Pediatric TB and Child Health Programming: Woefully Underdeveloped. Why, and What to Do? Devasena Gnanashanmugam, M.D. Consultant, CORE Group

Pediatric TB and child health programming_Gnanashanmuga_5.2.12m
Jun 20, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Pediatric TB and Child Health Programming: Woefully Underdeveloped. Why, and What to
Do?
Devasena Gnanashanmugam, M.D.Consultant, CORE Group

Goals of this discussion
• Overview of Childhood TB disease• How TB in children interfaces with other areas• Current challenges• Current recommended action• YOUR SUGGESTIONS

Focused Approach (“TB- centric”)
NCD
Maternal Health
Child Health
Environment
Education
Communicable Diseases
HIV
TB
Malaria
NTDs
Pediatric TB
Poverty
Nutrition Other

Global Health
Infectious Disease Burden
TBChild Health
Pediatric TB
Broad Approach
Malnutrition
Maternal health
Poverty
Education

Pediatric TB: How big is this problem?
• AT LEAST 500,000 cases of TB in children each year (likely more)
• AT LEAST 70,000 deaths each year• About 15% of global TB burden is due to
disease in children (higher & lower in some regions)
• Why don’t we have better data?

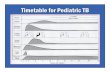
Clinical TBPrimary pulmonary infection
Miliary TB/ Meningitis/ other extrapulmonary forms
Primary pulmonary disease
Child
Well Adult
Successful Immune Response
Immunity (live MTB)
Spread by lymph/ blood
Exposure
Adapted from Kampmann 2011
Low bacterial burden
Late Reactivation of pulmonary disease
Higher bacterial burden
Future pool of TB disease

Child vs. Adult TBAdults• Disease develops
after years• Adults less
vulnerable to severe forms
• Disease in adults will manifest later in an epidemic
Children• Develop disease RAPIDLY
(weeks to months) after infection
• Disease can be crippling in children
• Deterioration in TB control impacts the youngest generation first
What is the same:• INH preventive therapy (IPT) can be given to prevent disease those who are
infected• Treatment is still many months of 4 (then 2) drugs

Childhood TB Neglected
“Pediatric TB is a public health dead end.”– Sentinel event: reflects recent infection &
transmission in the community – Window on transmission dynamics– Harbinger of future epidemics – Indicator of the effectiveness of control efforts

Childhood TB Neglected
“Treating adults with TB is enough to control TB in children”– Future reservoir of disease predicts the future global
TB burden– After transmission is over, treating adults is not helpful– Improving treatment in children largest impact on
disease control in children– Reducing long term trends of global TB must account for
disease in children – Millions of children would become sick while we wait
for adult TB control

Child Survival & TB
Mortality• 2nd leading cause of
death in Kolkata slum
• TB control decreases <5 yr mortality
TB?
Pneumonia• 8-15% of pneumonia
may be TB• Autopsies: 18-25%
pneumonia deaths

TB causes 6-15% of all maternal mortality
TB is a leading infectious cause of death in women.
TB in pregnant women increases HIV transmission
to the baby
Newborns of women with TB are at high risk of contracting
TB
HIV/TB infected women are twice as likely to die than HIV
infected women without TB
Babies born to HIV/TB infected women are
more likely to die than those of HIV women
without TB
Maternal Health & TB

Malnutrition predisposes to TB & makes TB worse
TB looks like malnutrition and makes malnutrition worse
• TB: 12-30% of cases of malnutrition
• TB: a catabolic process wasting (before diagnosis)
• TB Rx results in weight gain & improves nutritional states
• Malnutrition treatment guidelines to emphasize diagnosis of HIV + TB • Supplemental
nutrition improves health in TB patients
• Supplemental nutrition for TB programs could reduce incidence of active TB
Increased wasting results
in increased mortality
Malnutrition & TB

TB fuels poverty
Strongest risk factor for
childhood TB
Those treated for TB fall deeper into
poverty
TB left 10 million children orphaned
in 2010
Children no longer educated
Loss of family members
Children more susceptible to
TB
Close contact with infectious people
Overcrowding Poor nutrition
MEN: can no longer work and contribute to the
family
WOMEN: unable to care for children
Family cannot afford school fees/ uniforms
Children need to work to assist families

Risk of active TB is 5- 20x higher in
HIV infected children
More than 1/3 HIV infected children will die of TB compared
to <10% of HIV negative children
Risk of death due to TB is 5-6x more in
HIV infected children.
Youngest children have
highest mortality
TB is more difficult to diagnose in HIV infected children
Children with HIV & TB

Disaster Management
Converging epidemics
HIV
Malnutrition TB
Less than 5 years
old

Science
• Union Child Health Lung Section
• STOP TB Childhood TB subgroup
• CDC• WHO TB
website
Policy
• WHO guidance for NTPs
• WHO Rapid Advice on Treatment of TB in children
• UNION Desk guide
Practice…
- National programs to integrate pediatric guidances
- Research to develop more tools
Where are we now?

R&D challenges and needs
Challenges• BCG vaccine is poor• Diagnostic tests do not
detect disease reliably in children
• Pediatric drug formulations are lacking
• Children are not included in clinical trials
Needs• Better vaccine• Child appropriate
diagnostics• Child friendly
drugs• More clinical &
operational research

What can we do now?
• Perform contact investigation in all children exposed to TB
• Provide IPT to those <5 yrs who meet criteria
“Simple changes in detection and treatment of children with TB exposure and infection could save millions of lives.” J. Starke

Other items on the wish list
• Provide more data on scale and scope of disease• Provide family centered care, including household
focused case investigation• Integrate TB care within IMCI• Increase awareness building and advocacy to policy
makers, practitioners, scholars & donors• More training & knowledge building on childhood TB• Integrate TB services into existing MCH programs• Increased community level programming

Programs that have worked
• Indus Hospital, Pakistan (TB REACH/ STOP TB partnership grant)– Strengthened PPM– Approached CHWs & GPs to increase case detection– Used cash, training certificates, free diagnostic tests & free Rx as incentives– Used mobile technologies to increase case detection– Increased notification of children by 500%
• Dhaka, Bangladesh (Damien Foundation)– Community based screening of pediatric TB– CHWs & other clinicians trained to detect S/S of TB & make referrals– Community awareness building– Logistical support– Increased case detection in children 3x baseline levels
• MSF programs
• OperationASHAhttp://www.coregroup.org/our-technical-work/working-groups/tuberculosis/pediatrictb

Practical Examples of Action Items • Create & disseminate community education materials about pediatric
TB• Within MCH program, design and integrate educational materials and
systems designed to help prevent mother-to-child transmission of TB • Adapt a pediatric TB screening tool to support community-level case
finding and referral. • Within an IMCI, immunization or other child health effort, add
education and linkages related to childhood TB. • Add household TB contact tracing component to community health
portfolios• Advocate for government health service adoption of WHO guidelines
regarding pediatric TB (This is especially important in high HIV settings)
• Address the problem of TB and stigma, specifically in relation to children.

Your suggestions & comments…
Related Documents

![Pediatric TB radiographsnid]/05a...1 Pediatric TB radiographs Ann M. Loeffler, MD Curry International Tuberculosis Center Radiology Best quality frontal and lateral views of the chest](https://static.cupdf.com/doc/110x72/609633be3922801af21c02d2/pediatric-tb-radiographs-nid05a-1-pediatric-tb-radiographs-ann-m-loeffler.jpg)