Management of Bipolar Affective Disorders

Management of Bipolar Affective Disorders
Dec 30, 2015
Management of Bipolar Affective Disorders. Manic Episode. Persistently elevated,expansive or irritable mood for at least a week Presence of at least 3 typical symptoms: - PowerPoint PPT Presentation
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Management of Bipolar Affective Disorders
Manic Episode
• Persistently elevated,expansive or irritable mood for at least a week
• Presence of at least 3 typical symptoms:
decreased need for sleep, flight of ideas,grandiosity, uncharacteristic risk taking, distractibility, agitation, increase in pleasurable activities
• Marked impairment of functioning, necessity for hospitalisation, or psychotic features
Hypomania
• Impairment is less severe
• Psychotic features are absent
• Social and occupational functioning are not significantly impaired
• Hospitalisation is usually not required
Mixed Episode
• Depressive symptoms occur in the context of manic thinking
• Depressive and manic symptoms alternate from day to day or even hour to hour
• Unpleasant agitation is common
Bipolar Affective Disorder
• Bipolar I DisorderA recurrent mood disorder featuring one or more manic or mixed episodes, or both manic and mixed episodes and at least one major depressive episode
• Bipolar II DisorderCharacterised by one or more episodes of major depression and at least one hypomanic episode
• CyclothymiaPersistent instability of mood (> 2 years duration) featuring numerous periods of mild depression and elation, none of which meet the criteria for depression or mania
Cycle Frequency
• Manic episodes last between 2 weeks and 5 months
• Depressive episodes have a mean duration of 6 months
• 10-20% of people with bipolar disorder experience rapid cycling, characterised by 4 or more episodes of depression or mania per year and only short euthymic episode in between
• A rapid cycling pattern is often associated with a poor prognosis
Epidemiology
• Bipolar disorder (I +II) has a prevalence of 1.3% in the UK • Estimates suggest that approximately 0.5 million people
over 15 in England and Wales are affected
• Bipolar I disorder affects men and women equally, but bipolar II is commoner in women
• Unlike schizophrenia, it is prevalent in higher social classes
• In the USA, an average delay to diagnosis of 6 years is common
Course of the Illness
• Peak age of onset is 15-24 years
• If onset occurs >60 years think of an organic cause
• More than 90% of people who have a single manic episode will have a recurrence
• 10-15% will have more than 10 episodes in their lifetime
• Lifetime suicide risk is 15-19%
• Co-morbid drug and alcohol misuse is common
Aetiological Factors
• Genetic– Mode of inheritance is complex, likely to involve several genes
– Lifetime risk of developing bipolar disorder• First degree relatives 11%
• Monozygotic twins 79%
• Dizygotic twins 19%
Birth Effects
• Excess of spring and winter births and maternal fever
Pathophysiology
• Neurotransmitter Dysfunction– ? deficits in Na+K+ATPase and second messenger
systems– ?serotonin system dysfunction
Neuroendocrine Dysfunction– Grade II hypothyroidism is found in 25% of rapid
cycling bipolar patients compared with 2-5% in depression
Pathophysiology (cont)
Brain Structural Changes
Gross pathology associated with a poor prognosis
– smaller temporal lobes and caudate nuclei
– Patchy white matter lesions on MRI
– Pre-frontal-limbic subcortical abnormalities
– reduced blood flow in the pre-frontal cortex
– hypofrontal pattern of glucose metabolism
– frontal lobe dysfunction in BPD I
Fundamentals of Patient Management
• Diagnosis
• Access to services and safety
• Enhanced Care
Delays to Diagnosis
• Irritability or aggression may be misdiagnosed as personality disorder in the absence of mood elevation
• Adolescent behavioural disturbance
• Substance misuse
• Exclude causes of 2o mania
Access to Services and Safety
• Involve a psychiatrist in assessment and management
• Mania or psychotic depression are psychiatric emergencies
• Hospital admission or intensive community management
• The Mental Health Act is often required • Early Intervention Teams
Assessment of Risk
• Ideally involve an informant
• Suicide
• Excessive spending
• Sexual promiscuity
• Driving
• Violence
Enhanced Care
• Establish and maintain a therapeutic alliance– Treatment adherence– Education
Awareness of early signs of relapse– recognise stressors– manage sleep disturbance– promote regular patterns of activity– involve the family
• Manage functional impairments– withdrawal from work (average 12 weeks)– discourage major decisions– consider needs of children and carers
Treatment of different phases of bipolar disorder
• Acute manic or mixed episode
• Acute depressive episode
• Long-term treatment
• Pregnancy and the post-partum period
Acute Manic/Mixed Episode
• Use atypical antipsychotics + mood stabiliser
• Benzodiazepines are useful short term to promote sleep
• Additional medications should be tapered and stopped as symptoms improve
Acute Depressive Episode
• Risk of mania or rapid cycling with use of antidepressant
• Ideally treat with mood stabiliser alone
• SSRIs are less likely to promote manic switch
• Discontinue the antidepressant when symptoms remit (e.g. 12 weeks)
Treatment of bipolar depression
• Aim to treat depression without causing switching or destabilising mood
• Ideally use a mood stabiliser or a combination of 2• Lamotrigine is an antidepressant mood stabiliser• Use antidepressants with caution
– modern antidepressants (SSRI, SNRI)– short courses– long term treatment is only suitable for those who
repeatedly relapse on withdrawal

Mental Health Register
• Regular (annual) physical health checks
• Relevant blood tests
• Need to establish between primary and secondary care respective responsibilities
Longterm Treatment:Drugs
• Mood stabilisers are drugs that prevent relapse to either pole of the illness
• Some mood stabilisers are more effective against mania (lithium, olanzapine) or depression (lamotrigine)
Lithium
– response rate 70-80%
– associated with reduced suicide rate compared with other mood stabilisers
– associated with weight gain, polyuria, polydipsia
– toxic side effects and potentially fatal in overdose
– risk of irreversible renal and thyroid damage
– rapid discontinuation is linked to marked affective instability and suicide risk
Monitoring Lithium Therapy
• Serum Lithium levels 3-6 monthly
• U+E, Thyroid function and calcium every 6 months
Anticonvulsants as mood stabilisers
• Anticonvulsants as mood stabilisers– sodium valproate (Epilim, Depakote)– carbamazepine (tegretol)– lamotrigine (lamictal)– gabapentin– topiramate
Monitoring of full blood count and liver function are required 6 monthlyPotential for drug interactions
Antipsychotics
Atypical Antipsychotics
• Recently licensed for acute and maintenance treatment– Olanzapine– Quetiapine– Risperidone
6 monthly glucose monitoring required with atypical antipsychotics
Combination therapies
• Combination of two mood stabilisers
• An antipsychotic and a mood stabiliser
• An antidepressant and a mood stabiliser
• Short term add-ons (hypnotics and antipsychotics)
Non-pharmacological strategies
• Facilitate acceptance of the disorder • Identify and manage psychosocial stressors• Improve medication adherence• Recognition of early signs of relapse• Empower the individual• Identify and modify maladaptive thinking patterns
Does Cognitive Therapy improve Outcome in BPD?
• CBT has been shown to
– improve compliance with medication– reduce admissions / bed days for mania– improve social functioning
Bipolar Disorder and Pregnancy
• Compliance with treatment during pregnancy– maintenance of mental health– normal bonding
– risk of teratogenesis– neonatal side effects
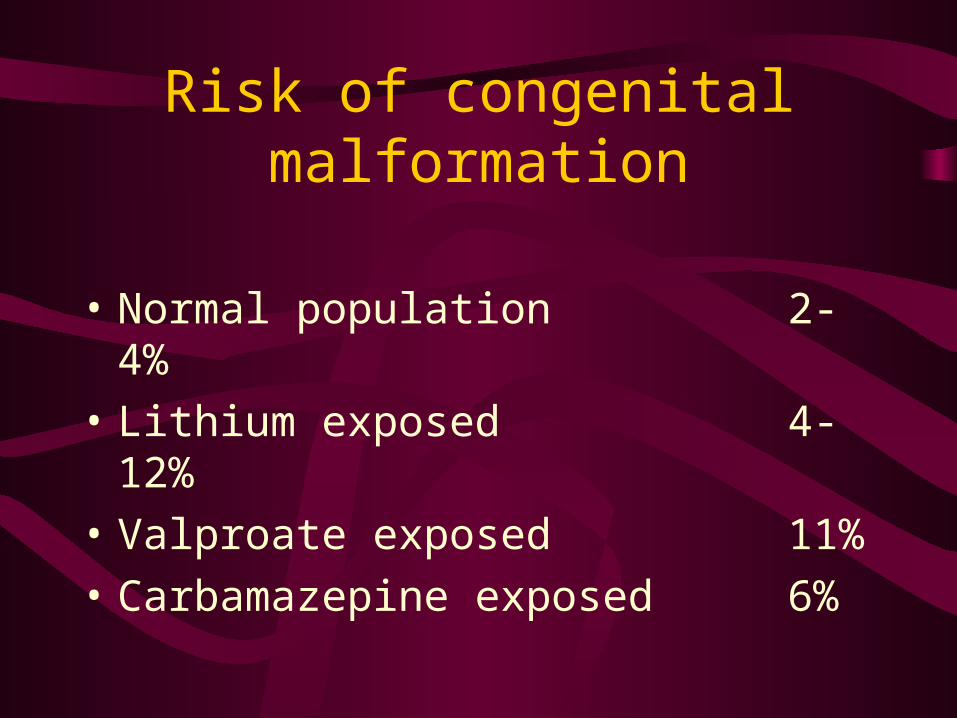
Risk of congenital malformation
• Normal population 2-4%
• Lithium exposed 4-12%
• Valproate exposed 11%
• Carbamazepine exposed 6%
Specific teratogenic associations
• Lithium 0.05-0.1% risk of cardiovascular
anomalies
• Valproate and Carbamazepine1-2 % risk of congenital abnormality
including neural tube defect and foetal hydantoin syndrome
Pregnancy and bipolar disorder
Pregnancy should be planned
Treatment options depend on patient history and preference– withdrawal of medication– change of medication– lowering dose (slow release formulations)
Those exposed to teratogens in the first trimester should be offered high resolution ultrasound scan at 16-18 weeks gestation
Maternal physiological changes result in variable serum levels of mood stabilisers especially lithium
Postpartum
• Toxic and withdrawal effects of mood stabilisers in neonates
• All drugs enter breast milk. Breast feeding not advised for lithium takers
• Increased risk of first admission post-partum
• Increased risk of suicide (and infanticide)
Evidence Based Guidelines for Treating Bipolar Disorder
• www.bap.domainwarehouse.com/consensus/FinalBipolarGuidelines.pdf
Related Documents