Endocrine – Adrenal Gland Part 1

Endocrine – Adrenal Gland
Feb 13, 2016
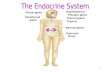
Endocrine – Adrenal Gland. Part 1. Adrenal Gland. Description AKA Suprarenal gland Location On top of each kidney Composed of: Adrenal cortex Adrenal Medulla. Hormone & Function. Adrenal Cortex Mineralocortioids Aldosterone Function Regulates electrolyte & fluid homeostasis. - PowerPoint PPT Presentation
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Endocrine – Adrenal Gland
Part 1

Adrenal Gland
• Description– AKA
• Suprarenal gland
– Location• On top of each kidney
– Composed of:• Adrenal cortex• Adrenal Medulla

Hormone & Function
• Adrenal Cortex– Mineralocortioids
• Aldosterone
– Function• Regulates electrolyte
& fluid homeostasis

Hormone & Function
• Adrenal Cortex– Glucocorticoids
• Cortisol• Hydrocortisone
– Function• Stim. gluconeogenesis
& blood glucose• Anti-inflammatory• Anti-immunity• Anti- allergy

Hormone & Function
• Adrenal Cortex– Androgen
• Sex hormones
– Function• Female
– Stim. Sex drive
• Men– Negligible

Hormone & Function
• Adrenal Medulla– Epinephrine
• Adrenaline
– Function• Prolong & SNS
(sympathetic nervous system) response to stress

Hormone & Function
• Adrenal Medulla– Norepinephrine– Function
• Prolong & SNS (sympathetic nervous system) response to stress

Effects of Epinephrine & Norepinephrine
a. cardiac outputb. metabolic ratec. Vasoconstrictiond. respiratory rate

Adrenal Cortex
• The cortex synthesizes & secretes 30+ different steroids. – Glucocorticoids– Mineralocorticoids– Androgens

Learning Tip
SALT, SUGAR & SEX• Aldosterone =
promotes salt retention
• Cortisol= sugar• Androgens = sex
hormones

Negative feedback loop
• Stress • Hypothalamus • Stimulates Anterior Pituitary • Secretes ACTH target cell • Adrenal cortex • Secretes Cortisol specific action• metabolic activity • Helps manage stress

Cushing disease/ syndrome
• Description– Cortisol excess

Cushing disease/ syndrome
• Pathyophysiology– Diurnal rhythm
• in AM
– Normal secretion of cortisol in times of stress– In Cushing's, cortisol is hypersecreted without
regard to stress or time of day.

Cushing disease/ syndrome
• Etiology– secretions ACTH– Pituitary CA– Lung tumor– **#1 prolonged use of glucocorticoid meds for
inflammatory disorders• Rheumatoid arthritis• COPD

Cushing disease/ syndrome
• Etiology– Iatrogenic
• Caused by treatment or diagnostic procedure
– Females > Male

Cushing disease/ syndrome
• Signs & Symptoms– Adiposity
• Deposits of adipose tissue in the face, neck & trunk
• Moon shaped face• Buffalo hump

Cushing disease/ syndrome
• S&S– Weight gain– Na & H20 retention– K+ is lost
• Hypokalemia– Purple striae on the
abdomen– Hirsutism–

Cushing disease/ syndrome
• S&S– This extremities d/t
muscle wasting– Boys = early onset of
puberty– Girls = masculine
characteristics– C/O fatigue, muscle
weakness, sleep disturbance, amenorrhea, libido, irritability, emotional labiality

Cushing disease/ syndrome
• S&S– Could be:
• Petechiae• Eccymoses• wound healing• Swollen ankles

Cushing disease/ syndrome
Complications• calcium reabsorption from the bone leading to
osteoporosis & pathologic fractures• Cortisol causes insulin resistance and• ↑hepatic gluconeogenesis and insulin resistance• Leads to glucose intolerance and diabetes mellitus

Cushing disease/ syndrome
Complications• Frequent infections & slow wound healing
– Suppressed inflammatory response can mask severe infections
– Cortisol is an immunosuppressive• Deceased ability to handle stress
– Psych problems i.e. mood swings

Cushing disease/ syndrome
• Diagnosis– Plasma Corticol level– ACTH level– Adrenalangiography

Cushing disease/ syndrome
Medical management• Early dectection key• #1 goal = restore
hormonal balance• Usually meds.

Cushing disease/ syndrome
Med. Management• Tx based on causative
factor• If adrenal cancer
– Surgery• If caused by steroid
meds – Change regiment– Risk to benefit
analysis

Cushing disease/ syndrome
• Surgical management• If pituitary gland
– Hypophysectomy• If adrenal tumor
– Adrenalectomy

Cushing disease/ syndrome
• Aminoglutethimide (cytadren)– Action
• Inhibits synthesis of adrenal steroids
– S/E• Dizziness or drowsiness
– Nrs.• Instruct to avoid
activities that need mental alertness

Cushing disease/ syndrome
• Ketoconazole (Nizoral)– Action
• Antifungal• Inhibits adrenal
steroidogenesis

Cushing disease/ syndrome
Diet• High in protein• High K+• Low sodium• Reduces carbs &
calories

Cushing disease/ syndrome
Nursing Management• Rx history• VS• Lung auscultation
– Crackles• Edema• Skin integrity• Glucose levels• S&S of infection

Adrenalectomy
• Pre-op– Electrolyte imbalance– Hyperglycemia– Prevent adrenal crisis
• Administer glucocorticoids!
• Sudden drop in hormones crisis

Adrenalectomy
• Post-op– Fluid & electrolyte
changes– Replace
glucocorticoids, mineralocorticoids for life
– Bilateral???

Addison’s Disease
• Description– corticol– Adrenal hypofunction– Adrenal insufficiency– Adrenalcortical
insufficiency

Addison’s Disease
• Pathophysiology– 90% of adrenal gland
destroyed– Autoimmune disease– Primary
• ACTH may be high
– Secondary• ACTH will be low

Addison’s Disease
Etiology• Primary
– Bilateral adrenalectomy
• Secondary– ACTH from pituitary– hypothalamus
stimulation

Addison’s Disease
Etiology• Prolonged use of
coticosteroid Rx • ACTH • hormonal release
from adrenal gland• *** esp. at risk if drugs
abruptly DC’ed– Taper dose

Addison’s Disease:Signs & Symptoms
• Hypotension– Lack of aldosterone
– Na+ & H2O loss– K+ reabsorption
• Tachycardia• Orthostatic
hypotension

Addison’s Disease:Signs & Symptoms
• Bronze coloration of skin
• Hypoglycemia• Vitiglio• Fatigue, muscle
weakness• Weight loss• Crave salty foods

Addison’s Disease:Signs & Symptoms
• tolerance for stress– Anxious– Irritable– Confused
• Pulse– Weak
• GI upset– N/V– Anorexia

Addison’s disease: Complications
• Adrenal crisis– Acute Addison’s dis– May occur
• Trauma• Surgery• Stress• Abrupt withdrawl of
cortisone meds

Addison’s disease: Complications
• Adrenal Crisis– S&S
• Na+ & H20 loss• Hypotension• Dehydration• Tachycardia
– IV & administer hydrocortisone

Addison’s disease: Medical Management
• Restore fluid and electrolyte balance
• Replacement of deficient adrenal hormones– Glucocorticoids
(hydrocortisone)– Mineralocorticoids
(fludrocortisone)

Addison’s disease: Pharmacological
• Lifetime steroids• Glucocorticoids
– Hydrocortisone (hydrocortone)
• Mineralocorticoids – Fludrocortisone
acetate (Florinef)• Diurnal rhythm
– 2/3 AM– 1/3 PM

Addison’s disease: Diet
• High in Na+• Low in K+

Addison’s disease: Nursing Management
• Diagnosis???• Fluid volume deficit
– r/t • Na+ level• Vomiting• renal losses
– A.M.B.• Poor skin turgor• Weight loss• Orthostatic
hypotension

Addison’s disease: Nursing Management
• qDay wts• I&O• Glucose• K+ & Na+• Skin turgor• Orthostatic
hypotension

Hypofunction Hyperfunction
Disorder Addison’s disease
Cushing syndrome
S&S Na+ & H20 lossHypotensionHypoglycemiaFatigueHyperkalemia
Na+ & H20 retention Wt. gainHyperglycemiaBuffalo humpMoon faceHypokalemia

Hypofunction Hyperfunction
Usual tx GlucocorticoidsMeneralocorticoidRestore fluid
Alter steroid RxSurgery
Nrs Dx Fluid volume deficit Fluid volume excessGlucose intolerance
Diet Na+ K+
Na+ K+

Pheochromocytoma:Description
• AKA chromaffin cell tumor
• Rare disease• Characterized by
paroxysmal or sustained hypertension– d/t excess secretion
of epi and norepi

Pheochromocytoma:Pathophysiology
• Caused by a tumor– Usually Rt. adrenal
• Etiology– Idiopathic
• Stress can bring on an attack

Pheochromocytoma:Signs & Symptoms
• HTN– > 115 mmHG diastolic– Intermittent– Unstable
• Tachycardia• Unrelenting H/A• Profuse diaphoresis• Palpitations

Pheochromocytoma:Signs & Symptoms
• Visual disturbances• N/V• Feeling of
apprehension• Elevated blood glucose
levels

Pheochromocytoma:Complications
• Stroke• Retinopathy• Heart disease• Kidney damage

Pheochromocytoma:Medical Management / Surgical
• Treatment of choice is…– Surgery
• Stable a surgery• Adrenal gland
removed• BP

Pheochromocytoma:Pharmacological
• Phentolamine mesylate (Regitine)
• Nitroprusside sodium (Nipride)– HTN

Pheochromocytoma:Diet
• protein• Avoid caffeine

Pheochromocytoma:Nursing Management
• Monitor BP• VS• Na+ levels
Related Documents