Suicidal Ideation and Behaviours after Traumatic Brain Injury: A Systematic Review Nazanin H. Bahraini, 1,2 Grahame K. Simpson, 3,4 Lisa A. Brenner, 1,2 Adam S. Hoffberg, 1 and Alexandra L. Schneider 1 1 Veterans Integrated Service Network (VISN) 19 Mental Illness Research Education and Clinical Center (MIRECC), Denver, Colorado, USA 2 University of Colorado, School of Medicine, Aurora, Colorado, USA 3 Liverpool Brain Injury Rehabilitation Unit, Liverpool Hospital, Sydney, Australia 4 Rehabilitation Studies Unit, Sydney School of Medicine, University of Sydney, Australia Traumatic brain injury (TBI) is prevalent among many populations and existing data suggest that those with TBI are at increased risk for death by suicide. This systematic review serves as an update to a previous review, with the aim of evaluating the current state of evidence regarding prevalence and risk of suicide deaths, post-TBI suicidal ideation and suicide attempts, and treatments to reduce suicide-related outcomes among TBI survivors. Review procedures followed the PRISMA statement guidelines. In all, 1014 abstracts and 83 full-text articles were reviewed to identify 16 studies meeting inclusion criteria. Risk of bias for individual studies ranged from low to high, and very few studies were designed to examine a priori hypotheses related to suicide outcomes of interest. Overall, findings from this systematic review supported an increased risk of suicide among TBI survivors compared to those with no history of TBI. Evidence pertaining to suicidal thoughts and attempts was less clear, mainly due to heterogeneity of methodological quality across studies. One small randomised controlled trial was identified that targeted suicide prevention in TBI survivors. Further research is needed to identify the prevalence of post-TBI ideation and attempts, and to establish evidence-based suicide prevention practices among TBI survivors. Keywords: suicide, suicide attempt, suicide ideation, traumatic brain injury, systematic review Suicide is a rare but devastating outcome post traumatic brain injury (TBI). However, death by suicide is only the tip of the iceberg, as much larger numbers of people with TBI make suicide attempts or report suicidal ideation. Historically, suicides after TBI were first documented among brain-injured Veterans from the First and Second World Wars (e.g., Russell, 1951). Early reports of civilian suicides were contained in broader TBI Address for correspondence: Nazanin H. Bahraini, VISN 19 MIRECC, 1055 Clermont Street, Denver, Colorado, 80220, USA. E-mail: [email protected] Disclaimer: This article is based on work supported, in part, by the Department of Veterans Affairs, but does not necessarily represent the views of the Department of Veterans Affairs or the United States Government. Drs Brenner and Simpson would also like to acknowledge that they are authors on 6 of the 16 papers reviewed. Efforts were made to reduce conflicts (i.e., other members of the team reviewed their articles in terms of risk of bias). outcome studies conducted in the United King- dom and Europe (e.g., Heiskanen & Sipponen, 1970; Lewin, Marshall, & Roberts, 1979). Since then, continued efforts to empirically investigate the prevalence of suicide and the impact of TBI on suicide risk have contributed to a growing body of literature on suicide-related outcomes among TBI survivors. Although studies examining preva- lence of suicidal ideation, behaviour and death by BRAIN IMPAIRMENT VOLUME 14 NUMBER 1MAY pp. 92–112 c The Author(s), published by Cambridge University Press on behalf of Australian Academic Press Pty Ltd 2013. This is a work of the U.S. Government and is not subject to copyright protection in the United States. doi: 10.1017/BrImp.2013.11 92 available at https://www.cambridge.org/core/terms. https://doi.org/10.1017/BrImp.2013.11 Downloaded from https://www.cambridge.org/core. IP address: 54.39.106.173, on 01 Jun 2020 at 14:08:43, subject to the Cambridge Core terms of use,

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Suicidal Ideation and Behavioursafter Traumatic Brain Injury:A Systematic Review
Nazanin H. Bahraini,1,2 Grahame K. Simpson,3,4 Lisa A. Brenner,1,2 Adam S. Hoffberg,1
and Alexandra L. Schneider1
1Veterans Integrated Service Network (VISN) 19 Mental Illness Research Education and Clinical Center
(MIRECC), Denver, Colorado, USA2
University of Colorado, School of Medicine, Aurora, Colorado, USA3
Liverpool Brain Injury Rehabilitation Unit, Liverpool Hospital, Sydney, Australia4
Rehabilitation Studies Unit, Sydney School of Medicine, University of Sydney, Australia
Traumatic brain injury (TBI) is prevalent among many populations and existingdata suggest that those with TBI are at increased risk for death by suicide. Thissystematic review serves as an update to a previous review, with the aim ofevaluating the current state of evidence regarding prevalence and risk of suicidedeaths, post-TBI suicidal ideation and suicide attempts, and treatments to reducesuicide-related outcomes among TBI survivors. Review procedures followed thePRISMA statement guidelines. In all, 1014 abstracts and 83 full-text articles werereviewed to identify 16 studies meeting inclusion criteria. Risk of bias for individualstudies ranged from low to high, and very few studies were designed to examinea priori hypotheses related to suicide outcomes of interest. Overall, findings fromthis systematic review supported an increased risk of suicide among TBI survivorscompared to those with no history of TBI. Evidence pertaining to suicidal thoughtsand attempts was less clear, mainly due to heterogeneity of methodological qualityacross studies. One small randomised controlled trial was identified that targetedsuicide prevention in TBI survivors. Further research is needed to identify theprevalence of post-TBI ideation and attempts, and to establish evidence-basedsuicide prevention practices among TBI survivors.
Keywords: suicide, suicide attempt, suicide ideation, traumatic brain injury, systematic review
Suicide is a rare but devastating outcome posttraumatic brain injury (TBI). However, death bysuicide is only the tip of the iceberg, as muchlarger numbers of people with TBI make suicideattempts or report suicidal ideation. Historically,suicides after TBI were first documented amongbrain-injured Veterans from the First and SecondWorld Wars (e.g., Russell, 1951). Early reports ofcivilian suicides were contained in broader TBI
Address for correspondence: Nazanin H. Bahraini, VISN 19 MIRECC, 1055 Clermont Street, Denver, Colorado,80220, USA. E-mail: [email protected]: This article is based on work supported, in part, by the Department of Veterans Affairs, but does notnecessarily represent the views of the Department of Veterans Affairs or the United States Government. Drs Brennerand Simpson would also like to acknowledge that they are authors on 6 of the 16 papers reviewed. Efforts were madeto reduce conflicts (i.e., other members of the team reviewed their articles in terms of risk of bias).
outcome studies conducted in the United King-dom and Europe (e.g., Heiskanen & Sipponen,1970; Lewin, Marshall, & Roberts, 1979). Sincethen, continued efforts to empirically investigatethe prevalence of suicide and the impact of TBIon suicide risk have contributed to a growing bodyof literature on suicide-related outcomes amongTBI survivors. Although studies examining preva-lence of suicidal ideation, behaviour and death by
BRAIN IMPAIRMENT VOLUME 14 NUMBER 1 MAY pp. 92–112 c© The Author(s), published by Cambridge University Press on behalf of AustralianAcademic Press Pty Ltd 2013. This is a work of the U.S. Government and is not subject to copyright protection in the United States.
doi: 10.1017/BrImp.2013.11
92
available at https://www.cambridge.org/core/terms. https://doi.org/10.1017/BrImp.2013.11Downloaded from https://www.cambridge.org/core. IP address: 54.39.106.173, on 01 Jun 2020 at 14:08:43, subject to the Cambridge Core terms of use,
SUICIDE AFTER TBI
suicide among TBI survivors have yielded variablerates, some studies have shown that, compared tothe general population, those with a history of TBIare at increased risk of suicidal ideation (Ansteyet al., 2004), suicide attempts (Silver, Kramer,Greenwald, & Weissman, 2001) and death by sui-cide (Teasdale & Engberg, 2001). However, notall studies have found such a relationship, withtwo mortality studies not reporting an elevatedrate of suicide deaths (Harrison-Felix, Whiteneck,DeVivo, Hammond, & Jha, 2006; Shavelle,Strauss, Whyte, Day, & Yu, 2001).
The purpose of this study was to conduct asystematic review of the literature in order to eval-uate the evidence regarding prevalence and risk ofsuicidal thoughts, behaviours and death by suicidefollowing TBI, and to examine the effectiveness ofinterventions to reduce suicide-related outcomesin those with TBI. The first dedicated review ad-dressing the prevalence of suicidal thoughts and be-haviours (deaths and attempts), risk factors for sui-cide and clinical management approaches amongsurvivors of TBI was published in 2007 (Simpson& Tate, 2007). A scoping methodology was cho-sen to ascertain both the breadth and depth of evi-dence within the field. The structured review iden-tified 48 peer-reviewed journal articles publishedbefore 2007 that addressed suicidality among sur-vivors of TBI. This relatively large number of cita-tions was deceptive, however, as few of the articlescomprised suicide-specific studies per se. In themajority of cases, suicidal behaviours were inci-dental to the primary focus of the studies, whichwere investigating general post-injury mortality,psychosocial outcomes or depression.
Based on the most robust studies available(three population studies, one meta-analysis),the review concluded that, in comparison to thegeneral population, individuals with TBI were ata 3.5–4 times greater risk of suicide (Harris &Barraclough, 1997; Teasdale & Engberg, 2001);had a significantly higher lifetime history ofsuicide attempts (8.1% in TBI survivors versus1.9% in the general population; Silver et al., 2001)and higher levels of suicidal ideation (Ansteyet al., 2004). The studies into suicide attemptsand suicide ideation found that the elevated ratesremained significant after adjusting for a range ofdemographic, socio-economic, psychosocial andpsychopathological covariates.
Furthermore, the 2007 review found evidencefor two domains of risk factors that modulatedlevels of suicidal behaviours. Importantly, the fol-lowing findings were all derived from multivariateanalyses that controlled for covariates, includingsex, age at injury, time post-injury, length of post-traumatic amnesia, pre-morbid psychiatric distur-
bance and post-injury psychopathlogy. The firstdomain was injury severity. People with severe TBIwere 1.4 times more likely to die by suicide thanpeople with mild injuries (95% confidence inter-val (CI), 1.15, 1.75; Teasdale & Engberg, 2001).The second domain was post-injury psychopathol-ogy. Post-injury substance abuse, suicide ideation,hopelessness and/or the presence of any post-injurypsychiatric history/emotional distress were signifi-cant predictors of either suicide attempts or suicideideation (Simpson & Tate, 2002, 2005; Teasdale& Engberg, 2001). The risk of attempts or sui-cidal ideation among individuals with such psy-chopathology was 4.9–8.7 times greater than forpeople with TBI and no post-injury history of psy-chopathology (Simpson & Tate, 2002, 2005; Teas-dale & Engberg, 2001). The review also found thatamong TBI survivors, little research into suicideprevention had been conducted. No treatments orclinical management approaches for people withTBI had been tested. The only experimental reportwas of the outcomes from a controlled trial of asuicide prevention training programme deliveredto rehabilitation and disability staff working in thefield of TBI (Simpson, Winstanley, & Bertapelle,2003).
Overall, the review found a consistent pictureof elevated suicidal behaviours after TBI, but theunderlying evidence-base was limited to a smallnumber of studies. In the introduction to a recentspecial issue on suicide and TBI, Simpson andBrenner (2011) observed that there had been an up-surge in research activity in this field over the previ-ous decade. Since the original 2007 review, severalnarrative reviews of the suicide literature focus-ing on TBI among civilians and/or military Vet-erans have been published (Brenner, Vanderploeg,& Terrio, 2009; Reeves & Brister, 2009; Reeves &Laizer, 2012; Simpson & Tate, 2009; Wassermanet al., 2008). These reviews have canvassed muchof the earlier literature, but have also highlighted anumber of newer studies.
Therefore, the current review investigated liter-ature published from the beginning of 2007. Whilecertain aspects of the original review (i.e., risk ofsuicidal outcomes following TBI and clinical man-agement of suicidal behaviours after TBI) havebeen preserved, the suicide nomenclature and re-view methodology have been updated to reflectcontemporary developments. The latest standard-ised suicide nomenclature (the Self-Directed Vio-lence Classification System; Brenner et al., 2011b)has been adopted, replacing the 1996 framework(O’Carroll et al., 1996) employed in the 2007study. With respect to methodology, the current re-view has been conducted in accordance with rele-vant items from the PRISMA (Preferred Reporting
93
available at https://www.cambridge.org/core/terms. https://doi.org/10.1017/BrImp.2013.11Downloaded from https://www.cambridge.org/core. IP address: 54.39.106.173, on 01 Jun 2020 at 14:08:43, subject to the Cambridge Core terms of use,

N. BAHRAINI ET AL.
Items for Systematic Reviews and Meta-Analyses)Statement (Liberati et al., 2009; Moher, Liberati,Tetzlaff, Altman, & the PRISMA Group, 2010).Items included in the PRISMA statement reflectseveral conceptual and practical advances in thescience of conducting systematic reviews (Moheret al., 2010), a number of which pertain to assess-ment of risk of bias.
Despite the centrality of risk of bias assess-ment in evaluating the strength of evidence insystematic reviews, there is little consensus onthe best approach or preferred tool for assess-ing risk of bias. Given that the current reviewwas designed to address multiple research ques-tions pertaining to TBI and suicide-related out-comes, approaches and tools selected would needto take into account the heterogeneity of stud-ies both with respect to design and study con-duct. In the absence of a gold-standard tool forassessing risk of bias across different types of stud-ies, a number of different potential tools and ap-proaches were considered for the current review.The two tools finally selected to rate the studydesigns targeted in this review, namely, the Re-search Triangle Institute (RTI) Risk of Bias tool(Viswanathan & Berkman, 2012) for observationalstudies and the PEDro rating scale (Sherrington,Herbert, Maher, & Moseley, 2000) for randomisedtrials, met many of the recommended criteriafor risk of bias measurement selection (Reeves,Deeks, Higgins, & Wells, 2008; Viswanathan et al.,2012). Specifically, they were designed for use insystematic reviews; demonstrated acceptable reli-ability and validity; provided explicit support forjudgements; were easy to use; addressed items re-lated to different sources of bias (i.e., study leveland outcome level); avoided the use of uniformweights across items (RTI Risk of Bias tool only);were specific to the study designs being evaluated;and, when possible, the risk of bias assessment wasnot presented as a composite score, or if a compos-ite score was used, its validity as an overall measureof methodological quality had been establishedpreviously (e.g., PEDro rating scale; deMorton,2009). Informed by these advances in methodol-ogy, the review addressed two key questions (KQ):
KQ1. Among adult survivors of TBI, what isthe association between history of TBI andpost-TBI death by suicide, suicide attemptsor suicidal ideation? KQ1 specifically in-vestigated the prevalence of the suicidal be-haviours (i.e., death by suicide, suicide at-tempts and suicidal ideation) and the extentto which the presence of TBI increased riskfor suicidal thoughts and behaviours.
KQ2. What interventions are effective in reducingsuicide-related outcomes in adult survivorsof TBI?
MethodsThe methodology and presentation of results fol-lowed the PRISMA Statement for reporting sys-tematic reviews of studies that evaluate health-care interventions (Liberati et al., 2009; Moher etal., 2010). In particular, the research group usedPRISMA items 1, 3–4, 6–13, 17–20 and 24–26,and the recommended study flow diagram. Itemsthat were not included were outside the scope ofthe current review. For example, heterogeneity ofmethods, study conduct and overall study qualityacross the relatively small number of studies iden-tified for each key question precluded quantitativesynthesis of results. As such, items 14–16 and 21–23 were not reported as they pertain to summarystatistics and meta-analyses. Following study se-lection and data extraction, risk of bias of eachoutcome of interest within individual studies wasassessed and incorporated in a qualitative synthesisof findings from all studies for each key questionand outcome.
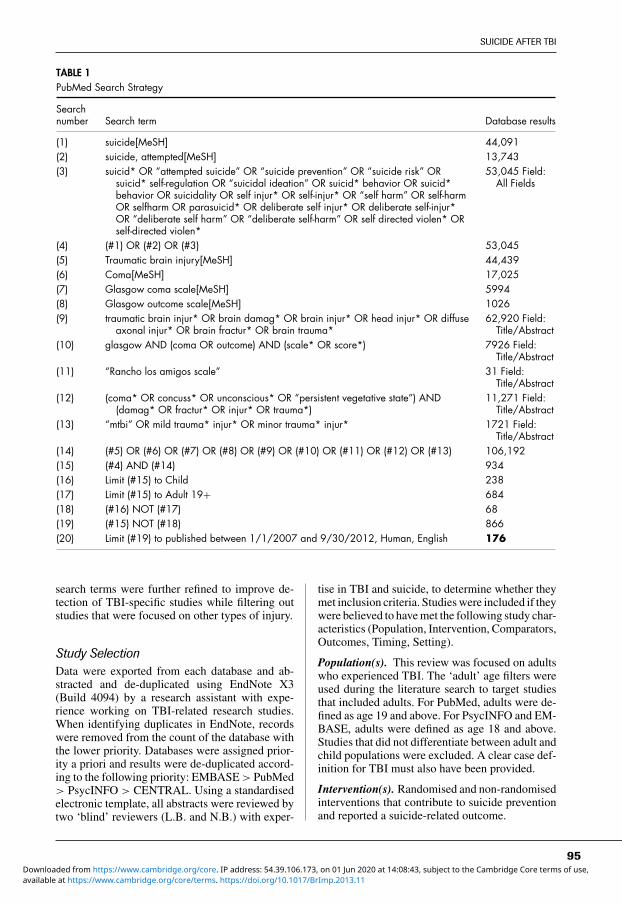
Search StrategyPubMed, PsycINFO, EMBASE and the CochraneCentral Register of Controlled Trials (Central)were searched on 1 October 2012 for peer-reviewed articles published in English from 1 Jan-uary 2007 through 1 October 2012 to gather rele-vant articles to address the aims examined in thekey research questions listed above. Terms relatingto suicide and self-directed violence were crossedwith terms related to traumatic brain injury (seeTable 1). Prior to the search strategy being fi-nalised, preliminary searches across all databaseswere conducted that included additional self-harmterms from the National Institute for Health andClinical Excellence (NICE) commissioned reporton self-harm (NICE, 2012). Searches were alsoconducted using additional brain injury terms fromthe World Health Organisation (WHO) report onmild traumatic brain injury (mTBI) (Carroll, Cas-sidy, Holm, Kraus, & Coronado, 2004). After run-ning the preliminary searches with these additionalterms and browsing the results, it was determinedby unanimous consensus within the research groupthat while highly sensitive, the search yield wasnot specific enough for the purposes of this review.For example, the vast majority of studies that wereidentified were not specific to TBI, but instead cov-ered a wide range of physical injuries and illnessesthroughout the body. Based on these issues, the
94
available at https://www.cambridge.org/core/terms. https://doi.org/10.1017/BrImp.2013.11Downloaded from https://www.cambridge.org/core. IP address: 54.39.106.173, on 01 Jun 2020 at 14:08:43, subject to the Cambridge Core terms of use,
SUICIDE AFTER TBI
TABLE 1PubMed Search Strategy
Searchnumber Search term Database results
(1) suicide[MeSH] 44,091(2) suicide, attempted[MeSH] 13,743(3) suicid* OR “attempted suicide” OR “suicide prevention” OR “suicide risk” OR
suicid* self-regulation OR “suicidal ideation” OR suicid* behavior OR suicid*behavior OR suicidality OR self injur* OR self-injur* OR “self harm” OR self-harmOR selfharm OR parasuicid* OR deliberate self injur* OR deliberate self-injur*OR “deliberate self harm” OR “deliberate self-harm” OR self directed violen* ORself-directed violen*
53,045 Field:All Fields
(4) (#1) OR (#2) OR (#3) 53,045(5) Traumatic brain injury[MeSH] 44,439(6) Coma[MeSH] 17,025(7) Glasgow coma scale[MeSH] 5994(8) Glasgow outcome scale[MeSH] 1026(9) traumatic brain injur* OR brain damag* OR brain injur* OR head injur* OR diffuse
axonal injur* OR brain fractur* OR brain trauma*62,920 Field:
Title/Abstract(10) glasgow AND (coma OR outcome) AND (scale* OR score*) 7926 Field:
Title/Abstract(11) “Rancho los amigos scale” 31 Field:
Title/Abstract(12) (coma* OR concuss* OR unconscious* OR “persistent vegetative state”) AND
(damag* OR fractur* OR injur* OR trauma*)11,271 Field:
Title/Abstract(13) “mtbi” OR mild trauma* injur* OR minor trauma* injur* 1721 Field:
Title/Abstract(14) (#5) OR (#6) OR (#7) OR (#8) OR (#9) OR (#10) OR (#11) OR (#12) OR (#13) 106,192(15) (#4) AND (#14) 934(16) Limit (#15) to Child 238(17) Limit (#15) to Adult 19+ 684(18) (#16) NOT (#17) 68(19) (#15) NOT (#18) 866(20) Limit (#19) to published between 1/1/2007 and 9/30/2012, Human, English 176
search terms were further refined to improve de-tection of TBI-specific studies while filtering outstudies that were focused on other types of injury.
Study SelectionData were exported from each database and ab-stracted and de-duplicated using EndNote X3(Build 4094) by a research assistant with expe-rience working on TBI-related research studies.When identifying duplicates in EndNote, recordswere removed from the count of the database withthe lower priority. Databases were assigned prior-ity a priori and results were de-duplicated accord-ing to the following priority: EMBASE > PubMed> PsycINFO > CENTRAL. Using a standardisedelectronic template, all abstracts were reviewed bytwo ‘blind’ reviewers (L.B. and N.B.) with exper-
tise in TBI and suicide, to determine whether theymet inclusion criteria. Studies were included if theywere believed to have met the following study char-acteristics (Population, Intervention, Comparators,Outcomes, Timing, Setting).
Population(s). This review was focused on adultswho experienced TBI. The ‘adult’ age filters wereused during the literature search to target studiesthat included adults. For PubMed, adults were de-fined as age 19 and above. For PsycINFO and EM-BASE, adults were defined as age 18 and above.Studies that did not differentiate between adult andchild populations were excluded. A clear case def-inition for TBI must also have been provided.
Intervention(s). Randomised and non-randomisedinterventions that contribute to suicide preventionand reported a suicide-related outcome.
95
available at https://www.cambridge.org/core/terms. https://doi.org/10.1017/BrImp.2013.11Downloaded from https://www.cambridge.org/core. IP address: 54.39.106.173, on 01 Jun 2020 at 14:08:43, subject to the Cambridge Core terms of use,
N. BAHRAINI ET AL.
Comparator(s). Similar populations that have notbeen diagnosed with TBI; comparison group wasnot required for inclusion.
Outcome(s). Suicidal ideation and/or behaviouras defined according to the Self-Directed Vio-lence Classification System (Brenner et al., 2011b),which can be accessed at http://www.mirecc.va.gov/visn19/docs/SDVCS.pdf
Timing. No limitations based on timing.
Setting. No limitations based on study setting.
Additional criteria included: (1) the full-textarticle was in English; (2) the article addressed aTBI population and measured post-TBI suicide-related outcomes (studies with samples from thegeneral population who suffered a TBI as a result ofself-inflicted injury were excluded); (3) the articlepresented original study data (dissertations, com-mentaries, editorials, letters, books/book chaptersand reviews were excluded); and (4) the studyused a quantitative design (qualitative studies wereexcluded). Although excluded, any systematic re-views and meta-analyses identified were reviewedfor additional reference mining. At the abstract re-view level (PRISMA Screening Stage), disagree-ments regarding inclusion criteria were resolvedby including a third reviewer for consensus.
Full-text was obtained for all articles that metthe screening inclusion criteria. Each article wasexamined by two reviewers (three ‘blind’ review-ers in total taking part). If upon full-text review(PRISMA Eligibility Stage), it was determined thatthe article did not meet inclusion criteria (as notedabove), it was excluded. Disagreements regardingthe inclusion of an article at the Eligibility Stagewere similarly resolved by consensus of a third re-viewer. Reviewers discussed any remaining stud-ies and ultimately reached a unanimous decisionregarding the inclusion status of all articles.
Additional searches were conducted of the ref-erence lists of all included articles, systematic re-views and meta-analyses identified in the literaturesearch, as well as the grey literature (using GoogleSearch and Google Scholar). For the grey litera-ture, an advanced search was conducted search-ing for all of the words ‘traumatic brain injury’and ‘suicide’. The first 11 pages of results werereviewed for possible inclusion according to thesame criteria as the database literature search. Anyreview articles identified in these searches werealso mined for additional references.
Data AbstractionThe following data were abstracted for observa-tional studies with prevalence of suicidal ideation
(SI), suicide attempt (SA) or both as outcomeof interest: study design, sample size and set-ting, sample demographics (sex, age), TBI sever-ity, source or measure of SI/SA, and time frame,time post-injury and prevalence of SI/SA. For ob-servational studies that investigated whether thepresence of TBI increased risk for SI/SA, data ab-stracted included additional information pertain-ing to analyses and results. Studies in which deathwas the outcome of interest abstracted the follow-ing: study design, population/sample, study admis-sion (target period), TBI severity, reference popu-lation, prevalence of suicide, and standard mor-tality ratios (SMR) or odds ratios (OR). Data ab-stracted from treatment studies included: design,sample size and setting, sample demographics (sex,age), TBI severity, time post injury, primary out-comes, measures of SI, attrition and treatmentoutcome.
Assessment of Risk of Bias of ObservationalStudiesProcedures and tools for assessing risk of biasfor observational studies were largely informed byguidelines established in the Agency for Health-care Research and Quality methods guide for sys-tematic reviews (Viswanathan & Berkman, 2012;Viswanathan et al., 2012) and included the proce-dures described below.
Classification of Study Design. Correct classi-fication of study design and identifying criticalsources of bias and confounding for that type ofdesign are critical to accurately assessing risk ofbias (Viswanathan & Berkman, 2012). The designfor each study meeting inclusion criteria followingfull-text review was assessed by two independentraters using the Taxonomy of Study Design Tool(Hartling et al., 2010). Disagreements were dis-cussed until consensus was achieved.
Risk of Bias Components Analysis. For ob-servational studies, the RTI Risk of Bias tool(Viswanathan & Berkman, 2012) was utilisedto assess risk of bias, confounding and preci-sion. Using a components approach, the RTItool was specifically developed to assess risk ofbias across different types of observational stud-ies (i.e., cohort, case-control, cross-sectional andcase-series). Sources of bias assessed include se-lection bias (e.g., differential selection of studyparticipants, inappropriate selection of controls,inclusion/exclusion criteria inconsistently appliedwithin or across groups), detection bias (e.g., inac-curate assessment or misclassification of exposureand outcomes, use of unreliable or poorly vali-dated measures), performance bias (e.g., variations
96
available at https://www.cambridge.org/core/terms. https://doi.org/10.1017/BrImp.2013.11Downloaded from https://www.cambridge.org/core. IP address: 54.39.106.173, on 01 Jun 2020 at 14:08:43, subject to the Cambridge Core terms of use,
SUICIDE AFTER TBI
in procedures administered, protocol deviations),reporting bias (i.e., differential or incomplete re-porting of outcomes and study findings), attritionbias (e.g., high or differential loss to follow-up),and confounding (e.g., failure to identify or ac-count for important confounders through design oranalysis) (Viswanathan et al., 2012). In addition torisk of bias, three additional RTI items rate the pre-cision of findings/estimates in situations where theheterogeneity of findings prevents pooling of data.Detailed instructions for the reviewer and responseoptions pertaining to each of the questions are pro-vided to increase clarity, accuracy and ease of use.In addition to completing response options, review-ers are instructed to provide an explanation for theirratings, thereby increasing the transparency of theevaluation.
Although the RTI Risk of Bias tool is a newtool, its development and refinement were basedon a rigorous, multiphase process that consistedof face validity testing, cognitive testing, con-tent validity testing and inter-rater reliability test-ing. Specifically, inter-rater reliability of the orig-inal 40-item measure ranged from 90% for ques-tions concerning presentation and 88% for thoseconcerning soundness of information, to 56% forquestions concerning follow-up (Viswanathan &Berkman, 2012). The items that had poor inter-rater reliability were either removed or revised toimprove clarity and usefulness. Following this pro-cess, further evaluation and testing of the measurethrough expert consensus contributed to the refined16-item measure used in this systematic review.
Prior to evaluating risk of bias for the individ-ual studies, reviewers met and discussed the formto clarify specific criteria pertaining to some of thequestions. Decisions were made regarding impor-tant confounding variables, measures and indica-tors of exposure status, and measures considered tobe valid and reliable. These criteria and guidelineswere added to the review form to help facilitateaccuracy and reliability across reviewers.
Each observational study that met inclusioncriteria following full-text review was evaluatedusing RTI items that reflected sources of bias spe-cific to its study design. For example, the number ofcore items pertaining to each of the observationaldesigns is as follows: case series (8), case-control(8), cohort (12) and cross-sectional (10). Each riskof bias criterion was evaluated using the appro-priate criteria for that study design and for eachpredetermined outcome. Following completion ofall items, indications of bias and precision weresummarised in a table by category (e.g., selectionbias, detection bias). These summary results wereused to evaluate the overall risk of bias for the studyfor each selected outcome.
Global rating of the risk of bias. Global ratingsof bias for each study were classified as low (re-sults are valid or represent true effects), moderate(results are valid and/or represent true effect; how-ever, study is susceptible to some bias, but not tothe degree that the results would be consideredinvalid), high (a study with significant flaws andmarked by biases of various natures that are likelyto invalidate the results) or unknown (missing in-formation which makes it difficult to judge limi-tations) (Viswanathan et al., 2012). Two review-ers independently assessed risk of bias (individualcriteria and global rating). Disagreements were re-solved through consensus and, if needed, a thirdresearcher was consulted. As two of the authorsof this review were also authors on 6 out of the16 papers evaluated, individuals were not primar-ily responsible for review of the articles on whichthey were authors.
Assessment of Risk of Bias of RandomisedTrialsThe single randomised clinical trial (RCT) in-cluded in this review was independently assessedby two reviewers using the PEDro scale (Sher-rington et al., 2000), an 11-item scale designedfor rating methodological quality of RCTs. Re-liability and validity of the scale has been es-tablished across several studies (deMorton, 2009;Macedo et al., 2010; Maher, Sherrington, Herbert,Moseley, & Elkins, 2003). Items address variouscomponents related to the conduct of the studyand sources of bias that can impact the validityof findings. These include, but are not limited to,randomisation, concealed allocation, blinding, out-come reporting and follow-up/attrition. Each satis-fied item (except for item 1) contributes one pointto the total PEDro score (range = 0–10 points).A search for the trial was then performed on Psy-cbite (www.psycbite.com), an extensive databaseof cognitive, behavioural and other treatments forpsychological problems resulting from acquiredbrain impairment (ABI) and independently ratedfor their methodological quality (Tate et al., 2004).Scores from the current review were compared tothe Psycbite PEDro score.
Current standards listed in the PRISMA state-ment indicate that critical appraisal of studiesshould consider both study level (e.g., alloca-tion concealment) and outcome level (e.g., re-liability and validity of outcome data) sourcesof bias. Although the PEDro scale incorporatesseveral items that address sources of bias withrespect to study-level characteristics (e.g., ran-domisation, allocation, ‘blinding’ of therapists),the number of items that specifically assess
97
available at https://www.cambridge.org/core/terms. https://doi.org/10.1017/BrImp.2013.11Downloaded from https://www.cambridge.org/core. IP address: 54.39.106.173, on 01 Jun 2020 at 14:08:43, subject to the Cambridge Core terms of use,

N. BAHRAINI ET AL.
outcome-measurement bias are limited and pri-marily focused on ‘blinding’ of outcome assessors.Taking this into consideration, information relatedto measurement bias not explicitly addressed bythe PEDro scale (i.e., reliability and validity ofmeasures used to assess exposure and outcomes)was noted and considered in conjunction with PE-Dro scores when determining the overall risk ofbias and quality rating for the trial.
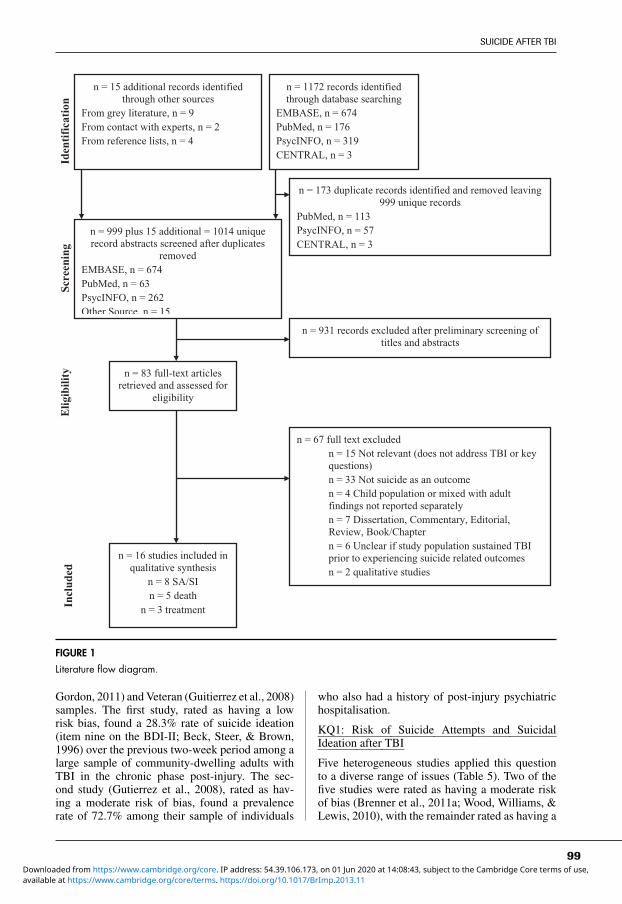
ResultsStudy SelectionA total of 999 titles and abstracts obtained fromthe electronic searches were reviewed. Fifteen ad-ditional studies were identified from other sources.Applying inclusionary/exclusionary criteria, 83 ar-ticles were reviewed (see Figure 1). Of these arti-cles, 67 were excluded as described in Figure 1.Thirteen studies were identified for KQ1 (fivedeaths, eight ideation and/or attempts) and threetreatment-related studies were identified for KQ2.
Study Characteristics and Risk of BiasIndividual study characteristics, indicators of biasand global ratings of bias for individual studies arepresented in Tables 2–6.
Synthesis of EvidenceKQ1: Death by Suicide
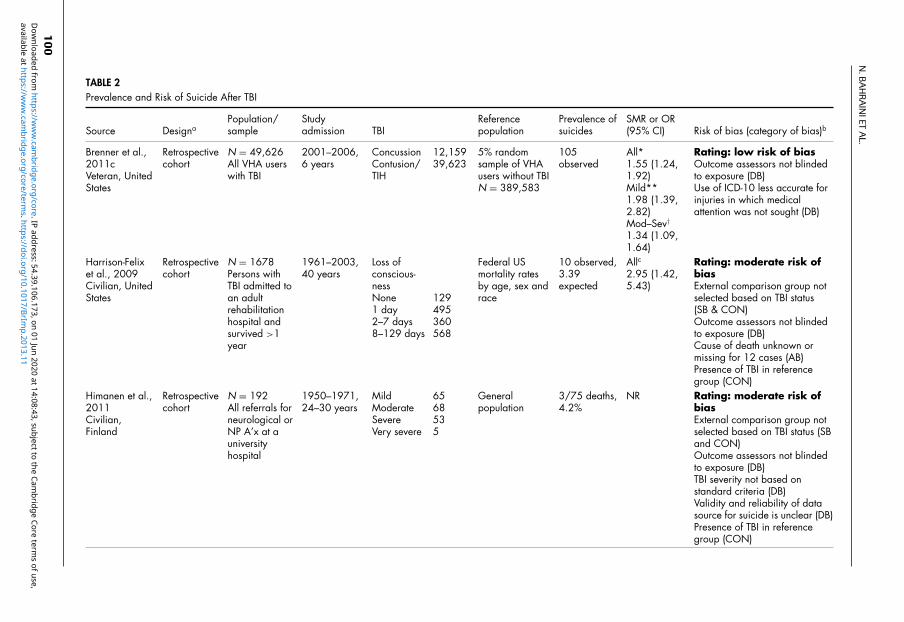
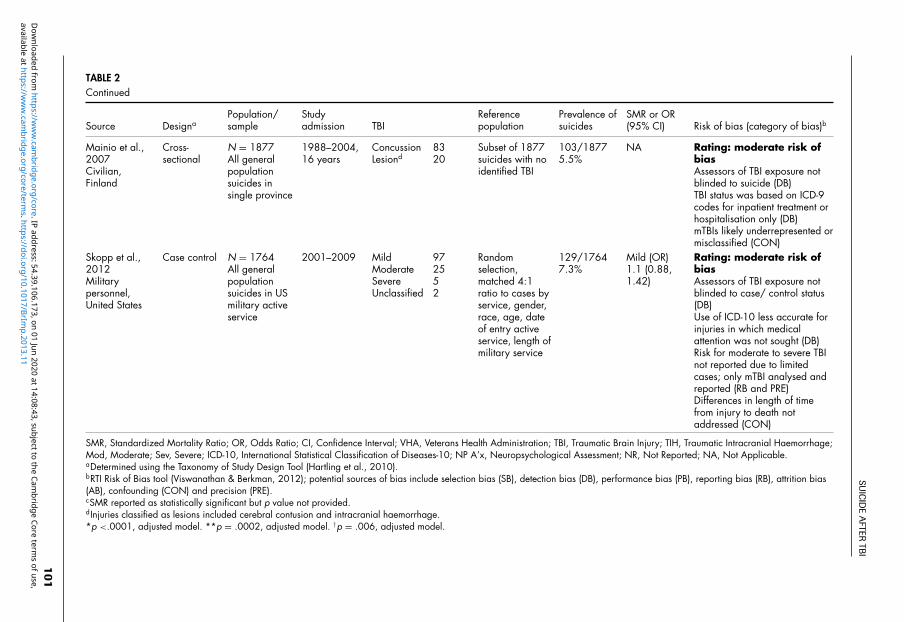
Death by suicide as an outcome was reported infive studies (Table 2). The purposes of the studiesvaried. One study specifically examined suicide-related mortality among military Veterans with andwithout TBI (Brenner, Ignacio, & Blow, 2011c).Two studies investigated mortality among civil-ians with TBI and included data on cause-specificdeaths, including suicide (Harrison-Felix et al.,2009; Himanen et al., 2011). Finally, two studiesexamined individuals with TBI who died by sui-cide among more broadly defined populations: (1)all suicides in a province of Finland (Mainio et al.,2007); and (2) all suicides among United Statesserving military (Skopp, Trofimovich, Grimes,Oetjen-Gerdes, & Gahm, 2012). Interestingly, therates of TBI among the general suicide deaths inboth studies were very similar (Finish study 5.5%;United States Military study, 7.3%). Three of thesestudies sought to quantify the level of risk of deathby suicide associated with TBI (Brenner et al.,2011c; Harrison-Felix et al., 2009; Skopp et al.,2012), while the other two were descriptive only.
Findings from two retrospective cohort stud-ies (Brenner et al., 2011c; Harrison-Felix et al.,2009) supported an increased risk for death by sui-
cide among persons with TBI, while results fromone case-control study (Skopp et al., 2012) didnot show a significantly higher rate of TBI amongthose who died by suicide. Global rating of bias forone of the cohort studies (Brenner et al., 2011c),was low, and results supported an increased riskfor death by suicide among US Veterans with TBI(ranging from 1.3 to 2.0 times higher than Vet-erans without TBI). Harrison-Felix et al. (2009)found elevated rates of suicide among a civiliancohort of TBI patients (about three times higherthan persons in the general population of similarage, sex and race). However, this study had a mod-erate risk of bias. Although a number of importantknown confounders were taken into account, pres-ence of TBI and other health-related risk factors inthe comparison group (i.e., US general population)introduced sources of selection bias and other po-tential confounders. Furthermore, use of nationaldeath rates as opposed to general population ratesfor the State of Colorado also contributed to themoderate rating as age-adjusted suicide rates in thestate of Colorado are notably higher than nationaldeath rates (Centers for Disease Control and Pre-vention, 2012). Lastly, using a case-control design,Skopp et al. (2012) compared the profile of mildTBI, psychiatric and relationship status among all1764 suicides that occurred among serving mili-tary in the United States from 2001 to 2009 witha matched control group. The authors did not finda significantly higher rate of mild TBI among thesuicide group compared to the controls. This studyalso had a moderate risk of bias.
KQ1: Suicide Attempts
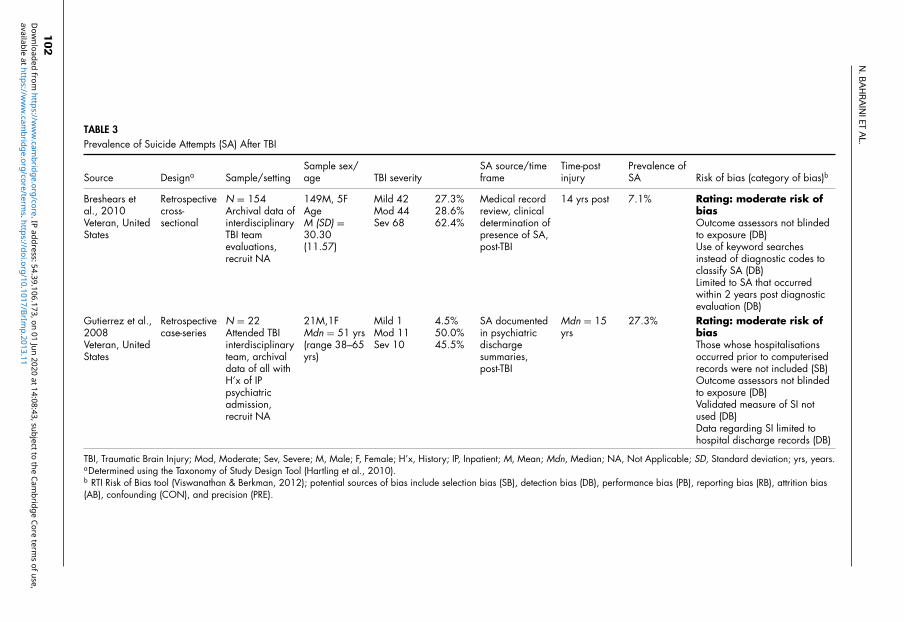
Two retrospective suicide-specific studies reportedthe prevalence of suicide attempts as an outcome(Table 3). Both studies conducted archival reviewsof the files of Veterans with mixed injury severity(mild to severe) in the chronic phase of TBI (14years, 15 years). Breshears, Brenner, Harwood andGutierrez (2010) found that 7.1% of their samplehad a post-injury history of a suicide attempt withinthe two-year study period, with almost half of theseindividuals having more than one event. Gutierrez,Brenner and Huggins (2008) identified a case seriesof 22 Veterans with TBI who had a post-injuryhistory of psychiatric inpatient admissions, witha file review finding reports of suicide attemptsamong 27.3% (6/22) of the sample. Both studieswere classified as having moderate risk of bias.
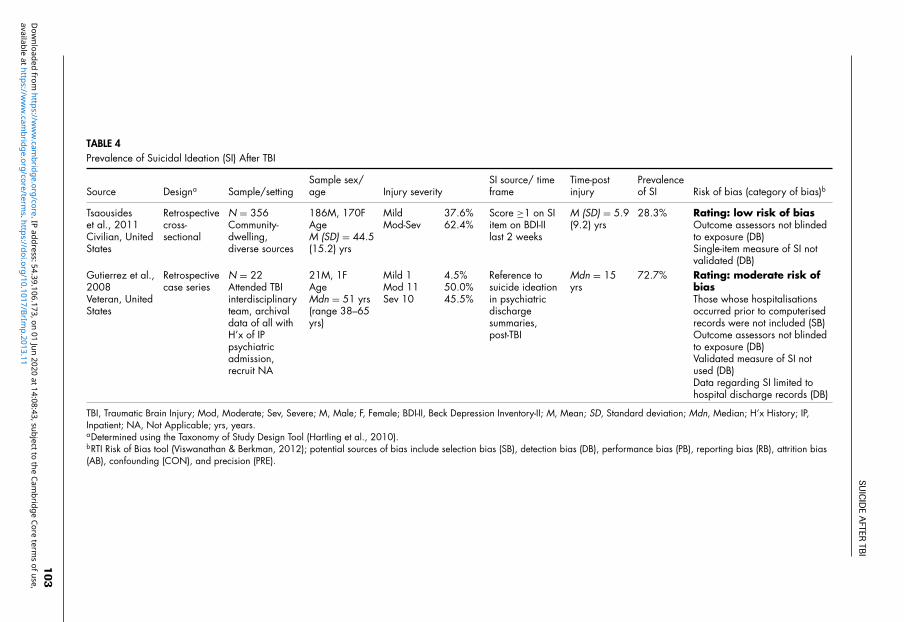
KQ1: Suicidal Ideation
Two retrospective single-centre studies reportedon the prevalence of suicide ideation as an out-come (Table 4). Both were suicide-specific stud-ies, addressing civilian (Tsaousides, Cantor, &
98
available at https://www.cambridge.org/core/terms. https://doi.org/10.1017/BrImp.2013.11Downloaded from https://www.cambridge.org/core. IP address: 54.39.106.173, on 01 Jun 2020 at 14:08:43, subject to the Cambridge Core terms of use,
SUICIDE AFTER TBI
Id
enti
fica
tion
Sc
reen
ing
n = 1172 records identified through database searching
EMBASE, n = 674 PubMed, n = 176 PsycINFO, n = 319 CENTRAL, n = 3
n = 15 additional records identified through other sources
From grey literature, n = 9 From contact with experts, n = 2 From reference lists, n = 4
n = 999 plus 15 additional = 1014 unique record abstracts screened after duplicates
removed EMBASE, n = 674 PubMed, n = 63 PsycINFO, n = 262 Other Source, n = 15
n = 173 duplicate records identified and removed leaving 999 unique records
PubMed, n = 113 PsycINFO, n = 57 CENTRAL, n = 3
n = 931 records excluded after preliminary screening of titles and abstracts
n = 83 full-text articles retrieved and assessed for
eligibility
n = 67 full text excluded n = 15 Not relevant (does not address TBI or key
questions) n = 33 Not suicide as an outcome n = 4 Child population or mixed with adult findings not reported separately n = 7 Dissertation, Commentary, Editorial, Review, Book/Chapter n = 6 Unclear if study population sustained TBI prior to experiencing suicide related outcomes n = 2 qualitative studies
n = 16 studies included in qualitative synthesis
n = 8 SA/SI n = 5 death
n = 3 treatment
Elig
ibili
ty
Incl
uded
FIGURE 1
Literature flow diagram.
Gordon, 2011) and Veteran (Guitierrez et al., 2008)samples. The first study, rated as having a lowrisk bias, found a 28.3% rate of suicide ideation(item nine on the BDI-II; Beck, Steer, & Brown,1996) over the previous two-week period among alarge sample of community-dwelling adults withTBI in the chronic phase post-injury. The sec-ond study (Gutierrez et al., 2008), rated as hav-ing a moderate risk of bias, found a prevalencerate of 72.7% among their sample of individuals
who also had a history of post-injury psychiatrichospitalisation.
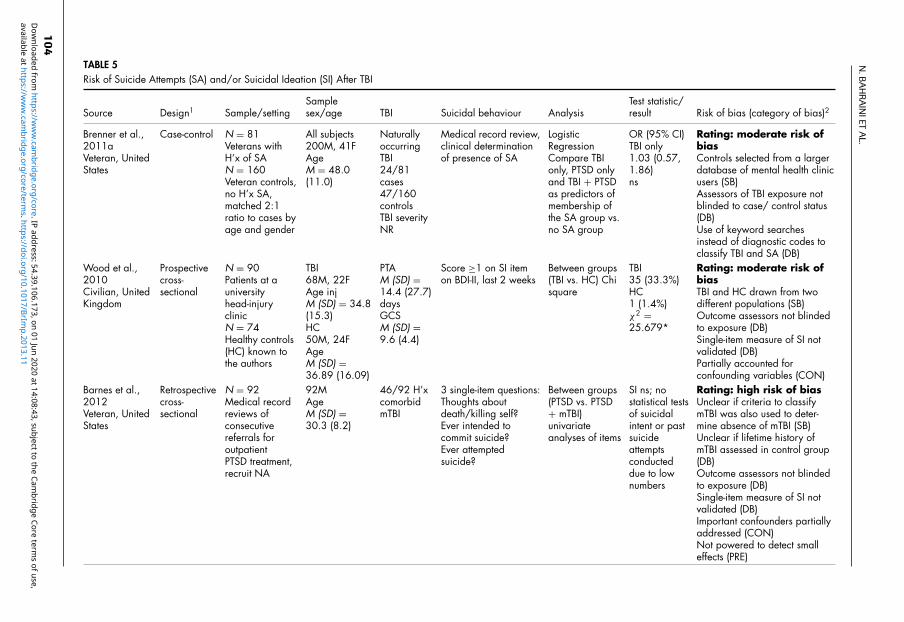
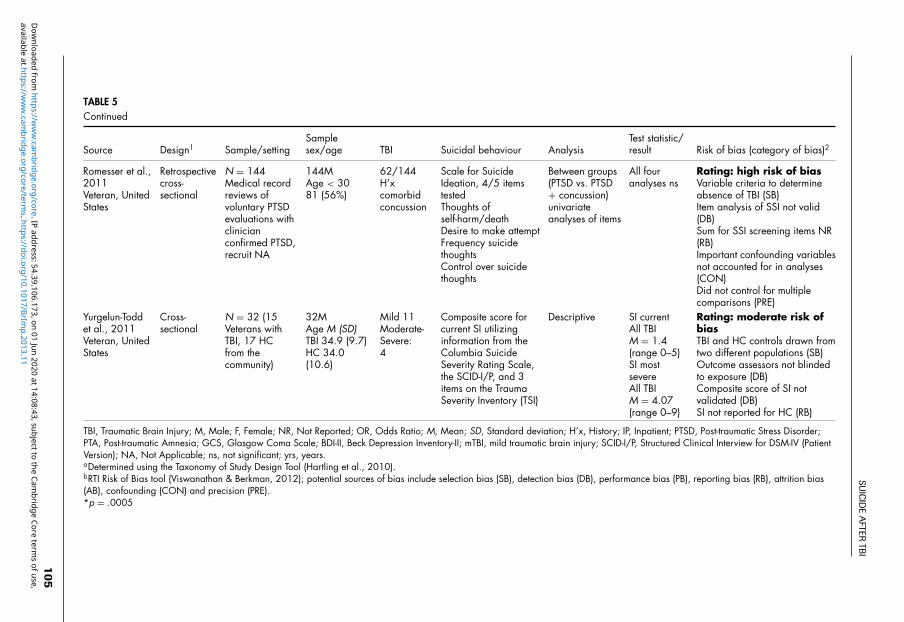
KQ1: Risk of Suicide Attempts and SuicidalIdeation after TBI
Five heterogeneous studies applied this questionto a diverse range of issues (Table 5). Two of thefive studies were rated as having a moderate riskof bias (Brenner et al., 2011a; Wood, Williams, &Lewis, 2010), with the remainder rated as having a
99
available at https://www.cambridge.org/core/terms. https://doi.org/10.1017/BrImp.2013.11Downloaded from https://www.cambridge.org/core. IP address: 54.39.106.173, on 01 Jun 2020 at 14:08:43, subject to the Cambridge Core terms of use,
N.B
AH
RA
INIET
AL.
TABLE 2Prevalence and Risk of Suicide After TBI
Source DesignaPopulation/sample
Studyadmission TBI
Referencepopulation
Prevalence ofsuicides
SMR or OR(95% CI) Risk of bias (category of bias)b
Brenner et al.,2011cVeteran, UnitedStates
Retrospectivecohort
N = 49,626All VHA userswith TBI
2001–2006,6 years
ConcussionContusion/TIH
12,15939,623
5% randomsample of VHAusers without TBIN = 389,583
105observed
All*1.55 (1.24,1.92)Mild**1.98 (1.39,2.82)Mod–Sev†1.34 (1.09,1.64)
Rating: low risk of biasOutcome assessors not blindedto exposure (DB)Use of ICD-10 less accurate forinjuries in which medicalattention was not sought (DB)
Harrison-Felixet al., 2009Civilian, UnitedStates
Retrospectivecohort
N = 1678Persons withTBI admitted toan adultrehabilitationhospital andsurvived >1year
1961–2003,40 years
Loss ofconscious-nessNone1 day2–7 days8–129 days
129495360568
Federal USmortality ratesby age, sex andrace
10 observed,3.39expected
Allc2.95 (1.42,5.43)
Rating: moderate risk ofbiasExternal comparison group notselected based on TBI status(SB & CON)Outcome assessors not blindedto exposure (DB)Cause of death unknown ormissing for 12 cases (AB)Presence of TBI in referencegroup (CON)
Himanen et al.,2011Civilian,Finland
Retrospectivecohort
N = 192All referrals forneurological orNP A’x at auniversityhospital
1950–1971,24–30 years
MildModerateSevereVery severe
6568535
Generalpopulation
3/75 deaths,4.2%
NR Rating: moderate risk ofbiasExternal comparison group notselected based on TBI status (SBand CON)Outcome assessors not blindedto exposure (DB)TBI severity not based onstandard criteria (DB)Validity and reliability of datasource for suicide is unclear (DB)Presence of TBI in referencegroup (CON)
100
available at https://ww
w.cam
bridge.org/core/terms. https://doi.org/10.1017/BrIm
p.2013.11D
ownloaded from
https://ww
w.cam
bridge.org/core. IP address: 54.39.106.173, on 01 Jun 2020 at 14:08:43, subject to the Cambridge Core term
s of use,
SUIC
IDE
AFTER
TBI
TABLE 2Continued
Source DesignaPopulation/sample
Studyadmission TBI
Referencepopulation
Prevalence ofsuicides
SMR or OR(95% CI) Risk of bias (category of bias)b
Mainio et al.,2007Civilian,Finland
Cross-sectional
N = 1877All generalpopulationsuicides insingle province
1988–2004,16 years
ConcussionLesiond
8320
Subset of 1877suicides with noidentified TBI
103/18775.5%
NA Rating: moderate risk ofbiasAssessors of TBI exposure notblinded to suicide (DB)TBI status was based on ICD-9codes for inpatient treatment orhospitalisation only (DB)mTBIs likely underrepresented ormisclassified (CON)
Skopp et al.,2012Militarypersonnel,United States
Case control N = 1764All generalpopulationsuicides in USmilitary activeservice
2001–2009 MildModerateSevereUnclassified
972552
Randomselection,matched 4:1ratio to cases byservice, gender,race, age, dateof entry activeservice, length ofmilitary service
129/17647.3%
Mild (OR)1.1 (0.88,1.42)
Rating: moderate risk ofbiasAssessors of TBI exposure notblinded to case/ control status(DB)Use of ICD-10 less accurate forinjuries in which medicalattention was not sought (DB)Risk for moderate to severe TBInot reported due to limitedcases; only mTBI analysed andreported (RB and PRE)Differences in length of timefrom injury to death notaddressed (CON)
SMR, Standardized Mortality Ratio; OR, Odds Ratio; CI, Confidence Interval; VHA, Veterans Health Administration; TBI, Traumatic Brain Injury; TIH, Traumatic Intracranial Haemorrhage;Mod, Moderate; Sev, Severe; ICD-10, International Statistical Classification of Diseases-10; NP A’x, Neuropsychological Assessment; NR, Not Reported; NA, Not Applicable.aDetermined using the Taxonomy of Study Design Tool (Hartling et al., 2010).bRTI Risk of Bias tool (Viswanathan & Berkman, 2012); potential sources of bias include selection bias (SB), detection bias (DB), performance bias (PB), reporting bias (RB), attrition bias(AB), confounding (CON) and precision (PRE).cSMR reported as statistically significant but p value not provided.dInjuries classified as lesions included cerebral contusion and intracranial haemorrhage.*p <.0001, adjusted model. **p = .0002, adjusted model. †p = .006, adjusted model.
101
available at https://ww
w.cam
bridge.org/core/terms. https://doi.org/10.1017/BrIm
p.2013.11D
ownloaded from
https://ww
w.cam
bridge.org/core. IP address: 54.39.106.173, on 01 Jun 2020 at 14:08:43, subject to the Cambridge Core term
s of use,
N.B
AH
RA
INIET
AL.
TABLE 3Prevalence of Suicide Attempts (SA) After TBI
Source Designa Sample/settingSample sex/age TBI severity
SA source/timeframe
Time-postinjury
Prevalence ofSA Risk of bias (category of bias)b
Breshears etal., 2010Veteran, UnitedStates
Retrospectivecross-sectional
N = 154Archival data ofinterdisciplinaryTBI teamevaluations,recruit NA
149M, 5FAgeM (SD) =30.30(11.57)
Mild 42Mod 44Sev 68
27.3%28.6%62.4%
Medical recordreview, clinicaldetermination ofpresence of SA,post-TBI
14 yrs post 7.1% Rating: moderate risk ofbiasOutcome assessors not blindedto exposure (DB)Use of keyword searchesinstead of diagnostic codes toclassify SA (DB)Limited to SA that occurredwithin 2 years post diagnosticevaluation (DB)
Gutierrez et al.,2008Veteran, UnitedStates
Retrospectivecase-series
N = 22Attended TBIinterdisciplinaryteam, archivaldata of all withH’x of IPpsychiatricadmission,recruit NA
21M,1FMdn = 51 yrs(range 38–65yrs)
Mild 1Mod 11Sev 10
4.5%50.0%45.5%
SA documentedin psychiatricdischargesummaries,post-TBI
Mdn = 15yrs
27.3% Rating: moderate risk ofbiasThose whose hospitalisationsoccurred prior to computerisedrecords were not included (SB)Outcome assessors not blindedto exposure (DB)Validated measure of SI notused (DB)Data regarding SI limited tohospital discharge records (DB)
TBI, Traumatic Brain Injury; Mod, Moderate; Sev, Severe; M, Male; F, Female; H’x, History; IP, Inpatient; M, Mean; Mdn, Median; NA, Not Applicable; SD, Standard deviation; yrs, years.aDetermined using the Taxonomy of Study Design Tool (Hartling et al., 2010).b RTI Risk of Bias tool (Viswanathan & Berkman, 2012); potential sources of bias include selection bias (SB), detection bias (DB), performance bias (PB), reporting bias (RB), attrition bias(AB), confounding (CON), and precision (PRE).
102
available at https://ww
w.cam
bridge.org/core/terms. https://doi.org/10.1017/BrIm
p.2013.11D
ownloaded from
https://ww
w.cam
bridge.org/core. IP address: 54.39.106.173, on 01 Jun 2020 at 14:08:43, subject to the Cambridge Core term
s of use,
SUIC
IDE
AFTER
TBI
TABLE 4Prevalence of Suicidal Ideation (SI) After TBI
Source Designa Sample/settingSample sex/age Injury severity
SI source/ timeframe
Time-postinjury
Prevalenceof SI Risk of bias (category of bias)b
Tsaousideset al., 2011Civilian, UnitedStates
Retrospectivecross-sectional
N = 356Community-dwelling,diverse sources
186M, 170FAgeM (SD) = 44.5(15.2) yrs
MildMod-Sev
37.6%62.4%
Score ≥1 on SIitem on BDI-IIlast 2 weeks
M (SD) = 5.9(9.2) yrs
28.3% Rating: low risk of biasOutcome assessors not blindedto exposure (DB)Single-item measure of SI notvalidated (DB)
Gutierrez et al.,2008Veteran, UnitedStates
Retrospectivecase series
N = 22Attended TBIinterdisciplinaryteam, archivaldata of all withH’x of IPpsychiatricadmission,recruit NA
21M, 1FAgeMdn = 51 yrs(range 38–65yrs)
Mild 1Mod 11Sev 10
4.5%50.0%45.5%
Reference tosuicide ideationin psychiatricdischargesummaries,post-TBI
Mdn = 15yrs
72.7% Rating: moderate risk ofbiasThose whose hospitalisationsoccurred prior to computerisedrecords were not included (SB)Outcome assessors not blindedto exposure (DB)Validated measure of SI notused (DB)Data regarding SI limited tohospital discharge records (DB)
TBI, Traumatic Brain Injury; Mod, Moderate; Sev, Severe; M, Male; F, Female; BDI-II, Beck Depression Inventory-II; M, Mean; SD, Standard deviation; Mdn, Median; H’x History; IP,Inpatient; NA, Not Applicable; yrs, years.aDetermined using the Taxonomy of Study Design Tool (Hartling et al., 2010).bRTI Risk of Bias tool (Viswanathan & Berkman, 2012); potential sources of bias include selection bias (SB), detection bias (DB), performance bias (PB), reporting bias (RB), attrition bias(AB), confounding (CON), and precision (PRE).
103
available at https://ww
w.cam
bridge.org/core/terms. https://doi.org/10.1017/BrIm
p.2013.11D
ownloaded from
https://ww
w.cam
bridge.org/core. IP address: 54.39.106.173, on 01 Jun 2020 at 14:08:43, subject to the Cambridge Core term
s of use,
N.B
AH
RA
INIET
AL.
TABLE 5Risk of Suicide Attempts (SA) and/or Suicidal Ideation (SI) After TBI
Source Design1 Sample/settingSamplesex/age TBI Suicidal behaviour Analysis
Test statistic/result Risk of bias (category of bias)2
Brenner et al.,2011aVeteran, UnitedStates
Case-control N = 81Veterans withH’x of SAN = 160Veteran controls,no H’x SA,matched 2:1ratio to cases byage and gender
All subjects200M, 41FAgeM = 48.0(11.0)
NaturallyoccurringTBI24/81cases47/160controlsTBI severityNR
Medical record review,clinical determinationof presence of SA
LogisticRegressionCompare TBIonly, PTSD onlyand TBI + PTSDas predictors ofmembership ofthe SA group vs.no SA group
OR (95% CI)TBI only1.03 (0.57,1.86)ns
Rating: moderate risk ofbiasControls selected from a largerdatabase of mental health clinicusers (SB)Assessors of TBI exposure notblinded to case/ control status(DB)Use of keyword searchesinstead of diagnostic codes toclassify TBI and SA (DB)
Wood et al.,2010Civilian, UnitedKingdom
Prospectivecross-sectional
N = 90Patients at auniversityhead-injuryclinicN = 74Healthy controls(HC) known tothe authors
TBI68M, 22FAge injM (SD) = 34.8(15.3)HC50M, 24FAgeM (SD) =36.89 (16.09)
PTAM (SD) =14.4 (27.7)daysGCSM (SD) =9.6 (4.4)
Score ≥1 on SI itemon BDI-II, last 2 weeks
Between groups(TBI vs. HC) Chisquare
TBI35 (33.3%)HC1 (1.4%)χ2 =25.679*
Rating: moderate risk ofbiasTBI and HC drawn from twodifferent populations (SB)Outcome assessors not blindedto exposure (DB)Single-item measure of SI notvalidated (DB)Partially accounted forconfounding variables (CON)
Barnes et al.,2012Veteran, UnitedStates
Retrospectivecross-sectional
N = 92Medical recordreviews ofconsecutivereferrals foroutpatientPTSD treatment,recruit NA
92MAgeM (SD) =30.3 (8.2)
46/92 H’xcomorbidmTBI
3 single-item questions:Thoughts aboutdeath/killing self?Ever intended tocommit suicide?Ever attemptedsuicide?
Between groups(PTSD vs. PTSD+ mTBI)univariateanalyses of items
SI ns; nostatistical testsof suicidalintent or pastsuicideattemptsconducteddue to lownumbers
Rating: high risk of biasUnclear if criteria to classifymTBI was also used to deter-mine absence of mTBI (SB)Unclear if lifetime history ofmTBI assessed in control group(DB)Outcome assessors not blindedto exposure (DB)Single-item measure of SI notvalidated (DB)Important confounders partiallyaddressed (CON)Not powered to detect smalleffects (PRE)
104
available at https://ww
w.cam
bridge.org/core/terms. https://doi.org/10.1017/BrIm
p.2013.11D
ownloaded from
https://ww
w.cam
bridge.org/core. IP address: 54.39.106.173, on 01 Jun 2020 at 14:08:43, subject to the Cambridge Core term
s of use,
SUIC
IDE
AFTER
TBI
TABLE 5Continued
Source Design1 Sample/settingSamplesex/age TBI Suicidal behaviour Analysis
Test statistic/result Risk of bias (category of bias)2
Romesser et al.,2011Veteran, UnitedStates
Retrospectivecross-sectional
N = 144Medical recordreviews ofvoluntary PTSDevaluations withclinicianconfirmed PTSD,recruit NA
144MAge < 3081 (56%)
62/144H’xcomorbidconcussion
Scale for SuicideIdeation, 4/5 itemstestedThoughts ofself-harm/deathDesire to make attemptFrequency suicidethoughtsControl over suicidethoughts
Between groups(PTSD vs. PTSD+ concussion)univariateanalyses of items
All fouranalyses ns
Rating: high risk of biasVariable criteria to determineabsence of TBI (SB)Item analysis of SSI not valid(DB)Sum for SSI screening items NR(RB)Important confounding variablesnot accounted for in analyses(CON)Did not control for multiplecomparisons (PRE)
Yurgelun-Toddet al., 2011Veteran, UnitedStates
Cross-sectional
N = 32 (15Veterans withTBI, 17 HCfrom thecommunity)
32MAge M (SD)TBI 34.9 (9.7)HC 34.0(10.6)
Mild 11Moderate-Severe:4
Composite score forcurrent SI utilizinginformation from theColumbia SuicideSeverity Rating Scale,the SCID-I/P, and 3items on the TraumaSeverity Inventory (TSI)
Descriptive SI currentAll TBIM = 1.4(range 0–5)SI mostsevereAll TBIM = 4.07(range 0–9)
Rating: moderate risk ofbiasTBI and HC controls drawn fromtwo different populations (SB)Outcome assessors not blindedto exposure (DB)Composite score of SI notvalidated (DB)SI not reported for HC (RB)
TBI, Traumatic Brain Injury; M, Male; F, Female; NR, Not Reported; OR, Odds Ratio; M, Mean; SD, Standard deviation; H’x, History; IP, Inpatient; PTSD, Post-traumatic Stress Disorder;PTA, Post-traumatic Amnesia; GCS, Glasgow Coma Scale; BDI-II, Beck Depression Inventory-II; mTBI, mild traumatic brain injury; SCID-I/P, Structured Clinical Interview for DSM-IV (PatientVersion); NA, Not Applicable; ns, not significant; yrs, years.aDetermined using the Taxonomy of Study Design Tool (Hartling et al., 2010).bRTI Risk of Bias tool (Viswanathan & Berkman, 2012); potential sources of bias include selection bias (SB), detection bias (DB), performance bias (PB), reporting bias (RB), attrition bias(AB), confounding (CON) and precision (PRE).*p = .0005
105
available at https://ww
w.cam
bridge.org/core/terms. https://doi.org/10.1017/BrIm
p.2013.11D
ownloaded from
https://ww
w.cam
bridge.org/core. IP address: 54.39.106.173, on 01 Jun 2020 at 14:08:43, subject to the Cambridge Core term
s of use,
N.B
AH
RA
INIET
AL.
TABLE 6Treatment Studies
Source Designa Sample, setting Sex, age
Injuryseverity/timepost-injury
Primary outcome,intervention
Measure ofsuicide ideation(SI)
Attrition, T’xOutcome Risk of Bias (category of bias)b
Simpson et al.,2011Civilian,Australia
RCT N = 17,Brain injurycommunityrehabilitationservice
16M,1FAgeM (SD) = 39.7(19)
Sev 17M (SD) yrs6.3(6.8) T’X7.6 (4.6)waitlist
Hopelessness,Beck HopelessnessScale20-h manualisedGroup CBTprogramme, 20hours
SecondaryoutcomeBeck Scale forSuicide Ideationrange 0–38
16 completeT’x,T’x gp n = 8M (SD)7.8 (10.7)Pre-T’x5.1(8.9)Post-T’xNS repeatedmeasuresanalysis
Rating: low risk of biasPEDro Rating: 8/10Therapists and patients notblinded to treatment condition(DB)Small sample limited power todetect treatment effect for SI(PREC)
Rapoport et al,2008Civilian,Canada
Before–AfterStudy
N = 65Mild–moderateTBI clinic,tertiary traumacare centre
38M, 27FAgeM (SD) =39.7 (19)
Mild 33Mod-Sev 32,timepost-injuryNR
DepressionFirst wave, n = 29fixed dosecitalopram, 20mg/day, 6 weeksSecond wave, n =36flexible dosecitalopram,Start 20 mg/day,titrating to max. 50mg/day, 10 wks
Secondaryoutcomesuicide ideationitem, HamiltonDepressionScale, range NR
54 complete 6wks of T’x,Specificsuicideideationvalues NR
Rating: unclear risk of biasOutcome assessors not blinded tointervention (DB)Single-item measure of SI notvalidated (DB)Numeric values for SI notreported (RB)Impact of loss to follow-up notassessed (AB)Partially accounted for importantconfounders (CON)
Rees & Bellon,2007Civilian,Australia
Before–AfterStudy
N = 20,Brain injurycommunityrehabilitationservice, 20% ofadmitted clientsover previous 10yrs
10M, 10FAgeM (SD) =31.2 (11.2)
PostConcussionSyndrome,GCS 13–15Ranchos LosAmigos scale5–7,timepost-injuryNR
Post ConcussionSyndrome symptoms(NSI)Individualclient-centredcounselling + CBT,minimum 62 h over 2yrs
SecondaryoutcomeSuicide ideationitem, BeckDepressionInventory-II,range NR
20 completeT’x,Yr 1 0.8 ±0.6Yr 2 0.3 ±0.6,Paired t-tests t= 3.9*
Rating: high risk of biasUnclear if eligibility criteria wasuniformly applied across patients(SB)Outcome assessors not blinded tointervention (DB)Single item measure of SI notvalidated (DB)Important aspects of theintervention not described (PB)
106
available at https://ww
w.cam
bridge.org/core/terms. https://doi.org/10.1017/BrIm
p.2013.11D
ownloaded from
https://ww
w.cam
bridge.org/core. IP address: 54.39.106.173, on 01 Jun 2020 at 14:08:43, subject to the Cambridge Core term
s of use,

SUICIDE AFTER TBI
TABL
E6
Con
tinue
d
Sour
ceD
esig
naSa
mpl
e,se
tting
Sex,
age
Inju
ryse
verit
y/tim
epo
st-in
jury
Prim
ary
outc
ome,
inte
rven
tion
Mea
sure
ofsu
icid
eid
eatio
n(S
I)A
ttriti
on,T
’xO
utco
me
Risk
ofBi
as(c
ateg
ory
ofbi
as)b
Har
ms/
adve
rse
even
tsre
late
dto
the
inte
rven
tion
notr
epor
ted
(RB)
Impo
rtant
conf
ound
ers
not
acco
unte
dfo
r(C
ON
)Sm
alls
ampl
esi
ze;d
idno
tadj
ustf
orm
ultip
leco
mpa
rison
s(P
RE)
RCT,
Rand
omis
edC
ontro
lled
Tria
l;M
od,M
oder
ate;
Sev,
Seve
re;M
,Mal
e;F,
Fem
ale;
yrs,
year
s;w
ks,w
eeks
.T’x
,Tre
atm
ent;
GC
S,G
lasg
owC
oma
Scal
e;N
R,N
otRe
porte
d;C
BT,
Cog
nitiv
eBe
havi
orTh
erap
y;m
g,m
illig
ram
;NSI
,Neu
robe
havi
oral
Sym
ptom
Inve
ntor
y;N
S,no
tsig
nific
ant.
aD
eter
min
edus
ing
the
Taxo
nom
yof
Stud
yD
esig
nto
ol(H
artli
nget
al.,
2010
).bRT
IRis
kof
Bias
tool
(Vis
wan
atha
n&
Berk
man
,201
2);p
oten
tials
ourc
esof
bias
incl
ude
sele
ctio
nbi
as(S
B),d
etec
tion
bias
(DB)
,per
form
ance
bias
(PB)
,rep
ortin
gbi
as(R
B),a
ttriti
onbi
as(A
B),c
onfo
undi
ng(C
ON
),an
dpr
ecis
ion
(PRE
).*
p<.0
5
high risk of bias. In a controlled prospective cross-sectional suicide-specific study, Wood et al. (2010)reported a 33.3% rate of suicide ideation (item nineon the BDI-II; Beck et al., 1996) among 90 patientsof mixed injury severity. This rate was significantlygreater than that reported by a matched comparisongroup of healthy controls.
Three studies examined the relationship be-tween post-traumatic stress disorder (PTSD), TBIor mild TBI and suicide risk in US Veteran sam-ples. In an archival case-controlled study (mod-erate risk of bias), Brenner et al. (2011a) exam-ined a sample of Veterans with a history of suicideattempts, and compared them to a matched con-trol group with no such history. The naturally oc-curring proportion of Veterans with TBI in bothgroups was high, virtually identical at approxi-mately 30%. In a series of logistic regressions,the relative association of PTSD versus TBI wastested, finding that while a history of PTSD was as-sociated with an increased risk for having a historyof suicide attempts, a similar relationship was notfound for TBI. Two other studies (Barnes, Walter,& Chard, 2012; Romesser et al., 2011; both highrisk of bias) examined whether a comorbid mildTBI among Veterans with PTSD played an addi-tive role, increasing the likelihood of suicidal be-haviours, compared to Veterans with PTSD alone.Both studies reported non-significant results. Theaim of the final study (Yurgelun-Todd et al., 2011)was to examine the relationship between frontalwhite matter systems and measures of impulsivityand suicidality in Veterans with TBI. Descriptivedata regarding SI were also reported. Risk of biaswas moderate.
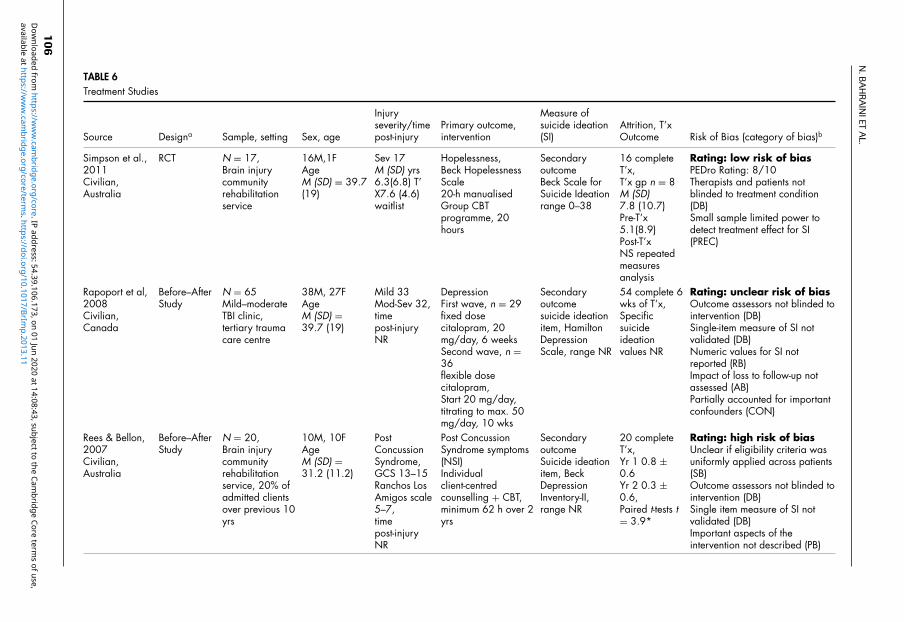
KQ2: Interventions for Reducing Suicide-related Outcomes in Persons with TBI
Three treatment studies (two psychosocial, onepharmacological) were identified in which suicideideation was an outcome (Table 6). However, sui-cide ideation was not the primary target of any ofthe three treatments. One study specifically aimedto reduce suicide risk by treating hopelessness. Itwas the only study which tested an a priori hy-pothesis pertaining to suicide ideation. The study’sprimary hypothesis was that a psychological treat-ment would reduce hopelessness after severe TBI(primary outcome). The study also hypothesisedthat this reduction in hopelessness would be asso-ciated with a related reduction in suicide ideation(a secondary outcome), due to the intercorrelationbetween the two clinical phenomena. This hypoth-esis was tested in a RCT (Simpson, Tate, Whit-ing, & Cotter, 2011; low risk of bias). Althoughthe suicide ideation scores decreased from pre- topost-intervention among the treatment group while
107
available at https://www.cambridge.org/core/terms. https://doi.org/10.1017/BrImp.2013.11Downloaded from https://www.cambridge.org/core. IP address: 54.39.106.173, on 01 Jun 2020 at 14:08:43, subject to the Cambridge Core terms of use,

N. BAHRAINI ET AL.
scores of the waiting list group members increased(suggesting increased ideation), these trends werenon-significant.
The other two studies were rated as an un-clear risk (Rapoport et al., 2008) and high riskof bias (Rees & Bellon, 2007). In both studies,changes in suicidal ideation were incidental to theprimary treatment target (depression, Rapoport etal., 2008; post-concussional symptoms, Rees &Bellon, 2007) and were reported along with othersymptoms on depression measures.
DiscussionThe World Health Organisation asserts that suicideis preventable (World Health Organisation, 2012).One application of this principle at an organisa-tional level is to ensure that sufficient knowledgeregarding those at risk is available to guide resourceallocation (e.g., research, clinical). The current re-view identified 16 studies that addressed the issueof suicide after TBI, of which three had a low riskof bias. These three studies investigated differentindicators of self-directed violence among thosewith TBI as their primary aim. Two of the stud-ies addressed the associations between TBI andsuicide deaths (Brenner et al., 2011c) or suicidalideation (Tsaousides et al., 2011). The third was anRCT of a suicide prevention treatment (Simpsonet al., 2011). Nine of the remaining studies weredetermined to have a moderate risk of bias, withthe final four being rated as having high or unclearlevels of bias.
The review found new robust evidence of theassociation between TBI and elevated risk of sui-cide. The report by Brenner et al. (2011c) was thefirst suicide-specific study among Veterans withTBI since Achte, Lonnqvist and Hillbom’s (1971)seminal work reporting on Second World War Fin-ish Veterans. This elevated rate among Veteranswas also reported in the meta-analysis by Harrisand Barraclough (1997) and complements the find-ings from the civilian population study by Teas-dale and Engberg (2001). The elevated rate of sui-cide was also found in a single-centre study in-vestigating mortality among a rehabilitation cohort(Harrison-Felix et al., 2009; moderate risk of bias).
These two positive findings contribute to thedebate about whether there is an elevated riskof suicide after TBI. Some studies have notfound a significant association (e.g., Harrison-Felix, Whiteneck, DeVivo, Hammond, & Jha,2004; Lewin et al., 1979; Shavelle et al., 2001).However, Harrison-Felix et al. (2004) have raisedthe issue that findings based on small numbersof suicides (e.g., one or two) need to be viewedwith caution because the corresponding standard-
ised mortality ratios are too unstable. Given thelow base rate of suicide (typically 1–2 per 10,000),studies investigating death by suicide need to beadequately powered. As such, large-scale studiesare required to address meaningfully this question.Interestingly, the large-scale studies conducted todate have all found evidence of increased suiciderisk.
In addition to issues of statistical power, selec-tion of an appropriate comparison group is one ofthe most critical aspects in the design of a cohortstudy. Understanding the true effect of TBI on sui-cidal outcomes requires selection of a comparisongroup that is similar to the exposed TBI cohort onall important characteristics except for TBI status.Of the three retrospective cohort studies, only one(Brenner et al., 2011c) used a comparison groupof persons without a history of TBI that were se-lected from the same source population as thosewith TBI, while the other two (Harrison-Felix etal., 2009; Himanen et al., 2011) relied on externalcomparison groups (i.e., general population rates)to examine the effect of TBI on overall mortality ordeath by suicide. Although convenient, use of ex-ternal comparison groups limits understanding ofthe true effects of TBI on suicide outcomes. Evenif the general population is chosen to be as similaras possible to the TBI cohort in relation to basicdemographic and geographic variables, presenceof TBI and other unidentified risk factors in thecomparison group may lead to either an underesti-mation or overestimation of its true effect.
Despite the upsurge of research activity in thearea of TBI and suicide in the past 5 years, therecontinues to be a dearth of quality research exam-ining the prevalence of suicidal ideation and at-tempts among those with TBI. Most notably, sincethe first review (Simpson & Tate, 2007), no newpopulation-level studies investigating ideation orattempts among those with TBI were identified. Atthe level of clinical studies, the 28.3% prevalencerate of suicide ideation found by Tsaousides et al.(2011; low risk of bias) was similar to rates re-ported in the three studies identified in the 2007review. Together, the four studies all highlight sig-nificant levels of suicide ideation present in thechronic phase post-TBI. The one study employ-ing a non-brain-damaged (healthy) control groupfound that the rate of suicide ideation among peo-ple with TBI was significantly higher (Wood et al.,2010; moderate risk of bias).
A new development in this review was theemergence of studies that examined whether theincreased risk of suicide identified in TBI sam-ples/populations could be detected among thegeneral population or other clinical groups (i.e.,PTSD). Two studies examined suicide deaths
108
available at https://www.cambridge.org/core/terms. https://doi.org/10.1017/BrImp.2013.11Downloaded from https://www.cambridge.org/core. IP address: 54.39.106.173, on 01 Jun 2020 at 14:08:43, subject to the Cambridge Core terms of use,

SUICIDE AFTER TBI
(Skopp et al., 2012) and suicide attempts (Brenneret al., 2011a) among active duty and Veteran pop-ulations. Using a case-control methodology (sui-cidal behaviour present versus absent), they inves-tigated whether a greater proportion of cases inthe suicide-present groups had a history of TBI.Neither of these studies found that TBI was a sig-nificant risk factor. Similarly, the two studies whichexamined whether the presence of co-morbid TBIin Veterans with PTSD added to the level of suici-dal ideation (Barnes et al., 2012; Romesser et al.,2011) were also non-significant. Potential reasonsfor these non-significant findings include study de-sign, the low-base rate of suicidal behaviour, smallsample sizes, and/or dependence on chart reviewfor data regarding exposure (TBI) and outcomes(suicidal thoughts or behaviours).
The review identified one RCT (Simpsonet al., 2011), a psychological treatment for hope-lessness among people with severe TBI. Althoughthe intervention did not directly target a suicidal be-haviour, hopelessness is one of the strongest pre-dictors of suicide and is closely correlated withsuicide ideation. Despite this advance, the treat-ment still requires replication in larger trials ofhigh-quality design.
Overall, the studies displaying moderate orhigh risk of bias varied significantly in terms ofmethodology and assessment of TBI. Many didnot use psychometrically sound tools to measureoutcomes of interest. Few studies adjusted the re-sults for the most important potential confoundingfactors (i.e., age and gender) contributing to sig-nificant sources of bias. The variability noted interms of both exposure and case ascertainment ofTBI and controls further calls into question thestrength of existing evidence. Moreover, few newstudies were identified wherein suicidal ideation,attempts or death were examined as primary out-comes in TBI-specific samples designed to addressthe association between TBI exposure and suicidaloutcomes. Some of the studies reviewed were no-table for their poor reporting of methods and pro-cedures. This lack of transparency made it difficultto rate bias and/or to determine the strength ofthe existing evidence pertaining to Key Questions1 and 2. As such, researchers are encouraged tofollow reporting guidelines specific to their studydesign (e.g., STROBE (von Elm et al., 2008) forobservational studies).
Some limitations of this review should be con-sidered in interpreting the results. Three additionalstudies addressing TBI and suicide were identified;however, they did not meet review inclusion crite-ria (McMillan & Teasdale, 2007; McMillan, Teas-dale, Weir, & Stewart, 2011; Ventura et al., 2010).In all three, findings regarding those younger than
age 18 were mixed with adult data; thereby pre-cluding separate evaluation regarding the results ofinterest. An inherent limitation of such high speci-ficity is the possibility of excluding quality studiesthat do not fit within the predetermined parame-ters, but may otherwise be important contributionsto the body of evidence. Additionally, it is impor-tant to note that two of the authors of the currentreview were also authors on 6 of the 16 papers re-viewed. As such, various procedures were imple-mented throughout the systematic review processto reduce biases and ensure objectivity when criti-cally appraising studies. Furthermore, individualswere not primarily responsible for review of thearticles on which they were authors.
Findings from this review highlight the needfor further research to establish the prevalence of SIand SA among those with a history of TBI. Under-standing the true prevalence of these outcomes inTBI populations will support validation of suicide-related outcome measures, and ultimately allow foraccurate assessment of change in interventional tri-als. Moreover, knowledge regarding the prevalenceof SI and SA will highlight the resources needed tocare for members of this population who, accord-ing to the data, are at risk of dying by suicide.
Although the question of increased risk ofsuicide-related outcomes following TBI was ad-dressed in the current review, specific factors thatcontribute to increased risk of these outcomes werenot examined. Future systematic reviews are alsoneeded to clarify the existing evidence regardingrisk and protective factors, as well as warning signsfor suicidal thoughts and behaviours among thosewith TBI. In addition, no reviews have been com-pleted in the aim of establishing evidence-basedassessment strategies regarding suicide risk.
Research examining the impact of TBI sever-ity on suicide risk is another area that warrantsfurther investigation. Although studies have shownan increased risk of suicide across all levels of TBIseverity, the extent to which TBI severity influ-ences the pathway to suicidal behaviour or the tra-jectory of risk has yet to be examined extensively.Along these lines, research examining neurobio-logical correlates and markers of suicide-relatedoutcome among TBI survivors (e.g., Yurgelun-Todd et al., 2011), and the influence of TBI severityon such markers, represent an emerging area of re-search that holds great potential for advancing thefield.
ReferencesAchte, K.A., Lonnqvist, J., & Hillbom, E. (1971). Sui-
cides following war brain injuries. Acta PsychiatricaScandinavica. Supplementum, 225, 1–94.
109
available at https://www.cambridge.org/core/terms. https://doi.org/10.1017/BrImp.2013.11Downloaded from https://www.cambridge.org/core. IP address: 54.39.106.173, on 01 Jun 2020 at 14:08:43, subject to the Cambridge Core terms of use,
N. BAHRAINI ET AL.
Anstey, K., Butterworth, P., Jorm, A.F., Chistensen, H.,Rodgers, B., & Windsor, T.D. (2004). A popula-tion survey found an association between self-reportsof traumatic brain injury and increased psychiatricsymptoms. Journal of Clinical Epidemiology, 57,1202–1209.
Barnes, S.M., Walter, K.H., & Chard, K.M. (2012). Doesa history of mild traumatic brain injury increase sui-cide risk in Veterans with PTSD? Rehabilitation Psy-chology, 57(1), 18–26.
Beck, A.T., Steer, R.A., & Brown, G.K. (1996). Manualfor the Beck Depression Inventory-II. San Antonio,TX: Psychological Corporation.
Brenner, L.A., Betthauser, L.M., Homaifar, B.Y.,Villarreal, E., Harwood, J.E., Staves, P.J., . . . Hug-gins, J.A. (2011a). Posttraumatic stress disorder,traumatic brain injury, and suicide attempt historyamong Veterans receiving mental health services.Suicide amd Life Threatening Behavior, 41, 416–423.
Brenner, L.A., Breshears, R.E., Betthauser, L.M., Bellon,K.K., Holman, E., Harwood, J.E., . . . Nagamoto,H.T. (2011b). Implementation of a suicide nomen-clature within two VA healthcare settings. Journalof Clinical Psychology in Medical Settings, 18(2),116–128.
Brenner, L.A., Ignacio, R.V., & Blow, F.C. (2011c).Suicide and traumatic brain injury among individu-als seeking Veterans Health Administration services.Journal of Head Trauma Rehabilitation, 26(4), 257–264.
Brenner, L.A., Vanderploeg, R.D., & Terrio, H. (2009).Assessment and diagnosis of mild traumatic braininjury, posttraumatic stress disorder, and other poly-trauma conditions: Burden of adversity hypothesis.Rehabilitation Psychology, 54, 239–246.
Breshears, R.E., Brenner, L.A., Harwood, J.E.F., &Gutierrez, P.M. (2010). Predicting suicidal behaviorin Veterans with traumatic brain injury: The utilityof the Personality Assessment Inventory. Journal ofPersonality Assessment, 92, 349–355.
Carroll, L.J., Cassidy, J.D., Holm, L., Kraus, J., &Coronado, V.G. (2004). Methodological issues andresearch recommendations for mild traumatic braininjury: The WHO Collaborating Centre Task Forceon mild traumatic brain injury [Supplemental mate-rial]. Journal of Rehabilitation Medicine, 43, 113–125.
Centers for Disease Control and Prevention. (2012). Sui-cide mortality. National Vital Statistics System. Re-trieved from http://www.cdc.gov/nchs/pressroom/states/SUICIDE_STATE_2010.pdf
deMorton, N.A. (2009). The PEDro scale is a valid mea-sure of the methodological quality of clinical trials:A demographic study. Australian Journal of Physio-therapy, 55, 129–133.
Gutierrez, P.M., Brenner, L.A., & Huggins, J.A. (2008).A preliminary investigation of suicidality in psychi-atrically hospitalized Veterans with traumatic braininjury. Archives of Suicide Research, 12(4), 336–343.
Harris, C., & Barraclough, B. (1997). Suicide as an out-come for mental disorders. British Journal of Psy-chiatry, 170, 205–228.
Harrison-Felix, C., Whiteneck, G., DeVivo, M.,Hammond, F.M., & Jha, A. (2004). Mortality fol-lowing rehabilitation in the Traumatic Brain InjuryModel Systems of Care. NeuroRehabilitation, 19,45–54.
Harrison-Felix, C., Whiteneck, G., DeVivo, M., Ham-mond, F.M., & Jha, A. (2006). Causes of death fol-lowing 1 year postinjury among individuals withtraumatic brain injury. Journal of Head Trauma Re-habilitation, 21, 22–33.
Harrison-Felix, C.L., Whiteneck, G.G., Jha, A.,DeVivo, M.J., Hammond, F.M., & Hart, D.M.(2009). Mortality over four decades after traumaticbrain injury rehabilitation: A retrospective cohortstudy. Archives of Physical Medicine and Rehabili-tation, 90(9), 1506–1513.
Hartling, L., Bond, K., Harvey, K., Santaguida, P.L.,Viswananthan, M., & Dryden, D.M. (2010). Meth-ods Research Report: Developing and testing a toolfor the classification of study designs in systematicreviews of interventions and exposures (Agency forHealthcare Research and Quality Publication No.11-EHC-007). Retrieved from http://effectivehealthcare.ahrq.gov/
Heiskanen, O., & Sipponen, P. (1970). Prognosis of se-vere brain injury. Acta Neurologica Scandinavica,46(3), 343–348.
Himanen, L., Portin, R., Hamalainen, P., Hurme, S.,Hiekkanen, H., & Tenovuo, O. (2011). Risk factorsfor reduced survival after traumatic brain injury: A30-year follow-up study. Brain Injury, 25(5), 443–452.
Lewin, W., Marshall, T.F., & Roberts, A.H. (1979). Long-term outcome after severe head injury. British Med-ical Journal, 2, 1533–1538.
Liberati, A., Altman, D.G., Tetzlaff, J., Mulrow, C.,Gøtzsche, P.C., Ioannidis, J.P., . . . Moher, D. (2009).The PRISMA statement for reporting systematic re-views and meta-analyses of studies that evaluatehealth care interventions: Explanation and elabora-tion. Journal of Clinical Epidemiology, 62(10), e1–e34.
Macedo, L.G., Elkins, M.R., Maher, C.G., Moseley,A.M., Herbert, R.D., & Sherrington, C. (2010).There was evidence of convergent and construct va-lidity of Physiotherapy Evidence Database qualityscale for physiotherapy trials. Journal of ClinicalEpidemiology, 63, 920–925.
Maher, C.G., Sherrington, C., Herbert, R.D., Moseley,A.M., & Elkins, M. (2003). Reliability of the PEDroscale for rating quality of randomized controlled tri-als. Physical Therapy, 83, 713–721.
Mainio, A., Kyllonen, T., Viilo, K., Hakko, H., Sarkioja,T., & Rasanen, P. (2007). Traumatic brain injury, psy-chiatric disorders and suicide: A population-basedstudy of suicide victims during the years 1988–2004in Northern Finland. Brain Injury, 21, 851–855.
110
available at https://www.cambridge.org/core/terms. https://doi.org/10.1017/BrImp.2013.11Downloaded from https://www.cambridge.org/core. IP address: 54.39.106.173, on 01 Jun 2020 at 14:08:43, subject to the Cambridge Core terms of use,
SUICIDE AFTER TBI
McMillan, T.M., & Teasdale, G.M. (2007). Death rateis increased for at least 7 years after head in-jury: A prospective study. Brain, 130(10), 2520–2527.
McMillan, T.M., Teasdale, G.M., Weir, C., & Stewart,E. (2011). Death after head injury: The 13 year out-come of a case-control study. Journal of Neurology,Neurosurgery, and Psychiatry, 82, 931–935.
Moher, D., Liberati, A., Tetzlaff, J., Altman, D.G., &The PRISMA Group. (2010). Preferred reportingitems for systematic reviews and meta-analyses:The PRISMA statement. International Journal ofSurgery, 8, 336–341.
NICE. (2012). Self-harm: Longer-term management(National Clinical Guideline Number 133). Re-trieved from http://www.nice.org.uk/nicemedia/live/13619/57179/57179.pdf
O’Carroll, P.W., Berman, A.L., Maris, R.W., Moscicky,E.K., Tanney, B.L., & Silverman, M.M. (1996). Be-yond the Tower of Babel: A nomenclature for suici-dology. Suicide and Life Threatening Behavior, 26,237–252.
Rapoport, M.J., Chan, F., Lanctot, K., Herrmann, N.,McCullagh, S., & Feinstein, A. (2008). An open-label study of citalopram for major depressionfollowing traumatic brain injury. Journal of Psy-chopharmacology, 22(8), 860–864.
Rees, R.J., & Bellon, M.L. (2007). Post concussion syn-drome ebb and flow: Longitudinal effects and man-agement. NeuroRehabilitation, 22, 229–242.
Reeves, B.C., Deeks, J.J., Higgins, J.P.T., & Wells, G.A.(2008). Chapter 13: Including non-randomized stud-ies. In J.P.T. Higgins & S. Green S (Eds.), Cochranehandbook for systematic reviews of interventions(Version 5.0.1). Retrieved from www.cochrane-handbook.org
Reeves, R.R., & Brister, J.C. (2009). Traumatic braininjury and suicide. In L. Sher & A. Vilens (Eds.),Terror and suicide (pp. 105–114). New York: NovaScience Publishers.
Reeves, R.R., & Laizer, J.T. (2012). Traumatic brain in-jury and suicide. Journal of Psychosocial Nursingand Mental Health Services, 50(3), 32–38.
Romesser, J., Shen, S., Reblin, M., Kircher, J., Allen, S.,Roberts, T., . . . Marchand, W.R. (2011). A prelimi-nary study of the effect of a diagnosis of concussionon PTSD symptoms and other psychiatric variablesat the time of treatment seeking among Veterans.Military Medicine, 176(3), 246–252.
Russell, W.R. (1951). Disability caused by brain wounds;A review of 1,166 cases. Journal of Neurology, Neu-rosurgery, and Psychiatry, 14(1), 35–39.
Shavelle, R.M., Strauss, D., Whyte, J., Day, S.M., &Yu, Y.L. (2001). Long term causes of death aftertraumatic brain injury. American Journal of PhysicalMedicine and Rehabilitation, 80(7), 510–516.
Sherrington, C., Herbert, R.D., Maher, C.G., & Moseley,A.M. (2000). PEDro: A database of randomized tri-als and systematic reviews in physiotherapy. ManualTherapy, 5, 223–226.
Silver, J.M., Kramer, R., Greenwald, S., & Weissman, M.(2001). The association between head injuries andpsychiatric disorders: Findings from the New HavenNIMH Epidemiologic Catchment Area Study. BrainInjury, 15, 935–945.
Simpson, G., & Brenner, L.A. (2011). Perspectives onsuicide and traumatic brain injury. Journal of HeadTrauma and Rehabilitation, 26(4), 241–243.
Simpson, G., & Tate, R. (2002). Suicidality after trau-matic brain injury: Demographic, injury and clinicalcorrelates. Psychological Medicine, 32(4), 687–697.
Simpson, G.K., & Tate, R.L. (2005) Clinical featuresof suicide attempts after traumatic brain injury.Journal of Nervous and Mental Disease, 19, 680–685.
Simpson, G., & Tate, R. (2007). Suicidality in peoplesurviving a traumatic brain injury: Prevalence, riskfactors and implications for clinical management.Brain Injury, 21(21), 1335–1351.
Simpson, G.K., & Tate, R.L. (2009). Suicidality and sui-cide prevention among war Veterans with traumaticbrain injury. In L. Sher & A. Vilens (Eds.), Suicidein the military (pp. 161–182). New York, NY: NovaScience Publishers.
Simpson, G.K., Tate, R.L., Whiting, D.L., & Cotter, R.E.(2011). Suicide prevention after traumatic brain in-jury: A randomized controlled trial of a program forthe psychological treatment of hopelessness. Jour-nal of Head Trauma Rehabilitation, 26(4), 290–300.
Simpson, G.K., Winstanley, J., & Bertapelle, T. (2003).Evaluation of a suicide prevention training workshopfor staff working in the field of traumatic brain injury.Journal of Head Trauma Rehabilitation, 18, 445–456.
Skopp, N.A., Trofimovich, L., Grimes, J., Oetjen-Gerdes,L., & Gahm, G.A. (2012). Relations between suicideand traumatic brain injury, psychiatric diagnoses,and relationship problems, Active Component, U.S.Armed Forces, 2001–2009. Medical SurveillanceMonthly Report, 19(2), 7–11.
Tate, R.L., Perdices, M., McDonald, S., Togher, L.,Moseley, A., & Winders, K., . . . Savage, S. (2004).Development of a database of rehabilitation therapiesfor the psychological consequences of acquired brainimpairment. Neuropsychological Rehabilitation, 14,517–534.
Teasdale, T.W., & Engberg, A.W. (2001). Suicide aftertraumatic brain injury: a population study. Journal ofNeurology, Neurosurgery, and Psychiatry, 71, 436–440.
Tsaousides, T., Cantor, J.B., & Gordon, W.A. (2011).Suicidal ideation following traumatic brain injury:Prevalence rates and correlates of adults living in thecommunity. Journal of Head Trauma Rehabilitation,26(4), 265–275.
Ventura, T., Harrison-Felix, C., Carlson, N., Digu-iseppi, C., Gabella, B., Brown, A., . . . White-neck, G. (2010). Mortality after discharge fromacute care hospitalization with traumatic brain
111
available at https://www.cambridge.org/core/terms. https://doi.org/10.1017/BrImp.2013.11Downloaded from https://www.cambridge.org/core. IP address: 54.39.106.173, on 01 Jun 2020 at 14:08:43, subject to the Cambridge Core terms of use,
N. BAHRAINI ET AL.
injury: A population-based study. Archives of Phys-ical Medicine and Rehabilitation, 91, 20–29.
Viswanathan, M., Ansari, M.T., Berkman, N.D., Chang,S., Hartling, L., McPheeters, L.M., . . . Treadwell,J.R. (2012). Assessing the risk of bias of individ-ual studies in systematic reviews of health care in-terventions. Agency for Healthcare Research andQuality Methods Guide for Comparative Effective-ness Reviews (AHRQ Publication No. 12-EHC047-EF). Retrieved from http://www.effectivehealthcare.ahrq.gov/
Viswanathan, M., & Berkman, N.D. (2012). Develop-ment of the RTI item bank on risk of bias and pre-cision of observational studies. Journal of ClinicalEpidemiology, 65(2), 163–178.
von Elm, E., Altman, D.G., Egger, M., Pocock, S.J.,Gøtzsche, P.C., & Vandenbroucke, J.P., STROBEInitiative. (2008). The strengthening the reportingof observational studies in epidemiology (STROBE)
statement: guidelines for reporting observationalstudies. Journal of Clinical Epidemiology, 61(4),344–349.
Wasserman, L., Shaw, T., Vu, M., Ko, C., Bollegala, D., &Bhalerao, S. (2008). An overview of traumatic braininjury and suicide. Brain Injury, 22(11), 811–819.
Wood, R.L.L., Williams, C., & Lewis, R. (2010). Role ofalexithymia in suicide ideation after traumatic braininjury. Journal of the International Neuropsycholog-ical Society, 16, 1108–1114.
World Health Organisation. (2012). Public health actionfor the prevention of suicides. Retrieved from http://apps.who.int/iris/bitstream/10665/75166/1/9789241503570_eng.pdf
Yurgelun-Todd, D.A., Bueler, C.E., McGlade, E.,Churchwell, J., Brenner, L.A., & Lopez-Larson,M. (2011). Neuroimaging correlates of traumaticbrain injury and suicidal behavior. Journal of HeadTrauma Rehabilitation, 26(4), 276–289.
112
available at https://www.cambridge.org/core/terms. https://doi.org/10.1017/BrImp.2013.11Downloaded from https://www.cambridge.org/core. IP address: 54.39.106.173, on 01 Jun 2020 at 14:08:43, subject to the Cambridge Core terms of use,
Related Documents











