1 Creative Coaching & Educational Strategies to Develop Critical Thinking Skills Part III: “At the Bedside” Methodist Urgent Assessment Team UAT, Stroke Team, UAT, Stroke Team, or Code Teams or Code Teams Dial 122 Dial 122 Team is expected to respond in five minutes or less from time called thus ensuring no delay of treatment or notification of physician occurs. MMCI Multi-disciplinary Team • CNS, Nursing Supervisor or ED Nurse Educator – Leadership role – Assist patient’s RN in calling MD – Collaborate with the MD – Develop Critical Thinking • ICU Nurse • Respiratory Therapist • What? No Physician? • Focus: Nurse-To-Nurse consult UAT Order Sets Management of Respiratory Distress Management of Chest pain – STEMI – NSTEMI UAT Order Sets Management of S/S Stroke Management of S/S Sepsis Management of Bleeding Diagnostics Post UAT • Informal debriefing with staff to build critical thinking skills • Thank you cards for calling the team • Provides “Just in Time” Teaching when a critical issue is identified and resolved

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
1
Creative Coaching & Educational Strategies to
Develop Critical Thinking Skills
Part III: “At the Bedside”
Methodist Urgent Assessment Team
UAT, Stroke Team, UAT, Stroke Team, or Code Teamsor Code TeamsDial 122Dial 122
Team is expected to respond in five minutes or less from time called thus ensuring no delay of treatment or notification of physician occurs.
MMCI Multi-disciplinary Team
• CNS, Nursing Supervisor or ED Nurse Educator– Leadership role– Assist patient’s RN in calling MD– Collaborate with the MD– Develop Critical Thinking
• ICU Nurse
• Respiratory Therapist
• What? No Physician?
• Focus: Nurse-To-Nurse consult
UAT Order Sets
Management of Respiratory Distress
Management of Chest pain– STEMI
– NSTEMI
UAT Order Sets
Management of S/S Stroke
Management of S/S Sepsis
Management of Bleeding
Diagnostics
Post UAT
• Informal debriefing with staff to build critical thinking skills
• Thank you cards for calling the team• Provides “Just in Time” Teaching when a
critical issue is identified and resolved
2
Clinical Outcomes
• Team meets monthly• Reviews data• Physician champion• Makes recommendations for improvement
or resolution of problems
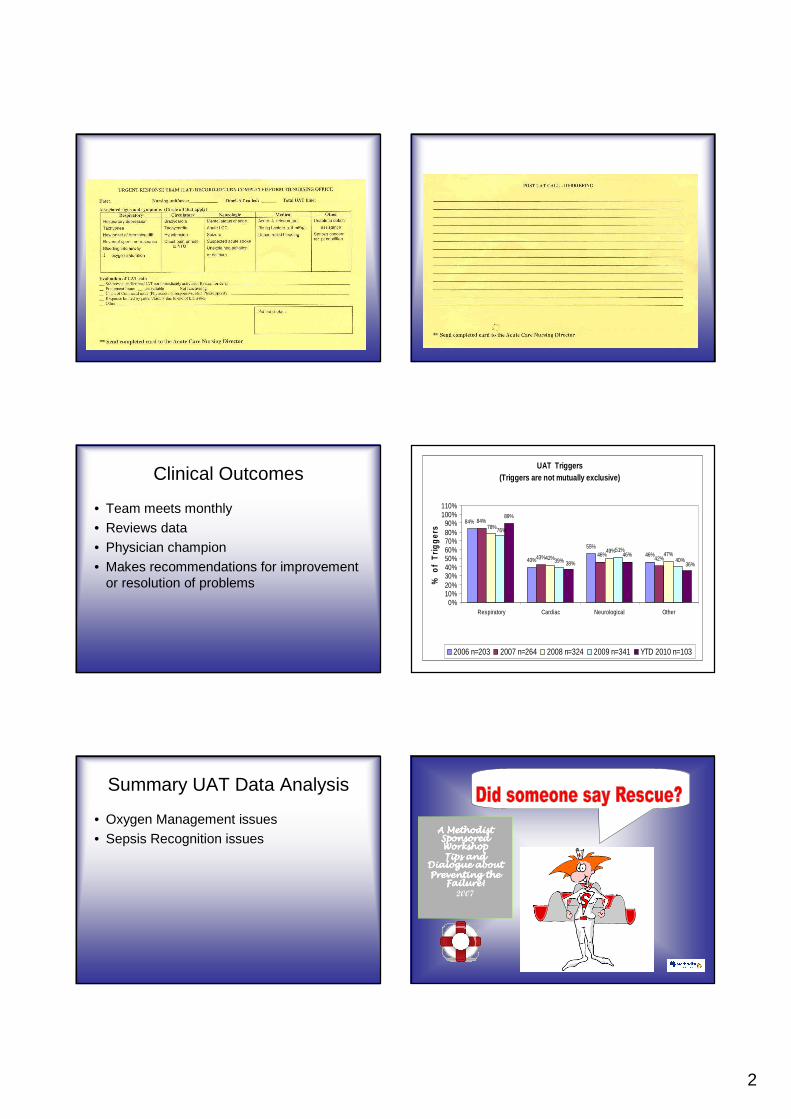
UAT Triggers(Triggers are not mutually exclusive)
40%
55%46%
84%
43% 42%42%47%
39%
89%
46%
84%
46%49%
78%76%
40%
51%
38% 36%
0%10%20%30%40%50%60%70%80%90%
100%110%
Respiratory Cardiac Neurological Other
% o
f T
rigge
rs
2006 n=203 2007 n=264 2008 n=324 2009 n=341 YTD 2010 n=103
Summary UAT Data Analysis
• Oxygen Management issues• Sepsis Recognition issues
A Methodist A Methodist A Methodist A Methodist Sponsored Sponsored Sponsored Sponsored Workshop Workshop Workshop Workshop Tips and Tips and Tips and Tips and
Dialogue about Dialogue about Dialogue about Dialogue about Preventing the Preventing the Preventing the Preventing the
Failure!Failure!Failure!Failure!2007
3
AgendaAgendaAgendaAgendaAgendaAgendaAgendaAgenda
• Urgent Assessment Team Updates & data results
• “Preventing a Crisis”• Oxygen Management Issues• Review of Sepsis – SIRS Criteria, • “How to Stay Out of Legal Hot
Water”•• Thank you for coming today!Thank you for coming today!
Failure to Rescue versus Preventing A Crisis (2008)
Case Studies
• Stimulate critical thinking by using real situations to think through situations before experiencing them with real patients
• Allow nurses to examine & reexamine nursing actions from a variety of perspectives
• Assist nurses to identify and select care options and set priorities
• Bridge the gap between novice and experienced nurses
• Need to be a good facilitator of the discussion
Building Case Studies
• Case Selection – base on real patients
• To protect specific patient information, data can be combined from similar cases so it represents many patients not just one.
• Leave scenario open-ended or lacking detail so case can evolve through discussion– What other assessments, interventions or
evaluations might be helpful?
.
Good Analytical Questions to Improve Critical Thinking
• How?• Why?
Better than• Who?• What?• When?• Where?
4
Source: Crit Care Nurse Q; Vol 35, No. 1, p 27.
Good Analytical Questions to Improve Critical Thinking Critical Thinking Habits of the MindCase Studies
• Confidence• Contextual Perspective• Inquisitiveness• Intellectual Integrity• Intuition• Open-Mindedness• Reflection
Preventing A CrisisPreventing A Crisis
Case # 9Case # 9
RCA ST
PreopPreop ~ What SCIP ~ What SCIP (surgical care improvement project)(surgical care improvement project)measure occurrence do you need to ensure?measure occurrence do you need to ensure?
�� 63 y/o male is scheduled for 63 y/o male is scheduled for thorocotomythorocotomyfor minor left upper for minor left upper lobectomylobectomy wedge wedge resection at 0900 this amresection at 0900 this am
�� PMHPMH∼∼ CAD CAD –– stentstent 4 years ago4 years ago∼∼ HypertensionHypertension∼∼ HyperlipidemiaHyperlipidemia
�� Home medsHome meds∼∼ AtenololAtenolol 50 mg daily 50 mg daily ------ last dose at 0800 last dose at 0800
yesterdayyesterday∼∼ CrestorCrestor 10 mg daily10 mg daily∼∼ ASA 81 mg daily ASA 81 mg daily –– stopped 2 weeks stopped 2 weeks preoppreop∼∼ PlavixPlavix 75 mg daily 75 mg daily –– stopped 5 days stopped 5 days preoppreop
Case # 9
�� AtenololAtenolol 50 mg should be given with sips 50 mg should be given with sips of water even when patient is NPO for of water even when patient is NPO for surgery.surgery.
�� SCIP measure: Beta Blocker needs to be SCIP measure: Beta Blocker needs to be given within 24 hours of incision time.given within 24 hours of incision time.
�� What would you do?What would you do?
Case # 9
This is the MT with a report This is the MT with a report about your patient in Room about your patient in Room
412~ Pt. has Sinus Rhythm with 412~ Pt. has Sinus Rhythm with STST-- segment elevationsegment elevation
5
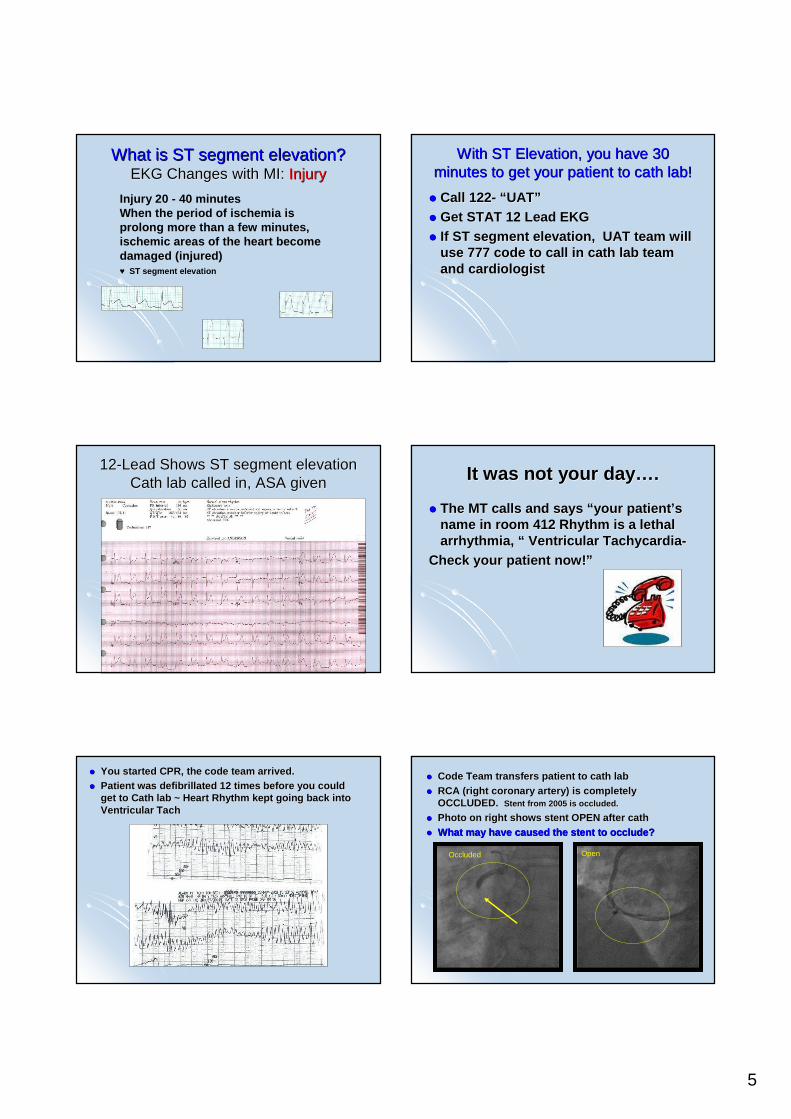
What is ST segment elevation?What is ST segment elevation?EKG Changes with MI: EKG Changes with MI: InjuryInjury
Injury 20 - 40 minutesWhen the period of ischemia is prolong more than a few minutes, ischemic areas of the heart become damaged (injured)♥ ST segment elevation
With ST Elevation, you have 30 With ST Elevation, you have 30 minutes to get your patient to minutes to get your patient to cathcath lab!lab!
�� Call 122Call 122 -- ““ UATUAT””�� Get STAT 12 Lead EKGGet STAT 12 Lead EKG�� If ST segment elevation, UAT team will If ST segment elevation, UAT team will
use 777 code to call in use 777 code to call in cathcath lab team lab team and cardiologistand cardiologist
1212--Lead Shows ST segment elevationLead Shows ST segment elevationCath lab called in, ASA givenCath lab called in, ASA given It was not your dayIt was not your day ……..
�� The MT calls and says The MT calls and says ““ your patientyour patient ’’s s name in room 412 Rhythm is a lethal name in room 412 Rhythm is a lethal arrhythmia, arrhythmia, ““ Ventricular TachycardiaVentricular Tachycardia --
Check your patient now!Check your patient now! ””
�� You started CPR, the code team arrived.You started CPR, the code team arrived.�� Patient was defibrillated 12 times before you could Patient was defibrillated 12 times before you could
get to Cath lab ~ Heart Rhythm kept going back into get to Cath lab ~ Heart Rhythm kept going back into Ventricular Ventricular TachTach
�� Code Team transfers patient to Code Team transfers patient to cathcath lablab�� RCA (right coronary artery) is completely RCA (right coronary artery) is completely
OCCLUDED. OCCLUDED. StentStent from 2005 is occluded.from 2005 is occluded.
�� Photo on right shows Photo on right shows stentstent OPEN after OPEN after cathcath�� What may have caused the What may have caused the stentstent to occlude?to occlude?
Occluded Open
6
Lessons LearnedLessons Learned
�� Any patient can have a myocardial infarctionAny patient can have a myocardial infarction∼∼ Prompt action with UAT if EKG shows acute Prompt action with UAT if EKG shows acute
changeschanges∼∼ Elevated Elevated troponinstroponins need to be called. Cardiology need to be called. Cardiology
consult is recommend consult is recommend ------ even if during the night.even if during the night.�� Note if Note if plavixplavix has been discontinued and has been discontinued and
make sure cardiologist knows that it is DC make sure cardiologist knows that it is DC for surgery.for surgery.
�� EffientEffient is a new anticoagulation medication is a new anticoagulation medication that is used instead of that is used instead of PlavixPlavix so make sure so make sure cardiologist also knows if this is DC.cardiologist also knows if this is DC.
�� Crisis averted due to prompt action of staffCrisis averted due to prompt action of staff
Preventing A CrisisPreventing A Crisis
Case # 11Case # 11
Resp D
Case #11 Case #11 ~10/4 at 1600~10/4 at 1600
�� 78 y/o female comes to ED from 78 y/o female comes to ED from nursing home for increasing SOB, nursing home for increasing SOB, decreased alertness, and is currently decreased alertness, and is currently being treated for UTI.being treated for UTI.
PMHPMH
�� HypothyroidismHypothyroidism�� Renal insufficiencyRenal insufficiency�� AnxietyAnxiety
�� BNP ~731BNP ~731�� TroponinTroponin ~ ~
0.160.16
Case #11 Case #11 ~ 10/4 at 1600~ 10/4 at 1600
Case # 11Case # 11
7
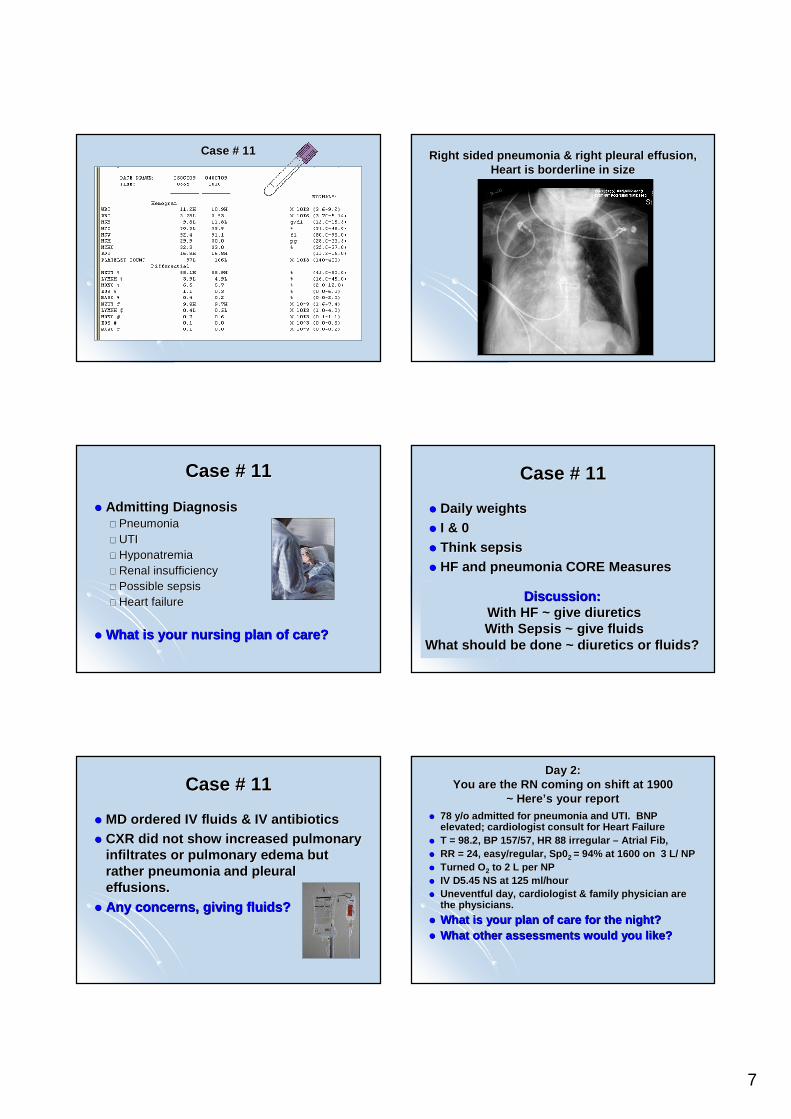
Case # 11Case # 11 Right sided pneumonia & right pleural effusion, Right sided pneumonia & right pleural effusion, Heart is borderline in sizeHeart is borderline in size
�� Admitting DiagnosisAdmitting Diagnosis∼∼ PneumoniaPneumonia∼∼ UTIUTI∼∼ HyponatremiaHyponatremia∼∼ Renal insufficiencyRenal insufficiency∼∼ Possible sepsisPossible sepsis∼∼ Heart failureHeart failure
�� What is your nursing plan of care?What is your nursing plan of care?
Case # 11Case # 11
Discussion:Discussion:With HF ~ give diureticsWith HF ~ give diureticsWith Sepsis ~ give fluidsWith Sepsis ~ give fluids
What should be done ~ diuretics or fluids?What should be done ~ diuretics or fluids?
�� Daily weightsDaily weights�� I & 0I & 0�� Think sepsisThink sepsis�� HF and pneumonia CORE MeasuresHF and pneumonia CORE Measures
Case # 11Case # 11
�� MD ordered IV fluids & IV antibioticsMD ordered IV fluids & IV antibiotics�� CXR did not show increased pulmonary CXR did not show increased pulmonary
infiltrates or pulmonary edema but infiltrates or pulmonary edema but rather pneumonia and pleural rather pneumonia and pleural effusions.effusions.
�� Any concerns, giving fluids?Any concerns, giving fluids?
Case # 11Case # 11Day 2: Day 2:
You are the RN coming on shift at 1900You are the RN coming on shift at 1900~ Here~ Here’’s your reports your report
�� 78 y/o admitted for pneumonia and UTI. BNP 78 y/o admitted for pneumonia and UTI. BNP elevated; cardiologist consult for Heart Failureelevated; cardiologist consult for Heart Failure
�� T = 98.2, BP 157/57, HR 88 irregular T = 98.2, BP 157/57, HR 88 irregular –– Atrial Fib,Atrial Fib,�� RR = 24, easy/regular, Sp0RR = 24, easy/regular, Sp0 2 2 = 94% at 1600 on 3 L/ NP= 94% at 1600 on 3 L/ NP�� Turned OTurned O 22 to 2 L per NPto 2 L per NP�� IV D5.45 NS at 125 ml/hourIV D5.45 NS at 125 ml/hour�� Uneventful day, cardiologist & family physician are Uneventful day, cardiologist & family physician are
the physicians.the physicians.
�� What is your plan of care for the night? What is your plan of care for the night? �� What other assessments would you like?What other assessments would you like?
8
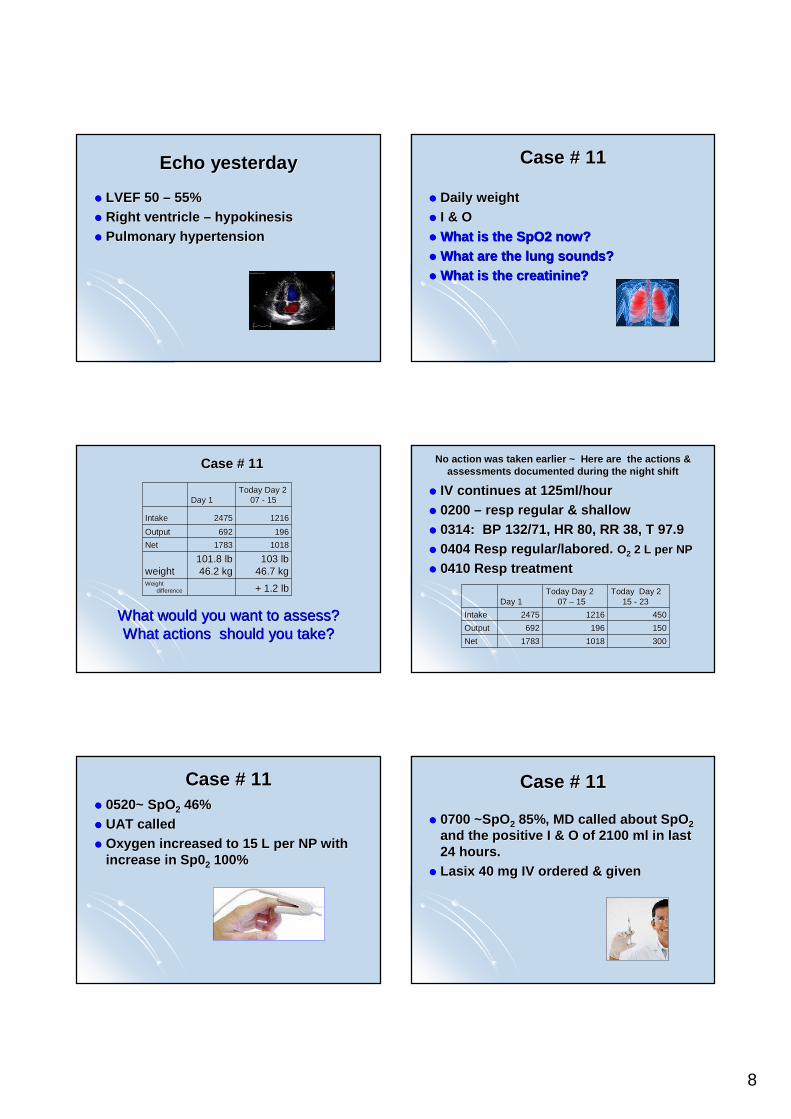
Echo yesterdayEcho yesterday
�� LVEF 50 LVEF 50 –– 55%55%�� Right ventricle Right ventricle –– hypokinesishypokinesis�� Pulmonary hypertensionPulmonary hypertension
�� Daily weightDaily weight�� I & OI & O�� What is the SpO2 now?What is the SpO2 now?�� What are the lung sounds?What are the lung sounds?�� What is the What is the creatininecreatinine ??
Case # 11Case # 11
What would you want to assess?What would you want to assess?What actions should you take?What actions should you take?
+ 1.2 lb+ 1.2 lbWeight Weight
differencedifference
103 lb103 lb46.7 kg46.7 kg
101.8 lb101.8 lb46.2 kg46.2 kgweightweight
1018101817831783NetNet
196196692692OutputOutput
1216121624752475IntakeIntake
Today Day 2 Today Day 2 07 07 -- 1515Day 1Day 1
Case # 11Case # 11 No action was taken earlier ~ Here are the action s & No action was taken earlier ~ Here are the action s & assessments documented during the night shiftassessments documented during the night shift
�� IV continues at 125ml/hourIV continues at 125ml/hour�� 0200 0200 –– respresp regular & shallowregular & shallow�� 0314: BP 132/71, HR 80, RR 38, T 97.90314: BP 132/71, HR 80, RR 38, T 97.9�� 0404 Resp regular/labored. 0404 Resp regular/labored. OO22 2 L per NP2 L per NP
�� 0410 Resp treatment0410 Resp treatment
3003001018101817831783NetNet
150150196196692692OutputOutput
4504501216121624752475IntakeIntake
Today Day 2 Today Day 2 15 15 -- 2323
Today Day 2 Today Day 2 07 07 –– 1515Day 1Day 1
�� 0520~ SpO0520~ SpO22 46% 46% �� UAT calledUAT called�� Oxygen increased to 15 L per NP with Oxygen increased to 15 L per NP with
increase in Sp0increase in Sp0 22 100%100%
Case # 11Case # 11
�� 0700 ~SpO0700 ~SpO22 85%, MD called about SpO85%, MD called about SpO 2 2 and the positive I & O of 2100 ml in last and the positive I & O of 2100 ml in last 24 hours.24 hours.
�� LasixLasix 40 mg IV ordered & given40 mg IV ordered & given
Case # 11Case # 11
9
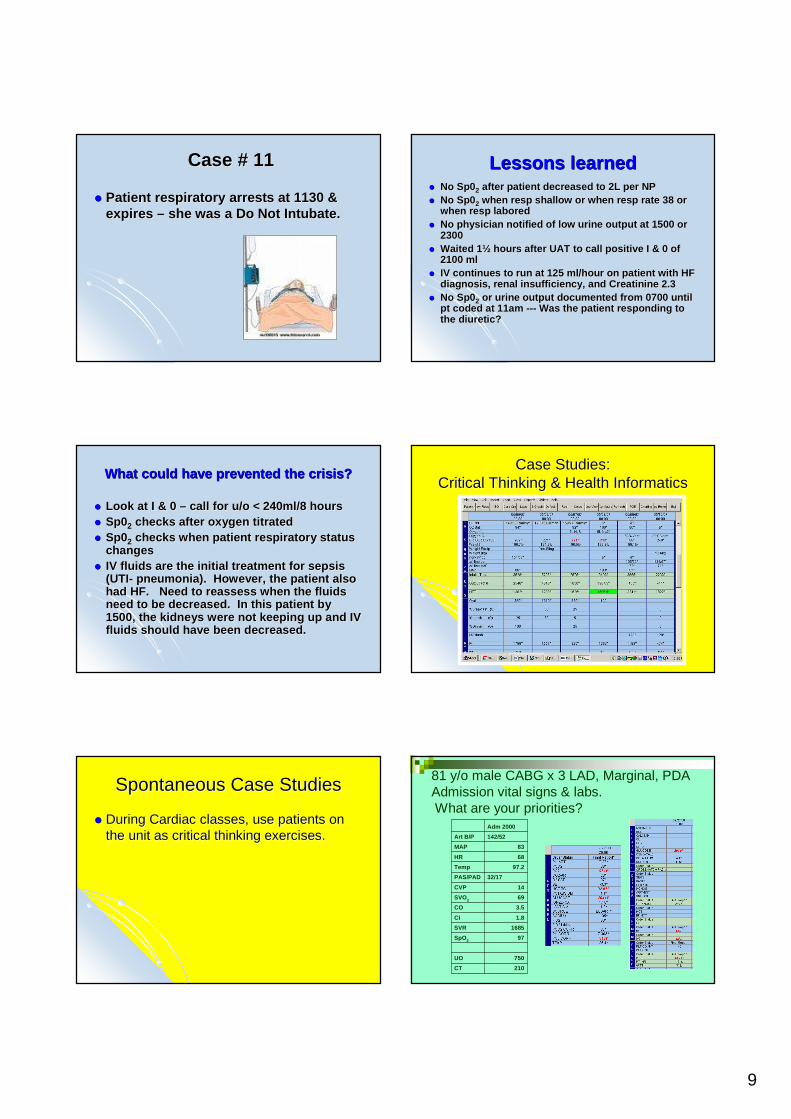
�� Patient respiratory arrests at 1130 & Patient respiratory arrests at 1130 & expires expires –– she was a Do Not she was a Do Not IntubateIntubate ..
Case # 11Case # 11 Lessons learnedLessons learned�� No Sp0No Sp0 22 after patient decreased to 2L per NPafter patient decreased to 2L per NP�� No Sp0No Sp0 22 when when respresp shallow or when shallow or when respresp rate 38 or rate 38 or
when when respresp laboredlabored�� No physician notified of low urine output at 1500 o r No physician notified of low urine output at 1500 o r
23002300�� Waited 1Waited 1 ½½ hours after UAT to call positive I & 0 of hours after UAT to call positive I & 0 of
2100 ml2100 ml�� IV continues to run at 125 ml/hour on patient with HF IV continues to run at 125 ml/hour on patient with HF
diagnosis, renal insufficiency, and diagnosis, renal insufficiency, and CreatinineCreatinine 2.32.3�� No Sp0No Sp0 22 or urine output documented from 0700 until or urine output documented from 0700 until
pt coded at 11am pt coded at 11am ------ Was the patient responding to Was the patient responding to the diuretic?the diuretic?
What could have prevented the crisis?What could have prevented the crisis?
�� Look at I & 0 Look at I & 0 –– call for u/o < 240ml/8 hourscall for u/o < 240ml/8 hours�� Sp0Sp022 checks after oxygen titratedchecks after oxygen titrated�� Sp0Sp022 checks when patient respiratory status checks when patient respiratory status
changeschanges�� IV fluids are the initial treatment for sepsis IV fluids are the initial treatment for sepsis
(UTI(UTI-- pneumonia). However, the patient also pneumonia). However, the patient also had HF. Need to reassess when the fluids had HF. Need to reassess when the fluids need to be decreased. In this patient by need to be decreased. In this patient by 1500, the kidneys were not keeping up and IV 1500, the kidneys were not keeping up and IV fluids should have been decreased.fluids should have been decreased.
Case Studies: Case Studies: Critical Thinking & Health InformaticsCritical Thinking & Health Informatics
Spontaneous Case StudiesSpontaneous Case Studies
�� During Cardiac classes, use patients on During Cardiac classes, use patients on the unit as critical thinking exercises.the unit as critical thinking exercises.
210CT
750UO
97SpO2
1685SVR
1.8CI
3.5CO
69SVO2
14CVP
32/17PAS/PAD
97.2Temp
68HR
83MAP
142/52Art B/P
Adm 2000
81 y/o male CABG x 3 LAD, Marginal, PDAAdmission vital signs & labs. What are your priorities?
10
29025030206040210CT
100425250175375250750UO
9998979710010097SpO2
13921234118613081685SVR
1.92.33.12.31.72.21.8CI
3.84.56.14.53.34.43.5CO
66707171647269SVO2
881212131614CVP
22/1123/1036/1628/1229/1436/1732/17PAS/PAD
99.199.398.699.19997.797.2Temp
86818574836468HR
79799482628683MAP
138/48142/47161/51151/45106/38148/57142/52Art B/P
2001002400230022002100Adm2000
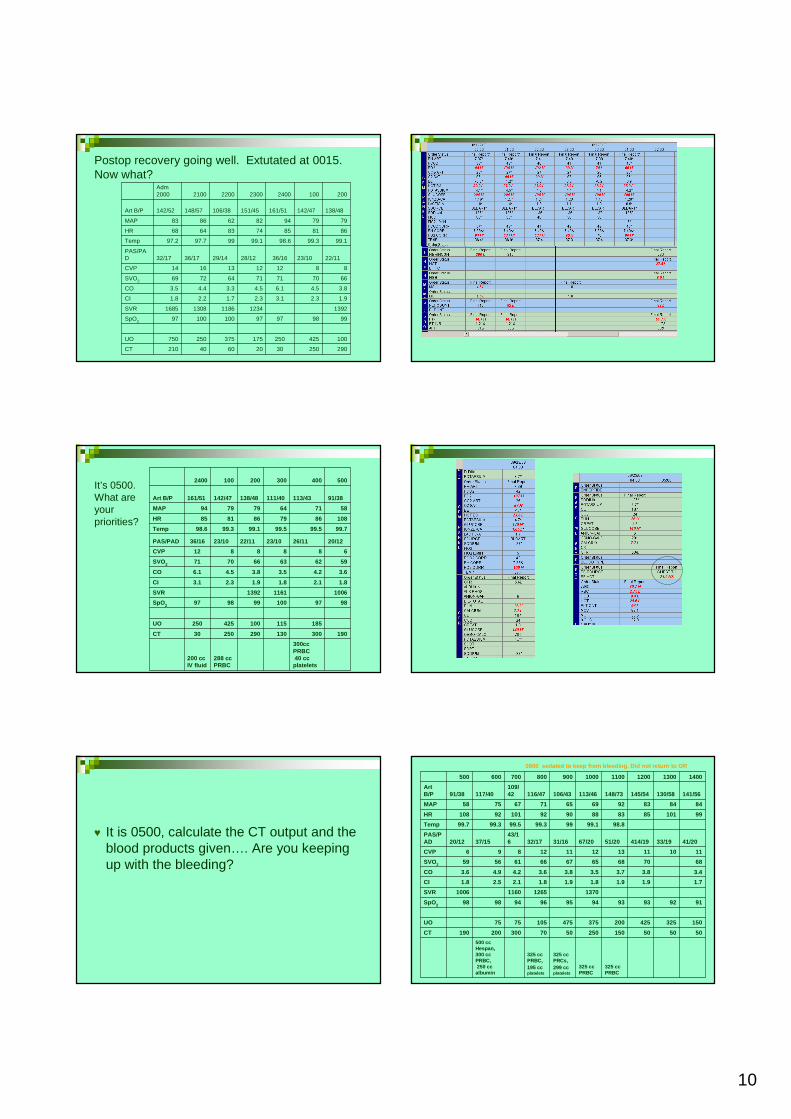
Postop recovery going well. Extutated at 0015. Now what?
300cc PRBC40 cc platelets
288 cc PRBC
200 cc IV fluid
19030013029025030CT
185115100425250UO
9897100999897SpO2
100611611392SVR
1.82.11.81.92.33.1CI
3.64.23.53.84.56.1CO
596263667071SVO2
6888812CVP
20/1226/1123/1022/1123/1036/16PAS/PAD
99.799.599.599.199.398.6Temp
1088679868185HR
587164797994MAP
91/38113/43111/40138/48142/47161/51Art B/P
5004003002001002400It’s 0500. What are your priorities?
♥ It is 0500, calculate the CT output and the blood products given…. Are you keeping up with the bleeding?
325 cc PRBC
325 cc PRBC
325 cc PRCs, 299 ccplatelets
325 cc PRBC, 195 ccplatelets
500 cc Hespan, 300 cc PRBC,250 cc
albumin
5050501502505070300200190CT
1503254252003754751057575UO
91929393949596949898SpO2
1370126511601006SVR
1.71.91.91.81.91.82.12.51.8CI
3.43.83.73.53.83.64.24.93.6CO
687068656766615659SVO2
11101113121112896CVP
41/2033/19414/1951/2067/2031/1632/1743/1637/1520/12
PAS/PAD
98.899.19999.399.599.399.7Temp
99101858388909210192108HR
84848392696571677558MAP
141/56130/58145/54148/73113/46106/43116/47109/42117/4091/38
Art B/P
14001300120011001000900800700600500
0800 sedated to keep from bleeding. Did not return to OR
11
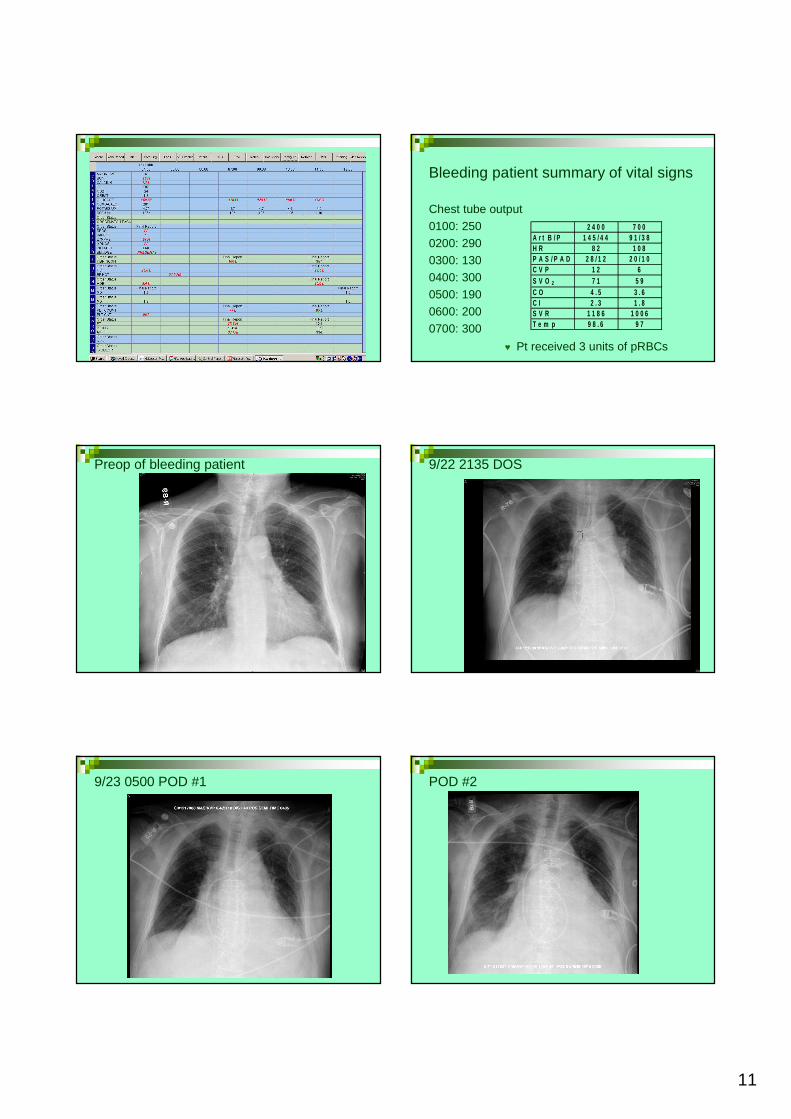
Bleeding patient summary of vital signs
Chest tube output
0100: 250
0200: 290
0300: 130
0400: 300
0500: 190
0600: 200
0700: 300
♥ Pt received 3 units of pRBCs
2 4 0 0 7 0 0A r t B / P 1 4 5 / 4 4 9 1 / 3 8H R 8 2 1 0 8P A S / P A D 2 8 / 1 2 2 0 / 1 0C V P 1 2 6S V O 2 7 1 5 9C O 4 . 5 3 . 6C I 2 . 3 1 . 8S V R 1 1 8 6 1 0 0 6T e m p 9 8 . 6 9 7
Preop of bleeding patient 9/22 2135 DOS
9/23 0500 POD #1 POD #2
12
POD #3 POD #4 What would you be assessing?
Scary Coronary EventsScary Coronary Events
Cheryl Herrmann, APN, CCRN, CCNS-CSC/CMCCardiac Clinical Nurse Specialist
www.cherylherrmann.com
Case Study #1Case Study #1
♥ 69 y/o female comes to ED with c/o of severe chest discomfort
♥ PMH: mild HTN and hyperlipidemia♥ B/P 173/89, HR 91, RR 21
SpO2 98% on 2 l/np
16:59
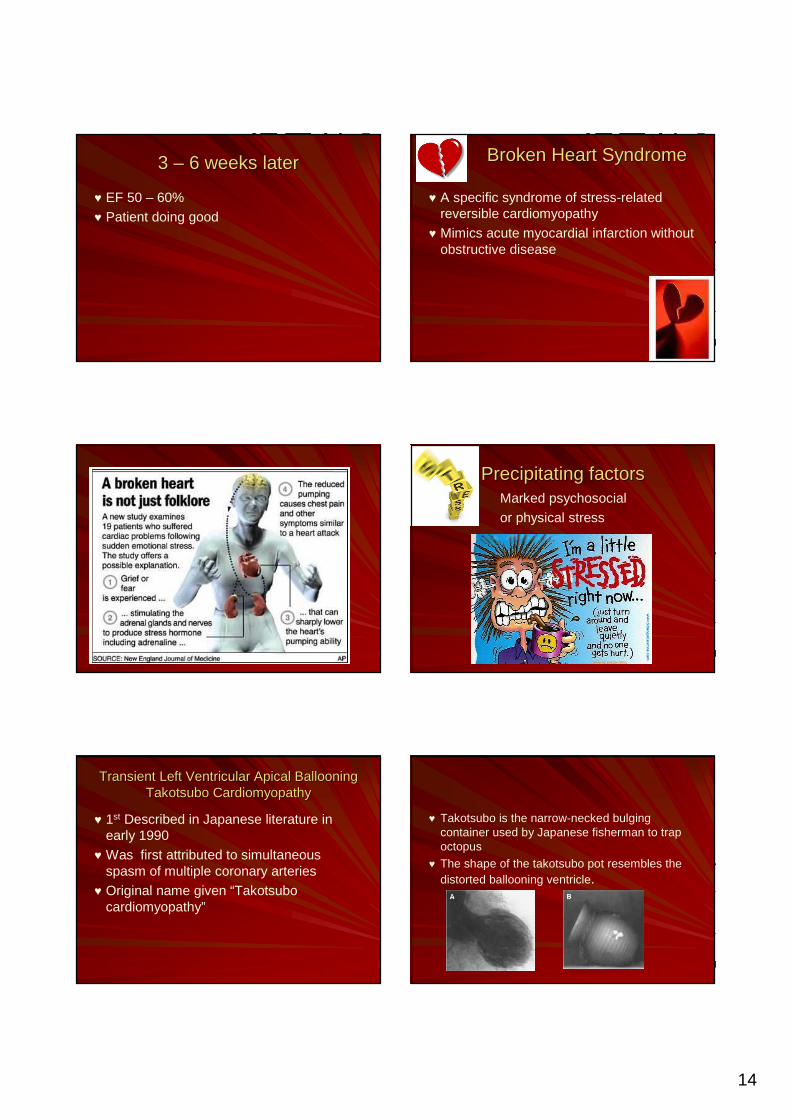
EKG on admissionEKG on admission
♥ NTG 0.4 mg SL x 3 in 30 minutes♥ ASA 81 mg po♥ Metoprolol 25 mg po♥ Retavase
13
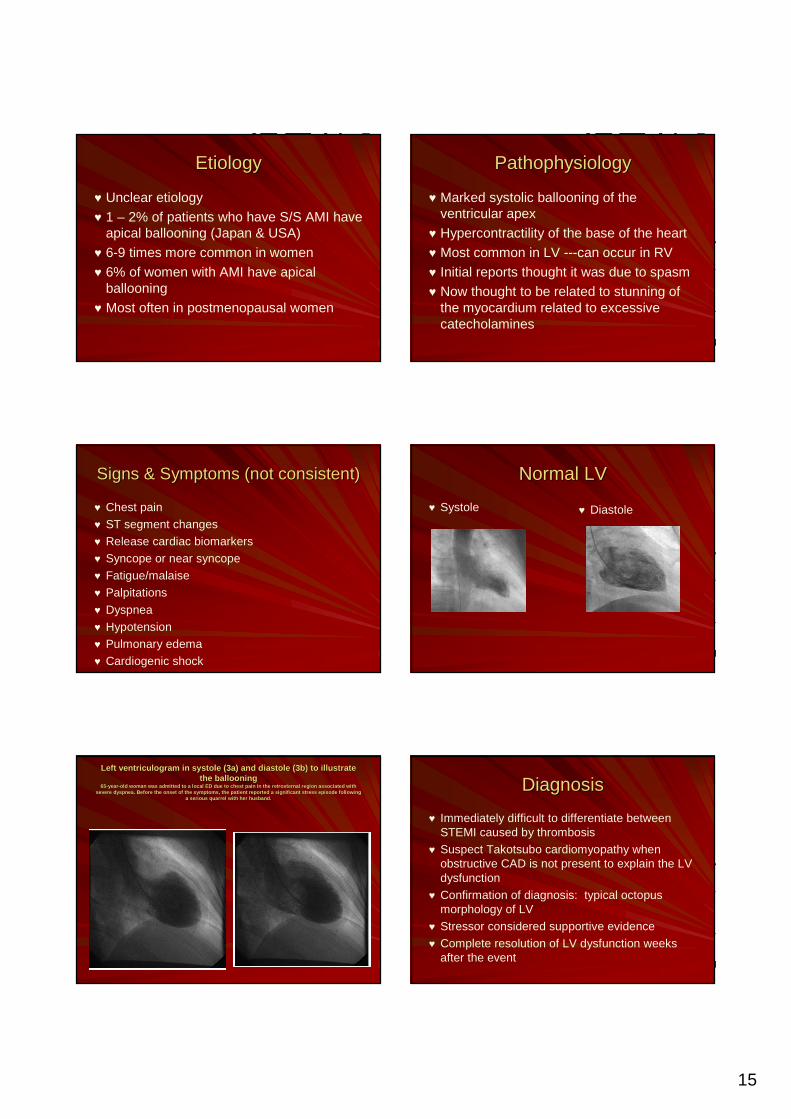
More historyMore history ……..
♥ A few hours earlier in the same ED, her husband came in full arrest and was not able to be resuscitated
No relief of symptomsNo relief of symptomsRepeat EKGRepeat EKG
No improvement No improvement InferolateralInferolateral leadsleads
Transported via helicopter to hospital with cardiac cath
Labs on admissionLabs on admission
♥ CK = 156
♥ CKMB = 10.7 ↑♥ Myoglobin = 298 ↑♥ Troponin I = 2.91 ↑♥ BNP = 35
Cardiac Cardiac CathCath findingsfindings
♥ Normal coronary anatomy – No CAD♥ Severe hypokinesis to akinesis of the
distal 2/3 anterolateral, apical, and inferior walls.
♥ The basal segments contract vigorously giving it very Japanese amphora shape suggestive of Takotsubo cardiomyopathy
♥ Markedly depressed LV function with ejection fraction = 5 – 10%
ManagementManagement
♥ Transferred to CVICU
♥ No IABP due to hemodynamicallystable and recent Retavase
♥ Diagnosis: Broken Heart Syndrome or Transient Apical Ballooning
Discharged the next day so she Discharged the next day so she could attend her husbandcould attend her husband’’s funerals funeral
♥ Discharge medications
♥ Aldactone 25 mg every day
♥ Alprazolam 0.5 mg prn
♥ Altace 2.5 mg every day
♥ ASA 81 mg every day
♥ Coreg 6.35 mg every 12 hours
♥ Coumadin 5 mg po every day
♥ Lasix 20 mg every other day
♥ Lipitor 40 mg po at hs
14
3 3 –– 6 weeks later6 weeks later
♥ EF 50 – 60%♥ Patient doing good
Broken Heart SyndromeBroken Heart Syndrome
♥ A specific syndrome of stress-related reversible cardiomyopathy
♥ Mimics acute myocardial infarction without obstructive disease
Precipitating factorsPrecipitating factorsMarked psychosocial or physical stress
Transient Left Ventricular Apical BallooningTransient Left Ventricular Apical BallooningTakotsubo CardiomyopathyTakotsubo Cardiomyopathy
♥ 1st Described in Japanese literature in early 1990
♥ Was first attributed to simultaneous spasm of multiple coronary arteries
♥ Original name given “Takotsubo cardiomyopathy”
♥ Takotsubo is the narrow-necked bulging container used by Japanese fisherman to trap octopus
♥ The shape of the takotsubo pot resembles the distorted ballooning ventricle.
15
EtiologyEtiology
♥ Unclear etiology♥ 1 – 2% of patients who have S/S AMI have
apical ballooning (Japan & USA)♥ 6-9 times more common in women♥ 6% of women with AMI have apical
ballooning♥ Most often in postmenopausal women
PathophysiologyPathophysiology
♥ Marked systolic ballooning of the ventricular apex
♥ Hypercontractility of the base of the heart♥ Most common in LV ---can occur in RV♥ Initial reports thought it was due to spasm♥ Now thought to be related to stunning of
the myocardium related to excessive catecholamines
Signs & Symptoms (not consistent)Signs & Symptoms (not consistent)
♥ Chest pain
♥ ST segment changes
♥ Release cardiac biomarkers
♥ Syncope or near syncope
♥ Fatigue/malaise
♥ Palpitations
♥ Dyspnea
♥ Hypotension
♥ Pulmonary edema
♥ Cardiogenic shock
♥ Lethal ventricular arrhythmias
Normal LVNormal LV
♥ Systole ♥ Diastole
Left Left ventriculogramventriculogram in systole (3a) and diastole (3b) to illustrate in systole (3a) and diastole (3b) to illustrate the ballooningthe ballooning
6565--yearyear --old woman was admitted to a local ED due to chest p ain in the old woman was admitted to a local ED due to chest p ain in the retrosternalretrosternal region associated with region associated with severe severe dyspneadyspnea . Before the onset of the symptoms, the patient rep orted a signi. Before the onset of the symptoms, the patient rep orted a signi ficant stress episode following ficant stress episode following
a serious quarrel with her husband.a serious quarrel with her husband.
DiagnosisDiagnosis
♥ Immediately difficult to differentiate between STEMI caused by thrombosis
♥ Suspect Takotsubo cardiomyopathy when obstructive CAD is not present to explain the LV dysfunction
♥ Confirmation of diagnosis: typical octopus morphology of LV
♥ Stressor considered supportive evidence
♥ Complete resolution of LV dysfunction weeks after the event
16
ManagementManagement
♥ Prompt recognition of apical ballooning prevents unnecessary administration of fibrinolytics with the ST segment elevation
♥ Specific guidelines do not exist♥ Mostly managed per NSTEMI and STEMI
guidelines
♥Proceed with STEMI treatment & emergent cardiac cath
Management of Management of CardiogenicCardiogenic shockshock
♥ Vasopressors♥ Pacemaker♥ Intraaortic balloon pump (IABP)♥ Support until LV recovers
Supportive ManagementSupportive Management
♥ Arrhythmias � antiarrhythmic drugs♥ Diuretics � pulmonary congestion♥ B Blockers, vasodilators, ACEI,
vasocontrictors, IABP � left sided HF♥ Short term anticoagulant � prevent LV
thrombus
PrognosisPrognosis
♥ Left ventricular function improves rapidly♥ Often within 7 – 30 days♥ EKG changes may be slower to resolve♥ Generally favorable prognosis♥ Mortality of 0 – 8%
Case Studies Summary
• Give information in pieces• Ask critical thinking questions and give
TIME to think through.• Facilitate discussion --- even let thinking
go the wrong direction and then redirect.
Creative Coaching & Educational Strategies to Develop Critical
Thinking Skills
Creative Unit Based Competencies
17
CVICU MANDATORY Competencies 2010It’s time again for unit specific competencies. In this packet, you will find tests you need to complete prior to competency day . If you do not have them competed prior to your scheduled day, then plan to stay until you complete them. The packets are given prior to competency day to give the “brain more time to think”. The packet may look a little overwhelming at first… However, the tests were identified as needed by the education council as “high risk, low use” areas in our clinical practice or items we, as a unit, have struggled with during the past year. Now is the time to become familiar with them so you can easily care for patients.
The Malignant Hyperthermia module is on the computer on the nursing education icon. Please complete prior to the education day. Please go to the computer to find the following resources to use for the tests:
MMCI CVICU-ICU IV Drips – Adult Standard ReferencesCSF drain checklist
Moderate Sedation PolicyAlgorithms
Arrhythmia Management Protocol (RNs < 2 years)Agratroban, Integrilin and Reopro preprinted orders
Please see me for any questions.ThanksCheryl
Critical Thinking Competency Packet• Cardiac Assessment Test• ABGs• IABP• Drug Calculation• Moderate Sedation• Code Blue/Arrhythmia protocols• Anticoagulation Medication Calculations
MANDATORY 2010 Cardiac Competency DaysMANDATORY CVICU Competency Days
Attend one08 – 1300 with Sim Man --- PMP – 5 th floor old Deck 1
Wednesday, May 5Thursday, May 13
Wednesday, May 26Wednesday, June 2Wednesday, June 9
Please read policies and come prepared. There are study guides in the
CVICU report room to check out.
CVICU• High risk Cardiac Surgery Algorithms• Setup for CCO insertion & recalibration• Manual CO and wedge• Defib/Cardioversion – include new R model• Pacemakers• Femostop, safe guard closure devices• Code Blue Responsibilities• Mock open chest code• IABP• VAD -- Biomedicus• ECMO • Intrathecal Catheter • Peds Code – Mariola• Monitor functions• EKG test – includes emergency meds!• RNs who have worked CVICU < 2 years take
test & measure intervals• Other RNs take arrhythmia test• Lift Comps per TMCs
• Bring completed:• CVICU Medication Calculation • Moderate Sedation Quiz • Malignant Hyperthermia module on educ icon• Cardiac Education Critical thinking
assessment• ABG assessment• CSF drain quiz• IABP quiz• VAD • High Risk Algorithms – be prepared to
discuss: • Anticoagulant dosing test • Arrhythmia protocol quiz (RNs < 2 years)• EKG Practice strips
Human Patient Simulation
Critical Thinking Habits of the MindComputer Assisted Simulation
• Confidence
• Contextual Perspective
• Creativity
• Flexibility
• Inquisitiveness
• Intellectual Integrity
• Perseverance
18
A reminder….
• Barriers to CT– Stress– Fatigue– Task Oriented– Fearful of making
mistakes– Position or role
boundaries
• Plan competency days and education days on different days!
Creating A Culture of Certification
• 2003 = N0 Staff RNs Certified – Cardiac & ICU Units• 2004 = 1 CCRN – Cardiac Units• 2008 = 38 Certified RNs – Cardiac Units• 2010 = 49 Certified RNs -- Cardiac & ICUs
– CCRN = 29– Cardiovascular = 13
– PCCN = 6– CCNS, CSC & CMC = 1
Certification MotivatorsPosted Questions in Jeopardy Format Do Study Questions with Staff
Certification Motivators2004 Methodist Designated Magnet Hospital
• CCRN/PCCN and Cardiovascular review classes
• Pass CCRN Book & CD with questions
• CDs from NTI Review classes
• Include Certification questions in Jeopardy game at Education Days
• Certification Luncheon
• Managers encouraged Certification Goals
• 2008: Tiered Nursing Levels - Must be certified to be at the highest level
Celebrating Success
• CCRN/PCCN Pins
• Recognized in Local Newspapers and Regional Advance for Nursing
• Certification on Name Tags
19
Name that Heart Rhythm Lunch & Learn with Pharmaceutical Representatives
• Share research studies for medicines, indications, actions, side effects.
• PharmDs also attend to give the balance of the studies.
• Staff can ask questions about medicines.
• Staff also love the free meal and pens!
Memorial Conferences
Chocolate Motivates…
And I learn what is going on.
Captivate Program
• Captivate makes it easy to quickly create interactive simulations and software demonstrations
• Create short 10 – 15 minute programs
• Short 6 question quiz at the end
• www.adobe.com
20
Alexander Johnson, RN, MS, CNS
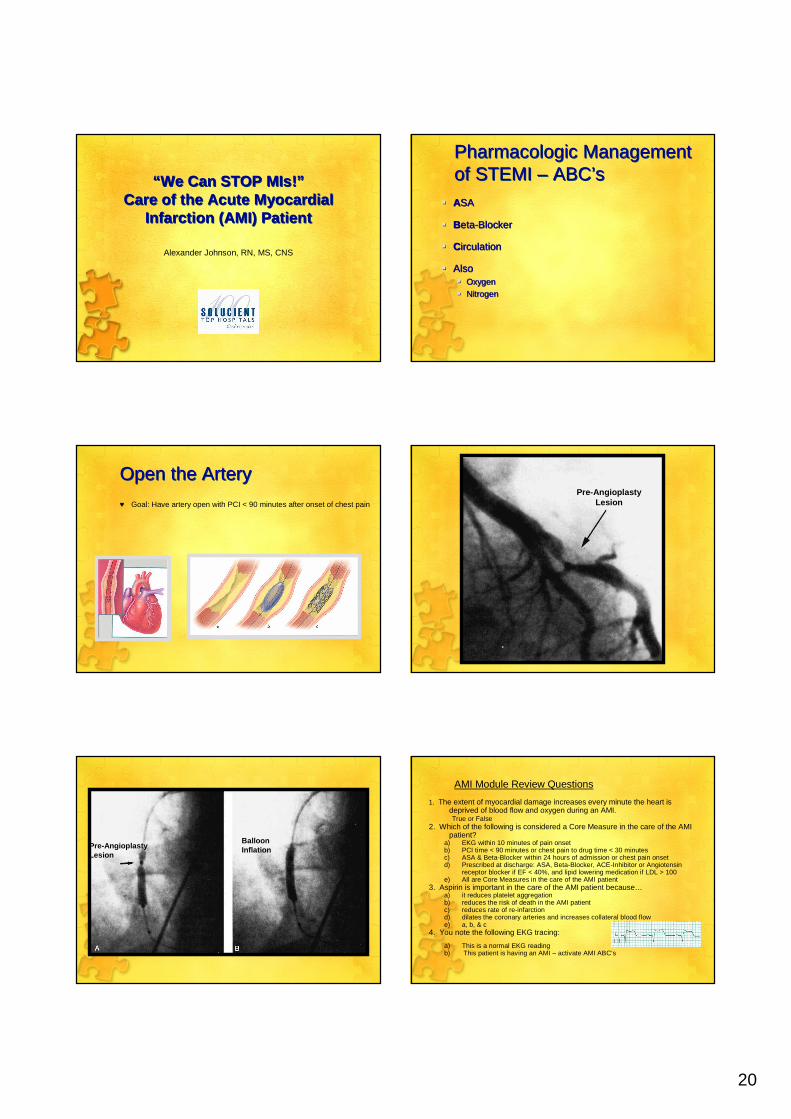
“We Can STOP MIs!”Care of the Acute Myocardial
Infarction (AMI) Patient
“We Can STOP MIs!”Care of the Acute Myocardial
Infarction (AMI) Patient
Pharmacologic Management of STEMI – ABC’sPharmacologic Management of STEMI – ABC’s
� ASA
� Beta-Blocker
� Circulation
� Also� Oxygen� Nitrogen
� ASA
� Beta-Blocker
� Circulation
� Also� Oxygen� Nitrogen
Open the Artery Open the Artery
♥ Goal: Have artery open with PCI < 90 minutes after onset of chest pain
Pre-Angioplasty Lesion
Pre-Angioplasty Lesion
Balloon Inflation
AMI Module Review Questions
1. The extent of myocardial damage increases every minute the heart is deprived of blood flow and oxygen during an AMI.True or False
2. Which of the following is considered a Core Measure in the care of the AMI patient?
a) EKG within 10 minutes of pain onsetb) PCI time < 90 minutes or chest pain to drug time < 30 minutesc) ASA & Beta-Blocker within 24 hours of admission or chest pain onsetd) Prescribed at discharge: ASA, Beta-Blocker, ACE-Inhibitor or Angiotensin
receptor blocker if EF < 40%, and lipid lowering medication if LDL > 100e) All are Core Measures in the care of the AMI patient
3. Aspirin is important in the care of the AMI patient because…a) it reduces platelet aggregationb) reduces the risk of death in the AMI patientc) reduces rate of re-infarctiond) dilates the coronary arteries and increases collateral blood flowe) a, b, & c
4. You note the following EKG tracing:
a) This is a normal EKG readingb) This patient is having an AMI – activate AMI ABC’s
21
Captivate Program
• Use for update on policies or other education
• www.adobe.com
• Buy the program (around $700) and pay to go to the class (around $800)
• Saves educator lecture time and staff attending class!
Lessons learned
• Games must be designed to produce learning not just a “fun” activity
• There is No such thing as a dumb question
Lessons learned
• To learn you need to hear something
–6 times –6 different ways
6
six
VI seis
IIII I
SIX
The Evidence SupportingCreative Learning
• Laughter & enjoying your self boosts the production of neurotransmitters that increase alertness & memory.
• When threatened, tired or helpless you loose your ability to– Recall information
– Notice things around you
– Ask questions
– Think creatively
Source: Prensky M. Digital Game-Based Learning. McGraw-Hill. 2001
Rapid Review
Learning Points
22
Evaluation of Critical Thinking Education at Methodist• Seven Disease Specific Certifications• The Joint Commission Survey• Top 100 Cardiac Hospitals • Patient Satisfaction 95% percentile• Magnet Hospital• Increased number of certified nurses• Decreased sepsis mortality
Testing Competence
Would you be able to work in our units?
- William Butler Yeats- William Butler Yeats
Education is not the filling of a pail but the lighting of a fire.
Education is not the Education is not the filling of a pail but the filling of a pail but the lighting of a fire.lighting of a fire.
Last but not least….End on Time
• Tell the expectation at the beginning of the class
23
Thank you for your attention
Any Questions?
Objectives
• Discuss the barriers to critical thinking.• Compare and contrast learning styles in
a multi generation workforce.• Design creative educational strategies to
develop critical thinking.• Analyze new ways to teach the same
content with improved effectiveness.
Methodist Medical Center of Illinois, [email protected]
www.cherylherrmann.com
Methodist Medical Center of Illinois, [email protected]
www.cherylherrmann.com
Creative Coaching & Educational Strategies to Develop
Critical Thinking Skills
Creative Coaching & Educational Strategies to Develop
Critical Thinking Skills
Workshop 1
Related Documents