20567651.3 December 2015 1 Project Report Stanton Territorial Hospital December 2015

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

20567651.3
December 2015
1
Project Report
Stanton Territorial Hospital
December 2015
20567651.3
December 2015
2
Purpose of this project report
The purpose of this project report (“Project Report”) is to provide key information to the public about
the Stanton Territorial Hospital Renewal Project (the “Project”). This Project Report describes the need
for the Project, how it will be delivered, how different procurement delivery methods were analyzed,
and how project benefits and innovations are expected to be achieved. A summary of the key aspects of
the Project Agreement is also provided at Section 4 of this Project Report.
In all of its procurement processes, the Government of the Northwest Territories (“GNWT”) is
committed to a high standard of disclosure as part of its accountability for the delivery of public
projects. Departments, Crown Corporations and other government agencies are publicly accountable for
projects through regular budgeting, auditing and reporting processes.
GNWT is accountable for the contents of this Project Report.
Defined terms and abbreviations
Capitalized terms used in this Project Report that are not defined are set out in the Glossary of Terms at
Section 6 of this Project Report.

20567651.3
December 2015
3
Table of contents
1. EXECUTIVE SUMMARY .................................................................................................................................. 5
2. PROJECT OVERVIEW ..................................................................................................................................... 7
2.1 BACKGROUND AND OBJECTIVES ............................................................................................................................... 7
2.2 SCOPE OF THE PROJECT ......................................................................................................................................... 8
2.2.1 The new Stanton Territorial Hospital ..................................................................................................... 8
2.2.2 Existing Hospital..................................................................................................................................... 9
2.3 PROJECT BENEFITS AND KEY FEATURES .................................................................................................................... 10
3. COMPETITIVE SELECTION PROCESS ............................................................................................................. 12
3.1 REQUEST FOR QUALIFICATIONS ............................................................................................................................. 12
3.2 REQUEST FOR PROPOSALS .................................................................................................................................... 13
3.3 EVALUATION OF PROPOSALS ................................................................................................................................. 14
3.3.1 Technical submissions .......................................................................................................................... 14
3.3.2 Financial submissions ........................................................................................................................... 14
3.3.3 Overall outcome ................................................................................................................................... 15
3.4 NEW BUILD SOLUTION ......................................................................................................................................... 15
3.5 FAIRNESS ADVISOR ............................................................................................................................................. 17
4. THE FINAL PROJECT AGREEMENT ................................................................................................................ 18
4.1 OVERVIEW ........................................................................................................................................................ 18
4.2 PROFILE OF THE PRIVATE SECTOR PARTNER ............................................................................................................. 18
4.3 KEY TERMS OF THE PROJECT AGREEMENT ................................................................................................................ 19
4.3.1 New hospital ........................................................................................................................................ 19
4.3.2 Existing Hospital................................................................................................................................... 19
4.4 PERFORMANCE-BASED PAYMENT PRINCIPLES ........................................................................................................... 20
4.5 ADJUSTMENTS TO THE AVAILABILITY PAYMENTS ....................................................................................................... 20
4.6 RISK ALLOCATION SUMMARY ................................................................................................................................ 21
4.7 FINANCIAL SUMMARY .......................................................................................................................................... 23
4.8 QUANTITATIVE BENEFITS ...................................................................................................................................... 23
4.9 ACCOUNTING TREATMENT .................................................................................................................................... 24
5. ONGOING PROJECT AGREEMENT MONITORING ......................................................................................... 25
5.1 DESIGN AND CONSTRUCTION PHASE ....................................................................................................................... 25
5.2 MAINTENANCE AND REHABILITATION PHASE ............................................................................................................ 25
5.3 END OF PROJECT AGREEMENT .............................................................................................................................. 26
5.4 QUALITY MANAGEMENT THROUGHOUT THE PROJECT TERM ........................................................................................ 26
6. GLOSSARY OF TERMS .................................................................................................................................. 27
APPENDIX A – P3 PROCUREMENT PROCESS ......................................................................................................... 29
METHODOLOGY ........................................................................................................................................................... 29
PROCUREMENT OPTIONS ............................................................................................................................................... 31
RESULTS OF THE PROCUREMENT OPTIONS ANALYSIS ........................................................................................................... 32

20567651.3
December 2015
4
ACHIEVING VALUE FOR MONEY ....................................................................................................................................... 32
20567651.3
December 2015
5
1. Executive summary
Figure 1 - Preliminary rendering of the Facility
The Stanton Territorial Hospital Renewal Project is a high priority project for GNWT in order to meet
changing healthcare needs and population growth in the Northwest Territories. The Project will involve
the construction of a new facility as well as the redevelopment and repurposing of the existing hospital
building. The new facility will provide state of the art health care and diagnostic services to residents of
the Northwest Territories and surrounding regions, and is expected to meet population growth through
to 2050.
The procurement process for the Project, led by GNWT, began in June 2014 with the RFQ phase. Three
teams were shortlisted for the RFP Phase in September 2014:
Boreal Health Partnership
EllisDon Infrastructure
Plenary Health
In September 2015, following a competitive selection process based on the principles of openness,
fairness, and transparency, GNWT entered into a performance based, fixed price Project Agreement
with Boreal Health Partnership to deliver the Project. Boreal Health Partnership will design, build,
finance, operate, maintain and perform life cycle rehabilitation on the Facility for a 30 year term
following a construction period of approximately 3 years.
20567651.3
December 2015
6
The Facility will have 100 inpatient beds in single patient rooms, compared to 67 in the Existing Hospital,
as well as:
A larger and better equipped emergency department as well as more space for ambulatory care
including specialist clinics, medical day care and dialysis
Enhanced medical technology throughout the hospital to improve quality of care and clinical
efficacy
Incorporation of sustainable energy engineering practices
Boreal Health Partnership will provide a range of services during the operating period including
Housekeeping, waste management, laundry and linen, and catering services
Roads, grounds, and landscape maintenance
Parking management and security services
Customer-related services, including technical support and assistance and operation of a help
desk
Maintaining the Facility over a 30-year operating phase including routine, planned and
unplanned maintenance
Returning the Facility in a fully maintained condition at the end of the Project Agreement term.
Boreal Health Partnership will receive a monthly service payment for these services, subject to
performance standards including Facility availability and quality of service. Payments will be reduced if
Boreal Health Partnership does not meet the rigorous performance standards contained within the
Project Agreement.
The Project Agreement also contains well defined specifications regarding the quality of the Facility after
the 30 year operating term, outlining the required remaining life of various components of the Facility. If
these specifications are not met, Boreal Health Partnership will be subject to financial penalty.
The Project is estimated to achieve value for money of $174.5 million in Net Present Cost terms
compared to traditional procurement, with a significant proportion of Project risk transferred from
GNWT to Boreal Health Partnership, including construction schedule risk as well as cost and
performance risk over the operating period.
An independent external Fairness Advisor, RFP Solutions, was engaged to monitor the competitive
selection process and concluded that it was fair and impartial.
20567651.3
December 2015
7
2. Project overview
2.1 Background and objectives
The existing Stanton Territorial Hospital (the “Existing Hospital”), located in Yellowknife, Northwest
Territories, is the main hospital for the Stanton Territorial Health Authority (“STHA”). The STHA provides
acute secondary, tertiary and other specialized health care to the residents of the Northwest Territories
as well as the Kitikmeot Region of Nunavut, servicing a total population of 47,500 (Census, 2011). The
Existing Hospital offers the highest level of hospital care and diagnostic and therapeutic services
available in the Northwest Territories.
The Existing Hospital has been in service for over 26 years, constructed in 1985-1987. It is located on Lot
1, Block 162, between the Old Airport Road and Frame Lake, and consists of three floors plus a
penthouse with a building gross square meters (GSM) total of 13,300.
The need for the Project is driven by the following:
Technical renewal
o The Existing Hospital is more than 25 years old and technical renewal is considered a
necessity in order to sustain a modern, up-to-date, safe, and comfortable health care
environment
Changing healthcare needs and program renewal
o In the 25 years since the Existing Hospital was built, the nature of health care in the
Northwest Territories and Canada has changed, with advances in patient care and
medicine as well as in standards of service delivery; notably infection control and spatial
standards
o Additionally, there has been an increased focus on ambulatory care which has outpaced
the demand for inpatient beds. As such, many departments in the Existing Hospital are
ill equipped for the nature and volume of services now demanded of the facility
Population growth
o The population of the primary catchment area for the STHA, which includes the
Northwest Territories and the Kitikmeot Region of Nunavut, is expected to grow by
approximately 13% over the next 35 years
o In order to meet forecasted growth the Existing Hospital requires both larger and better
equipped facilities, capable of handling and providing for a diversity of clinical and
diagnostic needs
20567651.3
December 2015
8
2.2 Scope of the Project
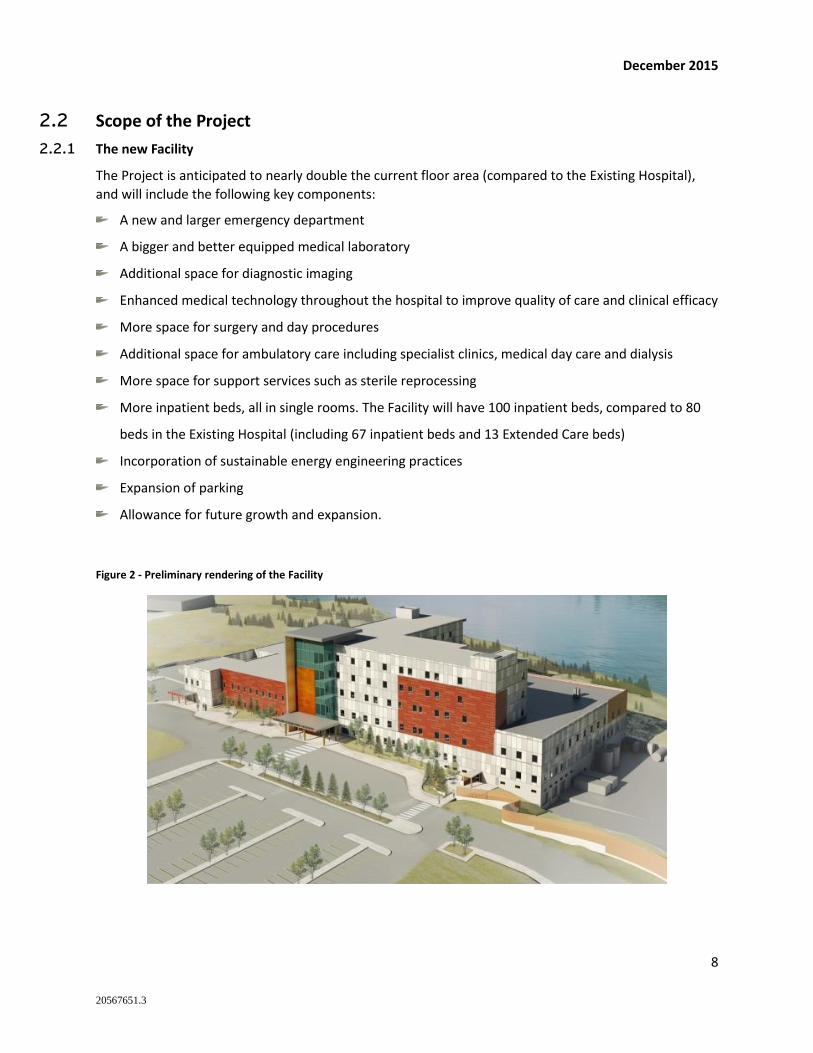
2.2.1 The new Facility
The Project is anticipated to nearly double the current floor area (compared to the Existing Hospital),
and will include the following key components:
A new and larger emergency department
A bigger and better equipped medical laboratory
Additional space for diagnostic imaging
Enhanced medical technology throughout the hospital to improve quality of care and clinical efficacy
More space for surgery and day procedures
Additional space for ambulatory care including specialist clinics, medical day care and dialysis
More space for support services such as sterile reprocessing
More inpatient beds, all in single rooms. The Facility will have 100 inpatient beds, compared to 80
beds in the Existing Hospital (including 67 inpatient beds and 13 Extended Care beds)
Incorporation of sustainable energy engineering practices
Expansion of parking
Allowance for future growth and expansion.
Figure 2 - Preliminary rendering of the Facility
20567651.3
December 2015
9
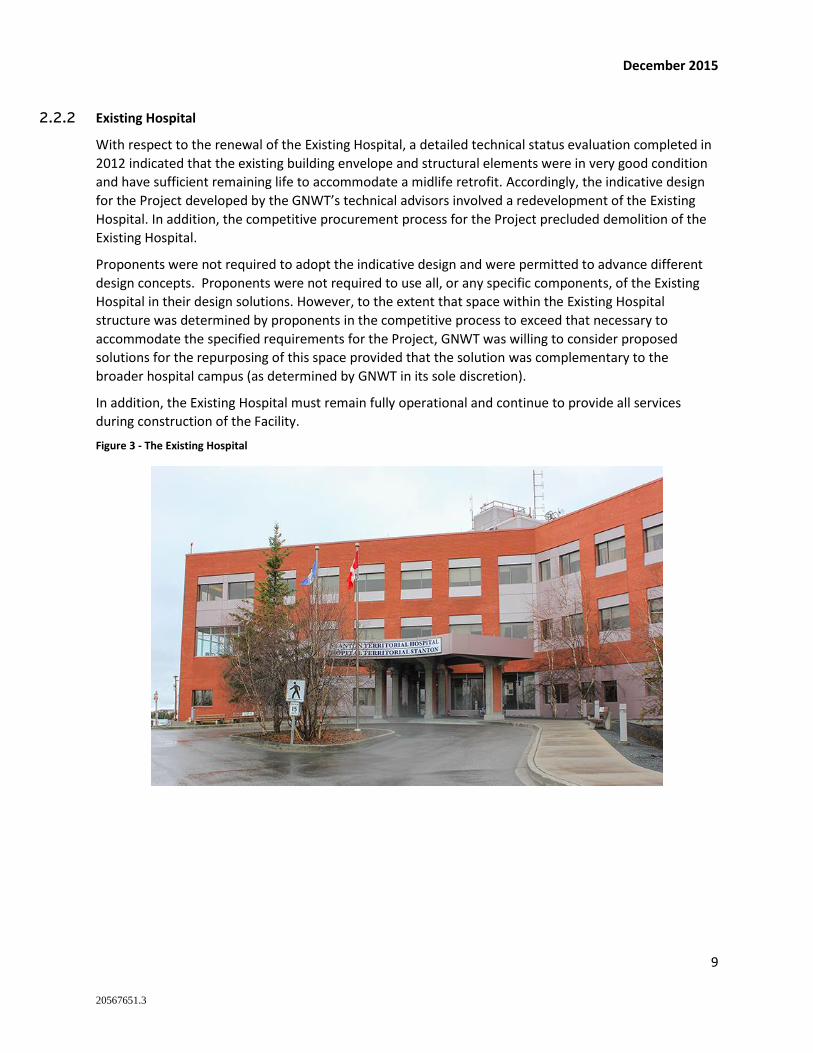
2.2.2 Existing Hospital
With respect to the renewal of the Existing Hospital, a detailed technical status evaluation completed in
2012 indicated that the existing building envelope and structural elements were in very good condition
and have sufficient remaining life to accommodate a midlife retrofit. Accordingly, the indicative design
for the Project developed by the GNWT’s technical advisors involved a redevelopment of the Existing
Hospital. In addition, the competitive procurement process for the Project precluded demolition of the
Existing Hospital.
Proponents were not required to adopt the indicative design and were permitted to advance different
design concepts. Proponents were not required to use all, or any specific components, of the Existing
Hospital in their design solutions. However, to the extent that space within the Existing Hospital
structure was determined by proponents in the competitive process to exceed that necessary to
accommodate the specified requirements for the Project, GNWT was willing to consider proposed
solutions for the repurposing of this space provided that the solution was complementary to the
broader hospital campus (as determined by GNWT in its sole discretion).
In addition, the Existing Hospital must remain fully operational and continue to provide all services
during construction of the Facility.
Figure 3 - The Existing Hospital
20567651.3
December 2015
10
2.3 Project benefits and key features
The benefits and key features of the Project include:
Improved health care facilities for residents of the Northwest Territories and Nunavut
Improved patient care and patient safety, specifically in relation to infection control, reduced
patient stay times, and improved patient satisfaction
Increased staff satisfaction and effectiveness while decreasing staff injuries and stress
Implementation of current health care standards and current health management systems
Creation of new and expanded care spaces to match increased service demands
Reduction of energy demands on the local infrastructure
The benefits listed above are anticipated to be achieved through:
Construction of a new, stand-alone facility
Incorporation of:
o single patient, safe, secure rooms
o acuity-adaptable rooms, sufficient numbers of bariatric, airborne infection rooms (AIR) and
o access to natural light and green space
o LEAN design principles that lead to an efficient design that maximizes clinical operations
o a quality acoustic environment and effective ventilation systems
o improved work settings with better floor layouts, appropriate lighting, and effective
ergonomics
Integration of Shared Support Services
Use of a Clinical Information System
Improved data networking and systems for tele-health capabilities
Incorporation of sustainable energy sources, including the use of a biomass boiler plant

20567651.3
December 2015
11
Figure 4 - Preliminary rendering of the Facility

20567651.3
December 2015
12
3. Competitive Selection Process
In accordance with GNWT’s P3 Management Framework1, GNWT undertook a procurement options
analysis to determine an optimal procurement method for the Project. Thorough and robust qualitative
and quantitative analyses resulted in the P3 method in the form of Design Build Finance Maintain
contract being the most beneficial method for delivering the Project. Further discussion of the
procurement options analysis undertaken is provided in Appendix A.
The procurement followed a rigorous, competitive, open, transparent and fair process. A two-step
process based on Canadian best-practice precedent was undertaken, entailing a Request for
Qualifications (RFQ) phase and a Request for Proposals (RFP) phase. These phases are described further
below.
3.1 Request for Qualifications
The release of the RFQ initiated the procurement phase of the Project by inviting interested teams to
indicate their interest in the Project through submission of an RFQ response. The RFQ was issued on
June 25, 2014, with three teams making submissions. The evaluation considered each team’s financial
capacity to undertake the Project and their technical experience of delivering projects of a similar scope
and size. All three teams were evaluated in accordance with the evaluation process by the evaluation
committee which included representatives from Stanton Territorial Health Authority, the Department of
Finance, Department of Procurement and Shared Services as well as external expert advisors. The three
teams were shortlisted for the RFP stage.
Table 1 - Short-listed Proponent Teams
Name Design Construction Financing
(Equity and Debt)
Facilities
Management
Boreal Health
Partnership
Kasian
Architecture
Interior Design
Planning Ltd.
Bird Design-Build
Construction Inc.
Clark Builders Ltd.
Equity Carillion Private
Finance Ltd
Hochtief PPP
Solutions GMBH
Bird Capital LP
Debt
CIBC World Markets
Inc.
Carillion Canada
Inc.
1 GNWT P3 Management Framework dated 11/5/2012
20567651.3
December 2015
13
Name Design Construction Financing
(Equity and Debt)
Facilities
Management
EllisDon
Infrastructure
Parkin Architects
Limited
EllisDon Design-
Build Inc. Equity EllisDon Capital
Ontario Pension
Board
Debt TD Securities Inc.
Cofely Services Inc.
EllisDon Facility
Services Inc.
Plenary Health B+H Architects PCL Constructors
Northern Inc. Equity PCL Investments
Canada Inc.
Plenary Group
(Canada) Ltd.
Debt Manufacturers Life
Insurance
Company
Johnson Controls
Canada LP
Compass Group
Canada Ltd.
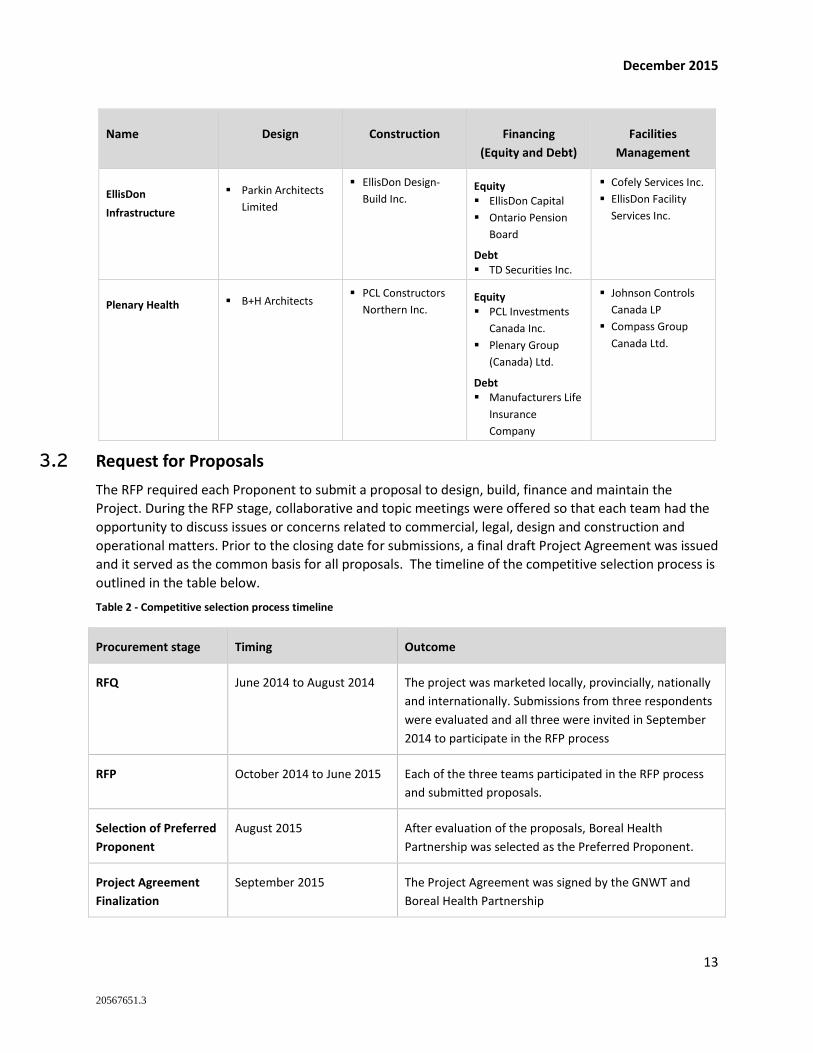
3.2 Request for Proposals
The RFP required each Proponent to submit a proposal to design, build, finance and maintain the
Project. During the RFP stage, collaborative and topic meetings were offered so that each team had the
opportunity to discuss issues or concerns related to commercial, legal, design and construction and
operational matters. Prior to the closing date for submissions, a final draft Project Agreement was issued
and it served as the common basis for all proposals. The timeline of the competitive selection process is
outlined in the table below.
Table 2 - Competitive selection process timeline
Procurement stage Timing Outcome
RFQ June 2014 to August 2014 The project was marketed locally, provincially, nationally
and internationally. Submissions from three respondents
were evaluated and all three were invited in September
2014 to participate in the RFP process
RFP October 2014 to June 2015 Each of the three teams participated in the RFP process
and submitted proposals.
Selection of Preferred
Proponent
August 2015 After evaluation of the proposals, Boreal Health
Partnership was selected as the Preferred Proponent.
Project Agreement
Finalization
September 2015 The Project Agreement was signed by the GNWT and
Boreal Health Partnership
20567651.3
December 2015
14
3.3 Evaluation of proposals
Proponents were required to submit technical and financial submissions as part of the RFP process. The
overall objective of the evaluation was to select the proposal that best met the requirements of the RFP
and achieved value for money. An evaluation committee was appointed to evaluate the proposals based
on the criteria set out in the RFP and to recommend a Preferred Proponent.
3.3.1 Technical submissions
Evaluation of technical submissions was completed in two stages:
1. evaluation of Initial Technical Submissions (“ITS”)
2. evaluation of Final Technical Submissions (“FTS”), submitted approximately 7 weeks after the
ITS.
The purpose of having both an Initial and Final Technical Submission was to reduce the potential for
proponents to be disqualified for non-compliance with the requirements of the RFP. The evaluation
committee first reviewed each proponent’s ITS to identify any areas of material non-compliance.
Proponents received feedback in respect of any related issues in advance of submitting their FTS, and
were allowed to make changes to address these issues subject to prior approval by GNWT.
Scoring in accordance with an Evaluation Framework was undertaken on the technical submissions, and
was divided across the following categories:
The proposed design and technical solution
Construction period work plans
Services and communications
Local and Northern content
Following proponents’ submission of the FTS, the evaluation committee determined whether these
submissions contained any material non-compliances and whether they satisfied the mandatory
requirements of the RFP and the Project Agreement.
3.3.2 Financial submissions
Proponents were required to submit a financial submission along with their FTS. The evaluation of the
financial submissions consisted of two steps:
The first step was to determine whether they substantially satisfied the financial requirements,
which included overall financial viability of the proponent team and the provision of sufficient
financing and a robust and deliverable financial plan.
If the Proponent satisfied all criteria in the first step above, the Net Present Cost (“NPC”) was
evaluated. NPC represents the sum of total payments made by GNWT to the Proponent over
the construction and operations terms discounted to today’s dollars. Proponents were assigned
a score based on their NPC.
20567651.3
December 2015
15
Affordability threshold
In addition to the evaluation criteria described above, the RFP included an affordability threshold
relating to capital costs included in financial submissions. This criterion sought to ensure that GNWT
received affordable proposals in the context of the available budget for the Project. This threshold was
set at $290 million in nominal terms, and captured all development, construction and commissioning
costs (including interest costs and financing fees). The threshold was not a mandatory requirement
linked to formal submission compliance, but submitting capital costs above the threshold did provide
GNWT with the discretion under the RFP to disqualify the submission.
The successful proposal from Boreal Health Partnership met the affordability threshold and will deliver
the Project scope as outlined in the Project Agreement.
3.3.3 Overall outcome
As a result of the final scoring from the FTS and financial submissions, it was determined that Boreal
Health Partnership had the highest overall score. Therefore the evaluation committee recommended
that Boreal Health Partnership be selected as the Preferred Proponent, and the Financial Management
Board accepted that recommendation.
3.4 New build solution
As discussed in Section 2.2, GNWT had prepared an indicative design for the Project that involved the
renovation and expansion of the Existing Hospital. Proponents were not required to adopt the
indicative design and were permitted to advance different design concepts. Proponents were not
required to use all, or any specific components, of the Existing Hospital in their design solutions.
However, components of the Existing Hospital which were not used for STHA purposes could not be
abandoned or demolished, but must be used and maintained in a manner permitted by the RFP.
Boreal Health Partnership’s successful proposal involved the development of a new stand-alone facility
to satisfy the requirements of STHA under the Project Agreement, and the repurposing of the Existing
Hospital to accommodate commercial tenancies (to the extent that the tenancies are complementary to
the hospital campus in GNWT’s sole discretion).
The proposed arrangement included:
Boreal Health Partnership and a third party developer jointly funding the initial remediation
work for the Existing Hospital, as well as providing additional funding to build out the Existing
Hospital to tenancy requirements pursuant to a business plan acceptable to GNWT
The developer bearing the risk associated with the occupancy, energy consumption and
operational and capital maintenance of the repurposed Existing Hospital throughout a 30 year
lease term. The developer is also responsible for the condition of the Existing Hospital upon
hand back to GNWT
GNWT sharing in the net commercial revenues generated by the repurposed Existing Hospital
(the evaluation of financial submissions did not reflect any potential future upside to GNWT).
The evaluation committee determined that:
the overall solution was compliant with the terms of the RFP and the Project Agreement;

20567651.3
December 2015
16
the key ownership, operation, tenancy, financial and lifecycle risks of the Existing Facility had
been transferred to Boreal Heath Partnership and a third party developer; and
GNWT had a realistic prospect of value capture through revenue sharing under the lease,
without retaining any economic downside risks (the evaluation of financial submissions did not
allocate any financial benefit or selection advantage to this potential economic benefit).

20567651.3
December 2015
17
3.5 Fairness Advisor
A Fairness Advisor, RFP Solutions, was engaged by GNWT to monitor the competitive selection process
and offer an assessment about the procedures and whether or not the competitive selection process
was carried out in a fair and reasonable manner.
The Fairness Advisor was provided access to all documents, meetings, and information related to the
evaluation processes throughout the RFQ and RFP stages. The Fairness Advisor issued reports to GNWT
for both the RFQ and RFP stages of the competitive selection process. The reports issued by the
Fairness Advisor concluded that the Evaluation Committee selected and recommended a Preferred
Proponent in accordance with the procurement process and evaluation criteria set out in the RFP. The
Evaluation Teams and Evaluation Committee acted in a professional and impartial manner while
reviewing the proposals of each Proponent.
Overall, the procurement process was followed in accordance with the terms of the RFQ and RFP and
appeared to be fair, transparent and unbiased. The final Fairness Advisor’s report has been released
publicly along with this Project Report.
20567651.3
December 2015
18
4. The Final Project Agreement
4.1 Overview
Private partner Boreal Health Partnership
Owner Government of the Northwest Territories
Government contributions to capital cost $152 million progress payments during construction
Construction complete 31 October 2018
Term of the Project Agreement 30 year operating term plus 38 months of construction
Total Availability Payments over the
operating term of the Project
$598.4 million
4.2 Profile of the Private Sector Partner
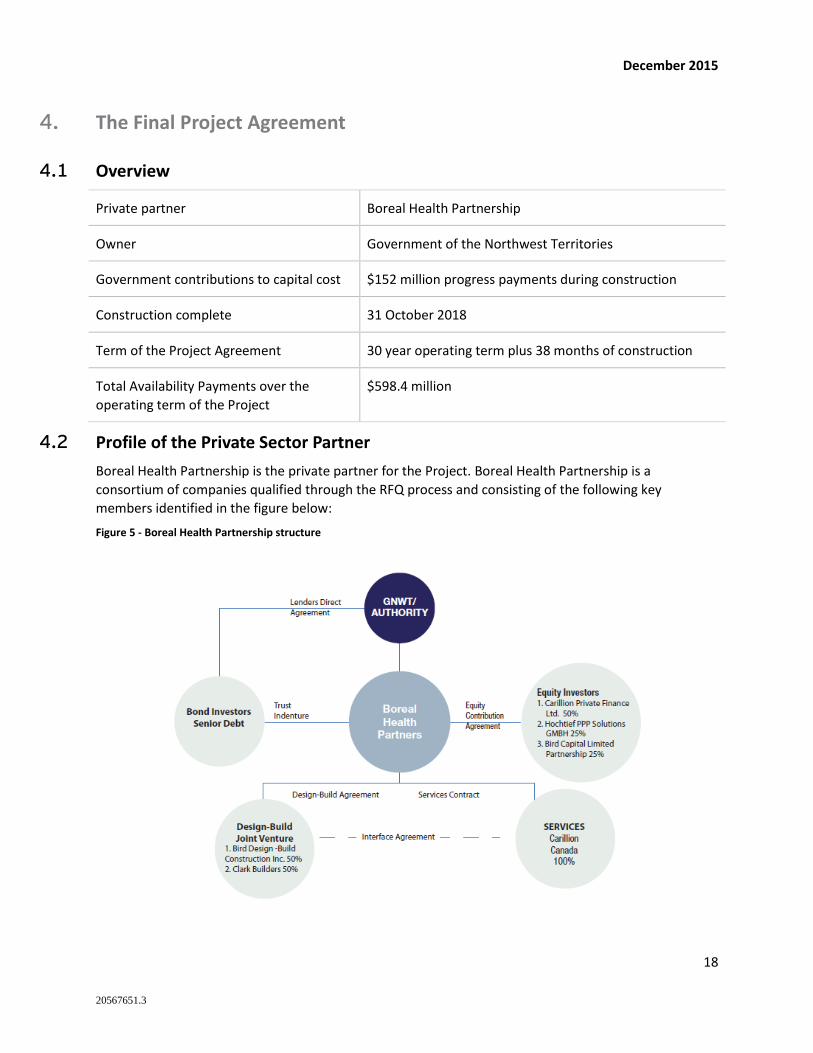
Boreal Health Partnership is the private partner for the Project. Boreal Health Partnership is a
consortium of companies qualified through the RFQ process and consisting of the following key
members identified in the figure below:
Figure 5 - Boreal Health Partnership structure
20567651.3
December 2015
19
4.3 Key terms of the Project Agreement
4.3.1 New Facility
Under the terms of the Project Agreement, Boreal Health Partnership is responsible for the following:
Construction Phase:
Arranging financing for the full construction cost of the Facility, with GNWT contributing $152
million during the period
Achieving required permits and approvals to commence construction
Designing and building the Facility within the specified and agreed timeline.
Operations Phase:
Housekeeping, waste management, laundry and linen, and catering services
Roads, grounds, and landscape maintenance
Parking management and security services
Customer-related services, including technical support and assistance and operation of a help
desk
Maintaining the Facility over a 30-year operating phase including routine, planned and
unplanned maintenance
Returning the Facility in a fully maintained condition at the end of the Project Agreement term.
4.3.2 Existing Hospital
As a companion contract to the Project Agreement, GNWT required Boreal Health Partnership and a
third party developer to enter into an Existing Hospital Remediation Agreement (the “Tripartite
Agreement”). The Tripartite Agreement includes terms requiring Boreal Health Partnership and the
developer to provide approximately $13 million of funding for undertaking a remediation of the Existing
Hospital, including removing any hazardous materials (which will be carried out by Boreal Health
Partnership) and completing certain renovation work (which will be carried out by the developer under
the Lease Agreement).
GNWT has entered into an Agreement to Lease with the developer, which contemplates that GNWT and
the developer will negotiate and enter into a Lease Agreement for the future development and use of
the Existing Hospital. Upon the completion of remediation work by Boreal Health Partnership at the
Existing Hospital, including removing any hazardous materials as set out in the Tripartite Agreement, the
Existing Facility will be leased to the developer. The Lease Agreement will more fully set out the
obligations of the developer to fund and carry out the renovation work required after handover to build
out the Existing Hospital to tenant requirements and pursuant to an acceptable business plan. Under the
terms of the Lease Agreement, the developer will assume occupancy, operational and capital
maintenance, energy and hand back risks associated with the Existing Hospital during the 30 year lease
term, and will share with GNWT the net commercial revenues generated by the Existing Hospital.

20567651.3
December 2015
20
4.4 Performance-based payment principles
During construction, GNWT will make construction payments based on a percentage of the eligible
construction costs incurred by Boreal Health Partnership in a specific month as certified by an
Independent Certifier2.
Boreal Health Partnership is incentivized to perform through a payment mechanism based on the
principles of performance, Facility availability and service quality. Once construction is complete and
Service Commencement has been achieved (the requirements of which are set out in the Project
Agreement), Boreal Health Partnership will begin receiving an Availability Payments from GNWT. These
payments will be made monthly and are based on the Facility availability and the quality of Facility
maintenance services provided by Boreal Health Partnership. Performance will be continuously
monitored based on key performance indicators. If the performance standards in the Project Agreement
are not met, GNWT may apply deductions to the Availability Payments.
Payment deductions are based on the severity of the failure to meet the performance indicator, the
importance of the room or department area affected, and the level of unavailability. An unavailability
deduction applies when a functional unit (room or department) fails to comply with the condition
specified in the Project Agreement. For example, if the temperature or humidity of a room is outside a
predetermined range, that room would be considered unavailable.
4.5 Adjustments to the Availability Payments
The Availability Payments may be adjusted according to the specific terms stated in the Project
Agreement, specifically:
Indexation: A proportion of the Availability Payment that will be adjusted for consumer price
index (CPI) on an annual basis, intended to reflect the proportion of index-linked operating
period costs relative to the overall cost base of the Contractor
Changes: In cases when GNWT requires changes to the physical infrastructure of the Facility or
the scope of services, GNWT will directly reimburse Boreal Health Partnership for the costs of
amendments either through a lump sum payment or a change to the Availability Payment
Change in Law: Under certain circumstances, GNWT may compensate Boreal Health Partnership
for changes in laws that cause them to incur additional costs
Market Testing: The housekeeping, janitorial, security, and catering services will be market
tested every six years
Compensation Events: The Project Agreement defines certain events, typically outside of Boreal
Health Partnership’s reasonable ability to control or mitigate impacts, where they are provided
the compensation to leave them in a no-better and no-worse position, potentially involving an
adjustment to Availability Payments.
2 The Independent Certifier is selected through a competitive tendering process and jointly funded by GNWT (50%) and Boreal
Health Partnership (50%) to provide independent oversight and monitoring of construction progress and quality
20567651.3
December 2015
21
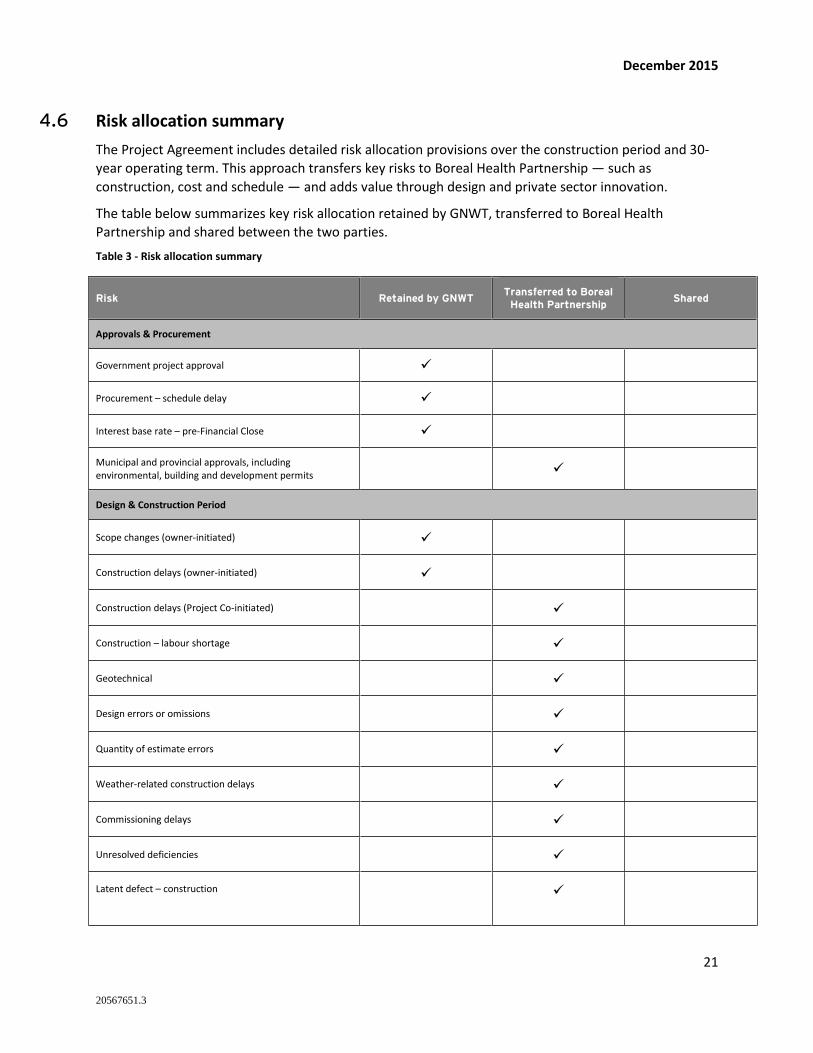
4.6 Risk allocation summary
The Project Agreement includes detailed risk allocation provisions over the construction period and 30-
year operating term. This approach transfers key risks to Boreal Health Partnership — such as
construction, cost and schedule — and adds value through design and private sector innovation.
The table below summarizes key risk allocation retained by GNWT, transferred to Boreal Health
Partnership and shared between the two parties.
Table 3 - Risk allocation summary
Risk Retained by GNWT Transferred to Boreal
Health Partnership Shared
Approvals & Procurement
Government project approval
Procurement – schedule delay
Interest base rate – pre-Financial Close
Municipal and provincial approvals, including environmental, building and development permits
Design & Construction Period
Scope changes (owner-initiated)
Construction delays (owner-initiated)
Construction delays (Project Co-initiated)
Construction – labour shortage
Geotechnical
Design errors or omissions
Quantity of estimate errors
Weather-related construction delays
Commissioning delays
Unresolved deficiencies
Latent defect – construction

20567651.3
December 2015
22
Risk Retained by GNWT Transferred to Boreal
Health Partnership Shared
Maintenance Period
Inaccurate measurement of asset expected life
Facility maintenance costs
Life Cycle (excluding IMIT components)
Life Cycle (IMIT components only)
Supervening Events
Change in Law
Force Majeure
Furthermore, following Substantial Completion of the new Facility and STHA completing the process of
decanting from the Existing Hospital into the new Facility, the third party developer of will thereafter
assume the following risks related to the Existing Hospital:
Capital, operating (including energy) and lifecycle expenditures
Tenancy / occupancy risks
Hand-back of the Existing Hospital in a prescribed condition
20567651.3
December 2015
23
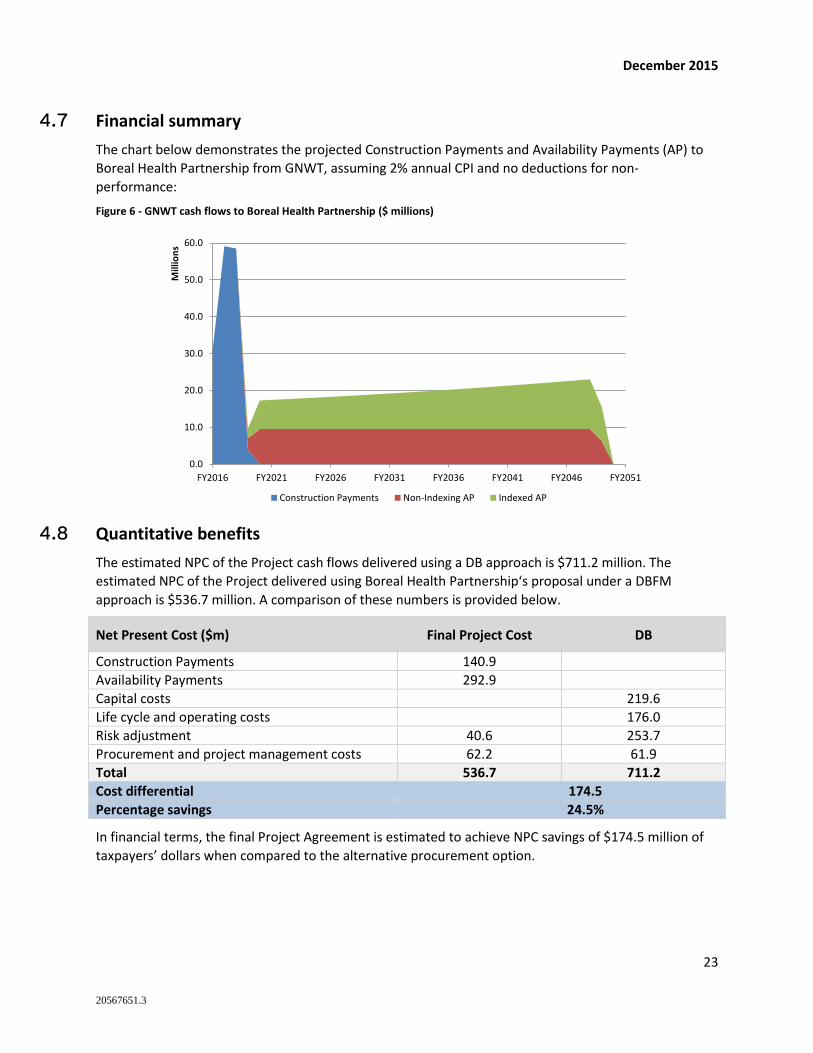
4.7 Financial summary
The chart below demonstrates the projected Construction Payments and Availability Payments (AP) to
Boreal Health Partnership from GNWT, assuming 2% annual CPI and no deductions for non-
performance:
Figure 6 - GNWT cash flows to Boreal Health Partnership ($ millions)
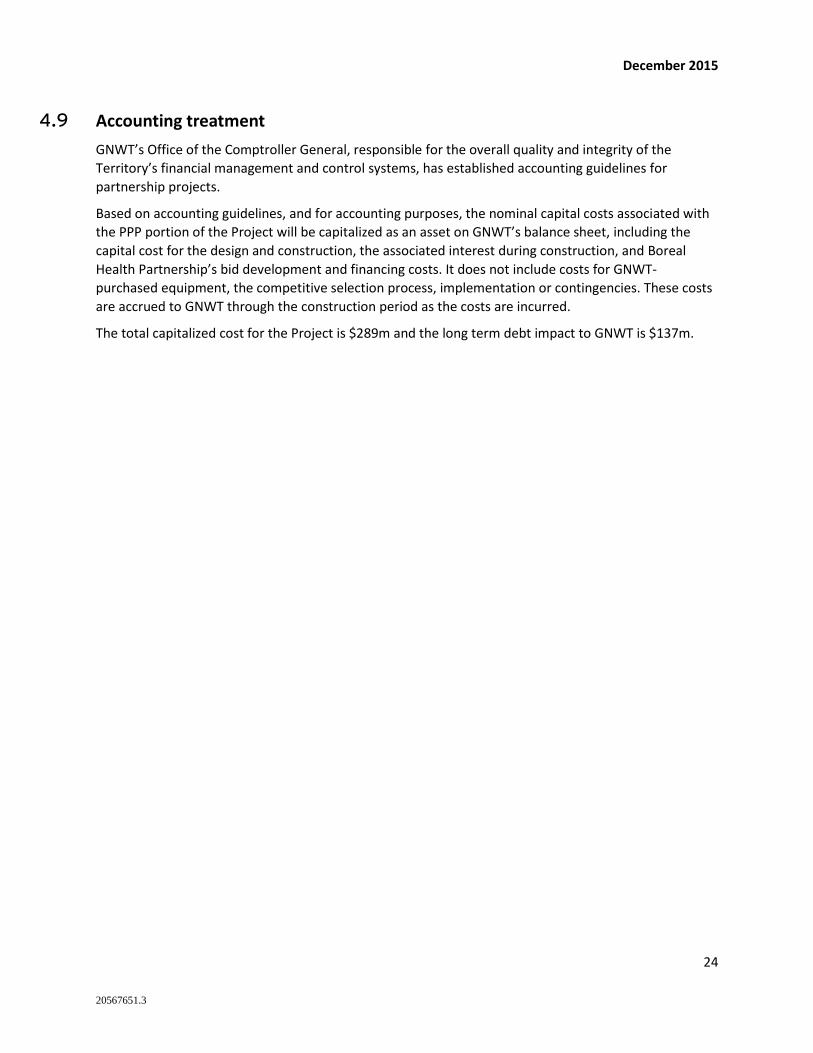
4.8 Quantitative benefits
The estimated NPC of the Project cash flows delivered using a DB approach is $711.2 million. The
estimated NPC of the Project delivered using Boreal Health Partnership‘s proposal under a DBFM
approach is $536.7 million. A comparison of these numbers is provided below.
Net Present Cost ($m) Final Project Cost DB
Construction Payments 140.9
Availability Payments 292.9
Capital costs 219.6
Life cycle and operating costs 176.0
Risk adjustment 40.6 253.7
Procurement and project management costs 62.2 61.9
Total 536.7 711.2
Cost differential 174.5
Percentage savings 24.5%
In financial terms, the final Project Agreement is estimated to achieve NPC savings of $174.5 million of
taxpayers’ dollars when compared to the alternative procurement option.
0.0
10.0
20.0
30.0
40.0
50.0
60.0
FY2016 FY2021 FY2026 FY2031 FY2036 FY2041 FY2046 FY2051
Mill
ion
s
Construction Payments Non-Indexing AP Indexed AP
20567651.3
December 2015
24
4.9 Accounting treatment
GNWT’s Office of the Comptroller General, responsible for the overall quality and integrity of the
Territory’s financial management and control systems, has established accounting guidelines for
partnership projects.
Based on accounting guidelines, and for accounting purposes, the nominal capital costs associated with
the PPP portion of the Project will be capitalized as an asset on GNWT’s balance sheet, including the
capital cost for the design and construction, the associated interest during construction, and Boreal
Health Partnership’s bid development and financing costs. It does not include costs for GNWT-
purchased equipment, the competitive selection process, implementation or contingencies. These costs
are accrued to GNWT through the construction period as the costs are incurred.
The total capitalized cost for the Project is $289m and the long term debt impact to GNWT is $137m.
20567651.3
December 2015
25
5. Ongoing Project Agreement monitoring
The Project Agreement with Boreal Health Partnership includes specific provisions to ensure project
delivery, performance and quality standards are met. Monitoring spans every phase of the Project, from
Financial Close through to design and construction, and maintenance.
There are a number of major phases in the project monitoring schedule, with roles and responsibilities
assigned to project participants at each stage.
5.1 Design and construction phase
The Project Agreement specifies monitoring mechanisms to ensure the timeliness of the Facility
completion and the quality of the construction:
During design and construction the Independent Certifier is responsible for reviewing and
monitoring construction progress and quality, as well as reviewing invoices for proposed design
changes.
In addition, at substantial completion, the Independent Certifier issues a certificate of
completion once Boreal Health Partnership has met the design and construction requirements
set out in the Project Agreement.
Boreal Health Partnership’s lenders will also review performance during the construction period.
The Construction Period Joint Committee oversees the construction of the Facility. The
committee comprises GNWT and Boreal Health Partnership design and construction
representatives. These key individuals will have the authority to act on each party’s behalf in the
matters of review, approval, confirmation and acceptance of design and construction issues. The
GNWT representative will be supported by a team of professionals and will have full access to
the construction site, design specifications and drawings. The GNWT representative will monitor
the construction and will report to GNWT regularly.
5.2 Maintenance and rehabilitation phase
Similarly to the design and construction phase, the Project Agreement provides service monitoring
protocols during the maintenance phase:
The Operating Period Joint Committee provides oversight and direction on matters related to
the maintenance and rehabilitation period. Both GNWT and Boreal Health Partnership will
appoint representatives. The role and authority of such representatives will be similar to the
representatives during the design and construction phase.
GNWT will perform inspections and testing to check reports and ensure the requirements
continue to be met.
Boreal Health Partnership’s lenders will also review performance during the maintenance and
rehabilitation period.
Boreal Health Partnership will provide various plans for GNWT’s review and approval, such as:
• Annual service plan and five year maintenance plan
20567651.3
December 2015
26
• Life cycle asset and rehabilitation plan
• Environment management plan
• Energy management plan
• Handback works plan
5.3 End of Project Agreement
At the end of the 30-year maintenance and rehabilitation period, the condition of the Facility must be in
compliance with the specifications in the Project Agreement. For example, the Facility’s structural
elements (walls, roofs, and floors) must have a minimum residual life expectancy of 30 years. As part of
the handback process, the following monitoring activities will take place:
GNWT and Boreal Health Partnership will undertake a number of activities to assess the
condition of the Facility prior to Project Agreement expiry. This assessment will ensure the asset
is in the condition specified in the Project Agreement prior to handback. Financial penalties will
be applied if the asset is not delivered to GNWT in the specified condition.
The compliance with handback requirements will be assessed by an independent qualified party,
similar to the Independent Certifier discussed in Section 5.1.
After the Project Agreement expires, GNWT will assume responsibility for maintaining the
Facility.
Under the terms of the Lease Agreement, upon expiry the developer must also return the Existing
Hospital to GNWT in a prescribed condition.
5.4 Quality management throughout the Project term
The performance-based structure of the Availability Payments creates an incentive for Boreal Health
Partnership to construct and maintain the Facility to the high standards described in the Project
Agreement. To enforce the performance standards and the above-mentioned structure, the Project
Agreement includes a performance monitoring plan. This plan is based on various types of service
performance reports delivered at different time intervals (monthly, quarterly, annually, etc) to GNWT by
Boreal Health Partnership, such as:
A summary of calls made to the facilities management help desk and their resolution
A summary of unavailability events and service failures, including resolution times
A calculation of the monthly Availability Payments owed to Boreal Health Partnership
The reports and underlying data are produced by Boreal Health Partnership, available to GNWT at the
scheduled reporting times, allow for a thorough review of provided services and performance. The
performance monitoring program ensures that the Facility is operated and maintained according to the
high standards stated in the Project Agreement. The Project Agreement contains strict penalties for
delay in provision or misrepresentation of data in the reports.
20567651.3
December 2015
27
6. Glossary of terms
Availability Payment The mechanism by which a private partner in a PPP arrangement is compensated.
According to performance standards specified in a Project Agreement, Availability
Payments are paid to the private partner for capital and operating costs, as well as
their required rate of return, over the term of the agreement
Discount Rate A rate used to relate present and future dollars. Discount rates are expressed as a
percentage and are used to reduce the value of future dollars in relation to present
dollars. This equalizes varying streams of costs and benefits so that different
alternatives can be compared on a like-for-like basis
Existing Hospital The existing hospital building and related structures, utility connections, and
landscaping present on the Existing Hospital lands
Facility The new Stanton Territorial Hospital that is to be constructed pursuant to the
Project Agreement
Financial Close The point in the procurement process where negotiations with a preferred
proponent are finalized, the lending requirements have been fulfilled and a Project
Agreement is executed, allowing construction to begin
GNWT Government of the Northwest Territories
Independent Certifier An independent, third-party certifier engaged jointly by the GNWT and the private
partner to verify and certify whether certain conditions of the Project Agreement
are being satisfied
Net Present Cost (NPC) The value of periodic future cost outlays when they are expressed in current, or
present day, dollars by discounting them using the Discount Rate.
Nominal Cost Costs calculated in nominal terms at current prices recognizing adjustments for
inflation
Performance
Specification
Specifications developed by GNWT that define the output and performance levels
required in relation to construction and life cycle performance of an asset, to
ensure the completed project satisfies the objectives of a project with respect to
meeting the GNWT’s service delivery needs
Preferred Proponent A proponent selected from a shortlist of bidders to enter into negotiations with
GNWT to reach Financial Close and deliver a project.
Project Stanton Territorial Hospital Renewal Project
20567651.3
December 2015
28
Project Agreement The Project Agreement sets out the requirements for the delivery of an asset
under a PPP in terms of cost, schedule and life cycle performance that typically
govern the performance-based payment of the ASP to a private partner.
Public Private
Partnership (PPP)
A project structured using a long-term, performance-based agreement with a
private sector partner to deliver and maintain an infrastructure asset, including
significant upfront capital investment
Request for Proposals
(RFP)
Document issued by GNWT for qualified proponents to submit formal proposals to
deliver a project
Request for
Qualifications (RFQ)
Document issued by GNWT inviting parties interested in participating in an RFP, to
submit their qualifications for delivering a project
Retained Risk Risks associated with delivering a project that are not transferred to the private
partner under a PPP, representing a cost to the project regardless of the
procurement approach
Service
Commencement
The date upon which the following activities have been achieved: the Independent
Certifier has issued a Certificate of Service Commencement with respect to the
Project; all necessary Permits have been issued for the use and operation of the
Facility; and Project Co has delivered to GNWT a report from the commissioning
agent retained by Project Co in accordance with the Project Agreement confirming
completion of all commissioning activities scheduled in the Commissioning Plan to
be completed before Service Commencement.
Traditional
Procurement
Methods by which the public sector has traditionally procured projects in the
Northwest Territories, through design bid build (DBB), design build (DB) contracts
or a combination of DBB and DB contracts
Transferred Risk Risk associated with delivering a project that is typically borne by the public sector
under traditional procurement that is transferred to the private sector under a PPP
Value for Money (VFM) Describes the benefits to the public expected to be realized through a particular
procurement method, which can be quantitative and/or qualitative in nature.
Quantitative value for money is achieved through the lower cost of a project
resulting from the procurement method, whereas qualitative value is achieved
when a particular procurement method better supports the goals and objectives of
a project without necessarily costing less.
20567651.3
December 2015
29
Appendix A – P3 Procurement Process
In accordance with GNWT’s P3 Management Framework3, GNWT undertook a procurement options
analysis to determine an optimal procurement method for the Project.
Methodology
The evaluation of procurement options is mainly concerned with identifying the method of delivering
the Project that will result in the greatest value for money on both a financial (quantitative) and
qualitative basis. The evaluation of procurement options involves two main steps:
The first step identifies key procurement objectives, against which a wide range of available
procurement options are compared, including both traditional and partnership methods, and
provides a qualitative assessment these options. This step is intended to identify the two
procurement methods most relevant to the project, which then form the basis of detailed
quantitative comparison
The second step in the assessment involves a more detailed, quantitative analysis that compares the
two methods
Multi Criteria Analysis was used to qualitatively assess a wide spectrum of potential procurement
options, including Design-Bid-Build, Design-Build, Design-Build-Finance, Design-Build-Finance-Maintain
and Design-Build-Finance-Operate-Maintain, for their alignment with the goals and objectives of the
Project. The Multi Criteria Analysis indicated that the DBFM procurement option was most closely
aligned with the criteria. Quantitative analysis was then undertaken to review whether DBFM would
provide VFM when compared to the DB procurement route which had traditionally been used to
procure projects of this nature by GNWT.
A VFM assessment was therefore completed to compare the life-cycle risk-adjusted costs of the two
selected procurement options: traditional DB and DBFM. The purpose of the VFM assessment was to
identify the procurement option that would provide the greatest value through the design, construction
and operations, maintenance and rehabilitation phases of the project. A financial model was developed
to compare which approach generated the greatest VFM.
The VFM assessment process included a comprehensive risk analysis to identify and quantify the risks
retained by the public sector under each procurement option. Other costs were also incorporated
including: design, construction, maintenance, and rehabilitation related costs; and transaction costs
(legal, fairness, technical advisors, project management, and contract management fees). Model
specific adjustments were made to ensure a fair comparison between procurement options. For
example, the DB model was adjusted to account for differences in tax treatment and insurance costs
between the public and private sectors (the “Competitive Neutrality” adjustment).
Differences in timing and cash flows between procurement options are an important consideration in
3 GNWT P3 Management Framework dated 11/5/2012
20567651.3
December 2015
30
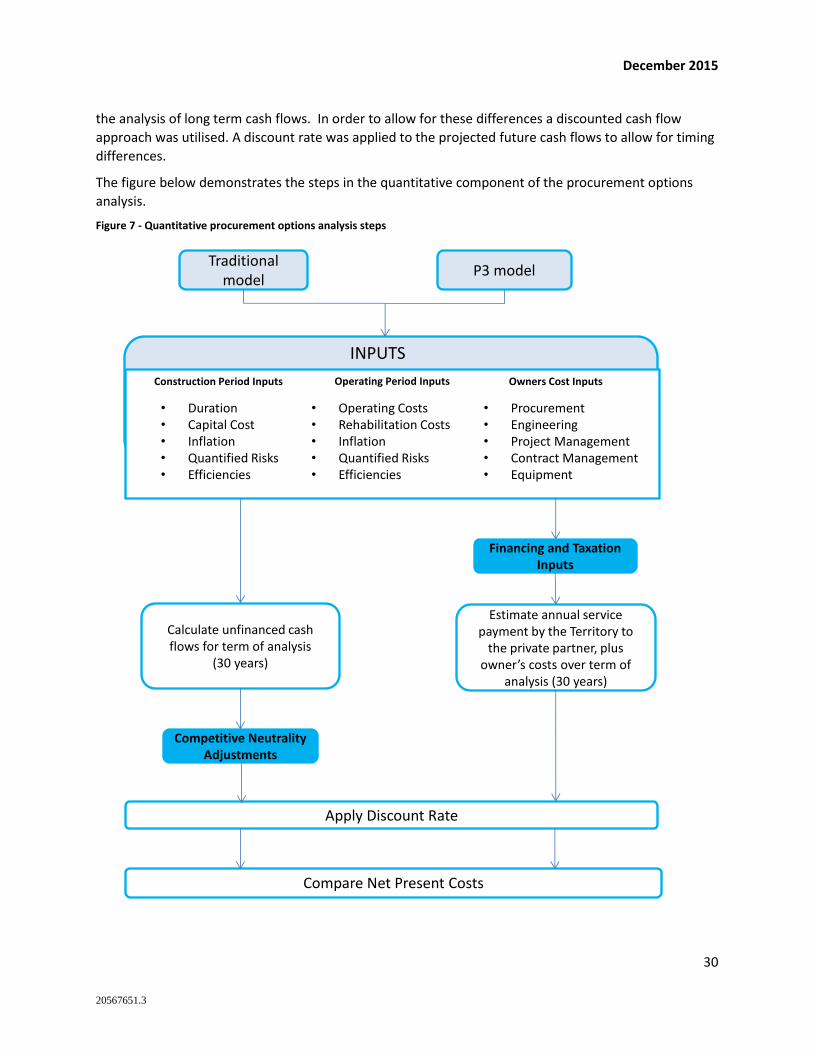
the analysis of long term cash flows. In order to allow for these differences a discounted cash flow
approach was utilised. A discount rate was applied to the projected future cash flows to allow for timing
differences.
The figure below demonstrates the steps in the quantitative component of the procurement options
analysis.
Figure 7 - Quantitative procurement options analysis steps
Traditional model
P3 model
INPUTS
Construction Period Inputs Operating Period Inputs Owners Cost Inputs
• Duration• Capital Cost• Inflation• Quantified Risks• Efficiencies
• Operating Costs• Rehabilitation Costs• Inflation• Quantified Risks• Efficiencies
• Procurement• Engineering• Project Management• Contract Management• Equipment
Financing and Taxation Inputs
Estimate annual service payment by the Territory to
the private partner, plus owner’s costs over term of
analysis (30 years)
Calculate unfinanced cash flows for term of analysis
(30 years)
Competitive Neutrality Adjustments
Apply Discount Rate
Compare Net Present Costs
20567651.3
December 2015
31
Procurement options
The process of considering procurement options began with the definition of key procurement
objectives, which were based on the project objectives. The following procurement objectives were
developed by the project team to provide guidance in the selection and analysis of procurement
options:
Maximize competition (between proponents /bidders)
Cost certainty
Risk allocation
Fairness, transparency, and integrity
Overall value for money
The qualitative analysis concluded that Design Build (DB) and Design Build Finance Maintain (DBFM),
were the two most appropriate traditional and partnership procurement options, respectively, and
should be compared in detail. The two options are described below.
Design Build (DB)
The GNWT would issue a tender call for both the design and construction of the Facility as a single
contract. The GNWT would evaluate all detailed design in accordance with its output specifications and
functional program. Following design approval, the selected contractor would proceed with construction
of the Facility. The GNWT would make monthly progress payments to the contractor during construction
and would take possession and maintain and operate the infrastructure following completion.
In the past, the GNWT has successfully delivered projects on time and on budget using the DB model.
Design Build Finance Maintain (DBFM)
This partnership delivery model involves a two-stage competitive selection process. The first stage is a
Request for Qualifications (RFQ), whereby respondent teams would submit qualifications to be received
and evaluated, resulting in a shortlist of Proponent teams. The second stage invites the proponent
teams to submit proposals as part of the Request for Proposals (RFP) process. At the RFP stage, the
GNWT would provide performance specifications and seek proposals from the proponents to design,
build, finance, and maintain the Facility.
The project team would evaluate these proposals to determine a preferred proponent with which it
would enter into a final Project Agreement. Under the Project Agreement, the proponent would be
required to design, build, finance, and maintain the project over the specified term of the agreement.
Availability payments would be made monthly to the private partner over the life of the agreement, in a
fixed amount determined at Financial Close. Payments only commence once the infrastructure is
completed. To ensure that the private partner receives full payment, they must meet defined and
measurable performance and availability standards on a continuous basis. The DBFM approach provides
a financial structure that aligns the incentives of the private partner and the GNWT. Under the DBFM
option, the private partner would be responsible for:
Arranging project financing, including debt and equity
Developing and constructing the Facility in accordance with a defined output specification
20567651.3
December 2015
32
Maintaining the infrastructure over the life of the Project Agreement and handing it back at the
end of the contract term in the prescribed condition.
Results of the Procurement Options Analysis
Based on the procurement options analyzed, the DBFM method was determined to be the preferred
procurement option, expected to best meet the GNWT’s procurement objectives and overall project
objectives.
Achieving value for money
Value for money is a term that captures both the quantitative and qualitative benefits that are expected
to be achieved by the decision to deliver the project using the partnership method.
Quantitative value for money is achieved through the lower project cost resulting from a particular
procurement method. Qualitative value is achieved when a particular procurement method is best able
to support the broader objectives of a project.
Partnership projects typically provide the following qualitative benefits:
o Competition and innovation: The competitive nature of the bidding process encourages the private
partner teams to develop innovative solutions in all aspects of the project from design and
construction through to operations.
o Schedule certainty: The private partner receives a significant portion of their payment through
monthly availability payments once the infrastructure is available for use, thereby providing a
financial incentive to complete the project on time.
o Cost certainty: The Project Agreement is a fixed price contract.
o Integration: The private partner is responsible for the design and construction, maintenance and
rehabilitation of the infrastructure. This creates opportunities and incentives to integrate these
functions to optimize performance of the infrastructure over the duration of the Project
Agreement.
o Life cycle maintenance: The private partner is responsible and accountable for ensuring the
infrastructure is maintained and rehabilitated over the duration of the Project Agreement
otherwise the Availability Payments may be reduced.
Related Documents











