Respectful Maternity Care (RMC) in Malawi: Secondary Analysis of Labor and Delivery Observations Reena Sethi Sr. M&E Advisor Jhpiego

Respectful Maternity Care (RMC) in Malawi: Secondary Analysis of Labor and Delivery Observations Reena Sethi Sr. M&E Advisor Jhpiego.
Dec 23, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Respectful Maternity Care (RMC) in Malawi:Secondary Analysis of Labor and Delivery Observations
Reena SethiSr. M&E AdvisorJhpiego
Presentation Outline
Objectives Setting Other studies on respectful maternity care
(RMC) in Malawi Descriptive results from labor and delivery
(L&D) observations Summary of findings Strengths and limitations
Objective of the Analysis
To present the frequency of observed RMC during labor and delivery among women delivering in 40 high-volume government health facilities in Malawi through secondary data analysis
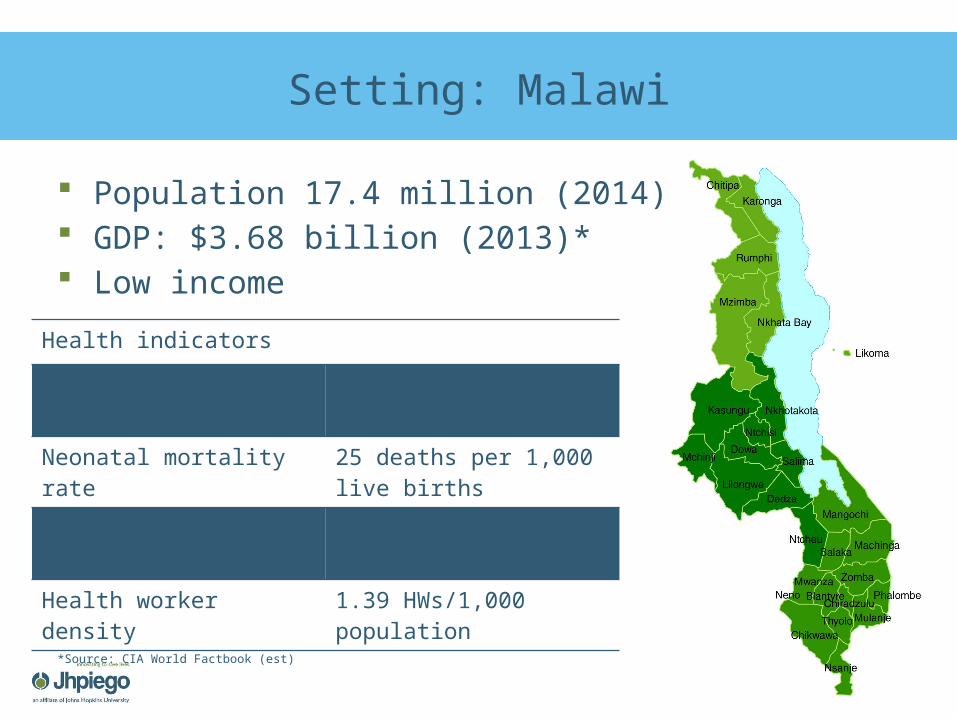
Setting: Malawi
Population 17.4 million (2014)* GDP: $3.68 billion (2013)* Low income
Health indicators
Maternal mortality ratio 460 deaths per 100,000 live births
Neonatal mortality rate 25 deaths per 1,000 live births
Total fertility rate 6.0 children born/woman
Health worker density 1.39 HWs/1,000 population
*Source: CIA World Factbook (est)
Setting: Malawi
Institutional delivery rate: 73%
71% of births attended by a skilled birth attendant
Source: Malawi DHS 2010
A Malawian mother with her two children in Mzimba District, Malawi.© 2008 Lisa Basalla, Courtesy of Photoshare
Previous Studies of RMC in Malawi
Seljeskog et al. 2006: Factors influencing women's choice of place of delivery in rural Malawi: An explorative study
• Staff in L&D wards did not communicate and kept women waiting
• Deliveries without provider assistance
• Privacy was difficult to achieve
Changole et al. 2010: Patients’ satisfaction with reproductive health services at Gogo Chatinkha Maternity Unit, Queen Elizabeth Central Hospital, Blantyre, Malawi
• 99.1% of respondents found their interaction with the provider was either good or very good
• 57.4% knew that it is the right of the patient to have considerate and respectful care
Studies of RMC in Malawi
Kumbani et al. 2012: Do Malawian women critically assess the quality of care? A qualitative study on women’s perceptions of perinatal care at a district hospital in Malawi
• Negative experiences of care included the following: Provider attitudes Delays in care Unavailability of birth
attendant
Kumbani et al. 2013: Why some women fail to give birth at health facilities: A qualitative study of women’s perceptions of perinatal care from rural Southern Malawi
• Health workers shouted at them
• Delays in care• Not always informed of
findings
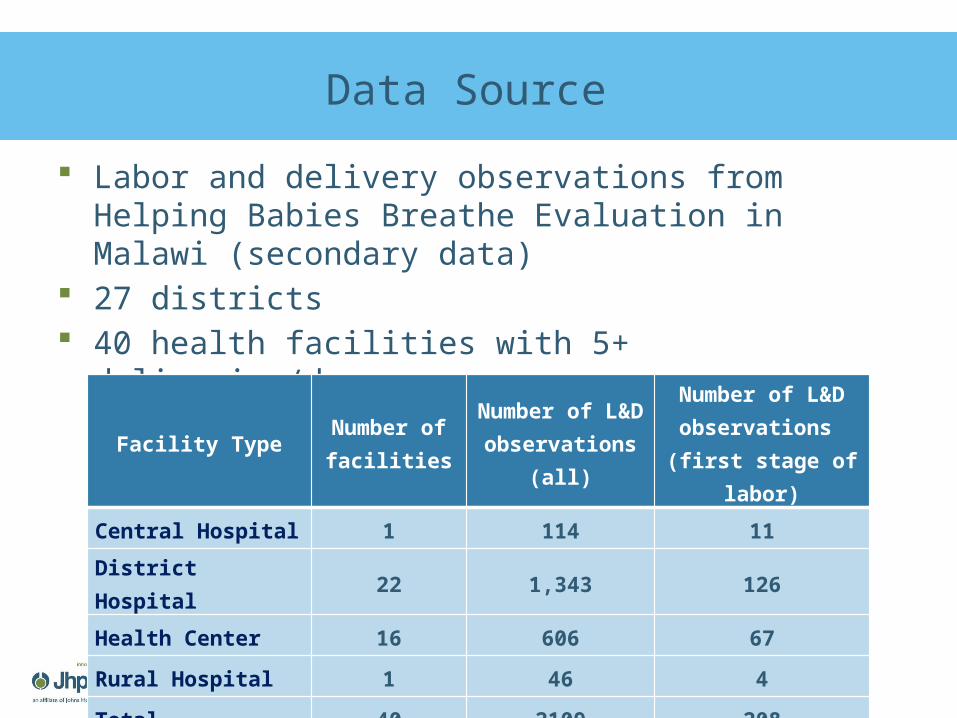
Data Source
Labor and delivery observations from Helping Babies Breathe Evaluation in Malawi (secondary data)
27 districts 40 health facilities with 5+ deliveries/day
Facility TypeNumber of facilities
Number of L&D
observations (all)
Number of L&D observations (first stage of
labor)
Central Hospital 1 114 11
District Hospital 22 1,343 126
Health Center 16 606 67
Rural Hospital 1 46 4
Total 40 2109 208
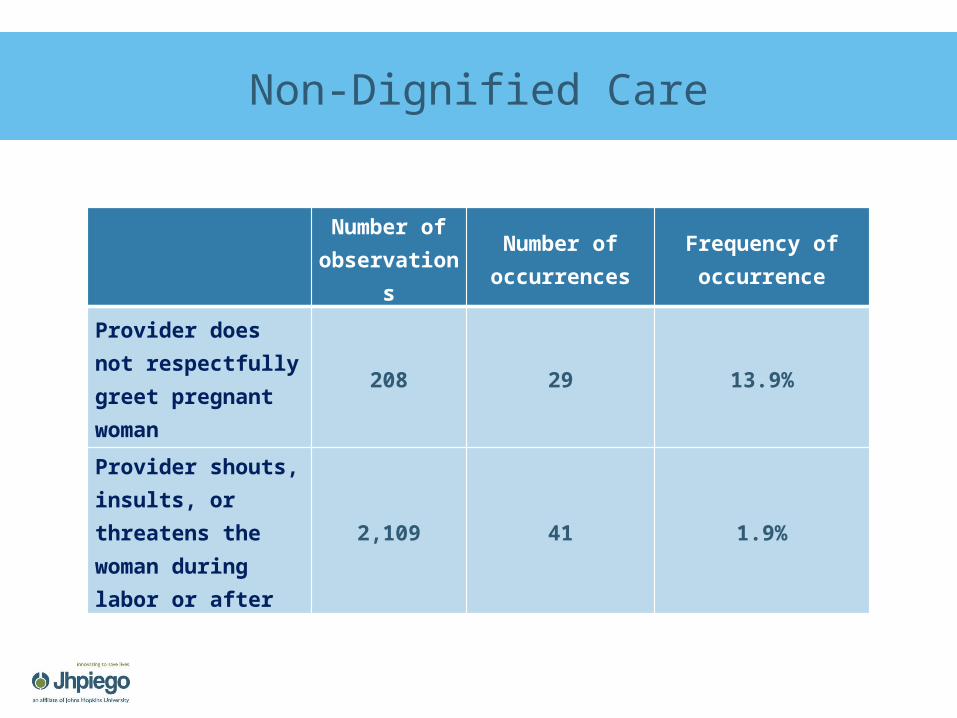
Non-Dignified Care
Number of observatio
ns
Number of occurrences
Frequency of occurrence
Provider does not respectfully greet pregnant woman
208 29 13.9%
Provider shouts, insults, or threatens the woman during labor or after
2,109 41 1.9%
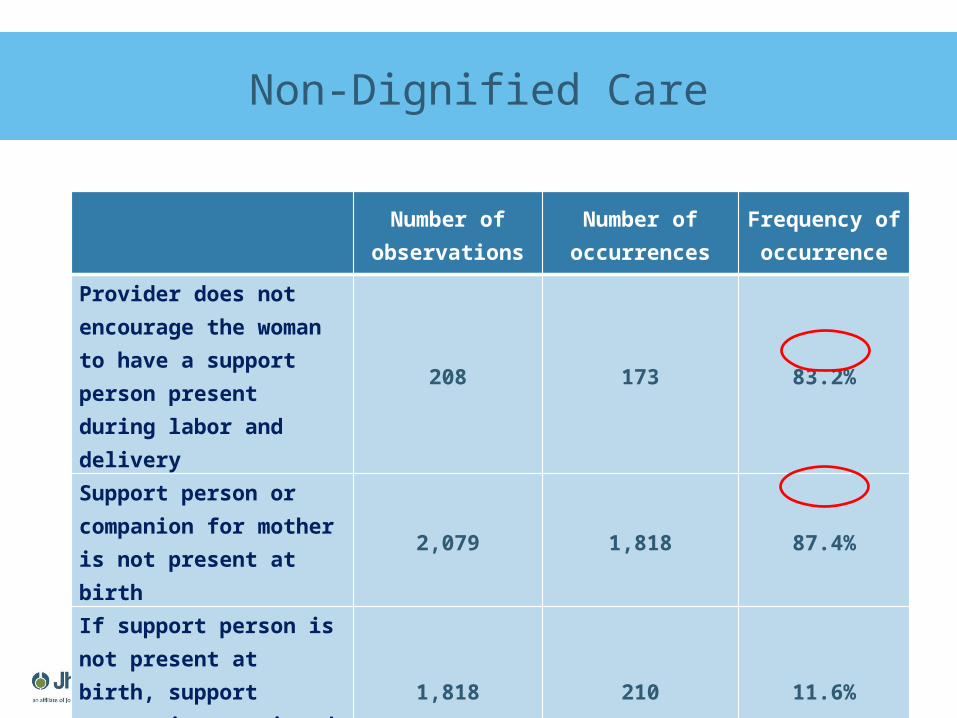
Non-Dignified Care
Number of observations
Number of occurrences
Frequency of occurrence
Provider does not encourage the woman to have a support person present during labor and delivery
208 173 83.2%
Support person or companion for mother is not present at birth
2,079 1,818 87.4%
If support person is not present at birth, support person is restricted from being present
1,818 210 11.6%
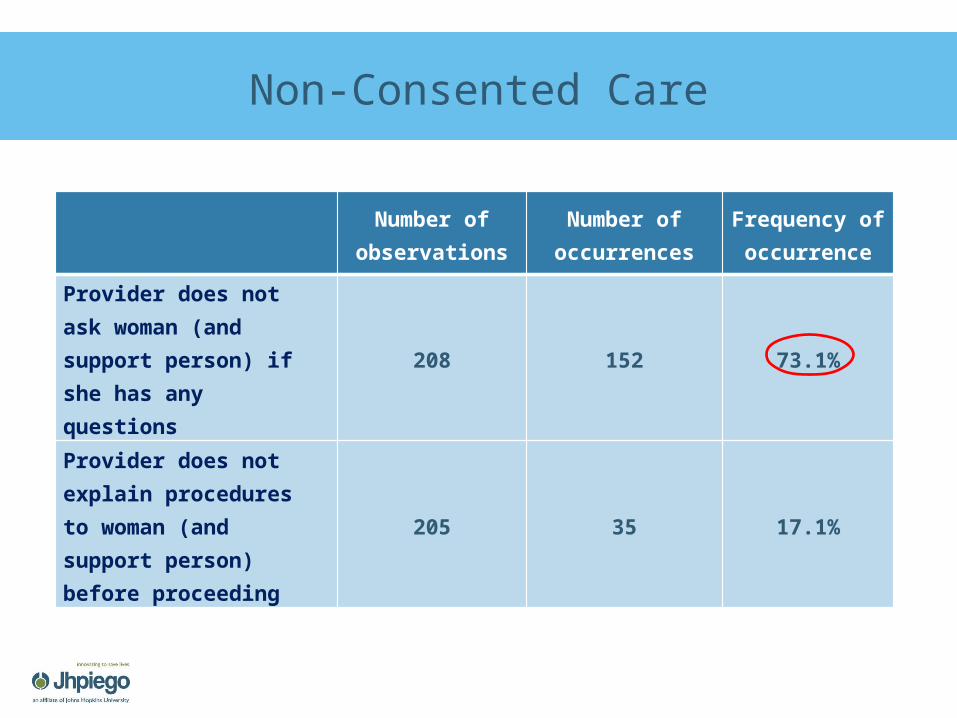
Non-Consented Care
Number of observations
Number of occurrences
Frequency of occurrence
Provider does not ask woman (and support person) if she has any questions
208 152 73.1%
Provider does not explain procedures to woman (and support person) before proceeding
205 35 17.1%
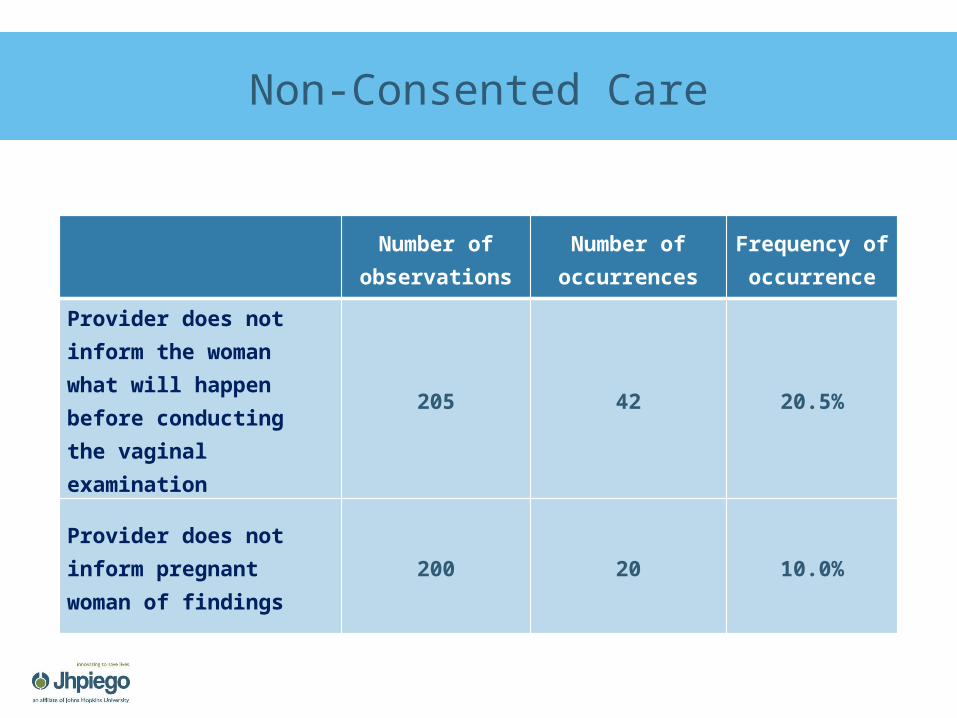
Non-Consented Care
Number of observations
Number of occurrences
Frequency of occurrence
Provider does not inform the woman what will happen before conducting the vaginal examination
205 42 20.5%
Provider does not inform pregnant woman of findings
200 20 10.0%
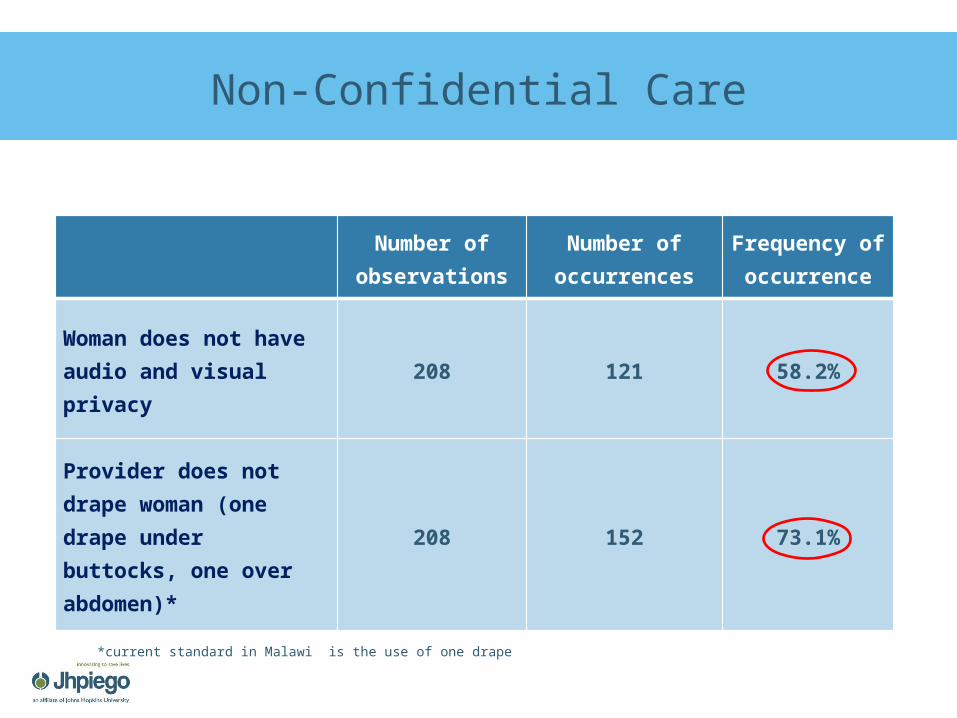
Non-Confidential Care
Number of observations
Number of occurrences
Frequency of occurrence
Woman does not have audio and visual privacy
208 121 58.2%
Provider does not drape woman (one drape under buttocks, one over abdomen)*
208 152 73.1%
*current standard in Malawi is the use of one drape
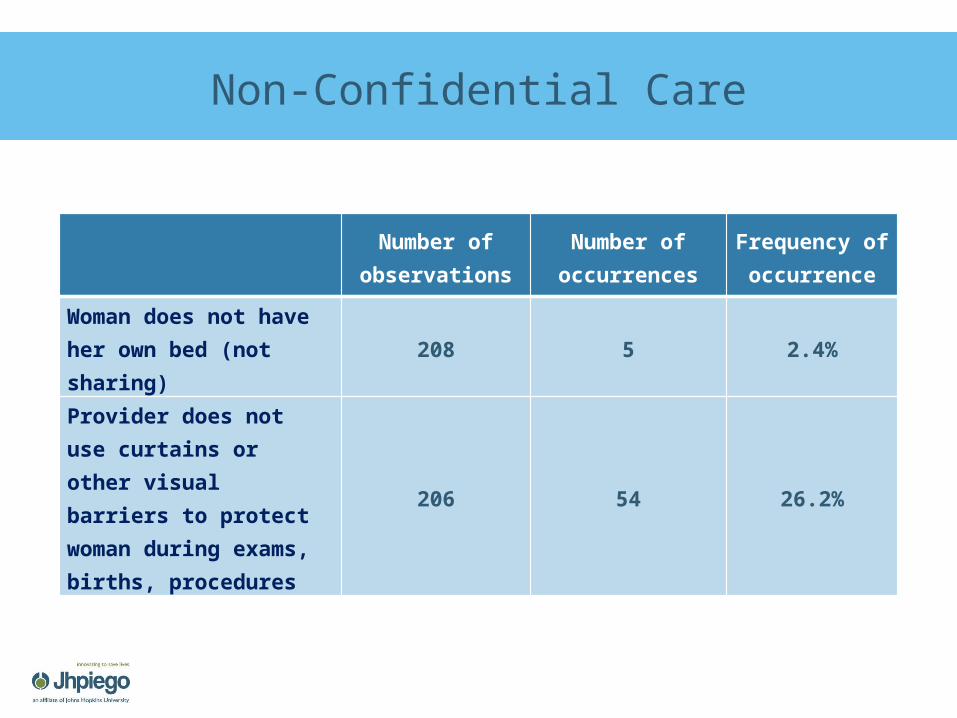
Non-Confidential Care
Number of observations
Number of occurrences
Frequency of occurrence
Woman does not have her own bed (not sharing)
208 5 2.4%
Provider does not use curtains or other visual barriers to protect woman during exams, births, procedures
206 54 26.2%
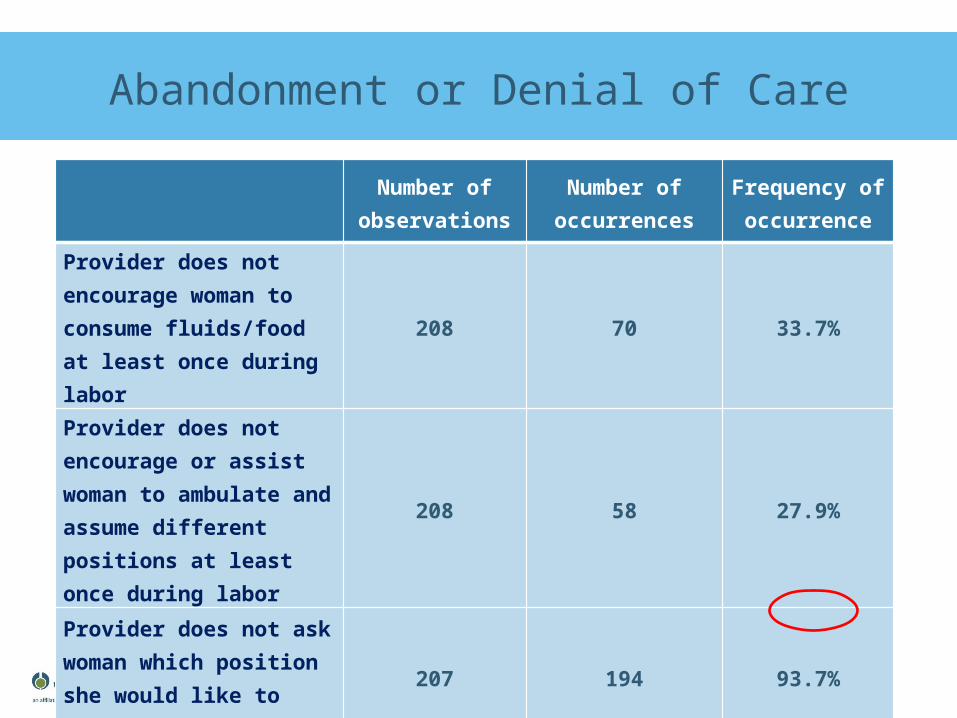
Abandonment or Denial of Care
Number of observations
Number of occurrences
Frequency of occurrence
Provider does not encourage woman to consume fluids/food at least once during labor
208 70 33.7%
Provider does not encourage or assist woman to ambulate and assume different positions at least once during labor
208 58 27.9%
Provider does not ask woman which position she would like to deliver in
207 194 93.7%
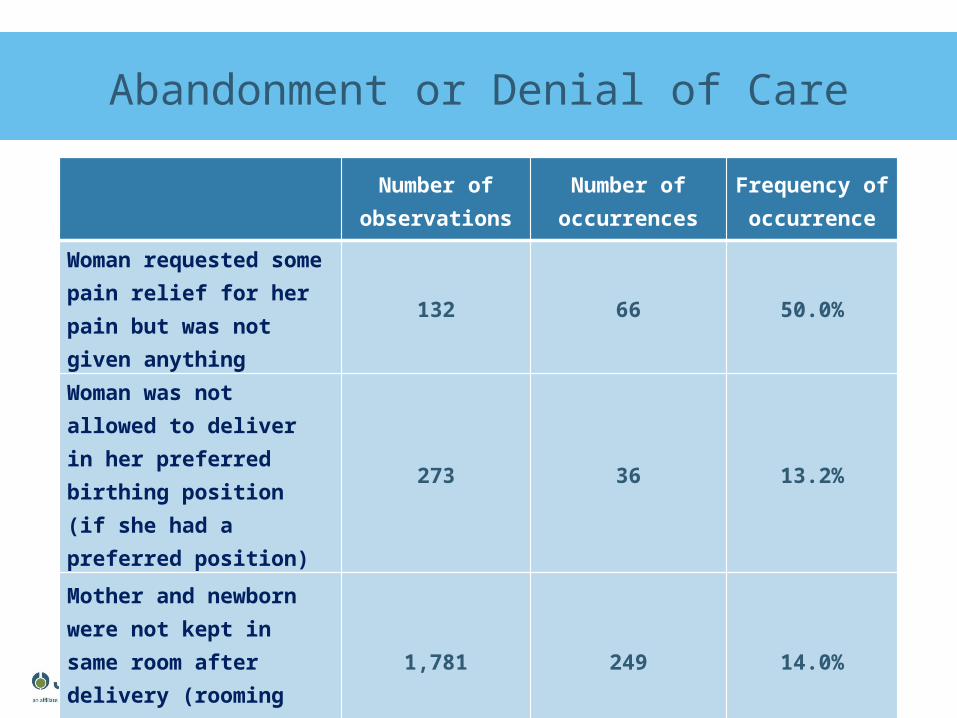
Abandonment or Denial of Care
Number of observations
Number of occurrences
Frequency of occurrence
Woman requested some pain relief for her pain but was not given anything
132 66 50.0%
Woman was not allowed to deliver in her preferred birthing position (if she had a preferred position)
273 36 13.2%
Mother and newborn were not kept in same room after delivery (rooming in)
1,781 249 14.0%
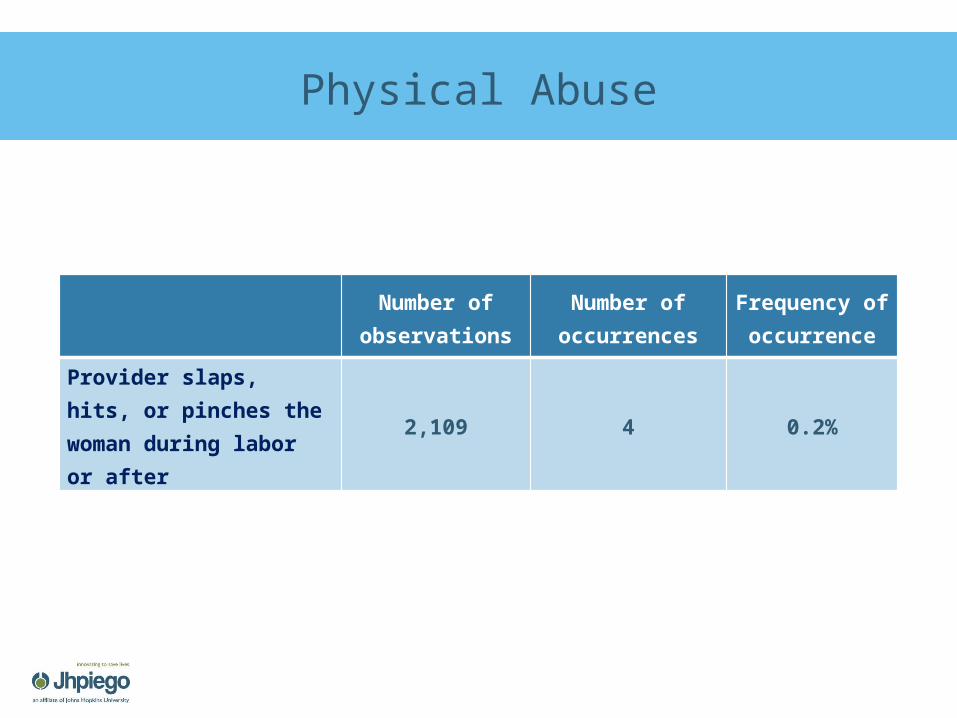
Physical Abuse
Number of observations
Number of occurrences
Frequency of occurrence
Provider slaps, hits, or pinches the woman during labor or after
2,109 4 0.2%
Summary of Findings
Physical abuse was rare Provider-client communication occurred more
frequently in the direction of the provider to the client and less frequently from the client to the provider
A small proportion of women had a support person present
Privacy was an issue in a majority of cases—both audio/visual privacy and personal privacy
Most women were not asked about their preferred birthing position
19
Recommendations
Reinforce RMC during BEmONC trainings and as part of quality improvement standards for labor and delivery
Include RMC in coaching and mentoring Maternity in-charges to facilitate RMC
through supervision
Strengths & Limitations
Direct observations may be an objective measurement method
Possible Hawthorne effect Unable to observe all components of
Rights of Childbearing Women framework Relatively small sample size for RMC items
in the first stage of labor
21
Thank you!
Malawi HBB Evaluation Team:
Shivam Gupta, Abigail Kazembe, Angella Mtimuni, Reena Sethi, Lolade Oseni, Tambudzai Rashidi, Evelyn Zimba, Stella Abwao, Barbara Rawlins, Fannie Kachale
Related Documents