GLOBAL TB PROGRAMME Knut Lönnroth Global TB Programme, WHO Monitoring social protection Sickness insurance Food package Disability grants Other welfare grants Travel vouchers Mechanisms Outcomes Case detection % with catastrophic cost Treatment outcome Access to social protection interventions for TB patients Housing support Other cash transfer Situation assessment Monitoring of coverage and outcomes Job security

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
GLOBAL TB PROGRAMME
Knut Lönnroth
Global TB Programme, WHO
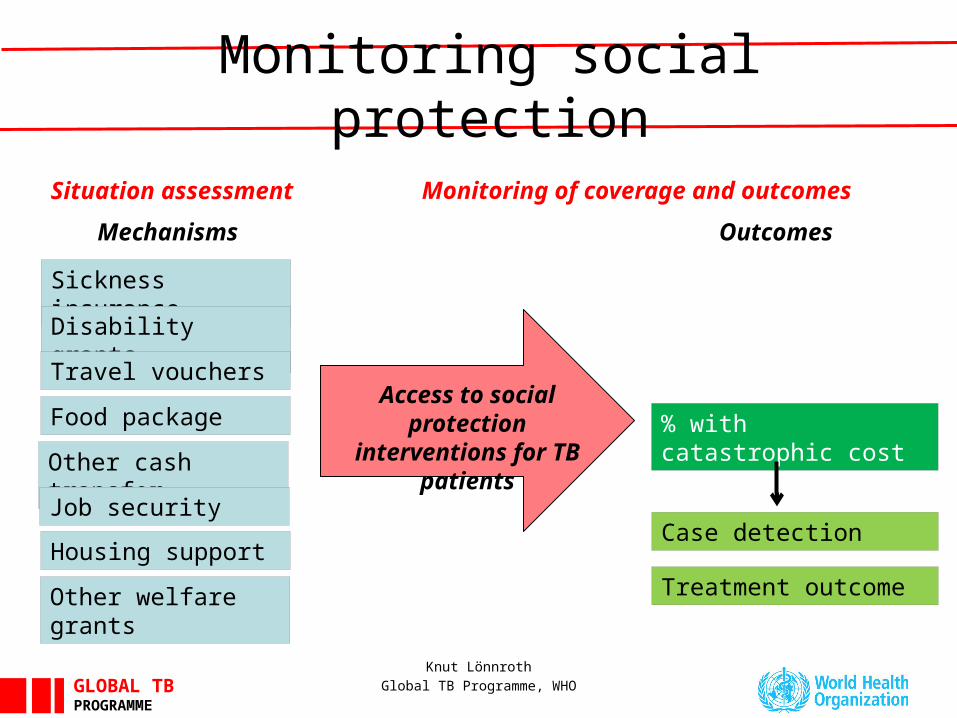
Monitoring social protection
Sickness insurance
Food package
Disability grants
Other welfare grants
Travel vouchers
Mechanisms Outcomes
Case detection
% with catastrophic cost
Treatment outcome
Access to social protection interventions
for TB patients
Housing support
Other cash transfer
Situation assessment Monitoring of coverage and outcomes
Job security
GLOBAL TB PROGRAMME
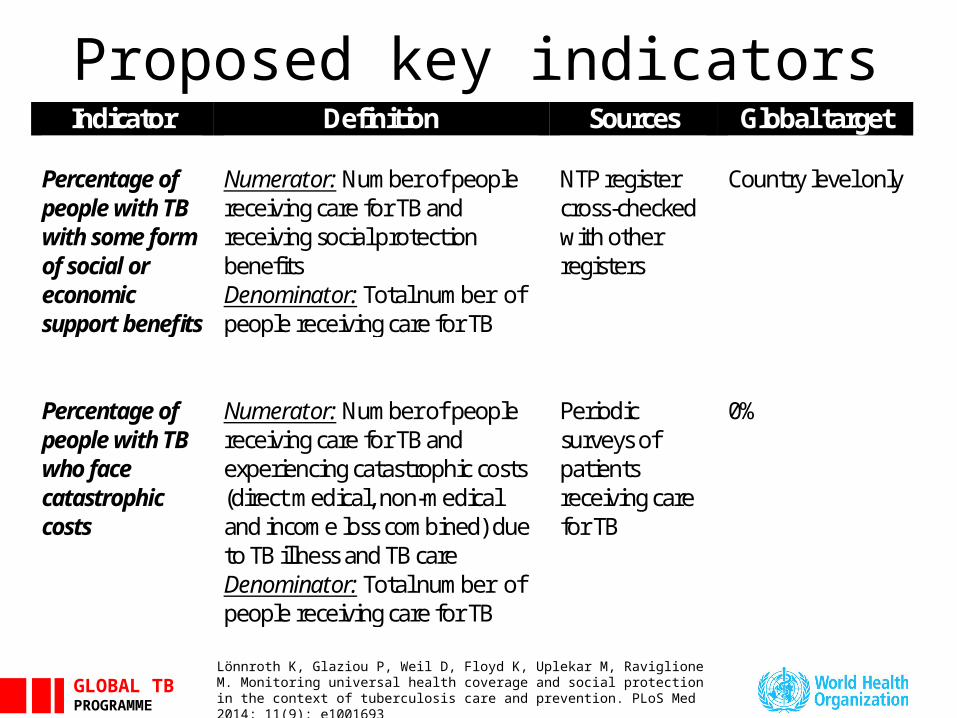
Proposed key indicatorsIndicator Definition Sources Global target
Percentage of people with TB with some form of social or economic support benefits
Numerator: Number of people receiving care for TB and receiving social protection benefits Denominator: Total number of people receiving care for TB
NTP register cross-checked with other registers
Country level only
Percentage of people with TB who face catastrophic costs
Numerator: Number of people receiving care for TB and experiencing catastrophic costs (direct medical, non-medical and income loss combined) due to TB illness and TB care Denominator: Total number of people receiving care for TB
Periodic surveys of patients receiving care for TB
0%
Lönnroth K, Glaziou P, Weil D, Floyd K, Uplekar M, Raviglione M. Monitoring universal health coverage and social protection in the context of tuberculosis care and prevention. PLoS Med 2014; 11(9): e1001693
GLOBAL TB PROGRAMME
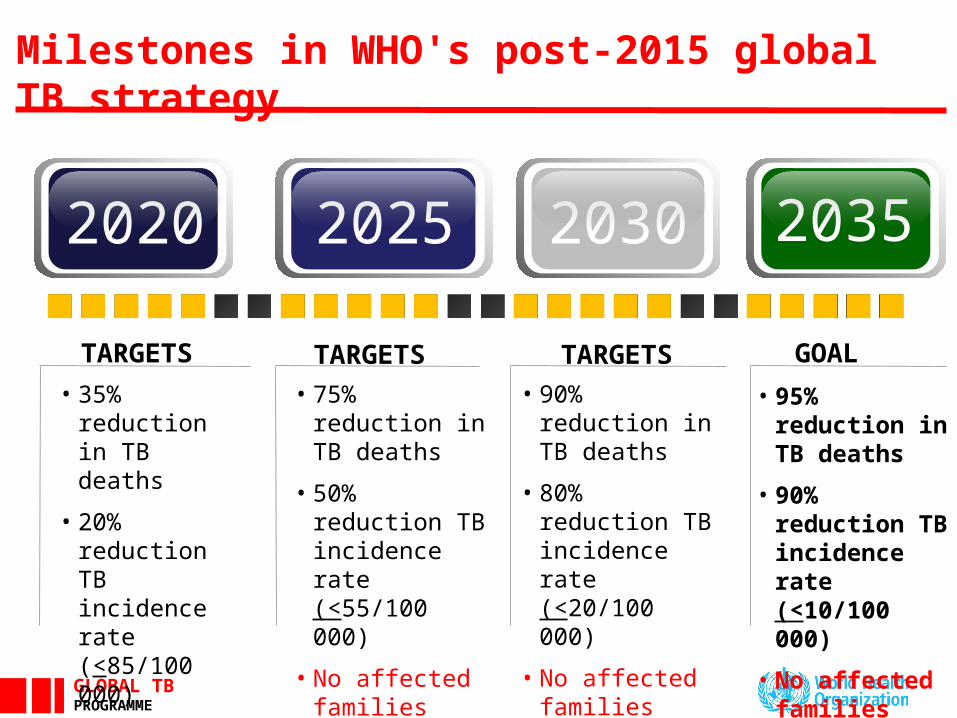
TARGETS• 35% reduction in
TB deaths
• 20% reduction TB incidence rate (<85/100 000)
• No affected families with catastrophic costs due to TB
TARGETS• 75% reduction in
TB deaths
• 50% reduction TB incidence rate (<55/100 000)
• No affected families with catastrophic costs due to TB
TARGETS• 90% reduction in
TB deaths
• 80% reduction TB incidence rate (<20/100 000)
• No affected families with catastrophic costs due to TB
GOAL
• 95% reduction in TB deaths
• 90% reduction TB incidence rate (<10/100 000)
• No affected families with catastrophic costs due to TB
20352020 20302025
Milestones in WHO's post-2015 global TB strategy
GLOBAL TB PROGRAMME
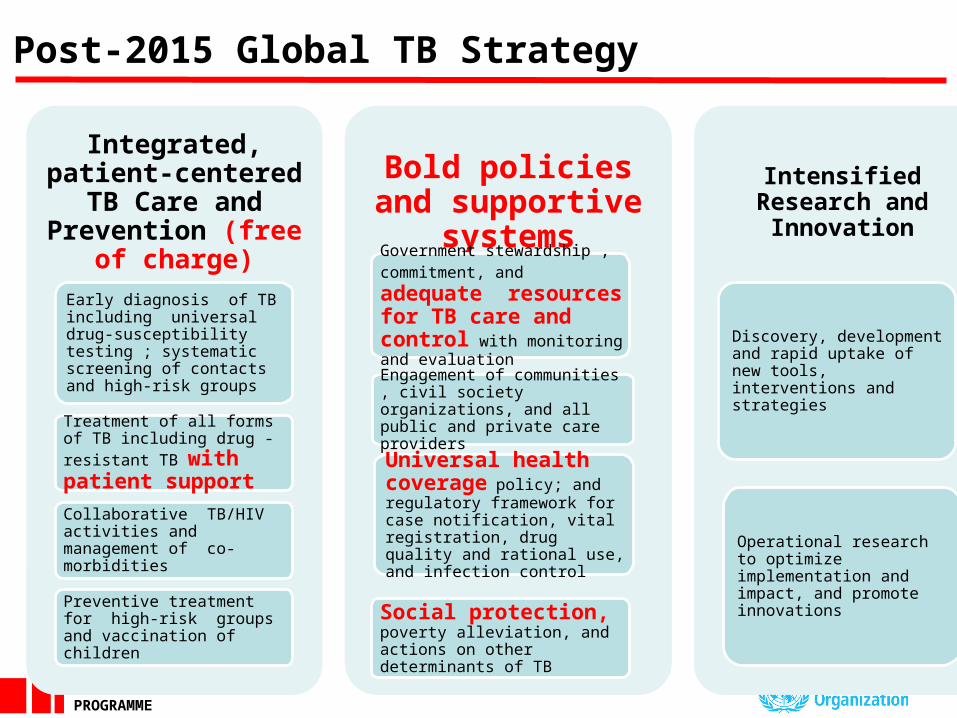
Integrated, patient-centered TB Care and
Prevention (free of charge)
Early diagnosis of TB including universal drug-susceptibility testing ; systematic screening of contacts and high-risk groups
Treatment of all forms of TB including drug -resistant TB with patient support
Collaborative TB/HIV activities and management of co-morbidities
Preventive treatment for high-risk groups and vaccination of children
Bold policies and supportive systemsGovernment stewardship , commitment, and adequate resources for TB care and control with monitoring and evaluation
Engagement of communities , civil society organizations, and all public and private care providers
Universal health coverage policy; and regulatory framework for case notification, vital registration, drug quality and rational use, and infection control
Social protection, poverty alleviation, and actions on other determinants of TB
Intensified Research and Innovation
Discovery, development and rapid uptake of new tools, interventions and strategies
Operational research to optimize implementation and impact, and promote innovations
Post-2015 Global TB Strategy
GLOBAL TB PROGRAMME
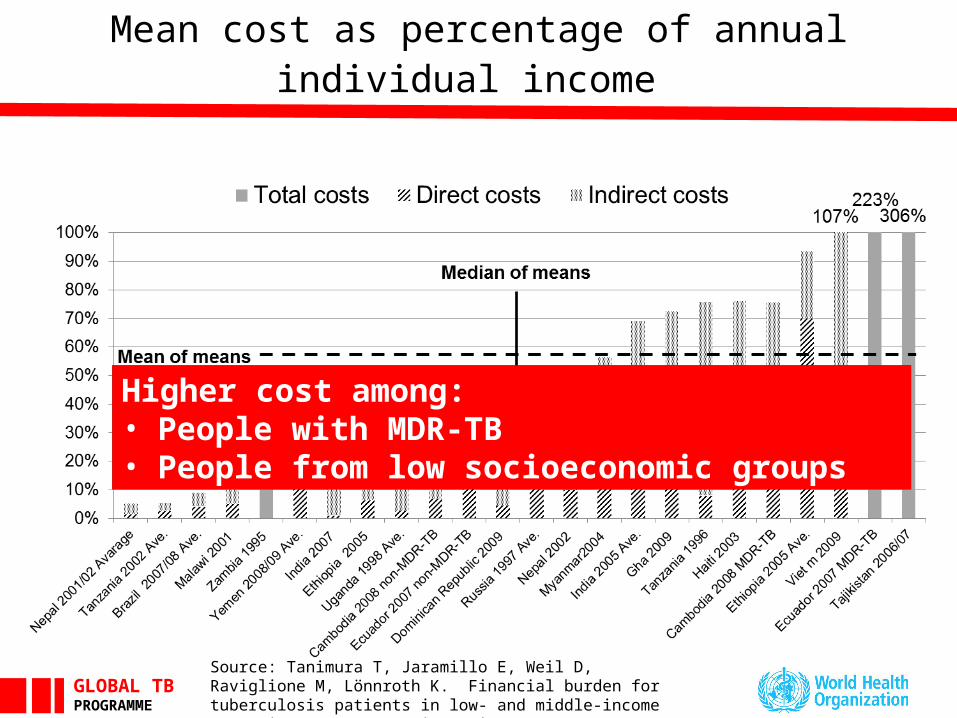
Mean cost as percentage of annual individual income
Higher cost among:• People with MDR-TB• People from low socioeconomic groups
Source: Tanimura T, Jaramillo E, Weil D, Raviglione M, Lönnroth K. Financial burden for tuberculosis patients in low- and middle-income countries – a systematic review. ERJ 2014
GLOBAL TB PROGRAMME
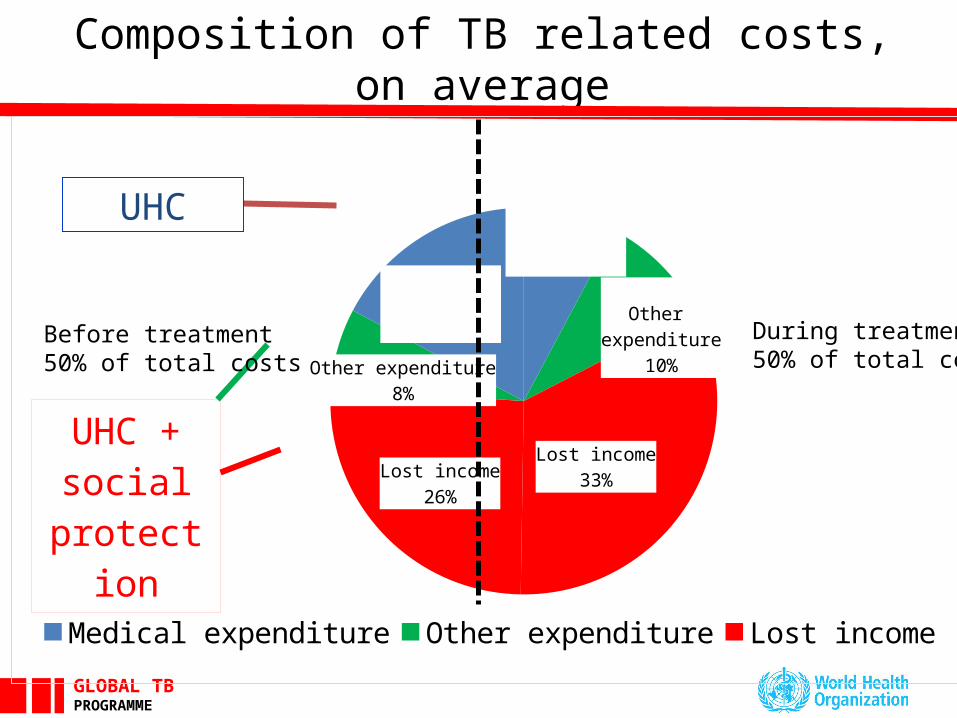
Composition of TB related costs, on average
Medical expenditure
8%
Other expenditure
10%
Lost income33%Lost income
26%
Other expenditure8%
Medical expenditure
17%
Medical expenditure Other expenditure Lost income
UHC + social pro-
tection
During treatment50% of total costs
Before treatment50% of total costs
UHC
GLOBAL TB PROGRAMME
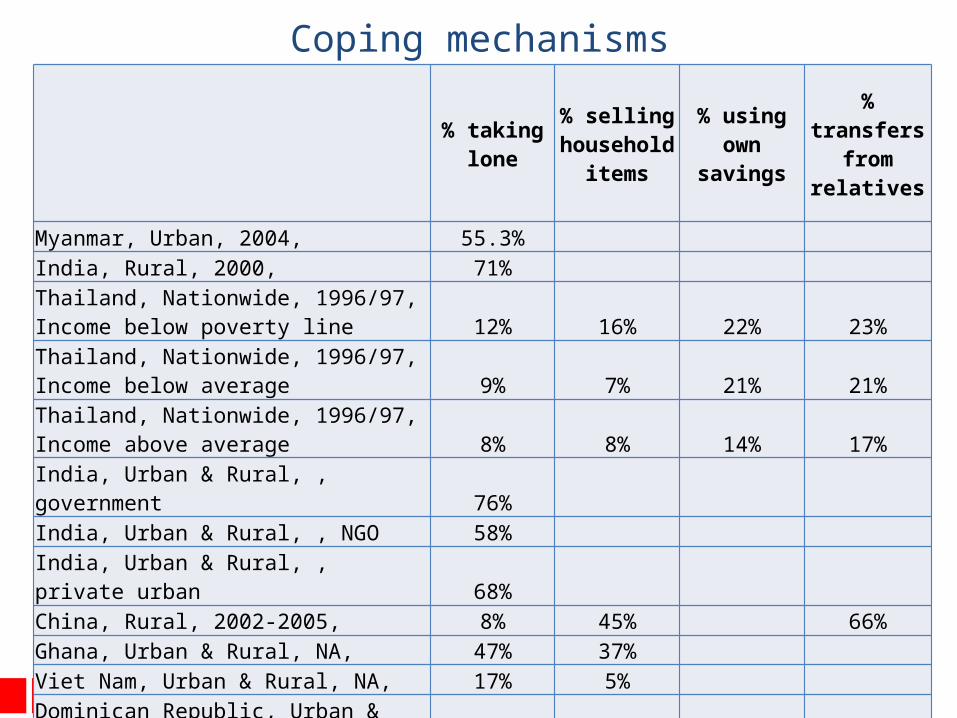
Coping mechanisms
% taking lone
% selling household
items
% using own
savings
% transfers from
relatives
Myanmar, Urban, 2004, 55.3% India, Rural, 2000, 71% Thailand, Nationwide, 1996/97, Income below poverty line 12% 16% 22% 23%Thailand, Nationwide, 1996/97, Income below average 9% 7% 21% 21%Thailand, Nationwide, 1996/97, Income above average 8% 8% 14% 17%India, Urban & Rural, , government 76%India, Urban & Rural, , NGO 58%India, Urban & Rural, , private urban 68%China, Rural, 2002-2005, 8% 45% 66%Ghana, Urban & Rural, NA, 47% 37% Viet Nam, Urban & Rural, NA, 17% 5%
Dominican Republic, Urban & Rural, NA, 45% 19% Tajikistan, Urban & Rural, 2006/07, 30% 49% 30%
GLOBAL TB PROGRAMME
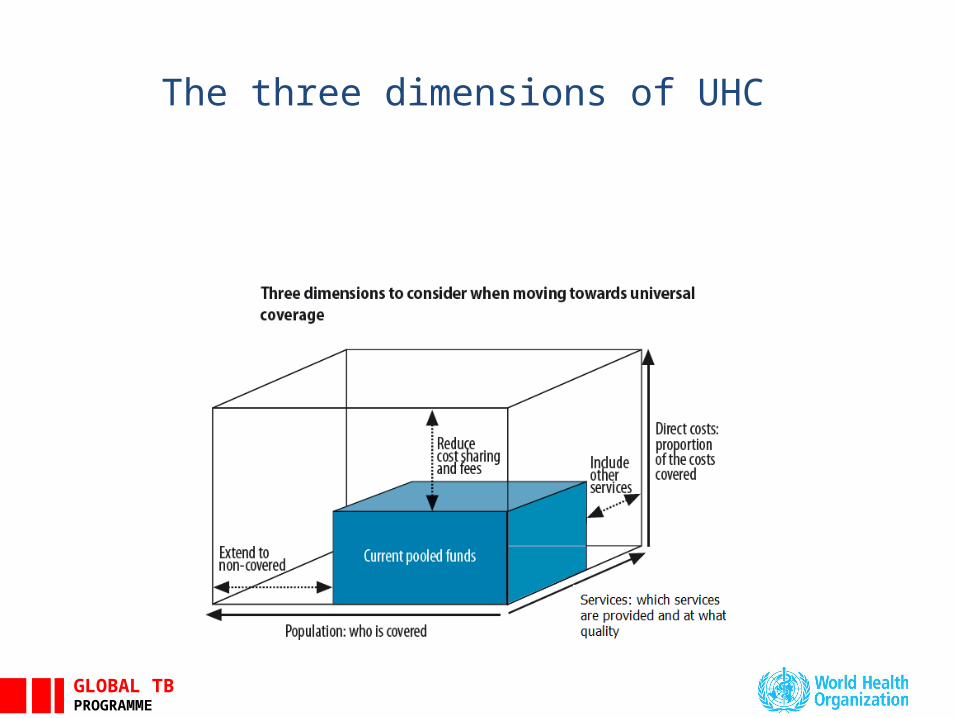
DefinitionsWHO definition of UHC:
a) universal access to needed health services;
b) without financial hardship in paying for them (i.e. concerned with out-of-pocket medical expenses only)
WHO definition of "catastrophic health expenditure”:
Direct health care expenditures corresponding to >40% of annual discretionary income" (income after basic needs, such as food and housing). (i.e. indirect costs of care and income loss are not included).
ILO definition of social protection:
c) Access to Essential Services (water and sanitation, health, education, etc);
d) Essential Social Transfers (cash and in kind, paid to the poor and vulnerable) To enhance food security and nutrition, To provide a minimum income security and access to services Income replacement and social support in the event of illness
GLOBAL TB PROGRAMME
The three dimensions of UHC
GLOBAL TB PROGRAMME
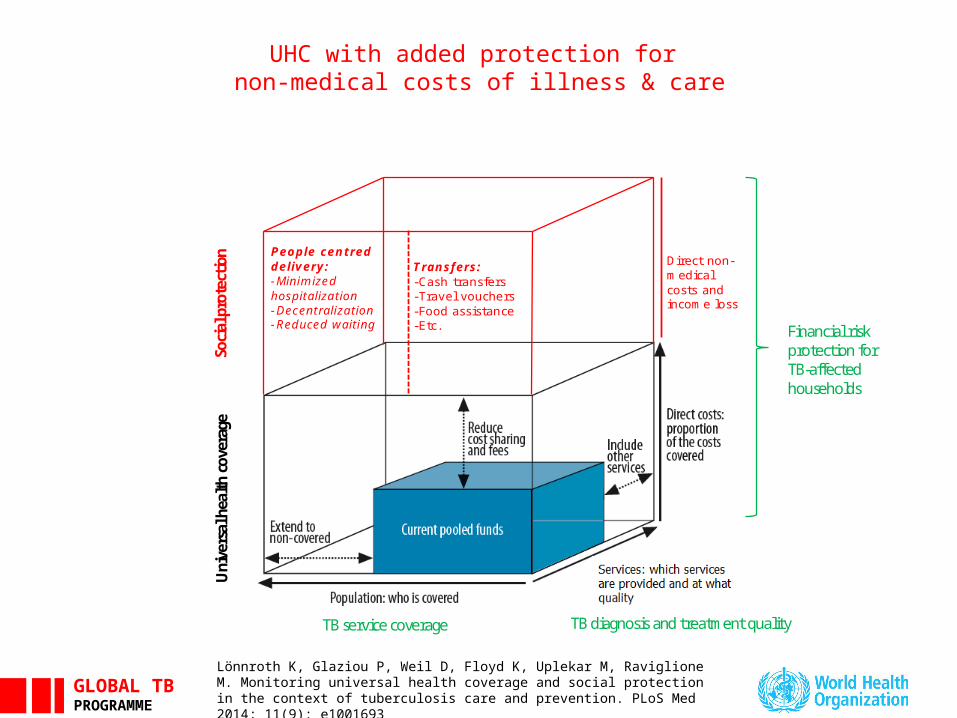
UHC with added protection for non-medical costs of illness & care
Direct non-medical costs and income loss
Transfers: -Cash transfers -Travel vouchers -Food assistance -Etc.
People centred delivery: -Minimized hospitalization -Decentralization -Reduced waiting
Uni
vers
al h
ealth
cov
erag
e
TB diagnosis and treatment quality TB service coverage
Financial risk protection for TB-affected households
Soci
al p
rote
ction
Lönnroth K, Glaziou P, Weil D, Floyd K, Uplekar M, Raviglione M. Monitoring universal health coverage and social protection in the context of tuberculosis care and prevention. PLoS Med 2014; 11(9): e1001693
GLOBAL TB PROGRAMME
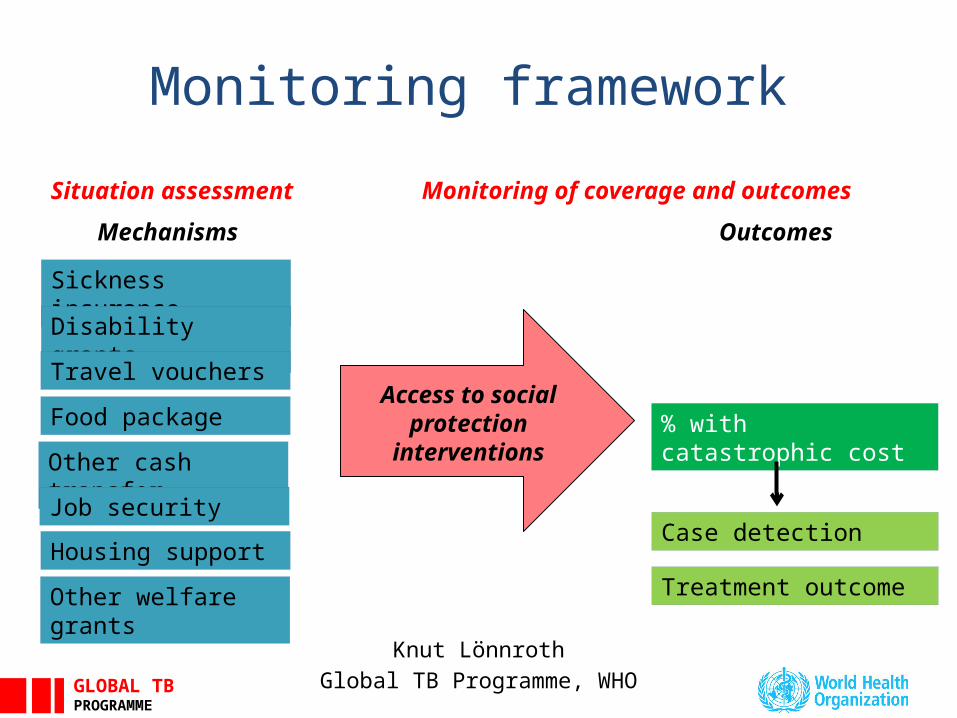
Knut Lönnroth
Global TB Programme, WHO
Sickness insurance
Food package
Disability grants
Other welfare grants
Travel vouchers
Mechanisms Outcomes
Case detection
% with catastrophic cost
Treatment outcome
Access to social protection
interventions
Housing support
Other cash transfer
Situation assessment Monitoring of coverage and outcomes
Job security
Monitoring framework
GLOBAL TB PROGRAMME
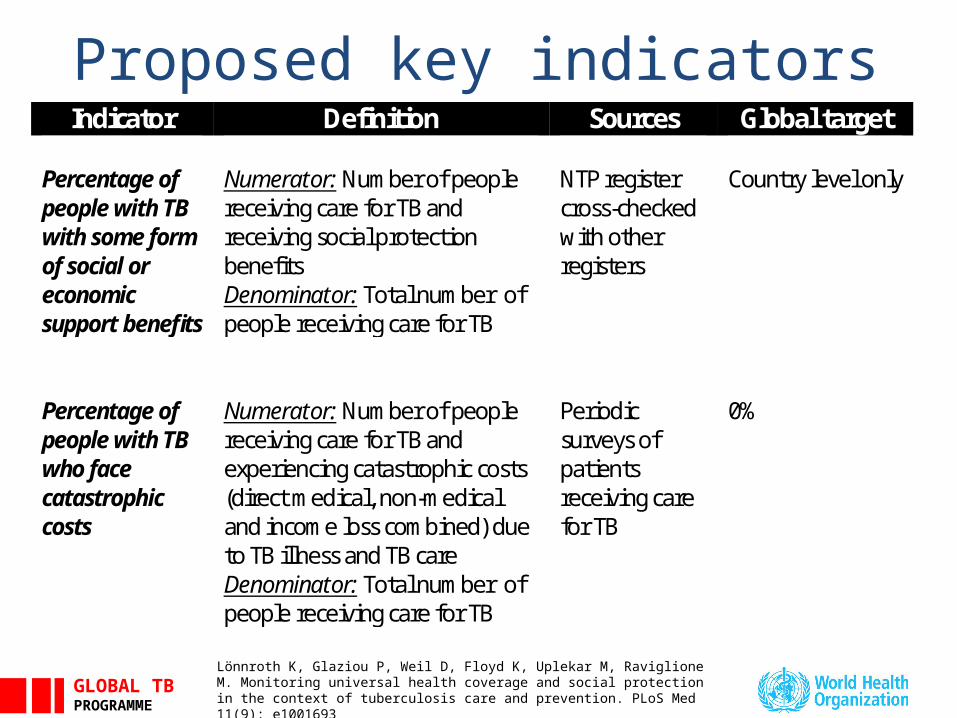
Proposed key indicatorsIndicator Definition Sources Global target
Percentage of people with TB with some form of social or economic support benefits
Numerator: Number of people receiving care for TB and receiving social protection benefits Denominator: Total number of people receiving care for TB
NTP register cross-checked with other registers
Country level only
Percentage of people with TB who face catastrophic costs
Numerator: Number of people receiving care for TB and experiencing catastrophic costs (direct medical, non-medical and income loss combined) due to TB illness and TB care Denominator: Total number of people receiving care for TB
Periodic surveys of patients receiving care for TB
0%
Lönnroth K, Glaziou P, Weil D, Floyd K, Uplekar M, Raviglione M. Monitoring universal health coverage and social protection in the context of tuberculosis care and prevention. PLoS Med 11(9): e1001693
GLOBAL TB PROGRAMME
Definition of catastrophic cost - options:
1. Total cost as percentage of annual household income (over a defined level) Requires collection of direct and indirect cost data plus income data Possible cut-off:
>20% (which is associated with poor treatment outcomes, Wingfield et al, 2014)? >10% (judged to have important financial implications, at least for poor families)?
2. Any occurrence of important "Dissaving" Requires much simpler questions about potentially irreversible coping
mechanisms: Taking out a loan Selling property/livestock/household items
Associated with total cost and total cost as percentage of income (Madan et al, 2014)
GLOBAL TB PROGRAMME
Data collection approaches
1. Routine surveillance data from TB register (monitoring access to social protection only)
2. TB patient survey (diagnosed cases)
3. TB prevalence surveys
4. Health expenditure subaccount for TB (too small sample probably)
GLOBAL TB PROGRAMME
The patient cost tool
• Generic survey instrument with tools for country adaptation (KNCV, WHO and JATA, 2010)
• Built on rich previous research • Study population: people diagnosed with TB• Recently adapted to people with MDR-TB
• Domains– Health seeking (provider utilization, delay)– Direct cost for diagnosis, treatment , transport, etc– Indirect costs (income loss)– Social consequences (divorce, interrupted education, etc)– Coping mechanisms (loans, selling goods, etc)– Patient characteristics (age, sex, socioeconomic status, etc)– Access to social protection
GLOBAL TB PROGRAMME
Where and how often?
Sample: • National random samples?• Sentinel sites?
Frequency:• Every 5 years?• More often?
Global monitoring:• Baseline in 2015/16• All countries or panel of countries?• Every year? Every 5 years?
GLOBAL TB PROGRAMME
Next steps• Further methodological development
Planned meeting on social protection interventions and monitoring, tentatively March 2015
Including meeting task force on monitoring social protections
• Demonstration studies in selected countries in all regions Select 2-3 countries in WPR?
• Continued support to countries so that baseline can be established for 2015-2016 All WPR priority countries?
Related Documents











