INTRODUCTION OF AEROSOLS Aerosol therapy refers to the delivery of a drug to the body via the airways by delivering it in an aerosolized form. Whereas the aerosolized drug may be intended for systemic use utilizing the vast surface area for absorption provided by the respiratory tract, the overwhelming majority of the aerosols are meant for topical use. Evidence of use of aerosol therapy has been found during the days of Hippocrates1 who utilized hot vapors for the management of respiratory diseases. However, the modern era of aerosol therapy began with the introduction of the Medihaler Epi in 1956.2 The last few years have seen a major evolution in our understanding of aerosol delivery to the human subjects. Modern technology along with increasing understanding of human pulmonary physiology has aided the development of improved systems of aerosol delivery. This form of therapy has revolutionized the management of patients with various pulmonary diseases. More and more bronchodilators and anti-inflammatory agents are becoming available for use as aerosol therapy. We attempt to summarize the basic principles of aerosol therapy and the equipments used for generation of aerosols, their clinical uses and limitations. Principles of aerosols An understanding of factors affecting delivery of aerosols is essential before using them. The pulmonary deposition of aerosol is achieved by way of three key mechanisms, namely inertial impaction, sedimentation and diffusion. These three mechanisms

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
INTRODUCTION OF AEROSOLS
Aerosol therapy refers to the delivery of a drug to the body via the airways by delivering it in an
aerosolized form. Whereas the aerosolized drug may be intended for systemic use utilizing the
vast surface area for absorption provided by the respiratory tract, the overwhelming majority of
the aerosols are meant for topical use. Evidence of use of aerosol therapy has been found during
the days of Hippocrates1 who utilized hot vapors for the management of respiratory diseases.
However, the modern era of aerosol therapy began with the introduction of the Medihaler Epi in
1956.2 The last few years have seen a major evolution in our understanding of aerosol delivery
to the human subjects. Modern technology along with increasing understanding of human
pulmonary physiology has aided the development of improved systems of aerosol delivery. This
form of therapy has revolutionized the management of patients with various pulmonary diseases.
More and more bronchodilators and anti-inflammatory agents are becoming available for use as
aerosol therapy. We attempt to summarize the basic principles of aerosol therapy and the
equipments used for generation of aerosols, their clinical uses and limitations.
Principles of aerosols
An understanding of factors affecting delivery of aerosols is essential before using them. The
pulmonary deposition of aerosol is achieved by way of three key mechanisms, namely inertial
impaction, sedimentation and diffusion. These three mechanisms operate in different
combinations for different aerosol drugs at different sites in the pulmonary tree. Whereas inertial
impaction is the predominant process in the oropharynx and the larger airways for aerosols with
relatively large particle size (>3μ), diffusion by way of Brownian motion is the dominant
mechanism for the smaller sized aerosols (<0.5μ). Aerosols with the particle size in the range of
1-3μ are subject to gravitational sedimentation in the small airways and the same tends to be
enhanced by breath holding. The fraction of drug eventually delivered at the desired site of
action also depends on the physical properties of the aerosol and also the host factors that include
pattern of ventilation, status of the airways and lung mechanics.
Factors that influence the penetration and deposition of aerosols
>100 microns – do not enter the respiratory tract (filtered out)
10 – 100 microns – trapped in the nose and mouth
2 – 5 microns – deposited in the bronchial airways
1 – 2 microns – deposit in the alveoli
< 1 microns – usually exhaled
Implications – you want large 10 micron for upper airway swelling, 2 – 5 microns for
bronchodilators in the airways and 1 – 2 microns for antibiotics and anti-inflammatory to the
lung alveoli.
FACTORS AFFECTING DELIVERY OF AEROSOLIZED DRUGS TO THE LUNGS
Physical Characteristics of the Aerosol Particle
Size (mass median aerodynamic diameter)
Density
Electrical charge
Hygroscopy
Shape
Velocity of the aerosol particles
Host Factors
Inspired volume
Inspiratory time
Inspiratory flow
Breath-hold duration
Timing of aerosol delivery during inspiration (with metered dose inhaler)
INDICATIONS FOR AEROSOL THERAPY
Humidification of the respiratory tract
Aid in mobilizing secretions
Deliver medications
ADVANTAGES OF AEROSOLS
The basic advantage of aerosol therapy lies in the delivery of high local concentrations of the
drug directly to the site of action with minimized risks of systemic effects. This is achieved with
a much lower dose compared to what may be required for systemic administration for equivalent
therapeutic response. The commonest aerosolized drugs are the bronchodilators and anti-
inflammatory agents used for obstructive airway diseases, such as asthma and chronic
obstructive pulmonary disease (COPD). Their efficiency results from local effects in the
airways.3 High local concentration of these agents in the lung maximize their intended effects
and minimize systemic absorption and the potential adverse reactions. Another advantage of this
mode of drug delivery is the rapidity of onset of action after the drug is inhaled as compared to
other modes of delivery. Certain other drugs, such as antibiotics, may also be used for local
effect in the lung parenchyma in patients with infectious diseases, such as pneumocystis carinii
pneumonia.
DISADVANTAGES OF AEROSOLS
Infection
Bronchospasm
Over hydration
AEROSOLS DEVICES
Metered dose inhalers
Dry powder inhalers
Nebulizers
METERED DOSE INHALERS
Introduction
The history of the MDI dates back to 1955. The first MDI included a 50μL metering device, a
10mL amber vial, and a plastic mouthpiece with molded nozzle to administer salts of
isoproterenol and epinephrine. The next year, a surfactant and micronized powder were
added to the propellant, creating the first commercially available formulation. Today the modern
MDI (Figure 1) comprises of a pressurized metal canister containing a mixture of propellants,
surfactants, preservatives, and the drug. Metered dose inhalers are the most commonly used
devices for generation of aerosol. They consist of a micronized form of the drug in a propellant
under pressure with surfactants to prevent clumping of drug crystals. Lubricants for the valve
mechanism and other solvents are the other constituents. When the device is actuated, the
propellant gets exposed to atmospheric pressure, which leads to aerosolisation of the drug. As it
travels through the air, the aerosol warms up leading to evaporation of the propellant that reduces
the particle size to the desirable range. The fraction of drug to the airways ranges from 5 percent
to 15 percent. Propellants used for aerosol generation in MDIs have generated some controversy.
The conventional propellants used in these devices have been chlorofluorocarbon (CFC). In the
year 1987, all substances that could deplete the ozone layer in earth’s atmosphere were banned.
Chlorofluorocarbon is also known to cause this effect and hence came under the imposed ban.
Although products used for medical purposes were exempted from the ban, newer propellants
have been developed. Already MDI using newer propellant like hydrofluoroalkane (HFA) have
become available.
Substitution of HFA for CFC has resulted in critical changes in the pharmacokinetic profile of
drugs; such as beclomethasone used for aerosol therapy. Among other differences, the CFC
based MDIs contain the drug in suspension form whereas the HFA ones have it in a solution
form. Moreover, no surfactant is used in the HFA devices. However, alcohol is added for
dispersal.
The particle size produced by HFA based MDIs is finer and softer and is generated at slower
speeds. Consequently, the oropharyngeal deposition is lesser with HFA based MDIs and delivery
to lower airways is double compared to that of CFC based MDIs. It is no surprise that the major
conclusion to come out of a study comparing the two different propellant based MDIs was that
only 50% of the usual dose used in CFC MDIs was required to produce the equivalent clinical
effect.
Metered dose inhalers have been popular because of ease of usage, small and compact size and
the relative cost-effectiveness. On the other hand, the commonest error in the usage of an MDI is
the lack of coordination between the actuation of the device and the initiation of inspiration.
Many other problems can also be associated with the use of MDI. The physician who prescribes
These devices should keep these things in mind and the same should be conveyed to the patient
as well.
1. Even with the best technique, only 10% to 20% of the total drug makes it to the large airways
and only 5% of the drug reaches the small airways.
2. Various additives and cold propellant in MDIs may cause airway irritation that may lead to
Cough or occasionally, bronchospasm. Since the drug contained is usually a bronchodilator, this
Effect may not be revealed clinically and may manifest as a poor response to the treatment.
3. The medication is held in a suspension with the propellant in the canister. To prevent
undesirable layering of the medication, it is imperative to shake the canister between each
actuation.
4. It is important to keep in mind that the MDI may continue to deliver the aerosol even after the
drug is finished. This aerosol consists only of the propellant at this time. This tends to occur
usually in patients who do not shake the canister well as a routine. Since most manufacturers do
not provide dose counters, patients must keep a track of the number of actuations. Such problems
can be taken care of by noting the manufacturer’s recommended number of actuations and
marking the estimated completion date.
5. Each actuation of the aerosol device leads to cooling of its contents temporally. A 30- to 60-
Second pause between actuations is recommended so as to allow the device to re-warm as the
predictability of the aerosol produced is poor when the contents are cool.
Steps for Ideal Use of an MDI
1. Shake the canister.
2. Hold the canister upright.
3. Gently exhale to functional residual capacity (do not exhale to residual volume).

4. Place the mouthpiece in mouth, between teeth, and close lips or keep the same 5 cm in front
with mouth open.
5. With initiation of inhalation, actuate the canister.
6. Slowly inhale up to the maximum capacity (total lung capacity).
7. Hold breath for 10 seconds or as long as possible.
8. Wait for at least 60 seconds before the next puff.
In breath-activated MDIs which have been available in the West, coordination between breathing
and actuation is not required. These devices consist of a mechanical flow trigger that gets
activated when inhalation flow reaches ≥ 30 L/min. However, a drawback is that the elderly
patient may be unable to use this device.
Valve Holding Chambers/Spacers
To overcome the major problem related to coordination, a valve holding chamber may be used as
an adjunct to the MDI (Figure 2). It is also useful for old patients and those who are unable to
hold breath. This adjunct has many advantages including improved coordination with the
inspiratory flow of the patient. When an MDI is used with spacer devices, reduction occurs in the
Overall particle size of the inhaled aerosol, as larger particles tends to stick to the chamber
walls/valves. This also leads to a reduction in particle velocity leading to decreased upper airway
deposition. It should be explained to the patient that the aerosol must be inhaled immediately
after the MDI is discharged into the chamber and only a single actuation should be discharged
into the chamber for each inhalation.
Following this, the patient should be instructed to breathe in and out for a few breaths before
actuating another discharge of MDI. The reduced oropharyngeal Aerosol Therapy G.C.
Khilnani and A. Banga
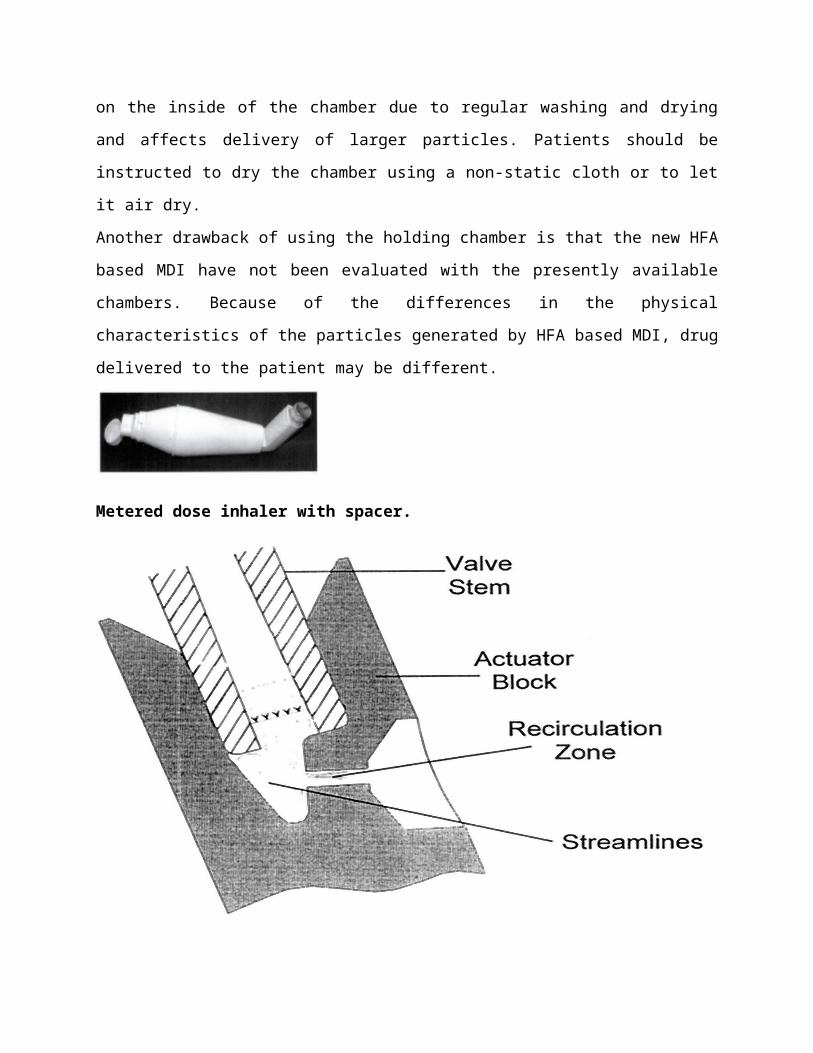
Figure 2. Metered dose inhaler with spacer.
Deposition associated with the use of a spacer chamber is an advantage when using
corticosteroid MDIs as the local adverse effects are then much less likely to occur. In spite of all
these advantages, it has been shown that no extra benefit in terms of delivery is achieved by
using a spacer device by the patients who follow the correct technique with MDI alone. Holding
chambers are also not totally free of problems. Electrostatic charge develops on the inside of the
chamber due to regular washing and drying and affects delivery of larger particles. Patients
should be instructed to dry the chamber using a non-static cloth or to let it air dry.
Another drawback of using the holding chamber is that the new HFA based MDI have not been
evaluated with the presently available chambers. Because of the differences in the physical
characteristics of the particles generated by HFA based MDI, drug delivered to the patient may
be different.
Metered dose inhaler with spacer.
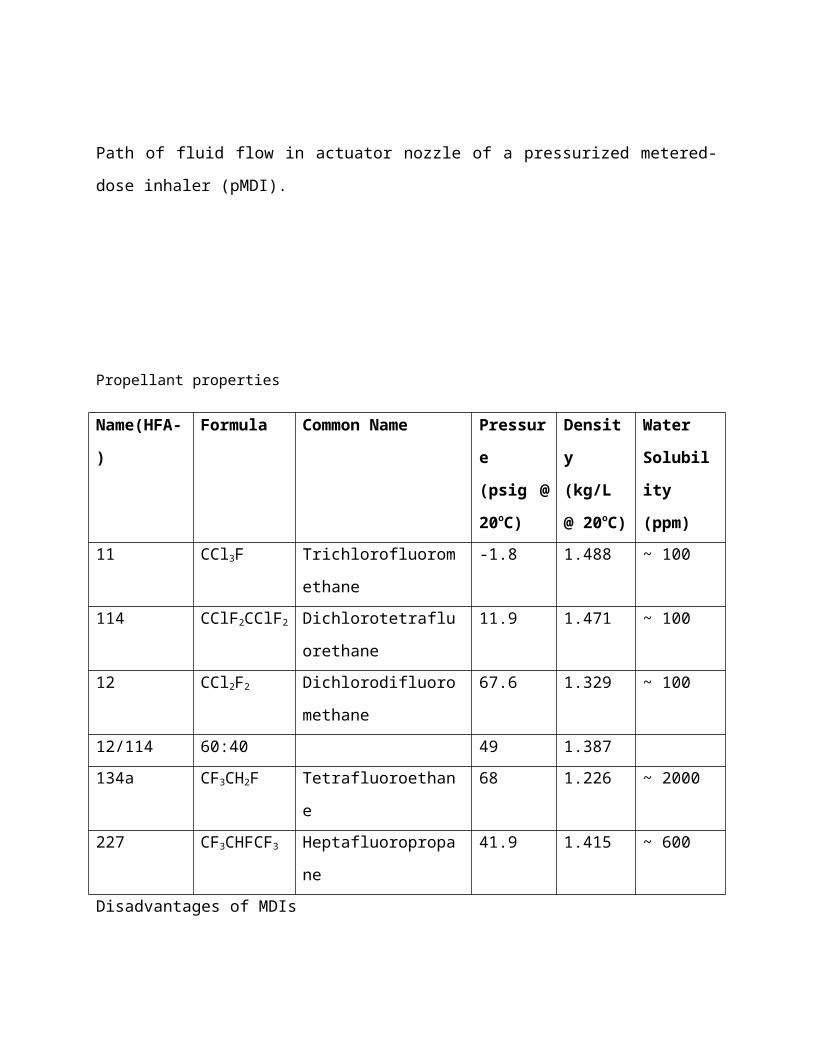
Path of fluid flow in actuator nozzle of a pressurized metered-dose inhaler (pMDI).
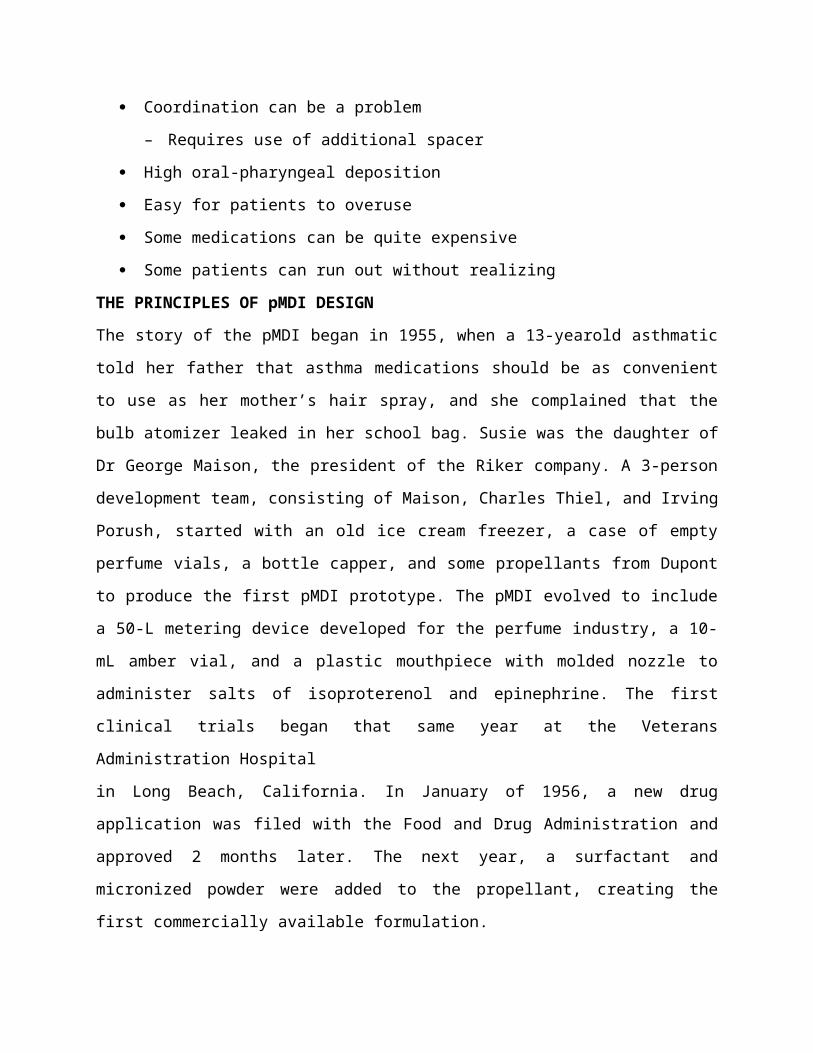
Propellant properties
Name(HFA-) Formula Common Name Pressure
(psig @
20oC)
Density
(kg/L @
20oC)
Water
Solubility
(ppm)
11 CCl3F Trichlorofluoromethane -1.8 1.488 ~ 100
114 CClF2CClF2 Dichlorotetrafluorethane 11.9 1.471 ~ 100
12 CCl2F2 Dichlorodifluoromethane 67.6 1.329 ~ 100
12/114 60:40 49 1.387
134a CF3CH2F Tetrafluoroethane 68 1.226 ~ 2000
227 CF3CHFCF3 Heptafluoropropane 41.9 1.415 ~ 600
Disadvantages of MDIs
Coordination can be a problem
– Requires use of additional spacer
High oral-pharyngeal deposition
Easy for patients to overuse
Some medications can be quite expensive
Some patients can run out without realizing
THE PRINCIPLES OF pMDI DESIGN
The story of the pMDI began in 1955, when a 13-yearold asthmatic told her father that asthma
medications should be as convenient to use as her mother’s hair spray, and she complained that
the bulb atomizer leaked in her school bag. Susie was the daughter of Dr George Maison, the
president of the Riker company. A 3-person development team, consisting of Maison, Charles
Thiel, and Irving Porush, started with an old ice cream freezer, a case of empty perfume vials, a
bottle capper, and some propellants from Dupont to produce the first pMDI prototype. The pMDI
evolved to include a 50-L metering device developed for the perfume industry, a 10-mL amber
vial, and a plastic mouthpiece with molded nozzle to administer salts of isoproterenol and
epinephrine. The first clinical trials began that same year at the Veterans Administration Hospital
in Long Beach, California. In January of 1956, a new drug application was filed with the Food
and Drug Administration and approved 2 months later. The next year, a surfactant and
micronized powder were added to the propellant, creating the first commercially available
formulation.
1 Today the pMDI is a pressurized metal canister containing a mixture of propellants,
surfactants, preservatives, and drug. The drug represents about 1% of the contents, while the
propellants are greater than 80% of the contents, by weight. Traditional Chlorofluorocarbon
pMDIs Chlorofluorocarbon (CFC) pMDIs have largely been incremental improvements over the
original devices from the mid-1950s. With the demands of both newer medications and the
requirements for new, non-ozone-depleting carriers, there have been more substantial changes in
pMDI design and function in the past decade.
Strengths. The pMDI is convenient, lightweight, portable, multidose, and can be stored in any
orientation without leakage. The pMDI reliably provides consistent dosing during the canister
life.
The traditional pMDI is an inexpensive dosage form.
This is much less expensive than any other aerosol device that has multidose convenience.
Limitations. The pMDI is not available for all drugs or dosages, making it difficult for clinicians
to prescribe the same type of device for diverse inhaled medications. These are exacerbated by
the trend of many pharmaceutical companies not to release newer inhaled drugs as pMDIs. The
design of the CFC-propellant pMDI requires initial and frequent priming. Failure to prime the
device results in administration of a substantially lower dose than that prescribed. Unfortunately,
frequent priming tends to waste drug to atmosphere. The greatest single limitation of the pMDI is
the inconsistent dosing that occurs with incorrect use. This includes the impact of hand-breath
asynchrony, excessive inspiratory flow velocity, nose-breathing, and the cold-Freon effect (the
patient stops inhalation when the cold aerosol plume reaches the hypopharynx). For an aerosol
device efficiently to deliver medication to the lower respiratory tract, most of the aerosol
medication particles must be of a size for inhalation and deposition in the airway, generally 0.5–
4.5 m mass median aerodynamic diameter. The patient must inhale the aerosol with a slow, deep
inhalation to maximize aerosol deposition in the airway, followed by a breath-hold to allow
sedimentation of the medication particles.
Extended use of the pMDI beyond the labeled number of doses results in a “tailing-off” effect at
the end of canister life. While the pMDI provides consistent dosing for the number of actuations
listed on the drug label, after that the dose fluctuates between the nominal dose and a negligible
dose. In the absence of a dose-counter, which is not provided with most pMDIs, the patient must
count the number of doses taken to determine the effective life of the pMDI. The method of
“floating” the pMDI canister in water to determine canister depletion is unreliable, and water
entering the nozzle can reduce the emitted dose of subsequent actuations. Environmental factors
such as temperature contribute to inconsistent doses. As the temperature of the canister drops, so
does the emitted dose of the CFC pMDI. This is the basis of recommendations to warm the
pMDI canister to hand temperature prior to use. Heating the canister beyond body temperature
may increase the emitted dose.
Hydrofluoroalkane pMDIs
There is a zone about 10–25 miles above the earth’s surface in which ozone is relatively highly
concentrated. Once released, CFCs rise to the stratosphere, where they are gradually broken
down by ultraviolet light to release chlorine, which depletes stratospheric ozone. This leads to
higher ultraviolet-B radiation levels, which increases the risk of skin cancer and cataracts and
causes important environmental damage. Albuterol pMDIs have historically used the CFCs
trichlorofluoromethane (CFC-11) and dichlorodifluoromethane (CFC-12) as propellants, both of
Which are potent ozone-depleting substances.
The production of ozone-depleting substances is being phased out under the terms of an
international agreement called the Montreal Protocol on Substances that Deplete the Ozone
Layer.17 The Food and Drug Administration has announced a final rule to amend the regulation
(21 Code of Federal Regulations 2.125) on the use of ozone-depleting substances in medical
products.
This rule establishes December 31, 2008, as the date by which production and sale of single-
ingredient albuterol CFC pMDIs must stop and removes the essential-use designation for
albuterol pMDIs. Since most of the pMDIs available in the United States have contained CFCs,
many of these are being reformulated. Several non-CFC products are currently approved and
marketed for a range of different drugs, including non-CFC pMDI versions of albuterol,
beclomethasone, fluticasone, and ipratropium, as well as dry powder versions of fluticasone,
formoterol, and salmeterol. Other non-CFC products are in the latter stages of development.
Hydrofluoroalkane (HFA) pMDIs require a different metering valve, with a smaller aperture,
which produces a much finer particle size with many medications. As well, particle size is
decreased for some corticosteroids (e.g., beclomethasone and flunisolide) that dissolve into
solution in HFA 134a but remain in suspension in CFC. No surfactant is used in the HFA
devices, but alcohol is added for dispersal. It is probable that a change to HFA devices will
require a reassessment of the age-related dose equivalence of CFC pMDIs, discussed later.
Strengths. The development of new environmentally friendly propellants presents an
opportunity for major design enhancements of the pMDI. While some manufacturers of HFA
pMDIs have focused on making the new de Environmental factors such as temperature
contribute to inconsistent doses. As the temperature of the canister drops, so does the emitted
dose of the CFC pMDI. This is the basis of recommendations to warm the pMDI canister to hand
temperature prior to use. Heating the canister beyond body temperature may increase the emitted
dose.
Hydrofluoroalkane pMDIs
There is a zone about 10–25 miles above the earth’s surface in which ozone is relatively highly
concentrated. Once released, CFCs rise to the stratosphere, where they are gradually broken
down by ultraviolet light to release chlorine, which depletes stratospheric ozone. This leads to
higher ultraviolet-B radiation levels, which increases the risk of skin cancer and cataracts and
causes important environmental damage. Albuterol pMDIs have historically used the CFCs
trichlorofluoromethane (CFC-11) and dichlorodifluoromethane (CFC-12) as propellants, both of
which are potent ozone-depleting substances.
The production of ozone-depleting substances is being phased out under the terms of an
international agreement called the Montreal Protocol on Substances that Deplete the Ozone
Layer. The Food and Drug Administration has announced a final rule to amend the regulation
(21 Code of Federal Regulations 2.125) on the use of ozone-depleting substances in medical
products.
This rule establishes December 31, 2008, as the date by which production and sale of single-
ingredient albuterol CFC pMDIs must stop and removes the essential-use designation for
albuterol pMDIs.
Since most of the pMDIs available in the United States have contained CFCs, many of these are
being reformulated.
Several non-CFC products are currently approved and marketed for a range of different drugs,
including non-CFC pMDI versions of albuterol, beclomethasone, fluticasone, and ipratropium, as
well as dry powder versions of fluticasone, formoterol, and salmeterol. Other non-CFC products
are in the latter stages of development.
Hydrofluoroalkane (HFA) pMDIs require a different metering valve, with a smaller aperture,
which produces a much finer particle size with many medications. As well, particle size is
decreased for some corticosteroids (e.g., beclomethasone and flunisolide) that dissolve into
solution in HFA 134a but remain in suspension in CFC. No surfactant is used in the HFA
devices, but alcohol is added for dispersal. It is probable that a change to HFA devices will
require a reassessment of the age-related dose equivalence of CFC pMDIs, discussed later.
Strengths. The development of new environmentally friendly propellants presents an
opportunity for major design enhancements of the pMDI. While some manufacturers of HFA
pMDIs have focused on making the new devices identical to their CFC predecessors, others have
Optimized the design to enhance aerosol delivery and canister/valve performance.
Opportunities inherent in the new propellants and valves include a reduced tailing-off effect at
the depletion of the canister’s contents. With HFA pMDIs, when the end of canister life is
reached, the emitted dose rapidly decreases to a negligible level. The HFA-propelled aerosol has
a lower velocity and gentler plume, which, combined with smaller particle size, results in less
oropharyngeal deposition.
20 These attributes make many of the new HFA propellant inhalers more reliable and efficient
than their CFC predecessors.
Limitations.
As a new device and a new carrier formulation, the HFA pMDI must meet more complex
regulatory requirements for a new drug application. In the United States, HFA pMDIs are
currently limited to only a few formulations. As well, the costs of manufacturing and
development are substantially higher with HFA systems.
Breath-Activated pMDIs
Pirbuterol (Maxair, 3M, St Paul Minnesota) and albuterol HPA (IVAX Laboratories, Miami,
Florida) are available in the Autohaler in North America. In Europe they also have the Easyhaler
breath-actuated device (Baker Norton, Ireland). These devices have a mechanical flow trigger
That activates the device when inhalation flow reaches 30 L/min, which decreases the need for
coordination.
They also produce softer mist. Because of the flow needed to activate these devices, patient
ability to use the device is age-dependent.
Pressurized Metered-Dose Inhaler Accessory Devices
A variety of pMDI accessory devices have been developed to overcome the limitations of pMDI
administration (handbreath coordination problems. Spacers and Valved Holding Chambers
Spacers and valved holding chambers are accessory devices that, when properly designed, reduce
oropharyngeal deposition of drug, ameliorate the bad taste of some medications, eliminate the
cold FREON effect, and, in the case of valved holding chambers, reduce drug loss associated
with poor hand-breath coordination. Table 3 outlines recommended steps for self-administering a
bronchodilator using a pMDI with a valved holding chamber.
Clinicians should be careful to distinguish spacers from valved holding chambers. A spacer
device is a simple open-ended tube or bag that, with sufficiently large volume, provides space for
the pMDI plume to expand by allowing the CFC propellant to evaporate. To perform this
function, a spacer device must have an internal volume of over 100 mL, and provide a distance
of 10–13 cm between the pMDI nozzle and the first wall or baffle in the plume’s path. Smaller
low-volume spacers can reduce respiratory dose by 60% and offer no protection against poor
coordination between actuation and breathing pattern. Spacers with internal volumes greater than
100 mL generally provide some protection against loss of dose from early firing of the pMDI,
although exhaling immediately following the actuation clears most of the aerosol from the
device, wasting the dose.
The valved holding chamber (usually 140–750 mL) allows the plume to expand, and
incorporates a one-way valve that permits the aerosol to be drawn from the chamber during
inhalation only, diverting exhaled gas to the atmosphere and not disturbing remaining aerosol
suspended in the chamber. Thus, the valved holding chamber combines the benefits of a spacer
with the advantage of protecting the patient from loss of dose due to poor handbreath
coordination.
Fink et al performed in vitro testing of drug delivered from a pMDI alone and from a pMDI in
combination with a variety of spacers and holding chambers, when actuation of the pMDI was
(1) synchronized with the beginning of inspiration, (2) one second before inspiration, or (3)
during exhalation. Figure 3 shows the mean proportion of drug available to the lower respiratory
tract with pMDI and a variety of small-volume spacers, large-volume spacers, bag holding
chambers, and valved holding chambers. The pMDI alone and small-volume spacers offered
little protection against drug loss with actuation 1 second before inhalation or with actuation
during exhalation. The large volume spacers offered good dose protection with actuation 1
second before inhalation, but not with actuation during exhalation. The valved holding chambers
provided good protection with actuation 1 second before inhalation and 70% of baseline dose
when the pMDI was actuated during exhalation.
A patient with a small tidal volume may use multiple breaths to empty the aerosol from the
chamber, 3–6 except when there is an exceptionally large dead space. A valved holding chamber
can also incorporate a mask to allow effective pMDI administration in a patient who is unable to
use a mouthpiece because of size, age, coordination, or mental status.5 For use with infants, it is
critical that these masks have minimal dead space, be comfortable to the child’s face, and that the
chamber have a valve that opens or closes with the low inspiratory flow generated by an infant.
The use of a valved holding chamber should be encouraged, especially for infants and small
children, and for any child with steroid administration. A valved holding chamber reduces the
need to coordinate the breath with actuation, reduces oral deposition (and, therefore, bad taste),
decreases cold FREON effect, and decreases MMAD, which increases respirable particle mass,
improves lower respiratory tract deposition, and significantly improves therapeutic effect. These
devices reduce the pharyngeal deposition of aerosol 10–15-fold, compared to administration
without a holding chamber. This decreases the swallowed amount, which is an important
consideration with steroid administration.
The high percentage of oropharyngeal drug deposition with steroid pMDIs can increase the risk
of oral yeast infections (thrush). Rinsing the mouth after steroid use can reduce this problem, but
most pMDI steroid aerosol impaction occurs deeper in the pharynx, which is not easily rinsed.
For this reason, steroid pMDIs should always be used in combination with a valved holding
chamber.
MDI CLEANINGMDI CLEANING
Patients are taught the following:
1. Once per week remove all canisters from their sleeves.
2. Wash the sleeve under warm running water, shake off excess water and air dry
3. After it is dry, replace canister and actuate the cannister once to seat the cannister and
clear out any moisture.
Washing all MDIs once per week at the same time is often more convenient and easier to
remember for our COPD patients.
DRUGS TO BE USED IN METERED DOSE INHALERS
Salbutamol
Terbutaline Sulphate
Salmeterol Xinafoate
Formoterol Fumarate
Ipratropium Bromide
Sodium Cromoglycate
Beclomethasone Dipropionate
Budesonide
Fluticasone propionate
Nedocromil
Sodium chromoglycate
Fenoterol hydrobromide
Eformoterol fumarate
SAFETY OF AEROSOL THERAPY
Although drugs delivered as aerosols have been largely found to be extremely safe, certain
clinical situations may require caution on the part of the clinician. Paradoxical bronchospasm is
known to occur with DPI formulations of anticholinergic drugs. High doses of β2- agonists
administered through the nebuliser have been reported in rare cases to lead to arrhythmias.
Inhaled corticosteroids may have local and systemic adverse effects. Among the local adverse
effects oral candidiasis, dysphonia and cough are well known. Incidence of oral candidiasis may
vary from 0%-77% depending on the definition used. The data on comparative risk of
developing candidiasis with different corticosteroids is conflicting.67-70 However, there seems
to be a trend towards higher incidence of candidiasis with fluticasone propionate, especially at
higher doses, in comparison to budesonide and ciclesonide. Moreover, fluticasone propionate
may also result in esophageal candidiasis, again in a dose dependent manner. Incidence of
dysphonia is to the tune of 5%-50% and is the result of vocal stress and is again dose dependent.
Cough occurs in as many as one-third of patients on inhaled corticosteroids with no difference
between different formulations. The usual interventions aimed at preventing these local adverse
effects consist of oral rinse after inhalations, reduction in frequency of inhaled corticosteroids
and use of spacer device or holding chamber. Nonetheless, there have been some contradictory
results with spacer devices where incidence of cough and dysphonia were noted to be higher
with their use. Among the systemic adverse effects, large doses of inhaled corticosteroids may
lead to suppression of hypothalamus-pituitary-adrenal axis and must be used cautiously in
growing children. A meta-analysis did not find an increase in the risk of loss of bone density and
fractures. However, the risk of glaucoma and cataracts tends to increase in patients taking long-
term inhaled corticosteroids. Risk of crossinfection with the use of nebuliser in hospital patients
is also well known and various methods for decontamination of nebulisers have been described.
CONCLUSIONS
Aerosol therapy has been around for more than 50 years and forms the cornerstone of
management of obstructive airway diseases. Recent times have witnessed many advances in this
field. Improved aerosol generators with different drug formulations are now available. However,
the fraction of total drug eventually delivered to the site of action still remains small. Metered
dose inhalers with or without a valved spacer have emerged as the preferred devices for aerosol
generation. This holds true for in-hospital patients as well as chronic therapy of patients with
obstructive airway diseases. Nebulisers are the generators of choice in an emergency setting.
Many new drugs, including insulin, are in the process of development to be used as aerosols that
are likely to improve management strategies for various diseases.
Related Documents
![Tiotropium Respimat Soft MistTM Inhaler: A Review of Its ...€¦ · metered-dose inhalers (pMDIs) [8]. This has the potential to reduce the extent of oropharyngeal deposition and](https://static.cupdf.com/doc/110x72/5f2c1debf40fb2326f462ad8/tiotropium-respimat-soft-misttm-inhaler-a-review-of-its-metered-dose-inhalers.jpg)










![[PPT]Respiratory Pharmacology - Pat Heyman - Family, …patheyman.com/sites/default/files/nursing/notes/06... · Web viewRespiratory Pharmacology Inhaled Drugs Metered Dose Inhalers](https://static.cupdf.com/doc/110x72/5b06e2ab7f8b9a5c308d908c/pptrespiratory-pharmacology-pat-heyman-family-viewrespiratory-pharmacology.jpg)