GA II 1 Glutaric Aciduria type II a Fatty acid oxidation defect NORAH A A KHATHLAN MD Consultant Pediatric Intensivist Director PICU 04/ 2007

GA II1 Glutaric Aciduria type II a Fatty acid oxidation defect NORAH A A KHATHLAN MD Consultant Pediatric Intensivist Director PICU 04/ 2007.
Dec 21, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

GA II 1
Glutaric Aciduria type II
a Fatty acid oxidation defect
NORAH A A KHATHLAN MD
Consultant Pediatric Intensivist
Director PICU
04/ 2007
GA II 2
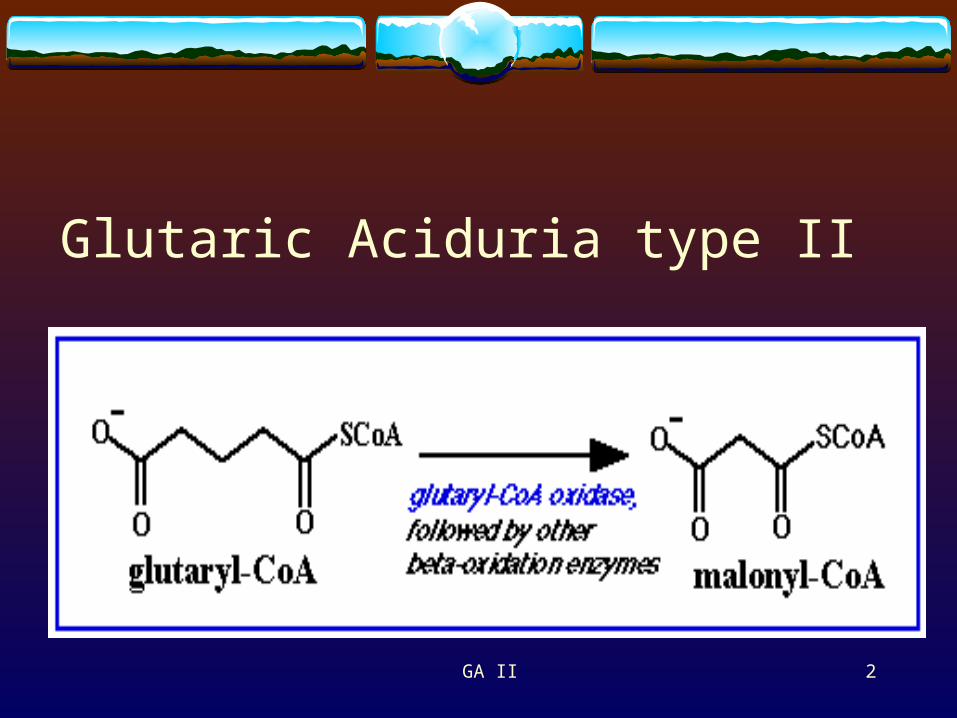
Glutaric Aciduria type II
GA II 3
Glutaric Acid
It is an intermediate in three major metabolic pathways:
-Fatty acid metabolism -Lysine metabolism -Tryptophan metabolism
GA II 4
Fatty acid oxidation defects Short chain acyl-CoA dehydrogenase def. (SCAD) Medium chain acyl-Co A dehydrogenase def. (MCAD) Long chain acyl-CoA dehydrogenase def. (LCAD) Multiple acyl-CoA dehydrogenase def. (MAD) Riboflavin responsive defects of ß-oxidation (RR-MAD) 3-Hydroxy-3-methylgtutaryl CoA lyase def. (HMG-CoA)
GA II 5
MAD deficiencies Defects in electron transfer flavoprotein ( ETF ) & its
dehydrogenase (ETF-DH). Impairs transfer of electrons into mitochondria electron
transfer chain. 2 Types:1. (MAD-S) severe neonatal form or. GLUTARIC ACIDURIA type II.2. ( MAD- M) mild “late onset” variant. ethyl-malonic-adipic aciduria.
GA II 6
Glutaric aciduria II ( MAD-S )
Severe neonatal form:
acidosis, hypoglycemia, coma, hypotonia & cardiomyopathies.
Two subgroups:1. With congenital anomalies.
2. Without congenital anomalies.
GA II 7
Clinical picture
Growth retardation. Special odor. Metabolic acidosis. Hypoglycemia. Dysmorphism. Early neonatal death. Def of electron transport chain flavoprotein or its oxidoreductase.
GA II 8
( MAD- S ) Abnormal liver (including function) Biliary atresia & stenosis Macrocephaly Large kidneys & Multiple renal cysts Organic aciduria Pancreas (exocrine), general abnormalities Undermineralization of skull
GA II 9
( MAD- S ) Macrocephaly. Brain, general abnormalities. Club foot/hindfoot, varus. Rocker-bottom feet / hindfeet. Fontanelles, delayed closure/large. Hamartoma of brain. Hypoglycaemia. Hypospadias.
GA II 10
Diagnosis Urinary organic acid profile. GCMSShows - Ethyl-malonic acid - Dicarboxylic acid - Lysine - Branched chain amino acid Blood metabolic screening : Tandem MS - Glutaric acid - Lysine - Leucine
GA II 11
Glutaric aciduria type II
Differentiate from GA type I.- Def. Of glutaryl CoA dehydrogenase.- Progressive dystonia & dyskinesia.- Vomiting , seizures, coma & Reye-like presentation.- Ketosis, hypoglycemia, hyperammonemia & hepatitis picture.- High conc of glutaric acid in serum & urine. 3- Hydroxyglutaric acid. C.F. 2- Hydroxyglutaric acid in GA II.
N.B. Glutaric aciduria type III is a peroxisomal disorder.Very long chain fatty acids
GA II 12
Treatment
Acute illnesses :1. Prompt treatment with D10% to suppress lipolysis.
2. Correct acidosis.
Chronic:1. Avoid starvation.
2. Special formula. (low protein-low fat).
3. Carnitine & riboflavin supplements.
GA II 13
Sick days plan for patients with G.A. II
Problems that may lead to significant metabolic illnesses in children with organic acidemias:
1. Fever - increases metabolic rate, increases rate of protein breakdown and dehydration.
2. Painful infections - Pain increases metabolic rate, infections of the mouth and throat often decrease appetite and fluid intake.
GA II 14
Sick days plan for patients with G.A. II
3. Vomiting - prevents calorie and fluid intake and may be a sign of metabolic illness.
4. Diarrhea - causes dehydration, sodium and bicarbonate loss, and acidemia - all of which decrease the ability of the liver and kidney to remove pathological metabolites from the blood.
GA II 15
Sick days plan for patients with G.A. II
5. Poor appetite - when calorie intake falls below 45 Cal/kg-day, then protein from muscle is broken down for energy .
6. When a sustained increase in protein catabolism is combined with dehydration and acidemia , then the catabolic state is associated with brain intoxication and injury.
GA II 16
Goals of treatment during illnesses:
Metabolic illnesses usually evolve over a 12-48 hour period. Early recognition of illness or the problems listed above and careful attention to specific goals of treatment will usually keep the metabolic disorder under control.
If the goals are not met and signs of illness develop then evaluation at hospitalization for emergency management may be necessary.
GA II 17
Goals of treatment during illnesses:
1. Minimum daily caloric intake 60 Cal/kg-day.
2. If eating is poor then give small amounts regularly every 2 hours.
GA II 18
Goals of treatment during illnesses:
3. If fever is high and diarrhea is frequent then weigh twice daily, A weight loss of more than 3-5% is significant in an infant with such disorders.
4. Treat fever and pain with high doses of Tylenol 130 mg every 4 hours as needed to keep fever under 38°C.
GA II 19
In-hospital management of acute illnesses
Successful therapy in part depends upon :
1. continued infusion of glucose at a rate of approximately twice the basal metabolic rate of the patient.
2. an initial insulin response to rapid glucose administration.
GA II 20
In-hospital management of acute illnesses cont.
3. If hyperglycemia (>200 mg/dl) persists beyond the first 120 minutes of therapy then regular insulin should be administered by IV bolus starting at 0.1 units/kg.
4. Insulin should be used to maintain the blood glucose between 100-150 mg/dl and should be discontinued when the blood glucose falls below 100 mg/dl.

GA II 21
In-hospital management of acute illnesses
“Hyperglycemia should not be considered an indication for lowering the rate of glucose infusion, to do so defeats the purpose of the therapy.”
GA II 22
In-hospital management of acute illnesses
Acidemia also must be managed aggressively. 1. Recovery may depend in part upon the renal clearance of non-
volatile dicarboxylic acids. 2. correction of acidemia, intravascular volume expansion to
establish vigorous urine output (initial bolus 20 ml/kg), and a urine pH greater than 7.5.
3. During correction of acidemia blood potassium may decrease, to allow urine alkalization potassium should be maintained 3.5 - 4.5 mEq/L, which can usually be accomplished with 10-20 mEq/L KCL in the IV fluid.
GA II 23
Pitfalls
If a metabolic disorder is still suspected with a negative screening repeat Tandem MS & request GCMS.
Do not lower the glucose infusion rate due to hyperglycemia….! Give insulin.
Minimal protein “TPN” helps to control catabolism.

GA II 24
THANK YOU
Related Documents











