doi:10.1006/phrs.2000.0786, available online at http://www.idealibrary.com on Pharmacological Research, Vol. 43, No. 6, 2001 PROPIONYL-L-CARNITINE AS PROTECTOR AGAINST ADRIAMYCIN-INDUCED CARDIOMYOPATHY MOHAMED M. SAYED-AHMED a,* , TAREK M. SALMAN c , HUSSIEN E. GABALLAH b , SHERIF A. ABOU EL-NAGA b , RAFFAELLA NICOLAI d and MENOTTI CALVANI d a Pharmacology Unit, b Medical Oncology Department, National Cancer Institute, Cairo University, c Biochemistry Department, Al-Azhar Faculty of Pharmacy, d Scientific Department, Sigma-Tau, Pomezia, Roma, Italy Accepted 28 November 2000 Propionyl-L-carnitine (PLC) is a naturally occurring compound that has been considered for the treatment of many forms of cardiomyopathies. In this study, the possible mechanisms whereby PLC could protect against adriamycin (ADR)-induced cardiomyopathy were carried out. Administration of ADR (3 mg kg -1 i.p., every other day over a period of 2 weeks) resulted in a significant two-fold increase in serum levels of creatine phosphokinase, lactate dehydrogenase and glutamic oxaloacetic transaminase, whereas daily administration of PLC (250 mg kg -1 , i.p. for 2 weeks) induced non-significant change. Daily administration of PLC to ADR-treated rats resulted in complete reversal of ADR-induced increase in cardiac enzymes except lactate dehydrogenase which was only reversed by 66%. In cardiac tissue homogenate, ADR caused a significant 53% increase in malonedialdehyde (MDA) and a significant 50% decrease in reduced glutathione (GSH) levels, whereas PLC induced a significant 33% decrease in MDA and a significant 41% increase in GSH levels. Daily administration of PLC to ADR-treated rats completely reversed the increase in MDA and the decrease in GSH induced by ADR to the normal levels. In rat heart mitochondria isolated 24 h after the last dose, ADR induced a significant 48% and 42% decrease in 14 CO 2 released from the oxidation of [1- 14 C]palmitoyl-CoA and [1- 14 C]palmitoylcarnitine, respectively, whereas PLC resulted in a significant 66% and 54% increase in the oxidation of both substrates, respectively. Interestingly, administration of PLC to ADR-treated rats resulted in complete recovery of the ADR- induced decrease in the oxidation of both substrates. In addition, in rat heart mitochondria, the oxidation of [1- 14 C]pyruvate, [1- 14 C]pyruvate and [1- 14 C]octanoate were not affected by ADR and/or PLC treatment. Moreover, ADR caused severe histopathological lesions manifested as toxic myocarditis which is protected by PLC. Worth mentioning is that PLC had no effect on the antitumour activity of ADR in solid Ehrlich carcinoma. Results from this study suggest that: (1) in the heart, PLC therapy completely protects against ADR-induced inhibition of mitochondrial β -oxidation of long-chain fatty acids; (2) PLC has and/or induces a powerful antioxidant defense mechanism against ADR-induced lipid peroxidation of cardiac membranes; and finally (3) PLC has no effect on the antitumour activity of ADR. c 2001 Academic Press KEY WORDS: cardiomyopathy, adriamycin, propionyl-L-carnitine, β -oxidation, malondialdehyde and reduced glutathione. INTRODUCTION Adriamycin (ADR) was among the first anthracycline antibiotics to be in clinical use in cancer chemother- apy [1]. It has a broad spectrum antitumour activity against a variety of hematological and solid tumours [2]. Unfortunately, the chronic administration of ADR is * Corresponding author. Pharmacology Unit, Cancer Biology Depart- ment, National Cancer Institute, Fum El-Khalig, Kasr El-Aini Street, Cairo, Egypt. associated with the development of dose-dependent and irreversible cardiomyopathy, which restricts its usefulness in cancer chemotherapy [3, 4]. Cardiomy- opathy is the major limiting complication of ADR that affects 30–40% of the patients who receive a cumula- tive dose more than 500 mg m -2 [5, 6]. Hence, even in responding tumours, it is necessary to stop ADR administration once a cumulative dose of 500 mg m -2 is reached to prevent the onset of irreversible cardiac damage [4, 6]. 1043–6618/01/060513–08/$35.00/0 c 2001 Academic Press

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

doi:10.1006/phrs.2000.0786, available online at http://www.idealibrary.com onPharmacological Research, Vol. 43, No. 6, 2001
PROPIONYL- L -CARNITINE AS PROTECTOR AGAINSTADRIAMYCIN-INDUCED CARDIOMYOPATHY
MOHAMED M. SAYED-AHMEDa,∗, TAREK M. SALMANc, HUSSIEN E. GABALLAHb, SHERIF A.ABOU EL-NAGAb, RAFFAELLA NICOLAI d and MENOTTI CALVANId
aPharmacology Unit, bMedical Oncology Department, National Cancer Institute, Cairo University,cBiochemistry Department, Al-Azhar Faculty of Pharmacy,dScientific Department, Sigma-Tau, Pomezia,
Roma, Italy
Accepted 28 November 2000
Propionyl-L-carnitine (PLC) is a naturally occurring compound that has been considered for thetreatment of many forms of cardiomyopathies. In this study, the possible mechanisms whereby PLCcould protect against adriamycin (ADR)-induced cardiomyopathy were carried out. Administrationof ADR (3 mg kg−1 i.p., every other day over a period of 2 weeks) resulted in a significant two-foldincrease in serum levels of creatine phosphokinase, lactate dehydrogenase and glutamic oxaloacetictransaminase, whereas daily administration of PLC (250 mg kg−1, i.p. for 2 weeks) inducednon-significant change. Daily administration of PLC to ADR-treated rats resulted in completereversal of ADR-induced increase in cardiac enzymes except lactate dehydrogenase which wasonly reversed by 66%. In cardiac tissue homogenate, ADR caused a significant 53% increase inmalonedialdehyde (MDA) and a significant 50% decrease in reduced glutathione (GSH) levels,whereas PLC induced a significant 33% decrease in MDA and a significant 41% increase in GSHlevels. Daily administration of PLC to ADR-treated rats completely reversed the increase in MDAand the decrease in GSH induced by ADR to the normal levels. In rat heart mitochondria isolated24 h after the last dose, ADR induced a significant 48% and 42% decrease in14CO2 released fromthe oxidation of [1-14C]palmitoyl-CoA and [1-14C]palmitoylcarnitine, respectively, whereas PLCresulted in a significant 66% and 54% increase in the oxidation of both substrates, respectively.Interestingly, administration of PLC to ADR-treated rats resulted in complete recovery of the ADR-induced decrease in the oxidation of both substrates. In addition, in rat heart mitochondria, theoxidation of [1-14C]pyruvate, [1-14C]pyruvate and [1-14C]octanoate were not affected by ADRand/or PLC treatment. Moreover, ADR caused severe histopathological lesions manifested astoxic myocarditis which is protected by PLC. Worth mentioning is that PLC had no effect onthe antitumour activity of ADR in solid Ehrlich carcinoma. Results from this study suggest that:(1) in the heart, PLC therapy completely protects against ADR-induced inhibition of mitochondrialβ-oxidation of long-chain fatty acids; (2) PLC has and/or induces a powerful antioxidant defensemechanism against ADR-induced lipid peroxidation of cardiac membranes; and finally (3) PLC hasno effect on the antitumour activity of ADR. c© 2001 Academic Press
KEY WORDS: cardiomyopathy, adriamycin, propionyl-L-carnitine,β-oxidation, malondialdehyde and reducedglutathione.
INTRODUCTION
Adriamycin (ADR) was among the first anthracyclineantibiotics to be in clinical use in cancer chemother-apy [1]. It has a broad spectrum antitumour activityagainst a variety of hematological and solid tumours [2].Unfortunately, the chronic administration of ADR is
∗Corresponding author. Pharmacology Unit, Cancer Biology Depart-ment, National Cancer Institute, Fum El-Khalig, Kasr El-Aini Street,Cairo, Egypt.
associated with the development of dose-dependentand irreversible cardiomyopathy, which restricts itsusefulness in cancer chemotherapy [3, 4]. Cardiomy-opathy is the major limiting complication of ADR thataffects 30–40% of the patients who receive a cumula-tive dose more than 500 mg m−2 [5, 6]. Hence, evenin responding tumours, it is necessary to stop ADRadministration once a cumulative dose of 500 mg m−2
is reached to prevent the onset of irreversible cardiacdamage [4, 6].
1043–6618/01/060513–08/$35.00/0 c© 2001 Academic Press

514 Pharmacological Research, Vol. 43, No. 6, 2001
In view of the irreplaceability of ADR in cancerchemotherapy, one of the research aims being pursuedmost intensively is the possibility of eliminating itscardiotoxicity or reducing it to an acceptable level. Inthis regard, various strategies have been tried, exempli-fied by the use of free radical scavengers [7, 8], ironchelators [9, 10], calcium antagonists [11], histamine andadrenergic receptor blockers [12]. Recent in vitro andin vivo studies have demonstrated thatL-carnitine hasthe potential ability to protect the myocardium againstADR-induced cardiotoxicity without interfering withits antitumour activity [13–16]. Propionyl-L-carnitine(PLC) is a naturally occurring short-chain derivativeof L-carnitine and it has several advantages overL-carnitine. First, PLC has a higher transport rate intocardiac myocytes thanL-carnitine, thus increasing themyocardial carnitine content [17]. Second, PLC hasa higher affinity for mascular carnitine transferasesthan L-carnitine or its other derivatives; therefore, PLCis highly specific for both skeletal and cardiac mus-cles [17, 18]. Third, the propionate group of PLC canbe used by mitochondria as an anaplerotic metabolicsubstrate, thus providing energy at the mitochondriallevel in the absence of oxygen consumption [18, 19].Finally, PLC suppresses the formation of hydroxylradicals, thus acting as a free radical scavenger [19, 20].Although many experimental and clinical studies havereported that PLC has a more pronounced protectiveeffect thanL-carnitine in the treatment of many forms ofischemia and cardiomyopathies [17, 19–21], its use asa protective agent against ADR-related cardiomyopathyis still relatively limited and its mode of action is stillunclear. A recent study from our laboratory [22] and anearlier one from an other [23] are the only two studieswhich have demonstrated that PLC has a considerableprotective effect against ADR-induced cardiotoxicity.Since these studies were performedin vitro using isolatedheart myocytes, mitochondria and slices in which theentire biological environment and the role of substratecompetition were lacking, therefore the protectionachieved by PLC was not complete and its mechanismwas unclear. Hence, the present study has been initiatedwith the following specific aims: (i) identifying themechanisms whereby daily administration of PLC couldprotect against ADR cardiotoxicity using the 2 weekADR cardiomyopathic rat model and (ii) to evaluate theeffect of PLC on the antitumour activity of ADR usingtumour growth delay (TGD) analysis in solid Ehrlichcarcinoma (SEC)-bearing mice.
MATERIALS AND METHODS
AnimalsMale Sprague–Dawley rats, weighing 200–250 g, and
female Swiss albino mice, weighing 20–22 g, wereobtained from the animal house of the National CancerInstitute (NCI), Cairo, Egypt. Animals were allowed free
access to standard diet essentially free fromL-carnitinederivatives and waterad libitum. A line of Ehrlich ascitescarcinoma (EAC) cells was supplied by the courtesy ofDr C. Benckuijsen, Amsterdam, the Netherlands, andmaintained in female mice by weekly i.p. transplantationsince 1982.
Materials[1-14C]pyruvate, [2-14C]pyruvate, [1-14C]palmitoyl-
CoA, [1-14C]palmitoyl-carnitine and [1-14C]octanoatewere purchased from New England Nuclear (Boston,MA, USA). Sigma was the source of bovine serumalbumin (BSA, essentially fatty acid free), palmitoyl-carnitine and palmitoyl-CoA. ADR was a generous giftfrom the NCI drug store. PLC (a product of Sigma-TauPharmaceuticals) was kindly supplied by Dr MenottiCalvani, Sigma Tau, Pomezia, Italy. All other chemicalsused were of the highest analytical grade.
ADR and PLC administration protocolIn this study, the ADR treatment regimen used to
develop a cumulative cardiotoxicity has been establishedby Beanlandset al. [24]. A total of 80 male Sprague–Dawley rats were used and divided at random into fourgroups, 20 animals each. In the first group animals wereinjected i.p. with ADR (18 mg kg−1) as a total cumulativedose divided into six equal doses 3 mg kg−1 each,every other day over a period of 2 weeks. At the endof this period, animals were sicker, weaker, and signsof cardiotoxicity including ascites, liver rigidity and a50% mortality rate were evident. Animals in the secondgroup were injected daily with PLC (250 mg kg−1, i.p.)for 2 weeks (no mortality was observed in this group).Animals in the third group were injected a combination ofADR and PLC exactly according to the first and secondregimens. In this group, PLC was injected 1 h beforeadministration of ADR (10% mortality was observed inthis group). In the fourth group, animals were injectedwith normal saline (0.5 ml per 200 g body weight, i.p.)and served as controls. At 24 h after the last injection,animals were anesthetized with ether, and blood sampleswere obtained by heart puncture. Serum was separated formeasurement of cardiac enzymes.
Assessment of cardiac enzymesSerum levels of creatine phosphokinase (CPK), lactate
dehydrogenase (LDH) and glutamic oxaloacetic transam-inase (GOT) were determined according to the methodsof Gruber [25], Swanson and Wilkinson [26], and Reit-man and Frankels [27], respectively.
Determination of malondialdehyde and reducedglutathione levels in cardiac tissue
Animals were killed by decapitation after exposureto ether in a dessicator kept in a well-functioninghood. Hearts were quickly excised, washed with saline,blotted with a piece of filter paper, and homogenized inice-bidistilled water in a Branson sonifier (250, VWR

Pharmacological Research, Vol. 43, No. 6, 2001 515
Scientific, Danbury, Conn., USA). Reduced glutathione(GSH) and malondialdehyde (MDA) levels in heart tissuehomogenate were determined spectrophotometrically us-ing the methods of Ellman [28] and Buege and Aust [29],respectively. Hearts were removed for histopathologicalexamination, fixed in 10% neutral buffered formalin andstained (H & E stain) for microscopic examination.
Isolation of rate heart mitochondriaRat heart mitochondria were isolated 24 h after the end
of the chronic treatment protocol according to Chappeland Hansford [30]. The isolation buffer contained 0.21 Mmannitol, 0.07 M sucrose, 5 mM Tris-HCl (pH 7.4), and1 mM EGTA.
Substrate oxidation in rat heart mitochondriaSubstrate oxidation in mitochondria was measured
using the method of Yanget al. [31]. The reactionmixture contained in a final volume of 0.9 ml was50 mM Tris-HCl (pH 7.4), 120 mM KCl, 0.5 mML-carnitine, 0.5 mM EDTA-K2 (pH 7.4), 2 mM KPi ,and 0.1 mg ml−1 BSA, which was placed in a 25-ml Erlenmeyer flask. To this suspension was added0.1 ml of a single metabolic substrate yielding a finalconcentration of 2 mM [1-14C]pyruvate, 2 mM [2-14C]pyruvate, 40µM [1-14C]palmitoyl-CoA, 50µM [1-14C]palmitoyl-carnitine and 0.2 mM [1-14C]octanoate.Substrate oxidation was initiated by the addition ofrat heart mitochondria (0.5–1 mg). The incubation wascontinued under shaking at 37◦C for 30 min. Aninjection of 0.3 ml of 1 M hyamine hydroxide wasadministered through the septum into the center wellto absorb the released14CO2, and the reaction wasterminated by injecting 1 ml of 7% perchloric acidthrough the septum into the incubation medium. Theflasks were shaken continuously for an additional 2 hat 37◦C. After that time, the plastic center well wasremoved, placed into a scintillation vial containing 10 mlof Scinti Verse BD, and counted in a liquid scintillationcounter (Betamatic Kontron, Sebai, Italy).
Effect of PLC and ADR on the tumour growth insolid Ehrlich carcinoma (SEC)-bearing mice
In this experiment, 2×106 EAC cells were transplantedsubcutaneously into the right thigh of the lower limbof each mouse. Mice with a palpable solid tumourmass (100 mm3) that developed within 7 days afterimplantation were divided into four groups and treated asfollows. In the first group, animals were treated i.p. withsingle 18 mg kg−1 ADR, whereas the second group weretreated i.p. with single 250 mg kg−1 PLC. Animals inthe third group were injected a combination of ADR andPLC exactly as the first and second regimens, whereasthe last group served as controls and were injected i.p.with normal saline. The change in tumour volume (TV)was measured every other day using a Vernir caliperand calculated by the following formula according to
Table IEffect of ADR, PLC, and their combination on serum cardiac
enzymes
Serum enzyme levels (U L−1)Groups LDH CPK GOT
Control 542± 24 515± 17 52± 2ADR 1260± 43a 1040± 46a 112± 6a
PLC 504± 36 585± 14 54± 3ADR + PLC 833± 58a,b 580± 27b 69± 7a,b
(1) Values are presented as mean± SEM (n = 10). (2) aIndicatesignificant change of ADR and ADR+PLCvscontrol (P<0.05).(3) bIndicate significant change of ADR+PLCvsADR (P<0.05).
Osmanet al. [32].
Tumour Volume (mm3) = 41(A/2)2× (B/2)/3,
whereA is the minor tumour axis andB is the major axis.TGD was then calculated as the additional days for
each individual treated tumour to reach 500 mm3 beyondthat of the control group.
Determination of proteinProtein concentration were determined by Bio-Rad
protein assay (Bio-Rad, Richmond, VA, USA) accordingto the published method of Bradford [33].
RESULTS
Twenty-four h after the last dose, ADR induced asignificant two-fold increase in serum levels of LDH,CPK, and GOT. Administration of PLC to ADR-treatedanimals resulted in complete reversal of the ADR-induced increase in cardiac enzymes except LDH whichis partially restored (TableI).
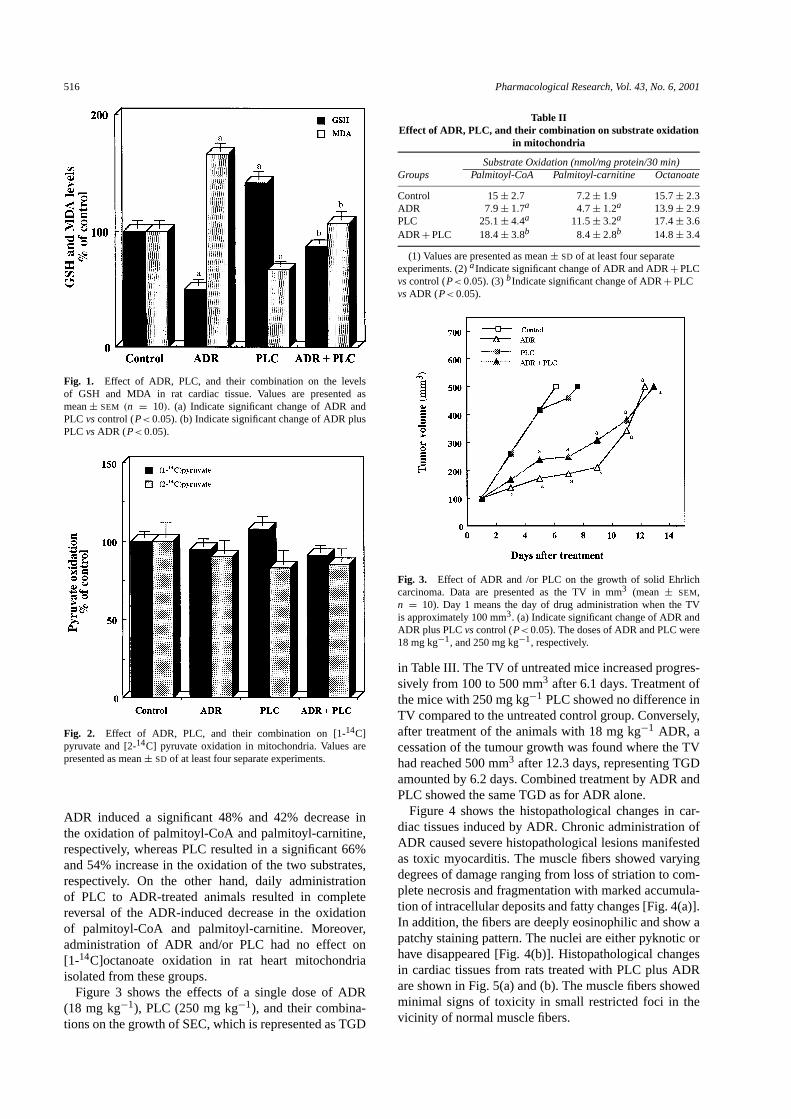
Figure1 shows the effects of 2 weeks of treatment withADR, PLC, and ADR plus PLC on MDA and GSH levelsin cardiac tissue homogenate. ADR caused a significant53% increase in MDA and a significant 50% decrease inGSH, whereas PLC induced a significant 33% decreasein MDA and a significant 41% increase in GSH levelsin cardiac tissues. Daily administration of PLC to ADR-treated rats resulted in complete recovery of the increasein MDA and the decrease in GSH induced by ADRto the normal levels. In rat heart mitochondria, ADRand/or PLC treatment showed no effect on the14CO2released from the oxidation of [1-14C]pyruvate, an indexof the pyruvate dehydrogenase (PDH) activity, and [2-14C]pyruvate, an index of the flux of acetyl-CoA throughKreb’s cycle (Fig.2).
The effects of ADR, PLC and ADR plus PLC on14CO2released from the oxidation of [1-14C]palmitoyl-CoA[an index of carnitine palmitoyltransferase I (CPT I)],[1-14C]palmitoyl-carnitine (CPT I-independent long-chainβ-oxidation substrate) and [1-14C]octanoate (CPTI-independent medium-chainβ-oxidation substrate) inisolated rat heart mitochondria are shown in TableII .
516 Pharmacological Research, Vol. 43, No. 6, 2001
Fig. 1. Effect of ADR, PLC, and their combination on the levelsof GSH and MDA in rat cardiac tissue. Values are presented asmean± SEM (n = 10). (a) Indicate significant change of ADR andPLC vscontrol (P<0.05). (b) Indicate significant change of ADR plusPLCvsADR (P<0.05).
Fig. 2. Effect of ADR, PLC, and their combination on [1-14C]pyruvate and [2-14C] pyruvate oxidation in mitochondria. Values arepresented as mean± SD of at least four separate experiments.
ADR induced a significant 48% and 42% decrease inthe oxidation of palmitoyl-CoA and palmitoyl-carnitine,respectively, whereas PLC resulted in a significant 66%and 54% increase in the oxidation of the two substrates,respectively. On the other hand, daily administrationof PLC to ADR-treated animals resulted in completereversal of the ADR-induced decrease in the oxidationof palmitoyl-CoA and palmitoyl-carnitine. Moreover,administration of ADR and/or PLC had no effect on[1-14C]octanoate oxidation in rat heart mitochondriaisolated from these groups.
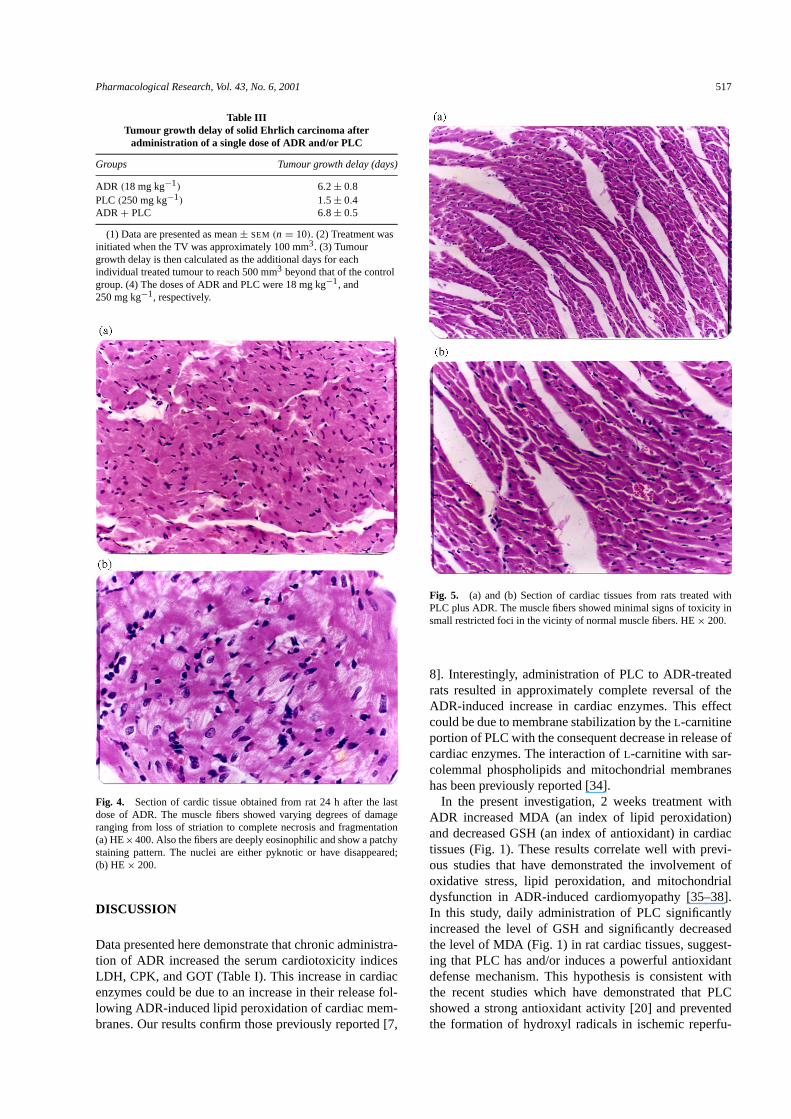
Figure 3 shows the effects of a single dose of ADR(18 mg kg−1), PLC (250 mg kg−1), and their combina-tions on the growth of SEC, which is represented as TGD
Table IIEffect of ADR, PLC, and their combination on substrate oxidation
in mitochondria
Substrate Oxidation (nmol/mg protein/30 min)Groups Palmitoyl-CoA Palmitoyl-carnitine Octanoate
Control 15± 2.7 7.2± 1.9 15.7± 2.3ADR 7.9± 1.7a 4.7± 1.2a 13.9± 2.9PLC 25.1± 4.4a 11.5± 3.2a 17.4± 3.6ADR+PLC 18.4± 3.8b 8.4± 2.8b 14.8± 3.4
(1) Values are presented as mean± SD of at least four separateexperiments. (2)aIndicate significant change of ADR and ADR+PLCvscontrol (P<0.05). (3)bIndicate significant change of ADR+PLCvsADR (P<0.05).
Fig. 3. Effect of ADR and /or PLC on the growth of solid Ehrlichcarcinoma. Data are presented as the TV in mm3 (mean± SEM,n = 10). Day 1 means the day of drug administration when the TVis approximately 100 mm3. (a) Indicate significant change of ADR andADR plus PLCvscontrol (P<0.05). The doses of ADR and PLC were18 mg kg−1, and 250 mg kg−1, respectively.
in TableIII . The TV of untreated mice increased progres-sively from 100 to 500 mm3 after 6.1 days. Treatment ofthe mice with 250 mg kg−1 PLC showed no difference inTV compared to the untreated control group. Conversely,after treatment of the animals with 18 mg kg−1 ADR, acessation of the tumour growth was found where the TVhad reached 500 mm3 after 12.3 days, representing TGDamounted by 6.2 days. Combined treatment by ADR andPLC showed the same TGD as for ADR alone.
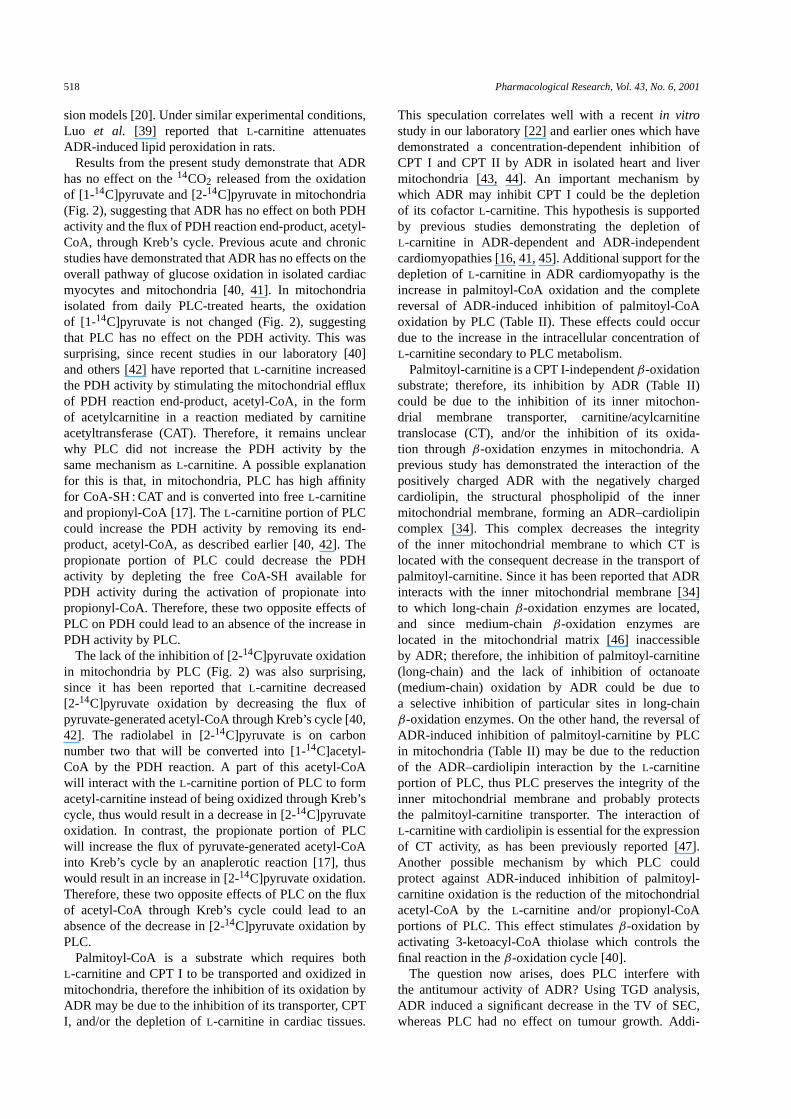
Figure 4 shows the histopathological changes in car-diac tissues induced by ADR. Chronic administration ofADR caused severe histopathological lesions manifestedas toxic myocarditis. The muscle fibers showed varyingdegrees of damage ranging from loss of striation to com-plete necrosis and fragmentation with marked accumula-tion of intracellular deposits and fatty changes [Fig.4(a)].In addition, the fibers are deeply eosinophilic and show apatchy staining pattern. The nuclei are either pyknotic orhave disappeared [Fig.4(b)]. Histopathological changesin cardiac tissues from rats treated with PLC plus ADRare shown in Fig.5(a) and (b). The muscle fibers showedminimal signs of toxicity in small restricted foci in thevicinity of normal muscle fibers.
Pharmacological Research, Vol. 43, No. 6, 2001 517
Table IIITumour growth delay of solid Ehrlich carcinoma after
administration of a single dose of ADR and/or PLC
Groups Tumour growth delay (days)
ADR (18 mg kg−1) 6.2± 0.8PLC (250 mg kg−1) 1.5± 0.4ADR + PLC 6.8± 0.5
(1) Data are presented as mean± SEM (n = 10). (2) Treatment wasinitiated when the TV was approximately 100 mm3. (3) Tumourgrowth delay is then calculated as the additional days for eachindividual treated tumour to reach 500 mm3 beyond that of the controlgroup. (4) The doses of ADR and PLC were 18 mg kg−1, and250 mg kg−1, respectively.
Fig. 4. Section of cardic tissue obtained from rat 24 h after the lastdose of ADR. The muscle fibers showed varying degrees of damageranging from loss of striation to complete necrosis and fragmentation(a) HE×400. Also the fibers are deeply eosinophilic and show a patchystaining pattern. The nuclei are either pyknotic or have disappeared;(b) HE× 200.
DISCUSSION
Data presented here demonstrate that chronic administra-tion of ADR increased the serum cardiotoxicity indicesLDH, CPK, and GOT (TableI). This increase in cardiacenzymes could be due to an increase in their release fol-lowing ADR-induced lipid peroxidation of cardiac mem-branes. Our results confirm those previously reported [7,
Fig. 5. (a) and (b) Section of cardiac tissues from rats treated withPLC plus ADR. The muscle fibers showed minimal signs of toxicity insmall restricted foci in the vicinty of normal muscle fibers. HE× 200.
8]. Interestingly, administration of PLC to ADR-treatedrats resulted in approximately complete reversal of theADR-induced increase in cardiac enzymes. This effectcould be due to membrane stabilization by theL-carnitineportion of PLC with the consequent decrease in release ofcardiac enzymes. The interaction ofL-carnitine with sar-colemmal phospholipids and mitochondrial membraneshas been previously reported [34].
In the present investigation, 2 weeks treatment withADR increased MDA (an index of lipid peroxidation)and decreased GSH (an index of antioxidant) in cardiactissues (Fig.1). These results correlate well with previ-ous studies that have demonstrated the involvement ofoxidative stress, lipid peroxidation, and mitochondrialdysfunction in ADR-induced cardiomyopathy [35–38].In this study, daily administration of PLC significantlyincreased the level of GSH and significantly decreasedthe level of MDA (Fig.1) in rat cardiac tissues, suggest-ing that PLC has and/or induces a powerful antioxidantdefense mechanism. This hypothesis is consistent withthe recent studies which have demonstrated that PLCshowed a strong antioxidant activity [20] and preventedthe formation of hydroxyl radicals in ischemic reperfu-
518 Pharmacological Research, Vol. 43, No. 6, 2001
sion models [20]. Under similar experimental conditions,Luo et al. [39] reported that L-carnitine attenuatesADR-induced lipid peroxidation in rats.
Results from the present study demonstrate that ADRhas no effect on the14CO2 released from the oxidationof [1-14C]pyruvate and [2-14C]pyruvate in mitochondria(Fig. 2), suggesting that ADR has no effect on both PDHactivity and the flux of PDH reaction end-product, acetyl-CoA, through Kreb’s cycle. Previous acute and chronicstudies have demonstrated that ADR has no effects on theoverall pathway of glucose oxidation in isolated cardiacmyocytes and mitochondria [40, 41]. In mitochondriaisolated from daily PLC-treated hearts, the oxidationof [1-14C]pyruvate is not changed (Fig.2), suggestingthat PLC has no effect on the PDH activity. This wassurprising, since recent studies in our laboratory [40]and others [42] have reported thatL-carnitine increasedthe PDH activity by stimulating the mitochondrial effluxof PDH reaction end-product, acetyl-CoA, in the formof acetylcarnitine in a reaction mediated by carnitineacetyltransferase (CAT). Therefore, it remains unclearwhy PLC did not increase the PDH activity by thesame mechanism asL-carnitine. A possible explanationfor this is that, in mitochondria, PLC has high affinityfor CoA-SH : CAT and is converted into freeL-carnitineand propionyl-CoA [17]. The L-carnitine portion of PLCcould increase the PDH activity by removing its end-product, acetyl-CoA, as described earlier [40, 42]. Thepropionate portion of PLC could decrease the PDHactivity by depleting the free CoA-SH available forPDH activity during the activation of propionate intopropionyl-CoA. Therefore, these two opposite effects ofPLC on PDH could lead to an absence of the increase inPDH activity by PLC.
The lack of the inhibition of [2-14C]pyruvate oxidationin mitochondria by PLC (Fig.2) was also surprising,since it has been reported thatL-carnitine decreased[2-14C]pyruvate oxidation by decreasing the flux ofpyruvate-generated acetyl-CoA through Kreb’s cycle [40,42]. The radiolabel in [2-14C]pyruvate is on carbonnumber two that will be converted into [1-14C]acetyl-CoA by the PDH reaction. A part of this acetyl-CoAwill interact with theL-carnitine portion of PLC to formacetyl-carnitine instead of being oxidized through Kreb’scycle, thus would result in a decrease in [2-14C]pyruvateoxidation. In contrast, the propionate portion of PLCwill increase the flux of pyruvate-generated acetyl-CoAinto Kreb’s cycle by an anaplerotic reaction [17], thuswould result in an increase in [2-14C]pyruvate oxidation.Therefore, these two opposite effects of PLC on the fluxof acetyl-CoA through Kreb’s cycle could lead to anabsence of the decrease in [2-14C]pyruvate oxidation byPLC.
Palmitoyl-CoA is a substrate which requires bothL-carnitine and CPT I to be transported and oxidized inmitochondria, therefore the inhibition of its oxidation byADR may be due to the inhibition of its transporter, CPTI, and/or the depletion ofL-carnitine in cardiac tissues.
This speculation correlates well with a recentin vitrostudy in our laboratory [22] and earlier ones which havedemonstrated a concentration-dependent inhibition ofCPT I and CPT II by ADR in isolated heart and livermitochondria [43, 44]. An important mechanism bywhich ADR may inhibit CPT I could be the depletionof its cofactorL-carnitine. This hypothesis is supportedby previous studies demonstrating the depletion ofL-carnitine in ADR-dependent and ADR-independentcardiomyopathies [16, 41, 45]. Additional support for thedepletion ofL-carnitine in ADR cardiomyopathy is theincrease in palmitoyl-CoA oxidation and the completereversal of ADR-induced inhibition of palmitoyl-CoAoxidation by PLC (TableII ). These effects could occurdue to the increase in the intracellular concentration ofL-carnitine secondary to PLC metabolism.
Palmitoyl-carnitine is a CPT I-independentβ-oxidationsubstrate; therefore, its inhibition by ADR (TableII )could be due to the inhibition of its inner mitochon-drial membrane transporter, carnitine/acylcarnitinetranslocase (CT), and/or the inhibition of its oxida-tion throughβ-oxidation enzymes in mitochondria. Aprevious study has demonstrated the interaction of thepositively charged ADR with the negatively chargedcardiolipin, the structural phospholipid of the innermitochondrial membrane, forming an ADR–cardiolipincomplex [34]. This complex decreases the integrityof the inner mitochondrial membrane to which CT islocated with the consequent decrease in the transport ofpalmitoyl-carnitine. Since it has been reported that ADRinteracts with the inner mitochondrial membrane [34]to which long-chainβ-oxidation enzymes are located,and since medium-chainβ-oxidation enzymes arelocated in the mitochondrial matrix [46] inaccessibleby ADR; therefore, the inhibition of palmitoyl-carnitine(long-chain) and the lack of inhibition of octanoate(medium-chain) oxidation by ADR could be due toa selective inhibition of particular sites in long-chainβ-oxidation enzymes. On the other hand, the reversal ofADR-induced inhibition of palmitoyl-carnitine by PLCin mitochondria (TableII ) may be due to the reductionof the ADR–cardiolipin interaction by theL-carnitineportion of PLC, thus PLC preserves the integrity of theinner mitochondrial membrane and probably protectsthe palmitoyl-carnitine transporter. The interaction ofL-carnitine with cardiolipin is essential for the expressionof CT activity, as has been previously reported [47].Another possible mechanism by which PLC couldprotect against ADR-induced inhibition of palmitoyl-carnitine oxidation is the reduction of the mitochondrialacetyl-CoA by theL-carnitine and/or propionyl-CoAportions of PLC. This effect stimulatesβ-oxidation byactivating 3-ketoacyl-CoA thiolase which controls thefinal reaction in theβ-oxidation cycle [40].
The question now arises, does PLC interfere withthe antitumour activity of ADR? Using TGD analysis,ADR induced a significant decrease in the TV of SEC,whereas PLC had no effect on tumour growth. Addi-

Pharmacological Research, Vol. 43, No. 6, 2001 519
tional administration of PLC to ADR-treated animalsshowed a similar TGD pattern as for ADR alone-treatedanimals. These results are consistent with previous stud-ies [16, 48], which have demonstrated thatL-carnitinehas no effect on the antitumour activity of ADR. Resultsfrom this study suggest that: (1) in the heart, PLC therapycompletely protects against ADR-induced inhibition ofmitochondrial β-oxidation of long-chain fatty acids;(2) PLC has and/or induces a powerful antioxidantdefense mechanism against ADR-induced lipid peroxi-dation of cardiac membranes; and finally (3) PLC has noeffect on the antitumour activity of ADR. In conclusion,these studies suggest that PLC can potentially be usedclinically as a protective agent against ADR-inducedcardiomyopathy without altering its antitumour effects.
REFERENCES
1. Arcamone F, Franceschi G, Tenco S, Selva S. Adriamycin (14-hydroxy daunorubicin), a novel antitumour antibiotic.TetrahedronLett1969;13: 1007–10.
2. Carter SK. Adriamycin—a review.J Natl Cancer Inst1975;55:1265–74.
3. Kantrowitz NE, Bristow MR. Cardiotoxicity of antitumor agents.Prog Cardiovasc Dis1984;27: 195–200.
4. Buzadar AV, Marcus C, Smith TL, Blumenschein GR. Early anddelayed clinical cardiotoxicity of doxorubicin.Cancer1985;55:2761–5.
5. Van Vleet J, Ferrans V, Weririch W. Cardiac disease induced bychronic adriamycin administration in dogs and an evaluation ofvitamin E and selenium as cardioprotectants.Am J Pathol1980;99: 13–42.
6. Lefrak EA, Pitha J, Rosenhiem J, Gotibieb JH. A clinicopatho-logical analysis of adriamycin cardiotoxicity.Cancer1973; 32:303–9.
7. Venkatesan N. Curcumin attenuation of acute adriamycin myocar-dial toxicity in rats.Br J Pharmacol1998;124:425–7.
8. Al-Shabanah O, Mansour M, El-Kashef H, Al-Bekairi A. Capto-pril ameliorates myocardial and hematological toxicities inducedby adriamycin.Biochem Mol Biol Int1998;17: 419–27.
9. Al-Harbi MM, Al-Gharably NM, Al-Shabanah OA, Al-BekairiAM, Osman AM, Tawafik HN. Prevention of doxorubicin-inducedmyocardial and haematological toxicities in rats by the ironchelator desferrioxamine.Cancer Chemother Pharmacol1992;31: 200–4.
10. Yeung TK, Jaenke RS, Wilding D, Creighton AM, Hopewell JW.The protective activity of ICRF-187 against doxorubicin-inducedcardiotoxicity in the rat.Cancer Chemother Pharmacol1992;30:58–64.
11. Rossi F, Filippelli W, Russo S, Filippelli A, Berrino L. Cardiotox-icity of doxorubicin: Effects of drugs inhibiting the release of va-soactive substances.Pharmacol Toxicol1994;75: 99–107.
12. Myers CE, Chabner BA. Anthracyclines. In:Cancer chemother-apy: principles and practice. Chabner BA, Collins JM, eds.Philadelphia: JB. Lippincott Co., 1990: 356–81.
13. Kawasaki N, Lee J, Shimizu H, Ueda T. Long-term l-carnitinetreatment prolongs the survival in rats with adriamycin-inducedheart failure.J Card Failure1996;2: 293–9.
14. Strauss M, Anselmi G, Hermoso T, Tejero F. Carnitine promotesheat shock protein in adriamycin-induced cardiomyopathy in aneonatal rat experimental model.J Mol Cell Cardiol 1998; 30:2319–25.
15. Andrieu-Abadie N, Jaffrezou J, Hatem S, Laurent G, Levade T,Mercadier J. L-carnitine prevents doxorubicin-induced apoptosisof cardiac myocytes: role of inhibition of ceramide generation.FASEB J1999;13: 1501–10.
16. Sayed-Ahmed MM, Sharawy SM, Shouman SA, Osman AM.Reversal of doxorubicin-induced cardiac metabolic damage byL-carnitine.Pharmacol Res1999;39: 289–95.
17. Paulson DJ, Traxler J, Schmidt M, Noonan J, Shug AL. Protectionof the ischemic myocardium by l-propionylcarnitine: Effects onthe recovery of cardiac output after ischemia and reperfusion,carnitine transport, and fatty acid oxidation.Cardiovasc Res1986;20: 536–41.
18. Ferrari R, De Giuli F. The propionyl-l-carnitine hypothesis: Analternative approach to treating heart failure.J Card Failure1997;3217–24.
19. Arsenian MA. Carnitine and its derivatives in cardiovasculardisease.Progress in Cardiovascular Diseases1997;40: 265–86.
20. Wiseman LR, Brogden RN. Propionyl L-carnitine.Drugs Aging1998;29: 243–8.
21. Capecchi PL, Laghi Pasini F, Quartarolo E, Di Perri T. Carnitinesincrease plasma levels of adenosine and ATP in humans.VascularMedicine1997;2: 77–81.
22. Sayed-Ahmed MM, Shouman SA, Rezk BM, Khalifa MH,Osman AM, El-Merzabani MM. Propionyl-l-carnitine as potentialprotective agent against adriamycin-induced impairment of fattyacid beta-oxidation in isolated heart mitochondria.Pharmacol Res2000;41: 143–50.
23. Neri B, Neri GC, Bandinelli M. Differences between carnitinederivatives and coenzyme Q10 in preventing in vitro doxorubicin-related cardiac damages.Oncology1988;45: 242–6.
24. Beanlands RSB, Shaikh A, Wen W, dawood F, Ugnat A,Mc Laaughlin PR, Carere R, Liu PP. Alteration in fatty acidmetabolism in adriamycin cardiomyopathy.J Mol Cell Cardiol1994;26: 109–19.
25. Gruber W. Inhibition of creatine kinase activity by Ca2+ and re-versing effect of EDTA.Clin Chem1978;24: 177–8.
26. Swanson JR, Wilkinson JH. Measurement of creatine kinase inserum. In:Standard methods of clinical chemistry, vol. 7, CooperGR, ed. New York: Academic Press, 1972: 33–42.
27. Reitman S, Frankel S. A colourimetric method for determinationof serum glutamic oxaloacetic and glutamic pyruvic transaminase.Am J Clin Pathol1967;28: 56–60.
28. Ellman GL. Tissue sulfhydryl groups.Arch Biochem Biophys1959;74: 214–8.
29. Buege JA, Aust SD. Microsomal lipid peroxidation.MethodsEnzymol1978;52: 302–6.
30. Chappel JB, Hansford RG.Subcellular components, 2nd edn.Birnie GD, ed. London: Butterworths, 1969: 77–91.
31. Yang SY, He XY, Schulz H. Fatty acid oxidation in rat brain islimited by the low activity of 3-ketoacyl-coenzyme A thiolase.JBiol Chem1987;262:13027–32.
32. Osman AM, Sayed-Ahmed MM, Khayyal MT, El-MerzabaniMM. Hyperthermic potentiation of cisplatin on solid ehrlich car-cinoma.Tumori1993;79: 268–72.
33. Bradford MM. A rapid and sensitive method for the quantita-tion of microgram quantities of protein utilizing the principleof protein-dye binding.Anal Biochem1976;72: 248–54.
34. Battelli D, Bellei M, Arrigoni-Martelli E, Muscatello U, Bobyl-eva V. Interaction of carnitine with mitochondrial cardiolipin.Biochem Biophys Acta1992;1117:33–6.
35. Singal PK, Siveski-Iliskovic N, Hill M, Thomas PT, Li T.Combination therapy with probucol prevents adriamycin-inducedcardiomyopathy.J Mol Cell Cardiol1995;27: 1055–63.
36. Van-Acker SA, Kramer K, Voest EE, Grimbergen JA, Zhang J,Van-der-viigh WJ, Bast A. Doxorubicin-induced cardiotoxicitymonitored by ECG in freely moving mice. A new model to testpotential protectors.Cancer Chemother Pharmacol1996;38: 95–101.
37. Nohl H, Gillc L, Stanick K. The exogenous NADH dehydrogenaseof heart mitochondria is the Key enzyme responsible for selectivecardiotoxicity of anthracyclines.Z Naturforsch1998;53: 279–85.
38. Yin X, Wu H, Chen Y, Kang YJ. Induction of antioxidants byadriamycin in mouse heart.Biochem Pharmacol1998;56: 87–93.
39. Luo X, Reichetzer B, Trinex J, Benson LN, Lehotay DC.L-carnitine attenuates doxorubicin-induced lipid peroxidation inrats.Free Radic Biol MedMay 1999;26: 1156–65.

520 Pharmacological Research, Vol. 43, No. 6, 2001
40. Sayed-Ahmed MM. Pharmacological and biochemical stud-ies on the mechanism(s) of adriamycin-induced cardiotoxicity.Ph.D.Thesis, Cairo University, 1995.
41. Abdel-aleem S, El-Merzabani MM, Sayed-Ahmed MM, TaylorDA, Lowe JE. Acute and chronic effects of adriamycin on fattyacid oxidation in isolated cardiac myocytes.J Mol Cell Cardiol1997;29: 789–97.
42. Abdel-aleem S, Sayed-Ahmed MM, Nada MA, Hendrickson SC,Louis JS, Walthhall HP, James EL. Regulation of fatty acidoxidation by acetyl-CoA generated from glucose utilization inisolated myocytes.J Mol Cell Cardiol1995;28: 825–33.
43. Brady LJ, Brady PS. Hepatic and cardiac carnitine palmitoyltrans-ferase activity. Effects of adriamycin and galactosamine.BiochemPharmacol1987;36: 3419–23.
44. Kashfi K, Israel M, Sweatman TW, Seahadri R, Cook GA.Inhibition of mitochondrial carnitine palmitoyltransferase by
adriamycin and adriamycin analogues.Biochem Biopharmacol1990;40: 1441–8.
45. Paulson DJ. Carnitine deficiency-induced cardiomyopathy.MolCell Biochem1998;180:33–41.
46. Nada MA, Rhead WJ, Sprecher H, Schulz H, Roe CR. Evidencefor intermediate channeling in mitochondrialβ-oxidation.J BiolChem1995;270:530–5.
47. Paradies G, Ruggiero FM, Petrosillo G, Quaglariello E. Alter-ations in carnitine/acylcarnitine translocase activity and in phos-pholipid composition in heart mitochondria from hypothyroid rats.Biochem Biophys Acta1997;1362:231–8.
48. Senekowitsch R, Lohninger A, Kriegel H, Staniek H, KrieglsteinerHB, Kaiser E. Protective effect of carnitine on adriamycin toxicityto heart. In: Carnitine—its role in lung and heart disorders.Proc Satell Symp ZAK. Graz, September 1985. Basel: Karger,1987: 126–37.
Related Documents











![Evaluation in Vitro of Adriamycin …...(CANCER RESEARCH 50. 6600-6607. October 15. 1990] Evaluation in Vitro of Adriamycin Immunoconjugates Synthesized Using an Acid-sensitive Hydrazone](https://static.cupdf.com/doc/110x72/5e8ee25f90cfc853e1716415/evaluation-in-vitro-of-adriamycin-cancer-research-50-6600-6607-october-15.jpg)