How Does Medical Marijuana Legalization Affect The Number of Marijuana Users? An Inclusion and Examination of Different Age Groups Anthony Duong † Abstract This paper studies the effect of medical marijuana legalization on the number of marijuana users in a given state’s general population. To measure the number of marijuana users in each state, I used survey data that covers multiple years. Given this data, I used a differences-in-differences model to see if the changes in marijuana use over time in legalized states are sig- nificantly different from those in non-legalized states. While my initial results showed that legalization signif- icantly increases the percentage of marijuana users in the general population, this was no longer the case when I specified the medical marijuana states that allow for home cultivation and those that do not. When I added home cultivation to the regression, the home cultiva- tion dimension of medical marijuana laws was shown to significantly increase the number of past month users. These results suggest that the marijuana demanders in the general population are not deterred by legal penal- ties, but that the reduction of supply side penalties via home cultivation increases the number of past month users. I. Introduction The main question that this paper seeks to answer is: ”How does the legalization of medical marijuana affect the number of † University of California, Santa Barbara, Department of Economics ([email protected]). Prepared for Economics 196A/B. I thank Professor Shelly Lundberg of UCSB for her expertise and guid- ance throughout the senior thesis process. I would also like to thank the Economics 196A-B class of 2014 for the helpful feedback for the last two school quarters. All errors are my own. 57

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

How Does Medical MarijuanaLegalization Affect The Number ofMarijuana Users? An Inclusion and
Examination of Different Age Groups
Anthony Duong †
Abstract
This paper studies the effect of medical marijuanalegalization on the number of marijuana users in a givenstate’s general population. To measure the numberof marijuana users in each state, I used survey datathat covers multiple years. Given this data, I useda differences-in-differences model to see if the changesin marijuana use over time in legalized states are sig-nificantly different from those in non-legalized states.While my initial results showed that legalization signif-icantly increases the percentage of marijuana users inthe general population, this was no longer the case whenI specified the medical marijuana states that allow forhome cultivation and those that do not. When I addedhome cultivation to the regression, the home cultiva-tion dimension of medical marijuana laws was shown tosignificantly increase the number of past month users.These results suggest that the marijuana demanders inthe general population are not deterred by legal penal-ties, but that the reduction of supply side penalties viahome cultivation increases the number of past monthusers.
I. Introduction
The main question that this paper seeks to answer is: ”Howdoes the legalization of medical marijuana affect the number of
†University of California, Santa Barbara, Department of Economics([email protected]). Prepared for Economics 196A/B. Ithank Professor Shelly Lundberg of UCSB for her expertise and guid-ance throughout the senior thesis process. I would also like to thank theEconomics 196A-B class of 2014 for the helpful feedback for the last twoschool quarters. All errors are my own.
57
marijuana users in a given state?”. Marijuana users were mea-sured in two ways: first time users, and past month users. Theformer has implications for medical marijuana legalization’sinfluence on introducing people to marijuana, while the latterhas implications for medical marijuana legalization’s influenceon those who have tried it to use it on a regular (monthly) ba-sis. Meanwhile, medical marijuana legalization, in its purestsense, is defined in this paper as the legality of qualifying pa-tients and their caregivers to consume marijuana. Most med-ical marijuana states require patients to be 18 to qualify, andin states that do not, minors rarely qualify for medical cards(Pacula, 2007).
To answer this question, I compared marijuana use overtime in medical marijuana states with marijuana use overtime in non-medical marijuana states. Using a differences-in-differences analysis, I attempted to estimate the policy effectof medical marijuana legalization. To do this, I examined thechanges in marijuana use in states that legalized medical mar-ijuana with the changes in marijuana use in states that didnot legalize marijuana, over the same time period. Further-more, I attempted to isolate medical marijuana legalization inits simplest form by distinguishing between medical marijuanastates that allowed patients to cultivate marijuana plants athome and those that did not in my final regressions. Datafor first time use and past month use came from the annualNational Survey on Drug Use and Health, while the data onmedical marijuana legalization and its components came fromprevious studies on the policy.
The results of my model including home cultivation indi-cate that medical marijuana legalization does not have a sig-nificant effect on the number of first time users or past monthusers. These new results contribute to the literature on mar-ijuana use because there has been little work studying therates of marijuana initiation within the general population;most studies focus on non-first time use among the youth.Another contribution includes estimating the effect of bothmedical marijuana legalization and home cultivation laws on
58

different age groups.
II. Literature Review
The marijuana regime literature is important for estimatingthe effects of marijuana policy liberalization on marijuana con-sumption. According to supporters of drug prohibition, in-creased marijuana consumption would have mostly negativeimplications. They argue that consuming illegal drugs likemarijuana is irrational because consumers tend to underesti-mate the drugs’ addictiveness, and that the drugs have nega-tive health consequences (Miron and Zwiebel, 1995). They alsostate that a negative externality of consuming illegal drugs isthat it causes users to commit crimes. Supporters of drug pol-icy liberalization argue that the negative externalities of con-sumption are small compared to those of prohibition such asresources expended on enforcement, and violent crime causedby an illegal drug trade (Miron and Zwiebel, 1995). Thus,supporters of drug policy liberalization assert that without re-gard to its high negative externalities, marijuana prohibitioncan only be justified if it reduces use that produces negativeexternalities or is individually irrational.
As medical marijuana legalization has taken place moreover time, study on the policy has grown within the marijuanaregime literature. Not only is medical marijuana legalizationan insightful topic because it affords even more legal protec-tion for patients than decriminalization can, but also becauseit grants legitimacy to some suppliers (dispensaries). For mostof recent history, almost nothing has been known about supplyside policies. However, Anderson and Rees (2014) were ableto study the effect of dispensaries on teen marijuana use byusing a differences-in-differences model comparing teen mar-ijuana use across years and counties. They used Los Ange-les County, which had hundreds of dispensaries open in the2000’s, as a treatment group, counties with no dispensaries inthe same period as the control group, and local Youth RiskBehavior Survey data to measure teen marijuana use. Theirresults revealed that dispensaries did not have a significant ef-
59
fect on teen marijuana use, since adults still faced high risksof selling marijuana to minors1. In a previous study, Ander-son and Rees (2013) compared trends in hospital admissions tonon-federal hospitals in Colorado (recorded by the Drug AbuseWarning Network) before and after Colorado’s mass openingof dispensaries to study the effect of dispensaries on marijuanause. Their results showed once again that dispensaries haveno effect on levels of marijuana use2.
While dispensary proliferations allow for groundbreakingstudy of reduced supply side penalties, the majority of medicalmarijuana legalization literature has focused on the demandside penalties. Harper, Strumpf and Kaufman (2012) used adifferences-in-differences model to estimate the effect of medi-cal marijuana legalization on state prevalence for past monthuse and perceived risk of monthly use. Over the period 2002-2009, they found no significant impact of legalization on eitherpast month use or perceived risk for any age group3. This is theonly study I came across that looked at the survey data for thegeneral population, as the rest of the studies either focused onadolescents or followed a cohort through time. One such studyby Anderson, Hansen and Rees (2013), used state and nationalYouth Risk Behavior Survey data to construct a linear proba-bility model, finding that legalization has no significant effecton teen marijuana use4. As the medical marijuana literaturehas developed, researchers have increasingly treated medicalmarijuana as a heterogeneous policy. Pacula, Powell, Heatonand Sevigny (2013) looked to isolate the different dimensionsof medical marijuana laws, such as requiring ”pain” for a card,allowing home cultivation, and allowing for dispensaries. Us-ing three different datasets, the National Longitudinal Survey,Youth Risk Behavior Survey, and the Treatment Episode DataSet to measure marijuana use, they ran regressions on differentdimensions of the medical marijuana law. Their differences-
1Anderson, Rees, and Hansen (2013), 19-20.2Anderson and Rees (2013), 4.3Harper, Strumpf, and Kaufman (2012), 210-211.4Anderson, Rees, and Hansen (2013), 17.
60

in-differences results suggested that home cultivation had apositive effect on heavy youth use and that dispensaries ledto more hospital admissions5. However, Anderson and Rees(2013) criticized this study’s inclusion of a dispensary dummy,noting that there are often many years in between the law al-lowing for the dispensary and when dispensaries actually beginto open6.
Given the flaws of a dichotomous dispensary variable, andthe results in Anderson and Rees (2014) and Anderson andRees (2013) that suggest dispensaries have no significant ef-fect on marijuana use, I wanted to study the home cultivationdimension of medical marijuana legalization. Pacula, Kilmer,Grossman and Chaloupka (2007) present the theory that anyreduction of legal penalties for suppliers, particularly homecultivation, will reduce price and increase marijuana use. Thefirst argument is that it is impractical to stop home cultiva-tors from being illegal sellers, while the second is that homecultivation creates ”social availability”7. This ”social avail-ability” argument states that minors would come into contactwith marijuana growers more often under home cultivationand have increased opportunities to try marijuana8. Therewas no specific variable for home cultivation, which motivatedmy inclusion of a home cultivation variable in my model.
I believed my model would contribute a new aspect to theliterature and also synthesize several distinct aspects of differ-ent studies that have not all been brought together in a singlestudy. I had yet to encounter a measure of first time use in theliterature - I had only come across survey data for use in thepast year or past month, or measures of the intensity of mari-juana use among past users. I obtained my measure from theNSDUH, which has the advantage over the NLSY or YRBSof surveying a representative population. This allowed me toaccount for legalization’s effect on the general population, but
5Pacula, Powell, Heaton, and Sevigny (2013), 22.6Anderson and Rees (2013).7Pacula, Kilmer, Grossman, and Chaloupka (2007), 6.8Pacula, Kilmer, Grossman, and Chaloupka (2007), 7.
61

also potentially examine preferences across age groups, anddiversion from adults to minors. While one aforementionedstudy used the NSDUH for estimating the effect of medicalmarijuana legalization, I was able to add the past three yearsof observations (in which several states legalized medical mar-ijuana). And unlike this study, I attempted to isolate homecultivation and as a result, medical marijuana legalization inits most basic sense.
III. Theory
My main hypothesis was that medical marijuana legalizationwould not increase the number of first time users or past monthusers because legal penalties do not deter consumers of mari-juana. Enforcement against consumers is impractical becauseas established by the literature, marijuana transactions mainlyoccur in the privacy of one’s residence9. Considering the diffi-culty for law enforcement to accurately guess when marijuanatransactions are occurring within a home, law enforcementneeds to violate civil liberties in order to curb these kinds oftransactions. And unlike for dealers of harder drugs, who com-mit large amounts of violent crime and reap much bigger prof-its, law enforcement has little support for invading the homesof potential marijuana dealers. Given a near non-existent riskof consuming marijuana, I maintained that marijuana legal-ization does not make it significantly easier for demanders ofmarijuana to consume it for the first time or on a regular basis.
While those 18 or older can obtain a medical card withrelative ease by claiming ailments that are difficult to ver-ify, I predicted that the number of first time and past monthusers in this age group would remain stable. This is becausethe legal protection afforded by medical marijuana legalizationwould only significantly benefit those who already consumemarijuana frequently. If that were the case, intensity of mar-ijuana use among already frequent users might increase, butnot necessarily the number of people who want to use mari-
9Pacula, Kilmer, Grossman, and Chaloupka (2007), 29.
62

juana for the first time or on a monthly basis. For the lattertypes, such modest use makes the expected risk of consump-tion quite small and the fixed cost of purchasing a medicalcard unjustifiable.
Since marijuana use is more common among 12-17 yearolds and 18-25 year olds (see Table 2), it may be argued that26+ year olds lack the underground networks to consume mar-ijuana in the absence of a medical legalization. While this maybe the case, 26+ year olds who have not tried marijuana forthe first time would not want to at their current age. As Iclaimed earlier, transactions in the black market occur withlittle risk to the dealer or consumer. Thus, I predicted thatthose who are 26+ and have not tried marijuana at their cur-rent age decided not to do so because they simply derive littleto no utility from it. I expected this to remain the case in ages26+ because marijuana use becomes less attractive as careerand family obligations become more time consuming and asleisure time decreases.
63

IV. Empirical Strategy
To turn my question into a testable hypothesis, I comparedmedical marijuana states and non-medical marijuana statesacross time in a difference-in-differences model. In essence,the model compares the changes in a variable over time fora treatment group and the changes in the same variable overthe same time for a control group to see if there is a significantdifference. If the difference is significant and shifts in groupcharacteristics have been controlled for, the treatment is saidto have a significant effect on the chosen variable.
For my study, I compared changes in marijuana use be-fore and after legalization in legalization states with changesin marijuana use in non-legalization states over the same timeperiod. Controlling for changes in state characteristics, anysignificant difference would have been caused by the passing ofa medical marijuana law. Knowing this, I expressed the modelin terms of a regression. In my regression, my dependent vari-able was whichever measure of marijuana use I was testing nfirst time use or past month use. To indicate whether a statewas a treatment state, I used a dummy variable that wouldequal 1 if the state would eventually have legalized medicalmarijuana. This variable accounts for inherent differences be-tween legalization states and non-legalization states that mightaffect marijuana use (such as liberal attitudes towards mari-juana use). The variable that estimates the effect of legaliza-tion (thus our variable of interest) is a dummy variable thatequals 1 in legalization states in years after the legalizationhas taken place. If this policy effect variable was significant atthe 5% level, then I would reject my hypothesis that medicalmarijuana legalization does affect marijuana use. Otherwise Iwould fail to reject my hypothesis. Finally, I added a dummyvariable for every year in the time period I studied minus one,to control for any time-related trends in marijuana use.
To control for differences across states, I added variablesfor policies that were not specifically medical marijuana legal-ization, and added some controls for time-variant state charac-teristics. First I added decriminalization variables because de-
64

criminalization may increase marijuana use via reduced penal-ties on the demand side. I also added each state’s unemploy-ment rate and median household income. The former may in-crease marijuana use by allowing for more leisure time, whilethe latter may increase use if marijuana is a normal good.Lastly, I added each state’s tax on a pack of cigarettes sincecigarettes and marijuana may be substitutes, in which caseincreased cigarette taxes could increase marijuana use.
Thus, the regression that I ran to estimate the effect ofmedical marijuana legalization on the percentage of first timemarijuana users was:
Firstuse =β0 + β1Mml + β2Post+ β3Decrim +
β4Postdecrim+ β5Y ear2012 + β6Y ear2011 + . . . +
β14Y ear2003 + β15Unemployment +
β16Medincome+ β17Cigtax+ E
where Firstuse is the percentage within a state that re-ported using marijuana for the first time in the last year. Mmlequals 1 if the state has ever passed a medical marijuana lawup until now and 0 otherwise. Post, the variable of interest,equals 1 if Mml equals 1 within that state, in a year after med-ical marijuana has been legalized in that state. Decrim equals1 if the state has ever passed a marijuana decriminalizationup to this date, and 0 otherwise. Postdecrim equals 1 if de-crim equals 1 for the state and the observation takes placein a year after the state has decriminalized marijuana. Thevariables year2003-year2012 are dummies indicating the yearto which the observation belongs to. Unemployment is thestate’s unemployment rate, Medincome is the state’s medianhousehold income, and Cigtax is the state’s tax on a pack ofcigarettes. I ran this regression on three age cohorts (12-17,18-25, and 26+). Lastly, I ran the same regression with Mon-thuse in place of Firstuse (for the general population as wellas the 12-17, 18-25, and 26+ cohorts).
In my final regressions, however, I added a variable forhome cultivation. 16 out of the 21 states allow patients and
65
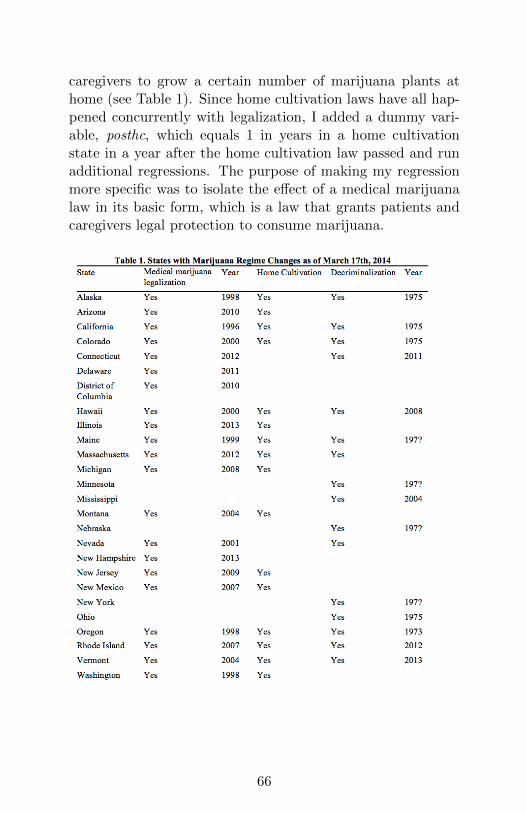
caregivers to grow a certain number of marijuana plants athome (see Table 1). Since home cultivation laws have all hap-pened concurrently with legalization, I added a dummy vari-able, posthc, which equals 1 in years in a home cultivationstate in a year after the home cultivation law passed and runadditional regressions. The purpose of making my regressionmore specific was to isolate the effect of a medical marijuanalaw in its basic form, which is a law that grants patients andcaregivers legal protection to consume marijuana.
66
V. Data Description
The dataset that I used to measure marijuana use was theNational Survey on Drug Use and Health (NSDUH), whichfit my differences-in-differences model in that it allowed forplenty of variation in time and space. The NSDUH, whichis an annual survey sponsored by the Substance Abuse andMental Health Services Administration (SAMHSA), providesinformation on the use of illicit drugs, alcohol, and tobacco inthe non-institutionalized population of the United States aged12 or older, with a sample of approximately 67,500 (Harper,2012). The fact that it is annual fit my model because I wasable to examine years before and after medical marijuana le-galizations. The data covered the period 2002-2012, or 11 con-secutive years of marijuana use outcomes. This time period fitwell n it was recent enough to capture pre-legalization andpost-legalization for 9 out of the 20 medical marijuana states(plus District of Columbia). Since the NSDUH covers all 50states and District of Columbia, I had 9 treatment groupsand 42 control groups in my difference-in-differences model.Finally, multiplying the number of years and the number ofstates gave me 561 observations of state marijuana use.
The way the NSDUH measures marijuana use and forwhom it measures marijuana use fit the purpose of my pa-per. I was interested in the number of marijuana users, andnot the frequency or intensity of marijuana use among pastusers. The NSDUH provides state prevalence rates for firsttime marijuana use in the past year, which accurately mea-sures marijuana initiates. It also provides prevalence rates forpast month use, which I believe is an indicator of an occasionaluser. These prevalence rates are also broken down into four agegroups: ages 12+ (the general population), 12-17(minors), 18-25, and 26+. This allowed me to run regressions on differentage groups, which could have implications for the exclusion-ary power of the medical card’s age requirement, preferencesacross age groups, and the prevalence of legal-to-black mar-ket diversion. This age group breakdown was also valuablefor the home cultivation variable, since that is another age-
67

exclusionary law.Though the NSDUH fit my model, the survey data has
some inherent flaws. First, their state level estimates are de-rived from Bayesian hierarchical models and are associatedwith some uncertainty (Harper, 2012). Also, a single preva-lence rate will be an estimate based on an average of datafrom two years. For example, NSDUH surveys are claimed tocover ”2010-2011” rather than just 2010 or 2011. This madechoosing which year to attribute to a give prevalence rate apersonal decision, but ultimately the results were not sensitiveto this decision. For independent variables, I simply codedthe various marijuana policies as 1 or 0, and use governmentdata on the controls for economic conditions. I coded medicalmarijuana legalization and home cultivation according to thelegal status of each state as listed in Pacula, Powell, Heatonand Sevigny (2013). The listing was verified by legal scholars,and for the most part overlapped with information I foundon http://medicalmarijuana.procon.org/. My criteria for de-criminalization was the elimination of jail time for carryingup to .8 ounces of marijuana. For decriminalization I foundnews reports documenting decriminalization laws, as well asthe website called NORML.org that linked me to state billspassing decriminalization.
While I considered the legal interpretation of each state’smedical marijuana laws accurate, there were still shortcomingsin my specification of medical marijuana legalization. As tobe expected with a policy that varies across states, the mainconcern is unobserved heterogeneity. While I could accuratelypinpoint medical marijuana legalization, as well as home cul-tivation, a major component that I was missing was the al-lowance of dispensaries. There is a shortage of accurate dataon the number of dispensaries in each state, let alone the num-ber of dispensaries in each state for every year in my model.As pointed out in the literature, the lag between the passingof a dispensary law and the actual opening of dispensaries ina state is significant and makes a dichotomous dispensary in-dicator inaccurate. Not being able to pick up the effect of
68
dispensaries may have led to the overestimation of at leastone of the medical marijuana legalization effect and the homecultivation effect.
VI. Results
I started off by running the simple model of the regression forboth measures of marijuana use. However, adding home cul-tivation to the regressions and running them again changedthe results. After I added home cultivation to the regressionsfor the total population, legalization was the only variablefor which significance changed. However, there were manychanges across age groups after adding home cultivation. WhileI believe home cultivation was a proper specification, somepart of the home cultivation model may be causing erroneousinteractions between variables.
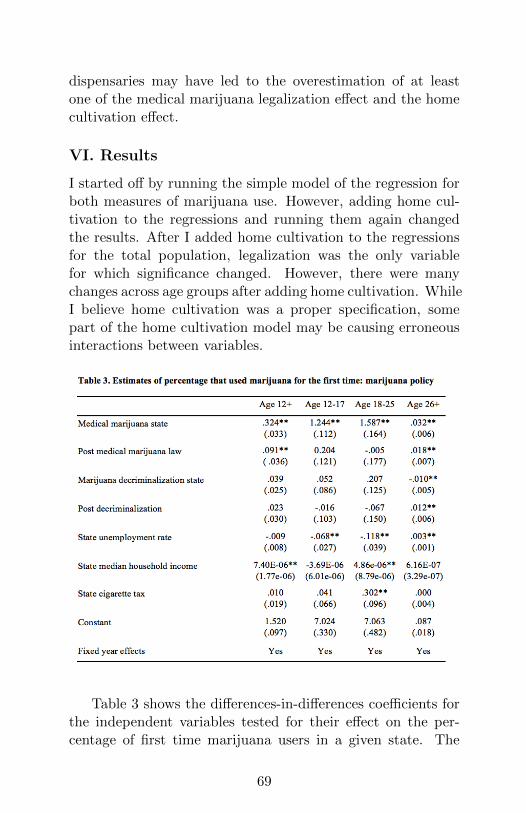
Table 3 shows the differences-in-differences coefficients forthe independent variables tested for their effect on the per-centage of first time marijuana users in a given state. The
69

coefficient on post-medical marijuana legalization tells us theeffect of medical marijuana legalization on first time marijuanause. This coefficient ended up positive and significant at the5% level. At this point, I rejected the null hypothesis thatmedical marijuana legalization has no significant effect on firsttime marijuana use. However, legalization was found to havedifferent significance for different age groups. For those ages12-17, as well as those ages 18-25, legalization’s coefficient wasinsignificant at the 5% level. The only age group for which le-galization had a significant effect was the 26 and older group,but the difference that legalization created in this group’s firsttime use was pivotal in making legalization’s effect on the totalpopulation significant.
Some of the coefficients on the controls had potentiallyvaluable implications. The coefficient for a state having passeda medical marijuana law at any point to this date was positiveand significant at the 5% level for all age groups (and would re-main so in every regression). This suggests medical marijuanastates contain characteristics besides for a medical marijuanalaw (such as liberal attitudes toward marijuana use) that havea positive and significant effect on the number of first timeusers in those states. Thus, prior to any exogenous shock,medical marijuana states can be expected to have a signifi-cantly higher percentage of first time users than non-medicalmarijuana states in any given year. Next, the coefficients forbelonging to a decriminalization state and the decriminaliza-tion law were insignificant on overall first time use, addingsupport to the idea the theory that penalties on marijuanaconsumers are largely ineffective.
70
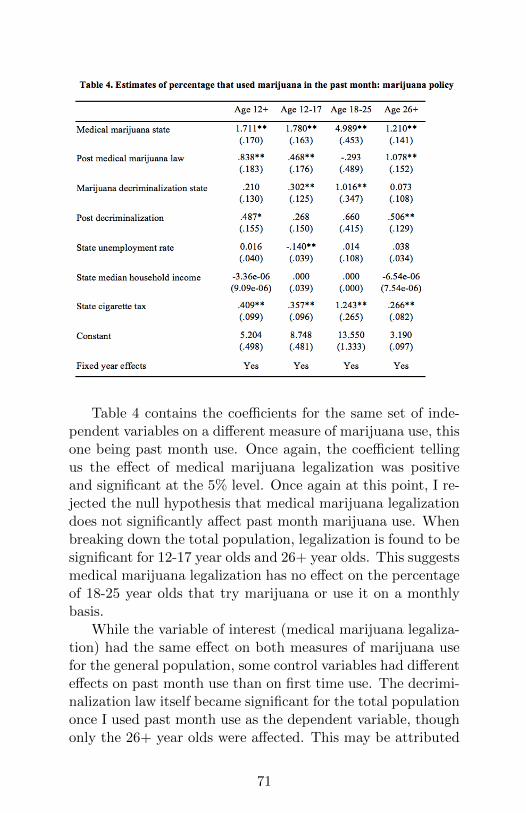
Table 4 contains the coefficients for the same set of inde-pendent variables on a different measure of marijuana use, thisone being past month use. Once again, the coefficient tellingus the effect of medical marijuana legalization was positiveand significant at the 5% level. Once again at this point, I re-jected the null hypothesis that medical marijuana legalizationdoes not significantly affect past month marijuana use. Whenbreaking down the total population, legalization is found to besignificant for 12-17 year olds and 26+ year olds. This suggestsmedical marijuana legalization has no effect on the percentageof 18-25 year olds that try marijuana or use it on a monthlybasis.
While the variable of interest (medical marijuana legaliza-tion) had the same effect on both measures of marijuana usefor the general population, some control variables had differenteffects on past month use than on first time use. The decrimi-nalization law itself became significant for the total populationonce I used past month use as the dependent variable, thoughonly the 26+ year olds were affected. This may be attributed
71
to a 26+ year olds being more risk averse than younger pop-ulations. Lastly, the state cigarette tax became positively sig-nificant for the total population. Perhaps, increased cigarettetaxes lead to people substituting occasional cigarette use withoccasional marijuana use.
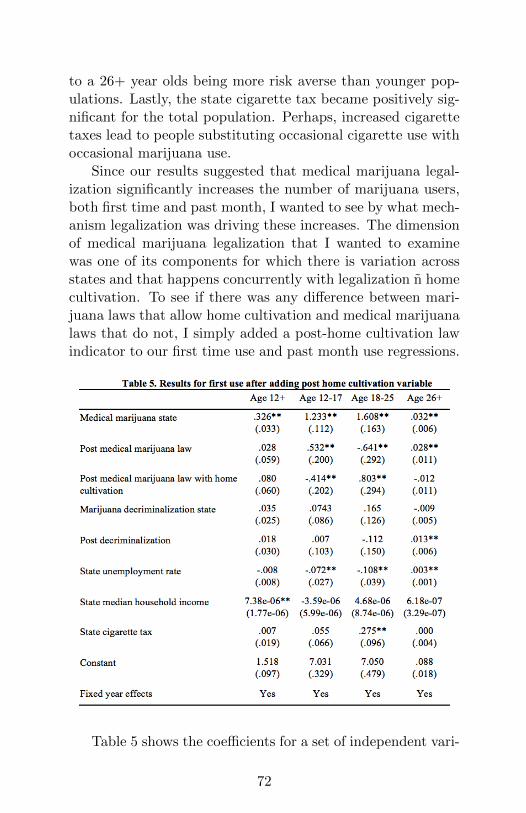
Since our results suggested that medical marijuana legal-ization significantly increases the number of marijuana users,both first time and past month, I wanted to see by what mech-anism legalization was driving these increases. The dimensionof medical marijuana legalization that I wanted to examinewas one of its components for which there is variation acrossstates and that happens concurrently with legalization n homecultivation. To see if there was any difference between mari-juana laws that allow home cultivation and medical marijuanalaws that do not, I simply added a post-home cultivation lawindicator to our first time use and past month use regressions.
Table 5 shows the coefficients for a set of independent vari-
72

ables that includes post-home cultivation, with respect to thedependent variable of first time use. After adding home culti-vation, the resulting coefficient for medical marijuana legaliza-tion lost its significance for the total population. It is positivelysignificant for 12-17 year olds and 26+ year olds, which sug-gests that there is some diversion of marijuana from the legalmarket to the black market and that 26+ year olds are respon-sive to legal penalties (meaning I reject my hypothesis for eachof these age groups). The fact that these groups were not piv-otal in making legalization significant for the entire populationsuggests that legalization does not increase the number of usersin a given state. Though home cultivation itself was insignifi-cant, it seemed to pick up some effects from decriminalizationstate, decriminalization itself, and unemployment, since theylost their significance for the total population as well. Over-all, while adding home cultivation makes medical marijuanalegalization insignificant and suggests that we should fail toreject my main hypothesis, there may be some error with thismodel. This is because the coefficients for medical marijuanalegalization’s effect on 18-25 year olds, and home cultivation’seffect on 12-17 year olds are significant and negative, which isdifficult to explain.
73
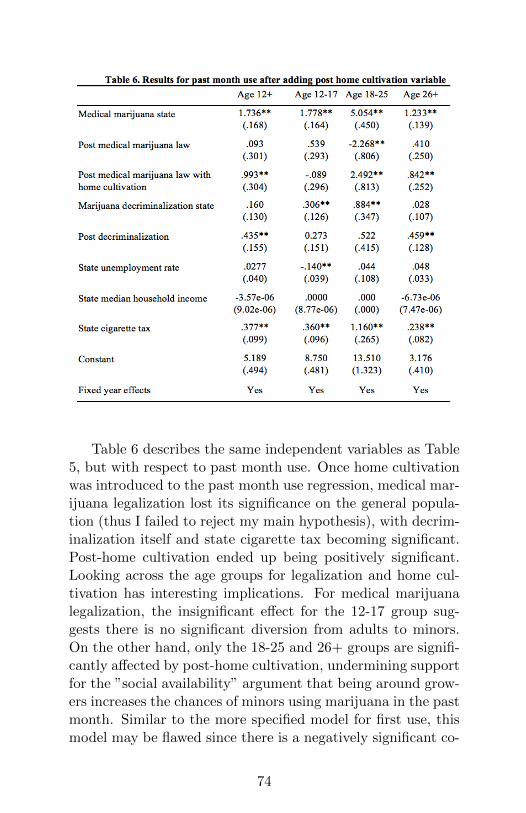
Table 6 describes the same independent variables as Table5, but with respect to past month use. Once home cultivationwas introduced to the past month use regression, medical mar-ijuana legalization lost its significance on the general popula-tion (thus I failed to reject my main hypothesis), with decrim-inalization itself and state cigarette tax becoming significant.Post-home cultivation ended up being positively significant.Looking across the age groups for legalization and home cul-tivation has interesting implications. For medical marijuanalegalization, the insignificant effect for the 12-17 group sug-gests there is no significant diversion from adults to minors.On the other hand, only the 18-25 and 26+ groups are signifi-cantly affected by post-home cultivation, undermining supportfor the ”social availability” argument that being around grow-ers increases the chances of minors using marijuana in the pastmonth. Similar to the more specified model for first use, thismodel may be flawed since there is a negatively significant co-
74

efficient for legalization on 18-25 year olds, which is difficultto explain.
VII. Conclusion
Since the literature currently focuses on teens, there is notmuch study of medical marijuana legalization’s effect on thegeneral population or specifically its effect on adult age users.Under legalization, the population over the age of 18 is thegroup that can gain legal protection to consume marijuanawith a medical card. Thus examining legalization’s effect onthis group should reveal just how much, if at all, legal penal-ties deter marijuana adult consumers. Also, adults can moreeasily obtain marijuana, and it may be difficult for law en-forcement to practically stop them from distributing or shar-ing with minors. Thus, legalization’s effect on adolescent usehas implications for the power of diversion from legal marketto black market, and for the effectiveness of age-exclusionarymeasures.
My results, after distinguishing between medical marijuanalaws with a home cultivation component and medical mari-juana laws in their essential form, suggest that medical mar-ijuana legalization does not significantly increase the numberof marijuana users or past month users in the general popula-tion. For the first use measure, legalization was found to besignificant for minors and 26+ year olds, suggesting diversioncontributed to first time use by minors and that 26+ year oldsare sensitive to legal risk. It is in the past month use regressionwhere the limitations of the home cultivation specification arefound: a negatively significant coefficient for legalization on18-25 year olds suggests some error.
One way this study could be improved would be to includea method of controlling for erroneous interactions between dif-ferent marijuana policy variables. In addition, state-level dataon both the first openings of dispensaries, and the number ofdispensaries operating in a given year would allow researchersto isolate components of medical marijuana legalization, bothsupply side and demand side, accurately and assess their ef-
75
fects on marijuana use.
References
[1] Anderson, D. Mark and Daniel I. Rees, 2014. ”The Legal-ization of Recreational Marijuana: How Likely is the WorstCase Scenario?” Journal of Policy Analysis and Manage-ment, 33 221-232.
[2] Anderson, D. Mark and Daniel I. Rees, 2013. ”The Roleof Dispensaries: The Devil is in the Details”. Journal ofPolicy Analysis and Management, 33 (2014) 235-240.
[3] Anderson, D. Mark and Daniel Rees and Benjamin Hansen,2013. Medical Marijuana Laws and Teen Marijuana Use.Under Review.
[4] Harper S., Strumpf EC, and JS Kaufman (2012). ”Do med-ical marijuana laws increase marijuana use? Replicationstudy and extension”. Annals of Epidemiology, 22, 207-212.
[5] Khatapoush S and D Hallfors (2004). ”Sending the wrongmessage: Did medical marijuana legalization in Californiachange attitudes about the use of marijuana?” Journal ofDrug Issues, 35, 751-770
[6] Miron, Jeffrey A., and Jeffrey Zwiebel. 1995. ”The Eco-nomic Case against Drug Prohibition.” Journal of Eco-nomic Perspectives, 9(4): 175-192.
[7] Pacula, Rosalie Liccardo & Beau Kilmer & Michael Gross-man & Frank J. Chaloupka, 2007. ”Risks and Prices: TheRole of User Sanctions in Marijuana Markets,” The B.E.Journal of Economic Analysis & Policy, Berkeley Elec-tronic Press, vol. 10(1).
76
[8] Pacula, Rosalie Liccardo, David Powell, Paul Heaton, andEric Sevigny. 2013. Assessing the Effects of Medical Mar-ijuana Laws on Marijuana and Alcohol Use: The Devil isin the Details. Working Paper Series (May).
[9] (n.d.). Retrieved February 17, 2014, fromwww.NORML.org.
[10] (n.d.) Retrieved February 17, 2014, fromhttp://medicalmarijuana.procon.org/.
77
Related Documents











