Clinical Diagnostics Software Solutions SPECIAL REPORT The Use of Spirometry Software Packages to Aid Compliance and Assist in Practice Workflows Joining the Team Doing What Doctors Do? Knowledge is Power Where Now for Diagnostic Support Systems? Sponsored by Published by Global Business Media

Special Report – Clinical Diagnostics Software Solutions
Mar 08, 2016
Primary Care – Special Report on Clinical Diagnostics Software Solutions
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Clinical Diagnostics Software Solutions
S p e c i a l R e p o R t
The Use of Spirometry Software Packages to Aid Compliance and Assist in Practice Workflows
Joining the Team
Doing What Doctors Do?
Knowledge is Power
Where Now for Diagnostic Support Systems?
Sponsored by
Published by Global Business Media
Micro Medical – the most comprehensive line of portable and primary care spirometers, with Spirometry PC Software (SPCS) and SentrySuite™ connectivity
From hospital to home,your patients are well taken care of.Highest standards of care with the right device for your patient.
Start your examination in the hospital, clinic, physician office and follow your
patients at home.
Download patient test results to your PC with Spirometry PC Software (SPCS),
or to SentrySuite and integrate with all your PFT tests.
Williams Medical Supplies exclusive UK business partners of Micro Medical
(Carefusion) Spirometers. For more information, please visit www.wms.co.uk
© 2012 CareFusion Corporation or one of its subsidiaries. All rights reserved. Jaeger, SentrySuite, MasterScreen, SensorMedics, Vmax and Spirometry PC Software are trademarks or registered trademarks of CareFusion Corporation or one of its subsidiaries.0000CF01428 Iss 2
MasterScreen SENSORMEDICS® VMAX® Micro Medical JAEGER® SentrySuite™
ND00105_CF_Generic_SPCS_Advert.indd 1 03/05/2012 13:44
SPECIAL REPORT: CLINICAL DIAGNOSTICS SOFTWARE SOLUTIONS
Published by Global Business Media
Global Business Media Limited 62 The Street Ashtead Surrey KT21 1AT United Kingdom
Switchboard: +44 (0)1737 850 939 Fax: +44 (0)1737 851 952 Email: [email protected] Website: www.globalbusinessmedia.org
PublisherKevin Bell
Business Development DirectorMarie-Anne Brooks
EditorJohn Hancock
Senior Project ManagerSteve Banks
Advertising ExecutivesMichael McCarthyAbigail Coombes
Production ManagerPaul Davies
For further information visit:www.globalbusinessmedia.org
The opinions and views expressed in the editorial content in this publication are those of the authors alone and do not necessarily represent the views of any organisation with which they may be associated.
Material in advertisements and promotional features may be considered to represent the views of the advertisers and promoters. The views and opinions expressed in this publication do not necessarily express the views of the Publishers or the Editor. While every care has been taken in the preparation of this publication, neither the Publishers nor the Editor are responsible for such opinions and views or for any inaccuracies in the articles.
© 2012. The entire contents of this publication are protected by copyright. Full details are available from the Publishers. All rights reserved. No part of this publication may be reproduced, stored in a retrieval system or transmitted in any form or by any means, electronic, mechanical photocopying, recording or otherwise, without the prior permission of the copyright owner.
Contents
Foreword 2 John Hancock, Editor
The Use of Spirometry Software Packages to Aid Compliance and Assist in Practice Workflows 3 Oisin McManigan, Senior Product and Marketing Manager – Micro Medical spirometers CareFusion 232 UK Ltd
What is Spirometry?Training is ImportantEnsuring ComplianceIntegrated Software Conclusion
Joining the Team 7 Peter Dunwell, Medical Correspondent
New Opportunities Need New StrategiesNot Stand-AloneA New Member for the Team
Doing What Doctors Do? 9 John Hancock
What is Clinical Diagnostic Software?What it should doWider Access Makes for Better Outcomes
Knowledge is Power 11 Camilla Slade, Staff Writer
A Major InvestmentThe Right SolutionKnowledge Makes Demands
Where Now for Diagnostic Support Systems? 13 John Hancock
CDSS – Leveraging SkillsEvidence of a Better FutureWhat’s in the Future?
References 15
WWW.PRImARyCAREREPORTS.CO.UK | 1
Clinical Diagnostics Software Solutions
S P E C I A L R E P O R T
The Use of Spirometry Software Packages to Aid Compliance and Assist in Practice Workfl ows
Joining the Team
Doing What Doctors Do?
Knowledge is Power
Where Now for Diagnostic Support Systems?
Sponsored by
Published by Global Business Media
Foreword
In all walks of life, technology-based systems
are enhancing the way in which tasks are
completed, quality of outcomes, and the retention
of large volumes of information to inform future
activities and decisions. But while many process
workers may welcome the additional capability
that IT and digital systems can bring to their
work, professionals often view askance the use
of IT-based systems, believing that, ‘no system
can replace the knowledge, experience and
understanding of a professional.’
That simply isn’t the case because a well-designed
IT-based system does not try to second-guess or,
worse still, replace the professional; what it does
is delivers vastly more volumes of data than any
professional could carry in their heads but without
the need to consult volumes and volumes of
technical books in order to assemble information
relevant to a particular decision or task.
This Special Report opens with an article that looks
at the use of spirometry software packages to aid
compliance and assist in practice workflows. It
goes on to stress the importance of such packages
to provide immediate feedback and guidance to the
user. Spirometry has been established in guidelines
as the recommended procedure for aiding the
diagnosis of asthma, and NICE guidelines state
that all health professionals involved in the care
of people with COPD should have access to
spirometry and be able to interpret the results.
However, it is important to choose the correct
software package from the many available to
assist in patient performance, practice workflows,
correct diagnosis and continuum of respiratory
care for patients.
Seen in this context, Clinical Diagnostic Software
(CDS) or Clinical Decision Support Systems (CDSS),
far from threatening the professional primacy of
GPs and other clinicians, can add enormous value
to the application of their professional skills and
support significantly improved outcomes. Also,
in the now time-honoured manner of IT systems,
they can improve efficiency and cost effectiveness
while generating, as they work, a well ordered and
easily interrogated audit trail of information used,
decisions taken and actions instigated.
Given that, GPs have now been placed at the
very heart of the National Health Service in every
sense and in particular in the sense that they will
be managing the whole patient journey from initial
presentation to, hopefully, cure or, as importantly,
long-term treatment programme. To shift the
centre of gravity of the NHS in this way speaks
of enormous faith in the capabilities of GPs but,
at the same time transfers significant levels of
responsibility and accountability both of which will
be more easily shouldered using a well-structured
system to support the key event in the GP patient
relationship: the consultation and diagnosis.
John Hancock
Editor
SPECIAL REPORT: CLINICAL DIAGNOSTICS SOFTWARE SOLUTIONS
2 | WWW.PRImARyCAREREPORTS.CO.UK
John Hancock has been Editor of Primary Care Reports since its launch. A journalist for nearly 25 years, John has written and edited articles, papers and books on a range of medical and management topics. Subjects have included management of long-term conditions, elective and non-elective surgery, Schizophrenia, health risks of travel, local health management and NHS management and reforms – including current changes.
SPECIAL REPORT: CLINICAL DIAGNOSTICS SOFTWARE SOLUTIONS
WWW.PRImARyCAREREPORTS.CO.UK | 3
Micro Medical – Spirometry Made Simple
Highest standards of care with the right device for your patient.
Spirometry PC software (SPCS)
• Quality assurance for each manoeuvre
• Guidance on between manoeuvre variability
• Confirmation of end of test
• Automatic PDF for exporting to patient records
• Links directly to many GP electronic health record systems
Williams Medical Supplies exclusive UK business partners, please visit www.wms.co.uk
© 2012 CareFusion Corporation or one of its subsidiaries. All rights reserved. 0000CF01428 Iss 2
MasterScreen SENSORMEDICS®
VMAX® Micro Medical
JAEGER® SentrySuite™
ND00108_CF_Generic_250x57_Advert.indd 1 14/05/2012 13:39
The Use of Spirometry Software Packages to Aid Compliance and Assist in Practice WorkflowsOisin McManigan, Senior Product and Marketing Manager –
Micro Medical spirometers
CareFusion 232 UK Ltd
What is Spirometry?Spirometry is an effort-dependent test that requires both patient cooperation and trained staff to ensure the results obtained are of sufficient quality and reproducibility to avoid misdiagnosis. To assist individuals performing spirometry in primary care, there is a strong need to provide clear software-driven feedback of each manoeuvre and possible errors in test technique to ensure the results obtained meet current guidelines. Spirometry PC software (SPCS) can assist the primary care health professional in this objective by ensuring compliance and quality are met and maximal effort is achieved from patients through on-screen feedback and clear messaging, to signify the test session is complete. Direct transfer of results into the patient’s health records along with graphical representation aides in quality assurance and diagnosis.
Spirometry has been established in guidelines as the recommended procedure for aiding the diagnosis of asthma and COPD (chronic obstructive pulmonary disease), both in the U.K through the NICE guidelines1 and internationally through the GOLD2 (Global Initiative for Obstructive Lung Disease) guidelines. International guidelines have also been published on lung function testing including spirometry by the American and European Thoracic societies, giving clear guidance on the test procedure, the reproducibility criteria, the number of tests that should be performed and the errors that users should be aware of when looking at the test technique and the results obtained from a manoeuvre to determine whether they are acceptable or not for diagnostic purposes. The NICE 2010 guidelines state that – “All health professionals involved in the care of people with
Spirometry quality control in primary care and the importance of computer software packages (SPCS) to provide immediate feedback and guidance to the user.
IMMEDIATE FEEDBACK SHOULD BE PROvIDED FOR WITHIN AND BETWEEN SPIROMETRy MANOEUvRES

SPECIAL REPORT: CLINICAL DIAGNOSTICS SOFTWARE SOLUTIONS
4 | WWW.PRImARyCAREREPORTS.CO.UK
Various studies have
shown that effective
training and quality
assurance are
required to ensure
successful provision
of quality spirometry
in primary care.
COPD should have access to spirometry and be able to interpret the results.”
Training is ImportantAny healthcare worker with up-to-date training may perform spirometry.
There has been much discussion, however, over the quality of spirometry performed within primary care along with proposed standards for general practice compliance to American Thoracic Society and European Respiratory Society recommendations3. Various studies have shown that effective training and quality assurance are required to ensure successful provision of quality spirometry in primary care. The proposed standards for general practice compliance recommend “A need for systems for assessing the quality of spirometry tests, either by direct observation by trained individuals or by building in practical guidance in the form of immediate feedback during the test procedure”4.
The current ATS/ERS standards for within and between manoeuvre acceptability criteria are summarised below:
However in a busy primary care practice compliance to these criteria can often be difficult and assistance from Spirometry PC software is invaluable.
Ensuring ComplianceThe software enables all of the manoeuvres in both graphical and tabulated form of the selected indices to be recorded for the patient’s spirometry. After each manoeuvre, on- screen quality prompts are displayed advising the operator of the quality of the blow performed with relevant messages that can be used as guidance for both the health care professional and the patient. Dependent on the quality of the manoeuvre, patients can then be encouraged to perform the test with better compliance to gain maximum effort and complete the test before they become fatigued. The quality prompts need to be clear and defined against each manoeuvre, so they are clearly understood by the operator and patient (Quality prompts for extrapolated volumes <5% or 0.150L of FVC are displayed as “Slow start” so the operator can encourage the patient to blow out harder and faster).
Software packages should advise when the criteria have been met for both the quality of each individual manoeuvre, and completion of the test session (between manoeuvre criteria) so that the operator knows their spirometry is both acceptable and reproducible and the test session is complete.
Computer animations built into the spirometry software can assist compliance to both the quality of the spirometry performed and the between manoeuvre reproducibility criteria. On-screen incentives provide a visual aid to the patient to assist in performing good manoeuvres which can help all patients, young or old, to comprehend the test technique and increase interaction between the healthcare professional and the patient. To avoid patients finishing the tests prematurely or performing sub maximal efforts, Spirometry PC software animations have the ability to alter the target so that the incentive is achieved. Incentive criteria can be set to either % of predicted FVC, or % of Best FVC performed, this has the advantage of increasing the target level to ensure maximal effort is achieved on each manoeuvre after an initial test blow is performed.
Within-manoeuvre criteria
Individual spirograms are ‘‘acceptable’’ if:
They are free from artefacts
Cough during the first second of exhalation
Glottis closure that influences the measurement
Early termination or cut-off
Effort that is not maximal throughout
Leak
Obstructed mouthpiece
They have good starts
Extrapolated volume, 5% of FvC or 0.15 L, whichever is greater
They show satisfactory exhalation
Duration of>6 s (3 s for children) or a plateau in the volume–time curve or
If the subject cannot or should not continue to exhale
Between-manoeuvre criteria
After three acceptable spirograms have been obtained, apply the following tests
The two largest values of FvC must be within 0.150 L of each other
The two largest values of FEv1 must be within 0.150 L of each other
If both of these criteria are met, the test session may be concluded
If both of these criteria are not met, continue testing until
Both of the criteria are met with analysis of additional acceptable spirograms or
A total of eight tests have been performed (optional) or
The patient/subject cannot or should not continue
Save, as a minimum, the three satisfactory manoeuvres
FvC: forced vital capacity; FEv1: forced expiratory volume in one second
Summary of within- and between-manoeuvre acceptability criteria
INCENTIvE ANIMATIONS ASSIST PATIENT COOPERATION
SPECIAL REPORT: CLINICAL DIAGNOSTICS SOFTWARE SOLUTIONS
WWW.PRImARyCAREREPORTS.CO.UK | 5
Micro Medical – Spirometry Made Simple
Highest standards of care with the right device for your patient.
Spirometry PC software (SPCS)
• Quality assurance for each manoeuvre
• Guidance on between manoeuvre variability
• Confirmation of end of test
• Automatic PDF for exporting to patient records
• Links directly to many GP electronic health record systems
Williams Medical Supplies exclusive UK business partners, please visit www.wms.co.uk
© 2012 CareFusion Corporation or one of its subsidiaries. All rights reserved. 0000CF01428 Iss 2
MasterScreen SENSORMEDICS®
VMAX® Micro Medical
JAEGER® SentrySuite™
ND00108_CF_Generic_250x57_Advert.indd 1 14/05/2012 13:39
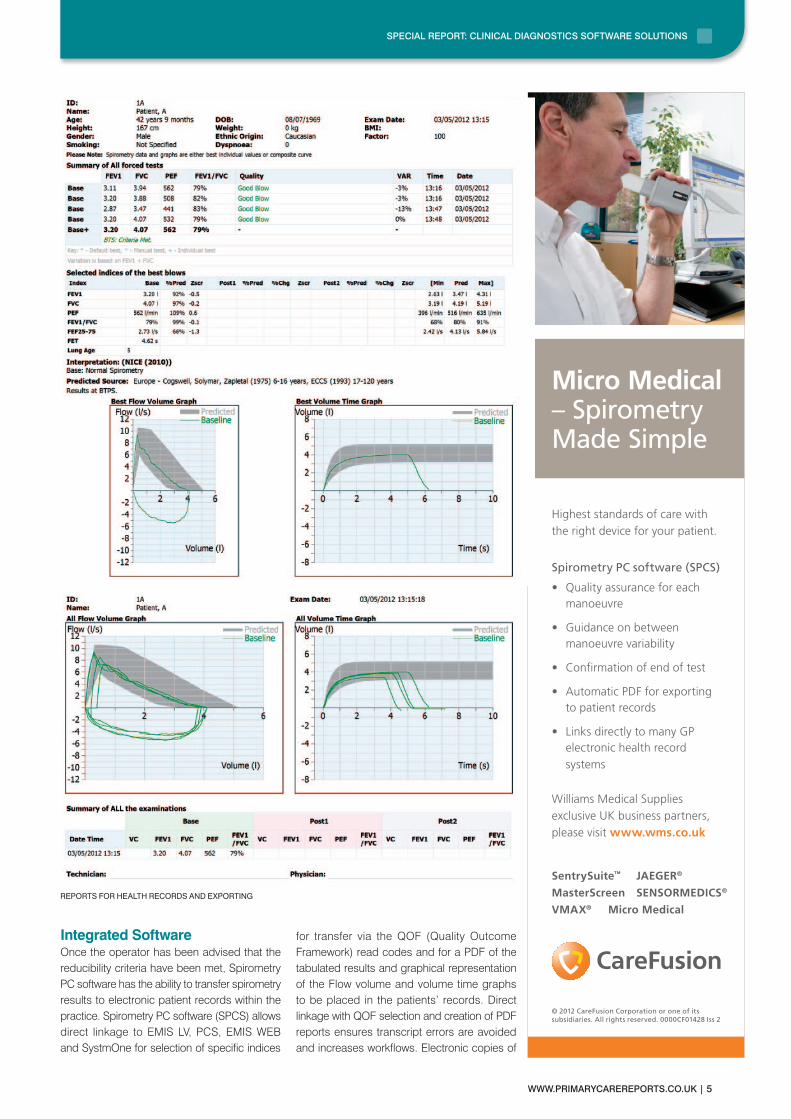
Integrated Software Once the operator has been advised that the reducibility criteria have been met, Spirometry PC software has the ability to transfer spirometry results to electronic patient records within the practice. Spirometry PC software (SPCS) allows direct linkage to EMIS LV, PCS, EMIS WEB and SystmOne for selection of specific indices
for transfer via the QOF (Quality Outcome Framework) read codes and for a PDF of the tabulated results and graphical representation of the Flow volume and volume time graphs to be placed in the patients’ records. Direct linkage with QOF selection and creation of PDF reports ensures transcript errors are avoided and increases workflows. Electronic copies of
REPORTS FOR HEALTH RECORDS AND ExPORTING
SPECIAL REPORT: CLINICAL DIAGNOSTICS SOFTWARE SOLUTIONS
6 | WWW.PRImARyCAREREPORTS.CO.UK
There are many
spirometers and software
packages available but
choosing the correct
one can assist in
patient performance,
compliance, practice
workflows, correct
diagnosis and continuum
of respiratory care for
your patients.
the reports also allow spirometry test sessions to be exported to other healthcare professionals where required for further evaluation and investigation. To ensure continuum of care and to avoid delays in patient diagnosis and treatment regimes, where possible, primary care spirometry software packages should have the ability to link into hospital based pulmonary function software such as Sentrysuite, allowing clear access to patients’ spirometry results performed prior to hospital referral.
ConclusionWith the correct choice of software packages, compliance to current guidelines on quality and reproducibility can be enhanced. Spirometry software packages have to be user friendly and give immediate feedback on both manoeuvre quality and reproducibility. The advice should be displayed clearly and visibly against each manoeuvre along with the variability between the manoeuvres. Once the criteria have been met the operator should be advised so that the test can be concluded. The spirometry report obtained should clearly state the quality and reproducibility, and where this has not been obtained, advise accordingly so that performance can be improved on future tests. There are many spirometers and software packages available but choosing the correct one can assist in patient performance, compliance, practice workflows, correct diagnosis and continuum of respiratory care for your patients.
References1. NICE Guidelines Chronic obstructive
pulmonary disease Management of chronic obstructive
pulmonary disease in adults in primary and secondary care. June 2010
2. The Global Strategy for the Diagnosis, Management and Prevention of COPD, Global Initiative for Chronic Obstructive Lung Disease (GOLD) 2011
3. ‘‘ATS/ERS TASK FORCE: STANDARDISATION OF LUNG FUNCTION TESTING’’
Standardisation of Spirometry M.R.Miller et al. Eur Respir J 2005; 26: 319–3384. Diagnostic Spirometry in Primary care Proposed Standards for general
practice compliant with American Thoracic Society and European Respiratory Society recommendations.
Mark Levy et al. Primary care Respiratory Journal (2009); 18(3): 130-147
ContactsCareFusion 232 UK Ltd.The Crescent, Jays Close, Basingstoke, Hants RG22 4BSTel: 0800 151 3580 Fax: 01256 330860www.carefusion.com/micromedical
Williams medical SuppliesCraiglas House, The maerdy Industrial Estate,Rhymney Tredegar NP22 5PyTel: 01685 846666Email: [email protected]

SPECIAL REPORT: CLINICAL DIAGNOSTICS SOFTWARE SOLUTIONS
WWW.PRImARyCAREREPORTS.CO.UK | 7
Micro Medical – Spirometry Made Simple
Highest standards of care with the right device for your patient.
Spirometry PC software (SPCS)
• Quality assurance for each manoeuvre
• Guidance on between manoeuvre variability
• Confirmation of end of test
• Automatic PDF for exporting to patient records
• Links directly to many GP electronic health record systems
Williams Medical Supplies exclusive UK business partners, please visit www.wms.co.uk
© 2012 CareFusion Corporation or one of its subsidiaries. All rights reserved. 0000CF01428 Iss 2
MasterScreen SENSORMEDICS®
VMAX® Micro Medical
JAEGER® SentrySuite™
ND00108_CF_Generic_250x57_Advert.indd 1 14/05/2012 13:39
Joining the TeamPeter Dunwell, Medical Correspondent
GPs face an ever rising tide of clinical, research, procedural and regulatory data, all of which has to some extent to be incorporated in every diagnosis. In one sense, the advent of electronic records and databases has exacerbated this challenge by bringing greater volumes of information into every consultation. This is paralleled with developments in the wider economy where data volumes have grown exponentially as the ability to harvest and manipulate that data has grown with electronic applications. And just as managers have developed decision support systems to better utilise all the data that might contribute to a decision so, in healthcare, decision support systems have been developed to assist in diagnosis.
New Opportunities Need New StrategiesHowever, in order to derive the maximum value from such a powerful tool, GPs will have to develop strategies that manage and leverage the best from those systems.
As part of the brief that its name suggests, NICE (the National Institute for Health and Clinical Excellence) assesses the technologies used in healthcare delivery, including technologies that record and evaluate a patient’s condition. As NICE, itself, says:
“These technologies may be used for various purposes: diagnosis, clinical monitoring, screening, treatment triage, assessing stages of disease progression, risk stratification and so on1.”
NICE has generated a Diagnostic Assessment Program Manual taking into account the views of various stakeholders from the NHS, the medical technologies industry, academia, patient care organisations and the Department of Health. This manual became the basis for all diagnostic evaluations started after 1 January 2012.
The systems in question, known as Clinical Diagnostic Software (CDS) or Clinical Decision Support Systems (CDSS), are IT applications designed to assist clinicians by marshalling input from the GP’s examination of the patient with other condition specific data and potential variables suggested by the patient’s condition,
before running this information against the decision support rules.
Apart from the obvious benefit of being able to incorporate more data into a diagnosis, CDSSs help to avoid reliance on memory which, in turn, reduces errors by reducing omissions and transcription faults as well as generating or adding to other relevant documents within the practice. It means that practice methodology must take into account that high-quality records are being generated automatically and must ensure that each piece of information is filed or lodged in all the places where it is needed. This will free up practice time and resources to develop some of the patient orientated services that current NHS reforms envisage. Also, subject to data protection and privacy rules, the system can become the foundation of the GP’s position at the centre of NHS healthcare delivery.
Of course, along with the availability of more information to the GP through the Freedom of Information Act and current practices, patients also have access to the information. While some doctors may once have viewed this as a two edged sword, a greater involvement by the patient in both understanding their condition and in decisions about their treatment should ultimately add to the quality of the service but, again, it may well require a change in process by some, especially older, GPs and a practice strategy of involving patients at the earliest possible stage.
Not Stand-AloneAs well as driving new strategies for the practice, any new IT system, including diagnostic support, will need to be integrated into other programmes used in the practice. In particular, software for functions associated with or concomitant upon diagnosis such as chronic disease management software and drug monitoring software would need to be linked to new diagnostic support software.
In its publication, ‘The Future Direction of General Practice – a Roadmap’ the Royal College of General Practitioners (RCGP) says that:
“Interfaces can be dangerous places for patients and systems need to evolve to ensure
Clinical Diagnostic Software facilitates better professional performance – what more could you ask of a newcomer

SPECIAL REPORT: CLINICAL DIAGNOSTICS SOFTWARE SOLUTIONS
8 | WWW.PRImARyCAREREPORTS.CO.UK
Systems need to
evolve to ensure better
coordination of care
throughout the health
and social care system…
This will require robust
models of clinical
governance, supported
by sophisticated
IT systems.
better coordination of care throughout the health and social care system... This will require robust models of clinical governance, supported by sophisticated IT systems – with appropriate safeguards for confidentiality. We believe that this is important to stop the worrying trend of fragmentation of care and to define, for patients, who is accountable for specific problems. The coordinating role of GPs is crucial as patients experience disruption of care when crossing interfaces between primary, secondary and social care access. However, very few systems achieve high levels of coordination of care. This is an important function of general practice...”2
Given patient workloads, condition complexities and regulatory imperatives that surround modern
practice, is hard to see how any system other than one based on IT could ever cope.
Taking advantage of this new technology, NICE has published and is developing a number of guides on diagnostic technologies in conditions whose frequency or seriousness warrants a structured methodology to help the GP not only complete the diagnosis but also understand what are the possibilities for treatment within the NHS. There are currently eight such guidelines in development ranging from uterine cervix conditions to small-cell lung cancer to liver conditions, breast cancer and a number of other cases that often present for diagnosis3 4.
A New Member for the TeamRCGP sums up the challenges that face GPs having to change the ways they have worked in the past when an IT system ‘joins’ the practice. In the College’s publication, ‘The Good Practice Guidelines for GP electronic patient records’ it states that:
“Many clinicians find a change to working paper light challenging. As well as the learning curve required to become familiar with the clinical information system, they also have to learn how to interact with the computer in the consulting room, in effect adding a new participant to their consultation.”5
That new participant should be viewed as a friend; not as a professional usurper.
MICROLAB SPIROMETER

SPECIAL REPORT: CLINICAL DIAGNOSTICS SOFTWARE SOLUTIONS
WWW.PRImARyCAREREPORTS.CO.UK | 9
Micro Medical – Spirometry Made Simple
Highest standards of care with the right device for your patient.
Spirometry PC software (SPCS)
• Quality assurance for each manoeuvre
• Guidance on between manoeuvre variability
• Confirmation of end of test
• Automatic PDF for exporting to patient records
• Links directly to many GP electronic health record systems
Williams Medical Supplies exclusive UK business partners, please visit www.wms.co.uk
© 2012 CareFusion Corporation or one of its subsidiaries. All rights reserved. 0000CF01428 Iss 2
MasterScreen SENSORMEDICS®
VMAX® Micro Medical
JAEGER® SentrySuite™
ND00108_CF_Generic_250x57_Advert.indd 1 14/05/2012 13:39
Doing What Doctors Do?John Hancock
It is, by now, well understood and well documented that NHS reforms, while they may impact at a number of levels, will most obviously bring changes to the role of GPs within the NHS. By putting GPs at the centre of health delivery, the reforms will open opportunities for local practices but will also shift new responsibilities onto GPs and other practice clinicians. GPs will need to take account of how they can best arrange things to deliver a wider range of services and meet greater responsibilities. One way to do this is to make greater use of technology in supporting the operation and delivery of healthcare and, within that technology spectrum, increasing numbers of doctors are making use of Clinical Diagnostic Software (CDS) also known as a Clinical Decision Support Systems (CDSS).
What is Clinical Diagnostic Software?According to SearchHealthIT6:
“A Clinical Decision Support System (CDSS) is an application that analyzes data to help healthcare providers make clinical decisions. [It] is an adaptation of the decision support system commonly used to support business management.”
And that’s an important point to bear in mind; decision support systems are not in themselves particularly revolutionary but are tried and proven software solutions that have worked in a variety of environments; in this case, using input from clinical records, patient examinations, drug and treatment histories and catalogues, known disease symptoms, clinical research, etc. Just as IT assists in other environments:
“CDSSs support healthcare workers in performing everyday functions by assisting in tasks that require the manipulation or interpretation of data. [They also] provide evidence based knowledge in the context of patient specific data. The growing popularity of CDSSs is due to the growing evidence supporting the claim that they improve patient safety and quality of care by facilitating the practice of evidence-based medicine.”7.
Against this, GPs have no need to fear that technology will eventually supplant profession or experience. In his paper, ‘Clinical Decision Support Systems’, Fahhad Farukhi8 cites Ralph Engle, one of the pioneers of computer assisted diagnosis who wrote:
“Our experience confirms the great difficulty and even impossibility, of incorporating the complexity of the human thought into a system that can be handled by a computer. We concluded that we should stop trying to make a computer act like a diagnostician and concentrate instead on ways of making computer-generated relevant information available to physicians as they make decisions.”9
As in other fields of human activity, IT will support the professional with a wider range of information and an array of possible courses of action but leaving the ultimate decision to the clinician who understands the patient, the condition and the environment within which any treatment program has to be delivered. Of course, using the old IT adage, ‘rubbish in, rubbish out’, CDSS relies for the quality of its output on the information that the clinician inputs to the system.
There are CDSSs that are knowledge-based and systems that are non-knowledge-based. The intricacies of how each operates is a little off our objective here but readers who are particularly interested in the inner workings of IT systems will be able to find plenty of material on the Internet10.
Clinical diagnostic software solutions will never replace the clinician but will make it easier for GPs to meet their new responsibilities in a reformed NHS
SPIROMETRy PC SOFTWARE PROvIDING
IMMEDIATE FEEDBACK WITH qUALITy
AND REPRODUCIBILITy STATEMENTS

SPECIAL REPORT: CLINICAL DIAGNOSTICS SOFTWARE SOLUTIONS
10 | WWW.PRImARyCAREREPORTS.CO.UK
“The growing popularity
of CDSSs is due to
the growing evidence
supporting the claim
that they improve patient
safety and quality of
care by facilitating the
practice of evidence-
based medicine.”
What it should doThe National Institute for Health and Clinical Excellence (NICE) has conducted a Diagnostics Assessment Programme to evaluate medical technologies including “innovative medical diagnostic technologies” as part of which process the organisation has created a definition of diagnosis which any CDSS should be able to match.
The bottom line is that, while information may be provided, it is entirely up to the GP as to how and even whether they use it to determine the diagnosis and treatment programme for a particular patient. In recognition of this reality, three types of decision support systems have evolved. Passive systems assemble information but do not offer explicit decisions suggestions or solutions while active systems do offer suggestions or solutions. Perhaps what many GPs will be most comfortable with will be a cooperative CDSS which works with the decision maker who can modify, complete or refine suggestions provided by the system12.
One thing that will be as true for CDSS as for other IT in a practice would be that it must be compliant with and able to work with other systems within the NHS.
There are a number of ways in which Clinical Diagnostic Software can assist a clinician with alerts and reminders, diagnostic assistance, prescription decision support, information retrieval, image recognition and interpretation and therapy critiquing and planning13. NICE says that:
“Diagnostic technologies may be used [by GPs] for various purposes: diagnosis, clinical monitoring, screening, treatment triage, assessing stages of disease progression, risk stratification, etc.”14.
Wider Access Makes for Better OutcomesEqually, CDSS does not only operate as a stand-alone system. Clinicians will be able to share knowledge and access specialist knowledge when faced with the possibility of rare complications or less frequently encountered conditions. Because of the information available to the system, it will also be possible for the GP to contact a specialist within a given field and, using a commonly accessible web platform, to set out the information used in diagnosis and to discuss a particular presentation. A good system will also alert GPs when any results returned from an external testing process fall outside of normally accepted parameters.
All of this will lead to better informed and earlier diagnoses with a clear decision trail that the GP can use for later reference and or present to other parties who might legitimately have an interest in the patient’s treatment. It should also ensure that GPs have more time within an appointment window to spend ‘with the patient’ as opposed to retrieving information and, because it marshals information in a logical format, a CDSS should also help when explaining conditions to patients and creating and maintaining patient records in the wider practice. And, working together, such systems will be able to identify health trends across the wider population.
All in all, Clinical Diagnostic Software will considerably aid practice effectiveness and efficiency. In an organisation where GPs will be the gatekeepers to the NHS, the planners of treatment routes and the instigators of specialist and treatment referrals within the system, a diagnostic software solution will support the kind of operational infrastructure that must become the norm in future GP practice.
NICE Diagnostic Assessment Programme: Definition of Diagnosis11
Diagnosis is the process of identifying whether the patient has a disease at the time of testing. It is performed for patients with specific complaints or in whom signs or symptoms have been noted that may indicate a disease. Tests can have several different uses in the process of diagnosis, for example:
• Ruling in or out a specific disease;• General examination looking for clues to
the cause of the symptoms;
• Staging, or additional testing to assess how advanced or severe the disease is;
• Monitoring a patient over time to determine changes in their condition;
• Screening tests to look for conditions in patients without signs or symptoms of the specific condition.
SPECIAL REPORT: CLINICAL DIAGNOSTICS SOFTWARE SOLUTIONS
WWW.PRImARyCAREREPORTS.CO.UK | 11
Micro Medical – Spirometry Made Simple
Highest standards of care with the right device for your patient.
Spirometry PC software (SPCS)
• Quality assurance for each manoeuvre
• Guidance on between manoeuvre variability
• Confirmation of end of test
• Automatic PDF for exporting to patient records
• Links directly to many GP electronic health record systems
Williams Medical Supplies exclusive UK business partners, please visit www.wms.co.uk
© 2012 CareFusion Corporation or one of its subsidiaries. All rights reserved. 0000CF01428 Iss 2
MasterScreen SENSORMEDICS®
VMAX® Micro Medical
JAEGER® SentrySuite™
ND00108_CF_Generic_250x57_Advert.indd 1 14/05/2012 13:39
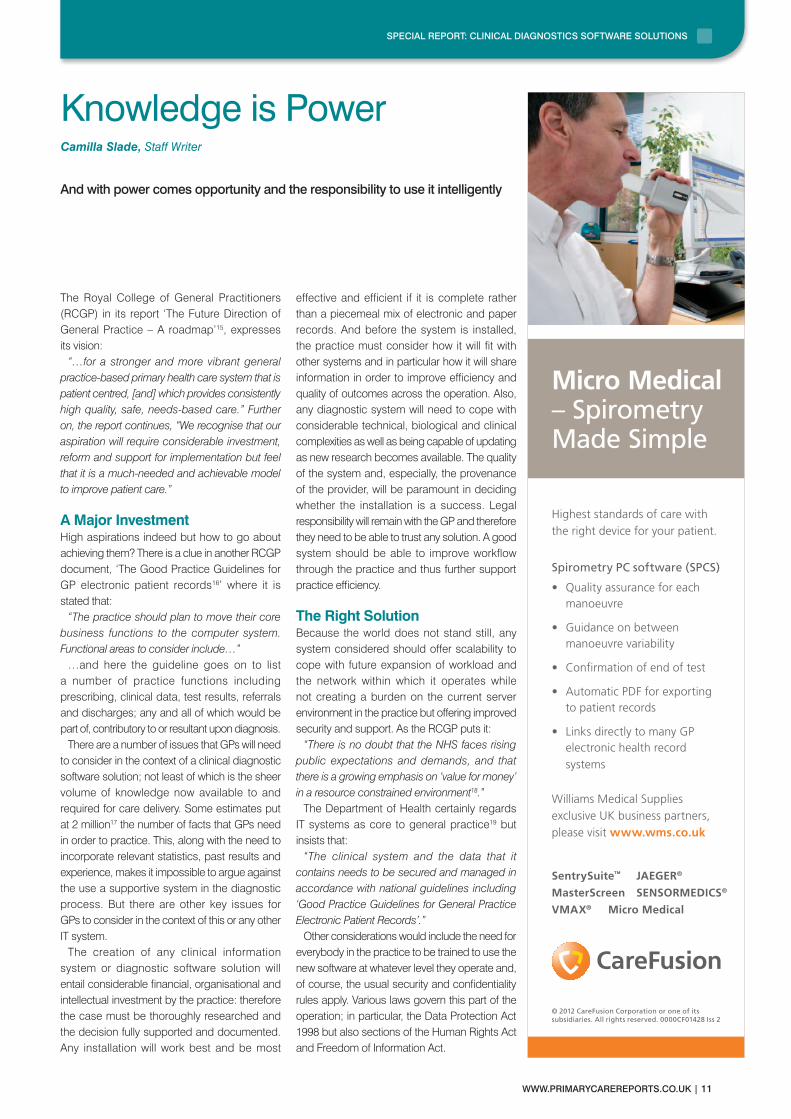
The Royal College of General Practitioners (RCGP) in its report ‘The Future Direction of General Practice – A roadmap’15, expresses its vision:
“…for a stronger and more vibrant general practice-based primary health care system that is patient centred, [and] which provides consistently high quality, safe, needs-based care.” Further on, the report continues, “We recognise that our aspiration will require considerable investment, reform and support for implementation but feel that it is a much-needed and achievable model to improve patient care.”
A Major InvestmentHigh aspirations indeed but how to go about achieving them? There is a clue in another RCGP document, ‘The Good Practice Guidelines for GP electronic patient records16’ where it is stated that:
“The practice should plan to move their core business functions to the computer system. Functional areas to consider include…”
…and here the guideline goes on to list a number of practice functions including prescribing, clinical data, test results, referrals and discharges; any and all of which would be part of, contributory to or resultant upon diagnosis.
There are a number of issues that GPs will need to consider in the context of a clinical diagnostic software solution; not least of which is the sheer volume of knowledge now available to and required for care delivery. Some estimates put at 2 million17 the number of facts that GPs need in order to practice. This, along with the need to incorporate relevant statistics, past results and experience, makes it impossible to argue against the use a supportive system in the diagnostic process. But there are other key issues for GPs to consider in the context of this or any other IT system.
The creation of any clinical information system or diagnostic software solution will entail considerable financial, organisational and intellectual investment by the practice: therefore the case must be thoroughly researched and the decision fully supported and documented. Any installation will work best and be most
effective and efficient if it is complete rather than a piecemeal mix of electronic and paper records. And before the system is installed, the practice must consider how it will fit with other systems and in particular how it will share information in order to improve efficiency and quality of outcomes across the operation. Also, any diagnostic system will need to cope with considerable technical, biological and clinical complexities as well as being capable of updating as new research becomes available. The quality of the system and, especially, the provenance of the provider, will be paramount in deciding whether the installation is a success. Legal responsibility will remain with the GP and therefore they need to be able to trust any solution. A good system should be able to improve workflow through the practice and thus further support practice efficiency.
The Right SolutionBecause the world does not stand still, any system considered should offer scalability to cope with future expansion of workload and the network within which it operates while not creating a burden on the current server environment in the practice but offering improved security and support. As the RCGP puts it:
“There is no doubt that the NHS faces rising public expectations and demands, and that there is a growing emphasis on ‘value for money’ in a resource constrained environment18.”
The Department of Health certainly regards IT systems as core to general practice19 but insists that:
“The clinical system and the data that it contains needs to be secured and managed in accordance with national guidelines including ‘Good Practice Guidelines for General Practice Electronic Patient Records’.”
Other considerations would include the need for everybody in the practice to be trained to use the new software at whatever level they operate and, of course, the usual security and confidentiality rules apply. Various laws govern this part of the operation; in particular, the Data Protection Act 1998 but also sections of the Human Rights Act and Freedom of Information Act.
Knowledge is PowerCamilla Slade, Staff Writer
And with power comes opportunity and the responsibility to use it intelligently

SPECIAL REPORT: CLINICAL DIAGNOSTICS SOFTWARE SOLUTIONS
12 | WWW.PRImARyCAREREPORTS.CO.UK
“The clinical system and
the data that it contains
needs to be secured and
managed in accordance
with national guidelines
including ‘Good Practice
Guidelines for General
Practice Electronic
Patient Records’.”
As well as having to give regard to the above issues when considering a diagnostic support system, GPs will have to also consider how the application of such a system might drive changes in practice methodology. The arrival of a system will among other things offer GPs guidelines through which they can model decisions and will offer the opportunity for greater consistency across the practice as long as everybody in the practice operates the system in the same manner.
Knowledge Makes DemandsKnowledge is a powerful tool and can drive continual performance improvement but users
need to understand that this is an opportunity and not a threat. As the RCGP Roadmap (see references above) puts it;
“GPs need increased access to diagnostics… GPs are hampered in their efforts to provide best clinical care through a lack of access to diagnostics… This creates bottlenecks and waiting lists.”
But there is also, according to the RCGP Good Practice Guidelines… an obligation on the practice to ensure that all possible sources of data are properly captured. As well as consultations this will include correspondence and reports from other parts of the practice or the Health Service.
The integration of decision support into Electronic Medical Record (EMR) systems offers significant potential to improve the health outcome and enhance quality of care through, for example, alerts and reminders and adherence to guidelines such as for screening and immunisation. But better health outcomes will not solely be achieved through adoption of technology as much as by the exchange of relevant information at the point of care20.
The arrival of clinical diagnostic software raises issues in both directions for GPs: there will be a number of system requirements with which the software will need to cope but, on the other hand, the software will create operational opportunities which if incorporated into practice methodology will considerably improve clinical and financial outcomes.
MICROLOOP SPIROMETER

SPECIAL REPORT: CLINICAL DIAGNOSTICS SOFTWARE SOLUTIONS
WWW.PRImARyCAREREPORTS.CO.UK | 13
Micro Medical – Spirometry Made Simple
Highest standards of care with the right device for your patient.
Spirometry PC software (SPCS)
• Quality assurance for each manoeuvre
• Guidance on between manoeuvre variability
• Confirmation of end of test
• Automatic PDF for exporting to patient records
• Links directly to many GP electronic health record systems
Williams Medical Supplies exclusive UK business partners, please visit www.wms.co.uk
© 2012 CareFusion Corporation or one of its subsidiaries. All rights reserved. 0000CF01428 Iss 2
MasterScreen SENSORMEDICS®
VMAX® Micro Medical
JAEGER® SentrySuite™
ND00108_CF_Generic_250x57_Advert.indd 1 14/05/2012 13:39
It is characteristic of human nature that when presented with something new, and especially something that threatens to take us out of our comfort zone, we naturally resist the change. At the same time, familiarity is often a rose tinted lens through which past practice appears a great deal better than it really was. The arrival of IT-based systems in all sorts of walks of life provides a very powerful illustration of this reality. In a popular UK television comedy show, a bank manager is regularly seen entering all the details for a couple seeking a loan only, finally, to turn to them with a glum face and the information that, “the computer says ‘no’.”
CDSS – Leveraging SkillsIt is a fundamental but widely held misunderstanding that computers think for themselves: they don’t; what they do is, within the parameters of their programming, collect, sort and present large quantities of data that the people who use them can then apply in a decision-making process. The one exception might seem to be those city financial systems that buy and sell without human intervention but even they only operate within pre-set thresholds.
In light of this it is not surprising that a number of GPs have struggled with the notion of allowing a computer system to share the diagnostic consultation with them; but once it is understood that the system supports the clinician’s decision and does not make that decision, it can be seen that Clinical Diagnostic Software (CDS) or Clinical Decision Support Systems (CDSS) far from threatening the GP’s role, by incorporating all relevant information about the patient, the symptoms and wider experience will actually enhance their effectiveness. Add to that a database of drugs, therapies and treatments for various conditions and the benefits become unarguable.
Evidence of a Better FutureAs long ago as 2005, a review into the operation of diagnostic systems concluded that they had
improved practitioner performance in 64% of the 100 studies included. Moreover they had also improved patient outcomes in 13% of those studies. But in order to get these kinds of results there was an obligation on the users. In the trials, certain CDSS features were associated with success including the system’s integration into the clinical workflow, it being electronic rather than paper-based and the decision support being at the time and location of the consultation21.
In the UK, the Royal College of General Practitioners (RCGP) in its2007 publication, ‘The Future Direction of General Practice: a roadmap’22 paints the picture of how the new order using IT based solutions might look using an example that will be familiar to GPs…
Where Now for Diagnostic Support Systems?John Hancock
Improvements will be more in how the technology is used than in the software itself
The future has to be better than the past: what better diagnostics and commissioning power could mean for patients
NowA 49-year-old woman presents with recurrent bouts of abdominal pain in the right upper quadrant. The GP suspects gallstones and requests an abdominal ultrasound, which is done after nine weeks. This confirms gallstones and the patient is referred to general surgery. After a wait of 13 weeks the patient is put on a waiting list for laparoscopic cholecystectomy. In the interim she has presented on two further occasions with similar pain to the accident & emergency unit of the local hospital. She has the operation six months later. She is discharged, develops a fever and presents to her GP. The practice has not received a discharge summary.
The future has to be better than the pastPatient has on-site, same-day liver function tests and other blood tests. An ultrasound is arranged for the same week at a local practice that has the facilities and a trained imaging specialist. This confirms the diagnosis and, using information about providers and surgeon, the patient elects to choose her hospital and is directly booked under a care pathway arrangement for a laparoscopic

SPECIAL REPORT: CLINICAL DIAGNOSTICS SOFTWARE SOLUTIONS
14 | WWW.PRImARyCAREREPORTS.CO.UK
The big change is likely
to be in the quality of
outcomes from using
a diagnostic support
programme resulting
from the ability of the
system to incorporate
ever greater ranges
of information on a
variety of levels.
This example is particularly pertinent because it also illustrates that clinical diagnostic solutions do not work in isolation but are a key element (the co-ordinating element) in a whole system that takes advantage of modern technology to improve the quality of healthcare and the outcomes from diagnosis. It also chimes well with a reformed NHS where the GP is at the centre of patient care throughout the system.
What’s in the Future?Clinical diagnostic support software is still a relatively new addition to the GP’s toolbox with a great deal of development still to be done. So, what will determine the future of CDS/CDSS and how might that future look?
While the quality and capability of the technology may well improve, the big change is likely to be in the quality of outcomes from using a diagnostic support programme resulting from the ability of the system to incorporate ever greater ranges of information on a variety of levels. Much of this will be the result of the development of artificial neural networks which, like human minds, can collect and manage information from the wider world (experience) from research, experiments and trials, from the patient’s family history and from the symptoms with which the individual patient presents.
Because healthcare needs grow exponentially with population growth and as the options for treatment and cure increase, the future of systems which can deploy a GP’s skills across a much wider range of tasks is assured. So the more important question is not how CDS/CDSS will develop but rather how skilled GP practices will become at organising themselves to get the very best value from the systems. As Syed Tirmizi, M.D. said in closing his presentation on ‘Clinical Decision Support Systems’23:
“This is not about technology… It is about results: improved health care quality [and] improved health outcomes.”
cholecystectomy. A patient adviser gives support and information of what to expect. On discharge a summary is delivered electronically.
Source: RCGP
SPECIAL REPORT: CLINICAL DIAGNOSTICS SOFTWARE SOLUTIONS
WWW.PRImARyCAREREPORTS.CO.UK | 15
References:1 NICE Diagnostics Assessment Program
http://www.nice.org.uk/aboutnice/whatwedo/aboutdiagnosticsassessment/DiagnosticsAssessmentProgrammeManual.jsp
2 RCGP ‘The Future Direction of General Practice – a Roadmap’ http://www.rcgp.org.uk/pdf/roadmap_embargoed%2011am%2013%20Sept.pdf 3 NICE: Diagnostic guidance in development http://guidance.nice.org.uk/Type/DT/Published
4 NICE: Diagnostic guidance in development http://guidance.nice.org.uk/DT/InDevelopment
5 RCGP The Good Practice Guidelines for GP electronic patient records http://www.rcgp.org.uk/pdf/Health_Informatics_Good_Practice_Guidelines_for_GP_electronic_patients.pdf
6 SearchHealthIT ‘clinical decision support system (CDSS)’ published October 2010 at http://searchhealthit.techtarget.com/definition/clinical-decision-support-system-CDSS
7 healthinfomatics http://healthinformatics.wikispaces.com/Clinical+Decision+Support+Systems
8 Clinical Decision Support Systems: Fahhad Farukhi http://www.cwru.edu/med/epidbio/mphp439/Clinical_Decision.htm
9 Engle RL. Attempts to use computers as diagnostic aids in medical decision making.
10 http://en.wikipedia.org/wiki/Clinical_decision_support_system
11 NICE Diagnostic Assessment Programme http://www.nice.org.uk/aboutnice/whatwedo/aboutdiagnosticsassessment/diagnosticsassessmentprogramme.jsp
12 Clinical Decision Support Systems. A paper by Syed Tirmizi, MD http://uk.search.yahoo.com/r/_ylt=A7x9QXhSVLpP9VoAtXhLBQx.;_ylu=X3oDMTE1YmtiajcxBHNlYwNzcgRwb3MDMjAEY29sbwNpcmQEdnRpZANVS0MwMDJfNzI-/SIG=12s9821ed/EXP=1337640146/**http%3a//gunston.gmu.edu/healthscience/740/Presentations/SyedTirmiziMD.ppt
13 healthinfomatics http://healthinformatics.wikispaces.com/Clinical+Decision+Support+Systems
14 NICE Diagnostics Assessment Programme manual http://www.nice.org.uk/media/A0B/97/DAPManualFINAL.pdf page 9.
15 The Future Direction of General Practice - A roadmap http://www.rcgp.org.uk/pdf/roadmap_embargoed%2011am%2013%20Sept.pdf
16 The Good Practice Guidelines for GP electronic patient records v4 (2010) http://www.rcgp.org.uk/pdf/Health_Informatics_Good_Practice_Guidelines_for_GP_electronic_patients.pdf
17 Clinical Decision Support Systems. A paper by Syed Tirmizi, MD http://uk.search.yahoo.com/r/_ylt=A7x9QXhSVLpP9VoAtXhLBQx.;_ylu=X3oDMTE1YmtiajcxBHNlYwNzcgRwb3MDMjAEY29sbwNpcmQEdnRpZANVS0MwMDJfNzI-/SIG=12s9821ed/EXP=1337640146/**http%3a//gunston.gmu.edu/healthscience/740/Presentations/SyedTirmiziMD.ppt
18 The Future Direction of General Practice - A roadmap http://www.rcgp.org.uk/pdf/roadmap_embargoed%2011am%2013%20Sept.pdf
19 Dep’t. of Health, ‘Modernising Information Management and Technology in General Practice’ http://www.dh.gov.uk/prod_consum_dh/groups/dh_digitalassets/@dh/@en/documents/digitalasset/dh_4138803.pdf
20 Centres for Disease Control and Prevention ‘Clinical Decision Support’ http://www.cdc.gov/osels/ph_informatics_technology/Clinical_Decision_Support.html
21 Wikipedia http://en.wikipedia.org/wiki/Clinical_decision_support_system
22 ‘The Future Direction of General Practice: a roadmap’ http://www.rcgp.org.uk/pdf/roadmap_embargoed%2011am%2013%20Sept.pdf
23 Clinical Decision Support Systems, Syed Tirmizi, MD http://uk.search.yahoo.com/r/_ylt=A7x9QXhSVLpP9VoAtXhLBQx.;_ylu=X3oDMTE1YmtiajcxBHNlYwNzcgRwb3MDMjAEY29sbwNpcmQEdnRpZANVS0MwMDJfNzI-/SIG=12s9821ed/EXP=1337640146/**http%3a//gunston.gmu.edu/healthscience/740/Presentations/SyedTirmiziMD.ppt
Global BusinessMedia
primary care Reports
the leading specialist online research and networking resource for General practitioners and other senior primary care professionals.
• Uptotheminutenewsandothercontentavailabletoallsiteusersona free-of-charge, open access basis.
• QualifiedsignedupmembersareabletoaccesspremiumcontentSpecialReports and interact with their peers using a variety of advanced online networking tools.
• Designedtohelpusersidentifynewsolutions,understandtheimplications of different choices and select the best options available.
• ThoughtLeadership–Adviceandguidancefrominternationallyrecognisedprimary care key opinion leaders.
• PeerInput–Contributionsfromseniorprimarycareprofessionals.
• IndependentEditorialContent–Expertandauthoritativeanalysisfrom award winning journalists and leading industry commentators.
• UnbiasedSupplierProvidedContent.
• Designedtofacilitatedebate.
• Writtentothehighestprofessionalstandards.
Visit: www.primarycarereports.co.uk
Related Documents











