1 How to overcome barriers to Palliative Care provision for patients with heart failure Dr. Piotr Sobanski Prof. Dr. Bernd Alt-Epping

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
1
How to overcome barriers to
Palliative Care provision
for patients with heart failure
Dr. Piotr Sobanski
Prof. Dr. Bernd Alt-Epping
2
When have you experienced
barriers in providing
Palliative Care for patients with heart failure?
3
In industrial countries, cardiovascular disease contributes
to the majority of deaths (e.g., 41% in Germany)
1.6-times more patients die from c.v. disease than from cancer
Patients with congestive heart failure (CHF) NYHA IV are facing a
lifetime prognosis that is worse than for the majority of cancer
patients in incurable, metastasized stages, with a 2-year mortality
of 40% to 45% (absolute risk), depending on the underlying
diagnostic CHF criteria (“more malignant than cancer”)
Still, the vast majority of patients in specialized palliative care
institutions suffer from advanced cancer
Background
4
A distinct symptom spectrum (Ostgathe 2010, etc.)
=> a traditional (pain-focused) PC approach will not work
Tiredness / weakness / fatigue
Resources
Non-linear disease trajectory
Specific ethical problems
Socialization – attitude – culture
Barriers to Palliative Care involvement in heart failure
5
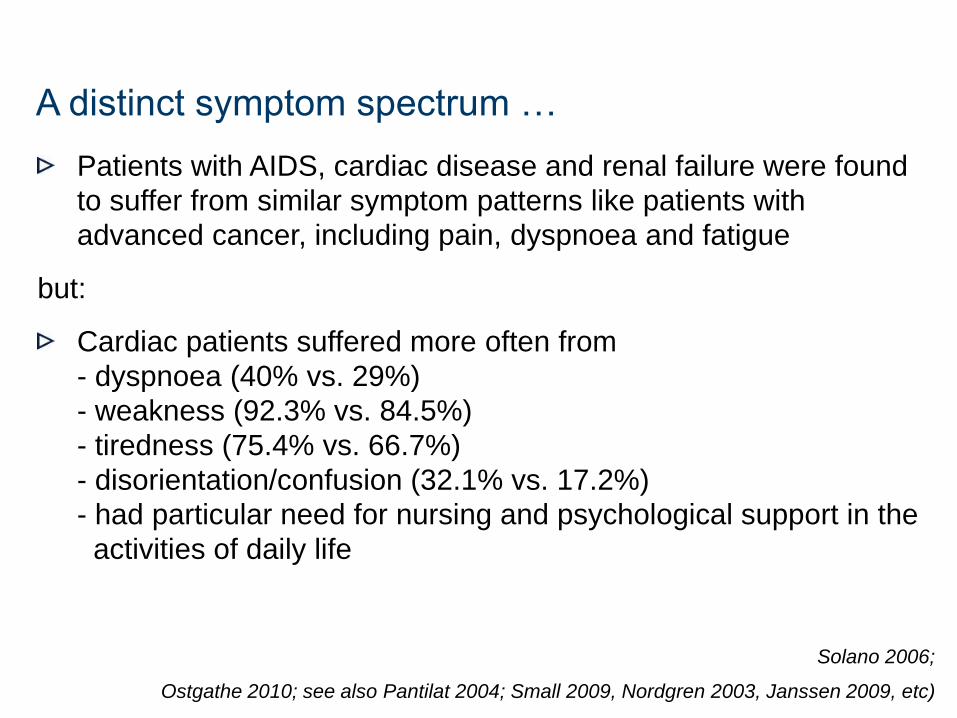
Patients with AIDS, cardiac disease and renal failure were found
to suffer from similar symptom patterns like patients with
advanced cancer, including pain, dyspnoea and fatigue
but:
Cardiac patients suffered more often from
- dyspnoea (40% vs. 29%)
- weakness (92.3% vs. 84.5%)
- tiredness (75.4% vs. 66.7%)
- disorientation/confusion (32.1% vs. 17.2%)
- had particular need for nursing and psychological support in the
activities of daily life
Solano 2006;
Ostgathe 2010; see also Pantilat 2004; Small 2009, Nordgren 2003, Janssen 2009, etc)
A distinct symptom spectrum …
6
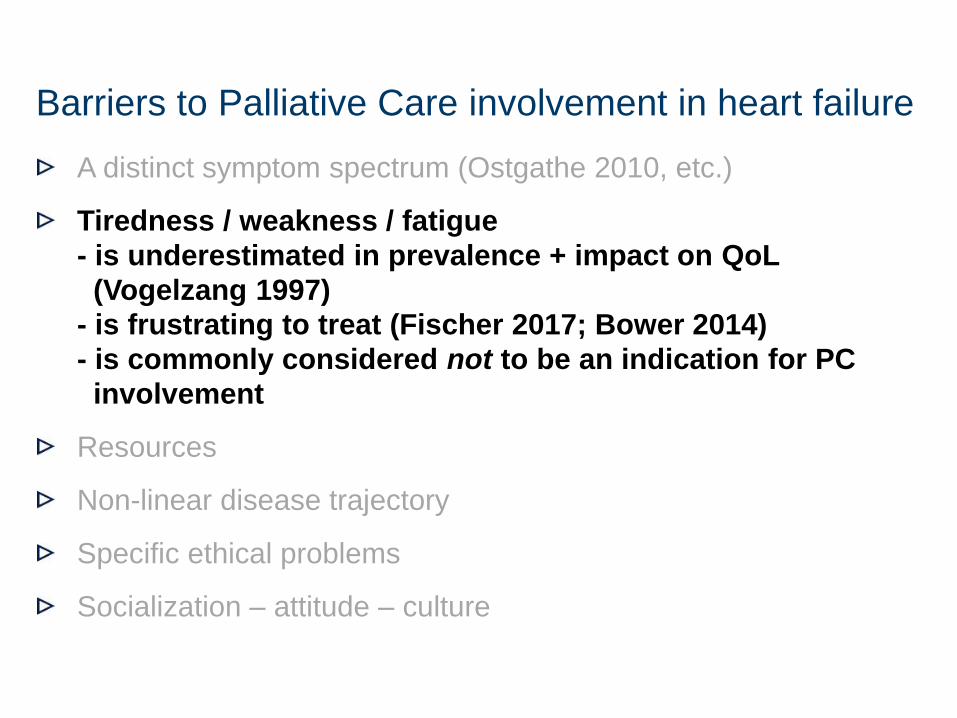
A distinct symptom spectrum (Ostgathe 2010, etc.)
Tiredness / weakness / fatigue
- is underestimated in prevalence + impact on QoL
(Vogelzang 1997)
- is frustrating to treat (Fischer 2017; Bower 2014)
- is commonly considered not to be an indication for PC
involvement
Resources
Non-linear disease trajectory
Specific ethical problems
Socialization – attitude – culture
Barriers to Palliative Care involvement in heart failure
7
A distinct symptom spectrum (Ostgathe 2010, etc.)
Tiredness / weakness / fatigue
Resources
Non-linear disease trajectory
Specific ethical problems
Socialization – attitude – culture
Barriers to Palliative Care involvement in heart failure

8
9
10
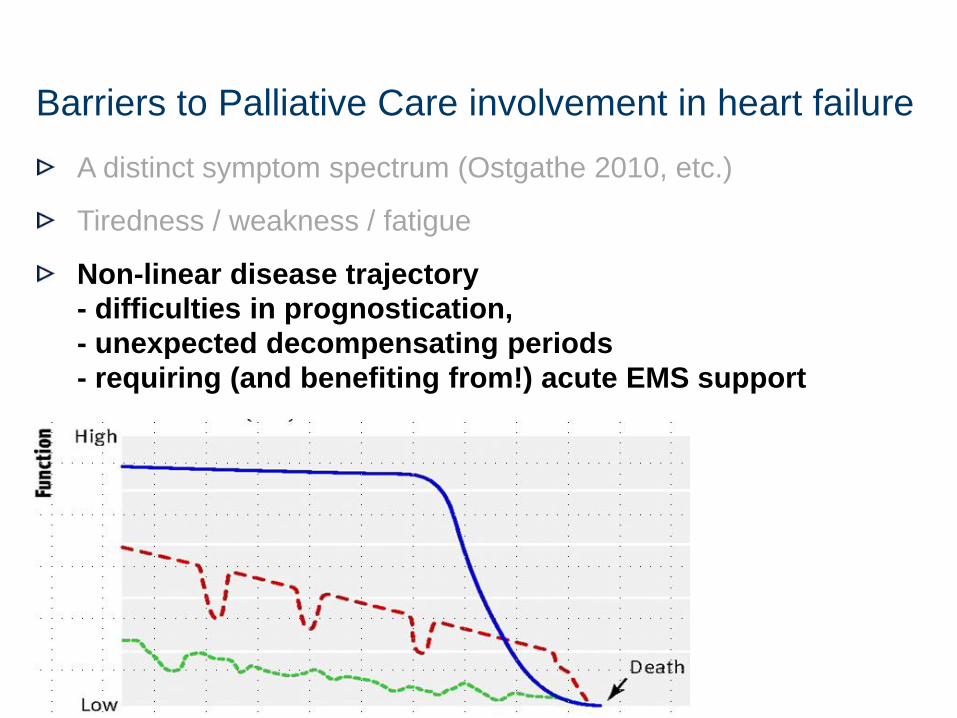
A distinct symptom spectrum (Ostgathe 2010, etc.)
Tiredness / weakness / fatigue
Non-linear disease trajectory
- difficulties in prognostication,
- unexpected decompensating periods
- requiring (and benefiting from!) acute EMS support
Specific ethical problems
Socialization – attitude – culture
Barriers to Palliative Care involvement in heart failure
11
A distinct symptom spectrum (Ostgathe 2010, etc.)
Tiredness / weakness / fatigue
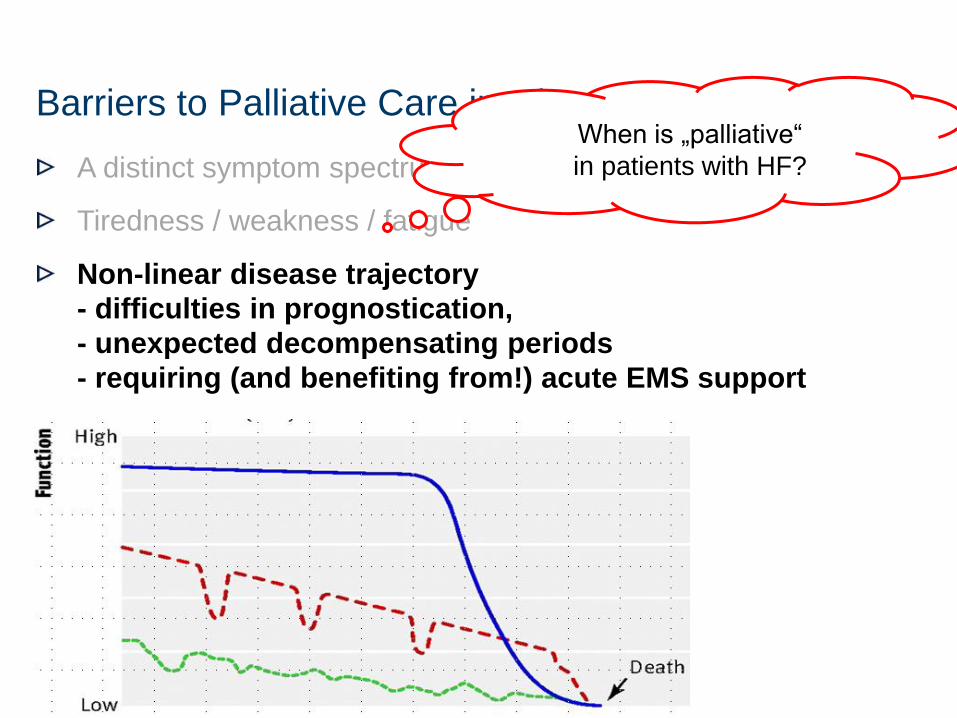
Non-linear disease trajectory
- difficulties in prognostication,
- unexpected decompensating periods
- requiring (and benefiting from!) acute EMS support
Specific ethical problems
Socialization – attitude – culture
Barriers to Palliative Care involvement in heart failure When is „palliative“
in patients with HF?
12
A distinct symptom spectrum (Ostgathe 2010, etc.)
Tiredness / weakness / fatigue
Non-linear disease trajectory
Specific ethical problems
when it comes to terminating interventional therapies
Socialization – attitude – culture
Barriers to Palliative Care involvement in heart failure
13
Redefining palliative treatment goals
when prognostication is difficult
PallCare for pts. where heart transplantation is still discussed
Advance care and emergency procedure planning
Ethical aspects of disabeling devices
(external / assisting or integral / internalized? Substitutive or
replacing? Immediate death after deactivation or forgoing a mere
risk reducing therapy?, etc…)
Non-cardiac PallCare pts. with unexpected cardiac complications
The role of formal ethics consultation
Ethically relevant problems in heart failure patients
14
Redefining palliative treatment goals
when prognostication is difficult
PallCare for pts. where heart transplantation is still discussed
Advance care and emergency procedure planning
Ethical aspects of disabeling devices
(external / assisting or integral / internalized? Substitutive or
replacing? Immediate death after deactivation or forgoing a mere
risk reducing therapy?, etc…)
Non-cardiac PallCare pts. with unexpected cardiac complications
The role of formal ethics consultation
Ethically relevant problems in heart failure patients
15
A distinct symptom spectrum (Ostgathe 2010, etc.)
Tiredness / weakness / fatigue
Non-linear disease trajectory
Specific ethical problems
Socialization – attitude – culture
- mechanistic / organ centred / disease centered approach
versus bio-psycho-social / holistic approach
Barriers to Palliative Care involvement in heart failure
Socialization – attitude – culture Fundamental conflict …
... between two approaches
Bio-psychosocial,
patient centered
Disease
centered
Palliative Medicine as a speciality
17
The clinical perspective (and role models)
The “cultural” attitude perspective
The perspective of associations and societies
and their guidelines and policies
… and … your perspective
How to overcome barriers to palliative care provision
18
The clinical perspective (and role models)
The “cultural” attitude perspective
The perspective of associations and societies
and their guidelines and policies
… and … your perspective
How to overcome barriers to palliative care provision
19
A broader “symptom-and-needs perspective” in PC,
a less prognosis-dependent approach
More community-based, more outreaching PC (primary PC)
less in-patient treatment on PC units
More advance care planning and anticipating crises
Defining red flag indications for involvement of specialized PC
- refractory/complex symptoms
- repeated hospital readmissions
- complex and conflicted decision-making
- grief and complicated bereavement after patients’ death
PC in “stand-by” on-demand mode, ready to intervene rapidly
after periods of stability
How to overcome: the clinical perspective
How to overcome: the clinical perspective
- technical elements
Acknowledging technical elements, helps to avoid feeling
PC is doing nothing else than waiting for death
1. Symptom management - can be recognized as potentially
superior to classical disease centered approach
2. Prescribing opioids for analgesia, what usually bears fears
3. PC measures to alleviate breathlessness
4. Managing of mood disorders
5. Creating early measurable Q indicators would provide
understandable PC outcomes (the added value)*
Mizuno A. J Card. 2017; Hibbert D. Social Science & Medicine 2003
/ Mack, Arch Intern Med 2010 / Mack, J Clin Oncol, 2010 /
Wright, JAMA 2008 / Zhang, Arch Intern Med, 2009
21
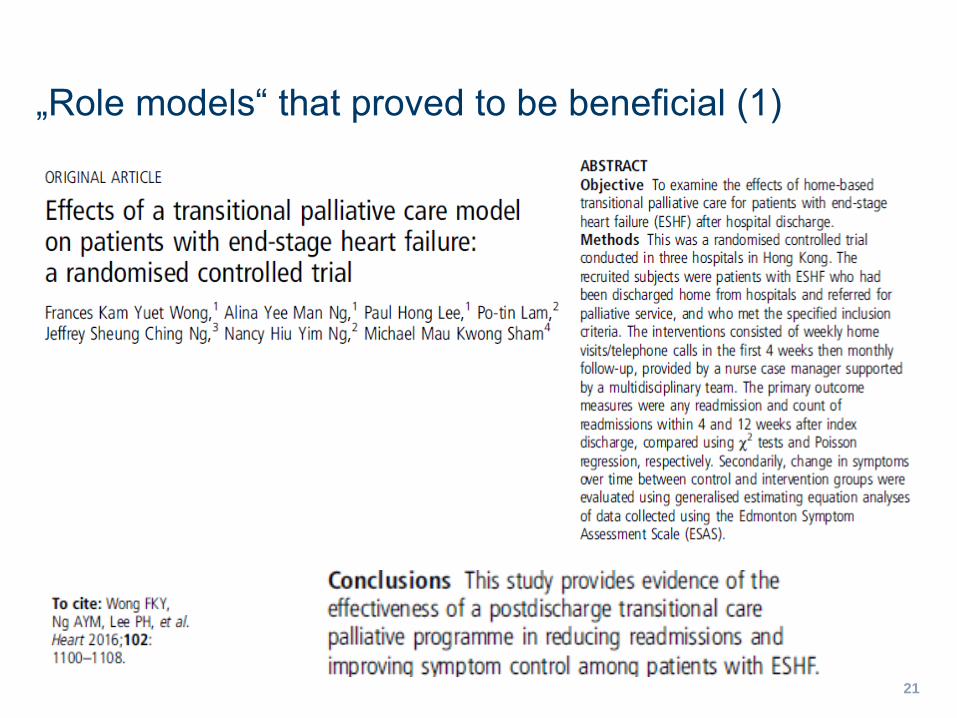
„Role models“ that proved to be beneficial (1)
22
„Role models“ that proved to be beneficial (2)
23
„Role models“ that proved to be beneficial (2)
Advance Care Planning
its principles may be transferred to EoL decisions in cardiology
Proved to be effective:
- significantly less “aggressive” therapies at EoL
- better QoL scores
- earlier hospice care
- higher rates of preference oriented therapy
- less costs (higher costs were associated with worse QoL
Mack, J Clin Oncol 2012 / Mack, Arch Intern Med 2010 / Mack, J Clin Oncol, 2010 /
Wright, JAMA 2008 / Zhang, Arch Intern Med, 2009
24
„Role models“ that proved to be beneficial (3)
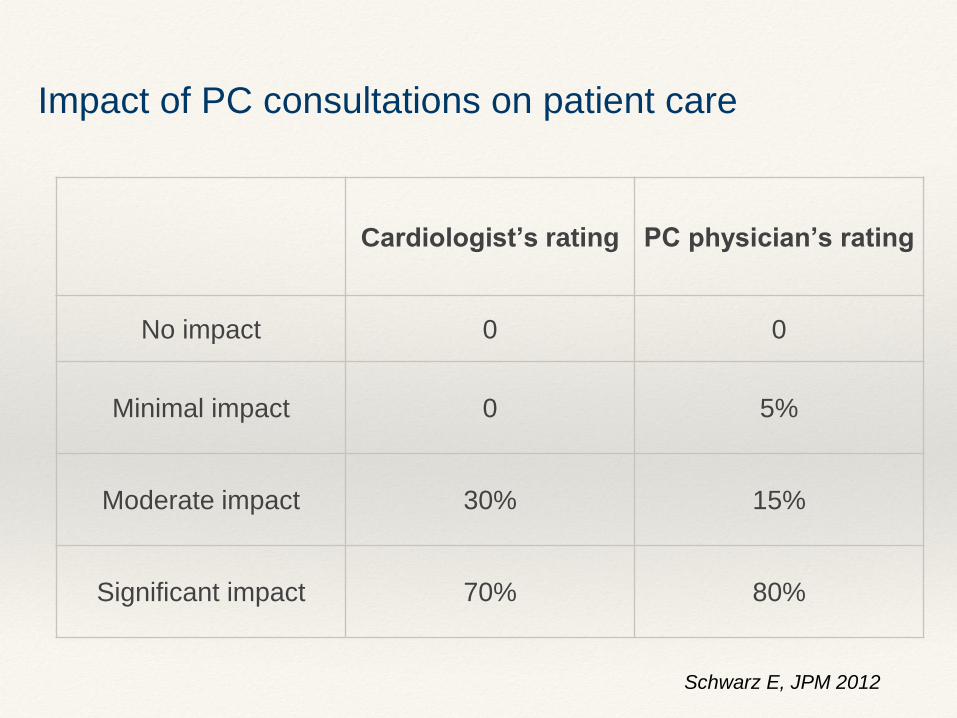
Impact of PC consultations on patient care
Cardiologist’s rating PC physician’s rating
No impact 0 0
Minimal impact 0 5%
Moderate impact 30% 15%
Significant impact 70% 80%
Schwarz E, JPM 2012
26
The clinical perspective (and role models)
The “cultural” attitude perspective
The perspective of associations and societies
and their guidelines and policies
… and … your perspective
How to overcome barriers to palliative care provision
27
Multidisciplinarity
Communication
Training
How to overcome: the cultural / attitude perspective
Implementing SPC in the cardiology
is like entering of a new terrain
❖ it is reasonable getting to known rules, habits and the
language of this new field in advance
but as well
❖ to reflect own rules, habit and language, and what is
welcomed by the other partners to build a dialog
All is about understanding of roles, respecting expertise
and ethos of professional mission/values/identity
from both partners and own perspectives
Multidisciplinarity: factors that facilitate cooperation
❖ coordination of cooperation
❖ communication with other providers
❖ integration in existing programs
❖ documentation of evidence of improving QoL
without increasing health care costs
Bekelman DB, JPallMed 2016
Incoherence of PC with orthodox medicine
Technical vs. indeterminate components of care
❖ PC focuses on holistic/psychosocial issues, as on key
components of PC.
❖ Classical („orthodox”) medicine prizes science and
rationality not these „indeterminate” holistic components.
❖ The technical components of PC can facilitate the dialog,
but the holistic, strengthen divergences and boundaries
Important misunderstandings with respect to PC
❖ referral criteria for PC are understood to be based on a
categorisation of patient as being beyond the help
❖ palliative treatment (almost) the same as in people not
being terminal (lack of easy recognisable symbolic step
„stopping chemotherapy”)
❖ symptom relief is what cardiologists and GP are always
doing …. and the psychosocial, ethical and spiritual
issues are not noticed
Hanratty B., BMJ 2002
Improvement of communication
between PC specialists and other disciplines …
❖ … can be preventive against burnout among PC
clinicians (especially working full time in hospices) -
burnout rate up to 62%*
❖ … can be preventive against burnout and improve self-
care among cardiological members of Heart Teams
implanting LVADs
*Kavalieratos D., JPSM 2017 ** Goldstein N, Circ. 2011
33
The clinical perspective (and role models)
The “cultural” attitude perspective
The perspective of associations and societies
and their guidelines and policies
… and … your perspective
How to overcome barriers to palliative care provision
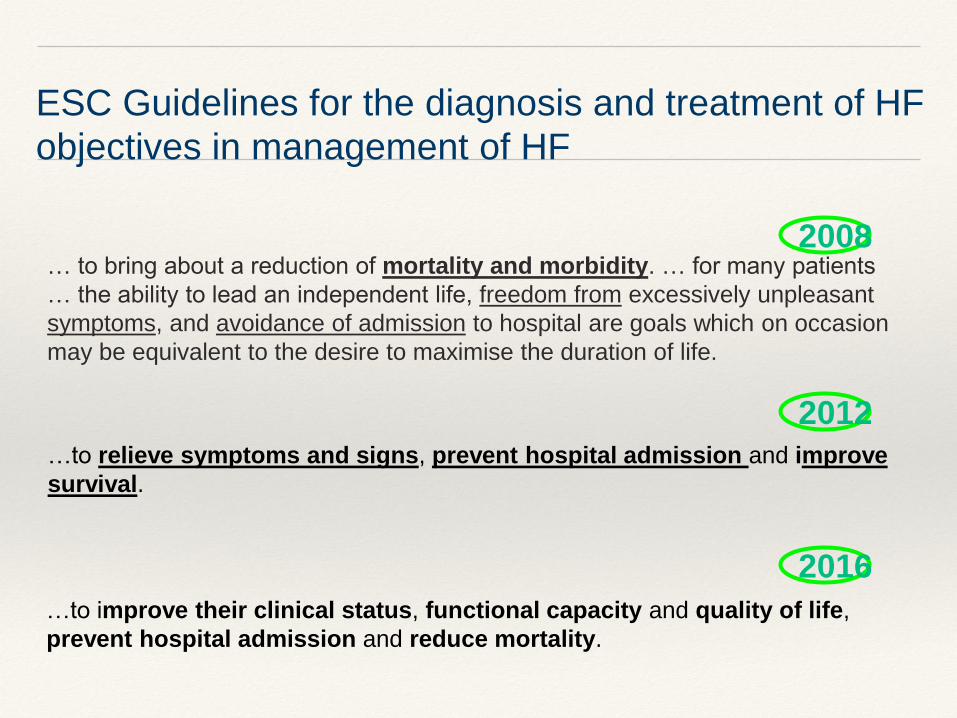
…to improve their clinical status, functional capacity and quality of life,
prevent hospital admission and reduce mortality.
…to relieve symptoms and signs, prevent hospital admission and improve
survival.
… to bring about a reduction of mortality and morbidity. … for many patients
… the ability to lead an independent life, freedom from excessively unpleasant
symptoms, and avoidance of admission to hospital are goals which on occasion
may be equivalent to the desire to maximise the duration of life.
2012
2008
2016
ESC Guidelines for the diagnosis and treatment of HF
objectives in management of HF
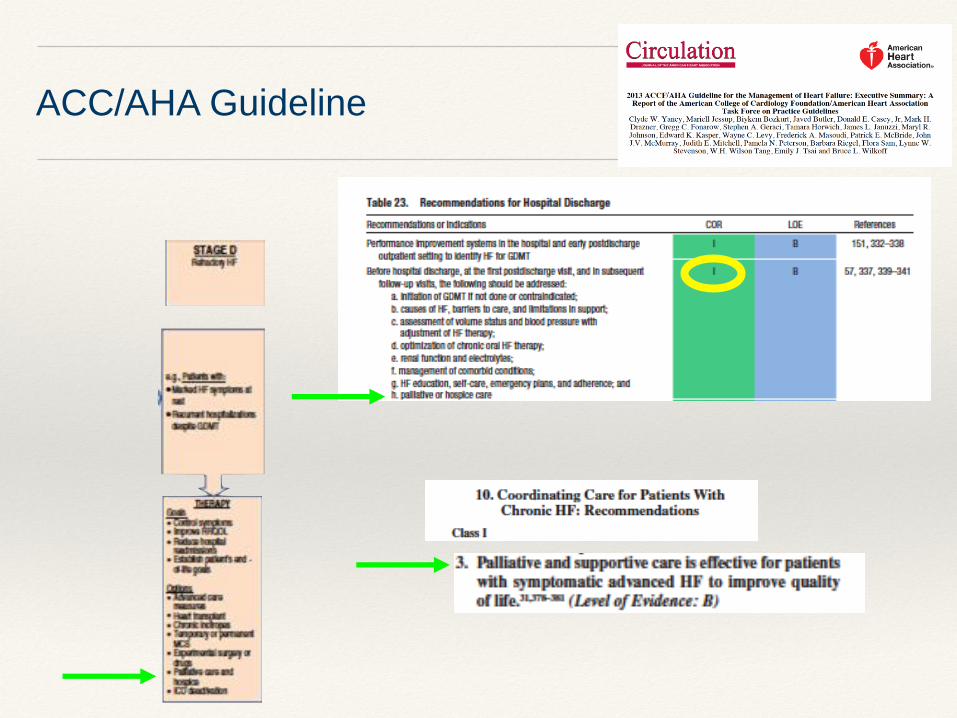
ACC/AHA Guideline
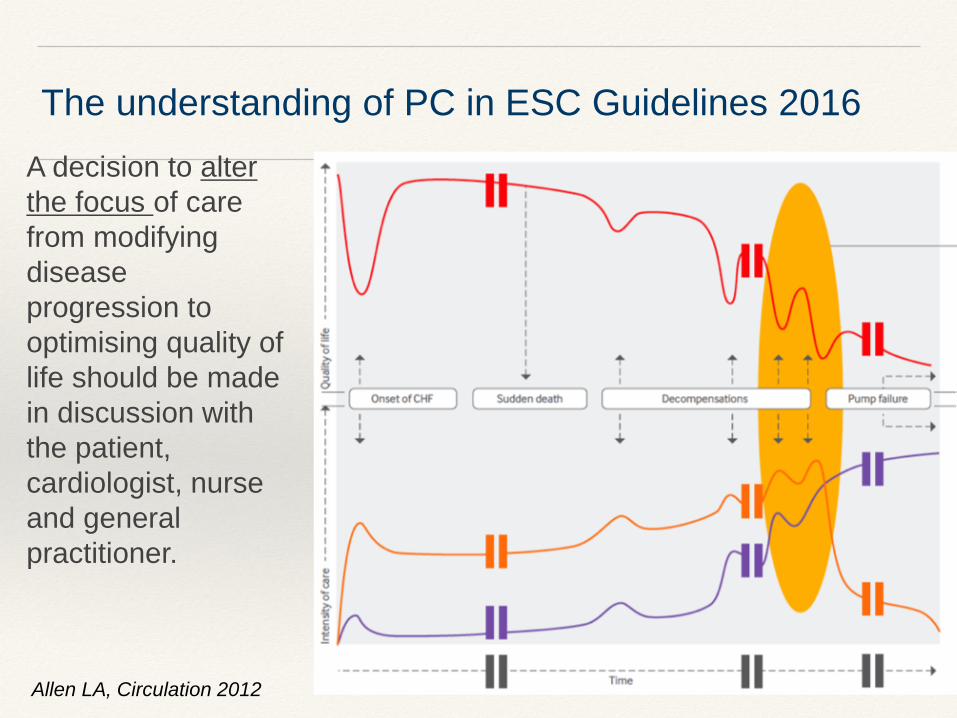
The understanding of PC in ESC Guidelines 2016
A decision to alter
the focus of care
from modifying
disease
progression to
optimising quality of
life should be made
in discussion with
the patient,
cardiologist, nurse
and general
practitioner.
Allen LA, Circulation 2012
37
Discordance between guidelines and real life in cardiology
Over half of US cardiologists recommend care that is discordant
with ACC/AHA guideline for HF, missing out elements of PC
(communication about prognosis, ACP, care coordination and
symptom control) in patients with late stage HF
The ratio (inversely proportional) between PC and intense medical
care in people with advanced HF varies between regions
suggesting local practice patterns matter
How to overcome: the perspective of associations
and societies and their guidelines and policies
Matlock D.D., JPM 2010; paper describes survey performed in 2004

38
39
The clinical perspective (and role models)
The “cultural” attitude perspective
The perspective of associations and societies
and their guidelines and policies
… and … your perspective
How to overcome barriers to palliative care provision
Related Documents











