EMERGENCY AND CRITICAL CARE IN THYROID STORM HARMOKO (090100254) HEMA THIYAGU (090100408) Pembimbing : dr. Dadik Wahyu Wijaya, Sp An

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
EMERGENCY AND CRITICAL CARE IN THYROID STORM
HARMOKO (090100254)HEMA THIYAGU (090100408)ANISSA ZAMANI (090100376)
Pembimbing : dr. Dadik Wahyu Wijaya, Sp An

previously undiagnosed hyperthyroidism
Thyroid gland secretes 2 hormones :– Thyroxine (tetraiodothyronine or T4)– Triiodothyronine (T3)– Secretion ratio T4 to T3 is 15:1– Iodine is attached to tyrosine amino acid residues of thyroglobulin in the gland (organification)– Coupling of these residues then produces T4 & T3
Thyroid Physiology
Thyroid Physiology (cont.)
T4 & T3 released by the gland are bound & transported by serum proteins :–Thyroxine-Binding Globulin (TBG) : 75 %–Thyroxine-Binding Prealbumin (TBPA)–Albumin
The free (or unbound) hormone levels are the levels which are maintained constant by feedback & regulate thyroid function
Total measured serum T4 includes bound & unbound
Variations in Thyroxine Binding Proteins
Causes of increased TBG levels :–Pregnancy, estrogens, cirrhosis, hepatitis, porphyrias
Causes of decreased TBG levels :–Protein malnutrition, nephrotic syndrome, hepatic failure, androgenic steroids, high dose glucocorticoids
Free T4 (FT4) usually constant in the above conditions
Thyroid Hormone Action in the Tissues
T4 deiodonated in periphery to T3–This is 80 % of T3 produced
Other metabolite of T4 is reverse T3 (rT3) which is metabolically inactive
T3 enters cells & binds to group of nuclear receptors, then affects wide range of cellular metabolic functions
Thyroid hormone required for normal cell metabolism
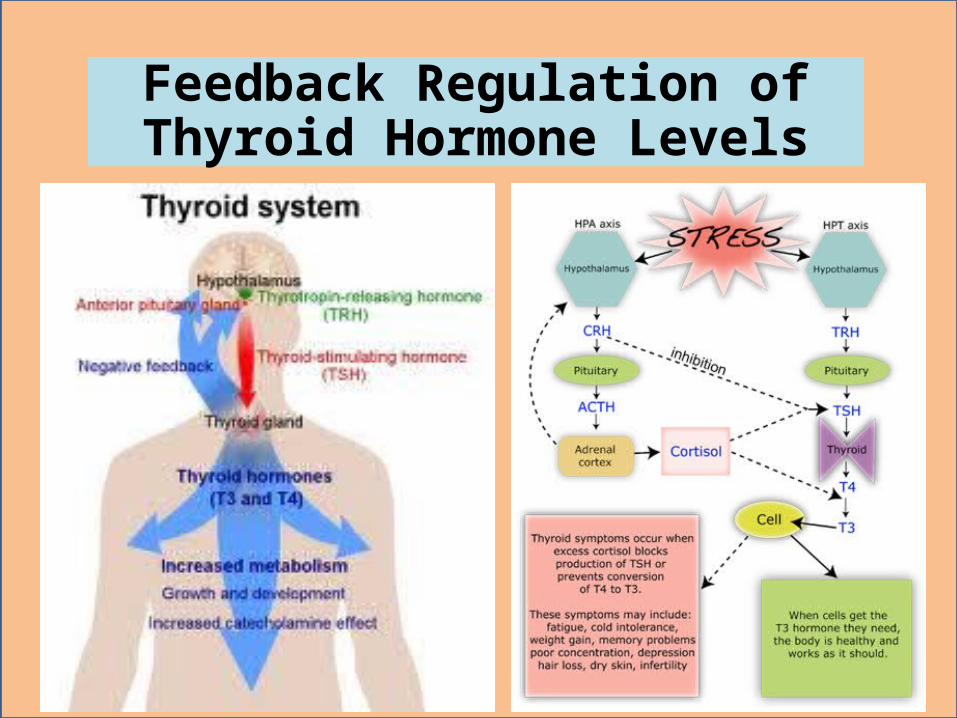
Feedback Regulation of Thyroid Hormone Levels
Normal regulation requires intact hypothalamic-pituitary system
Hypothalamus secretes Thyrotropin-Releasing Hormone (TRH)
TRH then stimulates synthesis & release of thyrotropin (Thyroid Stimulating Hormone or TSH) by the anterior pituitary
TSH then stimulates the thyroid gland to uptake iodine, synthesize & release T4 & T3
T4 & T3 levels feedback to both hypothalamus & pituitary affecting TRH & TSH release
Feedback Regulation of Thyroid Hormone Levels
Thyroid Function Tests
Radioimmunoassay for T4 (T4RIA) is most useful single test of thyroid function–Normal levels 4 to 12 mcg / dl
Free thyroid homone difficult to measure directly, so "indirect" tests developed –T3 Resin Uptake (T3RU) measures amount of radioactive T3 unbound when added to patient's serum
–Reflects of sites available for binding T4 &T3–Is indirect measure of level of circulating T4–Normal is 25 to 35 %
Other Thyroid Function Tests
Free T4 Index (FT4I)–Correlates with level of Free T4–Is the product of T4RIA & T3RU
T3 radioimmunoassay (less useful)–Normal 75 to 195 ng / dl
Serum TSH–Normal is 0.3 to 5.0 mcU / ml
TRH Stimulation Test–Measures TSH response to TRH IV injection–Normal is increase in TSH to 30 mcU / ml
Clinical Interpretation of Thyroid Function Tests
T3RU :–Low in hypothyroidism & high TBG states–High in hyperthyroidism & low TBG states–T4RIA & the T3RU go in same direction with thyroid disease & in opposite directions with TBG level abnormalities
TSH–Elevated in primary hypothyroidism–If patient hypothyroid & TSH is low, then lesion is in hypothalamic-pituitary axis, and TRH Stimulation Test should be done
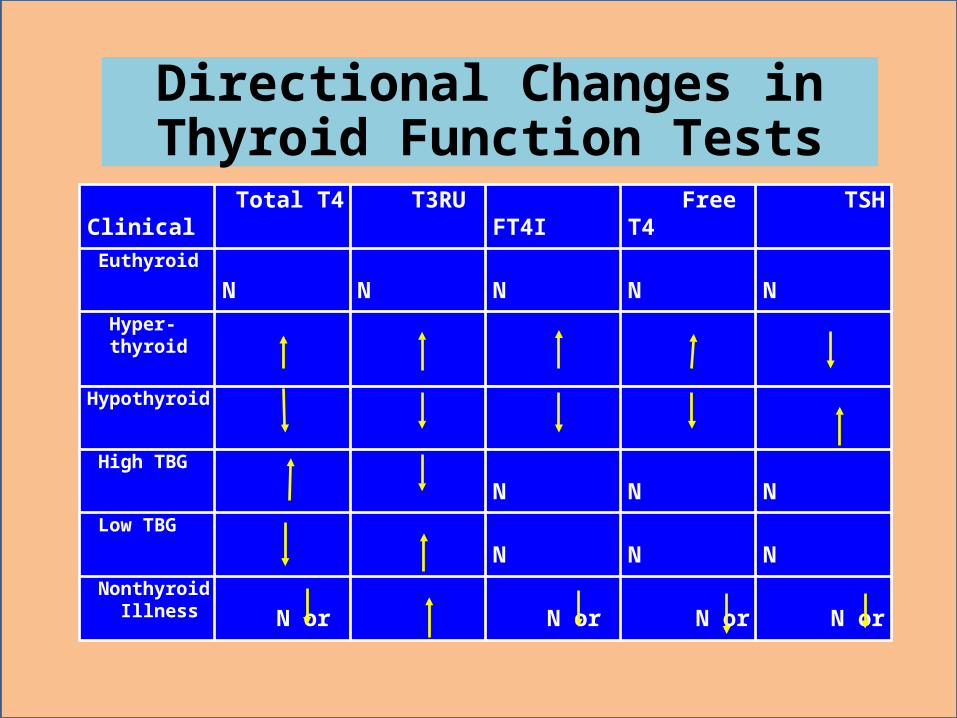
Directional Changes in Thyroid Function Tests
Clinical State
Total T4 T3RU FT4I Free T4 TSH
Euthyroid N N N N N
Hyper- thyroid
Hypothyroid
High TBG N N N
Low TBG N N N
Nonthyroid Illness N or N or N or N or
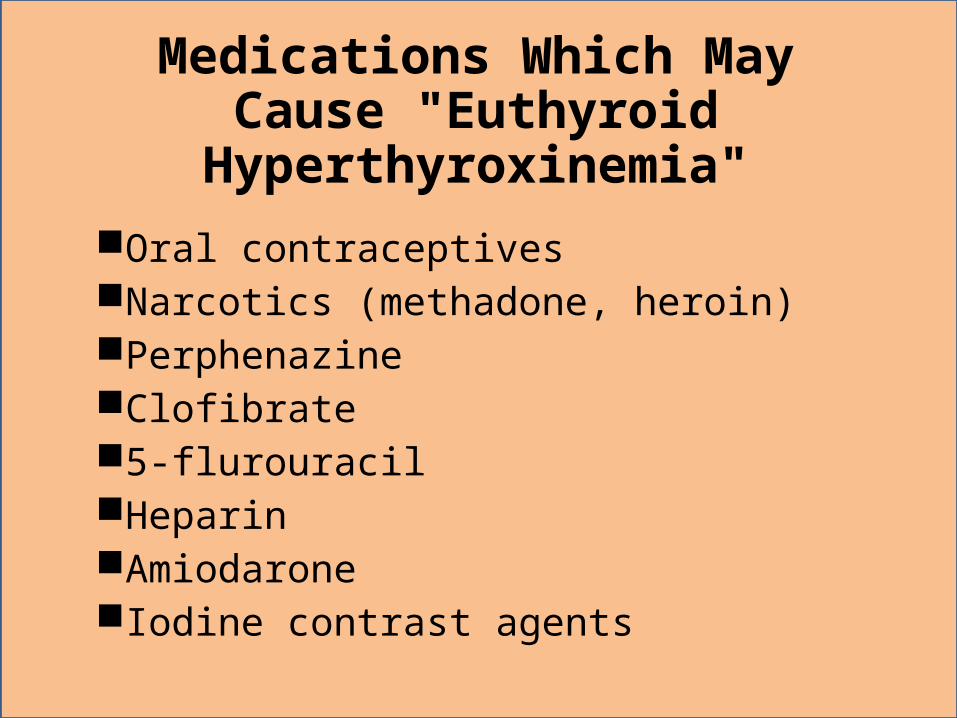
Medications Which May Cause "Euthyroid Hyperthyroxinemia"
Oral contraceptivesNarcotics (methadone, heroin)PerphenazineClofibrate5-flurouracilHeparinAmiodaroneIodine contrast agents
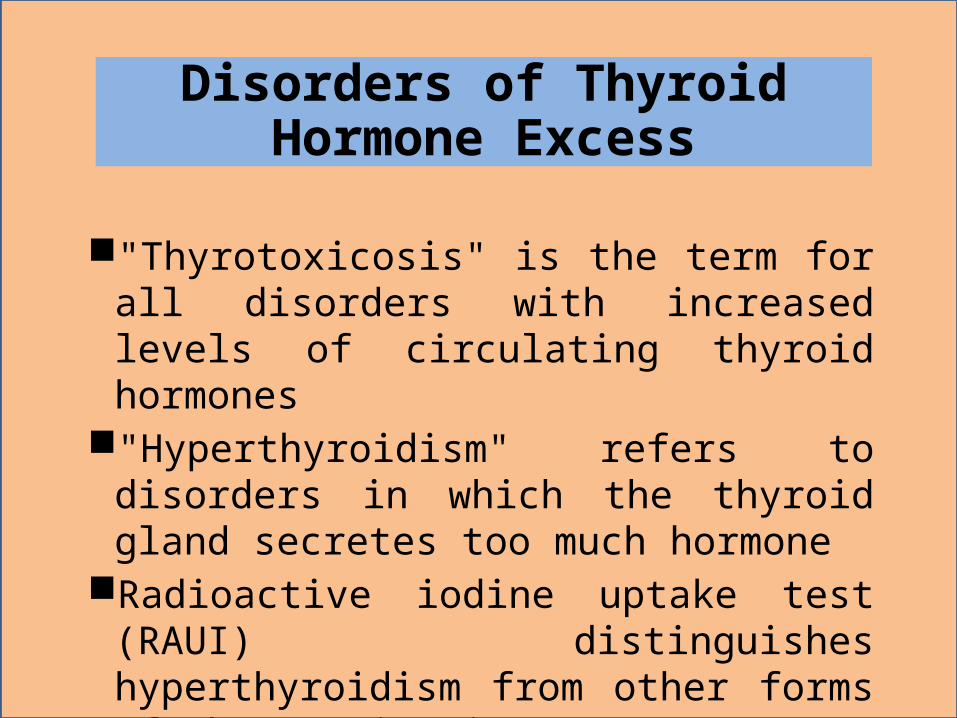
Disorders of Thyroid Hormone Excess
"Thyrotoxicosis" is the term for all disorders with increased levels of circulating thyroid hormones
"Hyperthyroidism" refers to disorders in which the thyroid gland secretes too much hormone
Radioactive iodine uptake test (RAUI) distinguishes hyperthyroidism from other forms of thyrotoxicosis
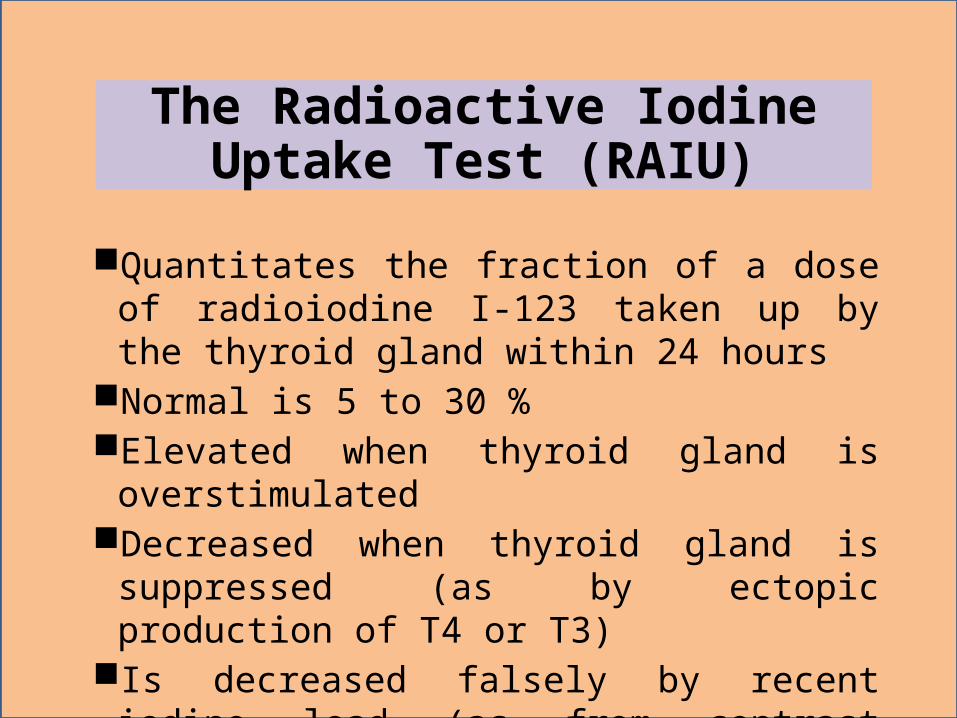
The Radioactive Iodine Uptake Test (RAIU)
Quantitates the fraction of a dose of radioiodine I-123 taken up by the thyroid gland within 24 hours
Normal is 5 to 30 %Elevated when thyroid gland is overstimulatedDecreased when thyroid gland is suppressed
(as by ectopic production of T4 or T3) Is decreased falsely by recent iodine load (as
from contrast computed tomography scan)
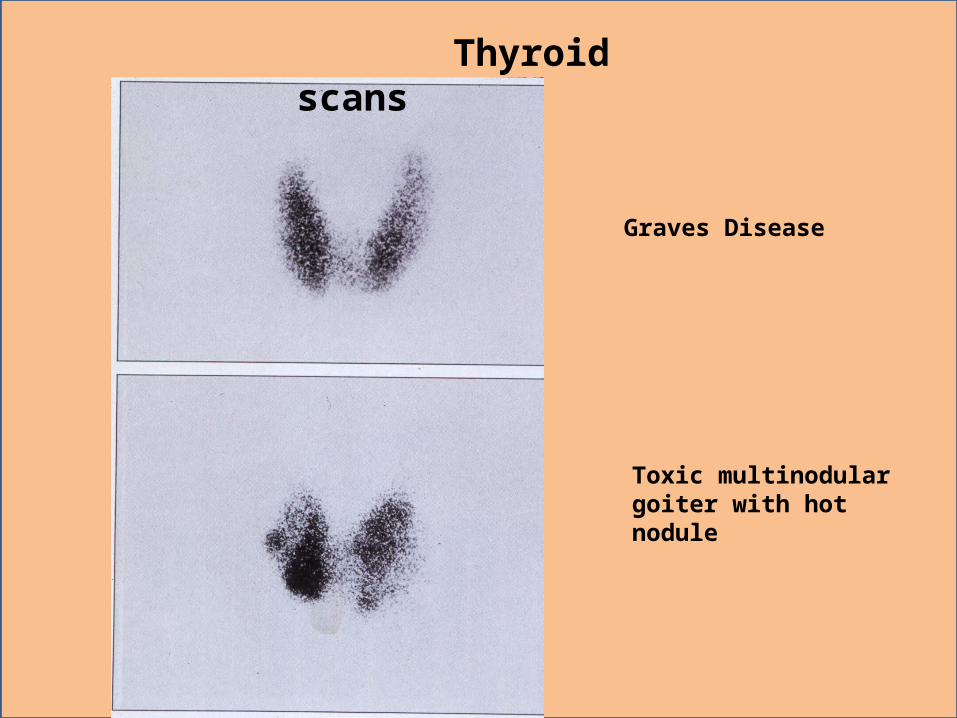
Graves Disease
Toxic multinodular goiter with hot nodule
Thyroid scans
Causes of Thyrotoxicosis with Elevated RAUI
Graves' DiseasePituitary tumor secreting excess TSHPituitary insensitivity to feedbackHydatidiform moleChoriocarcinomaTestis embryonal carcinomaToxic multinodular goiterToxic uninodular goiter
Causes of Thyrotoxicosis with Decreased RAUI
Acute autoimmune thyroiditis (may later lead to hypothyroidism)
Infectious thyroiditisPostpartum thyroiditisFactitious (taking PO excess thyroid
hormone)Metastatic thyroid cancerStruma ovarii (dermoid tumors or teratomas
of the ovary)
Medications Which Can Induce Hyperthyroidism
IodineAmiodaroneLithium
Features of Graves' Disease(Toxic Diffuse Goiter)
Most common cause of hyperthyroidism (70 to 85 % of all cases)
Caused by thyroid stimulating immunoglobulinsMainly in young adults ages 20 to 505 times more frequent in womenHalf of cases have infiltrative ophthalmopathy
with exopthalmos (not seen with other causes of hyperthyroidism)
5 % have pretibial myxedema
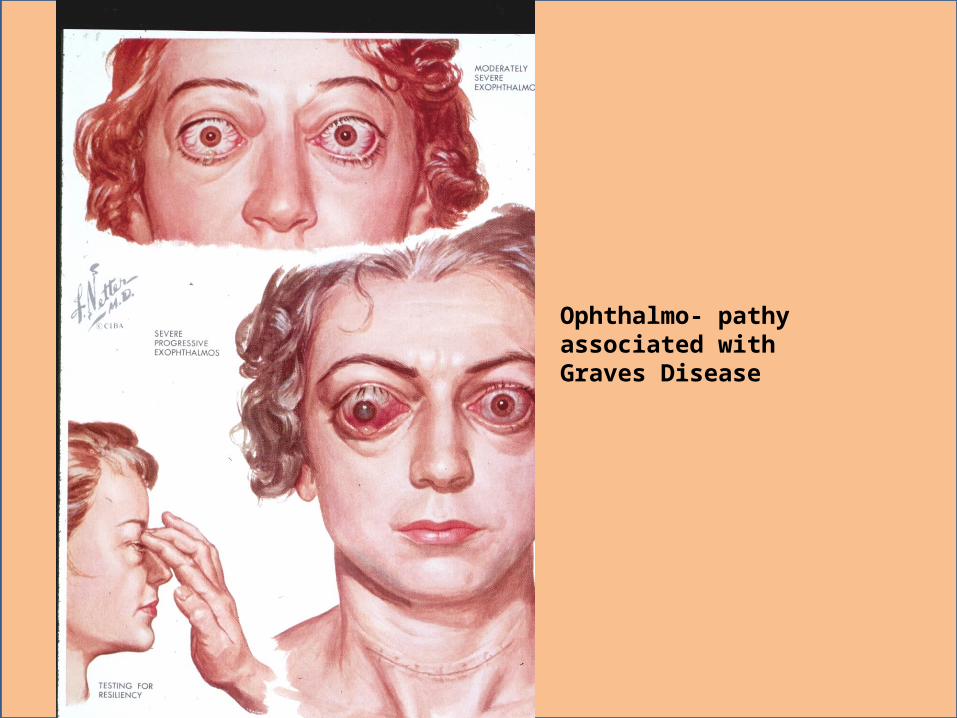
Ophthalmo- pathy associated with Graves Disease
Symptoms Suggestive of Thyrotoxicosis
Nervousness, restlessness,shortened attention span, emotional lability, difficulty sleeping
Increased appetiteWeight lossHeat intolerance, perhaps low feverDiaphoresisWeaknessMenstrual irregularities
Signs Suggestive of Thyrotoxicosis
Sinus tachycardia, PVC's, PAC's, atrial fibrillationTremor, hyperreflexia, muscle wastingWarm, erythematous, moist skinAlopecia, nail friability & separation from bedHyperventilationEyelid retraction, lid lag, persistent stareHyperactive bowel soundsWith Graves' : may have exopthalmos, tender
enlarged thyroid, & pretibial myxedema
Possible Complications of Thyrotoxicosis at Presentation
High output congestive heart failureDehydrationElectrolyte imbalance (from diarrhea)Corneal lesions from exopthalmosWorsening of preexistent angina
Thyroid StormDefinitions
"Exaggerated or florid state of thyrotoxicosis""Life threatening, sudden onset of thyroid
hyperactivity"May represent end stage of a continuum :
–Thyroid hyperactivity to thyrotoxicosis to thyrotoxic crisis to thyroid storm
"Probably reflects the addition of adrenergic hyperactivity, induced by a nonspecific stress, into the setting of untreated or undertreated hyperthyroidism"
THYROID STORM - ETIOLOGY
GRAVES DISEASE
INFECTION
TRAUMA SURGERY
THYROID STORM CLINICAL PRESENTATION
2 most important defining features :–High fever (usually over 40 degrees C)–Significantly abnormal mental statusƒ Agitation, confusion, psychosis, coma
May also exhibit :–Marked tachycardia–Vomiting, diarrhea–Jaundice (in 20 %)–Associated signs of Graves' disease
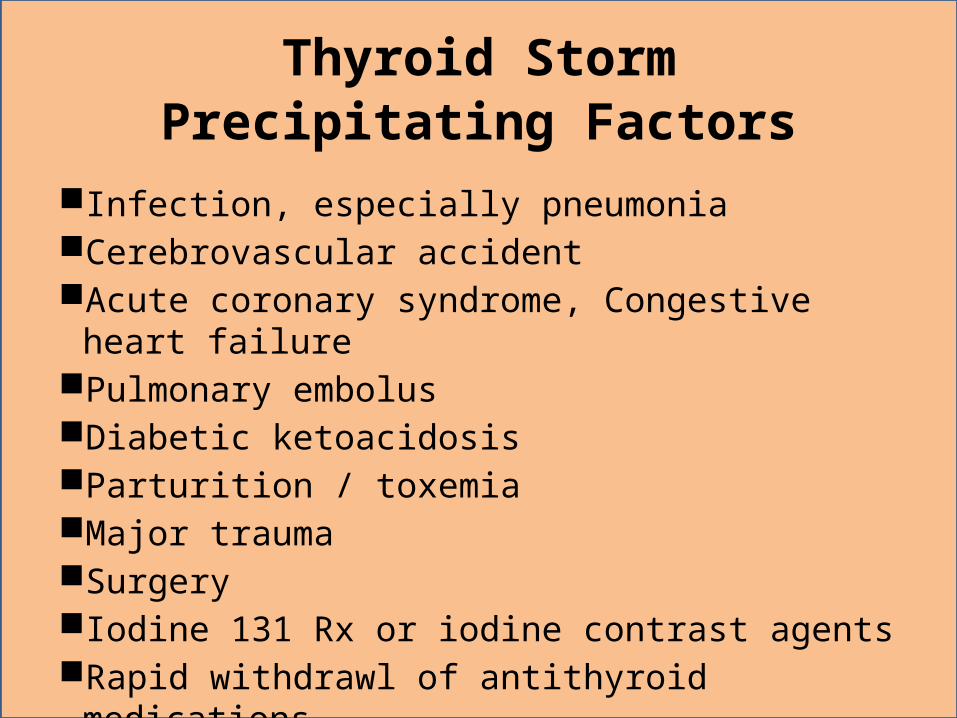
Thyroid StormPrecipitating Factors
Infection, especially pneumoniaCerebrovascular accidentAcute coronary syndrome, Congestive heart failurePulmonary embolusDiabetic ketoacidosisParturition / toxemiaMajor traumaSurgeryIodine 131 Rx or iodine contrast agentsRapid withdrawl of antithyroid medications
Thyroid StormDiagnosis
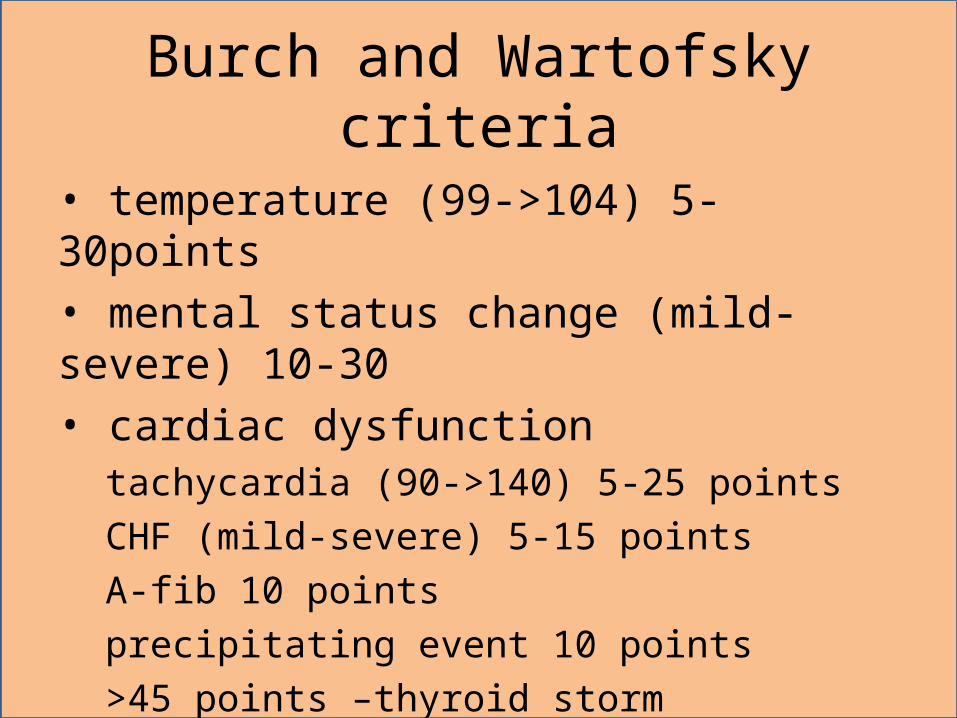
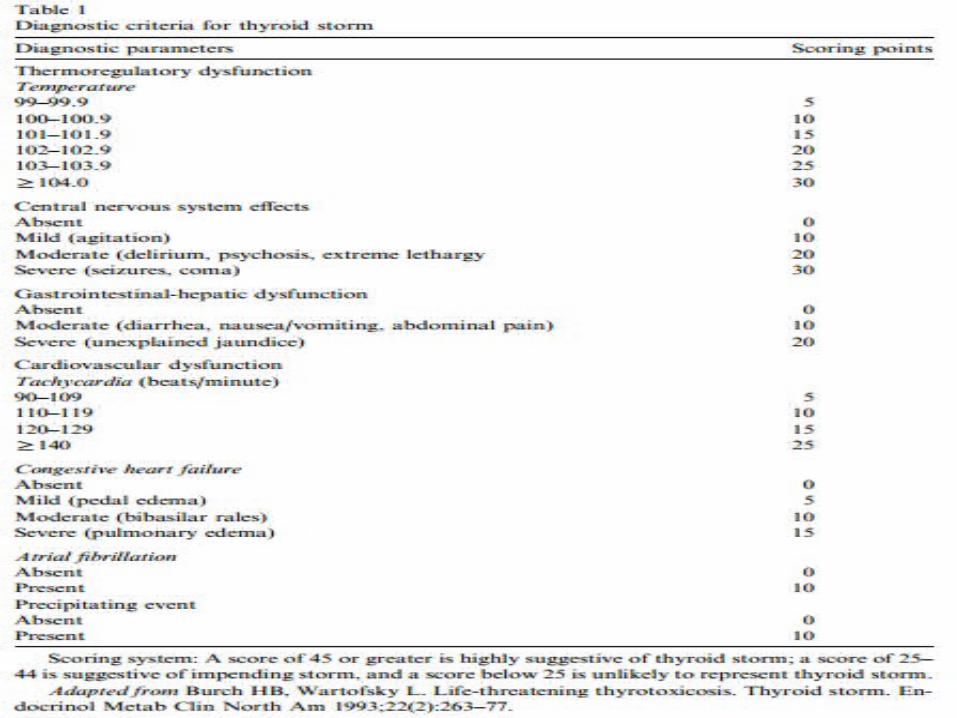
Burch and Wartofsky criteria
• temperature (99->104) 5-30points• mental status change (mild-severe) 10-30• cardiac dysfunction
tachycardia (90->140) 5-25 pointsCHF (mild-severe) 5-15 pointsA-fib 10 pointsprecipitating event 10 points>45 points –thyroid storm
Thyroid StormDifferential Diagnosis
Environmental heatstrokeCocaine, amphetamine, or phencyclidine
toxicityNeuroleptic malignant syndromeMeningitis or encephalitisIntracranial hemorrhageMalignant hyperthermiaFalciparum cerebral malaria
Progression of Neurologic Findings in Thyroid Storm
Emotional labilityRestlessnessHyperkinesisConfusionPsychosisLethargySomnolenceObtundationComa
Cardiovascular Findings in Thyroid Storm
Marked tachycardia–Sinus tach or atrial fibrillation
Increased myocardial irritability–PVC's, PAC's, first degree AV block
Wide pulse pressureApical systolic murmurLoud S1 and S2 valve soundsSome have high output CHF
Usual Indicated Initial Lab Studies for Thyroid Storm
Glucose (stat fingerstick because of altered mental status)
Pulse oximetry (+/- ABG)CBC, electrolytes, BUN, creatinineT4RIA, T3RU, TSH, +/- T3RIAUrinalysisLiver function testsSerum cortisol
Thyroid StormEmergent Rx
High flow O2Rapid cooling if markedly hyperthermic
–Ice packs, cooling blanket, mist / fans, nasogastric tube lavage, acetominophen (Salicylates contraindicated because cause peripheral deiodination to T3)
IV fluid bolus if dehydrated–May need inotropes instead if in CHF
Propranolol 1 mg doses or labetolol 10 to 20 mg doses IV & repeat doses as needed
Thyroid StormFurther Rx
IV diltiazem +/- digoxin for rate control for atrial fib
IV diuretics if in CHFIV hydrocortisone (or equivalent) 100 mgPropylthiouracil (PTU) 600 to 1200 mg PO
or by NGSodium iodide 1 gram IV one hour after the
PTUFind and treat the precipitating cause
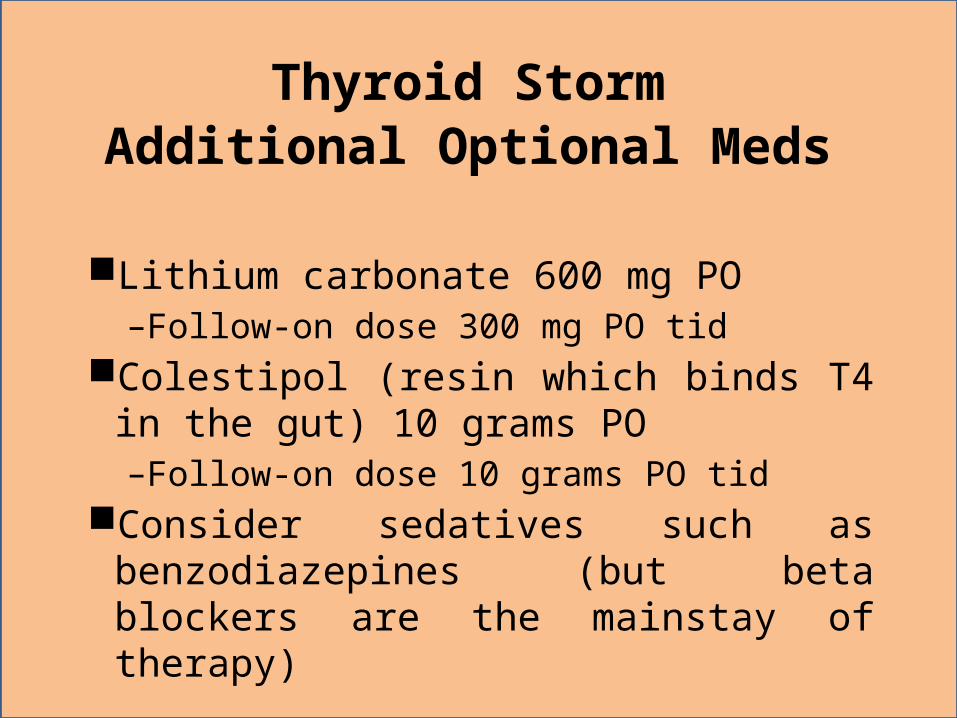
Thyroid StormAdditional Optional Meds
Lithium carbonate 600 mg PO–Follow-on dose 300 mg PO tid
Colestipol (resin which binds T4 in the gut) 10 grams PO–Follow-on dose 10 grams PO tid
Consider sedatives such as benzodiazepines (but beta blockers are the mainstay of therapy)
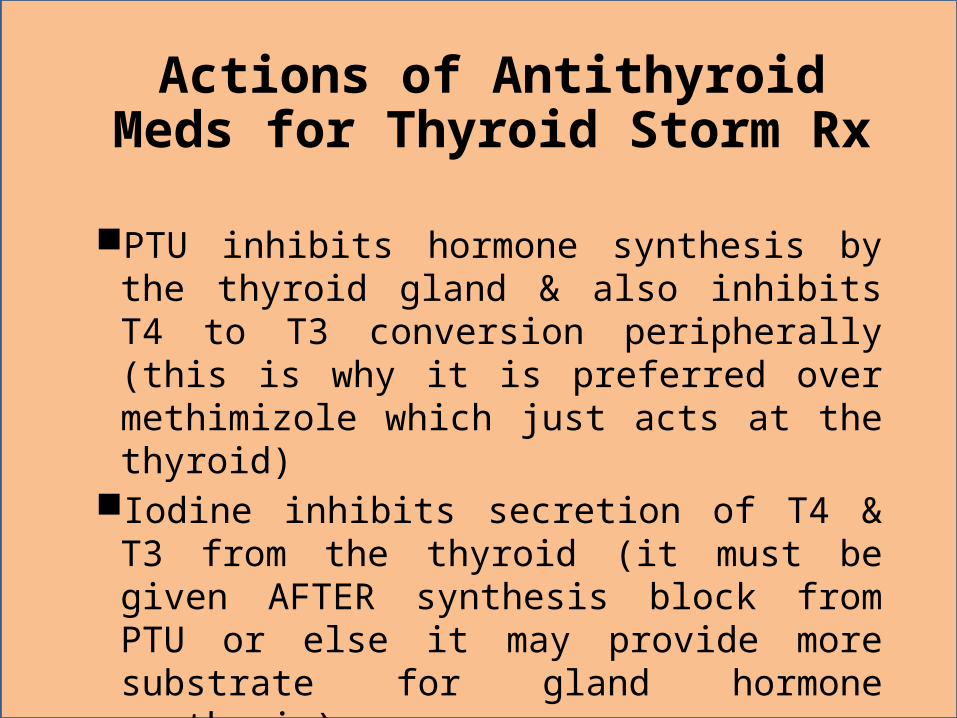
Actions of Antithyroid Meds for Thyroid Storm Rx
PTU inhibits hormone synthesis by the thyroid gland & also inhibits T4 to T3 conversion peripherally (this is why it is preferred over methimizole which just acts at the thyroid)
Iodine inhibits secretion of T4 & T3 from the thyroid (it must be given AFTER synthesis block from PTU or else it may provide more substrate for gland hormone synthesis)
Lithium can be used in patients alergic to iodine but can cause relapse when stopped
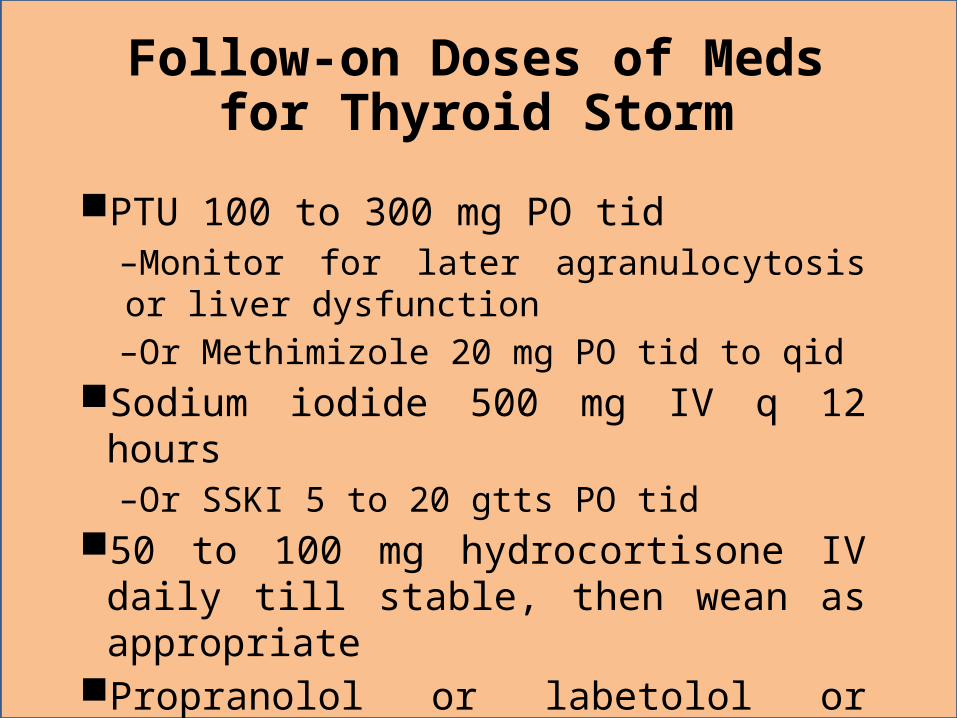
Follow-on Doses of Meds for Thyroid Storm
PTU 100 to 300 mg PO tid–Monitor for later agranulocytosis or liver dysfunction–Or Methimizole 20 mg PO tid to qid
Sodium iodide 500 mg IV q 12 hours–Or SSKI 5 to 20 gtts PO tid
50 to 100 mg hydrocortisone IV daily till stable, then wean as appropriate
Propranolol or labetolol or metoprolol (same daily doses as for hypertension)
Additional Rx for Thyroid Storm Not Responding to Initial Rx
Plasma exchange or plasmapheresisPeritoneal dialysis or charcoal
hemoperfusionEmergency surgery for partial or total
thyroidectomy
ANASTHESIA ASPECTS
Perioperative :• History taking and physical examination• Relative euthyroid before elective surgery• Benzodiazepine drug of choice for sedation• Quick preparation for emergent case
ANASTHESIA ASPECTS
Intraoperative :• Monitoring of hemodynamic and temperature• Avoid sympathetic stimulation drugs eg. Ketamine, pancuronium, adrenergic agonist• High dose thiopental has anti thyroid efect• Deep anesthesia sedation for preventing sympathetic stimulation
ANASTHESIA ASPECTS
Postoperative :• Thyroid storm onset 6-24 hours after surgery
Pr, 35 tahun,56 kg• KU : benjolan di leher • Telaah :⁻ Hal ini dialami pasien ± 1 tahun ini, awalnya benjolan kecil, lama
kelamaan makin membesar. Demam (+) dirasakan os ± 4 hari ini bersifat naik turun dan naik turun dengan pemakaian obat penurun panas.
⁻ Riwayat penurunan berat badan (+), ± 5 kg dalam 6 bulan ini, selera makan berkurang, os lebih suka udara dingin
⁻ Os juga lebih sering berkeringat terutama di telapak tangan, jantung sering berdebar-debar. Os juga merasa matanya makin membesar.
⁻ Riwayat keluar darah dari kemaluan (+), mual (+), muntah (+)• RPT : tidak jelas• RPO : tidak jelas
Primary Survey• A (Airway) : Airway Clear,
Gurgling/Snoring/Crowing : - /- /-• B (Breathing) : RR: 24x/menit, Suara Pernafasan :
Vesikuler, Suara Tambahan : -, Terpasang Nasal kanul dengan Oksigen 2 lpm.
• C (Circulation) : Terpasang IV line, dilakukan pemberian RL 20 gtt/i, Frekuensi Nadi 80 x/i, t/v kuat dan cukup, TD : 130/80 mmHg, Akral teraba hangat, merah, dan kering.
• D (Disability) : GCS 15, Sens: CM, Pupil Isokor diameter 3/3 mm, Refleks Cahaya +/+
• E (Exposure) : abdomen teraba soepel, ttb, peristaltik (+) N. Tampak benjolan pada leher.
Pemeriksaan Fisik • B1 (Breathing) : Airway clear, gurgling/snoring/crowing : - /- /- ,
SP : vesikuler, ST : -, RR : 24 x/i, SpO2 99%, Riwayat sesak/ asma / batuk / alergi (-), retraksi iga
(-), retraksi sternum (-). • B2 (Blood) : Akral merah/hangat/kering, HR : 80 x/i, t/v :
cukup, TD : 120/80 mmHg. T: 37.3oC• B3 (Brain) : Sensorium : Compos Mentis, GCS : 15
(E4V5M6), Pupil Isokor 3/3 mm, RC +/+• B4 (Bladder) : kateter (-), UOP : (+) sulit dinilai. • B5 (Bowel) : abdomen: soepel, peristaltik (+) N.• B6 (Bone) : Fraktur (-), edema (-) •
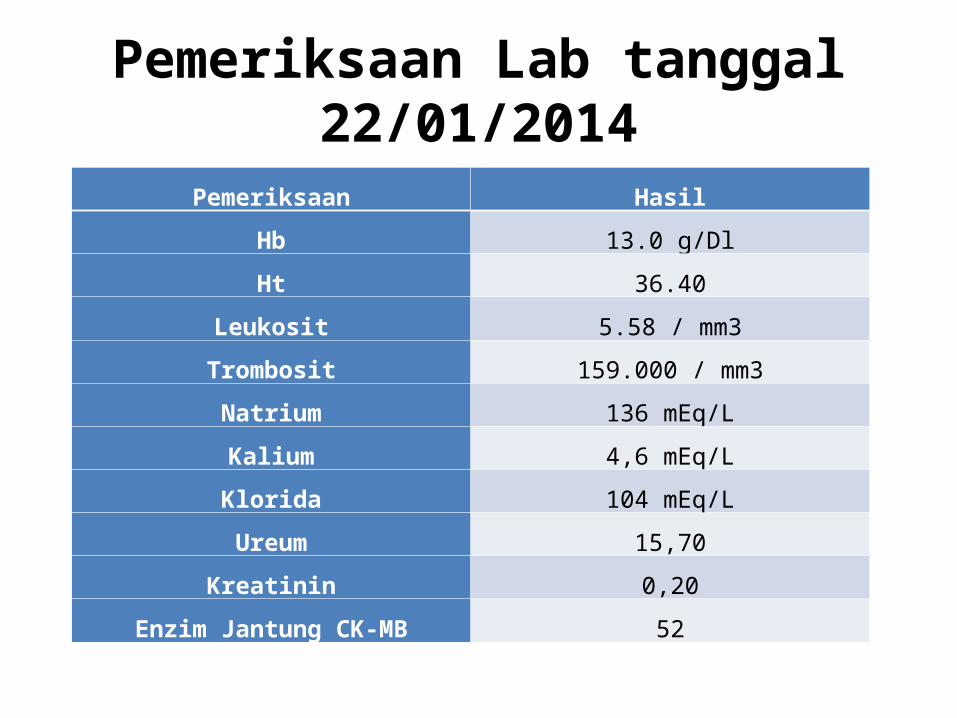
Pemeriksaan Lab tanggal 22/01/2014
Pemeriksaan Hasil
Hb 13.0 g/Dl
Ht 36.40
Leukosit 5.58 / mm3
Trombosit 159.000 / mm3
Natrium 136 mEq/L
Kalium 4,6 mEq/L
Klorida 104 mEq/L
Ureum 15,70
Kreatinin 0,20
Enzim Jantung CK-MB 52
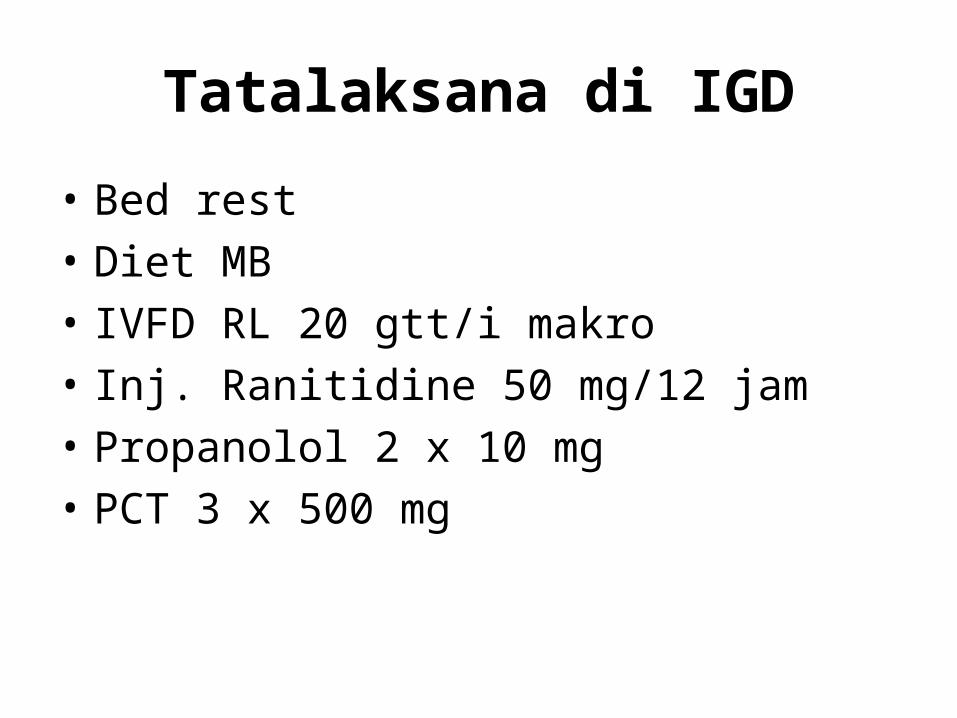
Tatalaksana di IGD
• Bed rest • Diet MB • IVFD RL 20 gtt/i makro • Inj. Ranitidine 50 mg/12 jam• Propanolol 2 x 10 mg• PCT 3 x 500 mg
FOLLOW UP

Tanggal 6/02/2014O : A : P : R :B1 : airway clear, RR 28 x/i, SP : vesikuler, ST : -, S/C/G: -/-/-B2 : akral : H/M/K, TD : 85/60 mmHg, HR : 130 x/i, t/v : kuat/cukup,T:38.6CB3 : sens : compos mentis, pupil isokor ø 3mm, RC +/+B4 : kateter : (+) terpasang, UOP : 100 ccB5 : abdomen : soepel, peristaltic (+)B6 : oedem (-)
Thyroid storm + post SVT dengan hemodinamik stabil + pulmonary hypertension
- Bed rest head up 30º- O2 nasal kanul 2 l/i.- IVFD NaCl 0.9% 30 gtt/i- Inj Ranitidine 1 amp/12 jam/IV- PTU 200 mg/4 jam/oral - Propanolol 80 mg/8jam/oral- Methylclopramide 125 mg/8jam/IVPCT k/p 4 x 1 tab
- Cek darah lengkap- AGDA- Elektrolit- KGD- HST- T3, T4, TSH- Albumin
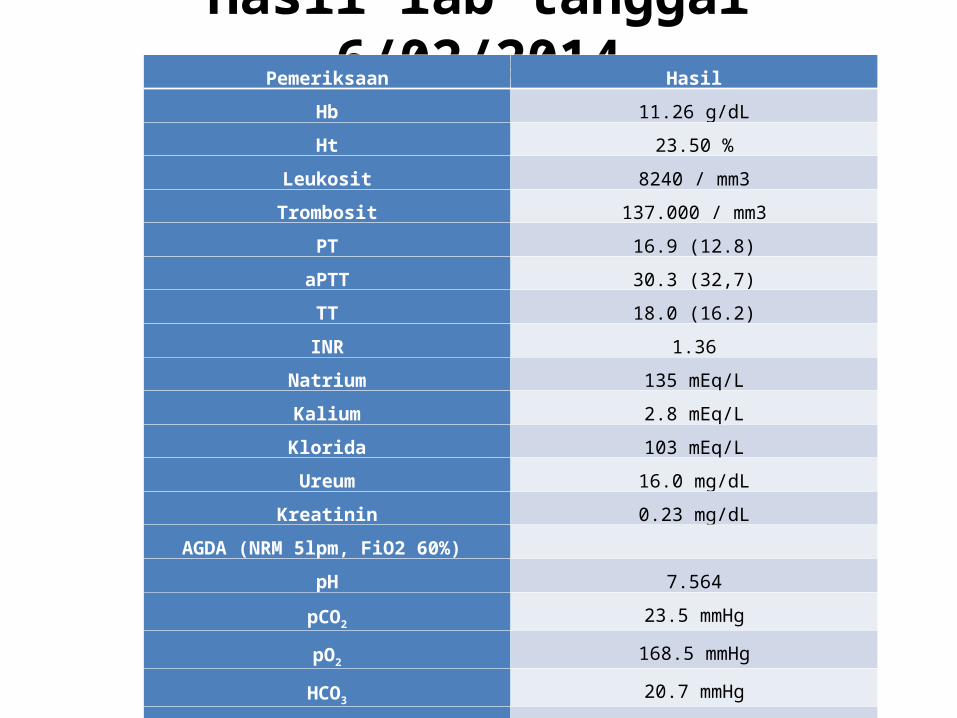
Hasil lab tanggal 6/02/2014Pemeriksaan Hasil
Hb 11.26 g/dL
Ht 23.50 %
Leukosit 8240 / mm3
Trombosit 137.000 / mm3
PT 16.9 (12.8)
aPTT 30.3 (32,7)
TT 18.0 (16.2)
INR 1.36
Natrium 135 mEq/L
Kalium 2.8 mEq/L
Klorida 103 mEq/L
Ureum 16.0 mg/dL
Kreatinin 0.23 mg/dL
AGDA (NRM 5lpm, FiO2 60%)
pH 7.564
pCO2 23.5 mmHg
pO2 168.5 mmHg
HCO3 20.7 mmHg
Total CO2 21.5 mmol/L
Base Excess -0.7 mmol/L
SaO2 99.6 %
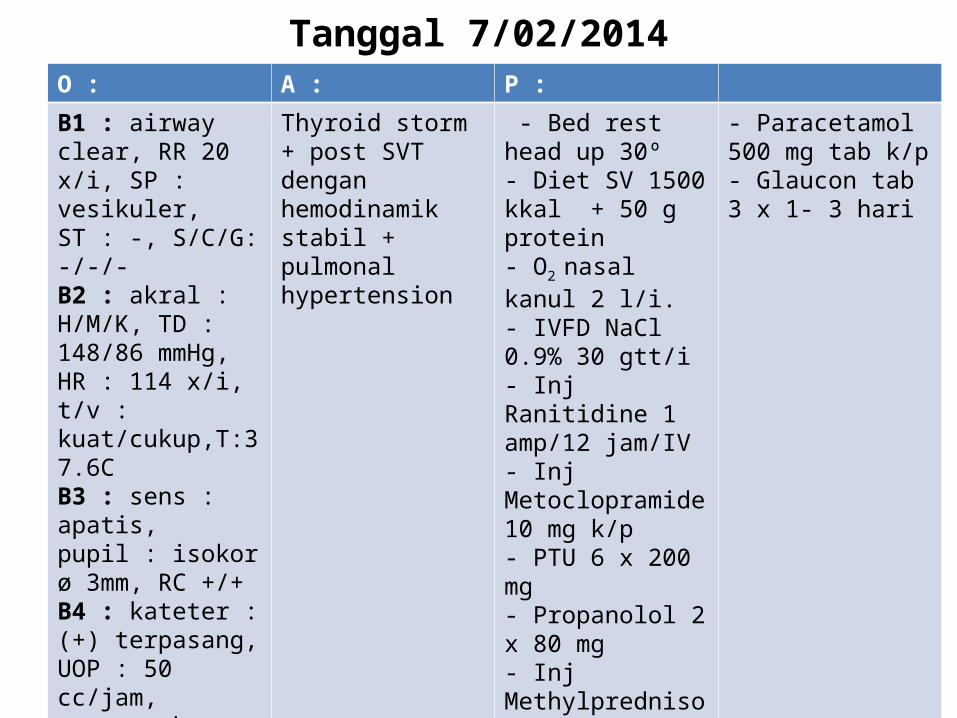
Tanggal 7/02/2014O : A : P :B1 : airway clear, RR 20 x/i, SP : vesikuler, ST : -, S/C/G: -/-/-B2 : akral : H/M/K, TD : 148/86 mmHg, HR : 114 x/i, t/v : kuat/cukup,T:37.6CB3 : sens : apatis, pupil : isokor ø 3mm, RC +/+B4 : kateter : (+) terpasang, UOP : 50 cc/jam, warna : kurang jernihB5 : abdomen : soepel, peristaltik (+) meningkat, mual (-), muntah (-) B6 : oedem (-)
Thyroid storm + post SVT dengan hemodinamik stabil + pulmonal hypertension
- Bed rest head up 30º- Diet SV 1500 kkal + 50 g protein- O2 nasal kanul 2 l/i.- IVFD NaCl 0.9% 30 gtt/i- Inj Ranitidine 1 amp/12 jam/IV- Inj Metoclopramide 10 mg k/p- PTU 6 x 200 mg - Propanolol 2 x 80 mg- Inj Methylprednisolone 125 mg/8 jam
- Paracetamol 500 mg tab k/p- Glaucon tab 3 x 1- 3 hari
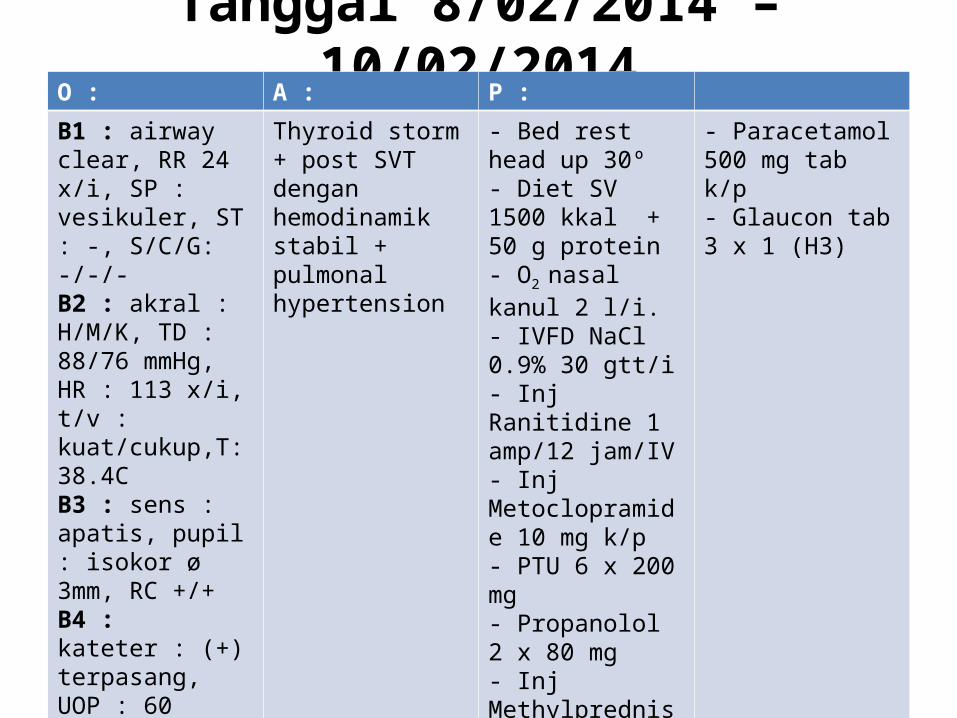
Tanggal 8/02/2014 – 10/02/2014O : A : P :B1 : airway clear, RR 24 x/i, SP : vesikuler, ST : -, S/C/G: -/-/-B2 : akral : H/M/K, TD : 88/76 mmHg, HR : 113 x/i, t/v : kuat/cukup,T: 38.4CB3 : sens : apatis, pupil : isokor ø 3mm, RC +/+B4 : kateter : (+) terpasang, UOP : 60 cc/jam, warna : kuning jernihB5 : abdomen : soepel, peristaltik (+) NB6 : oedem (-)
Thyroid storm + post SVT dengan hemodinamik stabil + pulmonal hypertension
- Bed rest head up 30º- Diet SV 1500 kkal + 50 g protein- O2 nasal kanul 2 l/i.- IVFD NaCl 0.9% 30 gtt/i- Inj Ranitidine 1 amp/12 jam/IV- Inj Metoclopramide 10 mg k/p- PTU 6 x 200 mg - Propanolol 2 x 80 mg- Inj Methylprednisolone 125 mg/8 jam
- Paracetamol 500 mg tab k/p- Glaucon tab 3 x 1 (H3)
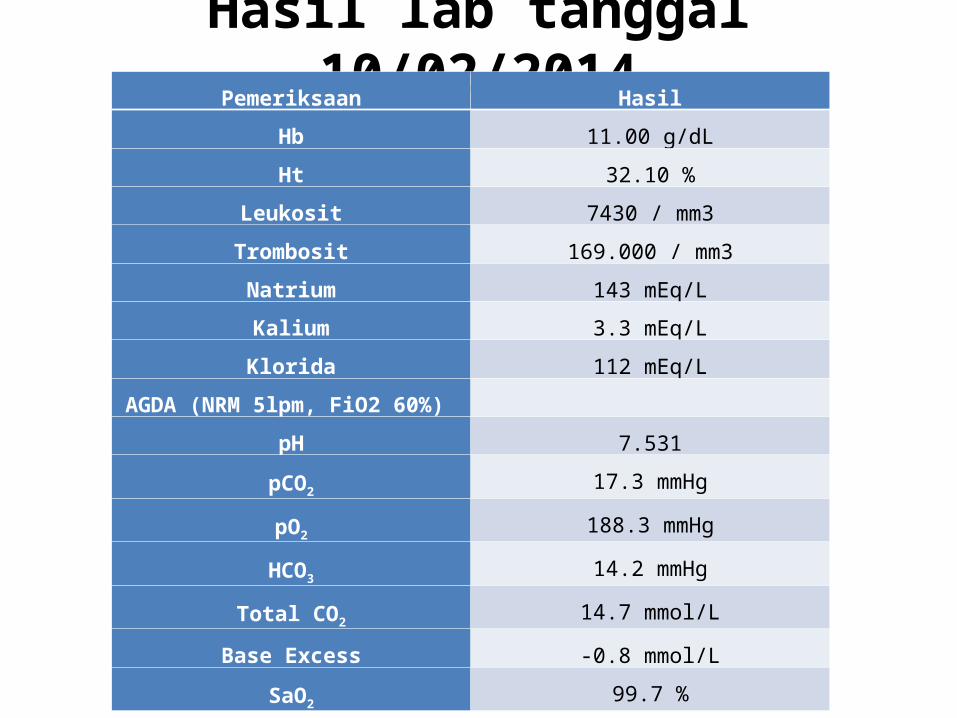
Hasil lab tanggal 10/02/2014Pemeriksaan Hasil
Hb 11.00 g/dL
Ht 32.10 %
Leukosit 7430 / mm3
Trombosit 169.000 / mm3
Natrium 143 mEq/L
Kalium 3.3 mEq/L
Klorida 112 mEq/L
AGDA (NRM 5lpm, FiO2 60%)
pH 7.531
pCO2 17.3 mmHg
pO2 188.3 mmHg
HCO3 14.2 mmHg
Total CO2 14.7 mmol/L
Base Excess -0.8 mmol/L
SaO2 99.7 %
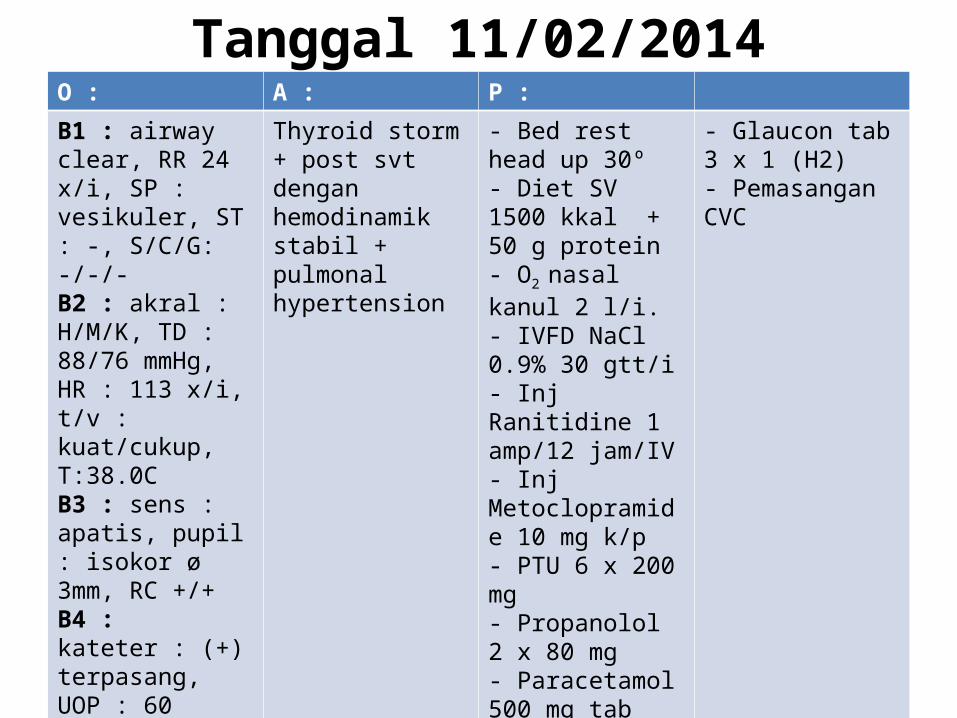
Tanggal 11/02/2014O : A : P :B1 : airway clear, RR 24 x/i, SP : vesikuler, ST : -, S/C/G: -/-/-B2 : akral : H/M/K, TD : 88/76 mmHg, HR : 113 x/i, t/v : kuat/cukup, T:38.0CB3 : sens : apatis, pupil : isokor ø 3mm, RC +/+B4 : kateter : (+) terpasang, UOP : 60 cc/jam, warna : kuning jernihB5 : abdomen : soepel, peristaltik (+) NB6 : oedem (-)
Thyroid storm + post svt dengan hemodinamik stabil + pulmonal hypertension
- Bed rest head up 30º- Diet SV 1500 kkal + 50 g protein- O2 nasal kanul 2 l/i.- IVFD NaCl 0.9% 30 gtt/i- Inj Ranitidine 1 amp/12 jam/IV- Inj Metoclopramide 10 mg k/p- PTU 6 x 200 mg - Propanolol 2 x 80 mg- Paracetamol 500 mg tab k/p
- Glaucon tab 3 x 1 (H2)- Pemasangan CVC
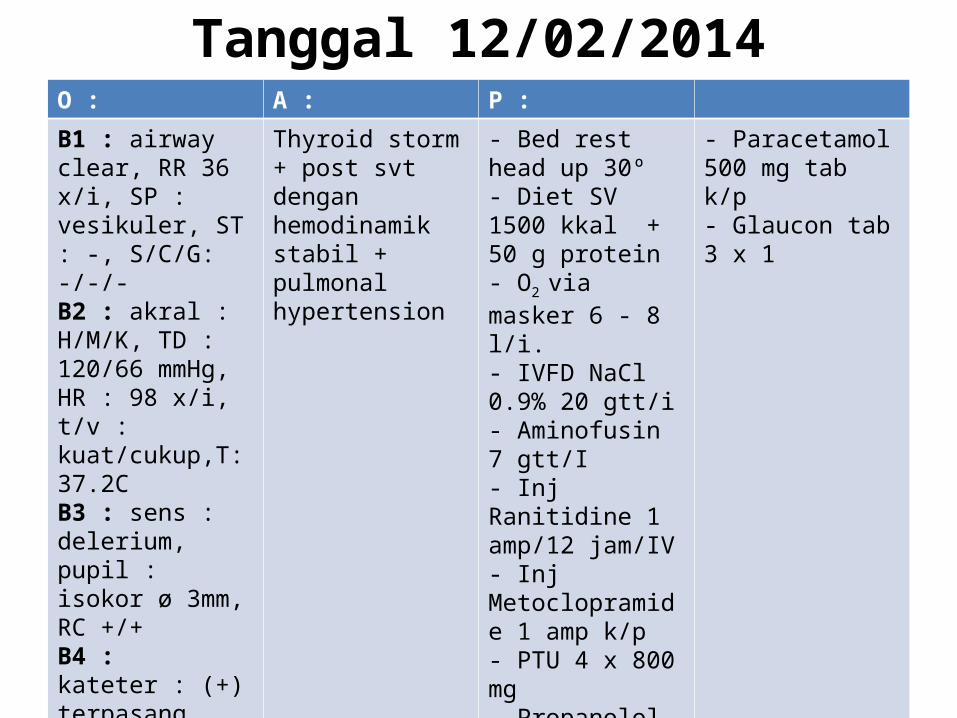
Tanggal 12/02/2014O : A : P :B1 : airway clear, RR 36 x/i, SP : vesikuler, ST : -, S/C/G: -/-/-B2 : akral : H/M/K, TD : 120/66 mmHg, HR : 98 x/i, t/v : kuat/cukup,T: 37.2CB3 : sens : delerium, pupil : isokor ø 3mm, RC +/+B4 : kateter : (+) terpasang, UOP : 100 cc/jam, warna : kuning jernihB5 : abdomen : soepel, peristaltik (+) NB6 : oedem (-)
Thyroid storm + post svt dengan hemodinamik stabil + pulmonal hypertension
- Bed rest head up 30º- Diet SV 1500 kkal + 50 g protein- O2 via masker 6 - 8 l/i.- IVFD NaCl 0.9% 20 gtt/i- Aminofusin 7 gtt/I - Inj Ranitidine 1 amp/12 jam/IV- Inj Metoclopramide 1 amp k/p- PTU 4 x 800 mg - Propanolol 3 x 100 mg
- Paracetamol 500 mg tab k/p- Glaucon tab 3 x 1
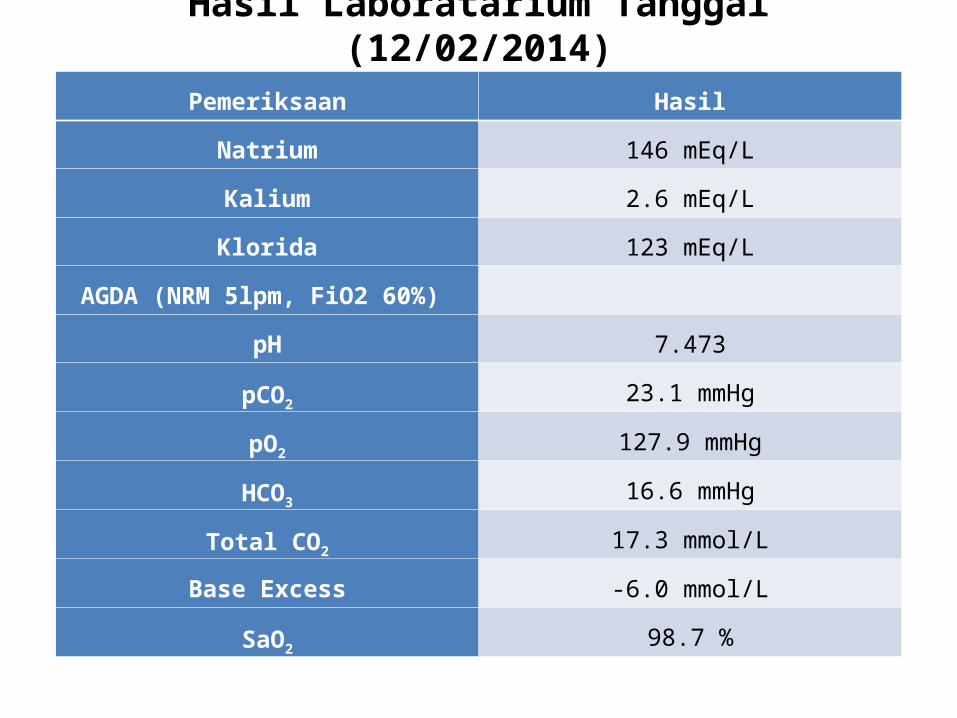
Hasil Laboratarium Tanggal (12/02/2014)
Pemeriksaan Hasil
Natrium 146 mEq/L
Kalium 2.6 mEq/L
Klorida 123 mEq/L
AGDA (NRM 5lpm, FiO2 60%)
pH 7.473
pCO2 23.1 mmHg
pO2 127.9 mmHg
HCO3 16.6 mmHg
Total CO2 17.3 mmol/L
Base Excess -6.0 mmol/L
SaO2 98.7 %
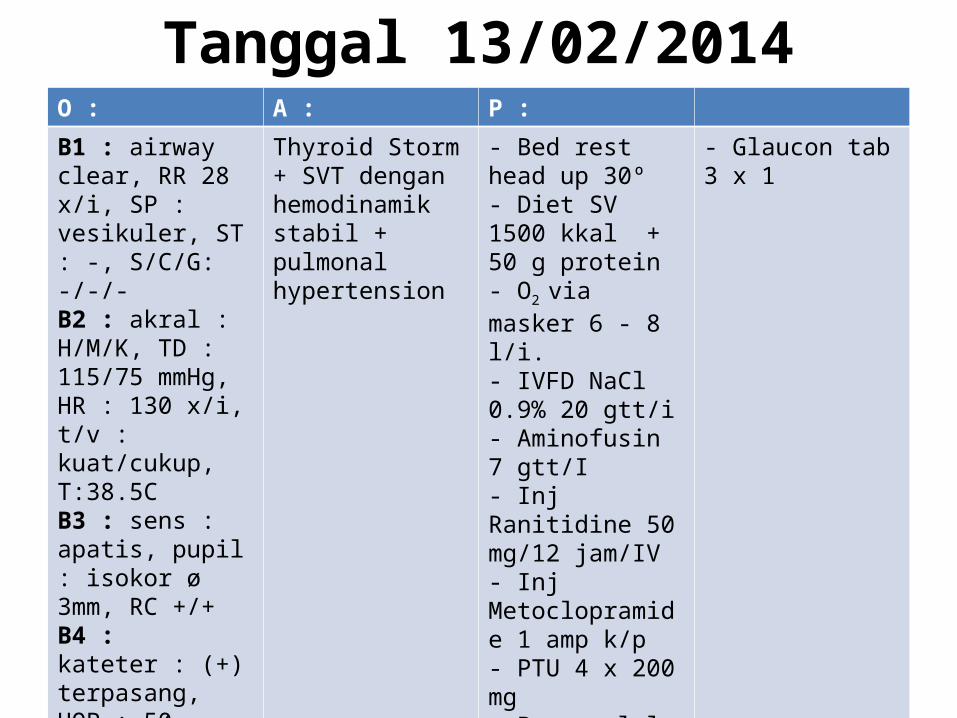
Tanggal 13/02/2014O : A : P :B1 : airway clear, RR 28 x/i, SP : vesikuler, ST : -, S/C/G: -/-/-B2 : akral : H/M/K, TD : 115/75 mmHg, HR : 130 x/i, t/v : kuat/cukup, T:38.5CB3 : sens : apatis, pupil : isokor ø 3mm, RC +/+B4 : kateter : (+) terpasang, UOP : 50 cc/jam, warna : kuning jernihB5 : abdomen : soepel, peristaltik (+) NB6 : oedem (-)
Thyroid Storm + SVT dengan hemodinamik stabil + pulmonal hypertension
- Bed rest head up 30º- Diet SV 1500 kkal + 50 g protein- O2 via masker 6 - 8 l/i.- IVFD NaCl 0.9% 20 gtt/i- Aminofusin 7 gtt/I - Inj Ranitidine 50 mg/12 jam/IV- Inj Metoclopramide 1 amp k/p- PTU 4 x 200 mg - Propanolol 3 x 100 mg
- Glaucon tab 3 x 1
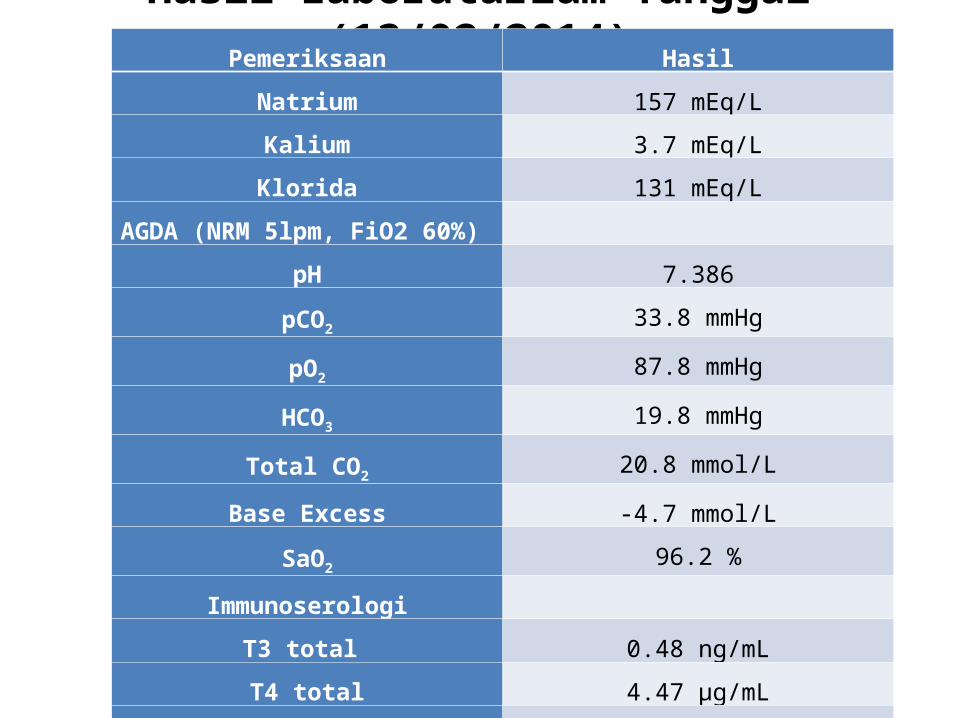
Hasil Laboratarium Tanggal (13/02/2014)Pemeriksaan Hasil
Natrium 157 mEq/L
Kalium 3.7 mEq/L
Klorida 131 mEq/L
AGDA (NRM 5lpm, FiO2 60%)
pH 7.386
pCO2 33.8 mmHg
pO2 87.8 mmHg
HCO3 19.8 mmHg
Total CO2 20.8 mmol/L
Base Excess -4.7 mmol/L
SaO2 96.2 %
Immunoserologi
T3 total 0.48 ng/mL
T4 total 4.47 µg/mL
TSH 0.005 µg/mL
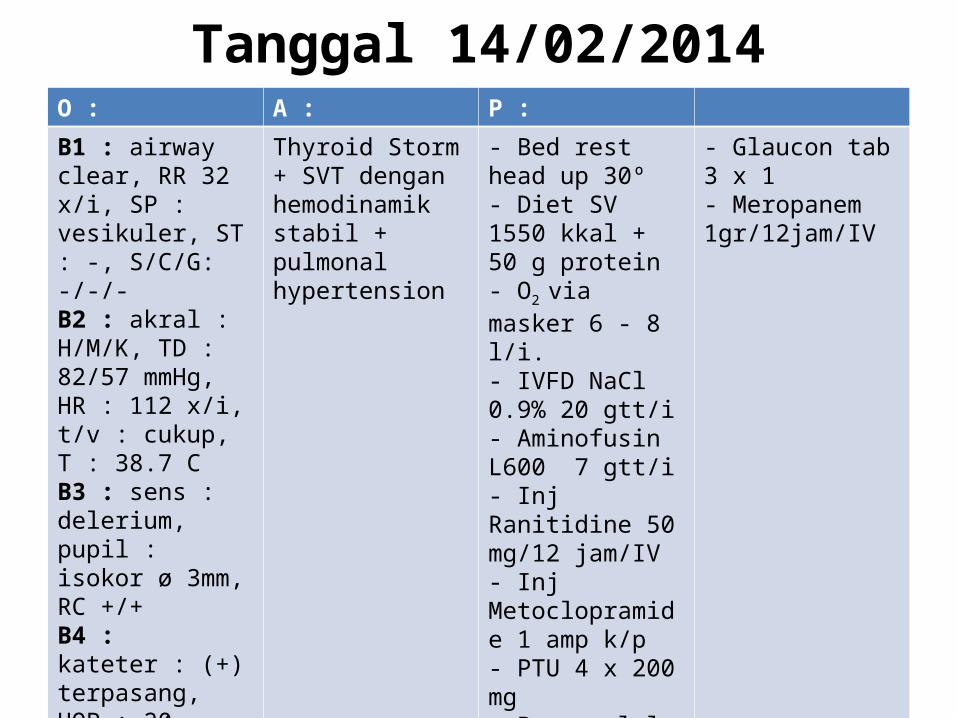
Tanggal 14/02/2014O : A : P :B1 : airway clear, RR 32 x/i, SP : vesikuler, ST : -, S/C/G: -/-/-B2 : akral : H/M/K, TD : 82/57 mmHg, HR : 112 x/i, t/v : cukup, T : 38.7 CB3 : sens : delerium, pupil : isokor ø 3mm, RC +/+B4 : kateter : (+) terpasang, UOP : 20 cc/jam, warna : kuning jernihB5 : abdomen : soepel, peristaltik (+) NB6 : oedem (-)
Thyroid Storm + SVT dengan hemodinamik stabil + pulmonal hypertension
- Bed rest head up 30º- Diet SV 1550 kkal + 50 g protein- O2 via masker 6 - 8 l/i.- IVFD NaCl 0.9% 20 gtt/i- Aminofusin L600 7 gtt/i- Inj Ranitidine 50 mg/12 jam/IV- Inj Metoclopramide 1 amp k/p- PTU 4 x 200 mg - Propanolol 3 x 100 mg
- Glaucon tab 3 x 1 - Meropanem 1gr/12jam/IV
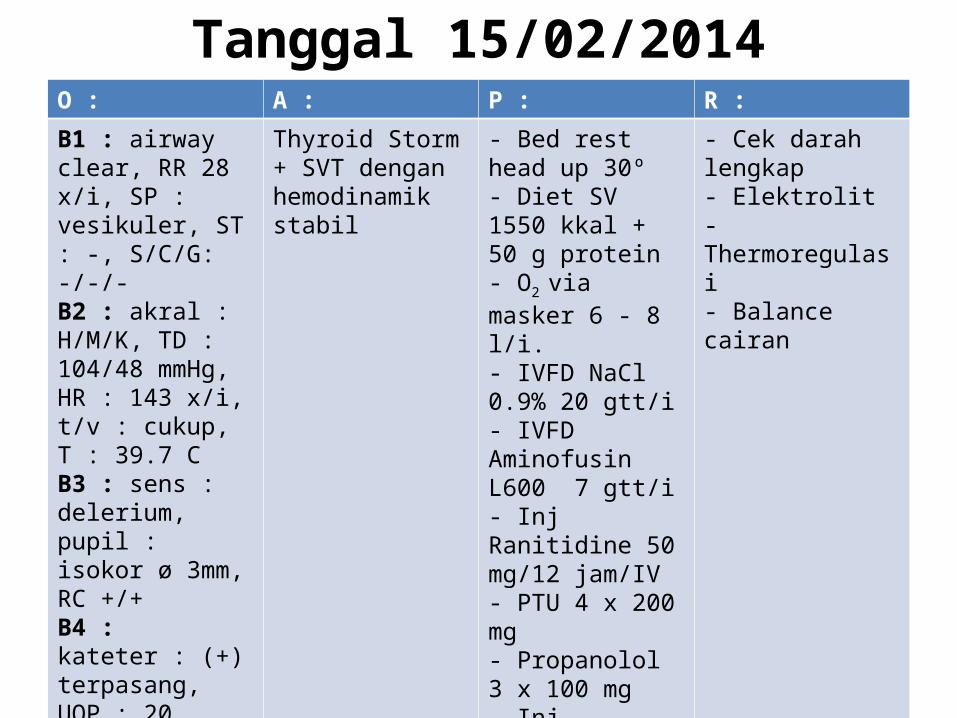
Tanggal 15/02/2014O : A : P : R :B1 : airway clear, RR 28 x/i, SP : vesikuler, ST : -, S/C/G: -/-/-B2 : akral : H/M/K, TD : 104/48 mmHg, HR : 143 x/i, t/v : cukup, T : 39.7 CB3 : sens : delerium, pupil : isokor ø 3mm, RC +/+B4 : kateter : (+) terpasang, UOP : 20 cc/jam, warna : kuning jernihB5 : abdomen : soepel, peristaltik (+) NB6 : oedem (-)
Thyroid Storm + SVT dengan hemodinamik stabil
- Bed rest head up 30º- Diet SV 1550 kkal + 50 g protein- O2 via masker 6 - 8 l/i.- IVFD NaCl 0.9% 20 gtt/i- IVFD Aminofusin L600 7 gtt/i- Inj Ranitidine 50 mg/12 jam/IV- PTU 4 x 200 mg - Propanolol 3 x 100 mg- Inj Methylprednisolon 125 mg/8 jam/IV - Glaucon tab 3 x 1 - Meropanem 1gr/12jam/IV
- Cek darah lengkap - Elektrolit- Thermoregulasi- Balance cairan
Related Documents