-
7/29/2019 Focused Cardiac Assessment
1/23
MaterialProtectedbyCopyright
Focused Cardiovascular Assessment
Thiscoursehasbeenawarded2.0(two)contacthours
Copyright2004byAMNHealthcareinassociationwithInteractMedical
AllRightsReserved.Reproductionanddistribution
OfthesematerialsareprohibitedwithouttheexpresswrittenauthorizationofAMNHealthcare.
CourseExpires:October17,2014
-
7/29/2019 Focused Cardiac Assessment
2/23
MaterialProtectedbyCopyright
Disclaimer
RN.comstrivestokeepitscontentfairandunbiased.
Theauthor(s),planningcommittee,andreviewershavenoconflictsofinterestinrelationtothiscourse.
ConflictofInterestisdefinedascircumstancesaconflictofinterestthatanindividualmayhave,which
couldpossiblyaffectEducationcontentaboutproductsorservicesofacommercialinterestwithwhich
he/shehasafinancialrelationship.
Thereisnocommercialsupportbeingusedforthiscourse.Participantsareadvisedthattheaccredited
statusofRN.comdoesnotimplyendorsementbytheproviderorANCCofanycommercialproducts
mentionedinthiscourse.
Thereisno"offlabel"usageofdrugsorproductsdiscussedinthiscourse.
YoumayfindthatbothgenericandtradenamesareusedincoursesproducedbyRN.com.Theuseof
tradenamesdoesnotindicateanypreferenceofonetradenamedagentorcompanyoveranother.
Tradenamesareprovidedtoenhancerecognitionofagentsdescribedinthecourse.
Note:Alldosagesgivenareforadultsunlessotherwisestated.Theinformationonmedications
containedinthiscourseisnotmeanttobeprescriptiveorallencompassing.Youareencouragedto
consultwithphysiciansandpharmacistsaboutallmedicationissuesforyourpatients.
Acknowledgements
RN.comacknowledgesthevaluablecontributionsof
NadineSalmon,MSN,BSN,IBCLC,theClinicalContentSpecialistforRN.com.NadineisaSouthAfrican
trainedRegisteredNurse,MidwifeandInternationalBoardCertifiedLactationConsultant.Nadine
obtainedanMSNatGrandCanyonUniversity,withanemphasisonNursingLeadership.Herclinical
backgroundisinLabor&DeliveryandPostpartumnursing,andshehasalsoworkedinMedicalSurgical
NursingandHomeHealth.Nadinehasworkexperienceinthreecountries,includingtheUnitedStates,
theUnitedKingdomandSouthAfrica.SheworkedfortheinternationalnursedivisionofAmerican
MobileHealthcare,priortojoiningtheEducationTeamatRN.com.NadineisanurseplannerforRN.com
andisresponsibleforallclinicalaspectsofcoursedevelopment.Sheupdatescoursecontenttocurrent
standards,anddevelopsnewcoursematerialsforRN.com.
LoriConstantineMSN,RN,CFNP,theoriginalauthorofthiscourse.
-
7/29/2019 Focused Cardiac Assessment
3/23
MaterialProtectedbyCopyright
Purpose&Objectives
Thiscoursediscussesspecificcardiovascularhistoryquestionsandexamtechniquesforyouradult
patient.Physicalexamtechniquessuchasinspection,palpation,percussion,andauscultationwillbe
highlighted.Additionally,throughoutthecourseyouwilllearnhowalterationsinyourcardiovascular
assessmentfindings
could
indicate
potential
cardiovascular
problems.
Aftersuccessfulcompletionofthiscourse,youwillbeableto:
1. Outlineasystemicapproachtocardiovascularassessment.
2. Discusshistoryquestionsthatwillhelpyoufocusyourcardiovascularassessment.
3. Recognizeabnormalcardiovascularassessmentfindingsassociatedwithinspection,
auscultation,percussion,andpalpation.
Introduction
Cardiovasculardiseaseistheleadingkillerforbothmenandwomenamongallracialandethnicgroups
intheU.S.AccordingtotheCentersforDiseaseControl(CDC)studiesamongcoronaryheartdisease
patients,90%ofpatientshavehadpriorexposuretoatleastoneheartdiseaseriskfactorthat
contributedtotheirdisease.
Athoroughcardiovascularassessmentwillhelptoidentifysignificantfactorsthatcaninfluence
cardiovascularhealthsuchashighbloodcholesterol,cigaretteuse,diabetes,orhypertension(CDC,
2011).Therefore,acardiovascularexamshouldbeapartofeveryabbreviatedandcomplete
assessment.
Afocusedcardiovascularassessmentisusuallyindicatedafteracomprehensiveassessmentindicatesa
potentialcardiovascularproblem.Thefocusedcardiovascularassessmentisalsoindicatedwhenan
intervalorabbreviatedassessmentshowsachangeinstatusfromyourpreviousassessmentorthe
reportyoureceived,whenanewsymptomemerges,orthepatientdevelopsanydistress.
Anadvantageofthefocusedassessmentisthatitallowsyoutoaskaboutsymptomsandmovequickly
toconductingafocusedphysicalexam.Basedupontheresultsofyourassessment,youmaychoosehow
oftentoperformintervalassessmentstomonitorthepatientsidentifiedproblem.Keepinmindthatall
assessments
should
consider
patients
privacy
and
foster
open,
honest
patient
communication.
-
7/29/2019 Focused Cardiac Assessment
4/23
MaterialProtectedbyCopyright
History
Thepurposeofthecardiovascularhealthhistoryistoprovideinformationaboutyourpatients
cardiovascularsymptomsandhowtheydeveloped.Acompletecardiovascularhistorywillgiveyou
indicationstopotentialorunderlyingcardiovascularillnessesordiseasestates.Obtaininga
cardiovascularhistory
will
guide
you
through
your
focused
physical
exam.
In
addition
to
obtaining
data
aboutthepatientscardiovascularstatus,youshouldobtaininformationaboutotherfactorsthatcan
impactphysicalstatusincludingspiritualneeds,culturalidiosyncrasies,andfunctionallivingstatus.
PastHealthHistory
Itisimportanttoaskquestionsaboutyourpatientspasthealthhistory.Thepasthealthhistoryshould
elicitinformationaboutthefollowingissues:hypertension,elevatedbloodcholesterolortriglycerides,
heartmurmurs,congenitalheartdisease,rheumaticfeverorunexplainedjointpainsasachildoryouth,
recurrenttonsillitisandanemia.Youwillalsowanttoaskaboutthepatientshistoryofheartdisease,
whenandhowitwastreated,lastEKG,stresstests,andserumcholesterollevels.Askthepatientthe
reasonsfor
any
previous
hospitalizations
and
the
nature
of
the
treatments
received
while
in
the
hospital.Askaboutcardiaccatheterizations,echocardiograms,stresstests,
andcardiacsurgeries(Kaplow&Hardin,2007).
CurrentLifestyleandPsychosocialStatus
Currentlifestyleandpsychosocialissuestoexplorewhenconductingyourfocusedcardiovascularhealth
historyinclude:
Nutrition:Haveyourpatientdescribetheirdailydiet.Askabouttheirusualweightandany
recentweightgainorweightloss.
Smoking:Askyourpatientiftheysmokecigarettesorothertobacco.Ascertainthepackperyear
smokinghistory.Thisisdonebymultiplyingthenumberofyearsyourpatienthassmokedwith
thenumberofpacksperdaytheyhavesmoked(CancerTreatmentCentersofAmerica,2011).
Alcohol:Askhowmuchalcoholthepatientnormallydrinksperdayorperweek.Askabout
whenthelastdrinkwasandtheusualnumberofdrinks
perepisode.
Exercise:Askaboutyourpatient'sactivitylevelandusualamountofexercisedonedailyor
weekly.Askwhattypeofexercisetheyparticipatein.
Drugs:
Ask
your
patient
about
all
medication
they
take
including
anti
hypertensives,
beta
blockers,calciumchannelblockers,digoxin,diuretics,aspirin,anticoagulants,overthecounter
drugs,herbalsupplements,orstreetdrugs.
SmokersPackPerDayHistory
2packsperdayx10years=20packyearhistory
1packperdayx20years=20packyearhistory
3packsperdayx7years=21packyearhistory
-
7/29/2019 Focused Cardiac Assessment
5/23
MaterialProtectedbyCopyright
FamilyHistory
Familyhistoryisanimportantfactorusedinidentifyingyourpatientsriskforcertaincardiovascular
diseases(Kaplow&Hardin,2007).
Askyourpatientaboutanycardiovascularfamilyhistorysuchashypertension,obesity,diabetes,
coronaryarterydisease,orsuddendeath.
TestYourself:
Whichofthefollowingdiseasesisassociatedwithcardiovasculardisease?
A. Hypothyroidism
B. LungCancer
C. Diabetes(correct)
D. InflammatoryBowelDisease
AssessmentofChestPainUsingPQRSTMnemonic
When examining the cardiovascular system, the mnemonic PQRST, is very useful inassessing chest pain. It provides a methodology in which communication to otherhealthcare providers will be most efficient and informative.
Assess the following characteristics with each new report of pain and following any
intervention:
(P) Provocative or Palliative: What makes the symptom(s) better or worse?
(Q) Quality: Describe the symptom(s).
(R) Region or Radiation: Where in the body does the symptom occur? Is there
radiation or extension of the symptom(s) to another area of the body?
(S) Severity: On a scale of 1-10, (10 being the worst) how bad is the symptom(s)?
(T) Timing: Does it occur in association with something else (e.g. eating, exertion,
movement)?
-
7/29/2019 Focused Cardiac Assessment
6/23
MaterialProtectedbyCopyright
ProvocativeorPalliativeFactors
Askthepatientaboutwhatstartsorworsensthepain.Chestdiscomfortprovokedbyexertionisaclassic
symptomofangina,althoughesophagealpaincanalsoresultfromexertion.Otherfactorsthatmay
provokeischemicpaininclude:
Cold
Emotionalstress
Sexualintercourse
Smoking
Meals
However,discomfortthatreliablyoccurswitheatingismostlikelyrelatedtoanuppergastrointestinal
disease.Painmadeworsebyswallowingislikelyofesophagealorigin.
Factorsthatinfluencepainshouldalsobeestablished.Painthatrespondstosublingualnitroglycerinor
cessationofactivitystronglysuggestsacardiacischemicetiology,whilepericarditispaintypically
improveswithsittingupandleaningforward.
PracticePearl
Patientswithahistoryofcoronaryheartdiseasetendtohavethesamequalityofchestpainwith
recurrentepisodes.
QualityofPain
Thepatient
with
myocardial
ischemia
often
denies
feeling
chest
pain
and
may
delay
seeking
treatment.Typicaldescriptionsofchestpainfrommyocardialischemiamayinclude:
Squeezing Abandlikesensationisfeltaroundthechest.
Tightness Thereisasensationofaknotbeingpresentinthecenterofthechest.
Pressure Asensationofalumpinthroatoraheavyweightonthechest.
ChestConstriction TheLevinesignisdisplayedbyapatientsufferingfromchestpaincausedbya
myocardialinfarction.Thepatienttypicallypressesaclenchedfistagainstthechesttoillustratethe
sensationofpressureandconstrictioninthechest.
Burning Infarctionpainisoftenmistakenforheartburnorindigestion,especiallyinwomen.
-
7/29/2019 Focused Cardiac Assessment
7/23
MaterialProtectedbyCopyright
RegionorRadiationofPainPainthatlocalizestoasmallareaofthechestismorelikelytoberelatedtoachestwallorpleuralorigin
ratherthantheheart.
Ischemiccardiacpainisadiffusetypeofnonlocalizedpain.
Thepainofmyocardialischemiaoftenradiatestotheneck,throat,lowerjaw,teeth,upperextremities,
orshoulder.
Ifthechestpainisradiatingtoseveralareas,thereisanincreasedchancethatthepatientishavinga
myocardialinfarction(MI).
SeverityandAssociatedSymptomsUsinga10pointnumericpainratingscaleorvisualanalogscaleoftenhelpspatientsdescribethe
intensityofpain.The10pointscoregradespaininseverityrangingfrom0(nopain)to10(most
excruciating).The
severity
of
pain
does
not
necessarily
correlate
with
the
degree
of
ischemia.
As
many
as1/3ofmyocardialinfarctionsmaygoundetectedbythepatient.Somepatientshavedifficultyputting
anumberonthepaininwhichcaseanadjectiveratingscalemaybemosthelpful.TheNumericPain
Scalebelowisarepresentationofonesuchnumericalscale.
NumericalPainScale
SeverityandAssociatedSymptomsOthersymptomsthatmaybeassociatedwithmyocardialischemiamayinclude:
Nausea
Vomiting
Diaphoresis Syncope
Palpitations
Exertionaldyspnea
Fatigue
Weakness
Dizziness
Lightheadedness
-
7/29/2019 Focused Cardiac Assessment
8/23
MaterialProtectedbyCopyright
Timing
Knowingtheonsetofchestpainisimportanttohelptodeterminethecauseandtreatmentofthepain.
Ischemicpainismostoftengradualwithanincreasingintensityovertime.Acrescendopatternofpain
canalsobecausedbyesophagealdisease.Painassociatedwithpneumothorax,aorticdissection,or
acutepulmonary
embolism
typically
has
an
abrupt
onset
with
the
initial
sensation
being
the
most
intense.
Understandingthedurationofpainandanypatternsarealsohelpful.Thepainfrommyocardial
ischemiagenerallylastsforafewminuteswhereasthepainfromanMImaybemoreprolonged.Chest
discomfortthatonlylastsforafewsecondsorpainthatisconstantfordaysorweeksisnotgenerally
duetoischemia.Myocardialischemiamayhaveacircadianpattern.Itismorelikelytooccurinthe
morningthanintheafternoon,correlatingwithanincreaseinsympathetictone.However,thispattern
maynotbeexhibitedinpatientswithdiabetesorpatientstakingbetablockersasthepatients
sympathetictoneisaltered.
Ifthe
patient
is
unable
to
qualify
and
quantify
their
pain,
the
following
questions
may
be
useful
in
gettingneededinformationregardingtheirpain.
Whatgetsthepainstarted?
Whathelpsthepainstop(rest,sittingupandleaningforward)?
Wouldyoudescribeitasmoreofadullpressureorsqueezingormoreofasharp,stabbing,or
rippingfeeling?
Doesthispainfeelsimilartowhenyouhadyourpreviousheartattack?
Isthepainmostlyinoneareaordoyoufeelitupintoyourneckandarms?
With0beingnopainand10beingthemostexcruciatingpainever,whatnumberwouldyou
givethepaintodescribetheseverity?
Whenapplying
anumber
is
difficult:
Would
you
describe
the
pain
as
mild,
moderate,
or
severe?
Areyoufeelingnauseous,dizzy,lightheaded,shortofbreath,ortired?
Doesthepainstartoffgraduallyandgetworse,orviceversa?
Howlongdoesthepainlast?
Whendoesthepainusuallyoccurmorning,afternoon,ornight?
ChestPainintheElderly
Itshouldbenoted,however,thattypicalclinicalmanifestationssuchaschestpainoccurinonly50%of
elderlypatientswithcoronaryarterydisease(CAD)(Milner,2001).Whenpainispresentinanolder
patientitisfrequentlyvagueandpoorlylocalizedorlocalizedtotheabdomenorepigastricarearather
thanthesubsternalarea.Elderlypatientsexperiencinganginaormyocardialischemiamaydescribetheir
symptomssimplyas:exertionaldyspnea(mostcommon),fatigue,syncope,nausea,anorexia,confusion,
ordyspneaatrest.
-
7/29/2019 Focused Cardiac Assessment
9/23
MaterialProtectedbyCopyright
TestYourself:
Chestpainintheelderlyisusuallywelldefined.
A. True
B. False(Correct)
OtherSymptoms:Dyspnea
Dyspnea(shortnessofbreath)thataccompanieschestpainmayalsobeduetoanumberofpulmonary
disorders.
Askyourpatientthefollowingquestionsrelatedtodyspnea:
Doyouevergetshortofbreath?
What
types
of
activity
and
how
much
activity
brings
on
the
shortness
of
breath?
Doestheshortnessofbreathcomeonsuddenlyorunexpectedly?
Doesthedyspneacomeandgoorisitconstant?
Istheshortnessofbreathassociatedwithchangeinposition?
Doestheshortnessofbreathwakeyouupatnight?
Doestheshortnessofbreathinterferewithactivitiesofdailyliving?
PracticePearl
Paroxysmalnocturnaldyspnea(PND)occursatnightwithcongestiveheartfailure.Layingdown
increasesthevolumeofthoracicblood.Theweakenedheartcannotaccommodatethisgreater
volume.Your
patient
will
complain
of
sleeping
for
about
two
hours
and
then
arising
suddenly
needingfreshair.
OtherSymptoms:OrthopneaandCoughing
Orthopnea
Askyourpatienthowmanypillowsheorshesleepsonatnight.Orthopneaistheinabilitytobreathe
wheninalyingposition.
CoughDoesyourpatienthaveaconsistentcough?Havethepatientdescribethefrequency,timing,severityof
cough,andanysputumproduction.Ifthepatientdoeshavesputumproductionaskaboutthecolorof
thesputum,ifithasanodor,andifitisbloodtinged.
PracticePearl
Hemoptysisisoftenpulmonaryinnature,butmayoccurwithcardiogenicpulmonaryedema.
-
7/29/2019 Focused Cardiac Assessment
10/23
MaterialProtectedbyCopyright
OtherSymptoms:Fatigue,Edema,CyanosisandPallor
Fatigue
Askyourpatientiftheytireeasily.Ifso,askaboutwhenthefatiguestarted.Wasitsuddenorgradual?
Hastherebeenanyrecentchangeinenergylevel?Alsoaskaboutthetimeofthedaythefatigueis
related
to,
e.g.
all
day,
morning
or
evening
to
establish
the
presence
of
a
circadian
rhythm,
which
may
indicateischemia.
PracticePearl
Cardiacrelatedfatigueisworseintheevening.Fatiguetoanxietyordepressionoccursalldayoris
worseinthemorning.
Edema,Cyanosis,andPallor
Doesyourpatienthaveanyswellingorskincolorchanges?Cyanosisorpalloroccurswithmyocardial
infarctionorlowcardiacoutput.Ifthepatienthasswelling,askaboutitslocation.Isitinthefeetand
legs?
If
so,
when
was
it
first
noticed?
Ask
about
any
recent
change
in
the
swelling,
if
it
is
unilateral
or
bilateral,andiftheswellingsubsidesaftersleepingorrestingwithfeetup.Alsoaskaboutany
associatedsymptomswiththeswellingsuchasdyspnea.
PracticePearl
Cardiacrelatededemaisworseintheeveningandbetterinthemorningafterrestingwiththefeet
up.
OtherSymptoms:Nocturia
Doesyourpatientgetupatnighttourinate?Askhowlongthishasbeenoccurringandiftherehave
beenanyrecentchangesinthispattern.
PracticePearl
Recumbencypromotesfluidreabsorptionandexcretion.Nocturiaoccurswithheartfailureinthe
patientwhoisambulatoryduringtheday.
-
7/29/2019 Focused Cardiac Assessment
11/23
MaterialProtectedbyCopyright
Pediatric,Pregnant,andAgingPatients
Additionalhistoryquestionsyoumaywishtoaskregardingyourinfant,pediatric,pregnant,oraging
patientarelistedontheleftsidebuttons.
ContentadaptedfromJarvis,1996.
AdditionalHistoryforInfants
Mothershealthduringpregnancy? Unexplainedfeverorrubellainthefirsttrimester? Other
infections,hypertension,drugstaken?
Evernoticedanycyanosiswhilefeeding,nursingorcrying?
Doesthebabyeatorplaywithouttiring?
Isthebabygrowingaccordingtonormalforageandgender?
Werethebabysmotormilestonesachievedasexpected
Howmanynapsperdayandlengthofnaps?
AdditionalHistoryforChildren
Activity Isthechildabletokeepupwithsameagedplaymates? Isthechildwillingorreluctant
toplay? Doesthechildpreferquietplay? Doesthechildeverhavebluespells?
Anyunexpectedjointpainorunexplainedfever?
Doesthechildhavefrequentheadachesornosebleeds?
Doesthechildhavefrequentrespiratoryinfections? Anyproventobestrepinfections?
Anyfamilyhistoryofcongenitaldiseases?
Anyoneinthefamilywithchromosomalabnormalities?
AdditionalHistory
for
Pregnant
Patients
BloodPressure Didyouhavehighbloodpressureinthisorotherpregnancies?Whatwasyour
bloodpressurebeforeyourpregnancy?
Hasyourpressurebeenmonitoredinthispregnancy?
Anyproteinintheurine?
Anyexcessiveweightgain?
Haveyouhadanyswellinginthefeet,legsorface?
Haveyouexperiencedanyfaintnesswiththispregnancy?
Haveyouexperiencedanydizzinesswiththispregnancy?
AdditionalHistory
for
Elderly
Patients
HeartandLungdisease Isthereahistoryofheartdisease,hypertension,coronaryartery
disease,emphysema,bronchitis?
Doyoutakeanymedicationsforyourillness?
Whatarethesideeffectsofthemedication(s)?
Haveyourecentlystoppedtakinganyofyourmedications? Ifso,whichonesandwhy?
-
7/29/2019 Focused Cardiac Assessment
12/23
MaterialProtectedbyCopyright
Doyourillnessesinterferewithyouractivitiesofdailyliving?
Doesyourhomehaveanystairs? Howoftendoyouneedtoclimbthem?
ThePhysicalExamWhenassessingthecardiovascularsystem,othersystems,suchasthecirculatoryandrespiratory
systems,alsoneedtobeevaluatedtoprovideacomprehensiveandholisticpicture.
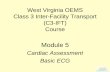
Inperformingacardiacassessment,avisualunderstandingoftheheartmaybeuseful:
A:AortaB:LeftventricleC:RightventricleD:Pulmonaryartery
ThecoronaryarteryRamusinterventricularisanteriorcanbeseeninthegroove(sulcus
interventricularis)between
the
ventricles.
(wikimedia.org,2007)
AssessmentofTheNeckVessels:InspectionWheninspectingtheneckvessels,lookforanyabnormalitiesyoucanobservewithyoureyes,ears,or
nose.
Themostimportantobservationtobemadeintheneckregionistheassessmentofjugularvenous
pulse.From
the
jugular
veins
you
can
estimate
central
venous
pressure
(CVP)
and
estimate
the
hearts
efficiencyasapump.
Ataglance,ifthepatientissittinginthesupinepositionat45degreesorhigher,youshouldnotbeable
toseejugularvenouspulsationsunlessthereisunderlyingpathology.
-
7/29/2019 Focused Cardiac Assessment
13/23
MaterialProtectedbyCopyright
AssessmentofTheNeckVessels: Auscultation
Whenauscultating,ensureyourroomisquiet,auscultateoverbareskin,andlistentoonesoundata
time.Yourbellordiaphragmshouldbeplacedonyourpatientsskinfirmlyenoughtoleaveaslightring
ontheirskinwhenremoved. Beawarethatyourpatientshairmayalsointerferewithtrue
identificationof
certain
sounds.
The
diaphragm
is
used
to
listen
to
high
pitched
sounds
and
the
bell
is
bestusedtoidentifylowpitchedsounds(Kaplow&Hardin,2007).Also,remembertocleanyour
stethoscopebetweenpatients.
Auscultatethecarotidarteriesinpersonsmiddleagedorolder,orthosewithahistoryofcardiovascular
disease.Youarelisteningforthepresenceofabruit,whichisablowingorswishingsound,indicating
turbulentbloodflow.Youmayneedtoaskyourpatienttoholdtheirbreathforashorttimesothatyou
donotconfusetrachealbreathsoundswithabruit.Typically,abruitisabsent.
TestYourself:
Abruitisoftenconfusedwith:
A. Rales
B. Crackles
C. Wheezes
D. Trachealbreathsounds(Correct)
AssessmentofTheNeckVessels:Palpation
Palpation,anothercommonlyusedphysicalexamtechnique,requiresyoutotouchyourpatientwith
differentpartsofyourhandusingdifferentstrengthpressures.Duringlightpalpation,youpresstheskin
aboutinchto3/4inchwiththepadsofyourfingers.Whenusingdeeppalpation,useyourfingerpads
andcompresstheskinabout1inchesto2inches.Palpationallowsyoutoassesstheneckfor
tenderness,abnormaltemperature,excessivemoisture,pulsations,ormasses.
Palpatethecarotidarteriesverygentlyandneveratthesametime.Feelthecontourandamplitudeof
thepulse.Normally,thecontourissmoothwitharapidupstrokeandnormalstrength(+2).Findings
shouldbesimilarbilaterally.
Therightbundlebranchspreadsthewaveofdepolarizationtotherightventricle.Likewise,theleft
bundlebranchspreadsthewaveofdepolarizationtoboththeinterventricularseptumandtheleft
ventricle.Theleftbundlefurtherdividesintothreebranchesorfasicles.Thebundlebranchesfurther
divideintoPurkinjefibers.
-
7/29/2019 Focused Cardiac Assessment
14/23
MaterialProtectedbyCopyright
CirculatoryAssessment:Inspection
Performingavisualassessmentofthecirculatorysystemisanimportantcomponentofa
comprehensivecardiovascularassessment.Areasforevaluationyoumayinspectincludeskincolor,
locationofanylesions,bruisesorrash,symmetryofmotion,sizeofbodyparts,andanyabnormal
findings,sounds,
and
odors.
Beginbyinspectingthepatientsskinforcolor,warmth,andmoisture.Cool,clammyskinresultsfrom
vasoconstriction.Warm,moistskinresultsfromvasodilation.Flushingofapatientsskinmaybedueto
medications,excessheat,anxiety,orfear.Pallorcanresultfromanemiaorincreasedperipheralvascular
resistancecausedbyatherosclerosis.Dependentrubor(redness)maybeasignofchronicarterial
insufficiency.Peripheralcyanosismaycauseabluishdiscolorationtothelipsandextremities.Inspect
theoralmucousmembranesforcyanosisthatmaynotbereadilyapparentontheskin.Examine
underneaththetongue,insidethecheeks,andthenailbedsforsignsofperipheralcyanosis.
Therearetwotypesofcyanosisthatmayoccurincompromisedpatients:centralandperipheral.Central
cyanosisis
consistent
with
reduced
oxygen
intake
or
transport
from
the
lungs.
Peripheral
cyanosis
suggestsconstrictionoftheperipheralarteries.Thisisusuallyfromstress,cold,oranxiety.Itmayalso
befromhypovolemia,shock,orvasoconstrictivediseases.
Notethepresenceofanyedema.Inspectyourpatientshairdistributionontheirskin.Lackofhairmay
alsoindicatearterialinsufficiency.
Next,assessarterialperfusiontothelowerextremities.Haveyourpatientliesupineonaflatsurface
andelevateoneofhislegsabovehisheartforaboutoneminute.Youmayneedtoassistwiththis
movement.Thenaskhimtositupanddanglehislegsoverthebedandinspectthecolorofbothlegs.
The
leg
that
was
elevated
should
show
slight
pallor
in
comparison
to
the
other
leg.
The
color
of
both
legs
shouldbeaboutthesameinabouttenseconds,oncetheveinshavehadtimetofill.
Edemacanresultfrommanydiseaseprocessesincludingheartfailure,liverfailure,orbyvenous
insufficiency,varicosities,andthrombophlebitis.
CirculatoryAssessment:Auscultation
Auscultateyourpatientsbloodpressure.Thesystolicreadingreflectsthepressureexertedbytheleft
ventricleduringcontraction.Thediastolicreadingreflectsthepressureinthearterieswhentheheartis
atrest.
Bloodpressure
is
lowest
in
the
newborn,
and
rises
with
age,
weight
gain,
stress,
anxiety,
and
during
exercise.
-
7/29/2019 Focused Cardiac Assessment
15/23
MaterialProtectedbyCopyright
CirculatoryAssessment:Auscultation
Whenauscultatingbloodpressure,besuretochooseanappropriatesizecufftoavoidfalsereadings.
Somehelpfulhintswhenassessingbloodpressureinclude:
Nevertakeabloodpressureinanarmonthesamesideasamastectomy.
Nevertakeabloodpressureinanarmwithanarteriovenousfistulaorshunt,orinanarmwitha
peripherallyinsertedcentralcatheter.
IfeitherthesystolicBPisover140orthediastolicpressureisover90onrepeated
measurements,thepatientisconsideredtohaveStage1Hypertension(highbloodpressure).
Hypertensionisriskfactorforheartdisease,stroke,andkidneydisease.
Diet,exercise,and,whennecessary,medicationscancontrolbloodpressure.
BloodPressureClassificationinAdults
Category
Normal
PreHypertension
StageIHypertension
StageIIHypertension
Systolic
160
Diastolic
And100
ClassificationandManagementofBloodPressureinAdults.NationalInstituteofHealth(2003).
CirculatoryAssessment:Palpation
Thenextpartofthecirculatorysystemexaminationispalpation.
Beginbypalpatingtheperipheralarteries.Theseincludethebrachial,radial,femoral,popliteal,dorsalis
pedis,andposteriortibial.
Notethecontourandamplitudeofeachpulsation.Theseshouldfeelsimilarbilaterally.
Asyoumoveawayfromthecoreofthebody,youmaynoticethatthecontourorupstrokeofthe
pulsationislessrapid.Thisisnormal,butitisimportanttoassessthatthearterieshavesimilarstrength
bilaterally.
-
7/29/2019 Focused Cardiac Assessment
16/23
MaterialProtectedbyCopyright
TestYourself:
Whenassessingnormalcirculationintheextremities,youanticipatefindingthat:
A. Bloodflowissimilarbilaterally.(Correct)
B. Thecontourandamplitudeofpulsationsaregreaterontheleftsideofthebody.
C. Thecontourandamplitudeofpulsationsaregreatontherightsideofthebody.
D. Asyoumovefurtherawayfromthecoreofthebody,thecontourpulsationsaremorerapid.
ThePrecordium:InspectionandAuscultation
Inspection
Inspecttheanteriorchestforpulsations.Youmayormaynotseetheapicalpulse.Ifitisvisible,youwill
seeitinthefourthorfifthintercostalsspace.
Auscultation
Beforeyoubeginyourauscultationoftheprecordium,prefaceyourexambytellingthepatientyouwill
belisteninginmanydifferentplacesforwhatmightbeawhile.Then,youmustidentifytheareasyou
needtoausculate.YoumaywanttoinchyourstethoscopeinaZpatternacrosstheprecordium,from
thebaseofthehearttotheapex.Concentratetothesoundofthelubandthedub.Theluborfirst
heartsoundisknownasS1.TheduborthesecondheartsoundisknownasS2.
HeartSounds:S1
S1,thelubofthelubdub,isproducedbytheclosureoftricuspidandmitralvalves.
Alterationsyou
may
auscultate
that
involve
S1
are
as
follows:
S1isaccentuatedinexercise,anemia,hyperthyroidism,andmitralstenosis.
S1isdiminishedinfirstdegreeheartblock.
S1splitismostaudibleintricuspidarea(Tlubdub)
(Kaplow&Hardin,2007)
HeartSounds:S2
S2,thedubofthelubdub,isproducedbytheclosureofaortic&pulmonicvalves.
Alterationsyou
may
auscultate
that
involve
S2
are
as
follows:
NormalphysiologicalsplittingofS2isbestheardatpulmonicarea.Itoccursoninspiration(lub
Tdub,lubdub).
SplittingofS2soundcanoccurwhentheaorticandpulmonaryvalvesdonotcloseatthesame
time(Kaplow&Hardin,2007).Thiscanindicatepulmonicstenosis,atrialseptaldefect,right
ventricularfailure,orleftbundlebranchblock.
-
7/29/2019 Focused Cardiac Assessment
17/23
MaterialProtectedbyCopyright
HeartSounds
ListentoactualheartsoundsusingtheAuscultationAssistant
http://www.wilkes.med.ucla.edu/intro.html
Thisgreattoolwillexposeyoutomanydifferentnormalandabnormalheartsounds.
HeartSounds:S3
Thethirdheartsoundisproducedbytherapidfillingoftheventricle(thatisnotcompletelyempty)
duringearlydiastole(Kaplow&Hardin,2007).S3isalsoknownasaventriculargallop(lubDUBtaor
Kentucky).
S3isnormalinpregnancy,children,adultslessthanthirtyyearsold,duringexercise,anxiety,oranemia.
Itisheardbestattheapexintheleftlateraldecubitusposition,usingthebell.
PathologicS3occursinpeopleovertheageof40,usuallyduetomyocardialfailure.
HeartSounds:S4
ThefourthheartsoundistypicallyheardinlatediastolebeforeS1,asaresultofincreasedventricular
resistancetoatrialfilling,duetoeitherdecreasedventricularcomplianceorincreasedventricular
volume.Itislowpitchedandbestheardwiththebell.S4isalsoknownasanatrialgallop(talubDUB
orTennessee).
S4isoftennormalinolderadultsandisheardbestattheapexintheleftlateraldecubitusposition.
PathologicalS4maybecausedbycoronaryarterydisease,hypertension,cardiomyopathy,oraortic
stenosis.
TestYourself:
Whichheartsoundisknownastheatrialgallop?
A. S1
B. S2
C. S3
D. S4(Correct)
-
7/29/2019 Focused Cardiac Assessment
18/23
MaterialProtectedbyCopyright
AbnormalHeartSoundsSummationGallop&OpeningSnap
SummationGallop
AsummationgallopisproducedwhenS3&S4mergeintoonesound.Itoftenoccursatratesgreater
than100beatsperminute.Itmayoccurinheartfailureandpericarditis.Summationgallopsoccurin
15%
of
all
myocardial
infarctions
and
are
common
following
cardiac
surgery.
They
are
best
heard
with
patientleaningforward,holdingbreathafterfullexpiration.
OpeningSnap
Attheendofventricularsystole,whentheaorticandpulmonicvalvesclose,S2isproduced.
ImmediatelyafterS2,theheartrelaxes,andventricularpressurefallsbelowthatofatrialpressure.This
allowstheatrioventricularvalvestoopen.Thisisthestartofdiastole.Normally,youcannothearthese
valvesopen.However,ifthemitralvalvebecomesstenoticorabnormallynarrowedtheywillcreatean
openingsnap.Thissoundusuallyprecedesthedevelopmentofadiastolicmurmurassociatedwith
mitralstenosis.Oncethevalvebecomesseriouslyimpairedandinflexible,theopeningsnapdisappears
(Kowalak,Johnson&Sussman,2002).
AnOpeningSnapisanabnormalheartsoundduetoastenoticvalveopening.Whenanormalcardiac
valveopens,thereisnosoundcreated.
AbnormalHeartSounds:EjectionClick&MidSystolicClick
EjectionClick
Similartoanopeningsnap,anejectionclickiscausedbystenoticvalveleaflets.Thissoundisproduced
whentheaorticorpulmonicvalvesopenatthebeginningofsystole.Itisabriefhighfrequencysound
bestheard
with
the
diaphragm
over
the
aortic
or
pulmonary
artery
or
Erbs
point,
or
near
the
apex
over
themitralarea(Kowalak,Johnson&Sussman,2002).
MidSystolicClick
Amidsystolicclickoccurswhenthemitralvalvesleafletsandcordaetendenaetense.Theanterioror
posteriororbothleafletscanprolapse.Everyonceinawhilemultipleclicksoccur.Theyareheardinmid
tolatesystole.Theyarebestheardoverthetricuspidareaandtowardsthemitralarea.Theyarecrisp,
highfrequencysounds(Kowalak,Johnson&Sussman,2002).
AbnormalHeartSounds:PericardialFrictionRub&MediastinalCrunch
PericardialFriction
Rub
Apericardialfrictionrubisusuallyheardbestandissometimespalpableoverthetricuspidandxyphoid
areas.Itoccurswheninflamedpericardialsurfacesrubtogether.Therubbingofthesesurfacesproduce
thecharacteristic,highpitched,gratingnoises.Todifferentiateapericardialfrictionrubfromapleural
frictionrub,havethepatientholdhisorherbreath.Whentheydothis,apericardialfrictionrubwill
continue,apleuralfrictionrubwillcease(Kowalak,Johnson&Sussman,2002).
-
7/29/2019 Focused Cardiac Assessment
19/23
MaterialProtectedbyCopyright
MediastinalCrunch
Amediastinalcrunchisproducedduetodisplacedairunderthesurfaceoftheskinnearthe
mediastinum.Patientswithmediastinalcrunchoftenhavesubcutaneousemphysema.Youcanassess
forthisbypalpatingcrepitationintheneck.Thenoisehasacrunchingqualityandisheardbestalong
theleftsternalborder.Itmaybelouderoninspiration(Kowalak,Johnson&Sussman,2002).
AbnormalHeartSounds:Murmurs
Amurmurisanabnormalheartsoundcausedbyturbulentbloodflow.Thesoundmayindicatethat
bloodisflowingthroughadamagedoroverworkedheartvalve,thattheremaybeaholeinoneofthe
heart'swalls,orthatthereisanarrowinginoneoftheheart'svessels.
Someheartmurmursareaharmlesstypecalledinnocentheartmurmurswhicharecommoninchildren
andusuallydonotrequiretreatment.
AuscultationofMurmurs
Ifyouauscultateamurmur,itisimportanttoassessanddocumentthefollowingqualitiesofthe
murmur:
Timing: Aretheysystolicordiastolic?
Anatomicallocationofmaximumintensity: Whereisthemurmurbestheard?
Frequency: Whatisthepitchofthemurmur?
Radiation: Canyouhearthemurmurinotherlocationssuchastheneckorupperchest?
Quality: Isthemurmurharsh,soft,orblowing?
Intensity: Describetheloudnessofthemurmuronascaleof1to6,asindicatedbyLevine's6point
gradingscale:
Grade Intensity
1 VeryFaint EasilyMissed
2 QuietBarelyAudible
3 ModeratelyloudbuteasilyheardsameintensityasS1orS2
4 Loud,butusuallynothrillpresent
5
Veryloud,
thrill
present
6 HeardwithstethoscopeoffchestThrillpresent
(Lippincott,Williams&Wilkins,2005)
-
7/29/2019 Focused Cardiac Assessment
20/23
MaterialProtectedbyCopyright
TimingandQualityofCommonMurmurs
Thefollowingtabledepictsthetimingandqualityofcommonmurmurs.
ThePrecordium:PalpitationandPercussion
Palpation
Palpate
the
apical
pulse,
normally
in
the
fourth
or
fifth
intercostal
space,
mid
clavicular
line.
It
should
be
feltasashort,gentletap.Itcanbepalpatedinabouthalfofpeople.Itismoredifficulttopalpatein
obesepatientsorthosewiththickchestwalls.Stress,fever,anxiety,hyperthyroidism,andanemiamay
increasetheamplitudeanddurationoftheapicalpulse.Whentheapicalpulseispalpatedlowerinthe
thoraciccageandhasagreateramplitudethanexpected,itisoftenduetocardiacpathology.
Percussion
Youmayusepercussiontooutlinethecardiacborder.Typically,however,achestxraycanrevealthe
sameresults.Therearetimes,however,thatchestxraysarenotavailableandpercussionmaybeone
ofyouronlytoolstoassesscardiacsize.
Toperform
effective
percussion,
press
the
distal
part
of
the
middle
finger
of
your
non
dominant
hand
firmlyonthebodypart,keepingtherestofthehandoffthebodysurface.Usingthemiddlefingerofthe
dominanthand,tapquicklyanddirectlyoverthepointwheretheothermiddlefingermakescontact
withthepatientsskin.Dullnessshouldbeheardovertheareawheretheheartislocated.
-
7/29/2019 Focused Cardiac Assessment
21/23
MaterialProtectedbyCopyright
RecordingFindings
Itisimportanttoaccuratelyandthoroughlyrecordanddocumentyourfindingsfromthecardiovascular
exam.
Standarddocumentationensuresthatallmembersofthehealthcareteaminterpretthefindings
accurately.
In
documenting
murmurs,
Levine's
six
point
grading
scale
is
the
most
accurate
way
to
record
findings,asistheuseofastandard4pointscaletoassessanddocumentedema.
Rememberthatyourrecordingsarepartofthemedicalrecord,andshouldbeasobjectiveandaccurate
aspossible.
Conclusion
Integratingthecardiovascularhealthhistoryandphysicalexamtakespractice.Itisnotenoughtosimply
asktherightquestionsandperformthephysicalexam.Asthepatientsnurse,youmustcriticallyanalyze
allofthedatayouareobtaining,synthesizethedataintorelevantproblemfocus,andidentifyaplanof
care
for
your
patient
based
upon
this
synthesis.
As
the
plan
of
care
is
being
carried
out,
reassessments
mustoccuronaperiodicbasis.Howoftenthesereassessmentsoccurisuniquetoeachpatient,based
upontheirphysicaldisorder.
IMPORTANTINFORMATION:
Thispublicationisintendedsolelyfortheeducationaluseofhealthcareprofessionalstakingthiscourse
fromRN.cominaccordancewithRN.comtermsofuse.Theguidanceprovidedinthispublicationis
generalinnature,andisnotdesignedtoaddressanyspecificsituation.Asalways,inassessingand
respondingtospecificpatientcaresituations,healthcareprofessionalsmustusetheirjudgment,aswell
asfollowthepoliciesoftheirorganizationandanyapplicablelaw.Organizationsusingthispublicationas
apart
of
their
own
educational
program
should
review
the
contents
of
this
publication
to
ensure
accuracyandconsistencywiththeirownstandardsandprotocols.Thecontentsofthispublicationare
thecopyrightedpropertyofRN.comandmaynotbereproducedordistributedwithoutwritten
permissionfromRN.com.
Healthcareproviders,hospitalsandhealthcareorganizationsthatusethispublicationagreetohold
harmlessandfullyindemnifyRN.com,includingitsparents,subsidiaries,affiliates,officers,directors,
andemployees,fromanyandallliabilityallegedlyarisingfromorrelatinginanywaytotheuseofthe
informationorproductsdiscussedinthispublication.
-
7/29/2019 Focused Cardiac Assessment
22/23
MaterialProtectedbyCopyright
References
AmericanAssociationofCriticalCareNurses(1998).TheCardiovascularSystem.InJ.Alspach
(Ed.),Corecurriculumforcriticalcarenursing
(5thed.,Rev.,pp.137338).Philadelphia:Saunders.
AuscultationAssistant.(2004).Availableathttp://www.wilkes.med.ucla.edu/intro.html.
BlumJ,SchadlerA,PrushCooperS.(2001).AssessmentandManagementofAcuteCardiac
ChestPain.CritCareNursClinofNorthAm.13(2):25969.
CancerTreatmentCentersofAmerica.(2011).Riskfactorsforlungcancer.RetrievedMay4,
2011,fromhttp://www.cancercenter.com/lungcancer/lungcancerriskfactors.cfm
CentersforDiseaseControl.(2006).HeartDiseasefactSheet.RetrievedOctober10,2007from:
http://www.cdc.gov/dhdsp/library/pdfs/fs_heart_disease.pdf
Jarvis,C.(1996).Physicalexaminationandhealthassessment.Philadelphia:W.B.Saunders.
Kaplow,RandHardin,S.(2007).CriticalCareNursing:SynergyforOptimalOutcomes.MA.Jones
andBartlett.
Kowalak,J.;Johnson,P.&Sussman,T.(Eds.).(2002).Auscultationskills:Heartandbreath
sounds.(2nded). (pp.2694). Springhouse,PA: Springhouse.
Lippincott,Williams&Wilkins(2005).
HeartSounds
Made
Incredibly
Easy.
PA.
McCaffery,M.&Pasero,C.(Eds.).(1999).Pain:ClinicalManual(2nded.).
(pp1718,63,108113). St.Louis: Mosby.
MilnerKA,FunkM,RichardsS,VaccarinoV,KrumholzHM.(2001).Symptompredictorsofacute
coronarysyndromesinyoungerandolderpatients.NursRes,50(4):233241.
NationalInstituteofHealth(NIH),2003.NationalHighBloodPressureEducationProgram
(2003).Part oftheSeventhReportoftheJointCommitteeonPrevention,Detection.
Evaluation,andTreatmentofHighBloodPressure.U.S.DepartmentofHealthandHuman
services,National
Institutes
of
Health,
National
Heart,
Lung
and
Blood
Institute.
Retrieved
and
updatedMay5,2011from:http://www.nhlbi.nih.gov/guidelines/hypertension/express.pdf
Shaw,M.(1998)Assessmentmadeincrediblyeasy!Springhouse,PA:Springhouse.
-
7/29/2019 Focused Cardiac Assessment
23/23
AtthetimethiscoursewasconstructedallURL'sinthereferencelistwerecurrentandaccessible.
rn.com.iscommittedtoprovidinghealthcareprofessionalswiththemostuptodateinformation
available.
Copyright2004,AMNHealthcare,Inc.