FOCUS ARTICLE Gender Differences in Pain Thuan T. T. Dao, DMD. MSc. Dip Prostho, PhD Associate Professor Faculty of Dentistry University of Toronto Toronto, Ontario, Canada Linda LeResche, ScD Research Professor Department of Oral Medicine University of Washington Seattle, Washington Correspondence to: Dr Thuan T. T. Dao Faculty of Dentistry University of Toronto 124 Edward Street Toronto. Ontario Canada M5G 1G6 Fax:416-979-4936 E-mail: thLan,[email protected] A review of the literature on gender and clinical pain reveals a dis- proportionate representation of women receiving treatment for fnany pain conditions and suggests that women report more severe pain, more frequent pain, and pain of longer duration than do men. Gender differences in pain perception have also been exten- sively studied in the laboratory, and ratings of experimentally induced pain also show some sex disparity, with females generally reporting lower pain thresholds and tolerance than males. However, there is little consensus on whether these apparent dif- ferences reflect the way men and women respond to pain, differing social rules for the expression of pain, or biologic differences in the way noxious stimuli are processed. In this paper, our working hypothesis is that the higher prevalence of chronic orofacial pain in women is a result of sex differences in generic pain mechanisms and of as-yet unidentified factors unique to the craniofacial sys- tem. We will review the evidence concerning gender differences in the prevalence of pain conditions, with a focus on orofacial pain conditions. Evidence and hypotheses concerning biologic and psy- chosocial factors that could influence prevalence rates will also he discussed. J OROFAC PAIN 2000;14:169-184. Key words: gender differences, pain, orofacial pain, pain measurement, epidemiology W ith the obvious anatomic and genetic differences between males and females, many people mtuitively believe that the sexes differ in their predisposition toward and responses to pain. This belief may have been perpetu- ated by the disproportionate representation of women receiving treatment for many pain conditions, and by studies that suggest that women report more severe pain, more frequent pain, and pain of longer duration than do men.'"^ However, there is little consen- sus on whether these apparent variations reflect the way men and women respond to pain, differing social rules for the expression of pain, or biologic differences in the way noxious stimuli are pro- cessed. While several studies have attempted to address this con- troversy, the different patterns of sex-specific prevalence reported for various clinical pain disorders and the inconsistencies in the findings across experimental studies, as reviewed in this paper, highlight the fact that the gender issue is still unresolved and needs further exploration. This article will review the evidence concern- ing gender differences in the prevalence of pain conditions, as well as evidence and hypotheses concerning biologic and psychosocial Journal of Orofacial Pain 169

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

FOCUS ARTICLE
Gender Differences in Pain
Thuan T. T. Dao, DMD. MSc. DipProstho, PhD
Associate ProfessorFaculty of DentistryUniversity of TorontoToronto, Ontario, Canada
Linda LeResche, ScDResearch ProfessorDepartment of Oral MedicineUniversity of WashingtonSeattle, Washington
Correspondence to:Dr Thuan T. T. DaoFaculty of DentistryUniversity of Toronto124 Edward StreetToronto. OntarioCanada M5G 1G6Fax:416-979-4936E-mail: thLan,[email protected]
A review of the literature on gender and clinical pain reveals a dis-proportionate representation of women receiving treatment forfnany pain conditions and suggests that women report more severepain, more frequent pain, and pain of longer duration than domen. Gender differences in pain perception have also been exten-sively studied in the laboratory, and ratings of experimentallyinduced pain also show some sex disparity, with females generallyreporting lower pain thresholds and tolerance than males.However, there is little consensus on whether these apparent dif-ferences reflect the way men and women respond to pain, differingsocial rules for the expression of pain, or biologic differences inthe way noxious stimuli are processed. In this paper, our workinghypothesis is that the higher prevalence of chronic orofacial painin women is a result of sex differences in generic pain mechanismsand of as-yet unidentified factors unique to the craniofacial sys-tem. We will review the evidence concerning gender differences inthe prevalence of pain conditions, with a focus on orofacial painconditions. Evidence and hypotheses concerning biologic and psy-chosocial factors that could influence prevalence rates will also hediscussed.J OROFAC PAIN 2000;14:169-184.
Key words: gender differences, pain, orofacial pain, painmeasurement, epidemiology
With the obvious anatomic and genetic differencesbetween males and females, many people mtuitivelybelieve that the sexes differ in their predisposition
toward and responses to pain. This belief may have been perpetu-ated by the disproportionate representation of women receivingtreatment for many pain conditions, and by studies that suggestthat women report more severe pain, more frequent pain, and painof longer duration than do men.'"^ However, there is little consen-sus on whether these apparent variations reflect the way men andwomen respond to pain, differing social rules for the expression ofpain, or biologic differences in the way noxious stimuli are pro-cessed. While several studies have attempted to address this con-troversy, the different patterns of sex-specific prevalence reportedfor various clinical pain disorders and the inconsistencies in thefindings across experimental studies, as reviewed in this paper,highlight the fact that the gender issue is still unresolved and needsfurther exploration. This article will review the evidence concern-ing gender differences in the prevalence of pain conditions, as wellas evidence and hypotheses concerning biologic and psychosocial
Journal of Orofacial Pain 1 6 9
Dao/LeResche
factors that could influence prevalence rates.Specifically, we will focus on chronic otofacia!pain conditions, most of which show a signifi-cantly higher prevalence in women than in men.
Statement of Position
Out working hypothesis is that the higher preva-lence of chronic orofacial pain in women versusmen is a result of sex differences in generic painmechanisms and as-yec unidentified factors uniqueto the craniofacial system.
Clinical Pain
Epidemiology
The volume of literature on clinical pain and gen-der is impressive. Overall, the information revealssome sex differences in the prevalence and mani-festations of signs and symptoms of a variety ofpain disorders. For instance, as summarized hyBerkley,'' several conditions in which chronic painis a prominent component appear to be associatedwith a higher female prevalence. The numher ofsuch conditions is more than twice that of disor-ders that have a male predilection. Interestingly,many of the pain conditions that primarily affectwomen are still of unknown origin. Some involvethe cardiovascular system (carotidynia, Raynaud'sdisease, chronic venous insufficiency, and migraineheadaches, especially migraine without aura] andgastrointestinal structures (irritable bowel syn-drome, esophagitis, reflux esophagitis with pepticulcer, proctalgia fugax, chronic constipation],while a large number are expressed in the headand neck region. These include temporomandibu-lar disorders (TMD), various types of headaches(with the exception of cluster and post-traumaticheadaches, which have a male predilection], occip-ital neuralgia, hemicrania continua, chronic parox-ysmal hemicrania, atypical odontalgia, burningmouth syndrome, and probably trigeminal neural-gia. With tegard to pain induced hy dental treat-ments, the perception of general pain intensity,analgesic consumption, pain when eating, and theinfluence of discomfort on daily life were ail signif-icantly greater in girls than in boys who receivedorthodontic treatments,^ Most studies of muscu-loskeletal pain indicate that women are more hkelyto report musculoskeletal pain than men. How-ever, some studies of neck, shoulder, back, andknee pain indicate equal prevalence among the 2
sexes, or, in a few cases, a higher rate in malesthan in females.* These conditions may be morestrongly related to occupation than to gender.However, it is important to note that pain disor-ders do not always have a female predilection. Infact, if we rely on the list provided by Berkley,'' thedisorders with no sex predilection added to thosewith higher male prevalence outnumber thoseassociated with higher female predilection. This isconsistent with the extensive review on gender andclinical pain experience published recently hyUnruh.2
It is also important to point out that the preva-lence of most pain disorders varies greatly withage, as well as with gender (eg, the probability ofexperiencing migraine headache is similar for boysand girls at age 12, whereas a 30-year-old womanis much more likely than a 30-year-old man toexperience this kind of pain). Thus, the fact thatthere are gender differences (across all age groups]in the prevalence of a given pain condition maynot be as informative as data on the overall sex-and age-specific prevalence pattern of that pain.^An analysis of prevalence hy both age and sexallows us to identify factors that vary across thelife span (eg, hormonal state, occupational role]that may possibly interact with gender to increasethe risk of developing particular pain conditions.
Gender Differences in the Epidemiology ofChronic Orofaciai Pain Conditions
Temporomandibular disorder pain is the mostcommon chronic orofacial pain condition. It israre in children prior to puberty.** Prevalence tatesfound in population-based epidemiologic studiesrange from about 8% to 15% for women andfrom about 3% to 10% for men. Given differencesin definitions and in populations examined in thedifferent studies, these rates are remarkably consis-tent. In nearly every study, TMD pain is found tobe 1.5 to 2 times more common in women than inmen. Also, in all studies where there is a clear pat-tern for age-specific prevalence, the age of peakprevalence is around 35 to 45 years.
Population-based data on trigeminal neuralgiacome primarily from 2 studies that measured therates of seeking treatment for these conditions in 2defined areas of the United States.''"^ To the extentthat people with trigémina! neuralgia consistentlyseek treatment for their problem, rates found inthese "treated incidence" studies approximate truepopulation-based incidence (onset) rates. How-ever, if not all cases come to treatment, the ratesand gender patterns may differ from those that
170 Volume 14. Number 3, 2000
Dao/LeResche
would be found in a survey of the general popula-tion. Overall incidence races are on the order of 3to 5 onsets per year per 100,000 people (about1/500 to 1/1,000 the rate of onset ot TMD pain).The incidence rate rises with age in both studies,hut one study shows a large sex difference, withhigher rates in women, while the other shows amuch smaller difference.
Burning mouth pain has been mvestigated in ahandful of population-based studies. These investi-gations have employed different definitions of theproblem, so the absolute rates vary greatly, from alow of 1% in a large study of the U.S. householdpopulation'^ that inquired about "a prolongedunexplained burning sensation in your tongue orany other part of your mouth," to a high of almost15% in a study of Finns over 30 years of age thatasked about smarting and ticklmg sensations, aswell as burmng, due to any cause.'- A tbird study,wbich used a definición of burning pain from anycause, found an mtermediate rare of 4.5%.'^ Bothincreasing age and female gender appear to be riskfactors for burning mouth pain. Prevalence races inwomen are about twice tbose in men.
Clinical studies of atypical odontalgia and atypi-cal facial pain indicate that women are much morelikely than men to seek care for these conditions,and that the mean age of persons seeking care isaround 40 to 55 years. Unfortunately, there are nopopulation-based studies of these conditions, andthe extent to which these clinic populations reflectthe underlying distribution of tbe conditions in cbepopulation is unknown.
Sex Differences in Symptom Expression
In addition to the data on pain prevalence by gen-der, tbere is also evidence suggesting tbat for sev-eral diseases, the presentation of illness may differsignificantly by gender, witb certain signs andsymptoms being much more common m one se.xthan in the other. For instance, disc degenerationhas been reported to be associated with neck painin men but not in women.'"* Migraine withoutaura is twice as prevalent in women as migrainewitb aura, while tbe opposite is true for men.'^Similarly, among patients diagnosed with acucemyocardial infarction, men were significantly morelikely than women to complain about neck, back,or jaw pains and nausea.'^ Different risk factorsand predictors of diseases bave also been observedfor tbe 2 genders. For example, risk of low backpain increases with beigbt among men but notamong women.'^ For acute appendicitis, previousabdominal surgeries, rectal digital tenderness.
rebound, and elevated body temperature are signif-icant predictors for men, but nor for women,whereas the absence of renal renderness is a goodpredictor for women but not for men.'^ Similarly,chest pain is a much poorer predictor of coronaryartery disease in women with abnormal angiogra-phy'"" or positive thallium-20 scans tban it is inmen witb tbesc findings.-**
Taken together, these data show that some paindisorders may not affect women and men the sameway. Since gender is only 1 of the multiple factorsthat have a profound impact on clinical painreports, inference about its specific role is at besttentative.
Methodologie Issues
While epidemiologic studies sometimes sbow anuneven sex distribution of pain disorders, they donot usually explain rbe nature of the differencesand tbe causes for observed discrepancies. Mostepidemiologic literature to date has been descrip-tive, and reports of gender differences are oftenpresented as secondary findings in studies thatwere not originally designed to address the genderissue. Sometimes the gender distribution isreported only as part of the sociodemographicdescription of the study population, and preva-lence rates are not reported by gender (or age).Clinical studies may also neglect to analyze out-comes by gender.
Other problems become evident when studiesthat report gender differences as incidental find-ings are reviewed (see Unruh'). In studies in whichthe gender composition of the sample is repre-sented m percentages without statistical analysis, itIS difficult to appreciate the significance of anyapparent disparities. Gender differences found dur-ing the review process may be inflated since theyare based on incidental findings on this topic, andthese are more frequently reported when they canbe statistically substantiated. The review may besimilarly biased during the electronic retrieval ofpublished papers, since those that use gender (or asynonym) as a keyword are more likely to surface,and these keywords are listed mostly when genderis considered an important aspect of the study orwhen gender differences have reached statisticalsignificance.
On the other hand, clinical studies that focusspecifically on the issue of gender and pain areoften observational and may not be designed toprovide explanations for the differences beinginvestigated. The interpretation of the extensive lit-erature on clinical pain prevalence is further
Journal of Orofacisl Pain 171
Dao/LeResche
Status oí pain subjectAge
Body sizeLeuel of anxiety
Heaim statusNLtrilive status
Hormonal statusEthnicityReligion
Sociaf and cjltuia! bell el sPast pair experiencesInvolvement in litigation
Dimension and natureof pain assessed
Sensory—pain intensityAHective—pair unpleasantness
Current or preuious painPain location
Environment in wi7iciipain is reported
Pain clinicWaiting rcom
HospitalHomeSchoolCountry
Time ol pain reportsPfiase ol menstrual cycie
Time ol dayTime ol year
Season—weather
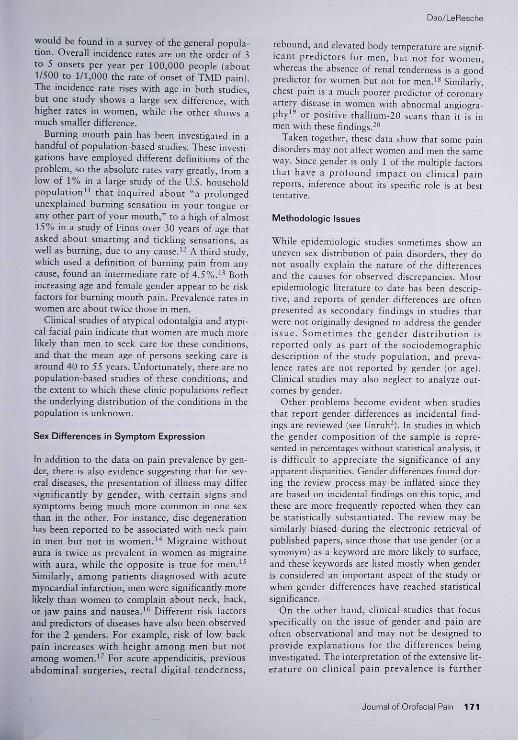
Fig 1 Iticeracting variables chat influence clinical pain reports.
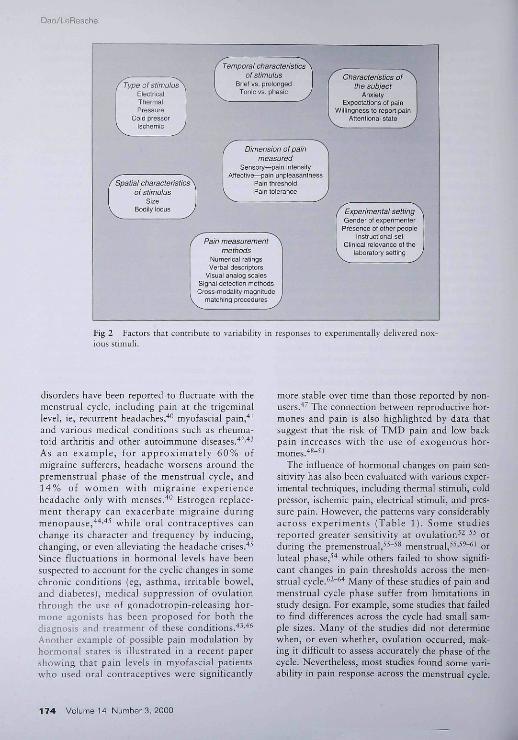
complicated with other méthodologie issties,including the validity and reliability oí pain mea-surement methods^' and representativeness ofstudy samples. The issue becomes more complexsince pain assessment relies on perceptions andreports (from both the patients and the mvestiga-tors) that are shaped hy many variables other thangender. Some of these interacting variables arehsted m Fig 1.
Data on gender prevalence may also vary acrossStudies due to characteristics of the study samples.Data collected from population-based studies areless prone to bias than those obtained from clinicalsamples, industrial settings, occupational groups,or databases of insurance companies, since theyare less influenced by factors that are specific tothe nature of the sample. For instance, it has beenargued that the overrepresentation of women withchronic orofacial pain in clinical samples does notnecessarily reflect the true gender ratio of thesepain conditions, but may instead reflect the possi-bility that female patients more readily seek treat-ment.' Although the data on gender differences inhealth care utilization for orofacial pain con-flict,̂ '̂̂ '̂̂ ^ Unruh's review suggested that for avariety of health problems, women report morevisits and more return visits than do men.̂ This is
consistent with the results of a survey showing thatamong chronic pain patients, women used healthcare services more often than men.̂ "" Similarly,Linton et al also reported that when spinal painwas at Its worst, men took sick leave, whereaswomen sought health care.̂ ^ These data highlightthe possibility that clinical samples may generatebiased findings on gender prevalence in pain; theimportance of using population-based samples tostudy gender differences in pain is thereby rein-forced.
Experimental Pain
Gender differences in pain have also been studiedextensively m the laboratory, where standardizedprotocols allow control for some variables that caninfluence pain reports. Fillingim and Maixner^^reviewed a large number of psychopbysical studies(ie, studies of the relationship between the physicalproperties of a pain stimulus and the sensory andbehavioral responses of the subject). They con-cluded that, overall, females exhibit greater sensi-bility to laboratory pain compared to males. In areview,'' Berkley also concluded that women havelower thresholds, rate similar stimuli as more
172 Volume 14, Number 3. 2000

Dao/LeResche
painful, and have less tolerance ior intense stimuli.However, both papers pointed out that findingsare not always consistent across studies. Whilemechanical pressure, electrical stimuli, and coldpressor stimulation are more reliahle in producinghigher pain ratings in females, studies usmg ther-mal stimuli (other than cold pressor) have gener-ated conflicting data. This variability is not sur-prising, given the differences in experimentalprotocols, the diversity of noxious stimuli thathave been employed {see Fillingim and Maixner'''),and reports that sex differences in responsivenessto painful and non-painful stimuli are dependenton the stimulation method.-" For instance, theduration and temporal sequence of application ofthe stimulus are important factors thar affect studyoutcomes. For a stimulus of a given intensity, pro-longed and repeated applications induce greaterpain than a single, hrief stimulus; in addition, theyare more likely to activate temporal summationmechanisms, and temporal summation of thermalpain has been reported to be greater in femalesthan in males.-^ The size of the stimulating tip isanother important factor. If spatial summation ismore pronounced and reaches a ceiling sooner infemales than in males, sex differences in responseto thermal stimuli may occur with small thermodesbut not with larger ones.-' Failure to find a genderdisparity in many srudies may also be a resulr ofsmall sample size, which results m a lack of powerto detect the difference being sought.-^
Results may also differ depending on the dimen-sion of pain being assessed and the environment inwhich the experimenr takes place, since pain is amultidimensional experience with both sensory/discriminative and cognitive/emotional compo-nents. As discussed by Fillingim and Maixner,-^ itis possible that gender has a selective influence onthese dimensions, while these, in turn, may be dif-ferently affected by various methods of pain induc-tion. While the selective effect of gender on thesensory and affective dimensions of experimentalpain has not been thoroughly investigated, it iswell known that threshold and tolerance measuresare susceptible to social environmental factors,including the gender of the experimenter,^" thepresence of other people, subjects' status and pamattitudes, instructional set,̂ '"^^ and the clinical rel-evance of the laboratory settings.̂ "* In addition,responses to threshold and tolerance tests may bemodulated by the subject's anxiety^^"^^ and expec-tations of pain tolerance, both of which have beenshown to differ between males and females.^^Other psychophysical techniques, such as signaldetection and magnitude matching procedures.
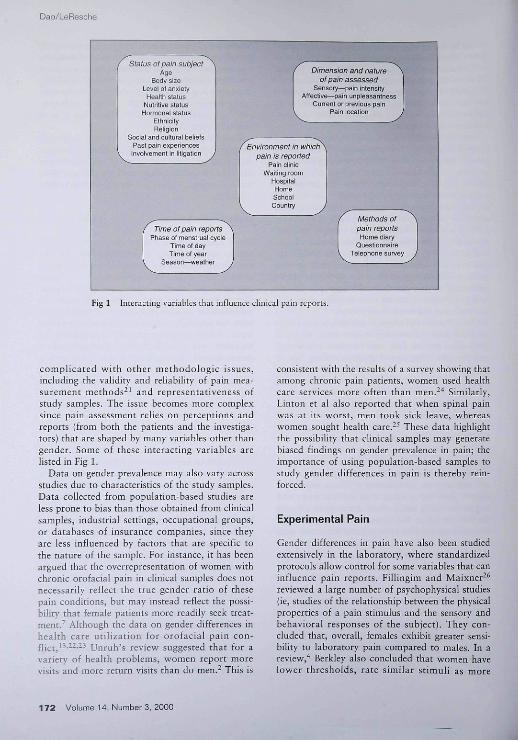
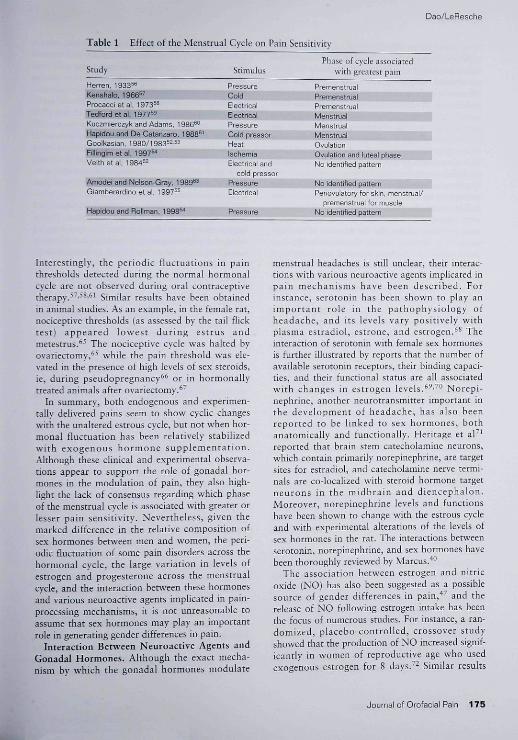
allow the investigator to estimate separately boththe sensory abilities of the subjects to discriminatedifferent levels of stimuli and their willingness toreport stimuli as painful (emotional or responsebias). By normalizing responses to painful stimuliagainst ratings of standard stimuli in both painfuland non-painful ranges, clinicians can controlresponse bias. Although these approaches may beinfluenced less by attitudinal variables and repre-sent a significant improvement over the thresholdand tolerance measures, their results are stillinconsistent across studies.'^ This is not unex-pected, given the numerous factors that may influ-ence responses to experimentally delivered noxiousstimuli. Some of the biologic, psychosocial, andcultural factors are already listed in Fig 1; othervariables more specific to a laboratory setting areincluded in Fig 2.
Overall, rarings of experimentally induced paindo sbow some sex disparir\', and females generallyreporr lower pain thresholds and tolerance thanmales. However, these differences are often smalland observed inconsistently, most likely because ofdifferences in the methodology employed and thenumerous variables that influence pain reports in alaboratory environment. In this context, the chni-ca! relevance of these findings remains limited.What remains to be determined is the extent towhich the contrast observed reflects a responsebias phenomenon shaped by various psychologic,social, and cultural factors or biologic differencesin pa in-procès s ing mechanisms.
Possible MechanJsms UnderlyingGender Differences in Pajn
Biologic Factors
While the debate continues over the controversiesabout the various aspects of sex disparity in pain,It is difficult to disagree with the vivid remarkmade by Berkley* that ". . . females and males dodiffer virtually absolutely and unarguably in threeaspects of their reproductive biology. Their pelvicreproductive organs differ and their hormonal con-ditions differ chronobiologically and composition-ally." The potential impact of those biologic differ-ences on pain will be discussed below.
Effect of Gonadal Hormones on Pain. An obvi-ous gender difference is the characteristic temporalfluctuations of hormonal states in females and thefrequent occurrence of pain associated with thereproductive cycle, ie, menstruation and ovulation.In addition to these non-pathologic pains, many
Journal of Orofacial Pain 173
Dao/LeResctie
Spatial characteristics^oí stimulus
SiíeBodily locus ,
Temporal characteristicsof stimulus
Brief vs. proiongedTonic vs. phasic
Dimension of painmeasured
Sensory—pain intersilyAffective—pain unpieasantnass
Pain IhreslioidPain loietance
Pain measurementmetiiods
Nun erica i ratingsVerbai descriptors
Visjal anaiog scalesSignal detection methodsCross-modafity magnitude
matching piocedures
Characteristics ofthe sutHjEct
AnxietyExpectations ot pain
Willingness to repcrt pairAttention a i state
Expérimentai settingGender of experimenter
Presence ol other peopieInstructional set
Ciinical reievance ûl the¡aboiatory setting
Fig 2 FaLtors that contribute to variability in responses to experimentally delivered nox-ions stimuli.
disorders have been reported to fluctuate with themenstrual cycle, including pain at the trigetninallevel, ¡e, recurrent headaches,''^ myofascial pain,''̂and various medical conditions such as rheuma-toid arthritis and other autoimmune diseases.''-'''^As an example, for approximately 60% ofmigraine sufferers, headache worsens around thepremenstrual phase of the menstrual cycle, and14% of women with migraine experienceheadache only with menses.''" Estrogen replace-ment therapy can exacerbate migraine duringmenopause,'''''''^ while oral contraceptives canchange its character and frequency by inducing,changing, or even alleviating the headache crises.''̂Since fluctuations in hormonal levels have beensuspected to account for the cyclic changes in somechronic conditions (eg, asthma, irritable bowel,and diabetes), medical suppression of ovulationthtough the use of gonadotropin-releasiug hor-mone agonists has been proposed for both thediagnosis and treatment of these conditions.''^•"^Another example of possible pain modulation byhormonal states is illustrated in a recent papershowing that pain levels in myofasciai patientswho used oral contraceptives were significantly
more stable over time than those reported by non-users.'*' The connection between reproductive hor-mones and pain is also highlighted by data thatsuggest that the risk of TMD pain and low backpain increases with the use of exogenous hor-mones.''^"^'
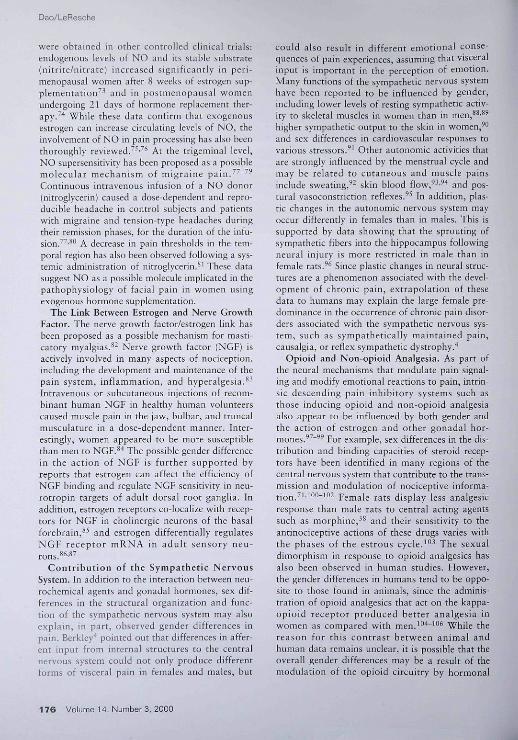
The influence of hormonal changes on pain sen-sitivit}' has also been evaluated with various exper-imental techniques, including thermal stimuh, coldpressor, ischémie pain, electrical stimuli, and pres-sure pain. However, the patterns vary considerablyacross experiments (Table 1). Some studiesreported greater sensitivity at ovulation^^" '̂̂ orduring the premenstrual,^^"^^ menstrua I,̂ •̂'̂ ~ '̂ orluteal phase,^'' while others failed to show signifi-cant changes in pain thresholds across the men-strua! cycle.̂ "̂̂ '̂ Many of these studies of pain andmenstrual cycle phase suffer from limitations instudy design. For example, some studies that failedto find differences across the cycle had small sam-ple sizes. Many of the studies did not determinewhen, or even whether, ovulation occurred, mak-ing it difficult to assess accurately the phase of thecycle. Nevertheless, most studies found some vari-ability in pain response across the menstrual cycle.
174 Volume 14, Number3, 2000
Dao/LeResche
Table 1 Effect of rhe Menstrual Cycle on Pain Sensitivity
Study StimulusPhase of cycle associated
with greatest pain
Herren. 1933^ PressureKenshalo, 1966^' ColdProcaccietal, 1973^" ElectricalTedtord et al, 1977=3 ElectricalKucjmierczyk and Adams, 1986^° PressureHapidou and De Catanzaro, 1988^' Cold pressorGooikasian, 1980/1983"" HeatRlllngim et al. 1997^ IschemiaVeithetal, 1984 '̂̂ Electrical and
cold pressorAmodei and Nelson-Gray, 1989®^ PressureGiamberardino et a). 1 997^^ Electncal
Hapidou and Roliman. 1998^ Pressure
Ovulation and Ijteal phaseNo identified pattern
No identified pattemPeriovuiatory for skin, menstnjai/
premenstruai for muscleNo identified pattern
Interestingly, the periodic fluctuations in painthresholds detected during the normal hormonalcycle are not observed during oral contraceptivetherapy.^ ,58,61 Sijnüaj results have been obtainedin animal studies. As an example, in the female rat,nociceptive thresholds (as assessed by the tail flicktest) appeared lowest during estrus andmetestrus.^' The nociceptive cycle was halted byovariectomy,̂ ^" while the pain threshold was ele-vated in the presence of high levels of sex steroids,ie, during pseudopregnancy^* or in hormonaliycreated animals after ovariectomy.^'
In summary, both endogenous and experimen-tally delivered pains seem to show cyclic changeswith the unaltered estrous cycle, but not when hor-monal fluctuation has been relatively stabilizedwith exogenous hormone supplementation.Although these clinical and experimental observa-tions appear to support the role of gonadal hor-mones in the modulation of pain, they also high-light the lack of consensus regarding which phaseof the menstrual cycle is associated with greater orlesser pain sensitivity. Nevertheless, given themarked difference in the relative composition ofsex hormones between men and women, the peri-odic fluctuation of some pain disorders across thehormonal cycle, the large variation in levels ofestrogen and progesterone across the menstrua!cycle, and the interaction berween these hormonesand various neuroactive agents implicated in pain-processing mechanisms, it is not unreasonable toassume that sex hormones may play an importantrole in generating gender differences in pain.
Interaction Between Neuroactive Agents andGonadal Hormones. Although the exact mecha-nism by which the gonadal hormones modulate
menstrual headaches is still unclear, their interac-tions with various neuroactive agents implicated inpain mechanisms have been described. Forinstance, serotonin has been shown to play animportant role in the pathophysiology ofheadache, and its levels vary positively withplasma estradiol, estrone, and estrogen.^^ Theinteraction of serotonin with female sex hormonesis further illustrated by reports that the number ofavailable serotonin receptors, their binding capaci-ties, and their functional status are ail associatedwith changes in estrogen levels.'^-^^ Norepi-nephrine, another neurotransmitter important inthe development of headache, has also beenreported to be linked to sex hormones, hothanatomically and functionally. Heritage et aF^reported that brain stem catecholamine neurons,which contain primarily norepinephrine, are targetsites for estradiol, and catecholamine nerve termi-nals are co-localized with steroid hormone targetneurons in the midbrain and diencephalon.Moreover, norepinephrine levels and functionshave been shown to change with the estrous cycleand with experimental alterations of the levels ofsex hormones in the rat. The interactions betweenserotonin, norepinephrine, and sex hormones havebeen thoroughly reviewed by Marcus.''"
The association between estrogen and nitricoxide (NO] has also been suggested as a possiblesource of gender differences in pain,"*' and therelease of NO following estrogen intake has beenthe focus of numerous studies. For instance, a ran-domized, placebo-controlled, crossover studyshowed that the production of NO increased signif-icantly in women of reproductive age who usedexogenous estrogen fot 8 days.'- Similar results
Journal of Orofacial Pain 175
Dao/LeResche
were obtained m other controlled clinical trials;endogenous levels of NO and its stable substrate(nirrice/nitrate) increased significantly in peri-menopausal women after 8 weeks of estrogen sup-plementation^' and in postmenopausal womenundergoing 21 days of bormone replacement ther-apy.̂ "̂ Wbile tbese data confirm that exogenousestrogen can increase circulating levels of NO, theinvolvement of NO in pain processing has also beenthoroughly reviewed.̂ ''•^^ At the trigémina! level,NO supersensitivity has been proposed as a possiblemolecular mecbanism of migraine pain.^^"''*Continuous intravenous infusion of a NO donor(nitroglycerin) caused a do se-de pendent and repro-ducible headache in conrrol subjects and patientswitb migraine and tension-type beadacbes duringtheir remission phases, for the duration of the infu-sion.̂ ''•̂ *' A decrease in pain thtesholds in the tem-poral region has also been observed following a sys-temic administration of nitroglycerin.*' Tbese datasuggest NO as a possible molecule implicated in tbepathophysiology of facial pain in women usingexogenous bormone supplementation.
Tbc Link Between Estrogen and Nerve GrowthFactor. The nerve growth factor/estrogen link hasbeen proposed as a possible mechanism for masti-catory myalgias.̂ ^ Nerve growth factor (NGF) isactively involved in many aspects of nociception,including the development and maintenance of thepain system, inflammation, and hyperalgesia.**'Intravenous or subcutaneous injections of recom-binanr human NGF in bealtby buman volunteerscaused muscle pain in the jaw, bulbar, and truncalmusculature in a dose-dependent manner. Inter-estingly, women appeared to be more susceptibletban men to NGF.'*'' The possible gender differencein the action of NGF is further supported byreports that estrogen can affect the efficiency ofNGF binding and regulate NGF sensitivitj' in neu-rotropin targets of adult dorsal root ganglia. Inaddition, estrogen receptors co-localize with recep-tors for NGF in cholinergic neurons of the basalforebrain,* -̂̂ and estrogen differentially regulatesNGF receptor mRNA in adult sensory neu-rons.̂ *'̂ ^
Contribution of the Sympathetic NervousSystem. In addition to the interaction between neu-rochemical agents and gonadal hormones, sex dif-ferences in the structural organization and func-tion of the sympathetic nervous system may alsoexplain, in part, observed gender differences inpain. Berkley'' pointed out that differences in affer-ent input from internal structures to the centralnervous system could not only produce differentforms of visceral pain in females and males, hut
could also result in different emotional conse-quences of pain experiences, assuming that visceralinput is important in the perception of emotion.Many functions of the sympathetic nervous systemhave been reported to be influenced by gender,including lower levels of resting sympathetic activ-ity to skeletal muscles in women than in men, "'̂ ^higher sympathetic output to the skin in women,'"and sex differences in cardiovascular responses tovarious Stressors.^' Other autonomie activities thatare strongly influenced by rbe menstrual cycle andmay be related to cutaneous and muscle painsinclude sweating,^' skin blood flow,̂ -̂̂ '' and pos-tural vasoconstriction reflexes. '̂' In addition, plas-tic changes in the autonomie nervous system mayoccur differently in females than in males. This issupported by data showing that the sprouting ofsympathetic fibers into tbe hippocampus followingneural injury is more restricted in male tban infemale rats.''^ Since plastic cbanges in neural struc-tures are a phenomenon associated witb the devel-opment of cbronic pain, extrapolation of thesedata to humans may explain the large female pre-dominance in the occurrence of chronic pain disor-ders associated with the sympathetic nervous sys-tem, such as sympathetically maintained pain,causalgia, or reflex sympathetic dystrophy.**
Opioid and Non-opioid Analgesia. As part ofthe neural mechanisms that modulate pain signal-ing and modify emotional reactions to pain, intrin-sic descending pain inhibitory systems such asthose inducing opioid and non-opioid analgesiaalso appear to be influenced by both gender andthe action of estrogen and other gonadal hor-mones.̂ ^" '̂' For example, sex differences in the dis-tribution and binding capacities of steroid recep-tors have been identified in many regions of tbecentral nervous system that contribute to the trans-mission and modulation of nociceptive informa-tion.^'''*"'"'"^ Female rats display less analgesicresponse tban male rats to central acting agentssucb as morphine,^^ and their sensitivity to theantinociceptive actions of these drugs varies withthe phases of the estrous cycle.'"^ The sexualdimorphism in response to opioid analgesics hasalso heen ohserved in human studies. However,the gender differences in humans tend to be oppo-site to those found in animals, since tbe adminis-tration of opioid analgesics that act on the kappa-opioid receptor produced better analgesia inwomen as compared witb men.'"*"'**^ While thereason for this contrast between animal andbuman data remains unclear, it is possible tbat theoverall gender differences may be a result of themodulation of the opioid circuitry by bormonal
176 Volume 14, Number3. 2000
Dso/LeResche
Status and chronobiologic factors such as thefemale estrous/menstrual cycle. "̂ " Mogil andKest'"^ suggest that analgesic mechanisms in eachsex may also have distinct and independent neu-ronal circuitry, since non-opioid stress-inducedanalgesia is mediated by N-methyl-D-aspartatereceptors in male but in not female mice,̂ ^ and anautosomal genetic locus that accounts for 25% ofthe overall variance in the trait in female mice hasheen identified.'"^ The neuroanatomic, neuro-chemical, and neurophysiologic gender differencesin opioid and non-opioid analgesia have been thor-oughly reviewed by Fillingim and Maixner.-^
Psychosocial Factors
In addition to the biologic factors mentionedabove, gender differences in pain report may beattributable to a number of psychologic and socialfaaors.
1. Males and females may differ in their sensitivityto physiologic signals. Once signals are per-ceived, there may be sex differences in whetheror not the signal is labeled a symptom.
2.Differences in the rearing of boys and girls mayinfluence the readiness of the sexes to expresspain.
3. Different occupational roles for men and womencarry with them exposure to different risks fordeveloping a variety of pain conditions.
4. Stress may exacerbate pain, and it is possiblethat men and women are exposed to differenttypes and levels of psychosocial stress.
5. Opportunities for different pain experiences mayprovide different opportunities for learningabout pain.
In this section, we review the evidence for each ofthese factors.
A number of lines of evidence suggest thatwomen may be more sensitive to painful stimulithan men. Several excellent recent reviews by painresearchers from different disciplines '̂'''̂ ^ all findsupport for this conclusion. Women seem to showgreater sensitivity and/or greater physiologicresponsiveness to stimuli in a number of other sen-sory modalities (eg, visual, auditory, tactile)'^"'"'as well as pain. Thus, it is plausible that anincreased sensitivity to pain in women is simply aresult of women having a more sensitive percep-tual apparatus than men. Whether or not this per-ceptual sensitivity is attributable to hormonalcauses remains to be investigated.
There is some evidence that men and womendiffer in their cognitive and emotional experiences
of pain. Once a change in physiologic signals isdetected, the change may be labeled as a symptomor simply as a change. Some evidence indicatesthat women are more likely than men to perceivephysical sensations as indicative of illness."^Furthermore, given that a sensation is classified asa symptom, ways of coping with that symptommay differ by gender. Specifically, women may bemore likely to regard pain as serious and attend topain sooner, in an effort to minimize its intrusive-ness, because they have multiple primary role obli-gations, from household management to child careand increased social responsibilities.- Prevention ofmultiple role disruption may also motivate womento use more social and professional support and touse short-term disability to avoid long-term dis-ability. The same review describes different copingstrategies for men, including denial, talking theproblem down, and using ten s i on-reducing activi-ties such as alcohol consumption, smoking, ordrug abuse, unless pain interferes with workresponsibilities.
There is, however, some contradictory evidenceconcerning whether health care use for pain differsin males and females. In the only study we couldidentify that examined predictors of trearment-seeking specifically for pain,-^ the major predictorsof use of health care in both genders were painseverity and persistence. That is, persons withmore severe, persistent pain were more likely toseek care. For some pain conditions, such as TMDpain, women in the community experience pain ofgreater average severity than do men. If it is truethat pain severity drives treatment-seeking andthat women, on average, experience more severepain than men, we would expect that the levels ofpain and pain-telated symptoms among men andwomen seeking pain treatment would he fairiycomparable, although women could outnumbermen in treatment settings. One study examinedthis question for TMD and, in fact, found thatpain levels, pain-related signs and symptoms, andpsychosocial profiles were roughly comparable formale and female patients seen in the same treat-ment setting.^'^
The observation that boys and girls are reareddifferently and given different expectations forpain-related behavior (eg, "big boys don't cry") isso obvious that there has been little research thatactually documents these socialization patternsand their influences on adult behavior. However,there is a body of research concerning the nonver-bal expression of emotions (including some studiesof the expression of pain). A systematic review ofthese studies of nonverbal behavior"'' indicates
Journal of Orofacisl Pain 177
Dao/LeResche
that sex differences in expressiveness are smallamong preschool children but are much greater inadults. This finding is certainly compatible withthe hypothesis that the reinforcement of differentpain behaviors in boys and girls can result in dif-ferent patterns of pain expression among adultmen and women.
Despite recent changes in some societies, menand women still tend to fulfill somewhat differentoccupational roles, as well as different social roleswithin the family. To the extent that differentexposures are associated with traditionally "male"or "female" occupations, different pain conditionswould be more likely to occur in males or females.For example, persons in jobs involving lifting are athigher risk for back pain, wbereas keyboard opera-tors are at higher risk for carpal runnel syndrome.
In addition, the differenr occupational and rolesituations of men and women may be associatedwith different stress levels. One aspect of the psy-chosocial work environment that has been receiv-ing increasing attention in health research is rheconcept of job strain, which is defined as the com-bination of higb job demands and low latitude inmaking decisions. Job strain has been found to beassociated witb myocardial infarction in men"^witb a range of measures of poor health status,including low vitality, poor mental health, andpain in women'""; and with musculoskeletal painof rhe neck, shoulders, and back in both men andwomen.^'^'1^^ In addition, high job strain hasbeen associated with increases in blood pressurein some studies, and one recent investigationfound that among white-collar women, the combi-nation of high job strain and large family respon-sibilities was associated witb significant increasesin diurnal blood pressure measurements.•'̂ ^ If per-sons of one sex or rhe other are more likely to beemployed in occupations with high job strain, thisfactor might interact with gender to increase theprobability of developing or maintaining a paincondition.
Finally, men and women may have differentbencbmarks for reporting pain, related to theirprior pain experience. For example, boys, at leastin earlier generations, were more likely to experi-ence pain from sports injuries than girls. On theother hand, after puberty, women's monthly men-strual cycles provide them with a set of physiologicsignals from their bodies that are not experiencedby men. These physiologic signals {sometimes of apainful nature) could have a sensitizing effect onpain perception'' or result in behavioral and socialrole responses (eg, taking medication, staying inbed) that can generalize to other types of pain.
These hypotheses concerning gender differencesin pain emerge from the concept that men's andwomen's responses to pain may be shaped differ-entially by psychologic and social factors. Weregard these hypotheses as testable scientific ques-tions, for wbich there are currently varying degreesof research evidence. Unforrunately, because paincomplaints are symptoms and frequently cannot besubstantiated by "objective" clinical findings, ahigher prevalence of pain or higher reported levelsof pain in women can reinforce negative stereo-types of women held by some healtb care profes-sionals. A study evaluating tbe contention thatphysicians have prejudicial attitudes toward femalepatients reported the physicians' belief that womenhave more psychosomatic illnesses, more emo-rional lability, and more complaints due to emo-tional factors.-'^" Clearly, the evidence reviewedabove indicates that both biologic and psychoso-cial factors are likely to play a part in gender dif-ferences in pain. Not only are a range of biologic,psychologic, and social factors likely to beinvolved, but tbese factors probably interact inways that are as yet unclear. To suggest thatobserved differences between men and women are"all in the head" {ie, the fault of the patient) issimplistic from a scientific point of view and notconstructive in terms of patient care.
Possible Additional MechanismsUnderlying Gender Differencesin Orofacial Pain
Biologic Factors
In addition to the role of female reproductive hor-mones in pain modulation already discussed, it hasbeen suggested that rhe female predisposition toTMD may be due to the effect of the reproductivehormones on the temporomandibular joint (TMJ)complex. In animals, sexual dimorphism in the dis-tribution of estrogen receptors in the TMJ hasbeen reported in studies showing that estrogenreceptors were found in female^^' but not malebaboons.'^^ In tbe rat, sex hormones can modulatethe collagen and protein content of TMJ discs; thissex difference in the collagen content of TMJ discswas eliminated by castration of both the male andfemale animals.'^^ Estrogen receptors have alsobeen found in the TMJ discs of both asymptomaticmale and female subjects and TMD patients.^^*More recently, an in vitro study showed that estro-gen can modulate the effect of relaxin on theexpression of tissue-degrading enzymes and their
178 Volume 14, Number 3, 2000
Dao/LeResche
inhibitors in fibrocartilagenous cells of the TMJ.'-^Although these findings suggest that the TMJ discmay be a potential target for sex hormones, theirchnical significance remains unclear. It is intetest-Ing to note that relaxin has been implicated in sys-temic ¡oint hypermobility,'--^ a condition thatseems to be more prevalent in women'-'' and thathas been reported (but not proven) to be associ-ated with TMO.!^"-'-*"
Sex differences in the perception of orofacialpain have also been attributed to dysregulation ofthe pain m.odulation system. In addition to thedata showing sex differences in temporal summa-don of thermal pain,-** there is evidence that TMDpatients have enhanced responses to noxious stim-uli'^^ and greater thermal temporal summationthan pain-free subjects.''- The neural mechanismsunderlying these phenomena are as yet unknown.Proposed mechanisms include impairments in cen-tral inhibitoty mechanisms, disorders m pathwaysmodulated by peripheral baroreceptor afferentinput, and alteration in central nervous systemprocesses that regulate the temporal processing ofpain.'^- Whether these mechanisms are generic orspeci6c to orofacial pain also remains to be deter-mined.
Psychosocial Factors
There is little evidence that the psychosocial fac-tors involved in chronic orofacial pain conditionsare quahtatively different from those involved inother chronic pain problems. In contrast, there isevidence that, although TMD pain is on averageless disabhng than back pain and headache, levelsof psychologic distress in persons with a TMD aresimilar to those of persons with other commonchronic pain conditions,' There is also no a priorireason to suspect that perceptual differencesbetween the sexes, cognitive differences m symp-tom labeling and pain coping, or gender differ-ences in pain expression would take differentforms depending on the site of pain. It is possiblethat different occupational and social tole expo-sures for men and women could influence theprevalence of specific orofacial pain conditions.However, we know of no research that specificallyaddresses this question. Thus, at this time, itappears that causes of the higher female-to-maleprevalence ratio for head and face pain than forpain elsewhere in the body are best sought in chebiologic rather than the psychosocial realm.
Summary and Conclusion
An analysis of the literature indicates that forendogenous pain, women tend to report higherpain levels and pain in more bodily regions thanmen. For no apparent reason, there are also sexdifferences in the manifestations of signs andsymptoms of various pain disorders. Systematicinvestigation of gender differences in pain is a rela-tively new field. It is not yet known why somechronic pain conditions are predominant in men,while others (in particular those disorders thatinvolve the craniofacia! area or are modulated bythe sympathetic nervous system) are more commonin women. It is also unclear why some types ofpain vary with hormonal fluctuations. Neverthe-less, several interesting hypotheses reviewed m thispaper are under active investigation.
Laboratory experiments have substantiated thegender disparity in responses co noxious stimuli.However, differences exist only for certain types ofstimuli, mean differences between the sexes aregenerally small, and results are often inconsistentbetween studies. Therefore, the relevance of theselaboratory findings to clinical conditions has beenquestioned. There are also other reasons why thesedata should be interpreted with caution. First,experimental pains are induced under acute condi-tions and do not reflect the persistent or recurrentnature of chronic pain conditions. Thus, they donot constitute a threat to the subject's health orcause a state of distress or disability that mayaffect the subject's perception and description ofthe pain signals. Second, the majoriry of experi-mental stimuli are delivered to the skin, whilechronic endogenous pains are felt mostly in deepstructures such as muscles, joints, or visceralorgans. Third, it is difficult to attribute the differ-ences to gender only, given the numerous interact-ing variables that may shape the responses to pain,as listed in Figs 1 and 2. Fourth, the experimentsare often carried out m healthy asymptomatic sub-jects, in whom changes in the peripheral and cen-tral nervous systems potentially induced bychronic pain have not taken place. In other words,as we have noted elsewhere,̂ "* to understand thewhole spectrum of pain response in male andfemale humans, pain must be studied in popula-tions, not only m petsons seeking treatment forpain, and not only m those who tj'pically partici-pate in laboratory pain research.
While evidence for sex differences in pain hasnot been established beyond doubt, distinctanatomic and hormonal features in women andmen provide compelling clues that their pain might
Joumal of Orofacial Pa¡n 179
Dao/LeResche
be modulated in a differential manner by a numberof biologic factors. The cyclic fluctuations of vari-ous pain disorders across the menstrual cycle,along with gender differences in the compositionof gonadal hormones, give rise to a number ofhypotheses related to the actions of estrogen, pro-gesterone, and testosterone. These hypotheses havebeen substantiated with clinical and experimentaldata on the interactions of the gonadal hormoneswith various neuroactive agents and on their effecton both opioid and non-opioid analgesia. In addi-tion, sex differences in the structural organizationand operation of the sympathetic nervous systemmay account, in part, for the apparent gender dif-ferences in pain. More recently, direct evidence forgender differences in pain processing has beenreported. For instance, Mogil et al'^^ presentedevidence illustrating the role of genetic backgroundin the perception of pain. Gender differences inforebrain cerebral activation patterns of the brainduring pain perception have also been reported. ' ^*
Several hypotheses concerning differential psy-chosocial influences on pain in women and men—notably, differences in perception, appraisal, pain-related behavior, and environmental influences—have also been reviewed here. Although infor-mation supporting the observation of sex differ-ences in pain continues to emerge, it is still frag-mented. While debates about the biologic orpsychosocial nature of gender differences in paincontinue, the answer is unlikely to be one or theother, since these aspects are undoubtedly interre-lated. Yet it is alarming to see how clinical deci-sions, probably influenced more by personalbeliefs than by scientific data on gender differ-ences, may lead to inadequate treatment of pain inwomen. For instance, nurses' choices of initialdoses of analgesic after appendectomy may beaffected by the patient's gender, potentially caus-ing inadequate analgesia in women."^ Cleeland etal'^^ reported that being female was a significantpredictor of inadequate pain management inpatients with metastatic cancer. Although coro-nary artery disease is the number one cause ofmortality in women, those women with new-onsetchest pain who present with similar symptoms asmen are approached, diagnosed, and treated lessaggressively than men.'-''' Similarly, in an emer-gency setting, women with acute non-pleuritic andnon-traumatic chest pain were evaluated and man-aged less aggressively than men.-̂ ^̂ These datastrongly suggest that the available information ongender differences should be interpreted with cau-tion. In other words, simply because women aremore likely to report pain than men and on aver-
age they report higher levels of pain than men,does not mean that women's pain reports shouldbe discounted. Rather, evaluation and treatment ofpain patients should be performed on an individ-ual basis. In the treatment context, whether genderdifferences in pain exist is perhaps not the mainissue; rather, our ultimate objective is to use all theavailable information about a patient, mcludinghis or her gender, in a judicious manner toimprove treatment strategies and the quality of lifeof those who experience pain.
References
1. Von Korff M, Dworkin SF, LeResche L, Kruger A. An epi-demjologic comparison of pain complaints. Pain1988;32:173-183.
2. Unruh AM. Gender variations in clinical pain experience.Pain 1996;65:123-167.
3. Andersson HI, Ejlertsson G, Leden I, Rosenberg G.Chronic pain in a geographically defined general popula-tions Studies of differences in age, gender, social class, andpain localization. Clin J Pain 1993;9:174-182.
4. Berkley KJ. Sex differences in pain. Behav Brain Sei1997;20:371-3SO.
5. Scheurer PA, Firestone AR, Burgin WB. Perception of painas a result of orthodontic treatment wich fixed appliances.Eur J Orthod 1996;18;349-3S7,
6. LeResche L. Epidemiologie perspectives on sex differencesin pain. In: Fillingim R (ed). Sex, Gender and Pain: Fromthe Benchrop to the Glinic. Searcle: lASP Press {in press).
7. LeResche L. Gender considerations in the epidemiology ofpain. In: Grombie IK, Croft PR, Linton SJ, LeResche L,Von Korff M |eds}. Epidemiology of Pain. Seattle: lASPPress, 1999.
8. LeResche L. Epidemiology of temporomandibular disor-ders: Implications for the investigation of etiologic factors.Grit Rev Oral Biol Med 1997;8:291-30S.
9. Katusic S, Beard CM, Bergscralh E. Kurlan_d LT. Incidenceand clinical features of trigémina! neuralgia, Rochester,Minnesota, 1945-19S4. Ann Neuro! 1990;27:89-95.
10. Rothman KJ, Monson RR. Epidemiology of trigeminalneuralgia. J Ghronic Dis 1973;26:3-12.
11. Lipton JA, Ship JA, Larach-Robinson D, Estimated preva-lence and distribution of reported orofacial pain in theUnited States. J Am Dent Assoc 1993;124:115-121.
12. Ta mm iai a-Sal on en T, Hiidenkari T, Parvinen T. Burningmouth in a Finnish adult population. Community DentOral Epidemiol 1993;21:67-71.
13. Locker D, Grushka M. Prevalence of ora) and facial painand discornfort: Preliminary results of a mail survey.Gommunity Dent Oral Epidemiol 1987;15:169-172.
14. Van Der Donk J, Schouten JS, Passchier J, van RomundeLK, Valkenburg HA. The associations of neck pain withradiological abnormalities of the cervical spine and per-sonality traits in a general population. J Rheuniatol
IS. Rasmussen BK, Jensen R, Schroll M, Olesen J. Inter-relations between migraine and tension-type headache inthe general population. Arch Neurol 1992;49:914-918.
180 Volume 14. Number 3, 2000
Dao/LeResche
16. Goldberg RJ, O'Donnell C, Yarzebski J, Bjgeluw C,Savageau J, Gore JM. Sex differences in symprom presen-tation associated with acute myocardial infarction; A pop-ulation-based perspective. Am Heart J 1998;I36:189-135,
17. Walsh K, Cruddüs M, Coggon D, Interaction of heightand mechanical loading of the spine in the development oflow-back pain. Scand J Work Environ HealthÍ991;17:42(M24.
18. Eskelinen M, Ikonen J, Lipponen P. Sex-specific diagnosticscores for acute appendicitis. Scand J Gastroenterol19i'4;29;59-66.
19. Sullivan AK, Holdright DR, Wright CA, Sparrow JL,Cunningham D, Fo.t KM, Chest pain m women: Clinical,investigative, and prognostic features. Br Med J1994308883886
20. Garber CE. Carleton RA, Heller GV. Comparison of"Rose Questionnaire Angina" to e.\ercise thallium scintig-taphy: Different findings in males and females. J ClinEpidemiol 1992;45:715-720.
21. Turk DC, Mehack R. Handbook of Pain Assessment,Nevu York: Guilford Press, 1992.
22. Agerberg G, Carlsson GE. Functional disorders of chemasticatory system. I. Distribution of symptoms accordingto age and sex as judged from investigation by question-naire. Acta Odontol Scand 1972;30:597-613.
23. Von Korff M, Wagner EH, Dworkin SF. Saunders KW.Chronic pain and ambulatory bealth care. PsycbosomMed 1991;53:61-79.
24. Weir R. Browne G, Tunks E, Gafni A, Roberts J. Genderdifferences in psychosocial adjustment to cbronic pain andexpenditures for health care services used. Clin J Pain1996;12:2 77-290.
25. Lioton SJ, Heilsing AL, Hallden K. A population-basedstudy of spinal pain among 35-45-year-old individuals.Prevalence, sick leave, and healtb care use. Spine 1998;23:1457-1463.
26. Fillingim RB, Malxner W. Gender differences in theresponses Co noxious stimuli. Pain Forum 1995;4:209-221.
27. Laucenbachcr S, Rollman GB. Sex differences in respon-siveness to painful and non-painful stimuli are dependentupon the srimulation method. Pain I993;53:255-264.
28. Fillingim RB, MaL>:ner W, Kincaid 5, Silva S, Sex differ-ences in temporal summation but not sensory-discrimina-dve processing of thermal pain. Pain 1998;75:121-127.
29. Riley JL, Robinson ME, Wise EA, Myers CD, FillingimRB. Sex differences in tbe perception of noxious experi-mental stimuli: A meta.analysis. Pain I998:74;181-187.
30. Levine FM, De Simone LL. The effects of experimentergender on pain report in male and female subjects. Pain1991;44:69-72.
31. Blitz B, Dinnerstein AJ. Effects of different types ofinstructions on pain parameters, J Abnorm Psychol19é8;73:276-280.
32. LeResche L, Burgess J, Dworkin SF. Reliability of visualanalog and verbal descriptor scales for "objective" mea-surement of cemporoniandibular disorder pain. J Dent Res1988;67:33-36.
33. Blitz B, Dinnerbtein AJ. Role of artentional focus in painperception: Manipulation of response to noxious stitnula-tion by instructions. J Abnorm Psychol 1971;77:42-45.
34. LeRescbe L. Gender differences in pain. Epidemiologieperspectives. Paiti Forum 1995;4:228-230.
35. Bayer TL, Baer PE, Early C. Situational and psycbophysio-logical factors in psychologically induced pain. Pain1991;44:45-50.
36. Shiomi K, Relations of pain threshold and pain tolerancein cold wacet with scotes on Maudsley PersonalityInventory and Manifest Anxiety Scale. Percept Mot Skills1978;47:1155-I158.
37. Arntz A, Dreessen L, Dejong P. The influence of anxietyon pain: Attentional and attributional mediators Pain1994;56i307-314,
38. Kepler KL, Kesc B, Kiefel JM, Cooper ML, Bodnat RJ.Roles of gender, gonadectomy and estrous phase in theanalgesic effects of i n trac ere bro ventricular morphine inrats. Pharmacol Biochem Behav 1989;34:119-127.
39. Roilman GB, Gender differences in pain. Role of anxiety.Pain Forum 1995;4:231-234.
4Ü. Marcus DA, Interrelationships of neurochemicals, oestro-gen, and recurring headache. Pain 1995;62:129-I39,
41. Dao TTT, Knight K, Ton-That V. Modulation of myofas-cia! pain patterns by oral contraceptives: A preliminaryreport |abstract|. J Dent Res 1997;76(special issue):148,
42. Ahmed SA, Peahale WJ, Talal N. Sex hormones, immuneresponses, and autoimmune diseases. Am J Patho!1985;]21:531-551,
43. Case AM, Reid RL. Effects of the menstrual cycle on med-ical disorders. Arch Intcm Med 1998;158:1405-1412.
44. Ayiward M, Holly F. Parker RJ, An evaluadon of clinicalresponse to piperazine ocstrone sulphate ("Harmogen"! inmenopausal patients. Curr Med Res Opin 1974;2Í41 7-423.
45. Kudrovi' L. The relationship of headache frequency to hor-mone use in migraine. Headache 1975;April:36-40.
46. Murray SC, Muse KN. Effective treatment of severe men-strual migraine headaches with gon a dotrop in-releasinghormone agonist and "add-back" therapy. Fértil Steril1997;67:390-393,
47. Dao TT, Knight K, Ton-Tbat V. Modulation of myofas-cial pain by the teproductive hormones: A preliminaryreport,JProsthetDentl998;79:663-670.
48. LeResche L, Saunders K, Barlow W, Von Korff M,Dworkin SF. Does oral contraceptive use increase the riskoí temporomandibukr (TMD) pain? In: lASP ScientificProgram Committee. 7th World Congress on Pain:Abstracts: August 22-27, 1993, Paris, France. Seattle:lASP Publications. 1993:294-295.
49. LeResche L, Saunders K, Von Korff MR, Barlow W,Dworkin SF. Use of exogenous hormones and risk of tem-poromandibular disorder pain. Pain 1997;69:153-160.
50. Brynhildsen JO, Bjors E, Skarsgard C, Hammar ML. Ishormone replacetnent therapy a risk factor for low backpain among postmenopausal women? Spine 1998;23:809-813,
51. Wreje U, Isacsson D, Aberg H. Oral contraceptives andback pain in women in a Swedish community. Inl JEpidemiol 1997;26:71-.74.
52. Gooikasian P. Cyclic changes in pain perception: An ROCanalysis. Percept Psychophys 19S0;27:499-504,
53. Gooikasian P. An ROC analysis of pain teactions in dys.menorrheic and non dysmenottheic women. PerceptPsychophy; !983;34:381-386.
54. Fillingim RB, Maixner W, Girdler SS, Light KC, HatrisMB, Sheps DS, Mason GA. Ischémie but nor thermal painsensitivity varies a c toss the menstrual cycle. Psychos o mMed 1997;59:512-520.
55. Giamberardino MA, Berkley KJ, lezïi S, De Bigontina P,Vecchiet L. Pain threshold variations in somatic wall tis-sues as a function of menstrual cycle, segmental site andtissue depth in non-dysmenorrheic women, dysmenorrheicwomen and men. Pain 1997;71:187-197.
Joumal of Otofacial Pain 181
Dao/LeResche
56. Herren RG. The effects of high and low sex hormone con-centration on the two-point threshold of pain and Couchupon tactile sensiljviry, J Exp Psychol 1933;16:324-327.
57. Kenshalo DR. Changes in the cool threshold associatedwith phases of the menstrual cycle. Appl Physiol1966;21;1031-1039.
58. Prncacci P, Corte MD, Zoppi M, Maresca M. Rhythmicchanges of the cutaneous pain threshold in man. A generalview. Chronobioiogia 1973;l:77-96.
59.Tedford WH Jr, Warren DE, Flynn WE. Alteration ofshock aversion threslinid during the menstrual cycle.Percept Psychophys 1977;21:193-196.
60. K-ucimietcïyk AR, Adams HE. Autonomie arousal andpain sensitivity in women with premenstrual syndrome atdifferent phase? of the menstrual cycle. ) Psychosom Res1986;30:421-428.
61. Hapidou EG, De Catanzaro D. Sensirivitj' to cold pressorpain in dysmenorrheic and non-dysmcnorrheic women as afunction of menstrual cycle phase. Pain 1988;34:2?7-283.
62. Veith JL, Anderson J, Slade SA, Thompson P, Laugel G,Getilaf S. Plasma ß-endorphm, pam thresholds and anxi-ety levels across rhe mensrrual cycle. Physiol Behav1984;32:31-34.
63. Ainodei N, Nekon-Gray RO. Reactions of dysmenorrheicand nondysmenorrheic women to experimentally inducedpain throughout the menstrual cycle. J Behav Med1989;12^373-3 85.
64. Hapidou EG, Rollman GB. Menstrual cycle modulation oftender points. Pain 1998;77:I51-161.
65. Martineï-Gomei M, Cruz Y, Salas M, Hudson R, PachecoP. Assessing pain threshold in the rat: Changes with estrusand time of day. Physiol Behav 1994;55:65]-657.
66. Gint?ler AR, Bohan MC. Pain thresholds are elevated dur-ing pseudopregnancy. Btain Res 1990;507:3]2-3Í6.
67. McCarthy MM, Caha M, Komisaruk BR, Beyer C.Modulation by estrogen and progesterone of the effect ofmuscimol on nociception in the spinal cord. PharmacolBiochem Behav 1990;37:123-128.
68. Guicheney P, Leger D, Barrât J, Trévoux R, De LignieresB, Roques P, Platelet serotonin content and plasma trypto-phan in peti- and postmenopausal women: Variationswith plasma oestrogen levels and depressive symptoms.Eur J Clin Invest 1988;18:297-304,
69. Maswood S, Stewart G, Uphouse L. Gender and estrouscycle effects of the 5-HTlA agonist, 8-OH-DPAT, onhypothalamic serotonin. Pharmacol Biochem Behav
70. Gundiah C, Simon LD, Auerhach SB. Differences in hypo-thalamic serotonin between escrous phases and gender: Anin VIVO microdialysis study. Brain Res 1998;785:91-96.
71. Heritage AS, Stumpf WE, Sar M, Grant L. Brainstem cate-cholamine neurons are target sites for sex steroid hor-mones. Science 1980i207:1377-1379,
72. Ramsay B, Johnson MR, Leone AM, Steer PJ. The effectof exogenous oestrogen on nitric oxide production inwomen: A placebo controlled crossover study. Br J ObstetGynaecol 1995; 102:417-419.
73. Sudhir K, Jennings GL, Funder JW, Komesaroff PA.Estrogen enhances basal nitric oxide release in rhe forearmvasculature in perimenopausal women, Hypertensioti1996;28;330-334.
74. Imthurn B, Rosselli M, Jaeger AW, Keller PJ, Dubey RK.Differential effects of hormone-replacement therapy onendogenous nitric OKide (nitrite/nitrate) levels in post-menopausal women substituted with 17 beta-estradiolvalerate and cyproterone acetate or medroxyptogesteroneacetate. J Clin Endocrino! Metab 1997;82:388-394.
75. Meiler ST, Gebhart GF. Nitric oxide (NO) and nocicep-tive processing in the spinal cord. Pain 1993;52:127-136,
76. Meiler ST, Gebhart GF. Spinal mediators of hyperalgesia.Drugs I994;47¡suppl5):10-20.
77. Olesen J, Iversen HK, Thomsen LL. Nitric oxide supersen-sitivity: A possible molecular mechanism of migraine pain.Neuroreport 1993;4:1027-1030.
78. Olesen J, Thomsen LL, Iversen H. Nitric oxide is a keymolecule in migraine and other vascular headaches.Trends Pharmacol Sci 1994;15:149-153.
79. lversen HK. Experimental headache in humans.Cephalalgia 199S;15:281-287.
80. Thomsen LL, lversen HK, Brinck TA, Olesen J. Arterialsupersensitiv icy to nitric oxide (nitroglycerinj in migrainesufferets. Cephalalgia 1993;13:395-399.
81. Thomsen LL, Brennum J, lversen HK, Olesen J. Effect of anitric oxide donor (glyceryl trinitratej on nociceptivethresholds in man. Cephalalgia 1996;16il69-174.
82. Stohler CS. Masticatory myalgias. Emphasis on the nervegrowth factor-estrogen link. Pain Forum 1997;6T176-180 .
83. Woolf CJ, Safieh-Garahedian B, Ma QP, Crllly P, WinterJ. Nerve growth factor contributes to the generation ofinflammatory sensory hyperiensitivity. Neiiroscience1994;62:327-33].
84. Petty BG, Cornblath DR, Adornato BT, Chaudhry V,Flexner C, Wachsman M, er al. The effect of systemicallyadmmistered recombinant human nerve growth factor inhealthy human subjects. Ami Neurol 1994;36:244-246.
85. Toran-Allerand CD, Miranda RC, Bentham WD, SohrabjiF, Brown TJ, Hochberg RB, MacLusky NJ, Estrogenreceptors colocalize with low-affinity nerve growth factorreceptors in cholinergic neurons of the basal forebrain.Proc Nati Acad Sei USA 1 9 9 2 ; 8 9 Í 4 6 6 8 ^ 6 7 2 .
86. Sohrabji F, Miranda RC, Toran-Allerand CD. Estrogendifferentially regulates estrogen and nerve growth factorreceptor mRNAs in adult sensory neurons. J Neurosci1994;14:459-471.
87. Toran-Allerand CD. Mechanisms of estrogen action dur-ing neural development: Mediation by interactions withthe neurotrophins and their receptors? J Steroid BiochemMolBiol1996;5Ê:169-17S.
88. Ng AV, Callisrer R, Johnson DG, Seals DR. Age and gen-der influence muscle sympathetic nerve activity at rest inhealthy humans. Hypertension 1993;21:498-503.
89. Ettinger SM, Silber DH, Collins BG, Gray KS, Sutiiff G,Whisler SK, et al. Influences of gender on sympatheticnerve responses to static exercise. J Appl Physiol 1996;80:245-251.
9Ü. Cooke JP, Creager MA, Osmundson PJ, Shepherd JT, Seïdifferences in control of cutaneous blood flow. Circulation1990;82:1607-1615.
91. Maixner W, Humphrey C. Gender differences in pain andcardiovascular responses to forearm ischemia. Clin J Pain1993;9:16-25.
92. Frascatolo P, Schutz Y, Jequier E. Influence of the men-strual cycle on the sweating response measured by directcalorimetry in women exposed to warm environmentalconditions. Eur J Appl Physiol 1992;64:449-454.
182 Volume 14, Number 3. 2000
Dao/LeResche
93. Bartelink ML. Wo Hers hei m H, Thecuwes A, van Duren D,Thien T. Changes in skin blood ñoiv during rhe mensirualcycle: The influente of the menstrual cycle on [he periph-eral circulation in healthy female volunteers. Clin Sei
94. Frascarolo P. Schuti Y, Jequier E. Decreased thermal con-duaance during the luteal phase ot the menstrual cycle inwomen, J Appl Physiol 1990:69:2029-2033,
95. Hassan AA, Carter G, Tooke JE. Postural vasoconstrictionin women duting the normal menstrual cycle. Clin Sei1 9 9 0 : 7 8 : J 9 - - Í 7 .
96. Milner TA, Loy R. (nieraction of age and sex in sympa-thetic axon ingroivth into the hippocampus following sep-tal atfetent damage, Anat Embryol 19S0;161:li9-168.
97. Ryan SM, Maier SF, The estrous cycle and estrogen mod-ulate stress-induced analgesia. Behav Neurosci 19S8;102:371-380-
98. Ralka A, Simpkins JW. Effects of escradiol and progesteroneon the sensitivit)' to pain and on morphine-induced antinoci-ception in female rats. Horm Behav l99I;2J:217-228.
99. Mogil JS, Sternberg WF, Kest B, Marek P, Liebeskind JC.Sex differences in the antagonism of swim stress-inducedanalgesia: Effects of gonadectomy and estrogen replace-ment, Paul 1993p3:17-25.
100. Brown TJ, Hochberg RB, Zielinski JE, MacLusky NJ.Regional sex differences m cell nuclear estrogen-bindmgcapacity in the rac hypothalamus and preoptic area.Endocrinology 1988;123:1761-1770.
IOL Morrell JI, McGinty JF, Pfaff DW. A subset of beta-endor-phin ot draorphin containing neurons in the medial basalhypothalamus accumulates estradiol. Neuroendocrinology
102. Morrell JL Krieger MS, Pfaff DW, Quantitative autotadio-graphic analysis of estradiol retention by cells in the pre-optic area, hypothalamus and amygdala. Esp Brain Res1986:62:343-354.
103. Banerjee P, Cfiatterjee T, Ghosh J. Ovariati steroids andmodulation of morphine-induced analgesia and catalepsyin female rats. Em^J Pharmacol 1983;96:291-294.
104. Gear RW, Gordon NC, Heller PH, Paul S, Miaskowski C,Levine JD. Gender difference in analgesic response to thekappa-opioid pentazocine. Neurosci Lett 1996;205i207-209.
105. Miaskowski C, Levine JD. Does opioid analgesia show agender preference for females? Pain Forum 1999^8:34-44.
106. Gear RW, Miaskowski C, Gordon NC, Paul SM, HellerPH, Levine JD. The kappa opioid nalhuphine producesgender- and dose-dependent analgesia and antianalgesia inpatients with postoperative pain. Pain 1999;83:339-345.
107. Page GG. The multi-issue nature of sex differences in opi-oid analgesia. Pain Forum 1999;8:45-47.
IOS. Mogil JS, Kest B. Sex differences in opioid analgesia. Ofmice and women. Pain Forum 1999^8:48-50.
109. Mogil JS, Richards SP, OToole LA, Helms ML, MitchellSR, Kest B, Belknap JK. Identification of a sex-specificquantitative trait locus mediating nonopioid stress-induced analgesia in female mice, j Neurosci 1997;17:7995-8002.
110. Gandelman R. Gonadal hornjones and sensory function.Neurosa Biobehav Rev Í983;7:l-17.
l l l .Velle W. Sex differences in sensory functions, PerspectBiol Med 1987;30:490-522.
112, Gijsbers van Wijk CM, van Vliet KP, Kolk AM, EveraerdWT. Symptom sensitivity and sex differences in physicalmorbidity: A review of health surveys in the United Statesand The Netherlands. Women Health 1991;17:91-124.
113. Bush FM, Harkins SW, Harrington WG, Price DD,Analysis of gender effects on pain perception and symp-tom presentation in temporomandibular pain. PainÍ993;53:73-S0.
114. Hall J. Nonverbal Sex Differences. Baltimore: JohnHopkins University Press, 1984.
115. Karasek RA, Theorell T, Schwartz JE, Schnall PL, PieperCF, Michela JL, Job characteristics in relation to theprevalence of myocardial infarction in the US HealthExamination Survey (HES) and the Health and NutritionExamination Survey (HANES), Am J Puhlic Health1988;78:910-91S.
116. Amick BC lU, Kawachi 1, Coakley EH, Lerner D, LevineS, Colditz GA. Relationship of job strain and iso-strain tohealth status in a cohort of women in the United States.ScandJ Work Environ Health 1998;24:54-61.
117. Hagen KB, Magnus P, Veileseti K. Neck/shoulder andlow-hack disorders in the forestry industry: Relationshipto work tasks and perceived psychosocial job stress.Ergonomics 1998;41:1510-1518.
118. Josephson M, Lagerstrom M, Hagberg M, "Wigaeus HE.Muículoskeletal symptoms and job strain among nursingpersonnel: A study over a three-year period. OccupEnviron Med 1997;54í681-685.
119. Brisson C, Laflamme N, Moisan J, Milot A, Masse B,Vezina M. Effect of family responsibilities and job strainon ambulatory blood pressure among white-collarwomen. Psychosom Med 1999;61:205-213.
120. Colameco S, Becker LA, Simpson M. Sex bias in theassessment of patient complaints. J Eam Pract 1983;16:1117-1121.
121. Aufdemorte TB, Van Sickels JE, Dolwick MF, SheridanPJ, Holt GR, Aragon SB, Gates G.\. Estrogen receptors inthe ternporomandibular joint of the baboon {Papio cyno-cephahn): An autoradiographic study. Otal Surg OralMed Oral Pathol 1986^61:307-314.
122. Milam SB, Aufdemorte TB, Sheridan PJ, Triplett RG, VanSitkels JE, Holt GR. Sexual dimorphism in the distribu-tion of estrogen receptors in the temporomandibular jointcomplex of the baboon. Oral Surg Oral Med Oral Pathol1987;64:527-532.
123. Abubaker AO, Hebda PC, Gunsolley JN. Effects of sexhormones on protein and collagen content of the temporo-mandibular joint disc of the rat. J Oral Maxillofac Surg1996;54:721-727.
124. Abubaker AO, Raslan WF, Sotereanos GC. Estrogen andprogesterone receptors in tempo rom andibiilat joint discsof symptomatic and asymptomatic persons: A preliminarystudy, J Oral Maxillofac Surg 1993;51:lÜ96-1100.
125. Kapila S, Xie Y. Targeted induction of collagenase andstromelysin by relaxin in unptimed and beta-estradiol-primed dianhrodial joint fibrocartilaginous cells but notin synoviocytes. Lab Invest 1998;78:925-938.
126. Larsson LG, Baum J, Mudholkat GS. Hypermobility:Features and differential incidence between the sexes.Arthritis Rheum 1987;30:1426-1430.
127. Harinstein D, Buckingham RE, Braun T, Oral K, BaumanDH, Killian PJ, Bidula LP. Systemic joint laxity (the hyper-mobile )oint syndrome) is associated with temporo-mandibular joint dysfunction. Arthritis Rheum 1988;31:1259-1264.
128. Bates RE Jr, Stewart CM, Atkinson WB. The relationshipbetween internal derangements of the temporomandibularjoint and systemic joint laxity. J Am Dent Assoc1984;109:446-447.
Journal of Orofacial Pain 183
Dao/LeResche and Eli
129. West:ling L. Ctaniomandibuiar disorders and general joinimobilitj'. Acta Odontol Scaiid 1989:47;293-299.
130. Westling L, Carlsson GE, Hdkiino M. Background factorsin craniomandibular disorders with special reference togeneral joint hyperniobility, parafunclion, and trauma. JCraniomandib Disord Facial Oral Pain 1990;4:89-98.
131. Maixner W, Fillingim R, Euoker D, Sigurdsson A. Sensi-tivity of patients with painful temporcimandibiilar disordersto experimentally evoked pain. Pain 1995;63:341-351.
132. Maixner W, Fillingim R, Sigurdsson A, Kincaid S, Silva S.Sensitivity of patients with painful remporomandibulardisorders to experitnentally evoked paini Evidence foealtered temporal summation of pain. Pain 1998;76:71-81.
133. Mogil JS, Richards SP, OToole LA, Helms ML. MitchellSR, Belknap JK. Genetic sensitivity to hot-plate nocicep-tion in DBA/2J and C57BL/6J inbred mouse strains:Possible sex-specific mediation by delta2-opioid receptors.Pain 1997;70:267-277.
134. Paulson PE, Minoshima S, Morrow TJ, Casey KL. Genderdifferences in pain perception and patterns of cerebralactivation during noxious heat stimulation in humans.Pain 1998;76:223-229,
135. Vallerand AH. Gender differences in pain. Image J NursSch 1995;27:235-237.
136. Gleeland CS, Gonin R, Hatfield AK, Edmonson JH, BlumRH, Stewart JA, Pandya Kj. Pain and irs treatment in out-patients with metasratic cancer. N Eng J Med 1994;330:592-596,
137. Lehmann JB, Wehner PS, Lehmann GU, Savory LM.Gender bias in the evaluation of chest pain in the emer-gency department. Am J Cardiol 1996;77:641-644.
138. Heston TF, Lewis LM. Gender bias in the evaluation andmanagement of acute nonttaumatic chest pain. The St.Louis Emergency Physicians' Association Restarth Group.FamPractResJ l992;12i3S3-389.
CRITICAL COMiMENTARY 1
CENDER DIFFERENCES IN PAIN
liana Eli. DMDAssociate ProfessorDepartment of Occlusion and Behavioral SciencesSchool of Dental MedicineTel Aviv UniversityTel Aviv. IsraelFax. -^972-3-6409250E-mail: [email protected]
The comprehensive review by Drs Dao andLeResche' concernmg gender differences inpain is a valuable addition to those recently
published in the scientific literature.^"'' As yet,there are no dcfiuite conclusions regarding theinteractions between pain and gender-related fac-tors in this relatively recent and rapidly expandingarea of research. The uniqueness of this focus arti-cle lies in the attempt of Dao and LeResche tosummarize the existing knowledge with regard tootofacial pain conditions. The multiple biologicand psychosocial factors that contribute to genderdifferences in pain are reviewed. I would like toadd several comments on the psychosocial natureof those differences.
Pain (acute and chronic] is a complex experienceof a multidisciphnary nature, which is always suh-jective and always associated with emotional andcognitive factors. The mere activity in the nocicep-tor and iiociceptive pathways by a noxious stimu-Ins is not pain, which always encompasses a psy-chologic state.^ Pain is strongly affected by stress,fear, anxiety, mood, control, attention, expecta-tions, modehng, suggestions, and sociocultural fac-tors. Men and women differ in their pain percep-tion and reaction according to tbeir accepted socialroles and individual cognitive and emotional fac-tors. Moreover, one may react differently to simi-lar pain stimulation under different conditions.
1 8 4 Volume 14, Number 3, 2000
Related Documents