345 © The Author 2014. Published by Oxford University Press on behalf of the European Orthodontic Society. All rights reserved. For permissions, please email: [email protected] Randomized controlled trial Five-year postretention outcomes of three retention methods—a randomized controlled trial Gudrun Edman Tynelius, Sofia Petrén, Lars Bondemark and Eva Lilja-Karlander Department of Orthodontics, Faculty of Odontology, Malmö University, Sweden Correspondence to: Gudrun Edman Tynelius, Harvigslund Stubbarp 112, S-274 91 Skurup, Sweden. E mail: [email protected] Summary Objective: Comparison of three different retention strategies 5 years or more postretention. Design, Setting, and Participants: Randomized, prospective, single-centre controlled trial. Forty- nine patients (33 girls and 16 boys) were randomly assigned to one of three retention methods during 2 years by picking a ballot shortly before start of retention treatment. Inclusion criteria were no previous orthodontics, permanent dentition, normal skeletal sagittal, vertical, and transversal relationships, Class I dental relationship, space deficiencies, treatment plan with extractions of four premolars followed by fixed straight-wire appliance. Maxillary and mandibular Little's irregularity index (LII), intercanine and intermolar width, arch length, and overbite/overjet were recorded in a blinded manner, altogether 10 measurements on each patient. Significant differences in means within groups assessed by t-test and between groups by one-way analysis of variance. Interventions: Retention methods: removable vacuum-formed retainer (VFR) covering the palate and the maxillary anterior teeth from canine-to-canine and bonded canine-to-canine retainer in the lower arch (group V-CTC); maxillary VFR combined with stripping of the lower anterior teeth (group V-S); and prefabricated positioner (group P). Results: Maxillary mean LII ranged from 1.8 to 2.6 mm, mean intercanine width 33.6–35.3 mm with a significant difference between groups V-S and P, mean intermolar width 46.8–47.4 mm and mean arch length 21.8–22.8 mm. Mandibular mean LII ranged from 2.0 to 3.4 mm with a significant difference between groups V-S and P, mean intercanine width from 25.4 to 26.6 mm, mean intermolar width from 40.8 to 40.9 mm and mean arch length from 16.9 to 17.3 mm. Mean overbite ranged from 1.8 to 2.7 mm and mean overjet from 3.7 to 4.1 mm. Limitations: A single centre study could be less generalizable. Conclusions: The three retention methods disclosed equally favourable clinical results. Trial registration: This trial was not registered. Protocol: The protocol was not published before trial commencement. Introduction A major challenge in orthodontic treatment is to inhibit relapse and ensure long-term stability of outcome. Growth, initial crowding, and patient compliance have traditionally been regarded as the main deter- minants of orthodontic treatment stability (1). As long as the maxilla and mandible are still growing, the position of the teeth and thus the result of retention treatment may be affected. Most current knowl- edge about long-term stability is based on retrospective studies (2–5). A recent review by the Cochrane group concluded that to date there is insufficient evidence to single out any particular retention strategy as the preferred method (6): it was recommended that future studies should include true randomization, reporting of dropouts, adequate sample size calculation, and a minimum follow-up period of 3 months. There are a number of recent studies of the short-term effects of different retention strategies. Two randomized controlled trials (RCTs) comparing two appliances have shown equal short-term European Journal of Orthodontics, 2015, 345–353 doi:10.1093/ejo/cju063 Advance Access publication 1 December 2014 Downloaded from https://academic.oup.com/ejo/article/37/4/345/2570543 by guest on 01 January 2022

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

345© The Author 2014. Published by Oxford University Press on behalf of the European Orthodontic Society. All rights reserved. For permissions, please email: [email protected]
Randomized controlled trial
Five-year postretention outcomes of three retention methods—a randomized controlled trialGudrun Edman Tynelius, Sofia Petrén, Lars Bondemark and Eva Lilja-Karlander
Department of Orthodontics, Faculty of Odontology, Malmö University, Sweden
Correspondence to: Gudrun Edman Tynelius, Harvigslund Stubbarp 112, S-274 91 Skurup, Sweden. E mail: [email protected]
Summary
Objective: Comparison of three different retention strategies 5 years or more postretention.Design, Setting, and Participants: Randomized, prospective, single-centre controlled trial. Forty-nine patients (33 girls and 16 boys) were randomly assigned to one of three retention methods during 2 years by picking a ballot shortly before start of retention treatment. Inclusion criteria were no previous orthodontics, permanent dentition, normal skeletal sagittal, vertical, and transversal relationships, Class I dental relationship, space deficiencies, treatment plan with extractions of four premolars followed by fixed straight-wire appliance. Maxillary and mandibular Little's irregularity index (LII), intercanine and intermolar width, arch length, and overbite/overjet were recorded in a blinded manner, altogether 10 measurements on each patient. Significant differences in means within groups assessed by t-test and between groups by one-way analysis of variance.Interventions: Retention methods: removable vacuum-formed retainer (VFR) covering the palate and the maxillary anterior teeth from canine-to-canine and bonded canine-to-canine retainer in the lower arch (group V-CTC); maxillary VFR combined with stripping of the lower anterior teeth (group V-S); and prefabricated positioner (group P).Results: Maxillary mean LII ranged from 1.8 to 2.6 mm, mean intercanine width 33.6–35.3 mm with a significant difference between groups V-S and P, mean intermolar width 46.8–47.4 mm and mean arch length 21.8–22.8 mm. Mandibular mean LII ranged from 2.0 to 3.4 mm with a significant difference between groups V-S and P, mean intercanine width from 25.4 to 26.6 mm, mean intermolar width from 40.8 to 40.9 mm and mean arch length from 16.9 to 17.3 mm. Mean overbite ranged from 1.8 to 2.7 mm and mean overjet from 3.7 to 4.1 mm.Limitations: A single centre study could be less generalizable.Conclusions: The three retention methods disclosed equally favourable clinical results.Trial registration: This trial was not registered.Protocol: The protocol was not published before trial commencement.
Introduction
A major challenge in orthodontic treatment is to inhibit relapse and ensure long-term stability of outcome. Growth, initial crowding, and patient compliance have traditionally been regarded as the main deter-minants of orthodontic treatment stability (1). As long as the maxilla and mandible are still growing, the position of the teeth and thus the result of retention treatment may be affected. Most current knowl-edge about long-term stability is based on retrospective studies (2–5).
A recent review by the Cochrane group concluded that to date there is insufficient evidence to single out any particular retention strategy as the preferred method (6): it was recommended that future studies should include true randomization, reporting of dropouts, adequate sample size calculation, and a minimum follow-up period of 3 months.
There are a number of recent studies of the short-term effects of different retention strategies. Two randomized controlled trials (RCTs) comparing two appliances have shown equal short-term
European Journal of Orthodontics, 2015, 345–353doi:10.1093/ejo/cju063
Advance Access publication 1 December 2014
Dow
nloaded from https://academ
ic.oup.com/ejo/article/37/4/345/2570543 by guest on 01 January 2022
effects in retaining the outcome of orthodontic treatment of the maxilla (7,8). Edman Tynelius et al. (9,10) compared the effect of three different retention strategies on maintaining the outcome of orthodontic treatment of both jaws and concluded that all three were equally successful after 1 and 2 years of retention. However, to our knowledge there is to date no RCT of the capacity of various retention methods to counteract relapse in the long term.
The aim of this study, in the form of an RCT, was to evaluate and compare the effects of three different retention strategies on counter-acting orthodontic treatment relapse at least 5 years postretention. The null hypothesis tested was that the three retention procedures achieve equivalent long-term results.
Subjects and methods
Trial designThe study was an RCT performed at a single centre by one expe-rienced orthodontic team. The Ethics Committee of Lund/Malmö University, Sweden, approved the protocol and the informed consent form (LU515-01).
Participants, eligibility, and settingThe study subjects comprised patients referred to an orthodontic clinic in the National Health Service (NHS), Ystad, Sweden. The NHS clinic was responsible for treatment of malocclusions of patients in the southeast County Council of Scania. The NHS in Sweden offers free dental care up to the age of 20 years, including orthodontic treatment for patients with severe malocclusion. Between 2001 and 2007, all the study participants had undergone orthodontic treat-ment by one experienced orthodontist (GET). Each patient and parent received oral as well as written information. Signed, written consent was required before inclusion in the trial.
The following inclusion criteria were met:
• No previous experience of orthodontic treatment• Permanent dentition• Normal skeletal sagittal, vertical, and transverse relationships• Class I molar relationship or a maximum of 3 mm anterior or
posterior deviation• Space deficiencies in both jaws• Treatment plan involving extraction of four premolars followed
by fixed straight-wire appliances in both jaws (11)
InterventionsThe three retention methods investigated were:
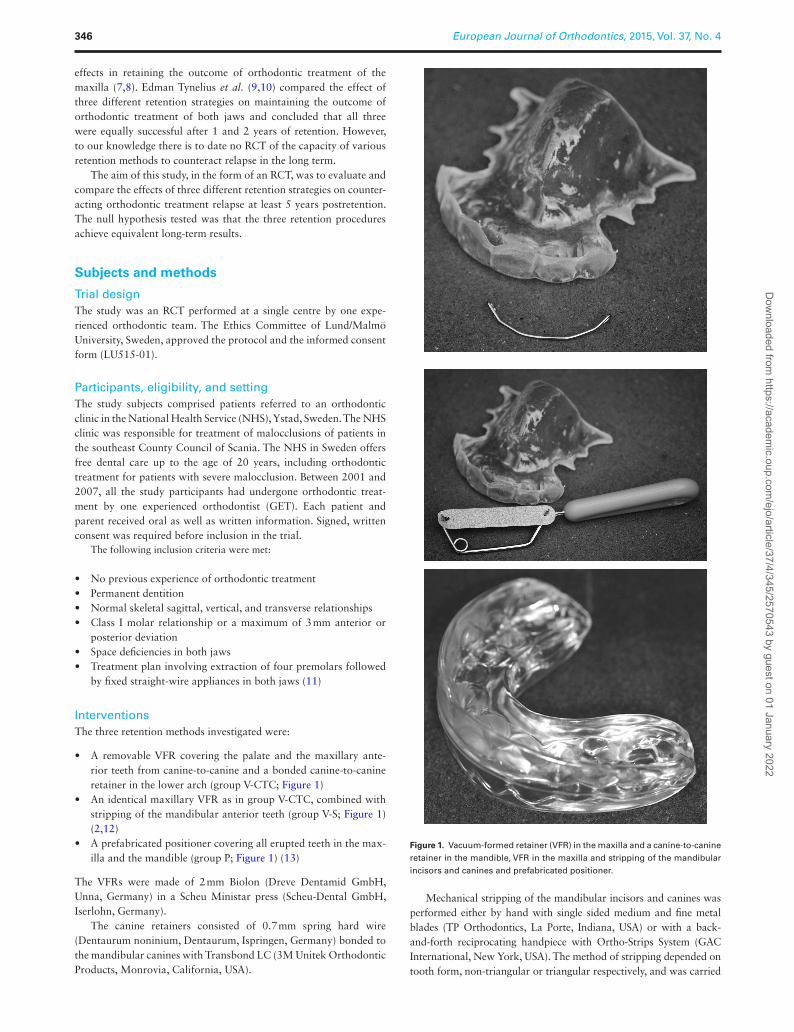
• A removable VFR covering the palate and the maxillary ante-rior teeth from canine-to-canine and a bonded canine-to-canine retainer in the lower arch (group V-CTC; Figure 1)
• An identical maxillary VFR as in group V-CTC, combined with stripping of the mandibular anterior teeth (group V-S; Figure 1) (2,12)
• A prefabricated positioner covering all erupted teeth in the max-illa and the mandible (group P; Figure 1) (13)
The VFRs were made of 2 mm Biolon (Dreve Dentamid GmbH, Unna, Germany) in a Scheu Ministar press (Scheu-Dental GmbH, Iserlohn, Germany).
The canine retainers consisted of 0.7 mm spring hard wire (Dentaurum noninium, Dentaurum, Ispringen, Germany) bonded to the mandibular canines with Transbond LC (3M Unitek Orthodontic Products, Monrovia, California, USA).
Mechanical stripping of the mandibular incisors and canines was performed either by hand with single sided medium and fine metal blades (TP Orthodontics, La Porte, Indiana, USA) or with a back-and-forth reciprocating handpiece with Ortho-Strips System (GAC International, New York, USA). The method of stripping depended on tooth form, non-triangular or triangular respectively, and was carried
Figure 1. Vacuum-formed retainer (VFR) in the maxilla and a canine-to-canine retainer in the mandible, VFR in the maxilla and stripping of the mandibular incisors and canines and prefabricated positioner.
European Journal of Orthodontics, 2015, Vol. 37, No. 4346D
ownloaded from
https://academic.oup.com
/ejo/article/37/4/345/2570543 by guest on 01 January 2022

out either at the appointment 5–6 weeks prior to debonding, or at debonding. The reason for this was to avoid inflicting damage to the papilla. When incisors were non-triangular, there was a greater risk of damage to the papilla with the reciprocating handpiece and, thus, single sided blades manually was the option. The aim of stripping was to achieve small but distinct enamel flattening of the contact surfaces. The reduction of any contact point between two teeth was approxi-mately the thickness of the coarse blade of either system, i.e. 0.22 mm for hand stripping or 0.34 mm for EVA-stripping.
The preformed positioner (Ortho-Tain Positioner, Ortho-Tain Inc., Toa Alta, Puerto Rico) was a soft plastic appliance covering all erupted teeth.
All retention appliances were distributed within 1 hour after debond-ing. The patients in groups V-CTC and V-S were instructed to wear the VFR 22–24 hours per day for 2 days and nights and then at night for 12 months. In group P, the positioner was to be worn for 30 minutes dur-ing the daytime and during sleep for 12 months. During day-time wear the patients were instructed to actively chew into their positioners. The second year of retention patients wore their retainers every other night.
OutcomesDental casts were measured on four occasions: before orthodontic treatment (T0), when the fixed orthodontic appliance was removed and the retention appliance inserted (T1), when the retention appliance was removed after 2 years (T2), and 5 years or more out of retention (T3).
The same examiner (GET) made the following linear measure-ments on dental casts with an electronic digital caliper (Mauser Digital 6, Winterthur, Switzerland) to a precision of 0.01 mm:
• LII in the maxilla and the mandible—the summed displacement of the anatomic contact points of the upper and lower incisors and canines not including the distal contact points of the canines to premolars (14)
• Intercanine width in the maxilla and the mandible—the distance between the canine cusp tips
• Intermolar width in the maxilla and the mandible—the distance between the mesiobuccal cusp tips of the first molars
• Arch length in the maxilla and the mandible—the perpendicular distance from the midpoint of the incisal edges of the central incisors to a line joining the mesial anatomic contact points of the first molars
• Overbite—the overlap of upper to lower central incisors• Overjet—the distance parallel to the occlusal plane from the
incisal edge of the most labial maxillary incisor to the opposing mandibular central incisor
Data on patient ages and treatment times were retrieved from the treatment records.
RandomizationThe generation of randomization sequence was performed in blocks of 15 to ensure that equal numbers of patients were allocated to each of the three retention groups. A ballot system was used for allocation, in lots of 15: five ballot sheets labelled ‘maxillary VFR and bonded mandibular canine-to-canine retainer’, five labelled ‘maxillary VFR and mandibular interproximal enamel reduction (stripping)’, and five with ‘positioner’ were placed in a basket by an independent person. The patient was then allocated to one of the three groups by picking a ballot from the basket shortly before debonding. When the first basket was empty, the second basket was prepared, and another 15 ballots were extracted successively as patients were recruited to the study. This procedure was altogether repeated five times and concluded in 75 randomized patients.
BlindingTo achieve blinding when measuring dental casts only one dental cast at a time was picked out of its box in a cross-sectional man-ner by an assistant, had its own protocol not showing any previous measurements and then a new dental cast from a different patient box was picked. Two dental casts from the same patients were never measured in connection with each other. As the study was prospec-tive with continuous patient visits it was inconvenient to anonymize dental casts from the start of the study.
Statistical analysisSample size calculationThe calculated sample size for each group was based on a significance level of 0.05 and 80 per cent power to detect a clinically meaningful difference of 2.0 mm (SD = 2.0 mm) of the LII. The power analysis showed that at least 16 patients would be required in each group. To compensate for dropouts in the follow-up study, 25 patients were enrolled in each group. Arithmetic means and standard deviations (SD) on group level at times corresponding to pre-treatment (T0), end of active treatment and start of retention (T1), end of 2 years of retention treatment (T2), and end of 5 years or more out of retention (T3) were calculated for each variable.
Primary and secondary outcomesSignificant differences in means between groups were assessed by one-way analysis of variance and within groups by t-test to the pre-vious time point using the Statistical Package for Social Sciences (ver-sion 22.0.0.0, IBM SPSS Inc., Chicago, Illinois, USA). P-values less than 5 per cent (P < 0.05) were considered statistically significant.
Error of methodTwenty randomly selected dental casts were measured by the same examiner (GET) on two separate occasions at an interval of 4 weeks. The error of the method did not exceed 0.45 mm for any of the 10 measurements (15). No significant mean differences between the two series of records were found using paired t-test.
Results
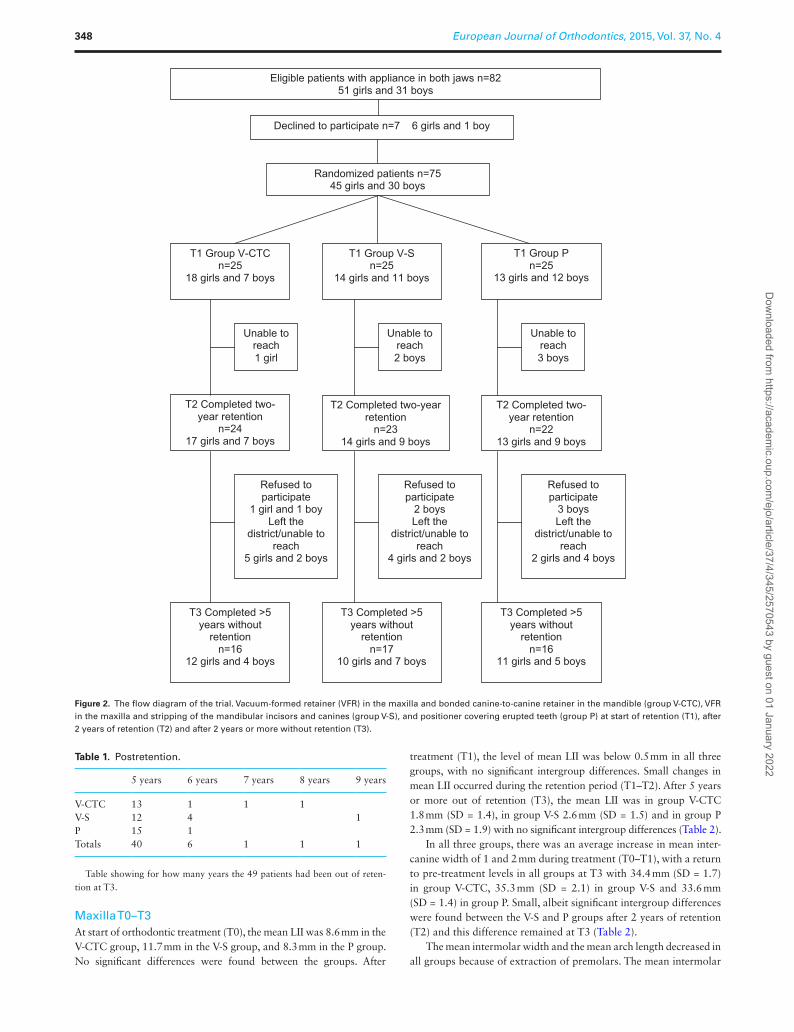
Participant flowA total of 82 patients fulfilled the inclusion criteria. Seven patients (6 girls, 1 boy) declined to participate, and thus 75 patients were rand-omized at the start of the trial. Out of these 75 patients, 26 failed to complete the trial: three declined to participate and 23 left the district or were unable to be contacted. Consequently, 49 patients (33 girls, 16 boys) attended their 5-year or more appointment (Figure 2). Out of these 49 patients, 9 were out of retention more than 5 years (Table 1).
Baseline dataThere were no significant intergroup differences with respect to age or active treatment time. The mean active orthodontic treatment time was 1.7 years (SD = 0.4) and the mean age at start of retention (T1) was 14.3 years (SD = 1.5). As there were no significant differ-ences between boys and girls in any of the study variables, the data for the genders were pooled for analysis (Tables 2–4).
HarmsNo harms were reported. In two cases, patients choose to keep their CTC in situ after 2 years of retention and consequently they were excluded from the long-term study.
G. Edman Tynelius et al. 347D
ownloaded from
https://academic.oup.com
/ejo/article/37/4/345/2570543 by guest on 01 January 2022
Maxilla T0–T3At start of orthodontic treatment (T0), the mean LII was 8.6 mm in the V-CTC group, 11.7 mm in the V-S group, and 8.3 mm in the P group. No significant differences were found between the groups. After
treatment (T1), the level of mean LII was below 0.5 mm in all three groups, with no significant intergroup differences. Small changes in mean LII occurred during the retention period (T1–T2). After 5 years or more out of retention (T3), the mean LII was in group V-CTC 1.8 mm (SD = 1.4), in group V-S 2.6 mm (SD = 1.5) and in group P 2.3 mm (SD = 1.9) with no significant intergroup differences (Table 2).
In all three groups, there was an average increase in mean inter-canine width of 1 and 2 mm during treatment (T0–T1), with a return to pre-treatment levels in all groups at T3 with 34.4 mm (SD = 1.7) in group V-CTC, 35.3 mm (SD = 2.1) in group V-S and 33.6 mm (SD = 1.4) in group P. Small, albeit significant intergroup differences were found between the V-S and P groups after 2 years of retention (T2) and this difference remained at T3 (Table 2).
The mean intermolar width and the mean arch length decreased in all groups because of extraction of premolars. The mean intermolar
Table 1. Postretention.
5 years 6 years 7 years 8 years 9 years
V-CTC 13 1 1 1V-S 12 4 1P 15 1Totals 40 6 1 1 1
Table showing for how many years the 49 patients had been out of reten-tion at T3.
T3 Completed >5 years without
retentionn=17
10 girls and 7 boys
T3 Completed >5 years without
retentionn=16
12 girls and 4 boys
T3 Completed >5 years without
retentionn=16
11 girls and 5 boys
T2 Completed two-year retention
n=2417 girls and 7 boys
T2 Completed two-yearretention
n=2314 girls and 9 boys
T2 Completed two-year retention
n=2213 girls and 9 boys
T1 Group V-CTCn=25
18 girls and 7 boys
T1 Group V-Sn=25
14 girls and 11 boys
T1 Group Pn=25
13 girls and 12 boys
Randomized patients n=7545 girls and 30 boys
Declined to participate n=7 6 girls and 1 boy
Eligible patients with appliance in both jaws n=8251 girls and 31 boys
Unable to reach1 girl
Unable to reach2 boys
Unable to reach3 boys
Refused to participate
1 girl and 1 boyLeft the
district/unable to reach
5 girls and 2 boys
Refused to participate
2 boysLeft the
district/unable to reach
4 girls and 2 boys
Refused to participate
3 boysLeft the
district/unable to reach
2 girls and 4 boys
Figure 2. The flow diagram of the trial. Vacuum-formed retainer (VFR) in the maxilla and bonded canine-to-canine retainer in the mandible (group V-CTC), VFR in the maxilla and stripping of the mandibular incisors and canines (group V-S), and positioner covering erupted teeth (group P) at start of retention (T1), after 2 years of retention (T2) and after 2 years or more without retention (T3).
European Journal of Orthodontics, 2015, Vol. 37, No. 4348D
ownloaded from
https://academic.oup.com
/ejo/article/37/4/345/2570543 by guest on 01 January 2022

Tab
le 2
. M
ean
pre
-tre
atm
ent
mea
sure
men
ts (
mm
) o
f th
e m
axill
a (T
0), a
t th
e en
d o
f tr
eatm
ent/
star
t o
f th
e re
ten
tio
n t
reat
men
t (T
1), a
t th
e en
d o
f 2
year
s o
f re
ten
tio
n t
reat
men
t (T
2), a
nd
aft
er
5 o
r m
ore
yea
rs p
ost
rete
nti
on
(T
3) i
n t
he
thre
e re
ten
tio
n g
rou
ps:
rem
ovab
le v
acu
um
-fo
rmed
ret
ain
er (
VFR
) an
d b
on
ded
man
dib
ula
r ca
nin
e-to
-can
ine
reta
iner
(V-
CT
C),
VFR
an
d m
and
ibu
lar
ante
rio
r st
rip
pin
g (
V-S
), a
nd
po
siti
on
er (
P).
LII,
Litt
le’s
Irre
gu
lari
ty In
dex
.
Max
illa
V-C
TC
(n
= 16
)95
% c
onfid
ence
inte
rval
for
m
ean
V-S
(n
= 17
)95
% c
onfid
ence
inte
rval
for
m
ean
P (n
= 1
6)95
% c
onfid
ence
inte
rval
for
m
ean
Ana
lysi
s of
va
rian
ce
Mea
nSt
anda
rd
devi
atio
nL
ower
bou
ndU
pper
bou
ndM
ean
Stan
dard
de
viat
ion
Low
er b
ound
Upp
er b
ound
Mea
nSt
anda
rd
devi
atio
nL
ower
bou
ndU
pper
bou
nd
LII
T0
8.6
4.9
5.5
11.6
11.7
5.1
8.7
14.8
8.3
4.1
5.7
11.0
NS
LII
T1
0.4*
**0.
40.
20.
70.
5***
0.5
0.3
0.8
0.5*
**0.
30.
30.
6N
SL
II T
20.
9*0.
90.
51.
41.
4**
1.0
0.9
1.9
1.7*
*1.
50.
92.
5N
SL
II T
31.
8**
1.4
1.1
2.5
2.6*
*1.
51.
83.
32.
3*1.
91.
43.
3N
SIn
terc
anin
e w
idth
T0
34.5
2.3
33.0
36.0
34.8
3.8
32.6
36.9
35.0
2.7
33.3
36.7
NS
Inte
rcan
ine
wid
th T
136
.3*
1.6
35.4
37.1
36.6
*2.
735
.238
.036
.4*
1.7
35.5
37.3
NS
Inte
rcan
ine
wid
th T
235
.1**
*1.
634
.235
.935
.9**
2.4
34.6
37.1
34.1
***
1.5
33.3
34.9
0.03
6* V
-S/P
Inte
rcan
ine
wid
th T
334
.4*
1.7
33.5
35.3
35.3
*2.
134
.236
.433
.6*
1.4
32.8
34.3
0.02
5* V
-S/P
Inte
rmol
ar w
idth
T0
48.7
2.9
47.2
50.3
49.8
4.6
47.3
52.3
49.8
3.2
48.0
51.6
NS
Inte
rmol
ar w
idth
T1
48.7
1.5
47.9
49.5
48.9
2.9
47.4
50.4
49.7
2.2
48.5
50.8
NS
Inte
rmol
ar w
idth
T2
47.6
**2.
046
.548
.647
.7**
3.5
46.0
49.5
48.1
***
2.0
47.0
49.1
NS
Inte
rmol
ar w
idth
T3
46.8
**1.
945
.747
.847
.2**
3.5
45.4
48.9
47.4
**1.
846
.448
.3N
SA
rch
leng
th T
028
.83.
227
.130
.529
.13.
127
.430
.729
.13.
127
.431
.1N
SA
rch
leng
th T
123
.1**
*1.
422
.423
.922
.6**
*2.
121
.523
.622
.5**
*3.
220
.824
.2N
SA
rch
leng
th T
223
.21.
722
.324
.122
.51.
821
.623
.422
.51.
721
.623
.5N
SA
rch
leng
th T
322
.8*
1.7
21.9
23.7
22.3
2.2
21.1
23.4
21.8
**1.
720
.922
.7N
S
Wit
hin
grou
ps t
he t
-tes
t sh
ows
the
sign
ifica
nce
corr
espo
ndin
g to
the
pre
viou
s ti
me
poin
t. N
S, n
ot s
igni
fican
t.*P
< 0
.05,
**P
< 0
.01,
***
P <
0.0
01.
G. Edman Tynelius et al. 349D
ownloaded from
https://academic.oup.com
/ejo/article/37/4/345/2570543 by guest on 01 January 2022
Tab
le 3
. M
ean
pre
-tre
atm
ent m
easu
rem
ents
(mm
) fo
r th
e m
and
ible
(T0)
, at t
he
end
of t
reat
men
t/st
art o
f th
e re
ten
tio
n tr
eatm
ent (
T1)
, at t
he
end
of 2
yea
rs o
f ret
enti
on
trea
tmen
t (T
2), a
nd
aft
er
5 o
r m
ore
yea
rs p
ost
rete
nti
on
(T
3) i
n t
he
thre
e re
ten
tio
n g
rou
ps:
rem
ovab
le v
acu
um
-fo
rmed
ret
ain
er (
VFR
) an
d b
on
ded
man
dib
ula
r ca
nin
e-to
-can
ine
reta
iner
(V-
CT
C),
VFR
an
d m
and
ibu
lar
ante
rio
r st
rip
pin
g (
V-S
), a
nd
po
siti
on
er (
P).
LII,
Litt
le’s
Irre
gu
lari
ty In
dex
.
Man
dibl
e
V-C
TC
(n
= 16
)95
% c
onfid
ence
inte
rval
for
m
ean
V-S
(n
= 17
)95
% c
onfid
ence
inte
rval
for
m
ean
P (n
= 1
6)95
% c
onfid
ence
inte
rval
for
m
ean
Mea
nSt
anda
rd
devi
atio
nL
ower
bou
ndU
pper
bou
ndM
ean
Stan
dard
de
viat
ion
Low
er b
ound
Upp
er b
ound
Mea
nSt
anda
rd
devi
atio
nL
ower
bou
ndU
pper
bou
ndA
naly
sis
of
vari
ance
LII
T0
6.2
4.0
4.1
8.4
7.0
4.3
4.7
9.3
5.6
3.4
3.8
7.4
NS
LII
T1
0.4*
**0.
30.
20.
60.
3***
0.5
0.1
0.5
0.3*
**0.
40.
10.
6N
SL
II T
20.
9*0.
70.
51.
21.
2**
1.1
0.7
1.8
2.1*
**1.
71.
33.
00.
015*
V-
CT
C/P
LII
T3
2.1*
**0.
91.
62.
52.
0**
1.9
1.1
3.0
3.4*
*2.
12.
34.
50.
037*
V-S
/PIn
terc
anin
e w
idth
T0
26.2
2.5
24.9
27.6
26.3
2.4
25.1
27.6
26.3
1.8
25.4
27.3
NS
Inte
rcan
ine
wid
th T
127
.31.
626
.428
.127
.7**
1.9
26.7
28.7
27.3
*1.
026
.827
.8N
SIn
terc
anin
e w
idth
T2
27.5
1.6
26.6
28.3
26.8
**2.
225
.728
.026
.0**
*1.
225
.326
.6N
SIn
terc
anin
e w
idth
T3
26.6
**1.
425
.927
.426
.5*
2.2
25.3
27.6
25.4
**1.
524
.626
.1N
SIn
term
olar
wid
th T
044
.22.
143
.145
.344
.83.
443
.146
.644
.72.
643
.446
.1N
SIn
term
olar
wid
th T
141
.8**
*1.
940
.742
.942
.2**
2.6
40.9
43.5
43.0
*2.
141
.944
.1N
SIn
term
olar
wid
th T
241
.91.
741
.042
.841
.62.
740
.243
.041
.5*
2.1
40.4
42.6
NS
Inte
rmol
ar w
idth
T3
40.9
**1.
740
.041
.840
.8**
*3.
139
.342
.440
.9**
2.7
39.4
42.3
NS
Arc
h le
ngth
T0
23.7
2.3
22.5
25.0
23.5
2.5
22.3
24.8
23.4
2.5
22.0
24.7
NS
Arc
h le
ngth
T1
17.9
***
1.3
17.2
18.6
17.9
***
1.7
17.0
18.8
17.4
***
1.3
16.7
18.1
NS
Arc
h le
ngth
T2
18.2
1.9
17.2
19.2
17.7
1.6
16.9
18.5
17.6
1.4
16.9
18.4
NS
Arc
h le
ngth
T3
17.1
***
1.7
16.2
18.0
17.3
**1.
716
.418
.216
.9**
*1.
216
.317
.5N
S
Wit
hin
grou
ps t
he t
-tes
t sh
ows
the
sign
ifica
nce
corr
espo
ndin
g to
the
pre
viou
s ti
me
poin
t. N
S, n
ot s
igni
fican
t.*P
< 0
.05,
**P
< 0
.01,
***
P <
0.0
01.
European Journal of Orthodontics, 2015, Vol. 37, No. 4350D
ownloaded from
https://academic.oup.com
/ejo/article/37/4/345/2570543 by guest on 01 January 2022
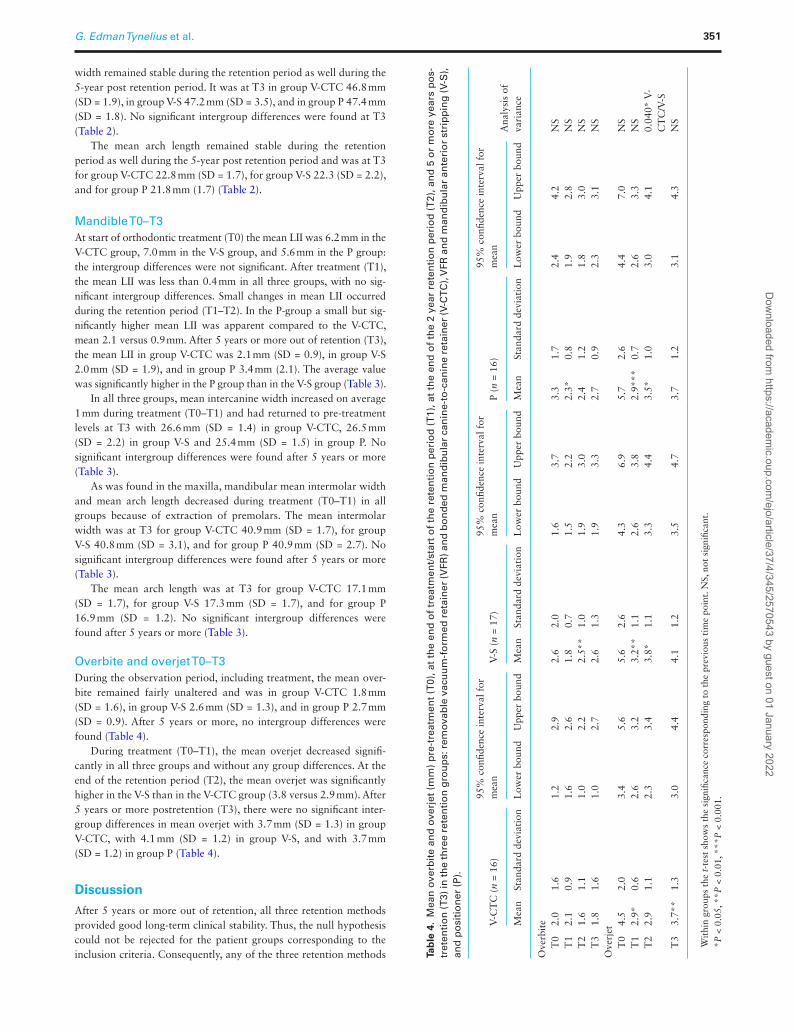
width remained stable during the retention period as well during the 5-year post retention period. It was at T3 in group V-CTC 46.8 mm (SD = 1.9), in group V-S 47.2 mm (SD = 3.5), and in group P 47.4 mm (SD = 1.8). No significant intergroup differences were found at T3 (Table 2).
The mean arch length remained stable during the retention period as well during the 5-year post retention period and was at T3 for group V-CTC 22.8 mm (SD = 1.7), for group V-S 22.3 (SD = 2.2), and for group P 21.8 mm (1.7) (Table 2).
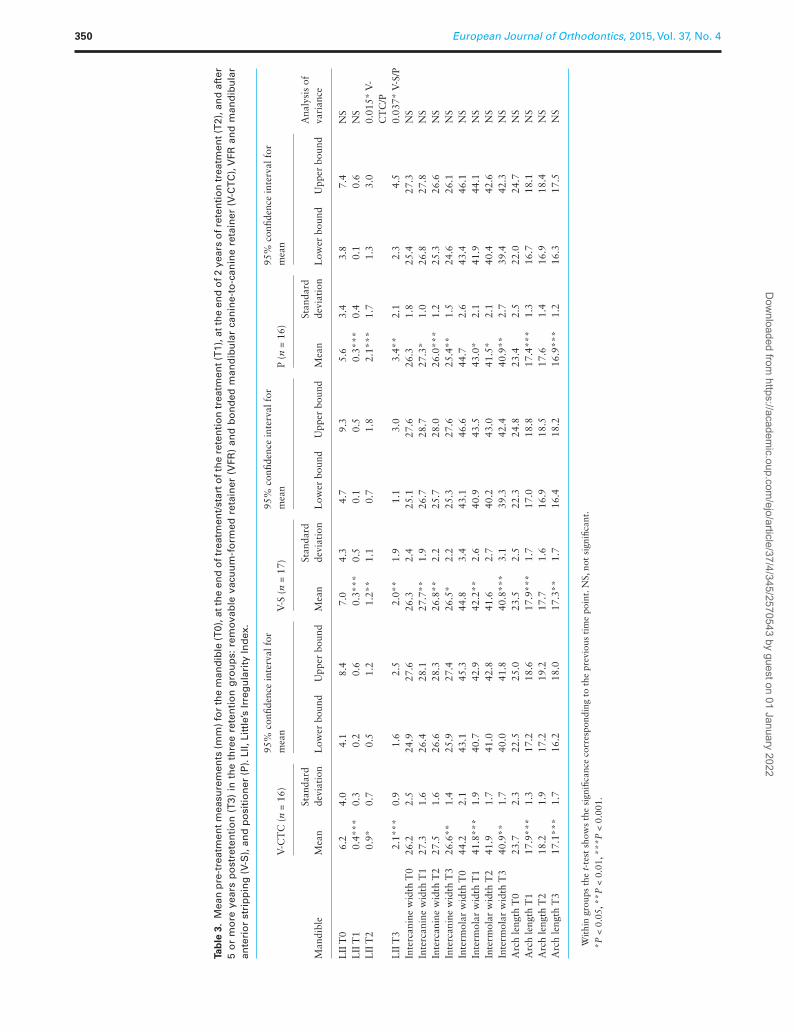
Mandible T0–T3At start of orthodontic treatment (T0) the mean LII was 6.2 mm in the V-CTC group, 7.0 mm in the V-S group, and 5.6 mm in the P group: the intergroup differences were not significant. After treatment (T1), the mean LII was less than 0.4 mm in all three groups, with no sig-nificant intergroup differences. Small changes in mean LII occurred during the retention period (T1–T2). In the P-group a small but sig-nificantly higher mean LII was apparent compared to the V-CTC, mean 2.1 versus 0.9 mm. After 5 years or more out of retention (T3), the mean LII in group V-CTC was 2.1 mm (SD = 0.9), in group V-S 2.0 mm (SD = 1.9), and in group P 3.4 mm (2.1). The average value was significantly higher in the P group than in the V-S group (Table 3).
In all three groups, mean intercanine width increased on average 1 mm during treatment (T0–T1) and had returned to pre-treatment levels at T3 with 26.6 mm (SD = 1.4) in group V-CTC, 26.5 mm (SD = 2.2) in group V-S and 25.4 mm (SD = 1.5) in group P. No significant intergroup differences were found after 5 years or more (Table 3).
As was found in the maxilla, mandibular mean intermolar width and mean arch length decreased during treatment (T0–T1) in all groups because of extraction of premolars. The mean intermolar width was at T3 for group V-CTC 40.9 mm (SD = 1.7), for group V-S 40.8 mm (SD = 3.1), and for group P 40.9 mm (SD = 2.7). No significant intergroup differences were found after 5 years or more (Table 3).
The mean arch length was at T3 for group V-CTC 17.1 mm (SD = 1.7), for group V-S 17.3 mm (SD = 1.7), and for group P 16.9 mm (SD = 1.2). No significant intergroup differences were found after 5 years or more (Table 3).
Overbite and overjet T0–T3During the observation period, including treatment, the mean over-bite remained fairly unaltered and was in group V-CTC 1.8 mm (SD = 1.6), in group V-S 2.6 mm (SD = 1.3), and in group P 2.7 mm (SD = 0.9). After 5 years or more, no intergroup differences were found (Table 4).
During treatment (T0–T1), the mean overjet decreased signifi-cantly in all three groups and without any group differences. At the end of the retention period (T2), the mean overjet was significantly higher in the V-S than in the V-CTC group (3.8 versus 2.9 mm). After 5 years or more postretention (T3), there were no significant inter-group differences in mean overjet with 3.7 mm (SD = 1.3) in group V-CTC, with 4.1 mm (SD = 1.2) in group V-S, and with 3.7 mm (SD = 1.2) in group P (Table 4).
Discussion
After 5 years or more out of retention, all three retention methods provided good long-term clinical stability. Thus, the null hypothesis could not be rejected for the patient groups corresponding to the inclusion criteria. Consequently, any of the three retention methods Ta
ble
4.
Mea
n o
verb
ite
and
ove
rjet
(m
m)
pre
-tre
atm
ent
(T0)
, at
the
end
of
trea
tmen
t/st
art
of
the
rete
nti
on
per
iod
(T
1), a
t th
e en
d o
f th
e 2
year
ret
enti
on
per
iod
(T
2), a
nd
5 o
r m
ore
yea
rs p
os-
tret
enti
on
(T3)
in th
e th
ree
rete
nti
on
gro
up
s: r
emov
able
vac
uu
m-f
orm
ed r
etai
ner
(VFR
) an
d b
on
ded
man
dib
ula
r ca
nin
e-to
-can
ine
reta
iner
(V-C
TC
), V
FR a
nd
man
dib
ula
r an
teri
or
stri
pp
ing
(V-S
),
and
po
siti
on
er (
P).
V-C
TC
(n
= 16
)95
% c
onfid
ence
inte
rval
for
m
ean
V-S
(n
= 17
)95
% c
onfid
ence
inte
rval
for
m
ean
P (n
= 1
6)95
% c
onfid
ence
inte
rval
for
m
ean
Ana
lysi
s of
va
rian
ceM
ean
Stan
dard
dev
iati
onL
ower
bou
ndU
pper
bou
ndM
ean
Stan
dard
dev
iati
onL
ower
bou
ndU
pper
bou
ndM
ean
Stan
dard
dev
iati
onL
ower
bou
ndU
pper
bou
nd
Ove
rbit
e
T0
2.0
1.6
1.2
2.9
2.6
2.0
1.6
3.7
3.3
1.7
2.4
4.2
NS
T
12.
10.
91.
62.
61.
80.
71.
52.
22.
3*0.
81.
92.
8N
S
T2
1.6
1.1
1.0
2.2
2.5*
*1.
01.
93.
02.
41.
21.
83.
0N
S
T3
1.8
1.6
1.0
2.7
2.6
1.3
1.9
3.3
2.7
0.9
2.3
3.1
NS
Ove
rjet
T
04.
52.
03.
45.
65.
62.
64.
36.
95.
72.
64.
47.
0N
S
T1
2.9*
0.6
2.6
3.2
3.2*
*1.
12.
63.
82.
9***
0.7
2.6
3.3
NS
T
22.
91.
12.
33.
43.
8*1.
13.
34.
43.
5*1.
03.
04.
10.
040*
V-
CT
C/V
-S
T3
3.7*
*1.
33.
04.
44.
11.
23.
54.
73.
71.
23.
14.
3N
S
Wit
hin
grou
ps t
he t
-tes
t sh
ows
the
sign
ifica
nce
corr
espo
ndin
g to
the
pre
viou
s ti
me
poin
t. N
S, n
ot s
igni
fican
t.*P
< 0
.05,
**P
< 0
.01,
***
P <
0.0
01.
G. Edman Tynelius et al. 351D
ownloaded from
https://academic.oup.com
/ejo/article/37/4/345/2570543 by guest on 01 January 2022

can be recommended in patients with space deficiency in both jaws, when treatment involves extraction of four premolars followed by fixed straight-wire appliances.
Main findingsThere are a number of studies evaluating stability after orthodontic treatment (3,6,16–19). However, to our knowledge, this is the first RCT specifically designed to evaluate and compare three different retention strategies for counteracting relapse at least 5 years out of retention. Thus, no comparison can be made with previous studies.
Whilst not directly comparable, a few RCTs of short-term stabil-ity of orthodontic treatment results have previously been published (7,8,20,21). These also demonstrated and confirmed our results that small but not clinically significant movements of teeth occurred.
From the second day after debonding, the patients in the V-CTC and V-S groups wore their VFRs only at night. This regimen was based on a report of equal stability of treatment result following full- or part-time wear of Essix retainers (8). Vacuum-formed Essix retainers have been shown to be superior to Hawley retainers in retaining the maxillary anterior teeth and were thus the option of choice (7). LII increased in patients with canine-to-canine retainers in the present study: this is in accordance with other studies (19). In group V-CTC, it was obvious that the canine-to-canine retainers held the intercanine width well at T2, but the extraction sites opened up during retention treatment, i.e. the arch length increased and the overjet decreased compared to group V-S. This is probably due to a proclination of the lower front teeth but it cannot be confirmed cephalometrically as we did not take cephalograms at T2. At T3, teeth were free to move without any influence of retention devices and, thus, the groups grew similar.
The finding that stripping of the mandibular anterior teeth with-out any adjunctive methods was sufficient to retain the treatment result on a short-term basis has not previously been demonstrated in an RCT. A retrospective study reported that stripping of lower anterior teeth in combination with overcorrection of rotated teeth was sufficient to prevent relapse over a 3-year period (18). Stripping of lower anterior teeth after debonding instead of wearing fixed or removable retention appliances would probably have advantages, not only for the patient but also for the clinician, in terms of cost, chair-time, and the issue of lost appliances.
The positioner is an eruption guidance appliance used in the early mixed dentition (13). No research has been presented about the effectiveness of prefabricated positioners for retention of ortho-dontic treatment results. This study showed that the appliance could be used in the permanent dentition as a retention device but in the long-term perspective the positioner held the maxillary intercanine distance less well than the VFR and likewise the mandibular LII compared to the V-S group. Because the positioner is prefabricated, it may be a less costly alternative to appliances made by dental tech-nicians. However, a drawback is that the fitting cannot be as precise as retention appliances made on individual dental casts. A further disadvantage is that compliance is essential, but as the subjects were randomly allocated, this uncontrolled factor was evenly distributed among the groups.
GeneralizabilityAn RCT was selected in order to reduce the risk of error from such factors as selection bias, the clinician's preferred treatment method and patient compliance. Furthermore, random allocation of sub-jects reduces bias and confounding variables by ensuring that both
known and unknown determinants of outcome are evenly distrib-uted among the subjects. The prospective design also ensures that the baseline characteristics, treatment progression, and side-effects can be strictly controlled and accurately observed.
The standardized treatment of all patients by the same orthodontic team makes it a valid comparison of the actual treatment methods. In most cases there was substantial pre-treatment crowding (T0). In all groups, the mean LII after treatment (T1) was below or equal to 0.5 mm in both jaws, indicating successfully treated cases (Tables 2 and 3). However, the mean intercanine width was generally somewhat expanded after treatment and relapse could be expected: the mean intercanine widths had returned to pre-treatment values in all groups.
LimitationsIn a long-term study, the effect of attrition on outcomes must be con-sidered and some attrition is inevitable. Hence, in the present study the attrition rate was acceptable and according to the sample size calcula-tion, the number of subjects remaining in each group was adequate to ensure that the outcomes were not biased by loss of data.
The standardized treatment of all patients by the same ortho-dontic team could be a drawback as the same possible mistakes may have been made on all patients.
The use of LII for measuring relapse of tooth positions may have some limitations: it tends to exaggerate cases with consid-erable irregularity but little length shortage, i.e. a rotated tooth without crowding (14). Another drawback with the LII is that it does not include the distal contact point of the canine. This means that canines can be in a very crowded position without LII showing it.
In any retention treatment with removable appliances, the responsibility and result lies with the patient and is out of control to the orthodontist.
At the final registration, all patients in this trial had reached adulthood. This means that overall growth had ceased but this does not imply that changes in occlusion, arch dimensions, and tooth position cannot occur. Thus, the increase in Little's index and dimin-ished intercanine widths found in all groups during the postretention period could coincide with the normal physiological changes during the same period of time (22,23).
New studies are needed to confirm the results of this study.
Conclusions
After 5 years or more out of retention, the three retention meth-ods had achieved equally favourable clinical results. Thus a maxil-lary VFR combined with a bonded canine-to-canine retainer in the mandible; a maxillary VFR combined with stripping of the man-dibular anterior teeth and a prefabricated positioner can all be rec-ommended. Hence, the clinician is not limited to routine use of a bonded mandibular canine-to-canine retainer: choice of retention method can be individualized, taking into account such variables as orthodontic diagnosis, the expected level of patient compliance and the patient’s wishes and financial considerations.
Funding
Scania County Council, Sweden; the Swedish Dental Society and the Faculty of Odontology, Malmö University, Sweden.
Conflict of interest statement. None declared.
European Journal of Orthodontics, 2015, Vol. 37, No. 4352D
ownloaded from
https://academic.oup.com
/ejo/article/37/4/345/2570543 by guest on 01 January 2022

References 1. Melrose, C. and Millett, D. (1998) Toward a perspective on orthodontic
retention? American Journal of Orthodontics and Dentofacial Orthope-dics, 113, 507–514.
2. Boese, L.R. (1980) Fiberotomy and reproximation without lower reten-tion 9 years in retrospect: part II. The Angle Orthodontist, 50, 169–178.
3. Little, R.M. (1990) Stability and relapse of dental arch alignment. British Journal of Orthodontics, 17, 235–241.
4. Zachrisson, B.U. (1997) Important aspects of long-term stability. Journal of Clinical Orthodontics, 31, 562–583.
5. Myser, S.A., Campel, P.M., Boley, J. and Buschang, P.H. (2013) Long-term stability: postretention changes of the mandibular anterior teeth. Ameri-can Journal of Orthodontics and Dentofacial Orthopedics, 44, 420–429.
6. Littlewood, S.J., Millett, D.T., Doubleday, B., Bearn, D.R. and Worthing-ton, H.V. (2006) Retention procedures for stabilising tooth position after treatment with orthodontic braces. The Cochrane Library, 3, CD002283.
7. Rowland, H., Hichens, L., Williams, A., Hills, P., Killingback, N., Ewings, P., Clark, S., Ireland, A.J. and Sandy, J.R. (2007) The effectiveness of Haw-ley and vacuum-formed retainers: a single-center randomized controlled trial. American Journal of Orthodontics and Dentofacial Orthopedics, 132, 730–737.
8. Gill, D.S., Naini, F.B., Jones, A. and Tredwin, C.J. (2007) Part-time ver-sus full-time retainer wear following fixed appliance therapy: a rand-omized prospective controlled trial. World Journal of Orthodontics, 8, 300–306.
9. Edman Tynelius, G., Bondemark, L. and Lilja-Karlander, E. (2010) Evalu-ation of orthodontic treatment after 1 year of retention – a randomized controlled trial. European Journal of Orthodontics, 32, 542–547.
10. Edman Tynelius, G., Bondemark, L. and Lilja-Karlander, E. (2013) A randomized controlled trial of three orthodontic retention methods in Class I four premolar extraction cases – stability after 2 years in retention. Orthodontics & Craniofacial Research, 16, 105–115.
11. McLaughlin, R.P., Bennett, J. and Trevisi, H. (2001) Systemized Orthodon-tic Treatment Mechanics. Mosby International Ltd, London.
12. Joseph, V.P., Rossouw, P.E. and Basson, N.J. (1992) Orthodontic micro-abrasive reproximation. American Journal of Orthodontics and Dentofa-cial Orthopedics, 102, 351–359.
13. Keski-Nisula, K., Hernesniemi, R., Heiskanen, M., Keski-Nisula, L. and Varrela, J. (2008) Orthodontic intervention in the early mixed dentition: a prospective, con-trolled study on the effects of the eruption guidance appliance. American Journal of Orthodontics and Dentofacial Orthopedics, 133, 254–260; quiz 328.e2.
14. Little, R.M. (1975) The irregularity index: a quantitative score of mandib-ular anterior alignment. American Journal of Orthodontics, 68, 554–563.
15. Dahlberg, G. (1940) Statistical Methods for Medical Biological Students. Allen and Unwin, London, pp. 122–132.
16. Reitan, K. (1967) Clinical and histologic observations on tooth movement during and after orthodontic treatment. American Journal of Orthodon-tics, 53, 721–745.
17. Taner, T., Haydar, B. and Kavuklu, I. (2000) Short-term effects of fiber-otomy on relapse of anterior crowding. American Journal of Orthodontics and Dentofacial Orthopedics, 118, 617–623.
18. Aasen, T.O. and Espeland, L. (2005) An approach to maintain orthodontic alignment of lower incisors without the use of retainers. European Journal of Orthodontics, 27, 209–214.
19. Atack, N., Harradine, N., Sandy, J.R. and Ireland, A.J. (2007) Which way forward? Fixed or removable lower retainers. The Angle Orthodontist, 77, 954–959.
20. Jäderberg, S., Feldmann, I. and Engström, C. (2012) Removable thermo-plastic appliances as orthodontic retainers—a prospective study of differ-ent wear regimens. European Journal of Orthodontics, 34, 475–479.
21. Lindauer, S.J. and Shoff, R.C. (1998) Comparison of Essix and Hawley retainers. Journal of Clinical Orthodontics, 32, 95–97.
22. Thilander, B. (2009) Dentoalveolar development in subjects with normal occlusion. A longitudinal study between the ages of 5 and 31 years. Euro-pean Journal of Orthodontics, 31, 109–120.
23. Tsiopas, N., Nilner, M., Bondemark, L. and Bjerklin, K. (2013) A 40 years follow-up of dental arch dimensions and incisor irregularity in adults. European Journal of Orthodontics, 35, 230–235.
G. Edman Tynelius et al. 353D
ownloaded from
https://academic.oup.com
/ejo/article/37/4/345/2570543 by guest on 01 January 2022
Related Documents











