Volume 29 Issue 1 Article 2 2017 Molar Distalization by Temporary Anchorage Devices (TAD s) – A Molar Distalization by Temporary Anchorage Devices (TAD s) – A Review Article Review Article Jun Ming Tan Postgraduate Student, Division of Orthodontic and Dentofacial Orthopedic, Department of Dentistry, National Taiwan University Hospital; Graduate Institute of Clinical Dentistry, School of Dentistry, National Taiwan University, [email protected] Yi-Min Liu Adjunct Attending Physician, Division of Orthodontic and Dentofacial Orthopedic, Department of Dentistry, National Taiwan University Hospital Hung-Cheng Chiu Adjunct Attending Physician, Division of Orthodontic and Dentofacial Orthopedic, Department of Dentistry, National Taiwan University Hospital Yi-Jane Chen Attending Physician, Division of Orthodontic and Dentofacial Orthopedic, Department of Dentistry, National Taiwan University Hospital; Graduate Institute of Clinical Dentistry, School of Dentistry, National Taiwan University Follow this and additional works at: https://www.tjo.org.tw/tjo Part of the Orthodontics and Orthodontology Commons Recommended Citation Recommended Citation Tan, Jun Ming; Liu, Yi-Min; Chiu, Hung-Cheng; and Chen, Yi-Jane (2017) "Molar Distalization by Temporary Anchorage Devices (TAD s) – A Review Article," Taiwanese Journal of Orthodontics: Vol. 29 : Iss. 1 , Article 2. DOI: 10.30036/TJO.201703_29(1).0002 Available at: https://www.tjo.org.tw/tjo/vol29/iss1/2 This Review Article is brought to you for free and open access by Taiwanese Journal of Orthodontics. It has been accepted for inclusion in Taiwanese Journal of Orthodontics by an authorized editor of Taiwanese Journal of Orthodontics.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Volume 29 Issue 1 Article 2
2017
Molar Distalization by Temporary Anchorage Devices (TAD s) – A Molar Distalization by Temporary Anchorage Devices (TAD s) – A
Review Article Review Article
Jun Ming Tan Postgraduate Student, Division of Orthodontic and Dentofacial Orthopedic, Department of Dentistry, National Taiwan University Hospital; Graduate Institute of Clinical Dentistry, School of Dentistry, National Taiwan University, [email protected]
Yi-Min Liu Adjunct Attending Physician, Division of Orthodontic and Dentofacial Orthopedic, Department of Dentistry, National Taiwan University Hospital
Hung-Cheng Chiu Adjunct Attending Physician, Division of Orthodontic and Dentofacial Orthopedic, Department of Dentistry, National Taiwan University Hospital
Yi-Jane Chen Attending Physician, Division of Orthodontic and Dentofacial Orthopedic, Department of Dentistry, National Taiwan University Hospital; Graduate Institute of Clinical Dentistry, School of Dentistry, National Taiwan University
Follow this and additional works at: https://www.tjo.org.tw/tjo
Part of the Orthodontics and Orthodontology Commons
Recommended Citation Recommended Citation Tan, Jun Ming; Liu, Yi-Min; Chiu, Hung-Cheng; and Chen, Yi-Jane (2017) "Molar Distalization by Temporary Anchorage Devices (TAD s) – A Review Article," Taiwanese Journal of Orthodontics: Vol. 29 : Iss. 1 , Article 2. DOI: 10.30036/TJO.201703_29(1).0002 Available at: https://www.tjo.org.tw/tjo/vol29/iss1/2
This Review Article is brought to you for free and open access by Taiwanese Journal of Orthodontics. It has been accepted for inclusion in Taiwanese Journal of Orthodontics by an authorized editor of Taiwanese Journal of Orthodontics.

8 Taiwanese Journal of Orthodontics. 2017, Vol. 29. No. 1
Review Article
Clinically, there are many ways to achieve molar distalization, such as skeletal anchorage, extraoral
anchorage, sliding jig, lip bumper, and pendulum, etc. Although several methods have been described to distalize
molars or total dentition, there is no strong scientific evidence of the effectiveness of various methods. To date,
temporary anchorage devices (TADs) are increasingly used as orthodontic anchorage sources because of its
strong anchorage, including endoosseous implants, miniplates, miniscrews and microscrews. Application of bony
anchorage makes teeth move more efficiently, without depending on patient compliance in wearing appliance.
However, only case reports and small case series have been published on the benefits of TADs in molar
distalization. Thus, the purpose of this study was to review the papers on methods of molar distalization with
use of TADs, potential side effects, and possible range of distalization. (Taiwanese Journal of Orthodontics.
29(1): 8-15, 2017)
Keywords: Molar Distalization; Temporary Anchorage Devices (TADs); Review Article
molar disTalizaTion by Temporary anchorage devices (Tads) – a review arTicle
Jun Ming Tan,1,4
Yi-Min Liu,2 Hung-Cheng Chiu,
2 Yi-Jane Chen,
3,4
1Postgraduate Student, Division of Orthodontic and Dentofacial Orthopedic,
Department of Dentistry, National Taiwan University Hospital2Adjunct Attending Physician, Division of Orthodontic and Dentofacial Orthopedic,
Department of Dentistry, National Taiwan University Hospital3Attending Physician, Division of Orthodontic and Dentofacial Orthopedic,
Department of Dentistry, National Taiwan University Hospital4Graduate Institute of Clinical Dentistry, School of Dentistry, National Taiwan University
Received: Stepmber 22, 2016 Revised: March 10, 2017 Accepted: March 13, 2017Reprints and correspondence to: Dr. Jun Ming Tan, No.1, Chang Te St., Zhongzheng Dist., Taipei City 100, Taiwan Tel: 02-23562347 E-mail: [email protected]
complaint of protrusive maxillary dentition with lip
protrusion, crowding of teeth, etc. In such circumstances,
the major orthodontic goal is to reduce the proclination
of the maxillary incisors and to gain space for crowding
teeth. Thus, the treatment plan often includes extraction
of bilateral premolars, followed by retraction of anterior
teeth with maximum anchorage.1 In some circumstances,
non-extraction treatment is planned in combination with
total arch distalization or molar distalization.
INTRODUCTION
Nowadays, facial esthetics has become a major
concern of many orthodontic patients. Especially the
alignment and angulation of maxillary anterior teeth
plays an important role in defining beauty and facial
harmony. Excessive labioversion of maxillary teeth
and crowding of teeth can ruin a pleasing smile. Many
patients seek for orthodontic treatment with the chief

9Taiwanese Journal of Orthodontics. 2017, Vol. 29. No. 1
Molar Distalization by TADs
1. Miniscrew Implant Supported Distalization Device
Papadopoulos in t roduced the Miniscrew
Implant Supported Distalization System (MISDS)
in 2008 (Figure 1, A).3 This appliance comprised
two miniscrew implants in the paramedian region
of the palate. The distalization force was applied by
the palatally positioned open nickel-titanium coil
springs, which passed through the center of resistance
of the maxillary molars. Squeezing the coil springs
and screwing the anteriorly positioned stop screws
following cementation activated the appliance.
Sar et al. compared the effects of the MISDS
and the Bone-Anchored Pendulum Appliance (BAPA)
(Figure 1, B)—for maxillary molar distalization and
evaluated the efficacy of two distalizing forces (Table
1).4 Some unwanted side effects were found with
implant-supported molar distalization appliances,
such as distal crown tipping accompanying molar
distalization. The point of force application passed
When non-extraction treatment plan is chosen, there
are several approaches to achieve distalization of arch
or molars, including pendulum, lip bumper, sliding jig,
extraoral anchorage, skeletal anchorage, etc. To date,
Temporary Anchorage Devices (TADs) are increasingly
used as orthodontic anchorage sources because of its
strong anchorage, which can avoid anchorage loss
of premolars and flaring of incisors during molar
distalization.2 Many types of TADs, include endo-osseous
implants, miniplates, miniscrews and microscrews can
provide reliable and stable anchorage to distalize arch
or molars. In this review article, effectiveness of bony
anchorage during distalization will be explored.
RESULTS
A Methods of molar distalization and related side effects
There are several methods to distalize molars by
using mini-implants, as follows,
Table I. Comparison between MISDS and BAPA in Sar et al.’ study
MISDS BAPASample Sizes 14 14Force applied Apex level Crown levelMolar Distalization (mm) 2.81 2.93Average distalization duration (months) 8.2 10.2Distalization rate (mm / month) 0.2 0.3Type of distalization Nearly bodily movement Crown tipping
Figure 1. A Miniscrew Implant Supported Distalization System(MISDS); B Bone-Anchored Pendulum Appliance (BAPA). From Sar et al., Angle Orthod. 2013 May;83(3):460-7.

10 Taiwanese Journal of Orthodontics. 2017, Vol. 29. No. 1
Tan JM, Liu YM, Chiu HC, Chen YJ
2. Direct use of mini-implants
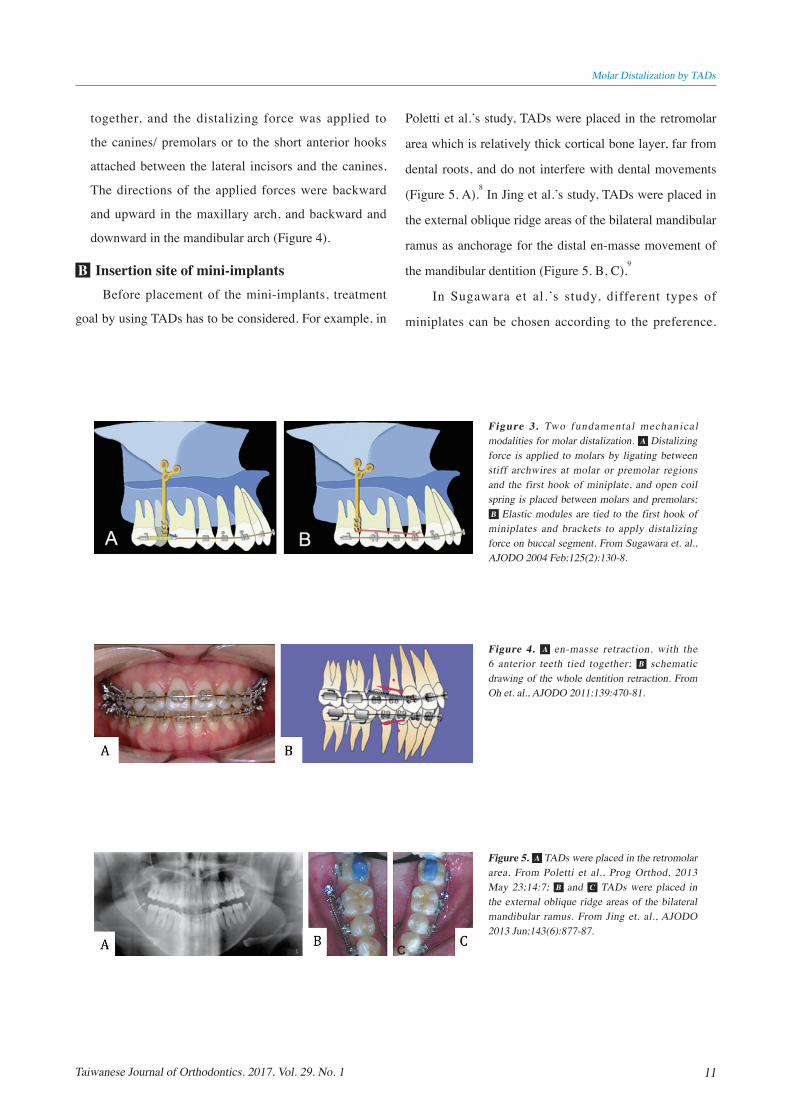
Sugawara et al. demonstrated two fundamental
methods of applying distalizing forces to the subjects in
his study.6 One is for single molar distalization (Figure 3.
A), the other is for en masse distalization (Figure 3. B).
Single Molar Distalization
Enough space for the molar distalization will
be needed. A retractive force is applied to the second
molars with an open coil spring. The first premolars/
first molars must be ligated firmly with TADs to avoid
the side effects of the reciprocal coil spring. After the
distalization of the second molars, distalization of the
first molars is done with the same procedure.
En masse Distalization
Direct retractive force is applied from the TADs to
the first premolars to perform en masse distalization.7
Elastic modules or Ni-Ti closing-coil springs usually
provide the retractive orthodontic force. During
en-masse retraction, the 6 anterior teeth were tied
below the center of resistance of the maxillary molars
in BAPA, whereas it passed through the center of
resistance in MISDS. This might cause clinically more
distal crown tipping in BAPA.
In Kyung et al.’s study,5 two midpalatal miniscrews
were placed. A screw-supported customized S-sheath
was fabricated and cemented on the top of 2 miniscrews
with flowable composite resin, then a removable
hook was placed into the sheath. A mesially extended
transpalatal arch (ME-TPA) was placed in the lingual
sheath of the maxillary first molar. Elastics were placed
from anterior hooks of the ME-TPA to distal hooks
extending from the S-sheath to the TPA (Figure 2. A).
After target was hit, the ME-TPA was replaced with a
modified TPA to maintain the position of the maxillary
first molars (Figure 2. B). When the force was applied
on the palatal side, the molar segment rotated mesially,
and the intermolar width increased. Thus, the ME-TPA
should be activated to counteract these complications
(Figure 2. C).
Figure 2. A A screw-supported S-sheath was fabricated on the palate. Elastics were placed from anterior hooks of the ME-TPA to distal hooks extending from the S-sheath to the TPA; B 7 months after start of treatment; C Complications in distal movements. From Kyung et. al., AJODO. 2009 Apr;135:S123-32.
11Taiwanese Journal of Orthodontics. 2017, Vol. 29. No. 1
Poletti et al.’s study, TADs were placed in the retromolar
area which is relatively thick cortical bone layer, far from
dental roots, and do not interfere with dental movements
(Figure 5. A).8 In Jing et al.’s study, TADs were placed in
the external oblique ridge areas of the bilateral mandibular
ramus as anchorage for the distal en-masse movement of
the mandibular dentition (Figure 5. B, C).9
In Sugawara et al.’s study, different types of
miniplates can be chosen according to the preference.
Molar Distalization by TADs
together, and the distalizing force was applied to
the canines/ premolars or to the short anterior hooks
attached between the lateral incisors and the canines.
The directions of the applied forces were backward
and upward in the maxillary arch, and backward and
downward in the mandibular arch (Figure 4).
B Insertion site of mini-implantsBefore placement of the mini-implants, treatment
goal by using TADs has to be considered. For example, in
Figure 3. Two fundamental mechanical modalities for molar distalization. A Distalizing force is applied to molars by ligating between stiff archwires at molar or premolar regions and the first hook of miniplate, and open coil spring is placed between molars and premolars; B Elastic modules are tied to the first hook of miniplates and brackets to apply distalizing force on buccal segment. From Sugawara et. al., AJODO 2004 Feb;125(2):130-8.
Figure 4. A en-masse retraction, with the 6 anterior teeth tied together; B schematic drawing of the whole dentition retraction. From Oh et. al., AJODO 2011;139:470-81.
Figure 5. A TADs were placed in the retromolar area, From Poletti et al., Prog Orthod. 2013 May 23;14:7; B and C TADs were placed in the external oblique ridge areas of the bilateral mandibular ramus. From Jing et. al., AJODO 2013 Jun;143(6):877-87.

12 Taiwanese Journal of Orthodontics. 2017, Vol. 29. No. 1
Tan JM, Liu YM, Chiu HC, Chen YJ
through the center of resistance of molars. Besides, during
molar distalization treatment, the second molar may
move into the maxillary tuberosity or retromolar region,
where there are abundant attached gingiva. This might
result in pseudopocket around the teeth, particularly on
the distal surface. An end tuft brush is recommended
during and after active orthodontic treatment. Sometimes,
additional periodontal surgery would be needed in cases
which swelling was not subsided during treatment or the
retention period.
E Post-treatment stability of molar distalizationThe post-treatment stability of orthodontic therapy
has been an important issue. Until now, little information
has been available about the post-treatment stability of
orthodontic treatment using implant anchorage. Sugawara
et al. found minimal short-term relapse, and no significant
correlation was found between the amount of relapse and
tipping ratio and the amount of tooth movement.6 Lima
et al. showed 4 years of stable retention after distalization
of the mandibular dentition in the treatment of class III
open bite adult patients.14
Many factors may affect post-
treatment stability, including prolonged or permanent
retention, maintaining pretreatment arch form and
intercanine width, obtaining proper occlusal relationship
and function, and taking into account muscle balance and
harmony.
The implantation sites of the anchor plates required
sufficiently thick cortical bone, at least 2 to 3 mm, to
enable fixation of the anchor plates with monocortical
titanium miniscrews.6 The anchor plates were placed at
the zygomatic buttress where cortical bone is thick enough
to distalize the maxillary molars (Figure 6).
Apart from aforementioned insertion site, there are
still many case reports showing different insertion areas
according to individual’s preferences and considerations,
such as palatal region, interdental area, etc.
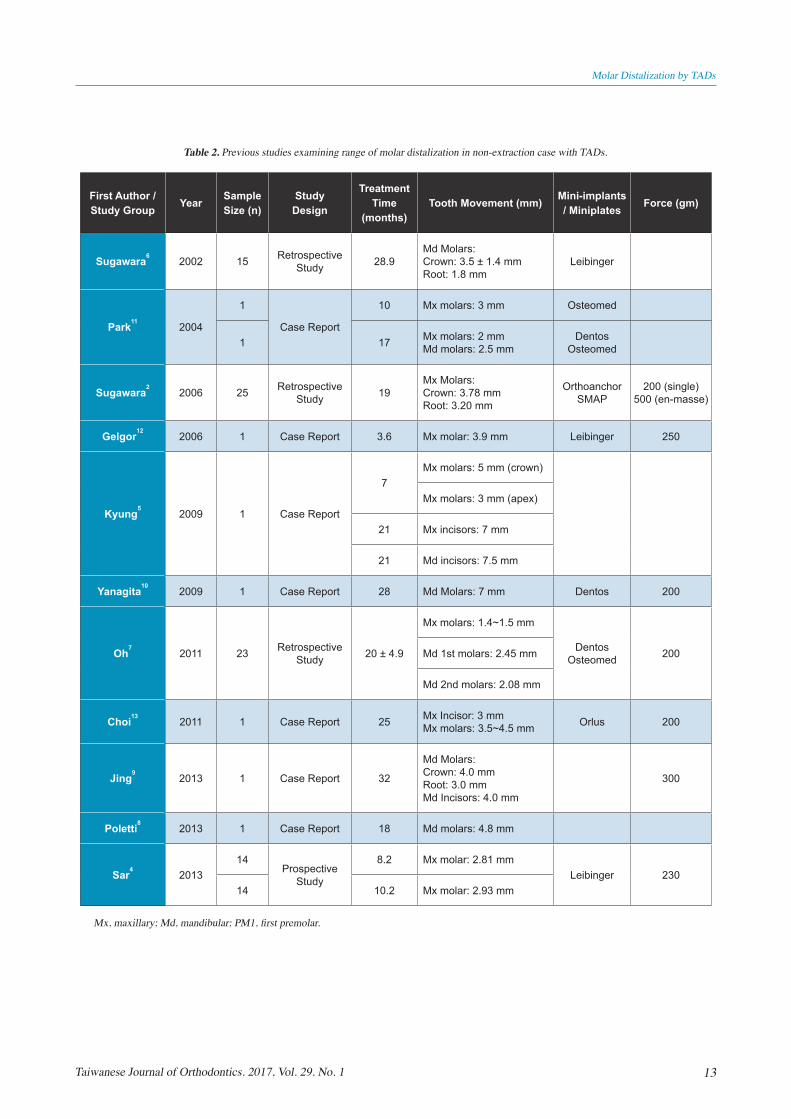
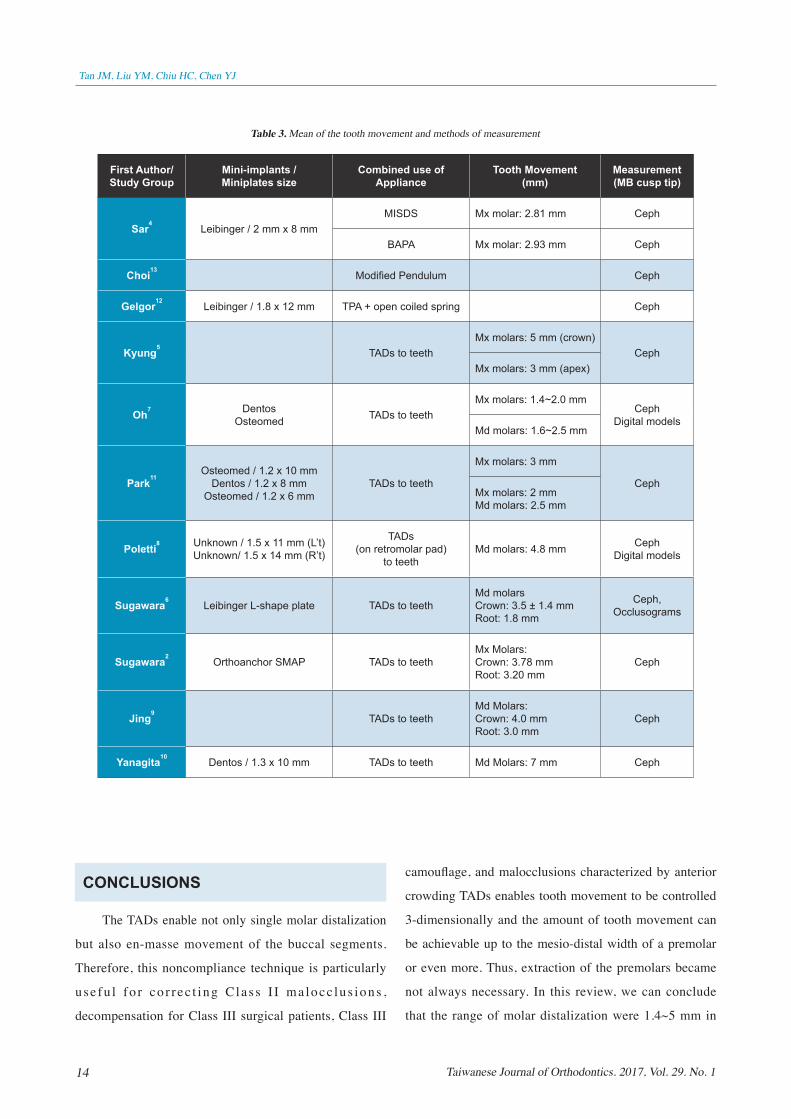
C Range of molar distalizationMany studies have demonstrated outstanding range
of tooth movement in non-extraction cases by using TADs
(Table 2). Table 3 shows the mean of tooth movement and
methods of measurement. The range of molar distalization
were 1.4~5 mm in maxillary molars, and 1.6~7 mm in
mandibular molars. Kyung et al. reported maxillary molar
distalization of 5 mm in his case report,5 while Yanagita et
al. reported maximum mandibular molar distalization of 7
mm in his case report.10
The force used to perform single
molar distalization and en-masse distalization were about
200~300 gm and 500 gm, respectively.
D Side effects of molar distalizationDistal crown tipping might occur during molar
distalization. To avoid distal crown tipping, we had
better make the point of force application nearly passes
Figure 6. Orthodontic titanium anchor plates for distal movement of maxillary molars. A three types of anchor plates with different length of shank; B , C and D anchor plates at the zygomatic buttress, From Sugawara et. al., AJODO 2006 Jun;129(6):723-33.
13Taiwanese Journal of Orthodontics. 2017, Vol. 29. No. 1
Molar Distalization by TADs
Table 2. Previous studies examining range of molar distalization in non-extraction case with TADs.
First Author / Study Group Year Sample
Size (n)Study
Design
Treatment Time
(months)Tooth Movement (mm) Mini-implants
/ Miniplates Force (gm)
Sugawara62002 15 Retrospective
Study 28.9Md Molars: Crown: 3.5 ± 1.4 mmRoot: 1.8 mm
Leibinger
Park112004
1
Case Report
10 Mx molars: 3 mm Osteomed
1 17 Mx molars: 2 mmMd molars: 2.5 mm
Dentos Osteomed
Sugawara22006 25 Retrospective
Study 19Mx Molars: Crown: 3.78 mmRoot: 3.20 mm
Orthoanchor SMAP
200 (single)500 (en-masse)
Gelgor122006 1 Case Report 3.6 Mx molar: 3.9 mm Leibinger 250
Kyung52009 1 Case Report
7Mx molars: 5 mm (crown)
Mx molars: 3 mm (apex)
21 Mx incisors: 7 mm
21 Md incisors: 7.5 mm
Yanagita102009 1 Case Report 28 Md Molars: 7 mm Dentos 200
Oh72011 23 Retrospective
Study 20 ± 4.9
Mx molars: 1.4~1.5 mm
Dentos Osteomed 200Md 1st molars: 2.45 mm
Md 2nd molars: 2.08 mm
Choi132011 1 Case Report 25 Mx Incisor: 3 mm
Mx molars: 3.5~4.5 mm Orlus 200
Jing92013 1 Case Report 32
Md Molars:Crown: 4.0 mmRoot: 3.0 mmMd Incisors: 4.0 mm
300
Poletti82013 1 Case Report 18 Md molars: 4.8 mm
Sar42013
14Prospective
Study
8.2 Mx molar: 2.81 mmLeibinger 230
14 10.2 Mx molar: 2.93 mm
Mx, maxillary; Md, mandibular; PM1, first premolar.
14 Taiwanese Journal of Orthodontics. 2017, Vol. 29. No. 1
Tan JM, Liu YM, Chiu HC, Chen YJ
camouflage, and malocclusions characterized by anterior
crowding TADs enables tooth movement to be controlled
3-dimensionally and the amount of tooth movement can
be achievable up to the mesio-distal width of a premolar
or even more. Thus, extraction of the premolars became
not always necessary. In this review, we can conclude
that the range of molar distalization were 1.4~5 mm in
CONCLUSIONS
The TADs enable not only single molar distalization
but also en-masse movement of the buccal segments.
Therefore, this noncompliance technique is particularly
use fu l fo r co r rec t ing C las s I I ma locc lus ions ,
decompensation for Class III surgical patients, Class III
Table 3. Mean of the tooth movement and methods of measurement
First Author/ Study Group
Mini-implants / Miniplates size
Combined use of Appliance
Tooth Movement(mm)
Measurement(MB cusp tip)
Sar4Leibinger / 2 mm x 8 mm
MISDS Mx molar: 2.81 mm Ceph
BAPA Mx molar: 2.93 mm Ceph
Choi13Modified Pendulum Ceph
Gelgor12Leibinger / 1.8 x 12 mm TPA + open coiled spring Ceph
Kyung5TADs to teeth
Mx molars: 5 mm (crown)Ceph
Mx molars: 3 mm (apex)
Oh7 DentosOsteomed TADs to teeth
Mx molars: 1.4~2.0 mmCeph
Digital modelsMd molars: 1.6~2.5 mm
Park11Osteomed / 1.2 x 10 mm
Dentos / 1.2 x 8 mmOsteomed / 1.2 x 6 mm
TADs to teeth
Mx molars: 3 mm
CephMx molars: 2 mmMd molars: 2.5 mm
Poletti8 Unknown / 1.5 x 11 mm (L’t)Unknown/ 1.5 x 14 mm (R’t)
TADs(on retromolar pad)
to teethMd molars: 4.8 mm Ceph
Digital models
Sugawara6Leibinger L-shape plate TADs to teeth
Md molarsCrown: 3.5 ± 1.4 mmRoot: 1.8 mm
Ceph, Occlusograms
Sugawara2Orthoanchor SMAP TADs to teeth
Mx Molars: Crown: 3.78 mmRoot: 3.20 mm
Ceph
Jing9TADs to teeth
Md Molars:Crown: 4.0 mmRoot: 3.0 mm
Ceph
Yanagita10Dentos / 1.3 x 10 mm TADs to teeth Md Molars: 7 mm Ceph

15Taiwanese Journal of Orthodontics. 2017, Vol. 29. No. 1
Molar Distalization by TADs
retraction of posterior teeth. Am J Orthod Dentofacial
Orthop. 2011 Apr;139(4):470-81.
8. Poletti L, Silvera AA, Ghislanzoni LT. Dentoalveolar
class III treatment using retromolar miniscrew
anchorage. Prog Orthod. 2013 May 23;14:7. doi:
10.1186/2196-1042-14-7.
9. Jing Y, Han X, Guo Y, Li J, Bai D. Nonsurgical
correction of a Class III malocclusion in an adult
by miniscrew-assis ted mandibular dent i t ion
distalization. Am J Orthod Dentofacial Orthop. 2013
Jun;143(6):877-87.
10. Yanagita T, Kuroda S, Takano-Yamamoto T,
Yamashiro T. Class III malocclusion with complex
problems of lateral open bite and severe crowding
successfully treated with miniscrew anchorage and
lingual orthodontic brackets. Am J Orthod Dentofacial
Orthop. 2011 May;139(5):679-89. doi: 10.1016/
j.ajodo.2009.07.023.
11. Hyo-Sang Park, Tae-Geon Kwon, Jae-Hyun Sung.
Nonextraction Treatment with Microscrew Implants.
Angle Orthod 2004;74:539–549.
12. Gelgor IE, Karaman AI, Buyukyilmaz T. Use of
the intraosseous screw for unilateral upper molar
distalization and found well balanced occlusion. Head
Face Med. 2006 Nov 9;2:38.
13. Choi YJ, Lee JS, Cha JY, Park YC. Total distalization
of the maxillary arch in a patient with skeletal Class II
malocclusion. Am J Orthod Dentofacial Orthop. 2011
Jun;139(6):823-33.
14. Lima CEO, Lima MTO. Directional force treatment
for an adult with class III malocclusion and open bite.
Am J Orthod Dentofacial Orthop. 2006;129(6):817–24.
maxillary molars, and 1.6~7 mm in mandibular molars.
Maximum maxillary molar distalization of 5 mm and
maximum mandibular molar distalization of 7 mm were
shown in case reports. Although TADs do help in molar
distalization, we still need to consider either extraction or
non-extraction method is the best and least time-consumed
way to achieve the goals of orthodontic treatment.
REFERENCE
1. Yao CC, Lai EH, Chang JZ, Chen I, Chen YJ.
Comparison of treatment outcomes between skeletal
anchorage and extraoral anchorage in adults with
maxillary dentoalveolar protrusion. Am J Orthod
Dentofacial Orthop. 2008 Nov;134(5):615-24.
2. Sugawara J, Kanzaki R, Takahashi I, Nagasaka H,
Nanda R. Distal movement of maxillary molars in
nongrowing patients with the skeletal anchorage
system. Am J Orthod Dentofacial Orthop. 2006
Jun;129(6):723-33.
3. Ramesh Sabhlok. Predictable Maxillary Molar
Distalization with micro-implant Anchorage in the
correction of class II Malocclusion.
4. Sar C, Kaya B, Ozsoy O, Özcirpici AA. Comparison
of two implant-supported molar distalization systems.
Angle Orthod. 2013 May;83(3):460-7.
5. Kyung SH, Lee JY, Shin JW, Hong C, Dietz V,
Gianelly AA. Distalization pattern of the maxillary
arch depending on the number of orthodontic
miniscrews. Am J Orthod Dentofacial Orthop. 2009
Apr;135(4 Suppl):S123-32.
6. Sugawara J, Daimaruya T, Umemori M, Nagasaka H,
Takahashi I, Kawamura H, Mitani H. Distal movement
of mandibular molars in adult patients with the
skeletal anchorage system. Am J Orthod Dentofacial
Orthop. 2004 Feb;125(2):130-8.
7. Oh YH, Park HS, Kwon TG. Treatment effects of
microimplant-aided sliding mechanics on distal
Related Documents











