Child and Adolescent Social Work Journal Volume 15, Number 4, August 1998 Risk and Resilience in Late Adolescence Dina M. Carbonell, Ph.D., Helen Z. Reinherz, Sc. D., and Rose M. Giaconia,, Ph.D. ABSTRACT: Differences among three outcome groups of late adolescents identified as at risk for major depression were investigated. Adolescents with major depression, with other psychiatric diagnoses, and with no diagnoses differed in major areas of functioning and well-being, with the most diffi- culties shown by those with depression. The phenomenon of resilience was examined among the at-risk adolescents with no diagnosis, revealing that family cohesion and social support are associated with resilience. Implications for social work practice and research include the need to focus on promoting family strengths. Introduction Depression among children and adolescents has been widely studied because of the toll it takes on effective functioning and on the emo- tional lives of young people. Strong relationships have been found be- tween childhood depression and problems in adulthood (Harrington, Rutter & Fombonne, 1996) and between depression and a variety of other adult problems (Egeland, Pianta & Ogawa, 1996; Grilo, Walker, Becker, Edell & McGlaskan, 1997), such as compromised functioning, substance use and dependency. The consequences of this devastating disorder make it compelling to identify both risk factors associated This work was supported by NIMH grant #MH41569-07. It was adapted from the doctoral dissertation of Dr. Carbonell at the College, completed in April, 1996. The authors wish to thank dissertation committee member Dr. William Beardslee for his contributions. The authors are associated with the Young Adult Research Project at the Simmons College School of Social Work. Address communications to Dr. Carbonell at Simmons College School of Social Work, 51 Commonwealth Avenue, Boston, Massachusetts 02116. 251 © 1998 Human Sciences Press, Inc.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Child and Adolescent Social Work JournalVolume 15, Number 4, August 1998
Risk and Resiliencein Late Adolescence
Dina M. Carbonell, Ph.D., Helen Z. Reinherz, Sc. D.,and Rose M. Giaconia,, Ph.D.
ABSTRACT: Differences among three outcome groups of late adolescentsidentified as at risk for major depression were investigated. Adolescents withmajor depression, with other psychiatric diagnoses, and with no diagnosesdiffered in major areas of functioning and well-being, with the most diffi-culties shown by those with depression. The phenomenon of resilience wasexamined among the at-risk adolescents with no diagnosis, revealing thatfamily cohesion and social support are associated with resilience. Implicationsfor social work practice and research include the need to focus on promotingfamily strengths.
Introduction
Depression among children and adolescents has been widely studiedbecause of the toll it takes on effective functioning and on the emo-tional lives of young people. Strong relationships have been found be-tween childhood depression and problems in adulthood (Harrington,Rutter & Fombonne, 1996) and between depression and a variety ofother adult problems (Egeland, Pianta & Ogawa, 1996; Grilo, Walker,Becker, Edell & McGlaskan, 1997), such as compromised functioning,substance use and dependency. The consequences of this devastatingdisorder make it compelling to identify both risk factors associated
This work was supported by NIMH grant #MH41569-07. It was adapted from thedoctoral dissertation of Dr. Carbonell at the College, completed in April, 1996. Theauthors wish to thank dissertation committee member Dr. William Beardslee for hiscontributions.
The authors are associated with the Young Adult Research Project at the SimmonsCollege School of Social Work. Address communications to Dr. Carbonell at SimmonsCollege School of Social Work, 51 Commonwealth Avenue, Boston, Massachusetts02116.
251 © 1998 Human Sciences Press, Inc.

with it and potential protective mechanisms that may be maximizedin order to enhance resistance to depression.
This study investigated differences among several groups of youngpeople at risk of developing major depression by late adolescence. Italso examined the phenomenon of resilience among late adolescentsat risk for major depression and focused on the relationship betweenpsychosocial resilience, family cohesion, and social support. Finally,the study investigated the importance of family and social support inpromoting well-being and positive functioning, with the purpose ofidentifying areas of potential intervention for clinical and preventionefforts (Beardslee et al., 1997).
Risk factors for emotional difficulties and poor functioning can bedistinct life events, individual characteristics, or ongoing circum-stances in a person's environment (Werner, 1989). Some examples ofcommon childhood risk factors are physical abuse, the loss of a par-ent, a learning disability, chronic poverty, serious illness, and wit-nessing violence. The presence of risk factors indicates that a child isin a group that has been identified as being more likely than othergroups to develop a difficulty (Kraemer et al., 1997). Risk factors donot predict a particular negative outcome with certainty; they simplyexpose individuals to circumstances associated with a higher inci-dence of that outcome.
Factors associated with resilience, defined as protective mecha-nisms (Rutter, 1987), are those that are defined as operating to pro-tect those at risk from the effects of the risk factors. They have beenstudied to increase the understanding of effective interventions withpopulations at risk. These factors can also be individual or environ-mental (Brooks, 1994), varying in how easily they are influenced bypsychosocial intervention. Rutter (1987) questioned whether protec-tive mechanisms are actually distinguishable from the opposite ofrisk factors; for example, a child at risk because of early parental lossmay not be at risk if the protective mechanism of positive substituteparenting is available.
The way in which protective mechanisms operate to promote re-silience in the presence of risk remains a topic of debate among re-searchers and clinicians. Various models have been developed and in-vestigated (Ensel & Lin, 1991), with the conclusion that a complexinteraction of individual and environmental factors promotes re-silience (Rutter, 1994). Despite the confusion that sometimes sur-rounds the constructs of risk, protective mechanisms, and resilience,research in these areas is compelling. The potential to decrease the
252 CHILD AND ADOLESCENT SOCIAL WORK JOURNAL

likelihood of serious emotional difficulties holds promise for prevent-ing human suffering and its concomitant interference with socialfunctioning.
Research Design
The current study was part of a larger longitudinal research projectat the Simmons College School of Social Work (Reinherz et al., 1993b)that has followed a community population since the respondents werein kindergarten. Extensive prospective data were gathered at inter-vals of three to six years (ages 5, 9, 15, and 18) through structuredinterviews and questionnaires administered to the respondents, theirparents, and their teachers. The interviews included multiple stan-dardized measures of academic, psychological, family, and social func-tioning. The study of risk and resilience in late adolescence was asubstudy of the longitudinal parent study.
The operational definition of risk for the current study was derivedfrom the research project's findings on risk for depression (Reinherzet al., 1993b). The research project had found that the presence of atleast three of the risk factors in the lives of the young people in-creased the odds of developing major depression by the age of eigh-teen.
The questions addressed in the risk and resilience study were thefollowing:
1) What differences in functioning and well-being are thereamong the three groups of at-risk adolescents: those with de-pression, those with another diagnosis, and those with no di-agnosis?
2) What family and social support factors distinguish adoles-cents who are resilient?
Population
The population for the study consisted primarily of white working-class and lower-middle-class (Hollingshead, 1971) families living in arelatively stable community bordering a large city in the North-eastern United States. Approximately four hundred respondents par-ticipated in the study at the age of eighteen. For most of the adoles-
DINA M. CARBONELL, HELEN Z. REINHERZ, AND ROSE M. GIACONIA 253
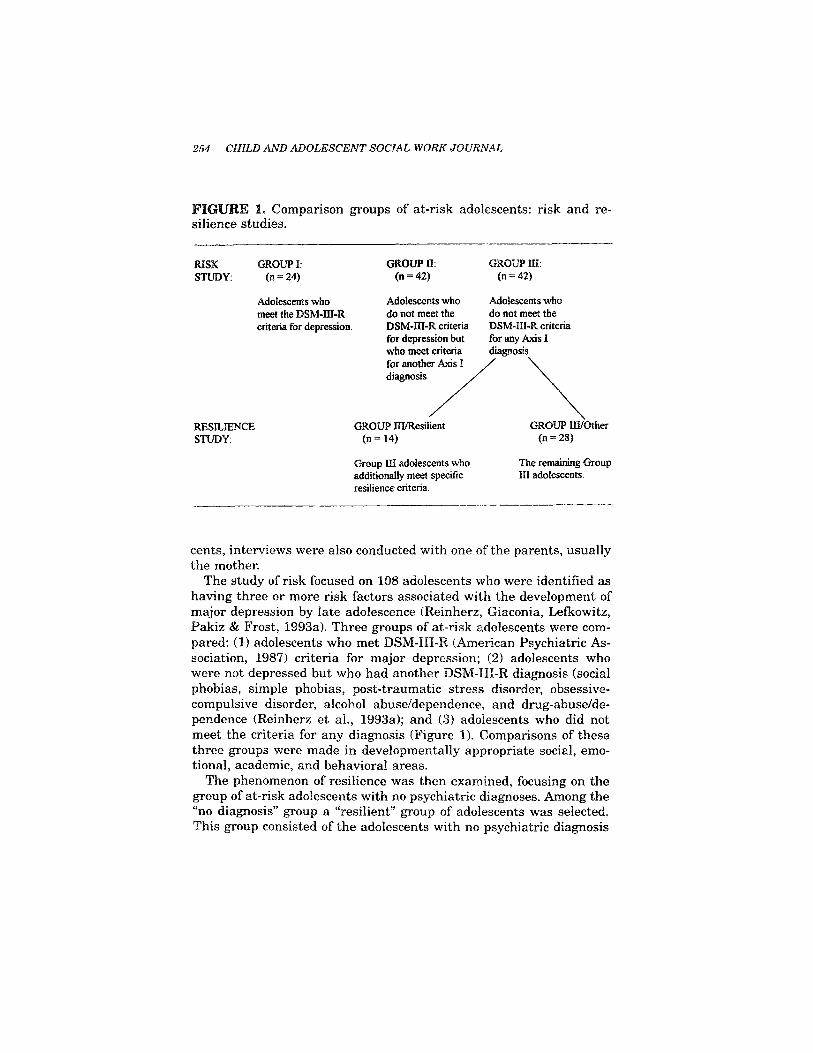
FIGURE 1. Comparison groups of at-risk adolescents: risk and re-silience studies.
cents, interviews were also conducted with one of the parents, usuallythe mother.
The study of risk focused on 108 adolescents who were identified ashaving three or more risk factors associated with the development ofmajor depression by late adolescence (Reinherz, Giaconia, Lefkowitz,Pakiz & Frost, 1993a). Three groups of at-risk adolescents were com-pared: (1) adolescents who met DSM-HI-R (American Psychiatric As-sociation, 1987) criteria for major depression; (2) adolescents whowere not depressed but who had another DSM-III-R diagnosis (socialphobias, simple phobias, post-traumatic stress disorder, obsessive-compulsive disorder, alcohol abuse/dependence, and drug-abuse/de-pendence (Reinherz et al., 1993a); and (3) adolescents who did notmeet the criteria for any diagnosis (Figure 1). Comparisons of thesethree groups were made in developmentally appropriate social, emo-tional, academic, and behavioral areas.
The phenomenon of resilience was then examined, focusing on thegroup of at-risk adolescents with no psychiatric diagnoses. Among the"no diagnosis" group a "resilient" group of adolescents was selected.This group consisted of the adolescents with no psychiatric diagnosis
254 CHILD AND ADOLESCENT SOCIAL WORK JOURNAL

who additionally exhibited a high level of positive functioning andwell-being. They were then compared to the remainder of the non-diagnosed youth. Figure 1 illustrates the design of the study.
Measures
Risk Factors
Risk factors for depression in late adolescence were derived from ear-lier analyses with the entire community sample (Reinherz et al.,1993b). These included a negative perception of one's role in the fam-ily at the age of nine, unpopularity at the age of nine, and anxiety atthe age of fifteen, reported by either the adolescent or by the parent.In addition, risk factors identified for female respondents includedfamily composition (position later in the sibling birth order, havingolder parents, and having at least three siblings), anxiety at the ageof nine, a poor self-concept at the age of nine, health problems arisingbetween the ages of ten and fifteen, the death of a parent by agefifteen, and pregnancy by the age of fifteen. For the male respon-dents, risk factors also included health problems at birth, a seriousillness by the age of five, dependency at the age of five, family conflictbetween the ages of ten and fifteen (also identified as a risk factor forboys in other research; see, e.g., Harold, Fincham, Osborne and Con-ger; 1997), and parental remarriage by the age of fifteen (Reinherz etal., 1993b).
Measures of Functioning and Well-Being
Behavioral Difficulties. Self-reported behavioral difficulties weremeasured through the Youth Self-Report (Achenbach, 1991), a 112-item instrument with an alpha measure of consistency of .92 on totalproblems in the present study. The three groups were compared oneach of the eight behavior clusters, on overall Internalizing Behaviorand Externalizing Behavior, and on Total Problems scores.
Academic Functioning. The academic functioning of the diagnosticgroups was compared using a measure of achievement (high schoolgrade point average), from respondents' transcripts, and graduationor continued enrollment in high school versus dropping out.
DINA M. CARBONELL, HELEN Z. REINHERZ, AND ROSE M. G1ACONIA 255
Self-Esteem. The Rosenberg Self-Esteem scale (Rosenberg, 1986)provided a measure of overall self-esteem. This scale had an alpha of.86 in the longitudinal study. It consists often items that ask for per-ceptions of oneself (e.g., "I feel I do not have much to be proud of," and"On the whole, I am satisfied with myself).
Socioemotional Adjustment. The diagnostic groups were comparedon anxiety and self-perceived unpopularity through subscales of thePiers-Harris Children's Self-Concept Scale (Piers, 1984). The longi-tudinal study yielded an internal consistency of .80 for the Anxietysubscale and of .70 for the Popularity subscale.
Intepersonal Problems. The Interpersonal Problems Scale (Reinherzet al., 1993a), with an alpha reliability of .75 in the parent study, wasused to compare the three groups on perceived difficulties in interper-sonal interaction. This six-item scale includes "having difficultiescommunicating with others," "experiencing conflicts with people towhom you are close," and "lacking a close companion or best friend."
Data Analysis
The three outcome groups were compared using a three-way ANOVAanalysis (Kerlinger, 1986). The resilient group was contrasted withthe remainder of the adolescents with no diagnosis through t-tests.
Findings
There were striking differences among the three outcome groups ontheir behavioral, academic, and psychosocial functioning. The de-pressed group reported greater behavioral difficulties than one orboth of the other groups on a majority of the scales, while the respon-dents with no diagnosis, not surprisingly, consistently emerged as theleast troubled group.
Differences in Behavioral Difficulties
Distinct differences were noted in overall behavioral functioningamong the three diagnostic groups. As anticipated, the depressedgroup reported greater difficulties of an internalizing nature, includ-ing social withdrawal, apathy, and feelings of worthlessness. Sur-prisingly, they also reported a greater number of externalizing behav-
256 CHILD AND ADOLESCENT SOCIAL WORK JOURNAL
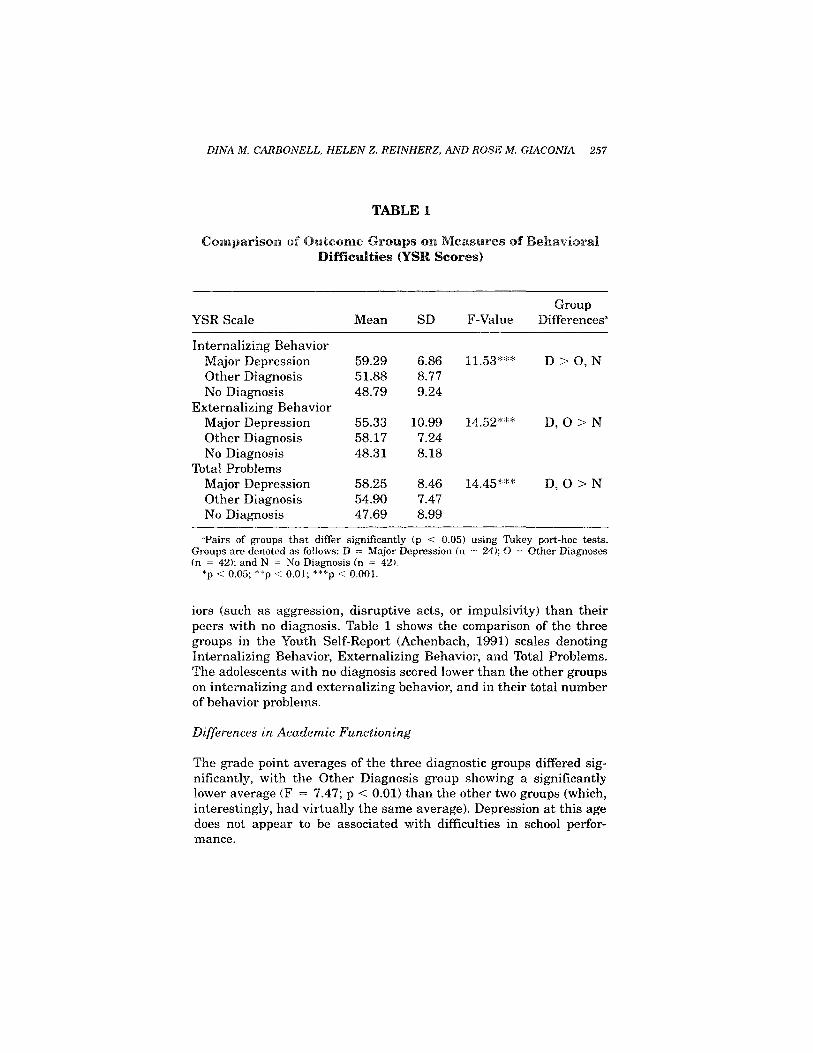
TABLE 1
Comparison of Outcome Groups on Measures of BehavioralDifficulties (YSR Scores)
YSR Scale
Internalizing BehaviorMajor DepressionOther DiagnosisNo Diagnosis
Externalizing BehaviorMajor DepressionOther DiagnosisNo Diagnosis
Total ProblemsMajor DepressionOther DiagnosisNo Diagnosis
Mean
59.2951.8848.79
55.3358.1748.31
58.2554.9047.69
SD
6.868.779.24
10.997.248.18
8.467.478.99
F-Value
11.53***
14.52***
14.45***
GroupDifferencesa
D > O, N
D, O> N
D, O >N
"Pairs of groups that differ significantly (p < 0.05) using Tukey port-hoc tests.Groups are denoted as follows: D = Major Depression (n = 24); O = Other Diagnoses(n = 42); and N = No Diagnosis (n = 42).
*p < 0.05; **p < 0.01; ***p < 0.001.
iors (such as aggression, disruptive acts, or impulsivity) than theirpeers with no diagnosis. Table 1 shows the comparison of the threegroups in the Youth Self-Report (Achenbach, 1991) scales denotingInternalizing Behavior, Externalizing Behavior, and Total Problems.The adolescents with no diagnosis scored lower than the other groupson internalizing and externalizing behavior, and in their total numberof behavior problems.
Differences in Academic Functioning
The grade point averages of the three diagnostic groups differed sig-nificantly, with the Other Diagnosis group showing a significantlylower average (F = 7.47; p < 0.01) than the other two groups (which,interestingly, had virtually the same average). Depression at this agedoes not appear to be associated with difficulties in school perfor-mance.
DINA M. CARBONELL, HELEN Z. REINHERZ, AND ROSE M. GIACONIA 257
The three groups were not found to differ significantly in schooldropout rates. However, since the total number of dropouts was only9, it would be difficult to conclude that there is no difference in therisk of dropping out among members of the three groups.
Differences in Social and Emotional Adjustment
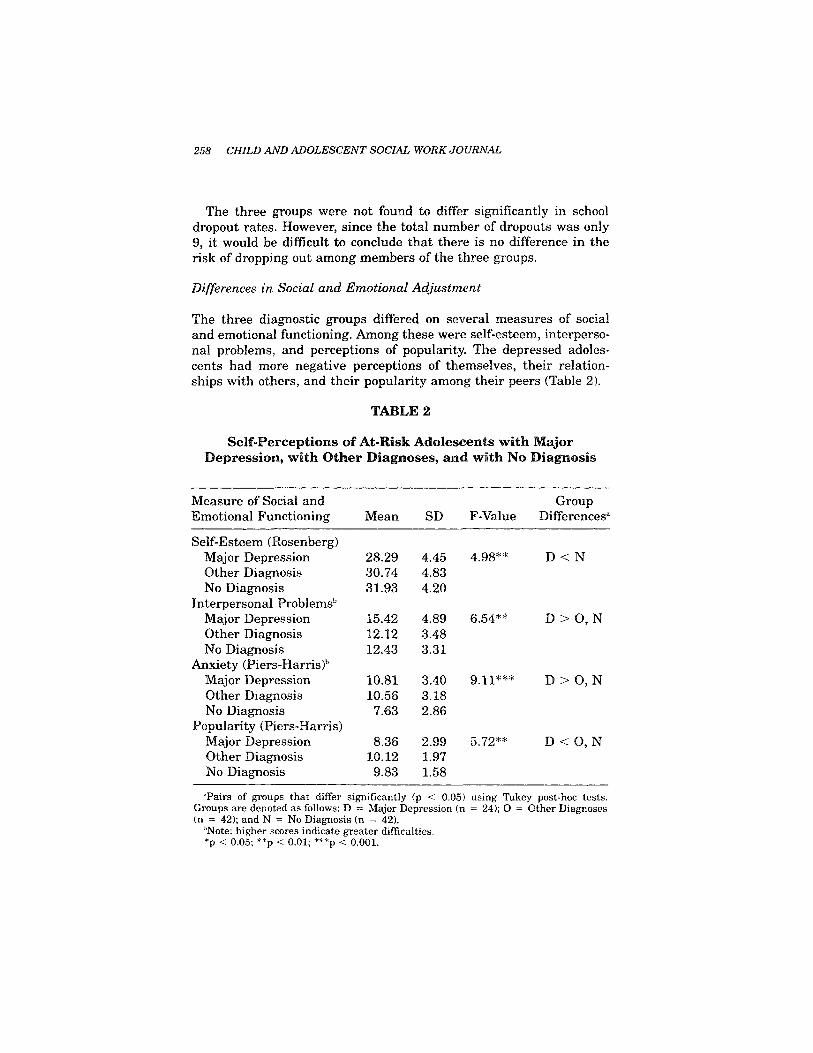
The three diagnostic groups differed on several measures of socialand emotional functioning. Among these were self-esteem, interperso-nal problems, and perceptions of popularity. The depressed adoles-cents had more negative perceptions of themselves, their relation-ships with others, and their popularity among their peers (Table 2).
TABLE 2
Self-Perceptions of At-Risk Adolescents with MajorDepression, with Other Diagnoses, and with No Diagnosis
Measure of Social andEmotional Functioning
Self-Esteem (Rosenberg)Major DepressionOther DiagnosisNo Diagnosis
Interpersonal Problemsb
Major DepressionOther DiagnosisNo Diagnosis
Anxiety (Piers-Harris)b
Major DepressionOther DiagnosisNo Diagnosis
Popularity (Piers-Harris)Major DepressionOther DiagnosisNo Diagnosis
Mean
28.2930.7431.93
15.4212.1212.43
10.8110.567.63
8.3610.129.83
SD
4.454.834.20
4.893.483.31
3.403.182.86
2.991.971.58
F-Value
4.98**
6.54**
9.11***
5.72**
GroupDifferencesa
D < N
D > O, N
D>0 , N
D < O, N
'Pairs of groups that differ significantly (p < 0.05) using Tukey post-hoc tests.Groups are denoted as follows: D = Major Expression (n = 24); O = Other Diagnoses(n = 42); and N = No Diagnosis (n = 42).
bNote: higher scores indicate greater difficulties.*p < 0.05; **p < 0.01; ***p < 0.001.
258 CHILD AND ADOLESCENT SOCIAL WORK JOURNAL

The adolescents with major depression had a significantly lowermean self-esteem score, reported a greater number of interpersonalproblems, saw themselves as less popular, and indicated greaterlevels of anxiety than the other adolescents. These findings are notsurprising in light of the relationship between depression and a nega-tive self-concept and a pessimistic view of others and of the world ingeneral.
Summary
The findings of this Study reveal some of the costs of risk factors inthe lives of adolescents. While the majority of respondents at risk formajor depression by the age of eighteen did not meet criteria for thediagnosis, over half of those at risk met diagnostic criteria for someDSM-III-R disorder, including depression.
The depressed adolescents reported experiencing the most diffi-culties in various areas of their lives. Their internalizing behaviorssignify risk for low achievement, a negative self-concept, a pessimisticoutlook on life, and the general lack of enjoyment that characterizesdepression. Additionally, their externalizing behavior problems makethem vulnerable to a broad range of social and interpersonal strug-gles.
The group with no diagnosis consistently showed more positiveemotional and behavioral adjustment than their peers who were de-pressed or who had another diagnosis. The next section will illustratethe phenomenon of resilience among members of this group.
Resilient Adolescents
The phenomenon of resilience among people at risk for emotional dif-ficulties is increasingly the focus of mental health research. The ques-tion of why some people face adversity with the ability to surmountits obstacles is compelling to professionals interested in preventingpsychosocial problems and in fostering positive functioning among at-risk groups (Feehan, McGee, Williams & Nada-Raja, 1995). The studyof resilience among young people is particularly important because ofits ability to inform work in the field of prevention and early interven-tion.
Psychological resilience has been defined as the capacity to be un-affected by, to recover from, or even to gain strength or to grow from
DINA M. CARBONELL, HELEN Z. REINHERZ, AND ROSE M. GIACONIA 259
difficult life experiences or circumstances (Egeland, Carlson & Sroufe,1993; Luthar, 1991). It is the phenomenon of unexpected or unlikelypositive outcomes among individuals at risk for psychosocial problems.
A multidimensional definition of resilience was central to the con-ceptual framework of this study. Global resilience, if it is defined asunusually positive adjustment despite the presence of risk, cannot bemerely a sense of feeling well or the ability to function in sociallyapproved ways. It must include both well-being and positive function-ing in a variety of domains, as advocated by Luthar, Doernberger, andZigler (1993). These domains need to reflect, the definition of positivefunctioning in an individual's own social and cultural group.
Specific Criteria for Resilience
Respondents were defined as resilient if they reached the thresholdfor being at risk for major depression and simultaneously met criteriafor positive functioning and well-being. Their positive functioning andwell-being comprised the realm of "doing well" in life, spanning bothbehavioral and affective arenas.
The fourteen adolescents who were resilient were compared to theother twenty-eight respondents who were at risk for depression anddid not meet diagnostic criteria for any disorder. This comparison wasmade to identify factors that were associated with positive function-ing and well-being.
The criteria for resilience were the following:
1) Resistance to major depression.
« The absence of lifetime clinical depression according to theDSM-III-R (American Psychiatric Association, 1987) criteriafor the syndrome.
e The presence of at least three of the risk factors for major de-pression for the population.
2) The absence of another lifetime DSM-III-R Axis 1 diagnosis in-cluded in the parent study (simple and social phobia, PTSD, alcoholor drug abuse or dependency, and obsessive compulsive disorder).
3) Positive functioning.
• The absence of significant externalizing behavioral difficultieson the Youth Self-Report (Achenbach, 1991).
260 CHILD AND ADOLESCENT SOCIAL WORK JOURNAL

• Age and culturally congruent role fulfillment that is perceivedas adequate, as indicated by completion of or continued enroll-ment in school and adequate grades.
4) A sense of well-being.
• Positive self-perception, as indicated by a score on the Rosen-berg Self-Esteem Scale (Rosenberg, 1986) that is above themedian for the total sample.
• Below the median score on the six-item Interpersonal Prob-lems Scale developed by the Longitudinal Research Project(Reinherz et al., 1993a).
These measures were selected as indicators of resilience because theyhave been identified as important in the research literature and be-cause they reflect the respondents' own definitions of feeling and do-ing well in life. They are also consistent with their social referencegroup.
To summarize, respondents were included in the resilient group ifthey were at risk for major depression, did not develop depression bylate adolescence, did not meet criteria for another disorder, were func-tioning in positive ways, and reported a sense of well-being.
Characteristics of Family Environment Associated with Resilience
Family factors included cohesion and functioning:(1) Family Cohesion—The perception of family cohesion was mea-
sured by the cohesion subscale of the Family Adaptability and Cohe-sion Evaluation Scales III (FACES III; Olson, Portner & Lavee, 1985),an instrument with a reliability of .84 in the longitudinal study. Theten-item cohesion subscale asks respondents to rate how often certainfamily behavior occurs in their families on a 5-point scale, from "al-most never" to "almost always." The statements include the followingexamples: "Family members ask each other for help" and "Family to-getherness is very important."
(2) Family Functioning—Six areas of family functioning (health/competence, conflict, communication, cohesion, directive leadership,and expressiveness) were measured through a 36-item self-report in-strument, the Self-Report Family Inventory (SFI; Beavers, Hampson& Hulgus, 1990). On this instrument respondents are asked to indi-cate, on a scale of 1 to 5, how closely each item fits a description of
DINA M. CARBONELL, HELEN Z. REINHERZ, AND ROSE M. GIACONIA 261
their families. The statements include the following: "Family mem-bers pay attention to each other's feelings," "We argue a lot and neversolve problems," and "Our happiest times are at home." Since itemsare coded to indicate problems in functioning, lower scores correspondto more positive family functioning.
Social Support Factors Associated with Resilience
Social support was measured with the Arizona Social Support Inter-view Scale (ASSIS; Barrera, 1980), which elicits perceptions of sup-port in the following areas:
• Assistance (helping with tasks or errands)8 Material aid (lending or giving something valuable)• Advice (being available to give advice)• Positive feedback (expressing approval of ideas or deeds)• Personal information (being available to talk about personal
things)
The ASSIS's focus on perceived support was consistent with thegoals of this study and with other literature on subjective measuresfor such constructs (e.g., Kraemer et al., 1997). This measure cap-tures the degree to which respondents feel they have support avail-able and their evaluation of that support.
Summary of Characteristics of Resilient Adolescents
The Resilient and Other non-diagnosed adolescents were comparedon measures of family environment and social support. Despite thesmall number of respondents included in the Resilient group, somestatistically significant differences emerged between the groups.
Differences in Family Environment
An assessment of the differences in the family environments of the 14resilient and 28 other adolescents with no diagnosis yielded some in-teresting findings despite the relatively small numbers in the twosubgroups. The measures used in this area are self-reports, reflectingthe respondents' perceptions of their own families.
The results on both measures of family environment (FACES III
262 CHILD AND ADOLESCENT SOCIAL WORK JOURNAL
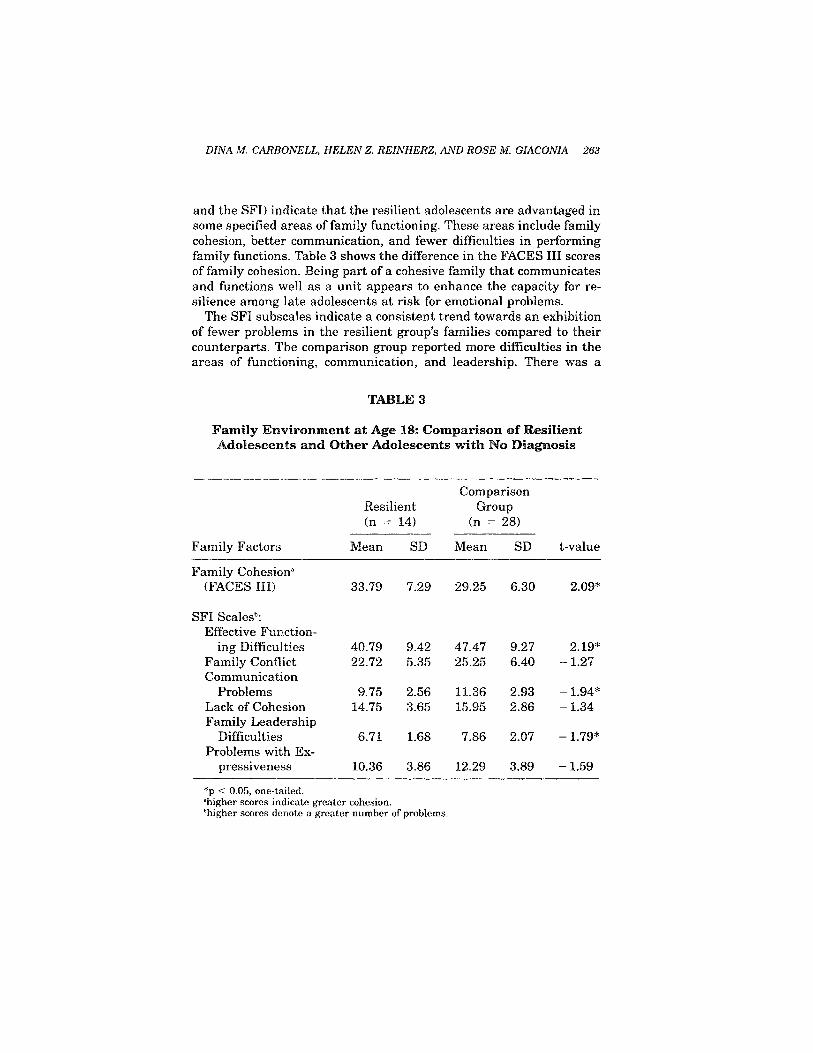
and the SFI) indicate that the resilient adolescents are advantaged insome specified areas of family functioning. These areas include familycohesion, better communication, and fewer difficulties in performingfamily functions. Table 3 shows the difference in the FACES III scoresof family cohesion. Being part of a cohesive family that communicatesand functions well as a unit appears to enhance the capacity for re-silience among late adolescents at risk for emotional problems.
The SFI subscales indicate a consistent trend towards an exhibitionof fewer problems in the resilient group's families compared to theircounterparts. The comparison group reported more difficulties in theareas of functioning, communication, and leadership. There was a
DIN A M. CARBONELL, HELEN Z. REINHERZ, AND ROSE M. GIACONIA 263
TABLES
Family Environment at Age 18: Comparison of ResilientAdolescents and Other Adolescents with No Diagnosis
Resilient(n = 14)
Family Factors
Family Cohesiona
(FACES III)
SFI Scalesb:Effective Function-
ing DifficultiesFamily ConflictCommunication
ProblemsLack of CohesionFamily Leadership
DifficultiesProblems with Ex-
pressiveness
Mean
33.79
40.7922.72
9.7514.75
6.71
10.36
SD
7.29
9.425.35
2.563.65
1.68
3.86
ComparisonGroup
(n = 28)
Mean
29.25
47.4725.25
11.3615.95
7.86
12.29
SD
6.30
9.276.40
2.932.86
2.07
3.89
t-value
2.09*
2.19*-1.27
- 1.94*-1.34
- 1.79*
-1.59
*p < 0.05, one-tailed,'higher scores indicate greater cohesion,'higher scores denote a greater number of problems.
similar trend, though not attaining significance, in the remaining twosubscales, reflecting conflict and expressiveness among family members.
Several other areas of family dynamics were examined for differ-ences among the two groups of adolescents with no diagnosis. Amongthese were parental satisfaction with grade-school performance, posi-tive sibling relationships in mid-adolescence, and supportive relation-ships with siblings in late adolescence.
Perception of parental support throughout their lives seems to beimportant for resilient teenagers. The parents of the resilient adoles-cents reported a higher level of satisfaction (and of concordance withtheir expectations) with their children's achievement in school bythird grade than the parents of the comparison group members (t =1.78, p < 0.05). Whether the children's actual performance levels dif-fered was not explored; however, the support and acceptance of par-ents in this area seems to be associated with positive functioning inlater years.
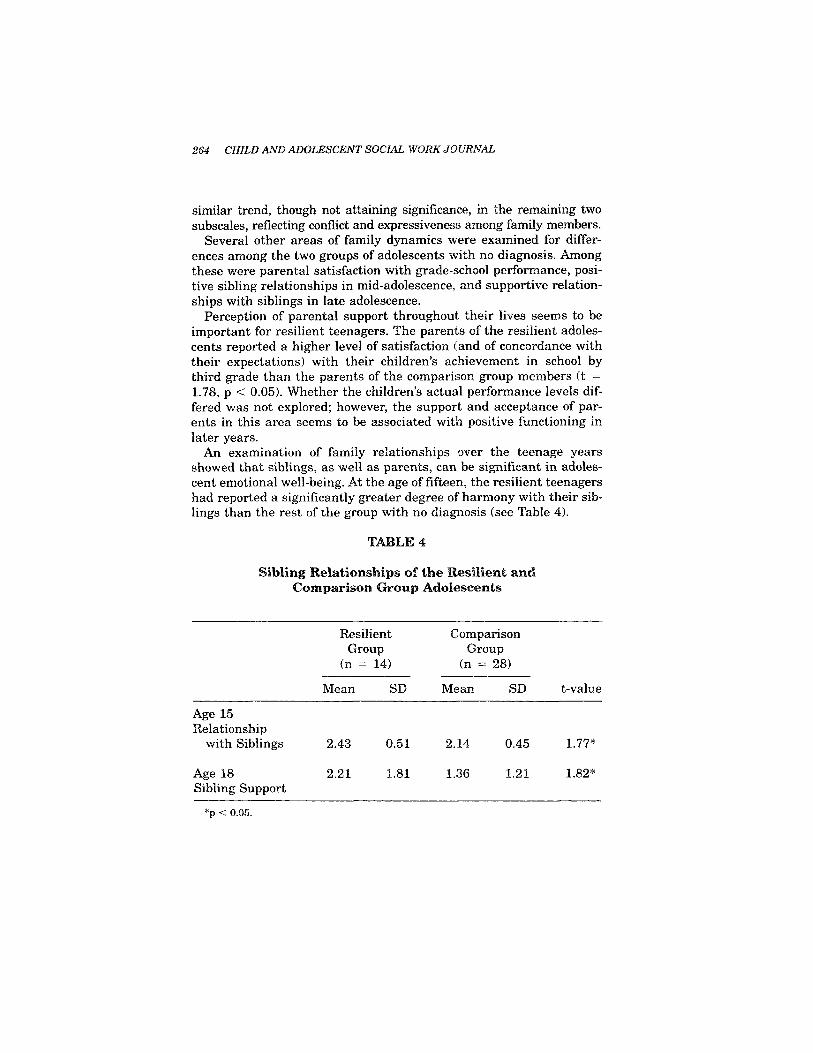
An examination of family relationships over the teenage yearsshowed that siblings, as well as parents, can be significant in adoles-cent emotional well-being. At the age of fifteen, the resilient teenagershad reported a significantly greater degree of harmony with their sib-lings than the rest of the group with no diagnosis (see Table 4).
264 CHILD AND ADOLESCENT SOCIAL WORK JOURNAL
TABLE 4
Sibling Relationships of the Resilient andComparison Group Adolescents
Age 15Relationship
with Siblings
Age 18Sibling Support
ResilientGroup
(n = 14)
Mean
2.43
2.21
SD
0.51
1.81
ComparisonGroup
(n = 28)
Mean
2.14
1.36
SD
0.45
1.21
t-value
1.77*
1.82*
*p < 0.05.

While family cohesion emerged as a significant factor in the lives ofresilient adolescents, no significant differences were reported by thetwo groups in how well they perceived getting along with their par-ents at the age of fifteen. As shown in Table 5, three years later, atthe age of eighteen, the resilient adolescents mentioned siblings assignificant supports more often than the rest of the group. The impor-tance of positive sibling relationships and support in the lives of re-silient adolescents at risk for major depression thus continuedthroughout the teenage years.
Differences in Social Support Networks
The fourteen resilient adolescents and the comparison group oftwenty-eight at-risk youth differed to some extent on their perceivedneed for support and on their level of satisfaction with the supportthey had received over the past few months. These differencesemerged despite the finding that they did not differ in their reports ofsupport network size and general composition.
The resilient group was compared to the remaining no diagnosisgroup on the number of people available to give support, the relation-
DINA M. CARBONELL, HELEN Z. RE1NHERZ, AND ROSE M. GIACONIA 265
TABLES
Level of Satisfaction with Social Support Available in thePast Six Months: Resilient and Comparison Group Members
Type of SupportAvailable
Concrete AssistanceFinancial HelpAdvicePositive FeedbackSharing of Personal
Information
ResilientGroup
(n = 14)
Mean
2.503.002.862.93
2.79
SD
0.860.000.360.27
0.58
ComparisonGroup
(n = 28)
Mean
2.782.892.822.50
2.89
SD
0.580.320.390.64
0.42
t-value
-1.241.80*0.293.06*
-0.65
*p < 0.05.

ship of those people to the respondents, the average depth of eachsupportive role, the perceived need for support beyond the amountthat was available, and the level of satisfaction with the support thatwas given. Table 5 shows these comparisons.
An important difference between the two groups consisted of re-ports by the resilient group of a greater level of satisfaction with thefinancial assistance and positive feedback they received than the com-parison group.
Interestingly, the comparison group also reported a greater need toreceive additional advice than the resilient group (t= -2.14, p <0.05), though the availability of people to provide advice did not actu-ally differ. This could indicate that the resilient adolescents had lessof a need to rely on others, perceived the advice as more effective oruseful, or felt more comfortable with autonomous decision-making.
Discussion
The finding that family cohesion continues to play a central role inthe well-being and functioning of young people emerging from adoles-cence is surprising. There is a commonly held belief that at that ageyouth function with relative autonomy. The family's ongoing impor-tance in their lives is demonstrated by its association with well-beingand positive functioning. Feeling close to one's family may actuallycontribute to competence in autonomous functioning.
The differences in perception of social support may indicate differ-ences in the quality of actual support received or a more positive in-terpretation of life on the part of the resilient adolescents. Their lowerneed for advice may reflect self-reliance, a stronger sense of auton-omy, or a greater general level of satisfaction with the support that isavailable to them. The difference in the positive feedback categorymay also reflect a greater ability among the resilient group to inter-nalize positive feedback, to trust its authenticity and significance, orto use it effectively to enhance well-being.
The salience of family environment and social support as factorsassociated with resilience among late adolescents at risk for majordepression is consistent with the literature (Brooks, 1994; Rutter,1987) and with the expectations of this investigation. Enhancing fam-ily environment and social support clearly is important in decreasingthe likelihood of depression as an outcome in late adolescence.
266 CHILD AND ADOLESCENT SOCIAL WORK JOURNAL

Daniel: A Case Study
Daniel was the second of four children born to Italian-American par-ents in professional-level occupations. Despite some health problemsat birth, he developed into a relatively healthy infant and toddler,suffering only from mild childhood illnesses. Daniel's risk factors formajor depression also included self-perceived unpopularity at the ageof nine and self- and mother reported anxiety in mid-adolescence.
Daniel's early development was unremarkable. At the age of four,he appeared to be a little fidgety and clumsy, described by his parentsas accident-prone. He also seemed serious, at times perhaps sad. Hisparents expressed concern with his mild tendency to have conflictswith other children outside of his sibling group. His kindergartenteacher identified some motor problems and mild inattentiveness andrestlessness as the only areas of concern in school. His interactionswith others were felt to be within acceptable parameters.
Preschool clinical interviews described Daniel as compliant, verbal,able to cope well with conflict, and capable of using reality and fan-tasy creatively. He was also described as friendly, outgoing, content,engaging, happy, confident, and adventurous. The only areas identi-fied as being of potential concern were his tendency to give up easilywhen frustrated, mild lack of coordination, and slight evidence of im-maturity.
Daniel's mother spoke of her preschool son as a child who was intel-ligent, active, and aggressive. She reported that he tended to crymore readily than his brothers and sister. She said that he sometimeshad fights with his siblings, but also seemed to be close to them. Hewas affectionate with people in the family, although he could bestrong-willed and a "sore loser." He later reported that around kinder-garten age he began occasionally to tell lies and to steal small thingsfrom those around him; however, these behaviors did not persist.
Daniel's family, which included live-in grandparents, was close-knit, sharing meals and enjoying a variety of mutual activities. Theywent to the beach and to the movies and spent time reading together.The family spoke the grandparents' primary language at home, sothat Daniel and his siblings were raised to be bilingual in Italian andEnglish.
During later childhood, Daniel would occasionally accompany hisfather to his job at a software laboratory. This experience may wellhave contributed to the boy's later interest in computers. His mother
DINA M. CARBONELL, HELEN Z. REINHERZ, AND ROSE M. GIACONIA 267

also returned to work when he was an infant, continuing a career asan occupational therapist. His parents tended to discuss family issueswith one another and to reach agreements together.
When Daniel was in the fourth grade, his teacher described him asa sad, inattentive child. His parents, on the other hand, said that hewas confident, independent, and expressive at home. However, theyalso described a nine-year-old who tended to be argumentative, un-popular, slow, impatient, and dissatisfied with life. He saw himself asunpopular with the other children. He seemed indifferent to the worldaround him at times, and to experience feelings of worthlessness.
This self-portrait of a withdrawn, isolated child was echoed by Dan-iel's fourth grade teacher. In school, he did not show aggressiveness orirritability; he was rather shy and unpopular, and unlikely to initiateinteraction with the other children. He rarely smiled or laughed. Heappeared slow and detached, often lost in his own thoughts or day-dreams. He spoke little in class and appeared to be performing belowthe expected level for his intelligence, which was judged to be averageat that time. He was often late for school, perhaps reflective of a lowlevel of interest, motivation, or satisfaction with his experiencesthere.
By the age of fifteen, Daniel's investment in school had changeddramatically. He was performing above average and had been placedin an advanced class. He was comfortable in school by this time,showed confidence in his abilities, and reported few behavioral or so-cial difficulties.
Daniel's mother described her adolescent son as someone whoworked hard. His school performance was important to her, and sheexpressed a high degree of satisfaction with his achievement. She wasnot working at this time, but his father had been able to developgreater autonomy in his career and served as a strong role model forDaniel.
In mid-adolescence, Daniel was participating in a few extra-curric-ular activities and was responsible for some household chores. He gotalong well with others. He reported having two or three close friendswith whom he spent time on a regular basis. He stated that he hadexperienced an increase in his peers' acceptance of him since enteringadolescence. He reported substantial social support networks, butsomewhat limited interpersonal closeness.
Daniel had close to an "A" average by the end of high school. Hewas occasionally truant from school, but this apparently did not keephim from performing well. In his senior year, he continued to enjoy
268 CHILD AND ADOLESCENT SOCIAL WORK JOURNAL

school and found most academic work interesting. He planned to at-tend college to study science, probably moving out of his parents'home at that time to live on campus. He expected to be successful inhis career. He found his parents and one teacher very helpful to himin making career plans and decisions.
At the end of high school, Daniel considered two or three other ado-lescents as close friends, seeing them weekly and enjoying spendingtime both alone and with others. This previously awkward andclumsy teenager now participated in sports and other activities. Hewas involved in church youth activities and valued this area of hislife. He also received numerous academic honors and awardsthroughout his high school years.
Daniel worked summers as a paid assistant in a computer facility,a position related to his career aspirations. He also performed a fewchores at home. In addition to these paid and unpaid responsibilities,he volunteered as a tutor and peer instructor.
In late adolescence, Daniel felt that he got along better with hisfamily members and with adults in general than most of his peers. Hedescribed his parents as supportive, though sometimes intrusive. Helisted large networks of people available to assist him and to offerhim emotional support, and was generally satisfied with this aspect ofhis life.
When asked what was most important to him, Daniel listed firsthis family, then his career, and then religious activities. The reversalof his life, from one of considerable difficulty to one he described aspositive and successful, may well have been fostered by his connec-tion to his family and to others in his life. He was able to find a senseof balance among different areas of his life by late adolescence, over-coming much of the sense of isolation and withdrawal that hadseemed to mark his early and middle childhood years.
Conclusion
The findings of this study indicate a strong relationship between re-silience among adolescents at risk for emotional problems and thepresence of family and social support. The quantitative findings wereechoed by the in-depth description of Daniel's life over the course ofhis childhood and adolescence. The continuing importance of the fam-ily in the lives of young people who are on the brink of adulthood maybe surprising in a culture that promotes and highly values autonomy
DINA M. CARBONELL, HELEN Z. REINHERZ, AND ROSE M. GIACONIA 269

and independence. It suggests that even if a significant degree of au-tonomy is achieved by the age of eighteen, the at-risk adolescent con-tinues to benefit greatly from ongoing family support. This phenome-non has led to research on prevention efforts geared towards familiesrather than towards individuals at risk for emotional disorders(Beardslee et al., 1997).
The primary descriptive trend which emerged from the study ofDaniel's life was one of family cohesion, social support, and an atmo-sphere of acceptance. His family members seemed willing to supportone another through hardship. They continued to believe in him dur-ing the time when he was functioning the least well.
The opportunity to discuss difficulties or worries with a receptivefamily member may make a child or adolescent less likely to find ob-stacles insurmountable. This youngster is also more likely to receivesupport in ways that reinforce a positive self-concept. Brooks (1994)defined self-esteem as appreciating one's own worth and importanceand being accountable to oneself and toward others. He viewed it as acontribution to the child's ability to grow both from success and fromfailure, within the context of interpersonal interaction.
The findings of this study are consistent with current social workknowledge. The ability to meet life's demands successfully is devel-oped largely through children's experiences of challenging events thatdo not become overwhelming. Family cohesion and social support mayprovide enough protection, directly or indirectly, to keep risk factorsfrom reaching the point of overwhelming the adolescent, keepingthem in the realm of challenging experiences that promote growthrather than elicit negative outcomes. Belonging in a family that offersa cohesive, well-functioning environment where members communi-cate openly with one another may foster important resources withinthe developing child. It may also protect the child more directly fromthe effects of a risk factor; anxiety, for example, may well elicit pro-tective responses from caring family members.
Resilient adolescents have learned to request and to use assistance,to feel supported in their efforts towards success, and to feel generallysatisfied. The knowledge that others are available to provide supportfosters a sense of security, making it more likely that an individualwill be willing to take risks in life and to venture in directions thatmay be unfamiliar. They are self-confident, independent, able to focustheir attention, and verbal (Hart, Hoffmann, Edelstein & Keller,1997). These factors, while described as individual characteristics, donot develop in a social vacuum. A cohesive family and a social envi-
270 CHILD AND ADOLESCENT SOCIAL WORK JOURNAL

ronment in which there are supportive people may create the culturenecessary for the development of resilience.
The limitations of the findings in this study stem primarily fromthe relatively small number of respondents who were included in thegroup of adolescents who were at risk for depression and were re-silient. Further limitations lie in the area of generalizability, as thecommunity sample was virtually exclusively white, relatively homo-geneous in the areas of ethnicity and socioeconomic status, and lo-cated in one community in New England. However, the findings raiseimportant questions and issues for broader populations of children:How do some children do well despite exposure to risk? Are thereways in which resilience-promoting factors can be provided or en-hanced? Can adversity, at tolerable levels and within a context ofsupport, be a challenge that promotes growth rather than a negativefactor in children's lives?
The findings from this study have implications for the developmentof further research, prevention programs for children, and social workservices for adolescents. The need to facilitate families' maintenanceof a cohesive, communicative, and supportive environment throughtheir adolescent member's pre-adult years calls for comprehensive in-tervention approaches. While increasing degrees of autonomy mayalso have importance in adolescence, the presence of strong familyrelationships does not wane in importance. The ability to promoteprotective mechanisms that meet the needs of young people who havespecific risk factors could be further developed through future re-search efforts.
DIN A M. CARBONELL, HELEN Z. REINHERZ, AND ROSE M. G1ACONIA 271
References
Achenbach, T. C. (1991). Manual for Youth Self-Report and 1991 Profile. Burlington,VT: University of Vermont Department of Psychiatry.
APA. (1987). Diagnostic and statistical manual of mental disorders, IH-R. (Third, Re-vised ed.). Washington, D.C.: American Psychiatric Association.
Barrera, M. (1980). A method for the assessment of social support networks in commu-nity survey research. Connections, 3(1) 8-13.
Beardslee, W. R., Versage, E. M., Wright, E. J., Salt, P., Rothberg, P. C., Drezner, K., &Gladstone, T. R. G. (1997). Examination of preventive interventions for familieswith depression: Evidence of change. Development and Psychopathology, 109-130.
Beavers, W. R., Hampson, R. B., & Hulgus, Y. F. (1990). Beavers systems model manual.Dallas, TX: Southwest Family Institute.
Brooks, R. B. (1994). Children at risk: Fostering resilience and hope. American Journalof Orthopsychiatry, 64(4), 545-553.
Egeland, B., Carlson, E., & Sroufe, L. A. (1993). Resilience as process. Development andPsychopathology, 8(4), 517-528.

Egeland, B., Pianta, R., & Ogawa, J. (1996). Early behavior problems: Pathways tomental disorders in adolescent development and psychopathology. Developmentand Psychopathology, 8(4), 735-749.
Ensel, W. M., & Lin, N. (1991). The life stress paradigm and psychological distress.Journal of Health and Social Behavior, 32(4), 321-341.
Feehan, M., McGee, R., Williams, S. M., & Nada-Raja, S. (1995). Models of adolescentpsychopathology: Childhood risk and the transition to adulthood. Journal of theAmerican Academy of Child and Adolescent Psychiatry 34(5), 670-679.
Grilo, C. M., Walker, M. L., Becker, D. F., Edell, W. S., & McGlaskan, T. H. (1997).Personality disorders in adolescents with major depression, substance use disor-ders, and coexisting major depression and substance use disorders. Journal of Con-sulting and Clinical Psychology, 65(2), 328-332.
Harold, G. T., Fincham, F. D., Osborne, L. N., & Conger, R. D. (1997). Mom and Dad areat it again: Adolescent perceptions of marital conflict and adolescent psychologicaldistress. Developmental Psychopathology, 33(2), 333-350.
Harrington, R., Rutter, M., & Fombonne, E. (1996). Developmental pathways in depres-sion: Multiple meanings, antecedents, and endpoints. Development and Psycho-pathology, 8(4), 601-606.
Hart, D., Hoffmann, V., Edelstein, W., & Keller, M. (1997). The relation of child person-ality types to adolescent behavior and development: A longitudinal study of Icelan-dic children. Developmental Psychology, 33(2), 195-205.
Hollingshead, A. G. (1971). Commentary on "The indiscriminate state of social classmeasurement". Social Forces, 49, 563-567.
Kerlinger, F. N. (1986). Foundations of social research, 3rd edition. Philadelphia: Holt,Rinehart and Winston.
Kraemer, H. C., Kazdin, A. E., Offord, D. R., Kessler, R. C., Jensen, P. S., & Kupfer,D. J. (1997). Coming to terms with the terms of risk. Archives of General Psychia-try, 54(4), 337-343.
Luthar, S. S. (1991). Vulnerability and resilience: A study of high-risk adolescents.Child Development, 62(3), 600-616.
Luthar, S. S., Doernberger, C. H., & Zigler, E. (1993). Resilience is not a unidimensionalconstruct: Insights from a prospective study of inner-city adolescents. Developmentand Psychopathology, 5(4), 703-717.
Olson, D. H., Portner, J.," & Lavee, Y. (1985). FACES III. In D. H. Olson, J. Portner, & Y.Lavee (Eds.), Family Inventories. St Paul, MN: Family Social Science, University ofMinnesota.
Piers, E. V. (1984). The Piers-Harris Children's Self-Concept Scale, Revised Manual.Los Angeles: Western Psychological Services.
Reinherz, H. Z., Giaconia, R. M., Lefkowitz, E. S., Pakiz, B., & Frost, A. K. (1993a).Prevalence of psychiatric disorders in a community population of older adolescents.Journal of the American Academy of Child and Adolescent Psychiatry, 32(2), 369-377.
Reinherz, H. Z., Giaconia, R. M., Pakiz, B., Silverman, A. B., Frost, A. K., & Lefkowitz,E. S. (1993b). Psychosocial risks for major depression in late adolescence: A longi-tudinal community study. Journal of the American Academy of Child and Adoles-cent Psychiatry, 36(6), 1155-1163.
Rosenberg, M. (1986). Conceiving the self. New York: Basic Books.Rutter, M. (1987). Psychosocial resilience and protective mechanisms. American Jour-
nal of Orthopsychiatry, 57(3), 316-331.Rutter, M. (1994). Beyond longitudinal data: Causes, consequences, changes, and conti-
nuity. Journal of Consulting ana' Clinical Psychology, 62(5), 928-940.Werner, E. E. (1989). High-risk children in young adulthood: A longitudinal study from
birth to 32 years, American Journal of Orthopsychiatry, 59(1), 72-81.
272 CHILD AND ADOLESCENT SOCIAL WORK JOURNAL
Related Documents











