Lingual Orthodontics and Forced Eruption: A Means for Osseous and Tissue Regeneration. Case Report Maria Giacinta Paolone*, Roberto Kaitsas**, Gaetano Paolone***, V assilios Kaitsas**** *Specialist in Orthodontics, Private Practice, Rome, Italy. **Oral Surgeon, Private Practice, Rome, Italy. ***Private Practice, Rome, Italy. ****Professor Dental Materials, Faculty of Chemistr y , Univeristy of Siena, Italy . Correspondence to: Maria Giacinta Paolone Viale dei Quattro Venti, 233 - 00152 Roma Italia T el/Fax: +39-06-583.58.57 e-mail: [email protected] 46 1 Lingual Orthodontics and Forced Eruption PROGRESS in ORTHODONTICS2008; 9(2):46-57 An hopeless upper central incisor was subjected to forced eruption in order to improve and develop the implant site by distraction of the pe- riodontal ligament-alveolar bone complex. The orthodontic extrusion was carried out with two aesthetic approaches: lingual orthodontics and a composite resin 2-2 veneer pontic. The first part of the extrusion was realized with lingual orthodontics alone, then, when the crown had been remodelled in its greatest part and the aesthetics was no mo- re acceptable to the patient a composite resin 2 -2 veneer pontic was bonded to the vestibular side of the other three incisors to mimetis e the extruded tooth and to be anchorage to the lingual mechanics. The or- thodontic preparation of the implant site allowed the correction of the periodontal defect due to the fracture, the enhancement of the alveo- lar bone and the soft tissue remodelling. M Gi Paolone, R Kaitsas, G Paolone, V Kaitsas. Lingual Orthodontics and Forced Eruption: A Means for Osseus and Tissue Regeneration. Case Report. Prog Orthod 2008;9(2):46-57. Introduction Orthodontic tooth movement can modify and improve the perio- dontal anatomy of the hard and soft tissues morphology even con- cerning periodontally damaged or fractured teeth 1-7 . Orthodontic ex- trusion or forced eruption is a non- surgical technique undertaken to increase the amount of available alveolar bone for implant site de- velopment and fixture place- ment 8,9 . The periodontal ligament can be used for distraction-osteo- genesis. The fibers of periodontal ligament are inserted in the perio- steum of the alveolar bone. If a tension is applied new bone is de- posited. If the force of tension is

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

8/8/2019 Lingual Incisor
http://slidepdf.com/reader/full/lingual-incisor 1/12
Lingual Orthodontics and Forced Eruption: A Means for Osseous and Tissue Regeneration.Case Report
Maria Giacinta Paolone*, Roberto Kaitsas**, Gaetano Paolone***, Vassilios Kaitsas****
*Specialist in Orthodontics, Private Practice, Rome, Italy.**Oral Surgeon, Private Practice, Rome, Italy.***Private Practice, Rome, Italy.****Professor Dental Materials, Faculty of Chemistry, Univeristy of Siena, Italy.
Correspondence to:Maria Giacinta Paolone
Viale dei Quattro Venti, 233 - 00152 Roma ItaliaTel/Fax: +39-06-583.58.57e-mail: [email protected]
46
1 Lingual Orthodontics and Forced Eruption
PROGRESS in ORTHODONTICS 2008; 9(2):46-5
An hopeless upper central incisor was subjected to forced eruption inorder to improve and develop the implant site by distraction of the pe-riodontal ligament-alveolar bone complex. The orthodontic extrusionwas carried out with two aesthetic approaches: lingual orthodonticsand a composite resin 2-2 veneer pontic. The first part of the extrusionwas realized with lingual orthodontics alone, then, when the crown
had been remodelled in its greatest part and the aesthetics was no mo-re acceptable to the patient a composite resin 2-2 veneer pontic wasbonded to the vestibular side of the other three incisors to mimetise theextruded tooth and to be anchorage to the lingual mechanics. The or-thodontic preparation of the implant site allowed the correction of theperiodontal defect due to the fracture, the enhancement of the alveo-lar bone and the soft tissue remodelling.
M Gi Paolone, R Kaitsas, G Paolone, V Kaitsas. Lingual Orthodontics andForced Eruption: A Means for Osseus and Tissue Regeneration. Case Report.Prog Orthod 2008;9(2):46-57.
Introduction
Orthodontic tooth movement canmodify and improve the perio-dontal anatomy of the hard andsoft tissues morphology even con-cerning periodontally damaged orfractured teeth1-7. Orthodontic ex-trusion or forced eruption is a non-surgical technique undertaken toincrease the amount of availablealveolar bone for implant site de-velopment and fixture place-
ment8,9. The periodontal ligamentcan be used for distraction-osteo-genesis. The fibers of periodontalligament are inserted in the perio-steum of the alveolar bone. If atension is applied new bone is de-posited. If the force of tension is
8/8/2019 Lingual Incisor
http://slidepdf.com/reader/full/lingual-incisor 2/12
and the consequent surgical thera-pies. The preservation of alveolardimension appears important in or-der to reduce further surgical pro-cedures14. The “orthodontic extru-sive remodelling”11 increases andmodifies not only the hard-tissueprofile but also the soft-tissue levelof the potential implant sites15-20.As the anterior and aestheticaspect of the mouth is often invol-ved in this condition, the literaturesuggests lingual devices as ae-sthetic anchoragage21-24.The aim of this work is the propo-sal of a “total” aesthetic approach
for orthodontic extrusion: the com-bination of a classical lingual ap-pliance and a composite resin 12-11-x-22 veneer pontic to minimisethe aesthetic impact of the extru-sion: this double aesthetic solutionallowed us as clinicians to propo-se the complete treatment includingimplant site development and re-duce compromises.
Case report
The patient was a Caucasian 57 years old male. His dental history in-cluded a previous episode of den-tal trauma 5 years previously treatedby another practitioner with root ca-nal treatment and a fixed crownand metal post core. The recent hi-
story of concerns related to a sub-sequent traumatic episode threemonths previously restored with aconsequent root fracture below thebone level on the mesio-vestibular si-de with the loss of the mesio-vesti-bular alveolar wall. The patient wasvery cooperative and presented no
47
Lingual Orthodontics and Forced Eruption 2
PROGRESS in ORTHODONTICS 2008; 9(2):46-57
Un incisivo centrale superiore condannato all’estrazione è stato sot- toposto ad estrusione forzata ed estrazione ortodontica al fine di svi- luppare un corretto sito implantare attraverso la distrazione del com- plesso legamento parodontale-osso alveolare. L’estrusione ortodonti- ca è stata realizzata attraverso due approcci estetici: l’ortodonzia lin- guale ed una mascherina in composito cementata sulla superificie ve-
stibolare dei rimanenti tre incisivi. La prima parte dell’estrusione è sta- ta eseguita con la sola ortodonzia linguale, appena la corona non erapiù accettabile esteticamente per il paziente, è stata cementata la ma- scherina in composito per mimetizzare il residuo radicolare estruso e per ancoraggio. La preparazione ortodontica del sito impiantare hapermesso la correzione del difetto parodontale dovuto alla frattura,l’aumento dell’osso alveolare ed il rimodellamento dei tessuti molli.
Key words: Orthodontic eruption, orthodontic extrusion, forcederuption, implant, implant site development, lingual orthodontics,osseous regeneration, tissue regeneration.
applied in a vertical extrusive di-rection the alveolar bone heightcan be improved if the force, thespeed and the inflammation is con-trolled. The biologic potential ofthe periodontal ligament stimula-ted by extrusive forces can enhan-ce the regenerative potential of fu-ture periodontal surgery includingguided tissue regeneration, elimi-nating an intra-bony defect andaugmenting a vertically reducedalveolar ridge deformity10. For the-se reasons a tooth of poor pro-gnosis should not be extracted asfirst choice but can offer with ad-
junctive procedures an an aid to
improve the osseous and tissueanatomy to provide a better andmore predictable implant surgeryand to obtain a better aestheticalprosthetic result11-13. The loss forfracture or periodontal reasons ofan anterior tooth and the subse-quent implant substitution is a chal-lenging procedure for both the sur-geon and prosthodontist due tohigh esthetic demands during andafter treatment. The vestibular cor-tical plate covering the roots of themaxillary teeth is very thin and itsporosity makes it susceptible toeasy resorption following perio-
dontal and periapical infections
8/8/2019 Lingual Incisor
http://slidepdf.com/reader/full/lingual-incisor 3/12
tion: crown lengthening was notappropriate due to a possible pooraesthetic result. Forced eruption fol-lowed by prosthetic restoration co-uld not be completed due to apoor crown-root ratio.The patient presented a class II pro-file with a retrognathic mandible,the profile confirmed a class II ske-letal pattern with a small mandi-
48
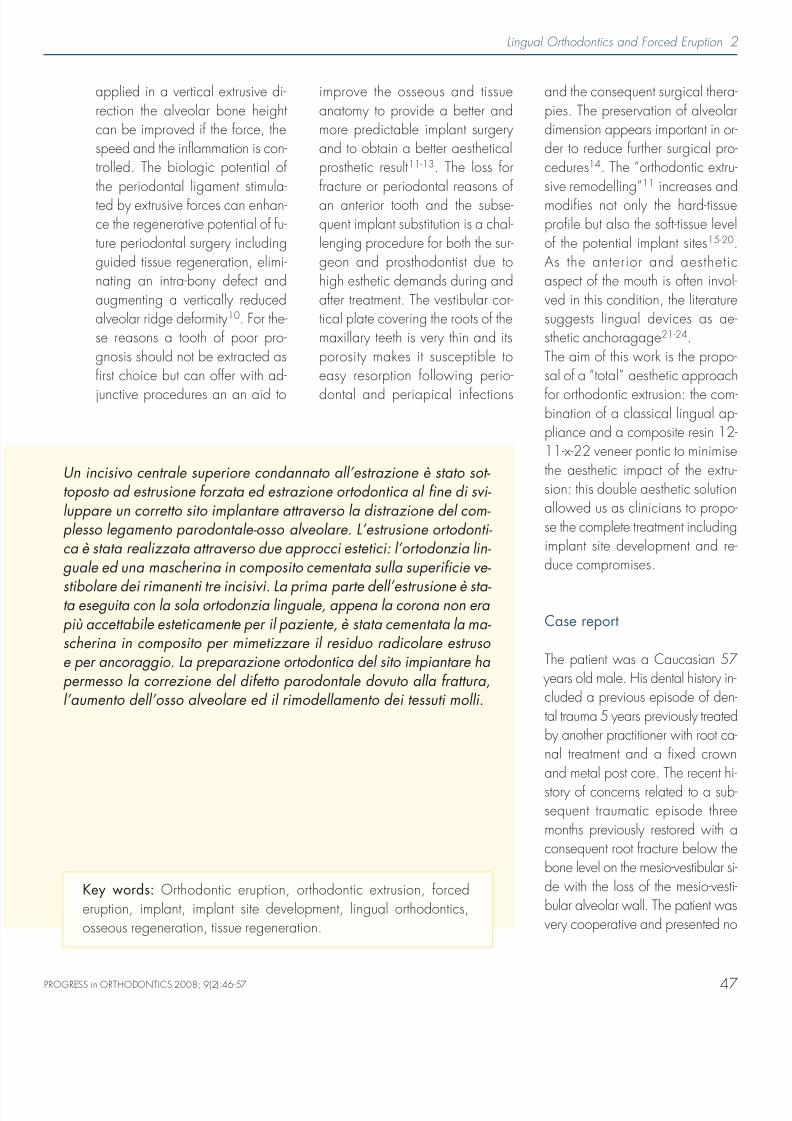
contraindication to orthodontic treat-ment. The probing evaluation re-vealed a mesio-vestibular defect of9mm on the mesial and 5 not onthe vestibular aspect (Tab. 1). Theradiographic examination confir-med the presence of the fracturewith a displaced root fragment be-low the bone level, the osseous de-fect, and the definite loss of the
3 Lingual Orthodontics and Forced Eruption
tooth (Fig. 1a-g).The treatment alternative wascrown lengthening and forced erup-tion followed by prosthetic restora-
Tab. 1 Periodontal probing of theupper two central incisors.
11 21V 212 953P 212 642
Fig. 1a-g Pre-treatment records.
a b
c d
e f g
PROGRESS in ORTHODONTICS 2008; 9(2):46-5

8/8/2019 Lingual Incisor
http://slidepdf.com/reader/full/lingual-incisor 4/12
49
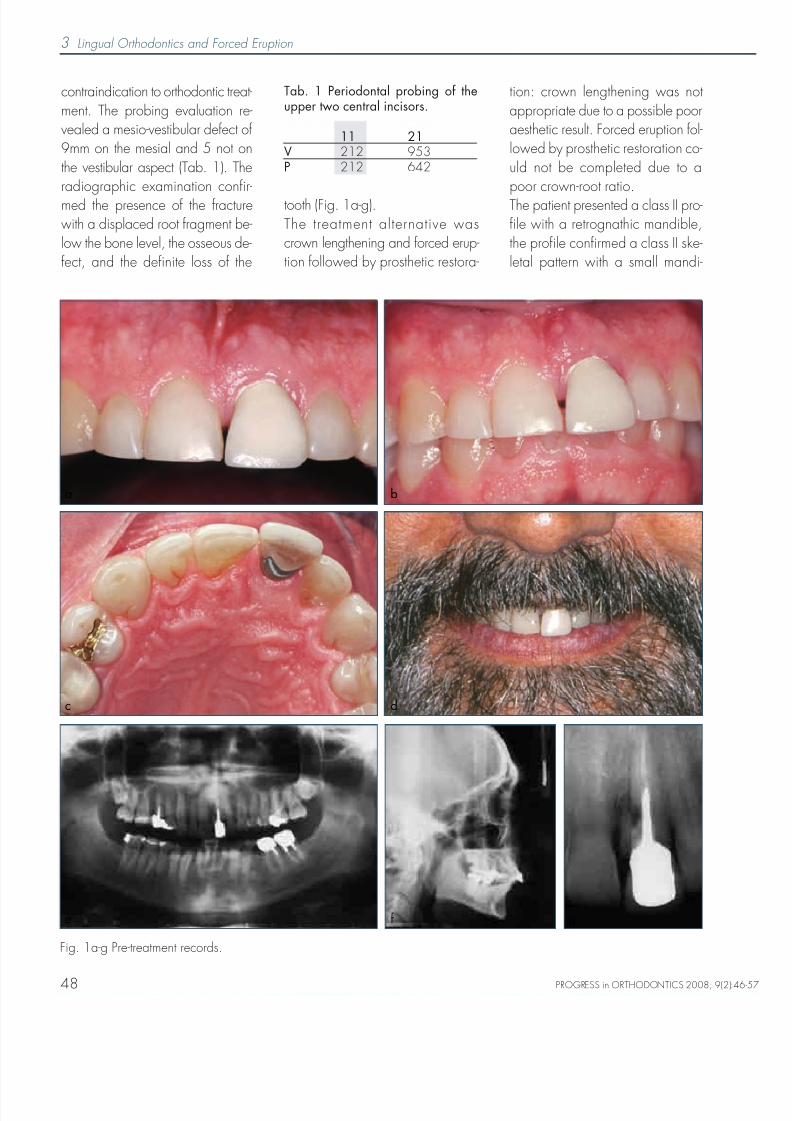
was performed with a lingual ap-pliance in order to preserve ae-sthetics during the mechanics. Thepatient refused a completed ortho-dontic treatment which should haveincluded maxillo-facial surgery. Forthis reason the lingual appliancewas applied only on the upper an-terior teeth including the first pre-molars in order to perform the onlyorthodontic extraction of the upperincisor. The patient was bondedwith lingual brackets (Ormco 7thgen) and a .016 CuNiTi for thefirst month (Fig. 2). The crown ofthe incisor was etched with HF (fluo-
ridric acid) and pretreated with si-lane. The brackets on the fracturedincisor was placed apically in rela-tion to the level of the others. The pa-tient was seen every two weeks toactivate the appliance, to obtain aslow and light osseous movement of0.5mm per month and to level theincisal edge. In the meanwhile thepatient was under periodontal con-
trol to reduce inflammation. Duringthe second month the extrusion wasperformed with a .016 TMA (Fig.3), then with .017x.017 TMA tocontrol and prevent radicular vesti-bular torque which could destroythe thin cortical plate17. The extru-sion movement was realised withlingual orthodontic mechanics andusing the traction to the pontic inorder to have a detailed control of
the radicular movement in terms offorce and direction. For this reasonAfter two months the brackets onthe incisor was re-bonded more api-cally, then, when it was no morepossible to use the crown for brac-ket bonding because the greatestpart of the crown had been reduced
Lingual Orthodontics and Forced Eruption 4
Une incisive centrale supérieure avec un pronostic défavorable aétée soumise à l’éruption othodontique forcée afin d’améliorer et dé-velopper le site implantaire par la distraction du complexe ligament-alvéolaire périodontale et os. L’extrusion orthodontique a été réalisée
avec deux approches esthétiques: l’orthodontie linguale et un veneer2-2 de résine composite. La première partie de l’extrusion a été faiteavec une orthodontie linguale seule, puis, quand la couronne avait étécoupée dans sa plus grande partie et l’esthétique ne semblait plus ac-ceptable au patient on a utilisé un veneer de résine composite 2-2 col-lée sur le côté vestibulairedles trois incisives saines pour simuler la dentsoumise à l’éruption othodontique forcée et pour être un ancrage àla mécanique linguale. La préparation orthodontique du site implan-taire a permis la correction du défaut périodontique, l’amelioration del’os alvéolaire et le remodelage du tissu mou.
Traduit par Maria Giacinta Paolone
Un mal pronóstico sometió la erupción forzada de un incisivo central superior, a fin de mejorar y desarrollar la zona implantar con la dis- tracción del ligamento periodontal en un hueso alveolar complicado.La extrusión ortodontica se realizo con métodos estéticos diferentes:con un “eneer pontic” de 2-2 . La primera parte de la extrusión se hi- zo con ortodoncia lingual y cuando la mayor parte de la corona fue remodelada, el paciente no acepto la situación estética. Entonces el “veneer pontic” de 2-2 se cemento por vestibular utilizando como an- claje la parte lingala.La preparación de ortodontica a de la zona del implante permitio lacorrección del defecto periodontal debido a la fractura, la mejora de los hueso alveolar y la remodelación de tejidos blandos.
Traducido por Santiago Isaza Penco
ble. The cephalometric evaluationconfirmed the facial analysis withan antero-posterior discrepancy(ANB 6°) a mandibular deficiency(SNB 71°) an almost normal ma-xilla (SNA 77°) and reduced man-dibular plane angles (FMA 19°,SNpM 32°). The patient referredno history of TMJ and muscularpain or sound. The dental exami-
nation showed the absence of theright second premolar and confir-med a dental molar class I and ca-nine class II with an increased OVJand OVB.At the very beginning the patientwas treated with a periodontal ap-proach with initial therapy. After 8weeks the periodontal re-evaluationwas realized. Orthodontic treatment
PROGRESS in ORTHODONTICS 2008; 9(2):46-57
8/8/2019 Lingual Incisor
http://slidepdf.com/reader/full/lingual-incisor 5/12
50
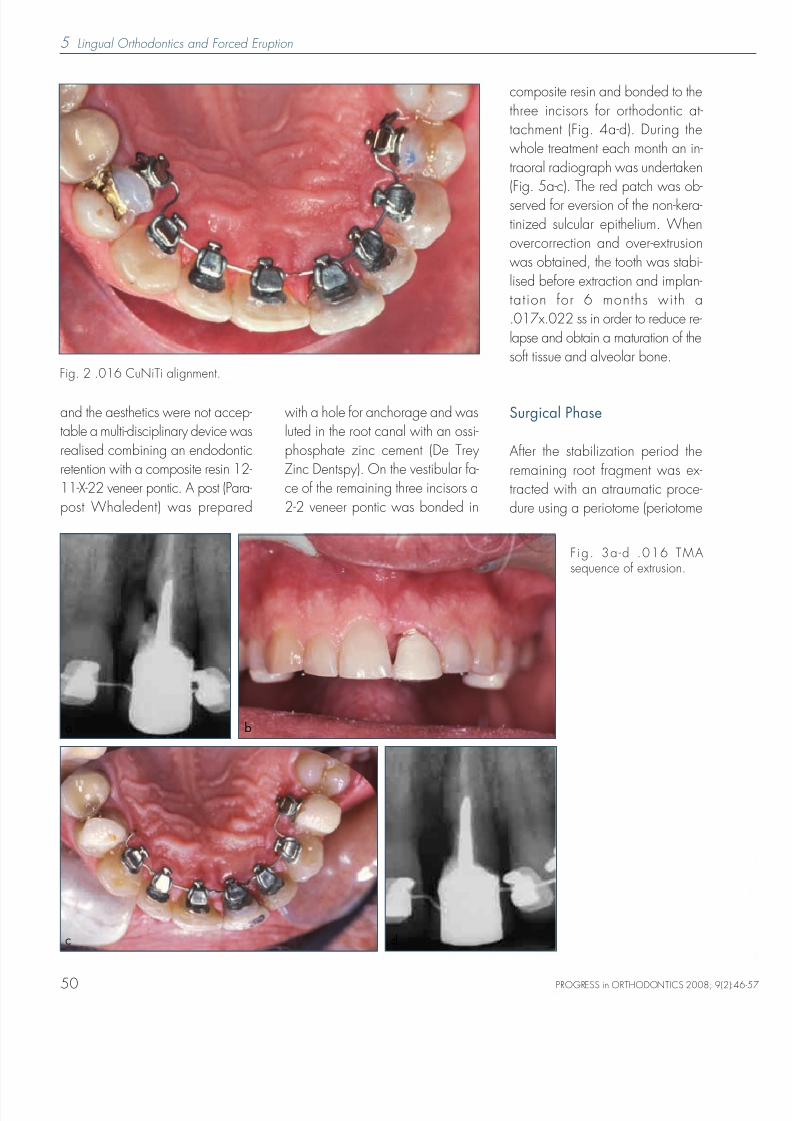
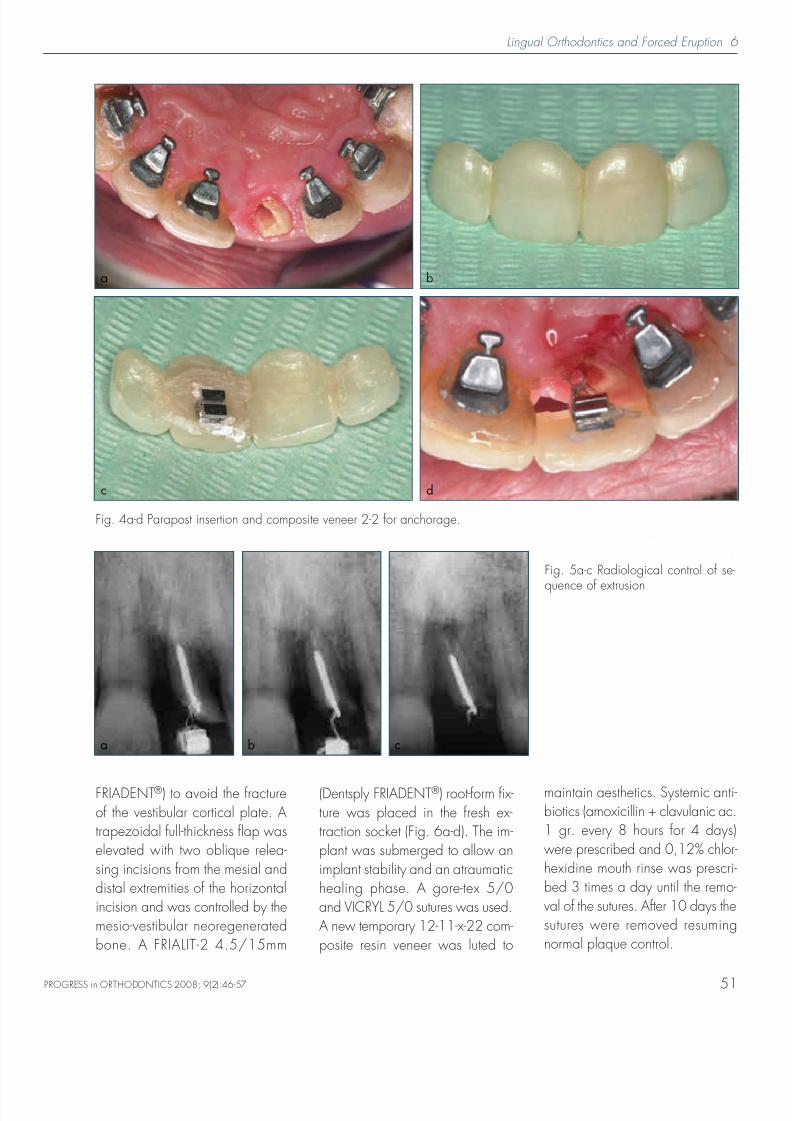
and the aesthetics were not accep-table a multi-disciplinary device wasrealised combining an endodonticretention with a composite resin 12-11-X-22 veneer pontic. A post (Para-post Whaledent) was prepared
with a hole for anchorage and wasluted in the root canal with an ossi-phosphate zinc cement (De TreyZinc Dentspy). On the vestibular fa-ce of the remaining three incisors a2-2 veneer pontic was bonded in
composite resin and bonded to thethree incisors for orthodontic at-tachment (Fig. 4a-d). During thewhole treatment each month an in-traoral radiograph was undertaken(Fig. 5a-c). The red patch was ob-served for eversion of the non-kera-tinized sulcular epithelium. Whenovercorrection and over-extrusionwas obtained, the tooth was stabi-lised before extraction and implan-tation for 6 months with a.017x.022 ss in order to reduce re-lapse and obtain a maturation of thesoft tissue and alveolar bone.
Surgical Phase
After the stabilization period theremaining root fragment was ex-tracted with an atraumatic proce-dure using a periotome (periotome
5 Lingual Orthodontics and Forced Eruption
Fig. 2 .016 CuNiTi alignment.
F ig. 3a-d .016 TMAsequence of extrusion.
ba
c d
PROGRESS in ORTHODONTICS 2008; 9(2):46-5
8/8/2019 Lingual Incisor
http://slidepdf.com/reader/full/lingual-incisor 6/12
51
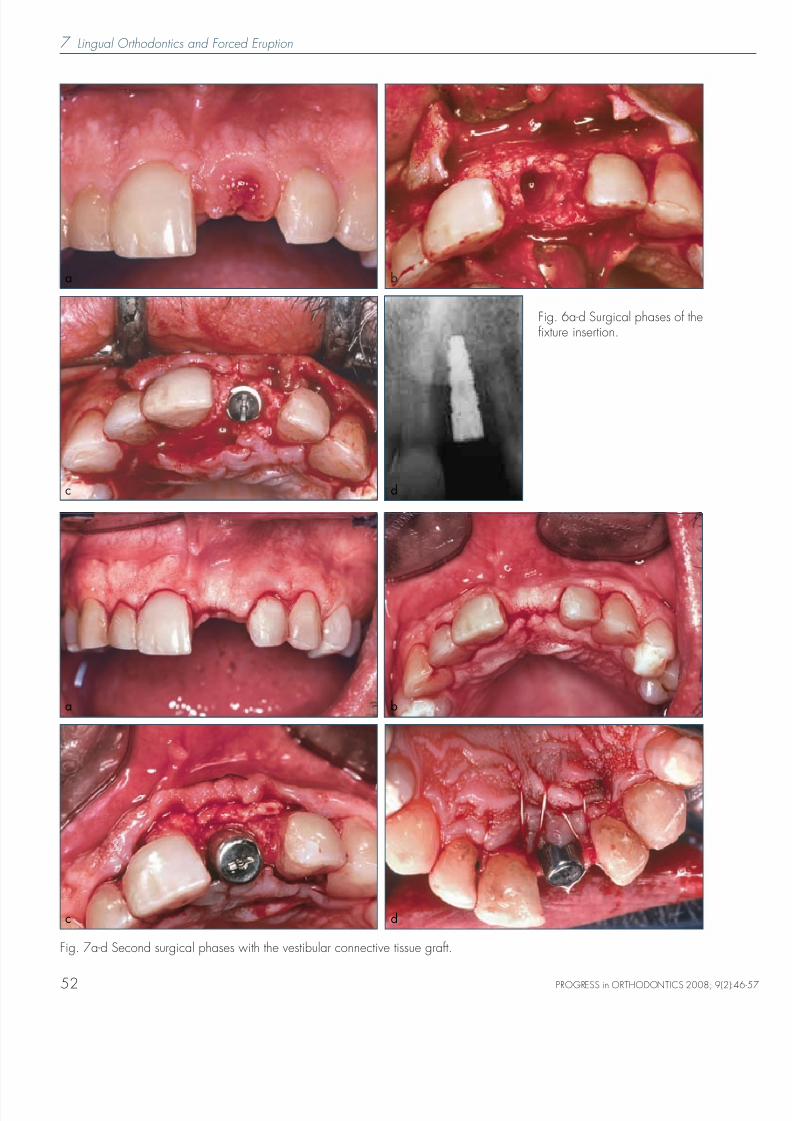
FRIADENT®) to avoid the fractureof the vestibular cortical plate. Atrapezoidal full-thickness flap waselevated with two oblique relea-sing incisions from the mesial anddistal extremities of the horizontalincision and was controlled by themesio-vestibular neoregeneratedbone. A FRIALIT-2 4.5/15mm
(Dentsply FRIADENT®) root-form fix-ture was placed in the fresh ex-traction socket (Fig. 6a-d). The im-plant was submerged to allow animplant stability and an atraumatichealing phase. A gore-tex 5/0and VICRYL 5/0 sutures was used.A new temporary 12-11-x-22 com-posite resin veneer was luted to
maintain aesthetics. Systemic anti-biotics (amoxicillin + clavulanic ac.1 gr. every 8 hours for 4 days)were prescribed and 0,12% chlor-hexidine mouth rinse was prescri-bed 3 times a day until the remo-val of the sutures. After 10 days thesutures were removed resumingnormal plaque control.
Lingual Orthodontics and Forced Eruption 6
Fig. 4a-d Parapost insertion and composite veneer 2-2 for anchorage.
ba
c d
Fig. 5a-c Radiological control of se-
quence of extrusion.
a b c
PROGRESS in ORTHODONTICS 2008; 9(2):46-57
8/8/2019 Lingual Incisor
http://slidepdf.com/reader/full/lingual-incisor 7/12
7 Lingual Orthodontics and Forced Eruption
52
Fig. 6a-d Surgical phases of thefixture insertion.
ba
c d
Fig. 7a-d Second surgical phases with the vestibular connective tissue graft.
ba
c d
PROGRESS in ORTHODONTICS 2008; 9(2):46-5
8/8/2019 Lingual Incisor
http://slidepdf.com/reader/full/lingual-incisor 8/12
After 6 months the second surgical
phase was attempted. The implantwas activated with a healing abut-ment of 5mm of height. At the sametime a vestibular connective tissuegraft was completed to increase thewidth of the vestibular tissue in orderto be used during the prosthetic pha-se25,26. An intrasulcular full-thicknessflap was elevated (a crestal incisionwas made in the implant zone) dra-wing the morphology of the future pa-
pillae near the edentolous area. Thecrestal part of the keratinized gingi-va was displaced vestibularly by theconnective graft. The incision wasextended horizontally to dissect thebuccal aspect of the adjacent pa-pillae, both mesially and distally. Do-nor connective tissue was harvestedreducing the palatal flap from the
same surgical site and secured in po-
sition suturing the graft within the ve-stibular flap, using it like an envelope,with interrupted bioabsorbable sutures(VICRYL 5/0). A ramp mattress sutu-re27 was used to maintain coronallypositioning of the vestibular flap andapically positioned the palatal flap(Fig. 7a-d). A mesio-distal and apicaldissection was performed to releaseresidual muscle tension and facilitatethe displacement of the flap for sutu-
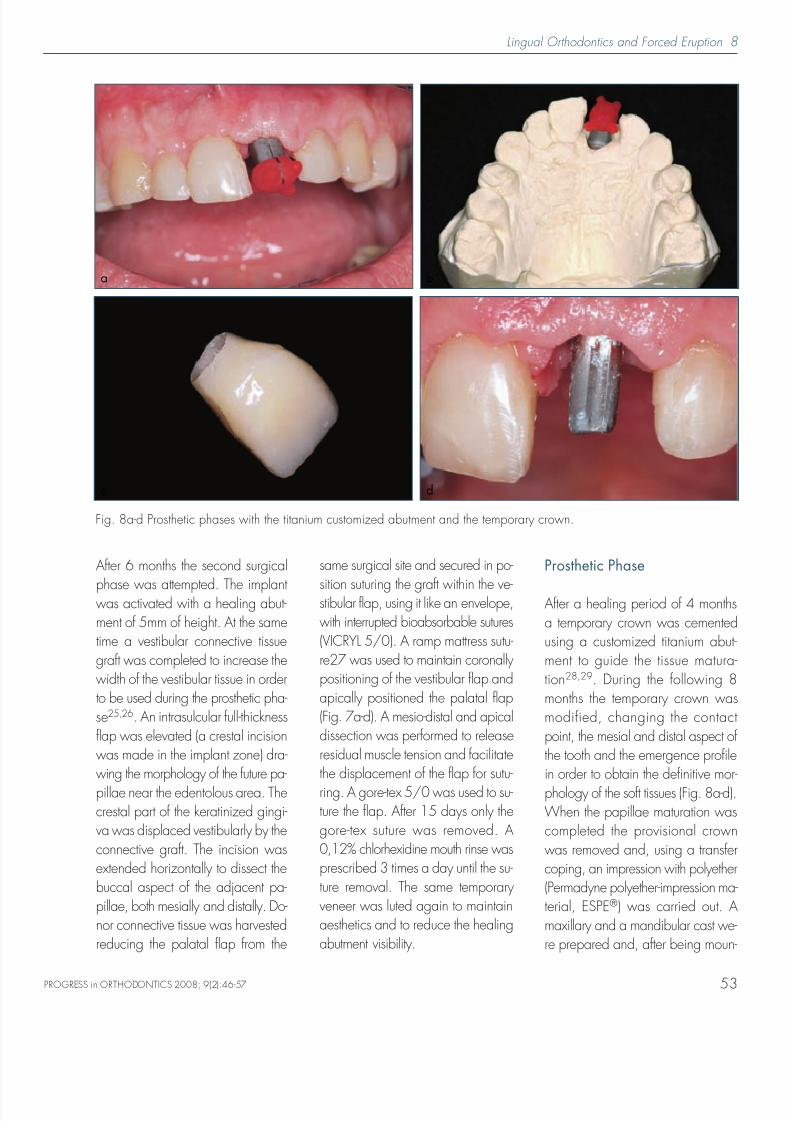
ring. A gore-tex 5/0 was used to su-ture the flap. After 15 days only thegore-tex suture was removed. A0,12% chlorhexidine mouth rinse wasprescribed 3 times a day until the su-ture removal. The same temporaryveneer was luted again to maintainaesthetics and to reduce the healingabutment visibility.
Prosthetic Phase
After a healing period of 4 monthsa temporary crown was cementedusing a customized titanium abut-ment to guide the tissue matura-tion28,29. During the following 8months the temporary crown wasmodified, changing the contactpoint, the mesial and distal aspect ofthe tooth and the emergence profilein order to obtain the definitive mor-
phology of the soft tissues (Fig. 8a-d).When the papillae maturation wascompleted the provisional crownwas removed and, using a transfercoping, an impression with polyether(Permadyne polyether-impression ma-terial, ESPE®) was carried out. Amaxillary and a mandibular cast we-re prepared and, after being moun-
Lingual Orthodontics and Forced Eruption 8
53
Fig. 8a-d Prosthetic phases with the titanium customized abutment and the temporary crown.
ba
c d
PROGRESS in ORTHODONTICS 2008; 9(2):46-57
8/8/2019 Lingual Incisor
http://slidepdf.com/reader/full/lingual-incisor 9/12
9 Lingual Orthodontics and Forced Eruption
54
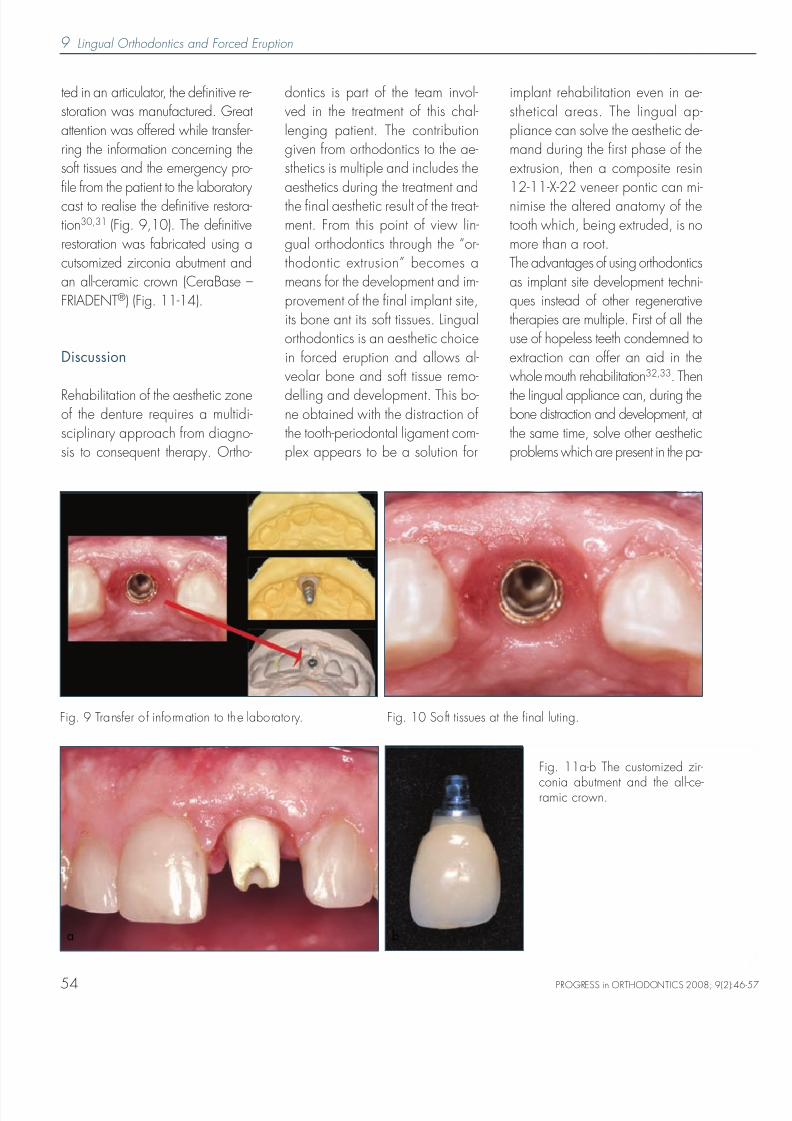
ted in an articulator, the definitive re-storation was manufactured. Greatattention was offered while transfer-ring the information concerning thesoft tissues and the emergency pro-file from the patient to the laboratorycast to realise the definitive restora-tion30,31 (Fig. 9,10). The definitiverestoration was fabricated using acutsomized zirconia abutment andan all-ceramic crown (CeraBase –FRIADENT®) (Fig. 11-14).
Discussion
Rehabilitation of the aesthetic zoneof the denture requires a multidi-sciplinary approach from diagno-sis to consequent therapy. Ortho-
dontics is part of the team invol-ved in the treatment of this chal-lenging patient. The contributiongiven from orthodontics to the ae-sthetics is multiple and includes theaesthetics during the treatment andthe final aesthetic result of the treat-ment. From this point of view lin-gual orthodontics through the “or-thodontic extrusion” becomes ameans for the development and im-provement of the final implant site,its bone ant its soft tissues. Lingualorthodontics is an aesthetic choicein forced eruption and allows al-veolar bone and soft tissue remo-
delling and development. This bo-ne obtained with the distraction ofthe tooth-periodontal ligament com-plex appears to be a solution for
implant rehabilitation even in ae-sthetical areas. The lingual ap-pliance can solve the aesthetic de-mand during the first phase of theextrusion, then a composite resin12-11-X-22 veneer pontic can mi-nimise the altered anatomy of thetooth which, being extruded, is nomore than a root.The advantages of using orthodonticsas implant site development techni-ques instead of other regenerativetherapies are multiple. First of all theuse of hopeless teeth condemned toextraction can offer an aid in thewhole mouth rehabilitation32,33. Then
the lingual appliance can, during thebone distraction and development, atthe same time, solve other aestheticproblems which are present in the pa-
Fig. 9 Transfer of information to the laboratory. Fig. 10 Soft tissues at the final luting.
Fig. 11a-b The customized zir-
conia abutment and the all-ce-ramic crown.
a b
PROGRESS in ORTHODONTICS 2008; 9(2):46-5
8/8/2019 Lingual Incisor
http://slidepdf.com/reader/full/lingual-incisor 10/12
Lingual Orthodontics and Forced Eruption 10
55
tient’s mouth. The lingual appliance al-so allows the use of the vestibularveneer to avoid the aesthetic pro-
blems of the missing teeth.Then it is possible to eliminate or re-duce eventually more complex re-generative techniques (such asGBR, ERE, osseous graft). Last butnot least, the orthodontically indu-ced implant site development ma-kes the subsequent surgical techni-cal phases easier such as fixture in-
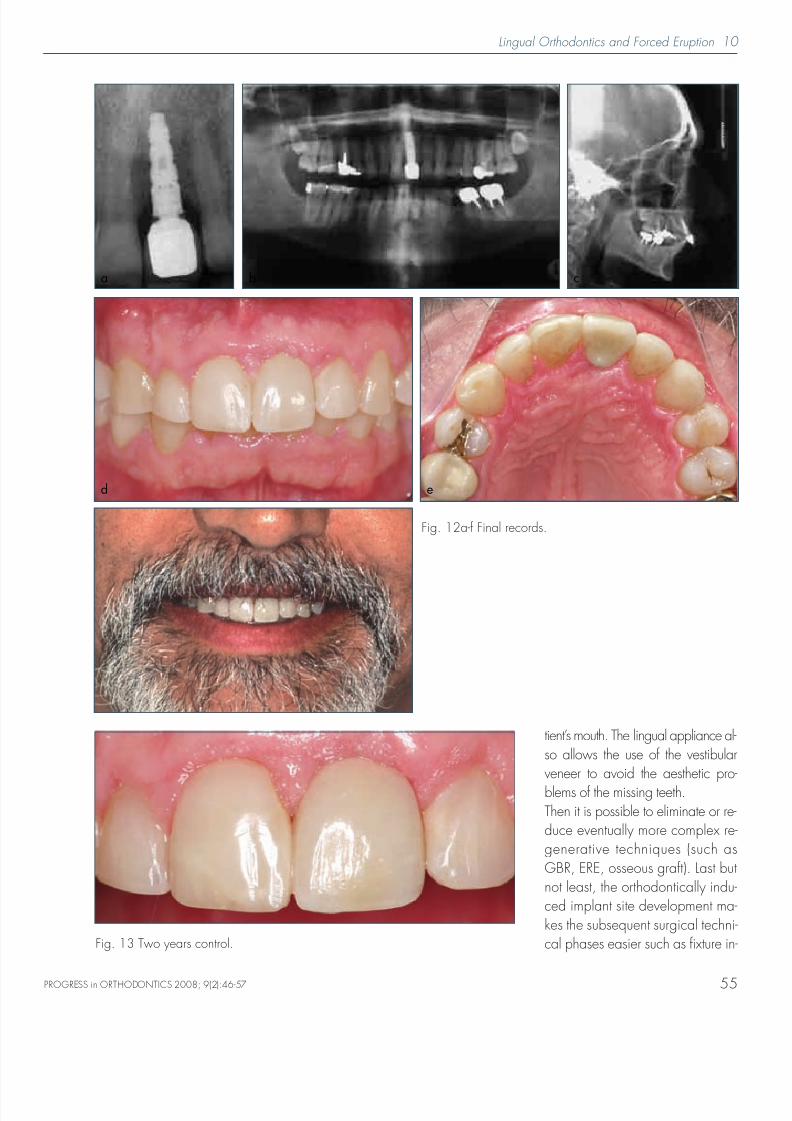
Fig. 12a-f Final records.
b ca
d e
Fig. 13 Two years control.
PROGRESS in ORTHODONTICS 2008; 9(2):46-57
8/8/2019 Lingual Incisor
http://slidepdf.com/reader/full/lingual-incisor 11/12
11 Lingual Orthodontics and Forced Eruption
56
sertion and mucogingival correc-tions, as seen in Fig. 15, due tothe increase of the soft tissues.Nevertheless the disadvantages
must be considered: the long timeof treatment, present with the non-resorbable membranes, the pooraesthetic aspect during orthodon-
tics, solved with the lingual ap-proach and the composite resinveneer pontic, and the difficult ac-ceptation and management of or-thodontics by the patient.There could have been many al-ternatives to the orthodontics-im-plant treatment. First of all the fixedpartial denture was not realizableas the proximal teeth were perio-dontal ly and endodont ical lyhealthy. The immediate post-ex-traction implant was not a possiblechoice due to the mesio-vestibularremaining defect that involved asoft tissues collapse and a difficult
guided bone regeneration.
Conclusion
Forced eruption is a well docu-mented technique to enhance theimplant site and to increase theamount of hard and soft tissues.The association of lingual ortho-
dontics and of a composite resin12-11-X-22 veneer pontic allowedthe realisation of the forced extru-sion of a lost left central incisor ina 57 years old male. The combi-nation of these two techniqueskept, during the whole treatment,acceptable aesthetics allowing cor-rect implant site development.
References
1. Ingber JS. Forced eruption. Part I. Amethod for treating nonrestorableteeth. J Periodontol 1976; 45:199-206.
2. Ingber JS. Forced eruption. Part II. Amethod for treating nonrestorableteeth. Periodontal and restorativeconsiderations. J Periodontol 1976;47(4):203-16.
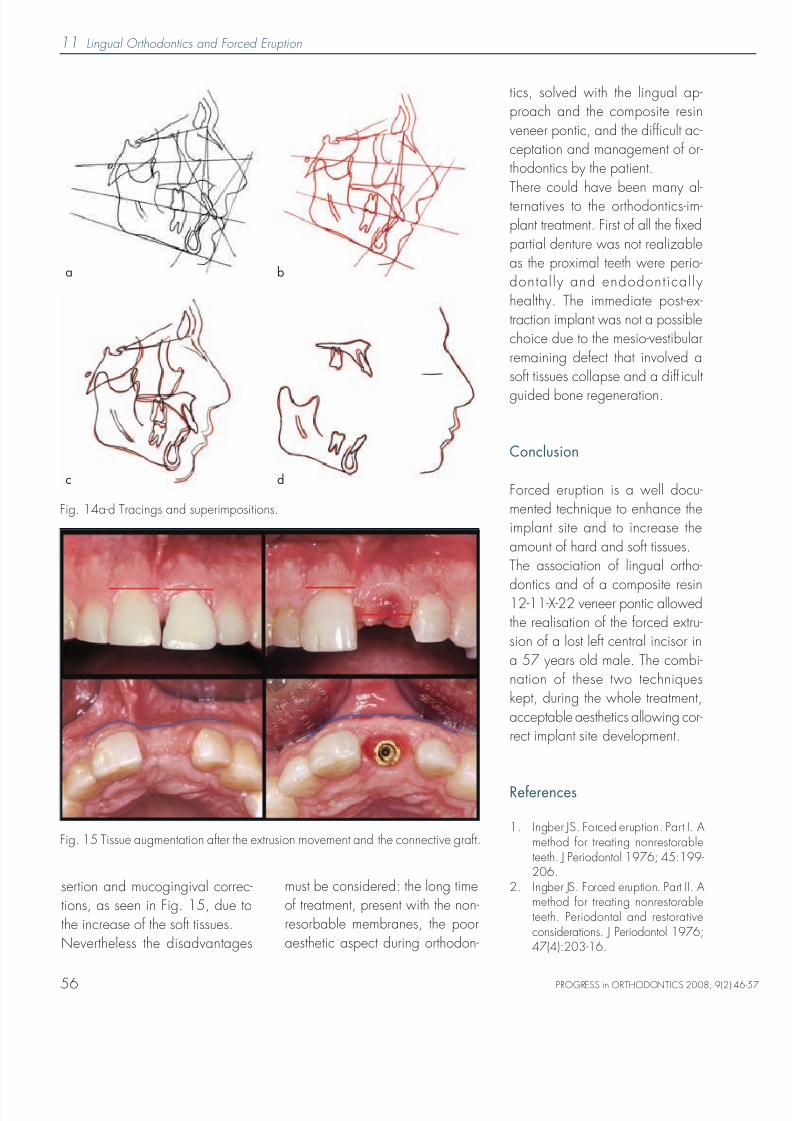
Fig. 14a-d Tracings and superimpositions.
a b
c d
Fig. 15 Tissue augmentation after the extrusion movement and the connective graft.
PROGRESS in ORTHODONTICS 2008; 9(2):46-5
8/8/2019 Lingual Incisor
http://slidepdf.com/reader/full/lingual-incisor 12/12
Lingual Orthodontics and Forced Eruption 12
57
3. Delivanis P, Delivanis H, KuftinecMM. Endodontic-orthodontic ma-nagement of fractured anterior teeth. J Am Dent Assoc 1978; 97:483-5.
4. Simon JH, Kelly WH, Gordon DG,Ericksen GW. Extrusion of endo-dontically treated teeth. J Am Dent
Assoc 1978; 97:17-23.5. Stern N, Becker A. Forced eruption:
biological and clinical considerations. J Oral Rehabil 1980; 7:395-402.
6. Shiloah J. Clinical crown lengthe-ning by vertical root movement. JProsthet Dent 1981; 45:602-5.
7. Cronin RJ, Wardle WL. Prosthodonticmanagement of vertical root extrusion. J Prosthet Dent 1981;46:498-504.
8. Mantzikos T, Shamus I. Forced erup-tion and implant site development:An ostheophysiologic response. Am
J Orthod Dentofacial Orthop1999;115:583-91.9. Ostojic S, Sieber R, Borer K, Lam-
brecht JT. Controlled orthodontic ex-trusion with subsequent implanta-tion. Schweiz Monatsschr Zahnmed2005;115:222-31.
10. Ogihara S, Marks MH. Enhancingthe regenerative potential of guidedtissue regeneration to treat an intra-bony defect and adjacent ridge de-formity by orthodontic extrusive force. J Periodontol 2006;77:2093-100.
11. Salama H, Salama M. The role of or-thodontic extrusive remodeling in the en-hancement of soft and hard tissue pro-files prior to implant placement: a syste-matic approach to the management ofextraction site defects. Int J PeriodonticsRestorative Dent 1993;13:312-33.
12. Yeo AB, Cheok CB. Managementstrategies of the unsalvageabletooth. Dent Update 2006;33:7-12.
13. Schwartz-Arad D, Levin L, AshkenaziM. Treatment options of untreatabletraumatized anterior maxillary teeth
for future use of dental implantation.Implant Dent 2004;13:120-8.14. Levin I, Ashkenazi M, Schwartz-Arad
D. Preservation of alveolar bone ofun-restorable traumatized maxillaryincisors for future. Refuat Hapeh Ve-
hashinayim 2004;21:54-9, 101-2.15. Chambrone L, Chambrone LA. For-
ced orthodontic eruption of fracturedteeth before implant placement: ca-se report. J Can Dent Assoc2005;71:257-61.
16. Erkut S, Arman A, Gulsahi A, Uckan
S, Gulsahi K. Forced eruption andimplant treatment in posterior maxil-la: a clinical report. J Prosthet Dent2007;97:70-4.
17. Hinds KF. Alveolar ridge develop-ment with forced eruption and dis-traction of retained natural dentition.Oral Maxillof Surg Clin N Am2004;16:75-89.
18. Bach N, Baylard JF, Voyer R. Or-thodontic extrusion: periodontal con-siderations and applications. J CanDent Assoc 2004;70:775-80.
19. Buskin R, Castellon P, Hochstedler JL.Orthodontic extrusion and ortho-dontic extraction in preprosthetictreatment using implant therapy.Pract Periodontics Aesthet Dent2000;12:213-9; quiz 220.
20. Danesh-Meyer MJ, Brice DM. Im-plant site development using ortho-dontic extrusion: a case report. N ZDent J 2000;96:18-22.
21. Chaushu S, Zahavi T, Becker A. For-ced eruption of maxillary incisorteeth from the lingual side. Quintes-
sence Int 2004;35:431-6.22. Geron S, Ziskind D. Lingual forcederuption orthodontic technique: cli-nical considerations for patient se-lection and clinical report. J ProsthetDent 2002;87:125-8.
23. Uddin M, Mosheshvili N, Segelnick SL.A new appliance for forced eruption.N Y State Dent J 2006;72:46-50.
24. Nozawa T, Sugiyama T, YamaguchiS, Ramos T, Komatsu S, EnomotoH, Ito K. Buccal and coronal boneaugmentation using forced eruption
and buccal root torque: a case re-port. Int J Periodontics Restorative
Dent 2003;23:585-91.25. Price RB, Price DE. Esthetic restora-
tion of a single-tooth dental implantusing a subepithelial connective tis-sue graft: a case report with 3-yearfollow-up. Int J Periodontics Restora-tive Dent 1999;19:92-101.
26. Evian CI, al-Maseeh J, SymeonidesE. Soft tissue augmentation for im-plant dentistry. Compend ContinEduc Dent 2003;24:195-8, 200-2, 204-6; quiz 208.
27. Tinti C, Benfenati SP. The ramp mat-tress suture: a new suturing techni-que combined with a surgical pro-cedure to obtain papillae betweenimplants in the buccal area. Int J Pe-riodontics Restorative Dent2000;22:63-9.
28. Chee WW, Donovan T. Use of pro-
visional restorations to enhance soft-tissue contours for implant restora-tions. Compend Contin Educ Dent1998;19:481-6, 488-9; quiz 490.
29. Bichacho N, Landsberg CJ. Singleimplant restorations: prostheticallyinduced soft tissue topography. PractPeriodontics Aesthet Dent1997;9:745-52; quiz 754.
30. Stumpel LJ, Haechler W, BedrossianE. Customized abutments to shapeand transfer peri-implant soft-tissuecontours. J Cal i f Dent Assoc
2000;28:301-9.31. Touati B, Guez G, Saadoun A. Ae-sthetic soft tissue integration and op-timized emergence profile: provi-sionalization and customized im-pression coping. Pract PeriodonticsAesthet Dent 1999;11:305-14;quiz 316.
32. Mantzikos T, Shamus I. Case re-port: forced eruption and implantsite development. Angle Orthod1998;68:179-86
33. Mantzikos T, Shamus I. Forced eruption
and implant site development: soft tis-sue response. Am J Orthod DentofacialOrthop 1997;112:596-606.
PROGRESS in ORTHODONTICS 2008; 9(2):46-57
Related Documents