Hepatitis B & Hepatitis C in HIV Dr K.Bujji Babu,MD Consultant HIV Physician Dr.Bujjibabu HIV Clinic.

Hepatitis B & Hepatitis C in HIV Dr K.Bujji Babu, MD Consultant HIV Physician Dr.Bujjibabu HIV Clinic.
Mar 26, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Hepatitis B & Hepatitis C in HIV
Dr K.Bujji Babu,MD
Consultant HIV Physician
Dr.Bujjibabu HIV Clinic.

HIVHIV Hepatitis BHepatitis B 40 million worldwide 1 million in the US RNA retrovirus Integrates in genome 1y target CD4 cells Reverse Transcriptase Nucleoside Analogues Mutations=Resistance
400 million worldwide 1.25 million in the US DNA hepadna virus Integrates into
genome 1y target hepatocytes Reverse Transcriptase Nucleoside Analogues Mutations=Resistance

HIV HBV Co-infectionHIV HBV Co-infection
About 10% of HIV+ patients are HBSAg+ (Rustgi VK, Ann Int Med 1984)
HIV+ pts 3-6x more likely to develop chronic HBV than HIV- (Bodsworth JID 1991)
HIV/HBV is associated with more cirrhosis than HBV alone (Colin JF Hepatology 1999 )

HBeAg and HBV DNA higher levels in HIV+ but AST/ALT lower(Perillo Ann Intern Med 1986)
Much lower rate of spontaneous HbeAg seroconversion (Krogsgaard Hepatology 1987)
HBV DNA found in HBcAb+ only patients (HBSAb and HBsAg negative) (Hofer Eur J Clin Microbiol 1998)
HIV HBV CoHIV HBV Co--infectioninfection

2 Studies found accelerated histologic progression of HBV in HIV+ (Colin Hepatology 1999 and Schechter AIDS 1989)
One study found RR of HIV progression to be 3.6 with HBV, 2 others did not (Scharschmidt Ann Int Med 1992, Eskild AIDS 1992)
Lamivudine active in > 80% of HIV+ and Neg patients (Benhamou Ann Int Med 1996)
HIV HBV CoHIV HBV Co--infectioninfection

HBV & HIV – Rx Guide lines HBV DNA > 105 copies/ml ALT consistently >2-fold above N bioptic detection of liver fibrosis
Healthy carriers don’t require treatment

HBV & HIV – Rx Guide lines Lamivudine and Tenofovir are
primarily indicated for HIV treatment, the status of HIV infection must be considered (e.g. necessity for treatment, prior therapies, resistance).
An individual decision must be reached.

HIV & HBV – Rx guide lines Adefovir can be given as mono Lamivudine or Tenofovir –no monotherapy On HAART - lamivudine (possibly plus
tenofovir) as a component of HAART Resistance with Lam, Tenofovir can be used
as an alternative component of HAART. Treatment to continue till seroconversion or
until there is loss of efficacy (renewed increase of transaminases and viral load)

Lamivudine in Pts Co- Lamivudine in Pts Co- infected with HBV and HIV infected with HBV and HIV
122 co-infected patients treated with lamivudine and antiretroviral therapy in CAESAR study
Safety data comparable across treatment arms
French study of 40 HIV/HBV co-infected patients (Benhamou, et al., Ann. Int. Med., Nov. 1996)

Inhib ition of HBV Polym erases Contain ing Inhib ition of HBV Polym erases Contain ing Lam ivudineLam ivudine --Resistant M utationsResistant M utations
Resistance is defined as a 5-fold increase of K i
Lam ivudine
Adefovir
Enzyme K i (M ) Fold Increase
K i (M ) Fold Increase
W ild type
0 .25 1 0 .10 1
V173L 0.31 1.2 0 .15 1.5
L180M 0.64 2.6 0 .23 2.3
M 204I 2.0 8 0 .13 1.3
M 204V 4.9 19.6 0 .22 2.2
L180M + M 204I
3 .8 15.2 0 .18 1.8
L180M + M 204V
6.3 25.2 0 .08 0.8

Adefovir OverviewAdefovir Overview
Nucleotide analogue that inhibits HBV polymerase via chain termination
Potent anti-HBV activity in early clinical studies
In vitro and in vivo activity against:
wild-type HBVlamivudine- and famciclovir-resistant HBV
N
N N
N
NH2
OP
O
(-) O
Adefovir (PMEA)
(-) O

-5
-4
-3
-2
-1
0
Weeks of adefovir dipivoxil
HB
V D
NA
(lo
g 10
copi
es/m
L)
35 35 35 33 33 33 33 31 31 31 31 31 31 29No. patients
BL 2 4 8 12 16 20 24 28 32 36 40 44 48
HBV DNA Response to ADVHBV DNA Response to ADVMean changes from baseline (8.64±0.08 log10 copies/mL) in serum HBV DNA measured by PCR during ADV
All time points were significantly
lower compared to baseline
p<0.0001
- 4.01±0.17 log10 copies/mL

Tenofovir Disoproxil Tenofovir Disoproxil FumarateFumarate
N
NN
N
NH2
OP
OO
O
O
O
O
O
O
O

TenofovirTenofovir Study 907Study 907AntiAnti--HBV Activity (n=12)HBV Activity (n=12)
Baseline HBV DNA (log10 c/mL) 8.7
Change from baseline to week 24 (log10 c/mL)
Mean -4.6
Median -4.4
Range -2.6 to -6.5

DAPDDAPDDioxolane purine nucleoside analogue
DAPD is deaminated by adenosine deaminase, yielding DAPD is deaminated by adenosine deaminase, yielding dioxolanedioxolane guanosine (DXG); the 5´guanosine (DXG); the 5´--triphosphate is active against triphosphate is active against HIV reverse transcriptase.HIV reverse transcriptase.
1-? -D-2,6-diaminopurinedioxolane
DAPD
dioxolanedioxolane guanosineguanosine
DXGDXG
NH2NHO
O
ON
NNH
O
N
NN
N
NH2
NH2
OHO
O

Monotherapy vs. Combination Monotherapy vs. Combination
Therapy for HBV (I)Therapy for HBV (I) Increased initial cost of combination therapy offset by
greater clinician and patient acceptance of treatment due to:
- greater efficacy, more frequent durable responses
- finite-length treatment regimens
Combination treatments need a virologic rationale from Phase II studies - clinical efficacy and safety still need to be established in large controlled Phase III trials
Combination treatments currently being investigated: Interferons plus lamivudine (Schering, Roche and GlaxoSmithKline)
Lamivudine plus adefovir (GlaxoSmithKline and Gilead)
LdT plus lamivudine (Novirio)

ConclusionsConclusions
HBV infection has worse outcomes in HIV Lamivudine resistance is becoming
increasinly common Newer drugs that have activity against LAM
resistant HBV are coming soon Treating HBV in HIV patients is getting more
challenging daily

Prevention Vaccine less effective due to
immunosuppression - 30 % (2.5 %) Vaccination repeated - double dose
in four steps (months 0,1,6 and12) Post Exposure Prophylaxis as in
normal individuals

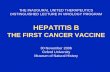
Worldwide Prevalence of Hepatitis C
<1
1-2.49
2.5-4.99
5-10
>10
No data
HCV Prevalence

HIV and HCV 30 % of HIV pts can have HCV infection Less likely to clear HCV in co-infected Higher HCV RNA viral load Rapid progression of liver disease -
CD4 <100; 10 yrs vs 20 yrs for Cirrhosis
In Haemophiliacs – higher mortality in co-infected

HCV and HIV
More rapid deterioration of HIV disease CD4 count may not rise much
blunted immune response - HAART

HCV co infection & HAART Drug induced heaptotoxicity more in
co infected – protease inhibitors & ATT 88% co infected pts tolerated HAART
well without hepatotoxicity Antiretrovirals safe in Chronic hepatitis
C Stop Rx – if symptomatic or Liver
enzymes > 5 x normal

HIV & HCV Screen by ELISA – Confirm by RNA
PCR If CD4 count < 100 – Anti HCV may
be low or undetectable
HCV RNA should be done if suspeected

HIV – HCV : Management Avoid Alcohol Vaccinate against HAV & HBV Look for Chronic Liver disease SGPT, HCV RNA – Limited usefulness Liver Biopsy for disease activity
Liver biopsy safe in HIV infected persons

HIV HCV - Treatment HCV to be treated before HIV Peg Interferons with Ribavarin ideal Limited data on its safety in co
infected Significant side effects for Peg IFN
and Ribavarin reported Drug interactions – Ribavarin vs HIV
drugs

CD4 count & HAART If > 350 , IFN and HAART 200 – 350, individual case < 200 IFN relative contra indication might
deteriorate Didanosine contraindicated - Pancreatitis,
mitochondrial toxicity,liver decompensation Zidovudine avoid - additive toxicities
anemia and leukopenia Stavudine - due to mitochondrial toxicity

Guide lines for therapy-HIV HCV Review HIV – CD4 counts HCV RNA, SGPT, Liver Biopsy Exclude co morbid conditionsDuring therapy Blood counts, SGPT, HCV RNA – Adjust HCV RNA at 24 wks – If detected – stop Birth control during & 6 months after
Rx

HCV anti bodiesHCV anti bodies
negativenegativePositivePositive
HCV RNAHCV RNA negativenegative
negativenegative
SGPT, GenotypeSGPT, Genotype elevatedelevated
normalnormal Peg IFNPeg IFN
Liver BxLiver Bx
negativenegative
Positive Positive

Related Documents