Relation of Atrial Fibrillation and Right-Sided Cardiac Thrombus to Outcomes in Patients With Acute Pulmonary Embolism Piotr Kukla, MD, PhD a, *, Wiliam F. McIntyre, MD b , Goran Koracevic, MD, PhD c , Dusanka Kutlesic-Kurtovic, MD c , Kamil Fijorek, MSc d , Vesna Atanaskovic, MD c , Ewa Krupa, MD e , Ewa Mirek-Bryniarska, MD, PhD f , Marek Jastrze ˛ bski, MD, PhD g , Leszek Bryniarski, MD, PhD g , Piotr Pruszczyk, MD, PhD h , and Adrian Baranchuk, MD i Atrial fibrillation (AF) can induce a hypercoagulable state in both the left and right atria. Thrombus in the right side of the heart (RHT) may lead to acute pulmonary embolism (APE). The aim of the study was to determine the prevalence of RHT and AF and to assess their impact on outcomes in patients with APE. The retrospective cohort included 1,006 patients (598 female), with a mean age of 66 – 15 years. The primary end point was all- cause mortality. The secondary end point was incidence of complications (death, cardio- genic shock, cardiac arrest, vasopressor/inotrope treatment, or ventilatory support). Atrial fibrillation was detected in 231 patients (24%). RHT was observed in 50 patients (5%). The combination of AF and RHT was observed in 16 patients (2%). The overall mortality rate was significantly higher in patients with RHT compared with those without (32% vs 14%, respectively, odds ratio [OR] 3.0, 95% confidence interval [CI] 1.6 to 5.6, p [ 0.001). The rate of complications was significantly higher in patients with RHT in comparison to those without (40% vs 22%, respectively, OR 2.4, 95% CI 1.3 to 4.4, p [ 0.004). The mortality rate in patients with both AF and RHT was significantly higher in comparison to those with AF but without RHT (50% vs 20%, respectively, OR 3.86, 95% CI 1.3 to 11.2, p [ 0.01). In multivariate analysis, RHT (p [ 0.03) was an independent predictor of death. In conclu- sion, AF is a frequent co-morbidity in patients with APE, and the presence of RHT is not uncommon. Among patients with APE, the presence of RHT increases the mortality approximately threefold regardless of the presence of known AF. Ó 2015 Elsevier Inc. All rights reserved. (Am J Cardiol 2015;-:-e-) The association between ischemic stroke and systemic emboli arising from left atrial thrombus in patients with atrial fibrillation (AF) is well described. The notion of a parallel right atrial process leading to pulmonary venous thromboemboli has also been proposed. 1 This theory can be supported by the observation of spontaneous echocardio- graphic contrast in both atria in patients with right-sided cardiac abnormalities, including AF. 2,3 Where it has been shown that the presence of AF provokes a hypercoagulable state and induces platelet aggregation, 4e6 it would seem sensible to infer that the hypercoagulable state exists in both the right and left atria. Reports that predate the era of widespread anticoagulation for patients with AF indicate that thrombus can develop in the right atrium. The landmark autopsy study by Aberg in 693 consecutive patients with AF showed that 13% of patients had clots in the left atrium and 8% had clots in the right atrium and that these occurred predominantly in the appendages. 7 The risk stratification of patients with acute pulmonary embolism (APE) remains a challenge. 8e10 Exploration of the link between APE, AF, and right heart thrombus (RHT) may provide further infor- mation about the pathophysiology of these disease processes and aid in risk stratification for patients with APE. The aim of this study was to determine the prevalence of RHT and AF and to assess their impact on outcomes in patients with APE. Methods This was a retrospective analysis of consecutive patients who were diagnosed with APE and were hospitalized in the cardiology departments of 8 community hospitals in 2 countries from 2004 to 2012. All clinical data were collected at the time admission or at the first occurrence during the a Department of Internal Medicine and Cardiology, Specialistic Hospital, Gorlice, Poland; b Section of Cardiology, Department of Internal Medicine, University of Manitoba, Winnipeg, Manitoba, Canada; c Department for Cardiovascular Diseases, Clinical Center, Nis, Serbia; d Department of Statistics, Cracow University of Economics, Cracow, Poland; e Department of Cardiology, Szczeklik Specialistic Hospital, Tarnów, Poland; f Depart- ment of Cardiology, Dietl Specialistic Hospital, Cracow, Poland; g First Department of Cardiology, Interventional Electrocardiology and Hyper- tension, Jagiellonian University, Cracow, Poland; h Department of Internal Medicine and Cardiology, Medical University of Warsaw, Poland; and i Division of Cardiology, Kingston General Hospital, Queen’s University, Kingston, Ontario, Canada. Manuscript received October 29, 2014; revised manuscript received and accepted December 23, 2014. See page 5 for disclosure information. *Corresponding author: Tel: (þ48) 18 35 53 417; fax: (þ48) 18 352 60 46. E-mail address: [email protected] (P. Kukla). 0002-9149/15/$ - see front matter Ó 2015 Elsevier Inc. All rights reserved. www.ajconline.org http://dx.doi.org/10.1016/j.amjcard.2014.12.049

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

aDeparGorlice, PoUniversityCardiovascStatistics, Cof Cardiolment of CDepartmentension, JaMedicineiDivision oKingston,manuscript
See pa*Corre
60 46.E-mail
0002-9149http://dx.do
Relation of Atrial Fibrillation and Right-Sided CardiacThrombus to Outcomes in Patients With Acute
Pulmonary Embolism
Piotr Kukla, MD, PhDa,*, Wiliam F. McIntyre, MDb, Goran Koracevic, MD, PhDc,Dusanka Kutlesic-Kurtovic, MDc, Kamil Fijorek, MScd, Vesna Atanaskovic, MDc, Ewa Krupa, MDe,Ewa Mirek-Bryniarska, MD, PhDf, Marek Jastrzebski, MD, PhDg, Leszek Bryniarski, MD, PhDg,
Piotr Pruszczyk, MD, PhDh, and Adrian Baranchuk, MDi
Atrial fibrillation (AF) can induce a hypercoagulable state in both the left and right atria.
tment oland; b
of Maular Dracow
ogy, Szardiolot of Cagielloniand Caf CardiOntarioreceive
ge 5 forspondin
addres
/15/$ -i.org/1
Thrombus in the right side of the heart (RHT) may lead to acute pulmonary embolism(APE). The aim of the study was to determine the prevalence of RHT and AF and to assesstheir impact on outcomes in patients with APE. The retrospective cohort included 1,006patients (598 female), with a mean age of 66 – 15 years. The primary end point was all-cause mortality. The secondary end point was incidence of complications (death, cardio-genic shock, cardiac arrest, vasopressor/inotrope treatment, or ventilatory support). Atrialfibrillation was detected in 231 patients (24%). RHT was observed in 50 patients (5%). Thecombination of AF and RHT was observed in 16 patients (2%). The overall mortality ratewas significantly higher in patients with RHT compared with those without (32% vs 14%,respectively, odds ratio [OR] 3.0, 95% confidence interval [CI] 1.6 to 5.6, p [ 0.001). Therate of complications was significantly higher in patients with RHT in comparison to thosewithout (40% vs 22%, respectively, OR 2.4, 95% CI 1.3 to 4.4, p [ 0.004). The mortalityrate in patients with both AF and RHT was significantly higher in comparison to those withAF but without RHT (50% vs 20%, respectively, OR 3.86, 95% CI 1.3 to 11.2, p [ 0.01). Inmultivariate analysis, RHT (p [ 0.03) was an independent predictor of death. In conclu-sion, AF is a frequent co-morbidity in patients with APE, and the presence of RHT is notuncommon. Among patients with APE, the presence of RHT increases the mortalityapproximately threefold regardless of the presence of known AF. � 2015 Elsevier Inc. Allrights reserved. (Am J Cardiol 2015;-:-e-)
The association between ischemic stroke and systemicemboli arising from left atrial thrombus in patients withatrial fibrillation (AF) is well described. The notion of aparallel right atrial process leading to pulmonary venousthromboemboli has also been proposed.1 This theory can besupported by the observation of spontaneous echocardio-graphic contrast in both atria in patients with right-sidedcardiac abnormalities, including AF.2,3 Where it has been
f Internal Medicine and Cardiology, Specialistic Hospital,Section of Cardiology, Department of Internal Medicine,nitoba, Winnipeg, Manitoba, Canada; cDepartment foriseases, Clinical Center, Nis, Serbia; dDepartment ofUniversity of Economics, Cracow, Poland; eDepartmentczeklik Specialistic Hospital, Tarnów, Poland; fDepart-gy, Dietl Specialistic Hospital, Cracow, Poland; gFirstrdiology, Interventional Electrocardiology and Hyper-an University, Cracow, Poland; hDepartment of Internalrdiology, Medical University of Warsaw, Poland; andology, Kingston General Hospital, Queen’s University,, Canada. Manuscript received October 29, 2014; revisedd and accepted December 23, 2014.disclosure information.g author: Tel: (þ48) 18 35 53 417; fax: (þ48) 18 352
s: [email protected] (P. Kukla).
see front matter � 2015 Elsevier Inc. All rights reserved.0.1016/j.amjcard.2014.12.049
shown that the presence of AF provokes a hypercoagulablestate and induces platelet aggregation,4e6 it would seemsensible to infer that the hypercoagulable state exists in boththe right and left atria. Reports that predate the era ofwidespread anticoagulation for patients with AF indicatethat thrombus can develop in the right atrium. The landmarkautopsy study by Aberg in 693 consecutive patients with AFshowed that 13% of patients had clots in the left atrium and8% had clots in the right atrium and that these occurredpredominantly in the appendages.7 The risk stratification ofpatients with acute pulmonary embolism (APE) remains achallenge.8e10 Exploration of the link between APE, AF,and right heart thrombus (RHT) may provide further infor-mation about the pathophysiology of these disease processesand aid in risk stratification for patients with APE. The aimof this study was to determine the prevalence of RHT andAF and to assess their impact on outcomes in patientswith APE.
Methods
This was a retrospective analysis of consecutive patientswho were diagnosed with APE and were hospitalized in thecardiology departments of 8 community hospitals in 2countries from 2004 to 2012. All clinical data were collectedat the time admission or at the first occurrence during the
www.ajconline.org
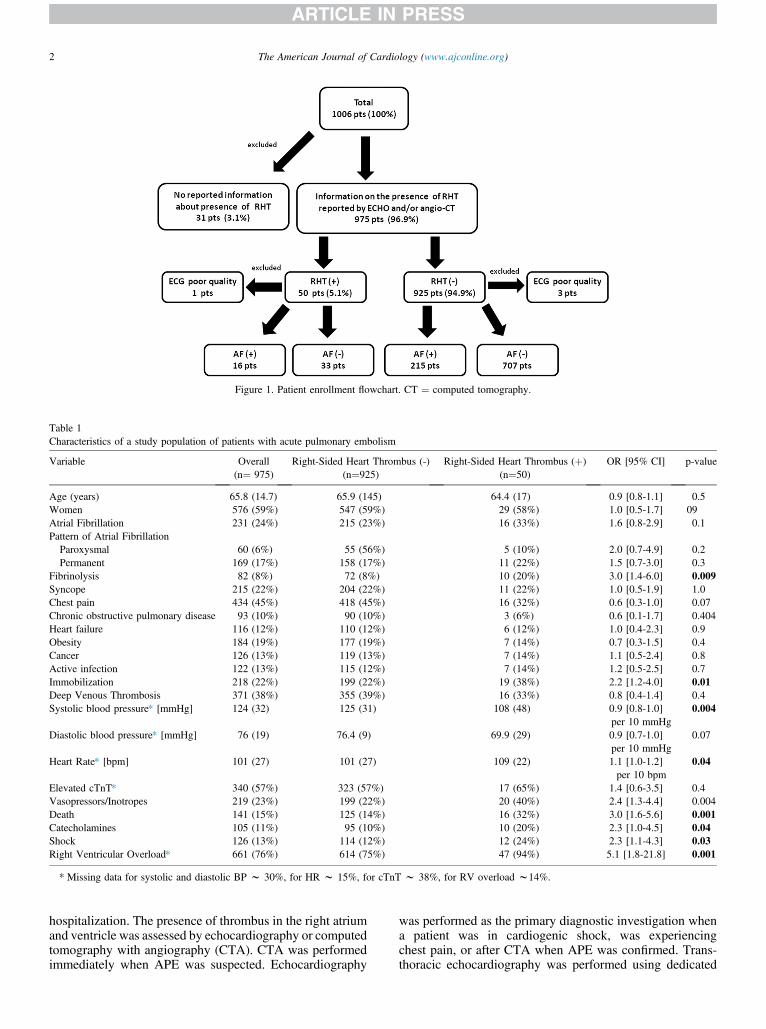
Figure 1. Patient enrollment flowchart. CT ¼ computed tomography.
Table 1Characteristics of a study population of patients with acute pulmonary embolism
Variable Overall(n¼ 975)
Right-Sided Heart Thrombus (-)(n¼925)
Right-Sided Heart Thrombus (þ)(n¼50)
OR [95% CI] p-value
Age (years) 65.8 (14.7) 65.9 (145) 64.4 (17) 0.9 [0.8-1.1] 0.5Women 576 (59%) 547 (59%) 29 (58%) 1.0 [0.5-1.7] 09Atrial Fibrillation 231 (24%) 215 (23%) 16 (33%) 1.6 [0.8-2.9] 0.1Pattern of Atrial FibrillationParoxysmal 60 (6%) 55 (56%) 5 (10%) 2.0 [0.7-4.9] 0.2Permanent 169 (17%) 158 (17%) 11 (22%) 1.5 [0.7-3.0] 0.3
Fibrinolysis 82 (8%) 72 (8%) 10 (20%) 3.0 [1.4-6.0] 0.009Syncope 215 (22%) 204 (22%) 11 (22%) 1.0 [0.5-1.9] 1.0Chest pain 434 (45%) 418 (45%) 16 (32%) 0.6 [0.3-1.0] 0.07Chronic obstructive pulmonary disease 93 (10%) 90 (10%) 3 (6%) 0.6 [0.1-1.7] 0.404Heart failure 116 (12%) 110 (12%) 6 (12%) 1.0 [0.4-2.3] 0.9Obesity 184 (19%) 177 (19%) 7 (14%) 0.7 [0.3-1.5] 0.4Cancer 126 (13%) 119 (13%) 7 (14%) 1.1 [0.5-2.4] 0.8Active infection 122 (13%) 115 (12%) 7 (14%) 1.2 [0.5-2.5] 0.7Immobilization 218 (22%) 199 (22%) 19 (38%) 2.2 [1.2-4.0] 0.01Deep Venous Thrombosis 371 (38%) 355 (39%) 16 (33%) 0.8 [0.4-1.4] 0.4Systolic blood pressure* [mmHg] 124 (32) 125 (31) 108 (48) 0.9 [0.8-1.0]
per 10 mmHg0.004
Diastolic blood pressure* [mmHg] 76 (19) 76.4 (9) 69.9 (29) 0.9 [0.7-1.0]per 10 mmHg
0.07
Heart Rate* [bpm] 101 (27) 101 (27) 109 (22) 1.1 [1.0-1.2]per 10 bpm
0.04
Elevated cTnT* 340 (57%) 323 (57%) 17 (65%) 1.4 [0.6-3.5] 0.4Vasopressors/Inotropes 219 (23%) 199 (22%) 20 (40%) 2.4 [1.3-4.4] 0.004Death 141 (15%) 125 (14%) 16 (32%) 3.0 [1.6-5.6] 0.001Catecholamines 105 (11%) 95 (10%) 10 (20%) 2.3 [1.0-4.5] 0.04Shock 126 (13%) 114 (12%) 12 (24%) 2.3 [1.1-4.3] 0.03Right Ventricular Overload* 661 (76%) 614 (75%) 47 (94%) 5.1 [1.8-21.8] 0.001
* Missing data for systolic and diastolic BP w 30%, for HR w 15%, for cTnT w 38%, for RV overload w14%.
2 The American Journal of Cardiology (www.ajconline.org)
hospitalization. The presence of thrombus in the right atriumand ventricle was assessed by echocardiography or computedtomography with angiography (CTA). CTA was performedimmediately when APE was suspected. Echocardiography
was performed as the primary diagnostic investigation whena patient was in cardiogenic shock, was experiencingchest pain, or after CTA when APE was confirmed. Trans-thoracic echocardiography was performed using dedicated
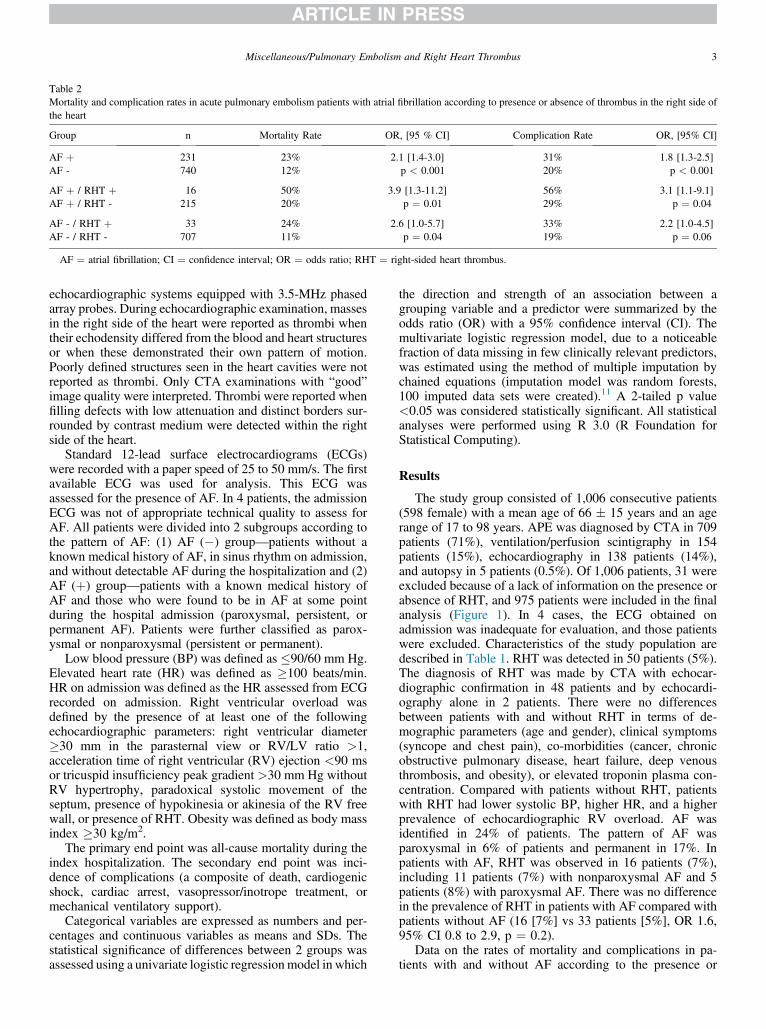
Table 2Mortality and complication rates in acute pulmonary embolism patients with atrial fibrillation according to presence or absence of thrombus in the right side ofthe heart
Group n Mortality Rate OR, [95 % CI] Complication Rate OR, [95% CI]
AF þ 231 23% 2.1 [1.4-3.0]p < 0.001
31% 1.8 [1.3-2.5]p < 0.001AF - 740 12% 20%
AF þ / RHT þ 16 50% 3.9 [1.3-11.2]p ¼ 0.01
56% 3.1 [1.1-9.1]p ¼ 0.04AF þ / RHT - 215 20% 29%
AF - / RHT þ 33 24% 2.6 [1.0-5.7]p ¼ 0.04
33% 2.2 [1.0-4.5]p ¼ 0.06AF - / RHT - 707 11% 19%
AF ¼ atrial fibrillation; CI ¼ confidence interval; OR ¼ odds ratio; RHT ¼ right-sided heart thrombus.
Miscellaneous/Pulmonary Embolism and Right Heart Thrombus 3
echocardiographic systems equipped with 3.5-MHz phasedarray probes. During echocardiographic examination, massesin the right side of the heart were reported as thrombi whentheir echodensity differed from the blood and heart structuresor when these demonstrated their own pattern of motion.Poorly defined structures seen in the heart cavities were notreported as thrombi. Only CTA examinations with “good”image quality were interpreted. Thrombi were reported whenfilling defects with low attenuation and distinct borders sur-rounded by contrast medium were detected within the rightside of the heart.
Standard 12-lead surface electrocardiograms (ECGs)were recorded with a paper speed of 25 to 50 mm/s. The firstavailable ECG was used for analysis. This ECG wasassessed for the presence of AF. In 4 patients, the admissionECG was not of appropriate technical quality to assess forAF. All patients were divided into 2 subgroups according tothe pattern of AF: (1) AF (�) group—patients without aknown medical history of AF, in sinus rhythm on admission,and without detectable AF during the hospitalization and (2)AF (þ) group—patients with a known medical history ofAF and those who were found to be in AF at some pointduring the hospital admission (paroxysmal, persistent, orpermanent AF). Patients were further classified as parox-ysmal or nonparoxysmal (persistent or permanent).
Low blood pressure (BP) was defined as �90/60 mm Hg.Elevated heart rate (HR) was defined as �100 beats/min.HR on admission was defined as the HR assessed from ECGrecorded on admission. Right ventricular overload wasdefined by the presence of at least one of the followingechocardiographic parameters: right ventricular diameter�30 mm in the parasternal view or RV/LV ratio >1,acceleration time of right ventricular (RV) ejection <90 msor tricuspid insufficiency peak gradient >30 mm Hg withoutRV hypertrophy, paradoxical systolic movement of theseptum, presence of hypokinesia or akinesia of the RV freewall, or presence of RHT. Obesity was defined as body massindex �30 kg/m2.
The primary end point was all-cause mortality during theindex hospitalization. The secondary end point was inci-dence of complications (a composite of death, cardiogenicshock, cardiac arrest, vasopressor/inotrope treatment, ormechanical ventilatory support).
Categorical variables are expressed as numbers and per-centages and continuous variables as means and SDs. Thestatistical significance of differences between 2 groups wasassessed using a univariate logistic regressionmodel in which
the direction and strength of an association between agrouping variable and a predictor were summarized by theodds ratio (OR) with a 95% confidence interval (CI). Themultivariate logistic regression model, due to a noticeablefraction of data missing in few clinically relevant predictors,was estimated using the method of multiple imputation bychained equations (imputation model was random forests,100 imputed data sets were created).11 A 2-tailed p value<0.05 was considered statistically significant. All statisticalanalyses were performed using R 3.0 (R Foundation forStatistical Computing).
Results
The study group consisted of 1,006 consecutive patients(598 female) with a mean age of 66 � 15 years and an agerange of 17 to 98 years. APE was diagnosed by CTA in 709patients (71%), ventilation/perfusion scintigraphy in 154patients (15%), echocardiography in 138 patients (14%),and autopsy in 5 patients (0.5%). Of 1,006 patients, 31 wereexcluded because of a lack of information on the presence orabsence of RHT, and 975 patients were included in the finalanalysis (Figure 1). In 4 cases, the ECG obtained onadmission was inadequate for evaluation, and those patientswere excluded. Characteristics of the study population aredescribed in Table 1. RHT was detected in 50 patients (5%).The diagnosis of RHT was made by CTA with echocar-diographic confirmation in 48 patients and by echocardi-ography alone in 2 patients. There were no differencesbetween patients with and without RHT in terms of de-mographic parameters (age and gender), clinical symptoms(syncope and chest pain), co-morbidities (cancer, chronicobstructive pulmonary disease, heart failure, deep venousthrombosis, and obesity), or elevated troponin plasma con-centration. Compared with patients without RHT, patientswith RHT had lower systolic BP, higher HR, and a higherprevalence of echocardiographic RV overload. AF wasidentified in 24% of patients. The pattern of AF wasparoxysmal in 6% of patients and permanent in 17%. Inpatients with AF, RHT was observed in 16 patients (7%),including 11 patients (7%) with nonparoxysmal AF and 5patients (8%) with paroxysmal AF. There was no differencein the prevalence of RHT in patients with AF compared withpatients without AF (16 [7%] vs 33 patients [5%], OR 1.6,95% CI 0.8 to 2.9, p ¼ 0.2).
Data on the rates of mortality and complications in pa-tients with and without AF according to the presence or
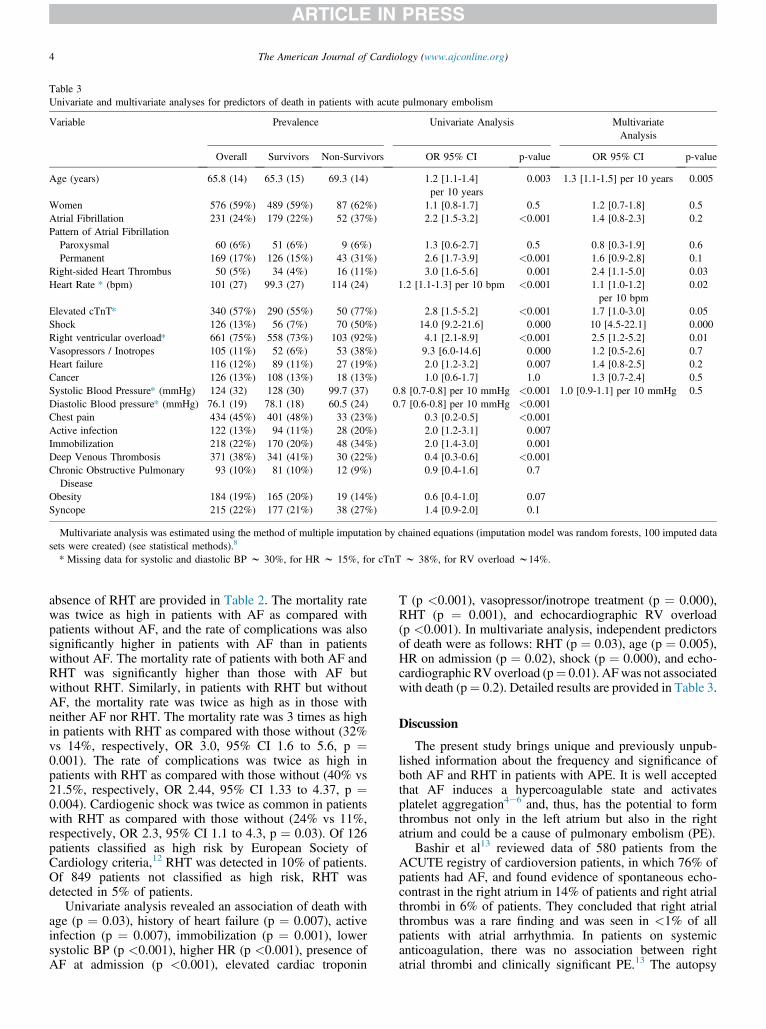
Table 3Univariate and multivariate analyses for predictors of death in patients with acute pulmonary embolism
Variable Prevalence Univariate Analysis MultivariateAnalysis
Overall Survivors Non-Survivors OR 95% CI p-value OR 95% CI p-value
Age (years) 65.8 (14) 65.3 (15) 69.3 (14) 1.2 [1.1-1.4]per 10 years
0.003 1.3 [1.1-1.5] per 10 years 0.005
Women 576 (59%) 489 (59%) 87 (62%) 1.1 [0.8-1.7] 0.5 1.2 [0.7-1.8] 0.5Atrial Fibrillation 231 (24%) 179 (22%) 52 (37%) 2.2 [1.5-3.2] <0.001 1.4 [0.8-2.3] 0.2Pattern of Atrial FibrillationParoxysmal 60 (6%) 51 (6%) 9 (6%) 1.3 [0.6-2.7] 0.5 0.8 [0.3-1.9] 0.6Permanent 169 (17%) 126 (15%) 43 (31%) 2.6 [1.7-3.9] <0.001 1.6 [0.9-2.8] 0.1
Right-sided Heart Thrombus 50 (5%) 34 (4%) 16 (11%) 3.0 [1.6-5.6] 0.001 2.4 [1.1-5.0] 0.03Heart Rate * (bpm) 101 (27) 99.3 (27) 114 (24) 1.2 [1.1-1.3] per 10 bpm <0.001 1.1 [1.0-1.2]
per 10 bpm0.02
Elevated cTnT* 340 (57%) 290 (55%) 50 (77%) 2.8 [1.5-5.2] <0.001 1.7 [1.0-3.0] 0.05Shock 126 (13%) 56 (7%) 70 (50%) 14.0 [9.2-21.6] 0.000 10 [4.5-22.1] 0.000Right ventricular overload* 661 (75%) 558 (73%) 103 (92%) 4.1 [2.1-8.9] <0.001 2.5 [1.2-5.2] 0.01Vasopressors / Inotropes 105 (11%) 52 (6%) 53 (38%) 9.3 [6.0-14.6] 0.000 1.2 [0.5-2.6] 0.7Heart failure 116 (12%) 89 (11%) 27 (19%) 2.0 [1.2-3.2] 0.007 1.4 [0.8-2.5] 0.2Cancer 126 (13%) 108 (13%) 18 (13%) 1.0 [0.6-1.7] 1.0 1.3 [0.7-2.4] 0.5Systolic Blood Pressure* (mmHg) 124 (32) 128 (30) 99.7 (37) 0.8 [0.7-0.8] per 10 mmHg <0.001 1.0 [0.9-1.1] per 10 mmHg 0.5Diastolic Blood pressure* (mmHg) 76.1 (19) 78.1 (18) 60.5 (24) 0.7 [0.6-0.8] per 10 mmHg <0.001Chest pain 434 (45%) 401 (48%) 33 (23%) 0.3 [0.2-0.5] <0.001Active infection 122 (13%) 94 (11%) 28 (20%) 2.0 [1.2-3.1] 0.007Immobilization 218 (22%) 170 (20%) 48 (34%) 2.0 [1.4-3.0] 0.001Deep Venous Thrombosis 371 (38%) 341 (41%) 30 (22%) 0.4 [0.3-0.6] <0.001Chronic Obstructive Pulmonary
Disease93 (10%) 81 (10%) 12 (9%) 0.9 [0.4-1.6] 0.7
Obesity 184 (19%) 165 (20%) 19 (14%) 0.6 [0.4-1.0] 0.07Syncope 215 (22%) 177 (21%) 38 (27%) 1.4 [0.9-2.0] 0.1
Multivariate analysis was estimated using the method of multiple imputation by chained equations (imputation model was random forests, 100 imputed datasets were created) (see statistical methods).8
* Missing data for systolic and diastolic BP w 30%, for HR w 15%, for cTnT w 38%, for RV overload w14%.
4 The American Journal of Cardiology (www.ajconline.org)
absence of RHT are provided in Table 2. The mortality ratewas twice as high in patients with AF as compared withpatients without AF, and the rate of complications was alsosignificantly higher in patients with AF than in patientswithout AF. The mortality rate of patients with both AF andRHT was significantly higher than those with AF butwithout RHT. Similarly, in patients with RHT but withoutAF, the mortality rate was twice as high as in those withneither AF nor RHT. The mortality rate was 3 times as highin patients with RHT as compared with those without (32%vs 14%, respectively, OR 3.0, 95% CI 1.6 to 5.6, p ¼0.001). The rate of complications was twice as high inpatients with RHT as compared with those without (40% vs21.5%, respectively, OR 2.44, 95% CI 1.33 to 4.37, p ¼0.004). Cardiogenic shock was twice as common in patientswith RHT as compared with those without (24% vs 11%,respectively, OR 2.3, 95% CI 1.1 to 4.3, p ¼ 0.03). Of 126patients classified as high risk by European Society ofCardiology criteria,12 RHT was detected in 10% of patients.Of 849 patients not classified as high risk, RHT wasdetected in 5% of patients.
Univariate analysis revealed an association of death withage (p ¼ 0.03), history of heart failure (p ¼ 0.007), activeinfection (p ¼ 0.007), immobilization (p ¼ 0.001), lowersystolic BP (p <0.001), higher HR (p <0.001), presence ofAF at admission (p <0.001), elevated cardiac troponin
T (p <0.001), vasopressor/inotrope treatment (p ¼ 0.000),RHT (p ¼ 0.001), and echocardiographic RV overload(p <0.001). In multivariate analysis, independent predictorsof death were as follows: RHT (p ¼ 0.03), age (p ¼ 0.005),HR on admission (p ¼ 0.02), shock (p ¼ 0.000), and echo-cardiographic RV overload (p¼ 0.01). AFwas not associatedwith death (p¼ 0.2). Detailed results are provided in Table 3.
Discussion
The present study brings unique and previously unpub-lished information about the frequency and significance ofboth AF and RHT in patients with APE. It is well acceptedthat AF induces a hypercoagulable state and activatesplatelet aggregation4e6 and, thus, has the potential to formthrombus not only in the left atrium but also in the rightatrium and could be a cause of pulmonary embolism (PE).
Bashir et al13 reviewed data of 580 patients from theACUTE registry of cardioversion patients, in which 76% ofpatients had AF, and found evidence of spontaneous echo-contrast in the right atrium in 14% of patients and right atrialthrombi in 6% of patients. They concluded that right atrialthrombus was a rare finding and was seen in <1% of allpatients with atrial arrhythmia. In patients on systemicanticoagulation, there was no association between rightatrial thrombi and clinically significant PE.13 The autopsy

Miscellaneous/Pulmonary Embolism and Right Heart Thrombus 5
study by Aberg7 in 693 consecutive patients with AFshowed that 13% had thrombus in the left atrium and 8%had thrombus in the right atrium. The same study showedthat the prevalence of APE was similar in patients with andwithout evidence of thrombosis been in the deep venoussystem (8% vs 8%).7 This suggests an origin of pulmonaryartery thrombus other than the systemic veins. Gex et al14
showed that the presence of AF does not increase theprobability of PE among all-comers when this diagnosis issuspected. Nevertheless, when the suspicion of APE isbased on new-onset dyspnea, the presence of AF signifi-cantly decreases the probability of PE (OR 0.5) as AF maymimic its clinical presentation. In contrast, in patients pre-senting with chest pain alone, the presence of AF tends toincrease the probability of PE (OR 2.4).14 In the Interna-tional Cooperative Pulmonary Embolism Registry(ICOPER) study, the prevalence of AF was identical inpatients with and without RHT (12%).15 To the best of ourknowledge, our study is the first to publish data on thereverse phenomenon (i.e., prevalence of RHT in patientswith and without AF).
In the present study, there was a trend toward a higherprevalence of AF in patients with RHT in comparison tothose without RHT (32% vs 23%, p ¼ NS); this held true forboth patients with paroxysmal (10% vs 6%, p ¼ NS) andnonparoxysmal AF (22% vs 17%, p ¼ NS). Our studyobserved no difference between the presence of RHT inpatients with AF and patients without AF (7% vs 5%, p ¼NS). When the pattern of AF was taken into consideration,RHT was detected in 7% of patients with nonparoxysmalAF and 8% of patients with paroxysmal AF. The mortalityrate was 3 times higher in patients with both AF and RHTthan in those with AF but without RHT (50% vs 21%,respectively, OR 3.86, 95% CI 1.3 to 11.2, p ¼ 0.01). Inturn, in patients with RHT but without AF, the mortality ratewas twice as high as in those without AF or RHT (24% vs11%, respectively, OR 2.3, 95% CI 1.1 to 4.3, p ¼ 0.03).Our study found that the presence of thrombus in the rightheart was an independent predictor of death and conferred adoubling in the risk of both in-hospital mortality and com-plications in patients with APE. This raises further questionsabout a possible association between AF, the formation ofthrombus in the right atrium, and subsequent pulmonarythromboembolism. The present multicenter retrospectiveregistry includes data on a large cohort of consecutive pa-tients with confirmed APE and reported on 975 patients,showing that RHT was observed in 5% patients. Before thepresent study, a few published data came from smaller co-horts of up to 200 patients and reported prevalence of RHTranging from 7% to 18 %.16e18 Somewhat different datacome from the large, multicenter, prospective ICOPERstudy, showing that RHT was present in 4% of patients.15
Similarly, Mansencal et al demonstrated free-floating RHTin 4% of patients among 340 consecutive patients with APE,including 22% of high-risk patients. Their study exhibitedvery high sensitivity and specificity for computed tomog-raphy to detect RHT thrombi—100% and 97%, respec-tively.19 More recently, the Italian Pulmonary EmbolismRegistry presented data on 1,716 patients, noting that RHTwas detected in 5% of patients and 16% of high-risk pa-tients.20 The presence of RHT significantly increased the
risk of dying (OR 3.9, 95% CI 2.0 to 7.7, p ¼ 0.0001) inunivariate analysis, but this result was not maintained in themultivariate model (OR 1.6, 95% CI 0.8 to 3.6, p ¼ 0.2).The investigators concluded that patients with RHT had amore severe presentation of PE but failed to confirm anassociation between RHT and prognosis.20
Among patients with RHT in the present study, weobserved lower systemic BP, higher HR, and frequent RVoverload. These results are in concordance with results fromthe ICOPER study.15 In our study, in-hospital mortalityamong patients with RHT was 32%. The ICOPER studyreported 14-day mortality at 21%,15 the study by Chapoutotet al18 at 29%, and the study by Chartier et al17 at 44%.
Our study was a retrospective observational study, andthus, there are predictors (systolic and diastolic BP, HR,cardiac troponin T plasma concentration, and RV overload)with a sizable fraction of missing data. To control for this,the multivariate logistic regression model was estimatedusing the method of multiple imputation by chained equa-tions with an imputation model of random forests for which100 imputed data sets were created. The present data setmay not include some patients who died before diagnosis ofAPE. It is also quite likely that we have underestimated thenumber of patients in the study who had paroxysmal AF.Our study was also not designed to analyze differencesbetween the treatment strategies (e.g., heparins, thrombol-ysis, embolectomy). It is also important to acknowledge thatin our study, the diagnosis of intracardiac thrombi wasdetermined retrospectively from available transthoracicechocardiography and CTA studies performed as percontemporary guidelines for the assessment of APE and thatthese techniques may miss some intracardiac thrombi thatmight have been detected by a more sensitive proceduresuch as transesophageal echocardiography. Thus, the trueprevalence of RHT may have been underestimated in thiscohort. The nature of thromboemboli makes it challengingto establish causation. Any given finding of RHT couldrepresent a consequence of AF, systemic venous clot intransit, or another unrelated entity. Similarly, our ability topredict the likelihood that a given thrombus may embolize isnot good. Any links between these 3 entities are a matter ofinference.
Disclosures
The authors have no conflicts of interest to disclose.
1. Flegel KM. When atrial fibrillation occurs with pulmonary embolism,is it the chicken or the eggs ? CMAJ 1999;160:1181e1182.
2. Black IW, Hopkins AP, Lee LCL, Walsh WF. Left atrial spontaneouscontrast echo: a clinical and echocardiographic analysis. J Am CollCardiol 1991;18:398e404.
3. DeGeorgia MA, Chimowitz MI, Hepner A, Armstrong WF. Right atrialspontaneous contrast: echocardiographic and clinical features. Int JCard Imaging 1994;10:227e232.
4. Lip GYH. Does atrial fibrillation confer a hypercoagulable state?Lancet 1995;346:1313e1314.
5. Kahn SR, Solymoss S, Flegel KM. Nonvalvular atrial fibrillation:evidence for a prothrombotic state. CMAJ 1997;157:673e681.
6. Sohara H, Amitani S, Kurose M, Miyahara K. Atrial fibrillation acti-vates platelets and coagulation in a time-dependent manner: a study inpatients with paroxysmal atrial fibrillation. J Am Coll Cardiol 1997;29:106e112.
6 The American Journal of Cardiology (www.ajconline.org)
7. Aberg H. Atrial fibrillation. I: a study of atrial thrombosis andsystemic embolism in a necropsy material. Acta Med Scand1969;185:373e379.
8. Kukla P, McIntyre WF, Fijorek K, Długopolski R, Mirek-Bryniarska E,Bryniarski KL, Jastrzebski M, Bryniarski L, Baranchuk A. T-waveinversion in patients with acute pulmonary embolism: prognostic value.Heart Lung 2015;44:68e71.
9. Kukla P, McIntyre WF, Fijorek K, Mirek-Bryniarska E, Bryniarski L,Krupa E, Jastrzebski M, Bryniarski KL, Zhong-qun Z, Baranchuk A.Electrocardiographic abnormalities in patients with acute pulmonaryembolism complicated by cardiogenic shock. Am J Emerg Med2014;32:507e510.
10. Kukla P, McIntyre WF, Fijorek K, Krupa E, Mirek-Bryniarska E,Jastrzebski M, Bryniarski KL, Zajchowski W, Bryniarski L, BaranchukA. Ischemic electrocardiographic patterns as prognosticators inintermediate-risk patients with acute pulmonary embolism. Am JEmerg Med 2014;32:1248e1252.
11. van Buuren S, Groothuis-Oudshoorn K. MICE: multivariate imputationby chained equations in R. J Stat Softw 2011;45:1e67.
12. Authors/Task Force MembersKonstantinides SV, Torbicki A, AgnelliG, Danchin N, Fitzmaurice D, Galiè N, Gibbs JS, Huisman MV,Humbert M, Kucher N, Lang I, Lankeit M, Lekakis J, Maack C, MayerE, Meneveau N, Perrier A, Pruszczyk P, Rasmussen LH, Schindler TH,Svitil P, Vonk Noordegraaf A, Zamorano JL, Zompatori M. Authors/Task Force Members. 2014 ESC Guidelines on the diagnosis andmanagement of acute pulmonary embolism: the Task Force for theDiagnosis and Management of Acute Pulmonary Embolism of theEuropean Society of Cardiology (ESC) Endorsed by the EuropeanRespiratory Society (ERS). Eur Heart J 2014; pii: ehu283.
13. Bashir M, Asher CR, Garcia MJ, Abdalla I, Jasper SE, Murray RD,Grimm RA, Thomas JD, Klein AL. Right atrial spontaneous echo
contrast and thrombi in atrial fibrillation: a transesophageal echocar-diography study. J Am Soc Echocardiogr 2001;14:122e127.
14. Gex G, Gerstel E, Righini M, LE Gal G, Aujesky D, Roy PM, SanchezO, Verschuren F, Rutschmann OT, Perneger T, Perrier A. Is atrialfibrillation associated with pulmonary embolism? J Thromb Haemost2012;10:347e351.
15. Torbicki A, Galie N, Covezzoli A, Rossi E, De Rosa M, Goldhaber SZ.Right heart thrombi in pulmonary embolism: results from the Inter-national Cooperative Pulmonary Embolism Registry. J Am Coll Car-diol 2003;41:2245e2251.
16. Casazza F, Bongarzoni A, Centonze F, Morpurgo M. Prevalence andprognostic significance of right-sided cardiac mobile thrombi in acutemassive pulmonary embolism. Am J Cardiol 1997;79:1433e1435.
17. Chartier L, Bera J, Delomez M, Asseman P, Beregi JP, Bauchart JJ,Warembourg H, Thery C. Free-floating thrombi in the right heart:diagnosis, management, and prognostic indexes in 38 consecutivepatients. Circulation 1999;99:2779e2783.
18. Chapoutot L, Nazeyrollas P, Metz D, Maes D, Maillier B, JennesseauxC, Elaerts J. Floating right heart thrombi and pulmonary embolism:diagnosis, outcome and therapeutic management. Cardiology 1996;87:169e174.
19. Mansencal N, Attias D, Caille V, Desperramons J, Guiader J, ElHajjam M, Lacombe P, Abi Nasr I, Jardin F, Vieillard-Baron A,Dubourg O. Computed tomography for the detection of free-floatingthrombi in the right heart in acute pulmonary embolism. Eur Radiol2011;21:240e245.
20. Casazza F, Becattini C, Guglielmelli E, Floriani I, Morrone V, CaponiC, Pizzorno N, Masotti L, Bongarzoni A, Pignataro L. Prognosticsignificance of free-floating right heart thromboemboli in acute pul-monary embolism: results from the Italian Pulmonary EmbolismRegistry. Thromb Haemost 2014;111:53e57.
Related Documents











