Healthy Hospitals Controlling Pests Without Harmful Pesticides Healthy Hospitals Controlling Pests Without Harmful Pesticides Written by Kagan Owens, Beyond Pesticides A R E P O R T B Y Healthy Hospitals Controlling Pests Without Harmful Pesticides Written by Kagan Owens, Beyond Pesticides A R E P O R T B Y

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Healthy HospitalsControlling Pests WithoutHarmful Pesticides
Healthy HospitalsControlling Pests WithoutHarmful PesticidesWritten by Kagan Owens, Beyond Pesticides
A R E P O R T B Y
Healthy HospitalsControlling Pests WithoutHarmful PesticidesWritten by Kagan Owens, Beyond Pesticides
A R E P O R T B Y
Beyond PesticidesBeyond Pesticides, founded in 1981 as the National Coalition Against the Misuse of Pesticides, is a national, community-basedorganization of grassroots groups and individuals, which bridges environment, health, urban, and rural concerns to: (i) stimulatewidespread education on the hazards of toxic pesticides, and the availability of effective alternative pest management approaches in thecontext of protecting the public’s health; (ii) influence decision makers responsible for pest management to use safe methods throughgrassroots action; and, (iii) encourage the adoption of local, state, and national polices that stringently restrict pesticide use and promotealternative approaches that respect health and the environment.
Beyond Pesticides ● 701 E Street, SE Suite 200 ● Washington DC 20003(202) 543-5450 ● [email protected] ● www.beyondpesticides.org
Health Care Without HarmHealth Care Without Harm (HCWH) is an international coalition of hospitals and health care systems, medical professionals, communitygroups, health-affected constituencies, labor unions, environmental and environmental health organizations and religious groups. Itsmission is to transform the health care industry worldwide, without compromising patient safety or care, so that it is ecologicallysustainable and no longer a source of harm to public health and the environment.
Health Care Without Harm ● 1755 S Street, NW, Suite 6B ● Washington DC 20009202-234-0091 ● [email protected] ● www.noharm.org
AcknowledgementsThis report is the vision of a Health Care Without Harm (HCWH) workgroup comprised of Jackie Hunt Christensen, Institute forAgriculture and Trade Policy; Mary Lamielle, National Center for Environmental Health Strategies, Inc.; Ann McCampbell, M.D.,Multiple Chemical Sensitivities Task Force of New Mexico; Alice Osherman, MCS: Health and Environment; Catherine Porter, Women’sCancer Resource Center; Peggy Wolff, Chemical Injury Information Network; Barbara Wilkie, Environmental Health Network; andCarolyn Wysocki, Ecological Health Organization. This workgroup consulted with Beyond Pesticides to compile the Hospital PesticideUse Survey data and create this report.
Beyond Pesticides and Health Care Without Harm would like to acknowledge all those who provided valuable input into Healthy Hospitals.Sincere appreciation goes to Ann McCampbell, M.D., Multiple Chemical Sensitivities Task Force of New Mexico, and Jay Feldman,Beyond Pesticides, for extensive contributions to the writing and production of this report. Special thanks to Charlotte Brody, R.N., HealthCare Without Harm; Jackie Hunt Christensen, Institute for Agriculture and Trade Policy; Lynn Garske, Kaiser Permanente; Kathy Gerwig,Kaiser Permanente; Mary Lamielle, National Center for Environmental Health Strategies, Inc.; Peter Orris, M.D., University of IllinoisSchool of Public Health; Catherine Porter, Women’s Cancer Resource Center; Ted Schettler, M.D., Science and Environmental HealthNetwork; Terry Shistar, Kaw Valley Greens; Julie Trocchio, Catholic Health Association; and Barbara Wilkie, Environmental HealthNetwork, for their thoughtful comments and editorial guidance. Thanks are also due to Beyond Pesticides staff, Meghan Taylor, andinterns, Cortney Piper and Edward J. Lubarsky, for their research assistance, and to Rick Bass, Brigham and Women’s Hospital, and DeannaSimon, San Francisco Department of the Environment.
Beyond Pesticides thanks its members, supporters and institutional donors for their financial support vital to this project, including theFiredoll Foundation, Health Care Without Harm, David Katz Foundation, Alida Messinger Lead Charitable Trust, David H. SmithFoundation, Lucy R. Waletzky Fund, and Wallace Genetic Foundation.
Health Care Without Harm also thanks its institutional donors for their support, including Lucy Waletzky.
This document is for educational purposes only and does not constitute legal or health advice. Health care providers and institutions shouldseek legal and medical advice to ensure that pest management programs meet legal and patient care responsibilities, including compliancewith applicable pesticide notification laws and regulations.

Healthy Hospitals Controlling Pests Without Harmful Pesticides
i
B E Y O N D P E S T I C I D E S & H E A L T H C A R E W I T H O U T H A R M
Table o
f Conte
nts Preface by Jackie Hunt Christensen . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1
Executive Summary. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2
I. The Pesticide Problem . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4Pesticide Toxicology . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4Health Effects of Pesticides . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4The Hazards of “Inert” Ingredients . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5Pesticide Exposure Routes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6Pesticide Efficacy and Resistance . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7Pesticide Regulation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10Limited and Misleading Information on Product Label . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10Missing Toxicity Data . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11Pesticide Laws Allow An “Acceptable” Risk . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11
II. Hospital Pesticide Use Survey Findings . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12Methodology . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12Summary of Survey Findings . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12Hospital Pest Management Plans . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13Hospital Integrated Pest Management (IPM) Programs . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13In-House versus Contract Pest Management . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14Hospital Pesticide Use . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15Least Hazardous Pesticide Use . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16Hospital Use of Cancelled Pesticide Products and Active Ingredients. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16Hospital Pesticide Use Notification . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 18Record Keeping . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 19Staff Training on Pesticide Health Effects. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 19Cost of Hospital Pest Management . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 19
III. Safer Pest Management Practices . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 24Integrated Pest Management (IPM): A Safer Solution . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 26Key Elements of an IPM Program . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 27Education . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 27Monitoring . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 27Pest Prevention . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 27Least Hazardous Approach to Pests . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 29Pesticide Use Notification . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 30Record Keeping . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 30IPM is Cost Effective . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 31Examples of Hospital IPM Programs . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 32
Veterans Hospitals . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 32Oregon Health and Science University. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 32
Healt
hy Ho
spita
ls
Contro
lling P
ests W
ithout
Harm
ful Pe
sticide
s
ii
San Francisco General Hospital. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 33Massachusetts General Hospital . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 33Brigham and Women’s Hospital . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 33Hackensack University Medical Center. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 33
IV. Conclusion and Recommendations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 38
V. Appendix . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 40Resource List . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 40Model Hospital Integrated Pest Management (IPM) Policy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 41Hospital Pesticide Use Cover Letter and Survey . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 43Hospital Pesticide Use Survey Results. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 47
VI. Endnotes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 52
Side Bars, Charts and Tables Figure 1. What Is In a Pesticide? . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4Figure 2. Pesticide Toxicity Warning Label. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5Figure 3. Hospital Pesticide Incident Reports . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6Figure 4. Illinois Hospital Pesticide Use Restriction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7Figure 5. Overview of Commonly Used Herbicides. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8Figure 6. Overview of Commonly Used Insecticides . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9Figure 7. Pesticide Registration Does Not Equal Safety . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10Figure 8. Hospitals with Written Pest Management Plans . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12Figure 9. Hospitals Using an IPM Approach . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13Figure 10. Hospital Structural Pest Management, Managed In-House or by Hired Company. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14Figure 11. Outdoor Hospital Pest Management, Managed In-House or by Hired Company. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14Figure 12. Hospitals’ Indoor Chemical Pesticide Use . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15Figure 13. Hospitals’ Outdoor Chemical Pesticide Use . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15Figure 14. Surveyed Hospitals Most Commonly Used Insecticides, By Chemical Family . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15Figure 15. Hospital Use of Cancelled Pesticide Products . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16Figure 16. Cancelled Pesticide Products Used at Surveyed Hospitals . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 17Figure 17. Hospitals Posting Indoor Pesticide Notification Signs. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 18Figure 18. Hospitals Posting Outdoor Pesticide Notification Signs . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 18Figure 19. Cost of Hospital Pest Management. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 19Figure 20. Health Effects of 37 Pesticide Active Ingredients Most Commonly Used at Surveyed Hospitals . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 20-21Figure 21. Ecological Effects of 37 Pesticide Active Ingredients Most Commonly Used at Surveyed Hospitals . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 22-23Figure 22. Health Care Community Supports IPM. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 25Figure 23. Integrated Pest Management (IPM) Defined . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 26Figure 24. Examples of Safer Pest Management for Hospital Pests. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 28Figure 25. Non-toxic Landscape and Grounds Management . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 29Figure 26. Overview of Select Least Hazardous Pesticides . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 29Figure 27. Baits: The Better Option. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 30Figure 28. Model Notification Program. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 30Figure 29. States With Lawn Notification Requirements . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 31Figure 30. A Closer Look at San Francisco General Hospital’s IPM Program . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 34-35Figure 31. A Closer Look at Brigham and Women’s Hospital’s IPM Program . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 36-37
B E Y O N D P E S T I C I D E S & H E A L T H C A R E W I T H O U T H A R M

Healthy Hospitals Controlling Pests Without Harmful Pesticides
1
B E Y O N D P E S T I C I D E S & H E A L T H C A R E W I T H O U T H A R M
P r e f a c eHealth Care Without Harm (HCWH) wasborn in September 1996 when representativesfrom 28 organizations gathered atCommonweal in Bolinas, California. Those ofus who participated had a very specific agenda:to see if we had “critical mass” in opposition tomedical waste incineration. We were focusedprimarily on the hazards of dioxin and mercu-ry emissions, although we certainly werethinking about the broader implications ofhealth care’s environmental impacts when wedeveloped our mission: “to transform thehealth care industry so that it is no longer asource of environmental harm, without com-promising safety or care.”
We knew that health care providers were notpolluting the environment and people’s bodiesout of any malicious intent, but because theylacked sufficient information about the hazardsof their activities. We believed that when giventhe data and the choice, the health care indus-try would choose to “first, do no harm,” andindeed, this has most often been the case.
Through the work of our member organiza-tions, Health Care Without Harm hassuccessfully influenced the reduction of hospi-tal emissions of dioxin and mercury and theclosure of many medical waste incinerators.Our 427 member organizations include healthcare systems, organizations of health profes-sionals, labor, environmental groups, religiousorganizations and health-advocacy groups in52 countries.
As Health Care Without Harm has grown andour membership has become more diverse, wehave looked beyond dioxin and mercury topursue other issues that were not previously “onthe radar screens” of health care administrators,staff, and clinicians, including the goal of mak-ing hospital environments safer for bothpatients and workers. These issues include:
● The potential health risks of phthalateplasticizers leaching from polyvinyl chlo-ride (PVC) medical devices;
● Economically and environmentally viablealternatives to medical waste incinerators,including low-cost options for developingcountries;
● The connection between what comes inthe front door of the facility (purchasing)and what goes out the back (environmen-tal services/housekeeping), and the needfor good communication between alldepartments; and,
● The potential adverse health impacts ofbuilding materials and furnishings used inconstruction or remodeling of a facility.
In this report, we shine the spotlight on pesti-cides, another avoidable hazard commonlypresent in hospitals. When we began to lookinto this issue, we discovered there was very lit-tle information available on the quantities ortypes of pesticides being applied inside andoutside of hospitals and clinics. Therefore, ourfirst step was to create a survey to gather dataourselves.
We began with U.S. News & World Report’s2001 “Top Hospitals” list of 171 hospitals thatreceived the survey, but focused on 100 facili-ties in or near cities where HCWH membergroups were located or had contacts. Of the
171 hospitals contacted, 22 surveys werereturned after numerous phone calls, lettersand in some cases, visits by HCWH members.Our survey process was not intended to gener-ate fully representative scientific data, but webelieve that the data collected provide aninstructive “snapshot” of what some of thenation’s preeminent health care facilities aredoing for pest control. The survey can also beused as a helpful tool for hospital or health sys-tems to assess their pest management andpesticide use and to monitor their progress overtime.
Although many people have come to assumethat applying pesticides is the only way to con-trol pests and ensure a clean, healthy healthcare facility, this report shows that pests can besuccessfully managed without toxic pesticidesand without having an adverse effect on thequality of patient care. Health care facilitieshave another opportunity to “first, do no harm”by changing the way they view pest control andby following this guide to safer and effectiveintegrated pest management.
Jackie Hunt ChristensenHealth Care Without HarmNovember 2003
Healt
hy Ho
spita
ls
Contro
lling P
ests W
ithout
Harm
ful Pe
sticide
s
2
E x e c u t i v eS u m m a r yHospitals are intended to be places for healthand healing. Yet the findings of a survey of topU.S. hospitals indicate that major hospitals inthe U.S. are regularly using toxic pesticides.This puts the health of patients and staff atrisk and raises questions about the safety ofhospitals.
In order to better understand the current stateof hospital pest management, Health CareWithout Harm (HCWH) distributed surveysto the 171 top U.S. hospital facilities, as citedin U.S. News and World Report (2001). Surveyresults show that while some hospitals reportusing least hazardous approaches and/or pro-vide notification of pesticide use, there is stillconsiderable pesticide use at hospital facilities,even at hospitals that report using the safermethod of pest management called IntegratedPest Management (IPM). The major findingsof the survey show that of the 22 respondinghospitals:
● 100% use chemical pesticide productseither on their grounds, inside the build-ings or both;
● 91% use chemical pesticide indoors and77% use chemical pesticides outdoors;
● 36% use pesticide products that are nolonger registered for use by the U.S.Environmental Protection Agency (EPA);
● 18% use a pesticide product in which theactive ingredient is being phased out by
EPA due to the unacceptable risk associ-ated with its use; and
● 73% hire a pest control company to man-age the majority of the hospital’s structur-al pest management program and 41%hire a pest control company to managethe majority of the hospital’s grounds;
The survey findings also indicate that at leastsome of the responding hospitals are making aneffort to reduce their pesticide use and/or noti-fy staff and patients when pesticides are used,thus reducing patients’ toxic exposure. Of theresponding hospitals:
● 73% report using an IPM approach topest management;
● 45% use one or more pesticide productscontaining boric acid, a least hazardouspesticide;
● 14% post notification signs for bothindoor and outdoor pesticide applica-tions; and,
● 27% have provided pesticide-poisoningtraining for their staff.
This landmark report is intended to informhospital officials, the public and policy makersabout (a) a number of potential health hazardsassociated with the use of pesticides in hospi-tals, (b) the findings of a national hospital pestmanagement practices survey, and (c) the avail-ability of and need for safer pest managementpractices and disclosure of hospital pesticideuse to patients, visitors and staff.
While it is essential that hospitals maintain aclean environment free of pests that threatenhealth, it is also important that patients, staff,and visitors be protected from exposure to pes-ticides. Hospital patients who have compromised
immune and nervous systems, the elderly,infants and children, and those who have anallergy or sensitivity to pesticides are particular-ly vulnerable to their toxic effects. Patientstaking certain medications may also haveheightened reactions to pesticides.
“Pest management in health care facilities dif-fers from control practices in other types ofinstitutions,” states the Department of VeteranAffairs. “The effect on patients in various stagesof debilitation and convalescence, and in variedphysical and attitudinal environments, requiresthat a cautious, conservation policy be adoptedconcerning all uses of pesticides. The use of anypesticide establishes a risk of uncertain magni-tude.”1
The American Medical Association’s Councilon Scientific Affairs states, “Particular uncer-tainty exists regarding the long-term healtheffects of low dose pesticide exposure. Currentsurveillance systems are inadequate to charac-terize potential exposure problems relatedeither to pesticide usage or pesticide-related ill-nesses. Considering these data gaps, it isprudent for homeowners, farmers, and workersto limit pesticide exposures to themselves andothers, and to use the least toxic chemical pes-ticide or nonchemical alternative.”2
Pesticides are hazardous chemicals designed tokill or repel insects, plants, and animals that areundesirable or that threaten human health.Many of them contain volatile compounds thatcontribute to poor indoor air quality. In addi-tion to killing pests and beneficial organisms,in humans pesticides can exacerbate asthmaand cause other acute adverse effects includingnausea, headaches, rashes, and dizziness. Manypesticides are also linked to chronic effects,such as cancer, birth defects, neurological and
B E Y O N D P E S T I C I D E S & H E A L T H C A R E W I T H O U T H A R M

Healthy Hospitals Controlling Pests Without Harmful Pesticides
3
B E Y O N D P E S T I C I D E S & H E A L T H C A R E W I T H O U T H A R M
reproductive disorders, and development ofchemical sensitivities. Pesticide poisonings arefrequently misdiagnosed or unrecognized,largely because most health care providersreceive minimal training in environmental ill-nesses and few people know when they havebeen exposed to a pesticide.
Why Focus on Hospitals? There are 5,810 registered hospitals in theU.S.3 that see about 32 million inpatients, 83million outpatients and 108 million emergencyroom patients per year.4 Thus a large number ofindividuals may be exposed to toxic pesticidesin health care settings. Some hospital patientsare especially vulnerable to the toxic effects ofpesticides.5
Hospitals have a special obligation to demon-strate leadership in instituting effective andsafer pest management in keeping with themedical profession’s basic tenet of “first, do noharm.”
Fortunately, a method of pest control calledIntegrated Pest Management (IPM) eliminatesor greatly reduces the need to respond to pestswith hazardous pesticide products and helpsensure a healthier environment for hospitalpatients, staff, and visitors. The focus of IPM isto prevent pest problems by reducing or elimi-nating sources of pest food, water, and shelterin hospitals and on their grounds and by main-taining healthy lawns and landscapes. The firstapproach to controlling a pest outbreak isimproving sanitation, making structural repairs(such as fixing leaky pipes and caulking cracks),and using physical or mechanical controls suchas screens, traps and weeders. A least hazardouschemical is used only when other strategieshave failed. If a pesticide is used, the hospital
community must be notified prior to the appli-cation in order to take necessary precautions.
IPM strategies are successfully being imple-mented at schools, parks, government facilitiesand hospitals nationwide. For example, IPMprograms at Oregon Health and SciencesUniversity, Brigham and Women’s Hospital,Harvard University, the City of San Francisco,Seattle Parks and Recreation Department, NewYork City Public Schools, the General ServicesAdministration demonstrate that IPM can beeconomically and effectively implemented.
This report, along with the 1995 reports, AFailure to Protect by Beyond Pesticides and theNew York Attorney’s General report PestManagement in New York State Hospitals, addsto the data available on the types and amountsof pesticides used at health care facilities acrossthe country. It confirms and elaborates on pre-vious findings that hazardous pesticides arecommonly used in U.S. hospitals.(Antimicrobial chemicals are not addressed inthis report.)
RecommendationsWhile some hospitals are using an IntegratedPest Management (IPM) approach to manag-ing pests, it appears that the majority of U.S.hospitals have an urgent need to adopt saferpest management practices. Implementation ofcost-effective IPM programs can eliminate theunnecessary use of hazardous pesticides thatthreaten the health of patients and staff.Hospitals, government entities, the public andthe pest management industry can all takeaction to increase the number of hospitalsadopting least hazardous IPM programs.
Healt
hy Ho
spita
ls
Contro
lling P
ests W
ithout
Harm
ful Pe
sticide
s
4
I . T h e P e s t i c i d eP r o b l e mThe U.S. Environmental Protection Agency(EPA) states that, “By their very nature, mostpesticides create some risk of harm to humans,animals, or the environment because they aredesigned to kill or otherwise adversely affectliving organisms.”6 And yet, with the wide-spread use of pesticides, including use inhospitals, people are frequently exposed tomultiple pesticides in the air they breathe, thewater they drink and the food they eat. It istherefore not surprising that pesticides are amajor source of environmental and publichealth poisonings.7
The U.S. uses an enormous volume of pesti-cides—approximately 4.5 billion poundsannually. Currently, there are 890 pesticideactive ingredients registered for use by EPA,8
320 of those are registered for use in hospitals9
and many others are registered for lawn andlandscape use.
Pesticide ToxicologyEveryday the public is exposed to toxic pesti-cides linked to a wide range of health problems.
Health Effects of PesticidesAlthough the toxicity of individual pesticidesvary, typical symptoms that can result from anacute pesticide exposure include nausea, dizzi-ness, headaches, aching joints, mentaldisorientation, inability to concentrate, vomit-ing, convulsions, skin irritations, flu-like
B E Y O N D P E S T I C I D E S & H E A L T H C A R E W I T H O U T H A R M
FIGURE 1. WHAT IS IN A PESTICIDE?
A pesticide product is a mixture of chemicals used to kill, repel or otherwise control insects, weeds,rodents, fungi or other pests. Pesticides include insecticides, herbicides, fungicides, rodenticides, andother products active against pests. Pesticide products are formulations of a number of differentmaterials, including active and “inert” ingredients, as well as contaminants and impurities. In addi-tion, pesticides, when subject to various environmental conditions, break down into other materialsknown as metabolites, which are sometimes more toxic than the parent material.
Active Ingredients, usually the only compo-nents of the formulation listed on the pesticidelabel, are biologically and chemically activeagainst a target pest. By definition it is thesechemicals that kill or repel living things. Activeingredients also include synergists.
“Inert” Ingredients are the carrier or stickingagent in the pesticide product. They may be sol-vents, stabilizers, preservatives, surfactants,sticking or spreading agents, or defoamers.10
Quite often these ingredients constitute over95% of the pesticide product. Some “inert”ingredients are as or more toxic than the activeingredient and/or may be an active ingredientin another pesticide product.
Synergists are chemicals that are added to apesticide product to increase the potency of theactive ingredient(s). Piperonyl butoxide (PBO)and n-octyl bicycloheptene dicarbozimide arepesticide synergists that reduce insects’ ability tobreakdown the active ingredient. PBO is a livertoxicant and a possible human carcinogen.11
Pyrethroid, pyrethrin, and carbamate-containingpesticide products are the pesticides that mostoften contain PBO.
Contaminants and Impurities are byproductsof the manufacturing process that are oftenfound in pesticide products and can contributeto a product’s toxicity. For example, dioxin hasbeen identified as a contaminant in some herbi-cides.12
Metabolites are breakdown products that formwhen a pesticide is exposed to air, water, soil,sunlight or living organisms. Often the metabo-lite is more hazardous than the parent com-pound.
General Use Pesticide vs. Restricted Use PesticideBy law, pesticide products must be registered byEPA and the state in which they are used, andapplied according to label instructions. Generaluse pesticides can be applied by anyone,whereas restricted use pesticides may only beapplied by licensed applicators.
Healthy Hospitals Controlling Pests Without Harmful Pesticides
5
B E Y O N D P E S T I C I D E S & H E A L T H C A R E W I T H O U T H A R M
symptoms and asthma-like problems.13 In somecases, a person can develop chronic healthproblems following an acute poisoning.14 Low-level pesticide exposure over a period of timemay also result in chronic health effects.Pesticides are linked to a wide range of chronichealth problems including cancer, birth defects,genetic damage, neurological, psychologicaland behavioral effects, blood disorders, chemi-cal sensitivities, reproductive effects, andabnormalities in liver, kidney, and immune sys-tem function.15
Many insecticides, herbicides and fungicidesare linked to certain types of cancer, includingthose of the lip, stomach, and prostate, as wellas leukemia, lymphatic cancers, and multiple
myeloma.16 Non-Hodgkin’s lymphoma hasbeen linked to the use of the commonly usedweed killer 2,4-D.17 Studies show that childrenliving in households where pesticides are usedsuffer elevated rates of leukemia, brain cancerand soft tissue sarcoma.18
Pregnant women, children, the chemically sen-sitive, elderly and chronically ill are at greaterrisk from pesticide exposure than others.Studies in laboratory animals raise concernsthat patients taking certain medications mayalso have heightened reactions to some pesti-cides.19 Pesticides can affect the immune andnervous system and result in increased prob-lems with allergies, asthma, andhypersensitivity to chemicals.20 Some individu-als with multiple chemical sensitivities (MCS),i.e. those with the most severe chemical sensi-tivities, have been reported to react adversely toeven minute levels of pesticide residues, includ-ing those resulting from pesticide applicationsmade months or even years earlier.21
Pesticide poisonings are frequently misdiagnosedor unrecognized. All too often victims of pesti-cide exposure never realize the source of theirsymptoms or illness, even after visiting a physi-cian.22 Unfortunately, most health care providersreceive minimal training in environmental ill-nesses. EPA and other government agencies haveteamed with the National EnvironmentalEducation & Training Foundation (NEETF) totry to address this problem. They have publishedthe National Strategies for Health Care Providers:Pesticides Initiative Implementation Plan, a 10-year plan designed to improve prevention,recognition and management of pesticide poi-sonings by increasing the education ofphysicians, nurses and other health careproviders about pesticides.23
The Hazards of “Inert” IngredientsWhile most discussion on pesticides focuses onactive ingredients, pesticide formulations con-tain a majority of so-called “inert” ingredients.They form the solution, dust, or granule inwhich the active ingredient is mixed and gener-ally make up the largest percentage ofingredients in a pesticide product. Many arepetrochemical solvents like acetone, fuel oil,toluene and other benzene-like chemicals.28
Despite the term “inert,” these ingredients maynot be chemically, biologically or toxicological-ly inert. In fact, “inert” ingredients can be moretoxic than the active ingredient and/or be anactive ingredient in another pesticide product.29
Under the Federal Insecticide, Fungicide andRodenticide Act (FIFRA), pesticide manufactur-ers are only required to reveal the activeingredients in a pesticide. The law allows“inert” ingredients to remain trade secret infor-mation. This leaves consumers and applicatorsunaware of the possible toxic chemicals presentin the “inert” ingredients of pesticide productsthey are using.
A 2000 report by the New York State AttorneyGeneral, The Secret Ingredients in Pesticides:Reducing the Risk, found that 72 percent of pes-ticide products available to consumers containover 95 percent “inert” ingredients; fewer than10 percent of pesticide products list any of the“inert” ingredients on their labels; and, of a1995 list of “inert” ingredients, 394 chemicalswere listed as active ingredients in other pesti-cide products.30
In general, EPA requires little toxicity datafrom manufacturers on “inert” ingredientsbefore registering a pesticide product. However,many of these chemicals are known to state,
FIGURE 2. PESTICIDE TOXICITY WARNING LABEL
Pesticide product labels contain a toxicity warningsignal word of either “Danger” for the highest toxicitycategory, “Warning” for moderate toxicity, or“Caution” for the lowest toxicity. The toxicity ratingsonly apply to the acute toxicity of the product. Thewarning labels, therefore, do not take into account aproduct’s ability to cause chronic effects such as can-cer, birth defects, genetic mutations, multiple chemi-cal sensitivities (MCS), or other long-term damage tothe respiratory, immune or neurological systems.
In addition, the acute toxicity categories ignore thesubstantial variations in health impacts of pesticideson different people. For example, individuals whohave allergies or sensitivities to pesticides can bemade very sick from exposures to pesticides even ifthose pesticides carry a low acute toxicity rating.
Healt
hy Ho
spita
ls
Contro
lling P
ests W
ithout
Harm
ful Pe
sticide
s
6
federal and international agencies to be haz-ardous to human health. According to aninvestigative report by the Northwest Coalitionfor Alternatives to Pesticides, 209 “inerts” usedin pesticide products are identified as haz-ardous pollutants in federal environmentalstatutes governing air and water quality, 14have been assessed as “extremely hazardous,” 84are reportable to the Toxic Chemical ReleaseInventory, 21 are known or suspected carcino-gens, and 127 are regarded as occupationalhazards.31
“Many consumers are mislead by the term ‘inertingredients,’ believing it to mean ‘harmless,’”states EPA. “Since neither the federal law northe regulations define the term ‘inert’ on thebasis of toxicity, hazard or risk to humans, non-target species, or the environment, it should notbe assumed that all inert ingredients are non-toxic.”32 In 1997, EPA began asking pesticideregistrants to voluntarily refer to “inert” ingredi-ents as “other” ingredients on product labels inorder to try to minimize the misconception thatinert ingredients are harmless.33 However, fewmanufacturers have done so.
Pesticide Exposure RoutesHuman exposure to pesticides takes place bybreathing in pesticide fumes or dust laden withpesticides, consuming water or food contami-nated with pesticides, or by touching surfacescontaminated with pesticides and absorbingthem through the skin. When an individualdetects a pesticide’s odor, that person is alsoinhaling the pesticide. And, even if no odor isdetected, such as after “low odor” products areapplied, one can still be breathing in the pesti-cide’s vapors. If touched, pesticide residues canbe absorbed through the skin. This type ofexposure commonly occurs when children or
FIGURE 3. HOSPITAL PESTICIDE INCIDENT REPORTS
A hospital staff person in Oklahoma became sick after she was exposed toDursban 4ETM (active ingredient chlorpyrifos) on the job. Following the exposure,she became sensitive to a host of chemicals.24 A medical professional diagnosedher as having been poisoned by the pesticide. After the incident was reported to theOklahoma Department of Agriculture and EPA, the hospital was cited for improperuse of pesticides.25
A woman in Pennsylvania was sitting in a hospital waiting room when she devel-oped difficulty breathing and nausea. She noticed a strong odor. It turned out to bethe fumes of the insecticide FicamTM (active ingredient bendiocarb) being sprayed bya commercial pest control company in an adjacent room. The applicator told herthat it would not hurt her and led her to believe that the pesticide was safe. Thewoman’s doctor conducted urine, blood and nerve tests and diagnosed her as hav-ing been poisoned by a pesticide. She reported the incident to the PennsylvaniaDepartment of Health, but their investigation found that the company had not mis-applied the pesticide and that there was nothing more they could do. The womanwrote a letter to the hospital voicing her concerns about chemicals used at the hos-pital. The hospital wrote a letter in response stating, “The pesticides used … areacceptable for use in medical facilities and do not jeopardize the health of staffand/or patients.” The hospital stated that the pest control contractor would makefuture pesticide applications “as late in the clinic day as possible.”26
A woman entered the outpatient area of a New Jersey hospital for laboratory test-ing early one Saturday morning. She immediately experienced a severe headache,weakness and tremors. She asked the only hospital employee in the vicinity if anychemicals had been used in the area. She was told that someone had just sprayedpesticides. She immediately returned home and later placed a number of calls tothe hospital but was unable to obtain any additional information on the pesticideapplication. In a separate incident at this same facility, the woman was beingdropped off at the entrance to the outpatient lab. As she began to get out of thecar, she saw an individual in protective clothing and a respirator spraying lawn carepesticides at the building entrance, about 10 feet from her. She left immediatelyand was driven home. Nevertheless, those few minutes of exposure were sufficientto cause a severe reaction that included visual disturbances, headache, difficultybreathing, tremors, severe weakness, and confusion. She was in bed for two daysfollowing the exposure with severe fatigue and weakness.27
B E Y O N D P E S T I C I D E S & H E A L T H C A R E W I T H O U T H A R M

Healthy Hospitals Controlling Pests Without Harmful Pesticides
7
B E Y O N D P E S T I C I D E S & H E A L T H C A R E W I T H O U T H A R M
pets roll around on lawns that have been treat-ed with herbicides. Despite a commonmisconception, harmful exposure to a pesticidedoes not end when a pesticide dries. Theresidues can linger for hours, days and evenmonths after an application.34 Pesticides can alsobe tracked inside from outdoor applications orcarried from a treated part of a building to anuntreated section.
In a study looking at the persistence of pesti-cides, airborne concentrations of seveninsecticides were tested for three days followingtheir application in separate rooms in an unoc-cupied dormitory. Six of the seven pesticideswere found in air samples in the room in whichthey were applied through the third day.35 EPA’sNon-Occupational Pesticide Exposure Study(NOPES) found that tested households had atleast 5 pesticides in indoor air, at levels often 10times greater than levels measured in outdoorair.36 A recent study found that 2,4-D, the mostcommonly applied lawn herbicide in the coun-try,37 is easily tracked indoors, contaminatingthe air and surfaces inside residences at levelsten times higher than pre-application levels.38
The type of pesticide formulation and applica-tion method influences the potential forhuman exposure. Spraying a pesticide suspendsthe chemical into the air resulting in a greater
potential for the chemical to drift from theapplication site. Baits generally are of low orvery low volatility and are not likely to pose thehigh exposure risks associated with sprays. Asmall percentage of sprayed pesticides, whetherapplied indoors or outdoors, reaches the targetorganism.39 When pesticides are sprayed out-doors there is almost inevitable pesticide drifton to non-target areas via wind or thermal cur-rents.40
Just this year, there have been several studiesthat confirm that exposure to pesticides andother chemicals leads to human contamination.In January 2003, the Centers for DiseaseControl and Prevention (CDC) released thesecond National Report on Human Exposure toEnvironmental Chemicals, which found evi-dence of 89 chemicals, out of 116 tested, in theblood or urine of study participants. The chem-icals found in study participants includedseveral types of pesticides (organophosphate,organochlorine, and carbamate insecticides;herbicides; pest repellents; and disinfectants).42
A similar study, Body Burden: the Pollution inPeople, led by Mount Sinai School of Medicinein New York in collaboration with theEnvironmental Working Group andCommonweal, was released in February 2003on chemicals found in nine study volunteers.These individuals were tested for 210 chemi-cals, the largest suite of industrial chemicalsever surveyed. The researchers found an averageof 91 industrial compounds, pollutants andother chemicals in the blood and urine of allnine volunteers. In total, 167 chemicals werefound in the group. This included the detec-tion of seven of nine organophosphatemetabolites tested and 10 of 23 organochlorinepesticides and metabolites tested.43
Pesticide Efficacy and ResistanceEPA continues to allow the release of synthetictoxic pesticides into the environment without afull assessment of the efficacy of these productsor the development of pest resistance over time.The result has been the release of hazardousmaterials, including arsenic, organochlorine,organophosphate, carbamate, syntheticpyrethroid and other chemical families, that nolonger eliminate pests, while leaving a trail ofadverse toxic effects.
Reliance on pesticides is a reactive measure, asymptomatic approach to managing pest prob-lems. Applying pesticides on a routine scheduletends to support the habit of ignoring the caus-es of pest infestations. Pesticides are oftentemporary fixes and ineffective over the longterm. Pesticides usually require repetitive use.Spraying for ants, for example, tends to killonly the worker insects, while the queen is safeback in the colony. Since the queen can pro-duce more worker ants, the pest problem is notsolved.44
Hundreds of species of insects, plantpathogens, fungi, nematodes, rodents andweeds have become resistant to pesticides.Resistance “… has become most serious sincethe discovery and widespread use of syntheticorganic compounds,” according to theNational Academy of Sciences (NAS). The1986 report explains why this is the case:
“Some individuals in a pest population may beable to survive initial applications of a chemicaldesigned to kill them, and this survival may bedue to genetic differences rather than to escapefrom full exposure. The breeding population thatsurvives initial applications of pesticide is made upof an ever-increasing proportion of individualsthat are able to resist the compound and to pass
FIGURE 4. ILLINOIS HOSPITAL PESTICIDE
USE RESTRICTION
Illinois is the only state with a law that prohibits theuse of certain pesticides while patients are in thetreated area.41
Healt
hy Ho
spita
ls
Contro
lling P
ests W
ithout
Harm
ful Pe
sticide
s
8B E Y O N D P E S T I C I D E S & H E A L T H C A R E W I T H O U T H A R M
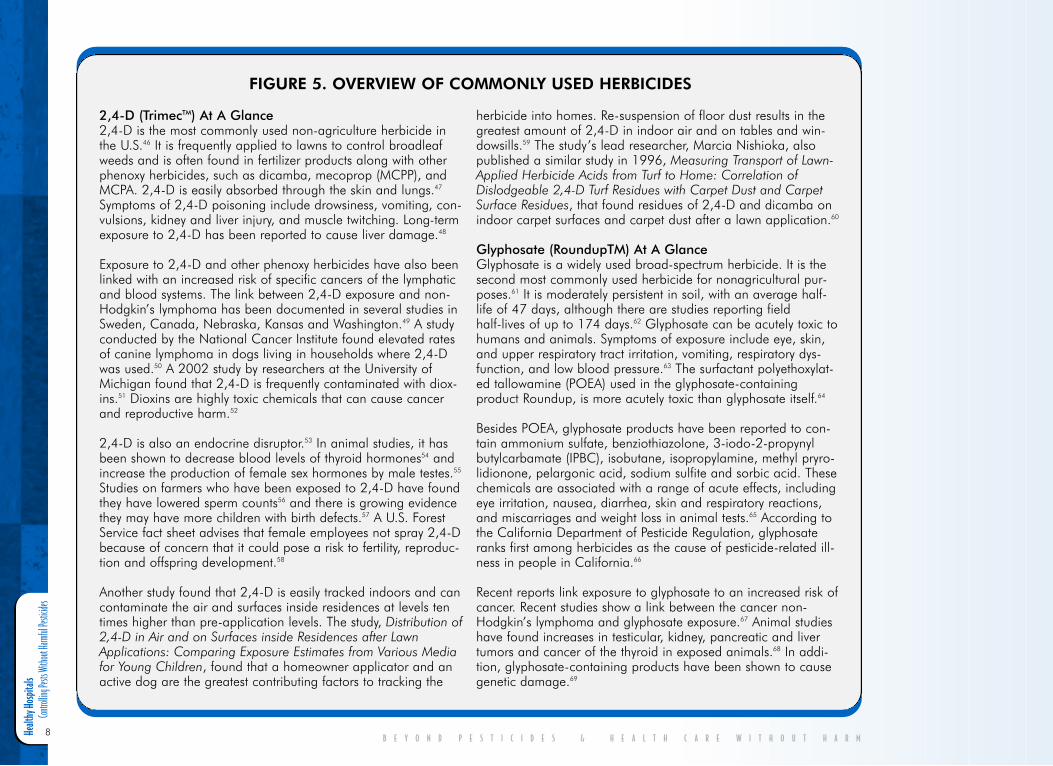
FIGURE 5. OVERVIEW OF COMMONLY USED HERBICIDES
2,4-D (TrimecTM) At A Glance2,4-D is the most commonly used non-agriculture herbicide inthe U.S.46 It is frequently applied to lawns to control broadleafweeds and is often found in fertilizer products along with otherphenoxy herbicides, such as dicamba, mecoprop (MCPP), andMCPA. 2,4-D is easily absorbed through the skin and lungs.47
Symptoms of 2,4-D poisoning include drowsiness, vomiting, con-vulsions, kidney and liver injury, and muscle twitching. Long-termexposure to 2,4-D has been reported to cause liver damage.48
Exposure to 2,4-D and other phenoxy herbicides have also beenlinked with an increased risk of specific cancers of the lymphaticand blood systems. The link between 2,4-D exposure and non-Hodgkin’s lymphoma has been documented in several studies inSweden, Canada, Nebraska, Kansas and Washington.49 A studyconducted by the National Cancer Institute found elevated ratesof canine lymphoma in dogs living in households where 2,4-Dwas used.50 A 2002 study by researchers at the University ofMichigan found that 2,4-D is frequently contaminated with diox-ins.51 Dioxins are highly toxic chemicals that can cause cancerand reproductive harm.52
2,4-D is also an endocrine disruptor.53 In animal studies, it hasbeen shown to decrease blood levels of thyroid hormones54 andincrease the production of female sex hormones by male testes.55
Studies on farmers who have been exposed to 2,4-D have foundthey have lowered sperm counts56 and there is growing evidencethey may have more children with birth defects.57 A U.S. ForestService fact sheet advises that female employees not spray 2,4-Dbecause of concern that it could pose a risk to fertility, reproduc-tion and offspring development.58
Another study found that 2,4-D is easily tracked indoors and cancontaminate the air and surfaces inside residences at levels tentimes higher than pre-application levels. The study, Distribution of2,4-D in Air and on Surfaces inside Residences after LawnApplications: Comparing Exposure Estimates from Various Mediafor Young Children, found that a homeowner applicator and anactive dog are the greatest contributing factors to tracking the
herbicide into homes. Re-suspension of floor dust results in thegreatest amount of 2,4-D in indoor air and on tables and win-dowsills.59 The study’s lead researcher, Marcia Nishioka, alsopublished a similar study in 1996, Measuring Transport of Lawn-Applied Herbicide Acids from Turf to Home: Correlation ofDislodgeable 2,4-D Turf Residues with Carpet Dust and CarpetSurface Residues, that found residues of 2,4-D and dicamba onindoor carpet surfaces and carpet dust after a lawn application.60
Glyphosate (RoundupTM) At A Glance Glyphosate is a widely used broad-spectrum herbicide. It is thesecond most commonly used herbicide for nonagricultural pur-poses.61 It is moderately persistent in soil, with an average half-life of 47 days, although there are studies reporting fieldhalf-lives of up to 174 days.62 Glyphosate can be acutely toxic tohumans and animals. Symptoms of exposure include eye, skin,and upper respiratory tract irritation, vomiting, respiratory dys-function, and low blood pressure.63 The surfactant polyethoxylat-ed tallowamine (POEA) used in the glyphosate-containingproduct Roundup, is more acutely toxic than glyphosate itself.64
Besides POEA, glyphosate products have been reported to con-tain ammonium sulfate, benziothiazolone, 3-iodo-2-propynylbutylcarbamate (IPBC), isobutane, isopropylamine, methyl pryro-lidionone, pelargonic acid, sodium sulfite and sorbic acid. Thesechemicals are associated with a range of acute effects, includingeye irritation, nausea, diarrhea, skin and respiratory reactions,and miscarriages and weight loss in animal tests.65 According tothe California Department of Pesticide Regulation, glyphosateranks first among herbicides as the cause of pesticide-related ill-ness in people in California.66
Recent reports link exposure to glyphosate to an increased risk ofcancer. Recent studies show a link between the cancer non-Hodgkin’s lymphoma and glyphosate exposure.67 Animal studieshave found increases in testicular, kidney, pancreatic and livertumors and cancer of the thyroid in exposed animals.68 In addi-tion, glyphosate-containing products have been shown to causegenetic damage.69
Healthy Hospitals Controlling Pests Without Harmful Pesticides
9
B E Y O N D P E S T I C I D E S & H E A L T H C A R E W I T H O U T H A R M
FIGURE 6. OVERVIEW OF COMMONLY USED INSECTICIDES
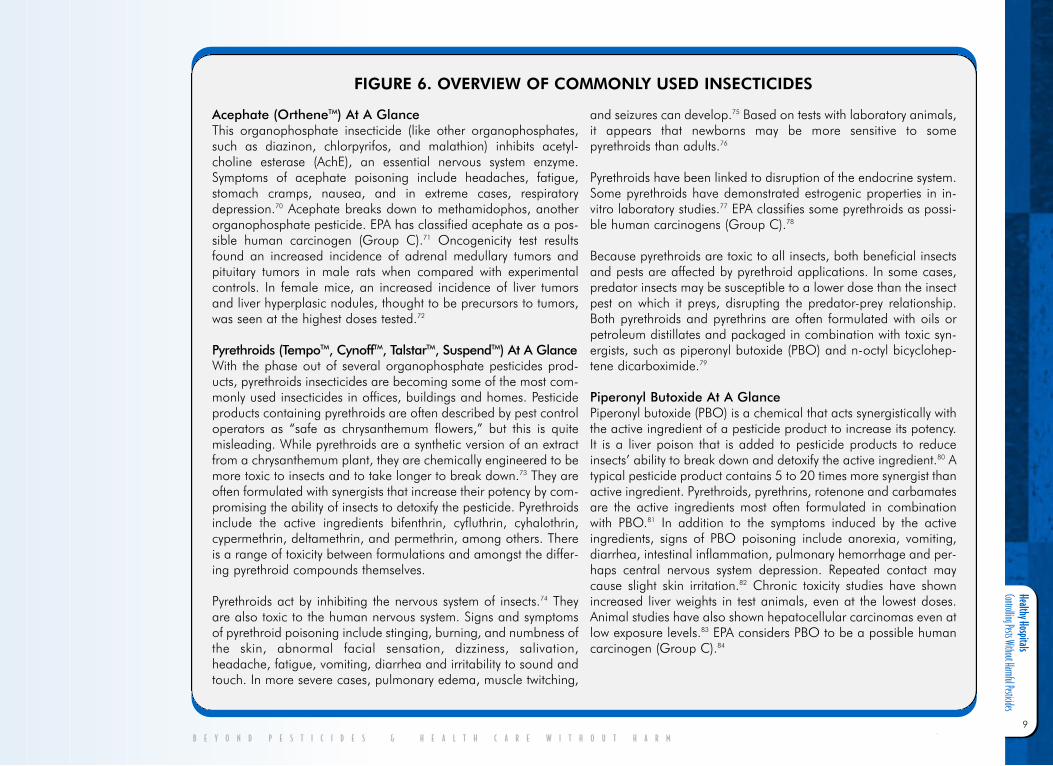
Acephate (OrtheneTM) At A GlanceThis organophosphate insecticide (like other organophosphates,such as diazinon, chlorpyrifos, and malathion) inhibits acetyl-choline esterase (AchE), an essential nervous system enzyme.Symptoms of acephate poisoning include headaches, fatigue,stomach cramps, nausea, and in extreme cases, respiratorydepression.70 Acephate breaks down to methamidophos, anotherorganophosphate pesticide. EPA has classified acephate as a pos-sible human carcinogen (Group C).71 Oncogenicity test resultsfound an increased incidence of adrenal medullary tumors andpituitary tumors in male rats when compared with experimentalcontrols. In female mice, an increased incidence of liver tumorsand liver hyperplasic nodules, thought to be precursors to tumors,was seen at the highest doses tested.72
Pyrethroids (TempoTM, CynoffTM, TalstarTM, SuspendTM) At A GlanceWith the phase out of several organophosphate pesticides prod-ucts, pyrethroids insecticides are becoming some of the most com-monly used insecticides in offices, buildings and homes. Pesticideproducts containing pyrethroids are often described by pest controloperators as “safe as chrysanthemum flowers,” but this is quitemisleading. While pyrethroids are a synthetic version of an extractfrom a chrysanthemum plant, they are chemically engineered to bemore toxic to insects and to take longer to break down.73 They areoften formulated with synergists that increase their potency by com-promising the ability of insects to detoxify the pesticide. Pyrethroidsinclude the active ingredients bifenthrin, cyfluthrin, cyhalothrin,cypermethrin, deltamethrin, and permethrin, among others. Thereis a range of toxicity between formulations and amongst the differ-ing pyrethroid compounds themselves.
Pyrethroids act by inhibiting the nervous system of insects.74 Theyare also toxic to the human nervous system. Signs and symptomsof pyrethroid poisoning include stinging, burning, and numbness ofthe skin, abnormal facial sensation, dizziness, salivation,headache, fatigue, vomiting, diarrhea and irritability to sound andtouch. In more severe cases, pulmonary edema, muscle twitching,
and seizures can develop.75 Based on tests with laboratory animals,it appears that newborns may be more sensitive to somepyrethroids than adults.76
Pyrethroids have been linked to disruption of the endocrine system.Some pyrethroids have demonstrated estrogenic properties in in-vitro laboratory studies.77 EPA classifies some pyrethroids as possi-ble human carcinogens (Group C).78
Because pyrethroids are toxic to all insects, both beneficial insectsand pests are affected by pyrethroid applications. In some cases,predator insects may be susceptible to a lower dose than the insectpest on which it preys, disrupting the predator-prey relationship.Both pyrethroids and pyrethrins are often formulated with oils orpetroleum distillates and packaged in combination with toxic syn-ergists, such as piperonyl butoxide (PBO) and n-octyl bicyclohep-tene dicarboximide.79
Piperonyl Butoxide At A GlancePiperonyl butoxide (PBO) is a chemical that acts synergistically withthe active ingredient of a pesticide product to increase its potency.It is a liver poison that is added to pesticide products to reduceinsects’ ability to break down and detoxify the active ingredient.80 Atypical pesticide product contains 5 to 20 times more synergist thanactive ingredient. Pyrethroids, pyrethrins, rotenone and carbamatesare the active ingredients most often formulated in combinationwith PBO.81 In addition to the symptoms induced by the activeingredients, signs of PBO poisoning include anorexia, vomiting,diarrhea, intestinal inflammation, pulmonary hemorrhage and per-haps central nervous system depression. Repeated contact maycause slight skin irritation.82 Chronic toxicity studies have shownincreased liver weights in test animals, even at the lowest doses.Animal studies have also shown hepatocellular carcinomas even atlow exposure levels.83 EPA considers PBO to be a possible humancarcinogen (Group C).84

Healt
hy Ho
spita
ls
Contro
lling P
ests W
ithout
Harm
ful Pe
sticide
s
10
this characteristic on to their offspring. Becausepesticide users often assume that the survivors didnot receive a lethal dose, they may react byincreasing the pesticide dosage and frequency ofapplication, which results in a further loss of sus-ceptible pests and an increase in the proportion ofresistant individuals.”45
Pesticide RegulationThere is a common misconception that if pes-ticides are registered by EPA then they are safeto use. The U.S. General Accounting Officehas told Congress on several occasions that,“The general public receives limited and mis-leading information on pesticide hazards” andis misled on pesticide safety by pesticide appli-cator statements characterizing pesticides as“safe” or “harmless.”85
While the Federal Insecticide, Fungicide andRodenticide Act (FIFRA) and the Food QualityProtection Act (FQPA) regulate pesticides, thereare a number of reasons why the two laws donot adequately protect human health and theenvironment:
1. When EPA registers a pesticide, it consid-ers economic costs and benefits in addi-tion to the potential adverse health andenvironmental impacts of a product. Thismeans that EPA can register any pesticide,regardless of its toxicity, if it believes theestimated benefits outweigh the hazards.
2. Most toxicity testing is only done on theactive ingredient. There is limited testingof inert ingredients or the full productformulation.
3. Pesticides are not tested for their cumula-tive effects or synergistic interactions withother pesticides, environmental pollu-tants, or pharmaceuticals.
4. There is inadequate testing for short- andlong-term neurological, immunological,and endocrine (hormone)-disruptingeffects.
5. There is inadequate testing for impactson vulnerable populations, such as chil-dren, pregnant women, the elderly, andthose with chemical sensitivities or otherchronic illnesses involving the immune,neurological, respiratory, and/orendocrine systems. Toxicity assessmentsare usually done for healthy adult males.
6. Many pesticides in common use were reg-istered before more stringent regulationswere enacted and have not completedEPA’s re-registration process to determinewhether they should continue to be regis-tered. In the meantime potentially haz-ardous exposures can continue.
7. There is inadequate tracking of pesticideuse, exposures, and poisonings.
Limited and Misleading Information on Product LabelMost pesticide information is made available tothe user through the label. Labels advise onappropriate application methods and may con-tain precautionary information, such asrecommending protective clothing. Healthinformation is usually limited to warningsabout possible immediate health effects result-ing from exposure to the active ingredient.Labels do not provide information on chroniceffects, or display EPA’s carcinogenicity rating.87
As stated earlier, “inert” ingredients are notrequired to be listed by name on a pesticidelabel. Manufacturers are also required to pro-vide Material Safety Data Sheets (MSDSs) ontheir pesticide products, but there is no govern-ment review or approval of the information
provided. Thus, while MSDSs provide moreinformation on health effects than productlabels, the information is still limited.Therefore, they should not be relied on forhealth information.88
B E Y O N D P E S T I C I D E S & H E A L T H C A R E W I T H O U T H A R M
FIGURE 7. PESTICIDE REGISTRATION DOES
NOT EQUAL SAFETY
After allowing DursbanTM, active ingredient chlorpyri-fos, to be used for 30 years, EPA reached an agree-ment with Dow AgroSciences to phase out manystructural uses of chlorpyrifos-containing products,because they posed an unacceptably high risk tochildren. Chlorpyrifos had been one of the mostcommonly used insecticides in homes, gardens,schools, office buildings, hospitals, and other indoorsettings. Although, as of December 31, 2001, it canno longer be purchased for many residential andnon-residential uses, chlorpyrifos products can con-tinue to be used until existing stocks are depleted.Agricultural, golf course, mosquito control and con-tainerized baits use are allowed to continue indefi-nitely.86

Healthy Hospitals Controlling Pests Without Harmful Pesticides
11
B E Y O N D P E S T I C I D E S & H E A L T H C A R E W I T H O U T H A R M
Missing Toxicity DataWhile the EPA pesticide registration and re-registration process is intended to evaluate thesafety of pesticides, there are numerous defi-ciencies in the process. EPA has identifiedmuch missing data on older pesticides that areundergoing the re-registration process. In addi-tion, if chemicals fall under the category ofterrestrial non-food use pesticides, the toxicitydata requirements are less rigorous. The batteryof chronic toxicity data, including the potentialto cause cancer, birth defects, and reproductiveeffects, is only required of pesticides if theyhave food or feed uses.89 While most common-ly used pesticides do also have food or feed usesand undergo some chronic toxicity testing, thisdoes not guarantee the existence of completetoxicity information. Moreover, public expo-sures to pesticides are generally underestimatedby EPA.
Pesticide Laws Allow An “Acceptable” RiskThe laws that regulate pesticides contain anassumption that toxic pesticides are necessarytools in pest management. EPA states that, “eco-nomic benefits from pesticide use are notachieved without potential risks to humanhealth and the environment due to the toxicityof pesticide chemicals.”90 Therefore, the lawallows harm and illness to occur when thesechemicals are used. In reality, there are usuallynon-toxic ways to manage pests. These includemaintenance practices that prevent or excludepests, and mechanical devices and biologicalmaterials that control them. In most cases, thecauses of an insect infestation or mold growth,for example, can be identified and corrected.Other times, the use of mechanical traps andpheromone attractants can be effective.Nevertheless, because the benefits of pesticidesare assumed to be high, it is rationalized thatsome degree of disease and poisoning are“acceptable.”91
Healt
hy Ho
spita
ls
Contro
lling P
ests W
ithout
Harm
ful Pe
sticide
s
12
I I . H o s p i t a lP e s t i c i d e U s eS u r v e y F i n d i n g s
Methodology Health Care Without Harm distributed aHospital Pesticide Use Survey to the top 171 hos-pitals listed by the U.S. News and World Reportin 2001 (for a copy of the survey, see pages 44-46). The survey included questions about theuse of chemical pesticides, methods of notify-ing staff, patients, and the public of pesticideapplications, record keeping, and IntegratedPest Management (IPM). It also asked for thenames of pesticides used at the site. In somecases the survey responses were incomplete.Hospitals were promised that their identitywould be kept confidential.
Twenty-two hospitals (13%) responded to thesurvey. Although this was a relatively lowresponse rate, the results were consistent withreported pesticide use in New York hospitals,92
schools and other public buildings andgrounds. It also highlighted the fact that it isoften very difficult to obtain information aboutpesticide usage in any location.
Because the surveys were returned by hospitalsthat elected to do so, it can be assumed thatthere is a potential bias in the respondents. Thesurvey findings probably over-represent hospi-tals that have begun to move away frompesticide dependency and/or towards providingpesticide use notification, and under-represents
the number and toxicity of pesticide productsthat are being used at hospitals nationwide.Thus, the use of pesticides in U.S. hospitals islikely to be greater than what is representedhere.
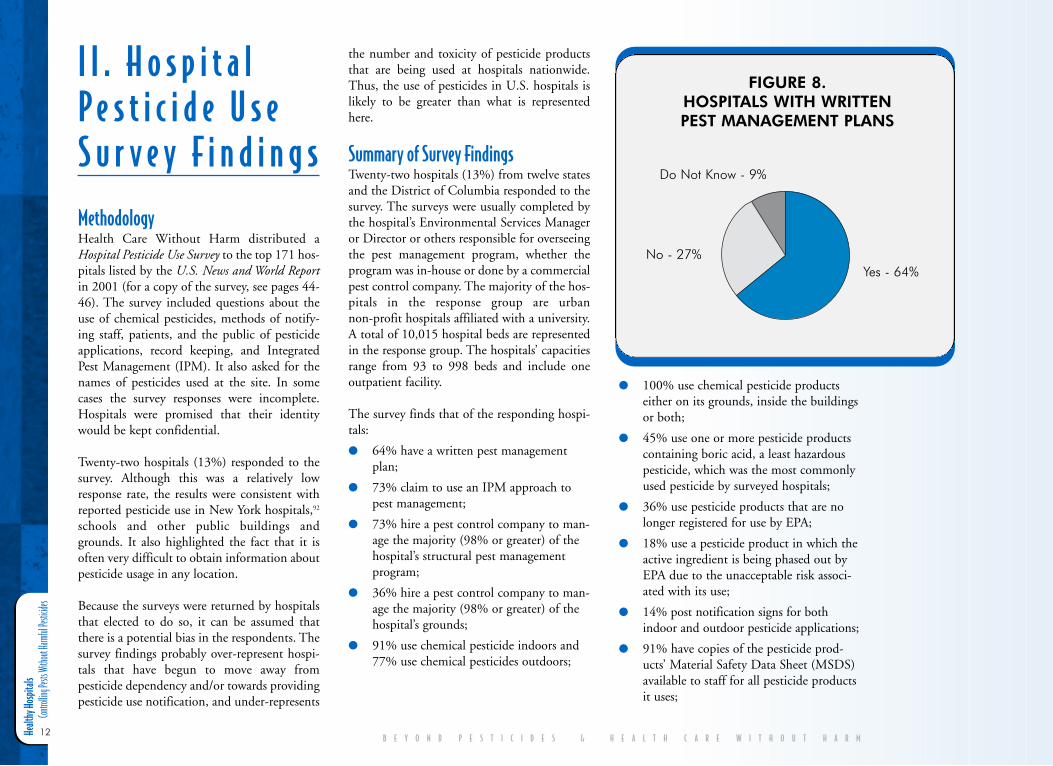
Summary of Survey FindingsTwenty-two hospitals (13%) from twelve statesand the District of Columbia responded to thesurvey. The surveys were usually completed bythe hospital’s Environmental Services Manageror Director or others responsible for overseeingthe pest management program, whether theprogram was in-house or done by a commercialpest control company. The majority of the hos-pitals in the response group are urbannon-profit hospitals affiliated with a university.A total of 10,015 hospital beds are representedin the response group. The hospitals’ capacitiesrange from 93 to 998 beds and include oneoutpatient facility.
The survey finds that of the responding hospi-tals:
● 64% have a written pest managementplan;
● 73% claim to use an IPM approach topest management;
● 73% hire a pest control company to man-age the majority (98% or greater) of thehospital’s structural pest managementprogram;
● 36% hire a pest control company to man-age the majority (98% or greater) of thehospital’s grounds;
● 91% use chemical pesticide indoors and77% use chemical pesticides outdoors;
● 100% use chemical pesticide productseither on its grounds, inside the buildingsor both;
● 45% use one or more pesticide productscontaining boric acid, a least hazardouspesticide, which was the most commonlyused pesticide by surveyed hospitals;
● 36% use pesticide products that are nolonger registered for use by EPA;
● 18% use a pesticide product in which theactive ingredient is being phased out byEPA due to the unacceptable risk associ-ated with its use;
● 14% post notification signs for bothindoor and outdoor pesticide applications;
● 91% have copies of the pesticide prod-ucts’ Material Safety Data Sheet (MSDS)available to staff for all pesticide productsit uses;
B E Y O N D P E S T I C I D E S & H E A L T H C A R E W I T H O U T H A R M
FIGURE 8. HOSPITALS WITH WRITTEN PEST MANAGEMENT PLANS
Do Not Know - 9%
No - 27%Yes - 64%
Healthy Hospitals Controlling Pests Without Harmful Pesticides
13
B E Y O N D P E S T I C I D E S & H E A L T H C A R E W I T H O U T H A R M
● 27% have provided pesticide-poisoningtraining to their staff;
● 77% keep records of structural pesticideapplications;
● 64% keep records of outdoor pesticideapplications; and,
● $55 per bed is the average annual cost ofpest management.
Hospital Pest Management PlansHospital pest management plans help direct ahospital in carrying out its pest control prac-tices. A total of 14 hospitals surveyed (64%)indicate that they have a written pest manage-ment plan. Two hospitals (9%) report they donot have a plan and six (27%) do not know ifthey have one or did not answer the question.
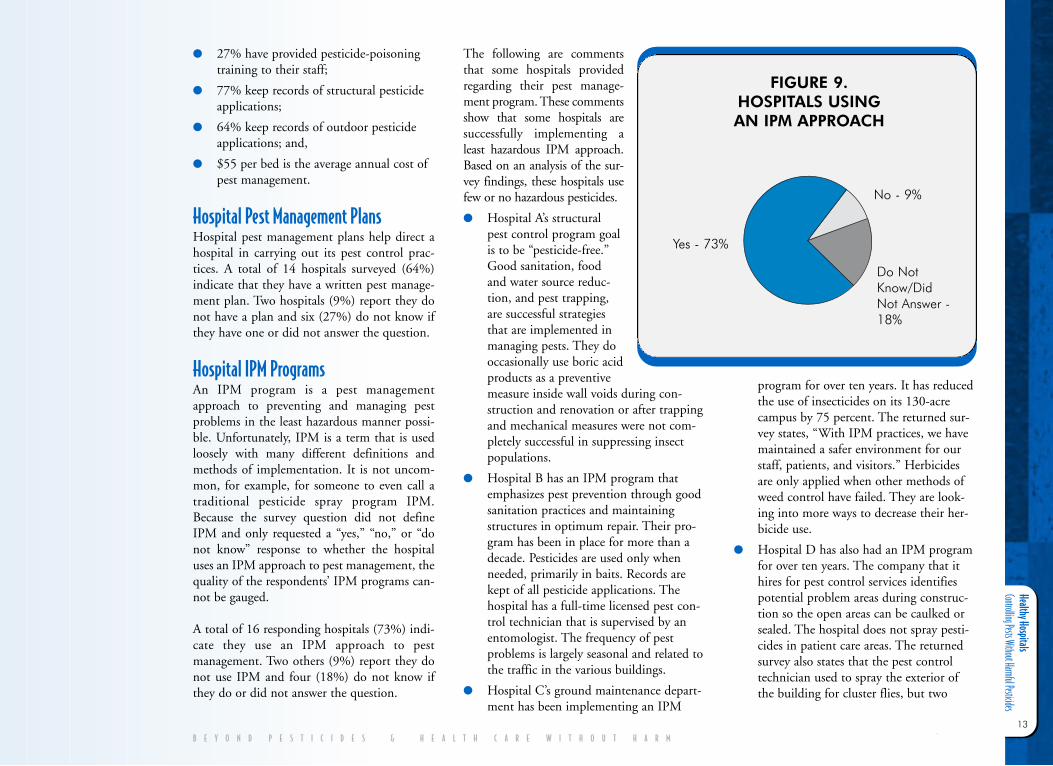
Hospital IPM ProgramsAn IPM program is a pest managementapproach to preventing and managing pestproblems in the least hazardous manner possi-ble. Unfortunately, IPM is a term that is usedloosely with many different definitions andmethods of implementation. It is not uncom-mon, for example, for someone to even call atraditional pesticide spray program IPM.Because the survey question did not defineIPM and only requested a “yes,” “no,” or “donot know” response to whether the hospitaluses an IPM approach to pest management, thequality of the respondents’ IPM programs can-not be gauged.
A total of 16 responding hospitals (73%) indi-cate they use an IPM approach to pestmanagement. Two others (9%) report they donot use IPM and four (18%) do not know ifthey do or did not answer the question.
The following are commentsthat some hospitals providedregarding their pest manage-ment program. These commentsshow that some hospitals aresuccessfully implementing aleast hazardous IPM approach.Based on an analysis of the sur-vey findings, these hospitals usefew or no hazardous pesticides.
● Hospital A’s structuralpest control program goalis to be “pesticide-free.”Good sanitation, foodand water source reduc-tion, and pest trapping,are successful strategiesthat are implemented inmanaging pests. They dooccasionally use boric acidproducts as a preventivemeasure inside wall voids during con-struction and renovation or after trappingand mechanical measures were not com-pletely successful in suppressing insectpopulations.
● Hospital B has an IPM program thatemphasizes pest prevention through goodsanitation practices and maintainingstructures in optimum repair. Their pro-gram has been in place for more than adecade. Pesticides are used only whenneeded, primarily in baits. Records arekept of all pesticide applications. Thehospital has a full-time licensed pest con-trol technician that is supervised by anentomologist. The frequency of pestproblems is largely seasonal and related tothe traffic in the various buildings.
● Hospital C’s ground maintenance depart-ment has been implementing an IPM
program for over ten years. It has reducedthe use of insecticides on its 130-acrecampus by 75 percent. The returned sur-vey states, “With IPM practices, we havemaintained a safer environment for ourstaff, patients, and visitors.” Herbicidesare only applied when other methods ofweed control have failed. They are look-ing into more ways to decrease their her-bicide use.
● Hospital D has also had an IPM programfor over ten years. The company that ithires for pest control services identifiespotential problem areas during construc-tion so the open areas can be caulked orsealed. The hospital does not spray pesti-cides in patient care areas. The returnedsurvey also states that the pest controltechnician used to spray the exterior ofthe building for cluster flies, but two
FIGURE 9. HOSPITALS USING AN IPM APPROACH
Yes - 73%
No - 9%
Do NotKnow/DidNot Answer -18%
Healt
hy Ho
spita
ls
Contro
lling P
ests W
ithout
Harm
ful Pe
sticide
s
14
years ago started usingVictorTM fly paper andCluster BustersTM to trap theflies.
While the returned surveys indi-cate that the majority ofresponding hospitals have IPMprograms, many hospital IPMpractices are severely underminedby a continued reliance on haz-ardous pesticides. For example,five of the 16 responding hospi-tals (31%) state that their IPMprogram uses between 18 and 38pesticide products. This high-lights the fact that there are manydifferent definitions of IPM.While true least hazardous IPMprograms use few or no syntheticpesticides, the term IPM isincreasingly being used by the pest controlindustry to describe programs that include syn-thetic pesticides or are, in fact, just traditionalspray programs.
In-House versus ContractPest ManagementFor three years in a row, the Hospitals andHealth Networks’ (HHN) ContractManagement Survey found that pest controltopped the list of hospital-contracted services.More than 85 percent of respondents reportedhiring outside vendors to manage pest prob-lems, citing cost savings and availability ofspecialized expertise as the top reasons for out-sourcing. HHN expects the number ofhospitals that outsource for lawn care andgrounds to continue to rise.93
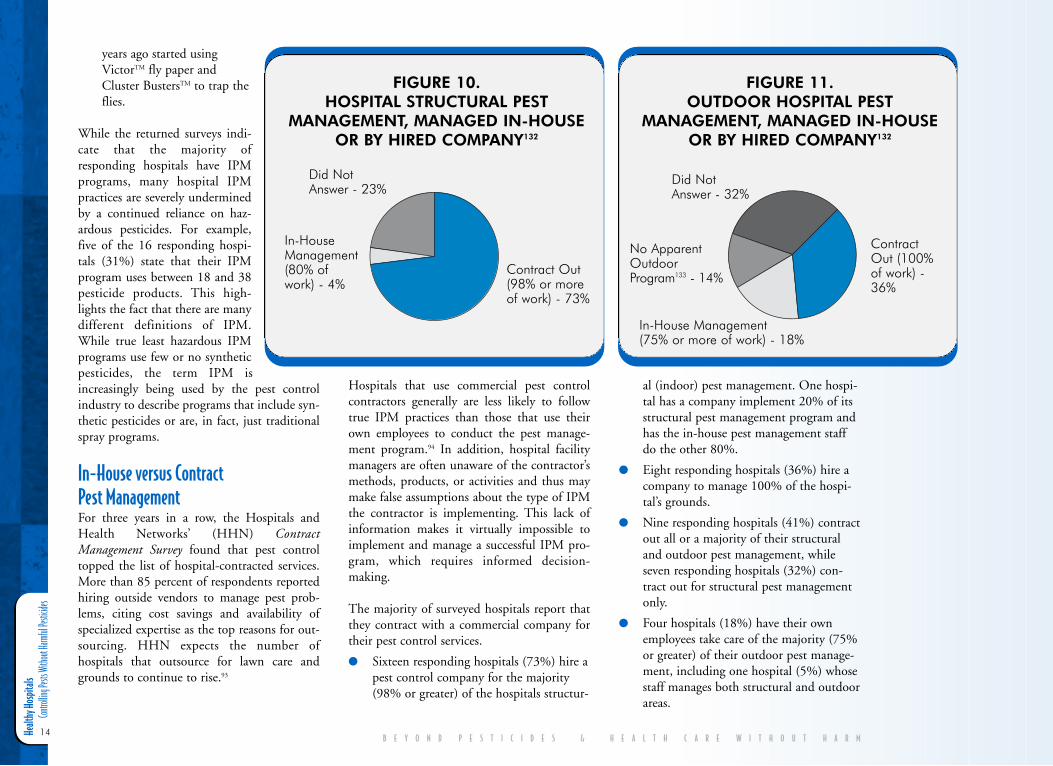
Hospitals that use commercial pest controlcontractors generally are less likely to followtrue IPM practices than those that use theirown employees to conduct the pest manage-ment program.94 In addition, hospital facilitymanagers are often unaware of the contractor’smethods, products, or activities and thus maymake false assumptions about the type of IPMthe contractor is implementing. This lack ofinformation makes it virtually impossible toimplement and manage a successful IPM pro-gram, which requires informed decision-making.
The majority of surveyed hospitals report thatthey contract with a commercial company fortheir pest control services.
● Sixteen responding hospitals (73%) hire apest control company for the majority(98% or greater) of the hospitals structur-
al (indoor) pest management. One hospi-tal has a company implement 20% of itsstructural pest management program andhas the in-house pest management staffdo the other 80%.
● Eight responding hospitals (36%) hire acompany to manage 100% of the hospi-tal’s grounds.
● Nine responding hospitals (41%) contractout all or a majority of their structuraland outdoor pest management, whileseven responding hospitals (32%) con-tract out for structural pest managementonly.
● Four hospitals (18%) have their ownemployees take care of the majority (75%or greater) of their outdoor pest manage-ment, including one hospital (5%) whosestaff manages both structural and outdoorareas.
B E Y O N D P E S T I C I D E S & H E A L T H C A R E W I T H O U T H A R M
FIGURE 10. HOSPITAL STRUCTURAL PEST
MANAGEMENT, MANAGED IN-HOUSEOR BY HIRED COMPANY132
Did NotAnswer - 23%
In-HouseManagement(80% ofwork) - 4%
Contract Out(98% or moreof work) - 73%
FIGURE 11. OUTDOOR HOSPITAL PEST
MANAGEMENT, MANAGED IN-HOUSEOR BY HIRED COMPANY132
Did NotAnswer - 32%
ContractOut (100%of work) -36%
In-House Management (75% or more of work) - 18%
No ApparentOutdoor Program133 - 14%
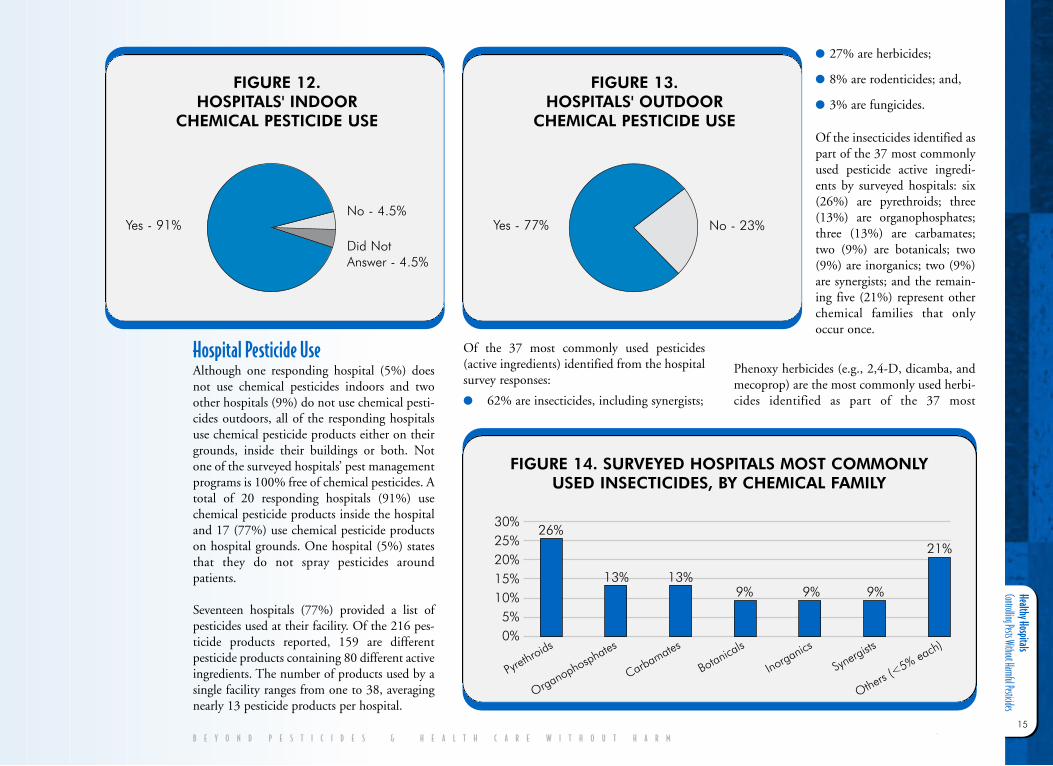
Healthy Hospitals Controlling Pests Without Harmful Pesticides
15
B E Y O N D P E S T I C I D E S & H E A L T H C A R E W I T H O U T H A R M
Hospital Pesticide UseAlthough one responding hospital (5%) doesnot use chemical pesticides indoors and twoother hospitals (9%) do not use chemical pesti-cides outdoors, all of the responding hospitalsuse chemical pesticide products either on theirgrounds, inside their buildings or both. Notone of the surveyed hospitals’ pest managementprograms is 100% free of chemical pesticides. Atotal of 20 responding hospitals (91%) usechemical pesticide products inside the hospitaland 17 (77%) use chemical pesticide productson hospital grounds. One hospital (5%) statesthat they do not spray pesticides aroundpatients.
Seventeen hospitals (77%) provided a list ofpesticides used at their facility. Of the 216 pes-ticide products reported, 159 are differentpesticide products containing 80 different activeingredients. The number of products used by asingle facility ranges from one to 38, averagingnearly 13 pesticide products per hospital.
Of the 37 most commonly used pesticides(active ingredients) identified from the hospitalsurvey responses:
● 62% are insecticides, including synergists;
● 27% are herbicides;
● 8% are rodenticides; and,
● 3% are fungicides.
Of the insecticides identified aspart of the 37 most commonlyused pesticide active ingredi-ents by surveyed hospitals: six(26%) are pyrethroids; three(13%) are organophosphates;three (13%) are carbamates;two (9%) are botanicals; two(9%) are inorganics; two (9%)are synergists; and the remain-ing five (21%) represent otherchemical families that onlyoccur once.
Phenoxy herbicides (e.g., 2,4-D, dicamba, andmecoprop) are the most commonly used herbi-cides identified as part of the 37 most
FIGURE 12. HOSPITALS' INDOOR
CHEMICAL PESTICIDE USE
FIGURE 13. HOSPITALS' OUTDOOR
CHEMICAL PESTICIDE USE
Yes - 77% No - 23%
FIGURE 14. SURVEYED HOSPITALS MOST COMMONLY USED INSECTICIDES, BY CHEMICAL FAMILY
30%25%20%15%10%5%0%
Yes - 91%No - 4.5%
Did NotAnswer - 4.5%
Pyrethroids
Organophosphates
Carbamates
Botanicals
Inorganics
Synerg
ists
Others (<5% ea
ch)
26%
13% 13%9% 9% 9%
21%
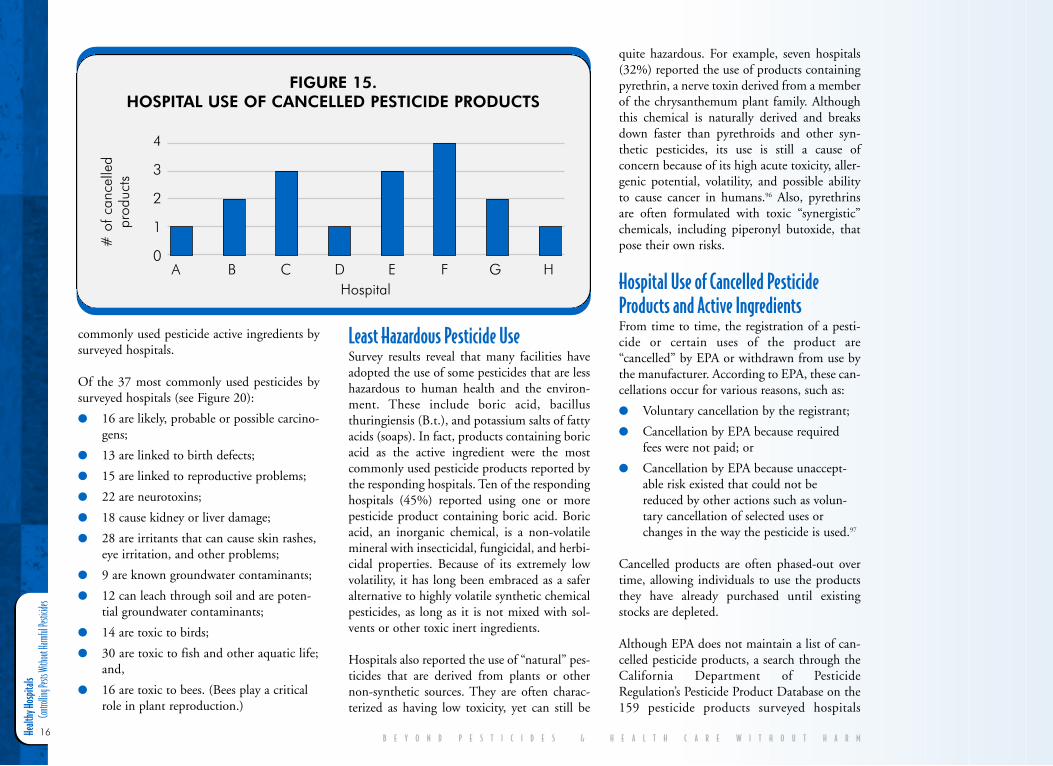
Healt
hy Ho
spita
ls
Contro
lling P
ests W
ithout
Harm
ful Pe
sticide
s
16
commonly used pesticide active ingredients bysurveyed hospitals.
Of the 37 most commonly used pesticides bysurveyed hospitals (see Figure 20):
● 16 are likely, probable or possible carcino-gens;
● 13 are linked to birth defects;
● 15 are linked to reproductive problems;
● 22 are neurotoxins;
● 18 cause kidney or liver damage;
● 28 are irritants that can cause skin rashes,eye irritation, and other problems;
● 9 are known groundwater contaminants;
● 12 can leach through soil and are poten-tial groundwater contaminants;
● 14 are toxic to birds;
● 30 are toxic to fish and other aquatic life;and,
● 16 are toxic to bees. (Bees play a criticalrole in plant reproduction.)
Least Hazardous Pesticide UseSurvey results reveal that many facilities haveadopted the use of some pesticides that are lesshazardous to human health and the environ-ment. These include boric acid, bacillusthuringiensis (B.t.), and potassium salts of fattyacids (soaps). In fact, products containing boricacid as the active ingredient were the mostcommonly used pesticide products reported bythe responding hospitals. Ten of the respondinghospitals (45%) reported using one or morepesticide product containing boric acid. Boricacid, an inorganic chemical, is a non-volatilemineral with insecticidal, fungicidal, and herbi-cidal properties. Because of its extremely lowvolatility, it has long been embraced as a saferalternative to highly volatile synthetic chemicalpesticides, as long as it is not mixed with sol-vents or other toxic inert ingredients.
Hospitals also reported the use of “natural” pes-ticides that are derived from plants or othernon-synthetic sources. They are often charac-terized as having low toxicity, yet can still be
quite hazardous. For example, seven hospitals(32%) reported the use of products containingpyrethrin, a nerve toxin derived from a memberof the chrysanthemum plant family. Althoughthis chemical is naturally derived and breaksdown faster than pyrethroids and other syn-thetic pesticides, its use is still a cause ofconcern because of its high acute toxicity, aller-genic potential, volatility, and possible abilityto cause cancer in humans.96 Also, pyrethrinsare often formulated with toxic “synergistic”chemicals, including piperonyl butoxide, thatpose their own risks.
Hospital Use of Cancelled PesticideProducts and Active IngredientsFrom time to time, the registration of a pesti-cide or certain uses of the product are“cancelled” by EPA or withdrawn from use bythe manufacturer. According to EPA, these can-cellations occur for various reasons, such as:
● Voluntary cancellation by the registrant;
● Cancellation by EPA because requiredfees were not paid; or
● Cancellation by EPA because unaccept-able risk existed that could not bereduced by other actions such as volun-tary cancellation of selected uses orchanges in the way the pesticide is used.97
Cancelled products are often phased-out overtime, allowing individuals to use the productsthey have already purchased until existingstocks are depleted.
Although EPA does not maintain a list of can-celled pesticide products, a search through theCalifornia Department of PesticideRegulation’s Pesticide Product Database on the159 pesticide products surveyed hospitals
B E Y O N D P E S T I C I D E S & H E A L T H C A R E W I T H O U T H A R M
FIGURE 15. HOSPITAL USE OF CANCELLED PESTICIDE PRODUCTS
4
3
2
1
0
# o
f can
celle
dpr
oduc
ts
A B C D E F G HHospital
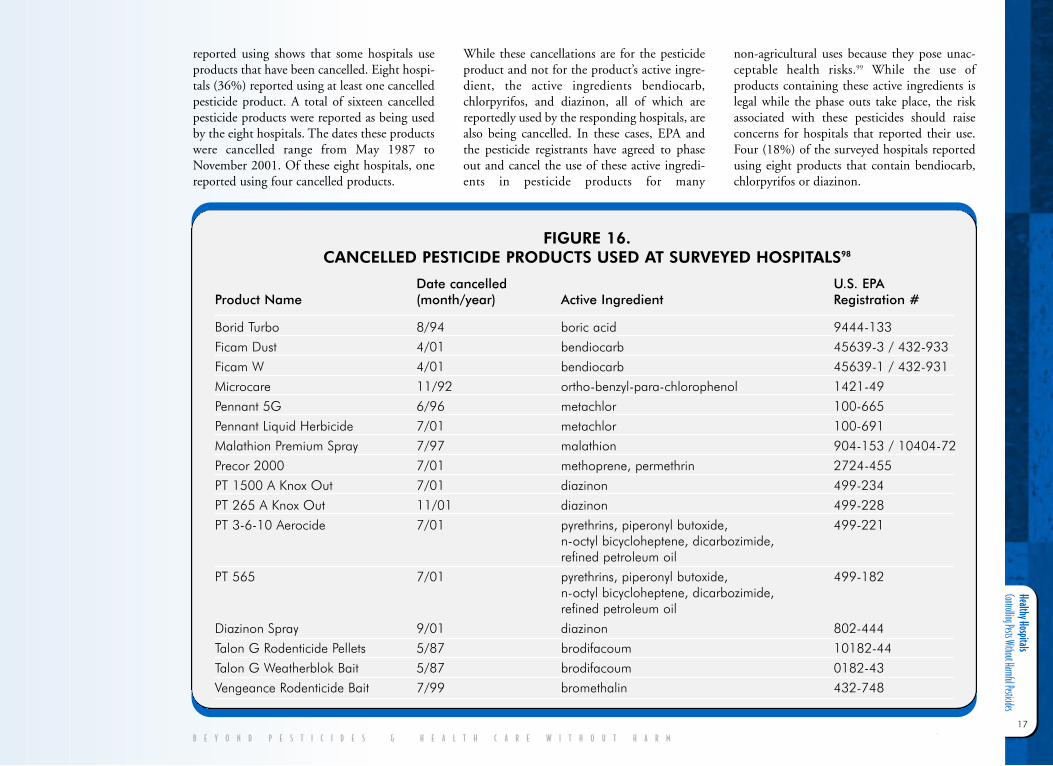
Healthy Hospitals Controlling Pests Without Harmful Pesticides
17
B E Y O N D P E S T I C I D E S & H E A L T H C A R E W I T H O U T H A R M
reported using shows that some hospitals useproducts that have been cancelled. Eight hospi-tals (36%) reported using at least one cancelledpesticide product. A total of sixteen cancelledpesticide products were reported as being usedby the eight hospitals. The dates these productswere cancelled range from May 1987 toNovember 2001. Of these eight hospitals, onereported using four cancelled products.
While these cancellations are for the pesticideproduct and not for the product’s active ingre-dient, the active ingredients bendiocarb,chlorpyrifos, and diazinon, all of which arereportedly used by the responding hospitals, arealso being cancelled. In these cases, EPA andthe pesticide registrants have agreed to phaseout and cancel the use of these active ingredi-ents in pesticide products for many
non-agricultural uses because they pose unac-ceptable health risks.99 While the use ofproducts containing these active ingredients islegal while the phase outs take place, the riskassociated with these pesticides should raiseconcerns for hospitals that reported their use.Four (18%) of the surveyed hospitals reportedusing eight products that contain bendiocarb,chlorpyrifos or diazinon.
FIGURE 16. CANCELLED PESTICIDE PRODUCTS USED AT SURVEYED HOSPITALS98
Date cancelled U.S. EPA Product Name (month/year) Active Ingredient Registration #
Borid Turbo 8/94 boric acid 9444-133Ficam Dust 4/01 bendiocarb 45639-3 / 432-933Ficam W 4/01 bendiocarb 45639-1 / 432-931Microcare 11/92 ortho-benzyl-para-chlorophenol 1421-49Pennant 5G 6/96 metachlor 100-665Pennant Liquid Herbicide 7/01 metachlor 100-691Malathion Premium Spray 7/97 malathion 904-153 / 10404-72Precor 2000 7/01 methoprene, permethrin 2724-455PT 1500 A Knox Out 7/01 diazinon 499-234PT 265 A Knox Out 11/01 diazinon 499-228PT 3-6-10 Aerocide 7/01 pyrethrins, piperonyl butoxide, 499-221
n-octyl bicycloheptene, dicarbozimide, refined petroleum oil
PT 565 7/01 pyrethrins, piperonyl butoxide, 499-182n-octyl bicycloheptene, dicarbozimide, refined petroleum oil
Diazinon Spray 9/01 diazinon 802-444Talon G Rodenticide Pellets 5/87 brodifacoum 10182-44Talon G Weatherblok Bait 5/87 brodifacoum 0182-43Vengeance Rodenticide Bait 7/99 bromethalin 432-748
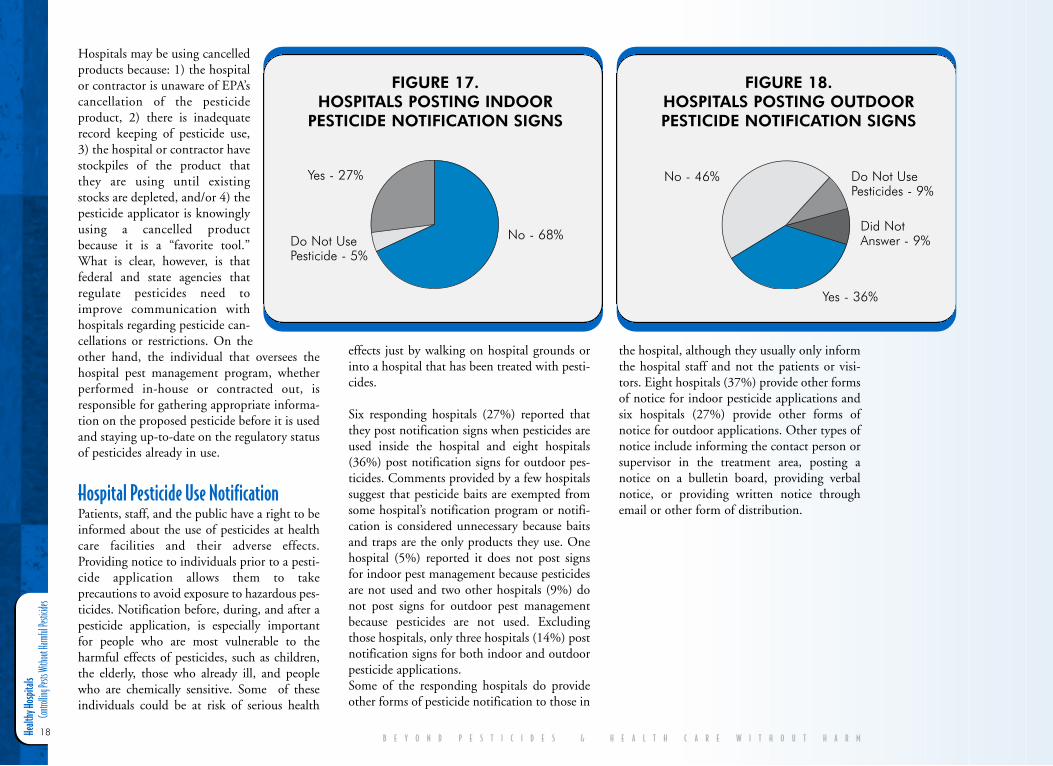
Healt
hy Ho
spita
ls
Contro
lling P
ests W
ithout
Harm
ful Pe
sticide
s
18
Hospitals may be using cancelledproducts because: 1) the hospitalor contractor is unaware of EPA’scancellation of the pesticideproduct, 2) there is inadequaterecord keeping of pesticide use,3) the hospital or contractor havestockpiles of the product thatthey are using until existingstocks are depleted, and/or 4) thepesticide applicator is knowinglyusing a cancelled productbecause it is a “favorite tool.”What is clear, however, is thatfederal and state agencies thatregulate pesticides need toimprove communication withhospitals regarding pesticide can-cellations or restrictions. On theother hand, the individual that oversees thehospital pest management program, whetherperformed in-house or contracted out, isresponsible for gathering appropriate informa-tion on the proposed pesticide before it is usedand staying up-to-date on the regulatory statusof pesticides already in use.
Hospital Pesticide Use NotificationPatients, staff, and the public have a right to beinformed about the use of pesticides at healthcare facilities and their adverse effects.Providing notice to individuals prior to a pesti-cide application allows them to takeprecautions to avoid exposure to hazardous pes-ticides. Notification before, during, and after apesticide application, is especially importantfor people who are most vulnerable to theharmful effects of pesticides, such as children,the elderly, those who already ill, and peoplewho are chemically sensitive. Some of theseindividuals could be at risk of serious health
effects just by walking on hospital grounds orinto a hospital that has been treated with pesti-cides.
Six responding hospitals (27%) reported thatthey post notification signs when pesticides areused inside the hospital and eight hospitals(36%) post notification signs for outdoor pes-ticides. Comments provided by a few hospitalssuggest that pesticide baits are exempted fromsome hospital’s notification program or notifi-cation is considered unnecessary because baitsand traps are the only products they use. Onehospital (5%) reported it does not post signsfor indoor pest management because pesticidesare not used and two other hospitals (9%) donot post signs for outdoor pest managementbecause pesticides are not used. Excludingthose hospitals, only three hospitals (14%) postnotification signs for both indoor and outdoorpesticide applications.Some of the responding hospitals do provideother forms of pesticide notification to those in
the hospital, although they usually only informthe hospital staff and not the patients or visi-tors. Eight hospitals (37%) provide other formsof notice for indoor pesticide applications andsix hospitals (27%) provide other forms ofnotice for outdoor applications. Other types ofnotice include informing the contact person orsupervisor in the treatment area, posting anotice on a bulletin board, providing verbalnotice, or providing written notice throughemail or other form of distribution.
B E Y O N D P E S T I C I D E S & H E A L T H C A R E W I T H O U T H A R M
FIGURE 17. HOSPITALS POSTING INDOOR
PESTICIDE NOTIFICATION SIGNS
Yes - 27%
Do Not UsePesticide - 5%
No - 68%
FIGURE 18. HOSPITALS POSTING OUTDOORPESTICIDE NOTIFICATION SIGNS
No - 46% Do Not UsePesticides - 9%
Did NotAnswer - 9%
Yes - 36%
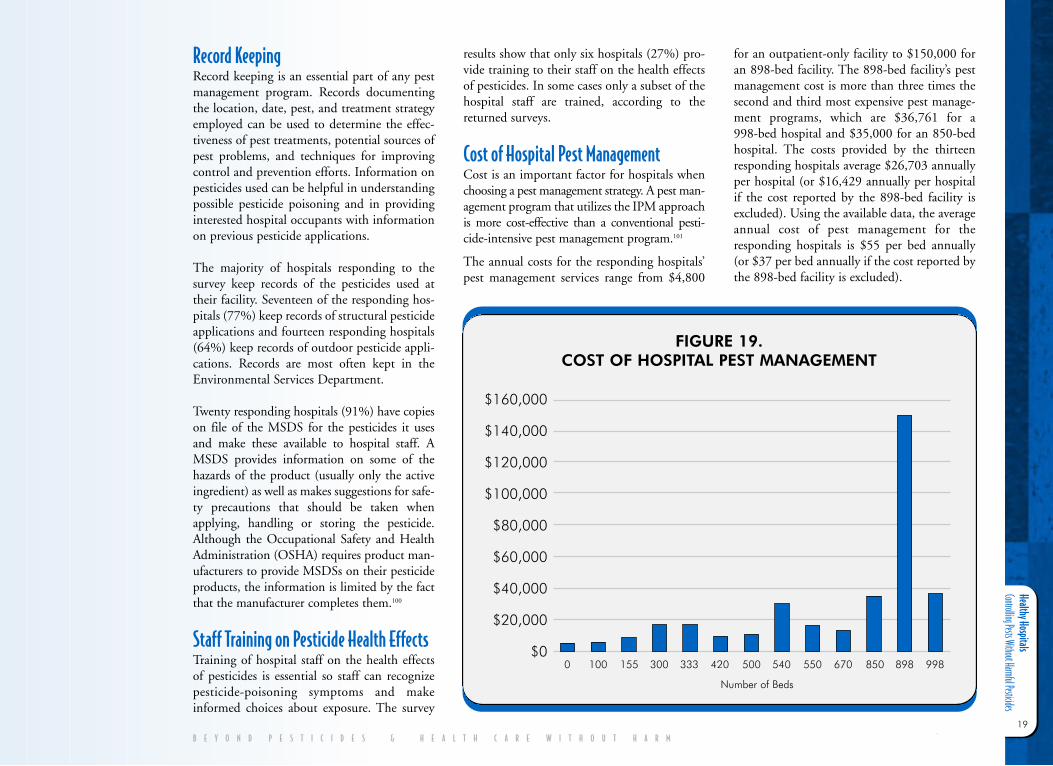
Healthy Hospitals Controlling Pests Without Harmful Pesticides
19
B E Y O N D P E S T I C I D E S & H E A L T H C A R E W I T H O U T H A R M
Record KeepingRecord keeping is an essential part of any pestmanagement program. Records documentingthe location, date, pest, and treatment strategyemployed can be used to determine the effec-tiveness of pest treatments, potential sources ofpest problems, and techniques for improvingcontrol and prevention efforts. Information onpesticides used can be helpful in understandingpossible pesticide poisoning and in providinginterested hospital occupants with informationon previous pesticide applications.
The majority of hospitals responding to thesurvey keep records of the pesticides used attheir facility. Seventeen of the responding hos-pitals (77%) keep records of structural pesticideapplications and fourteen responding hospitals(64%) keep records of outdoor pesticide appli-cations. Records are most often kept in theEnvironmental Services Department.
Twenty responding hospitals (91%) have copieson file of the MSDS for the pesticides it usesand make these available to hospital staff. AMSDS provides information on some of thehazards of the product (usually only the activeingredient) as well as makes suggestions for safe-ty precautions that should be taken whenapplying, handling or storing the pesticide.Although the Occupational Safety and HealthAdministration (OSHA) requires product man-ufacturers to provide MSDSs on their pesticideproducts, the information is limited by the factthat the manufacturer completes them.100
Staff Training on Pesticide Health EffectsTraining of hospital staff on the health effectsof pesticides is essential so staff can recognizepesticide-poisoning symptoms and makeinformed choices about exposure. The survey
results show that only six hospitals (27%) pro-vide training to their staff on the health effectsof pesticides. In some cases only a subset of thehospital staff are trained, according to thereturned surveys.
Cost of Hospital Pest ManagementCost is an important factor for hospitals whenchoosing a pest management strategy. A pest man-agement program that utilizes the IPM approachis more cost-effective than a conventional pesti-cide-intensive pest management program.101
The annual costs for the responding hospitals’pest management services range from $4,800
for an outpatient-only facility to $150,000 foran 898-bed facility. The 898-bed facility’s pestmanagement cost is more than three times thesecond and third most expensive pest manage-ment programs, which are $36,761 for a998-bed hospital and $35,000 for an 850-bedhospital. The costs provided by the thirteenresponding hospitals average $26,703 annuallyper hospital (or $16,429 annually per hospitalif the cost reported by the 898-bed facility isexcluded). Using the available data, the averageannual cost of pest management for theresponding hospitals is $55 per bed annually(or $37 per bed annually if the cost reported bythe 898-bed facility is excluded).
FIGURE 19. COST OF HOSPITAL PEST MANAGEMENT
$160,000
$140,000
$120,000
$100,000
$80,000
$60,000
$40,000
$20,000
$00 100 155 300 333 420 500 540 550 670 850 898 998
Number of Beds
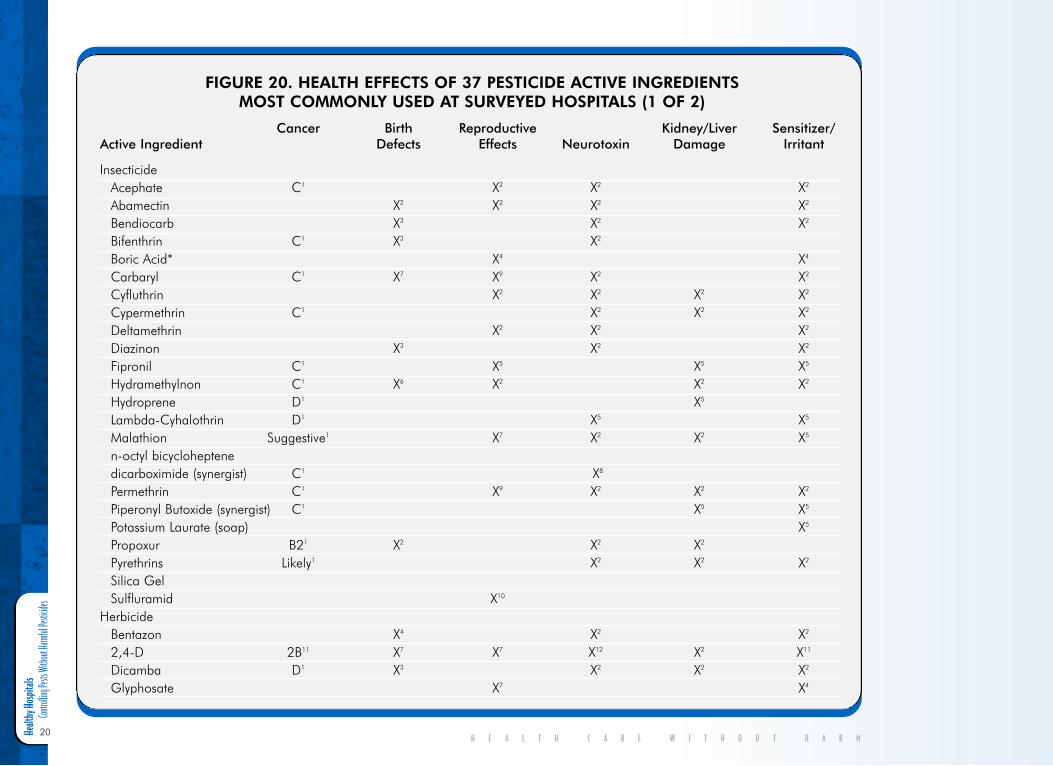
Healt
hy Ho
spita
ls
Contro
lling P
ests W
ithout
Harm
ful Pe
sticide
s
20H E A L T H C A R E W I T H O U T H A R M
FIGURE 20. HEALTH EFFECTS OF 37 PESTICIDE ACTIVE INGREDIENTS MOST COMMONLY USED AT SURVEYED HOSPITALS (1 OF 2)
Cancer Birth Reproductive Kidney/Liver Sensitizer/ Active Ingredient Defects Effects Neurotoxin Damage Irritant
InsecticideAcephate C1 X2 X2 X2
Abamectin X2 X2 X2 X2
Bendiocarb X3 X2 X2
Bifenthrin C1 X3 X2
Boric Acid* X4 X4
Carbaryl C1 X7 X9 X2 X2
Cyfluthrin X2 X2 X2 X2
Cypermethrin C1 X2 X2 X2
Deltamethrin X2 X2 X2
Diazinon X3 X2 X2
Fipronil C1 X5 X5 X5
Hydramethylnon C1 X6 X2 X2 X2
Hydroprene D1 X5
Lambda-Cyhalothrin D1 X5 X5
Malathion Suggestive1 X7 X2 X2 X5
n-octyl bicycloheptene dicarboximide (synergist) C1 X8
Permethrin C1 X9 X2 X2 X2
Piperonyl Butoxide (synergist) C1 X5 X5
Potassium Laurate (soap) X5
Propoxur B21 X2 X2 X2
Pyrethrins Likely1 X2 X2 X2
Silica Gel Sulfluramid X10
HerbicideBentazon X4 X2 X2
2,4-D 2B11 X7 X7 X12 X2 X11
Dicamba D1 X3 X2 X2 X2
Glyphosate X7 X4
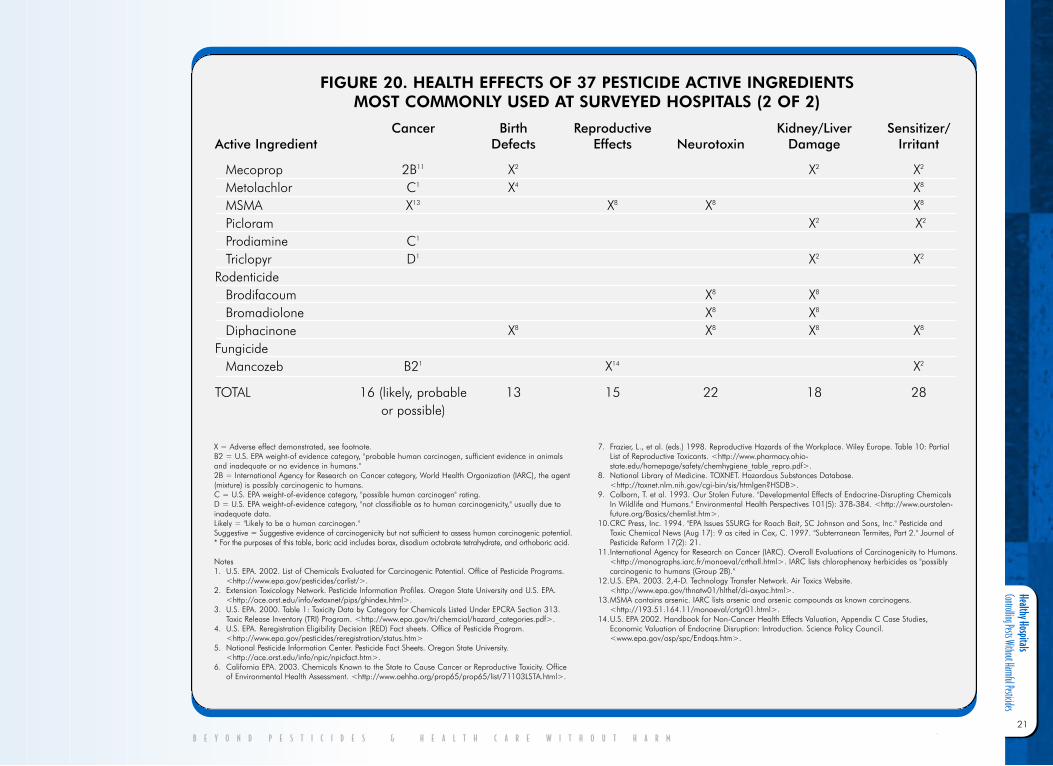
Healthy Hospitals Controlling Pests Without Harmful Pesticides
21
B E Y O N D P E S T I C I D E S & H E A L T H C A R E W I T H O U T H A R M
FIGURE 20. HEALTH EFFECTS OF 37 PESTICIDE ACTIVE INGREDIENTS MOST COMMONLY USED AT SURVEYED HOSPITALS (2 OF 2)
Cancer Birth Reproductive Kidney/Liver Sensitizer/ Active Ingredient Defects Effects Neurotoxin Damage Irritant
Mecoprop 2B11 X2 X2 X2
Metolachlor C1 X4 X8
MSMA X13 X8 X8 X8
Picloram X2 X2
Prodiamine C1
Triclopyr D1 X2 X2
RodenticideBrodifacoum X8 X8
Bromadiolone X8 X8
Diphacinone X8 X8 X8 X8
FungicideMancozeb B21 X14 X2
TOTAL 16 (likely, probable 13 15 22 18 28or possible)
X = Adverse effect demonstrated, see footnote.B2 = U.S. EPA weight-of evidence category, "probable human carcinogen, sufficient evidence in animalsand inadequate or no evidence in humans."2B = International Agency for Research on Cancer category, World Health Organization (IARC), the agent(mixture) is possibly carcinogenic to humans.C = U.S. EPA weight-of-evidence category, "possible human carcinogen" rating.D = U.S. EPA weight-of-evidence category, "not classifiable as to human carcinogenicity," usually due toinadequate data.Likely = "Likely to be a human carcinogen."Suggestive = Suggestive evidence of carcinogenicity but not sufficient to assess human carcinogenic potential.* For the purposes of this table, boric acid includes borax, disodium octobrate tetrahydrate, and orthoboric acid.
Notes 1. U.S. EPA. 2002. List of Chemicals Evaluated for Carcinogenic Potential. Office of Pesticide Programs.
<http://www.epa.gov/pesticides/carlist/>.2. Extension Toxicology Network. Pesticide Information Profiles. Oregon State University and U.S. EPA.
<http://ace.orst.edu/info/extoxnet/pips/ghindex.html>.3. U.S. EPA. 2000. Table 1: Toxicity Data by Category for Chemicals Listed Under EPCRA Section 313.
Toxic Release Inventory (TRI) Program. <http://www.epa.gov/tri/chemcial/hazard_categories.pdf>.4. U.S. EPA. Reregistration Eligibility Decision (RED) Fact sheets. Office of Pesticide Program.
<http://www.epa.gov/pesticides/reregistration/status.htm>5. National Pesticide Information Center. Pesticide Fact Sheets. Oregon State University.
<http://ace.orst.edu/info/npic/npicfact.htm>.6. California EPA. 2003. Chemicals Known to the State to Cause Cancer or Reproductive Toxicity. Office
of Environmental Health Assessment. <http://www.oehha.org/prop65/prop65/list/71103LSTA.html>.
7. Frazier, L., et al. (eds.) 1998. Reproductive Hazards of the Workplace. Wiley Europe. Table 10: PartialList of Reproductive Toxicants. <http://www.pharmacy.ohio-state.edu/homepage/safety/chemhygiene_table_repro.pdf>.
8. National Library of Medicine. TOXNET. Hazardous Substances Database.<http://toxnet.nlm.nih.gov/cgi-bin/sis/htmlgen?HSDB>.
9. Colborn, T. et al. 1993. Our Stolen Future. "Developmental Effects of Endocrine-Disrupting ChemicalsIn Wildlife and Humans." Environmental Health Perspectives 101(5): 378-384. <http://www.ourstolen-future.org/Basics/chemlist.htm>.
10.CRC Press, Inc. 1994. "EPA Issues SSURG for Roach Bait, SC Johnson and Sons, Inc." Pesticide andToxic Chemical News (Aug 17): 9 as cited in Cox, C. 1997. "Subterranean Termites, Part 2." Journal ofPesticide Reform 17(2): 21.
11.International Agency for Research on Cancer (IARC). Overall Evaluations of Carcinogenicity to Humans.<http://monographs.iarc.fr/monoeval/crthall.html>. IARC lists chlorophenoxy herbicides as "possiblycarcinogenic to humans (Group 2B)."
12.U.S. EPA. 2003. 2,4-D. Technology Transfer Network. Air Toxics Website.<http://www.epa.gov/thnatw01/hlthef/di-oxyac.html>.
13.MSMA contains arsenic. IARC lists arsenic and arsenic compounds as known carcinogens.<http://193.51.164.11/monoeval/crtgr01.html>.
14.U.S. EPA 2002. Handbook for Non-Cancer Health Effects Valuation, Appendix C Case Studies,Economic Valuation of Endocrine Disruption: Introduction. Science Policy Council.<www.epa.gov/osp/spc/Endoqs.htm>.
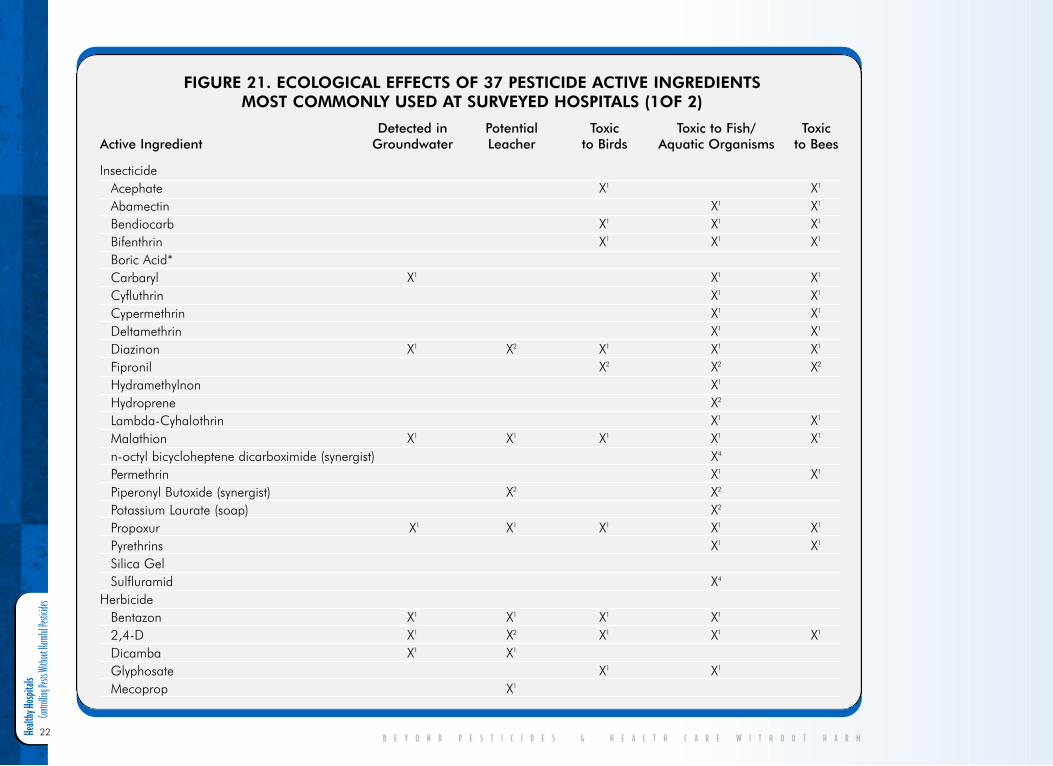
Healt
hy Ho
spita
ls
Contro
lling P
ests W
ithout
Harm
ful Pe
sticide
s
22B E Y O N D P E S T I C I D E S & H E A L T H C A R E W I T H O U T H A R M
FIGURE 21. ECOLOGICAL EFFECTS OF 37 PESTICIDE ACTIVE INGREDIENTS MOST COMMONLY USED AT SURVEYED HOSPITALS (1OF 2)
Detected in Potential Toxic Toxic to Fish/ Toxic Active Ingredient Groundwater Leacher to Birds Aquatic Organisms to Bees
InsecticideAcephate X1 X1
Abamectin X1 X1
Bendiocarb X1 X1 X1
Bifenthrin X1 X1 X1
Boric Acid*Carbaryl X1 X1 X1
Cyfluthrin X1 X1
Cypermethrin X1 X1
Deltamethrin X1 X1
Diazinon X1 X2 X1 X1 X1
Fipronil X2 X2 X2
Hydramethylnon X1
Hydroprene X2
Lambda-Cyhalothrin X1 X1
Malathion X1 X1 X1 X1 X1
n-octyl bicycloheptene dicarboximide (synergist) X4
Permethrin X1 X1
Piperonyl Butoxide (synergist) X2 X2
Potassium Laurate (soap) X2
Propoxur X1 X1 X1 X1 X1
Pyrethrins X1 X1
Silica Gel Sulfluramid X4
HerbicideBentazon X1 X1 X1 X1
2,4-D X1 X2 X1 X1 X1
Dicamba X1 X1
Glyphosate X1 X1
Mecoprop X1
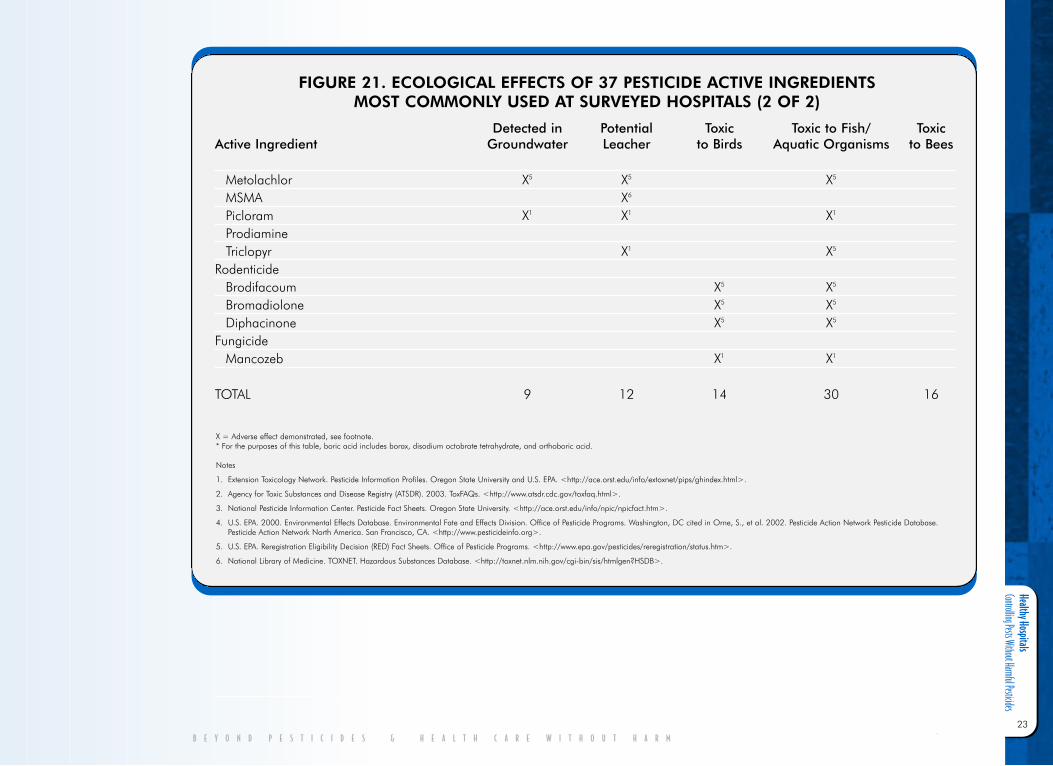
Healthy Hospitals Controlling Pests Without Harmful Pesticides
23
B E Y O N D P E S T I C I D E S & H E A L T H C A R E W I T H O U T H A R M
FIGURE 21. ECOLOGICAL EFFECTS OF 37 PESTICIDE ACTIVE INGREDIENTS MOST COMMONLY USED AT SURVEYED HOSPITALS (2 OF 2)
Detected in Potential Toxic Toxic to Fish/ Toxic Active Ingredient Groundwater Leacher to Birds Aquatic Organisms to Bees
Metolachlor X5 X5 X5
MSMA X6
Picloram X1 X1 X1
ProdiamineTriclopyr X1 X5
RodenticideBrodifacoum X5 X5
Bromadiolone X5 X5
Diphacinone X5 X5
FungicideMancozeb X1 X1
TOTAL 9 12 14 30 16
X = Adverse effect demonstrated, see footnote.* For the purposes of this table, boric acid includes borax, disodium octobrate tetrahydrate, and orthoboric acid.
Notes
1. Extension Toxicology Network. Pesticide Information Profiles. Oregon State University and U.S. EPA. <http://ace.orst.edu/info/extoxnet/pips/ghindex.html>.
2. Agency for Toxic Substances and Disease Registry (ATSDR). 2003. ToxFAQs. <http://www.atsdr.cdc.gov/toxfaq.html>.
3. National Pesticide Information Center. Pesticide Fact Sheets. Oregon State University. <http://ace.orst.edu/info/npic/npicfact.htm>.
4. U.S. EPA. 2000. Environmental Effects Database. Environmental Fate and Effects Division. Office of Pesticide Programs. Washington, DC cited in Orne, S., et al. 2002. Pesticide Action Network Pesticide Database.Pesticide Action Network North America. San Francisco, CA. <http://www.pesticideinfo.org>.
5. U.S. EPA. Reregistration Eligibility Decision (RED) Fact Sheets. Office of Pesticide Programs. <http://www.epa.gov/pesticides/reregistration/status.htm>.
6. National Library of Medicine. TOXNET. Hazardous Substances Database. <http://toxnet.nlm.nih.gov/cgi-bin/sis/htmlgen?HSDB>.

Healt
hy Ho
spita
ls
Contro
lling P
ests W
ithout
Harm
ful Pe
sticide
s
24
1 1 1 . S a f e r P e s tM a n a g e m e n tP r a c t i c e s Many hospital occupants are especially vulner-able to pesticides yet pests are unacceptable insuch an environment. Therefore, it is vital thatthe hospital employ a pest management pro-gram that effectively prevents and controls pestproblems using the least hazardous approach.As required by the Centers for Medicare andMedicaid Services (CMS) of the Department ofHealth and Human Services, “hospital must be… maintained to ensure the safety of thepatient.”102
Like other public buildings, hospitals experi-ence their share of pest problems ranging frommice, ants, flies, and spiders inside facilities toweeds and other insects on hospital grounds.Although many pests are only nuisances, somepests like flies, cockroaches, yellowjackets,rodents, and termites have the potential tocause harm by spreading disease, triggeringallergies or asthma attacks, causing painfulstings which can be life-threatening to thosewith allergies, contaminating food, or causingstructural damage.
Pest problems usually signal larger problemswith a health care facility’s sanitation, mainte-nance, and soil health. Pests are attracted byimproperly stored food, waste scraps, foodgifts, and water sources. Frequent sites of pestinfestations include hospital cafeterias, loadingdocks, storage areas, bathrooms, waste disposal
areas, and patient rooms, especially in long-term care facilities. Pests most frequently entera hospital through open or leaky doors (exacer-bated by typically heavy foot traffic in and outof hospital facilities), windows, wall, ceiling,and floor cracks, and gaps around plumbingand other pipes that enter the building. Theycan also enter a hospital by hitchhiking a ridein cardboard boxes, suitcases, and flowers,among other things. According to IPM expertGary Alpert, a major pest problem for hospitalsin Massachusetts is the American cockroachwhich often results from broken sewer lines,dried up floor drains, and water traps that needrepair. On hospital grounds, unhealthy lawnsand landscape and/or poor soil conditions fos-ter weed growth and insect infestations.
But the solution to a pest problem must not bemore harmful than the pest problem it ismeant to solve. In typical pesticide spray pro-grams it is not unusual to overestimate the riskof the pest and underestimate the risk of thepesticide. For example, many pests like com-mon house spiders may be a nuisance but arenot harmful. Most pesticides however, areassociated with a variety of health risks. TheAmerican Medical Association’s Council onScientific Affairs states, “Particular uncertaintyexists regarding the long-term health effects oflow dose pesticide exposure. Current surveil-lance systems are inadequate to characterizepotential exposure problems related either topesticide usage or pesticide-related illnesses.Considering these data gaps, it is prudent forhomeowners, farmers, and workers to limitpesticides exposures to themselves and others,and to use the least toxic chemical pesticide ornonchemical alternative.”103
Fortunately there is a method of pest controlcalled IPM that can control pests without the
use of toxic pesticides. Cities, counties, govern-ment agencies, and schools nationwide areincreasingly adopting IPM programs. TheGeneral Services Administration has had astructural IPM program since 1989 and theNational Park Service has had a structural andoutdoor IPM program since the early 1980’s.104
The City of San Francisco adopted an IPMordinance in 1996. The City of Santa Fe adopt-ed an IPM ordinance in 2001 and has almostcompletely eliminated its use of toxic pesticides.
Washington, Oregon, Michigan, andConnecticut have all passed laws that requirestate agencies to adopt an IPM program at thefacilities under their control. Washington andOregon statutes are similar, requiring every per-son responsible for pest management in eachagency to be trained in IPM. These laws estab-lish an Interagency IPM CoordinatingCommittee consisting of an IPM representativefrom each agency and require the Committeemeetings be open to the public.105
Perhaps the greatest increase in IPM programsis occurring in schools, which like hospitalshave a special obligation to protect their vulner-able occupants from toxic exposures. The threelargest school districts in the continental U.S.,New York Public Schools, Los Angeles UnifiedSchool District, and Chicago Public Schools,are successfully implementing IPM programsthat have significantly reduced the amount ofpesticides used, decreased the number of pestproblems, and have kept costs at or lower thana conventional pest program. And as the hospi-tal survey shows, IPM is also being practiced insome U.S. hospitals.
B E Y O N D P E S T I C I D E S & H E A L T H C A R E W I T H O U T H A R M
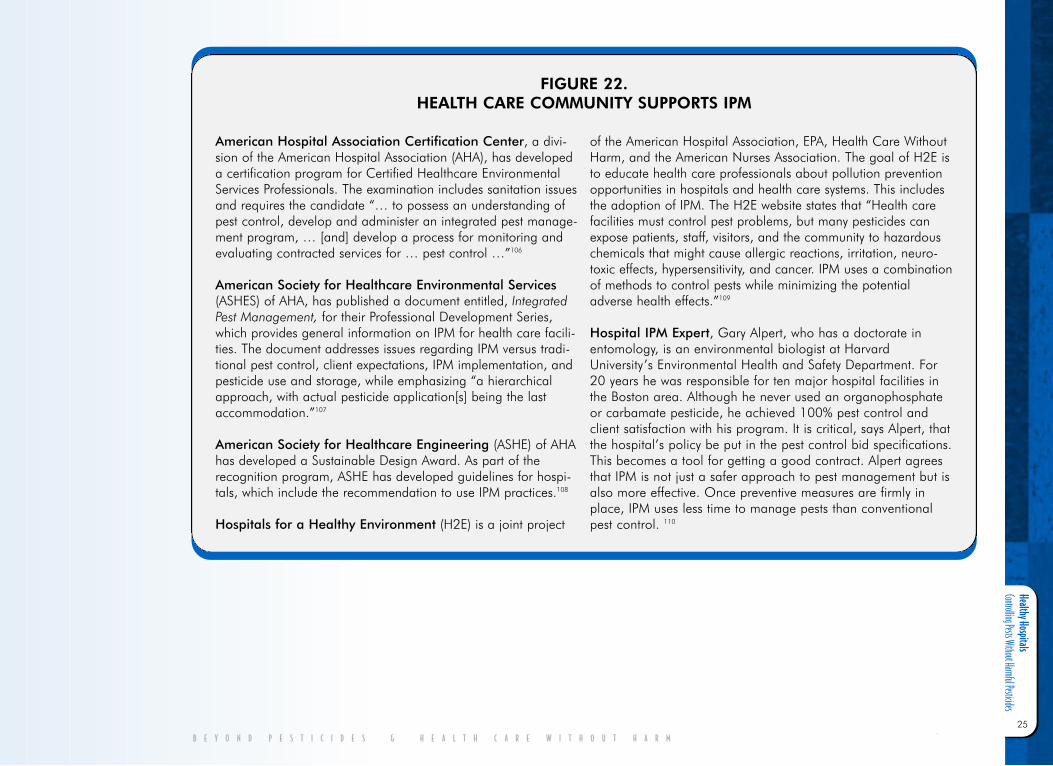
Healthy Hospitals Controlling Pests Without Harmful Pesticides
25
B E Y O N D P E S T I C I D E S & H E A L T H C A R E W I T H O U T H A R M
American Hospital Association Certification Center, a divi-sion of the American Hospital Association (AHA), has developeda certification program for Certified Healthcare EnvironmentalServices Professionals. The examination includes sanitation issuesand requires the candidate “… to possess an understanding ofpest control, develop and administer an integrated pest manage-ment program, … [and] develop a process for monitoring andevaluating contracted services for … pest control …”106
American Society for Healthcare Environmental Services(ASHES) of AHA, has published a document entitled, IntegratedPest Management, for their Professional Development Series,which provides general information on IPM for health care facili-ties. The document addresses issues regarding IPM versus tradi-tional pest control, client expectations, IPM implementation, andpesticide use and storage, while emphasizing “a hierarchicalapproach, with actual pesticide application[s] being the lastaccommodation.”107
American Society for Healthcare Engineering (ASHE) of AHAhas developed a Sustainable Design Award. As part of therecognition program, ASHE has developed guidelines for hospi-tals, which include the recommendation to use IPM practices.108
Hospitals for a Healthy Environment (H2E) is a joint project
of the American Hospital Association, EPA, Health Care WithoutHarm, and the American Nurses Association. The goal of H2E isto educate health care professionals about pollution preventionopportunities in hospitals and health care systems. This includesthe adoption of IPM. The H2E website states that “Health carefacilities must control pest problems, but many pesticides canexpose patients, staff, visitors, and the community to hazardouschemicals that might cause allergic reactions, irritation, neuro-toxic effects, hypersensitivity, and cancer. IPM uses a combinationof methods to control pests while minimizing the potentialadverse health effects.”109
Hospital IPM Expert, Gary Alpert, who has a doctorate inentomology, is an environmental biologist at HarvardUniversity’s Environmental Health and Safety Department. For20 years he was responsible for ten major hospital facilities inthe Boston area. Although he never used an organophosphateor carbamate pesticide, he achieved 100% pest control andclient satisfaction with his program. It is critical, says Alpert, thatthe hospital’s policy be put in the pest control bid specifications.This becomes a tool for getting a good contract. Alpert agreesthat IPM is not just a safer approach to pest management but isalso more effective. Once preventive measures are firmly inplace, IPM uses less time to manage pests than conventionalpest control. 110
FIGURE 22. HEALTH CARE COMMUNITY SUPPORTS IPM
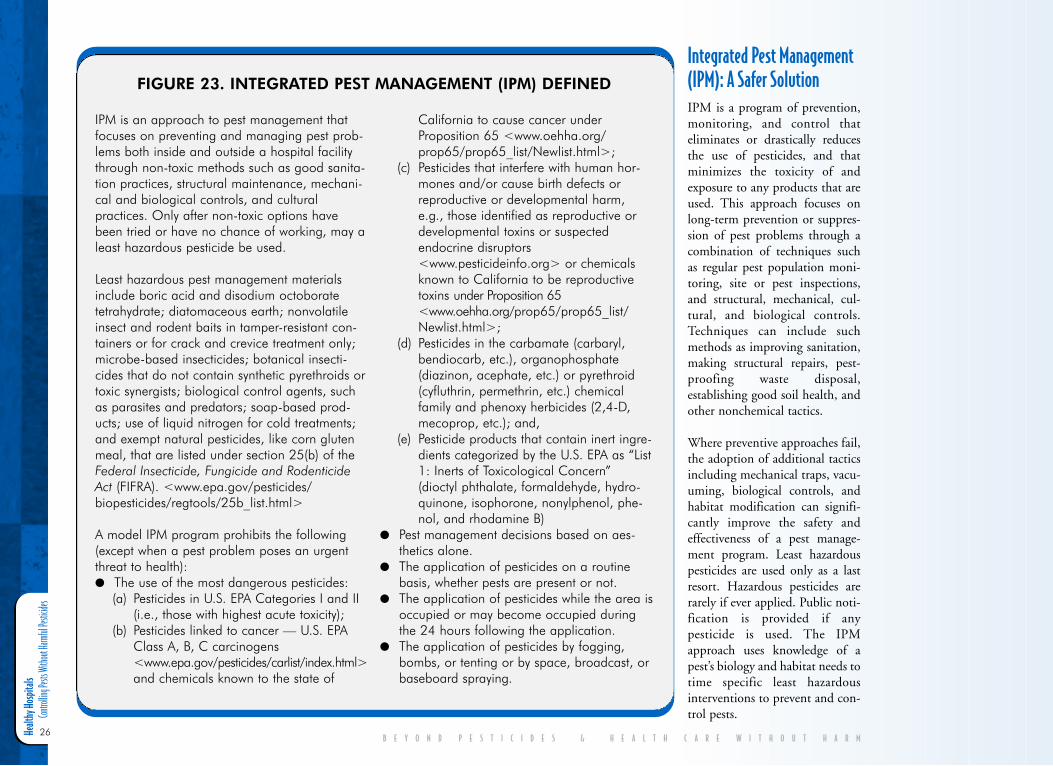
Healt
hy Ho
spita
ls
Contro
lling P
ests W
ithout
Harm
ful Pe
sticide
s
26
Integrated Pest Management(IPM): A Safer SolutionIPM is a program of prevention,monitoring, and control thateliminates or drastically reducesthe use of pesticides, and thatminimizes the toxicity of andexposure to any products that areused. This approach focuses onlong-term prevention or suppres-sion of pest problems through acombination of techniques suchas regular pest population moni-toring, site or pest inspections,and structural, mechanical, cul-tural, and biological controls.Techniques can include suchmethods as improving sanitation,making structural repairs, pest-proofing waste disposal,establishing good soil health, andother nonchemical tactics.
Where preventive approaches fail,the adoption of additional tacticsincluding mechanical traps, vacu-uming, biological controls, andhabitat modification can signifi-cantly improve the safety andeffectiveness of a pest manage-ment program. Least hazardouspesticides are used only as a lastresort. Hazardous pesticides arerarely if ever applied. Public noti-fication is provided if anypesticide is used. The IPMapproach uses knowledge of apest’s biology and habitat needs totime specific least hazardousinterventions to prevent and con-trol pests.
B E Y O N D P E S T I C I D E S & H E A L T H C A R E W I T H O U T H A R M
IPM is an approach to pest management thatfocuses on preventing and managing pest prob-lems both inside and outside a hospital facilitythrough non-toxic methods such as good sanita-tion practices, structural maintenance, mechani-cal and biological controls, and culturalpractices. Only after non-toxic options havebeen tried or have no chance of working, may aleast hazardous pesticide be used.
Least hazardous pest management materialsinclude boric acid and disodium octoboratetetrahydrate; diatomaceous earth; nonvolatileinsect and rodent baits in tamper-resistant con-tainers or for crack and crevice treatment only;microbe-based insecticides; botanical insecti-cides that do not contain synthetic pyrethroids ortoxic synergists; biological control agents, suchas parasites and predators; soap-based prod-ucts; use of liquid nitrogen for cold treatments;and exempt natural pesticides, like corn glutenmeal, that are listed under section 25(b) of theFederal Insecticide, Fungicide and RodenticideAct (FIFRA). <www.epa.gov/pesticides/biopesticides/regtools/25b_list.html>
A model IPM program prohibits the following(except when a pest problem poses an urgentthreat to health): ● The use of the most dangerous pesticides:
(a) Pesticides in U.S. EPA Categories I and II(i.e., those with highest acute toxicity);
(b) Pesticides linked to cancer — U.S. EPAClass A, B, C carcinogens <www.epa.gov/pesticides/carlist/index.html>and chemicals known to the state of
California to cause cancer underProposition 65 <www.oehha.org/prop65/prop65_list/Newlist.html>;
(c) Pesticides that interfere with human hor-mones and/or cause birth defects orreproductive or developmental harm,e.g., those identified as reproductive ordevelopmental toxins or suspectedendocrine disruptors<www.pesticideinfo.org> or chemicalsknown to California to be reproductivetoxins under Proposition 65<www.oehha.org/prop65/prop65_list/Newlist.html>;
(d) Pesticides in the carbamate (carbaryl,bendiocarb, etc.), organophosphate(diazinon, acephate, etc.) or pyrethroid(cyfluthrin, permethrin, etc.) chemicalfamily and phenoxy herbicides (2,4-D,mecoprop, etc.); and,
(e) Pesticide products that contain inert ingre-dients categorized by the U.S. EPA as “List1: Inerts of Toxicological Concern”(dioctyl phthalate, formaldehyde, hydro-quinone, isophorone, nonylphenol, phe-nol, and rhodamine B)
● Pest management decisions based on aes-thetics alone.
● The application of pesticides on a routinebasis, whether pests are present or not.
● The application of pesticides while the area isoccupied or may become occupied duringthe 24 hours following the application.
● The application of pesticides by fogging,bombs, or tenting or by space, broadcast, orbaseboard spraying.
FIGURE 23. INTEGRATED PEST MANAGEMENT (IPM) DEFINED

Healthy Hospitals Controlling Pests Without Harmful Pesticides
27
B E Y O N D P E S T I C I D E S & H E A L T H C A R E W I T H O U T H A R M
Hospitals deciding to use an IPM programshould adopt a written IPM policy that clearlyspecifies the program’s goals and establishes aprocess for decision-making. This will helpensure the program’s implementation successand longevity. An IPM policy gives facilitymanagers and commercial pest control contrac-tors guidance on how to prevent and managepest problems in the least hazardous mannerpossible.
It is important to involve staff from varioushospital departments in the creation and imple-mentation of the IPM program, including legaland risk management staff, administrators, cus-todians, maintenance personnel, and cafeteriastaff. Medical oversight should also be providedto ensure that the health needs of patients andemployees are protected. An IPM coordinatorshould be designated to manage or oversee theIPM program. The most appropriate person tobe the IPM coordinator is usually the currentstaff person in charge of the hospital’s pest con-trol (often the environmental services manager)and/or the person in charge of grounds andmaintenance. The coordinator’s job shouldinclude supervising staff in managing pests,doing the work himself or herself, and/or over-seeing a contractor’s work. In any case,decisions about a hospital’s pest managementare best done by a knowledgeable person whodoes not have a financial interest in selling apesticide product or service. The IPM coordi-nator should also determine the needs of thevarious areas of the hospital and set “actionthresholds,” or pest population levels thatrequire remedial action for human health oreconomic reasons.
Hospital administrators and the IPM coordina-tor should be aware that while true IPM usesfew or no pesticides, some pest control compa-
nies call their traditional pesticide spray pro-grams IPM. The main difference in IPMprograms comes down to the emphasis onchemical controls. Therefore, prior to hiring acompany, it is important to evaluate the detailsof its IPM program to determine whether itconforms to the criteria discussed in this reportand the hospital’s IPM policy. Monthly orother regular pesticide spraying, even if it is acrack and crevice application, is not IPM.
Key Elements of an IPM Program
Education Education, in the form of workshops, trainingsessions, and written materials, is an essentialcomponent of an IPM program. It takes coop-eration and resource sharing between severalhospital departments to get the necessary train-ing to the appropriate staff. All hospitaloccupants, including administrators, cafeteriastaff, doctors, nurses, patients, volunteers, andvisitors should be informed about the advan-tages of IPM and the hazards of pesticides.Educational programs should emphasize theneed for hospital occupants to monitor andreport pest problems and reactions to pest con-trol products, and stress the importance ofproperly sealing food containers, minimizingdispersion of crumbs, and appropriately dispos-ing of food waste.
MonitoringRegular site inspections and pest trappings(e.g., with mousetraps or glue boards) helpdetermine whether pests are present andwhether they are present at a level that requirescontrol measures. Monitoring can also helpestablish possible causes of a pest problem(such as leaky pipes, food crumbs, cracks in the
walls, or drought-stressed plants) and the out-comes of control measures used. Monitoring iscritical to reducing pest management costsbecause it helps pest managers target theirintervention to only those areas where pestpopulations are present at a level that warrantsaction.
Pest PreventionNon-chemical prevention is the primary meansof pest management in an IPM program. Keyelements include habitat modification thatreduces or eliminates sources of food, water,shelter, and entryways for pests as well as themaintenance of healthy lawns and landscapes.Taking preventative measures as simple as thor-oughly cleaning food storage areas, caulkingcracks, daily removal of waste to dumpsters,educating hospital staff and occupants aboutthe importance of proper waste disposal, spread-ing mulch to combat weeds, landscaping withpest- and drought-resistant plants, using weed-free seed, and installing rat-proof wastecompactors can markedly reduce pest problems.
Buildings should be designed to be as pestresistant as possible by:
● Caulking cracks and gaps in the buildingto block pest entry;
● Using door sweeps and screens;
● Grading away from the building to preventwater pooling that fosters mold growth;
● Landscaping with indigenous vegetationthat is naturally pest resistant;
● Avoiding indoor plantings that fostermold growth and can be attractants forpests; and,
● Keeping vegetation away from buildingsto reduce mold growth and pests’ accessto the building.
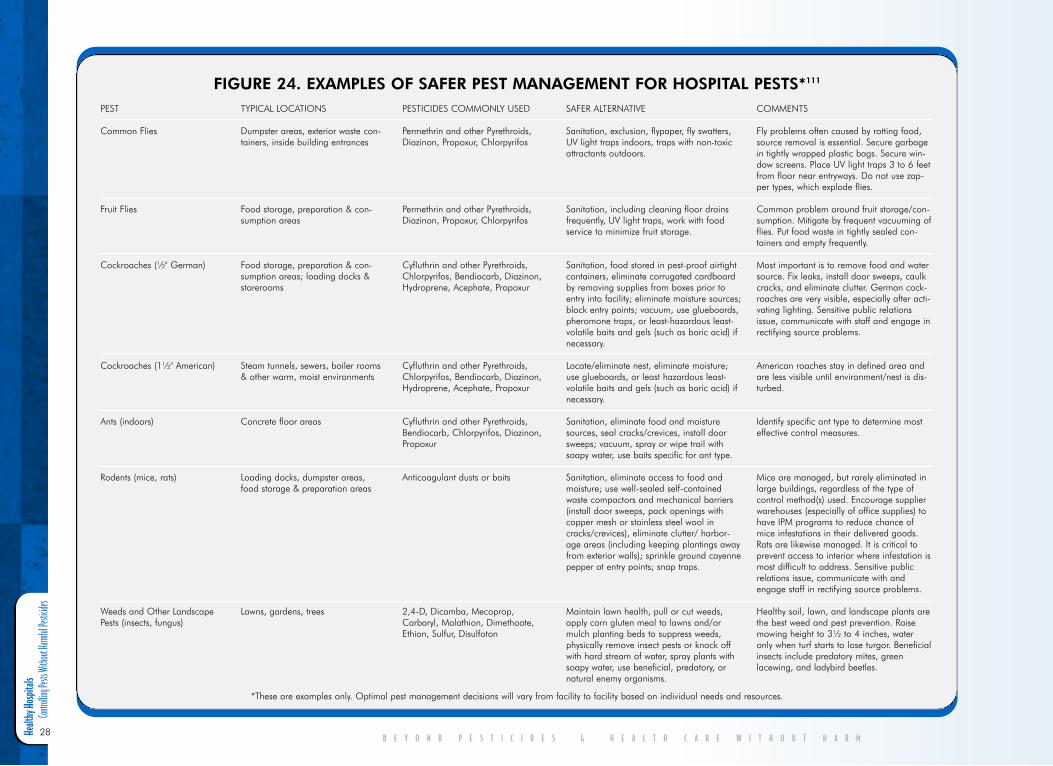
Healt
hy Ho
spita
ls
Contro
lling P
ests W
ithout
Harm
ful Pe
sticide
s
28B E Y O N D P E S T I C I D E S & H E A L T H C A R E W I T H O U T H A R M
PEST
Common Flies
Fruit Flies
Cockroaches (½" German)
Cockroaches (1½" American)
Ants (indoors)
Rodents (mice, rats)
Weeds and Other Landscape Pests (insects, fungus)
TYPICAL LOCATIONS
Dumpster areas, exterior waste con-tainers, inside building entrances
Food storage, preparation & con-sumption areas
Food storage, preparation & con-sumption areas; loading docks &storerooms
Steam tunnels, sewers, boiler rooms& other warm, moist environments
Concrete floor areas
Loading docks, dumpster areas,food storage & preparation areas
Lawns, gardens, trees
PESTICIDES COMMONLY USED
Permethrin and other Pyrethroids,Diazinon, Propoxur, Chlorpyrifos
Permethrin and other Pyrethroids,Diazinon, Propoxur, Chlorpyrifos
Cyfluthrin and other Pyrethroids,Chlorpyrifos, Bendiocarb, Diazinon,Hydroprene, Acephate, Propoxur
Cyfluthrin and other Pyrethroids,Chlorpyrifos, Bendiocarb, Diazinon,Hydroprene, Acephate, Propoxur
Cyfluthrin and other Pyrethroids,Bendiocarb, Chlorpyrifos, Diazinon,Propoxur
Anticoagulant dusts or baits
2,4-D, Dicamba, Mecoprop,Carbaryl, Malathion, Dimethoate,Ethion, Sulfur, Disulfoton
COMMENTS
Fly problems often caused by rotting food,source removal is essential. Secure garbagein tightly wrapped plastic bags. Secure win-dow screens. Place UV light traps 3 to 6 feetfrom floor near entryways. Do not use zap-per types, which explode flies.
Common problem around fruit storage/con-sumption. Mitigate by frequent vacuuming offlies. Put food waste in tightly sealed con-tainers and empty frequently.
Most important is to remove food and watersource. Fix leaks, install door sweeps, caulkcracks, and eliminate clutter. German cock-roaches are very visible, especially after acti-vating lighting. Sensitive public relationsissue, communicate with staff and engage inrectifying source problems.
American roaches stay in defined area andare less visible until environment/nest is dis-turbed.
Identify specific ant type to determine mosteffective control measures.
Mice are managed, but rarely eliminated inlarge buildings, regardless of the type ofcontrol method(s) used. Encourage supplierwarehouses (especially of office supplies) tohave IPM programs to reduce chance ofmice infestations in their delivered goods.Rats are likewise managed. It is critical toprevent access to interior where infestation ismost difficult to address. Sensitive publicrelations issue, communicate with andengage staff in rectifying source problems.
Healthy soil, lawn, and landscape plants arethe best weed and pest prevention. Raisemowing height to 3½ to 4 inches, wateronly when turf starts to lose turgor. Beneficialinsects include predatory mites, greenlacewing, and ladybird beetles.
SAFER ALTERNATIVE
Sanitation, exclusion, flypaper, fly swatters,UV light traps indoors, traps with non-toxicattractants outdoors.
Sanitation, including cleaning floor drainsfrequently, UV light traps, work with foodservice to minimize fruit storage.
Sanitation, food stored in pest-proof airtightcontainers, eliminate corrugated cardboardby removing supplies from boxes prior toentry into facility; eliminate moisture sources;block entry points; vacuum, use glueboards,pheromone traps, or least-hazardous least-volatile baits and gels (such as boric acid) ifnecessary.
Locate/eliminate nest, eliminate moisture;use glueboards, or least hazardous least-volatile baits and gels (such as boric acid) ifnecessary.
Sanitation, eliminate food and moisturesources, seal cracks/crevices, install doorsweeps; vacuum, spray or wipe trail withsoapy water, use baits specific for ant type.
Sanitation, eliminate access to food andmoisture; use well-sealed self-containedwaste compactors and mechanical barriers(install door sweeps, pack openings withcopper mesh or stainless steel wool incracks/crevices), eliminate clutter/ harbor-age areas (including keeping plantings awayfrom exterior walls); sprinkle ground cayennepepper at entry points; snap traps.
Maintain lawn health, pull or cut weeds,apply corn gluten meal to lawns and/ormulch planting beds to suppress weeds,physically remove insect pests or knock offwith hard stream of water, spray plants withsoapy water, use beneficial, predatory, ornatural enemy organisms.
FIGURE 24. EXAMPLES OF SAFER PEST MANAGEMENT FOR HOSPITAL PESTS*111
*These are examples only. Optimal pest management decisions will vary from facility to facility based on individual needs and resources.
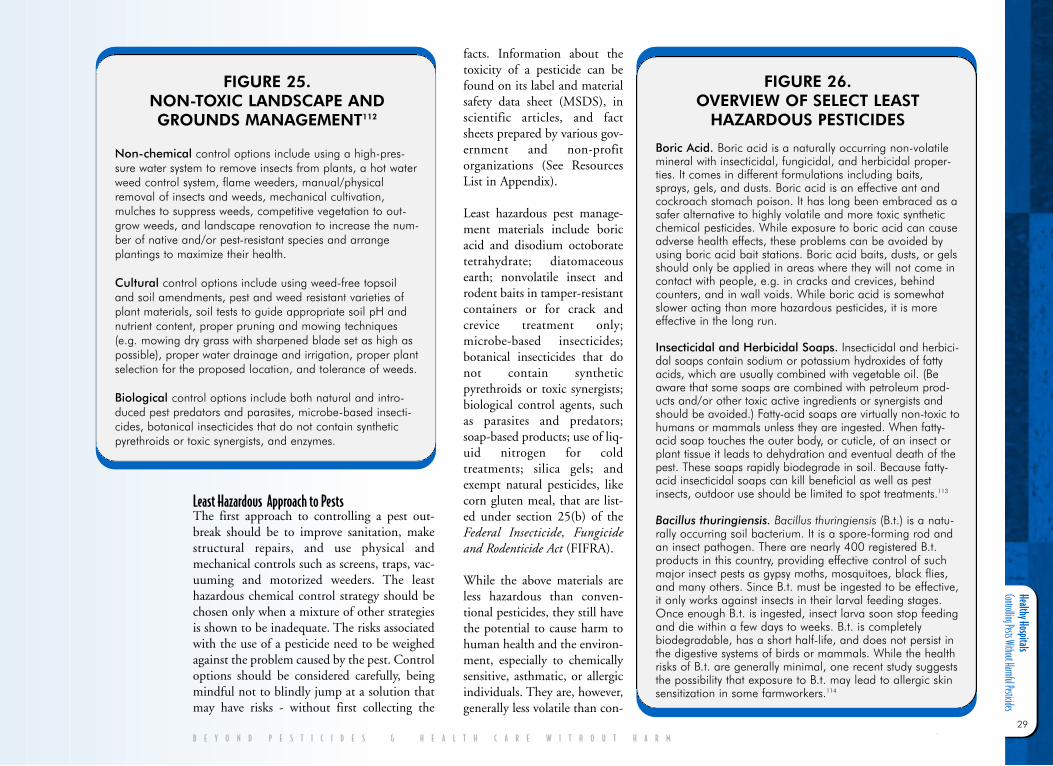
Healthy Hospitals Controlling Pests Without Harmful Pesticides
29
B E Y O N D P E S T I C I D E S & H E A L T H C A R E W I T H O U T H A R M
Least Hazardous Approach to Pests The first approach to controlling a pest out-break should be to improve sanitation, makestructural repairs, and use physical andmechanical controls such as screens, traps, vac-uuming and motorized weeders. The leasthazardous chemical control strategy should bechosen only when a mixture of other strategiesis shown to be inadequate. The risks associatedwith the use of a pesticide need to be weighedagainst the problem caused by the pest. Controloptions should be considered carefully, beingmindful not to blindly jump at a solution thatmay have risks - without first collecting the
facts. Information about thetoxicity of a pesticide can befound on its label and materialsafety data sheet (MSDS), inscientific articles, and factsheets prepared by various gov-ernment and non-profitorganizations (See ResourcesList in Appendix).
Least hazardous pest manage-ment materials include boricacid and disodium octoboratetetrahydrate; diatomaceousearth; nonvolatile insect androdent baits in tamper-resistantcontainers or for crack andcrevice treatment only;microbe-based insecticides;botanical insecticides that donot contain syntheticpyrethroids or toxic synergists;biological control agents, suchas parasites and predators;soap-based products; use of liq-uid nitrogen for coldtreatments; silica gels; andexempt natural pesticides, likecorn gluten meal, that are list-ed under section 25(b) of theFederal Insecticide, Fungicideand Rodenticide Act (FIFRA).
While the above materials areless hazardous than conven-tional pesticides, they still havethe potential to cause harm tohuman health and the environ-ment, especially to chemicallysensitive, asthmatic, or allergicindividuals. They are, however,generally less volatile than con-
FIGURE 25. NON-TOXIC LANDSCAPE ANDGROUNDS MANAGEMENT112
Non-chemical control options include using a high-pres-sure water system to remove insects from plants, a hot waterweed control system, flame weeders, manual/physicalremoval of insects and weeds, mechanical cultivation,mulches to suppress weeds, competitive vegetation to out-grow weeds, and landscape renovation to increase the num-ber of native and/or pest-resistant species and arrangeplantings to maximize their health.
Cultural control options include using weed-free topsoiland soil amendments, pest and weed resistant varieties ofplant materials, soil tests to guide appropriate soil pH andnutrient content, proper pruning and mowing techniques(e.g. mowing dry grass with sharpened blade set as high aspossible), proper water drainage and irrigation, proper plantselection for the proposed location, and tolerance of weeds.
Biological control options include both natural and intro-duced pest predators and parasites, microbe-based insecti-cides, botanical insecticides that do not contain syntheticpyrethroids or toxic synergists, and enzymes.
FIGURE 26. OVERVIEW OF SELECT LEAST
HAZARDOUS PESTICIDES
Boric Acid. Boric acid is a naturally occurring non-volatilemineral with insecticidal, fungicidal, and herbicidal proper-ties. It comes in different formulations including baits,sprays, gels, and dusts. Boric acid is an effective ant andcockroach stomach poison. It has long been embraced as asafer alternative to highly volatile and more toxic syntheticchemical pesticides. While exposure to boric acid can causeadverse health effects, these problems can be avoided byusing boric acid bait stations. Boric acid baits, dusts, or gelsshould only be applied in areas where they will not come incontact with people, e.g. in cracks and crevices, behindcounters, and in wall voids. While boric acid is somewhatslower acting than more hazardous pesticides, it is moreeffective in the long run.
Insecticidal and Herbicidal Soaps. Insecticidal and herbici-dal soaps contain sodium or potassium hydroxides of fattyacids, which are usually combined with vegetable oil. (Beaware that some soaps are combined with petroleum prod-ucts and/or other toxic active ingredients or synergists andshould be avoided.) Fatty-acid soaps are virtually non-toxic tohumans or mammals unless they are ingested. When fatty-acid soap touches the outer body, or cuticle, of an insect orplant tissue it leads to dehydration and eventual death of thepest. These soaps rapidly biodegrade in soil. Because fatty-acid insecticidal soaps can kill beneficial as well as pestinsects, outdoor use should be limited to spot treatments.113
Bacillus thuringiensis. Bacillus thuringiensis (B.t.) is a natu-rally occurring soil bacterium. It is a spore-forming rod andan insect pathogen. There are nearly 400 registered B.t.products in this country, providing effective control of suchmajor insect pests as gypsy moths, mosquitoes, black flies,and many others. Since B.t. must be ingested to be effective,it only works against insects in their larval feeding stages.Once enough B.t. is ingested, insect larva soon stop feedingand die within a few days to weeks. B.t. is completelybiodegradable, has a short half-life, and does not persist inthe digestive systems of birds or mammals. While the healthrisks of B.t. are generally minimal, one recent study suggeststhe possibility that exposure to B.t. may lead to allergic skinsensitization in some farmworkers.114
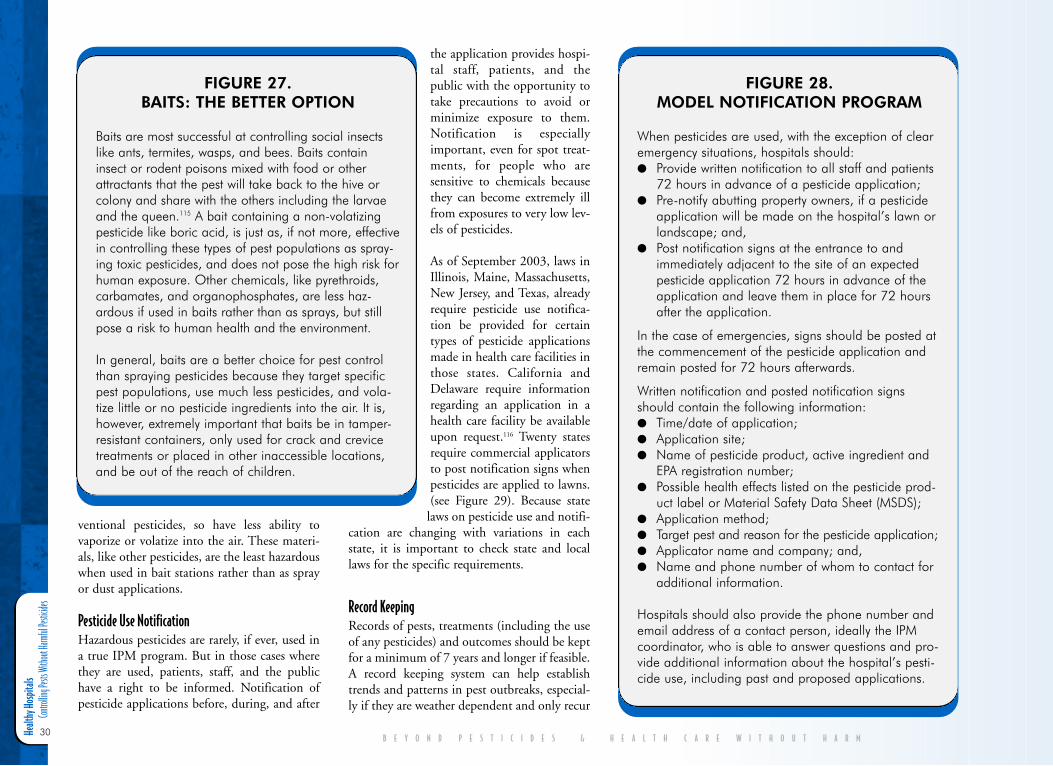
Healt
hy Ho
spita
ls
Contro
lling P
ests W
ithout
Harm
ful Pe
sticide
s
30
ventional pesticides, so have less ability tovaporize or volatize into the air. These materi-als, like other pesticides, are the least hazardouswhen used in bait stations rather than as sprayor dust applications.
Pesticide Use Notification Hazardous pesticides are rarely, if ever, used ina true IPM program. But in those cases wherethey are used, patients, staff, and the publichave a right to be informed. Notification ofpesticide applications before, during, and after
the application provides hospi-tal staff, patients, and thepublic with the opportunity totake precautions to avoid orminimize exposure to them.Notification is especiallyimportant, even for spot treat-ments, for people who aresensitive to chemicals becausethey can become extremely illfrom exposures to very low lev-els of pesticides.
As of September 2003, laws inIllinois, Maine, Massachusetts,New Jersey, and Texas, alreadyrequire pesticide use notifica-tion be provided for certaintypes of pesticide applicationsmade in health care facilities inthose states. California andDelaware require informationregarding an application in ahealth care facility be availableupon request.116 Twenty statesrequire commercial applicatorsto post notification signs whenpesticides are applied to lawns.(see Figure 29). Because state
laws on pesticide use and notifi-cation are changing with variations in eachstate, it is important to check state and locallaws for the specific requirements.
Record Keeping Records of pests, treatments (including the useof any pesticides) and outcomes should be keptfor a minimum of 7 years and longer if feasible.A record keeping system can help establishtrends and patterns in pest outbreaks, especial-ly if they are weather dependent and only recur
B E Y O N D P E S T I C I D E S & H E A L T H C A R E W I T H O U T H A R M
FIGURE 27. BAITS: THE BETTER OPTION
Baits are most successful at controlling social insectslike ants, termites, wasps, and bees. Baits containinsect or rodent poisons mixed with food or otherattractants that the pest will take back to the hive orcolony and share with the others including the larvaeand the queen.115 A bait containing a non-volatizingpesticide like boric acid, is just as, if not more, effectivein controlling these types of pest populations as spray-ing toxic pesticides, and does not pose the high risk forhuman exposure. Other chemicals, like pyrethroids,carbamates, and organophosphates, are less haz-ardous if used in baits rather than as sprays, but stillpose a risk to human health and the environment.
In general, baits are a better choice for pest controlthan spraying pesticides because they target specificpest populations, use much less pesticides, and vola-tize little or no pesticide ingredients into the air. It is,however, extremely important that baits be in tamper-resistant containers, only used for crack and crevicetreatments or placed in other inaccessible locations,and be out of the reach of children.
FIGURE 28. MODEL NOTIFICATION PROGRAM
When pesticides are used, with the exception of clearemergency situations, hospitals should:● Provide written notification to all staff and patients
72 hours in advance of a pesticide application;● Pre-notify abutting property owners, if a pesticide
application will be made on the hospital’s lawn orlandscape; and,
● Post notification signs at the entrance to andimmediately adjacent to the site of an expectedpesticide application 72 hours in advance of theapplication and leave them in place for 72 hoursafter the application.
In the case of emergencies, signs should be posted atthe commencement of the pesticide application andremain posted for 72 hours afterwards.
Written notification and posted notification signsshould contain the following information: ● Time/date of application; ● Application site;● Name of pesticide product, active ingredient and
EPA registration number;● Possible health effects listed on the pesticide prod-
uct label or Material Safety Data Sheet (MSDS);● Application method; ● Target pest and reason for the pesticide application; ● Applicator name and company; and,● Name and phone number of whom to contact for
additional information.
Hospitals should also provide the phone number andemail address of a contact person, ideally the IPMcoordinator, who is able to answer questions and pro-vide additional information about the hospital’s pesti-cide use, including past and proposed applications.
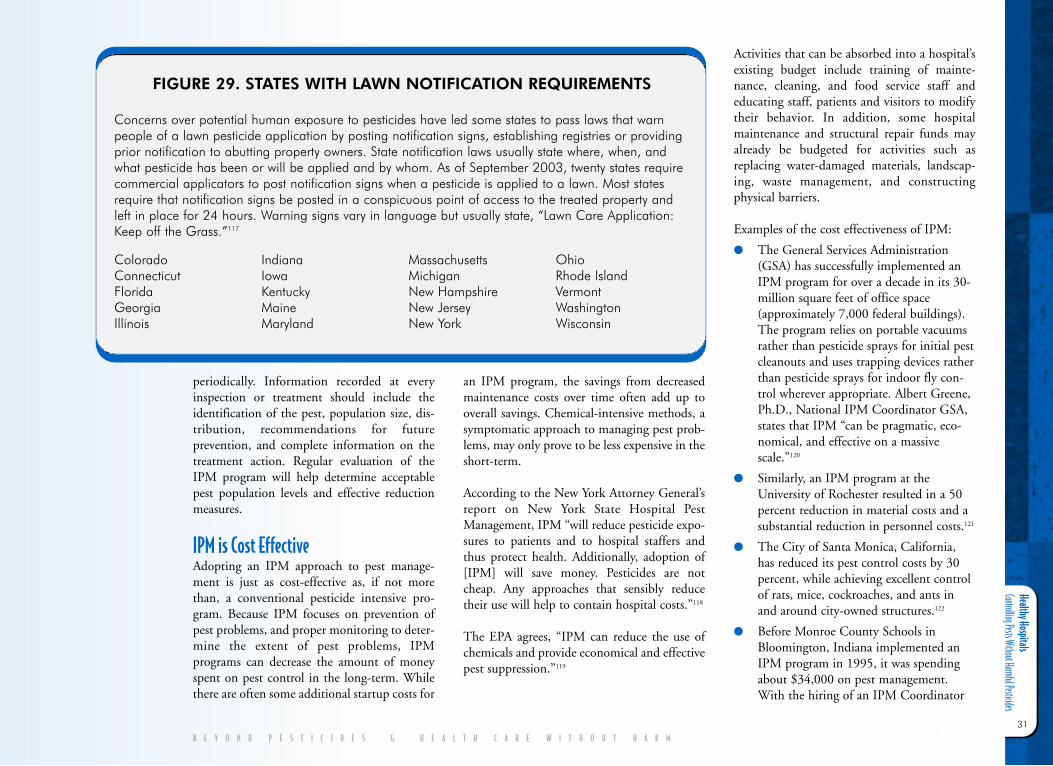
Healthy Hospitals Controlling Pests Without Harmful Pesticides
31
B E Y O N D P E S T I C I D E S & H E A L T H C A R E W I T H O U T H A R M
periodically. Information recorded at everyinspection or treatment should include theidentification of the pest, population size, dis-tribution, recommendations for futureprevention, and complete information on thetreatment action. Regular evaluation of theIPM program will help determine acceptablepest population levels and effective reductionmeasures.
IPM is Cost EffectiveAdopting an IPM approach to pest manage-ment is just as cost-effective as, if not morethan, a conventional pesticide intensive pro-gram. Because IPM focuses on prevention ofpest problems, and proper monitoring to deter-mine the extent of pest problems, IPMprograms can decrease the amount of moneyspent on pest control in the long-term. Whilethere are often some additional startup costs for
an IPM program, the savings from decreasedmaintenance costs over time often add up tooverall savings. Chemical-intensive methods, asymptomatic approach to managing pest prob-lems, may only prove to be less expensive in theshort-term.
According to the New York Attorney General’sreport on New York State Hospital PestManagement, IPM “will reduce pesticide expo-sures to patients and to hospital staffers andthus protect health. Additionally, adoption of[IPM] will save money. Pesticides are notcheap. Any approaches that sensibly reducetheir use will help to contain hospital costs.”118
The EPA agrees, “IPM can reduce the use ofchemicals and provide economical and effectivepest suppression.”119
Activities that can be absorbed into a hospital’sexisting budget include training of mainte-nance, cleaning, and food service staff andeducating staff, patients and visitors to modifytheir behavior. In addition, some hospitalmaintenance and structural repair funds mayalready be budgeted for activities such asreplacing water-damaged materials, landscap-ing, waste management, and constructingphysical barriers.
Examples of the cost effectiveness of IPM:
● The General Services Administration(GSA) has successfully implemented anIPM program for over a decade in its 30-million square feet of office space(approximately 7,000 federal buildings).The program relies on portable vacuumsrather than pesticide sprays for initial pestcleanouts and uses trapping devices ratherthan pesticide sprays for indoor fly con-trol wherever appropriate. Albert Greene,Ph.D., National IPM Coordinator GSA,states that IPM “can be pragmatic, eco-nomical, and effective on a massivescale.”120
● Similarly, an IPM program at theUniversity of Rochester resulted in a 50percent reduction in material costs and asubstantial reduction in personnel costs.121
● The City of Santa Monica, California,has reduced its pest control costs by 30percent, while achieving excellent controlof rats, mice, cockroaches, and ants inand around city-owned structures.122
● Before Monroe County Schools inBloomington, Indiana implemented anIPM program in 1995, it was spendingabout $34,000 on pest management.With the hiring of an IPM Coordinator
Concerns over potential human exposure to pesticides have led some states to pass laws that warnpeople of a lawn pesticide application by posting notification signs, establishing registries or providingprior notification to abutting property owners. State notification laws usually state where, when, andwhat pesticide has been or will be applied and by whom. As of September 2003, twenty states requirecommercial applicators to post notification signs when a pesticide is applied to a lawn. Most statesrequire that notification signs be posted in a conspicuous point of access to the treated property andleft in place for 24 hours. Warning signs vary in language but usually state, “Lawn Care Application:Keep off the Grass.”117
FIGURE 29. STATES WITH LAWN NOTIFICATION REQUIREMENTS
ColoradoConnecticutFlorida GeorgiaIllinois
IndianaIowaKentuckyMaineMaryland
Massachusetts MichiganNew Hampshire New JerseyNew York
OhioRhode Island VermontWashingtonWisconsin

Healt
hy Ho
spita
ls
Contro
lling P
ests W
ithout
Harm
ful Pe
sticide
s
32
in 1997, and spending less than $1,000per year on products, the school district issaving around $13,600 annually in pestmanagement costs.123 Conventional pesti-cide use has dropped by approximately 90percent with the IPM program, and allaerosol and liquid pesticides have beendiscontinued.124
Examples of Hospital IPM ProgramsThe following hospital facilities have institutedIPM policies that have significantly decreasedtheir unnecessary use of pesticides.
Veterans HospitalsAs highlighted in the 1995 Beyond Pesticidesreport, A Failure to Protect, which surveyed sixveterans hospitals, the Department of VeteransAffairs (VA) has an IPM policy that says thatdue to “the rising public concern over the accu-mulation of pesticides in the environment andresulting adverse effects on some wildlife popu-lations and hazards to human health, theconcept of IPM has become the economically-efficient, environmentally preferable approachto pest control.”125 The VA policy describes spe-cific IPM tasks in detail including inspections,environmental sanitation, no chemical controlmethods where appropriate alternatives exist,identification of sensitive areas and the selec-tion, and use of the least hazardous pesticidewhen needed. VA requires a pest managementplan for each facility. Its policy discourages theperiodic application of pesticides as a preven-tive measure, promoting instead the use ofnon-chemical methods to prevent and managepests. The “control of pests through alternativemethods (environmental sanitation, trapping,exclusion, etc.) is the first choice, and only afterthese methods have failed should the least toxic
pesticide be employed and only to the extentnecessary for effective control.”126
“Everybody’s knee-jerk reaction is to haul outsome pesticide and just kill the critters,” saysWayne Warren, director of environmental pro-gram services for the Veterans HealthAdministration. “That’s not always the bestthing to do.” Warren suggests that more hospi-tals should be using vacuum cleaners as part oftheir pest management program as they poseno health hazard to the operator, are effective inremoving pests, and can be used anywhere inthe facility.127
Oregon Health and Science University The Oregon Health and Science University(OHSU) includes four schools, two hospitals,dozens of primary care and specialty clinics,research institutes and centers, and communityservice programs. The Facilities Managementand Construction office of the GroundsDepartment has nine staff to maintain their120-acre campus in Portland, which includesthe state run hospital.128 The OHSU outdoorIPM policy states that its intent “is to providean acceptable level of pest control while insur-ing minimal human exposure to hazardousmaterials, minimizing the health risks, inflict-ing minimal environmental hazard upon theenvironment, providing for effective monitor-ing through inspections and record keeping,and evaluating the effect of the IPM program.”The policy establishes the GroundsCoordinator as being responsible for the imple-mentation of the campus-wide IPM program.The policy states, “Once the threshold has beensurpassed, treatment and control options willbe determined. The least toxic alternative thatwill obtain the necessary control of the pest willbe used.” The policy contains a prioritizedfour-option system for making pest manage-
ment decisions. The fourth, or last, option tobe considered is chemical controls, whichshould be “the least toxic to the environment,as well as the least toxic to the applicator andthe campus patients, visitors, and staff.” Eventhe listing of this last option is prioritized –spot treatment is to be used before “a compre-hensive treatment, the use of which wouldlikely be unusual.”
OHSU’s policy also has a notification compo-nent that states, “The use of any control optionthat may have an impact on persons or depart-ments in the immediate area should beaccompanied by proper notification of theaction to be taken. This notification willinclude Facilities Management andConstruction Public Safety Dispatch, so build-ing air intakes can be secured and alertinganyone with open windows of the immediatetreatment area.” The policy recommends thatapplications be scheduled at times of least effecton the public. If pedestrians or vehicles will bepresent during the application, barriers andtraffic flaggers are used to divert them from theapplication area. Other provisions in theOHSU policy include pesticide safety trainingfor all applicators and the requirement to keepdetailed records of pests, interventions, andpesticide use. The IPM program is evaluatedannually. Although in-house staff currentlyimplement the facility’s IPM policy, there is aprovision in the policy requiring outside con-tractors to follow the policy as well.
B E Y O N D P E S T I C I D E S & H E A L T H C A R E W I T H O U T H A R M
Healthy Hospitals Controlling Pests Without Harmful Pesticides
33
B E Y O N D P E S T I C I D E S & H E A L T H C A R E W I T H O U T H A R M
San Francisco General HospitalIn October 1996, San Francisco passed agroundbreaking policy to reduce the use of pes-ticides on city property by city departments,agencies, and contractors, including SanFrancisco General Hospital (SFGH). The land-mark ordinance bans pesticides suspected ofcausing cancer and reproductive harm andthose that are most acutely toxic. It alsorequires an IPM approach to pest management,posting notices of most pesticide applications72 hours before and after an application, andthe exclusive use of approved pesticides. Theresulting pest management program empha-sizes education and developing less-harmfulalternatives to toxic chemicals, such asmulching, hand weeding, using flamers andnatural predators. The program also recom-mends planting foliage that is suitable to SanFrancisco’s climate and, therefore, more natu-rally resistant to pests. (For more information,see Figure 30 on page 34.)
Massachusetts General Hospital The hospital’s pest management program isbased on IPM principles that emphasize pre-vention through physical exclusion andattention to sanitation. MGH “stronglyoppose[s] the use of pesticides in the work-place.” Baits and traps are more likely to beemployed than pesticide sprays. Yet, if pesticidesprays are used, they are not to be applied in anoccupied room. The hospital uses triangularwall sconces that emit a blue light to attract fly-ing insects, which then stick to an adhesiveboard on the bottom of the trap. These trapsare effective in keeping flying insects fromentering the facility and moving into sensitiveareas.129
Brigham and Women’s HospitalBrigham and Women’s Hospital is a 700-bedtertiary care hospital in an urban setting thatanchors the Longwood Medical Area ofBoston. Combined inpatient and outpatientvolume correlates to a facility of nearly 3.5 mil-lion square feet. The Environmental ServicesDepartment of Brigham and Women’s Hospitalis responsible for the facility’s pest managementprogram. Their IPM policy was adopted inJanuary 1989 and has been regularly updatedsince then. As written in the policy, the purposeis, “To ensure a healthy, sanitary, and attractiveenvironment for patients, staff, and visitorsthrough the application of integrated pest man-agement principles.” Pest management servicesare required to be provided by an outside con-tractor, but the contactor must meet thepolicy’s vendor qualifications. The policy states,“The use of chemical pesticides is strongly dis-couraged and only authorized by the Directoron a case-by-case basis. Upon exhaustion ofalternative, non-pesticide treatments the ven-dor may recommend limited use of the leasthazardous effective chemical pesticide. TheDirector will review such recommendationand, if in concurrence, will submit the relevantMaterial Safety Data Sheets to theEnvironmental Health and Safety Departmentfor review and recommendations prior to theauthorization of limited pesticide use. A recordof the chemical application … will beentered… for future reference. Wherever possi-ble, application of chemical pesticides will belimited to wall voids, mechanical spaces, etc. tominimize the potential for human exposure.Aerosolized pesticides will not be used in areaswhere human exposure potential exists. Anylimited use of pesticides will be implementedonly with the awareness and approval of themanager of the area being serviced.” Other pro-
visions in the policy include the requirementfor weekly communication between the pestcontrol service contractor and the Director;posting of notification signs for lawn pesticideapplications; and prohibition of storing or mix-ing pesticides within the hospital facility. Baitsand hospital disinfectants are excluded fromthe policy. (For more information, see Figure 31on page 36.)
Hackensack University Medical CenterHackensack University Medical Center(HUMC) is a 683-bed tertiary care teachingand research hospital in New Jersey covering2.2 million square feet. The buildings range inage from 3 years to 106 years old. The hospitalinitiated its IPM program in the late 1990’susing a local pest control contractor. Staff wasre-trained and educated in new policies andpractices. Buildings were examined and repairproblems were addressed. According to thosethat oversee the program, the use of pesticidesis strongly discouraged. Preventive measures arealways the first step, such as weekly monitoringof specific areas (food, medical waste and solidwaste areas) and the use of mechanical traps.Sightings are immediately reported to environ-mental services and are dealt with in the mosthumane and least hazardous way. This includesevaluating the type of infestation, the efficacyand toxicity of the available alternatives, andthe manner in which products are applied.HUMC reports that it has not observed anyinfestations since its conversion to IPM.130
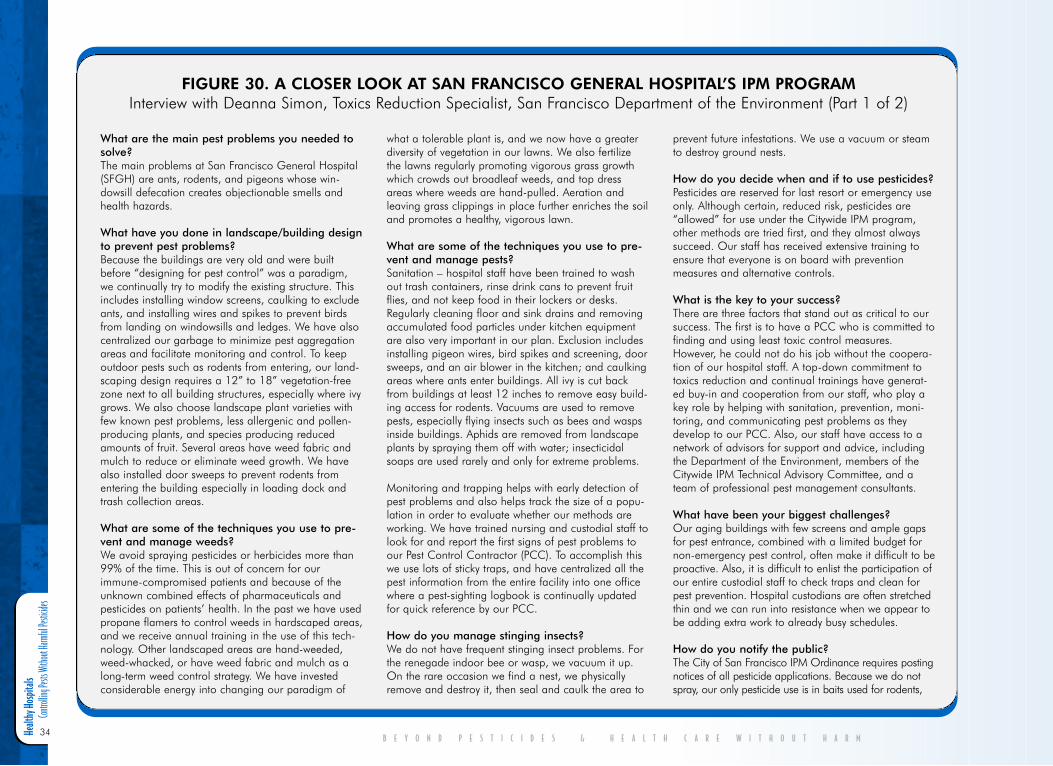
Healt
hy Ho
spita
ls
Contro
lling P
ests W
ithout
Harm
ful Pe
sticide
s
34B E Y O N D P E S T I C I D E S & H E A L T H C A R E W I T H O U T H A R M
What are the main pest problems you needed tosolve? The main problems at San Francisco General Hospital(SFGH) are ants, rodents, and pigeons whose win-dowsill defecation creates objectionable smells andhealth hazards.
What have you done in landscape/building designto prevent pest problems?Because the buildings are very old and were builtbefore “designing for pest control” was a paradigm,we continually try to modify the existing structure. Thisincludes installing window screens, caulking to excludeants, and installing wires and spikes to prevent birdsfrom landing on windowsills and ledges. We have alsocentralized our garbage to minimize pest aggregationareas and facilitate monitoring and control. To keepoutdoor pests such as rodents from entering, our land-scaping design requires a 12” to 18” vegetation-freezone next to all building structures, especially where ivygrows. We also choose landscape plant varieties withfew known pest problems, less allergenic and pollen-producing plants, and species producing reducedamounts of fruit. Several areas have weed fabric andmulch to reduce or eliminate weed growth. We havealso installed door sweeps to prevent rodents fromentering the building especially in loading dock andtrash collection areas.
What are some of the techniques you use to pre-vent and manage weeds?We avoid spraying pesticides or herbicides more than99% of the time. This is out of concern for ourimmune-compromised patients and because of theunknown combined effects of pharmaceuticals andpesticides on patients’ health. In the past we have usedpropane flamers to control weeds in hardscaped areas,and we receive annual training in the use of this tech-nology. Other landscaped areas are hand-weeded,weed-whacked, or have weed fabric and mulch as along-term weed control strategy. We have investedconsiderable energy into changing our paradigm of
what a tolerable plant is, and we now have a greaterdiversity of vegetation in our lawns. We also fertilizethe lawns regularly promoting vigorous grass growthwhich crowds out broadleaf weeds, and top dressareas where weeds are hand-pulled. Aeration andleaving grass clippings in place further enriches the soiland promotes a healthy, vigorous lawn.
What are some of the techniques you use to pre-vent and manage pests?Sanitation – hospital staff have been trained to washout trash containers, rinse drink cans to prevent fruitflies, and not keep food in their lockers or desks.Regularly cleaning floor and sink drains and removingaccumulated food particles under kitchen equipmentare also very important in our plan. Exclusion includesinstalling pigeon wires, bird spikes and screening, doorsweeps, and an air blower in the kitchen; and caulkingareas where ants enter buildings. All ivy is cut backfrom buildings at least 12 inches to remove easy build-ing access for rodents. Vacuums are used to removepests, especially flying insects such as bees and waspsinside buildings. Aphids are removed from landscapeplants by spraying them off with water; insecticidalsoaps are used rarely and only for extreme problems.
Monitoring and trapping helps with early detection ofpest problems and also helps track the size of a popu-lation in order to evaluate whether our methods areworking. We have trained nursing and custodial staff tolook for and report the first signs of pest problems toour Pest Control Contractor (PCC). To accomplish thiswe use lots of sticky traps, and have centralized all thepest information from the entire facility into one officewhere a pest-sighting logbook is continually updatedfor quick reference by our PCC.
How do you manage stinging insects? We do not have frequent stinging insect problems. Forthe renegade indoor bee or wasp, we vacuum it up.On the rare occasion we find a nest, we physicallyremove and destroy it, then seal and caulk the area to
prevent future infestations. We use a vacuum or steamto destroy ground nests.
How do you decide when and if to use pesticides?Pesticides are reserved for last resort or emergency useonly. Although certain, reduced risk, pesticides are“allowed” for use under the Citywide IPM program,other methods are tried first, and they almost alwayssucceed. Our staff has received extensive training toensure that everyone is on board with preventionmeasures and alternative controls.
What is the key to your success?There are three factors that stand out as critical to oursuccess. The first is to have a PCC who is committed tofinding and using least toxic control measures.However, he could not do his job without the coopera-tion of our hospital staff. A top-down commitment totoxics reduction and continual trainings have generat-ed buy-in and cooperation from our staff, who play akey role by helping with sanitation, prevention, moni-toring, and communicating pest problems as theydevelop to our PCC. Also, our staff have access to anetwork of advisors for support and advice, includingthe Department of the Environment, members of theCitywide IPM Technical Advisory Committee, and ateam of professional pest management consultants.
What have been your biggest challenges?Our aging buildings with few screens and ample gapsfor pest entrance, combined with a limited budget fornon-emergency pest control, often make it difficult to beproactive. Also, it is difficult to enlist the participation ofour entire custodial staff to check traps and clean forpest prevention. Hospital custodians are often stretchedthin and we can run into resistance when we appear tobe adding extra work to already busy schedules.
How do you notify the public?The City of San Francisco IPM Ordinance requires postingnotices of all pesticide applications. Because we do notspray, our only pesticide use is in baits used for rodents,
FIGURE 30. A CLOSER LOOK AT SAN FRANCISCO GENERAL HOSPITAL’S IPM PROGRAMInterview with Deanna Simon, Toxics Reduction Specialist, San Francisco Department of the Environment (Part 1 of 2)
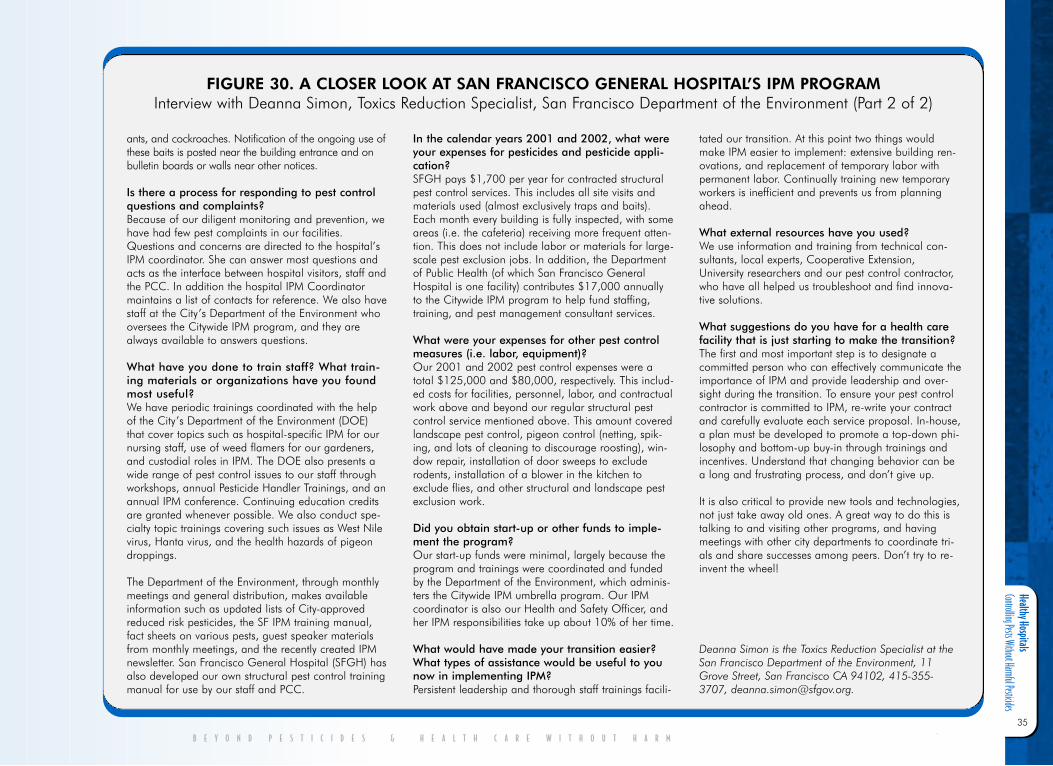
Healthy Hospitals Controlling Pests Without Harmful Pesticides
35
B E Y O N D P E S T I C I D E S & H E A L T H C A R E W I T H O U T H A R M
ants, and cockroaches. Notification of the ongoing use ofthese baits is posted near the building entrance and onbulletin boards or walls near other notices.
Is there a process for responding to pest controlquestions and complaints?Because of our diligent monitoring and prevention, wehave had few pest complaints in our facilities.Questions and concerns are directed to the hospital’sIPM coordinator. She can answer most questions andacts as the interface between hospital visitors, staff andthe PCC. In addition the hospital IPM Coordinatormaintains a list of contacts for reference. We also havestaff at the City’s Department of the Environment whooversees the Citywide IPM program, and they arealways available to answers questions.
What have you done to train staff? What train-ing materials or organizations have you foundmost useful?We have periodic trainings coordinated with the helpof the City’s Department of the Environment (DOE)that cover topics such as hospital-specific IPM for ournursing staff, use of weed flamers for our gardeners,and custodial roles in IPM. The DOE also presents awide range of pest control issues to our staff throughworkshops, annual Pesticide Handler Trainings, and anannual IPM conference. Continuing education creditsare granted whenever possible. We also conduct spe-cialty topic trainings covering such issues as West Nilevirus, Hanta virus, and the health hazards of pigeondroppings.
The Department of the Environment, through monthlymeetings and general distribution, makes availableinformation such as updated lists of City-approvedreduced risk pesticides, the SF IPM training manual,fact sheets on various pests, guest speaker materialsfrom monthly meetings, and the recently created IPMnewsletter. San Francisco General Hospital (SFGH) hasalso developed our own structural pest control trainingmanual for use by our staff and PCC.
In the calendar years 2001 and 2002, what wereyour expenses for pesticides and pesticide appli-cation?SFGH pays $1,700 per year for contracted structuralpest control services. This includes all site visits andmaterials used (almost exclusively traps and baits).Each month every building is fully inspected, with someareas (i.e. the cafeteria) receiving more frequent atten-tion. This does not include labor or materials for large-scale pest exclusion jobs. In addition, the Departmentof Public Health (of which San Francisco GeneralHospital is one facility) contributes $17,000 annuallyto the Citywide IPM program to help fund staffing,training, and pest management consultant services.
What were your expenses for other pest controlmeasures (i.e. labor, equipment)? Our 2001 and 2002 pest control expenses were atotal $125,000 and $80,000, respectively. This includ-ed costs for facilities, personnel, labor, and contractualwork above and beyond our regular structural pestcontrol service mentioned above. This amount coveredlandscape pest control, pigeon control (netting, spik-ing, and lots of cleaning to discourage roosting), win-dow repair, installation of door sweeps to excluderodents, installation of a blower in the kitchen toexclude flies, and other structural and landscape pestexclusion work.
Did you obtain start-up or other funds to imple-ment the program?Our start-up funds were minimal, largely because theprogram and trainings were coordinated and fundedby the Department of the Environment, which adminis-ters the Citywide IPM umbrella program. Our IPMcoordinator is also our Health and Safety Officer, andher IPM responsibilities take up about 10% of her time.
What would have made your transition easier?What types of assistance would be useful to younow in implementing IPM?Persistent leadership and thorough staff trainings facili-
tated our transition. At this point two things wouldmake IPM easier to implement: extensive building ren-ovations, and replacement of temporary labor withpermanent labor. Continually training new temporaryworkers is inefficient and prevents us from planningahead.
What external resources have you used?We use information and training from technical con-sultants, local experts, Cooperative Extension,University researchers and our pest control contractor,who have all helped us troubleshoot and find innova-tive solutions.
What suggestions do you have for a health carefacility that is just starting to make the transition? The first and most important step is to designate acommitted person who can effectively communicate theimportance of IPM and provide leadership and over-sight during the transition. To ensure your pest controlcontractor is committed to IPM, re-write your contractand carefully evaluate each service proposal. In-house,a plan must be developed to promote a top-down phi-losophy and bottom-up buy-in through trainings andincentives. Understand that changing behavior can bea long and frustrating process, and don’t give up.
It is also critical to provide new tools and technologies,not just take away old ones. A great way to do this istalking to and visiting other programs, and havingmeetings with other city departments to coordinate tri-als and share successes among peers. Don’t try to re-invent the wheel!
Deanna Simon is the Toxics Reduction Specialist at theSan Francisco Department of the Environment, 11Grove Street, San Francisco CA 94102, 415-355-3707, [email protected].
FIGURE 30. A CLOSER LOOK AT SAN FRANCISCO GENERAL HOSPITAL’S IPM PROGRAMInterview with Deanna Simon, Toxics Reduction Specialist, San Francisco Department of the Environment (Part 2 of 2)
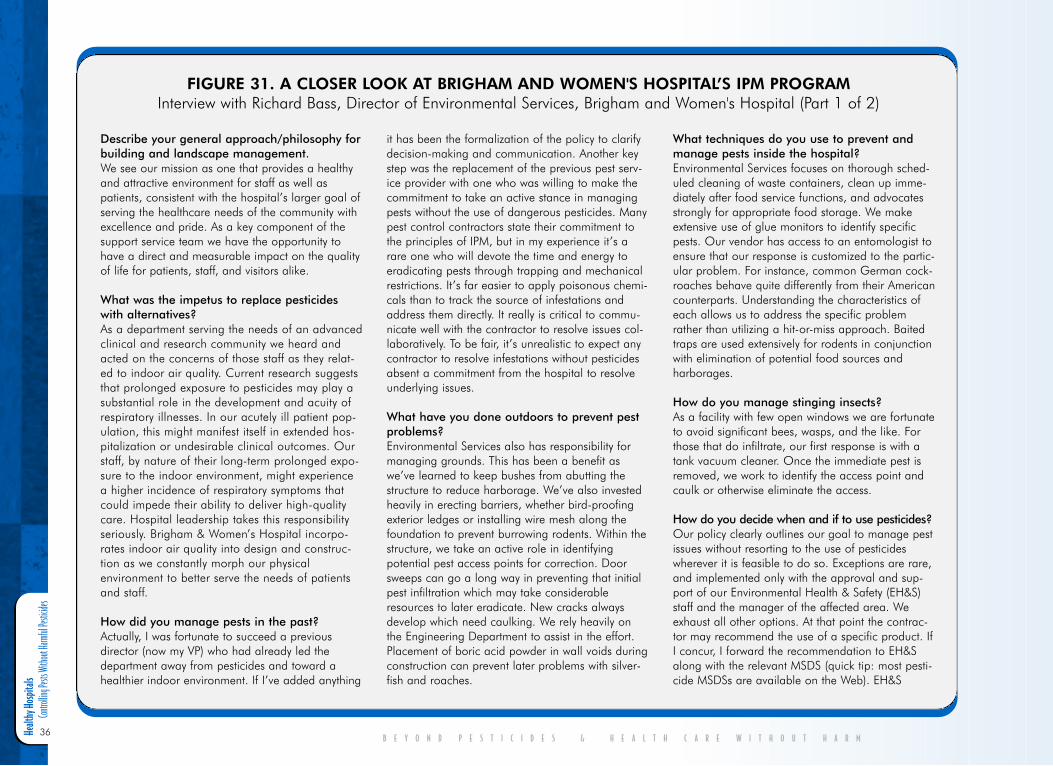
Healt
hy Ho
spita
ls
Contro
lling P
ests W
ithout
Harm
ful Pe
sticide
s
36B E Y O N D P E S T I C I D E S & H E A L T H C A R E W I T H O U T H A R M
Describe your general approach/philosophy forbuilding and landscape management.We see our mission as one that provides a healthyand attractive environment for staff as well aspatients, consistent with the hospital’s larger goal ofserving the healthcare needs of the community withexcellence and pride. As a key component of thesupport service team we have the opportunity tohave a direct and measurable impact on the qualityof life for patients, staff, and visitors alike.
What was the impetus to replace pesticideswith alternatives?As a department serving the needs of an advancedclinical and research community we heard andacted on the concerns of those staff as they relat-ed to indoor air quality. Current research suggeststhat prolonged exposure to pesticides may play asubstantial role in the development and acuity ofrespiratory illnesses. In our acutely ill patient pop-ulation, this might manifest itself in extended hos-pitalization or undesirable clinical outcomes. Ourstaff, by nature of their long-term prolonged expo-sure to the indoor environment, might experiencea higher incidence of respiratory symptoms thatcould impede their ability to deliver high-qualitycare. Hospital leadership takes this responsibilityseriously. Brigham & Women’s Hospital incorpo-rates indoor air quality into design and construc-tion as we constantly morph our physicalenvironment to better serve the needs of patientsand staff.
How did you manage pests in the past?Actually, I was fortunate to succeed a previousdirector (now my VP) who had already led thedepartment away from pesticides and toward ahealthier indoor environment. If I’ve added anything
it has been the formalization of the policy to clarifydecision-making and communication. Another keystep was the replacement of the previous pest serv-ice provider with one who was willing to make thecommitment to take an active stance in managingpests without the use of dangerous pesticides. Manypest control contractors state their commitment tothe principles of IPM, but in my experience it’s arare one who will devote the time and energy toeradicating pests through trapping and mechanicalrestrictions. It’s far easier to apply poisonous chemi-cals than to track the source of infestations andaddress them directly. It really is critical to commu-nicate well with the contractor to resolve issues col-laboratively. To be fair, it’s unrealistic to expect anycontractor to resolve infestations without pesticidesabsent a commitment from the hospital to resolveunderlying issues.
What have you done outdoors to prevent pestproblems?Environmental Services also has responsibility formanaging grounds. This has been a benefit aswe’ve learned to keep bushes from abutting thestructure to reduce harborage. We’ve also investedheavily in erecting barriers, whether bird-proofingexterior ledges or installing wire mesh along thefoundation to prevent burrowing rodents. Within thestructure, we take an active role in identifyingpotential pest access points for correction. Doorsweeps can go a long way in preventing that initialpest infiltration which may take considerableresources to later eradicate. New cracks alwaysdevelop which need caulking. We rely heavily onthe Engineering Department to assist in the effort.Placement of boric acid powder in wall voids duringconstruction can prevent later problems with silver-fish and roaches.
What techniques do you use to prevent andmanage pests inside the hospital?Environmental Services focuses on thorough sched-uled cleaning of waste containers, clean up imme-diately after food service functions, and advocatesstrongly for appropriate food storage. We makeextensive use of glue monitors to identify specificpests. Our vendor has access to an entomologist toensure that our response is customized to the partic-ular problem. For instance, common German cock-roaches behave quite differently from their Americancounterparts. Understanding the characteristics ofeach allows us to address the specific problemrather than utilizing a hit-or-miss approach. Baitedtraps are used extensively for rodents in conjunctionwith elimination of potential food sources andharborages.
How do you manage stinging insects?As a facility with few open windows we are fortunateto avoid significant bees, wasps, and the like. Forthose that do infiltrate, our first response is with atank vacuum cleaner. Once the immediate pest isremoved, we work to identify the access point andcaulk or otherwise eliminate the access.
How do you decide when and if to use pesticides?Our policy clearly outlines our goal to manage pestissues without resorting to the use of pesticideswherever it is feasible to do so. Exceptions are rare,and implemented only with the approval and sup-port of our Environmental Health & Safety (EH&S)staff and the manager of the affected area. Weexhaust all other options. At that point the contrac-tor may recommend the use of a specific product. IfI concur, I forward the recommendation to EH&Salong with the relevant MSDS (quick tip: most pesti-cide MSDSs are available on the Web). EH&S
FIGURE 31. A CLOSER LOOK AT BRIGHAM AND WOMEN'S HOSPITAL’S IPM PROGRAMInterview with Richard Bass, Director of Environmental Services, Brigham and Women's Hospital (Part 1 of 2)
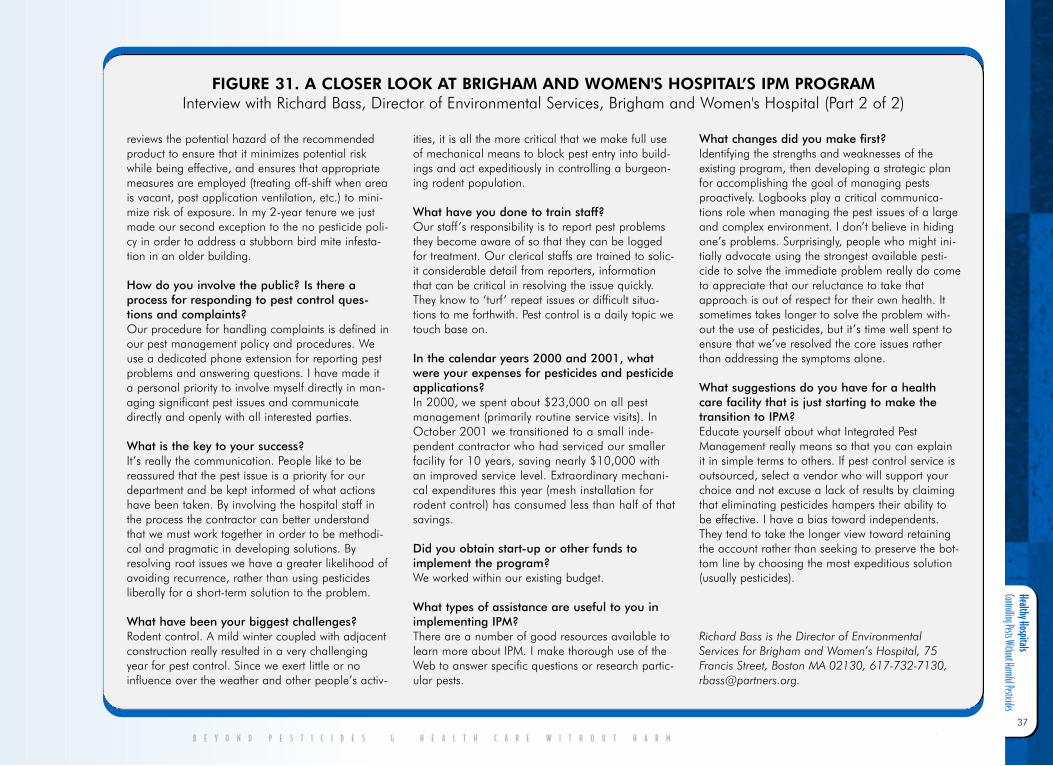
Healthy Hospitals Controlling Pests Without Harmful Pesticides
37
B E Y O N D P E S T I C I D E S & H E A L T H C A R E W I T H O U T H A R M
reviews the potential hazard of the recommendedproduct to ensure that it minimizes potential riskwhile being effective, and ensures that appropriatemeasures are employed (treating off-shift when areais vacant, post application ventilation, etc.) to mini-mize risk of exposure. In my 2-year tenure we justmade our second exception to the no pesticide poli-cy in order to address a stubborn bird mite infesta-tion in an older building.
How do you involve the public? Is there aprocess for responding to pest control ques-tions and complaints?Our procedure for handling complaints is defined inour pest management policy and procedures. Weuse a dedicated phone extension for reporting pestproblems and answering questions. I have made ita personal priority to involve myself directly in man-aging significant pest issues and communicatedirectly and openly with all interested parties.
What is the key to your success?It’s really the communication. People like to bereassured that the pest issue is a priority for ourdepartment and be kept informed of what actionshave been taken. By involving the hospital staff inthe process the contractor can better understandthat we must work together in order to be methodi-cal and pragmatic in developing solutions. Byresolving root issues we have a greater likelihood ofavoiding recurrence, rather than using pesticidesliberally for a short-term solution to the problem.
What have been your biggest challenges?Rodent control. A mild winter coupled with adjacentconstruction really resulted in a very challengingyear for pest control. Since we exert little or noinfluence over the weather and other people’s activ-
ities, it is all the more critical that we make full useof mechanical means to block pest entry into build-ings and act expeditiously in controlling a burgeon-ing rodent population.
What have you done to train staff?Our staff’s responsibility is to report pest problemsthey become aware of so that they can be loggedfor treatment. Our clerical staffs are trained to solic-it considerable detail from reporters, informationthat can be critical in resolving the issue quickly.They know to ‘turf’ repeat issues or difficult situa-tions to me forthwith. Pest control is a daily topic wetouch base on.
In the calendar years 2000 and 2001, whatwere your expenses for pesticides and pesticideapplications?In 2000, we spent about $23,000 on all pestmanagement (primarily routine service visits). InOctober 2001 we transitioned to a small inde-pendent contractor who had serviced our smallerfacility for 10 years, saving nearly $10,000 withan improved service level. Extraordinary mechani-cal expenditures this year (mesh installation forrodent control) has consumed less than half of thatsavings.
Did you obtain start-up or other funds toimplement the program?We worked within our existing budget.
What types of assistance are useful to you inimplementing IPM?There are a number of good resources available tolearn more about IPM. I make thorough use of theWeb to answer specific questions or research partic-ular pests.
What changes did you make first?Identifying the strengths and weaknesses of theexisting program, then developing a strategic planfor accomplishing the goal of managing pestsproactively. Logbooks play a critical communica-tions role when managing the pest issues of a largeand complex environment. I don’t believe in hidingone’s problems. Surprisingly, people who might ini-tially advocate using the strongest available pesti-cide to solve the immediate problem really do cometo appreciate that our reluctance to take thatapproach is out of respect for their own health. Itsometimes takes longer to solve the problem with-out the use of pesticides, but it’s time well spent toensure that we’ve resolved the core issues ratherthan addressing the symptoms alone.
What suggestions do you have for a healthcare facility that is just starting to make thetransition to IPM?Educate yourself about what Integrated PestManagement really means so that you can explainit in simple terms to others. If pest control service isoutsourced, select a vendor who will support yourchoice and not excuse a lack of results by claimingthat eliminating pesticides hampers their ability tobe effective. I have a bias toward independents.They tend to take the longer view toward retainingthe account rather than seeking to preserve the bot-tom line by choosing the most expeditious solution(usually pesticides).
Richard Bass is the Director of EnvironmentalServices for Brigham and Women’s Hospital, 75Francis Street, Boston MA 02130, 617-732-7130,[email protected].
FIGURE 31. A CLOSER LOOK AT BRIGHAM AND WOMEN'S HOSPITAL’S IPM PROGRAMInterview with Richard Bass, Director of Environmental Services, Brigham and Women's Hospital (Part 2 of 2)
Healt
hy Ho
spita
ls
Contro
lling P
ests W
ithout
Harm
ful Pe
sticide
s
38
IV. Conclusion andR e c o m m e n d a t i o n sInadequacies in federal laws have resulted inthe availability of pesticide products withknown adverse human health and environmen-tal effects. With approximately 320 activeingredients in 1,600 pesticide products regis-tered for hospital use by EPA,131 this isespecially of concern. Hospitals are meant to beplaces of health and healing. Their strategies forcontrolling pest populations must protect hos-pital occupants from the hazards of pesticidesas well as pests.
From the hospital survey results reported, it isapparent that many hospitals control their pestproblems with hazardous pesticides; often donot notify their staff, patients or the publicabout pesticide applications; and, do not edu-cate their staff or others on the negative healthconsequences associated with many pesticides.These practices put staff, patients, and otherhospital occupants at an unacceptable risk forpesticide injury.
Fortunately, an IPM program can safeguardthe hospital community against harm frompests while simultaneously protecting it fromthe hazards of pesticides. The survey findingsshow that some hospitals have already imple-mented IPM programs. Yet, the results alsosuggest that the majority of U.S. hospitals havean urgent need to adopt safer pest manage-ment practices.
Beyond Pesticides and Health Care WithoutHarm acknowledge health institutions’ para-mount concern for the health of their staff,patients, and the public. With good informa-tion and proper tools, health institutions canadopt safer pest management practices in orderto reduce their patients and staff ’s exposure tohazardous chemicals. Hospitals have a specialobligation to protect their patients and to leadthe way in modeling safe and effective pestmanagement. Adopting an integrated pestmanagement program helps health careproviders to live up to their code to “First, dono harm.”
RecommendationsHospitals, government entities, the public, andthe pest management industry can all takeaction to increase the number of hospitalsadopting least hazardous IPM programs andproviding pesticide use notification.
Health care facilities should:
● Develop an IPM policy and guidancematerials that contain a strong and cleardefinition of IPM that includes the keyelements outlined in this report.
● Implement an IPM program that selectsthe least hazardous pesticides only afternon-toxic methods of pest control havebeen tried and found ineffective. If hospi-tal staff implements pest management,provide staff with IPM education andtechnical training. If pest management isimplemented by a commercial applicator,have a clear written contract that includesthe IPM policy.
● Provide notification to the staff, patients,and other hospital occupants when pesti-
cides are used in the hospital building oron the hospital’s grounds.
● Provide prior notification of pesticidesused on hospital grounds to neighboringproperty owners or residents.
● Publicize the phone number and emailaddress for a contact person, ideally theIPM coordinator, who is able to answerquestions or provide additional informa-tion about the hospital’s pest manage-ment program and its pesticide use.
● Educate all hospital staff about the haz-ards of pesticides and the advantages andprinciples of IPM.
● Maintain pest management records for atleast seven years.
● Stay up-to-date on the registration statusof pesticides used at the hospital and onnew alternative pest management prod-ucts and methods.
● Establish additional guidelines to addressthe needs of patients and staff that aremore sensitive to pesticides, such as chil-dren, the elderly, those with compromisedimmune or nervous systems, people withasthma, allergies, and chemical sensitivi-ties or those undergoing chemotherapy.
● Report any incidents where a patient, vis-itor or hospital staff member is made sickby a pesticide used at the hospital to EPAand state health agencies.
● Provide pesticide-free areas for patientswho have a medical condition and/or dis-ability that makes them more susceptibleto becoming ill from pesticides.
● Work with the Joint Commission onAccreditation for HealthcareOrganizations (JCAHO) to develop,monitor, and support an Environment of
B E Y O N D P E S T I C I D E S & H E A L T H C A R E W I T H O U T H A R M

Healthy Hospitals Controlling Pests Without Harmful Pesticides
39
B E Y O N D P E S T I C I D E S & H E A L T H C A R E W I T H O U T H A R M
Care Standard that requires hospitals tohave a written IPM Plan that includes thekey elements outlined in this report.
Federal, state, and local government entitiesshould:
● Develop hospital IPM policy and guid-ance materials that contain a strong andclear definition of IPM that includes thekey elements outlined in this report.
● Pass legislation to require hospitals toadopt IPM policies and disclose pesticideuse to workers and the public throughposting, individual notification, and uponrequest.
● Develop an IPM training and certifica-tion process for commercial pest controloperators and hospital employees.Commercial operators without certifica-tion should not be eligible for hospitalcontracts.
● Prohibit the use of hazardous pesticides athospitals when less hazardous alternativepractices exist.
The public should:
● Advocate for the adoption of strong IPMprograms at hospitals.
● Inquire about the pest management ofhospital buildings and grounds in theircommunities.
● Advocate for public policies that promotesafer pest management practices andstrengthen restrictions on hazardous pesti-cides.
The pest management industry should:
● Become informed and acquire expertisein true least hazardous IPM.
● Expand the number of businesses thatprovide these IPM services.
● Disclose pest management practices andpesticide use to the public.
● Work for the adoption of industry-wideIPM standards for training and certifica-tion.
For more information, contact BeyondPesticides or Health Care Without Harm or seethe Resource List in the Appendix for a list oforganizations, IPM companies, and govern-ment contacts.
Healt
hy Ho
spita
ls
Contro
lling P
ests W
ithout
Harm
ful Pe
sticide
s
40
V . A p p e n d i x
Resource ListFor more information on pesticides and imple-menting a hospital IPM program, contact thefollowing organizations, consultants, govern-ment entities, and/or consult BeyondPesticides’ Safety Source for Pest Managementto find pest management companies that prac-tice IPM.
Beyond Pesticides701 E Street, SE, Suite 200Washington DC 20003202-543-5450 [email protected] www.beyondpesticides.org
Bio-Integral Resource CenterPO Box 7414Berkeley CA [email protected] www.birc.org
Californians for Pesticide Reform49 Powell Street, #530San Francisco CA [email protected]
Health Care Without Harm1755 S Street, NW, Suite 6BWashington DC [email protected]
International Pest Management Institute275 South 3rd Street, #312Burbank CA 91502818-843-8304 [email protected]
IPM Institute of North America1914 Rowley AvenueMadison WI [email protected]
National Center for Environmental Health Strategies1100 Rural AvenueVoorhees NJ [email protected]
National Pesticide Information CenterOregon State University333 WenigerCorvallis OR [email protected]://npic.orst.edu
Northwest Coalition for Alternatives to PesticidesPO Box 1393Eugene OR 97440-1393 541-344-5044 [email protected] www.pesticide.org
Pesticide Action Network North America49 Powell Street, Suite 500San Francisco CA [email protected] ● www.pesticideinfo.org
U.S. Environmental Protection AgencyOffice of Pesticide ProgramsAriel Rios Building1200 Pennsylvania Ave., NWMail Code 3213AWashington, DC 20460202-260-2090www.epa.gov/pesticides
Hospital IPM CompaniesThe Safety Source for Pest Management: ANational Directory of Least-toxic ServiceProviders at www.beyondpesticides.org/safe-tysource provides a list of pest managementcompanies that practice IPM. Companies arelisted in the directory because they have com-pleted the Beyond Pesticides questionnaire andindicate that they use one or more practicesand/or materials that Beyond Pesticides catego-rizes as “non-toxic” or “least-toxic.” Included inthe directory are the companies’ surveyresponses in their own words. Many of thecompanies in the directory operate businessesthat Beyond Pesticides considers “mixed opera-tions” because they may also use products thatare classified as “toxic.” As a customer, it isimportant to talk with the service providerabout the products that they use, learn abouttheir potential to cause adverse effects, anddecide what action is most appropriate for thepest problem needing to be addressed.
B E Y O N D P E S T I C I D E S & H E A L T H C A R E W I T H O U T H A R M
Healthy Hospitals Controlling Pests Without Harmful Pesticides
41
B E Y O N D P E S T I C I D E S & H E A L T H C A R E W I T H O U T H A R M
Model Hospital Integrated PestManagement (IPM) Policy*
Section 1. Policy Goals. (a) To manage pests in a manner that will
not harm humans or the environment.
(b) To reduce or eliminate the use of toxicpesticides.
(c) To provide ample notification to the hos-pital community in the event that a haz-ardous pesticide product is applied.
Section 2. General.The requirements of this policy apply to hospi-tal buildings and grounds. This policy shallapply to any person that applies a pesticide orengages in other pest control activities in abuilding or on the grounds, including a custo-dian, staff member, or commercial applicator.All individuals that apply a pesticide must belicensed by the state.
Section 3. Director of Environmental Services.The Director of Environmental Services, orother appropriate staff person, is responsible fordeveloping and overseeing the implementationof the integrated pest management (IPM) pro-gram. The Director shall designate a contactperson for inquiries about the IPM program;maintain Material Safety Data Sheets (MSDSs)and labels for all pesticides which may be usedinside or outside the facilities; maintain sched-uling of all pest monitoring and pesticideusage; stay up-to-date on new IPM materialsand methods; obtain periodic updates andtraining from IPM experts; on request makethe hospital’s pest management and pesticideuse data available to the public for review; and,present an annual report to the Board, CEO, or
other appropriate administrator evaluating theprogress of the integrated pest managementprogram. The Director is also responsible forcoordinating the training of individuals thatimplement the IPM program.
Section 4. Integrated Pest Management.Integrated pest management is an approach topest control that eliminates or mitigates eco-nomic and health damage caused by pests,while minimizing or eliminating the use of pes-ticides and their risk to human health and theenvironment. IPM involves site or pest inspec-tions; pest population monitoring; and theevaluation of the need for action. The primarycontrol methods focus on pest prevention andinclude improving sanitation, making structur-al repairs, and using mechanical, physical,cultural, and biological controls. A least haz-ardous pesticide is only applied if non-toxicmethods have been ineffective or are not appro-priate.
Each pest control technician, whether a hospi-tal employee or outside contractor, isresponsible for documenting a pest problem,actions taken to correct the problem and theiroutcomes, and findings relevant to the sourceof the infestation. The pest control technicianshall fill out a Service Report Form, which shallbe kept in a logbook at the hospital’sEnvironmental Services Department. A log-book shall be kept in a central location andshall be used to document the pest control pro-gram. The hospital staff and/or pest controltechnician shall report the presence of pests ina timely manner.
Section 5. Pesticide Notification.Not less than 72 hours before a pesticide isapplied in a hospital building or on hospital
grounds, the Director shall provide to each staffmember and patient that is expected to beresiding in the area to be treated, written noticeof the proposed pesticide application. TheDirector shall pre-notify abutting propertyowners, if a pesticide application will be madeon the hospital’s lawn or landscape. Noticeshall include the brand name, active ingredient,and U.S. Environmental Protection Agencyregistration number of the pesticide to be used;a description of the location where the pesticidewill be applied; a description of the date andtime of application, except that, in the case ofoutdoor pesticide applications, each noticeshall include three dates, in chronologicalorder, that the outdoor pesticide applicationsmay take place if the preceding date is canceleddue to weather; the target pest and descriptionof potential adverse effects of the pesticidebased on the label or MSDS for the pesticide; adescription of the reasons for the application ofthe pesticide; the application method; theapplicator’s name and company; the name andtelephone number of whom to contact formore information; and any additional warninginformation related to the pesticide.
At least 72 hours before a pesticide is used at ahospital facility, the pest control applicatorshall post a sign that provides notice of theapplication of the pesticide in a prominentplace that is in or adjacent to the location to betreated and at each entrance to the building orgrounds to be treated. Signs shall contain thesame information as written notices and remainin place during the pesticide application andfor at least 72 hours afterwards.
Healt
hy Ho
spita
ls
Contro
lling P
ests W
ithout
Harm
ful Pe
sticide
s
42
Section 6. Emergency Pesticide Use.If a hospital applies a pesticide due to an emer-gency, care shall be taken to make sure the areais unoccupied prior to the pesticide applicationand notification shall be provided to all staffand patients expected to be residing near thetreated area within 72 hours after an applica-tion takes place. A sign that meets therequirements under Section 5 shall be postedwarning of the pesticide application no laterthan the time the application commences.
Section 7. Hospital Pesticide Use. The following are prohibited (except when apest problem causes an urgent threat to health):
(a) The use of the most dangerous pesticides:
(1) Pesticides in U.S. EPA Categories Iand II (i.e., those with highest acutetoxicity);
(2) Pesticides linked to cancer — U.S.EPA Class A, B, C carcinogens<www.epa.gov/pesticides/carlist/index.html> and chemicals known to thestate of California to cause cancerunder Proposition 65<www.oehha.org/prop65/prop65_list/Newlist.html>;
(3) Pesticides that interfere with humanhormones and/or cause birth defectsor reproductive or developmentalharm, e.g., those identified as repro-ductive or developmental toxins orsuspected endocrine disruptors<www.pesticideinfo.org> or chemi-cals known to California to be repro-ductive toxins under Proposition 65<www.oehha.org/prop65/prop65_list/Newlist.html>;
(4) Pesticides in the carbamate (carbaryl,bendiocarb, etc.), organophosphate
(diazinon, acephate, etc.) orpyrethroid (cyfluthrin, permethrin,etc.) chemical family and phenoxyherbicides (2,4-D, mecoprop, etc.);and,
(5) Pesticide products that contain inertingredients categorized by the U.S.EPA as “List 1: Inerts ofToxicological Concern” (dioctylphthalate, formaldehyde, hydro-quinone, isophorone, nonylphenol,phenol, and rhodamine B)
(b) Pest management decisions based on aes-thetics alone.
(c) The application of pesticides on a routinebasis, whether pests are present or not.
(d) The application of pesticides while thearea is occupied or may become occupiedduring the 24 hours following the appli-cation.
(e) The application of pesticides by fogging,bombs, or tenting or by space, broadcast,or baseboard spraying.
Section 8. Record Keeping.(a) Written or electronic records shall be kept
of all pest monitoring data, including thepresence or absence of pests, factors con-tributing to pest infestations, interven-tions, and their outcomes.
(b) Written or electronic records of all pesti-cide applications made at the hospitalfacility shall be maintained on site for aperiod of not less than seven years, andshall be made available to the publicupon request. The record shall be com-pleted on the day of the pesticide applica-tion, and shall include, but is not limitedto the:
(1) target pest and reason for the appli-cation(s);
(2) date and time of the application;
(3) application area;
(4) brand name and active ingredients ofthe pesticide product;
(5) name of the pesticide manufacturer;
(6) U.S EPA registration number;
(7) method of application and quantityof pesticide used;
(8) least hazardous and non-chemicalalternative methods or treatmentsthat were tried and/or unavailable toaccomplish the desired objectives andthe reasons why the application ofthe proposed pesticide was chosen;
(9) possible adverse health effects tohumans as stated on the label orMSDS; and,
(10) name, address, and phone numberof the individual who applied thepesticide.
Section 9. Reporting.The Director shall annually review its IPM pro-gram to evaluate its effectiveness and to identifyareas where improvement is needed. The reportshall be submitted to the hospital’s Board,CEO, or other appropriate administrator andmade available to the staff and public uponrequest.
*This document is for educational purposes onlyand does not constitute legal or health advice.Health care providers and institutions should seeklegal and medical advice to ensure that pest man-agement programs meet legal and patient careresponsibilities, including compliance with appli-cable pesticide notification laws and regulations.
B E Y O N D P E S T I C I D E S & H E A L T H C A R E W I T H O U T H A R M
Healthy Hospitals Controlling Pests Without Harmful Pesticides
43
B E Y O N D P E S T I C I D E S & H E A L T H C A R E W I T H O U T H A R M
Cover Letter and Survey
Dear Facilities Manager:
As you may be aware, Health Care Without Harm: The Campaign for Environmentally Responsible Health Care (HCWH)
is an international coalition composed of over 340 member-organizations in 36 countries. These members include health
care systems, organizations of health professionals, labor, environmental groups, religious organizations and health-advoca-
cy groups. The mission of HCWH is to transform the health care industry so that it is no longer a source of environmental
harm, without compromising safety or care.
HCWH has assisted numerous medical facilities in reducing their dioxin and mercury emissions. Now we are expanding
our focus to help hospitals reduce their pesticide use and find less-toxic ways to manage pests within and outside their build-
ings. This is desirable because exposures to many commonly used pesticides can cause wheezing, vomiting, diarrhea,
headache, seizures and other serious health problems. Pesticides are also increasingly being linked with a myriad of chronic
illnesses including cancer, asthma, birth defects, hormone disruption, learning disabilities, Parkinson’s disease and multiple
chemical sensitivities.
Before HCWH can work with hospitals on their pest management, we must first gain a better understanding of what pes-
ticide products are currently being used. Enclosed you will find a survey of pest control practices and pesticides use that
HCWH is distributing to the top 171 hospitals in the United States (as determined by U.S. NEWS & WORLD REPORT,
2001). The purpose of this survey is to determine which pesticides are being used in the nation’s hospitals. A member of
HCWH will be contacting you to see if you need help with the survey. We will then work with interested hospitals to
develop or improve safer integrated pest management (IPM) programs for their facilities.
Aggregate data from the survey will also be used to write a report on the current state of pesticide use in U.S. hospitals.
Other than an appendix listing the 171 facilities on the U.S. News list, no hospital names will be mentioned in the report
except those hospitals demonstrating best-practices pest management techniques and/or model IPM programs. All hospitals
that complete a survey will automatically receive a copy of the report. Other hospitals can obtain a copy by visiting our web-
site, www.noharm.org.
Thank you for taking the time to complete this survey. We look forward to continuing our work with hospitals to make
them as environmentally safe as possible.
Sincerely,
Catherine Porter, Co-Chair, Health-Affected Work Group, Health Care Without Harm
Healt
hy Ho
spita
ls
Contro
lling P
ests W
ithout
Harm
ful Pe
sticide
s
44
P e s t i c i d e U s e S u r v e yPlease complete and return to HCWH by January 15, 2002
Date survey was completed: _______________________________________________________________________________________________
Name of hospital: ______________________________________________________________________________________________________
Address: ______________________________________________________________________________________________________________
Main information phone number: __________________________________________________________________________________________
Name of person completing survey: _________________________________________________________________________________________
Job title: ______________________________________________________________________________________________________________
Direct phone: __________________________________________________________________________________________________________
Hospital type: ❏ Non-profit ❏ Urban ❏ For-profit ❏ Suburban ❏ Rural
Number of beds: ______________________ Affiliated with a university? Y N
Specialty: ❏ General ❏ Children’s ❏ Women’s ❏ Cancer ❏ Eye ❏ Rehabilitation/Orthopedic ❏ Other
Part IFor each question below, circle the response that best fits the situation at your facility.
1. Does your facility use chemical pesticide products inside the hospital? Y N
2. Does your facility use chemical pesticide products on hospital grounds? Y N
3. Are Material Safety Data Sheets (MSDS) on file and available to hospital staff for all pesticides used in your hospital or on hospital grounds? Y N
4. Are hospital staff members given training on the health effects of pesticides? Y N
5. Do you post warning signs when pesticides are used in the hospital? Y N No pesticides used
6. Do you post warning signs when pesticides are used on hospital grounds? Y N No pesticides used
B E Y O N D P E S T I C I D E S & H E A L T H C A R E W I T H O U T H A R M
Healthy Hospitals Controlling Pests Without Harmful Pesticides
45
B E Y O N D P E S T I C I D E S & H E A L T H C A R E W I T H O U T H A R M
7. Do you provide other forms of notification to staff, patients, or others when pesticides are used in the hospital? Y N No pesticides used
If “yes” to #7, please describe the forms of notification and to whom they are directed (e.g., table tents in hospital cafeteria to inform hospital staff about monthly roach spraying):
_____________________________________________________________________________________________________________
_____________________________________________________________________________________________________________
8. Do you provide other forms of notification to staff, patients, or others when pesticides are used on hospital grounds? Y N No pesticides used
If “yes” to #8, please describe the forms of notification and to whom they are directed
_______________________________________________________________________________________________________________
_______________________________________________________________________________________________________________
9. Does anyone keep records of pesticides used in the hospital? Y N No pesticides used
10. If yes, who keeps the records? (Title/position of record keeper)
_______________________________________________________________________________________________________________
11. If records are kept by a contractor, are copies also kept at the hospital? Y N
12. Does anyone keep records of pesticides used on hospital grounds? Y N No pesticides used
13. If yes, who keeps the records? (Title/position of record keeper)
_______________________________________________________________________________________________________________
14. If records are kept by a contractor, are copies also kept at the hospital? Y N
15. What percentage of your pest management is handled by outside contractors? _____ % indoors ______% outdoors
16. What percentage of your pest management is handled by staff/employees? _____ % indoors ______% outdoors
17. Does your hospital have a written pest management plan? Y N Don’t know
18. Does your hospital use an integrated pest management (IPM) approach to pest management? Y N Don’t know
19. What is the approximate cost per year for your hospital’s pest management? $______________________
Healt
hy Ho
spita
ls
Contro
lling P
ests W
ithout
Harm
ful Pe
sticide
s
46
Part IIPlease use the following chart to list all chemical pesticide products (excluding disinfectants) used in your hospital or on its grounds in the past year. “Pesticides” refer to products usedto kill or repel pests (e.g., insects, rodents, birds, weeds). Please attach additional sheets if necessary.
1 Please list each pesticide product applied in your hospital or on its grounds in the last year.2 Active ingredients can be found on the product labels. 3 Identify the indoor and outdoor area(s) where this pesticide was applied (e.g., cafeteria, patient room(s), building perimeter, lawn, shrubs). 4 Identify the method of pesticide application (e.g., spray, granules, fog, bait). 5 Identify the frequency of application to each area (e.g., weekly, monthly, twice a year) and whether the applications were made on a regular calendar basis or only as needed based upon pest populations.
Part IIIIn the space below (or as an attachment), please add any comments or information that you would like to share about how your hospital manages pests.
____________________________________________________________________________________________________________________________________
____________________________________________________________________________________________________________________________________
____________________________________________________________________________________________________________________________________
____________________________________________________________________________________________________________________________________
Thank you for your cooperation in completing this survey. Please return the completed form to Health Care Without Harm, 1755 “S” St NW, Suite 6B, Washington,DC 20009 or fax to 202-234-9121 by January 15, 2002.
B E Y O N D P E S T I C I D E S & H E A L T H C A R E W I T H O U T H A R M
Brand name & EPA registration #1
Example:Tempo 20 WPEPA #3125-380
Active ingredient(s)2
Cyfluthrin
Areas treated3
CafeteriaLoading dockBuilding perimeter
Method of application4
SpraySpraySpray
Frequency of application & whetherapplied regularly or as-needed5
Monthly (regular)Every 3 mos. (as needed)Monthly (regular)
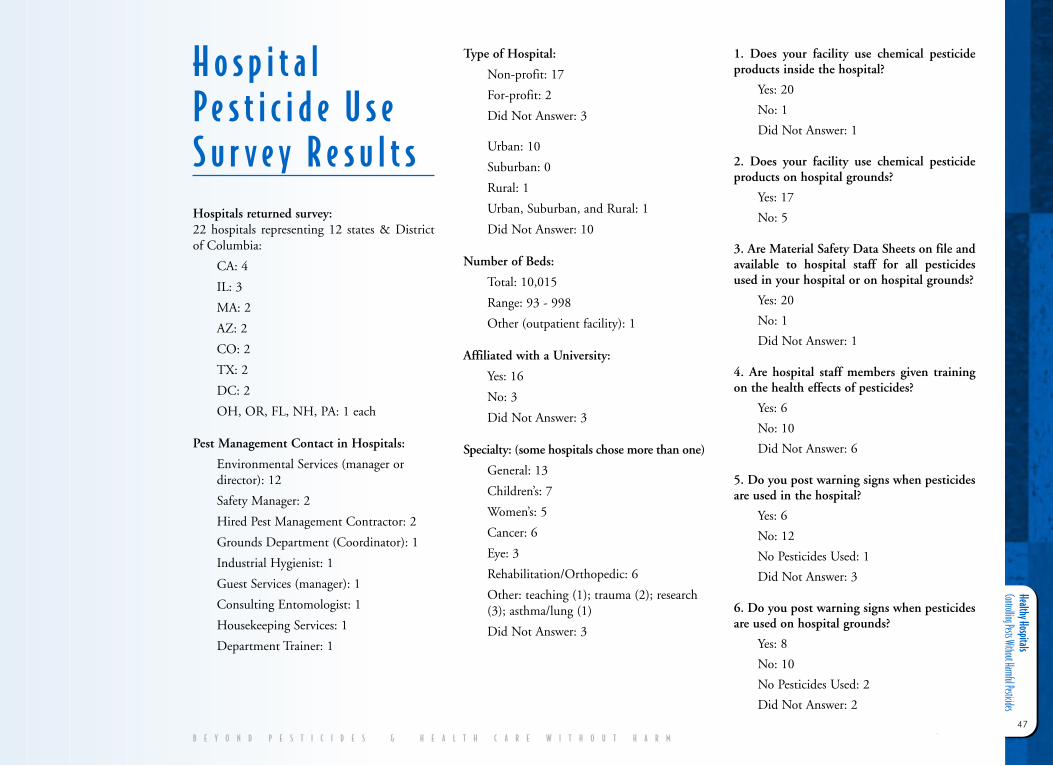
Healthy Hospitals Controlling Pests Without Harmful Pesticides
47
B E Y O N D P E S T I C I D E S & H E A L T H C A R E W I T H O U T H A R M
H o s p i t a lP e s t i c i d e U s eS u r v e y R e s u l t sHospitals returned survey: 22 hospitals representing 12 states & Districtof Columbia:
CA: 4
IL: 3
MA: 2
AZ: 2
CO: 2
TX: 2
DC: 2
OH, OR, FL, NH, PA: 1 each
Pest Management Contact in Hospitals:
Environmental Services (manager ordirector): 12
Safety Manager: 2
Hired Pest Management Contractor: 2
Grounds Department (Coordinator): 1
Industrial Hygienist: 1
Guest Services (manager): 1
Consulting Entomologist: 1
Housekeeping Services: 1
Department Trainer: 1
Type of Hospital:
Non-profit: 17
For-profit: 2
Did Not Answer: 3
Urban: 10
Suburban: 0
Rural: 1
Urban, Suburban, and Rural: 1
Did Not Answer: 10
Number of Beds:
Total: 10,015
Range: 93 - 998
Other (outpatient facility): 1
Affiliated with a University:
Yes: 16
No: 3
Did Not Answer: 3
Specialty: (some hospitals chose more than one)
General: 13
Children’s: 7
Women’s: 5
Cancer: 6
Eye: 3
Rehabilitation/Orthopedic: 6
Other: teaching (1); trauma (2); research(3); asthma/lung (1)
Did Not Answer: 3
1. Does your facility use chemical pesticideproducts inside the hospital?
Yes: 20
No: 1
Did Not Answer: 1
2. Does your facility use chemical pesticideproducts on hospital grounds?
Yes: 17
No: 5
3. Are Material Safety Data Sheets on file andavailable to hospital staff for all pesticidesused in your hospital or on hospital grounds?
Yes: 20
No: 1
Did Not Answer: 1
4. Are hospital staff members given trainingon the health effects of pesticides?
Yes: 6
No: 10
Did Not Answer: 6
5. Do you post warning signs when pesticidesare used in the hospital?
Yes: 6
No: 12
No Pesticides Used: 1
Did Not Answer: 3
6. Do you post warning signs when pesticidesare used on hospital grounds?
Yes: 8
No: 10
No Pesticides Used: 2
Did Not Answer: 2
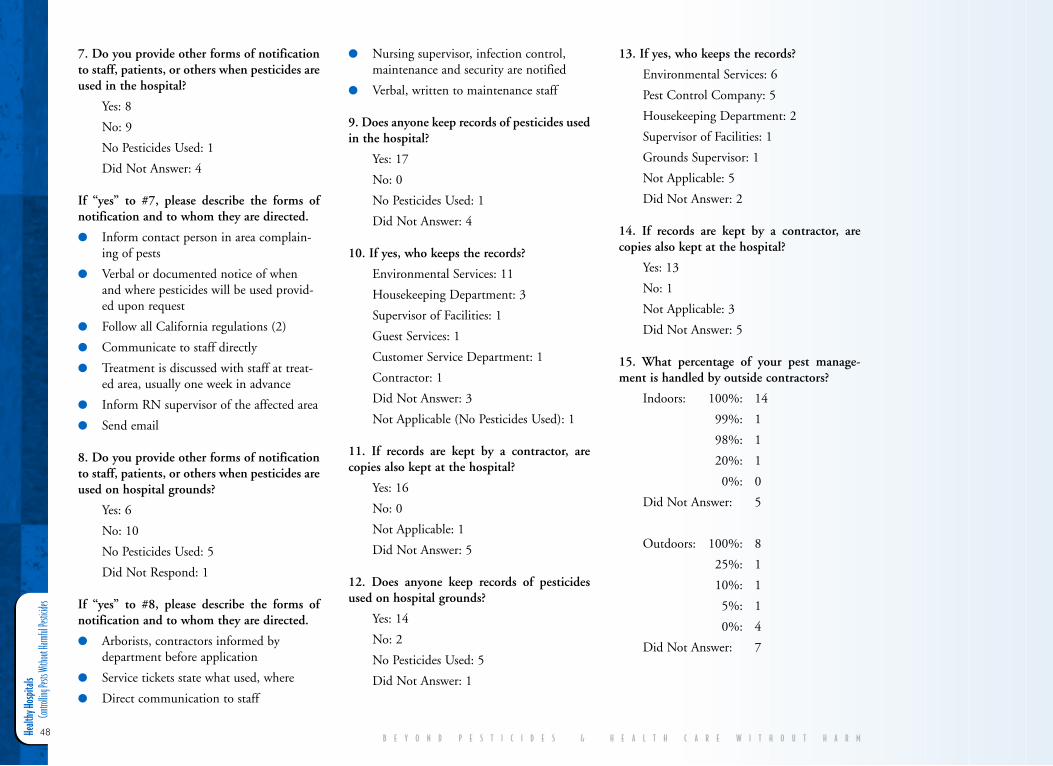
Healt
hy Ho
spita
ls
Contro
lling P
ests W
ithout
Harm
ful Pe
sticide
s
48
7. Do you provide other forms of notificationto staff, patients, or others when pesticides areused in the hospital?
Yes: 8
No: 9
No Pesticides Used: 1
Did Not Answer: 4
If “yes” to #7, please describe the forms ofnotification and to whom they are directed.
● Inform contact person in area complain-ing of pests
● Verbal or documented notice of whenand where pesticides will be used provid-ed upon request
● Follow all California regulations (2)
● Communicate to staff directly
● Treatment is discussed with staff at treat-ed area, usually one week in advance
● Inform RN supervisor of the affected area
● Send email
8. Do you provide other forms of notificationto staff, patients, or others when pesticides areused on hospital grounds?
Yes: 6
No: 10
No Pesticides Used: 5
Did Not Respond: 1
If “yes” to #8, please describe the forms ofnotification and to whom they are directed.
● Arborists, contractors informed bydepartment before application
● Service tickets state what used, where
● Direct communication to staff
● Nursing supervisor, infection control,maintenance and security are notified
● Verbal, written to maintenance staff
9. Does anyone keep records of pesticides usedin the hospital?
Yes: 17
No: 0
No Pesticides Used: 1
Did Not Answer: 4
10. If yes, who keeps the records?
Environmental Services: 11
Housekeeping Department: 3
Supervisor of Facilities: 1
Guest Services: 1
Customer Service Department: 1
Contractor: 1
Did Not Answer: 3
Not Applicable (No Pesticides Used): 1
11. If records are kept by a contractor, arecopies also kept at the hospital?
Yes: 16
No: 0
Not Applicable: 1
Did Not Answer: 5
12. Does anyone keep records of pesticidesused on hospital grounds?
Yes: 14
No: 2
No Pesticides Used: 5
Did Not Answer: 1
13. If yes, who keeps the records?
Environmental Services: 6
Pest Control Company: 5
Housekeeping Department: 2
Supervisor of Facilities: 1
Grounds Supervisor: 1
Not Applicable: 5
Did Not Answer: 2
14. If records are kept by a contractor, arecopies also kept at the hospital?
Yes: 13
No: 1
Not Applicable: 3
Did Not Answer: 5
15. What percentage of your pest manage-ment is handled by outside contractors?
Indoors: 100%: 14
99%: 1
98%: 1
20%: 1
0%: 0
Did Not Answer: 5
Outdoors: 100%: 8
25%: 1
10%: 1
5%: 1
0%: 4
Did Not Answer: 7
B E Y O N D P E S T I C I D E S & H E A L T H C A R E W I T H O U T H A R M
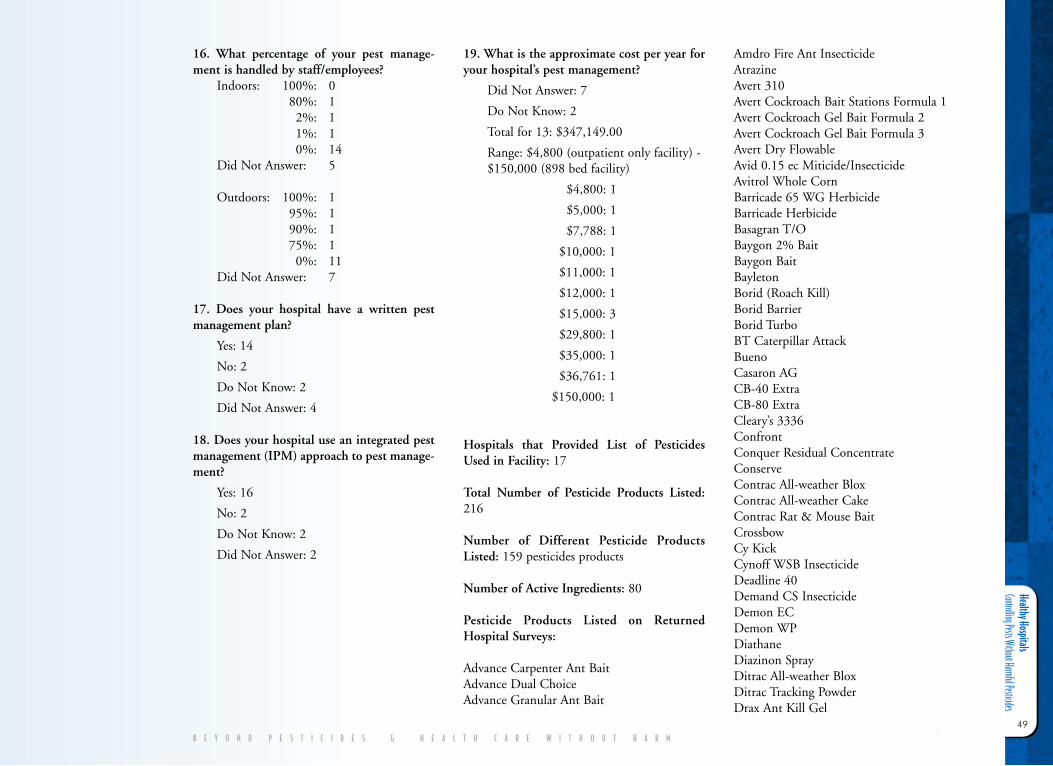
Healthy Hospitals Controlling Pests Without Harmful Pesticides
49
B E Y O N D P E S T I C I D E S & H E A L T H C A R E W I T H O U T H A R M
16. What percentage of your pest manage-ment is handled by staff/employees?
Indoors: 100%: 080%: 12%: 11%: 10%: 14
Did Not Answer: 5
Outdoors: 100%: 195%: 190%: 175%: 10%: 11
Did Not Answer: 7
17. Does your hospital have a written pestmanagement plan?
Yes: 14
No: 2
Do Not Know: 2
Did Not Answer: 4
18. Does your hospital use an integrated pestmanagement (IPM) approach to pest manage-ment?
Yes: 16
No: 2
Do Not Know: 2
Did Not Answer: 2
19. What is the approximate cost per year foryour hospital’s pest management?
Did Not Answer: 7
Do Not Know: 2
Total for 13: $347,149.00
Range: $4,800 (outpatient only facility) -$150,000 (898 bed facility)
$4,800: 1
$5,000: 1
$7,788: 1
$10,000: 1
$11,000: 1
$12,000: 1
$15,000: 3
$29,800: 1
$35,000: 1
$36,761: 1
$150,000: 1
Hospitals that Provided List of PesticidesUsed in Facility: 17
Total Number of Pesticide Products Listed:216
Number of Different Pesticide ProductsListed: 159 pesticides products
Number of Active Ingredients: 80
Pesticide Products Listed on ReturnedHospital Surveys:
Advance Carpenter Ant BaitAdvance Dual ChoiceAdvance Granular Ant Bait
Amdro Fire Ant InsecticideAtrazineAvert 310Avert Cockroach Bait Stations Formula 1Avert Cockroach Gel Bait Formula 2Avert Cockroach Gel Bait Formula 3Avert Dry FlowableAvid 0.15 ec Miticide/InsecticideAvitrol Whole CornBarricade 65 WG HerbicideBarricade HerbicideBasagran T/OBaygon 2% BaitBaygon BaitBayletonBorid (Roach Kill)Borid BarrierBorid TurboBT Caterpillar AttackBueno Casaron AGCB-40 ExtraCB-80 ExtraCleary’s 3336ConfrontConquer Residual ConcentrateConserveContrac All-weather BloxContrac All-weather CakeContrac Rat & Mouse BaitCrossbowCy KickCynoff WSB InsecticideDeadline 40 Demand CS InsecticideDemon ECDemon WPDiathaneDiazinon SprayDitrac All-weather BloxDitrac Tracking PowderDrax Ant Kill Gel
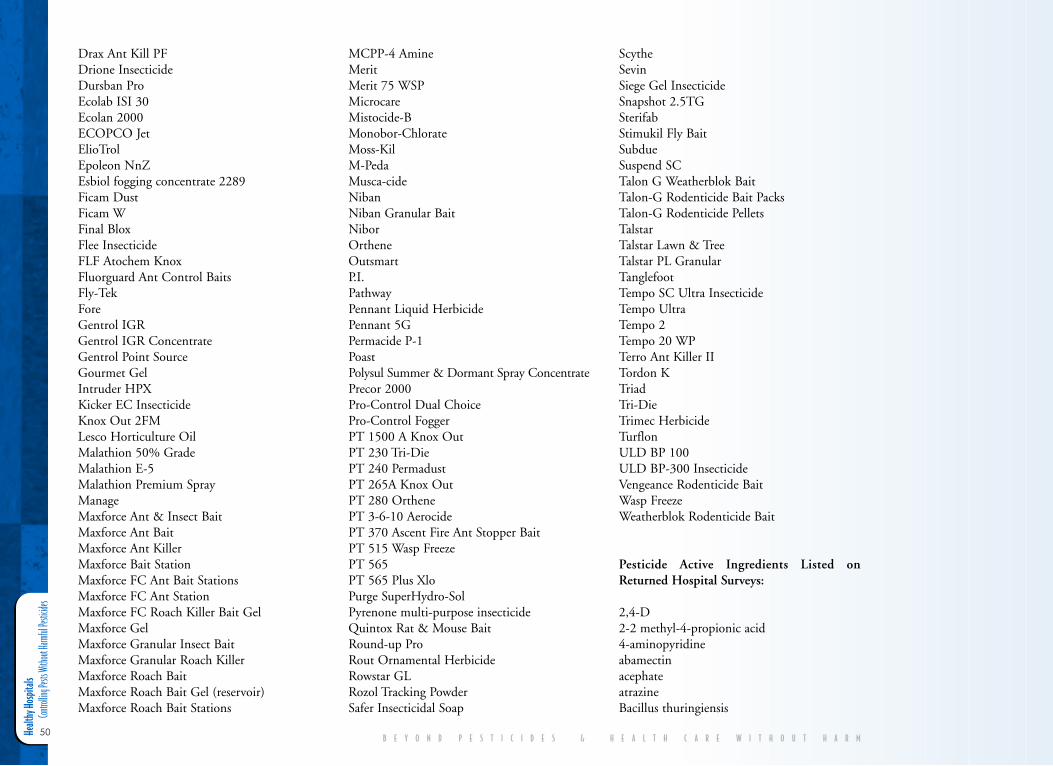
Healt
hy Ho
spita
ls
Contro
lling P
ests W
ithout
Harm
ful Pe
sticide
s
50
Drax Ant Kill PFDrione InsecticideDursban ProEcolab ISI 30Ecolan 2000 ECOPCO JetElioTrolEpoleon NnZEsbiol fogging concentrate 2289Ficam DustFicam WFinal BloxFlee InsecticideFLF Atochem KnoxFluorguard Ant Control BaitsFly-TekForeGentrol IGRGentrol IGR ConcentrateGentrol Point SourceGourmet GelIntruder HPXKicker EC InsecticideKnox Out 2FMLesco Horticulture OilMalathion 50% GradeMalathion E-5Malathion Premium SprayManageMaxforce Ant & Insect BaitMaxforce Ant BaitMaxforce Ant KillerMaxforce Bait StationMaxforce FC Ant Bait StationsMaxforce FC Ant StationMaxforce FC Roach Killer Bait GelMaxforce GelMaxforce Granular Insect BaitMaxforce Granular Roach KillerMaxforce Roach BaitMaxforce Roach Bait Gel (reservoir)Maxforce Roach Bait Stations
MCPP-4 AmineMerit Merit 75 WSPMicrocare Mistocide-BMonobor-ChlorateMoss-KilM-PedaMusca-cideNibanNiban Granular BaitNiborOrthene OutsmartP.I.PathwayPennant Liquid HerbicidePennant 5GPermacide P-1PoastPolysul Summer & Dormant Spray ConcentratePrecor 2000 Pro-Control Dual ChoicePro-Control FoggerPT 1500 A Knox Out PT 230 Tri-DiePT 240 PermadustPT 265A Knox OutPT 280 OrthenePT 3-6-10 AerocidePT 370 Ascent Fire Ant Stopper BaitPT 515 Wasp FreezePT 565 PT 565 Plus XloPurge SuperHydro-SolPyrenone multi-purpose insecticide Quintox Rat & Mouse BaitRound-up ProRout Ornamental HerbicideRowstar GLRozol Tracking PowderSafer Insecticidal Soap
ScytheSevinSiege Gel InsecticideSnapshot 2.5TGSterifabStimukil Fly BaitSubdueSuspend SCTalon G Weatherblok BaitTalon-G Rodenticide Bait PacksTalon-G Rodenticide PelletsTalstarTalstar Lawn & TreeTalstar PL GranularTanglefootTempo SC Ultra InsecticideTempo UltraTempo 2Tempo 20 WPTerro Ant Killer IITordon KTriadTri-DieTrimec HerbicideTurflonULD BP 100ULD BP-300 InsecticideVengeance Rodenticide Bait Wasp FreezeWeatherblok Rodenticide Bait
Pesticide Active Ingredients Listed onReturned Hospital Surveys:
2,4-D2-2 methyl-4-propionic acid4-aminopyridineabamectinacephateatrazineBacillus thuringiensis
B E Y O N D P E S T I C I D E S & H E A L T H C A R E W I T H O U T H A R M
Healthy Hospitals Controlling Pests Without Harmful Pesticides
51
B E Y O N D P E S T I C I D E S & H E A L T H C A R E W I T H O U T H A R M
bendiocarbbifenthrinboraxboric acidbrodifacoumbromadiolonebromethalincalcium polysulfidecarbarylchlorophacinone-liphadionechlorpyrifoscholecalciferolclopyralidcyfluthrincypermethrindeltamethrindiazinondicambadichlobenildiphacinonedisodium octaborate tetrahydrated-trans allethrinesfenvalerateeugenolfipronilglyphosatehalosulfuron-methylhydramethylnonhydropreneimidaclopridisoxaben lambda-cyhalothrinmalathionmancozebmecopropmefenoxammetaldehydemethomylmethoprenemetolachlorMSMA (monosodium acid methane arsonate)muscalure
n-octyl bicycloheptene dicarboximideortho-benzyl-para-chlorophenoloryzalinoxadiazonoxyflurfenpelargonic acidpermethrinpetroleum hydrocarbonphenothrinphenylethyl propionatepiclorampiperonyl butoxidepolybutenespotassium salts of fatty acidsprodiaminepropoxurpyrethrin refined petroleum oils-bioallethrinsethoxydimsilica gelsodium chloratesodium salt of bentazonspinosadsulfuramidthiophanate methyltriadimefontriclopyrtrifluralin(z)-9-tricosenezinc chloride
Healt
hy Ho
spita
ls
Contro
lling P
ests W
ithout
Harm
ful Pe
sticide
s
52
V I . E N D N O T E S1. Department of Veterans Affairs. 1986. Pest Management Operations,
Chapter 2. Environmental Management Service. February 3. p.5.
2. American Medical Association, Council on Scientific Affairs. 1997.“Educational and Informational Strategies to Reduce Pesticide Risks.”Prevention Magazine 26:191-200. < http://www.ama-assn.org/ama/pub/article/2036-2492.html>.
3. American Hospital Association. 2001. Fast Facts on U.S. Hospitals fromHospital StatisticsTM. Chicago, IL.
4. CDC. 2002. “Hospital Utilization.” National Center for Health Statistics.Center for Disease Control and Prevention. U.S. Department of Healthand Human Services. Hyattsville, MD.
5. Vacco, D. 1995. Pest Management in New York State Hospitals: RiskReduction and Health Promotion. Attorney General of New York State.New York State Department of Law. December 5; Duerhing, C. 1996.The Healthy Hospital Part Two: Pesticide Risks and Alternatives. Medical andLegal Briefs 2(1) July/August.
6. U.S. EPA. 2002. What is a Pesticide? Office of Pesticide Programs.<http://www.epa.gov/opp00001/whatis.htm>.
7. Reigart, J., et al. 1999. Recognition and Management of PesticidePoisonings. 5th edition. Office of Prevention, Pesticides and ToxicSubstances. U.S. EPA. 735-R-98-003; National Environmental Educationand Training Foundation. 2002. National Strategies for Health CareProviders: Pesticides Initiative Implementation Plan. Washington, DC.<http://www.neetf.org/pubs/NEETFImplement.pdf>.
8. Aspelin, A. et al. 1999. Pesticide Industry Sales and Usage: 1996 and 1997Market Estimates. Office of Prevention, Pesticides and Toxic Substances,U.S. EPA. 733-R-99-001. Washington DC.
9. Murray, Linda. 2002. Personal Communication. Communications Office.Office of Pesticide Programs. U.S. EPA. Washington DC. This numberincludes all active pesticides, including germicides and antimicrobials.
10. U.S. EPA. 2003. Label Review Manual Chapter 6: Ingredient Statement.Office of Pesticide Programs.<http://www.epa.gov/oppfod01/labeling/lrm/chap-06.htm>.
11. National Pesticide Telecommunications Network. 2000. PiperonylButoxide Technical Fact Sheet. U.S. EPA and Oregon State University.<http://ace.orst.edu/info/npic/factsheets/pbotech.pdf>
12. Extension Toxicology Network. 1996. DCPA, Chlorthal, Chlorthal-dimethyl. Pesticide Information Profiles. Oregon State University and U.S. EPA. <http://ace.orst.edu/info/extoxnet/pips/DCPA.htm>; Garabrant,
D, et al. 2002. “Review of 2,4-Dichlorophenoxyacetic Acid (2,4-D)Epidemiology and Toxicology.” Critical Reviews in Toxicology 32(4): 233-257; U.S. EPA. 1994. Estimating Exposure to Dioxin-like Compounds,Volume 11: Properties, sources, occurrence and background exposures.Review Draft. Office of Research and Development. Washington DC ascited in Cox, C. 1999. “2,4-D: Toxicology, Part 2.” Journal of PesticideReform 19(2): 14-19; Cornell University. 1983. Chemical Fact Sheet forDicamba. <pmep.cce.cornell.edu/profiles/herb-growthreg/dalapon-ethep-hon/ dicamba/herb-prof-dicamba.html>; Briggs. S. 1992. Basic Guide toPesticides: Their Characteristics and Hazards. Rachel Carson Council. SilverSpring, MD.
13. Reigart, J., et al. 1999; Box S. et al. 1996. “A Systemic Reaction FollowingExposure To a Pyrethroid Insecticide.” Human and Experimental Toxicology15:389-90; Underner, et al. 1987. “Occupational Asthma in the RuralEnvironment.” Rev Pneumonol Clin 43:26-35; Weiner, A. 1961.“Bronchial Asthma Due To The Organic Phosphate Insecticides.” Annalsof Allergy 15: 211-212; Wagner, S. 2000. “Fatal Asthma In A Child AfterUse of An Animal Shampoo Containing Pyrethrin.” Western Journal ofMedicine 173:86-87; Field, M. 2002. “Asthma the Breathtaking Disease.”Johns Hopkins Public Health. Spring. <http://www.jhsph.edu/Magazine/Asthma.html>; Eskenazi, B., et al. 1999. “Exposures of Children toOrganophosphate Pesticides and Their Potential Adverse Health Effects.”Environmental Health Perspectives 107(Supp 3): 409-419; Senthilselvan, A.,et al. 1992. “Association of Asthma With Use of Pesticides: Results of across-sectional survey of farmers.” American Review of Respiratory Disease146:884-887.
14. Blondell, J., et al. 1997. Review of Chlorpyrifos Poisoning DataMemorandum. Office of Prevention, Pesticides and Toxic Substances. U.S.EPA. Washington, DC; Abou-Donia, M., et al. 1990. “Mechanisms ofOrganophophorus Ester-induced Delayed Neurotoxicity: type I and typeII.” Annual Review of Pharmacology and Toxicology 30: 405-440; Reigert, J.1999; Ashford, N., et al. 1998. Chemical Exposures, Low Levels and HighStakes. 2nd edition. Van Nostrand Reinhold. New York, NY.
15. Ashford, N., et al. 1998; Ziem, G., et al. 1997. “Profile of Patients withChemical Injury and Sensitivity.” Environmental Health Perspectives 105,Suppl. 3; Miller, C., et al. 1995. “Chemical Sensitivity Attributed toPesticide Exposure Versus Remodeling.” Archives of Environmental Health50(2); Guillette, E., et al. 1998. “An Anthropological Approach to theEvaluation of Preschool Children Exposed to Pesticides in Mexico.”Environmental Health Perspectives 106(6): 347-353; Schettler, T., et al.2000. “Known and Suspected Developmental Neurotoxicants.” In HarmsWay: Toxic Threats to Child Development. Greater Boston Physicians forSocial Responsibility. Cambridge, MA; Multigner, et al. “Contribution ofEnvironmental Factors to the Risk of Male Infertility.” HumanReproduction; Repetto, R., et al.1996. Pesticides and Immune System: The
B E Y O N D P E S T I C I D E S & H E A L T H C A R E W I T H O U T H A R M
Healthy Hospitals Controlling Pests Without Harmful Pesticides
53
B E Y O N D P E S T I C I D E S & H E A L T H C A R E W I T H O U T H A R M
Public Health Risk. World Resources Institute. Washington, DC; Schettler,T., et al. 2000. Generations at Risk: Reproductive Health and theEnvironment. MIT Press. Cambridge, MA; Reigart, J., et al. 1999;Schubert, S., et al. 1996. Voices for Pesticide Reform: The Case for SafePractices and Sound Policy. Beyond Pesticides and Northwest Coalition forAlternatives to Pesticides. Washington, DC; Winrow, C., et al. 2003.“Loss of Neuropathy Target Esterase in Mice Links OrganophosphateExposure to Hyperactivity.” Nature Genetics <http://www.nature.com/cgi-taf/DynaPage.taf?file=/ng/journal/vaop/ncurrent/abs/ng1131.html>.
16. Blair, A., et al. 1992. “Clues to Cancer Etiology from Studies of Farmers.”Scandinavian Journal of Work, Environment and Health 18(4): 209-215;Wiklund, K., et al. 1995. “Cancer Risks Among Male Farmers inSweden.” European Journal of Cancer Prevention 4(1): 81-90; NationalResearch Council. 1993. Veterans and Agent Orange: Health Effects ofHerbicides Used in Vietnam. National Academy Press. Washington DC;Alavanja, M., et al. 2003. “National Cancer Institute, Use of AgriculturalPesticides and Prostate Cancer Risk in the Agricultural Health StudyCohort.” American Journal of Epidemiology 157(9): 800-14; Statement ofLeon F. Burmeister, Professor, Department of Preventive Medicine andEnvironmental Health, University of Iowa, before the Subcommittee onDepartment Operations, Research, and Foreign Agriculture, Committeeon Agriculture, U.S. House of Representatives, May 21, 1985.
17. Hoar, S., et al. 1986. “Agricultural Herbicide Use and a Risk ofLymphoma and Soft-Tissue Sarcoma.” Journal of the American MedicalAssociation 259(9): 1141-1147; Wigle, D., et al. 1990. “Mortality Study ofCanadian Farm Operators: Non-Hodgkin’s Lymphoma Mortality andAgricultural Practices in Saskatchewan.” Journal of the National CancerInstitute 82(7): 575-582; Woods, J. 1989. “Non-Hodgkin's LymphomaAmong Phenoxy Herbicide-Exposed Farm Workers in WesternWashington State.” Chemosphere 18(1-6): 401-406; Zahm, S., et al. 1990.“A Case Control Study of Non-Hodgkin’s Lymphoma on the Herbicide2,4-dichlorophenoxyacetic acid (2,4-D) in Eastern Nebraska.”Epidemiology 1(5): 349-356.
18. Ma, X. et al. 2002. “Critical Windows of Exposure to HouseholdPesticides and Risks of Childhood Leukemia.” Environmental HealthPerspectives 110(9): 955-960; Buckley, J. et al. 2000. “Pesticide Exposurein Children with non-Hodgkin Lymphoma.” Cancer 89(11): 2315-2321;Zahm, S. et al. 1998. “Pesticides and Childhood Cancer.” EnvironmentalHealth Perspectives 106(Supp. 3): 893-908; Gold, E., et al. 1979. “RiskFactors for Brain Tumors in Children.” American Journal of Epidemiology109(3): 309-319; Lowengart, R. et al. 1987. “Childhood Leukemia andParents’ Occupational and Home Exposures.” Journal of the NationalCancer Institute 79:39; Reeves, J.D. 1982. “Household Insecticide-Associated Blood Dyscrasias in Children” (letter). American Journal ofPediatric Hematology/Oncology 4:438-439; Davis, J.R., et al. 1993. “Family
Pesticide Use and Childhood Brain Cancer.” Archives of EnvironmentalContamination and Toxicology 24:87-92; Leiss, J., et al. 1995. “HomePesticide Use and Childhood Cancer: A Case-Control Study.” AmericanJournal of Public Health 85:249-252.
19. Dalvi, P., et al. 2002. “Effect of Cytochrome P450 Inducers on theMetabolism and Toxicity of Thiram in Rats.” Veterinary and HumanToxicology 44(6); Agyeman, A., et al. 1998. “The Actions of the H2-block-er Cimetidine on the Toxicity and Biotransformation of thePhosphorothioate insecticide parathion.” Toxicology 128(3); Dayal, M., etal. 2003. “Effect of Pretreatment of Cytochrome P450 (P450) Modifierson Neurobehavioral Toxicity Induced by Deltamethrin.” Food andChemical Toxicology 41(3); Wu, H., et al. 1996. “Influence of Cimetidineon the Toxicity and Toxicokinetics of Diazinon in the Rat.” Human andExperimental Toxicology 15(5).
20. US EPA. 1996. Environmental Health Threats to Children. Office of theAdministrator. 175-F-96-001. September; National Research Council.1993. Pesticides in the Diets of Infants and Children. National Academy ofSciences. National Academy Press. Washington, DC; Calabrese, E. 1986.Age and Susceptibility to Toxic Substances. John Wiley & Sons; Repetto, R.,et al.1996. Pesticides and Immune System: The Public Health Risk. WorldResources Institute. Washington, DC; Whalen, M., et al. 2003.“Immunomodulation of Human Natural Killer Cell Cytotoxic Functionby Triazine and Carbamate Pesticides.” Chem Biol Interact 145(3): 311-9;Qiao, D., et al. 2001. “Developmental Neurotoxicity of ChlorpyrifosModeled in Vitro: Comparative Effects of Metabolites and OtherCholinesterase Inhibitors on DNA Synthesis in PC12 and C6 Cells.”Environmental Health Perspectives 109(9): 909-913; ; U.S. EPA. 2003.Aging Initiative: Protecting the Health of Older Americans.<http://www.epa.gov/aging>; U.S. EPA and U.S. Consumer ProductSafety Commission. 1995. The Inside Story: A Guide to Indoor AirQuality.” Office of Radiation and Indoor Air. Washington, DC. EPA 402-K-93-007; Paigen, B. 1986. “Children and Toxic Chemicals.” Journal ofPesticide Reform (Summer); Box S., et al. 1996; Underner, et al. 1987;Weiner, A. 1961; Reigart, J. et al. 1999; Wagner, S. 2000; Field, M.2002; Eskenazi, B., et al. 1999; Senthilselvan, A., et al. 1992; Hardman,J., et al. 1996. Goodman and Gilman’s The Pharmacological Basis ofTherapeutics. 9th ed. McGraw-Hill. New York, NY; Extension ToxicologyNetwork. 1994. Pyrethrins and Pyrethroids Pesticide Information Profiles.Oregon State University and U.S. EPA.<http://ace.orst.edu/info/extoxnet/pips/pyrethri.htm>; ExtensionToxicology Network. 1996. Malathion Pesticide Information Profiles.Oregon State University and U.S. EPA.<http://ace.orst.edu/info/extoxnet/pips/malathio.htm>.
21. Bartha, L., et al. 1999. “Multiple Chemical Sensitivity: A 1999Consensus.” Archives of Environmental Health 54(3); McCampbell, A.
Healt
hy Ho
spita
ls
Contro
lling P
ests W
ithout
Harm
ful Pe
sticide
s
54
2002. “Pesticide Sensitivities.” Encyclopedia of Pest Management. DavidPimentel, Cornell University, editor. Marcel Dekker, Inc. New York. Pgs505-9; Dettelbach Pesticide Corporation. 1985 Orkinban PlusConcentrate Label. EPA Registration No. 6754-48; Rea, W., et al. 1992.Considerations for the Diagnosis of Chemical Sensitivity. MultipleChemical Sensitivities, Addendum to Biologic Markers in Immunotoxicology.National Research Council. National Academy Press. Washington, DC;Ziem, G. 1992. “Multiple Chemical Sensitivity: Treatment and Follow-upwith Avoidance and Control of Chemical Exposures.” Toxicology andIndustrial Health 8:73-86.
22. Reigart, R., et al. 1999; National Environmental Education and TrainingFoundation. 2002. National Strategies for Health Care Providers: PesticidesInitiative Implementation Plan. Washington DC.<http://www.neetf.org/pubs/NEETFImplement.pdf>.
23. National Environmental Education and Training Foundation. 2002.
24. People with chemical sensitivities have been reported to be made sick afterexposures to everyday chemicals like perfume, fresh paint, pesticides, newcarpets, tobacco smoke, vehicle exhaust, etc. Ziem, G., et al. 1997.
25. Birkey, E. 1997. Beyond Pesticides Pesticide Incident Record Form.Beyond Pesticides Pesticide Incident Record Database.
26. Anonymous. 2002. Beyond Pesticides Pesticide Incident Record Form.Beyond Pesticides Pesticide Incident Record Database.
27. Lamielle, M. 2002. Personal Communication. Voorhees, NJ.
28. U.S. EPA. 2003. List of Other (Inert) Pesticide Ingredients. Office ofPesticide Programs. <http://www.epa.gov/opprd001/inerts/lists.html>.
29. NCAP. 1998. Worst Kept Secrets: Toxic Inert Ingredients in Pesticides.Northwest Coalition for Alternatives to Pesticides. Eugene, OR.
30. Spitzer, E. 2000. The Secret Ingredients in Pesticides: Reducing the Risk.Office of New York State Attorney General. Environmental ProtectionBureau.
31. NCAP. 1998.
32. U.S. EPA. 2003. Inert Ingredients in Pesticide Products. Office ofPesticide Programs. <http://www.epa.gov/opprd001/inerts/>.
33. U.S. EPA. 1997. Pesticide Registration Notice 97-6. Use of Term “Inert”in the Label Ingredients Statement. Office of Pesticide Programs.<http://www.epa.gov/opppmsd1/PR_Notices/pr97-6.html>.
34. Gurunathan, S., et al. 1998. “Accumulation of Chlorpyrifos on ResidentialSurfaces and Toys Accessible to Children,” Environmental HealthPerspectives 106(1); Lewis, R., et al. 1991. “Determination of Routes ofExposure of Infants and Toddlers to Household Pesticides: A Pilot Study.”U.S. EPA. Methods of Research Branch. Research Triangle Park, NC.
35. Wright, C., et al. 1981. “Insecticides in the Ambient Air of RoomsFollowing Their Application for Control of Pests.” Bulletin ofEnvironmental Contamination & Toxicology, 26: 548-553.
36. U.S. EPA. 1990. “Nonoccupational Pesticide Exposure Study” (NOPES).Atmospheric Research and Exposure Assessment Laboratory. ResearchTriangle Park, NC. EPA/600/3-90/003.
37. Donaldson, D., et al. 2002. Pesticide Industry Sales and Usage Reports:1998-1999 Market Estimates. Biological and Economic Analysis Division.Office of Pesticide Programs. U.S. EPA.<http://www.epa.gov/oppbead1/pestsales/99pestsales/market_esti-mates1999.pdf>.
38. Nishioka, M., et al. 2001. “Distribution of 2,4-D in Air and on SurfacesInside Residences after Lawn Applications: Comparing Exposure Estimatesfrom Various Media for Young Children.” Environmental HealthPerspectives 109(11).
39. Pimentel, D. 1995. “Amounts of Pesticides Reaching Target Pests:Environmental Impacts and Ethics.” Journal of Agricultural andEnvironmental Ethics 8(1): 17-29.
40. U.S. EPA. 1999. Spray Drift of Pesticides. Office of Pesticide Programs.< http://www.epa.gov/pesticides/factsheets/spraydrift.htm>.
41. Owens, K., et al. 1999. “The Building of State Indoor Pesticide Policies.”Pesticides and You 18(4): 9-17.
42. CDC. 2003. National Report on Human Exposure to EnvironmentalChemicals. Centers for Disease Control and Prevention. National Centerfor Environmental Health. Atlanta, GA. <http://www.cdc.gov/exposurereport>.
43. Environmental Working Group. 2003. Body Burden: The Pollution InPeople. Washington, DC. <http://www.ewg.org/reports/bodyburden/>.
44. Alpert, G. 2002. Personal Communication. Harvard University.Massachusetts.
45. National Academy of Sciences. 1986. Pesticide Resistance: Strategies andTactics for Management. National Academy Press. Washington DC.
46. Donaldson, D., et al. 2002. <http://www.epa.gov/oppbead1/pestsales/99pestsales/usage1999_3.html#3_7>.
47. Extension Toxicology Network. 1996. Extoxnet Pesticide InformationProfile: 2,4-D. Oregon State University and U.S. EPA.<http://ace.orst.edu/info/extoxnet/pips/24-D.htm>.
48. Ibid.
49. Hoar, S. et al.1986; Zahm, S.H., et al. 1990.
50. Hayes, H., et al. 1991. “Case-Control Study of Canine MalignantLymphoma: Positive Association With Dog Owner’s Use of 2,4-
B E Y O N D P E S T I C I D E S & H E A L T H C A R E W I T H O U T H A R M
Healthy Hospitals Controlling Pests Without Harmful Pesticides
55
B E Y O N D P E S T I C I D E S & H E A L T H C A R E W I T H O U T H A R M
Dichlorophenoxyacetic Acid Herbicides.” Journal of the National CancerInstitute 83 (17): 1226-1231.
51. Garabrant, D, et al. 2002. “Review of 2,4-Dichlorophenoxyacetic Acid(2,4-D) Epidemiology and Toxicology.” Critical Reviews in Toxicology32(4): 233-257.
52. Health Care Without Harm. 2002. Dioxin, PVC, and Health CareInstitutions. Going Green Fact Sheet. <http://www.noharm.org/library/docs/Going_Green_3-1_Dioxin_PVC_and_Health_Care.pdf>.
53. Colborn, T., et al. 1993. “Developmental Effects of Endocrine DisruptingChemicals in Wildlife and Humans.” Environmental Health Perspectives101:378-384.
54. Rawlings, N., et al. 1998. “Effects of The Pesticides Carbofuran,Chlorpyrifos, Dimethoate, Lindane, Triallate, Trifluralin, 2,4-D andPentachlorphenol on the Metabolic Endocrine and ReproductiveEndocrine System in Ewes.” Journal of Toxicology and EnvironmentalHealth 54: 21-36.
55. Liu, R., et al. 1996. “The Direct Effect of Hepatic PeroxisomeProliferators on Rate Leydig Cell Function in Vitro.” Fundamentals ofApplied Toxicology 30: 102-108.
56. Munro, I., et al. 1992. “A Comprehensive, Integrated Review andEvaluation of the Scientific Evidence Relating to the Safety of theHerbicide 2,4-D.” Journal of the American College of Toxicology 5: 559-664.
57. Schreinemachers, D. 2003. “Birth Malformations and Other AdversePerinatal Outcomes in Four U.S. Wheat-Producing States.” EnvironmentalHealth Perspectives 111: 1259-1264; Gary, V., et al. 1996. “PesticideAppliers, Biocides, and Birth Defects in Rural Minnesota.” EnvironmentalHealth Perspectives 104: 394-399.
58. Information Ventures, Inc. under U.S. Forest Service Contract. 1995. 2,4-D Pesticide Fact Sheet. Prepared for the U.S. Department of Agriculture,Forest Service. < http://infoventures.com/e-hlth/pestcide/24d.html>.
59. Nishioka, M., et al. 2000. “Distribution of 2,4-D in Air and on SurfacesInside Residences After Lawn Applications: Comparing ExposureEstimates from Various Media for Young Children.” Environmental HealthPerspectives 109(11).
60. Nishioka, M., et al. 1996. “Measuring Transport of Lawn-AppliedHerbicide Acids from Turf to Home: Correlation of Dislodgeable 2,4-DTurf Residues with Carpet Dust and Carpet Surface Residues.”Environmental Science & Technology (30): 3313-3320.
61. Donaldson, D., et al. 2002.
62. Extension Toxicology Network. 1996. Pesticide Information Profiles:Glyphosate. <http://ace.orst.edu/cgi-bin/mfs/01/pips/glyphosa.htm>.
63. Reigart, J., et al. 1999; Sawada, Y., et al. 1988. “Probable Toxicity ofSurface-Active Agent In Commercial Herbicide Containing Glyphosate.”Lancet 1(8580): 299.
64. Sawada, Y. 1988.; Peluso, M., et al. 1998. “P-Post-labeling Detection ofDNA adducts in Mice Treated with the Herbicide Roundup”Environmental and Molecular Mutagenesis 31:55-59.
65. Cox, C. 1998. “Herbicide Fact Sheet: Glyphosate (Roundup).” Journal ofPesticide Reform 18(3): 4.
66. California Department of Pesticide Regulation. 1998. California PesticideIllness Surveillance Program Report- 1998. Table 4.<http://www.cdpr.ca.gov/docs/dprdocs/pisp/1998pisp.htm>.
67. Hardell, L., et al. 1999. “A Case Control Study of Non Hodgkin’sLymphoma and Exposure to Pesticides.” American Cancer Society.http://www.poptel.org.uk/panap/archives/nhl.htm#Note48; Hardell, L., etal. 2002. “Exposure to Pesticides as Risk Factor for Non-Hodgkin’sLymphoma and Hairy Cell Leukemia: Pooled Analysis of Two SwedishCase-Control Studies.” Leukemia and Lymphoma 43(5): 1043-9 .
68. Cox, C. 1998. “Glyphosate (Roundup) Herbicide Fact Sheet.” Journal ofPesticide Reform 18(3): 3-17. Updated April 2003.
69. Peluso, M., et al. 1998. “32-P-postlabeling Detection of DNA Adducts inMice Treated with the Herbicide Roundup.” Environmental and MolecularMutagenesis 31: 55-59.
70. National Pesticide Telecommunications Network. 2000. Acephate GeneralFact Sheet. Oregon State University and U.S. EPA.<http://ace.orst.edu/info/npic/npicfact.htm>.
71. U.S. EPA. 2002. List of Chemicals Evaluated for Carcinogenic Potential.Science Information Management Branch. Health Effects Division. Officeof Pesticide Programs. May 10. <http://www.epa.gov/pesticides/carlist/>.
72. National Pesticide Information Retrieval System. 1987. Acephate FactSheet No. 140. Purdue University.
73. Gosselin, R. 1984. Clinical Toxicology of Commercial Products. Williamsand Wilkins. Baltimore, MD.
74. National Pesticide Telecommunications Network. 1997. Permethrin. U.S.EPA and Oregon State University. <http://ace.orst.edu/info/npic/fact-sheets/permethrin.pdf>.
75. Reigart, J., et al. 1999.
76. Cantalamessa, F. 1993. “Acute Toxicity of Two Pyrethroids, Permethrinand Cypermethrin, in Neonatal and Adult Rats.” Archives of Toxicology 67:510-513.
77. Go, V., et al. 1999. “Estrogenic Potential of Certain PyrethroidCompounds in the MCF-7 Human Breast Carcinoma Cell Line.”Environmental Health Perspectives 107(3).
Healt
hy Ho
spita
ls
Contro
lling P
ests W
ithout
Harm
ful Pe
sticide
s
56
78. U.S. EPA. 2002. Chemicals Evaluated for Carcinogenic Potential.
79. Gosselin, R. 1984.
80. National Pesticide Telecommunications Network. 2000. PiperonylButoxide Technical Fact Sheet. Oregon State University and U.S. EPA. <http://ace.orst.edu/info/npic/factsheets/pbotech.pdf>; Kasai, S., et al.2000. “Overexpression of Cytochrome P450 CYP6D1 is Associated withMonooxygenase-Mediated Pyrethroid Resistance in House Flies fromGeorgia.” Pesticide Biochemistry and Physiology 68: 34-41.
81. Gosselin, R. 1984.
82. Ibid.
83. Takahashi, O., et al. 1994. “Chronic Toxicity Studies of PiperonylButoxide in F344 Rats: Induction of Hepatocellular Carcinoma.”Fundamentals of Applied Toxicology 22:293-303.
84. U.S. EPA. 2002. Chemicals Evaluated for Carcinogenic Potential.
85. U.S. General Accounting Office. 1997. Nonagricultural Pesticides: Risksand Regulation. GAO/RCED-86-97. Washington, DC.
86. U.S. EPA. 2000. Chlorpyrifos Revised Risk Assessment and Agreementwith Registrants. Washington, DC.
87. Keifer, M. (ed). 1997. “Human Health Effects of Pesticides.” OccupationalMedicine: State of the Art Reviews. Haley and Belfus, Inc. Philadelphia, PA.
88. Reigart, J., et al. 1999. p. 22.
89. 40 CFR 158. Code of Federal Regulations. Title 40, Chapter I, Part 158Data Requirements for Registration.<http://www.access.gpo.gov/nara/cfr/waisidx_02/40cfr158_02.html>.
90. Aspelin, A., et al. 1999. Pesticide Industry Sales and Usage: 1996 and 1997Market Estimates. Office of Prevention, Pesticides and Toxic Substances.U.S. EPA. 733-R-99-001. Washington DC. Page 2.
91. Shistar, T. 1990. The Benefit Side of Risk-Benefit Analysis. NationalCoalition Against the Misuse of Pesticides (Beyond Pesticides).Washington DC.
92. Vacco, D. 1995.
93. Sunseri, R. 1999. “Outsourcing on the Outs.” Hospitals and HealthNetworks. October.
94. Feldman, J. 1995. A Failure to Protect: The Unnecessary Use of HazardousPesticides at Federal Facilities Threatens Human Health and theEnvironment. National Coalition Against the Misuse of Pesticides (BeyondPesticides). Washington, DC.
96. U.S. EPA. 2002. Chemicals Evaluated for Carcinogenic Potential.
97. U.S. EPA. 2003. Restricted and Cancelled Uses. Office of PesticidePrograms. <http://www.epa.gov/pesticides/regulating/restricted.htm#can-celed>.
98. Each product was identified as “cancelled” by using the Pesticide ActionNetwork North America database, <http://www.pesticideinfo.org>.
99. U.S. EPA. 2001. Diazinon Revised Risk Assessment and Agreement withRegistrants. Office of Prevention, Pesticides and Toxic Substances.Washington DC.<http://www.epa.gov/oppsrrd1/op/diazinon/agreement/pdf>; U.S. EPA.1999. Reregistration Eligibility Document Facts: Bendiocarb. Office ofPrevention, Pesticides and Toxic Substances. Washington DC.<http://www.epa.gov/oppsrrd1/REDs/factsheets/0409fact.pdf>; U.S. EPA.2000. Chlorpyrifos Revised Risk Assessment and Agreement withRegistrants. Office of Prevention, Pesticides and Toxic Substances.Washington DC. <http://www.epa.gov/oppsrrd1/op/chlorpyrifos/agree-ment.pdf>.
100. Reigart, J., et al. 1999. p.22.
101. Beyond Pesticides. 2002. “Schools Save Money with Integrated PestManagement.” Pesticides and You 22(1): 18-19; Beyond Pesticides and theSchool Pesticide Reform Coalition. 2003. Safer Schools: Achieving AHealthy Learning Environment Through Integrated Pest Management.Washington DC. <www.beyondpesticides.org/schools/publications/IPMsuccessstories.pdf>.
102. 42CFR482.41. Code of Federal Regulations. Title 42, Volume 3. Revisedas of October 1, 2001. U.S. Government Printing Office via GPO Access.Page 502-503. <http://frwebgate.access.gpo.gov/cgi-bin/get-cfr.cgi>.
103. American Medical Association, Council on Scientific Affairs. 1997.
104. The National Parks Service, through its IPM program, has “reduced pesti-cide use by over 60 percent while improving the effectiveness of pestmanagement efforts.” National Park Service Integrated Pest ManagementManual. <http://www.colostate.edu/Depts/IPM/natparks/natpark>.
105. Owens, K, et al. 1999.
106. American Hospital Association. 2000. Certified Healthcare EnvironmentalServices Professional: Candidate Handbook. American Hospital AssociationCertification Center. Chicago, IL.
107. American Society for Healthcare Environmental Services. 2000. IntegratedPest Management (IPM). Professional Development Series. AmericanHospital Association. Catalogue No. 197107. June.
108. American Society for Healthcare Engineering. <http://www.hospitalcon-nect.com/ashe/recognition/sustainable.html>.
109. Hospitals for a Healthy Environment. 2002. <http://www.h2e-online.org/tols/chem-ipm.htm>.
B E Y O N D P E S T I C I D E S & H E A L T H C A R E W I T H O U T H A R M
Healthy Hospitals Controlling Pests Without Harmful Pesticides
57
B E Y O N D P E S T I C I D E S & H E A L T H C A R E W I T H O U T H A R M
110. Alpert, G. 2002.
111. Bass, R. Email communication. Director of Environmental Services.Brigham and Women’s Hospitals. Boston MA; Currie, B. 2003. Emailcommunication. International Pest Management Institute. Prescott, AZ.Ware, G. 1996. Complete Guide to Pest Control With and WithoutChemicals. Thomson Publications. Fresno, CA; Beyond Pesticides. 2002.Building Blocks for School IPM: A Least-toxic Pest Management Manual.Washington, DC.
112. Adapted from the Oregon Health and Science University Integrated PestManagement Policy. 2002.
113. Olkowski , D., et al. 1991. Common Sense Pest Control. Tauton Press.Newtown, CT.
114. Berstein L., et al. 1999. “Immune Responses in Farm Workers afterExposure to Bacillus thuringiensis Pesticides.” Environmental HealthPerspectives 107(7):575-82.
115. Alpert, G. 2002.
116. Owens, K, et al. 1999.
117. Beyond Pesticides. 2001. State Lawn Notification Laws: A BeyondPesticide Fact Sheet. Washington DC.
118. Vacco, D. 1995.
119. U.S. EPA. 1993. Pest Control in the School Environment: AdoptingIntegrated Pest Management. 735-F-93-012. Office of Pesticide Programs.Washington, DC.
120. Greene, A. 1993. “Integrated Pest Management for Buildings.” Pesticidesand You 13(2-3). Washington, DC.
121. Spitzer, E. 2000. Pesticide Use at New York Schools: Reducing the Risk.Office of the Attorney General. Environmental Protection Bureau citingCastronovo, P. 1999. Personal Communication. University of Rochester.April 9.
122. Spitzer, E. 2000. citing U.S. EPA. 1998. The City of Santa Monica’sEnvironmental Purchasing - A Case Study. Office of Pollution, Preventionand Toxics. EPA 742-R-98-001.
123. Carter, J. 2001. Personal Communication. Director of Planning. MonroeCounty Community School Corporation. Bloomington, IN.
124. Safer Pest Control Project. 1998. Cost of IPM in Schools. Chicago, IL.<http://www.spea.indiana.edu/pestmanagement/mccsc.html>.
125. Department of Veterans Affairs. 1986. Pest Management Operations.Environmental Management Service. Chapter 2, February 3.
126. Feldman, J., et al. 1995.
127. Quayle, C. 2000. “Battling Bugs: Pest Management Can Help You Winthe War.” Health Facilities Management. Health Forum, Inc. July.
128. Way, P. 2002. Email communication. Grounds Coordinator. OHSUFacilities Management and Construction, Grounds Department.
129. Pest Control Services. 2000. Pest Management at MGH. HarvardUniversity. <http://www.mgh.harvard.edu/depts/esd/pest.html>.
130. Premus, R. 2003. Email Communication. Director of EnvironmentalPrograms, The Deirdre Imus Environmental Center for PediatricOncology at Hackensack University Medical Center.
131. This number includes all active pesticides, including germicides andantimicrobials. Murray, Linda. 2002.
132. The data in this cgart reflects the author’s synthesis of two related surveyquestions that yielded some inconsistent responses.
133. Hospitals that have no apparent outdoor pest management program arethose that indicated they neither hire an outside contractor nor have in-house staff manage outdoor areas.

701 E Street, SE Suite 200Washington DC 20003
(202) [email protected]
1755 S Street , NW, Suite 6BWashington, DC 20009 U.S.A .
(202) [email protected]
www.noharm.org
Related Documents











