Phase Ib Dose - Finding Study of Axitinib Plus Pembrolizumab in Treatment - Naïve Patients With Advanced Renal Cell Carcinoma TK Choueiri 1 , ER Plimack 2 , S Gupta 3 , I Puzanov 4 , DF McDermott 5 , J Tarazi 6 , S Keefe 7 , B Rosbrook 6 , MB Atkins 8 1 Dana-Farber Cancer Institute, Boston, MA; 2 Fox Chase Cancer Center, Philadelphia, PA; 3 Masonic Cancer Center, University of Minnesota, Minneapolis, MN; 4 Vanderbilt University Medical Center, Nashville, TN; 5 Beth Israel Deaconess Medical Center, Boston, MA; 6 Pfizer Oncology, San Diego, CA; 7 Merck & Co., Inc., Kenilworth, NJ; 8 Georgetown-Lombardi Comprehensive Cancer Center, Washington, DC Kidney Cancer Association 14th International Symposium, November 6–7, 2015, Miami, FL

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Phase Ib Dose-Finding Study of Axitinib Plus
Pembrolizumab in Treatment-Naïve Patients
With Advanced Renal Cell Carcinoma
TK Choueiri1, ER Plimack2, S Gupta3, I Puzanov4,
DF McDermott5, J Tarazi6, S Keefe7, B Rosbrook6, MB Atkins8
1Dana-Farber Cancer Institute, Boston, MA; 2Fox Chase Cancer Center, Philadelphia, PA;3Masonic Cancer Center, University of Minnesota, Minneapolis, MN; 4Vanderbilt University
Medical Center, Nashville, TN; 5Beth Israel Deaconess Medical Center, Boston, MA; 6Pfizer Oncology, San Diego, CA; 7Merck & Co., Inc., Kenilworth, NJ;
8Georgetown-Lombardi Comprehensive Cancer Center, Washington, DC
Kidney Cancer Association 14th International Symposium, November 6–7, 2015, Miami, FL
Disclosures
2
● TK Choueiri has received institutional research funding
from Pfizer and has an advisory role at Pfizer, Novartis,
GlaxoSmithKline, Genentech, Merck, Bayer, and Onyx
Background
3
1. Grepin R, Pages G. J Oncol 2010;2010:1-8.
2. Bergers G, Hanahan D. Nature Rev Cancer 2008;8:592-603.
3. Hutson TE, et al. Lancet Oncol 2013;14:1287-94.
4. Rini BI, et al. Lancet Oncol 2013;14(12):1233-42.
5. Motzer RJ, et al. N Engl J Med. 2015 Sep 25 [Epub ahead of print].
6. Atkins MB, et al J Clin Oncol 2015;33 (suppl; abstr 3009).
● Most patients with renal cell carcinoma (RCC) treated
with vascular endothelial growth factor receptor
(VEGFR) inhibitors eventually progress on therapy.1,2
● Axitinib, an inhibitor of VEGFR 1–3, is approved for
2nd-line treatment of advanced RCC and has shown
clinical activity and an acceptable safety profile in the
first-line setting.3,4
● Agents that block the PD-1/PD-L1 interaction have
shown efficacy in patients whose disease has
progressed following VEGF-pathway inhibitor therapy.5
● Pembrolizumab inhibits PD-1 and has antitumor activity
in several malignancies, including RCC.6
Background (II)
4
● We hypothesize that a combination therapy regimen of
axitinib plus pembrolizumab may provide clinical
benefit in treatment-naïve patients with advanced RCC
vs VEGF-pathway–directed therapy alone.
● This ongoing, open-label phase Ib, multicenter study*
consists of a dose-finding phase to determine the maximum
tolerated dose (MTD) and a dose-expansion phase.
● The primary objectives:
● To assess the safety and tolerability of axitinib plus
pembrolizumab in treatment-naïve patients with advanced RCC.
● To estimate MTD and select the recommended Phase 2 dose
(RP2D).
● Here we report the results from the dose-finding phase.
* ClinicalTrials.gov identifier: NCT02133742
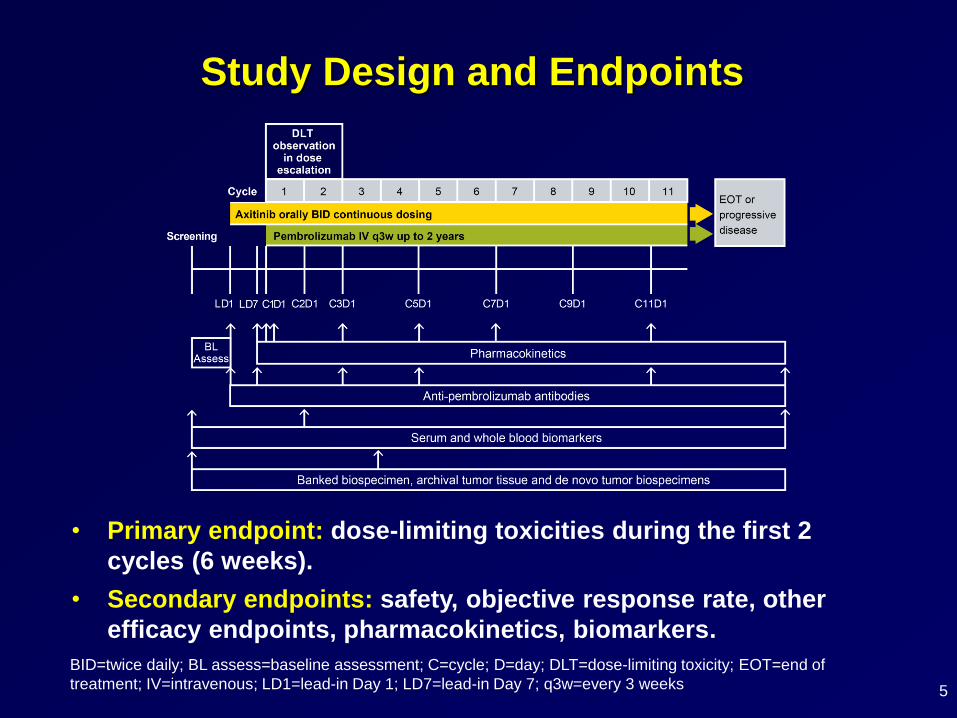
Study Design and Endpoints
5
BID=twice daily; BL assess=baseline assessment; C=cycle; D=day; DLT=dose-limiting toxicity; EOT=end of
treatment; IV=intravenous; LD1=lead-in Day 1; LD7=lead-in Day 7; q3w=every 3 weeks
• Primary endpoint: dose-limiting toxicities during the first 2
cycles (6 weeks).
• Secondary endpoints: safety, objective response rate, other
efficacy endpoints, pharmacokinetics, biomarkers.
Patient Population
6
● Histologically or cytologically confirmed clear-cell
advanced RCC with primary tumor resected.
● Mandatory archival tumor biospecimen.
● ≥1 measureable lesion, as defined by RECIST v1.1.
● ECOG performance status 0 or 1.
● Controlled hypertension.
ECOG PS=Eastern Cooperative Oncology Group performance status; RCC=renal cell carcinoma;
RECIST=Response Evaluation Criteria in Solid Tumors
Key inclusion criteria
Key exclusion criteria
● Prior treatment with systemic therapy for advanced
RCC.
Treatment
7
● Axitinib 5 mg BID orally (starting dose) beginning on Day –7.
● Pembrolizumab 2 mg/kg IV q3w up to 2 years.
● Dose levels (DL)
DL 1: axitinib 5 mg BID + pembrolizumab 2 mg/kg q3w.
DL –1 (if DL 1 beyond MTD): axitinib 3 mg BID +
pembrolizumab 2 mg/kg q3w.
● Dose-finding component of the trial is completed when 10
DLT-evaluable patients have been treated at the highest dose
of axitinib + pembrolizumab associated with DLT rate <0.33.
● Treatment continues until confirmed disease progression or
unacceptable toxicity.
BID=twice daily; DL= dose level; DLT= dose-limiting toxicity; IV=intravenous; q3w= 3-week cycle ;
MTD=maximum tolerated dose.
DLT Definition
8
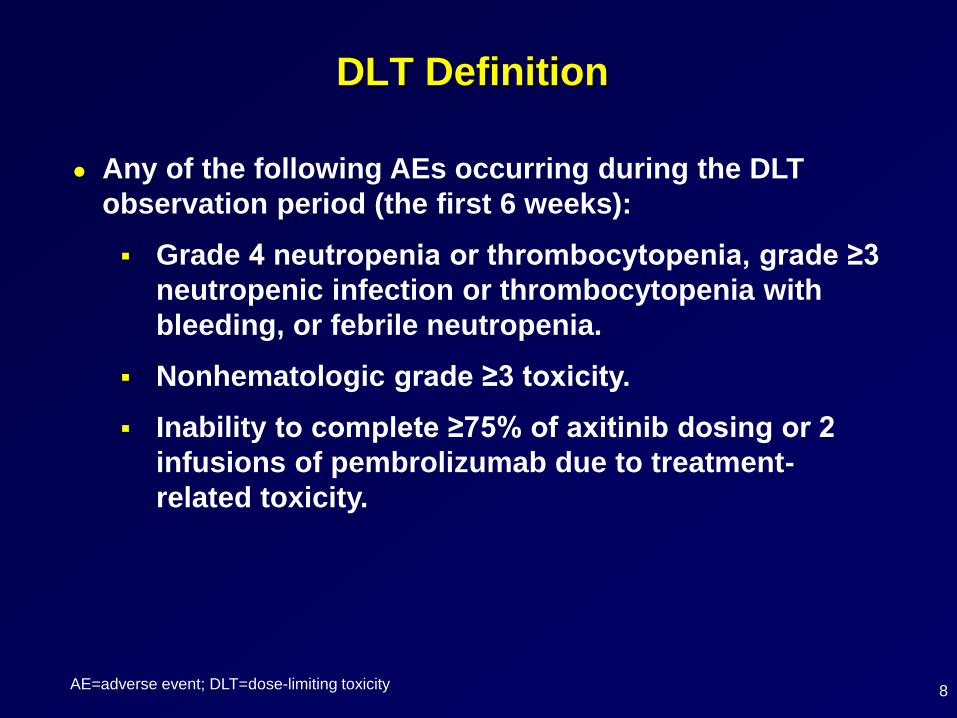
● Any of the following AEs occurring during the DLT
observation period (the first 6 weeks):
Grade 4 neutropenia or thrombocytopenia, grade ≥3
neutropenic infection or thrombocytopenia with
bleeding, or febrile neutropenia.
Nonhematologic grade ≥3 toxicity.
Inability to complete ≥75% of axitinib dosing or 2
infusions of pembrolizumab due to treatment-
related toxicity.
AE=adverse event; DLT=dose-limiting toxicity
Results: Patients
9
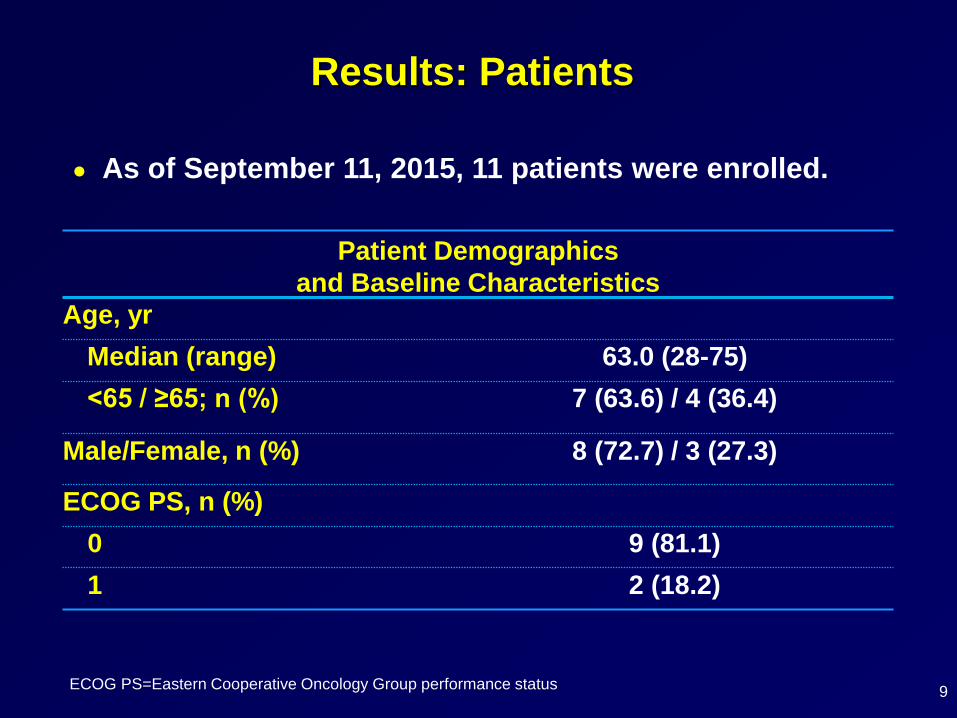
● As of September 11, 2015, 11 patients were enrolled.
Patient Demographics
and Baseline Characteristics
Age, yr
Median (range) 63.0 (28-75)
<65 / ≥65; n (%) 7 (63.6) / 4 (36.4)
Male/Female, n (%) 8 (72.7) / 3 (27.3)
ECOG PS, n (%)
0 9 (81.1)
1 2 (18.2)
ECOG PS=Eastern Cooperative Oncology Group performance status
DLTs
10
● 3 DLTs were reported: transient ischemic attack (n=1)
and <75% of planned axitinib dose received due to
treatment-related toxicity (n=2).
● MTD was determined to be axitinib 5 mg BID +
pembrolizumab 2 mg/kg q3w.
● 9 patients remain on treatment and without confirmed
progression.
BID=twice daily; DLT=dose-limiting toxicity; MTD=maximum tolerated dose; q3w=3-week cycle;
RP2D=recommended phase II dose
Administered Dose and Duration of Treatment
11
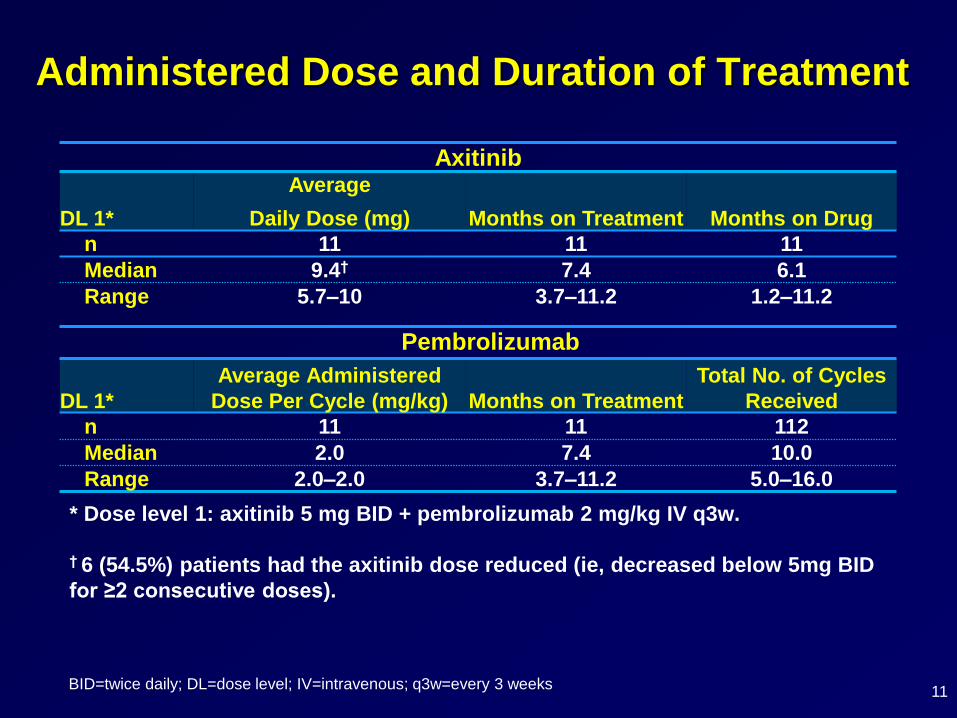
Axitinib
DL 1*
Average
Daily Dose (mg) Months on Treatment Months on Drug
n 11 11 11
Median 9.4† 7.4 6.1
Range 5.7–10 3.7–11.2 1.2–11.2
Pembrolizumab
DL 1*
Average Administered
Dose Per Cycle (mg/kg) Months on Treatment
Total No. of Cycles
Received
n 11 11 112
Median 2.0 7.4 10.0
Range 2.0–2.0 3.7–11.2 5.0–16.0
BID=twice daily; DL=dose level; IV=intravenous; q3w=every 3 weeks
* Dose level 1: axitinib 5 mg BID + pembrolizumab 2 mg/kg IV q3w.
† 6 (54.5%) patients had the axitinib dose reduced (ie, decreased below 5mg BID
for ≥2 consecutive doses).
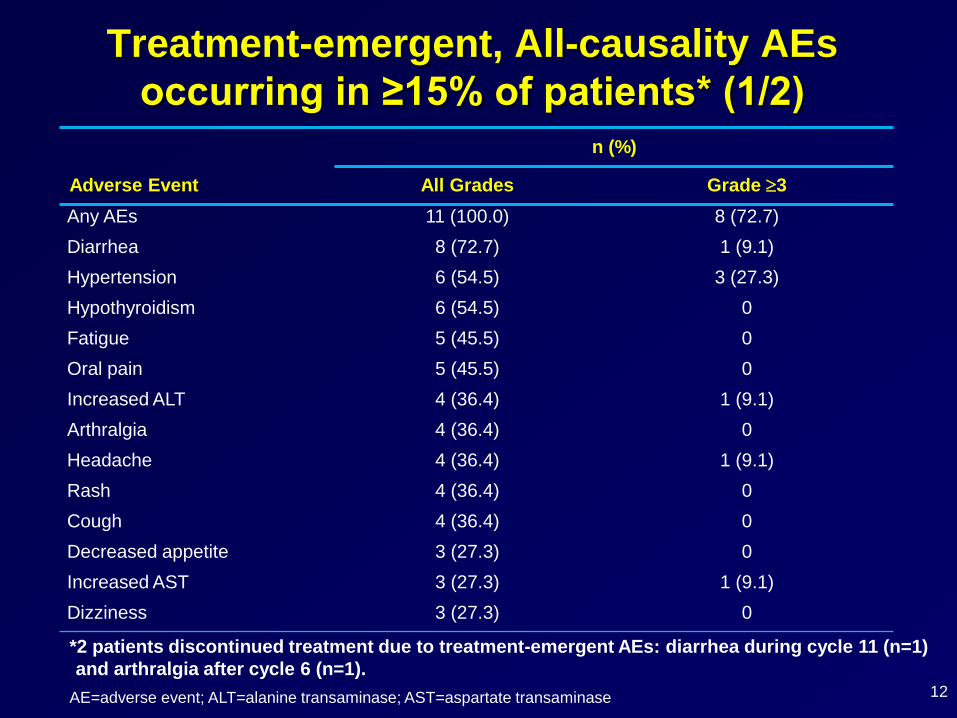
Treatment-emergent, All-causality AEs
occurring in ≥15% of patients* (1/2)
12
n (%)
Adverse Event All Grades Grade 3
Any AEs 11 (100.0) 8 (72.7)
Diarrhea 8 (72.7) 1 (9.1)
Hypertension 6 (54.5) 3 (27.3)
Hypothyroidism 6 (54.5) 0
Fatigue 5 (45.5) 0
Oral pain 5 (45.5) 0
Increased ALT 4 (36.4) 1 (9.1)
Arthralgia 4 (36.4) 0
Headache 4 (36.4) 1 (9.1)
Rash 4 (36.4) 0
Cough 4 (36.4) 0
Decreased appetite 3 (27.3) 0
Increased AST 3 (27.3) 1 (9.1)
Dizziness 3 (27.3) 0
AE=adverse event; ALT=alanine transaminase; AST=aspartate transaminase
*2 patients discontinued treatment due to treatment-emergent AEs: diarrhea during cycle 11 (n=1)
and arthralgia after cycle 6 (n=1).
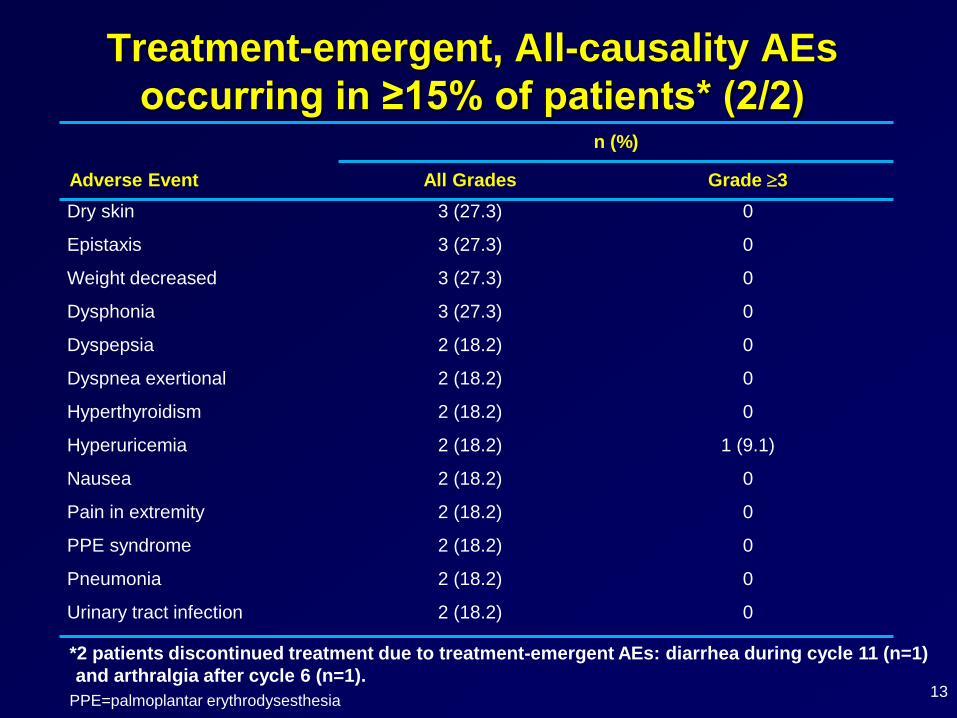
Treatment-emergent, All-causality AEs
occurring in ≥15% of patients* (2/2)
13
n (%)
Adverse Event All Grades Grade 3
Dry skin 3 (27.3) 0
Epistaxis 3 (27.3) 0
Weight decreased 3 (27.3) 0
Dysphonia 3 (27.3) 0
Dyspepsia 2 (18.2) 0
Dyspnea exertional 2 (18.2) 0
Hyperthyroidism 2 (18.2) 0
Hyperuricemia 2 (18.2) 1 (9.1)
Nausea 2 (18.2) 0
Pain in extremity 2 (18.2) 0
PPE syndrome 2 (18.2) 0
Pneumonia 2 (18.2) 0
Urinary tract infection 2 (18.2) 0
PPE=palmoplantar erythrodysesthesia
*2 patients discontinued treatment due to treatment-emergent AEs: diarrhea during cycle 11 (n=1)
and arthralgia after cycle 6 (n=1).
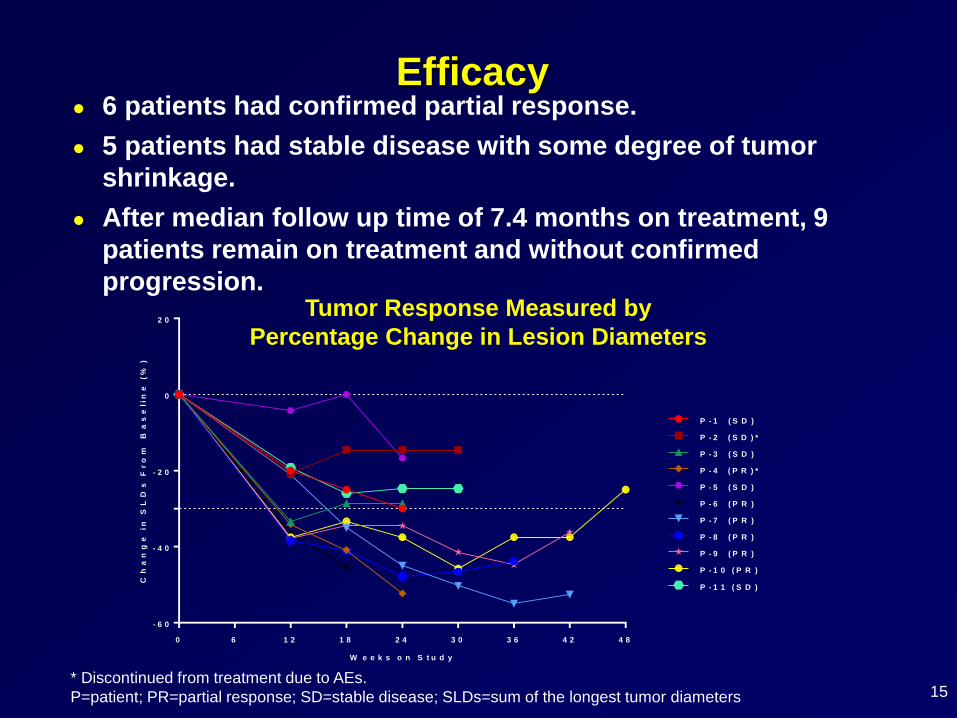
Efficacy● 6 patients had confirmed partial response.
● 5 patients had stable disease with some degree of tumor
shrinkage.
● After median follow up time of 7.4 months on treatment, 9
patients remain on treatment and without confirmed
progression.Tumor Response Measured by
Percentage Change in Lesion Diameters
* Discontinued from treatment due to AEs.
P=patient; PR=partial response; SD=stable disease; SLDs=sum of the longest tumor diameters
0 6 1 2 1 8 2 4 3 0 3 6 4 2 4 8
- 6 0
- 4 0
- 2 0
0
2 0
W e e k s o n S t u d y
Ch
an
ge
in
S
LD
s F
ro
m B
as
elin
e (
%)
P - 1 ( S D )
P - 2 ( S D ) *
P - 6 ( P R )
P - 3 ( S D )
P - 4 ( P R ) *
P - 5 ( S D )
P - 7 ( P R )
P - 8 ( P R )
P - 9 ( P R )
P - 1 0 ( P R )
P - 1 1 ( S D )
15
Conclusions
15
● Preliminary results indicate combination axitinib plus
pembrolizumab is well tolerated at standard doses of
each agent and exhibits antitumor activity in treatment-
naïve patients with advanced RCC.
● There were no treatment discontinuations due to
hepatotoxicity.
● Enrollment completed with 41 additional patients
enrolled in the dose expansion phase to confirm the
RP2D and further evaluate safety and antitumor activity
of this combination.
Acknowledgments
● This study is sponsored by Pfizer Inc and
Merck & Co., Inc.
● Medical writing support was provided by Vardit Dror,
PhD, of Engage Scientific Solutions, and was funded
by Pfizer.
Related Documents