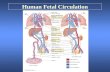
Special circulation - fetal Fetal circulation.
Jan 18, 2016
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript





Special circulation - fetal

Fetal circulation

birthChanges in pressure closure of foramen ovale• Umbilical artery ligation 2x increase of peripheral
resistance increase of blood pressure in left heart and systemic circulation
• Lung inflation + vasodilatation 5x decrease of resistance decrease of blood pressure in right heart
Changes in pO2 closure of ductus arteriosus• pO2 from 20 to 100 mm Hg vasoconstriction
closure 1-8 days later + fibrotization after 1-4 monthsVascular spasm closure of ductus venosusChange HbF into HbA

Relative blood distribution

Specific circulation – coronary blood flow

Specific circulation – brain and blood-brain barrier

Specific circulation – portal systems

Specific circulation – countercurrent mechanism

Specific circulation – liver and intestine Hepatic
sinuses
Blood supply to enterocytes

The goals of regulationThe goals of regulation
To increase blood flow where necessary(working muscle, digestion, gland secretion etc)
To regulate temperatureskin vasodilatation/vasoconstriction resulting in heat spare/loss
To maintain constant blood flow where necessary and/or functional(brain, heart, … kidney, lungs)

heart (cardiomotor) inotropy, bathmotropy, chronotropy, dromotropy
blood (volume) vasomotor
vasodilatation x vasoconstriction
principlesprinciples
β-2 adrenergic receptor↑Gs activity → ↑AC activity → ↑cAMP → ↑PKA activity → phosphorylation of MLCK → ↓MLCK activity → dephosphorylation of MLC
↑α1 adrenergic receptorActivation of Gq --> ↑PLC activity --> ↑IP3 and DAG --> activation of IP3 receptor in SR --> ↑intracellular Ca2+

Regulation of blood Regulation of blood circulationcirculation
Mechanisms of regulation: Local
Humoral (chemical) – O2, CO2, H+
Nervous Enzymatic and hormonal
General/systematic Fast = short-term (regulate blood pressure) Slow = long-term (regulate blood volume) –
several days

Local chemical regulatory Local chemical regulatory mechanismsmechanisms
The most obvious in the heart and the brain Goal: autonomic regulation of resistance
by organ based on its metabolic needs Principle: accumulation of products of
metabolism (CO2, H+, lactic acid ) or consumption of substances necessary for proper function (O2) directly affects smooth muscles of vessels and induce vasodilatation

Figure 1: Brain maps illustrating increasing activity and functional connectivity of perisylvian and extrasylvian areas in both hemispheres as
subjects read words, sentences and narratives. These emergent, context-dependent effects are demonstrated using both fMRI and EEG coherence methods.

Figure 44: Across-subjects (N=10) z-statistic maps overlaid on an anatomical template.
Congruent audiovisual speech activated the auditory and the visual cortical areas, as well as the inferior frontal, the premotor and the visual-parietal areas bilaterally (upper panel).
Incongruent audiovisual speech caused a similar but more extensive pattern of brain activity (middle panel). The difference reached significance in three left hemisphere areas: Brocat’s area (BA44/45), superior parietal lobule (BA7) and prefrontal cortex (BA10) (lower panel). In the contrast ’Congruent > Incongruent’ no statistically significant voxels were detected. Activation images were thresholded using clusters determined by voxel-wise Z>3.0 and a cluster significance threshold of p<0.05, corrected for multiple comparisons.

Local nervousLocal nervous The most obvious in the skin and mucous Goal: central regulation of blood distribution Principle: Autonomic nervous system
Sympaticus Vasoconstriction – activation of α receptors in vessels-
noradrenalin (glands, GIT, skin, mucous, kidneys, other inner organs)
Vasodilatation – activation of β receptors in vessels – adrenalin (heart, brain, skeletal muscles)
Parasympaticus - Acetylcholin Vasoconstriction – heart Vasodilatation – salivatory glands, GIT, external genitals

Platelets Thromboxan A – vasoconstriction
Endothelium Prostacyclin – vasodilatation Endothel-derived relaxing factor = NO
(arginin =>nitric oxid synthetase=>NO=>G-cyclase =>cGMP => vasodilatation)
Endothelin1 most potent vaso/venoconstrictor, receptors in smooth muscles, besides circulation in kidney GFR. Activated by Angiotensin-II, catecholamines etc
Local enzymatic and Local enzymatic and hormonalhormonal
bala
nce

Local enzymatic and Local enzymatic and hormonalhormonal
Plasma protein - Kinin ↑ = vasodilatation bradykinin and kallikrein A role in inflammation, coagulation, pain and
gland secretion (sweat, salivatory, pancreas -> increases blood flow locally)
Hormones of adrenal medula: adrenalin (vasodilatation), noradrenalin (vasoconstriction)

General fast & slow General fast & slow regulatory mechanisms regulatory mechanisms

General fast (short-General fast (short-term) regulatory term) regulatory
mechanisms mechanisms Nervous autonomic reflexes
Baroreflex glomus caroticum, glomus aorticum Afferentation: IX and X spinal nerve Centre: medulla oblongata, nucleus
tractus solitarii Efferentation: X spinal nerve (ps),
sympathetic fibers Effectors: heart (atriums), vessels Effect: After acute increase of blood
pressure – activation of receptors – decrease of blood pressure (vasodilatation, decrease of effect of sympathetic nerves)

right: Pathways within the lower brain stem and spinal cord that subserve the baroreceptor and chemoreceptor reflex control of the sympathetic outflow to the heart and blood vessels. The open triangles indicate excitatory synaptic inputs and the filled triangles inhibitory synaptic inputs. CVLM, caudal ventrolateral medulla; IML intermediolateral cell column in the spinal cord; KF, Kölliker-Fuse nucleus in pons; NTS, nucleus tractus solidarus.
SYMP
PARASYMP

Carotid sinus massagePurpose
Sinus, in this case, means an area in a blood vessel that is bigger than the rest of the vessel. This is a normal dilation of the vessel. Located in the neck just below the angle of the jaw, the
carotid sinus sits above the point where the carotid artery divides into its two main
branches. Rubbing the carotid sinus stimulates an area in the artery wall that contains nerve endings. These nerves respond to changes in blood pressure and are capable of slowing the
heart rate. The response to this simple procedure often slows a rapid heart rate (for
example, atrial flutter or atrial tachycardia) and can provide important diagnostic information to
the physician.Description
The patient will be asked to lie down, with the neck fully extended and the head turned away from the side being massaged. While watching an electrocardiogram monitor, the doctor will gently touch the carotid sinus. If there is no change in the heart rate on the monitor, the pressure is applied more firmly with a gentle
rotating motion. After massaging one side of the neck, the massage will be repeated on the other side. Both sides of the neck are never massaged
at the same time.

General fast (short-General fast (short-term) regulatory term) regulatory
mechanismsmechanisms Humoral mechanisms
Adrenalin – β receptors → vasodilatation → ↓ peripheral resistance → blood from skin and GIT to skeletal muscles, heart and brain → ↑ minute heart volume
Noradrenalin – α receptors → vasoconstriction → ↑ blood pressure
Renin-angiotensin – activated by ↓ pressure in vas afferens

slow (long-term)slow (long-term)
Regulatory mechanisms of water and electrolytes exchanges
autoregulation of total blood volume by kidneys When ↓ blood volume → ↓ of filtration pressure in glomeruli →
↓ production of urine → ↑ volume of circulating blood → ↑ blood pressure
Increase of ADH (vasopressin) ↑ ADH → ↑ of the permeability of collecting ductus for the
water → water is reabsorbed → ↑ volume of circulating blood → ↑ blood pressure
Increase of Aldosterone ↑ aldosterone → ↑ reabsorbtion Na+ and water → ↓ volume of
urine → ↑ volume of circulating blood → ↑ blood pressure

IntracIntracardardial regulatory ial regulatory mechanisms (2)mechanisms (2)
Ionotropic effect of heart rhythm ↑ heart frequency → ↑ amount of Ca2+
that goes into heart cells → ↑ Ca2+ available for tubules of sarkoplasmatic reticulum → ↑ Ca2+ that is freed by each contraction → ↑ strength of contraction

IntracIntracaarrddial regulatory ial regulatory mechanisms (1)mechanisms (1)
Frank-Starling’s law = initial length of the fibers is determined by the degree of diastolic filling of the heart, and the pressure developed in the ventricle is proportionate to the total tension developed.
The developed tension increases as the diastolic volume increases until it reaches a maximum, then tends to decrease.
Ganong: Review of Medical Physiology

MyoMyoccardardiumium – correlation – correlation lengthlength x x tensiontension
Frank-Starling’s law = initial length of the fibers is determined by the degree of diastolic filling of the heart, and the pressure developed in the ventricle is proportionate to the total tension developed.
The developed tension increases as the diastolic volume increases until it reaches a maximum, then tends to decrease.
Ganong: Review of Medical Physiology
beta receptor activation blockage

Related Documents