Lethal photosensitization and guided bone regeneration in treatment of peri-implantitis: an experimental study in dogs Jamil Awad Shibli Marilia Compagnoni Martins Fernando Salimon Ribeiro Valdir Gouveia Garcia Francisco Humberto Nociti Jr Elcio Marcantonio Jr Authors’ affiliations: Jamil Awad Shibli, Department of Periodontology, Dental Research Division, Guarulhos University, Guarulhos, SP, Brazil Marilia Compagnoni Martins, Fernando Salimon Ribeiro, Elcio Marcantonio Jr, Department of Periodontology, Dental School of Araraquara, State University of Sao Paulo (UNESP), Araraquara, SP, Brazil Valdir Gouveia Garcia, Dental School of Marı ´lia, University of Marı ´lia (UNIMAR), Marı ´lia, SP, Brazil; Dental School of Arac ¸atuba, State University of Sao Paulo (UNESP), Arac ¸atuba, SP, Brazil Francisco Humberto Nociti Jr, Department of Periodontology, Dental School of Piracicaba, University of Campinas, (UNICAMP) SP, Brazil Correspondence to: Elico Marcantonio Jr Departmento de Periodontia Faculdade de Odontologia de Araraquara-UNESP R. Humaita ´, 1680 14801-903 Araraquara, SP Brazil Tel.: þ 55 16 3301 6369 Fax: þ 55 16 3301 6314 e-mail: [email protected] Key words: guided bone regeneration, histology, peri-implantitis, photodynamic therapy/ photosensitizers, re-osseointegration Abstract: The purpose of this study was to evaluate the effect of lethal photosensitization and guided bone regeneration (GBR) on the treatment of ligature-induced peri-implantitis in different implant surfaces. The treatment outcome was evaluated by clinical and histometric methods. A total of 40 dental implants with four different surface coatings (10 commercially pure titanium surface (cpTi); 10 titanium plasma-sprayed (TPS); 10 acid-etched surface; 10 surface-oxide sandblasted) were inserted into five mongrel dogs. After 3 months, the animals with ligature-induced peri-implantitis were subjected to surgical treatment using a split-mouth design. The controls were treated by debridment and GBR, while the test side received an additional therapy with photosensitization, using a GaAlAs diode laser, with a wavelength of 830 nm and a power output of 50 mW for 80 s (4 J/cm 2 ), and sensitized toluidine blue O (100 mg/ml). The animals were sacrificed 5 months after therapy. The control sites presented an earlier exposition of the membranes on all coating surfaces, while the test group presented a higher bone height gain. Re-osseointegration ranged between 41.9% for the cpTi surface and 31.19% for the TPS surface in the test sites; however differences were not achieved between the surfaces. The lethal photosensitization associated with GBR allowed for better re-osseointegration at the area adjacent to the peri- implant defect regardless of the implant surface. Animal studies have shown that bacterial biofilm accumulation around dental im- plants promoted by ligature placement may develop peri-implant tissue breakdown, also known, as peri-implantitis (Lang et al. 1993; Schou et al. 1993; Ericsson et al. 1996). Plaque-induced peri-implantitis has been indicated as one of the etiological factors associated with long-term failure of dental implants (Quirynen et al. 2002). Different implant surfaces have been proposed in order to improve clinical and histological outcome of dental implants and, therefore, the interaction between different implant surfaces and peri-implan- titis therapy may be of interest. Recent studies (Persson et al. 2001b; Kolonidis et al. 2003; Schou et al. 2003a; Shibli et al. 2003b, 2003c) have investi- gated the importance of implant surface cleanliness after peri-implantitis treat- ment. It has been hypothesized that surface contaminants, released from contaminated implant surfaces, enhance and perpetuate the inflammatory response, thus altering the healing process, and possibly leading to the dissolution of titanium (Baier et al. 1984, 1988; Olefjord & Hansson 1993; Esposito et al. 1999; Shibli et al. 2004). In addition, the alterations of the titanium oxide layer may not allow re-osseointegra- tion. In earlier studies, Shibli et al. (2003b, Copyright r Blackwell Munksgaard 2006 Date: Accepted 15 January 2005 To cite this article: Shibli JA, Martins MC, Ribeiro FS, Garcia VG, Nociti Jr FH, Marcantonio Jr E. Lethal photosensitization and guided bone regeneration in treatment of peri- implantitis: an experimental study in dogs. Clin. Oral Impl. Res. 17, 2006; 273–281 doi: 10.1111/j.1600-0501.2005.01167.x 273

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Lethal photosensitization and guidedbone regeneration in treatment ofperi-implantitis: an experimentalstudy in dogs
Jamil Awad ShibliMarilia Compagnoni MartinsFernando Salimon RibeiroValdir Gouveia GarciaFrancisco Humberto Nociti JrElcio Marcantonio Jr
Authors’ affiliations:Jamil Awad Shibli, Department of Periodontology,Dental Research Division, Guarulhos University,Guarulhos, SP, BrazilMarilia Compagnoni Martins, Fernando SalimonRibeiro, Elcio Marcantonio Jr, Department ofPeriodontology, Dental School of Araraquara, StateUniversity of Sao Paulo (UNESP), Araraquara, SP,BrazilValdir Gouveia Garcia, Dental School of Marılia,University of Marılia (UNIMAR), Marılia, SP,Brazil; Dental School of Aracatuba, State Universityof Sao Paulo (UNESP), Aracatuba, SP, BrazilFrancisco Humberto Nociti Jr, Department ofPeriodontology, Dental School of Piracicaba,University of Campinas, (UNICAMP) SP, Brazil
Correspondence to:Elico Marcantonio JrDepartmento de PeriodontiaFaculdade de Odontologia de Araraquara-UNESPR. Humaita, 168014801-903 Araraquara, SPBrazilTel.:þ 55 16 3301 6369Fax: þ55 16 3301 6314e-mail: [email protected]
Key words: guided bone regeneration, histology, peri-implantitis, photodynamic therapy/
photosensitizers, re-osseointegration
Abstract: The purpose of this study was to evaluate the effect of lethal photosensitization
and guided bone regeneration (GBR) on the treatment of ligature-induced peri-implantitis
in different implant surfaces. The treatment outcome was evaluated by clinical and
histometric methods. A total of 40 dental implants with four different surface coatings (10
commercially pure titanium surface (cpTi); 10 titanium plasma-sprayed (TPS); 10 acid-etched
surface; 10 surface-oxide sandblasted) were inserted into five mongrel dogs. After 3
months, the animals with ligature-induced peri-implantitis were subjected to surgical
treatment using a split-mouth design. The controls were treated by debridment and GBR,
while the test side received an additional therapy with photosensitization, using a GaAlAs
diode laser, with a wavelength of 830 nm and a power output of 50 mW for 80 s (4 J/cm2),
and sensitized toluidine blue O (100 mg/ml). The animals were sacrificed 5 months after
therapy. The control sites presented an earlier exposition of the membranes on all coating
surfaces, while the test group presented a higher bone height gain. Re-osseointegration
ranged between 41.9% for the cpTi surface and 31.19% for the TPS surface in the test sites;
however differences were not achieved between the surfaces. The lethal photosensitization
associated with GBR allowed for better re-osseointegration at the area adjacent to the peri-
implant defect regardless of the implant surface.
Animal studies have shown that bacterial
biofilm accumulation around dental im-
plants promoted by ligature placement
may develop peri-implant tissue breakdown,
also known, as peri-implantitis (Lang et al.
1993; Schou et al. 1993; Ericsson et al.
1996). Plaque-induced peri-implantitis has
been indicated as one of the etiological
factors associated with long-term failure of
dental implants (Quirynen et al. 2002).
Different implant surfaces have been
proposed in order to improve clinical and
histological outcome of dental implants
and, therefore, the interaction between
different implant surfaces and peri-implan-
titis therapy may be of interest.
Recent studies (Persson et al. 2001b;
Kolonidis et al. 2003; Schou et al. 2003a;
Shibli et al. 2003b, 2003c) have investi-
gated the importance of implant surface
cleanliness after peri-implantitis treat-
ment. It has been hypothesized that surface
contaminants, released from contaminated
implant surfaces, enhance and perpetuate
the inflammatory response, thus altering
the healing process, and possibly leading to
the dissolution of titanium (Baier et al.
1984, 1988; Olefjord & Hansson 1993;
Esposito et al. 1999; Shibli et al. 2004). In
addition, the alterations of the titanium
oxide layer may not allow re-osseointegra-
tion. In earlier studies, Shibli et al. (2003b,Copyright r Blackwell Munksgaard 2006
Date:Accepted 15 January 2005
To cite this article:Shibli JA, Martins MC, Ribeiro FS, Garcia VG, Nociti JrFH, Marcantonio Jr E. Lethal photosensitization andguided bone regeneration in treatment of peri-implantitis: an experimental study in dogs.Clin. Oral Impl. Res. 17, 2006; 273–281doi: 10.1111/j.1600-0501.2005.01167.x
273
2003c) demonstrated the potential use
of photodynamic therapy associated with
guided bone regeneration (GBR) in the
treatment of experimental peri-implant le-
sions. The average re-osseointegration ob-
tained in this study was 25.15%, similar to
previous studies that have used mechanical
treatment associated with systemic antibio-
tics (Persson et al. 1999; Wetzel et al. 1999;
Nociti et al. 2001a; Schou et al. 2003a,
2003c). Photodynamic therapy uses a low-
power laser, following the application of a
photosensitizing substance, such as tolui-
dine blue O (TBO). The mechanism by
which TBO kills microorganisms, such as
Porphyromonas gingivalis, Prevotella inter-
media, Actinobacillus actinomycetemco-
mitans, and Fusobacterium nucleatum, is
currently under research. However, it is
believed that lethal photosensitization of
these microorganisms may involve changes
in their membranes, on the plasma mem-
brane proteins, and DNA damage mediated
by singlet oxygen (Dobson et al. 1992;
Sarkar & Wilson 1993; Henry et al. 1995;
Bhatti et al. 1997, 1998; Wainwright 1998;
Bhatti et al. 2000).
The objective of this study was to eval-
uate the efficacy of lethal photosensitiza-
tion associated with GBR, for the
treatment of ligature-induced peri-implan-
titis in dogs, using different dental implant-
coated surfaces.
Material and methods
Animals and anesthesia
The outline of the experiment is presented
in Fig. 1. Briefly, five healthy male mon-
grel dogs, with an average age of 2 years and
an average weight of 18 kg, were used in
the study. Animal selection, management,
and surgical protocol followed routines
approved for this study by the local In-
stitutional Animal Care and Ethics
Committee.
All surgical and clinical procedures, as
well as laser irradiation, were performed
under general anesthesia accomplished
with 0.05 mg/kg of subcutaneous prea-
nesthesia sedation (Atropine sulfate –
0.5 mg, Ariston Inds. Quımica e Farms.
LTDA, Sao Paulo, Brazil), intravenous in-
jection of chlorpromazine (Amplictil
25 mg, Rhodia Farma LTDA, Sao Paulo,
Brazil), and thiopental (Tiopental – AB-
BOTT Laboratorios do Brasil Ltda, Sao
Paulo, Brazil).
Tooth extraction
An edentulous ridge was created by the
extraction of all mandibular premolars and
first molars. The alveoli were allowed to
heal for a period of 3 months. The upper
premolars were also extracted to prevent
occlusion trauma interference during pla-
que-induced peri-implantitis. During the
healing period, bacterial biofilm control
was performed by scrubbing with 0.12%
chlorhexidine daily, in addition to scaling
and root planning once a month, until
cotton ligatures were placed.
Implant design, surface, and surgery
Forty dental implants of four different
surfaces were used: 10 commercially pure
titanium implants (cpTi; Sterngold, Im-
plamed, Attleboro, MA, USA); 10 titanium
plasma-sprayed (TPS; Sterngold, Im-
plamed); 10 hybrid surfaces – machined
titanium in the three first screws and acid
etched in other screws – acid (Osseotites
-
3is
Implants Innovations, Palm Beach
Gardens, FL, USA), and 10 sandblasted
with titaniun oxide – oxide (Porous, Con-
exao Implants, Sao Paulo, SP, Brazil).
All implants were 10 mm in length and
3.75 mm in diameter.
The implants were randomly distributed
among the dogs, so that each dental im-
plant surface could be represented on
each mandibular side. Dental implants
were placed after full thickness flap surgery
under aseptic conditions. The recipient
sites were prepared according to the surgi-
cal techniques indicated by each implant
manufacturer. The flaps were sutured with
single interrupted sutures, submerging all
implants. Potassic and sodic benzilpenici-
lin (Fort Dodge Saude Animal LTDA,
Campinas, SP, Brazil) was given once a
week for 2 weeks, in order to prevent post-
surgical infection, pain was controlled
with paracetamol (ABBOTT Laboratorios
do Brasil Ltda), and the sutures were re-
moved after 10 days.
Experimental peri-implantitis
Three months after dental implant installa-
tion, healing abutments were installed,
according to the instructions of each dental
implant system. After 2 months of a pla-
que control program and the healing of the
soft tissue, cotton floss ligatures were
placed around the dental implants, as pre-
viously described (Shibli et al. 2003a). At
90 days, when approximately 40% of the
initial bone support was lost, the ligatures
were removed, and a 2-month plaque
control program was initiated by daily
scrubbing of the implants with 0.12%
chlorhexidine and scaling of the abutment
surface.
Randomization of the mandibular quad-
rants and a split-mouth design was estab-
lished as follows: control side – mechanical
debridment and GBR, and test side – me-
chanical debridment, lethal photosensitiza-
tion, and GBR to compare the effect of
lethal photosensitization (Table 1).
Clinical evaluation and treatment
A crestal incision was made through the
mucosa, and buccal and lingual full-thick-
ness flaps surgery was performed to remove
Extraction
Implant
Abutment
+Lig. –Lig.
Treatment
Biopsy
–8 –5 –2 0 3 5 9
0.12% chlorhexidine 0.12% chlorhexidine
Membrane removal
10 months
Fig. 1. Outline of the experiment. Animals n¼ 5, dental implants n¼ 40. Ligatures were placed at 0 month
(þLig.) and removed at 3 months (�Lig.).
Shibli et al . Lethal photosensitization in treatment of peri-implantitis
274 | Clin. Oral Impl. Res. 17, 2006 / 273–281

the abutments and the granulation tissue
present in bone craters around the dental
implants. A plastic scaller (Implacare–
IMPHDL6, Hu-friedy Mfg Co Inc., Chi-
cago, IL, USA) was used to prevent any
damage to exposed dental implant surface.
Pre- and post-treatment bone defects were
measured by a single trained examiner, i.e.,
the distance from the top of the cover screw
to the bottom of the peri-implant defect,
using a periodontal probe (PCPUNC 15
Hu-friedy Mfg Co Inc.), at four sites (me-
sial, buccal, distal, and lingual).
The implant surfaces of the test group
received 100mg/ml TBO (Sigma LTDA,
Poole, UK) injected into the peri-implant
defect, as far as the bony edge, on the
previously contaminated implant surface,
using a thin needle as previously described
(Shibli et al. 2003b, 2003c). TBO was
placed for 1 min, and then carefully re-
moved. The stained area was subsequently
irradiated with a GaAlAs diode laser
(Thera-Lase, DMC Equipamentos LTDA,
Sao Carlos, SP, Brazil) with a measured
power output of 50 mW, to emit radiation
in collimated beams (1 cm2) with a wave-
length of 830 nm, for 80 s, and a total
energy of 4 J (energy density of 4 J/cm2).
The diode laser was in contact with the
mesial, distal, buccal, and lingual surfaces
by a scanning method, for 20 s, on each
surface. Multiple perforations of the bone
surface were previously made to facilitate
the filling of the defect with the coagulum.
All the sites, including control sides,
received a PTFE membrane (TefGen-
PLUS, Lifecore Biomedical Inc., Chasca,
MN, USA), allowing implant penetration
through the site. The membrane was ad-
justed to extend circumferentially 3–5 mm
over the adjacent alveolar bone, avoiding
ingrowths of the soft connective tissue.
The membranes were stabilized at the
buccal and lingual sites not only by cpTi
tacks (INP Implantes Nacionais and Prot-
eses Comercio Ltda, Sao Paulo, SP, Brazil)
but also by cover screws. To allow flap
apposition and closure after placement,
incisions were made buccally and lingually
after membrane placement. Primary
wound closure was achieved with horizon-
tal mattress sutures alternated with
interrupted sutures. Anti-inflammatory
medication (2 mg betamethasone Celes-
tone, Schering-Plough S/A, Rio de Janeiro,
RJ, Brazil) was administered twice a day
and appropriate analgesia (paracetamol) for
3 days following surgery in order to reduce
postoperative swelling and pain. Antibio-
tics were administered neither before
nor after the surgical treatment of the
peri-implant defect. Two weeks after local
therapy, the sutures were removed and a
fluorochrome (Oxytetracycline 25 mg/kg
body weight; Pfizer do Brasil, Sao Paulo,
SP, Brazil) was injected intravenously (i.v.).
Four months after treatment, the PTFE
membranes were surgically removed in
both groups and the implants were allowed
to heal for 1 month. Four days before the
euthanasia, a second fluorochrome (18 mg/
kg red alizarine body weight; Sigma
Chemical Co., St Louis, MO, USA) was
injected i.v. for observation of the
remodelation of peri-implant bone tissue
at 5 months after treatment. Five months
after treatment, the animals were sacri-
ficed by induction of deep anesthesia fol-
lowed by intravenous sodium pentobarbital
euthanasia.
Histological procedures
The mandibles were removed and block
biopsies of each implant site were dissected
and fixed in 4% neutral formalin for 48 h.
The biopsies were then prepared for ground
sectioning according to the methods pre-
viously described by Donath & Breuner
(1982). The specimens were cut in a me-
sio-distal plane using a cutting–grinding
unit (Exacts
Cutting, System, Apparatebau
Gmbh, Hamburg, Germany). One central
section of each biopsy was prepared and
reduced to a final thickness of 50–70mm,
by micro-grinding and polishing using a
micro-grinding unit (Exacts
Cutting, Sys-
tem, Apparatebau Gmbh). Before staining,
each section was evaluated with respect to
the location of the fluorochrome marker
by microscopy (Leitz DM-RBE micro-
scopy, Leica, Bensheim, Germany)
equipped with an image system (Qwin,
Leica). In the unstained sections, fluores-
cence light and a filter cube compatible
with the fluorochrome were used to assess
the bone defect border, as well as the
remodeling of the new bone.
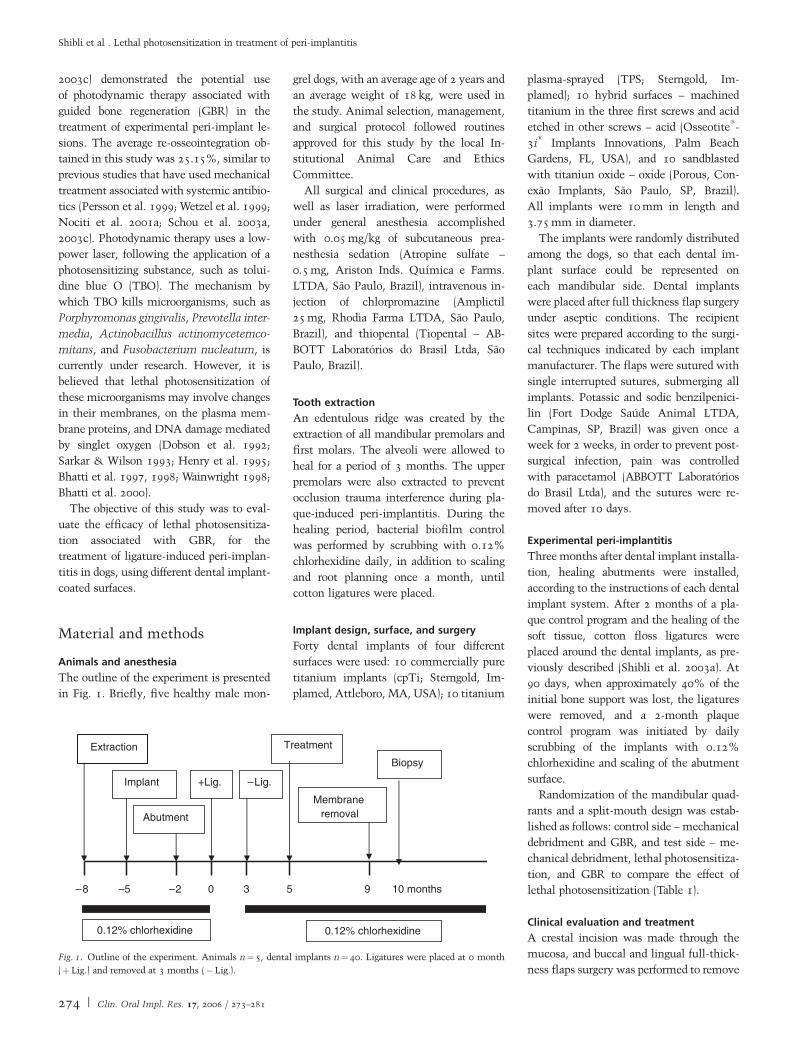
The sections were stained in toluidine
blue in order to assess the histometric para-
meters: (1) Distance from the original
bottom of the defect – identified by the
difference in coloration after staining and
by the fluorochrome (a) to the most coronal
point of the newly formed bone with in-
timate contact with the implant surface, (b)
(¼ re-osseointegation); (2) area of (a) to the
most apical border of the newly formed
bone, (c) to implant shoulder, (d) (¼bone fill); (3) percentage of osseointegration
(mineralized bone contact with the im-
plant surface); and (4) bone area within the
limits of the implant threads at the portion
of the implant, apical of the peri-implant
defect, where peri-implantitis did not
occur (Fig. 2).
Data analysis
Data were obtained in pixels and pixels2
and transformed into percentage to prevent
the possible influence of the different
macrostructure of the different implant
Table 1. Distribution of dental implants with different surfaces in five dogs
Animal Test side Control side
PM2 PM3 PM4 M PM2 PM3 PM4 M
1 cpTi TPS Oxide Acid Acid Oxide TPS cpTi2 TPS Oxide Acid cpTi Oxide TPS cpTi Acid3 Oxide cpTi TPS Acid TPS cpTi Acid Oxide4 cpTi Acid Oxide TPS Acid TPS Oxide cpTi5 Acid TPS CpTi Oxide cpTi Acid Oxide TPS
PM2, PM3, PM4, and M, mandibular premolars and molar; cpTi, commercially pure titanium; TPS, titanium plasma-sprayed; Oxide, surface sandblasted with
titanium oxide; Acid, acid-etched surface.
Shibli et al . Lethal photosensitization in treatment of peri-implantitis
275 | Clin. Oral Impl. Res. 17, 2006 / 273–281
systems evaluated in this study. The data
relative to defect depth, percentage of os-
seointegration, and bone area within the
limits of the threads were obtained from all
implants, independent of group.
Paired t-test and parametric analysis of
variance were performed to assess the dif-
ferences between test and control groups
and among the several implant surfaces,
respectively. The unit of analysis was the
animal (n¼5), and the level of significance
was 0.05.
Results
Clinical observations
One cpTi (test group) and one oxide surface
(control group) were lost during the experi-
mental peri-implantitis phase in two ani-
mals. All the other remaining implants
were included in the evaluation. The den-
tal implants of the test group successfully
integrated to the bone and survived the
subsequent periods of treatment. However,
89.47% of the control sites depicted earlier
exposition of the membranes when com-
pared with the 15.79% of the test sites
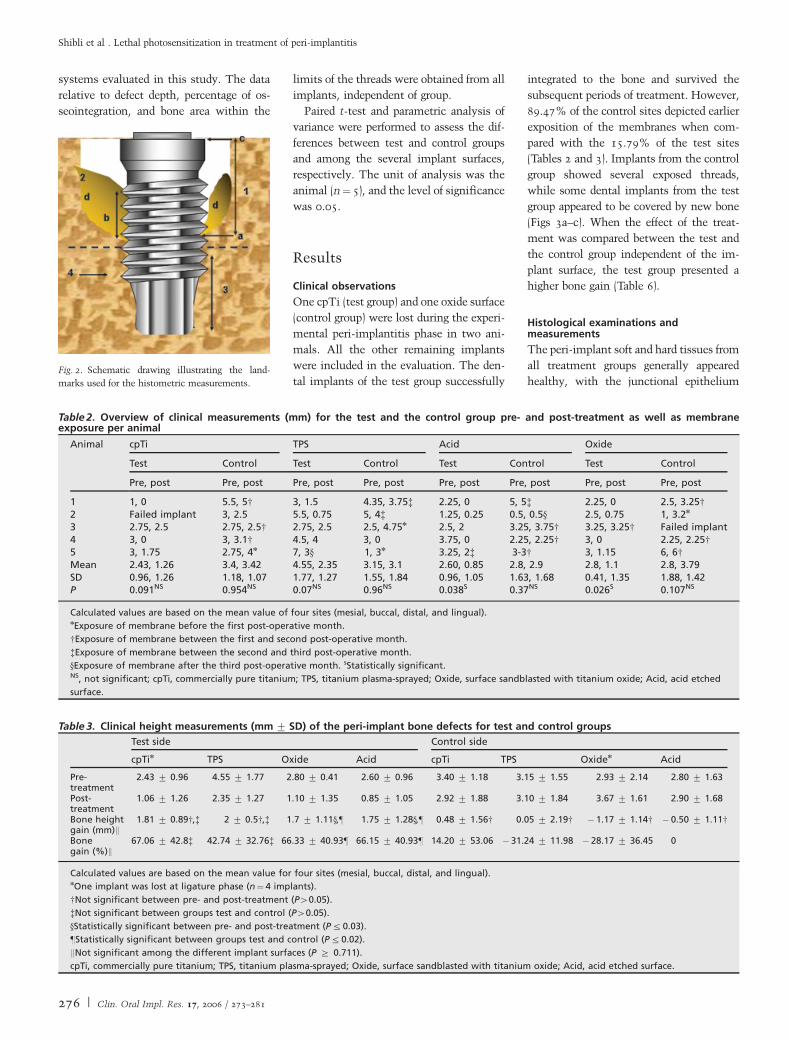
(Tables 2 and 3). Implants from the control
group showed several exposed threads,
while some dental implants from the test
group appeared to be covered by new bone
(Figs 3a–c). When the effect of the treat-
ment was compared between the test and
the control group independent of the im-
plant surface, the test group presented a
higher bone gain (Table 6).
Histological examinations andmeasurements
The peri-implant soft and hard tissues from
all treatment groups generally appeared
healthy, with the junctional epithelium
Table 2. Overview of clinical measurements (mm) for the test and the control group pre- and post-treatment as well as membraneexposure per animal
Animal cpTi TPS Acid Oxide
Test Control Test Control Test Control Test Control
Pre, post Pre, post Pre, post Pre, post Pre, post Pre, post Pre, post Pre, post
1 1, 0 5.5, 5w 3, 1.5 4.35, 3.75z 2.25, 0 5, 5z 2.25, 0 2.5, 3.25w2 Failed implant 3, 2.5 5.5, 0.75 5, 4z 1.25, 0.25 0.5, 0.5y 2.5, 0.75 1, 3.2n
3 2.75, 2.5 2.75, 2.5w 2.75, 2.5 2.5, 4.75n 2.5, 2 3.25, 3.75w 3.25, 3.25w Failed implant4 3, 0 3, 3.1w 4.5, 4 3, 0 3.75, 0 2.25, 2.25w 3, 0 2.25, 2.25w5 3, 1.75 2.75, 4n 7, 3y 1, 3n 3.25, 2z 3-3w 3, 1.15 6, 6wMean 2.43, 1.26 3.4, 3.42 4.55, 2.35 3.15, 3.1 2.60, 0.85 2.8, 2.9 2.8, 1.1 2.8, 3.79SD 0.96, 1.26 1.18, 1.07 1.77, 1.27 1.55, 1.84 0.96, 1.05 1.63, 1.68 0.41, 1.35 1.88, 1.42P 0.091NS 0.954NS 0.07NS 0.96NS 0.038S 0.37NS 0.026S 0.107NS
Calculated values are based on the mean value of four sites (mesial, buccal, distal, and lingual).nExposure of membrane before the first post-operative month.
wExposure of membrane between the first and second post-operative month.
zExposure of membrane between the second and third post-operative month.
yExposure of membrane after the third post-operative month. sStatistically significant.NS, not significant; cpTi, commercially pure titanium; TPS, titanium plasma-sprayed; Oxide, surface sandblasted with titanium oxide; Acid, acid etched
surface.
Table 3. Clinical height measurements (mm� SD) of the peri-implant bone defects for test and control groups
Test side Control side
cpTin TPS Oxide Acid cpTi TPS Oxiden Acid
Pre-treatment
2.43 � 0.96 4.55 � 1.77 2.80 � 0.41 2.60 � 0.96 3.40 � 1.18 3.15 � 1.55 2.93 � 2.14 2.80 � 1.63
Post-treatment
1.06 � 1.26 2.35 � 1.27 1.10 � 1.35 0.85 � 1.05 2.92 � 1.88 3.10 � 1.84 3.67 � 1.61 2.90 � 1.68
Bone heightgain (mm)k
1.81 � 0.89w,z 2 � 0.5w,z 1.7 � 1.11y,z 1.75 � 1.28y,z 0.48 � 1.56w 0.05 � 2.19w � 1.17 � 1.14w � 0.50 � 1.11w
Bonegain (%)k
67.06 � 42.8z 42.74 � 32.76z 66.33 � 40.93z 66.15 � 40.93z 14.20 � 53.06 � 31.24 � 11.98 � 28.17 � 36.45 0
Calculated values are based on the mean value for four sites (mesial, buccal, distal, and lingual).nOne implant was lost at ligature phase (n¼ 4 implants).
wNot significant between pre- and post-treatment (P40.05).
zNot significant between groups test and control (P40.05).
yStatistically significant between pre- and post-treatment (P�0.03).
zStatistically significant between groups test and control (P�0.02).
kNot significant among the different implant surfaces (P � 0.711).
cpTi, commercially pure titanium; TPS, titanium plasma-sprayed; Oxide, surface sandblasted with titanium oxide; Acid, acid etched surface.
Fig. 2. Schematic drawing illustrating the land-
marks used for the histometric measurements.
Shibli et al . Lethal photosensitization in treatment of peri-implantitis
276 | Clin. Oral Impl. Res. 17, 2006 / 273–281
extending a short distance apical to the
implant shoulder. The connective tissue
seemed to be compromised primarily by
dense collagenous fibers, which ran parallel
to the previously ‘contaminated’ implant
surface. The old bone was mostly lamellar
and compact, and numerous osteocytes
were presented in their lacunae, while
the newly formed bone exhibited different
stages of maturation and remodelation,
mainly in the test group.
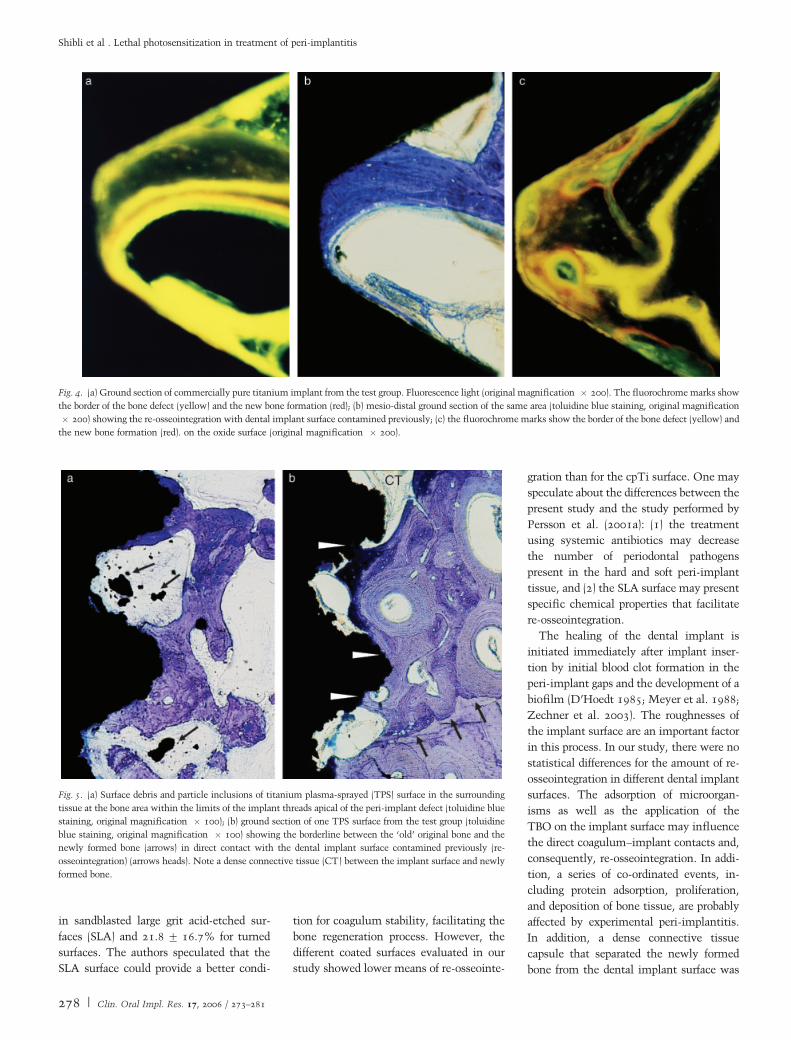
The biopsies from the sites where the
membrane had been exposed showed very
few spicules of bone at the base of the
connective tissue cap. In some cases, os-
teoblasts were connected to newly formed
bone, indicating ongoing bone formation,
and minor apposition of new bone could be
found, specifically at the apical regions of
the originally induced defects; however,
the bone tissue appeared immature. The
bone marker projected in a lateral–coronal
direction and separated a triangular-shaped
portion of newly formed regenerated bone
from the ‘old’ bone (Figs 4a–c).
Only the TPS implants presented surface
debris or particle inclusions in the sur-
rounding tissue at the bone area, within
the limits of the implant threads at the
apical portion of the peri-implant defect,
where peri-implantitis did not occur (Figs
5a and b).
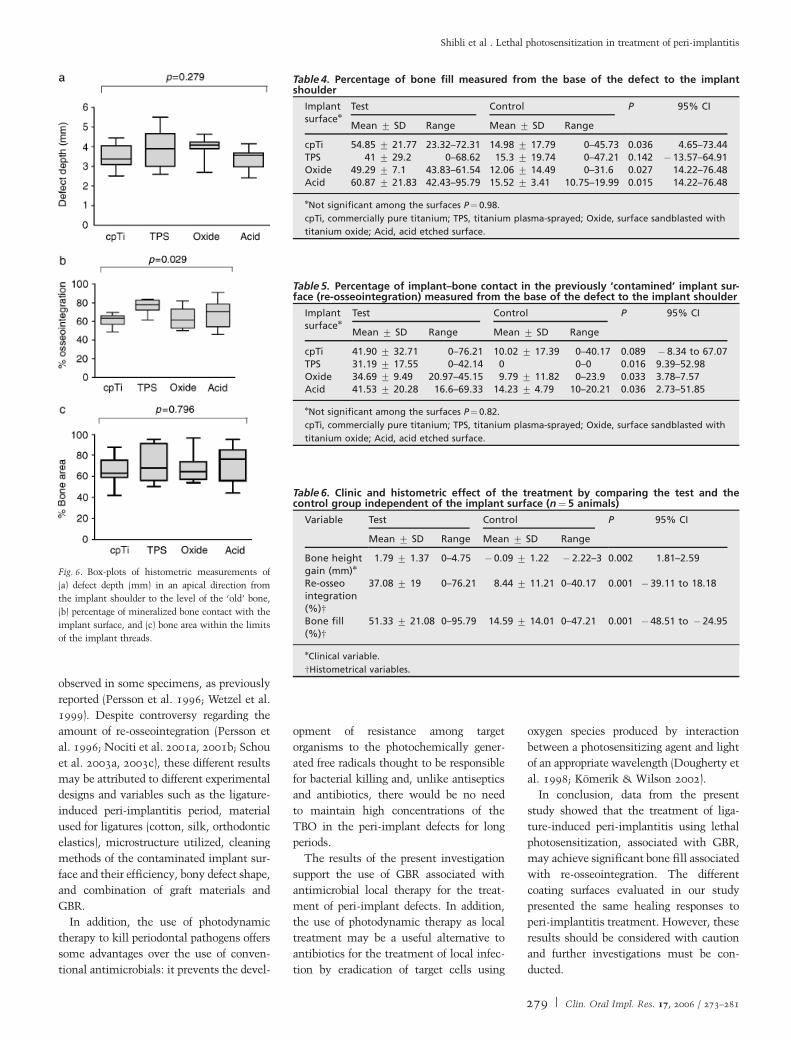
The defect depth, the percentage of
mineralized bone contact with the dental
implant surface, and the bone area within
the limits of the threads are presented in
Fig. 6. The highest percentage of osseointe-
gration was 73.58% of the TPS surface and
the lowest was 61.48% of the cpTi surface
(P¼ 0.029).
Bone filling was statistically significant
between the test and control groups
(P�0.036) (Tables 4 and 6). In some speci-
mens, the lateral aspect of the coronal part
of the dental implant was covered by a
dense connective tissue capsule separating
the newly formed bone from the dental
implant surface (Fig. 5b).
The mean percentage of re-osseointegra-
tion was 31–41% for the test group and 0–
14% for the control group (Tables 5 and 6).
In some specimens in the control group,
there was no contact between new bone
and the previously contaminated implant
surface (Figs 7a and b).
Discussion
The difficulties in obtaining re-osseointe-
gration after treatment of peri-implantitis
have been documented in several animal
studies (Grunder et al. 1993; Ericsson et al.
1996; Persson et al. 1996; Hanisch et al.
1997; Wetzel et al. 1999; Shibli et al.
2003b). Recently, Kolonidis et al. (2003)
showed that re-osseointegration occurred
on a surface previously contaminated
with bacterial biofilm. However, the ani-
mal model used by Kolonidis et al. (2003) is
not comparable, either with the animal
model used in our study, or with the pre-
viously cited studies (Grunder et al. 1993;
Ericsson et al. 1996; Persson et al. 1996,
1999; Wetzel et al. 1999; Nociti et al.
2001a, 2001b; Persson et al. 2001a; Shibli
et al. 2003b) because of lack of important
factors such as peri-implant soft and hard
tissue breakdown induced by ligatures, the
presence of bone defect, and presence of
bone debris at the implant surface.
The amount of bone regeneration was
significantly influenced by the photosensi-
tization treatment. The earlier exposition
of the membranes, as well as the mainte-
nance of these barriers can jeopardize tissue
regeneration (Lekholm et al. 1993;
Machado et al. 1999; Haas et al. 2000).
The complications because of membrane
exposition in the control group may sup-
port the findings that the presence of perio-
dontal pathogens at the dental implant
fixture altered the cell responses, together
with enhanced protease activities and for-
eign body reactions, decreasing the efficacy
of GBR (Wakabayashi et al. 1996; Slots et
al. 1999). The control group presented 5.6
times more earlier membrane exposition
when compared with the test group. In the
present investigation, the clinical evalua-
tion pre- and post-treatment revealed a
variable degree of appreciable hard-tissue
fill of the peri-implant defects, mainly for
the test group.
The histometric analysis depicts a statis-
tically higher amount of new bone forma-
tion for the test group. Although the
percentages of bone fill observed in studies
such as those by Wetzel et al. (1999) and
Persson et al. (1999) were lower, our
results ranged between 41% for the TPS
surface and 60.87% for the acid surface, in
agreement with Persson et al. (1996, 1999),
although the last two studies cited utilized
smooth surfaces.
Re-osseointegration was achieved on all
dental implant surfaces of the test group,
principally at the base of the angular bony
defect, in agreement with previous studies
(Jovanovic et al. 1993; Singh et al. 1993;
Persson et al. 1996; Shibli et al. 2003b).
The higher percentage of re-osseointegra-
tion observed in our investigation was
41.90%, of the cpTi surface, and the low-
est was on the TPS surface (31.19%),
which is in agreement with the results
described by Hanisch et al. (1997) and
higher when compared with the results
presented by Wetzel et al. (1999) and Shibli
et al. (2003b).
On the other hand, Persson et al. (2001a)
found 83.7� 8.6% of re-osseointegration
Fig. 3. (a) Peri-implant defect adjacent to commer-
cially pure titanium (left) and acid surface (right)
after mechanical debridment; (b) clinical view of the
same defect 4 months after lethal photosensitization
and guided bone regeneration. Note the contour of
the newly formed bone (arrows) on the peri-implant
defect; (c) clinical view of peri-implant defects from
the control group covered by fibrous tissue after
membrane removal. The membrane exposure oc-
curred after 1 month post-treatment.
Shibli et al . Lethal photosensitization in treatment of peri-implantitis
277 | Clin. Oral Impl. Res. 17, 2006 / 273–281
in sandblasted large grit acid-etched sur-
faces (SLA) and 21.8� 16.7% for turned
surfaces. The authors speculated that the
SLA surface could provide a better condi-
tion for coagulum stability, facilitating the
bone regeneration process. However, the
different coated surfaces evaluated in our
study showed lower means of re-osseointe-
gration than for the cpTi surface. One may
speculate about the differences between the
present study and the study performed by
Persson et al. (2001a): (1) the treatment
using systemic antibiotics may decrease
the number of periodontal pathogens
present in the hard and soft peri-implant
tissue, and (2) the SLA surface may present
specific chemical properties that facilitate
re-osseointegration.
The healing of the dental implant is
initiated immediately after implant inser-
tion by initial blood clot formation in the
peri-implant gaps and the development of a
biofilm (D’Hoedt 1985; Meyer et al. 1988;
Zechner et al. 2003). The roughnesses of
the implant surface are an important factor
in this process. In our study, there were no
statistical differences for the amount of re-
osseointegration in different dental implant
surfaces. The adsorption of microorgan-
isms as well as the application of the
TBO on the implant surface may influence
the direct coagulum–implant contacts and,
consequently, re-osseointegration. In addi-
tion, a series of co-ordinated events, in-
cluding protein adsorption, proliferation,
and deposition of bone tissue, are probably
affected by experimental peri-implantitis.
In addition, a dense connective tissue
capsule that separated the newly formed
bone from the dental implant surface was
Fig. 4. (a) Ground section of commercially pure titanium implant from the test group. Fluorescence light (original magnification � 200). The fluorochrome marks show
the border of the bone defect (yellow) and the new bone formation (red); (b) mesio-distal ground section of the same area (toluidine blue staining, original magnification
� 200) showing the re-osseointegration with dental implant surface contamined previously; (c) the fluorochrome marks show the border of the bone defect (yellow) and
the new bone formation (red). on the oxide surface (original magnification � 200).
Fig. 5. (a) Surface debris and particle inclusions of titanium plasma-sprayed (TPS) surface in the surrounding
tissue at the bone area within the limits of the implant threads apical of the peri-implant defect (toluidine blue
staining, original magnification � 100); (b) ground section of one TPS surface from the test group (toluidine
blue staining, original magnification � 100) showing the borderline between the ‘old’ original bone and the
newly formed bone (arrows) in direct contact with the dental implant surface contamined previously (re-
osseointegration) (arrows heads). Note a dense connective tissue (CT) between the implant surface and newly
formed bone.
Shibli et al . Lethal photosensitization in treatment of peri-implantitis
278 | Clin. Oral Impl. Res. 17, 2006 / 273–281
observed in some specimens, as previously
reported (Persson et al. 1996; Wetzel et al.
1999). Despite controversy regarding the
amount of re-osseointegration (Persson et
al. 1996; Nociti et al. 2001a, 2001b; Schou
et al. 2003a, 2003c), these different results
may be attributed to different experimental
designs and variables such as the ligature-
induced peri-implantitis period, material
used for ligatures (cotton, silk, orthodontic
elastics), microstructure utilized, cleaning
methods of the contaminated implant sur-
face and their efficiency, bony defect shape,
and combination of graft materials and
GBR.
In addition, the use of photodynamic
therapy to kill periodontal pathogens offers
some advantages over the use of conven-
tional antimicrobials: it prevents the devel-
opment of resistance among target
organisms to the photochemically gener-
ated free radicals thought to be responsible
for bacterial killing and, unlike antiseptics
and antibiotics, there would be no need
to maintain high concentrations of the
TBO in the peri-implant defects for long
periods.
The results of the present investigation
support the use of GBR associated with
antimicrobial local therapy for the treat-
ment of peri-implant defects. In addition,
the use of photodynamic therapy as local
treatment may be a useful alternative to
antibiotics for the treatment of local infec-
tion by eradication of target cells using
oxygen species produced by interaction
between a photosensitizing agent and light
of an appropriate wavelength (Dougherty et
al. 1998; Komerik & Wilson 2002).
In conclusion, data from the present
study showed that the treatment of liga-
ture-induced peri-implantitis using lethal
photosensitization, associated with GBR,
may achieve significant bone fill associated
with re-osseointegration. The different
coating surfaces evaluated in our study
presented the same healing responses to
peri-implantitis treatment. However, these
results should be considered with caution
and further investigations must be con-
ducted.
Table 4. Percentage of bone fill measured from the base of the defect to the implantshoulder
Implantsurfacen
Test Control P 95% CI
Mean � SD Range Mean � SD Range
cpTi 54.85 � 21.77 23.32–72.31 14.98 � 17.79 0–45.73 0.036 4.65–73.44TPS 41 � 29.2 0–68.62 15.3 � 19.74 0–47.21 0.142 � 13.57–64.91Oxide 49.29 � 7.1 43.83–61.54 12.06 � 14.49 0–31.6 0.027 14.22–76.48Acid 60.87 � 21.83 42.43–95.79 15.52 � 3.41 10.75–19.99 0.015 14.22–76.48
nNot significant among the surfaces P¼ 0.98.
cpTi, commercially pure titanium; TPS, titanium plasma-sprayed; Oxide, surface sandblasted with
titanium oxide; Acid, acid etched surface.
Fig. 6. Box-plots of histometric measurements of
(a) defect depth (mm) in an apical direction from
the implant shoulder to the level of the ‘old’ bone,
(b) percentage of mineralized bone contact with the
implant surface, and (c) bone area within the limits
of the implant threads.
Table 6. Clinic and histometric effect of the treatment by comparing the test and thecontrol group independent of the implant surface (n¼5 animals)
Variable Test Control P 95% CI
Mean � SD Range Mean � SD Range
Bone heightgain (mm)n
1.79 � 1.37 0–4.75 � 0.09 � 1.22 � 2.22–3 0.002 1.81–2.59
Re-osseointegration(%)w
37.08 � 19 0–76.21 8.44 � 11.21 0–40.17 0.001 � 39.11 to 18.18
Bone fill(%)w
51.33 � 21.08 0–95.79 14.59 � 14.01 0–47.21 0.001 � 48.51 to � 24.95
nClinical variable.
wHistometrical variables.
Table 5. Percentage of implant–bone contact in the previously ‘contamined’ implant sur-face (re-osseointegration) measured from the base of the defect to the implant shoulder
Implantsurfacen
Test Control P 95% CI
Mean � SD Range Mean � SD Range
cpTi 41.90 � 32.71 0–76.21 10.02 � 17.39 0–40.17 0.089 � 8.34 to 67.07TPS 31.19 � 17.55 0–42.14 0 0–0 0.016 9.39–52.98Oxide 34.69 � 9.49 20.97–45.15 9.79 � 11.82 0–23.9 0.033 3.78–7.57Acid 41.53 � 20.28 16.6–69.33 14.23 � 4.79 10–20.21 0.036 2.73–51.85
nNot significant among the surfaces P¼ 0.82.
cpTi, commercially pure titanium; TPS, titanium plasma-sprayed; Oxide, surface sandblasted with
titanium oxide; Acid, acid etched surface.
Shibli et al . Lethal photosensitization in treatment of peri-implantitis
279 | Clin. Oral Impl. Res. 17, 2006 / 273–281

Acknowledgements: This research
was supported by FAPESP (Fundacao de
Amparo a Pesquisa do Estado de Sao
Paulo, SP, Brazil) grant no. 00/02433-1
and FUNDUNESP (Fundacao para o
Desenvolvimento da UNESP, Sao Paulo,
Brazil). The authors appreciate the
assistance of Dr Vagner Samy Lemo in
all the surgical phases. The authors are
also indebted to Conexao Implants,
Brazil, for providing the oxide dental
implants, INP – Brazil for the titanium
tacks, and Implamed Brazil for cpTi and
TPS implants.
Source of support: FAPESP (00/02433-1)
and FUNDUNESP.
References
Baier, R.E. & Meyer, A.E. (1988) Implant surface
preparation. International Journal of Oral &
Maxillofacial Implants 3: 9–20.
Baier, R.E., Meyer, A.E., Natiella, J.R., Natiella,
R.R. & Carter, J.M. (1984) Surface properties
determine bioadhesive outcomes: methods and
results. Journal of Biomedical Materials Research
18: 337–355.
Bhatti, M., MacRobert, A., Henderson, B.,
Shepherd, P., Cridland, J. & Wilson, M. (2000)
Antibody-target lethal photosensitization of
Porphyromonas gingivalis. Antimicrobians
Agents Chemotherapics 44: 2615–2618.
Bhatti, M., MacRobert, A., Meghji, S., Henderson,
B. & Wilson, M. (1997) Effect of dosimetric and
physiological factors on the lethal photosensitiza-
tion of Porphyromonas gingivalis in vitro. Photo-
chemistry and Photobiology 65: 1026–1031.
Bhatti, M., MacRobert, A., Meghji, S., Henderson,
B. & Wilson, M. (1998) A study of the uptake of
toluidine blue O by Porphyromonas gingivalis and
the mechanism of lethal photosensitization.
Photochemistry and Photobiology 68: 370–376.
D’Hoedt, B. (1985) The influence of implant mate-
rials and material surfaces on blood clotting: a
scanning electron microscopy study. In: van
Steenburgh, D., Albrektsson, T., Branemark,
P.I., Henry, P.J., Holt, R. & Linden, C. eds.
Tissue integration in oral and maxillofacial recon-
struction. Proceedings of an International Con-
gress. Current Clinical Practice Series 29: 46–50.
Dobson, J. & Wilson, M. (1992) Sensitization of oral
bacteria in biofilms to killing by light from a low
power laser. Archives of Oral Biology 37: 883–
887.
Donath, K. & Breuner, G.A. (1982) A method for
undecalcified bones and teeth with attached soft
tissues. The Sage Schliff technique. Journal of
Oral Pathology 11: 318–325.
Dougherty, T.J., Gomer, C.J., Henderson, B.W.,
Jori, G., Kessel, D., Korbelik, M. & Moan, J.
(1998) Photodynamic therapy. Journal of the Na-
tional Cancer Institute 90: 889–905.
Ericsson, I., Persson, L.G., Berglundh, T., Edlund,
T. & Lindhe, J. (1996) The effect of antimicrobial
therapy on peri-implantitis lesion. An experimen-
tal study in dog. Clinical Oral Implants Research
7: 320–328.
Esposito, E., Lausmaa, J., Hirsch, J.M. & Thomsen,
P. (1999) Surface analysis of failed oral titanium
implants. Journal of Biomedical Materials Re-
search (Applied Biomaterials) 48: 559–568.
Grunder, U., Hurzeler, M.B., Schupbach, P. &
Strub, J.R. (1993) Treatment of ligature-induced
peri-implantitis using guided tissue regeneration:
a clinical and histological study in the beagle dog.
International Journal of Oral & Maxillofacial
Implants 8: 282–293.
Hass, R., Baron, M., Dortbudak, O. & Watzek, G.
(2000) Lethal photosensitization, autogenous
bone, and e-PTFE membrane for the treatment
of peri-implantitis: preliminary results. Interna-
tional Journal of Oral & Maxillofacial Implants
15: 374–382.
Hanisch, O., Tatakis, D.N., Boskovic, M., Rohrer,
M.D. & Wikesjo, U.M.E. (1997) Bone formation
and re-osseointegration in peri-implantitis defects
following surgical implantation of rhBMP-2. In-
ternational Journal of Oral & Maxillofacial Im-
plants 12: 604–610.
Henry, C.A., Judy, M., Dyer, B., Wagner, M. &
Matthews, J. (1995) Sensitivity of Porphyromonas
and Prevotella species in liquid media to argon
laser. Photochemistry and Photobiology 61: 410–
413.
Jovanovic, S.A., Keney, E.B., Carranza, F.A. &
Donath, K. (1993) The regenerative potencial of
plaque induced peri-implant bone defects treated
Fig. 7. (a) Ground section of acid surface implant (test group) shown in Figs 3a and b. (toluidine blue staining,
original magnification � 25) showing the borderline (arrows) between the ‘old’ original bone and the newly
formed bone; (b) mesio-distal ground section of one oxide surface from the control group shown in Fig. 5c
(Toluidine blue staining, original magnification � 16). Note the connective tissue covering the dental implant
surface and the absence of newly regenerated bone.
Shibli et al . Lethal photosensitization in treatment of peri-implantitis
280 | Clin. Oral Impl. Res. 17, 2006 / 273–281

by submerged membrane technique: an experi-
mental study. International Journal of Oral &
Maxillofacial Implants 8: 13–18.
Kolonidis, S., Renvert, S., Hammerle, C.H.F., Lang,
N.P., Harris, D. & Claffey, N. (2003) Osseointe-
gration on implant surfaces previously contam-
ined with plaque. An experimental study in the
dog. Clinical Oral Implants Research 14: 373–
380.
Komerik, N. & Wilson, M. (2002) Factors influen-
cing the susceptibility of Gram-negative bacteria
to toluidine blue O-mediated lethal photosensiti-
zation. Journal of Applied Microbiology 92: 618–
623.
Lang, N.P., Bragger, U., Walther, D., Beamer, B. &
Kornman, K.S. (1993) Ligature-induced peri-im-
plant infection in cynomolgus monkeys. I. Clin-
ical and radiographic findings. Clinical Oral
Implants Research 4: 2–11.
Lekholm, U., Becker, W., Dahlin, C., Becker, B.,
Donath, K. & Morrison, E. (1993) The role of
early versus late removal of GTAM membranes
on bone formation at oral implants placed into
immediate extraction sockets. An experimental
study in dogs. Clinical Oral Implants Research 4:
121–129.
Machado, M.A., Stefani, C.M., Sallum, E.A.,
Sallum, A.W., Tramontina, V.A., Nogueira-Filho,
G.R. & Nociti Jr., F.H. (2000) Treatment of
ligature-induced peri-implantitis defects by
regenerative procedures. Part II: a histometric
study in dogs. Journal of Oral Science 42: 163–
168.
Meyer, A., Baier, R., Natiella, J. & Meenagha, M.
(1998) Investigation of tissue/implant interactions
during the first two hours of implantation. Journal
of Oral Implantology 14: 363–379.
Nociti Jr, F.H., Machado, M.A.N., Stefani, C.M. &
Sallum, E.A. (2001b) Absorbable versus nona-
borbable membranes and bone grafts in the treat-
ment of ligature-induce peri-implantitis defects in
dogs: a histometric investigation. International
Journal of Oral & Maxillofacial Implants 16:
646–652.
Nociti Jr, F.H., Machado, M.A.N., Stefani, C.M.,
Sallum, E.A. & Sallum, A.W. (2001a) Absorbable
versus nonaborbable membranes and bone
grafts in the treatment of ligature-induce peri-
implantitis defects in dogs. Part I. A clinical
investigation. Clinical Oral Implants Research
12: 115–120.
Olefjord, I. & Hansson, S. (1993) Surface analysis of
four dental implant systems. International Jour-
nal of Oral & Maxillofacial Implants 8: 32–40.
Persson, L.G., Araujo, M.G., Berglundh, T., Gron-
dahl, K. & Lindhe, J. (1999) Resolution of peri-
implantitis following treatment. An experimental
study in the dog. Clinical Oral Implants Re-
search 10: 195–203.
Persson, L.G., Berglundh, T., Lindhe, J. & Sen-
nerby, L. (2001a) Re-osseointegration after peri-
implantitis at different implant surfaces. An ex-
perimental study in the dog. Clinical Oral Im-
plants Research 12: 595–603.
Persson, L.G., Ericsson, I., Berglundh, T. & Lindhe,
J. (1996) Guided bone regeneration in the treat-
ment of periimplantitis. Clinical Oral Implants
Research 7: 366–372.
Persson, L.G., Ericsson, I., Berglundh, T. & Lindhe,
J. (2001b) Osseointegration following treatment of
peri-implantitis and replacement of implant com-
ponents. An experimental study in the dog. Jour-
nal of Clinical Periodontology 28: 258–263.
Quirynen, M., De Soete, M. & van Steenberghe, D.
(2002) Infectious risks for oral implants: a review
of the literature. Clinical Oral Implants Research
12: 1–19.
Sarkar, S. & Wilson, M. (1993) Lethal photosensi-
tization of bacteria in subgingival plaque samples
from patients with chronic periodontitis. Journal
of Periodontal Research 28: 204–210.
Schou, S., Holmstrup, P., Keiding, N. & Fiehn, N.E.
(1993) Ligature induced marginal inflamation
around osseointegrated implants and ankylosed
teeth. Clinical and radiographic observations in
cynomolgus monkeys (Macaca fascicularis).
Clinical Oral Implants Research 4: 12–22.
Schou, S., Holmstrup, P., J�rgensen, T., Skovgaard,
L.T., Stolze, K., Hj�rting-Hansen, E. & Wenzel,
A. (2003a) Implant surface preparation in the
surgical treatment of experimental peri-implanti-
tis with autogenous bone graft and ePTFE mem-
brane in cynomolgus monkeys. Clinical Oral
Implants Research 14: 412–422.
Schou, S., Holmstrup, P., J�rgensen, T., Stolze, K.,
Hj�rting-Hansen, E. & Wenzel, A. (2003b) Auto-
genous bone graft and ePTFE membrane in the
treatment of peri-implantitis. I. Clinical and radio-
graphic observations in cynomolgus monkeys.
Clinical Oral Implants Research 14: 391–403.
Schou, S., Holmstrup, P., Skovgaard, L.T., Stolze,
K., Hj�rting-Hansen, E. & Gundersen, H.J.G.
(2003c) Autogenous bone graft and ePTFE mem-
brane in the treatment of peri-implantitis. II.
Stereologic and histologic observations in cyno-
molgus monkeys. Clinical Oral Implants Re-
search 14: 404–411.
Shibli, J.A., Martins, M.C., Lotufo, R.F. & Marcan-
tonio Jr, E. (2003a) Microbiologic and radiographic
analysis of ligature-induced peri-implantitis. In-
ternational Journal of Oral & Maxillofacial Im-
plants 18: 383–390.
Shibli, J.A., Martins, M.C., Nociti Jr, F.H., Garcia,
V.G. & Marcantonio Jr, E. (2003b) Treatment of
ligature-induced peri-implantitis by lethal photo-
sensitization and guided bone regeneration: a
histologic study in dogs. Journal of Perio-
dontology 74: 338–345.
Shibli, J.A., Martins, M.C., Theodoro, L.H., Lotufo,
R.F.M., Garcia, V.G. & Marcantonio Jr, E.
(2003c) Lethal photosensitization in microbiolo-
gical treatment of ligature-induced peri-implanti-
tis: a preliminary study in dogs. Journal of Oral
Science 45: 17–23.
Shibli, J.A., Theodoro, L.H., Haypek, P., Garcia,
V.G. & Marcantonio Jr, E. (2004) The effect of
CO2 laser irradiation on failed implant surfaces.
Implant Dentistry 13: 104–114.
Singh, G., O’Neal, R.B., Brennam, W.A., Strong,
S.L., Horner, J.A. & Van Dyke, T.E.
(1993) Surgical treatment of induced peri-
implantitis in the micro pig: clinical and histolo-
gical analysis. Journal of Periodontology 64:
984–989.
Slots, J., MacDonald, E.S. & Nowzary, H. (1999)
Infectious aspects of periodontal regeneration.
Periodontology 2000 19: 164–172.
Wakabayashi, R.C., Wong, F., Richards, D.W. &
Johnson, P.W. (1996) Protease repertories of cells
adherent to membranes recovered after guided
tissue regeneration. Journal of Periodontal Re-
search 31: 171–180.
Wetzel, A.C., Vlassis, J., Hammerle, C.H.F. &
Lang, N.P. (1999) Attempts to obtain re-osseon-
tegration following experimental peri-implantitis
in dogs. Clinical Oral Implants Research 10:
111–119.
Zechner, W., Tangl, S., Furst, G., Tepper, G.,
Thams, U., Mailath, G. & Watzek, G. (2003)
Osseous healing characteristics of three different
implant types. A histological and histomorpho-
metric study in mini-pigs. Clinical Oral Implants
Research 14: 150–157.
Shibli et al . Lethal photosensitization in treatment of peri-implantitis
281 | Clin. Oral Impl. Res. 17, 2006 / 273–281
Related Documents