PROS AND CONS IN SURVEILLANCE IMAGING IN LYMPHOMA BY : SUMMAR ELMORSHIDY ASSISTANT LECTURER OF CLINICAL ONCOLOGY CLINICAL ONCOLOGY DEPARTMENT ASSIUT UNIVERSITY HOSPITALS

Pros and cons in surveillance imaging in lymphoma
Jul 17, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
PROS AND CONS IN SURVEILLANCE IMAGING IN LYMPHOMA
BY : SUMMAR ELMORSHIDY ASSISTANT LECTURER OF CLINICAL ONCOLOGY CLINICAL ONCOLOGY DEPARTMENT ASSIUT UNIVERSITY HOSPITALS
Introduction
Despite improvements in survival rates, relapses after first-line therapy can occur in 20-50% of patients with advanced-stage Hodgkin’s lymphoma (HL) or diffuse large-B-cell lymphoma (DLBCL).
In both diseases, treatment failures are usually
observed within 3 years of completion of treatment with the majority of relapses occurring in the first 12 months for HL and 18 months for DLBCL.
However, no consensus exists on an optimal surveillance strategy to determine a preclinical relapse after first remission.
Most modern reviews continue to show that the majority of lymphoma relapses are identified through signs or symptoms, regardless of the imaging schedule.
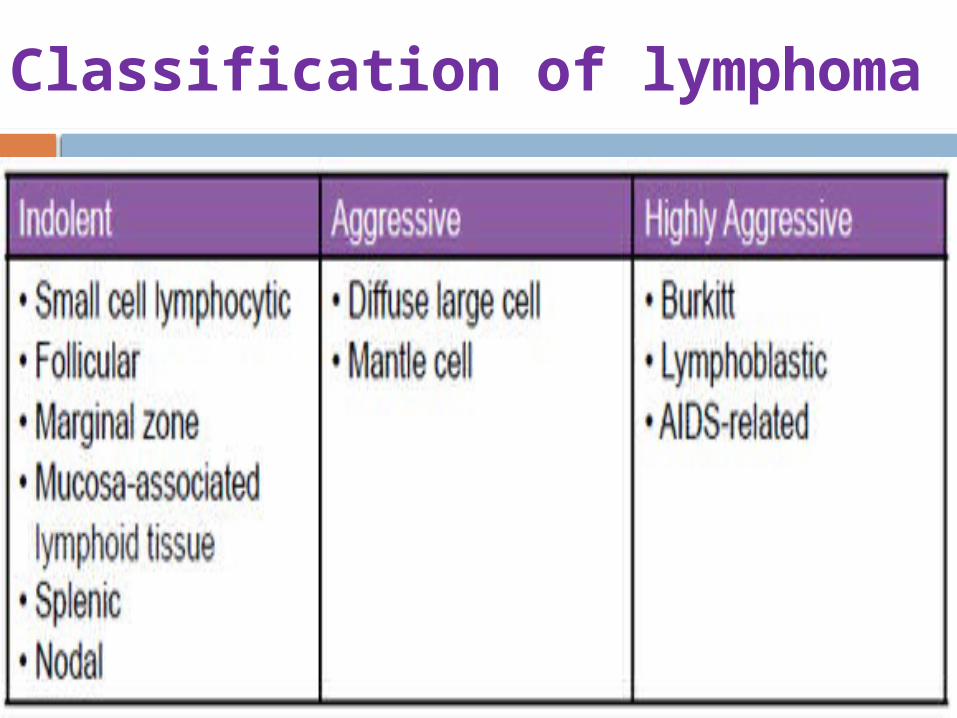
Classification of lymphoma
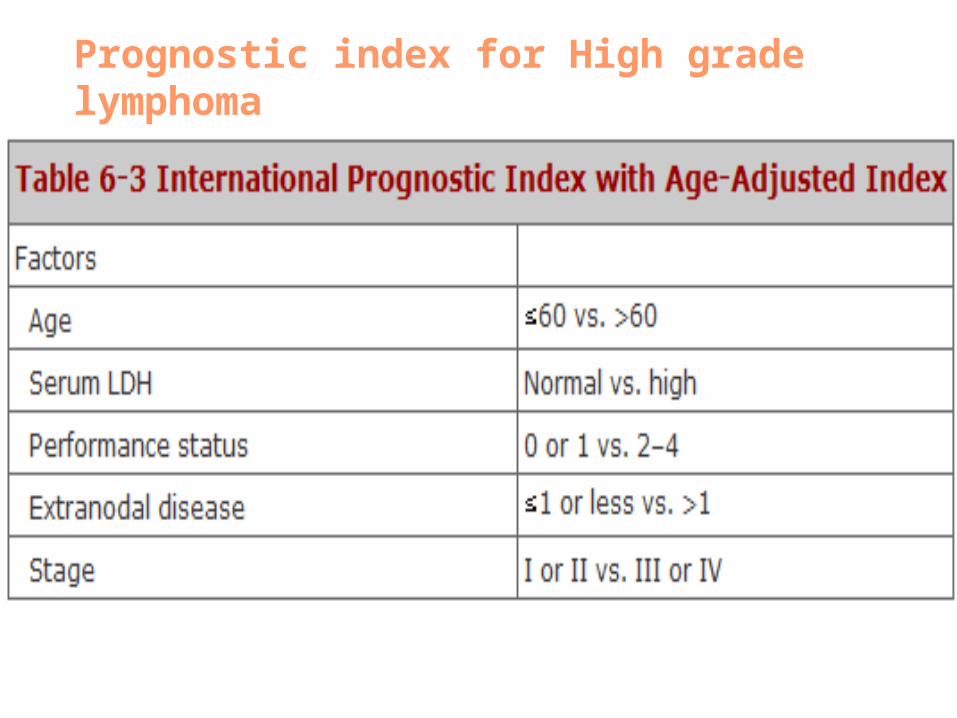
Prognostic index for High grade lymphoma
Response evaluation criteria in lymphoma
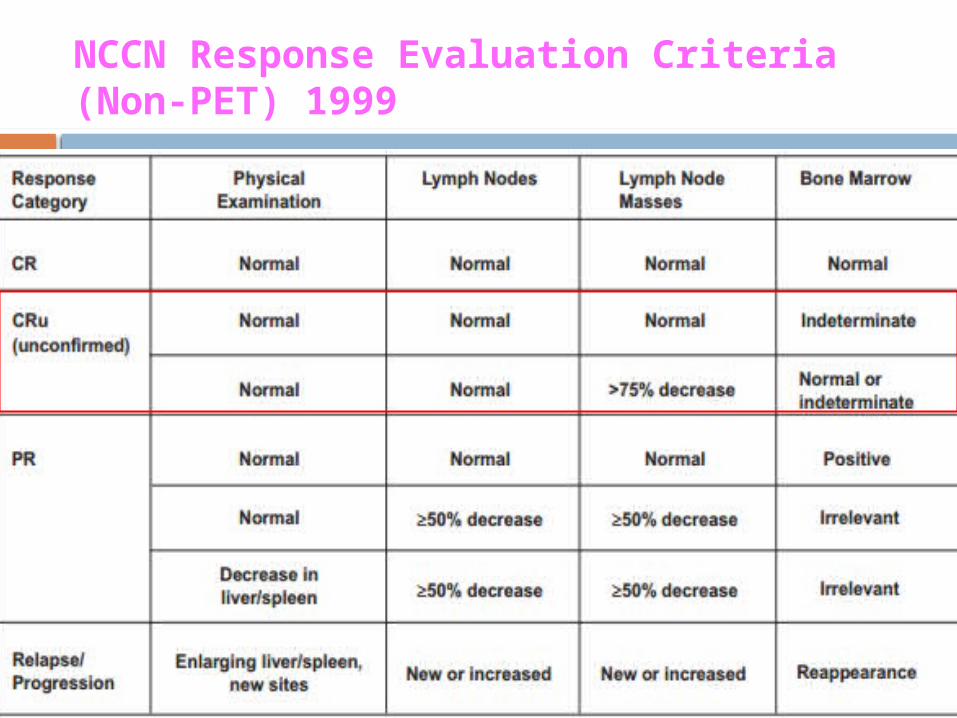
NCCN Response Evaluation Criteria (Non-PET) 1999
CR is defined by the disappearance of all known sites involved at baseline. LN O must be decreased to <1.5 cm. Enlarged spleen and liver should return to normal
size and lymphoma-related nodules should disappear. BM must show no infiltration if involved at baseline. CRu (CR unconfirmed) referred to residual tissue(>75% size reduction) of undetermined significance.This category disappeared with the advent of PET.
The original response evaluation criteria included CRu (Complete Response uncertain)
It was not possible to determine whether residual masses on CT scan were residual lymphoma, scar tissue or nonmalignant process
Advent of PET in early 2000’s changed the scenario
Should PET be used for monitoring response
to therapy? Interim PET
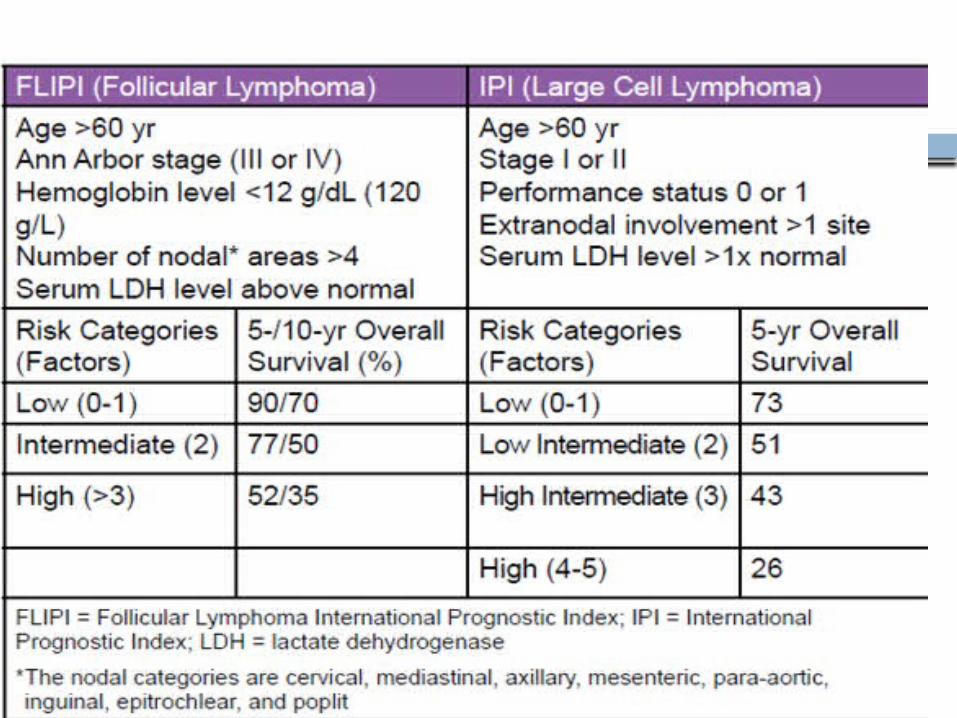
. The International Prognostic Index (IPI) and the follicularlymphoma IPI (FLIPI) are currently used clinical prognostic indices for diffuse large B-cell lymphoma and follicular lymphoma, respectively.
However, each of these prognostic models uses static pretreatment characteristics to predict the likelihood ofresponse and survival in a given patient. PET, on the other hand,relies on the dynamic properties of the tumor mass both during and after treatment to predict outcome.
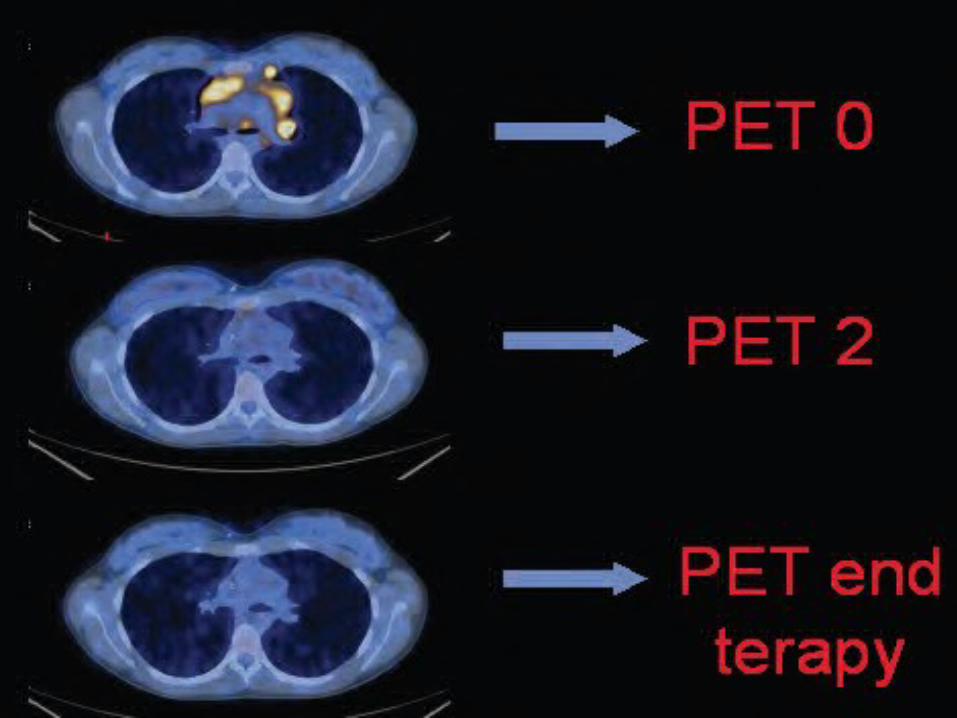
Interim PET during treatment (after 2-3 cycles) is considered a surrogate test for chemosensitivity in lymphoma to predict final treatment outcome.
In a study of advanced-stage HL, interim PET after 2 courses of ABVD was the most important independent prognostic factor for PFS.
The 5-point scale (Deauville’s criteria) is a standardized method for interim PET reporting,comparing residual FDG uptake to the mediastinum or liver background

End of treatment (EOT) response assessment
EOT PET has a high negative predictive value and lower positive predictive value, possiblydue to inflammatory reactions causing false-positive images.
A positive EOT PET in a single residual mass has a sensitivity of 43-100% in HL and 37-87% in DLBCL, while the specificity is 67-100% and 75-100%, respectively.
In HL, a high proportion of patients with a PET-neg
residual mass after chemotherapy remain free of disease (high negative predictive value).
Sensitivity and specificity of EOT PET in predicting
disease relapse in DLBCL were 33-77% and 82-100%, respectively.
A recent trial suggests that EOT PET in FL is the
most potent predictor of remission duration after
standard R-CHOP treatment.
Published Guidelines for Hodgkin Lymphoma
2014 NCCN Guidelines for Hodgkin Lymphoma NCCN, the American College of Radiology (ACR)
Appropriateness Criteria, and ESMO have also published guidelines for follow-up of Hodgkin lymphoma.
NCCN and ACR also include guidelines for imaging studies to detect second malignancies related to prior therapy for Hodgkin lymphoma. These NCCN Guidelines recommend:
Chest imaging (chest radiograph or CT) every 6 to 12 months for the first 2 to 5 years
Abdominal/pelvic CT scans every 6 to 12 months for the first 2 to 3 years (this is a category 2B recommendation, which means that there was lower-level evidence and nonuniform consensus)
Annual chest imaging after 5 years for patients at increased risk for lung cancer (optional for patients who did not receive radiotherapy to the chest, were treated with nonalkylating agents, and have no other risk factors)
Annual breast screening in women to start 8 to 10 years posttherapy or at age 40 years, whichever comes first, if chest or axillary radiation were administered
The American Cancer Society recommends breast MRI for women who received irradiation to the chest between the ages of 10 and 30 years.
Surveillance PET scans are not recommended.
Published guidelines for the survillance imaging in NHL
FOLLICULAR LYMPHOMA : H&P every 3 to 6 months for the first 5 years
then annually or as clinicalIy indicated.Surveillance imaging :Up to 2 years post completion of treatment .CT SCAN no more than 6 months
interval.DLBCL : H&P every 3 to 6 months for the first 5 years
then annually or as clinicalIy indicated.Repeat CT scan only if clinically indicated .
Prerequisites of surveillannce Imaging
the
probability of relapse in the population being tested as well as
SENSETIVITY
SPECIFICITY frequency OF THE TEST .
WHO BENEFITS from THE SURVEILLANCE IMAGING.
The benefits of monitoring for the
recurrence depend on
The prevalence of relapse in both HL and DLBCL is rare, with reportedly only one relapse per 68 visits in HL and per 40–45 visits for patients with aggressive non-Hodgkin’s lymphoma (NHL) based on routine CT scans.
While PET/CT has not been closely investigated in a surveillance setting, it has become clear that its accuracy is superior to that of CT imaging.
According to results from a meta-analysis, FDG-PET predicts disease relapse with a sensitivity and specificity of
50-100% and 67-100%, respectively, for HL and 33-77% and 82-100%, respectively, for NHL,
There are many reports of the sensitivity and
specificity of computed tomography (CT) scanning in
detecting lymphoma., a reasonable average would
be a sensitivity of approximately 60% to
65% and specificity of approximately 90%
to 95%.

ROLE OF SURVEILLANCE IMAGING
Most surveillance approaches in lymphoma have focused on early
detection of recurrence, with the hope of prolonged survival and
potential cure.
Because many patients with lymphoma relapsing after complete
remission have a chance for a durable second remission with salvage
therapy (ie, usually autologous hematopoietic stem-cell
transplantation), it is reasonable to consider the possibility that early
detection of relapse in asymptomatic patients might increase the
chance for cure. To achieve this goal, screening for early relapse with
surveillance imaging would need to be accurate and not associated
with excessive toxicity or cost
A report by Liedtke et al found that patients with relapsed
diffuse large B-cell lymphoma detected by surveillance CT
scan were likely to have low-volume disease, and the
lymphoma was likely to be chemosensitive. However, they
found only a non significant trend toward better survival.
Studies of Hodgkin’s lymphoma, including that reported
by Voss et al,1 have not shown improved treatment outcome
with routine imaging using CTscans.
There are fewer reports on using surveillance CT scans for
follicular lymphoma in remission. This lymphoma typically
grows slowly, and asymptomatic relapse might be present for
an extended time.
Gerlinger et al described 71 patients who achieved complete remission from relapsed follicular lymphoma through autotransplantation and were observed with annual surveillance imaging.
Surveillance imaging detected relapse in 16 patients, and routine clinical evaluation found relapse in 18 patients.
The relapses detected by surveillance imaging did not require therapy for a longer time compared with the clinical relapses, but overall survival was not affected.
ROLE OF PET-CT IN SURVEILLANCE IMAGING OF
LYMPHOMA: A FOX HUNT
PET is a noninvasive, 3-dimensional, metabolic imaging technique that
uses a radiopharmaceutical to target a specific physiologic process (eg,
glucose metabolism, amino acid metabolism, DNA synthesis).
The most widely used pharmaceutical is the radiolabeled glucose
analog fluorine-18-deoxyglucose (FDG). FDG is transported into cells and
phosphorylated in a similar manner to glucose. However, because FDG-6-
phosphate is not a substrate for glucose-6-phosphate isomerase and
because FDG-6-phosphate is typically not dephosphorylated in tumors, it
becomes trapped in the cell and reaches a near equilibrium state at
approximately 60 minutes after injection. The positron-emitting 18F
isotope to which FDG is linked decays, and the emitted positron
annihilates after“bumping” into an electron, generating 2 511-KeV
photons emittedin nearly opposite directions that are detected by the
PET scanner.
Should surveillance PET scanning be part ofstandard of care?PET for posttherapy surveillance While PET/CT has not been closely investigated in a surveillance setting,
it has become clear that its accuracy is superior to that of CT imaging.
According to results from a meta-analysis, FDG-PET predicts disease relapse with a sensitivity and specificity of 50- 100% and 67-100%, respectively, for HL and 33-77% and 82-100%, respectively, for NHL, irrespective of the association of a residual mass on CT.
Even with its relatively high sensitivity, the risks and benefits of routine
surveillance PET/CT imaging remain controversial, mainly, because of its cost, radiation burden and the high rate of false-positive results (30-80%)3,8-12 with potential consequences of overtreatment.
a Trial of the role of PET in posttreatment surveillanceof
lymphoma rem Jerusalem e t al prospectively evaluated 36
HL patients who underwent PET every 4 to 6 months for 2
years at the completion of treatment. One patient had
residual disease and 4 relapsed during follow-up; however, in
2 of these patients, there were disease-related symptoms.
Thus, PET identified disease before the onset of symptoms
only 3 of 36 patients with confirmed relapsed disease but
resulted in false-positive studies in another 6 patients.
In general, surveillance PET/CT scanning to detect relapse has a higher false positive rate than CT scans and has not had an impact on survival.
A report from Denmark described 53 patients with Hodgkin’s lymphoma who underwent 127 surveillance PET/CT scans. The positive predictive value was 19%, and the negative predictive value was 100%.
How to increase benefits of surveillance PET :
A multitude of variables should be considered in order to increase the benefits of surveillance PET/CT imaging in the proper population of patients.
Presence of clinical symptoms: In a number of studies,
relapses were reported to be associated with clinical symptoms in 55-80% of patients during follow-up :
In a large group of uniformly treated patients with aggressive NHL
(n=108), 80% of relapses were diagnosed on the basis of clinical symptoms while planned surveillance imaging identified recurrence in 22% of the cases preceding symptoms.
Patients were 4.1 times more likely to have low-risk disease if relapse was
diagnosed by routine imaging compared with those diagnosed by clinical findings with median overall 5-year survivals of 54% and 43%, respectively (P=0.13).
Pre-therapy risk for recurrence. Early response profile: early response profile
as evidenced by interim PET imaging. Interim PET/CT after two chemotherapy cycles
in both HL and DLBCL has been proposed as a surrogate test for chemosensitivity, proving to be the most powerful independent prognosticator for treatment outcome.
Cost-benefit ratio and survival benefit.
Site of relapse. One important issue to consider in an attempt to decrease false positive readings is that approximately 75% of relapses involve the initial disease sites although new sites of disease can also arise in 25% of patients. It is, therefore, crucial to interpret the follow up PET scans with the full knowledge of the extent of the original disease.
What are the current limitations of PET scans?
False-positive and false-negative PET results have the potential to impact patient management. False positives arise because FDG is taken up in any process associated with increased glycolysis, for example, inflammation, infection, granulomatous disease such as sarcoidosis.
Castellucci et al reported that 21.3% of positive PET scans reviewed (n 134) had nontumoral uptake.
Abnormal FDG uptake has also been associated with hyperplasia of the thymus in HL patients. Similarly, abnormal uptake has been associated with hyperplasia in the bone marrow and spleen in patients receiving granulocyte colony-stimulating factor after chemotherapy.
To minimize the frequency of false-positive PET, the imaging subcommittee of the International Harmonization Project (IHP) recommended performing PET at least 3 weeks following chemotherapy and preferably 8 to 12 weeks after radiation therapy.
Potential risks of surveillance imaging
These include the possibility of inducing a second
cancer because of the radiation dose:
• The risk of causing cancer through medical imaging has
recently been highlighted reports suggested that medical
imaging might be a significant cause of cancer in the
United States. This seems to be a particular concern in
young patients.
• The anticipated incidence of second cancers was higher
in younger patients than in older patients and higher in
women than in men largely because of the risk of
inducing breast cancer in young women.
The risk of biopsies is necessary to document relapse after a positive image, and potential anxiety and fear associated with these images, which could lower quality of life:
It is difficult to quantitate the risk of injury after biopsies performed to document recurrence in patients with abnormal images. Given the low positive predictive value of surveillance images, treatment should never be instituted in this setting without documentation of relapse by biopsy
The financial cost of surveillance
imaging is considerable:
At the University of Nebraska Medical Center, the
current charge for a CTscan of the chest, abdomen,
and pelvis is $6,931, and the charge for a
PET/CT scan is $7271. Thus, total charges for patients
receiving five to 10 surveillance images via one of
these techniques would range from $34,655 to
$72,710. Multiplied by all the patients who achieve
remissionfrom lymphoma in the United States, this is
not an insignificant contribution to health care costs,
particularly in light of the lack of proof of benefit.
So, what is the answer to the question, “Who benefits from surveillance imaging?”
The report by Voss et al1 in JCO suggests that the answer is not children with Hodgkin’s lymphoma who achieve remission.
However, it is still possible that in high-risk patients (ie, where the higher chance of relapse would increase the positive predictive value of an abnormal image) for whom potentially curative salvage therapy is available, these images might improve survival.

A clinical trial in this group of patients comparing routine follow-up using history, physical examination,
and laboratory studies with the same evaluation plus surveillance imaging could have an important impact on practice—either to make surveillance routine or to decrease its use.
Until such a trial is completed, surveillance imaging for patients with lymphoma in remission should not be routinely performed.

THANK
YOU
Related Documents