: What we are doing now:
Key Feature Evaluation eg. Induction of Labour
n Assess and document n Acceptable indication, priority, EDD,
Cx status, contra-indications, maternal preferences, consent
n Utilize the appropriate method n Eg. foley, PGE2, Oxytocin; appropriate
fetal surveillance, documentation n Manage complications
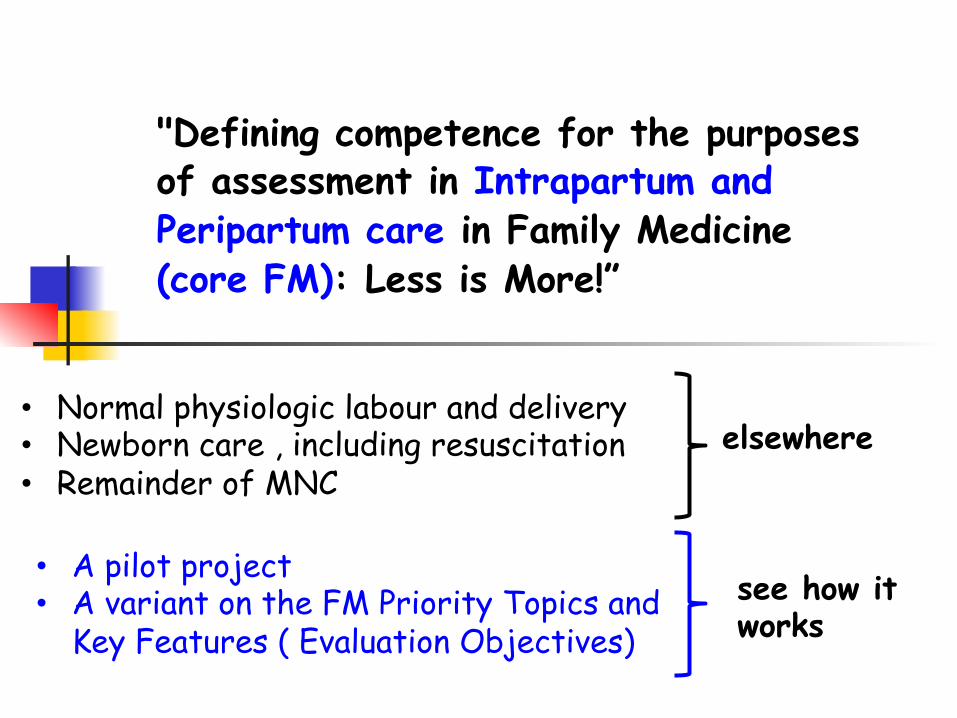
"Defining competence for the purposes of assessment in Intrapartum and Peripartum care in Family Medicine (core FM): Less is More!”
• Normal physiologic labour and delivery • Newborn care , including resuscitation • Remainder of MNC
elsewhere
• A pilot project • A variant on the FM Priority Topics and
Key Features ( Evaluation Objectives) see how it works
7
Albert Schweitzer

Intrapartum care as as Assessment priority for FM
• Complex situations - lots of process Competency is doing the right thing. at the right time, in the right way , for the right reasons
• “Shoulder to shoulder” experience
• Higher level cognitive skills for all of FM Generalisable to overall competence
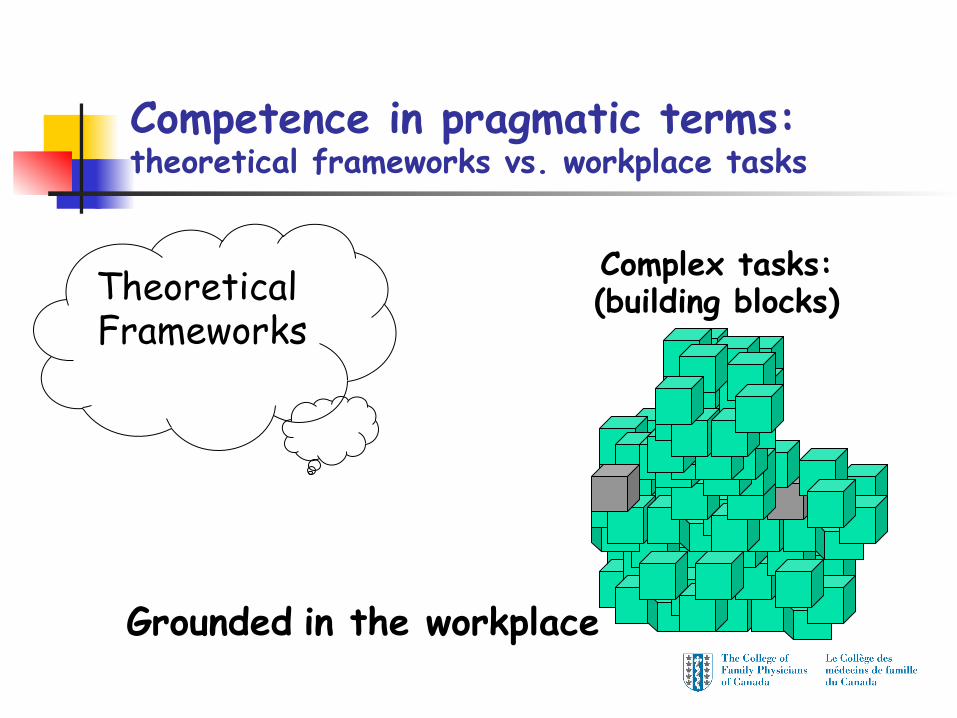
Competence in pragmatic terms: theoretical frameworks vs. workplace tasks
Theoretical Frameworks
Grounded in the workplace
Complex tasks: (building blocks)
Which building blocks (competencies) are most important?
Priority topics n Problems , situations that must be able to
deal with in a competent fashion
Key Features (what is a competent fashion) n The key cognitive skills necessary to deal
well with this problem , in this context
How do we find out what these are?
Identifying Priority Topics & Key Features
Modified Delphi n individual work ( questionnaires , assignments) n group review and modifications n multiple iterations ‘til saturation
n Nominal working group (6 members): practitioners n Validation group (30-40): practitioners
n Stratified representativity ( demographics) n Randomly selected and invited

12
1 Gesta&onal hypertension / pre eclampsia
2 Post-‐partum hemorrhage 3 Team ( working with , in)
4 Fetal health surveillance during labour
5 Limits (knowing and applying)
6 Shoulder dystocia
7 Perineal lacera&ons (repair)
8 Assisted delivery ( Vacuum extrac&on)
9 Labour dystocia 10 Inducing labour
11 BreasDeeding difficulty
12 Peripartum mental health
13 PROM
14 Gesta&onal Diabetes
15 3rd trimester bleeding
16 Fever
17 Pain in Labour
18 TOLAC (Trial of labour aNer Caesarian)
19 Pre-‐term labour
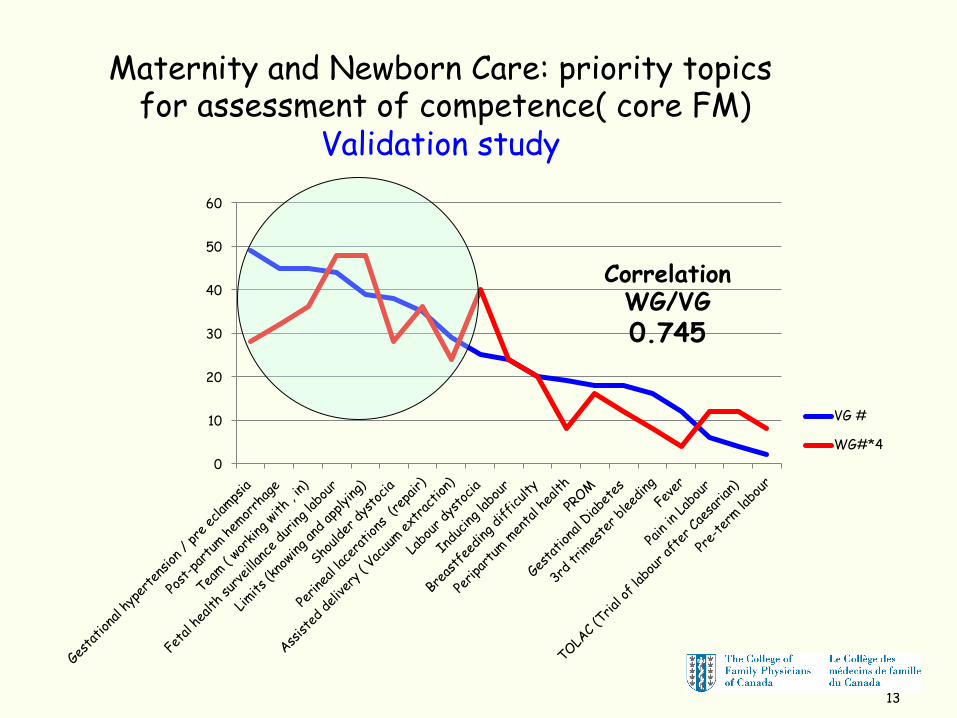
Priority topics ( MNC – core FM): peripartum only
13
0
10
20
30
40
50
60
VG #
WG#*4
Correlation WG/VG 0.745
Maternity and Newborn Care: priority topics for assessment of competence( core FM)
Validation study
14
Procedure skills( MNC: core FM): peripartum only
Validation and working groups • manage shoulder dystocia • repair perineal lacerations • vacuum extraction
Validation group “only” (=more discussion/optional) • amniotomy • place fetal scalp electrode
Excluded from priorities (both groups) • breech delivery • perform episiotomy
15
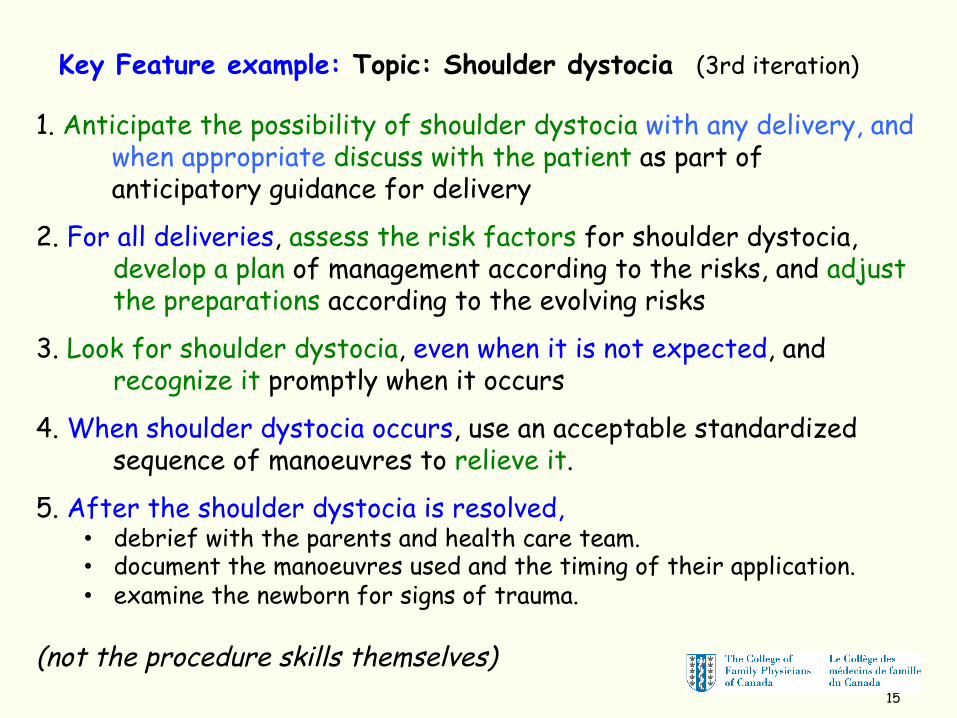
1. Anticipate the possibility of shoulder dystocia with any delivery, and when appropriate discuss with the patient as part of anticipatory guidance for delivery
2. For all deliveries, assess the risk factors for shoulder dystocia, develop a plan of management according to the risks, and adjust the preparations according to the evolving risks
3. Look for shoulder dystocia, even when it is not expected, and recognize it promptly when it occurs
4. When shoulder dystocia occurs, use an acceptable standardized sequence of manoeuvres to relieve it.
5. After the shoulder dystocia is resolved, • debrief with the parents and health care team. • document the manoeuvres used and the timing of their application. • examine the newborn for signs of trauma.
(not the procedure skills themselves)
Key Feature example: Topic: Shoulder dystocia (3rd iteration)
16
“Example is not the main thing in influencing others. It is the only thing.”
“You don’t have to be an angel to be a saint”
Albert Schweitzer
What next?
n WG assumes ongoing role n Complete the Key Features for all priority
topics n Develop a plan to try out formally n Start to try them out informally: do they
work? n Trainee orientation and expectations n Help with feedback and formative assessment
Back to Family Medicine “curriculum committee”
18
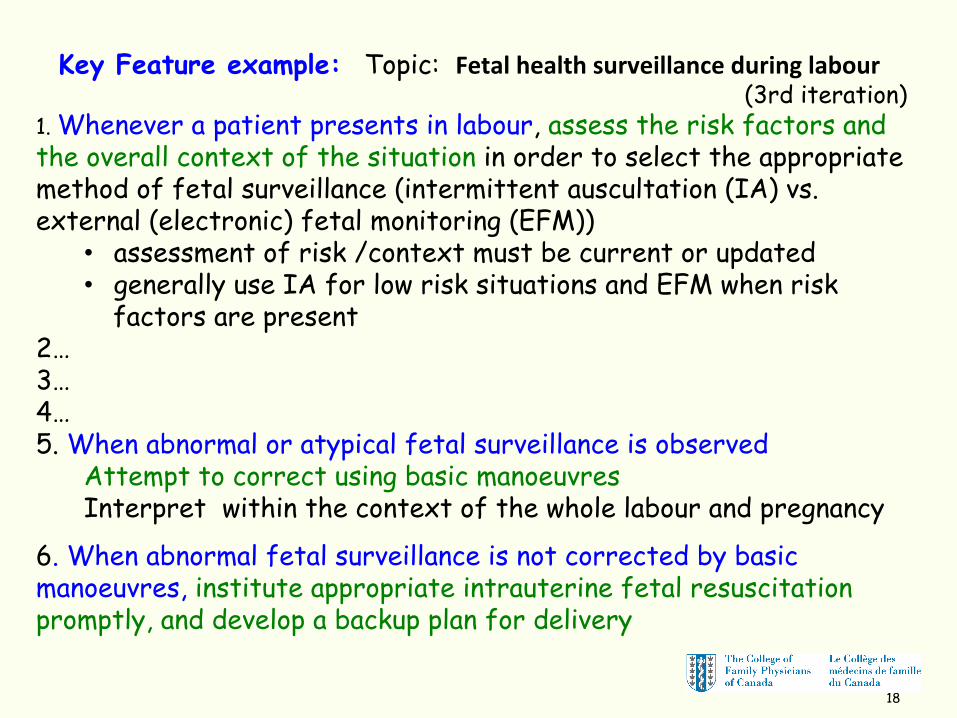
1. Whenever a patient presents in labour, assess the risk factors and the overall context of the situation in order to select the appropriate method of fetal surveillance (intermittent auscultation (IA) vs. external (electronic) fetal monitoring (EFM))
• assessment of risk /context must be current or updated • generally use IA for low risk situations and EFM when risk
factors are present 2… 3… 4… 5. When abnormal or atypical fetal surveillance is observed
Attempt to correct using basic manoeuvres Interpret within the context of the whole labour and pregnancy
6. When abnormal fetal surveillance is not corrected by basic manoeuvres, institute appropriate intrauterine fetal resuscitation promptly, and develop a backup plan for delivery
Key Feature example: Topic: Fetal health surveillance during labour (3rd iteration)

Demographics – Validation Group MNC
26 6
12 20
10 22
7 13
8
10 22
1
26 6
7 22
0 5 10 15 20 25 30
Female Male
Less than 10 More than 10
Rural Urban
West Ontario Quebec
Broad Mixed
Focused
Teaching Non-Teaching
Program Director Not Program Director
Related Documents











