Nursing Best Practice Guideline Shaping the future of Nursing Integrating Smoking Cessation into Daily Nursing Practice Revised March 2007

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Nursing Best Practice GuidelineShaping the future of Nursing
Integrating Smoking Cessationinto Daily Nursing Practice
Revised March 2007
Greetings from Doris Grinspun
Executive Director
Registered Nurses’ Association of Ontario
It is with great excitement that the Registered Nurses’ Association of Ontario (RNAO)
disseminates this revised nursing best practice guideline to you. Evidence-based practice
supports the excellence in service that nurses are committed to deliver in our day-to-day
practice. The RNAO is committed to ensuring that the evidence supporting guideline
recommendations is the best available, and this guideline has been recently reviewed and
revised to reflect the current state of knowledge.
We offer our endless thanks to the many institutions and individuals that are making RNAO’s vision for
Nursing Best Practice Guidelines (NBPGs) a reality. The Government of Ontario recognized RNAO’s ability
to lead this program and is providing multi-year funding. Tazim Virani – NBPG program director – with her
fearless determination and skills, is moving the program forward faster and stronger than ever imagined.
The nursing community, with its commitment and passion for excellence in nursing care, is providing the
knowledge and countless hours essential to the creation, evaluation and revision of each guideline.
Employers have responded enthusiastically to the request for proposals (RFP), and are opening their
organizations to pilot test the NBPGs.
Now comes the true test in this phenomenal journey: Will nurses utilize the guidelines in their day-to-day practice?
Successful uptake of these NBPGs requires a concerted effort of four groups: nurses themselves, other
healthcare colleagues, nurse educators in academic and practice settings, and employers. After lodging
these guidelines into their minds and hearts, knowledgeable and skillful nurses and nursing students need
healthy and supportive work environments to help bring these guidelines to life.
We ask that you share this NBPG, and others, with members of the interdisciplinary team. There is much to
learn from one another. Together, we can ensure that Ontarians receive the best possible care every time
they come in contact with us. Let’s make them the real winners of this important effort!
RNAO will continue to work hard at developing and evaluating future guidelines. We wish you the best for a
successful implementation!
Doris Grinspun, RN, MSN, PhD (cand), OOnt
Executive Director
Registered Nurses’ Association of Ontario
5
Nursing Best Practice Guideline
Project Team:
Tazim Virani, RN, MScN, PhD(cand)Program Director
Heather McConnell, RN, BScN, MA(Ed)Program Manager
Samantha Mayo, RN, BScN, MNProgram Coordinator
Janet Chee, RN, BScN, MNProgram Coordinator
Julie BurrisProgram Assistant
Jill-Marie Burke, BAPublic Relations/Communications
Elizabeth Chiu, HBSc, MPCProgram Assistant
Meagan Cleary, BAProgram Assistant
Carrie ScottProgram Assistant
Citlali Villa SinghProgram Assistant
Keith Powell, BA, AITWeb Editor
Integrating Smoking Cessation intoDaily Nursing Practice
Registered Nurses’ Association of Ontario
Nursing Best Practice Guidelines Program
158 Pearl St.
Toronto, Ontario M5H 1L3
Website: www.rnao.org/bestpractices

Janet Nevala, RN, BScN Team Leader
Consultant, The Program Training and
Consultation Centre
Ottawa, Ontario
Carol Bossenberry, RN, BN, TTSTobacco Use Prevention Coordinator
Oxford County Public Health &
Emergency Services
Woodstock, Ontario
Jennifer Hart, MPADirector, Clinical Tobacco Intervention Program
Ontario Medical Association
Toronto, Ontario
Sherrie Hertz, BScPhm., R.PhDirector, Pharmacy Programs
Ontario Pharmacists’ Association
Don Mills, Ontario
Sharon Lawler, RN, BA, MEdCo-Director and Manager,
Leave the Pack Behind Program
Community Health Science Dept.
Brock University
St. Catharines, Ontario
Joan Mitchell, RN(EC),Primary Health Care Nurse Practitioner
Byron Family Medical Centre
London, Ontario
Annette Railton, RN, BScNOperating Room (CPT)
Welland Hospital Site Niagara Health System
Welland, Ontario
Annette Schultz, RN, PhDAssistant Professor, Cancer Prevention
Cancer Nursing Research
Faculty of Nursing, University of Manitoba
Winnipeg, Manitoba
Declarations of interest and confidentiality were
made by members of the guideline revision panel.
Further details are available from the Registered
Nurses’ Association of Ontario.
The RNAO also wishes to acknowledge Dawn
Kingston, RN, BSc, MSc, PhD (student) for her
work in conducting the quality appraisal of the
literature and preparation of evidence tables.
The RNAO would also like to acknowledge Bonnie
Quinlan, RN for her contribution to this guideline
revision as a reviewer.
Integrating Smoking Cessation into Daily Nursing Practice
6
Revision Panel Members (2006/2007)
Declarations of interest and confidentiality were made by all members of the guideline development panel.
Further details are available from the Registered Nurses’ Association of Ontario

7
Nursing Best Practice Guideline
Janet Nevala, RN, BScNTeam Leader
Coordinator, Program Training and
Consultation Centre
Ontario Tobacco Strategy
City of Ottawa
Ottawa, Ontario
Carol Bossenberry, RN, BNTobacco Use Prevention Coordinator
County of Oxford, Department of Public
Health & Emergency Services
Woodstock, Ontario
Debbie Cooke, RN, BACardiac Prevention and Rehabilitation Nurse
Smoking Cessation Counsellor
University of Ottawa Heart Institute
Cardiac Prevention and Rehabilitation
Ottawa, Ontario
Nancy Edwards, RN, PhDProfessor, School of Nursing
Director, Community Health Research Unit
University of Ottawa
Ottawa, Ontario
Sharon Lawler, RN, BA, MEdManager, Leave The Pack Behind
Community Health Sciences Department
Brock University
St. Catharines, Ontario
Heather Logan*, RN, BScN, MHSc(c)Manager, Cancer Control Policy
Canadian Cancer Society
National Cancer Institute of Canada
Toronto, Ontario
Joan Mitchell, RN(EC)Primary Healthcare Nurse Practitioner
Community Care Access Centre
London Middlesex
London, Ontario
Shirley Saasto-Stopyra*, RN, PHNONA Representative (Local 014)
Public Health Nurse
Family Health Program
Thunder Bay District Health Unit
Thunder Bay, Ontario
Josephine Santos, RN, MNFacilitator, Project Coordinator
Nursing Best Practice Guideline Project
Registered Nurses’ Association of Ontario
Toronto, Ontario
Louise Walker*, BA, BScProvincial Coordinator, Smokers’ Helpline
Canadian Cancer Society
Ontario Division
Hamilton, Ontario
*Contributed to the initial development
of the guideline
Original Contributors
Development Panel Members (2003)

Integrating Smoking Cessation into Daily Nursing Practice
8
Stakeholder Acknowledgment
The Registered Nurses’ Association of Ontario wishes to acknowledge the following individuals and/or groups for their
contribution in reviewing this nursing best practice guideline and providing valuable feedback during the initial
development of this document (2001–2003):
Monique Bouvier Centre for Addiction and Mental Health, Hammond, Ontario
Wendy Burgoyne Algoma Best Start, Wawa, Ontario
Ruth Busija-Lowe Registered Nurse (retired), Woodstock, Ontario
Donald Déry Tobacco Project Officer, City of Ottawa, Agent de projet sur letabagisme, Ottawa, Ontario
Dr. Roberta Ferrence Director, Centre for Addiction and Mental Health,Ontario Tobacco Research Unit, Toronto, Ontario
Sherrie Hertz Program Manager, Clinical Tobacco Intervention Drug Information Pharmacist,Ontario Pharmacists’ Association, North York, Ontario
Simon Hoad Health Promotion Planner, Thunder Bay District Health Unit,Thunder Bay, Ontario
Colleen Kearns Public Health Nurse, Prenatal Tobacco Use Prevention, City of Ottawa,Ottawa, Ontario
Cheryl Kee Acute Care Nurse Practitioner-Cardiology, London Health Sciences Centre,London, Ontario
Dana Martin Registered Nurse, Gane Yohs Health Centre, Ohsweken Ontario
Elizabeth Martin Manager of Operations, Woodingford Lodge, Woodstock, Ontario
Dr. Paul W. McDonald Director, Centre for Applied Health Research, University of Waterloo,Waterloo, Ontario
Dr. William McLeish Oxford Interagency Council on Smoking and Health, Woodstock, Ontario
Phil Onafrychuk Occupational Health Nurse, Timberjack Inc., Woodstock, Ontario OntarioPhysical and Health Education Association, Toronto, Ontario
Dr. Andrew Pipe Director, Smoking Cessation Program, University of Ottawa Heart Institute,Ottawa, Ontario
Nancy Pogson Public Health Nurse, Kitchener, Ontario
Lorraine Repo Coordinator, Healthy Babies/Healthy Children, Thunder Bay District Health Unit,Thunder Bay, Ontario
Linda Ritchie Chair, Department of Nursing, Brock University, St. Catharines, Ontario
Sherryl Smith Health Promotion Coordinator, Somerset West Community Health Centre,Ottawa, Ontario
Tracey E. Taylor Program Manager, Healthy Lifestyles and Disease Prevention Branch, Social andPublic Health Services Department, City of Hamilton, Hamilton, Ontario

9
Nursing Best Practice Guideline
A special acknowledgment also goes to:
Barbara Willson, RN, MSc, and Anne Tait, RN, BScN, who served as Project Coordinators at the onset of the
guideline development.
RNAO also wishes to acknowledge the Centre for Addiction and Mental Health in Toronto, Ontario for their role in pilot
testing this guideline.
As well, RNAO sincerely acknowledges the leadership and dedication of the researchers who have directed the
evaluation phase of the Nursing Best Practice Guidelines Project, in 2002–2003. The Evaluation Team was comprised of:
Principal Investigators: Nancy Edwards, RN, PhD; Barbara Davies, RN, PhD – University of Ottawa
Evaluation Team: Maureen Dobbins, RN, PhD; Jenny Ploeg, RN, PhD; Jennifer Skelly, RN, PhD – McMaster University
Patricia Griffin, RN, PhD – University of Ottawa
Project Staff: Barbara Helliwell, BA(Hons); Marilynn Kuhn, MHA; Diana Ehlers, MA(SW), MA(Dem);
Christy-Ann Drouin, BBA; Sabrina Farmer, BA; Mandy Fisher, BN, MSc(cand); Lian Kitts, RN;
Elana Ptack, BA – University of Ottawa
Registered Nurses’ Association of Ontario
Nursing Best Practice Guidelines Program
158 Pearl St.
Toronto, Ontario M5H 1L3
Website: www.rnao.org/bestpractices

Integrating Smoking Cessation intoDaily Nursing Practice
Disclaimer
These best practice guidelines are related only to nursing practice and not intended to take into account
fiscal efficiencies. These guidelines are not binding for nurses and their use should be flexible to
accommodate client/family wishes and local circumstances. They neither constitute a liability or discharge
from liability. While every effort has been made to ensure the accuracy of the contents at the time of
publication, neither the authors nor the Registered Nurses’ Association of Ontario (RNAO) give any
guarantee as to the accuracy of the information contained in them nor accept any liability, with respect to
loss, damage, injury or expense arising from any such errors or omission in the contents of this work. Any
reference throughout the document to specific pharmaceutical products as examples does not imply
endorsement of any of these products.
Copyright
First published in 2003 by the Registered Nurses’ Association of Ontario. This document was revised in
March 2007.
With the exception of those portions of this document for which a specific prohibition or limitation against
copying appears, the balance of this document may be produced, reproduced and published in its entirety
only, in any form, including in electronic form, for educational or non-commercial purposes, without
requiring the consent or permission of the Registered Nurses’ Association of Ontario, provided that an
appropriate credit or citation appears in the copied work as follows:
Registered Nurses’ Association of Ontario (2007). Integrating Smoking Cessation into Daily Nursing
Practice. Revised. Toronto, Canada: Registered Nurses’ Association of Ontario.
Integrating Smoking Cessation into Daily Nursing Practice
10

11
How to Use this Document
This nursing best practice guideline is a comprehensive document providing resources necessaryfor the support of evidence-based nursing practice. The document should be reviewed and applied,based on the specific needs of the organization or practice setting/environment, as well as the needs andwishes of the client. Guidelines should not be applied in a “cookbook” fashion but used as a tool to assist indecision making for individualized client care, as well as ensuring that appropriate structures andsupports are in place to provide the best possible care.
Nurses, other healthcare professionals and administrators who are leading and facilitating practice changeswill find this document valuable for the development of policies, procedures, protocols, educationalprograms, assessments and documentation tools. It is recommended that the nursing best practiceguidelines be used as a resource tool. Nurses providing direct client care will benefit from reviewing therecommendations, the evidence in support of the recommendations and the process that was used todevelop the guidelines. However, it is highly recommended that practice settings/environments adaptthese guidelines in formats that would be user-friendly for daily use. This guideline has some suggestedformats for such local adaptation and tailoring.
Organizations wishing to use the guideline may decide to do so in a number of ways:■ Assess current nursing and healthcare practices using the recommendations in the guideline.■ Identify recommendations that will address identified needs or gaps in services.■ Systematically develop a plan to implement the recommendations using associated tools and resources.
RNAO is interested in hearing how you have implemented this guideline. Please contact us toshare your story. Implementation resources will be made available through the RNAO website atwww.rnao.org/bestpractices to assist individuals and organizations to implement best practice guidelines.
Nursing Best Practice Guideline

Table of Contents
Summary of Recommendations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14
Interpretation of Evidence . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16
Responsibility for Guideline Development. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16
Purpose & Scope . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 17
Original Development Process – 2001 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 19
Revision Process 2006/2007 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 20
Definition of Terms. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 22
Background Context . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 23
Practice Recommendations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 26
Education Recommendations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 34
Organization & Policy Recommendations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 35
Evaluation & Monitoring . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 38
Implementation Strategies. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 40
Research Gaps & Future Implications. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 41
Process for Update/Review of Guideline . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 42
References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 43
Bibliography . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 47
Integrating Smoking Cessation into Daily Nursing Practice
12

13
Appendix A – Search Strategy for Existing Evidence . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 54
Appendix B – Glossary of Terms. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 57
Appendix C – The Health Risks of Smoking . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 60
Appendix D – The Benefits of Quitting Smoking . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 65
Appendix E – Stages of Change Model . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 67
Appendix F – Identifying Your Client’s Readiness to Quit . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 69
Appendix G – Motivational Interviewing. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 70
Appendix H – Ask, Advise, Assist, Arrange Protocol . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 74
Appendix I – The WHY Test . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 76
Appendix J – Fagerstrom Test for Nicotine Dependence (Revised Version). . . . . . . . . . . . . . . . . . . . . . . . . . . 78
Appendix K – Intensive Nursing Intervention: Tips for the Client . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 79
Appendix L – Quit Smoking First-Line Medications Compared . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 80
Appendix M – Strategies to Avoid Relapse. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 83
Appendix N – List of Resources Available for Smoking Cessation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 84
Appendix O – Description of the Toolkit . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 87
Nursing Best Practice Guideline

Integrating Smoking Cessation into Daily Nursing Practice
14
Summary of RecommendationsRECOMMENDATION *STRENGTH OF EVIDENCE
Practice 1.0 Nurses implement minimal tobacco use intervention using theRecommendations "Ask, Advise, Assist, Arrange" protocol with all clients. A
2.0 Nurses introduce intensive smoking cessation intervention (more than10 minutes duration) when their knowledge and time enables them to Aengage in more intensive counselling.
3.0 Nurses recognize that tobacco users may relapse several times before achievingabstinence and need to re-engage clients in the smoking cessation process. B
4.0 Nurses should be knowledgeable about community smoking cessationresources, for referral and follow-up. C
5.0 Nurses implement smoking cessation interventions, paying particular attentionto gender, ethnicity and age-related issues, and tailor strategies to the diverse Cneeds of populations.
6.0 Nurses implement, wherever possible, intensive intervention with womenwho are pregnant and postpartum. A
7.0 Nurses encourage persons who smoke, as well as those who do not, tomake their homes smoke-free, to protect children, families and themselves Afrom exposure to second-hand smoke.
Education 8.0 All nursing programs should include content about tobacco use, associatedRecommendations health risks and smoking cessation interventions as core concepts in C
nursing curricula.
Organization & Policy 9.0 Organizations and Regional Health Authorities should consider smokingRecommendations cessation as integral to nursing practice, and thereby integrate a variety of
professional development opportunities to support nurses in effectivelydeveloping skills in smoking cessation intervention and counselling. B
All corporate hospital orientation programs should include training touse brief smoking cessation interventions as well as information onpharmacotherapy to support hospitalized persons who smoke.
10.0 Nurses seek opportunities to be actively involved in advocating for effectivesmoking cessation services, including "stop smoking medications”. C
11.0 Nurses seek opportunities to be actively involved in advocating for smoke-freespaces and protection against second-hand smoke. C
12.0 Nursing best practice guidelines can be successfully implemented only wherethere are adequate planning, resources, organizational and administrativesupport, as well as appropriate facilitation. Organizations may wish todevelop a plan for implementation that includes:
■ An assessment of organizational readiness and barriers to education. C■ Involvement of all members (whether in a direct or indirect supportive
function) who will contribute to the implementation process.
*See page 16 for details regarding “Interpretation of Evidence”

15
Nursing Best Practice Guideline
Summary of RecommendationsRECOMMENDATION *STRENGTH OF EVIDENCE
■ Dedication of a qualified individual to provide the support needed for theeducation and implementation process.
■ Ongoing opportunities for discussion and education to reinforce theimportance of best practices.
■ Opportunities for reflection on personal and organizational experiencein implementing guidelines. C
In this regard, RNAO (through a panel of nurses, researchers andadministrators) has developed the Toolkit: Implementation of clinical practiceguidelines, based on available evidence, theoretical perspectives andconsensus. The Toolkit is recommended for guiding the implementation ofthe RNAO guideline Integrating Smoking Cessation into Daily Nursing Practice.

Integrating Smoking Cessation into Daily Nursing Practice
16
Interpretation of EvidenceWhen this RNAO guideline was originally published, the material was a synthesis of a number of
source guidelines. At that time, in order to fully inform the reader, every effort was made to maintain
the original level of evidence cited in the source document. No alterations were made to the wording of
the source documents involving recommendations based on randomized controlled trials or research
studies. Where a source document demonstrated an "expert opinion" level of evidence, wording may
have been altered and the notation of RNAO Consensus Panel 2003 added. In the guidelines reviewed,
the panel assigned each recommendation a rating of A, B or C to indicate the strength of the evidence
supporting the recommendation.
Through the revision process, additional literature was reviewed and used to update the
recommendations and discussion of evidence. As these materials were considered, the strength of
evidence were updated to reflect the state of the knowledge in that area. It is important to clarify that
these ratings represent the strength of the supporting evidence to date.
Strength of Evidence
A Requires at least two randomized controlled trials as part of the body of literature of overall quality
and consistency addressing the specific recommendations.
B Requires availability of well conducted clinical studies, but no randomized controlled trials on the
topic of recommendations.
C Requires evidence from expert committee reports or opinions and/or clinical experience of
respected authorities. Indicates absence of directly applicable studies of good quality.
Responsibility for DevelopmentThe Registered Nurses’ Association of Ontario (RNAO), with funding from the Government
of Ontario, has embarked on a multi-year program of nursing best practice guideline development, pilot
implementation, evaluation, dissemination and support of uptake. This guideline was originally developed,
and subsequently revised, by a panel of nurses and researchers convened by the RNAO and conducting its
work independent of any bias or influence from the Government of Ontario.

17
Purpose and ScopeThis best practice guideline is intended to provide direction to nurses during daily practice in all care
settings, both institutional and community. This guideline does not describe in-depth interventions for
special populations such as youths, although the recommendations may also be applied to this group.
This guideline contains recommendations for all Registered Nurses (RNs) and Registered Practical Nurses
(RPNs). It is acknowledged that the individual competency of nurses varies between individuals and across
categories of nursing professionals, and is based on knowledge, skills, attitudes and judgment, enhanced
over time by experience and education.
Best practice guidelines are systematically developed statements to assist nurses and clients in decision making
about appropriate healthcare (Field & Lohr, 1990). This guideline focuses on four areas of smoking cessation:
1. Practice recommendations, directed at the nurse and nursing practice.
2. Education recommendations, directed at competencies required for practice.
3. Organization and policy recommendations, directed at the organizational setting and the environment
to facilitate nursing practice.
4. Evaluation and monitoring criteria.
Although this best practice guideline contains recommendations for Registered Nurses (RNs) and
Registered Practical Nurses (RPNs), it is acknowledged by the development panel that promotion of
smoking cessation is enhanced by the involvement of healthcare providers from a range of disciplines.
Thus, other healthcare providers may also find this guideline useful in their practice.
Rationale for a Smoking Cessation GuidelineGlobally, efforts to reduce tobacco use and exposure to second-hand smoke are gaining momentum. Both
the federal and provincial governments’ efforts to regulate advertising, packaging, restricting minor’s
access by increasing cost of cigarettes through taxation and imposing restrictions on public exposure to
second-hand smoke are good examples. The movement to reduce tobacco use has been furthered by
knowledge of the health effects that tobacco use poses and the recognition that tobacco use is an addiction.
There is also heightened public awareness about the dangers of second-hand smoke through media
campaigns. In Ontario, the Smoke-Free Ontario strategy introduced in May 2006, will improve the health
of Ontarians by preventing children and youth from starting to smoke, helping Ontarians quit smoking and
protecting Ontarians from involuntary exposure to second-hand smoke (Ontario Ministry of Health Promotion,
2006). See Appendix N for further information regarding resources to support smoking cessation.
The most important outcome of this guideline is to motivate and support all nurses to identify the tobacco
use status of their clients and encourage them to intervene with those identified as individuals who smoke
in a sensitive, non-judgmental manner about the importance of cessation.
It is suggested that if a substantial number of healthcare providers implement minimal smoking cessation
interventions, there will be a significant reduction in the number of tobacco users, a decrease in related
tobacco diseases and a lowering of healthcare costs. Tobacco-related diseases cost the Ontario economy at
least $1.7 billion in healthcare annually, result in more than $2.6 billion in productivity losses and account
for at least 500,000 hospital days each year (Ontario Ministry of Health Promotion, 2006).
Nursing Best Practice Guideline
Guiding Principles/Assumptions about Smoking CessationThe guiding principles and assumptions that underlie this nursing best practice guideline related to
smoking cessation are as follows:
1. Regular tobacco use is an addiction that requires support and repeated interventions.
2. The offer of assistance to quit smoking will benefit every person who smokes.
3. The client has the right to accept or refuse smoking cessation intervention.
4. Individuals who smoke deserve to be treated with respect, dignity and sensitivity, while receiving
smoking cessation intervention.
5. The public values and trusts specific advice provided by nurses in the practice of their profession.
6. Nurses are key members of the healthcare team and have a unique, credible and powerful
position within the team.
7. Nurses are involved with clients at multiple entry points to care. This provides many
opportunities to identify persons who smoke and implement smoking cessation interventions.
8. Actively implementing smoking cessation interventions in every care setting will increase
successful quitting.
9. Nurses who currently smoke have a professional responsibility and can effectively provide
smoking cessation intervention.
10. Nursing students have the right to education about evidence-based practice interventions and
strategies for smoking cessation.
11. Nurses have the right to education to enable them to provide the best evidence-based
standard of care.
12. Nurses are ideally positioned to provide a leadership role related to smoking cessation at the
individual, program and/or policy level.
Integrating Smoking Cessation into Daily Nursing Practice
18
19
Original Development Process – 2001/2003In February of 2001, a panel of nurses and researchers with expertise in practice and research related
to smoking cessation, from community and academic settings, was convened under the auspices of the
RNAO. At the onset the panel discussed and came to consensus on the scope of the best practice guideline.
A search of the literature for systematic reviews, clinical practice guidelines, relevant articles and websites
was conducted.
The panel identified a total of 14 clinical practice guidelines related to smoking cessation. An initial
screening was conducted using the following inclusion criteria:
■ Guideline was in English.■ Guideline was dated no earlier than 1996.■ Guideline was strictly about the topic area.■ Guideline was evidence-based (e.g., contained references, description of evidence, sources of evidence).■ Guideline was available and accessible for retrieval.
Eight guidelines were short-listed for critical appraisal using the Appraisal Instrument for Clinical Practice
Guidelines (Cluzeau et al., 1997). This appraisal tool allows for evaluation in three key dimensions.
The panel, following the appraisal process, identified the following guidelines, and related updates, to
adapt and modify in the development of recommendations:
■ Canadian Nurses Association. (1997). Guidelines for registered nurses working with Canadians affected
by tobacco. Ottawa, Ontario: Canadian Nurses Association.
■ Institute for Clinical Systems Improvement. (2000a). Tobacco use prevention and cessation for adults
and mature adolescents. Bloomington, MN: Institute for Clinical Systems Improvement (ICSI)
[On-line]. Available: http://www/icsi.org/guidelst.htm#guidelines*
■ Institute for Clinical Systems Improvement. (2000b). Tobacco use prevention and cessation for infants,
children and adolescents. Bloomington, MN: Institute for Clinical Systems Improvement (ICSI)
[On-line]. Available: http://www/icsi.org/guidelst.htm#guidelines*
■ National Health Committee. (1999a). Guidelines for smoking cessation: Literature review and
background information. New Zealand Guidelines Group [On-line]. Available:
http://www.nzgg.org.nz/library.cfm*
■ National Health Committee. (1999b). Guidelines for smoking cessation: Quit Now. New Zealand
Guidelines Group [On-line]. Available: http://www.nzgg.org.nz/library.cfm*
■ Royal College of Nursing. (1999). Clearing the air: A nurses guide to smoking and tobacco control.
London, England: The Royal College of Nursing.
Nursing Best Practice Guideline

■ University of Toronto Department of Family & Community Medicine. (2000). Smoking cessation
guidelines: How to treat your patient’s tobacco addiction. Toronto, Ontario: Pegasus Healthcare
International.
■ U.S. Department of Health and Human Services, Public Health Service. (2000). Clinical practice
guideline: Treating tobacco use and dependence. Office of the Surgeon General [On-line]. Available:
http://www.surgeongeneral.gov/tobacco/treating_tobacco_use.pdf*
A critique of systematic review articles and pertinent literature was conducted to update the existing
guidelines. Through a process of evidence gathering, synthesis and consensus, a draft set of
recommendations was established. This draft document was submitted to a set of external stakeholders for
review and feedback – an acknowledgment of these reviewers is provided at the front of this document.
Stakeholders represented various healthcare professional groups, clients and families, as well as
professional associations. External stakeholders were provided with specific questions for comment, as
well as the opportunity to give overall feedback and general impressions. The results were compiled and
reviewed by the development panel – discussion and consensus resulted in revisions to the draft document
prior to pilot testing.
A pilot implementation practice setting was identified through a "Request for Proposal" (RFP) process.
Practice settings in Ontario were asked to submit a proposal if they were interested in pilot testing the
recommendations of the guideline. These proposals were then subjected to a review process, from which a
successful practice setting was identified. A nine month pilot implementation was undertaken to test and
evaluate the recommendations. The evaluation took place in a recently amalgamated organization
comprised of four different sites and serving clients with addictions and mental health. An
acknowledgment of this organization is included at the front of this document. The development panel
reconvened after the pilot implementation in order to review the experiences of the pilot site, consider the
evaluation results and review any new literature published since the initial development phase. All these
sources of information were used to update/revise the document prior to publication.
* During the original guideline development process between 2001-2003, these materials were retrieved online at the indicated
web addresses and were current at that time, however, these links may no longer be active.
Revision Process – 2006/2007The Registered Nurses’ Association of Ontario (RNAO) has made a commitment to ensure
that this best practice guideline is based on the best available evidence. In order to meet this commitment,
a monitoring and revision process has been established for each published guideline.
A “current awareness” review has been completed twice each year since the nursing best practice guideline
Integrating Smoking Cessation into Daily Nursing Practice (2003) was originally published. Guideline
development staff reviewed abstracts published in key databases on the topic of smoking cessation,
focusing on systematic reviews, randomized controlled trials and recently published clinical practice
guidelines. The purpose of this review was to identify evidence that would impact on the
recommendations, either further supporting the published recommendations, or indicating that a
Integrating Smoking Cessation into Daily Nursing Practice
20
21
recommendation was no longer appropriate. In the latter case, an “action alert” would be issued, or a full
review would be conducted prior to the three-year schedule. No evidence of this nature was identified
during the ongoing monitoring phase, and this guideline moved into the revision phase as originally scheduled.
In June of 2006, a panel of nurses with expertise in smoking cessation from a range of practice settings
(including institutional, community and academic sectors) was convened by the RNAO. This group was
invited to participate as a review panel to revise the Integrating Smoking Cessation into Daily Nursing
Practice guideline that was originally published in October 2003. This panel was comprised of members of
the original development panel, as well as other recommended specialists.
The panel members were given the mandate to review the guideline, focusing on the currency of the
recommendations and evidence, keeping to the original scope of the document. This work was conducted
as follows:
Planning:■ Clinical questions were identified to structure the literature search.■ Search terms were generated with input from the panel team leader for each recommendation in
the guideline.■ Literature search was conducted by a health sciences librarian. ■ Structured website search was conducted by program staff, focusing on recently published
clinical guidelines.
Critical Appraisal:■ Search results were reviewed by a Research Assistant assigned to the panel. This review included
assessing for inclusion/exclusion related to the clinical questions. See Appendix A for a detailed
description of the search strategy. ■ Studies that met the inclusion/exclusion criteria were retrieved. Quality appraisal and data extraction
was conducted by the Research Assistant. These results were summarized and circulated to the panel.■ Panel members reviewed identified guidelines with the AGREE Instrument (AGREE Collaboration, 2001). See
Appendix A for details of this review.
Panel Review:■ Panel members reviewed the data extraction tables, systematic reviews, and where appropriate,
original studies and clinical guidelines. ■ Recommendations for additional search strategies were identified, if required. ■ Through a process of consensus, recommendations for revision to the guideline were identified.
Nursing Best Practice Guideline

Integrating Smoking Cessation into Daily Nursing Practice
22
Definition of TermsAn additional Glossary of Terms related to clinical aspects of the document is located in Appendix B.
Clinical Practice Guidelines or Best Practice Guidelines: Systematically developed
statements (based on best available evidence) to assist practitioner and client decisions about
appropriate healthcare for specific clinical (practice) circumstances (Field & Lohr, 1990).
Consensus: A process for making policy decisions, not a scientific method for creating new
knowledge. At its best, consensus development merely makes the best use of available information,
be that of scientific data or the collective wisdom of the participants (Black et al., 1999).
Education Recommendations: Statements of educational requirements and educational
approaches/strategies for the introduction, implementation and sustainability of the best
practice guideline.
Evidence: Evidence is information that comes closest to the facts of a matter. The form it takes
depends on context. The findings of high-quality, methodologically appropriate research are the most
accurate evidence. Because research is often incomplete and sometimes contradictory or
unavailable, other kinds of information are necessary supplements to or stand-ins for research. The
evidence base for a decision is the multiple forms of evidence combined to balance rigour with
expedience – while privileging the former over the latter. (Canadian Health Services Research Foundation, 2006).
Meta-Analysis: The use of statistical methods to summarize the results of independent studies,
thus providing more precise estimates of the effects of healthcare than those derived from the
individual studies included in a review (Clarke & Oxman, 1999).
Organization & Policy Recommendations: Statements of conditions required for a
practice setting that enables the successful implementation of the best practice guideline. The
conditions for success are largely the responsibility of the organization, although they may have
implications for policy at a broader government or societal level.
Practice Recommendations: Statements of best practice directed at the practice of
healthcare professionals that are ideally evidence-based.
Randomized Controlled Trial: For the purposes of this guideline, a study in which subjects
are assigned to conditions on the basis of chance, and where at least one of the conditions is a control
or comparison condition.
Stakeholder: A stakeholder is an individual, group or organization with a vested interest in the
decisions and actions of organizations who may attempt to influence decisions and actions (Baker et
al., 1999). Stakeholders include all individuals or groups who will be directly or indirectly affected by
the change or solution to the problem. Stakeholders can be of various types, and can be divided into
opponents, supporters and neutrals (Ontario Public Health Association, 1996).

23
Nursing Best Practice Guideline
Systematic Review: Application of a rigorous scientific approach to the preparation of a review
article (National Health and Medical Research Council, 1998). Systematic reviews establish where
the effects of healthcare are consistent and research results can be applied across populations, settings,
and differences in treatment (e.g., dose); and where effects may vary significantly. The use of explicit,
systematic methods in reviews limits bias (systematic errors) and reduces chance effects, thus providing
more reliable results upon which to draw conclusions and make decisions (Clarke & Oxman, 1999).
Background ContextFacts on Tobacco Use (adapted from several sources; see Appendix C for references)■ Tobacco use is the leading preventable cause of premature death, disease and disability.■ Tobacco use increases the risk of cardiovascular disease, cancers, respiratory diseases, adverse effects
in pregnancy, gastrointestinal problems and tooth and gum problems.■ In 2005, 16 percent of Ontario adults aged 18 years and older were current smokers of cigarettes
(i.e., smoked daily or occasionally in the past month and smoked at least 100 cigarettes in their
lifetime) which is lower than the current national rate of 20% (Ontario Tobacco Research Unit, 2006).
■ More than 47,000 Canadians, aged 35 or older, are estimated to die annually as a direct result of smoking.■ Tobacco kills over 16,000 Ontario residents each year (Ontario Ministry of Health Promotion, 2006).
■ In 2002, the total economic cost of tobacco use in Ontario was almost $6.1 billion (Ontario Tobacco
Research Unit, 2006).
■ Smoking is responsible for about one-third of potential years of life lost due to cancer, about one-quarter
of potential years of life lost due to diseases of the heart and about one-half of potential years of life
lost due to respiratory disease.■ 80 percent of persons who smoke, who have been identified and advised to stop smoking, report that
they want to stop smoking (Brodish, 1998).
■ Cigarettes and other forms of tobacco are addictive. Smoking is both a psychological and a physical
addiction. Nicotine is one of the most highly addictive substances known.■ Second-hand smoke or environmental tobacco smoke is a toxic mixture of chemicals produced during
the burning and smoking of tobacco products.■ There are approximately 4,000 chemical compounds in second-hand smoke. More than 40 of them are
known to cause cancer.■ The average additional annual cost to an employer of employing a person who smokes has been
estimated by the Conference Board of Canada to be $3,396.00 (Conference Board of Canada, 2006).

Benefits of Quitting SmokingQuitting smoking is the single most effective thing that a person who smokes can do to enhance the quality
and length of their life. For some conditions, such as ischemic heart disease, the benefits of quitting
smoking are substantial, both immediately and in the long term. The risks of dying from tobacco-related
diseases are reduced over time, in comparison with those who continue to smoke (Health Canada, 2001). The
risk of smoking related disease continues to decrease as the duration of abstinence increases. (See
Appendix D for a list of health benefits.)
Understanding Tobacco Addiction■ Tobacco contains nicotine, which is a powerful and highly addictive substance. Smoking delivers
nicotine to the brain very rapidly and effectively, bringing on the rapid onset and maintenance of
addiction. The resulting physiological need for tobacco, as well as the accompanying psychological
need, explains the continuing use of tobacco products in spite of all the known health risks.
■ Nicotine dependence consists of both physical and behavioural components. Tobacco use triggers the
release of dopamine – a chemical in the brain that is associated with feelings of pleasure (relief of
withdrawal symptoms). Persons who smoke need greater and greater amounts of nicotine to achieve the
same levels of satisfaction. Further smoking alleviates the withdrawal symptoms that set in as soon as
the effects of nicotine wear off.
■ Smoking cessation is not a single event but a process that involves a change in lifestyle, values, social
circles, thinking and feeling patterns, and coping skills.
■ Most researchers agree that individual users of tobacco differ to the degree to which they are dependent
(Heatherton, Koslowski, Frecker & Fagerstrom, 1991).
■ Historically, addiction to nicotine is one of the hardest substance use dependencies to break.
Pharmacologic and behavioural characteristics that determine tobacco addiction are similar to those that
determine addiction to drugs such as heroin and cocaine (Surgeon General of the United States, 2000).
Integrating Smoking Cessation into Daily Nursing Practice
24

25
How to Help People Stop Smoking■ The most important step in addressing tobacco use and dependence is screening for tobacco use and
offering minimal smoking cessation intervention messages to all persons who smoke, at every
opportunity. When surveyed, over half of Ontarians who currently smoke expressed an intention to
quit smoking within six months of their interview; one quarter indicated a serious intention to quit
within 30 days (Ontario Tobacco Research Unit, 2006).
■ Organization of the clinical environment indicates to the client that the healthcare team will provide
cessation assistance. A powerful message can be delivered to clients, families, the public and staff by
prominently displaying "quit smoking" posters and ensuring cessation materials are visible, accessible
and available.
■ A cueing system for the chart (e.g., labeling each client’s smoking status clearly and visibly with stickers,
stamps or on a flow sheet) prompts healthcare providers to consistently and effectively integrate
smoking cessation into their care.
■ Prochaska and DiClemente’s Stages of Change Model (see Appendix E), recognizes that individuals who
smoke are at different stages of readiness to quit smoking. The use of the model can assist nurses in
smoking cessation intervention by understanding the various stages of willingness to change. Progress
is accomplished when a person who smokes moves onto the next stage or closer to the stage of quitting.
Appendix F shows an example of how to assess and identify a client’s readiness to quit.
■ Provide information and support for the use of pharmacological and non-pharmacological aids for
persons who smoke, who want to quit. The risks of short term nicotine replacement therapy as an aid to
smoking cessation in healthy people are acceptable and substantially outweighed by the risks of
cigarette smoking (Surgeon General of the United States, 2000).
Nursing Best Practice Guideline

Integrating Smoking Cessation into Daily Nursing Practice
26
Practice Recommendations
Recommendation 1.0Nurses implement minimal tobacco use intervention using the “Ask, Advise, Assist, Arrange”
protocol with all clients. (Strength of Evidence =A)
Minimal Smoking Cessation Intervention (Lasting 1 to 3 minutes)Every nurse will:
ASK: About tobacco use with all clients (e.g., “have you used any form of tobacco in the
past six months?”) and assess readiness to quit. If time allows, assess the person’s
level of motivation to change behavior, using motivational interviewing
techniques (see Appendix G).■ Document tobacco use status (e.g. non-smoker, smoker, ex-smoker).
ADVISE: Every tobacco user of the importance of quitting in a non-judgmental and
unambiguous manner.
ASSIST: By providing minimal intervention:■ Refer to the Canadian Cancer Society’s Smokers’ Helpline 1-877-513-5333 or
www.smokershelpline.ca.■ Offer support and self-help resources, such as booklets (See Appendix N for a
listof resources).■ Inform about, or refer to a community stop smoking clinic or service. ■ Refer to other healthcare provider.
ARRANGE: Follow-up or referral.
For a flow chart of the Ask, Advise, Assist and Arrange protocol for minimal intervention, see Appendix H.
Discussion of EvidenceIt is essential to provide at least a minimal intervention (1 – 3 minute duration) to all tobacco users at every
appropriate occasion. There is good evidence that even brief advice from health professionals has a
significant effect on smoking cessation rates (National Health Committee, 2002). Brief advice from a health
professional decreases the proportion of people smoking by about 2 percent per year (NHS Centre for Reviews
and Dissemination – The University of York, 1998). The literature suggests that minimal intervention may encourage
a committed person who smokes to think about their smoking and to start to look at the disadvantages as
well as the benefits. It has also been stated that for clients not ready to quit at this time, providing self-help
material will increase their awareness and motivation to quit (U.S. Dept. of Health and Human Services, 2000).
All nurses have opportunities to assist clients to stop smoking through brief counselling and minimal
interventions. The results indicate, with reasonable evidence, that minimal interventions can be effective
as the nurses provide clients with information about the potential benefits of smoking cessation and
counselling (Rice & Stead, 2003).
A study conducted by the University of Ulster (2001), showed that nurses constitute 65 percent of the
healthcare workforce and are well placed to share the health promotion message with a large proportion of

27
Nursing Best Practice Guideline
the population. Healthcare personnel should treat inquiries about tobacco use and smoking cessation as a
standard assessment question at every visit, recording current use, history and amount (Fiore et al., 2000; Fiore,
Jorenby, & Baker, 1997).
Recommendation 2.0Nurses introduce intensive smoking cessation intervention (more than 10 minutes duration) when
their knowledge and time enables them to engage in more intensive counselling.
(Strength of Evidence =A)
Intensive Smoking Cessation Intervention (Lasting more than 10 minutes)Every nurse will:
ASK: About tobacco use with all clients (e.g., “have you used any form of tobacco in the
past six months?”) and assess readiness to quit. If time allows, assess person’s level
of motivation to change behaviour, using motivational interviewing techniques
(see Appendix G).■ Document tobacco use status (e.g. non-smoker, smoker, ex-smoker).
ADVISE: Every tobacco user of the importance of quitting in a non-judgmental and
unambiguous manner.
ASSIST: By providing intensive intervention:■ Determine and discuss the stage of change (Appendix E);■ Reasons for smoking (WHY Test) (Appendix I);■ Nicotine Dependence (Fagerstrom Test) (Appendix J);■ Discuss strategies to quit and treatment options■ Offer information re: pharmacotherapy options (see Discussion of Evidence);■ Set a quit date;■ Review quitting history, past quit attempts and discuss these experiences; ■ Review potential challenges and triggers (Appendix M); and■ Encourage support of family and friends.
ARRANGE: Follow-up or referral.■ Schedule follow-up or refer to a community stop smoking clinic or service
For a flow chart of the Ask, Advise, Assist and Arrange protocol for intensive intervention, see Appendix H.
Discussion of EvidenceMotivation is the key to giving up smoking (Royal College of Nursing, 1999). It was found that increasing the
intensity of advice (time spent giving advice and duration of follow up) improves effectiveness, decreasing
the proportion of persons who smoke by approximately 3 to 5 percent (U.S. Dept. of Health and Human Services,
2000). Counselling interventions could include areas such as smoking history, motivation to quit,
identification of high risk situations and help with problem solving strategies to deal with high risk
situations (Lancaster & Stead, 2003a). The more components added to the intervention, the more intensive the
intervention (Rice, 1999). Individual counselling increases the likelihood of cessation compared to less
intensive support (Lancaster & Stead, 2003b).

Intensive intervention is appropriate for all persons who smoke and are willing to participate and is
especially recommended to be offered to “special populations” (pregnant women, cardiovascular clients,
clients with other chemical dependencies or psychiatric disorders and various health issues) of persons
who smoke.
Proactive telephone counselling, group counselling and individual counselling formats are effective and
should be used in smoking cessation interventions (U.S. Dept. of Health and Human Services, 2000). Research
shows that telephone counselling can significantly improve quit rates in young adults and older adults
wanting to quit (Rabius et al, 2004). All Canadian provinces have telephone quitlines for persons who smoke.
For a list of telephone resources, see Appendix N.
Proactive counselling helps persons who smoke to quit. In a review conducted by Stead, Lancaster and Perera
(2003), it was found that a call from a counsellor is likely to increase the chances of quitting by approximately
50 percent and certainly by 2 to 4 percentage points, compared to a minimal intervention such as providing
standard self-help materials. Smoking cessation interventions that are delivered in multiple formats increase
abstinence rates and should be encouraged (U.S. Dept. of Health and Human Services, 2000).
In a systematic review conducted by Rigotti, Munafo, Murphy and Stead (2003), it was found that smoking
cessation interventions delivered during a period of hospitalization, with follow-up support after
discharge, increased smoking cessation. However, there was no clear evidence that clients with different
clinical diagnoses responded in different ways.
Pharmacotherapy OptionsBefore recommending over-the-counter (OTC) drugs, nurses must have knowledge, skill and judgment
about the client’s situation, their condition and medication profile and the medication (College of Nurses of
Ontario, 2003). Pharmacological therapy should be recommended to all clients except in the presence of
special circumstances or in cases of contraindications (Orsetti, Dwyer, Sheldon, Thomas & Harrison, 2001). In
special circumstances or in cases of contraindications, nurses must work in collaboration with the client’s
physician to determine the appropriate treatment for the client.
It is found that pharmacological options approximately double the long term abstinence rates over those
produced by placebo interventions (U.S. Dept. of Health and Human Services, 2000; University of Toronto, 2000). As part
of tobacco-dependence treatment, nicotine replacement therapy (NRT) and bupropion hydrochloride
should be considered first as they have been proven to significantly improve cessation rates. Nicotine is
highly addictive and by using NRT or Zyban® instead of smoking, thousands of other chemicals associated
with tobacco smoke are no longer being inhaled (University of Toronto, 2000). The therapy used must depend
on such factors as ease of administration, cost, compliance and particular vulnerabilities to side effects
(National Health Committee, 1999a). Client preference, previous experience and contraindications should also
be considered in recommending which pharmacological option to pursue.
The following first-line medications have been documented to significantly increase the rate of long-term
smoking abstinence, and each has been approved as safe and efficacious by the U.S. Food and Drug
Administration (Anderson, Jorenby, Scott & Fiore, 2002).
Integrating Smoking Cessation into Daily Nursing Practice
28

29
A) Nicotine Replacement Therapy (NRT) NRT is the most commonly used pharmacological treatment for smoking cessation, which provides a
“clean” alternative source of nicotine that the person who smokes would have otherwise received from
tobacco. The aim of NRT is to partially replace the nicotine otherwise obtained from cigarettes. This may
reduce the incidence and intensity of withdrawal symptoms induced by nicotine abstinence during the
first few weeks of smoking cessation (Ontario Tobacco Research Unit, 2000b). It should be noted that oral nicotine
replacement products reduce the effects of irritability, anxiety and overall withdrawal discomfort (West &
Shiffman, 2001). The advantage of using NRT is that it supplies nicotine in a safe manner without the harmful
constituents contained in tobacco smoke (National Health Committee, 1999a). Systematic reviews show that all
forms of NRT increase quit rates at 12 months, approximately 1.5 to 2 fold compared with placebo,
regardless of the setting (National Health Committee, 2002).
Perhaps the most useful approach to pharmacotherapies is to recognize that non-pharmacological
interventions (counselling and other supports) remain vital contributors to successful smoking cessation;
they should not be considered inferior to drug treatment. In fact, a robust evidence base exists supporting
the combination of non-pharmacological and pharmacological interventions to aid in smoking cessation
(Coleman, 2004).
Types of NRT:1. Nicotine patch (e.g., Habitrol®, Nicoderm®)■ Can be purchased over the counter (no prescription needed).■ Is available in three strengths (7 mg, 14 mg, and 21 mg,).■ Provides a rate-controlled delivery of nicotine that is absorbed through the skin.■ Is applied to non-hairy, clean, dry site above waist and held in place for 10 seconds to secure. The
placement site must be changed with each application.■ Usual schedule –21 mg x 4 wks, 14 mg x 4 wk, 7 mg x 2 wks (start with strength matching to
nicotine dependence).■ Has a slow onset and contains lower levels of nicotine than cigarettes and higher levels than gum.■ May cause sleep disturbance (if these become serious, patch should be removed once in bed and
immediately reapplied in the morning).
2. Nicotine gum (e.g., Nicorette®, Nicorette® Plus)■ Can be purchased over the counter (no prescription needed).■ Substitutes a piece of gum for the craving for a cigarette, providing gratification for oral needs and
nicotine cravings. ■ Is absorbed by buccal mucosa.■ Is not chewed continuously, rather, chewed 2-3 times, then parked between the cheek and the gum.
“Bite, bite and park” between cheek and gums – wait a minute then repeat over 30 mins or less.■ 1 - 2 pieces per hour, or with urge, up to 20 pieces day, gradually reduced over 4-12 weeks. ■ 25 cigs or more/day = 4 mg gum. (Nicorette® Plus) <25 cigs/day = 2 mg gum (Nicorette®). ■ Absorption diminished by concomitant use with coffee, tea, alcohol, juice and soft drinks.
Nursing Best Practice Guideline
There is evidence that combining the nicotine patch with nicotine gum increases long-term abstinence
rates over those produced by a single form of NRT (Centres for Disease Control and Prevention, 1999). Bupropion
hydrochloride can be used in combination with nicotine replacement therapies (U.S. Department of Health and
Human Services, Public Health Service, 2000).
3. Nicotine inhaler (e.g. Nicorette® inhaler)■ Can be purchased over the counter (no prescription needed). ■ Is a mouthpiece with a nicotine cartridge insert. A 10 mg inhaler cartridge delivers 4 mg nicotine vapor
with 2 mg absorbed. One puff delivers less nicotine than one puff from a cigarette. ■ Addresses both the physical and behavioural dependency of smoking as it mimics the hand-to-mouth
ritual of smoking. ■ ‘Puff (into mouth) and hold’. Nicotine is absorbed by blood vessels in the buccal cavity. The number of
puffs taken depends on the amount of nicotine required to meet individual’s cravings and dependence
(most users require > 2 puffs at a time). The same cartridge may be used to address the next craving.
Once opened, each cartridge should be changed every 2-4 hours, as the unused nicotine will evaporate. ■ Manufacturer recommends starting dose of 6 - 12 cartridges per day but many need significantly less.
Taper amount over 3 months (max. 6 months).■ Acidic foods or drinks interfere with absorption. Do not eat or drink (except water) for 15 minutes prior.
4. Options such as nicotine nasal spray, sublingual tablets and lozenges are not currently available in
Canada, but have been tested in placebo controlled trials, demonstrated to be effective and recommended
as first-line pharmacotherapies in the United States (University of Toronto, 2000).
B) Bupropion Hydrochloride (Zyban®)Bupropion hydrochloride is also marketed as the anti-depressant medication Wellbutrin®. It is a non-
nicotine medication and requires a prescription. The exact mechanism by which bupropion hydrochloride
works is unknown, but it is presumed to alleviate cravings associated with nicotine withdrawal affecting
noradrenaline and dopamine, two chemicals in the brain that may be key components of the nicotine
addiction pathway (National Health Committee, 1999a).
C) Other Options:Varenicline tartate will be available in Canada in 2007, and was approved by the U.S. Food and Drug
Administration in May 2006. Studies have shown Varenicline to increase the odds of quitting by four times
compared to placebo, and double compared to Zyban® at 12 weeks and at 1 year. Varenicline targets nicotinic
acetylcholine receptors to decrease craving, withdrawal and the reinforcement associated with smoking
cigarettes. Studies have found varenicline to be safe and well tolerated, with the most common adverse
effects reported being nausea and sleep disturbances (Gonzales et al., 2006; Jorenby et al., 2006; Tonstad et al., 2006).
Clonidine and Nortriptyline are second-line prescription medications used in smoking cessation. These
are pharmacotherapies for which there is evidence of efficacy for treating tobacco dependence, but which
have a more limited role than first-line medications.
For a comparison and explanation of the medications used in smoking cessation treatment, see Appendix L.
Integrating Smoking Cessation into Daily Nursing Practice
30

31
Non-Pharmacological InterventionsThere are numerous options to assist a person who smokes, who is planning to stop smoking:
■ Self-help books and materials;■ Individual counselling (e.g., physicians, nurses/nurse practitioners, pharmacists, dentists);■ Group programs; and■ Mutual aid and self-help group support.
While acupuncture and hypnotherapy are popular, there is insufficient evidence to support their
effectiveness (Joanna Briggs Institute, 2001). However, if the individual has faith in acupuncture or
hypnotherapy, they may benefit from the counselling that these approaches offer (U.S. Dept. of Health and
Human Services, 2000; University of Toronto, 2000). Other potential quit methods that haven’t been clinically
proven include herbal supplements, herbal patches and laser therapy.
Recommendation 3.0Nurses recognize that tobacco users may relapse several times before achieving abstinence and
need to re-engage clients in the smoking cessation process.
(Strength of Evidence = B)
Discussion of EvidenceNicotine dependence is increasingly being recognized as a chronic, relapsing condition similar to that of
other addictive substances.
Most relapse occurs within the first three months after quitting. Because of the chronic, relapsing nature of
tobacco dependence, relapse prevention is especially important during this period. Strategies designed to
prevent relapse should be included in the initial preparation for a quit attempt. It is important to encourage
clients to report difficulties (lapses, depression, side effects) promptly while continuing their efforts to quit
(U.S. Dept. of Health and Human Services, 2000). A variety of interventions targeting relapse prevention exist. In one
significant review, researchers conclude that there is insufficient evidence to recommend particular
interventions for relapse prevention; rather, they recommend continued focus on primary cessation
attempts as well as the identification and resolution of tempting or high-risk situations (Hajek et al., 2006).
Relapse is perfectly normal and does not mean that a person who smokes has failed. Researchers have
found that the more past attempts to stop smoking a person has made, the more likely they will be to
successfully stop in the future. All experiences learned in previous attempts are useful and can be built on
for a future successful attempt (Royal College of Nurses, 1999). Even after withdrawal symptoms pass, the risk
of relapse continues to be high, largely due to exposure to temptations, social situations and other
smoking triggers. All attempts to quit should be congratulated. Never condemn the person who smokes
for lapsing. Encourage the person who smokes to take time to plan for their next stop smoke attempt and
to use the information learned from the last one (University of Toronto, 2000). For Strategies to Avoid Relapse,
see Appendix M.
Nursing Best Practice Guideline

Integrating Smoking Cessation into Daily Nursing Practice
32
Recommendation 4.0Nurses should be knowledgeable about community smoking cessation resources, for referral and
follow-up. (Strength of Evidence = C – RNAO Consensus Panel, 2003/2007)
Discussion of EvidenceThere is evidence that self-help materials alone are of some benefit. A Cochrane review by Lancaster and
Stead (2003b) did not find evidence that self-help materials produce incremental benefits over other
minimal interventions, such as advice from a healthcare professional or nicotine replacement therapy.
However, they found there is increasing evidence that materials that are individually tailored to the person
who smokes have an effect. Tailoring materials to the characteristics of an individual who smokes and
adding follow-up telephone calls improves effectiveness (National Health Committee, 1999a).
The following are examples of community resources (for a complete listing, see Appendix N):■ The Canadian Cancer Society Smokers’ Helpline number is 1-877-513-5333.■ Local smoking cessation programs (inquire via local Public Health Unit).■ Employee Assistance Programs, accessible through an individual’s employer.■ Physicians and other healthcare providers.
Recommendation 5.0Nurses implement smoking cessation interventions, paying particular attention to gender,
ethnicity and age-related issues, and tailor strategies to the diverse needs of populations.
(Strength of Evidence = C – RNAO Consensus Panel, 2003/2007)
Discussion of EvidenceThere is substantial evidence in the literature citing the long-term benefits of “targeting” smoking cessation
interventions at different populations (e.g., youth, women, older adults, ethnic groups). The Royal College
of Nursing (1999), states that nurses are in a unique position, and have access to the population at all levels,
citing several examples of successful implementation of smoking cessation programs with different target
groups. The RNAO guideline development panel supports this concept of tailoring strategies where
possible, during the implementation of minimal intervention.
In 2005, males aged 25-29 had the highest prevalence of current smoking at 39 percent, almost double that
of their female counterpart (21 percent) (Ontario Tobacco Research Unit, 2006). More research is needed to
determine the most effective quit methods as many young adults do not consider themselves ‘smokers’
because they don’t smoke every day or they only smoke in certain situations. Please see Appendix N for
resources which may be of use to nurses working with this population.
Additional research is also needed in the area of co-morbidity and smoking. Eighty percent of alcohol dependent
people currently smoke and concurrent cannabis use is becoming increasingly relevant to smoking cessation as
it has been linked to depression, suicidal ideation and difficulty of tobacco cessation (Wilhelm, et al. 2006). These
populations require the nurse’s special attention and consultation with other mental health practitioners to
establish a smoking cessation care plan, especially with the use of nicotine replacement therapies.

33
Recommendation 6.0Nurses implement, wherever possible, intensive intervention with women who are pregnant
and postpartum. (Strength of Evidence = A)
Discussion of EvidenceIn 2005, 10 percent of mothers in Ontario (aged 20-44) who gave birth in the past five years had smoked
during their most recent pregnancy, with 5 percent having smoked daily and 5 percent having smoked
occasionally (Ontario Tobacco Research Unit, 2006).
Pregnancy, and the period preceding and following, provides a unique opportunity to help women stop
smoking. Many women are motivated to quit smoking during pregnancy and healthcare professionals can
take advantage of this motivation by reinforcing the knowledge that cessation will reduce health risks to the
fetus and that there are postpartum benefits to both the mother and the child. Women who stop smoking
before or during the first trimester of pregnancy reduce risks to their baby to a level comparable to that of
women who have never smoked (National Health Committee, 2002). Self-help manuals, particularly material
specifically directed to pregnancy, are more effective in this population than in other groups (National Health
Committee, 1999a).
Smoking during pregnancy has harmful effects for both the woman and the fetus. Approaches to smoking
cessation for pregnant women often focus on the health of the fetus and give less attention to the woman’s own
health. Greaves et al., (2003) emphasize a woman-centred approach, focusing on the health of the woman in
addition to the health of the fetus, thus encouraging a sustained abstinence in the postpartum period.
Stopping smoking during pregnancy may be treated as a suspension of the habit and is not always a change
that is intentional or permanent or made for personal benefit. The research on process of change for
smoking cessation suggests that pregnant women may experience the stages of quitting in a unique way,
moving through the pre-contemplation and contemplation stages into preparation and action stages very
quickly (Prochaska et al. 1983; 2001) which may be detrimental to smoking cessation and maintenance,
resulting in postpartum relapse. Another study found that some women reported that they had never really
quit because they quit for the fetus/baby and not for themselves (Bottoroff et al., 2000).
There are many helpful resource agencies, websites and help lines that the consumer can access to increase
their knowledge base about smoking cessation. Information for accessing these resources, like the Ontario
program PREGNETS which provides information for pregnant women who intend to quit smoking, are
listed in Appendix N. However, programs are still needed to raise awareness and motivate behavioural
change among pregnant women and their partners, to reduce the harmful effects of prenatal and postnatal
exposure to tobacco smoke (Ontario Tobacco Research Unit, 2000b).
According to the National Health Committee (2002), “NRT should be considered when a pregnant/lactating
woman is unable to quit, and when the likelihood of quitting, with its potential benefits, outweighs the risks
of NRT and potential continued smoking” (p. 22). A nurse can then recommend NRT to the client and suggest
that the pregnant woman discuss this option with the healthcare provider who is monitoring her pregnancy.
Nursing Best Practice Guideline

Integrating Smoking Cessation into Daily Nursing Practice
34
Recommendation 7.0Nurses encourage persons who smoke, as well as those who do not, to make their homes smoke-free,
to protect children, families and themselves from exposure to second-hand smoke.
(Strength of Evidence = A)
Discussion of EvidenceAll involuntary exposure to tobacco smoke is harmful and should be eliminated (Ontario Tobacco Research Unit,
2000a). The scientific evidence indicates that there is no risk-free level of exposure to second-hand smoke.
Second-hand smoke causes premature death and disease in children and in adults who do not smoke.
Children who are exposed to second-hand smoke are at an increased risk for Sudden Infant Death
Syndrome (SIDS), acute respiratory infections, ear problems, and more severe asthma. Smoking by parents
causes respiratory symptoms and slows lung growth in their children. Exposure of non-smoking women to
environmental tobacco smoke during pregnancy also causes reductions in fetal growth (Ontario Tobacco
Research Unit, 2000a). Children do not choose this exposure. Their right to grow up in an environment free
from tobacco smoke must be safeguarded through actions by national and local governments, voluntary
bodies, community leaders, health workers, educators and parents (Ontario Tobacco Research Unit, 2000a).
Exposure of adults to second-hand smoke has immediate adverse effects on the cardiovascular system and
causes coronary heart disease and lung cancer (U.S. Department of Health and Human Services, 2006). In 2005,
more than 600,000 Ontarians (7.3 percent) 12 years and older were exposed every day or almost every day
to second-hand smoke at home (Ontario Tobacco Research Unit, 2006). A short-term objective of the Smoke-free
Ontario Strategy is to increase the adoption of voluntary policies to make homes smoke-free (Ontario Tobacco
Research Unit, 2006).
Education RecommendationsEducation is the foundation of the success of all activities in smoking cessation. Education must be
continually reinforced, and the best methods for educating must be chosen, in order to ensure practice
change in the adoption of the best practice guidelines. The literature demonstrates that initiating and
maintaining behavioural change is a complex process that requires the implementation of intensive and
sustained efforts using strategies that influence a number of factors.
Recommendation 8.0All nursing programs should include content about tobacco use, associated health risks and
smoking cessation interventions as core concepts in nursing curricula.
(Strength of Evidence = C – RNAO Consensus Panel, 2003/2007)
Discussion of EvidenceSeveral sources, including the U.S. Department of Health and Human Services (2000), widely support the
inclusion of education and training in tobacco dependence treatments in the required curricula of all
clinical disciplines. The RNAO guideline development panel also supports this need for educational
programs at all levels of nursing.

35
Nurses require education and guidance so they can develop their understanding and a positive view as to
the effectiveness of smoking cessation programs (Lawvere, 2003). Nurses described concern about their
ability to motivate their clients. Education about the health risks of tobacco, assessing clients’ nicotine
dependency and motivation to cease smoking is necessary to include in nursing curricula (Pelkonen, 2001).
Organization & Policy RecommendationsRecommendation 9.0Organizations and Regional Health Authorities should consider smoking cessation as integral to
nursing practice, and thereby integrate a variety of professional development opportunities to
support nurses in effectively developing skills in smoking cessation intervention and counselling.
All corporate hospital orientation programs should include training to use brief smoking cessation
interventions as well as information on pharmacotherapy to support hospitalized persons who smoke.
(Strength of Evidence =B)
Discussion of EvidenceEducational development in the area of smoking cessation, for nurses in all specializations and practice
settings, is needed to provide additional background knowledge and expertise in the practice of smoking
cessation interventions. In particular, there is a need to educate nurses concerning the mechanisms
underlying the additive nature of tobacco use (Schultz, Bottorff & Johnson, 2005); tobacco use is not a habit or
choice. Increased awareness and knowledge would assist nurses in adequately treating withdrawal
symptoms, which is necessary to support abstinence from tobacco use and eventual successful cessation.
As well, organizations must provide professional development opportunities for nurses that are tailored to
individual and group learning styles. Health professionals who receive training are much more likely to
intervene with people who smoke than those who are not trained (University of Toronto, 2000).
To promote providers addressing tobacco cessation, organizations need to systemically approach tobacco
cessation through education, resources, cues embedded in patient care documents, and feedback to providers.
The healthcare system should ensure the following:
1. Nurses have sufficient training to treat tobacco dependence. For example, in Ontario, the Centre for
Addiction and Mental Health launched a workshop Training Enhancement in Applied Cessation
Counselling and Health (TEACH) that trains practitioners in the area of tobacco cessation.
2. Healthcare providers and clients have cessation resources; for example, access to patient resources that
address stopping smoking (which includes addressing relapse and community supports available to
address the process of stopping); protecting their environment from tobacco smoke exposure; options
to refer for future cessation support.
3. Environmental prompts promote the integration of cessation support being offered by health providers
(U.S. Dept. of Health and Human Services, 2000). For example, patient history forms, patient care forms, referral
forms, and discharge forms should include cues regarding tobacco use status and cessation support.
Currently, many of these components of health records document tobacco use while indications of
cessation support are absent (Schultz et al., 2006).
Nursing Best Practice Guideline

4. Healthcare providers are given feedback about their tobacco dependence treatment practices (U.S.
Dept. of Health and Human Services, 2000) and are referred to self-help resources specifically tailored
for nurses and students who wish to stop smoking (i.e. Nurses Quit Net available on-line at
www.tobaccofreenurses.org).
For a list of training and self help resources available to nurses, please see Appendix N.
Recommendation 10.0Nurses seek opportunities to be actively involved in advocating for effective smoking cessation
services, including “stop smoking medications”.
(Strength of Evidence = C – RNAO Consensus Panel, 2003/2007)
Discussion of EvidenceSuggested advocacy roles for nurses can include:■ Lobbying governments and third-party payers for funding to support the provision of smoking cessation
services by health professionals.
■ Advocating for the provincial government to have the Ontario Drug Benefit Plan (ODB) cover the cost of
all nicotine replacement products and other smoking cessation related pharmaceuticals. At present,
nicotine replacement products are not covered by most insurance plans.
■ Advocating for employer sponsors, (for example, health insurance companies) to cover the cost of all
nicotine replacement products and other smoking cessation related pharmaceuticals. In the longer
term, the health consequences of tobacco use may prove more costly to the insurance industry than
covering the cost of NRT products and other pharmaceuticals.
Recommendation 11.0Nurses seek opportunities to be actively involved in advocating for smoke-free spaces and protection
against second-hand smoke. (Strength of Evidence = C – RNAO Consensus Panel, 2003/2007)
Discussion of EvidenceSmoke-free workplaces are associated with a decrease in prevalence of tobacco consumption of nearly four
percent (Fichtenberg & Glantz, 2002; Moher et al., 2003; Smedlsund et al., 2004). Smoke-free workplaces also make it easier
for persons who smoke to reduce or stop smoking, and substantially reduce tobacco industry sales (Fichtenberg &
Glantz, 2002). Most adults spend about a third of their day in a workplace environment, therefore the workplace
is a setting through which large groups of people who smoke can potentially be reached by smoking cessation
messages. The workplace has the potential for a higher participation than non-workplace environments and
may encourage sustained peer group support and positive peer pressure (Moher, 2004).
On June 27, 2006 the U.S. Surgeon General released a report on involuntary exposure to second-hand
smoke, concluding that secondhand smoke causes disease and death in children and non-smoking adults.
The report finds a causal relationship between second-hand smoke exposure and Sudden Infant Death
Syndrome (SIDS), and declares that the home is becoming the predominant location for exposure of
children and adults to second-hand smoke.
Integrating Smoking Cessation into Daily Nursing Practice
36

37
Eliminating smoking in indoor spaces fully protects those who do not smoke from exposure to second-hand
smoke. Separating persons who smoke from those who do not, cleaning the air, and ventilating buildings
alone cannot eliminate exposures of nonsmokers to second-hand smoke (U.S. Department of Health and Human
Services, 2006).
Nurses can help by:■ Promoting smoke-free environments, such as smoke-free initiatives on hospital grounds. Nurses can
provide smoke-free task force leaders with valuable information and strategies to support patients,
families, public and staff during implementation.
■ Advocating for smoke-free outdoor recreation areas, and encouraging nurses to set an example by being
smoke-free.
■ Supporting and educating the public regarding the Ontario legislation that shields workers and the public
from the harmful effects of tobacco by banning smoking in enclosed public places and enclosed workplaces.
Recommendation 12.0Nursing best practice guidelines can be successfully implemented only when there is adequate
planning, resources, organizational and administrative support, as well as appropriate facilitation.
Organizations may wish to develop a plan for implementation that includes:■ An assessment of organizational readiness and barriers to education.■ Involvement of all members (whether in a direct or indirect supportive function) who will
contribute to the implementation process.■ Dedication of a qualified individual to provide the support needed for the education and
implementation process.■ Ongoing opportunities for discussion and education to reinforce the importance of best practices.■ Opportunities for reflection on personal and organizational experience in implementing guidelines.
In this regard, RNAO (through a panel of nurses, researchers and administrators) has developed the
“Toolkit: Implementation of clinical practice guidelines” based on available evidence, theoretical
perspectives and consensus. The Toolkit is recommended for guiding the implementation of the
RNAO guideline Integrating Smoking Cessation into Daily Nursing Practice.
Strength of Evidence = C
A critical step in the implementation of guidelines must be the formal adoption of the guidelines.
Organizations need to consider how to formally incorporate the recommendations to be adopted into their
policy and procedure structure (Graham et al., 2002). This initial step paves the way for general acceptance
and integration of the guideline into such systems as the quality management process.
New initiatives such as the implementation of a best practice guideline require strong leadership from
nurses who are able to transform the evidence-based recommendations into useful tools that will assist in
directing practice. Refer to Appendix O for a description of the Toolkit.
Nursing Best Practice Guideline

Integrating Smoking Cessation into Daily Nursing Practice
38
Evaluation & MonitoringResearch on smoking and tobacco use has begun to focus not just on outcomes, e.g., quitting, reduction,
and cessation, but on stages of smoking behaviour, based on stages of change. Understanding the cycle is important
for developing and implementing interventions directed specifically to the individual’s current stage of change.
Minimal intervention has been shown to decrease the proportion of persons who smoke by around 2 percent.
Organizations implementing the recommendations in this nursing best practice guideline are advised to consider how
the implementation and its impact will be monitored and evaluated. The following table, based on the framework
outlined in the RNAO Toolkit: Implementation of clinical practice guidelines (2002), illustrates some suggested
indicators for monitoring and evaluation.
Objectives
Organization/Unit
Provider
■ To evaluate the supportsavailable in theorganization that allow fornurses to implementminimal and intensivesmoking cessationinterventions.
■ Review of best practicerecommendations byorganizational committee(s)responsible for policies orprocedures, e.g., list ofreferral sources for smokingcessation.
■ Availability of clienteducation resources that areconsistent with the guidelinerecommendations.
■ Organizational missionstatement that supports asmoke-free environment.
■ Percentage of nurses andother healthcareprofessionals attendingeducation sessions onsmoking cessation.
■ To evaluate changes inpractice that lead towardsintegration of minimal andintensive smokingcessation interventionsinto daily nursing practice.
■ Documentation systemsavailable for recordingsmoking status and relatedstrategies.
■ Nurses’ self-assessedknowledge of theimportance of:■ Assessing and
implementing minimalor intensive smokingcessation interventionsusing the Ask, Advise,Assist and Arrangeprotocol.
■ Documenting thesmoking cessationinterventions providedto clients.
■ Understanding thevarious stages ofreadiness to quitsmoking.
■ To evaluate the impactof implementing therecommendations.
■ Smoke-free environment.■ Incorporation of smoking
cessation intervention educationin staff orientation program.
■ Incorporation of smokingcessation intervention in clientinformation material.
■ Organizational policy reflectingcommitment for a smoke-freeenvironment and support forsmoking cessation.
■ Number of institutions wheresmoking cessation is measured asa quality indicator.
■ Percentage of persons who smokeindicating they were advised toquit smoking by one or morenurses and/or other healthcareprofessionals during their mostrecent contact as indicated inchart audits.
■ Percentage of nurses and/or otherhealthcare professionals referringclients for follow-up to communitysmoking cessation programs.
■ Percentage of clients admittedto unit/facility with theirsmoking status and smokinghistory recorded.
■ Percentage of clients withdocumented interventionscharted.
Indicator Structure Process Outcome
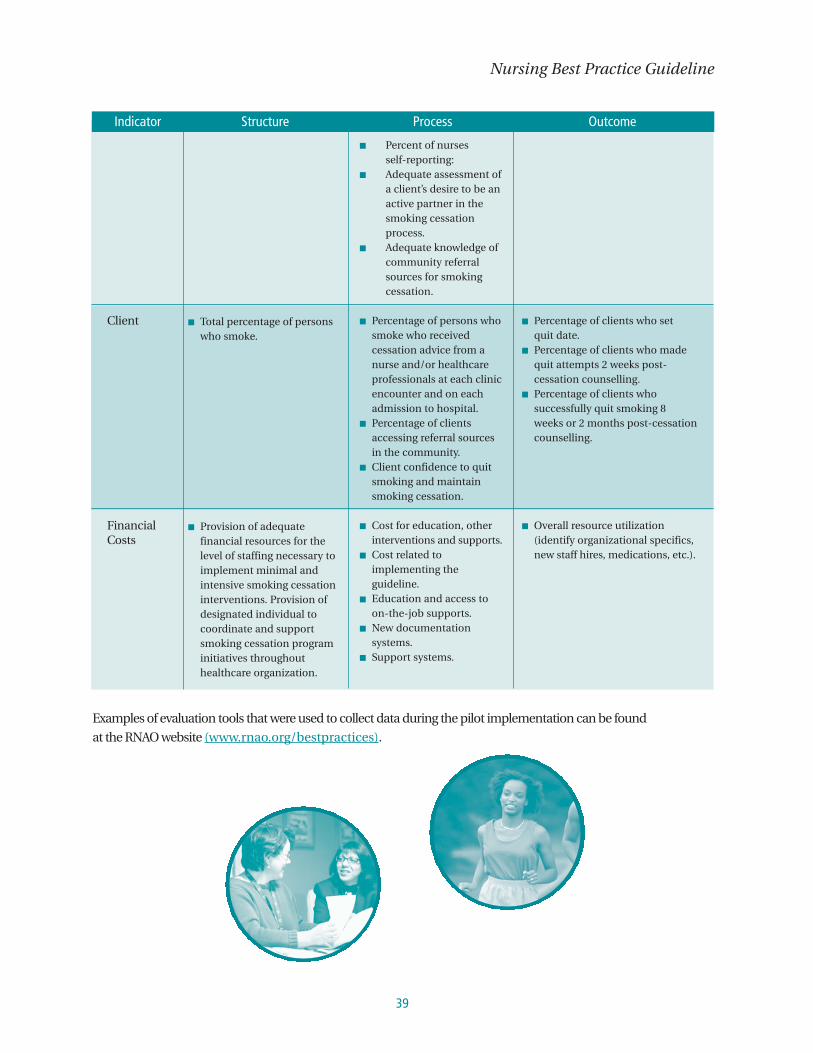
39
Nursing Best Practice Guideline
Client
FinancialCosts
■ Total percentage of personswho smoke.
■ Provision of adequatefinancial resources for thelevel of staffing necessary toimplement minimal andintensive smoking cessationinterventions. Provision ofdesignated individual tocoordinate and supportsmoking cessation programinitiatives throughouthealthcare organization.
■ Percent of nursesself-reporting:
■ Adequate assessment ofa client’s desire to be anactive partner in thesmoking cessationprocess.
■ Adequate knowledge ofcommunity referralsources for smokingcessation.
■ Percentage of persons whosmoke who receivedcessation advice from anurse and/or healthcareprofessionals at each clinicencounter and on eachadmission to hospital.
■ Percentage of clientsaccessing referral sourcesin the community.
■ Client confidence to quitsmoking and maintainsmoking cessation.
■ Cost for education, otherinterventions and supports.
■ Cost related toimplementing theguideline.
■ Education and access toon-the-job supports.
■ New documentationsystems.
■ Support systems.
■ Percentage of clients who setquit date.
■ Percentage of clients who madequit attempts 2 weeks post-cessation counselling.
■ Percentage of clients whosuccessfully quit smoking 8weeks or 2 months post-cessationcounselling.
■ Overall resource utilization(identify organizational specifics,new staff hires, medications, etc.).
Indicator Structure Process Outcome
Examples of evaluation tools that were used to collect data during the pilot implementation can be found
at the RNAO website (www.rnao.org/bestpractices).

Implementation StrategiesThe Registered Nurses’ Association of Ontario and the guideline development panel have
compiled a list of implementation strategies to assist healthcare organizations or healthcare disciplines
who are interested in implementing this guideline. At the time of its original publication, this best practice
guideline was pilot tested in four clinical settings within one organization, and many of these strategies
were found to be helpful during the implementation. A summary of these strategies follows:
■ Have a dedicated person such as a clinical resource nurse who will provide support, clinical expertise
and leadership. The individual should also have good interpersonal, facilitation and project
management skills.
■ Establish a steering committee comprised of key stakeholders and members committed
to leading the initiative. A work plan can assist as a means of keeping track of activities, responsibilities
and timelines.
■ Provide educational sessions and ongoing support for implementation. At the pilot site, a core
education session of approximately two hours was developed by a steering committee. The education
session consisted of a Powerpoint presentation, discussion of case scenarios and was designed to be
informal and interactive. The content drew on the recommendations contained in this guideline.
Reminders, such as buttons, posters, laminated cards summarizing the steps in the Ask, Advise, Assist
and Arrange strategy, were also used as education strategies.
■ Attitudes on smoking are shaped by a number of factors including an individual's personal value system.
Early attention to attitudes and values is needed by providing staff the opportunity to talk and problem
solve on the job. This can be achieved using case scenarios to reflect the situations each group of
participants faced with their clients.
■ Organizational support, such as having the structures in place to facilitate the implementation.
Examples include: hiring of replacement staff so participants would not be distracted by concerns about
work and having an organizational philosophy that reflects the value of best practices through policies
and procedures and documentation tools.
■ Teamwork and collaboration through interdisciplinary work is beneficial in helping clients quit
smoking. It is essential to be cognizant of smoking cessation programs and to tap the resources that are
available in the community. An example would be linking and developing partnerships with nicotine
addiction clinics for referral process. The RNAO’s Advanced Clinical/Practice Fellowship (ACPF) Project
is a resource for registered nurses. They apply for a fellowship and have an opportunity to work with a
mentor who has expertise in smoking cessation programs. With the ACPF, the nurse fellow will also have
the opportunity to learn more about new resources.
In addition to the tips mentioned above, the RNAO has developed resources that are available on the
website. A Toolkit for implementing guidelines can be helpful if used appropriately. A brief description of
the Toolkit can be found in Appendix O. A full version of the document in .pdf format is also available at the
RNAO website, www.rnao.org/bestpractices.
Integrating Smoking Cessation into Daily Nursing Practice
40

41
An e-learning module on smoking cessation has also been developed by the RNAO. The e-learning module
can be used in conjunction with other teaching/learning modalities and it is available at
www.rnao.org/smokingcessation.
The Program Training and Consultation Centre’s website also provides resources that might be helpful
as teaching tools. These teaching tools are available at www.ptcc.on.ca. (See Appendix N for listing of
other resources.)
It is most important to emphasize the minimal intervention aspect of this best practice guideline.
This takes less than three minutes. Nurses and others need to know that minimal intervention can
be easily integrated in their daily practice. The minimal intervention is crucial for implementation.
It can be implemented not only by nurses, but by all healthcare providers in any clinical setting.
Research Gaps & Future ImplicationsIn reviewing the evidence for the revision of this guideline, it is clear that future research opportunities involve:
■ Interventions to prevent relapse in individuals who have recently quit smoking.■ Attitudes of nurses towards smoking cessation counselling, and the impact on practice.■ The needs of special populations as they are reflected in program development and delivery.■ The benefits of NRT, to persons of various levels of nicotine dependency.■ The impact of the cost of accessing NRT on smoking cessationoutcomes.
Nursing Best Practice Guideline

Integrating Smoking Cessation into Daily Nursing Practice
42
Process for Update/Review of GuidelineThe Registered Nurses’ Association of Ontario proposes to update the Best Practice
Guidelines as follows:
1. Each nursing best practice guideline will be reviewed by a team of specialists (Review Team) in the
topic area every three years following the last set of revisions.
2. During the three-year period between development and revision, RNAO Nursing Best Practice
Guidelines program staff will regularly monitor relevant literature in the field.
3. Based on the results of this monitoring, program staff will recommend an earlier revision period.
Appropriate consultation with a team of members comprised of original panel members and other
specialists in the field will help inform the decision to review and revise the guideline earlier than
the three-year milestone.
4. Three months prior to the three-year review milestone, the program staff will commence the
planning of the review process by:
a. Inviting specialists in the field to participate in the Review team. The Review Team will be
comprised of members from the original panel as well as other recommended specialists.
b. Compiling feedback received, questions encountered during the dissemination phase as well as
other comments and experiences of implementation sites.
c. Compiling new clinical practice guidelines in the field, systematic reviews, meta-analysis papers,
technical reviews and randomized controlled trial research, and other relevant literature.
d. Developing a detailed work plan with target dates and deliverables.
The revised guideline will undergo dissemination based on established structures and processes.
43
ReferencesAmerican Psychiatric Association. 2000. (DSM-IV-TR) Diagnostic and statistical manual of mental disorders, 4th edition, textrevision. Washington, DC: American Psychiatric Press, Inc.
Anderson, J. E., Jorenby, D. E., Scott, W. J., & Fiore, M. C. (2002). Treating tobacco use and dependence: An evidence-basedclinical practice guideline for smoking cessation. Chest, 121(3), 932-941.
Baker, C., Ogden, S., Prapaipanich, W., Keith, C. K., Beattie, L. C., & Nickleson, L. (1999). Hospital consolidation: Applyingstakeholder analysis to merger life cycle. Journal of Nursing Administration, 29(3), 11-20. Bandura, A. (1977). Social learningtheory. New York: General Learning Press.
Bandura, A. (1986). Social foundations of thought and action: A social cognitive theory. Englewood Cliffs, NJ: Prentice-Hall.
Berger, B.A. (2004a). Assessing and interviewing patients for meaningful behavior change. Part 1. The Case Manager, 15(5), 46-50.
Berger, B.A. (2004b). Assessing and interviewing patients for meaningful behavior change. Part 2. The Case Manager, 15(5), 58-62.
Black, N., Murphy, M., Lamping, D., McKee, M., Sanderson, C., Ashkam, J. et al. (1999). Consensus development methods:Review of best practice in creating clinical guidelines. Journal of Health Services Research and Policy, 4(4), 236-248.
Bottoroff, J. B., Johnson, J. L., Irwin, L., & Ratner, P. (2000). Narratives of smoking relapse: The stories of postpartum women.Research in Nursing and Health, 23, 126-134.
Brodish, P. H. (1998). The irreversible health effects of cigarette smoking. American Council on Science and Health [On-line].Available: http://www.acsh. org/publications/booklets/iesmoke.pdf
Canadian Cancer Society. (2003). Canadian cancer statistics. Canadian Cancer Society [On-line]. Available: www.cancer.ca
Canadian Council on Smoking and Health. (2003). Guide your patients to smoke-free future: A program of the CanadianCouncil on Smoking and Health. Ottawa, Ontario: Canadian Council on Smoking and Health.
Canadian Nurses Association. (1997). Guidelines for registered nurses working with Canadians affected by tobacco. Ottawa,Ontario: Canadian Nurses Association.
Centres for Disease Control and Prevention. (1999). Best practices for comprehensive tobacco control programs. Centres ofDisease Control and Prevention [On-line]. Available: http://www.cdc.gov/tobacco/bestprac.htm
Clarke, M. & Oxman, A. D. (1999). Cochrane Reviewers’ Handbook 4.0 (updated July 1999) (Version 4.0) [Computer software].Oxford: Review Manager (RevMan).
Cluzeau, F., Littlejohns, P., Grimshaw, J., et al. (1997). Appraisal instrument for clinical guidelines. St. Georges’s Hospital MedicalSchool, England [Online]. Available: http://sghms.ac.uk/phs/hceu/
Coleman, T. (2004). ABC of smoking cessation: Use of simple advice and behavioural support. British Medical Journal, 14; 2004328, 397-399.
College of Nurses of Ontario. (2003). Medication standards for Registered Nurses and Registered Practical Nurses in Ontario.Toronto, Ontario: College of Nurses of Ontario.
Conference Board of Canada. (2006). Smoking and the bottom line: The costs of smoking in the workplace. Conference Boardof Canada [On-line]. Available: http://sso.conferenceboard.ca/e-Library/LayoutAbstract.asp?DID=1754
Fichtenberg, C. M. & Glantz, S. A. (2002). Effect of smoke-free workplaces on smoking behaviour: Systematic review. BritishMedical Journal, 325,188-191.
Field, M. & Lohr, K. N. (1990). Guidelines for clinical practice: Directions for a new program. Washington, DC: Institute ofMedicine, National Academy Press.
Fiore, M. C. (1997). AHCPR Smoking cessation guideline: A fundamental review. Tobacco Control, 6(Suppl. 1), S4-S8.
Fiore, M. C., Bailey, W. C., Cohen, S. J., et al. (2000). Treating tobacco use and dependence. Clinical practice guideline.Rockville, MD: U.S. Department of Health and Human Services, Public Health Service.
Fiore, M. C., Jorenby, D. E., & Baker, T. B. (1997). Smoking cessation: Principles and practice based upon the AHCPR guideline,1996. Annals of Behavioural Medicine, 19(3), 213-219.
Nursing Best Practice Guideline

Graham, I., Harrison, M., Brouwers, M., Davies, B., & Dunn, S. (2002). Facilitating the use of evidence in practice: Evaluatingand adapting clinical practice guidelines for local use by health care organizations. Journal of Gynecology, Obstetric andNeonatal Nursing, 31(5), 599-611.
Greaves, L., Cormier, R., Devries, K., Bottorff, J., Johnson, J., Kirkland, S. & Aboussafy, D. (2003) Expecting to quit: A bestpractices review of smoking cessation interventions for pregnant and postpartum girls and women. Vancouver: BritishColumbia Centre of Excellence for Women’s Health. (Project funded by Health Canada)
Gonzales D, Rennard, S. I, Nides, M., Oncken, C., Azoulay, S., Billing, C. B, Watsky, E. J, Gong, J., Williams, K. E, Reeves, K. R;Varenicline Phase 3 Study Group. (2006) Varenicline, an alpha4beta2 nicotinic acetylcholine receptor partial agonist, vssustained-release bupropion and placebo for smoking cessation: A randomized controlled trial. Journal of the American MedicalAssociation, 296(1), 47-55.
Hajek, P., Stead, L. F, West, R., Jarvis, M., Lancaster, T. (2006) Relapse prevention interventions for smoking cessation. (Review)Issue 2. Cochrane Collaboration. John Wiley and Sons Ltd.
Health Canada. (1997a). Asking to listen: Helping pregnant and postpartum women and their families to quit or reducesmoking. Ottawa: Ontario, Minister of Public Works and Government Services Canada. Video Recording
Health Canada. (1997b). Helping pregnant and postpartum women and their families to quit or reduce smoking. Ottawa:Ontario: Minister of Public Works and Government Services Canada.
Health Canada. (2001). Educational resources and research – Smoking cessation – living smoke free: Clinical practice guidelines.Health Canada [On-line]. Available: http://www.hc-sc.gc.ca/hppb/cessation/resources.clinical.html
Health Canada. (2003). Facts about tobacco. Health Canada [On-line]. Available: www.hc.-sc.ca/hecs-sesc/tobacco/facts/index.html
Heart and Stroke Foundation of Ontario and Registered Nurses’ Association of Ontario. (2005). Nursing Management ofHypertension. Toronto, Canada: Heart and Stroke Foundation and Registered Nurses’ Association of Ontario.
Heatherton, T. D., Koslowski, L. T., Frecker, R. C., & Fagerstrom, K. O. (1991). The Fagerstrom Test for Nicotine Dependence: Arevision of the Fagerstrom Tolerance Questionnaire. British Journal of Addiction, 86, 1119-1127.
Institute for Clinical Systems Improvement. (2000a). Tobacco use prevention and cessation for adults and mature adolescents.Bloomington, MN: Institute for Clinical Systems Improvement (ICSI) [On-line]. Available:http://www.icsi.org/guidelst.htm#guidelines
Institute for Clinical Systems Improvement. (2000b). Tobacco use prevention and cessation for infants, children and adolescents.Bloomington, MN: Institute for Clinical Systems Improvement (ICSI). [On-line]. Available:http://www.icsi.org/guidelst.htm#guidelines
Joanna Briggs Institute. (2001). Best practice evidence based practice information sheets for health professionals: Smokingcessation interventions and strategies. Joanna Briggs Institute [On-line]. Available:http://www.joannabriggs.edu.au/pdf/BPlssmok.pdf
Jorenby, D. E, Hays, J. T, Rigotti, N. A, Azoulay, S., Watsky, E. J, Williams, K. E, Billing, C. B, Gong, J., Reeves, K. R; Varenicline Phase 3Study Group. (2006). Efficacy of varenicline, an alpha4beta2 nicotinic acetylcholine receptor partial agonist, vs placebo or sustained-release bupropion for smoking cessation: A randomized controlled trial. Journal of the American Medical Association, 296(1), 56-63.
Katz, D. A., Muehlenbruch, D. R., Brown, R. B., Fiore, M. C., Baker, T. B., & AHRQ Smoking Cessation Guideline Study Group.(2002). Effectiveness of a clinic-based strategy for implementing the AHRQ smoking cessation guideline in primary care.Preventive Medicine, 35(3), 293-302.
Lancaster, T. & Stead, L. F. (2003a). Self-help interventions for smoking cessation. (Cochrane Review). In The Cochrane Library,Issue 3. Oxford: Update Software.
Lancaster, T. & Stead, L. F. (2003b). Individual behavioural counselling for smoking cessation. (Cochrane Review). In TheCochrane Library, Issue 3. Oxford: Update Software.
Lawvere, S., Mahoney, M. C., Englert, J. J., Murphy, J. M., Hyland, A., Klein, S. B. et al. (2003). Nurse practitioners' knowledge,practice and attitudes about tobacco cessation & lung cancer screening. Journal of the American Academy of NursePractitioners, 15, 376-381.
Madjar, I. & Walton, J. A. (2001). What is problematic about evidence? In J. M, Morse, J. M., Swanson, & A. J., Kuzel (Eds.),The Nature of Qualitative Evidence (pp. 28-45). Thousand Oaks: Sage.
Miller, W. & Rollnick, S. (1991). Motivational interviewing: Preparing people to change addictive behavior. New York: The Guilford Press.
Integrating Smoking Cessation into Daily Nursing Practice
44

45
Moher, M., Hey, K., & Lancaster, T. (2005). Workplace interventions for smoking cessation. The Cochrane Library(Oxford) (ID #CD003440),
National Health and Medical Research Council. (1998). A guide to the development, implementation and evaluation of clinicalpractice guidelines. National Health and Medical Research Council. [On-line].Available: http://www.nhmrc.gov.au/publications/ pdf/cp30.pdf
National Health Committee. (1999a). Guidelines for smoking cessation: Literature review and background information. NewZealand Guidelines Group [On-line]. Available: http://www.nzgg.org.nz/library.cfm
National Health Committee. (1999b). Guidelines for smoking cessation: Quit Now! New Zealand Guidelines Group [On-line].Available: http://www.nzgg.org.nz/library.cfm
National Health Committee (2002). Guidelines for smoking cessation: Quit now! (revised 2002). The New Zealand GuidelinesGroup [On-line]. Available: www.nzgg.org.nz/library/gl_complete/smoking/index.cfm
NHS Centre for Reviews and Dissemination – The University of York. (1998). Smoking cessation: What the Health Service can do?NHS Centre for Reviews and Dissemination, The University of York [On-line]. Available: http://www.york.ac.uk/inst/crd/em31.htm
Ontario Ministry of Health Promotion. (2006). Frequently asked questions about Ontario's smoke-free strategy. Retrieved[Electronic Version] from http://www.mhp.gov.on.ca/english/health/smoke_free/faqs.asp
Ontario Public Health Association. (1996). Making a difference! A workshop on the basics of policy change. Toronto, Ontario:Government of Ontario.
Ontario Tobacco Research Unit – University of Toronto. (2001). Protection from second-hand tobacco smoke in Ontario – Areview of the evidence regarding best practices. National Clearinghouse on Tobacco and Health Programs [On-line]. Available:http://www.ncth.ca
Ontario Tobacco Research Unit. (1995). Facts on tobacco: Prevention, protection and cessation. Toronto, Ontario: AddictionResearch Foundation of Ontario.
Ontario Tobacco Research Unit. (2000a). Monitoring the Ontario tobacco strategy: Progress toward our goals 1999/2000.Toronto, Ontario: Ontario Tobacco Research Unit.
Ontario Tobacco Research Unit. (2000b). Special report: Monitoring the Ontario tobacco strategy, smoking cessation in Ontario1998/1999 – Current trends, interventions and initiatives. Toronto, Ontario: Ontario Tobacco Research Unit – Centre for HealthPromotion - University of Toronto.
Ontario Tobacco Research Unit. (2006). Indicators of smoke-free Ontario progress, special reports: Monitoring and evaluationseries. 12(2). Toronto; Ontario Tobacco Research Unit.
Orsetti, K., Dwyer, S., Sheldon, S., Thomas, L., & Harrison, V. (2001). UMHS Smoking cessation guideline. University ofMichigan Health System [On-line]. Available: http://cme.med.umich.edu// pdf/guideline/smoking.pdf
Pelkonen, M. & Kankkunen, P. (2001). Nurses' competence in advising and supporting clients to cease smoking: a surveyamong Finnish nurses. Journal of Clinical Nursing, 10, 437-441.
Prochaska, J. O. & DiClemente, C. C. (1983). Stages and processes of self-change of smoking: Toward an integrative model ofchange. Journal of Consulting and Clinical Psychology, 51(3), 390-395.
Prochaska, J. O., Velicer, W. F., Fava, J. L., Ruggiero, L., Laforge, R. G., Rossi, J. S. (2001). Counselor and stimuluscontrol enhancements of a stage-matched expert system intervention for smokers in a managed care setting. PreventiveMedicine, 32, 23-32.
Program Training and Consultation Centre. (1995). Info Pack: Understanding and using the stages of change, Ottawa, OntarioTobacco Strategy.
Public Health and Long-Term Care Branch – City of Ottawa. (2001). Health benefits of quitting smoking. Ottawa, Ontario:Pubic Health and Long-Term Care Branch – City of Ottawa.
Rabius, V., McAlister, A. L., Geiger, A., Huang, P., & Todd, R. (2004). Telephone counseling increases cessation rates amongyoung adult smokers. Health Psychology, 23, 539-541.
Registered Nurses' Association of Ontario. (2003). Integrating Smoking Cessation into Daily Nursing Practice. Toronto, Canada:Registered Nurses' Association of Ontario.
Registered Nurses' Association of Ontario. (2002). Toolkit: Implementation of clinical practice guidelines. Toronto, Canada:Registered Nurses' Association of Ontario.
Nursing Best Practice Guideline

Rice, V. (1999). Nursing intervention and smoking cessation: A meta-analysis. Heart & Lung, 28, 438-454.
Rice, V. & Stead, L. (2003). Nursing interventions for smoking cessation. (Cochrane Review). In The Cochrane Library, Issue 3.Oxford: Update Software.
Rigotti, N., Munafo, M., Murphy, M. & Stead, L. (2003). Interventions for smoking cessation in hospitalized patients(Cochrane Review). In The Cochrane Library, Issue 4. Oxford: Update Software.
Rollnick, S. & Miller, W. (1995). What is motivational interviewing? Behavioural and Cognitive Psychotherapy, 23, 325-334.
Royal College of Nursing. (1999). Clearing the air: A nurses guide to smoking and tobacco control. London, England: The RoyalCollege of Nursing.
Royal College of Nursing. (2002). Clearing the air: A nurses guide to smoking and tobacco control. London, England: The RoyalCollege of Nursing.
Royal College of Physicians of London. (2000). Nicotine addiction in Britain: A report of the Tobacco Advisory Groupof the Royal College of Physicians. Royal College of Physicians of London [On-line]. Available:www.rcplondon.ac.uk/pubs/wp_nicotine_summary.htm
Schabas, R. E. (1996). Tobacco sounding the alarm: Report of the Chief Medical Officer of Health Ottawa, Ontario: Queen’sPrinter of Ontario.
Schultz, A. S. H., Bottorff, J. L., Johnson, J. L. (2006). Tobacco within acute care hospitals: An ethnographic study of nurses’workplace. Tobacco Control, 15(4):317-22.
Smith, D., Heckemeyer, C., Kratt, P., & Mason, D. (1997). Motivational interviewing to improve adherence to a behaviouralweight control program for older obese women with NIDDM: A pilot study. Diabetes Care, 20, 52-54.
Stead, L., Lancaster, T., & Perera, R. (2003). Telephone counselling for smoking cessation (Cochrane Review). In The CochraneLibrary, Issue 3. Oxford: Update Software.
Surgeon General of the United States. (2000). Clinical practice guideline: Treating tobacco use and dependence. Surgeon General,U.S. Department of Health and Human Services [On-line]. Available: www.surgeongeneral.gov/tobacco/treating_tobacco_use.pdf
Tonstad, S., Tonnesen, P., Hajek, P., Williams, K. E., Billing, C. B., Reeves, K. R.; Varenicline Phase 3 Study Group. (2006). Effectof maintenance therapy with varenicline on smoking cessation: A randomized controlled trial. Journal of the American MedicalAssociation, 296(1), 64-71.
U. S. Department of Health and Human Services. (2000). Reducing tobacco use: A report of the Surgeon General. (Rep. No.S / N 017-001-00544- 4). Atlanta, GA: U. S. Department of Health and Human Services, Centres for Chronic Disease Controland Prevention, Office on Smoking and Health.
U. S. Department of Health and Human Services Public Health Service. (2000). Clinical practice guideline: Treating tobacco useand dependence. Office of the Surgeon General. Retrieved [Electronic Version] fromhttp://www.surgeongeneral.gov/tobacco/treating_tobacco_use.pdf
U. S. Department of Health and Human Services. (2006). The health consequences of involuntary exposure to tobacco smoke:A report of the surgeon general. Atlanta, GA: US Department of Health and Human Services, Centres for Disease Control andPrevention, Coordinating Centre for Health Promotion, National Centre for Chronic Disease Prevention and Health Promotion,Office on Smoking and Health. Retrieved [Electronic Version] from www.surgeongeneral.gov/library
University of Toronto Department of Family & Community Medicine. (1998). Project CREATE: Smoking cessation module.(vols. 3) Toronto, Ontario: Project CREATE.
University of Toronto Department of Family & Community Medicine. (2000). Smoking cessation guidelines: How to treat yourpatient’s tobacco addiction. Toronto, Ontario: Pegasus Healthcare International.
University of Ulster. (2001). Tobacco & health activities. University of Ulster, Ireland [On-line]. Available:http://www.dmc.ni.co.uk/UCF/tobacco.htm
West, R. & Shiffman, S. (2001). Effect of oral nicotine dosing forms on cigarette withdrawal symptoms and craving: Asystematic review. Psychopharmacology, 155, 115-122.
Wilhelm, K., Wedgewood, L., Niven, H., Kay-Lambkin, F. (2006). Smoking cessation and depression: Current knowledge andfuture directions. Drug and Alcohol Review, 25, 97-107.
World Health Organization. (1995). Tobacco costs more than you think. World no-tobacco day. World Health Organization.
Integrating Smoking Cessation into Daily Nursing Practice
46

47
BibliographyAbdullah, A. S. M., Mak, Y. W., Loke, A. Y., & Lam, T. (2005). Smoking cessation intervention in parents of young children: Arandomised controlled trial. Addiction, 100, 1731-1740.
Adams, C., Munsasinghe, I., & Bryar, R. (2000). Clinical effectiveness information bulletin. CPHVA: Clinical EffectivenessInformation Bulletin, 1-4.
Agency for Quality in Medicine–Joint Institution of the German Medical Association and the Association of the Statutory HealthInsurance Physicians. (1999). Evaluation criteria for clinical practice guidelines in Germany. Agency for Quality in Medicine[On-line]. Available: http://www.azq.de
Ahluwalia, J. S., Harris, K. J., Catley, D., Okuyemi, K. S., & Mayo, M. S. (2002). Sustained-release bupropion for smokingcessation in African Americans: A randomized controlled trial. JAMA: Journal of the American Medical Association, 288, 468-474.
American Medical Association. (1997). Guidelines for adolescent preventive services (GAPS). National Guideline Clearinghouse[On-line]. Available: http://www.guideline.gov/guidelines/ngc_676.html
American Psychiatric Press. (1996). Practice guideline for the treatment of patients with nicotine dependence. NationalGuideline Clearinghouse [On-line]. Available: http://www.guideline.gov/index.asp
Andrews, O. J., Tingen, M. S., & Harper, J. R. (1999). A model nurse practitioner-manager smoking cessation clinic. OncologyNurses Forum, 26(10), 1603-1608.
Aquilino, M. L., Goody, C. M., & Lowe, J. B. (2003). WIC providers’ perspectives on offering smoking cessation interventions.MCN: The American Journal of Maternal/Child Nursing, 28, 326-332.
Ashley, M. J., Ferrence, R., Boadway, T., Pipe, A., Cameron, R., Schabas, R. et al. (1999). Actions will speak louder than words:Getting serious about tobacco control in Ontario. Toronto, Ontario: Ontario Tobacco Research Unit – Centre for HealthPromotion – University of Toronto.
Barta, S. K. & Stacy, R. D. (2005). The effects of a theory-based training program on nurses’ self-efficacy and behavior forsmoking cessation counselling. Journal of Continuing Education in Nursing, 36, 117-123.
Bell, R. M. & Tingen, M. S. (2001). The impact of tobacco use in women: Exploring smoking cessation strategies.Clinical Journal of Oncology Nursing, 5(3), 101-104.
Bolman, C., de Vries, H., & van Breukelen, G. (2002). Evaluation of a nurse-managed minimal-contact smoking cessationintervention for cardiac inpatients. Health Education Research, 17, 99-116.
Borland, R., Segan, C. J., Livingston, P. M., & Owen, N. (2001). The effectiveness of callback counselling for smoking cessation:A randomized trial. Addiction, 96, 881-889.
Borland, R., Balmford, J., Segan, C., Livingston, P., & Owen, N. (2003). The effectiveness of personalized smoking cessationstrategies for callers to a Quitline service. Addiction, 98, 837-846.
Borland, R., Balmford, J., & Hunt, D. (2004). The effectiveness of personally tailored computer-generated advice letters forsmoking cessation. Addiction, 99, 369-377.
Boyle, R. G., Solberg, L. I., Asche, S. E., Boucher, J. L., Pronk, N. P., & Jensen, C. J. (2005). Offering telephone counselling tosmokers using pharmacotherapy. Nicotine & Tobacco Research, 7,.
Browman, G. P., Levine, M. N., Mohide, A., Hayward, R. S. A., Pritchard, K. I., Gafni, A. et al. (1995). The practice guidelines developmentcycle: A conceptual tool for practice guidelines development and implementation. Journal of Clinical Oncology, 13(2), 502-512.
Buchanan, L. M., El Banna, M., White, A., Moses, S., Siedlik, C., & Wood, M. (2004). An exploratory study of multicomponenttreatment intervention for tobacco dependency. Journal of Nursing Scholarship, 36, 324-330.
Burns, D., Gritz, E., Kritseller, J., Ostroff, J., Vries, D. H., & Yao, H. (2000). Reversing the effects of tobacco-related illness withcessation. Cancer Information Service, 2-8.
Canadian Association of Occupational Therapists, Canadian Association of Social Workers, Canadian Dental Association, CanadianMedical Association, Canadian Nurses Association, Canadian Pharmacists Association et al. (2001). Tobacco: The role of healthprofessionals in smoking cessation - Joint Statement. Canadian Nurses Association [On-line]. Available: http://www.can-nurses.ca
Canadian Cancer Society/National Cancer Institute of Canada/University of Waterloo. (2000). Encouraging to quit: An easy andeffective intervention for the dental office. Canadian Cancer Society [On-line]. Available: http://www.cancer.ca/tobacco
Nursing Best Practice Guideline

CDC – National Centre for Chronic Disease Preventions and Health Promotion. (1994). Guidelines for school health programsto prevent tobacco use and addiction. CDC – National Centre for Chronic Disease Prevention and Health Promotion [On-line].Available: http://www.cdc.gov/mmwr/preview/mmwrhtml/00026213.htm
Chalmers, K., Bramadat, I. J., Cantin, B., Shuttleworth, E., & Scott-Findlay, S. (2000). Smoking characteristics of Manitobanurses. Canadian Nurse, 31-34.
Chan, S. S., Lam, T. H., Salili, F., Leung, G. M., Wong, D. C., Botelho, R. J. et al. (2005). A randomized controlled trial of anindividualized motivational intervention on smoking cessation for parents of sick children: A pilot study. Applied NursingResearch, 18, 178-181.
Chouinard, M. & Robichaud-Ekstrand, S. (2005). The effectiveness of a nursing inpatient smoking cessation program inindividuals with cardiovascular disease. Nursing Research, 54, 243-254.
Cluzeau, F., Littlejohns, P., Grimshaw, J., Feder, G., & Moran, S. (1999). Development and application of a generic methodologyto assess the quality of clinical guidelines. International Journal for Quality in Healthcare, 11, 21-28.
Collins, B. N., Wileyto, E. P., Patterson, F., Rukstalis, M., Audrain-McGovern, J., Kaufmann, V. et al. (2004). Gender differences insmoking cessation in a placebo-controlled trial of bupropion with behavioral counselling. Nicotine & Tobacco Research, 6, 27-37.
Cornuz, J., Humair, J., Seematter, L., Stoianov, R., van Melle, G., Stalder, H. et al. (2002). Efficacy of resident training insmoking cessation: A randomized, controlled trial of a program based on application of behavioral theory and practice withstandardized patients. Annals of Internal Medicine, 136, 429-437.
Covey, L. S., Glassman, A. H., Stetner, F., Rivelli, S., & Stage, K. (2002). A randomized trial of sertraline as a cessation aid forsmokers with a history of major depression. American Journal of Psychiatry, 159, 1731-1737.
Dawes, M., Davies, T. P., Gray, M. A., Mant, J., Seers, K., & Snowball, R. (1999). Evidence-based practice: A primer for healthcareprofessionals. A Primer For Healthcare Professionals (pp. 127-131). Toronto, Ontario: Churchill Livingstone.
Edwards, N., Aubin, P., & Morrison, M. (2000). The effectiveness of postpartum smoking relapse prevention strategies: Asystematic review of the evidence 1992-1999 – CHRU Publication No. M00-1. Ottawa, Ontario: Community Health ResearchUnit, University of Ottawa.
Edwards, N., Kuhn, M., & Hotz, S. (1997). Smoking relapse prevention - pregnant & postpartum women - CHRU PublicationNo. M99 - 15. Ottawa, Ontario: Community Health Research Unit, University of Ottawa.
Ellis, G., Rodger, J., McAlpine, C., & Langhorne, P. (2005). The impact of stroke nurse specialist input on risk factormodification: A randomised controlled trial. Age and Ageing, 34, 389-392.
Emmons, K. M., Puleo, E., Park, E., Gritz, E. R., Butterfield, R. M., Weeks, J. C. et al. (2005). Peer-delivered smoking counselling forchildhood cancer survivors increases rate of cessation: The partnership for health study. Journal of Clinical Oncology, 23, 6516-6523.
Etter, J. & Perneger, T. V. (2004). Post-intervention effect of a computer tailored smoking cessation programme. Journal ofEpidemiology and Community Health, 58, 849-851.
Etter, J.-F. (2005). Comparing the efficacy of two internet-based, computer-tailored smoking cessation programs: A randomizedtrial. Journal of Medical Internet Research, 7.
Etter, J.F. (2002). Using new information technology to treat tobacco dependence. Respiration, 69, 111-114.
Etter, J. F. & Perneger, T. V. (2001). Effectiveness of a computer-tailored smoking cessation program: A randomized trial.Archives of Internal Medicine, 161, 2596-2601.
Foley, K. L., Crandall, S. J., George, G., Roman, M., & Spangler, J. G. (2003). Reliability of a smoking cessation risk factorinterview scale (SCRFIS) for use with standardized patient instructors. Journal of Cancer Education, 18, 134-141.
Fowler, G. (2000). Helping smokers to stop: An evidence-based approach. The Practitioner, 244, 37-41.
Friend, K. & Levy, D. T. (2001). Smoking treatment interventions and policies to promote their use: A critical review. Nicotineand Tobacco Research, 3, 299-310.
Glavas, D., Rumboldt, M., & Rumboldt, Z. (2003). Smoking cessation with nicotine replacement therapy among health careworkers: Randomized double-blind study. Croatian Medical Journal, 44, 219-224.
Grandes, G., Cortada, J. M., & Arrazoa, A. (2000). An evidence-based programme for smoking cessation: Effectiveness inroutine general practice. British Journal of General Practice, 50, 803-807.
Hajek, P., Taylor, T. Z., & Mills, P. (2002). Brief intervention during hospital admission to help patients to give up smoking aftermyocardial infarction and bypass surgery: Randomized controlled trial. British Medical Journal, 324, 87-89.
Integrating Smoking Cessation into Daily Nursing Practice
48
49
Hall, S. M., Humfleet, G. L., Reus, V. I., Munoz, R. F., & Cullen, J. (2004). Extended nortriptyline and psychological treatment forcigarette smoking. American Journal of Psychiatry, 161, 2100-2107.
Hand, S., Edwards, S., Campbell, I. A., & Cannings, R. (2002). Controlled trial of three weeks nicotine replacement treatment inhospital patients also given advice and support. Thorax, 57, 715-718.
Harrington, P. (2001). WHO evidence based recommendations on the treatment of tobacco dependence. Monaldi Archives forChest Disease, 56(5), 462-466.
Haustein, K.O. (2003). What can we do in secondary prevention of cigarette smoking? European Journal of CardiovascularPrevention & Rehabilitation, 10, 476-485.
Health Canada. (2003). Quitting: Guide to tobacco use cessation programs in Canada. The Community Health Research Unit[On-line]. Available: www.hc.sc.gc.ca/hecs-sesc/tobacco/quitting/cessation/tobeng2.html
Health Education Authority. (1998). Stopping smoking made easier. London, England: Health Education Authority.
Hebert, R. (2005). What’s new in nicotine & tobacco research? Nicotine & Tobacco Research, 7, 309-315.
Hennrikus, D. J., Jeffery, R. W., Lando, H. A., Murray, D. M., Brelje, K., Davidann, B. et al. (2002). The SUCCESS project: theeffect of program format and incentives on participation and cessation in worksite smoking cessation programs. AmericanJournal of Public Health, 92, 274-279.
Hennrikus, D. J., Lando, H. A., McCarty, M. C., Klevan, D., Holtan, N., Huebsch, J. A. et al. (2005). The TEAM project: Theeffectiveness of smoking cessation intervention with hospital patients. Preventive Medicine, 40, 249-258.
Hilleman, D. E., Mohiuddin, S. M., & Packard, K. A. (2004). Comparison of conservative and aggressive smoking cessationtreatment strategies following coronary artery bypass graft surgery. Chest, 125, 435-438.
Hopper, J. A. & Gallagher, R. E. (2003). Tobacco cessation: New challenges, new opportunities. Journal of Cancer Education, 18, 128-133.
Hornberger, C. A. & Edwards, L. C. (2004). Survey of tobacco cessation curricula in Kansas nursing programs.Nurse Educator, 29, 212-216.
Hudmon, K. S., Corelli, R. L., Chung, E., Gundersen, B., Kroon, L. A., Sakamoto, L. M. et al. (2003). Development and implementationof a tobacco cessation training program for students in the health professions. Journal of Cancer Education, 18, 142-149.
Hudmon, K. S., Kroon, L. A., Corelli, R. L., Saunders, K. C., Spitz, M. R., Bates, T. R. et al. (2004). Training future pharmacists ata minority educational institution: Evaluation of the Rx for change tobacco cessation training program. Cancer Epidemiology,Biomarkers & Prevention, 13, 477-481.
Hughes, J. R., Stead, L. F., & Lancaster, T. (2003). Antidepressants for smoking cessation. (Cochrane Review). In The CochraneLibrary, Issue 3. Oxford: Update Software.
Humair, J. P. & Cornuz, J. (2003). A new curriculum using active learning methods and standardized patients to train residentsin smoking cessation. Journal of General Internal Medicine, 18, 1023-1027.
Institute for Clinical Systems Improvement. (2004). Tobacco use prevention and cessation for adults and mature adolescents.Bloomington, MN: Institute for Clinical Systems Improvement (ICSI).
Jackson, G., Bobak, A., Chorlton, I., Hall, R., Matthews, H., Stapleton, J. et al. (2001). Smoking cessation: A consensusstatement with special reference to primary care. International Journal of Clinical Practice, 55(6), 385-392.
Johnston, J. M., Chan, S. S. C., Chan, S. K. K., Lam, T. H., Chi, I., & Leung, G. M. (2005). Training nurses and social workers insmoking cessation counselling: A population needs assessment in Hong Kong. Preventive Medicine, 40, 389-406.
Johnson, J. L., MacDonald, S., Reist, D. & Bahadori, K. (2006). Tobacco reduction in the context of mental illness andaddictions: A review of the evidence. Vancouver: Provincial Health Services Authority.
Jonsdottir, H., Jonsdottir, R., Geirsdottir, T., Sveinsdottir, K. S., & Sigurdardottir, T. (2004). Multicomponent individualizedsmoking cessation intervention for patients with lung disease. Journal of Advanced Nursing, 48, 594-604.
Jorenby, D. E. & Fiore, M. C. (1999). The Agency for Healthcare Policy and Research smoking cessation clinical practiceguideline: Basics and beyond. Tobacco Use & Cessation, 26(3), 513-529.
Joseph, J. C. (1999). ASHP therapeutic position statement on smoking cessation. American Society of Health SystemPharmacists, 56, 460-464.
Joza, J. & Wynn, M. (2001). Starting a smoking cessation group. Ottawa, Ontario: Ontario Ministry of Health and Long-TermCare, The Program Training and Consultation Centre.
Nursing Best Practice Guideline

Kattapong, J. V., Locher, T. L., Secker-Walker, R. H., & Bell, T. A. (1998). Tobacco-cessation patient counselling. American Journalof Preventive Medicine, 15(2), 160-162.
Karnath, B. (2002). Smoking cessation. American Journal of Medicine, 112, 399-405.
Kim, J. R., Lee, M. S., Hwang, J. Y., & Lee, J. D. (2005). Efficacy of a smoking cessation intervention using the AHCPR guidelinetailored for Koreans: A randomized controlled trial. Health Promotion International, 20, 51-59.
Knishkowy, B. & Palti, H. (1997). GAPS (AMA guidelines for adolescent preventive services). Where are the gaps? Archives ofPediatrics and Adolescent Medicine, 151(2), 123-128.
Krumholz et al. (2001). Myocardial infarction: A nurse-led smoking cessation program was costeffective. Journal of theAmerican College of Cardiology [On-line].Available: http://www.eboncall.co.uk/jsp/cat/cat_display.jsp?stylesheet=/s.../catMain.xslt&resource_id=52
Kuhn, M. & Edwards, N. (1997). Smoking relapse prevention among pregnant and postpartum women – CHRU PublicationNo. M99-9. Ottawa, Ontario: Community Health Research Unit, University of Ottawa.
Lancaster, T., Stead, L., Silagy, C., & Sowden, A. (2000). Effectiveness of interventions to help people stop smoking: Findingsfrom the Cochrane Library. British Medical Journal, 321(5), 355-358.
Lancaster, T., Silagy, C., & Fowler, G. (2003). Training health professionals in smoking cessation. (Cochrane Review). In TheCochrane Library, Issue 3. Oxford: Update Software.
Lancaster, T., Stead, L., Silagy, C. (2001). Review: Advice from doctors, counselling by nurses, behavioural interventions, nicotinereplacement therapy, and several pharmacological treatments increase smoknig cessation rates. Evidence Based Nursing, 4, 13.
Lumley, J., Oliver, S., & Waters, E. (1999). Interventions for promoting smoking cessation during pregnancy. (Cochrane Review).In The Cochrane Library, Issue 3. Oxford: Update Software.
Lancaster, T. & Stead, L. F. (2005). Individual behavioural counselling for smoking cessation. The Cochrane Library. (Oxford)(4): (ID #CD001292), ID.
Lawvere, S., Mahoney, M. C., Englert, J. J., Murphy, J. M., Hyland, A., Klein, S. B. et al. (2003). Nurse practitioners’knowledge, practice and attitudes about tobacco cessation & lung cancer screening. Journal of the American Academy ofNurse Practitioners,15, 376-381.
Macleod, Z. R., Charles, M. A., Arnaldi, V. C., & Adams, I. M. (2003). Telephone counselling as an adjunct to nicotine patchesin smoking cessation: A randomised controlled trial. Medical Journal of Australia, 179, 349-352.
Marable, S., Crim, C., Dennis, G. C., Epps, R. P., Freeman, H., Mills, S. et al. (2002). Tobacco control: Consensus report of thenational medical association. Journal of the National Medical Association, 94(2), 78-87.
Margolin, A. (2003). Acupuncture for substance abuse. Current Psychiatry Reports, 5, 333-339.
Marlow, S. P. & Stoller, J. K. (2003). Smoking cessation. Respiratory Care, 48, 1238-1256.
Maseeh, A. & Kwatra, G. (2005). A review of smoking cessation interventions. Medgenmed Medscape General Medicine, 7, 17.
Massachusetts Department of Public Health. (2002). Best practice initiative: Massachusetts tobacco control program.Massachusetts Tobacco Control Program, ASH Best Practice Initiative [On-line]. Available:http://www.osophs.dhhs.gov/ophs/BestPractice/MA.htm
McAlister, A. L., Rabius, V., Geiger, A., Glynn, T. J., Huang, P., & Todd, R. (2004). Telephone assistance for smoking cessation:one year cost effectiveness estimations. Tobacco Control, 13, 85-86.
McCarty, M. C., Zander, K. M., Hennrikus, D. J., & Lando, H. A. (2001). Barriers among nurses to providing smoking cessationadvice to hospitalized smokers. American Journal of Health Promotion,16, 85-87.
McClure, J. B., Westbrook, E., Curry, S. J., & Wetter, D. W. (2005). Proactive, motivationally enhanced smoking cessationcounselling among women with elevated cervical cancer risk. Nicotine & Tobacco Research, 7, 881-889.
McKenna, H., Slater, P., Dr. Bunting, B., McCance, T., Spiers, A., & McElwee, G. (2001). Smoking in nursing: A study ofqualified nurses smoking behaviour and attitudes in Northern Ireland. University of Ulster, Centre for Nursing Research, Ireland[On-line]. Available: http://www.ulst.ac.uk/faculty/shse/research/cnr/smok.htm
Mermelstein, R., Hedeker, D., & Wong, S. C. (2003). Extended telephone counselling for smoking cessation: Does contentmatter? Journal of Consulting & Clinical Psychology, 71, 565-574.
Integrating Smoking Cessation into Daily Nursing Practice
50

51
Milch, C. E., Edmunson, J. M., Beshansky, J. R., Griffith, J. L., & Selker, H. P. (2004). Smoking cessation in primary care: Aclinical effectiveness trial of two simple interventions. Preventive Medicine, 38, 284-294.
Miller, N., Frieden, T. R., Liu, S. Y., Matte, T. D., Mostashari, F., Deitcher, D. R. et al. (2005). Effectiveness of a large-scaledistribution programme of free nicotine patches: A prospective evaluation. Lancet, 365, 1849-1854.
Ministry of Health and Long-Term Care. (2003). Tobacco: Tobacco Strategy. Ministry of Health and Long-Term Care [On-line].Available: www.health.gov.on.ca/english/public/pub/tobacco.html
Moher, M., Hey, K., & Lancaster, T. (2005). Workplace interventions for smoking cessation. The Cochrane Library. (Oxford)(4): (ID #CD003440).
Molyneux, A., Lewis, S., Leivers, U., Anderton, A., Antoniak, M., Brackenridge, A. et al. (2003). Clinical trial comparingnicotine replacement therapy (NRT) plus brief counselling, brief counselling alone, and minimal intervention on smokingcessation in hospital inpatients . Thorax, 58, 484-488.
Moner, S. E. (1994). Smoking and pregnancy. In Canadian Task Force on the Periodic Health Examination (Ed.), Canadian guideto clinical preventive healthcare. (pp. 26-36). Ottawa, Ontario: Health Canada.
Montalto, N. J. (2002). Recommendations for the treatment of nicotine dependency. Journal of the American OsteopathicAssociation, 102(6), 342-348.
Moores, L. K. (2000). Smoking and postoperative pulmonary complications. An evidence-based review of the recent literature.Clinics in Chest Medicine, 21, 139-146.
Mullen, D. P. (1999). Maternal smoking during pregnancy and evidence-based intervention to promote cessation. Tobacco Use& Cessation, 26(3), 577-589.
National Advisory Committee on Health and Disability. (2002). Guidelines for smoking cessation. (Revised 2002). Wellington,NZ: National Advisory Committee on Health and Disability (National Health Committee).
National Electronic Library for Health. (2003). A guide to effective smoking cessation interventions for the healthcare system.National Electronic Library for Health [On-line]. Available: www.nelh. nhs.uk/guidelinesb/html/smoking-recs.htm
National Institute for Health and Clinical Excellence. (2002). Brief interventions and referral for smoking cessation in primarycare and other settings. National Institute for Health and Clinical Excellence.
National Institute of Health. (1993). Nurses: Help your patients stop smoking. Bethesda, MA.
National Institute of Health, National Heart, Lung, and Blood Institute – Smoking Education Program, NIH Publication No. 92-2962.
NHS Centre for Reviews and Dissemination – The University of York. (1999a). Getting evidence into practice. NHS Centre forReviews and Dissemination, University of York [On-line]. Available: http://www.york.ac.uk/inst/crd/ehc51.htm
NHS Centre for Reviews and Dissemination – The University of York. (1999b). Preventing the uptake of smoking in young people.NHS Centre for Reviews and Dissemination, The University of York [On-line]. Available: http://www.york.ac.uk/inst/crd/em31.htm
O’Brien, G. (2006). Addictive Behaviors. In S.M. Lewis, M.M. Heitkemper & S, H, Dirksen (Eds.), Medical-Surgerical Nursing inCanada. Toronto: Mosby.
Ontario Public Health Research Education & Development Program. (2001). Smoking cessation during pregnancy. EffectivePublic Health Practice Project Highlights for Policy Development.
Park, E.-W., Schultz, J. K., Tudiver, F., Campbell, T., & Becker, L. (2003). Enhancing partner support to improve smokingcessation. (Cochrane Review). In The Cochrane Library, Issue 3. Oxford: Update Software.
Pelkonen, M. & Kankkunen, P. (2001). Nurses’ competence in advising and supporting clients to cease smoking: A surveyamong Finnish nurses. Journal of Clinical Nursing, 10, 437-441.
Peterson, J., Mecredy, D., & Goodfellow, R. (2001). The “3D” smoking cessation kit: An evaluation of a campaign to promotebrief intervention by healthcare professionals. Communiqué: Public Health Research, Education and Development Program, 19-23.
Prabhakaran, L. & Choo, Y. M. (2004). Effectiveness of nurse clinician-led outpatient smoking cessation clinic in a hospital inSingapore. Singapore Nursing Journal, 31, 6-14.
Puska, P. M., Barrueco, M., Roussos, C., Hider, A., & Hogue, S. (2005). The participation of health professionals in asmoking-cessation programme positively influences the smoking cessation advice given to patients. International Journal ofClinical Practice, 59, 447-452.
Nursing Best Practice Guideline
Rabius, V., McAlister, A. L., Geiger, A., Huang, P., & Todd, R. (2004). Telephone counselling increases cessation rates amongyoung adult smokers. Health Psychology, 23, 539-541.
Ratner, P. A., Johnson, J. L., Richardson, C. G., Bottorff, J. L., Moffat, B., Mackay, M. et al. (2004). Efficacy of asmoking-cessation intervention for elective-surgical patients. Research in Nursing & Health, 27, 148-16.
Raw, M., McNeill, A., & West, R. (1998). Smoking cessation guidelines for health professionals. A guide to effective smokingcessation interventions for the healthcare system. Thorax, 53(Suppl. 5, Part 1), S1-S19.
Raw, M., McNeill, A., & West, R. (1999). Smoking cessation: Evidence based recommendations for the healthcare system.British Medical Journal, 318, 182-185.
Reid, R., Pipe, A., Higginson, L., Johnson, K., D’Angelo, M. S., Cooke, D. et al. (2003). Stepped care approach to smokingcessation in patients hospitalized for coronary artery disease. Journal of Cardiopulmonary Rehabilitation, 23, 176-182.
Rice, V. H. & Stead, L. F. (2005). Nursing interventions for smoking cessation. The Cochrane Library. (Oxford) (4): (ID #CD001188).
Richmond, R. L. (1999). Physicians can make a difference with smokers: Evidence-based clinical approaches. InternationalJournal of Tuberculosis and Lung Disease, 3(2),100-112.
Rodriguez-Artalejo, F., Lafuente, U. P., Guallar-Castillon, P., Garteizaurrekoa, D. P., Sainz, M. O., Diez Azcarate, J. I. et al.(2003). One year effectiveness of an individualised smoking cessation intervention at the workplace: A randomised controlledtrial. Occupational & Environmental Medicine, 60, 358-363.
Rohsenow, D. J., Monti, P. M., Colby, S. M., & Martin, R. A. (2002). Brief interventions for smoking cessation in alcoholicsmokers. Alcoholism: Clinical and Experimental Research, 26, 1950-1951.
Romand, R., Gourgou, S., & Sancho-Garnier, H. (2005). A randomized trial assessing the Five-Day Plan for smoking cessation.Addiction, 100, 1546-1554.
Sauerbeck, L. R., Khoury, J. C., Woo, D., Kissela, B. M., Moomaw, C. J., & Broderick, J. P. (2005). Smoking cessation afterstroke: education and its effect on behavior. Journal of Neuroscience Nursing, 37, 316-319.
Scal, P., Hennrikus, D., Ehrlich, L., Ireland, M., & Borowsky, I. (2004). Preparing residents to counsel about smoking. ClinicalPediatrics,43, 703-708.
Schultz, A. S. H., Johnson, J. L., & Bottorff, J. L. (2006). Registered nurses’ perspectives on tobacco reduction: Views fromWestern Canada. Canadian Journal of Nursing Research
Schultz, A. S. H. (2003). Nursing and tobacco reduction: A review of the literature. International Journal of Nursing Studies. 40(6), 571-586.
Schuurmans, M. M., Diacon, A. H., Van, B., & Bolliger, C. T. (2004). Effect of pre-treatment with nicotine patch on withdrawalsymptoms and abstinence rates in smokers subsequently quitting with the nicotine patch: A randomized controlled trial.Addiction, 99, 634-640.
Shuster, G. (2005). 4 interaction dynamics occurred in telephone counselling for smoking cessation. Evidence-Based Nursing, 8, 31.
Silagy, C., Lancaster, T., Stead, L., Mant, D., & Fowler, G. (2003). Nicotine replacement therapy for smoking cessation.(Cochrane Review). In The Cochrane Library, Issue 3. Oxford: Update Software.
Silagy, C. & Stead, L. F. (2003). Physician advice for smoking cessation. (Cochrane Review). In The Cochrane Library,Issue 3. Oxford: Update Software.
Simon, J. A., Carmody, T. P., Hudes, E. S., Snyder, E., & Murray, J. (2003). Intensive smoking cessation counselling versusminimal counselling among hospitalized smokers treated with transdermal nicotine replacement: A randomized trial. AmericanJournal of Medicine, 114, 555-562
Singapore Ministry of Health. (2002). Smoking cessation. Singapore: Singapore Ministry of Health.
Singleton, J. K., Levin, R. F., Feldman, H. R., & Truglio-Londrigan, M. (2005). Evidence for smoking cessation: Implications forgender-specific strategies. Worldviews on Evidence-Based Nursing, 2, 63-74.
Smith, P. M., Cameron, R., McDonald, P. W., Kawash, B., Madill, C., & Brown, K. S. (2004). Telephone counselling forpopulation-based smoking cessation. American Journal of Health Behavior, 28, 231-241.
Snowball, R. (1999). Critical appraisal of clinical guidelines. In M.Dawes, P. Davies, A. Gray, J. Mant, K. Seers, & R. Snowball(Eds.), Evidence-based practice: A primer for healthcare professionals (pp. 127-131). Toronto, Ontario: Churchill-Livingstone.
Sowden, A., Arblaster, L., & Stead, L. F. (2003). Community interventions for preventing smoking in young people(Cochrane Review). In The Cochrane Library, Issue 3. Oxford: Update Software.
Integrating Smoking Cessation into Daily Nursing Practice
52

53
Stead, L. F. & Lancaster, T. (1999). Group behaviour therapy programmes for smoking cessation. (Cochrane Review). In TheCochrane Library, Issue 3. Oxford: Update Software.
Stead, L. F., Lancaster, T., & Perera, R. (2005). Telephone counselling for smoking cessation. The Cochrane Library. (Oxford)(4): (ID #CD002850), ID
Steptoe, A., Kerry, S., Rink, E., & Hilton, S. (2001). The impact of behavioral counselling on stage of change in fat intake,physical activity, and cigarette smoking in adults at increased risk of coronary heart disease. American Journal of PublicHealth, 91, 265-269.
Strecher, V. J., Marcus, A., Bishop, K., Fleisher, L., Stengle, W., Levinson, A. et al. (2005). A randomized controlled trialof multiple tailored messages for smoking cessation among callers to the cancer information service. Journal of HealthCommunication, 10, Suppl-18.
Swan, G. E., Javitz, H. S., Jack, L. M., Curry, S. J., & McAfee, T. (2004). Heterogeneity in 12-month outcome among female andmale smokers. Addiction, 99, 237-250.
Surgeon General of the United States. (2001). Women and smoking: A report of the Surgeon General – 2001. CDC – NationalCentre for Chronic Disease Prevention and Health Promotion [On-line]. Available: http://www.cdc.gov/tobacco/sgrpage.htm
Sutherland, G. (2002). Current approaches to the management of smoking cessation. Drugs, 62(Suppl. 2), 53-61.
Tashkin, D. P., Kanner, R., Bailey, W., Buist, S., Anderson, P., Nides, M. A. et al. (2001). Smoking cessation in patients with chronicobstructive pulmonary disease: A double-blind, placebo-controlled, randomised trial. Lancet, 357, 1571-1575.
Thomson, C. C. & Rigotti, N. A. (2003). Hospital- and clinic-based smoking cessation interventions for smokers withcardiovascular disease. Progress in Cardiovascular Diseases, 2003 May-Jun; 45, 459-479.
Tompkins, N. O., Dino, A., Zedosky, L. K., Harman, M., & Shaler, G. (1999). A collaborative partnership to enhanceschool-based tobacco control policies in West Virginia. American Journal of Preventive Medicine, 16(3S), 29-34.
Ussher, M., West, R., McEwen, A., Taylor, A., & Steptoe, A. (2003). Efficacy of exercise counselling as an aid for smokingcessation: A randomized controlled trial. Addiction, 98, 523-532.
U. S. Department of Health and Human Services Public Health Service. (2000). Quick reference guide for clinicians: Treatingtobacco use and dependence. Centers for Disease Control and Prevention [On-line].Available: http://www.phppo.cdc.gov/c.../showarticle.asp?a_artid=1292++++&TopNum=50&CallPg=Adv
United States Preventive Services Task Force – Federal Government Agency, U.S. (1996). Counselling to prevent tobacco use.National Guideline Clearinghouse [On-line]. Available: www.guideline.gov/index.asp
Wadland, W. C., Soffelmayr, B., & Ives, K. (2001). Enhancing smoking cessation of low-income smokers in managed care.Journal of Family Practice, 50, 138-144.
Wetter, D. W., Fiore, M. C., Gritz, E., Lando, H. A., Stitzer, M. L., Hasselblad, V. et al. (1998). The Agency for Healthcare Policyand Research smoking cessation clinical practice guideline. American Psychological Association, 53, 657-669.
Whitlock, E. P., Orleans, C. T., Pender, N., & Allan, J. (2002). Evaluating primary care behavioural counselling interventions: Anevidence-based approach. American Journal of Preventive Medicine, 22, 267-284.
Wilson, D. M. (1999). Steps of smoking cessation: Steps of change. The example of a “closet smoker”. Patient CareCanada, 10, 44-57.
Windsor, R. A., Woodby, L. L., Miller, T. M., Hardin, J. M., Crawford, M. A., & DiClemente, C. C. (2000). Effectiveness ofAgency for Healthcare Policy and Research clinical practice guideline and patient education methods for pregnant smokers inMedicaid maternity care. American Journal of Obstetrics and Gynecology, 182 (Number I, Part I), 68-75.
Young, J. M. & Ward, J. E. (2001). Implementing guidelines for smoking cessation advice in Australian general practice:Opinions, current practices, readiness to change and perceived barriers. Family Practice, 18(1), 14-20.
Young, J. M. & Ward, J. (2002). Can distance learning improve smoking cessation advice in family practice? A randomized trial.Journal of Continuing Education in the Health Professions, 22, 84-93.
Zhu, S. H., Anderson, C. M., Tedeschi, G. J., Rosbrook, B., Johnson, C. E., Byrd, M. et al. (2002). Evidence of real-worldeffectiveness of a telephone quitline for smokers. New England Journal of Medicine, 347, 1087-1093.
Nursing Best Practice Guideline
Appendix A: Search Strategyfor Existing EvidenceThe search strategy utilized during the revision of this guideline focused on two key areas. One was the
identification of new guidelines published on the topic smoking cessation since the original guideline was
published in 2003, and the second was to identify systematic reviews and primary studies published in this
area from 2003 to 2006.
STEP 1 – DATABASE SearchA database search for existing evidence related to smoking cessation was conducted by a university health
sciences library. An initial search of the Medline, Embase and CINAHL databases for guidelines and studies
published from 2003 to 2006 was conducted in March 2006, using the following search terms and key
words: “smoking cessation”, “smoking addiction(s)”, “relapse”, “practice guidelines”, “practice guideline”,
“clinical practice guideline”, “clinical practice guidelines”, “standards”, “consensus statement(s)”,
“consensus”, “evidence based guidelines” and “best practice guidelines”. In addition, a search of the
Cochrane Library database for systematic reviews was conducted using the above search terms.
STEP 2 – Structured Website SearchOne individual searched an established list of websites for guidelines related to the topic area in April 2006.
This list of sites, reviewed and updated in April 2006, was compiled based on existing knowledge of
evidence-based practice websites, known guideline developers, and recommendations from the literature.
Presence or absence of guidelines was noted for each site searched as well as date searched. The websites
at times did not house a guideline but directed to another website or source for guideline retrieval.
Guidelines were either downloaded if full versions were available or were ordered by phone/email.
■ Agency for Healthcare Research and Quality: http://www.ahrq.gov
■ Alberta Heritage Foundation for Medical Research - Health Technology Assessment: http://www.ahfmr.ab.ca//hta
■ Alberta Medical Association - Clinical Practice Guidelines: http://www.albertadoctors.org
■ Bandolier Journal: http://www.jr2.ox.ac.uk/bandolier
■ British Columbia Council on Clinical Practice Guidelines: http://www.hlth.gov.bc.ca/msp/protoguides/index.html
■ Canadian Coordinating Office for Health Technology Assessment: http://www.ccohta.ca
■ Canadian Institute of Health Information: http://www.cihi.ca
■ Canadian Health Network: www.canadian-health-network.ca
■ Centers for Disease Control and Prevention: http://www.cdc.gov
■ Clinical Evidence: www.clinicalevidence.com
■ CMA Infobase: Clinical Practice Guidelines: http://mdm.ca/cpgsnew/cpgs/index.asp
■ Cochrane Database of Systematic Reviews: www.thecochranelibrary.com
■ Database of Abstracts of Reviews of Effectiveness (DARE): http://www.update-software.com/cochrane
■ European Observatory on health Care for Chronic Conditions, World Health Organization:
http://www.euro.who.int/observatory/About/london/20041215_3
■ Evidence-based On-Call: http://www.eboncall.org
■ Guidelines Advisory Committee: http://gacguidelines.ca
■ Guidelines International Network: www.g-i-n.net
Integrating Smoking Cessation into Daily Nursing Practice
54

55
■ Institute for Clinical Systems Improvement: http://www.icsi.org/index.asp
■ Institute for Clinical Evaluative Sciences: www.ices.on.ca
■ Joanna Briggs Institute: http://www.joannabriggs.edu.au
■ Medic8.com: http://www.medic8.com/ClinicalGuidelines.htm
■ Monash University Centre for Clinical Effectiveness: http://www.mihsr.monash.org/cce
■ National Electronic Library for Health: http://www.nelh.nhs.uk
■ National Guideline Clearinghouse: http://www.guidelines.gov
■ National Institute for Clinical Excellence (NICE): http://www.nice.org.uk
■ New Zealand Guidelines Group: http://www.nzgg.org.nz
■ NHS Centre for Reviews and Dissemination: http://www.york.ac.uk/inst/crd
■ NHS R & D Health Technology Assessment Programme: http://www.hta.nhsweb.nhs.uk/htapubs.htm
■ NIH Consensus Development Program: http://consensus.nih.gov/about/about.htm
■ PEDro: The Physiotherapy Evidence Database: http://www.pedro.fhs.usyd.edu.au/index.html
■ Periodic Task Force on Preventive Health Care: http://www.ctfphc.org
■ Queen’s University at Kingston: http://post.queensu.ca/~bhc/gim/cpgs.html
■ Royal College of General Practitioners: http://www.rcgp.org.uk
■ Royal College of Nursing: http://www.rcn.org.uk/index.php
■ Royal College of Physicians: http://www.rcplondon.ac.uk
■ Sarah Cole Hirsh Institute – Online Journal of Issues in Nursing: http://fpb.cwru.edu/HirshInstitute
■ Scottish Intercollegiate Guidelines Network: http://www.sign.ac.uk
■ SUMSearch: http://sumsearch.uthscsa.edu
■ The Qualitative Report: http://www.nova.edu/ssss/QR
■ TRIP Database: http://www.tripdatabase.com
■ U.S. Preventive Service Task Force: http://www.ahrq.gov/clinic/uspstfix.htm
■ University of California, San Francisco: http://medicine.ucsf.edu/resources/guidelines/index.html
■ University of Laval – Directory of Clinical Information Websites: http://132.203.128.28/medecine
■ Virginia Henderson International Nursing Library: www.nursinglibrary.org
STEP 3 – Search Engine Web SearchA website search for existing practice guidelines on smoking cessation was conducted via the search engine
“Google”, using key search terms. One individual conducted this search, noting the results of the search, the
websites reviewed, date and a summary of the results. The search results were further reviewed by a second
individual who identified guidelines and literature not previously retrieved.
STEP 4 – Hand Search/Panel Contributions Additionally, panel members were asked to review personal archives to identify guidelines not previously found
through the above search strategy. Results of this strategy revealed no additional clinical practice guidelines.
SEARCH RESULTS:The search strategy described above resulted in the retrieval of 362 abstracts on the topic of smoking
cessation. These abstracts were then screened by a research assistant related to duplications and
inclusion/exclusion criteria. A total of 83 abstracts were identified for article retrieval and critical appraisal.
Nursing Best Practice Guideline
In addition, four recently published clinical practice guidelines were identified for review and critical
appraisal by the panel, using the “Appraisal of Guidelines for Research and Evaluation” (AGREE
Collaboration, 2001) instrument. These guidelines included:
■ Institute for Clinical Systems Improvement. (2004). Tobacco use prevention and cessation for adults and
mature adolescents. Bloomington, MN: Institute for Clinical Systems Improvement (ICSI).■ National Advisory Committee on Health and Disability. (2002) Guidelines for smoking cessation: (Revised
2002.) Wellington, NZ: National Advisory Committee on Health and Disability (National Health Committee).■ Singapore Ministry of Health. (2002). Smoking cessation. Singapore: Singapore Ministry of Health.■ National Institute for Health and Clinical Excellence. (2006) Brief interventions and referral for smoking
cessation in primary care and other settings. National Institute for Health and Clinical Excellence.
Integrating Smoking Cessation into Daily Nursing Practice
56

57
Nursing Best Practice Guideline
Appendix B: Glossary of TermsAcupuncture: A treatment involving the placement of needles in specific areas of the body, in this
instance with the intent to promote abstinence from tobacco use.
Bupropion HCI (bupropion sustained-release) (Zyban®): A non-nicotine
aid to smoking cessation originally developed and marketed as an antidepressant. It is chemically
unrelated to tricyclics, tetracyclics, selective serotonin re-uptake inhibitors and other known
antidepressant medications. Its mechanism of action is presumed to be mediated through its
capacity to block the re-uptake of dopamine and norepinephrine centrally.
Clonidine: An alpha-2-adrenergic agonist typically used as an anti-hypertensive medication, but
also documented in this guideline as an effective medication for smoking cessation. The U.S. Food
and Drug Administration (FDA) has not approved clonidine as a smoking cessation aid.
Continuous abstinence: A measure of tobacco abstinence based on whether subjects are
continuously abstinent from smoking/tobacco use from their quit day to a designated outcome point
(e.g., end of treatment, 6 months after the quit day).
Cotinine: Cotinine is nicotine’s major metabolite, which has a significantly longer half-life than
nicotine. This is often used to estimate a client’s tobacco/nicotine self-administration prior to
quitting, and to confirm abstinence self-reports during follow up. Cotinine can be measured in urine,
saliva or blood.
Dependence: Is defined by the DSM IV (American Psychiatric Association, 2000) as: tolerance to a
substance; withdrawal from a substance; taking a substance for a longer period and in larger amounts
than intended; having a persistent desire or unsuccessful efforts to cut down or control substance
use; spending a great deal of time obtaining, using or recovering from the effects of the substance,
giving up important social, occupational, or recreational activities because of substance use;
substance use continues despite knowledge of having a persistent or recurrent physical or
psychological problem that is likely to have been caused or exacerbated by the substance.
Diazepam: A benzodiazepine anxiolytic medication intended to reduce anxiety.
Environmental tobacco smoke (ETS): Also known as “second-hand smoke.” The
smoke inhaled by an individual not actively engaged in smoking, but due to exposure to ambient
tobacco smoke.
First-line pharmacotherapy for tobacco dependence: First-line pharmacotherapies
have been found to be safe and effective for tobacco dependence treatment and have been approved
by the FDA for this use. First-line medications have an established empirical record of efficacy,
and should be considered first as part of tobacco dependence treatment, except in cases
of contraindications.

Hotline/help-line: See telephone hotline/help-line.
Hypnosis (hypnotherapy): A treatment by which a healthcare provider attempts to induce an
altered attention state and heightened suggestibility in a tobacco user for the purpose of promoting
abstinence from tobacco use.
Informal support: Support and resources provided by persons associated with the individual
receiving care. Persons providing informal support can include: family, friends, members of a
religious group, and neighbours.
Intensive intervention: Refers to interventions that involve extended contact between
healthcare provider and client (greater than 10 minutes of time spent in intervention).
Interdisciplinary: A process where healthcare professionals representing expertise from various
healthcare disciplines participate in the support of clients/families in the care process.
Minimal intervention: Refers to interventions in which there is brief contact between
healthcare provider and client (1 to 3 minutes of time spent in intervention).
Motivational Interviewing: Is a directive, client-centred counselling style for eliciting
behaviour change by helping clients to explore and resolve ambivalence. Compared with
nondirective counselling, it is more focused and goal directed. Motivation to change is elicited from
the client not imposed from without by healthcare providers, peers, or others.
Nicotine: This is often used to assess a client’s tobacco/nicotine self-administration prior to quitting, and
to confirm abstinence self-reports during follow up. Nicotine can be measured in urine, blood and saliva.
Nicotine replacement therapy (NRT): Refers to a medication containing nicotine that is
intended to promote smoking cessation. The nicotine chewing gum, nicotine inhaler and nicotine
patch are currently approved for use in Canada.
Person-to-person intervention: In-person or face-to-face contact between a healthcare
provider and a client, for the purpose of tobacco use assessment or intervention.
Point prevalence: A measure of tobacco abstinence based on smoking/tobacco use occurrence
within a set time period (usually 7 days) prior to a follow-up assessment.
Practical counselling (problem solving/skills training): Refers to a tobacco use
treatment, in which tobacco users are trained to identify and cope with events or problems that increase
the likelihood of their tobacco use. For example, quitters might be trained to anticipate stressful events
and to use coping skills such as distraction or deep breathing to cope with an urge to smoke. Related and
similar interventions are coping skills training, relapse prevention and stress management.
Proactive telephone counselling: Treatment initiated by a healthcare provider who
telephones and counsels the client over the telephone.
Integrating Smoking Cessation into Daily Nursing Practice
58
59
Psychosocial interventions: Refers to intervention strategies that are designed to increase
tobacco abstinence rates due to psychological or social support mechanisms. These interventions
comprise such treatment strategies as counselling, self-help and behavioural treatment and
contingency contracting.
Quit day: The day of a given cessation attempt during which a client tries to abstain totally from
tobacco use. Also refers to a motivational intervention, whereby a client commits to quit tobacco use
on a specified day.
Relaxation/breathing: An intervention strategy in which clients are trained in relaxation
techniques. Interventions using meditation and breathing exercises fit this category. This category
should be distinguished from the category of problem solving, which includes a much wider range of
stress-reduction/management strategies.
Second-hand smoke: See “environmental tobacco smoke”.
Second-line pharmacotherapy for tobacco dependence: Second-line medications
are pharmacotherapies for which there is evidence of efficacy for treating tobacco dependence, but
they have a more limited role than first-line medications. Second-line treatments should be
considered for use on a case-by-case basis, after first-line treatments have been used or considered.
Self-help: An intervention strategy in which the client uses a non-pharmacologic, physical aid to
achieve abstinence from tobacco. Self-help strategies typically involve little contact with a healthcare
provider, although some strategies (e.g., hotline/help-line) involve client-initiated contact. Examples
of types of self-help materials include: pamphlets, booklets, mailings, manuals, videos, audio tapes,
referrals to 12-step programs, mass media community-level interventions, list of community
programs, reactive telephone hotlines/help-lines and computer programs/internet resources.
Smokeless tobacco: Any used form of unburned tobacco, including chewing tobacco and snuff.
Smoking cessation: Smoking cessation is a process whereby a person who uses tobacco
products quits smoking and stops using tobacco products for a minimum of 24 hours.
Smoking cessation intervention: Smoking cessation intervention is formally identifying,
assisting, motivating and advising the person who smokes to become, and remain, smoke-free.
Telephone hotline/help-line: A reactive telephone line dedicated to over-the-phone smoking
intervention. A hotline/help-line treatment occurs when a hotline/help-line number is provided to a
client, or a referral to a hotline/help-line is made. The key distinction between hotline/help-line and
proactive telephone counselling is that in the former the client must initiate clinical contact.
Transdermal nicotine: Refers to delivery of nicotine by diffusion through the skin. Often used
as a synonym for a “nicotine patch.”
Nursing Best Practice Guideline

Appendix C: The Health Risks of SmokingToxic Components of cigarettesExposure to these chemicals occurs whenever a tobacco product is burned:
■ Tar■ Nicotine■ Carbon monoxide■ Formaldehyde■ Hydrogen cyanide■ Benzene
For further details on the toxic components of cigarettes, visit Health Canada’s Toxic Emissions Statement,
webpage at: http://www.hc-sc.gc.ca/hl-vs/tobac-tabac/legislation/label-etiquette/tox/index_e.html
■ More than 47,000 people die prematurely each year in Canada due to tobacco use.■ The average person who smokes will die about eight years earlier than a similar non-smoker.
Tobacco use increases the risk of:
1. Cardiovascular disease 7. Rheumatologic conditions
2. Cancers 8. Kidney damage
3. Respiratory diseases 9. Type 2 Diabetes
4. Adverse effects in pregnancy 10. Skin conditions
and early childhood 11. Cataracts
5. Gastrointestinal problems 12. Tooth and gum problems
6. Orthopedic conditions
1. Cardiovascular Disease■ About 30 percent of all heart disease deaths are due to smoking. ■ Smoking accounts for about three quarters of all cases of peripheral vascular disease. The risk of peripheral
vascular disease may be as much as 16 times higher in persons who smoke than in those who do not.■ Smoking is a dominant cause of heart disease, stroke and diseases of the blood vessels.■ Each year in Canada, more than 17,600 cardiovascular deaths result from smoking.■ Each year in Canada, more than 2,000 deaths from stroke result from smoking.■ Many of these deaths occur prematurely, before the age of 70.■ The incidence of coronary heart disease (CHD) is 2 to 4 times greater in smokers. ■ Health Canada estimates that at least 700 non-smokers will die each year of coronary heart disease
caused by exposure to second-hand smoke.■ Smoking is a major risk factor for heart attacks and sudden cardiac death.■ Smoking acts synergistically with other risk factors (high cholesterol and blood pressure) to increase
the risk of CHD.■ Smoking increases the risk of recurrence in persons who have survived a heart attack.■ Smoking increases the risk of stroke in women more so than men.■ Quitting smoking substantially reduces the risk of CHD and stroke.
Integrating Smoking Cessation into Daily Nursing Practice
60

61
2. Cancers■ Smoking is responsible for more than 21,000 deaths (Canadian Cancer Society et al., 2000) from cancer
each year, almost 30 percent of all cancer deaths. The risk of developing cancer increases with duration
of smoking, number of cigarettes smoked per day and degree of inhalation. The risk of lung cancer is
significantly reduced with smoking cessation in comparison to those individuals who continue to smoke.■ Smoking causes cancer of the lung, oral cavity, larynx, esophagus, pancreas, kidney and urinary bladder.■ Recent evidence links smoking with cancer of the large intestine and some forms of leukemia. Tobacco
causes 80 to 85 percent of all lung cancers and 30 percent of the total cancer burden.■ Smokeless tobacco is a major cause of cancer of the mouth.■ Cigarette smoking is estimated to account for about 30 to 40 percent of bladder cancers.■ Since 1993, lung cancer exceeded breast cancer as the leading cause of cancer deaths in Canadian women.
3. Respiratory Diseases■ Each year smoking is responsible for more than 8,000 deaths in Canada from respiratory diseases.
Chronic Obstructive Pulmonary Disease (COPD) includes chronic bronchitis, chronic airway
obstruction, emphysema and related disorders. Persons with these conditions often suffer long periods
of disability marked by progressive shortness of breath and limitations in daily activities.■ Smoking accounts for 80 to 90 percent of all COPD deaths.■ Smoking far outweighs all other factors, including air pollution and occupational exposures, in causing
these conditions.■ Smoking depresses the body’s immune system and other defense mechanisms.■ Smokers are at increased risk of respiratory infections compared to non-smokers.■ Smoking may increase susceptibility to the common cold.
4. Adverse Effects in Pregnancy and Early Childhood■ Bleeding during pregnancy.■ Ectopic pregnancy.■ Miscarriage.■ Premature delivery.■ Stillbirth.■ Abnormalities of the placenta.
■ An increased risk of childhood allergies.■ Higher blood pressure in childhood. ■ A greater likelihood of obesity. ■ Being shorter in childhood. ■ Poorer lung function. ■ A greater likelihood that the child will have asthma.■ Women who smoke during pregnancy risk complications including.■ Low birth-weight newborn (less than 2500 grams).■ Babies receive nicotine and carbon monoxide from their mother’s blood.■ Smoking may contribute to Sudden Infant Death Syndrome (SIDS).■ Nicotine and other chemical components of cigarette smoke are found in the breast milk of nursing
mothers who smoke or are exposed to environmental tobacco smoke (ETS).■ Smoking appears to decrease the quantity of breast milk which, combined with the effects on the
quality of breast milk, may lead to early weaning.
Nursing Best Practice Guideline

5. Gastrointestinal Problems■ Peptic ulcer disease is more likely to occur in smokers than non-smokers.■ When ulcers are present, they heal less readily in smokers and are likely to recur.■ Smoking increases the risk of death from ulcers.■ Smoking is a risk factor for Chronic Bowel Disease and Crohn’s Disease.
6. Orthopedic Conditions■ Osteoporosis
■ Smoking increases the chances of developing osteoporosis and of breaking bones. Smoking
decreases the amount of calcium absorbed from food.
7. Rheumatologic Conditions■ Rheumatoid arthritis.
8. Kidney Damage■ Smoking worsens kidney damage in people who have medical problems that affect the kidneys, such
as diabetes or high blood pressure.
9. Type 2 Diabetes ■ Persons who smoke are at least 50 percent more likely than nonsmokers to get Type 2 diabetes.■ Among people who have diabetes, those who smoke are more likely to develop diabetes-related kidney
damage, nerve damage, eye problems and heart disease.
10. Skin Conditions■ Contact allergies occur more often in persons who smoke than in those who do not.
11. Cataracts
12. Tooth and Gum Problems■ Smoking causes oral cancer.■ Smokers are more likely than non-smokers to lose their natural teeth, for their remaining teeth to be
decayed, and to have significant gum loss (periodontal disease).
Additional Hazards for Males■ Erectile dysfunction.
■ Men who smoke are about twice as likely as men who don’t smoke to suffer from erectile
dysfunction and impotence. ■ Fertility may be impaired in men who smoke.
Additional Hazards for Women■ Smoking is a risk for cancer of the cervix.■ Natural menopause occurs earlier.■ Smoking increases the risk of menstrual disorders.■ Fertility may be impaired in women who smoke.■ Smoking, and the use of oral contraceptives, greatly increases the risk of strokes, heart attacks and
other vascular complications.
Integrating Smoking Cessation into Daily Nursing Practice
62
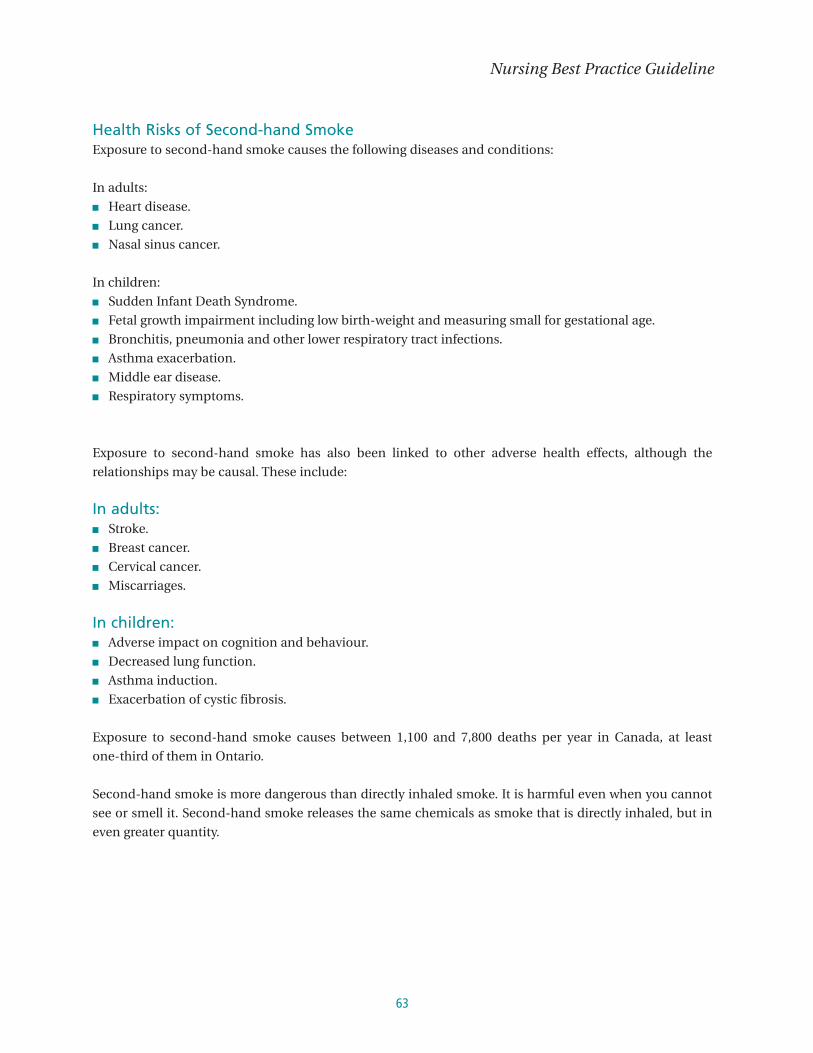
63
Health Risks of Second-hand SmokeExposure to second-hand smoke causes the following diseases and conditions:
In adults:■ Heart disease.■ Lung cancer.■ Nasal sinus cancer.
In children:■ Sudden Infant Death Syndrome.■ Fetal growth impairment including low birth-weight and measuring small for gestational age.■ Bronchitis, pneumonia and other lower respiratory tract infections.■ Asthma exacerbation.■ Middle ear disease.■ Respiratory symptoms.
Exposure to second-hand smoke has also been linked to other adverse health effects, although the
relationships may be causal. These include:
In adults:■ Stroke.■ Breast cancer.■ Cervical cancer.■ Miscarriages.
In children:■ Adverse impact on cognition and behaviour.■ Decreased lung function.■ Asthma induction.■ Exacerbation of cystic fibrosis.
Exposure to second-hand smoke causes between 1,100 and 7,800 deaths per year in Canada, at least
one-third of them in Ontario.
Second-hand smoke is more dangerous than directly inhaled smoke. It is harmful even when you cannot
see or smell it. Second-hand smoke releases the same chemicals as smoke that is directly inhaled, but in
even greater quantity.
Nursing Best Practice Guideline
References:1. Anda RF, Williamson D.F., Escobedo L.G., Remington .PL. (1990). Smoking and the risk of peptic ulcer disease among
women in the United States. Archives of Internal Medicine, 1990, 150, 1437-1441.
2. Ayanian J.Z., Cleary P.D. Perceived risks of heart disease and cancer among cigarette smokers. Journal of the AmericanMedical Association, 1999, 281, 1019-1021.
3. Barry J., Mead K., Nabel E.G., Rocco M.B., Campbell S., Fenton T., Mudge G.H. Jr. Effect of smoking on the activity ofischemic heart disease. Journal of the American Medical Association, 1989, 261, 398-402.
4. Brodish, P.H. (1998). The irreversible health effects of cigarette smoking. American Council on Science and Health [On-line].Available: http://www.acsh.org/publications/booklets/iesmoke.pdf*
5. Burke K.E. (1990). Facial wrinkles: Prevention and nonsurgical correction. Postgraduate Medicine, 88, 207-228.
6. Canadian Cancer Society. (2003). Canadian cancer statistics. Canadian Cancer Society [On-line]. Available: www.cancer.ca
7. Cole C.W., Hill G.B., Farzad E., Bouchard A., Moher D., Rody K., Shea B. (1993). Cigarette smoking and peripheral arterialocclusive disease. Surgery, 114, 753-757.
8. Health Canada. (2003). Facts about tobacco. Health Canada [On-line].Available: www.hc.-sc.ca/hecs-sesc/tobacco/facts/index.html*
9. Koh J.S., Kang H., Choi S.W., Kim H.O. (2002). Cigarette smoking associated with premature facial wrinkling: imageanalysis of facial skin replicas. International Journal of Dermatology, 41, 21-27.
10. McVary M.T., Carrier S., Wessels H.; Subcommittee on Smoking and Erectile Dysfunction Socioeconomic Committee, SexualMedicine Society of North America. (2001) Smoking and erectile dysfunction: evidence based analysis. Journal of Urology,166, 1624-1632.
11. Ontario Tobacco Research Unit – University of Toronto. (2001). Protection from second-hand tobacco smoke in Ontario – Areview of the evidence regarding best practices. National Clearinghouse on Tobacco and Health Programs [On-line].Available: http://www.ncth.ca*
12. Ontario Tobacco Research Unit. (1995). Facts on Tobacco: Prevention, protection and cessation. Toronto, Ontario: AddictionResearch Foundation of Ontario.
13. Salminen E., Pukkala E., Teppo L. (1994). Bladder cancer and the risk of smoking-related cancers during followup. Journalof Urology, 152, 1420-1423.
14. Saraiya M., Berg C.J., Kendrick J.S., Strauss L.T., Atrash H.K., Ahn Y.W. Cigarette smoking as a risk factor for ectopicpregnancy. American Journal of Obstetrics and Gynecology, 1998, 178, 493-498.
15. Schabas, R.E. (1996). Tobacco: Sounding the alarm: Report of the Chief Medical Officer of Health, Ottawa: Queen’s Printerof Ontario.
16. Schmitz M.A., Finnegan M., Natarajan R., Champine J. (1999) Effect of smoking on tibial shaft fracture healing. ClinicalOrthopedics, 365, 184-200.
17. World Health Organization. (1995). Tobacco costs more than you think. World no-tobacco day. World Health Organization.
* At the time of the original publication, these resources were retrieved at the web addresses above. These links mayno longer be active.
Integrating Smoking Cessation into Daily Nursing Practice
64
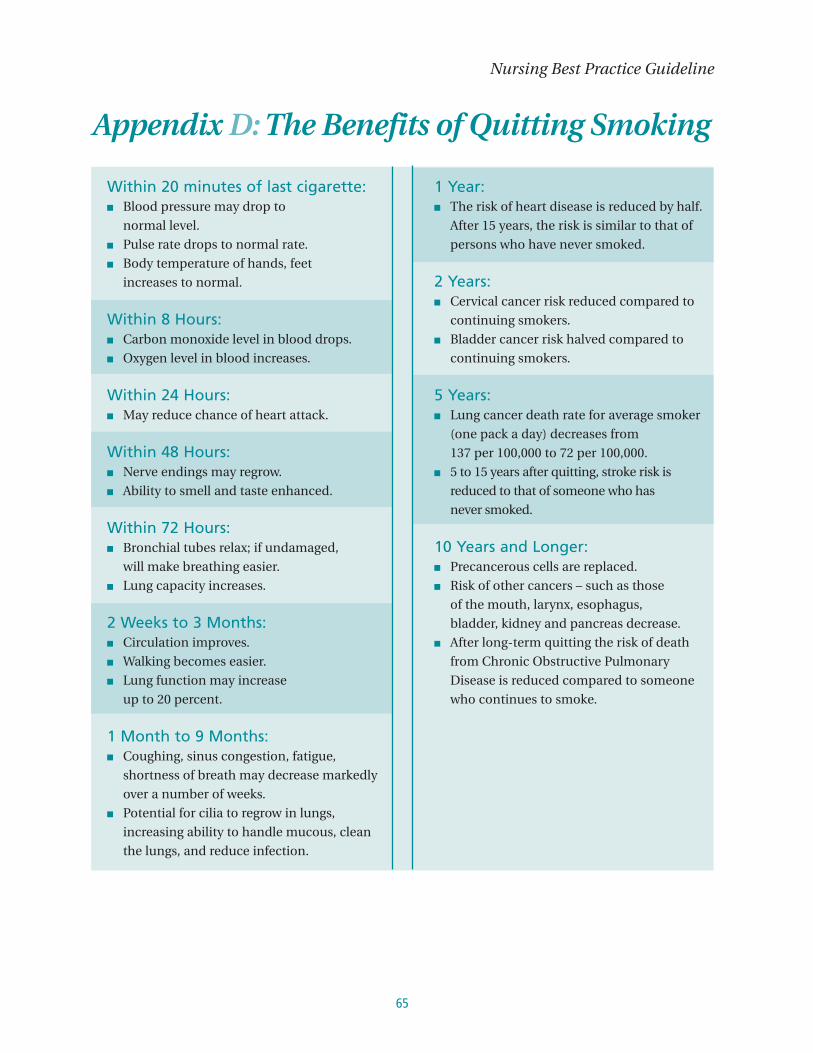
65
Nursing Best Practice Guideline
Within 20 minutes of last cigarette:■ Blood pressure may drop to
normal level.■ Pulse rate drops to normal rate.■ Body temperature of hands, feet
increases to normal.
Within 8 Hours:■ Carbon monoxide level in blood drops.■ Oxygen level in blood increases.
Within 24 Hours:■ May reduce chance of heart attack.
Within 48 Hours:■ Nerve endings may regrow.■ Ability to smell and taste enhanced.
Within 72 Hours:■ Bronchial tubes relax; if undamaged,
will make breathing easier.■ Lung capacity increases.
2 Weeks to 3 Months:■ Circulation improves.■ Walking becomes easier.■ Lung function may increase
up to 20 percent.
1 Month to 9 Months:■ Coughing, sinus congestion, fatigue,
shortness of breath may decrease markedly
over a number of weeks.■ Potential for cilia to regrow in lungs,
increasing ability to handle mucous, clean
the lungs, and reduce infection.
1 Year:■ The risk of heart disease is reduced by half.
After 15 years, the risk is similar to that of
persons who have never smoked.
2 Years:■ Cervical cancer risk reduced compared to
continuing smokers.■ Bladder cancer risk halved compared to
continuing smokers.
5 Years:■ Lung cancer death rate for average smoker
(one pack a day) decreases from
137 per 100,000 to 72 per 100,000.■ 5 to 15 years after quitting, stroke risk is
reduced to that of someone who has
never smoked.
10 Years and Longer:■ Precancerous cells are replaced.■ Risk of other cancers – such as those
of the mouth, larynx, esophagus,
bladder, kidney and pancreas decrease.■ After long-term quitting the risk of death
from Chronic Obstructive Pulmonary
Disease is reduced compared to someone
who continues to smoke.
Appendix D: The Benefits of Quitting Smoking

Time periods mentioned are to be taken as a general measure only and will naturally vary from individual
to individual and are dependent upon length of habit and amount of cigarettes smoked.
Reprinted with permission. Public Health and Long-Term Care Branch – City of Ottawa (2006). Health Benefits of QuittingSmoking. Ottawa, Ontario: Public Health and Long-Term Care Branch – City of Ottawa.
Originally adapted from:
1. Summary of the Health Benefits of Smoking cessation: A report of the Surgeon General, (1990). CDC, U.S. PublicHealth Services.
2. American Cancer Society, New York Times.
3. Metropolitan Toronto Interagency Council on Smoking and Health.
Integrating Smoking Cessation into Daily Nursing Practice
66

67
Appendix E: Stages of Change ModelPre-contemplation■ Unaware or unwilling to change.■ Not thinking of quitting in the next 6 months.
Goal:■ To help the client begin to think seriously about quitting .
What to do■ ASK regarding feelings about smoking.■ ASK about the pros and possible cons of smoking.■ ADVISE by offering quitting information and assistance at any time.
Contemplation■ Ambivalent, but thinking about quitting within 6 months.
Goal:■ To help smoker move towards a decision to stop smoking.■ To help the client feel more confident.
What to do■ ASK about the pros and cons of both continuing to smoke and quitting■ (decision balance).■ Acknowledge ambivalent feelings.■ ASSIST by reinforcing their reasons for change, and exploring new ones.■ Suggest they cut back or stop for a day.■ ASSIST by offering a future visit and information.
Preparation■ Getting ready to stop within the next 30 days.■ Have set stop smoking date.■ Have made a 24 hour quit attempt in the last 12 months.
Goal:■ To help smoker prepare for and anticipate positively a quit date.
What to do■ ASK about concerns, preparations and lessons learned from previous attempts.■ ADVISE by identifying barriers to stopping and elicit solutions.■ ASSIST by Booklet, Action Plan, Nicotine Replacement, Date for quitting (BAND).
Nursing Best Practice Guideline

Action■ Have quit smoking within past 6 months and are actively applying cessation skills.
Goal:■ To help client stay off tobacco products and recover from relapses.
What To Do■ ASK how the client is doing: relapses, temptations, successes, NRT use.■ ADVISE re: relapse prevention, weight gain, triggers.■ ASSIST by focusing on successes, encourage self rewards and increase support, elicit solutions for problems.
Maintenance■ Quit for more than 6 months.■ Integrating smoke-free living into their routine.
Goal:■ To help client remain smoke-free for a life time.
What To Do■ ASK how the client is doing: risk situations, relapses.■ ASSIST by offering suggestions for difficult times, support, encouragement.■ Congratulate!
The Cycle of Change■ Most smokers will cycle through the stages 3 to 4 times before quitting for life.■ Each attempt offers new opportunities to learn new skills and new techniques that will help them
in their next attempt.
Relapse: a normal event in the process of making behavioural change
Reference:Canadian Council on Smoking and Health. (2003). Guide your patients to a smoke-free future: A program of the CanadianCouncil on Smoking and Health. Ottawa, Ontario: Canadian Council on Smoking and Health.
Prochaska, J.O. & DiClemente, C.C. (1983). Stages and processes of self-change of smoking. Toward an integrative modelof change. Journal of Counselling and Clinical Psychology, 51(3), 390-395.
University of Toronto Department of Family & Community Medicine. (1998). Project CREATE: Smoking cessation module.(Vols. 3) Toronto, Ontario: Project CREATE.
Integrating Smoking Cessation into Daily Nursing Practice
68

69
Appendix F: Identifying Your Client’sReadiness to Quit
Question: Have you quit smoking cigarettes? Check one:
Answer Stage❏ Yes, I have, for more than 6 months. ❏ Defines maintenance.
❏ Yes, I have, but for less than 6 months ❏ Defines action.
❏ No, but I intend to in the next 30 days ❏ Defines preparation.
and have tried for at least 24 hours in
the past year.
❏ No, but I intend to in the next 6 months ❏ Defines contemplation.
❏ No, and I do not intend to in the ❏ Defines pre-contemplation.
next 6 months.
Reprinted with permission. Program Training and Consultation Centre (1995). Info Pack: Understanding and using the stages ofchange. Ottawa, ON: Ontario Tobacco Strategy.
Nursing Best Practice Guideline

Appendix G: Motivational InterviewingAdapted from the Heart and Stroke Foundation of Ontario and RNAO’s Nursing Management of
Hypertension (2005) guideline.
Motivational Interviewing is a focused, goal directed client-centred counselling style for eliciting
behaviour change by helping clients explore and resolve ambivalence (Miller & Rollnick, 1991; Rollnick & Miller,
1995). To enhance motivation and change, motivational interviewing, through an assessment of the change
process, systematically directs the client toward motivation for change; offers advice and feedback where
appropriate, selectively uses empathic reflection to reinforce certain processes, and seeks to elicit and
amplify the client’s discrepancies about their unhealthy behaviour(s). Motivational interviewing is
facilitative rather than coercive and tentatively challenging rather than directly confrontational. The
strategies support the client through the change process by fostering self-reflection rather than arguments
between practitioner and client (Botelho & Skinner, 1995).
Searching for a method to facilitate behaviour change in clients with substance abuse, psychologists
William Miller and Stephen Rollnick developed motivational interviewing. Behaviour change should be
negotiated, not dictated. Healthcare practitioners do not motivate clients, but assess motivation and apply
the appropriate skills and strategies to address readiness to change. This point is critical. Clients vary in
their readiness to change a behaviour (e.g., take medications, make lifestyle changes) and must be assessed
to determine how prepared they are to do what is needed to integrate change into their lives. How
important do they think the changes are? Are they confident they can do so? Will they need help? Do they
understand the benefits? What barriers do they perceive? How will they reduce them? By assessing the
degree of readiness, nurses can choose specific communication skills and appropriate strategies to
facilitate change. This is the heart of motivational interviewing (Berger, 2004a,b). The role of the nurse is to
understand and accept, in a non-judgmental way, clients’ needs and concerns and not be coercive by
trying to talk them in or out of these behaviours. This will create a favourable and supportive climate for
change – problems are attacked, not people.
Motivational interviewing, designed to take 3-5 minutes per session, is a psychosocial or socio-behavioural
approach to client care that contrasts with the traditional biomedical approach. The psychosocial model is
client-centred and stresses that the client’s needs and concerns must be appropriately addressed;
otherwise, non-adherence may occur. Asking if there are questions or concerns the client may have about
the illness or treatments is a positive way of assessing this possibility. The psychosocial model also views
the encounter between client and healthcare provider as a meeting of experts. The nurse or other
healthcare providers may be an expert on disease management, but clients are experts on themselves and
how they will be affected by the proposed changes in their lives. It is the client’s decision (with input from
healthcare providers) to choose healthy or unhealthy behaviours. Clients manage their illness, not nurses.
However, nurses can create an environment through caring, sufficient information, and understanding to
improve the chance that the client will manage their illness effectively (Berger, 2004a,b).
Change and resistance are opposite sides of the same coin. Change often evokes resistance because change
inherently questions one’s motivation and ability to do what is needed. If the pros of the change outweigh the
cons, clients will make the change. Alternatively, ambivalence kills change. When people are ambivalent, they
do nothing. The pros and cons of the change seem the same. Some examples of ambiguity are: client doubts
Integrating Smoking Cessation into Daily Nursing Practice
70

71
that the medication will actually work; they are unclear about what to do; or if they doubt they have the
necessary skills. Resistance is information and provides insight into what the person is thinking and feeling: “I
need to explore this and see if it works for me.” Exploring and understanding what has been said with the client,
not persuasion or criticism, are the keys to managing resistance. If nurses try to move people too quickly
toward a behaviour change, they will dig in and resist. An appropriate response to a client who indicates that
he/she does not want to take a medication would be: “What bothers you the most about taking this medicine?”
This way the client can explain their reasoning, and the nurse can specifically address his/her concern.
Motivational interviewing creates dissonance in a person. Dissonance, or an inconsistency between two
behaviours (attitudes, values, etc.), creates a discomfort that, in itself, can be motivating. For example, if a
person’s attitudes are inconsistent with their behaviours, dissonance occurs. Dissonance is uncomfortable
and the person may be motivated to explore ways to reduce this uncomfortable feeling. The spirit of
motivational interviewing is collaboration, evocation and autonomy. Healthcare professionals using this
approach desire a relationship with the client in which they can collaborate on mutually agreed upon goals.
Questions are asked to determine and understand the client’s resistance or ambivalence – the client knows
the answers, not the healthcare provider. Additionally, clients must make informed choices. It is not
enough to simply provide information. One needs to evaluate that the client has understood the
information, knows how to use it, and has a feeling of self-efficacy or confidence in their ability to do what
is needed. This includes assessing the client’s understanding of the illness and its treatment.
How does motivational interviewing work?Motivational interviewing uses the general process of elicit-provide-elicit. The nurse elicits information
from clients to better understand who they are and what they already know about the illness and its
management interventions. This is done to facilitate clients’ movement forward with the treatment plan.
Then, nurses elicit information again to check for concerns or questions resulting from the new information.
Motivational interviewing uses five principles or counselling techniques to assess and create motivation
within the client (Berger, 2004a,b; Miller & Rollnick, 1991; Smith, Heckemeyer, Kraft & Mason, 1997).
1. Express empathy – Empathy is defined as the “ability of the provider to accurately reflect what the
client is saying” (Moyers, 2000; p.155). Empathy is an objective identification with the affective state of
another (not his or her experience) – nurses identify with the client’s affect (emotions), not with the
experience. Empathetic responding, through active listening, helps identify and understand resistance and
reasons for unhealthy behaviours (or non-adherence). For example, your client smokes and you are
advising him to quit. You ask him what he likes about smoking, and he says it relaxes him. Instead of
creating defensiveness by asking, “Can’t you think of something else to relax you?” you state empathetically,
“It would be difficult to give up something that was relaxing.” As a result, the client sees you as an advocate,
and is in a better position to hear what you have to say.
2. Avoid arguments – By avoiding arguments, the client is more likely to see the healthcare provider
as being on his/her side. It is important to note that motivational interviewing is confrontational; however,
it should not be argumentative or judgmental. For example, “Mrs. Jones, I see that you have been getting
your medication refilled about every 40 days or so, but you receive only a 30-day supply. Can you tell me
what happened?” Also, it should be noted that feelings a client may express (e.g., fear or concern) are not
arguable but real for the client.
Nursing Best Practice Guideline

3. Develop discrepancy (dissonance) – Creating dissonance can be achieved in two major ways.
The goal is to elicit from the client those aspects of his or her life that are important but may be
compromised because of the behaviour. For example, the client may say that he or she enjoys going to the
bar and drinking with his or her friends for most of the weekend, and how he or she hates taking
medication especially those that do not make him or her feel well. In the next sentence, he or she may add
that since he or she was diagnosed as having high blood pressure, he or she is very worried about having a
stroke. The healthcare provider needs to understand what is important to the client in terms of short- and
long-term goals. Ask the client about the pros and cons of the changes that are needed and then listen
carefully for discrepancies that allow for the creation of dissonance. Remember, dissonance is motivating.
We develop discrepancies by repeating back the pros and cons as stated by the client. Then, ask the client
to discuss his or her goals relative to the treatment.
4. Roll with resistance – Ignore antagonistic elements in the client’s comments in order to focus on
the important underlying issues. For example, the client says, “Look, I haven’t had any real problems with
my smoking so far, so don’t worry about it.” Instead of rejecting this comment by saying, “If you continue
smoking, I can assure you that you will suffer some major consequences,” the healthcare provider can roll
with the expressed resistance by saying, “I hope your health continues to stay that way. I would like you to
consider getting your lungs checked because early stages of cancer and lung disease may not have
symptoms. That way, you can make a better decision about whether you want to keep smoking. I am
worried that your smoking is going to make your heart disease much worse in the future. However, the
decision to smoke or quit smoking is yours.” Do not meet resistance with confrontation but instead utilize
reflection to create dissonance. This allows the client to hear information without being chastised. In the
end, the decision belongs to the client.
5. Support self-efficacy – A person’s belief in the possibility of change (Bandura, 1977; 1982) is an
important motivator. Clients, based on their abilities and the resources and strengths they possess, need to
be encouraged by the healthcare provider. Questions such as: “What worked before?” or “What do you
think helped you to be successful last time?” provide valuable information about the client’s strengths.
Examine past successes (or failures) and offer genuine support for the successes. It is important to notice
not only actual changes in behaviour, but also contemplated changes, expressed in a positive manner. The
client must be able to imagine that success is a possibility before actually trying to change.
When using Motivational Interviewing,there are six general skills that should be utilized.
1. Asking open-ended questions: Asking questions in such a way that it is the client who is
encouraged to do most of the talking. Some examples: “What concerns you about your health?” or ”What
is it that you like about smoking” or “What reasons might you have for not quitting smoking?” or “Tell me
about the difficulties you encounter when trying to refill your prescriptions.” Miller and Rollnick (1991)
recommend not asking more than three questions in a row. Asking open-ended questions sets the stage for
reflective listening, affirmations and summation.
2. Reflective listening: As a foundational skill in motivational interviewing, reflective listening is
useful to address resistance. Reflections can be simple “you’re feeling sad” to more complex, “It sounds like
you are concerned what smoking all these years may have done to your overall health.” Reflective
Integrating Smoking Cessation into Daily Nursing Practice
72

73
statements, whether simple, amplified or double sided, tells the client that you have heard what he or she
is saying and encourages them to explore their feelings. Simple reflection acknowledges the client’s
thoughts, feelings and positions in a neutral manner.
3. Affirmations: Support for what the client is saying should occur frequently throughout the
conversation. Praising or complimenting and exploring past successes help to build a therapeutic relationship.
4. Summarizing or reframing: Reframing pulls the information together so that the client can reflect upon
it. By reframing, you tell the client that you have been listening and are open to exploring the situation further.
The summary links together the main points of the interview, both past and present. The ambivalence is
clear and the reflection in the end encourages the client to address the ambivalence (whether to continue
to struggle to get her prescriptions filled or ask someone to help).
5. Self-motivational statements: Clients must be responsible for change and motivated to
acknowledge ambivalence when change is being considered and set the stage for dialogue to occur. The
client argues the pros and cons of changing the behavour and the healthcare provider gets insight into the
client’s feelings and values as he listens to the argument.
6. Personalized feedback: This can be done on a one-to-one basis or through the use of standardized
tools; for example, a chart showing the change of blood pressure toward the target levels as the client
adheres to the goals set at a previous visit. The feedback must not be confrontational to the client. Instead,
the data will do the confronting if the client has not been adherent.
References:Bandura, A. (1977). Social learning theory. New York: General Learning Press.
Bandura, A. (1986). Social foundations of thought and action: A social cognitive theory. Englewood Cliffs, NJ: Prentice-Hall.
Berger, B.A. (2004a). Assessing and interviewing patients for meaningful behavior change. Part 1. The Case Manager, 15(5), 46-50.
Berger, B.A. (2004b). Assessing and interviewing patients for meaningful behavior change. Part 2. The Case Manager, 15(5), 58-62.
Botelho, R.J. & Skinner, H. (1995). Motivating change in health behavior. Implications for health promotion and dieseaseprevention. Primary Care, 22(4), 565-589.
Heart and Stroke Foundation of Ontario and Registered Nurses’ Association of Ontario. (2005). Nursing Management ofHypertension. Toronto, Canada: Heart and Stroke Foundation and Registered Nurses’ Association of Ontario.
Miller, W. & Rollnick, S. (1991). Motivational interviewing: Preparing people to change addictive behavior. New York:The Guilford Press.
Rollnick, S. & Miller, W. (1995). What is motivational interviewing? Behavioural and Cognitive Psychotherapy, 23, 325-334.
Smith, D., Heckemeyer, C., Kratt, P., & Mason, D. (1997). Motivational interviewing to improve adherence to a behaviouralweight control program for older obese women with NIDDM: A pilot study. Diabetes Care, 20, 52-54.
Nursing Best Practice Guideline

ARRANGEFollow-up
or refer client to smoking cessation program.
Support use of telephone counselling or community/public health programs.
Integrating Smoking Cessation into Daily Nursing Practice
74
Minimal Intervention 1 – 3 minutes
Provide basic information about smoking
and successful stopping■ Referral to community resource.■ Pharmacotherapy, i.e. NRT
(for hospitalized patients this should
be a standard of care)■ Self-help material.■ Referral to other healthcare provider.■ Smokers’ Helpline (1-877-513-5333).
Intensive InterventionPersonalize tobacco use to current health OR illness,
readiness to stop and the impact of tobacco use on
others in the household (social and economic costs).
Discuss strategies to quit and treatment options –
check client preferences■ Determine & discuss the stage of change.■ Reasons for smoking (WHY Test).■ Nicotine Dependence (Fagerstrom Test).■ Offer information re:
pharmacotherapy options.■ Set a quit date.■ Review quitting history.■ Review potential challenges and triggers.■ Encourage support of family and friends
Appendix H:Ask, Advise, Assist, Arrange Protocol
ASK“Have you used any form of tobacco in the past 6 months?”
Do you smoke (even a puff now and again) or use tobacco products of any kind?
(cigarettes, pipe, cigars, chew, spit, bidis)
Yes ❏ No ❏
Non-Smoker ❏ Smoker ❏ Ex-Smoker (greater than 6 months) ❏ Quit Date ___________
Have you ever considered stopping?
ADVISE“As your nurse, the most important advice I can give you is to quit smoking.”
ASSISTOffer help for a stop smoking attempt

75
References:Fiore, M. C. (1997). AHCPR smoking cessation guideline: A fundamental review. Tobacco Control, 6 (Suppl. 1), S4-S8.
National Health Committee. (1999a). Guidelines for smoking cessation: Literature review and background information. NewZealand Guidelines Group [On-line]. Available: http://www.nzgg.org.nz/library.cfm*
National Health Committee. (1999b). Guidelines for smoking cessation: Quit Now. New Zealand Guidelines Group [On-line].Available: http://www.nzgg.org.nz/library.cfm*
U.S. Department of Health and Human Services, Public Health Service. (2000). Clinical practice guideline: Treating tobacco useand dependence. Office of the Surgeon General [On-line].Available: http://www.surgeongeneral.gov/tobacco/treating_tobacco_use.pdf*
* At the time of the original publication, these resources were retrieved at the web addresses above. These links may nolonger be active.
Nursing Best Practice Guideline

Appendix I: The WHY TestNext to the following statements, mark the number that best describes your own experience.
1 = Never 2 = Rarely 3 = Once in a while 4 = Most of the time 5 = Always
❏ A. I smoke to keep myself from slowing down.
❏ B. Handling a cigarette is part of the enjoyment of smoking it.
❏ C. Smoking is pleasant and relaxing.
❏ D. I light up a cigarette when I feel angry about something.
❏ E. When I’m out of cigarettes, it’s near-torture until I can get them.
❏ F. I smoke automatically, without even being aware of it.
❏ G. I smoke when other people around me are smoking.
❏ H. I smoke to perk myself up.
❏ I. Part of enjoying smoking is preparing to light up.
❏ J. I get pleasure from smoking.
❏ K. When I feel uncomfortable or upset, I light up a cigarette.
❏ L. I’m very much aware of it when I‘m not smoking a cigarette.
❏ M. I often light up a cigarette while one is still burning in the ashtray.
❏ N. I smoke cigarettes with friends when I’m having a good time.
❏ O. When I smoke, part of my enjoyment is watching the smoke as I exhale it.
❏ P. I want a cigarette most often when I am comfortable and relaxed.
❏ Q. I smoke when I’m “blue” and want to take my mind off what’s bothering me.
❏ R. I get a real craving for a cigarette when I haven’t had one in a while.
❏ S. I’ve found a cigarette in my mouth and haven’t remembered that it was there.
❏ T. I always smoke when I’m out with friends at a party, bar, etc.
❏ U. I smoke cigarettes to get a lift.
Integrating Smoking Cessation into Daily Nursing Practice
76

77
SCORECARDWrite the number you put beside each letter in The WHY Test beside the same letter on the scorecard. For
example, if you marked a “3” beside question “C” on the test, put a “3” beside the letter “C” on the
scorecard. Then, add up the numbers to get the totals for each category.
A ___ H ___ U ___ “IT STIMULATES ME”
With a high score here, you feel that smoking gives you energy, keeps you
Stimulation Total ___ going. So, think about alternatives that give you energy, such as washing
your face, brisk walking and jogging.
B ___ I ___ O ___ “I WANT SOMETHING IN MY HAND”
There are a lot of things you can do with your hands without lighting up.
Handling Total ___ Try doodling with a pencil, knitting or get a “dummy” cigarette you can
play with.
C ___ J ___ P ___ “IT FEELS GOOD”
A high score means that you get a lot of physical pleasure out of smoking.
Pleasure/Relaxation Total ___ Various forms of exercise can be effective alternatives. People in this
category may be helped by the use of nicotine chewing pieces or a
nicotine transdermal patch if medically indicated.
D ___ K ___ Q ___ “IT’S A CRUTCH”
Finding cigarettes to be comforting in moments of stress can make
Crutch/Tension Total ___ stopping tough, but there are many better ways to deal with stress. Learn
to use relaxation breathing or another technique for deep relaxation
instead. People in this category may be helped by the use of nicotine
chewing pieces or a nicotine transdermal patch if medically indicated.
E ___ L ___ R ___ “I’M HOOKED”
In addition to having a psychological dependency to smoking, you may
Craving Addiction Total ___ also be physically addicted to nicotine. It’s a hard addiction to break, but it
can be done. People in this category are the ones most likely to benefit
from the use of nicotine chewing pieces or a nicotine transdermal patch if
medically indicated.
F ___ M ___ S ___ “IT’S PART OF MY ROUTINE”
If cigarettes are merely part of your routine, one key to success is being
Habit Total ___ aware of every cigarette you smoke. Keeping a diary or writing down
every cigarette on the inside of your cigarette pack is a good way to do it.
G ___ N ___ T ___ “I’M A SOCIAL SMOKER”
You smoke in social situations, when people around you are smoking and
Social Smoker Total ___ when you are offered cigarettes. It is important for you to remind others
that you are a non-smoker. You may want to change your social habits to
avoid the “triggers” which may lead to smoking again.
Source: Health Canada. (1997). Helping pregnant and postpartum women and their families to quit or reduce
smoking. Reproduced with permission of the Ministry of Public Works and Government Services Canada.
Nursing Best Practice Guideline

Appendix J: Fagerstrom Test for NicotineDependence (Revised Version)
The following test is designed to help you determine the strength of your nicotine addiction. Circle the appropriate
score for each question. Total the number of points to arrive at your score. The highest possible score is 10.
How soon after you wake up Within 5 min............................3 points
do you smoke your first cigarette? 5-30 min..................................2 points
31-60 min................................1 point
after 60 min.............................0 points
Do you find it hard not to smoke in places that Yes...........................................1 point
you shouldn’t smoke such as in church, in school, No ...........................................0 points
in a movie, on the bus, in court or in a hospital?
Which cigarette would you hate The first one in the morning ....1 point
most to have to give up? Any other one..........................0 points
How many cigarettes do you smoke each day? 10-fewer..................................0 points
11-20.......................................1 point
21-30.......................................2 points
31 or more...............................3 points
Do you smoke more in the first few hours after waking Yes...........................................1 point
than you do during the rest of the day? No ...........................................0 points
Do you still smoke, even if you are so sick that you are in Yes...........................................1 point
bed most of the day, or if you have the flu or a severe cough? No ...........................................0 points
Total ........................................................................................................................................___points
Interpretation of Scoring
7 to 10: You are highly dependent on nicotine and may benefit from a smoking cessation
program based on treatment for nicotine addiction. Start with 21 mg patch or 4 mg gum.
4 to 6: You have a low to moderate dependence on nicotine, however this does not rule out a smoking
cessation program based on treatment for nicotine addiction. Start with 14 mg patch or 2 mg gum.
< 4: You have a low to moderate addiction, but are not likely to need Nicotine Replacement Therapy.
Reprinted with permission of Dr. Karl Fagerstrom.
BPG Head to come
78

79
Appendix K: Intensive Nursing InterventionTips for the Client■ Make a plan ahead of time for coping with stressful situations.■ Pick a day for stopping that will be relatively stress-free and stick to this date.■ Think positively – you can do it – and concentrate on the benefits of not smoking.■ Take it one day at a time.■ Congratulate yourself frequently.■ Ask a friend to stop with you and support each other.■ Remember that using NRT doubles the chances of quitting and lessens withdrawal symptoms.■ Avoid visiting places where you usually smoke (when you first stop smoking).■ Keep yourself busy and try to increase your level of physical activity.■ Count or save the money you would have spent on cigarettes and treat yourself to something special.■ Don’t try “just one” cigarette – it will take you back to the beginning.
Reprinted with permission.
Royal College of Nursing. (2002). Clearing the air: A nurses guide to smoking and tobacco control. London, England: The RoyalCollege of Nursing.
Nursing Best Practice Guideline

Appendix L: Quit SmokingFirst-Line Medications Compared
Quit Smoking Aid How to use How long to take it Possible side effects
Integrating Smoking Cessation into Daily Nursing Practice
80
-Nicotine gum(Nicorette®)
Available over thecounter
• “bite & park” gum
• 1 piece of gum every1-2 hours
• 2 mg if you’re alight smoker(20 cigarettes per day)
• 4 mg if you’re aheavy smoker(> 20 cigarettes per day)
• stop smoking beforestarting
• several weeks to severalmonths or longer ifnecessary
• burning in throat
• hiccups if chewedtoo quickly
• dental problems
Nicotine patch(Habitrol®, Nicoderm®)
Available over thecounter
• if you’re a light smoker(>20 cigarettes per day),start 14 or 7 mg
• if you’re a heavysmoker (> 20 cigarettesper day) start 21 mg for4-8 weeks. Discusstapering to lower doseswith your doctor.
• 8-12 weeks or longer ifnecessary
• local skin reaction
• disturbed sleep,nightmares
Nicotine Inhaler Consists of amouthpiece anda cartridge containingnicotine. Inhaledinto the mouth andheld so nicotine isabsorbed into buccalmucosa. Mostusers require 2-10 puffsper craving.
6-12 cartridges a day forapproximately 3 months isrecommended by themanufacturer, althoughmany may needsignificantly less.
• burning throat, cough,sneezing and hiccups.
Bupropion(Zyban®)
Available only byprescription
• 150 mg once a day (inthe morning) for 3days, then twice a day(morning and evening,with at least 8 hoursbetween doses)
• start 7-14 days beforequit date
• 7-12 weeks or longer ifnecessary
• dry mouth
• insomnia
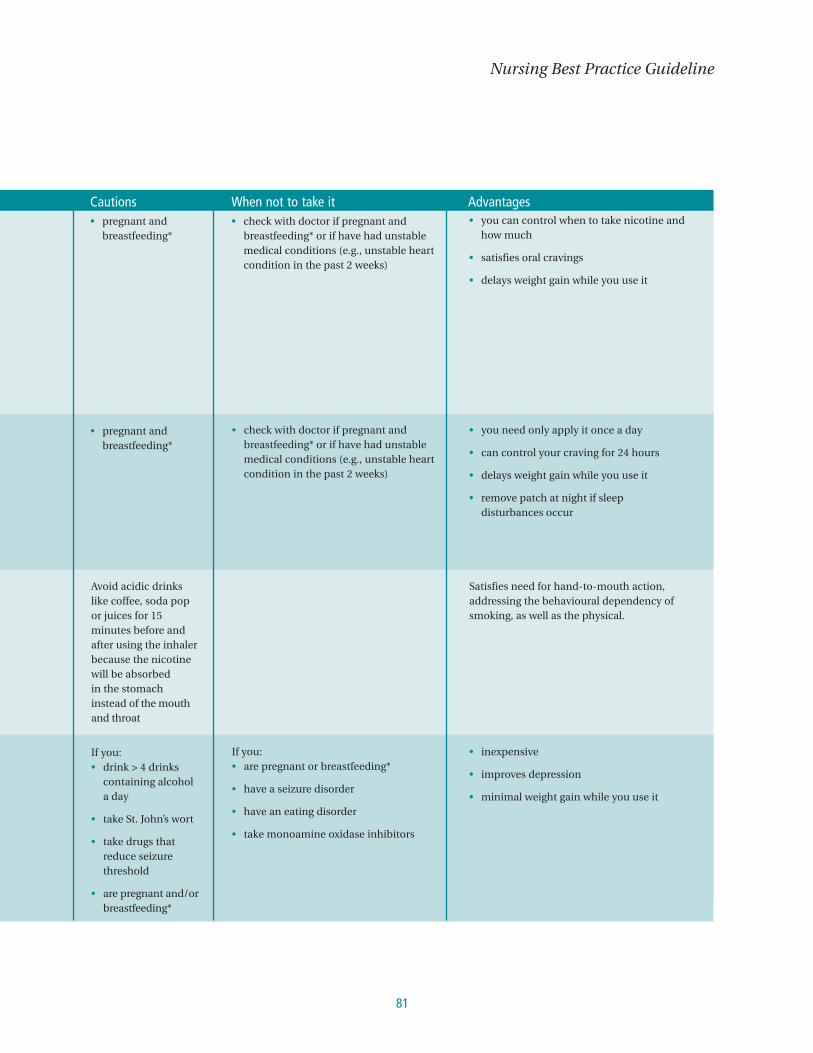
81
Nursing Best Practice Guideline
Cautions When not to take it Advantages• pregnant and
breastfeeding*• check with doctor if pregnant and
breastfeeding* or if have had unstablemedical conditions (e.g., unstable heartcondition in the past 2 weeks)
• you can control when to take nicotine andhow much
• satisfies oral cravings
• delays weight gain while you use it
• pregnant andbreastfeeding*
• check with doctor if pregnant andbreastfeeding* or if have had unstablemedical conditions (e.g., unstable heartcondition in the past 2 weeks)
• you need only apply it once a day
• can control your craving for 24 hours
• delays weight gain while you use it
• remove patch at night if sleep disturbances occur
Avoid acidic drinkslike coffee, soda popor juices for 15minutes before andafter using the inhalerbecause the nicotinewill be absorbedin the stomachinstead of the mouthand throat
Satisfies need for hand-to-mouth action,addressing the behavioural dependency ofsmoking, as well as the physical.
If you:• drink > 4 drinks
containing alcohola day
• take St. John’s wort
• take drugs thatreduce seizurethreshold
• are pregnant and/orbreastfeeding*
If you:• are pregnant or breastfeeding*
• have a seizure disorder
• have an eating disorder
• take monoamine oxidase inhibitors
• inexpensive
• improves depression
• minimal weight gain while you use it

Integrating Smoking Cessation into Daily Nursing Practice
82
Nicorette® (nicotine polacrilex); registered trademark of Aventis Pharma Inc. Habitrol® (nicotine): registered trademark of Novartis Consumer Health Canada Inc.Nicoderm® (nicotine): registered trademark of Aventis Pharma Inc. Zyban® (bupropion HCL): registered trademark of Glaxo Wellcome Inc.
*Many doctors believe that using nicotine gum or the patch is better than smoking during pregnancy because, bystopping smoking, you are not inhaling thousands of toxic chemicals from cigarette smoke. However, there is notenough evidence to show that using nicotine gum or the patch is safer than smoking during pregnancy.
If you are pregnant or breastfeeding, always check with your doctor before using nicotine gum or the patch.
NB: Additional products may be available
Reprinted with permission:University of Toronto Department of Family & Community Medicine. (2000). Smoking cessation guidelines: How to treatyour patient’s tobacco addiction. Toronto, Ontario: Pegasus Healthcare International.

83
Appendix M: Strategies to Avoid Relapse■ Encourage client to identify tempting situations and develop a specific plan to handle them (e.g., write
down three strategies and carry this list at all times).■ Reframe a lapse (slip) as a learning opportunity, not a failure.■ Recommend that the client:
■ learn stress management and relaxation techniques;■ learn to balance lifestyle so that pressures and triggers are not overwhelming.
Common Factors Associated with Relapse:■ Alcohol use■ Negative mood or depression■ Negative self-talk■ Other smokers in household■ Prolonged withdrawal symptoms■ Exposure to high-risk situations, such as social situations, arguments, and other sources of stress■ Dietary restriction■ Lack of cessation support■ Problems with pharmacotherapy, such as under-dosing, side effects, compliance or premature
discontinuation■ Recreational drug abuse
Reprinted with permission:
University of Toronto Department of Family & Community Medicine. (2000). Smoking cessation guidelines: How to treat yourpatient’s tobacco addiction. Toronto, Ontario: Pegasus Healthcare International.
Nursing Best Practice Guideline
Appendix N: List of Resources Available forSmoking Cessation
Integrating Smoking Cessation into Daily Nursing Practice
84
■ Canadian Cancer SocietyNational Office, Suite 200
10 Alcorn Avenue
Toronto, Ontario M4V 3B1
www.cancer.ca
E-mail: [email protected]
Toll Free: 1-888-939-3333
Offers booklets and self-help resources for
smokers, such as “For Smokers who want to
Quit”, and “For Smokers who don’t want to
Quit”, available in English, French and Chinese.
Ontario Smoker’s Helpline:
1-877-513-5333 www.smokershelpline.ca
Offers a free self-help smoking cessation
program called One Step at a Time.
■ Canadian Council of TobaccoControl (CCTC)170 Laurier Avenue West, Suite 100
Ottawa, Ontario K1P 5V5
Tel: 613-567-3050
www.cctc.ca
E-mail: [email protected]
This is a national, non-profit organization
specializing in tobacco and health issues.
■ Canadian Health Network (CHN)www.canadian-health-network.ca
CHN is a national, non-profit, bilingual
web-based health information service,
sponsored by Health Canada.
■ Centre for Addiction andMental Health33 Russell Street
Toronto, Ontario M5S 2S1
416-535-8501 ext 1600
Operates a Smoking Cessation Clinic and
has launched a workshop, TEACH The Training
Enhancement in Applied Cessation Counselling
and Health for health practitioners
■ TEACH(Training Enhancement in AppliedCessation Counselling and Health)33 Russell Street, Room 1081
Toronto, Ontario M5S 2S1
Tel: 416-535-8501 ext.1600
Fax: 416-260-418
E-mail: [email protected]
www.teachproject.ca
Trains practitioners in tobacco cessation
interventions.
■ Health CanadaTobacco Control Programme P.L. 3507C
Ottawa, Ontario K1A 0K9
Tel: 1-866-318-1116
(Monday-Friday, 8 a.m. to 4 p.m. ET;
voice-mail available at all other times)
Fax: 613-954-2284
www.gosmokefree.ca
E-mail: [email protected]
This website contains a variety of new tools to
help Canadians quit smoking. Persons who
smoke can sign up with the e-Quit program for
a 30-day series of free e-mail messages to help
them through the cessation process.

85
■ Heart & Stroke Foundation of Canada222 Queen Street, Suite 1402
Ottawa, Ontario K1P 5V9
Tel: 613-569-4361
www.heartandstroke.ca
E-mail: [email protected]
■ Leave the Pack BehindBrock University
500 Glenridge Avenue,
St. Catharines, Ontario
Tel: 905-688-5550 ext. 4992
www.LeaveThePackBehind.org
■ Physicians for aSmoke-free Canada (PSC)1226 A Wellington Street
Ottawa, Ontario K1Y 3A1
Tel: 613-233-4878
Fax: 613-233-7797
www.smoke-free.ca
PSC is a national health organization, founded
in 1985 as a registered charity. It is a unique
organization of Canadian physicians who
share one goal: the reduction of tobacco-caused
illness through reduced smoking and reduced
exposure to second-hand smoke. It also provides
information on a variety of tobacco issues.
■ Pregnetswww.pregnets.org
Up-to-date information on smoking cessation
practices for pregnant and postpartum women
can be found here.
Nursing Best Practice Guideline
■ Program Trainingand Consultation CentreToll free: 1-800-363-7822
www.ptcc-cfc.on.ca
Provides training and consultation services
in Ontario to implement effective community-
based tobacco use reduction strategies.
■ The Lung Association National Office1900 City Park Drive, Suite 508
Blair Business Park
Gloucester, Ontario K1J 1A3
Tel: 613-747-6776
www.lung.ca
E-mail: [email protected]
■ Ontario Lung AssociationTel: (416)-864-9911
Toll Free: 1-800-972-2636
www.on.lung.ca
Nurses Quit Net available on-line for nurses
and nursing students who want to quit
smoking; www.tobaccofreenurses.org
■ Registered Nurses Association ofOntario (RNAO)www.rnao.org/smokingcessation
RNAO offers an e-learning course to help
educate health professionals on smoking
cessation interventions.
Additional Online Support Help to Quit Smoking
■ American Cancer SocietyGreat American Smoke Out
www.cancer.org/docroot/PED/ped_10_4.asp?sitearea=PED
■ Centers for Disease Control and Prevention (CDC)Quit Tips: Don’t let another year go up in smoke
http://www.cdc.gov/tobacco/quit/quittip.htm
■ Nicotine Anonymoushttp://www.nicotine-anonymous.org
Nicotine Anonymous is a non-profit 12 Step help program for those who would like to cease using
tobacco and nicotine products. Group support and recovery using the 12 Steps, as adapted from
Alcoholics Anonymous, help to achieve abstinence from nicotine.
■ Smokefree.govwww.smokefree.gov
■ The Foundation for a Smoke Free Americawww.tobaccofree.org
Integrating Smoking Cessation into Daily Nursing Practice
86

87
Nursing Best Practice Guideline
Appendix O: Description of the ToolkitThe Toolkit provides step-by-step directions to individuals and groups involved in planning, coordinating,
and facilitating the guideline implementation. Specifically, the Toolkit addresses the following key steps in
implementing a guideline:
1. Identifying a well-developed, evidence-based clinical practice guideline
2. Identification, assessment and engagement of stakeholders
3. Assessment of environmental readiness for guideline implementation
4. Identifying and planning evidence-based implementation strategies
5. Planning and implementing evaluation
6. Identifying and securing required resources for implementation
Implementing guidelines in practice that result in successful practice changes and positive clinical impact
is a complex undertaking. The Toolkit is one key resource for managing this process.
The Toolkit is available through the Registered Nurses’ Association of Ontario.
The document is available in a bound format for a nominal fee, and is also
available free of charge from the RNAO website. For more information, an
order form or to download the Toolkit, please visit the RNAO website at
www.rnao.org/bestpractices.

Nursing Best Practice Guideline
Integrating Smoking Cessationinto Daily Nursing Practice
This program is funded by the Government of Ontario
Revised March 2007
0-920166-83-0
Related Documents











