Regenerative Endodontic Procedures for Traumatized Teeth after Horizontal Root Fracture, Avulsion, and Perforating Root Resorption Tarek Mohamed A. Saoud, BDS, MSc, PhD,* Sonali Mistry, MDSc, † Bill Kahler, DClinDent, PhD, † Asgeir Sigurdsson, DDS, MS, ‡ and Louis M. Lin, BDS, DMD, PhD ‡ Abstract Introduction: Traumatic injury to the teeth can cause horizontal root fractures and inflammatory root resorp- tions (external and internal). Traditionally, traumatized teeth with horizontal root fractures resulting in pulp necrosis and inflammatory root resorptions are treated with conventional root canal therapy. Methods: A 15-year-old boy had a history of traumatic injury to mature tooth #8 resulting in horizontal root fracture and pulp necrosis of the coronal fragment. A 7-year- old girl suffered an avulsion injury to immature tooth #9, which developed inflammatory replacement resorp- tion and subsequently root fractured 15 months later. Another 16-year-old boy also suffered a history of trau- matic injury to mature tooth #8, resulting in perforating root resorption. All teeth were treated with regenerative endodontic procedures using chemomechanical deb- ridement, calcium hydroxide/triple antibiotic paste dres- sing, EDTA rinse, induction of periapical bleeding into the canal space, and a coronal mineral trioxide aggre- gate plug. In the tooth presenting with horizontal root fracture, only the coronal fragment was treated to pre- serve pulp vitality in the apical fragment for possible pulp tissue regeneration. Results: After regenerative endodontic procedures, clinical signs/symptoms sub- sided, and inflammatory osteolytic lesions resolved in all traumatized teeth. Two teeth were followed for 19 months and 1 tooth for 5 years. At the last review of the teeth with horizontal root fractures, the first case showed healing by calcified tissue and the second case showed healing by fibrous connective and hard tis- sue. Tooth with perforating root resorption demon- strated a decrease in size of the resorptive defect. Conclusions: Based on these case reports, regenerative endodontic procedures have the potential to be used to treat traumatized teeth with horizontal root fracture and inflammatory root resorption. (J Endod 2016;-:1–7) Key Words Avulsion, dental trauma, horizontal root fracture, regenerative endodontic procedures, root resorption T raumatic injury to the teeth can cause a vari- ety of damage to the teeth and supporting structures including root fractures and root and bone resorp- tions (1, 2). Horizontal root fracture is caused by direct physical impact to the tooth. External inflammatory root resorption is caused by damage to the root surface in association with the presence of an infected, necrotic pulp in the canal space (3, 4). In order for external inflammatory root resorption to take place, the protective layer of precementum must be damaged, likely because of trauma or inflammation of the periodontal ligament, thus leading to exposure of the underlying dentin (3, 4). In addition, the canal space has to contain infected, necrotic pulp tissue. The toxic products from bacteria and tissue breakdown in the canal space diffuse through the dentinal tubules communicating with the root surface denuded of cementum to initiate inflammatory processes (3–5). Internal inflammatory root resorption occurs in teeth containing infected, necrotic pulps. It is assumed that the odontoblasts and unmineralized predentin lining the canal space must be damaged and the mineralized component of dentin exposed in order for internal inflammatory root resorption to take place (3–5). However, the predisposing factors to the damage of predentin are not clear. Trauma, caries, periodontal infection, calcium hydroxide, vital root resection, orthodontic treatment, and tooth crack have been proposed (5). The cellular and molecular mechanisms of internal/external root resorption are not as clear as that of bone resorption. In bone, there is a cross talk between osteocytes, osteoblasts, and osteoclasts to orchestrate the complex biological processes of resorption and repair (6–8). The primary cause of external/internal inflammatory root resorption and no healing of horizontal root fractures is the presence of infected, From the *Department of Restorative Dentistry and Endodontics, Faculty of Dentistry, University of Benghazi, Benghazi, Libya; † School of Dentistry, University of Queensland, Brisbane, Australia; and ‡ Department of Endodontics, College of Dentistry, New York University, New York, New York. Address requests for reprints to Dr Louis M. Lin, Department of Endodontics, College of Dentistry, New York University, 345 East 24th Street, New York, NY 10010. E-mail address: [email protected] 0099-2399/$ - see front matter Copyright ª 2016 American Association of Endodontists. http://dx.doi.org/10.1016/j.joen.2016.04.028 Significance Traumatized teeth that became necrotic and in- fected with horizontal root fracture, avulsion, and root resorptions are traditionally treated with root canal filling. However, regenerative endodontic therapy also has a potential to be used in the man- agement of traumatized devitalized teeth with aforementioned conditions, as demonstrated by the cases presented. Clinical Research JOE — Volume -, Number -, - 2016 Regenerative Endodontic Procedures 1

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Clinical Research
Regenerative Endodontic Proceduresfor Traumatized Teeth after HorizontalRoot Fracture, Avulsion, and PerforatingRoot Resorption
Tarek Mohamed A. Saoud, BDS, MSc, PhD,* Sonali Mistry, MDSc,†
Bill Kahler, DClinDent, PhD,† Asgeir Sigurdsson, DDS, MS,‡ and Louis M. Lin, BDS, DMD, PhD‡
Abstract
SignificanceTraumatized teeth that became necrotic and in-fected with horizontal root fracture, avulsion, androot resorptions are traditionally treated with rootcanal filling. However, regenerative endodontictherapy also has a potential to be used in the man-agement of traumatized devitalized teeth withaforementioned conditions, as demonstrated bythe cases presented.
Introduction: Traumatic injury to the teeth can causehorizontal root fractures and inflammatory root resorp-tions (external and internal). Traditionally, traumatizedteeth with horizontal root fractures resulting in pulpnecrosis and inflammatory root resorptions are treatedwith conventional root canal therapy. Methods: A15-year-old boy had a history of traumatic injury tomature tooth #8 resulting in horizontal root fractureand pulp necrosis of the coronal fragment. A 7-year-old girl suffered an avulsion injury to immature tooth#9, which developed inflammatory replacement resorp-tion and subsequently root fractured 15 months later.Another 16-year-old boy also suffered a history of trau-matic injury to mature tooth #8, resulting in perforatingroot resorption. All teeth were treated with regenerativeendodontic procedures using chemomechanical deb-ridement, calcium hydroxide/triple antibiotic paste dres-sing, EDTA rinse, induction of periapical bleeding intothe canal space, and a coronal mineral trioxide aggre-gate plug. In the tooth presenting with horizontal rootfracture, only the coronal fragment was treated to pre-serve pulp vitality in the apical fragment for possiblepulp tissue regeneration. Results: After regenerativeendodontic procedures, clinical signs/symptoms sub-sided, and inflammatory osteolytic lesions resolved inall traumatized teeth. Two teeth were followed for19 months and 1 tooth for 5 years. At the last reviewof the teeth with horizontal root fractures, the firstcase showed healing by calcified tissue and the secondcase showed healing by fibrous connective and hard tis-sue. Tooth with perforating root resorption demon-strated a decrease in size of the resorptive defect.Conclusions: Based on these case reports, regenerativeendodontic procedures have the potential to be used totreat traumatized teeth with horizontal root fracture andinflammatory root resorption. (J Endod 2016;-:1–7)
From the *Department of Restorative Dentistry and EndodonticQueensland, Brisbane, Australia; and ‡Department of Endodontics,
Address requests for reprints to Dr Louis M. Lin, Department of EE-mail address: [email protected]/$ - see front matter
Copyright ª 2016 American Association of Endodontists.http://dx.doi.org/10.1016/j.joen.2016.04.028
JOE — Volume -, Number -, - 2016
Key WordsAvulsion, dental trauma, horizontal root fracture, regenerative endodontic procedures,root resorption
Traumatic injury to theteeth can cause a vari-
ety of damage to the teethand supporting structuresincluding root fracturesand root and bone resorp-tions (1, 2). Horizontalroot fracture is caused bydirect physical impact tothe tooth. Externalinflammatory root
resorption is caused by damage to the root surface in association with the presenceof an infected, necrotic pulp in the canal space (3, 4). In order for externalinflammatory root resorption to take place, the protective layer of precementummust be damaged, likely because of trauma or inflammation of the periodontalligament, thus leading to exposure of the underlying dentin (3, 4). In addition, thecanal space has to contain infected, necrotic pulp tissue. The toxic products frombacteria and tissue breakdown in the canal space diffuse through the dentinaltubules communicating with the root surface denuded of cementum to initiateinflammatory processes (3–5). Internal inflammatory root resorption occurs inteeth containing infected, necrotic pulps. It is assumed that the odontoblasts andunmineralized predentin lining the canal space must be damaged and themineralized component of dentin exposed in order for internal inflammatory rootresorption to take place (3–5). However, the predisposing factors to the damage ofpredentin are not clear. Trauma, caries, periodontal infection, calcium hydroxide,vital root resection, orthodontic treatment, and tooth crack have been proposed(5). The cellular and molecular mechanisms of internal/external root resorption arenot as clear as that of bone resorption. In bone, there is a cross talk betweenosteocytes, osteoblasts, and osteoclasts to orchestrate the complex biological processesof resorption and repair (6–8). The primary cause of external/internal inflammatoryroot resorption and no healing of horizontal root fractures is the presence of infected,s, Faculty of Dentistry, University of Benghazi, Benghazi, Libya; †School of Dentistry, University ofCollege of Dentistry, New York University, New York, New York.ndodontics, College of Dentistry, New York University, 345 East 24th Street, New York, NY 10010.
Regenerative Endodontic Procedures 1
Clinical Research
necrotic pulp in the canal space. Therefore, control of root canalinfection should be able to arrest and repair inflammatory rootresorption and achieve healing of horizontal root fractures by theformation of hard tissue, soft tissue, or a combination of hardand soft tissue and not by granulation tissue between fracturefragments (3).Traditionally, traumatized teeth with a horizontal root fracture hav-ing pulp necrosis and external/internal inflammatory root resorptionassociated with infected, necrotic pulp in the canal space are treatedwith conventional root canal therapy, including chemomechanicaldebridement of the canal space and root canal filling. Recently, theconcept of regenerative endodontic procedures (REPs) has beenused to manage horizontal root fractures (9) and externalinflammatory root resorption (10, 11) after traumatic injury. Thepurpose of these case reports was to present the potential of usingREPs to manage 3 traumatized teeth, 1 with horizontal root fracture,1 after avulsion that subsequently root fractured, and 1 withperforating root resorption, in terms of elimination of clinical signs/symptoms and resolution of inflammatory osteolytic lesions as well astissue responses to REPs.
Case 1: Horizontal Root FractureA 15-year-old boy suffered from a traumatic injury to his maxillary
anterior teeth 4 weeks ago. The boy complained of severe pain to tooth#8 to touch and biting. Clinical examination showed that tooth #8 wasslightly displaced labially and not discolored. The tooth responded to
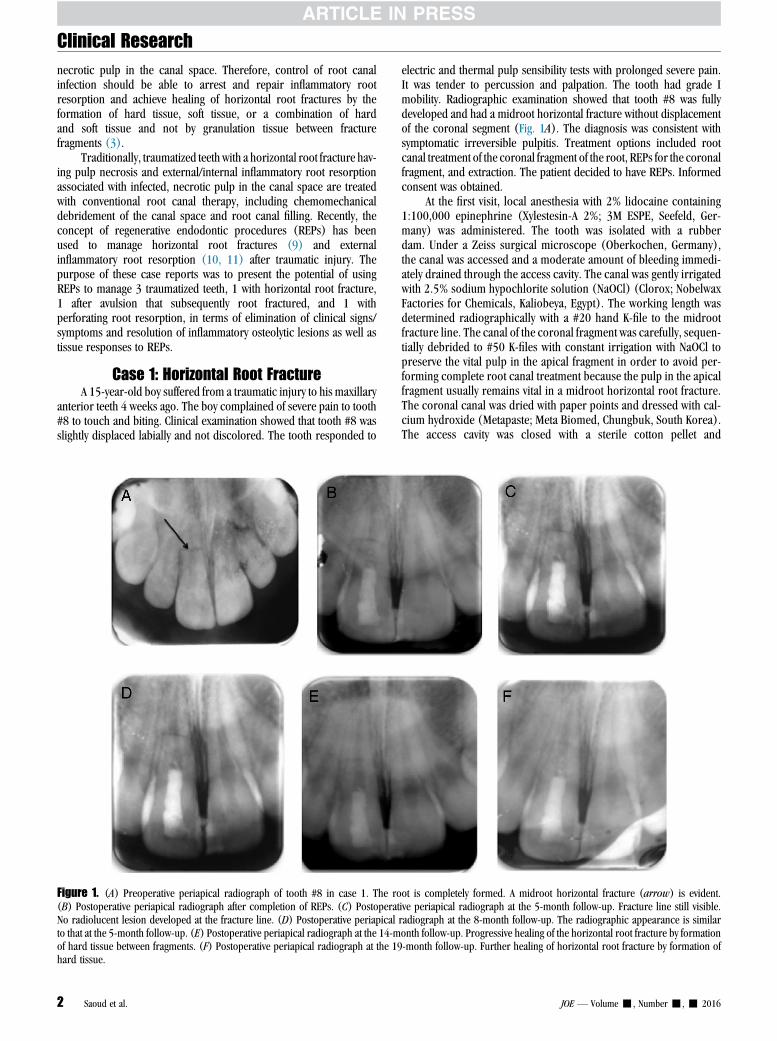
Figure 1. (A) Preoperative periapical radiograph of tooth #8 in case 1. The ro(B) Postoperative periapical radiograph after completion of REPs. (C) PostoperatNo radiolucent lesion developed at the fracture line. (D) Postoperative periapicalto that at the 5-month follow-up. (E) Postoperative periapical radiograph at the 14-mof hard tissue between fragments. (F) Postoperative periapical radiograph at the 19hard tissue.
2 Saoud et al.
electric and thermal pulp sensibility tests with prolonged severe pain.It was tender to percussion and palpation. The tooth had grade Imobility. Radiographic examination showed that tooth #8 was fullydeveloped and had a midroot horizontal fracture without displacementof the coronal segment (Fig. 1A). The diagnosis was consistent withsymptomatic irreversible pulpitis. Treatment options included rootcanal treatment of the coronal fragment of the root, REPs for the coronalfragment, and extraction. The patient decided to have REPs. Informedconsent was obtained.
At the first visit, local anesthesia with 2% lidocaine containing1:100,000 epinephrine (Xylestesin-A 2%; 3M ESPE, Seefeld, Ger-many) was administered. The tooth was isolated with a rubberdam. Under a Zeiss surgical microscope (Oberkochen, Germany),the canal was accessed and a moderate amount of bleeding immedi-ately drained through the access cavity. The canal was gently irrigatedwith 2.5% sodium hypochlorite solution (NaOCl) (Clorox; NobelwaxFactories for Chemicals, Kaliobeya, Egypt). The working length wasdetermined radiographically with a #20 hand K-file to the midrootfracture line. The canal of the coronal fragment was carefully, sequen-tially debrided to #50 K-files with constant irrigation with NaOCl topreserve the vital pulp in the apical fragment in order to avoid per-forming complete root canal treatment because the pulp in the apicalfragment usually remains vital in a midroot horizontal root fracture.The coronal canal was dried with paper points and dressed with cal-cium hydroxide (Metapaste; Meta Biomed, Chungbuk, South Korea).The access cavity was closed with a sterile cotton pellet and
ot is completely formed. A midroot horizontal fracture (arrow) is evident.ive periapical radiograph at the 5-month follow-up. Fracture line still visible.radiograph at the 8-month follow-up. The radiographic appearance is similaronth follow-up. Progressive healing of the horizontal root fracture by formation-month follow-up. Further healing of horizontal root fracture by formation of
JOE — Volume -, Number -, - 2016
Clinical Research
intermediate restorative material (IRM) (Dentsply DeTrey, Konstanz,Germany).At the second treatment visit, tooth #8 was asymptomatic. Localinfiltration anesthesia with 3% Carbocaine (Septodont, Paris, France)without a vasoconstrictor was administered. The tooth was isolatedwith a rubber dam and the access cavity reopened. Metapaste dressingwas gently flushed out of the coronal canal space with NaOCl followed bysterile saline solution. The coronal canal was dried and rinsed with 17%EDTA solution (Pulpdent, Watertown, MA) and dried. The length of thetooth was determined to be 20 mm from the incisor edge to the radio-graphic apex on the digital radiograph. A #20 hand K-file measuring18 mmwas used to gently penetrate into the apical fragment of the canalcontaining vital pulp to carefully provoke bleeding into the coronalcanal space. If the vital pulp in the apical fragment were severelydamaged by the bleeding induction procedure, the potential of pulp tis-sue regeneration into the coronal fragment by a regenerative procedureof the vital pulp tissue in the apical fragment would be compromised.After approximately 10 to 15 minutes, blood became semicoagulated;a 3-mm thickness of a mineral trioxide aggregate (MTA) (DentsplyTulsa Dental, Tulsa, OK) plug was gently placed over the blood clot fol-lowed by a moist cotton pellet. The access cavity was closed with IRMand later restored with light-cured composite resin (Ice Composite;Southern Dental Industry, Victoria, Australia) (Fig. 1B).
The tooth was asymptomatic at the 5- and 8- month follow-upexaminations. However, the fracture line was still visible (Fig. 1C and
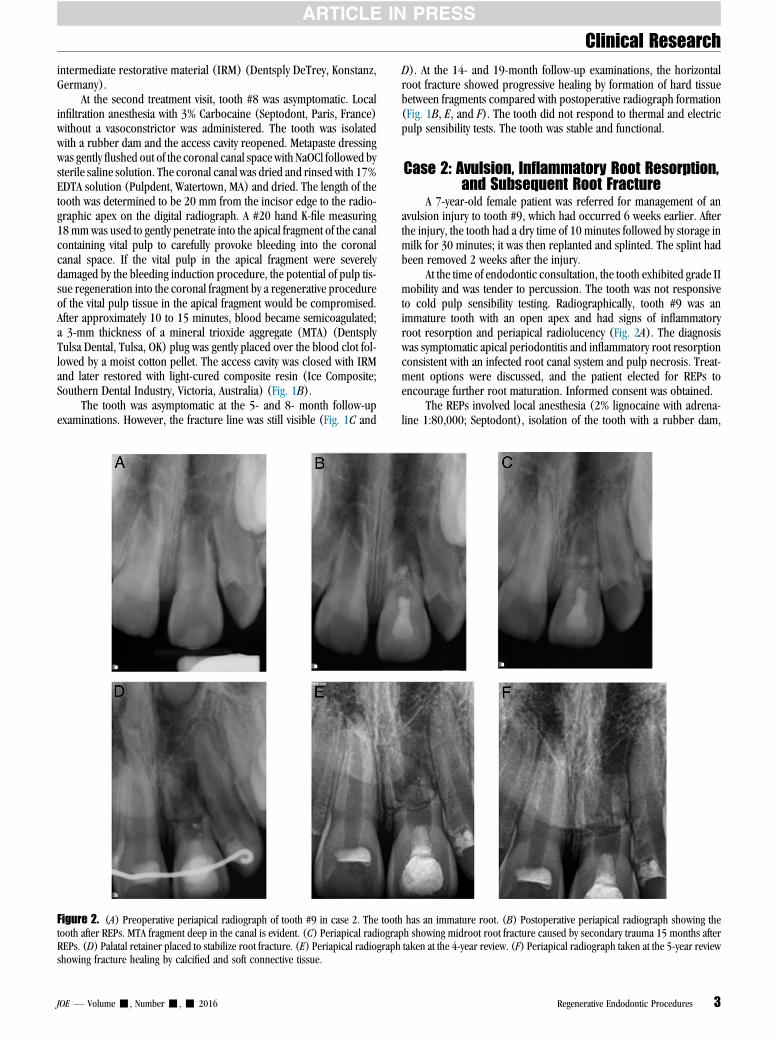
Figure 2. (A) Preoperative periapical radiograph of tooth #9 in case 2. The toothtooth after REPs. MTA fragment deep in the canal is evident. (C) Periapical radiograREPs. (D) Palatal retainer placed to stabilize root fracture. (E) Periapical radiographshowing fracture healing by calcified and soft connective tissue.
JOE — Volume -, Number -, - 2016
D). At the 14- and 19-month follow-up examinations, the horizontalroot fracture showed progressive healing by formation of hard tissuebetween fragments compared with postoperative radiograph formation(Fig. 1B, E, and F). The tooth did not respond to thermal and electricpulp sensibility tests. The tooth was stable and functional.
Case 2: Avulsion, Inflammatory Root Resorption,and Subsequent Root Fracture
A 7-year-old female patient was referred for management of anavulsion injury to tooth #9, which had occurred 6 weeks earlier. Afterthe injury, the tooth had a dry time of 10 minutes followed by storage inmilk for 30 minutes; it was then replanted and splinted. The splint hadbeen removed 2 weeks after the injury.
At the time of endodontic consultation, the tooth exhibited grade IImobility and was tender to percussion. The tooth was not responsiveto cold pulp sensibility testing. Radiographically, tooth #9 was animmature tooth with an open apex and had signs of inflammatoryroot resorption and periapical radiolucency (Fig. 2A). The diagnosiswas symptomatic apical periodontitis and inflammatory root resorptionconsistent with an infected root canal system and pulp necrosis. Treat-ment options were discussed, and the patient elected for REPs toencourage further root maturation. Informed consent was obtained.
The REPs involved local anesthesia (2% lignocaine with adrena-line 1:80,000; Septodont), isolation of the tooth with a rubber dam,
has an immature root. (B) Postoperative periapical radiograph showing theph showing midroot root fracture caused by secondary trauma 15 months aftertaken at the 4-year review. (F) Periapical radiograph taken at the 5-year review
Regenerative Endodontic Procedures 3
Clinical Research
and access into the canal where the pulp was necrotic and had an over-flowing purulent exudate. There was minimal filing of the canal, whichwas irrigated with 1% NaOCl. The canal was dried with paper points andthen medicated with triple antibiotic paste (TAP) (metronidazole500 mg [Flagyl; Amriya Pharm Ind, Alexandria, Egypt]; ciprofloxacin200 mg [Ciprofloxazine; European Egyptian Pharm Ind, Alexandria,Egypt]; and minocycline 100 mg [Minocin; Wyeth, Guangzou, China]).The access cavity was closed with a cotton pellet followed by Cavit(3M ESPE) and glass ionomer cement (Fuji IX, GC, Tokyo, Japan).After 4 weeks, the tooth was asymptomatic. A local anestheticwithout a vasoconstrictor (Scandonest 3% Plain, Septodont Inc,France) was administered. The tooth was isolated under a rubberdam; the canal was accessed and irrigated with 17% EDTA and dried.Bleeding was induced with the use of a size 25 K-file that was bentapically to lacerate periapical tissue 2 mm beyond the apex. MTA wasplaced in the coronal third of the canal although some MTA fragmentdisplaced further into the canal. The access cavity was restored withlight-cured composite resin (Fig. 2B).
Fifteen months after REPs, there was evidence of arrest of inflam-matory root resorption and continued root development with somehard tissue formation in the apical root canal space (Fig. 2C). However,the avulsed tooth sustained further trauma, resulting in a midroot hor-izontal root fracture (Fig. 2C). Teeth #8, #9, and #10 were splinted for6 weeks after root fracture. To provide further long-term stability to thetooth, a fixed palatal retainer across all the maxillary incisor teeth wasplaced (Fig. 2D).
The root fracture showed deposition of calcific tissue formationand connective tissue healing between the separated fragments at the4- and 5-year reviews (Fig. 2E and F). The tooth was not responsiveto thermal and electric pulp sensibility testing and showed no furtherroot maturation (Fig. 2E and F). However, some calcified tissue wasapparent adjacent to the fracture in the apical root fragment (Fig. 2Eand F). The tooth remained stable and functional.
Case 3: Perforating Root ResorptionA 16-year-old boy had a history of traumatic injury to his maxillary
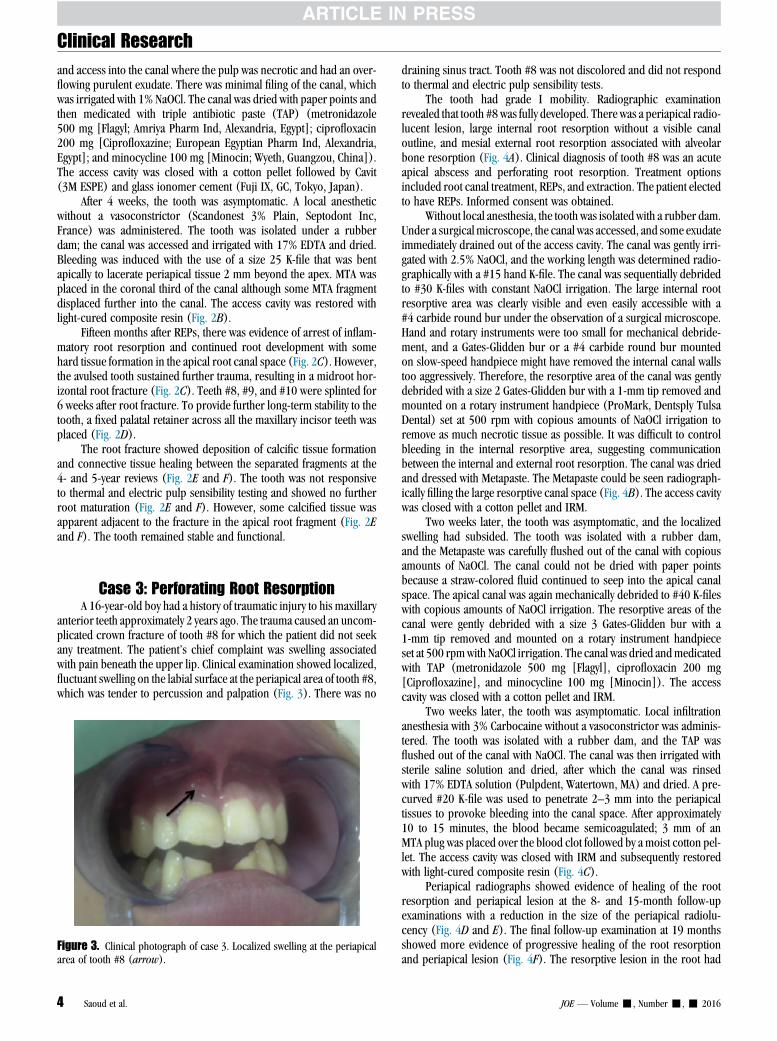
anterior teeth approximately 2 years ago. The trauma caused an uncom-plicated crown fracture of tooth #8 for which the patient did not seekany treatment. The patient’s chief complaint was swelling associatedwith pain beneath the upper lip. Clinical examination showed localized,fluctuant swelling on the labial surface at the periapical area of tooth #8,which was tender to percussion and palpation (Fig. 3). There was no
Figure 3. Clinical photograph of case 3. Localized swelling at the periapicalarea of tooth #8 (arrow).
4 Saoud et al.
draining sinus tract. Tooth #8 was not discolored and did not respondto thermal and electric pulp sensibility tests.
The tooth had grade I mobility. Radiographic examinationrevealed that tooth #8 was fully developed. There was a periapical radio-lucent lesion, large internal root resorption without a visible canaloutline, and mesial external root resorption associated with alveolarbone resorption (Fig. 4A). Clinical diagnosis of tooth #8 was an acuteapical abscess and perforating root resorption. Treatment optionsincluded root canal treatment, REPs, and extraction. The patient electedto have REPs. Informed consent was obtained.
Without local anesthesia, the tooth was isolated with a rubber dam.Under a surgicalmicroscope, the canal was accessed, and some exudateimmediately drained out of the access cavity. The canal was gently irri-gated with 2.5% NaOCl, and the working length was determined radio-graphically with a #15 hand K-file. The canal was sequentially debridedto #30 K-files with constant NaOCl irrigation. The large internal rootresorptive area was clearly visible and even easily accessible with a#4 carbide round bur under the observation of a surgical microscope.Hand and rotary instruments were too small for mechanical debride-ment, and a Gates-Glidden bur or a #4 carbide round bur mountedon slow-speed handpiece might have removed the internal canal wallstoo aggressively. Therefore, the resorptive area of the canal was gentlydebrided with a size 2 Gates-Glidden bur with a 1-mm tip removed andmounted on a rotary instrument handpiece (ProMark, Dentsply TulsaDental) set at 500 rpm with copious amounts of NaOCl irrigation toremove as much necrotic tissue as possible. It was difficult to controlbleeding in the internal resorptive area, suggesting communicationbetween the internal and external root resorption. The canal was driedand dressed with Metapaste. The Metapaste could be seen radiograph-ically filling the large resorptive canal space (Fig. 4B). The access cavitywas closed with a cotton pellet and IRM.
Two weeks later, the tooth was asymptomatic, and the localizedswelling had subsided. The tooth was isolated with a rubber dam,and the Metapaste was carefully flushed out of the canal with copiousamounts of NaOCl. The canal could not be dried with paper pointsbecause a straw-colored fluid continued to seep into the apical canalspace. The apical canal was again mechanically debrided to #40 K-fileswith copious amounts of NaOCl irrigation. The resorptive areas of thecanal were gently debrided with a size 3 Gates-Glidden bur with a1-mm tip removed and mounted on a rotary instrument handpieceset at 500 rpmwith NaOCl irrigation. The canal was dried andmedicatedwith TAP (metronidazole 500 mg [Flagyl], ciprofloxacin 200 mg[Ciprofloxazine], and minocycline 100 mg [Minocin]). The accesscavity was closed with a cotton pellet and IRM.
Two weeks later, the tooth was asymptomatic. Local infiltrationanesthesia with 3% Carbocaine without a vasoconstrictor was adminis-tered. The tooth was isolated with a rubber dam, and the TAP wasflushed out of the canal with NaOCl. The canal was then irrigated withsterile saline solution and dried, after which the canal was rinsedwith 17% EDTA solution (Pulpdent, Watertown, MA) and dried. A pre-curved #20 K-file was used to penetrate 2–3 mm into the periapicaltissues to provoke bleeding into the canal space. After approximately10 to 15 minutes, the blood became semicoagulated; 3 mm of anMTA plug was placed over the blood clot followed by a moist cotton pel-let. The access cavity was closed with IRM and subsequently restoredwith light-cured composite resin (Fig. 4C).
Periapical radiographs showed evidence of healing of the rootresorption and periapical lesion at the 8- and 15-month follow-upexaminations with a reduction in the size of the periapical radiolu-cency (Fig. 4D and E). The final follow-up examination at 19 monthsshowed more evidence of progressive healing of the root resorptionand periapical lesion (Fig. 4F). The resorptive lesion in the root had
JOE — Volume -, Number -, - 2016
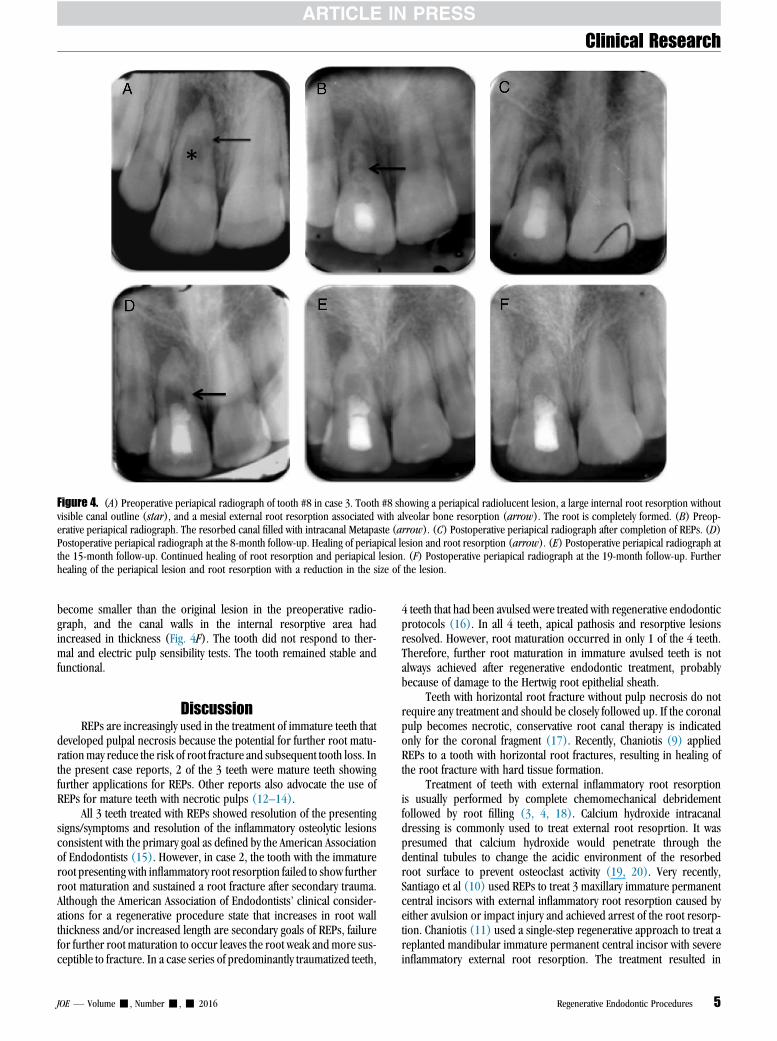
Figure 4. (A) Preoperative periapical radiograph of tooth #8 in case 3. Tooth #8 showing a periapical radiolucent lesion, a large internal root resorption withoutvisible canal outline (star), and a mesial external root resorption associated with alveolar bone resorption (arrow). The root is completely formed. (B) Preop-erative periapical radiograph. The resorbed canal filled with intracanal Metapaste (arrow). (C) Postoperative periapical radiograph after completion of REPs. (D)Postoperative periapical radiograph at the 8-month follow-up. Healing of periapical lesion and root resorption (arrow). (E) Postoperative periapical radiograph atthe 15-month follow-up. Continued healing of root resorption and periapical lesion. (F) Postoperative periapical radiograph at the 19-month follow-up. Furtherhealing of the periapical lesion and root resorption with a reduction in the size of the lesion.
Clinical Research
become smaller than the original lesion in the preoperative radio-graph, and the canal walls in the internal resorptive area hadincreased in thickness (Fig. 4F). The tooth did not respond to ther-mal and electric pulp sensibility tests. The tooth remained stable andfunctional.
DiscussionREPs are increasingly used in the treatment of immature teeth that
developed pulpal necrosis because the potential for further root matu-rationmay reduce the risk of root fracture and subsequent tooth loss. Inthe present case reports, 2 of the 3 teeth were mature teeth showingfurther applications for REPs. Other reports also advocate the use ofREPs for mature teeth with necrotic pulps (12–14).
All 3 teeth treated with REPs showed resolution of the presentingsigns/symptoms and resolution of the inflammatory osteolytic lesionsconsistent with the primary goal as defined by the American Associationof Endodontists (15). However, in case 2, the tooth with the immatureroot presenting with inflammatory root resorption failed to show furtherroot maturation and sustained a root fracture after secondary trauma.Although the American Association of Endodontists’ clinical consider-ations for a regenerative procedure state that increases in root wallthickness and/or increased length are secondary goals of REPs, failurefor further root maturation to occur leaves the root weak and more sus-ceptible to fracture. In a case series of predominantly traumatized teeth,
JOE — Volume -, Number -, - 2016
4 teeth that had been avulsed were treated with regenerative endodonticprotocols (16). In all 4 teeth, apical pathosis and resorptive lesionsresolved. However, root maturation occurred in only 1 of the 4 teeth.Therefore, further root maturation in immature avulsed teeth is notalways achieved after regenerative endodontic treatment, probablybecause of damage to the Hertwig root epithelial sheath.
Teeth with horizontal root fracture without pulp necrosis do notrequire any treatment and should be closely followed up. If the coronalpulp becomes necrotic, conservative root canal therapy is indicatedonly for the coronal fragment (17). Recently, Chaniotis (9) appliedREPs to a tooth with horizontal root fractures, resulting in healing ofthe root fracture with hard tissue formation.
Treatment of teeth with external inflammatory root resorptionis usually performed by complete chemomechanical debridementfollowed by root filling (3, 4, 18). Calcium hydroxide intracanaldressing is commonly used to treat external root resoprtion. It waspresumed that calcium hydroxide would penetrate through thedentinal tubules to change the acidic environment of the resorbedroot surface to prevent osteoclast activity (19, 20). Very recently,Santiago et al (10) used REPs to treat 3 maxillary immature permanentcentral incisors with external inflammatory root resorption caused byeither avulsion or impact injury and achieved arrest of the root resorp-tion. Chaniotis (11) used a single-step regenerative approach to treat areplanted mandibular immature permanent central incisor with severeinflammatory external root resorption. The treatment resulted in
Regenerative Endodontic Procedures 5

Clinical Research
healing of the root resorption and continued root development withthickening of the canal walls in the apical canal.For teeth with internal root resorption, the treatment is similar toexternal root resorption; however, the infected, necrotic pulp tissue inthe internal resorptive defect must be removed (3–5). For perforatingroot resorption, a long-term calcium hydroxide intracanal dressing isusually required to induce calcified tissue formation to close the canalwall defect on the periodontal ligament side before root filling (21).This treatment procedure is similar to calcium hydroxide apexificationto induce apical hard tissue barrier formation. Histologically, the apicalcalcified tissue barrier formed in calcium hydroxide apexificationis cementumlike or bonelike tissue (22) because stem cells in the peri-odontal ligament are capable of differentiating into cementoblasts andosteoblasts but not odontoblasts upon receiving appropriate bioactivesignaling molecules (23). Nevertheless, it has also been shown that along-term calcium hydroxide dressing in the canal space of immaturepermanent teeth could weaken the fragile thin root structure, thusincreasing the likelihood of root fractures (24).
Pulp infection is the primary cause of persistent inflammatory rootresorption and no healing of horizontal root fracture by granulation tis-sue of traumatized teeth. Therefore, elimination of pulp infection shouldbe able to result in healing of root resorption and horizontal root frac-ture by hard tissue, soft tissue, or a combination of hard and soft tissue.The primary goal, elimination of the clinical symptoms/signs and reso-lution of the lesion caused by infection, is similar in both traditional andregenerative endodontic therapy of traumatized teeth with inflammatoryroot resorption and horizontal root fracture. The main differencebetween the 2 treatments is that regenerative endodontic therapy isintended to restore the vitality, immunity, and sensitivity of tissue inthe canal space, whereas traditional root canal therapy is intended toseal the canal space with biocompatible foreign materials to preventreinfection. Only vital tissue has the ability to regenerate, repair, andmount an immune-inflammatory defense response.
In case 1 of a traumatized tooth with a horizontal root fracture, thepulp tissue in the apical fragment usually remains vital (17). Therefore,it was decided to performREPs limited to the coronal fragment based onthe availability of vital pulp tissue in the apical fragment. Bleeding wascarefully induced from the vital pulp tissue in the apical fragment intothe coronal canal, hoping that the apical pulp tissue would proliferateinto the coronal fragment and not be traumatized and become necrotic.This procedure is similar to a previous attempt to regenerate coronalpulp tissue in an immature tooth with irreversible pulpitis by applyingREPs (25). Because the horizontal root fracture in case 1 appeared toheal with hard tissue, it is reasonable to speculate, although there is nohistologic confirmation, that the vital pulp tissue in the apical canalspace likely proliferates into the coronal canal space. Consequently,the pulpal side of the horizontal root fracture was repaired by reparativedentin produced by newly developed odontoblasts differentiated fromstem cells in the vital dental pulp. The periodontal side of the horizontalroot fracture was likely repaired by cementum produced by newlydeveloped cementoblasts differentiated from periodontal ligamentstem cells because the periodontal ligament space was discernible atthe fracture line. Histologically, case 1 may be similar to healing bycalcified tissue in a transverse root-fractured tooth without irreversiblepulp damage (26). If the canal space of the coronal fragment weretreated with traditional root canal therapy and filled with gutta-percha in case 1, the horizontal root fracture would likely be repairedby fibrous connective tissue, cementum, or bone but not by dentinbecause no dental pulp stem cells would be available. In case 2, therewas no further root maturation, whichmight be caused by damage to theHertwig epithelial root sheath caused by avulsion (27). Healing of thehorizontal root fracture may have been more derived from periodontal
6 Saoud et al.
tissues. The size of the fracture defect or the critical size of the lesionbetween the coronal and apical fragments may determine the natureof wound healing. The secondary trauma most likely did not devitalizeavulsed tooth #9 after REPs because some hard tissue was formed adja-cent to the horizontal fracture line in the apical fragment. Importantly,the tooth remained stable and functional.
In case 3, it is not known if the perforating root resorption wasinitiated by internal root resorption, external root resorption, orconcomitant internal and external root resorption. For external inflam-matory root resorption, both traditional root canal treatment and REPsshould be able to achieve a similar treatment outcome as long as rootcanal infection is controlled. Although external root resorption involvesdentin and cementum, the resorptive defect can only be repaired bycementum (28). As mentioned previously, stem cells in the periodontalligament are capable of differentiating into cementoblasts and osteo-blasts and not odontoblasts (23). Repair of bone resorption requiresa cross talk between osteocytes, osteoblasts, and osteoclasts (6–8).However, the cellular and molecular mechanisms of root repair areunclear. It is believed that the mechanism of bone and rootresorption and repair is similar (29).
If perforating root resorption in case 3 were treated with traditionalroot canal therapy using calcium hydroxide and root filling (3, 4, 30),the size of the internal root resorption would remain the same.Therefore, the tooth would be more prone to fracture. However, byusing REPs, the size of internal root resorption was reduced becauseof thickening of the canal walls in the internal resorptive area, thusstrengthening the tooth. This is similar to thickening of the canal wallsin some immature permanent teeth with necrotic pulps after REPs(31). The tissues formed in the canal space of the traumatized toothwith internal root resorption after REPs in case 3 are not known becauseno histology is available. However, in animal models, the tissues formedin the canal space of immature and mature teeth with necrotic pulps afterregenerative procedures are similar; they are cementumlike, bonelike,and periodontal ligament–like tissue, and thickening of the canal wallswas caused by deposition of cementum (32, 33). Therefore, it may bespeculated that thickening of the internal resorptive canal walls wasalso caused by deposition of cementumlike and non-dentinlike tissuein case 3. REPs may be used to treat teeth with large internal rootresorption to reduce resorption size and strengthen the tooth.
ConclusionFrom these and other case reports (9–11), REPs have the potential
to treat teeth with horizontal root fractures, avulsions, and inflammatoryroot resorption.
AcknowledgmentsThe authors deny any conflicts of interest related to this study.
References1. https://www.iadt-dentaltrauma.org/1-9%20%20iadt%20guidelines%20combined%
20-%20lr%20-%2011-5-2013.pdf. Accessed January 15, 2016.2. http://www.aae.org/uploadedfiles/publications_and_research/newsletters/endodon
tics_colleagues_for_excellence_newsletter/ecfe_summer2014%20final.pdf. Acces-sed January 15, 2016.
3. Yu CY, Abbott PV. Response of the pulp, periradicular and soft tissues followingtrauma to the permanent teeth. Aust Dent J 2016;61(suppl 1):39–58.
4. Heithersay GS. Management of root resorption. Aust Dent J 2007;52:S105–21.5. Patel S, Ricucci D, Durak C, Tay F. Internal root resorption: a review. J Endod 2010;
36:1107–21.6. Teitelbaum SL. Bone resorption by osteoclasts. Science 2000;289:1504–8.7. Raggatt LJ, Partridge NC. Cellular and molecular mechanism of bone remodeling.
J Biol Chem 2010;285:25103–8.
JOE — Volume -, Number -, - 2016
https://www.iadt-dentaltrauma.org/1-9%20%20iadt%20guidelines%20combined%20-%20lr%20-%2011-5-2013.pdf

Clinical Research
8. Robling AG, Castillo AB, Tunner CH. Biomechanical and molecular regulation ofbone remodeling. Annu Rev Biomed Eng 2006;8:455–98.9. Chaniotis A. The use of MTA/blood mixture to induce hard tissue healing in a root
fractured maxillary central incisor. Case report and treatment considerations. IntEndod J 2014;47:989–99.
10. Santiago CN, Pinto SS, Sassone LM, et al. Revascularization technique for the treat-ment of external inflammatory root resorption: a report of 3 cases. J Endod 2015;41:1560–4.
11. Chaniotis A. The use of a single-step regenerative approach for the treatment of areplanted mandibular central incisor with severe resorption. Int Endod J 2016;49:802–12.
12. Paryani K, Kim SG. Regenerative endodontic treatment of permanent teeth aftercompletion of root development: a report of 2 cases. J Endod 2013;39:929–34.
13. Wang Y, Zhu X, Zhang C. Pulp revascularization on permanent teeth with openapices in a middle-aged patient. J Endod 2015;41:1571–5.
14. Saoud TM, Martin G, Chen YH, et al. Treatment of mature permanent teeth withnecrotic pulps and apical periodontitis using regenerative endodontic procedures:a case series. J Endod 2016;42:57–65.
15. American Association of Endodontists. AAE clinical considerations for a regener-ative procedure. Available at: www.aae.org/Dental_Professional/Considerations forRegenerative Procedures.aspx. Accessed January 15, 2016.
16. McTigue DJ, Subramanian K, Kumar A. Management of immature permanent teethwith pulpal necrosis-a case series. Pediatr Dent 2013;35:55–60.
17. Andreasen JO, Hjorting-Hansen E. Intraalveolar root fractures: radiographic andhistologic study of 50 cases. J Oral Surg 1967;25:414–26.
18. Cvek M. Treatment on non-vital permanent incisors with calcium hydroxide. II.Effect on external root resorption in luxated teeth compared with effect of root fillingwith gutta-percha. Odontol Revy 1973;24:343–54.
19. Tronstad L, Andreasen JO, Hasselgren G, Kristenson L. pH changes in dental tissuesafter root canal filling with calcium hydroxide. J Endod 1981;7:17–21.
20. Hammartstr€om LE, Blomlof LB, Feiglin B, Lindskog S. Effects of calcium hydroxidetreatment on periodontal healing and resorption. Endod Dent Traumatol 1986;2:184–9.
JOE — Volume -, Number -, - 2016
21. Andreasen JO, Andreasen FM, Anderson J. Textbook and Color Atlas of TraumaticInjuries to the Teeth, 4th ed. Chichester, UK: Wiley-Blackwell; 2007.
22. Cvek M, Sundstr€om B. Treatment of non-vital permanent incisors with calciumhydroxide. V. Histologic appearance of roentgenographically demonstrable apicalclosure of immature roots. Odontol Revy 1974;25:379–92.
23. Seo BM, Miura M, Gronthos S, et al. Investigation of multipotent postnatal stem cellsfrom human periodontal ligament. Lancet 2004;364:149–55.
24. Andreasen JO, Farik B, Munksgaard EC. Long-term calcium hydroxide as aroot canal dressing may increase risk of root fracture. Dent Traumatol2002;18:134–7.
25. Shimizu E, Ricucci D, Albert J, et al. Clinical, radiographic, and histological obser-vation of a human immature permanent teeth with chronic apical abscess after revi-talization treatment. J Endod 2013;39:1078–83.
26. Heithersay GS, Kahler B. Healing responses following transverse root fracture: a his-torical review and case reports showing healing with (a) calcified tissue and (b)dense fibrous connective tissue. Dent Traumatol 2013;29:253–65.
27. Andreasen JO, Kristerson L, Andreasen FM. Damage of the Hertwig’s epithelial rootsheath: effect upon root growth after autotransplantation of teeth in monkeys. DentTraumatol 1988;4:145–51.
28. Bosshardt DD, Schroeder HE. How repair cementum becomes attached to theresorbed root of human permanent teeth. Acta Anat (Basel) 1994;150:253–66.
29. Hammarstr€om L, Lindskog S. General morphological aspects of resorption of teethand alveolar bone. Int Enod J 1985;18:93–108.
30. Fuss Z, Tsesis I, Lin S. Root resorption—diagnosis, classification and treatmentchoices based on stimulation factors. Dent Traumatol 2003;19:175–82.
31. Diogenes A, Henry MA, Teixeira FB, Hargreaves KM. An update on clinical regener-ative endodontics. Endod Topics 2013;28:2–239.
32. Wang X, Thibodeau B, Trope M, et al. Histological characterization of regeneratedtissues in canal space after revitalization/revascularization procedure of immaturedog teeth with apical periodontitis. J Endod 2010;36:56–63.
33. Gomes-Filho JE, Duarte PC, Ervolino E, et al. Histologic characterization of engi-neered tissues in the canal space of closed-apex teeth with apical periodontitis.J Endod 2013;39:1549–56.
Regenerative Endodontic Procedures 7
Related Documents











