Early Intervention for Children With Autism Spectrum Disorder Under 3 Years of Age: Recommendations for Practice and Research abstract This article reviews current evidence for autism spectrum disorder (ASD) interventions for children aged ,3 years, based on peer- reviewed articles published up to December 2013. Several groups have adapted treatments initially designed for older, preschool-aged children with ASD, integrating best practice in behavioral teaching methods into a developmental framework based on current scientific understanding of how infants and toddlers learn. The central role of parents has been emphasized, and interventions are designed to in- corporate learning opportunities into everyday activities, capitalize on “teachable moments,” and facilitate the generalization of skills be- yond the familiar home setting. Our review identified several compre- hensive and targeted treatment models with evidence of clear benefits. Although some trials were limited to 8- to 12-week outcome data, enhanced outcomes associated with some interventions were evaluated over periods as long as 2 years. Based on this review, recommendations are proposed for clinical practice and future re- search. Pediatrics 2015;136:S60–S81 AUTHORS: Lonnie Zwaigenbaum, MD, a Margaret L. Bauman, MD, b Roula Choueiri, MD, c Connie Kasari, PhD, d Alice Carter, PhD, e Doreen Granpeesheh, PhD, BCBA-D, f Zoe Mailloux, OTD, OTR/L, FAOTA, g Susanne Smith Roley, OTD, OTR/L, FAOTA, h Sheldon Wagner, PhD, i Deborah Fein, PhD, j Karen Pierce, PhD, k Timothy Buie, MD, l Patricia A. Davis, MD, m Craig Newschaffer, PhD, n Diana Robins, PhD, n Amy Wetherby, PhD, o Wendy L. Stone, PhD, p Nurit Yirmiya, PhD, q Annette Estes, PhD, r Robin L. Hansen, MD, s James C. McPartland, PhD, t and Marvin R. Natowicz, MD, PhD u a Department of Pediatrics, University of Alberta, Edmonton, Alberta, Canada; b Department of Anatomy and Neurobiology, Boston University School of Medicine, Boston, Massachusetts; c Division of Developmental and Behavioral Pediatrics, University of Massachusetts Memorial Children’ s Medical Center, Worcester, Massachusetts; d Graduate School of Education & Information Studies, University of California Los Angeles, Los Angeles, California; e Department of Psychology, University of Massachusetts, Boston, Massachusetts; f Center for Autism and Related Disorders, Tarzana, California; g Department of Occupational Therapy, Thomas Jefferson University, Philadelphia, Pennsylvania; h USC Mrs T.H. Chan Division of Occupational Science and Occupational Therapy, Los Angeles, California; i Behavioral Development & Educational Services, New Bedford, Massachusetts; j Department of Psychology, University of Connecticut, Storrs, Connecticut; k Department of Neurosciences, University of California San Diego, La Jolla, California; l Harvard Medical School and Massachusetts General Hospital for Children, Boston, Massachusetts; m Integrated Center for Child Development, Newton, Massachusetts; n A.J. Drexel Autism Institute, Drexel University, Philadelphia, Pennsylvania; o Department of Clinical Sciences, Florida State University College of Medicine, Tallahassee, Florida; p Departments of Psychology, and r Speech and Hearing Sciences, University of Washington, Seattle, Washington; q Department of Psychology, Hebrew University of Jerusalem Mount Scopus, Jerusalem, Israel; s Department of Pediatrics, University of California Davis MIND Institute, Sacramento, California; t Yale Child Study Center, New Haven, Connecticut; and u Genomic Medicine Institute, Cleveland Clinic, Cleveland, Ohio ABBREVIATIONS ABA—applied behavior analysis ASD—autism spectrum disorder ESDM—Early Start Denver Model GRADE—Grading of Recommendations Assessment, Development, and Evaluation (Continued on last page) S60 ZWAIGENBAUM et al by guest on March 4, 2020 www.aappublications.org/news Downloaded from

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Early Intervention for Children With Autism SpectrumDisorder Under 3 Years of Age: Recommendations forPractice and Research
abstractThis article reviews current evidence for autism spectrum disorder(ASD) interventions for children aged ,3 years, based on peer-reviewed articles published up to December 2013. Several groupshave adapted treatments initially designed for older, preschool-agedchildren with ASD, integrating best practice in behavioral teachingmethods into a developmental framework based on current scientificunderstanding of how infants and toddlers learn. The central role ofparents has been emphasized, and interventions are designed to in-corporate learning opportunities into everyday activities, capitalize on“teachable moments,” and facilitate the generalization of skills be-yond the familiar home setting. Our review identified several compre-hensive and targeted treatment models with evidence of clearbenefits. Although some trials were limited to 8- to 12-week outcomedata, enhanced outcomes associated with some interventions wereevaluated over periods as long as 2 years. Based on this review,recommendations are proposed for clinical practice and future re-search. Pediatrics 2015;136:S60–S81
AUTHORS: Lonnie Zwaigenbaum, MD,a Margaret L.Bauman, MD,b Roula Choueiri, MD,c Connie Kasari, PhD,d
Alice Carter, PhD,e Doreen Granpeesheh, PhD, BCBA-D,f ZoeMailloux, OTD, OTR/L, FAOTA,g Susanne Smith Roley, OTD,OTR/L, FAOTA,h Sheldon Wagner, PhD,i Deborah Fein, PhD,j
Karen Pierce, PhD,k Timothy Buie, MD,l Patricia A. Davis,MD,m Craig Newschaffer, PhD,n Diana Robins, PhD,n AmyWetherby, PhD,o Wendy L. Stone, PhD,p Nurit Yirmiya, PhD,q
Annette Estes, PhD,r Robin L. Hansen, MD,s James C.McPartland, PhD,t and Marvin R. Natowicz, MD, PhDu
aDepartment of Pediatrics, University of Alberta, Edmonton,Alberta, Canada; bDepartment of Anatomy and Neurobiology,Boston University School of Medicine, Boston, Massachusetts;cDivision of Developmental and Behavioral Pediatrics, Universityof Massachusetts Memorial Children’s Medical Center, Worcester,Massachusetts; dGraduate School of Education & InformationStudies, University of California Los Angeles, Los Angeles,California; eDepartment of Psychology, University ofMassachusetts, Boston, Massachusetts; fCenter for Autism andRelated Disorders, Tarzana, California; gDepartment ofOccupational Therapy, Thomas Jefferson University, Philadelphia,Pennsylvania; hUSC Mrs T.H. Chan Division of OccupationalScience and Occupational Therapy, Los Angeles, California;iBehavioral Development & Educational Services, New Bedford,Massachusetts; jDepartment of Psychology, University ofConnecticut, Storrs, Connecticut; kDepartment of Neurosciences,University of California San Diego, La Jolla, California; lHarvardMedical School and Massachusetts General Hospital for Children,Boston, Massachusetts; mIntegrated Center for ChildDevelopment, Newton, Massachusetts; nA.J. Drexel AutismInstitute, Drexel University, Philadelphia, Pennsylvania;oDepartment of Clinical Sciences, Florida State University Collegeof Medicine, Tallahassee, Florida; pDepartments of Psychology,and rSpeech and Hearing Sciences, University of Washington,Seattle, Washington; qDepartment of Psychology, HebrewUniversity of Jerusalem Mount Scopus, Jerusalem, Israel;sDepartment of Pediatrics, University of California Davis MINDInstitute, Sacramento, California; tYale Child Study Center, NewHaven, Connecticut; and uGenomic Medicine Institute, ClevelandClinic, Cleveland, Ohio
ABBREVIATIONSABA—applied behavior analysisASD—autism spectrum disorderESDM—Early Start Denver ModelGRADE—Grading of Recommendations Assessment, Development,and Evaluation
(Continued on last page)
S60 ZWAIGENBAUM et al by guest on March 4, 2020www.aappublications.org/newsDownloaded from

The ultimate goal of early detection andscreening is to ensure that childrenwith autism spectrum disorder (ASD)can access evidence-based inter-ventions toprovide thebestopportunityfor optimal development and out-comes.1 With the advances reviewed byZwaigenbaum et al2,3 in this specialissue of Pediatrics, and the growingevidence that ASD can be diagnosedaccurately before 2 years of age,4,5 theneed for ASD treatment programsspecifically designed for this age grouphas never been greater. Some authorshave also argued that the second yearof life is a particularly critical de-velopmental period for children withASD, for various reasons. First, thesecond year is a dynamic period ofbrain growth, during which increasesin brain volume and atypical connec-tivity associated with ASD first emerge6,7
but also a time of substantial neuralplasticity providing greater potentialto alter developmental course.8 Sec-ond, a proportion of children with ASDreportedly regress in the second year.Recent research has indicated onlymodest agreement between retroac-tively reported regression and analysisof behavioral change as observed onserial home videos9 and that acute skillloss may exist along a continuum ofgradually declining trajectories of so-cial and communicative behavior.10,11
However, interventions during this pe-riod may counter the developmentalcascade that contributes to pro-gressive symptom development andultimately prevent ASD-related impair-ments before they fully manifest.8
Intervention approaches for childrenaged ,2 to 3 years need to be de-velopmentally appropriate. We cannotassume that findings from treatmentresearch involving older children withASD will generalize to infants and tod-dlers, who differ with respect to thenature of their social relationships aswell as their cognitive and communi-
cative processes. Infants depend onexperiential learning within their nat-ural environments and on interactionsrooted in social play that occur withinthe context of everyday caregivingactivities.1 Fortunately, over the pastseveral years, a growing number ofstudies have evaluated interventionsspecifically designed for children aged,2 to 3 years. An updated review ofthese interventions may provide neededdirection and guidelines to cliniciansand policy makers.
METHODS
Theworkinggroupconductedasearchofthe literature published online between2000 and 2012 related to interventionprograms provided to children with ASDaged ,3 years. The working groupsummarized published research oninterventions developed for use in chil-dren aged#36 months, even if the agerange of samples of children beingevaluated extended beyond age 3 years(Table 1). A PubMed search was con-ducted on June 30, 2010, for articlespublished since January 1, 2000, byusing the search terms (“child de-velopmental disorders, pervasive” or“autistic disorder/” or “autism [tw]” or“autistic [tw]”) and (“Early Intervention/”or “intervention [tw]”), with an agefilter (“infant, birth-23 months” or “Pre-school child, 2-5 years”) and limited toEnglish-language articles. This searchyielded 419 references, which werereviewed by Drs Zwaigenbaum andBauman, who selected articles focus-ing on clinical trials of developmental/behavioral interventions (ie, not medi-cations or trials of other biomedicaltherapies) that included children aged,36 months. Search results werecomplemented by additional pub-lications identified by working groupmembers. Hence, although the searchstrategy was comprehensive, selectionof articles was not systematic, which isan important limitation. A scoping ap-
proach, with some discretion of themultidisciplinary expert working group,was used instead to select articles ofhighest relevance.
Each selected study was assessed, andworking group members were asked toarrive at a consensus evaluation on eacharticle after a detailed discussion. Thesearch was updated by using the samestrategy to add articles published toDecember 31, 2013, which yielded anadditional 323 references; selectionwas again limited to clinical trials ofdevelopmental/behavioral interventionsthat included children aged,36months.The working group reviewed and ap-proved the final wording of the summaryand recommendations.
We recognize that in addition to com-prehensive early intervention programs,themanagement and treatment of youngchildren with ASD often involves speechand language and occupational andphysical therapies, as well as manage-ment of comorbid conditions such asassociated medical disorders (eg, sleep,gastrointestinal),12 anxiety, and chal-lenging and maladaptive behaviors.However, a review of these targetedinterventions was beyond the scope ofthe current initiative.
LITERATURE REVIEW
Table 1 summarizes the key featuresand outcomes of 24 randomized con-trolled, quasi-experimental, and open-label studies involving children withASD aged ,3 years reviewed by theworking group.13–38 Because few stud-ies focused exclusively on this agegroup, studies in which participantsincluded some children aged.3 yearswere assessed as long as there wassufficient information to draw infer-ences about younger children. Thegroup reviewed additional reports,which have not been listed in Table 1,including single-subject studies,39–44
other relevant studies,16,45–50 meta-analyses,51,52 and reviews.53–56
SUPPLEMENT ARTICLE
PEDIATRICS Volume 136, Supplement 1, October 2015 S61 by guest on March 4, 2020www.aappublications.org/newsDownloaded from
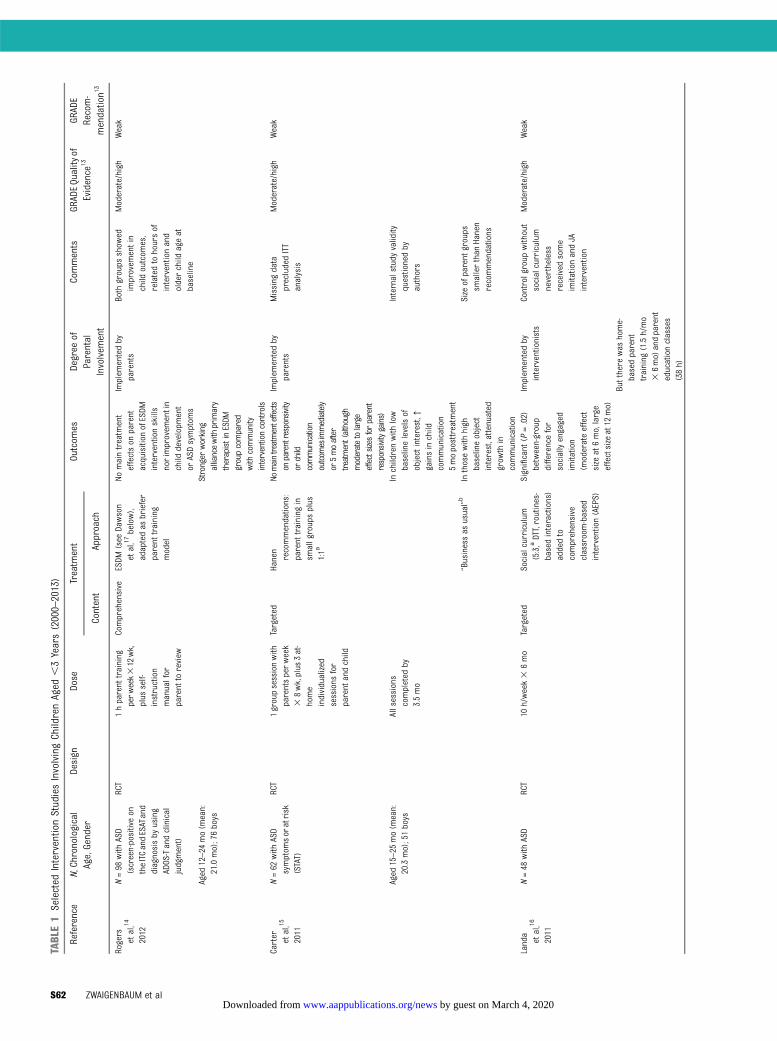
TABLE1
Selected
InterventionStudiesInvolvingChildrenAged
,3Years(2000–2013)
Reference
N,Chronological
Age,Gender
Design
Dose
Treatm
ent
Outcom
esDegree
ofParental
Involvem
ent
Comments
GRADEQuality
ofEvidence
13GR
ADE
Recom-
mendation1
3Content
Approach
Rogers
etal,14
2012
N=98
with
ASD
(screen-positiveon
theITCandESATand
diagnosisby
using
ADOS-Tandclinical
judgment)
RCT
1hparent
training
perw
eek312wk,
plus
self-
instruction
manualfor
parent
toreview
Comprehensive
ESDM
(see
Dawson
etal,17
below),
adaptedas
briefer
parent
training
model
Nomaintreatm
ent
effectson
parent
acquisition
ofESDM
interventionskills
norimprovem
entin
child
developm
ent
orASDsymptom
s
Implem
entedby
parents
Both
groups
show
edimprovem
entin
child
outcom
es,
relatedtohoursof
interventionand
olderchild
ageat
baseline
Moderate/high
Weak
Aged
12–24
mo(m
ean:
21.0mo);76boys
Stronger
working
alliancewith
primary
therapistinESDM
groupcompared
with
community
interventioncontrols
Carter etal,15
2011
N=62
with
ASD
symptom
soratrisk
(STAT)
RCT
1groupsessionwith
parentsperweek
38wk,plus
3at-
home
individualized
sessions
for
parent
andchild
Targeted
Hanen
recommendations:
parent
training
insm
allgroupsplus
1:1a
Nomaintreatmenteffects
onparentresponsivity
orchild
communication
outcom
esimmediately
or5moafter
treatment(although
moderatetolarge
effectsizes
forparent
responsivitygains)
Implem
entedby
parents
Missing
data
precludedITT
analysis
Moderate/high
Weak
Aged
15–25
mo(m
ean:
20.3mo);51boys
Allsessions
completed
by3.5mo
Inchildrenwith
low
baselinelevelsof
objectinterest,↑
gainsinchild
communication
5moposttreatm
ent
Internalstudyvalidity
questionedby
authors
“Businessas
usual”b
Inthosewith
high
baselineobject
interest,attenuated
grow
thin
communication
Size
ofparent
groups
smallerthan
Hanen
recommendations
Landa
etal,16
2011
N=48
with
ASD
RCT
10h/week3
6mo
Targeted
Socialcurriculum
(5:3,aDTT,routines-
basedinteractions)
addedto
comprehensive
classroom-based
intervention(AEPS)
Significant
(P=.02)
between-group
differencefor
sociallyengaged
imitation
(moderateeffect
size
at6mo,large
effectsizeat12
mo)
Implem
entedby
interventionists
Controlgroup
without
socialcurriculum
nevertheless
received
some
imitationandJA
intervention
Moderate/high
Weak
Butthere
was
home-
basedparent
training
(1.5h/mo
36mo)andparent
educationclasses
(38h)
S62 ZWAIGENBAUM et al by guest on March 4, 2020www.aappublications.org/newsDownloaded from
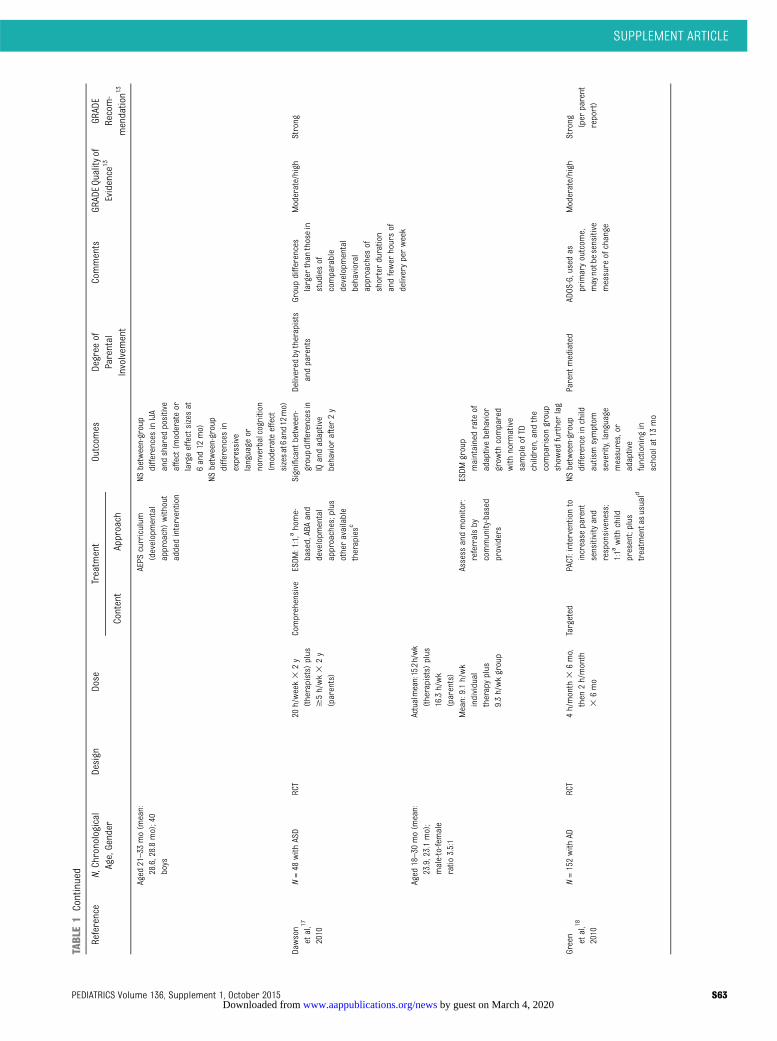
TABLE1
Continued
Reference
N,Chronological
Age,Gender
Design
Dose
Treatm
ent
Outcom
esDegree
ofParental
Involvem
ent
Comments
GRADEQuality
ofEvidence
13GR
ADE
Recom-
mendation1
3Content
Approach
Aged
21–33
mo(m
ean:
28.6,28.8mo);40
boys
AEPS
curriculum
(developmental
approach)without
addedintervention
NSbetween-group
differences
inIJA
andshared
positive
affect(m
oderateor
largeeffectsizesat
6and12
mo)
NSbetween-group
differences
inexpressive
language
ornonverbalcognition
(moderateeffect
sizesat6and12mo)
Dawson
etal,17
2010
N=48
with
ASD
RCT
20h/week3
2y
(therapists)
plus
$5h/wk3
2y
(parents)
Comprehensive
ESDM
:1:1,ahome-
based,ABAand
developm
ental
approaches;plus
otheravailable
therapiesc
Significant
between-
groupdifferencesin
IQandadaptive
behavior
after2y
Delivered
bytherapists
andparents
Groupdifferences
larger
than
thosein
studiesof
comparable
developm
ental
behavioral
approaches
ofshorterduration
andfewer
hoursof
deliveryperweek
Moderate/high
Strong
Aged
18–30
mo(m
ean:
23.9,23.1mo);
male-to-female
ratio
3.5:1
Actualmean:15.2h/wk
(therapists)
plus
16.3h/wk
(parents)
Mean:9.1h/wk
individual
therapyplus
9.3h/wkgroup
Assess
andmonitor:
referralsby
community-based
providers
ESDM
group
maintainedrateof
adaptivebehavior
grow
thcompared
with
norm
ative
sampleofTD
children,andthe
comparisongroup
show
edfurtherlag
Green
etal,18
2010
N=152with
ADRCT
4h/month
36mo,
then
2h/month
36mo
Targeted
PACT:interventionto
increase
parent
sensitivityand
responsiveness;
1:1a
with
child
present;plus
treatm
entasusuald
NSbetween-group
differenceinchild
autismsymptom
severity,language
measures,or
adaptive
functioning
inschoolat13
mo
Parent
mediated
ADOS-G,usedas
primaryoutcom
e,maynotbesensitive
measure
ofchange
Moderate/high
Strong (per
parent
report)
SUPPLEMENT ARTICLE
PEDIATRICS Volume 136, Supplement 1, October 2015 S63 by guest on March 4, 2020www.aappublications.org/newsDownloaded from
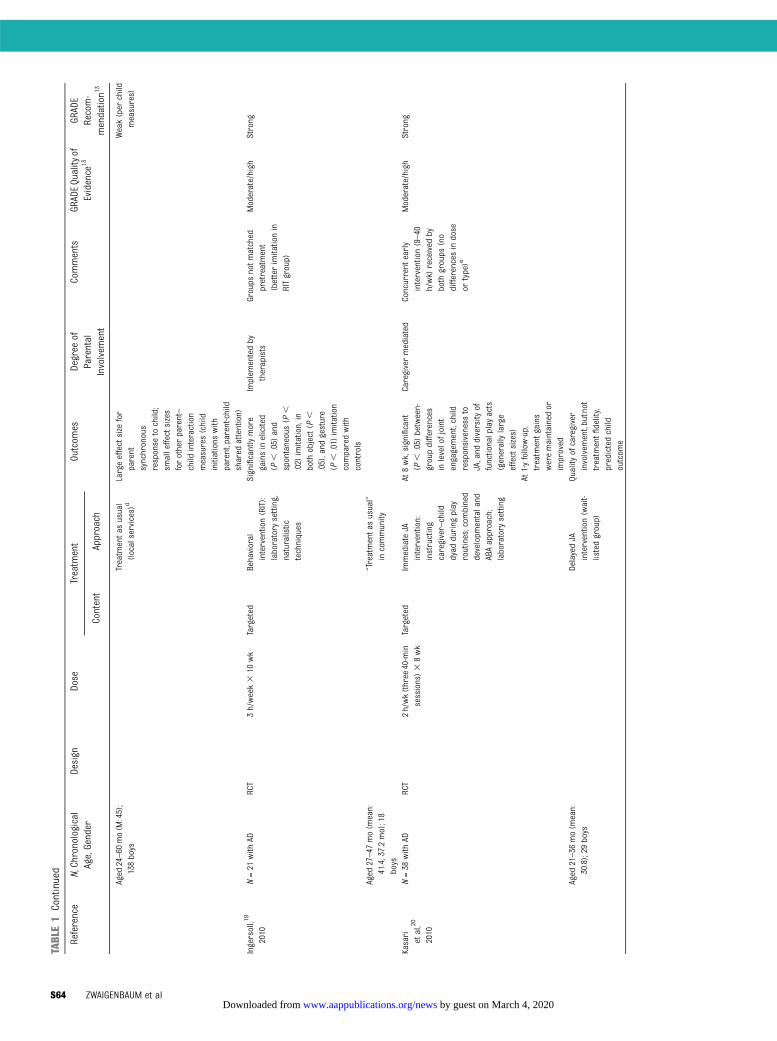
TABLE1
Continued
Reference
N,Chronological
Age,Gender
Design
Dose
Treatm
ent
Outcom
esDegree
ofParental
Involvem
ent
Comments
GRADEQuality
ofEvidence
13GR
ADE
Recom-
mendation1
3Content
Approach
Aged
24–60
mo(M
:45);
138boys
Treatm
entasusual
(localservices)d
Largeeffectsize
for
parent
synchronous
response
tochild;
smalleffectsizes
forotherparent–
child
interaction
measures(child
initiations
with
parent,parent-child
shared
attention)
Weak(per
child
measures)
Ingersoll,19
2010
N=21
with
ADRCT
3h/week3
10wk
Targeted
Behavioral
intervention(RIT):
laboratory
setting,
naturalistic
techniques
Significantlymore
gainsinelicited
(P,
.05)
and
spontaneous(P
,.02)
imitation,in
both
object(P
,.05),and
gesture
(P,
.01)
imitation
comparedwith
controls
Implem
entedby
therapists
Groups
notmatched
pretreatment
(betterimitationin
RITgroup)
Moderate/high
Strong
Aged
27–47
mo(m
ean:
41.4,37.2mo);18
boys
“Treatmentas
usual”
incommunity
Kasari
etal,20
2010
N=38
with
ADRCT
2h/wk(three
40-min
sessions)3
8wk
Targeted
ImmediateJA
intervention:
instructing
caregiver–child
dyad
during
play
routines;com
bined
developm
entaland
ABAapproach;
laboratory
setting
At8wk,significant
(P,
.05)
between-
groupdifferences
inlevelofjoint
engagement,child
responsiveness
toJA,and
diversity
offunctionalplayacts
(generallylarge
effectsizes)
Caregivermediated
Concurrent
early
intervention(9–40
h/wk)
received
byboth
groups
(no
differences
indose
ortype)e
Moderate/high
Strong
At1-yfollow-up,
treatm
entgains
weremaintainedor
improved
Aged
21–36
mo(m
ean:
30.8);29
boys
DelayedJA
intervention(wait-
listedgroup)
Quality
ofcaregiver
involvem
ent,butnot
treatm
entfidelity,
predictedchild
outcom
e
S64 ZWAIGENBAUM et al by guest on March 4, 2020www.aappublications.org/newsDownloaded from
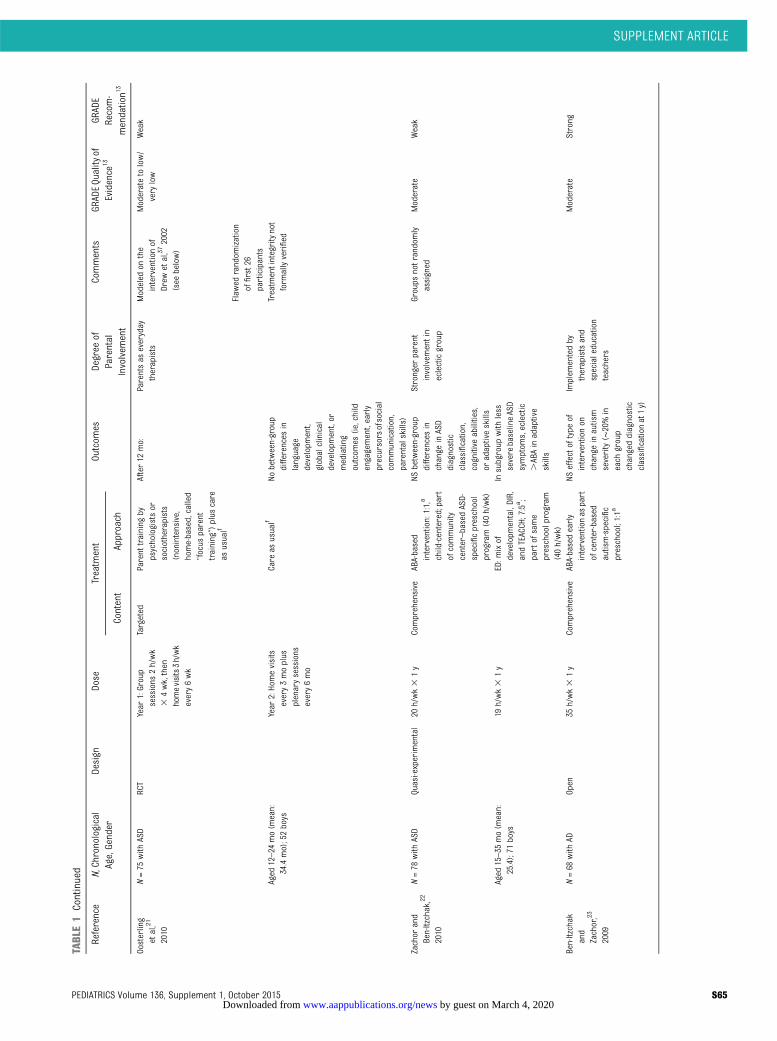
TABLE1
Continued
Reference
N,Chronological
Age,Gender
Design
Dose
Treatm
ent
Outcom
esDegree
ofParental
Involvem
ent
Comments
GRADEQuality
ofEvidence
13GR
ADE
Recom-
mendation1
3Content
Approach
Oosterling
etal,21
2010
N=75
with
ASD
RCT
Year
1:Group
sessions
2h/wk
34wk,then
homevisits3h/wk
every6wk
Targeted
Parent
training
bypsychologistsor
sociotherapists
(nonintensive,
home-based,called
“focus
parent
training”)plus
care
asusualf
After12
mo:
Parentsas
everyday
therapists
Modeled
onthe
interventionof
Drew
etal,37
2002
(see
below)
Moderatetolow/
very
low
Weak
Flaw
edrandom
ization
offirst26
participants
Aged
12–24
mo(m
ean:
34.4mo);52boys
Year
2:Homevisits
every3moplus
plenarysessions
every6mo
Care
asusualf
Nobetween-group
differences
inlanguage
developm
ent,
globalclinical
developm
ent,or
mediating
outcom
es(ie,child
engagement,early
precursorsofsocial
communication,
parentalskills)
Treatm
entintegritynot
form
allyverified
Zachor
and
Ben-Itzchak,22
2010
N=78
with
ASD
Quasi-experimental
20h/wk3
1y
Comprehensive
ABA-based
intervention:1:1,a
child-centered;part
ofcommunity
center–basedASD-
specificpreschool
program(40h/wk)
NSbetween-group
differences
inchange
inASD
diagnostic
classification,
cognitive
abilities,
oradaptiveskills
Stronger
parent
involvem
entin
eclecticgroup
Groups
notrandom
lyassigned
Moderate
Weak
Aged
15–35
mo(m
ean:
25.4);71
boys
19h/wk3
1y
ED:m
ixof
developm
ental,DIR,
andTEACCH;7:5a ;
partofsame
preschoolprogram
(40h/wk)
Insubgroup
with
less
severebaselineASD
symptom
s,eclectic
.ABAinadaptive
skills
Ben-Itzchak
and
Zachor,23
2009
N=68
with
ADOpen
35h/wk3
1y
Comprehensive
ABA-basedearly
interventionas
part
ofcenter-based
autism-specific
preschool;1:1a
NSeffectoftype
ofinterventionon
change
inautism
severity(∼
20%in
each
group
changeddiagnostic
classificationat1y)
Implem
entedby
therapistsand
specialeducation
teachers
Moderate
Strong
SUPPLEMENT ARTICLE
PEDIATRICS Volume 136, Supplement 1, October 2015 S65 by guest on March 4, 2020www.aappublications.org/newsDownloaded from
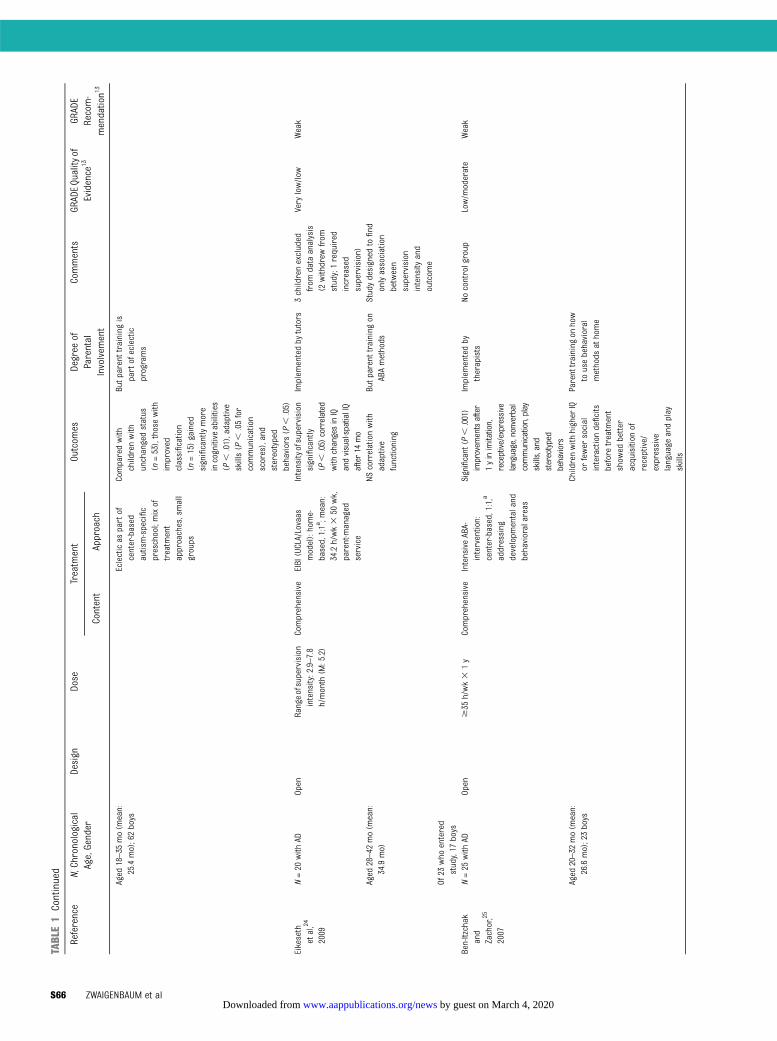
TABLE1
Continued
Reference
N,Chronological
Age,Gender
Design
Dose
Treatm
ent
Outcom
esDegree
ofParental
Involvem
ent
Comments
GRADEQuality
ofEvidence
13GR
ADE
Recom-
mendation1
3Content
Approach
Aged
18–35
mo(m
ean:
25.4mo);62boys
Eclecticas
partof
center-based
autism-specific
preschool;mixof
treatm
ent
approaches,small
groups
Comparedwith
childrenwith
unchangedstatus
(n=53),thosewith
improved
classification
(n=15)gained
significantlymore
incognitive
abilities
(P,
.01),adaptive
skills(P
,.05for
communication
scores),and
stereotyped
behaviors(P
,.05)
Butp
arenttrainingis
partofeclectic
programs
Eikeseth
etal,24
2009
N=20
with
ADOpen
Rangeofsupervision
intensity:2.9–7.8
h/month
(M:5.2)
Comprehensive
EIBI(UCLA/Lovaas
model):home-
based,1:1a;m
ean:
34.2h/wk3
50wk,
parent-managed
service
Intensity
ofsupervision
significantly
(P,
.05)correlated
with
changesinIQ
andvisual-spatialIQ
after14
mo
Implem
entedby
tutors
3childrenexcluded
from
data
analysis
(2withdrew
from
study;1required
increased
supervision)
Very
low/low
Weak
Aged
28–42
mo(m
ean:
34.9mo)
NScorrelationwith
adaptive
functioning
Butp
arenttrainingon
ABAmethods
Studydesigned
tofind
onlyassociation
between
supervision
intensity
and
outcom
eOf
23who
entered
study,17
boys
Ben-Itzchak
and
Zachor,25
2007
N=25
with
ADOpen
$35
h/wk3
1y
Comprehensive
IntensiveABA-
intervention:
center-based,1:1,a
addressing
developm
entaland
behavioralareas
Significant(P
,.001)
improvem
entsafter
1yinimitation,
receptive/expressive
language,nonverbal
communication,play
skills,and
stereotyped
behaviors
Implem
entedby
therapists
Nocontrolgroup
Low/m
oderate
Weak
Aged
20–32
mo(m
ean:
26.6mo);23boys
Childrenwith
higher
IQor
fewer
social
interactiondeficits
before
treatm
ent
show
edbetter
acquisition
ofreceptive/
expressive
language
andplay
skills
Parenttraining
onhow
tousebehavioral
methods
athome
S66 ZWAIGENBAUM et al by guest on March 4, 2020www.aappublications.org/newsDownloaded from
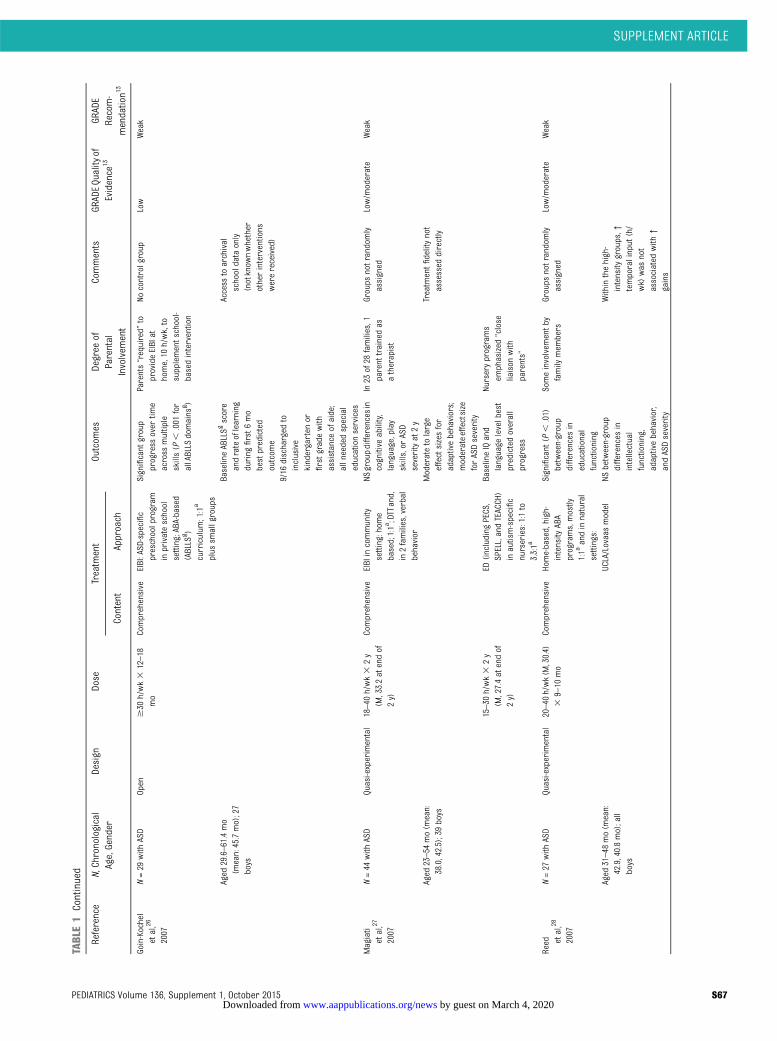
TABLE1
Continued
Reference
N,Chronological
Age,Gender
Design
Dose
Treatm
ent
Outcom
esDegree
ofParental
Involvem
ent
Comments
GRADEQuality
ofEvidence
13GR
ADE
Recom-
mendation1
3Content
Approach
Goin-Kochel
etal,26
2007
N=29
with
ASD
Open
$30
h/wk3
12–18
mo
Comprehensive
EIBI:ASD-specific
preschoolprogram
inprivateschool
setting;ABA-based
(ABLLS
g )curriculum
;1:1a
plus
smallgroups
Significant
group
progress
over
time
across
multiple
skills(P
,.001
for
allABLLS
domains
g )
Parents“required”
toprovideEIBIat
home,10
h/wk,to
supplementschool-
basedintervention
Nocontrolgroup
Low
Weak
Aged
29.6–61.4mo
(mean:45.7mo);27
boys
BaselineABLLSg
score
andrateoflearning
during
first6mo
bestpredicted
outcom
e
Access
toarchival
schooldata
only
(notknow
nwhether
otherinterventions
werereceived)
9/16
discharged
toinclusive
kindergarten
orfirstgradewith
assistance
ofaide;
allneededspecial
educationservices
Magiati
etal,27
2007
N=44
with
ASD
Quasi-experimental
18–40
h/wk3
2y
(M,33.2atendof
2y)
Comprehensive
EIBIincommunity
setting:home
based;1:1a;DTTand,
in2families,verbal
behavior
NSgroupdifferencesin
cognitive
ability,
language,play
skills,or
ASD
severityat2y
In23
of28
families,1
parent
trainedas
atherapist
Groups
notrandom
lyassigned
Low/m
oderate
Weak
Aged
23–54
mo(m
ean:
38.0,42.5);39boys
Moderatetolarge
effectsizesfor
adaptivebehaviors;
moderateeffectsize
forASDseverity
Treatm
entfidelitynot
assessed
directly
15–30
h/wk3
2y
(M,27.4atendof
2y)
ED(including
PECS,
SPELL,andTEACCH)
inautism-specific
nurseries:1:1to
3.3:1a
BaselineIQand
language
levelbest
predictedoverall
progress
Nurseryprograms
emphasized
“close
liaison
with
parents”
Reed et
al,28
2007
N=27
with
ASD
Quasi-experimental
20–40
h/wk(M
,30.4)
39–10
mo
Comprehensive
Home-based,high-
intensity
ABA
programs,mostly
1:1a
andinnatural
settings:
Significant
(P,
.01)
between-group
differences
ineducational
functioning
Someinvolvem
entby
family
mem
bers
Groups
notrandom
lyassigned
Low/m
oderate
Weak
Aged
31–48
mo(m
ean:
42.9,40.8mo);all
boys
UCLA/Lovaasmodel
NSbetween-group
differences
inintellectual
functioning,
adaptivebehavior,
andASDseverity
Withinthehigh-
intensity
groups,↑
temporalinput
(h/
wk)
was
not
associated
with
↑gains
SUPPLEMENT ARTICLE
PEDIATRICS Volume 136, Supplement 1, October 2015 S67 by guest on March 4, 2020www.aappublications.org/newsDownloaded from
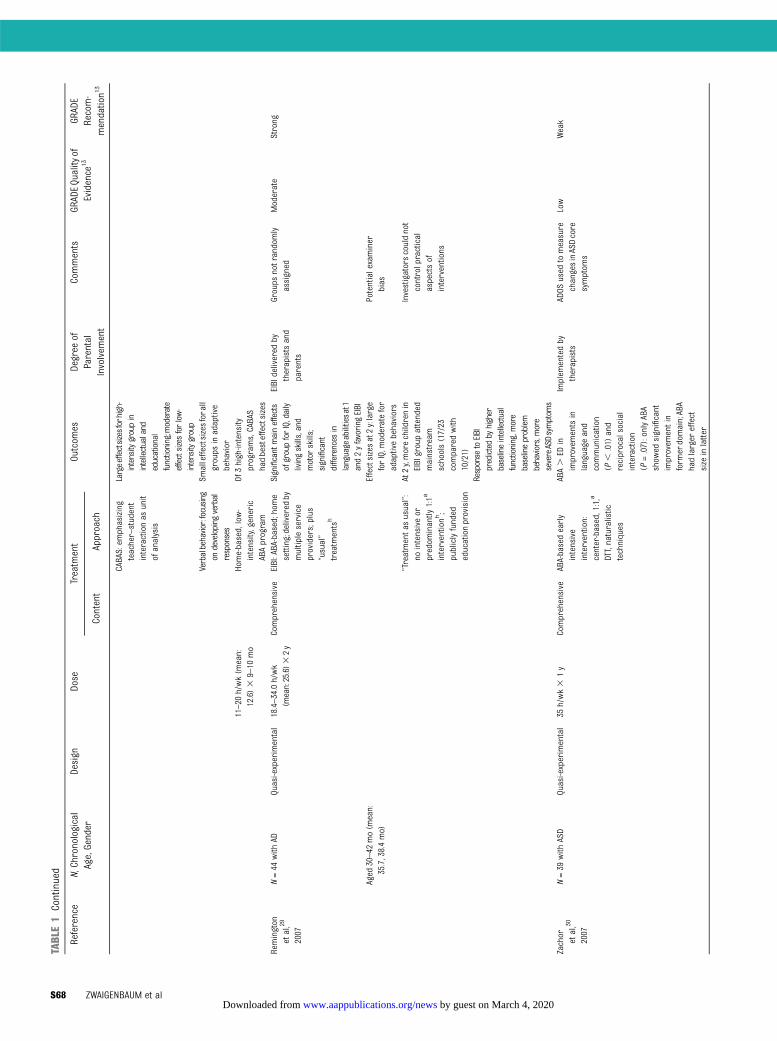
TABLE1
Continued
Reference
N,Chronological
Age,Gender
Design
Dose
Treatm
ent
Outcom
esDegree
ofParental
Involvem
ent
Comments
GRADEQuality
ofEvidence
13GR
ADE
Recom-
mendation1
3Content
Approach
CABAS:em
phasizing
teacher–student
interactionas
unit
ofanalysis
Largeeffectsizesforhigh-
intensity
groupin
intellectualand
educational
functioning;moderate
effectsizesforlow-
intensity
group
Verbalbehavior:focusing
ondeveloping
verbal
responses
Smalleffectsizesforall
groups
inadaptive
behavior
11–20
h/wk(m
ean:
12.6)3
9–10
mo
Home-based,low-
intensity,generic
ABAprogram
Of3high-intensity
programs,CABAS
hadbesteffectsizes
Remington
etal,29
2007
N=44
with
ADQuasi-experimental
18.4–34.0h/wk
(mean:25.6)3
2y
Comprehensive
EIBI:ABA-based;hom
esetting;delivered
bymultipleservice
providers;plus
“usual”
treatm
entsh
Significantmaineffects
ofgroupforIQ,daily
livingskills,and
motor
skills;
significant
differences
inlanguageabilitiesat1
and2yfavoring
EIBI
EIBIdelivered
bytherapistsand
parents
Groups
notrandom
lyassigned
Moderate
Strong
Aged
30–42
mo(m
ean:
35.7,38.4mo)
Effectsizesat2y:large
forIQ,m
oderatefor
adaptivebehaviors
Potentialexaminer
bias
“Treatmentas
usual”:
nointensiveor
predom
inantly
1:1a
interventionh;
publiclyfunded
educationprovision
At2y,morechildrenin
EIBIgroupattended
mainstream
schools(17/23
comparedwith
10/21)
Investigatorscouldnot
controlpractical
aspectsof
interventions
Response
toEIBI
predictedby
higher
baselineintellectual
functioning,m
ore
baselineproblem
behaviors,m
ore
severeASDsymptom
sZachor
etal,30
2007
N=39
with
ASD
Quasi-experimental
35h/wk3
1y
Comprehensive
ABA-basedearly
intensive
intervention:
center-based,1:1,a
DTT,naturalistic
techniques
ABA.
EDin
improvem
entsin
language
and
communication
(P,
.01)
and
reciprocalsocial
interaction
(P=.07):onlyABA
show
edsignificant
improvem
entin
form
erdomain;ABA
hadlarger
effect
size
inlatter
Implem
entedby
therapists
ADOS
used
tomeasure
changesinASDcore
symptom
s
Low
Weak
S68 ZWAIGENBAUM et al by guest on March 4, 2020www.aappublications.org/newsDownloaded from
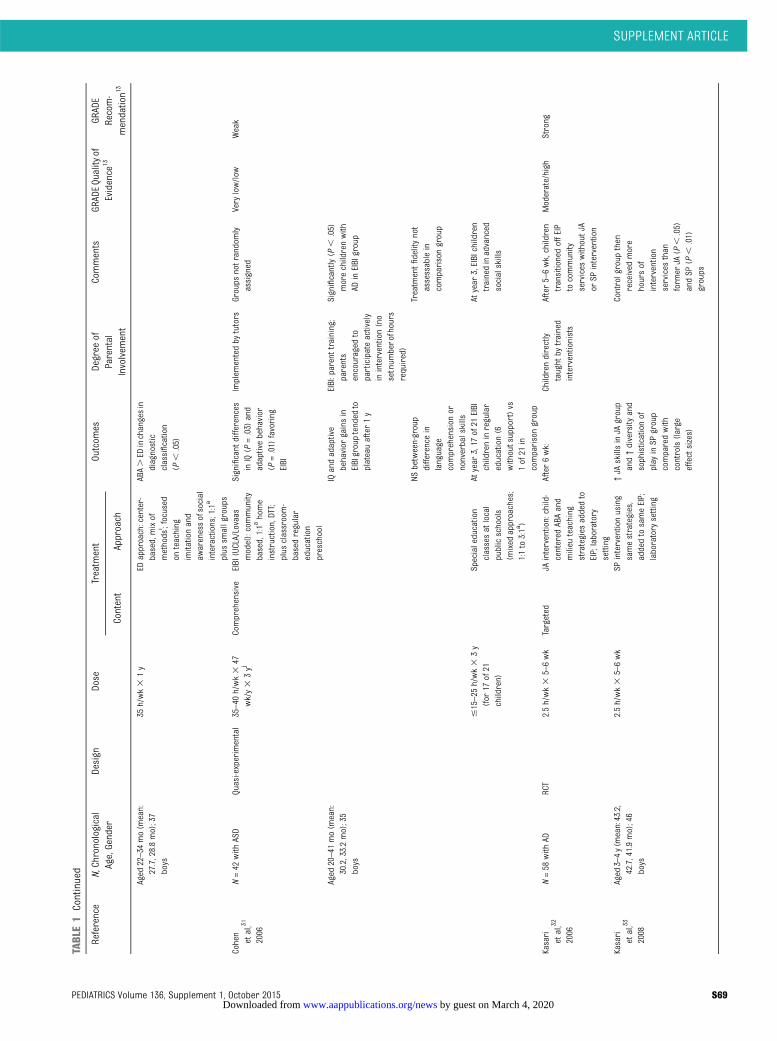
TABLE1
Continued
Reference
N,Chronological
Age,Gender
Design
Dose
Treatm
ent
Outcom
esDegree
ofParental
Involvem
ent
Comments
GRADEQuality
ofEvidence
13GR
ADE
Recom-
mendation1
3Content
Approach
Aged
22–34
mo(m
ean:
27.7,28.8mo);37
boys
35h/wk3
1y
EDapproach:center-
based,mixof
methods
i ;focused
onteaching
imitationand
awarenessofsocial
interactions;1:1a
plus
smallgroups
ABA.ED
inchangesin
diagnostic
classification
(P,
.05)
Cohen
etal,31
2006
N=42
with
ASD
Quasi-experimental
35–40
h/wk3
47wk/y3
3yj
Comprehensive
EIBI(UCLA/Lovaas
model):community
based,1:1a
home
instruction,DTT;
plus
classroom-
basedregular
education
preschool
Significant
differences
inIQ(P
=.03)
and
adaptivebehavior
(P=.01)
favoring
EIBI
Implem
entedby
tutors
Groups
notrandom
lyassigned
Very
low/low
Weak
Aged
20–41
mo(m
ean:
30.2,33.2mo);35
boys
IQandadaptive
behavior
gainsin
EIBIgrouptended
toplateauafter1y
EIBI:parenttraining;
parents
encouraged
toparticipateactively
inintervention(no
setnum
berofhours
required)
Significantly(P
,.05)
morechildrenwith
ADinEIBIgroup
NSbetween-group
differencein
language
comprehension
ornonverbalskills
Treatm
entfidelitynot
assessablein
comparisongroup
#15–25
h/wk3
3y
(for
17of21
children)
Specialeducation
classesatlocal
publicschools
(mixed
approaches;
1:1to3:1a)
Atyear
3,17
of21
EIBI
childreninregular
education(6
withoutsupport)vs
1of21
incomparisongroup
Atyear
3,EIBIchildren
trainedinadvanced
socialskills
Kasari
etal,32
2006
N=58
with
ADRCT
2.5h/wk3
5–6wk
Targeted
JAintervention:child-
centered
ABAand
milieu
teaching
strategies
addedto
EIP;laboratory
setting
After6wk:
Childrendirectly
taught
bytrained
interventionists
After5–6wk,children
transitionedoffEIP
tocommunity
services
withoutJA
orSP
intervention
Moderate/high
Strong
Kasari
etal,33
2008
Aged
3–4y(m
ean:43.2,
42.7,41.9mo);46
boys
2.5h/wk3
5–6wk
SPinterventionusing
samestrategies,
addedtosameEIP;
laboratory
setting
↑JA
skillsinJA
group
and↑diversity
and
sophisticationof
play
inSP
group
comparedwith
controls(large
effectsizes)
Controlgroup
then
received
more
hoursof
intervention
services
than
form
erJA
(P,
.05)
andSP
(P,
.01)
groups
SUPPLEMENT ARTICLE
PEDIATRICS Volume 136, Supplement 1, October 2015 S69 by guest on March 4, 2020www.aappublications.org/newsDownloaded from
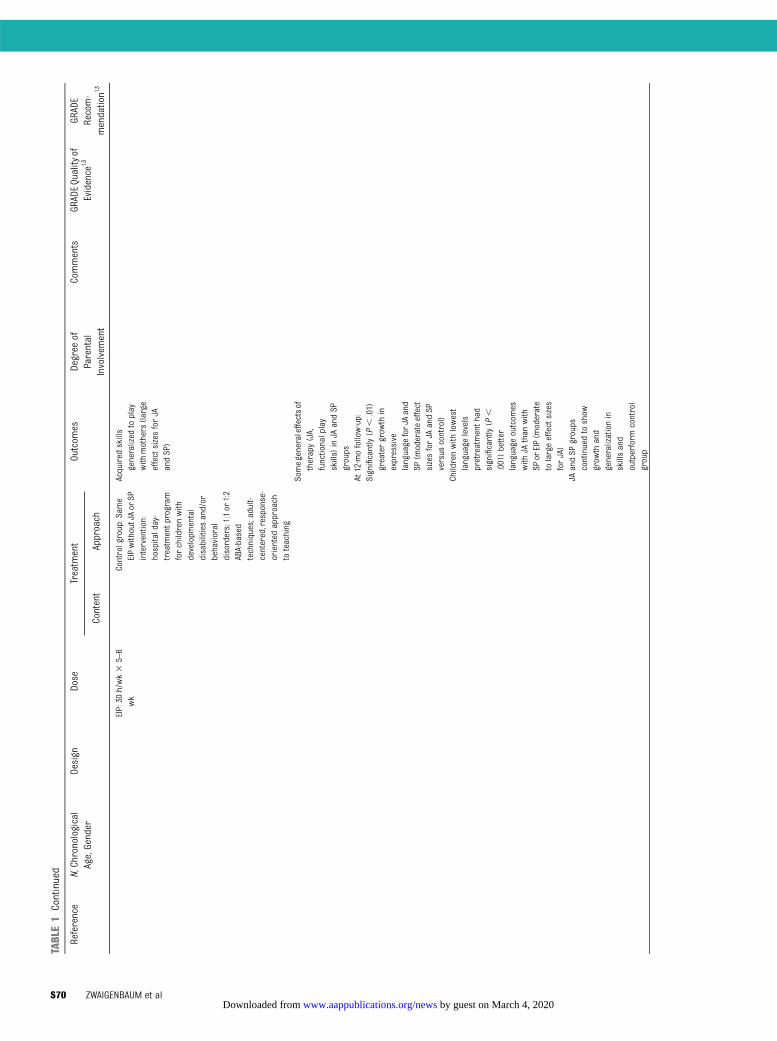
TABLE1
Continued
Reference
N,Chronological
Age,Gender
Design
Dose
Treatm
ent
Outcom
esDegree
ofParental
Involvem
ent
Comments
GRADEQuality
ofEvidence
13GR
ADE
Recom-
mendation1
3Content
Approach
EIP:30
h/wk3
5–6
wk
Controlgroup:Sam
eEIPwithoutJAor
SPintervention:
hospitalday-
treatm
entprogram
forchildrenwith
developm
ental
disabilitiesand/or
behavioral
disorders;1:1or
1:2
ABA-based
techniques;adult-
centered,response-
oriented
approach
toteaching
Acquired
skills
generalized
toplay
with
mothers(large
effectsizesforJA
andSP)
Somegeneraleffectsof
therapy(JA,
functionalplay
skills)
inJA
andSP
groups
At12-mofollow-up:
Significantly(P
,.01)
greatergrow
thin
expressive
language
forJA
and
SP(m
oderateeffect
sizesforJA
andSP
versus
control)
Childrenwith
lowest
language
levels
pretreatmenthad
significantly(P
,.001)better
language
outcom
eswith
JAthan
with
SPor
EIP(m
oderate
tolargeeffectsizes
forJA)
JAandSP
groups
continuedto
show
grow
thand
generalizationin
skillsand
outperform
control
group
S70 ZWAIGENBAUM et al by guest on March 4, 2020www.aappublications.org/newsDownloaded from
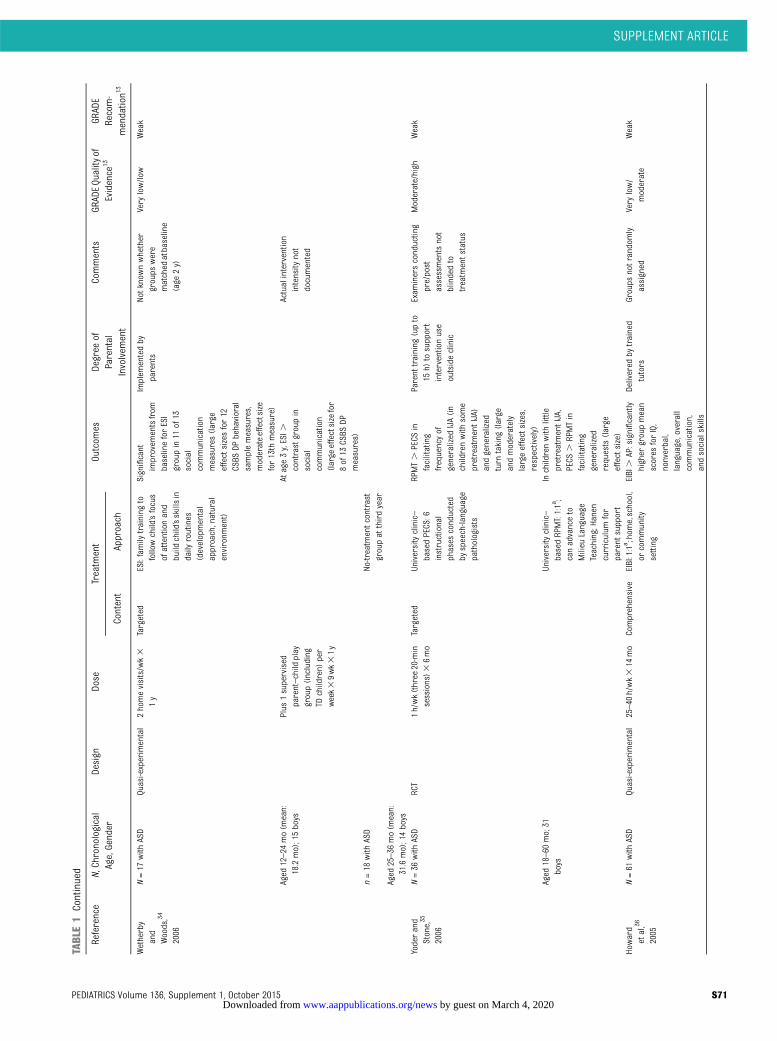
TABLE1
Continued
Reference
N,Chronological
Age,Gender
Design
Dose
Treatm
ent
Outcom
esDegree
ofParental
Involvem
ent
Comments
GRADEQuality
ofEvidence
13GR
ADE
Recom-
mendation1
3Content
Approach
Wetherby
and
Woods,34
2006
N=17
with
ASD
Quasi-experimental
2homevisits/wk3
1y
Targeted
ESI:family
training
tofollowchild’sfocus
ofattentionand
build
child’sskillsin
daily
routines
(developmental
approach,natural
environm
ent)
Significant
improvem
entsfrom
baselineforESI
groupin11
of13
social
communication
measures(large
effectsizesfor12
CSBS
DPbehavioral
samplemeasures,
moderateeffectsize
for13th
measure)
Implem
entedby
parents
Notknow
nwhether
groups
were
matched
atbaseline
(age
2y)
Very
low/low
Weak
Aged
12–24
mo(m
ean:
18.2mo);15boys
Plus
1supervised
parent–child
play
group(including
TDchildren)
per
week39wk31y
Atage3y,ESI.
contrastgroupin
social
communication
(large
effectsizefor
8of13
CSBS
DPmeasures)
Actualintervention
intensity
not
documented
n=18
with
ASD
No-treatm
entcontrast
groupat
thirdyear
Aged
25–36
mo(m
ean:
31.6mo);14boys
Yoderand
Stone,35
2006
N=36
with
ASD
RCT
1h/wk(three
20-min
sessions)3
6mo
Targeted
Universityclinic–
basedPECS:6
instructional
phases
conducted
byspeech-language
pathologists
RPMT.
PECS
infacilitating
frequencyof
generalized
IJA(in
childrenwith
some
pretreatmentIJA)
andgeneralized
turn
taking
(large
andmoderately
largeeffectsizes,
respectively)
Parent
training
(upto
15h)
tosupport
interventionuse
outsideclinic
Exam
inersconducting
pre/post
assessmentsnot
blindedto
treatm
entstatus
Moderate/high
Weak
Aged
18–60
mo;31
boys
Universityclinic–
basedRPMT:1:1a;
canadvanceto
Milieu
Language
Teaching;Hanen
curriculum
for
parent
support
Inchildrenwith
little
pretreatmentIJA,
PECS
.RPMTin
facilitating
generalized
requests(large
effectsize)
Howard
etal,36
2005
N=61
with
ASD
Quasi-experimental
25–40
h/wk3
14mo
Comprehensive
EIBI:1:1a ;home,school,
orcommunity
setting
EIBI.
AP:significantly
higher
groupmean
scores
forIQ,
nonverbal,
language,overall
communication,
andsocialskills
Delivered
bytrained
tutors
Groups
notrandom
lyassigned
Very
low/
moderate
Weak
SUPPLEMENT ARTICLE
PEDIATRICS Volume 136, Supplement 1, October 2015 S71 by guest on March 4, 2020www.aappublications.org/newsDownloaded from
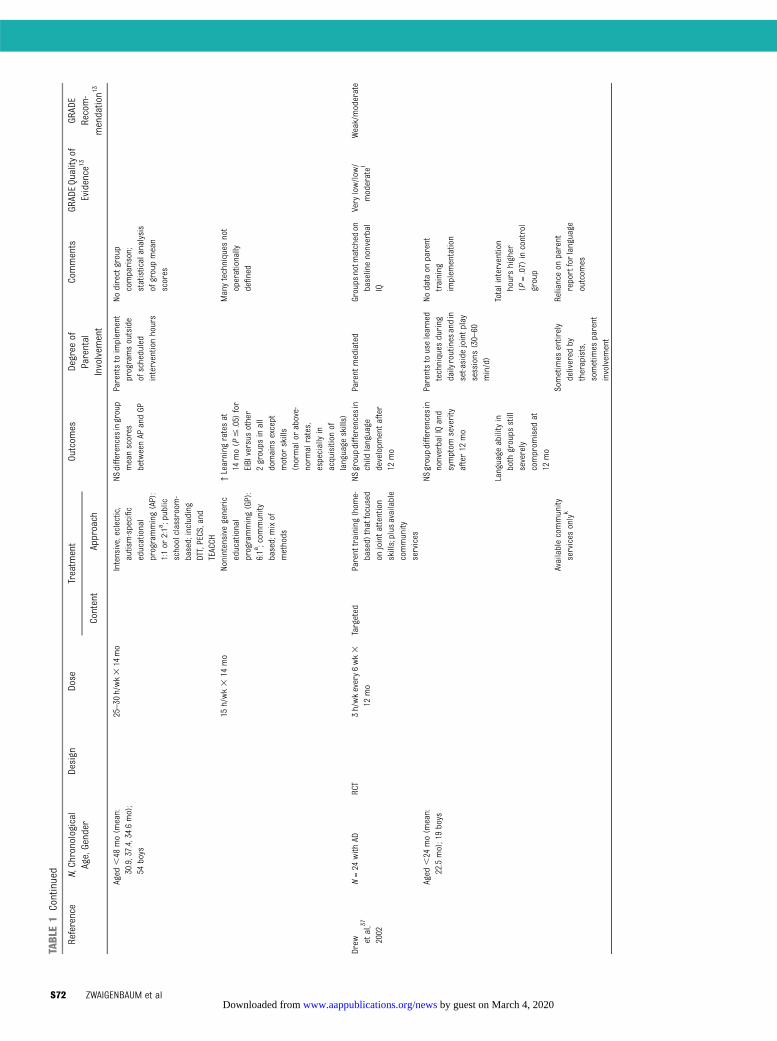
TABLE1
Continued
Reference
N,Chronological
Age,Gender
Design
Dose
Treatm
ent
Outcom
esDegree
ofParental
Involvem
ent
Comments
GRADEQuality
ofEvidence
13GR
ADE
Recom-
mendation1
3Content
Approach
Aged
,48
mo(m
ean:
30.9,37.4,34.6mo);
54boys
25–30
h/wk3
14mo
Intensive,eclectic,
autism-specific
educational
programming(AP):
1:1or
2:1a;public
schoolclassroom-
based;including
DTT,PECS,and
TEACCH
NSdifferencesingroup
meanscores
betweenAP
andGP
Parentstoimplem
ent
programsoutside
ofscheduled
interventionhours
Nodirectgroup
comparison;
statisticalanalysis
ofgroupmean
scores
15h/wk3
14mo
Nonintensive
generic
educational
programming(GP):
6:1a;com
munity
based;mixof
methods
↑Learning
ratesat
14mo(P
#.05)
for
EIBIversus
other
2groups
inall
domains
except
motor
skills
(normalor
above-
norm
alrates,
especiallyin
acquisition
oflanguage
skills)
Manytechniques
not
operationally
defined
Drew et
al,37
2002
N=24
with
ADRCT
3h/wkevery6wk3
12mo
Targeted
Parenttraining
(hom
e-based)thatfocused
onjointattention
skills;plus
available
community
services
NSgroupdifferencesin
child
language
developm
entafter
12mo
Parent
mediated
Groups
notm
atched
onbaselinenonverbal
IQ
Very
low/low
/moderatel
Weak/moderate
Aged
,24
mo(m
ean:
22.5mo);19boys
NSgroupdifferencesin
nonverbalIQand
symptom
severity
after12
mo
Parentstouselearned
techniques
during
dailyroutinesandin
set-aside
jointp
lay
sessions
(30–60
min/d)
Nodata
onparent
training
implem
entation
Language
abilityin
both
groups
still
severely
comprom
ised
at12
mo
Totalintervention
hourshigher
(P=.07)
incontrol
group
Availablecommunity
services
onlyk
Sometimes
entirely
delivered
bytherapists,
sometimes
parent
involvem
ent
Relianceon
parent
reportforlanguage
outcom
es
S72 ZWAIGENBAUM et al by guest on March 4, 2020www.aappublications.org/newsDownloaded from
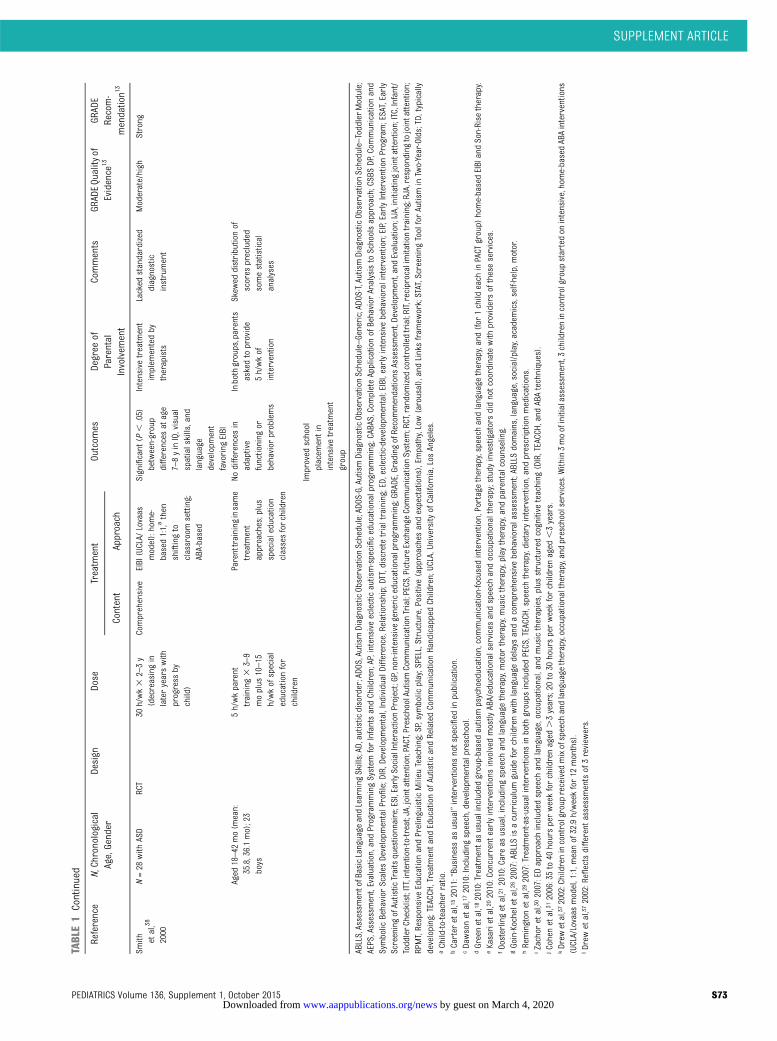
TABLE1
Continued
Reference
N,Chronological
Age,Gender
Design
Dose
Treatm
ent
Outcom
esDegree
ofParental
Involvem
ent
Comments
GRADEQuality
ofEvidence
13GR
ADE
Recom-
mendation1
3Content
Approach
Smith etal,38
2000
N=28
with
ASD
RCT
30h/wk3
2–3y
(decreasingin
lateryearswith
progress
bychild)
Comprehensive
EIBI(UCLA/
Lovaas
model):home-
based1:1,athen
shiftingto
classroomsetting;
ABA-based
Significant
(P,
.05)
between-group
differences
atage
7–8yinIQ,visual
spatialskills,and
language
developm
ent
favoring
EIBI
Intensivetreatm
ent
implem
entedby
therapists
Lacked
standardized
diagnostic
instrument
Moderate/high
Strong
Aged
18–42
mo(m
ean:
35.8,36.1mo);23
boys
5h/wkparent
training
33–9
moplus
10–15
h/wkofspecial
educationfor
children
Parenttraining
insame
treatm
ent
approaches;plus
specialeducation
classesforchildren
Nodifferences
inadaptive
functioning
orbehavior
problems
Inbothgroups,parents
askedtoprovide
5h/wkof
intervention
Skew
eddistributionof
scores
precluded
somestatistical
analyses
Improved
school
placem
entin
intensivetreatm
ent
group
ABLLS,AssessmentofBasicLanguage
andLearning
Skills;AD,autistic
disorder;ADO
S,AutismDiagnosticObservationSchedule;ADO
S-G,AutismDiagnosticObservationSchedule–Generic;ADOS-T,AutismDiagnosticObservationSchedule–ToddlerModule;
AEPS,Assessm
ent,Evaluation,andProgrammingSystem
forInfantsandChildren;AP,intensive
eclecticautism-specificeducationalprogram
ming;CABAS,CompleteApplicationofBehavior
AnalysistoSchoolsapproach;CSBSDP,Com
municationand
Symbolic
Behavior
Scales
Developm
entalProfile;DIR,Developmental,IndividualDifference,Relationship;DTT,discretetrialtraining;ED,eclectic-developmental;EIBI,earlyintensivebehavioralintervention;EIP,EarlyInterventionProgram;ESAT,Early
ScreeningofAutistic
Traitsquestionnaire;ESI,EarlySocialInteractionProject;GP,non-intensivegenericeducationalprogram
ming;GRADE,GradingofRecommendations
Assessment,Developm
ent,andEvaluation;IJA,initiatingjointattention;ITC,Infant/
ToddlerChecklist;ITT,intention-to-treat;JA,jointattention;PACT,PreschoolAutismCommunicationTrial;PECS,PictureExchange
CommunicationSystem
;RCT,randomized
controlledtrial;RIT,reciprocalimitationtraining;RJA,respondingtojointattention;
RPMT,Responsive
EducationandPrelinguistic
Milieu
Teaching;SP,symbolic
play;SPELL,Structure,Positive
(approachesandexpectations),Em
pathy,Low(arousal),andLinksfram
ework;STAT,Screening
ToolforAutisminTwo-Year-Olds;TD,typically
developing;TEACCH,Treatm
entandEducationofAutistic
andRelatedCommunicationHandicappedChildren;UCLA,University
ofCalifornia,LosAngeles.
aChild-to-teacherratio.
bCarter
etal,15
2011:“Business
asusual”interventions
notspecified
inpublication.
cDawsonetal,17
2010:Including
speech,developmentalpreschool.
dGreenetal,18
2010:Treatmentasusualincludedgroup-basedautismpsychoeducation,communication-focusedintervention,Portagetherapy,speech
andlanguage
therapy,and(for
1child
each
inPACT
group)
home-basedEIBIandSon-Rise
therapy.
eKasarietal,20
2010:Concurrentearlyinterventions
involved
mostly
ABA/educationalservicesandspeech
andoccupationaltherapy;study
investigatorsdidnotcoordinatewith
providersoftheseservices.
fOosterlingetal,21
2010:Careas
usual,includingspeech
andlanguage
therapy,motor
therapy,musictherapy,play
therapy,andparentalcounseling.
gGoin-Kocheletal,262007:ABLLS
isacurriculum
guideforchildrenwith
language
delays
andacomprehensive
behavioralassessment;ABLLSdomains,language,social/play,academ
ics,self-help,m
otor.
hRemington
etal,29
2007:Treatment-as-usualinterventions
inboth
groups
included
PECS,TEACCH,speech
therapy,dietaryintervention,andprescriptionmedications.
iZachor
etal,30
2007:EDapproach
included
speech
andlanguage,occupational,andmusictherapies,plus
structured
cognitive
teaching
(DIR,TEACCH,andABAtechniques).
jCohenetal,31
2006:35to40
hoursperweekforchildrenaged
.3years;20
to30
hoursperweekforchildrenaged
,3years.
kDrew
etal,37
2002:Childrenincontrolgroup
received
mixofspeech
andlanguage
therapy,occupationaltherapy,and
preschoolservices.Within3moofinitialassessment,3childrenincontrolgroup
startedon
intensive,home-basedABAinterventions
(UCLA/Lovaas
model,1:1,m
eanof32.9h/weekfor12
months).
lDrew
etal,37
2002:Reflectsdifferent
assessmentsof3review
ers.
SUPPLEMENT ARTICLE
PEDIATRICS Volume 136, Supplement 1, October 2015 S73 by guest on March 4, 2020www.aappublications.org/newsDownloaded from

Comparedwith early interventionmodelsevaluated for preschool-aged children(aged 3–5 years), programs for childrenaged ,3 years were more likely to usedevelopmental approaches, more in-tensively involve parents, and target so-cial communication. These studies variedin sample size and severity of diagnosis,dose (level of intensity/frequency of ser-vice delivery), duration, agent (parent,therapist, or a combination), and for-mat of delivery (parent-managed/home-based and/or center-based in a clinic orschool) of the intervention. Some inter-ventionswere comprehensive, defined asaddressing multiple core ASD deficits,while others targeted specific areas offunctioning. A word of caution is war-ranted when interpreting any 1 inter-ventional study or model. In some cases,elements of a particular programmaticapproach varied from study to study (eg,the addition of training in advanced so-cial skills in 1 early intensive behavioralintervention program).31 Furthermore,reported group differences may not re-flect the range of individual responses inany 1 study, and participants who dem-onstrated gains in some end points mayhave continued to show impairment inothers.
Six randomized controlled trials wereconsidered to produce strong recom-mendations and an assessment that thedesirable effects of an interventionclearly outweighed the undesirableeffects. Only 2 studies focused solely onchildren aged,3 years; 1was related toa comprehensive treatment approach,17
and 1 was a targeted intervention pro-gram.20 The remaining 4 studies in-cluded preschool-aged children as wellas some children aged ,3 years or fo-cused on developmental tasks of infancy.Two of these studies evaluated the samesample of children aged 3 or 4 years atthe beginning of treatment.32,33
To briefly summarize these 6 stud-ies17–20,32,33,38: both of the comprehen-sive intervention programs (Early Start
Denver Model [ESDM] and the UCLA/Lovaas model) and the 4 targetedinterventions (focusing on social com-munication or imitation skills) exhibitedsignificantly improved outcomes rela-tive to comparison groups after thera-peutic durations of 8 weeks to 2 to 3years. Several of the 6 studies reportedeffect sizes: large effect sizes after 6 and8 weeks of therapy for increases in jointattention skills,20,32 a moderate effectsize after 12 months for expressive lan-guage growth,33 and small effect sizesafter 13 months for parent–child in-teraction measures.18 It is notable thattargeted interventions generally fo-cused on outcomes related to ASD-specific characteristics, whereas thecomprehensive models included teach-ing to the core deficits but often did notmeasure changes in these core deficits(or obtained nonsignificant findings);they instead focused on gains in generalfunctioning (eg, cognitive and/or adap-tive skills). Two nonrandomized con-trolled studies were rated as producingstrong recommendations: comprehen-sive applied behavior analysis (ABA)-type interventions were associatedwith significantly improved outcomesrelative to the comparison group after2 years (compared with publicly fundededucational services)29 and with signifi-cantly improved outcomes in a subsetof participants after 1 year (comparedwith an eclectic mix of treatments).23
Although other studies included in thepresent review exhibited less thanmoderate quality of evidence and/orproduced weak recommendations, itwas agreed that the findings in thesestudies might nevertheless informtreatment options as well as future re-search. Specifically, there were studiesrated as having a strong quality of evi-dence but equivocal findings.16 For ex-ample, a recent trial evaluated the ESDMin a brief format: 1 hour per week ofparent training for 12 weeks, as op-posed to the original ESDM, which in-
volved 20 hours per week of therapistinvolvement plus additional parent-mediated intervention for 2 years.14
The study failed to detect improvementsin parental intervention skill acquisitionand child-related outcomes relative tocommunity intervention controls.
Based on expert opinion that arosefrom the review and discussion of theexisting evidence, members of theworking group agreed on several sum-mary statements intended to guideclinical practice and future research.Practice recommendations are high-lighted in statements 1 through 4;consensus regarding future researchdirections is highlighted in statements5 through 9. Statement 10 focuses onthe importance of considering the po-tential impact of medical comorbiditieson treatment and developmental out-comes.
SUMMARY STATEMENTS
Statement 1: Current bestpractices for interventions forchildren aged ,3 years withsuspected or confirmed ASDshould include a combination ofdevelopmental and behavioralapproaches and begin as early aspossible.
Based on current outcome data, theworking group supported the provisionof interventions targeted to the specificdeficits of ASD (eg, language skills, jointattention, emotional reciprocity) (Ta-ble 1) for children aged,3 years thatintegrate both behavioral and de-velopmental approaches. Behavioralinterventions are techniques based onbehavioral analysis of antecedents andconsequences of specific behaviors,and they use principles derived fromexperimental psychology research tosystematically change behavior. De-velopmental models of interventionuse developmental theory to designapproaches to target ASD deficits.57
Developmental approaches often
S74 ZWAIGENBAUM et al by guest on March 4, 2020www.aappublications.org/newsDownloaded from

underlie community services, such aspublic school programs implementedby special education specialists andspeech and language pathologists.56
However, the distinction between be-havioral and developmental strategiesmay not be very helpful, as many in-tervention programs blend features ofboth approaches. The curricula ofa behavioral intervention may be de-velopmentally informed and based ondevelopmental sequences, whereasa developmental program could usebehavioral techniques to teach a cur-riculum.
Our analysis supports the effectivenessof integrated developmental and be-havioral interventions, outside of thelaboratory setting, in improving de-velopmental quotients, adaptive func-tioning, and language skills.17,29
In line with the American Academy ofPediatrics, the working group recom-mended initiating interventionsas soonas a diagnosis of ASD is seriouslyconsidered or determined.57 Dataavailable since 2001 support the factthat early intensive education andtherapies can yield significantly im-proved developmental outcomes. Inaddition, it has been suggested thatinterventions initiated before 3 years ofage may have a greater positive impactthan those begun after the age of5 years.58–60
Statement 2: Current bestpractices for children aged ,3years with suspected or confirmedASD should have active involvementof families and/or caregivers aspart of the intervention.
There is a consensus that effective earlyintervention includes a family and/orcaregiver component.57 For many in-tervention programs, this approachwould mean parental involvement asa co-therapist, with appropriate su-pervision, training, and monitoring aspart of the intervention. Specifically,
parents should help set goals and pri-orities for their child’s treatment,identify and locate needed support forthemselves, and teach or reinforcetheir child’s new skills at home and inthe community.60
Active family involvement can havea positive impact on developmentaloutcomes. Parental or caregiver in-volvement increases the amount of in-tervention time delivered to the childinasmuch as children in this age rangeare likely to spend more time withtheir parents in their home andneighborhoods than in other settings.Furthermore, parents and caregiverscan capitalize on teachable momentsas they occur, provide learning oppor-tunities during daily routines, and fa-cilitate the generalization of learnedskills across environments.15 Familyinvolvement is also likely to be cost-effective and increases the sense ofempowerment on the part of parentsand caregivers. In the 2 comprehensivedevelopmental/behavioral programsfor which we have moderate or highevidence of effectiveness,17,29 parentswere supported in complementingeducators and therapists in the de-livery of the interventions because ofthe importance of, and challenges in-herent in, carrying over services andgeneralizing skills across multiple set-tings. Importantly, the concept of pa-rental involvement is consistent withthe recommended broader best prac-tices that support working with youngchildren in natural environments. Sev-eral parent-mediated interventionshave shown positive parent and/orchild outcomes. However, the extentto which these interventions are aseffective as therapist-mediated inter-ventions or are more effective whenadded into comprehensive child ser-vices, or with the combination oftherapist plus parent mediated inter-ventions, requires further study.18,20
Statement 3: Interventions shouldenhance developmental progressand improve functioning related toboth the core and associatedfeatures of ASD, including socialcommunication, emotional/behavioral regulation, andadaptive behaviors.
Many behavioral interventions for ASDfocus on cognitive, behavioral, andlanguage outcomes, but interventionsalso need to address social com-munication challenges central to thediagnosis. Sensory dysregulation,challenging behaviors, andmotor skillsare also common in children with ASDandshouldbe targetedby interventionswhen needed.
Despite an apparent lack of change onstandardized measures of social com-munication symptoms in 2 randomizedcontrolled trials,17,37 a growing bodyof research describes the beneficialeffects early intervention has on thedevelopment of communication andsocial functioning. (This lack of changemay reflect the utilization of symptommeasures such as the Autism Di-agnostic Observation Schedule, which,as a diagnostic tool, was designed to berelatively stable; measures specificallydesigned and validated as being sen-sitive to change are needed.) Specifi-cally, targeted interventions have beenassociated with gains in imitation,16,19
joint attention,16,20,32,34 social engage-ment,20,32,33 other social communica-tion measures,34 and functional andsymbolic play.20,32
Impaired effortful control (ie, a reducedability to regulate attention, emotions,andbehavior toachievegoals)hasbeenreported in children with ASD as earlyas at 24 months of age.61 Interventionsdealing with attention regulation inyoung children with ASD have not yetbeen reported, but in typically de-veloping children, short-term train-ing has improved attention controlmeasures associated with effortful
SUPPLEMENT ARTICLE
PEDIATRICS Volume 136, Supplement 1, October 2015 S75 by guest on March 4, 2020www.aappublications.org/newsDownloaded from

control.62 Comprehensive inter-ventions that blend developmental andbehavioral approaches have success-fully improved adaptive functioningin many studies.17,23,29,31 Thus, futureintervention studies should addressand assess various developmentaldomains as intervention and outcometargets.
Statement 4: Intervention servicesshould consider the socioculturalbeliefs of the family and familydynamics and supports, as well aseconomic capability, in terms ofboth the delivery and assessmentof factors that moderateoutcomes.
Socioeconomic status, family charac-teristics, and cultural factors maypresent barriers to service provision.Families with lower socioeconomicstatus are likely to have less access toservices. Because cultural values anddifferences can affect the goals andpriorities of the family andmay in somecases lead to misunderstandings,clinicians and other service providersshould aim to understand the values,beliefs, and accompanying practices offamilies of differing cultures and as-similate that knowledge into theirpractice parameters as it relates toautism occurring in ethnically diversepopulations. Culturally competent careextends beyondfluency in a non-Englishlanguage. As a minimum, culturallyappropriate programmaterials shouldbe developed for families. In addition,training programs should be createdthat can help service providers learnhow to promote culturally responsiveassessment and intervention ser-vices.56
Management of a child with ASD shouldfocus on the family as well as on thechild.57 Important considerations forthe clinician include the well-being ofeach person in the family, the comfortand support of each family member,
the lifestyle that has evolved aroundthe child with ASD, and the unmetneeds among family members orproblem areas that might otherwise gounaddressed.56 Service providers canbe of assistance by monitoring thephysical and mental health of thefamily as well as that of the child withASD. Finally, respect for the percep-tions, priorities, and preferences offamily members is an important“family-centered” tenet to bear in mindwhen working with children on theautism spectrum and their complexneeds.63
Statement 5: Intervention researchshould include socially andculturally diverse populations ofparticipants and evaluate familialfactors that may affectparticipation, acceptability, andoutcomes of therapeuticapproaches as well as willingnessto participate in investigativestudies.
Parents are expected to play a prom-inent role in supporting optimal de-velopment and thus interventionprogram delivery for their children,particularly at a very young age. Animportant focus of intervention re-search should therefore include fac-tors such as cultural background andother family characteristics that mayinfluence participation in treatmentprograms and interventional results.Due to attitudes concerning child-hoodrearing and independence, shameregarding developmental delays andASD, or other societal and culturalbeliefs, parents may be reluctant toenroll a child in a research study. Cu-mulatively, such decisions can diminishthe generalizability and clinical appli-cability of reported interventions. Inaddition, when there is participation,cultural differences and language bar-riers might influence and moderatetreatment effects.
In addition to any cultural issues, whenparents are expected to be the thera-peutic provider, assessment shouldfocus on more than just fidelity ofimplementation and adherence tointervention goals. The quality ofa parent’s involvement, considerationof a parent’s other responsibilities androles,20 and potential family stres-sors15 arising from fulfilling their rolein an intervention or from coping withcare for a child with ASD warrant ex-amination to determine whether mod-erators of treatment are present or areneeded. Apart from any possible re-luctance by families to participate inresearch, there is also a need forinvestigators to make a particular ef-fort to recruit as culturally diversea research sample as possible.
Statement 6: Future researchshould prioritize well-definedsampling strategies, rigorousinvestigative design, fidelity ofimplementation, and meaningfuloutcome measurements.
The methodologic rigor of interventiontrials in ASD is improving, but continuedattention to key aspects of researchdesign is needed to further develop theevidence base for toddlers.
Future directions include identifyingcharacteristics of children and familieswhowouldbenefitmost fromparticularinterventions to support a more in-dividualized approach, as well as sys-tematically varying components ofmultifaceted intervention programs toidentify critical ingredients. Thoroughcharacterization of research partic-ipants would help to define the subsetof children and families who moststrongly benefit from particular in-tervention approaches. In addition, toavoidsystematicbias fromconfoundingfactors, research participants shouldbe randomly allocated to the treatmentapproaches that are being com-pared, and each treatment (including
S76 ZWAIGENBAUM et al by guest on March 4, 2020www.aappublications.org/newsDownloaded from

community-based “as-usual” treatment)should be thoroughly described. Al-though the optimal study design tominimize bias in treatment research isa randomized controlled trial, it is ac-knowledged that contexts occur inwhich other methods may be appropri-ate. For example, to determine whetheran intervention holds promise, it is im-portant that intervention proceduresare carefully tested for feasibility andacceptability. Moreover, single casedesigns, carefully implemented andwithattention to appropriate measurement,may also be informative.64 Attention toand systematic evaluation of fidelity ofimplementation and selection of well-validated measures of key constructs(eg, joint attention, imitation, otherindicators of age-appropriate social andcommunication skills and function) thatare responsive to change are also es-sential.
Statement 7: Research is needed todetermine the specific activecomponents of effectiveinterventions, including but notlimited to the type of treatmentprovided, the agent implementingthe intervention(s) (parent,therapist, teacher, orcombination), consistency ofservice provision acrossenvironments and betweenproviders, and duration oftreatment and hours per week.
Information is lacking regarding thefeatures of an intervention that drive itseffectiveness, but progress is beingmade on identifying these activeingredients or mechanisms of change.Without appropriate study designs tocarefully examine the effect of specificintervention strategies such as treat-ment type, dose, and agent, we may beunable to determine which of the po-tentially significant elements in an in-tervention model are responsible forchange and for which subgroups. With
such information, future interventionprograms can be refined.
Intensity of intervention
The National Research Council hasrecommended a minimum intensity of5 hours a day, 5 days a week, for inter-ventions.60 However, some recent studieshave suggested the possibility of positiveoutcomes with fewer hours of directtherapist involvement for young toddlerswith ASD, particularly when parents areactively engaged in the treatment pro-cess. For example, gains in some socialcommunication skills (eg, play, joint at-tention, imitation) were demonstrated insome studies when directly targeted ininterventions of relatively low intensity(based on hours per week or length oftreatment).16,18,20 Notably, the “real-life”intensity of the intervention may beinfluenced by the degree to whichparents are implementing the strategiesin natural routines throughout the day.The effectiveness of interventions is alsolikely to be influenced by whether train-ing and ongoing supports allow parentsto correctly implement the treatmentstrategies (ie, with fidelity to the treat-ment procedures as originally designed),as has been reported in the treatment ofpreschool-aged children with ASDs.65 Inaddition, other factors can affect the ex-tent to which such interventions are ef-fective, including age, degree ofimpairment, and the extent to whichthe child receives other services.
Treatment content
A recent study in toddlers with ASD hasattempted to determine the additivevalue of joint attention, imitation, andaffect on an intervention when appliedwithin 2 developmental/behavioraltoddler classroom environments.16
The investigators evaluated impact in 1study group, and another group re-ceived the same overall comprehen-sive intervention but without theingredient of interest. Few differences
emerged in this study except forthe apparent benefit of imitation in 1group. Nonetheless, this researchparadigm provides a possible modelthrough which intervention researchmay be implemented. Similarly, otherinvestigators have evaluated the addi-tive effects of joint attention or playskills into an ABA program that did notinclude a focus on these developmentalskills. Teaching these skills increasedtheir spontaneous occurrence in gen-eralized contexts and further predictedgreater language outcomes comparedwith the children in the ABA programwithout a focus on play and joint at-tention.33,59
Incorporating teaching targets of jointattention, play, and imitation are clearlyindicated for early intervention pro-grams for ASD. However, given theheterogeneity of the disorder, it will becritical to determine how treatmentstrategies can be most effectively tai-lored to the needs of subgroups ofchildren with ASD who have particularclinical profiles.
Statement 8: Adopting a commonset of research-validated coremeasures of ASD symptoms(including but not limited tocognitive function, communication,and adaptive behavior) that can beused across multiple sites willfacilitate comparisons acrossstudies of children with ASD aged,3 years.
The interpretation of study findings isoftenhamperedwhen investigatorsusedifferent variables, or measures, toreport outcomes. A consistent set ofcore measures relevant to the specificintervention goal(s) of interest shouldbe adopted for studies of toddlers withASD as well as for older children. Out-come measures do not need to beidentical across studies, but agreementon a subset of standardized instru-ments to use (which may assess
SUPPLEMENT ARTICLE
PEDIATRICS Volume 136, Supplement 1, October 2015 S77 by guest on March 4, 2020www.aappublications.org/newsDownloaded from

changes incognitive function,coreautismsymptoms, and adaptive and languagebehavior) would facilitate future com-parisons.Someearlydevelopmentalskillscould yield “early-read” measures thatare important to later developmentaloutcomes. These early-read measuresmay include joint attention, shared affect,and imitation skills, with the expectationthat these early developmental tasksmaypredict better functioning in later cogni-tion, language, and adaptive behavior.Early-read measures may provide im-portant information on the effectivenessof short-term interventions and may alsooffer information on active ingredientsessential to include in comprehensiveintervention programs. Additional meas-ures related to the impact that havinga child with ASD has on family life andparental stress would also be important.
Statement 9: Future researchshould examine biological andbehavioral heterogeneity asmoderators of individualresponses to interventions.
In any sample population, positive re-sponsestoaninterventioncanrangefromdramatic to extremely limited. Factorsthat underlie such heterogeneity—pos-siblemoderators of individual responses—can include age at onset of intervention,patient characteristics (eg, baselinestage of development of cognitive func-tion, language and preverbal skills,adaptive behavior, sociocultural char-acteristics), and symptom severity. Asimportant, however, is the increasingappreciation that ASD is a heterogeneousdisorder—etiologically, biologically, andclinically. Given this heterogeneity, it ishighly likely that specific subsets of indi-viduals with ASD may respond to specificinterventions more effectively than toothers, perhaps based on etiology andunderlying biological factors alone. Thus,there is a critical need to begin to identifysubtypes of individuals with ASD, to un-derstand the cause of their disorder as
well as the associated neurobiologicalmechanisms at work in each case, andto be able to offer more directedinterventions depending on the bi-ological subtype when available andpresent.
A number of genetic and neurobiolog-ical subgroups are already known to beassociated with ASD. The most well-known groups are children with frag-ile X syndrome, tuberous sclerosis, andduplication 15q. Other genetic dis-orders have been identified as beingassociated with ASD features, anda growing number of candidate genesare being explored. For example,Campbell et al66 reported that childrenwith ASD and MET gene mutations weremore likely to have gastrointestinaldisorders, raising the possibility thatmedical comorbidities in children withASD could index underlying geneticheterogeneity. It is thus important forfuture research to determine both bi-ological and clinical subtypes withinthe autism spectrum that may ulti-mately affect the effectiveness oftreatment and intervention.
Todate, fewstudieshavebeendesignedor powered for analysis of heteroge-neous effects.67 Treatment modifierswere recently identified in 2 studiesbased on appropriate study designand statistical analysis. In both stud-ies, a measure developed to index thelevel of initial object exploration de-termined the extent to which a childwould benefit more from 1 language-based intervention versus another35
or the extent to which children hadbetter communication outcomes froma parent-mediated intervention.15 Ob-ject exploration can reflect a child’sflexibility in play and play level, both ofwhich may influence later cognitiveand language outcomes.59 Furtherstudies like these are needed beforewe can make informed choices andpersonalize the treatment of each in-dividual child.
Statement 10: Interventionproviders should consider medicaldisorders that may affect a child’sclinical presentation (especiallybehavior) and response to anintervention and should refer toappropriate health care providersas indicated.
It has become increasingly evident in theASD population that changes in behaviormay be associated with an underlyingmedical condition.13 For example, clinicalexperience would suggest that a childwith ASD exhibiting behavioral changesmight be experiencing pain or discomfortowing to amedical problem such as otitismedia, a dental abscess, or constipation.Frequently encountered medical factorsin ASD include: seizures, particularly inchildren who also have severe intellect-ual disability, motor deficits, or a positivefamily history of epilepsy68,69; other gas-trointestinal symptoms57,70; and sleepdisturbances affecting daytime function-ing. The full effect of medical factors onthe clinical presentation of children aged,3 years with ASD is not known, nor hasthe association between medical factorsand maladaptive behaviors such as ag-gression and self-injury been well studiedin general in ASD. Nevertheless, bestpractices would indicate that a patientwith a potential medical comorbidity bereferred to a medical specialist for ap-propriate evaluation, diagnosis, andmanagement. It is important that futureresearch address these and other po-tential medical factors, how they may bemore reliably identified (especially innonverbal or hypo-verbal ASD individu-als), and what effect treatment of theseconditions may have on behavior, de-velopmental trajectory, and learning.
ACKNOWLEDGMENTSTheconferencechairsandworkinggroupsacknowledge the preconference contribu-tions of Tony Charman, PhD, and GaryMesibov, PhD, who were unable to attendthe conference. We also acknowledge the
S78 ZWAIGENBAUM et al by guest on March 4, 2020www.aappublications.org/newsDownloaded from

efforts of Katherine F. Murray, BSN, RN,Massachusetts General Hospital for Chil-dren, incoordinating the forumandsubse-quentconferencereportprocess,andSiforNg in the conference report process.
Themeeting and consensus report weresponsored by the Autism Forum. An im-portant goal of the forum is to identifyearly indicators of ASDs that may leadto effective health care services. Autism
Forum programs are developed underthe guidance of its parent organization,the Northwest Autism Foundation. Forthis project, the Autism Research Insti-tute provided financial support.
REFERENCES
1. Zwaigenbaum L, Bryson S, Lord C, et al.Clinical assessment and management oftoddlers with suspected autism spectrumdisorder: insights from studies of high-riskinfants. Pediatrics. 2009;123(5):1383–1391
2. Zwaigenbaum L, Bauman ML, Stone WL,et al. Early identification of autism spec-trum disorder: recommendations forpractice and research. Pediatrics. 2015;136(suppl X):XXX–XXX
3. Zwaigenbaum L, Bauman ML, Fein D, et al.Early screening of autism spectrum disor-der: recommendations for practice andresearch. Pediatrics. 2015;136(suppl X):XXX–XXX
4. Guthrie W, Swineford LB, Nottke C,Wetherby AM. Early diagnosis of autismspectrum disorder: stability and change inclinical diagnosis and symptom pre-sentation. J Child Psychol Psychiatry. 2013;54(5):582–590
5. Chawarska K, Klin A, Paul R, Volkmar F.Autism spectrum disorder in the secondyear: stability and change in syndromeexpression. J Child Psychol Psychiatry.2007;48(2):128–138
6. Courchesne E, Campbell K, Solso S. Braingrowth across the life span in autism: age-specific changes in anatomical pathology.Brain Res. 2011;1380:138–145
7. Lewis JD, Evans AC, Pruett JR, et al. Net-work inefficiencies in autism spectrumdisorder at 24 months. Transl Psychiatry.2014;4:e388
8. Dawson G. Early behavioral intervention,brain plasticity, and the prevention of au-tism spectrum disorder. Dev Psychopathol.2008;20(3):775–803
9. Ozonoff S, Iosif AM, Young GS, et al. Onsetpatterns in autism: correspondence betweenhome video and parent report. J Am AcadChild Adolesc Psychiatry. 2011;50(8):796–806.e1
10. Landa RJ, Gross AL, Stuart EA, Faherty A.Developmental trajectories in children withand without autism spectrum disorders:the first 3 years. Child Dev. 2013;84(2):429–442
11. Ozonoff S, Iosif AM, Baguio F, et al. A pro-spective study of the emergence of earlybehavioral signs of autism. J Am Acad
Child Adolesc Psychiatry. 2010;49(3):256–66.e1, 2
12. Bauman ML. Medical comorbidities in au-tism: challenges to diagnosis and treat-ment. Neurotherapeutics. 2010;7(3):320–327
13. Guyatt GH, Oxman AD, Vist GE, et al; GRADEWorking Group. GRADE: an emerging con-sensus on rating quality of evidence andstrength of recommendations. BMJ. 2008;336(7650):924–926
14. Rogers SJ, Estes A, Lord C, et al. Effects ofa brief Early Start Denver model (ESDM)-based parent intervention on toddlers atrisk for autism spectrum disorders: a ran-domized controlled trial. J Am Acad ChildAdolesc Psychiatry. 2012;51(10):1052–1065
15. Carter AS, Messinger DS, Stone WL, CelimliS, Nahmias AS, Yoder P. A randomizedcontrolled trial of Hanen’s ‘More ThanWords’ in toddlers with early autismsymptoms. J Child Psychol Psychiatry. 2011;52(7):741–752
16. Landa RJ, Holman KC, O’Neill AH, Stuart EA.Intervention targeting development of so-cially synchronous engagement in toddlerswith autism spectrum disorder: a random-ized controlled trial. J Child Psychol Psy-chiatry. 2011;52(1):13–21
17. Dawson G, Rogers S, Munson J, et al. Ran-domized, controlled trial of an intervention fortoddlers with autism: the Early Start DenverModel. Pediatrics. 2010;125(1). Available at:www.pediatrics.org/cgi/content/full/125/1/e17
18. Green J, Charman T, McConachie H, et al;PACT Consor t ium. Parent-mediatedcommunication-focused treatment in chil-dren with autism (PACT): a randomisedcontrolled trial. Lancet. 2010;375(9732):2152–2160
19. Ingersoll B. Pilot randomized controlledtrial of reciprocal imitation training forteaching elicited and spontaneous imita-tion to children with autism. J Autism DevDisord. 2010;40(9):1154–1160
20. Kasari C, Gulsrud AC, Wong C, Kwon S, LockeJ. Randomized controlled caregiver medi-ated joint engagement intervention fortoddlers with autism. J Autism Dev Disord.2010;40(9):1045–1056
21. Oosterling I, Visser J, Swinkels S, et al.Randomized controlled trial of the focusparent training for toddlers with autism: 1-year outcome. J Autism Dev Disord. 2010;40(12):1447–1458
22. Zachor DA, Ben-Itzchak E. Treatment ap-proach, autism severity and interventionoutcomes in young children. Res AutismSpectr Disord. 2010;4(3):425–432
23. Ben-Itzchak E, Zachor DA. Change in autismclassification with early intervention: pre-dictors and outcomes. Res Autism SpectrDisord. 2009;3(4):967–976
24. Eikeseth S, Hayward D, Gale C, Gitlesen JP,Eldevik S. Intensity of supervision and out-come for preschool aged children receivingearly and intensive behavioral inter-ventions: a preliminary study. Res AutismSpectr Disord. 2009;3(1):67–73
25. Ben-Itzchak E, Zachor DA. The effects of in-tellectual functioning and autism severityon outcome of early behavioral in-tervention for children with autism. ResDev Disabil. 2007;28(3):287–303
26. Goin-Kochel RP, Myers BJ, Hendricks DR,Carr SE, Wiley SB. Early responsiveness tointensive behavioral intervention predictsoutcomes among preschool children withautism. Int J Disabil Dev Educ. 2007;54(2):151–175
27. Magiati I, Charman T, Howlin P. A two-yearprospective follow-up study of community-based early intensive behavioural in-tervention and specialist nursery provisionfor children with autism spectrum dis-orders. J Child Psychol Psychiatry. 2007;48(8):803–812
28. Reed P, Osborne LA, Corness M. Brief re-port: relative effectiveness of differenthome-based behavioral approaches toearly teaching intervention. J Autism DevDisord. 2007;37(9):1815–1821
29. Remington B, Hastings RP, Kovshoff H, et al.Early intensive behavioral intervention:outcomes for children with autism andtheir parents after two years. Am J MentRetard. 2007;112(6):418–438
30. Zachor DA, Ben Itzchak E, Rabinovitch AL,Lahat E. Change in autism core symptomswith intervention. Res Autism Spectr Dis-ord. 2007;1(4):304–317
SUPPLEMENT ARTICLE
PEDIATRICS Volume 136, Supplement 1, October 2015 S79 by guest on March 4, 2020www.aappublications.org/newsDownloaded from

31. Cohen H, Amerine-Dickens M, Smith T. Earlyintensive behavioral treatment: replicationof the UCLA model in a community setting.J Dev Behav Pediatr. 2006;27(suppl 2):S145–S155
32. Kasari C, Freeman S, Paparella T. Joint at-tention and symbolic play in young childrenwith autism: a randomized controlled in-tervention study. J Child Psychol Psychiatry.2006;47(6):611–620
33. Kasari C, Paparella T, Freeman S, JahromiLB. Language outcome in autism: random-ized comparison of joint attention and playinterventions. J Consult Clin Psychol. 2008;76(1):125–137
34. Wetherby AM, Woods JJ. Early Social In-teraction Project for children with autismspectrum disorders beginning in thesecond year of life: a preliminary study.Top Early Child Spec Educ. 2006;26(2):67–82
35. Yoder P, Stone WL. Randomized comparisonof two communication interventions forpreschoolers with autism spectrum dis-orders. J Consult Clin Psychol. 2006;74(3):426–435
36. Howard JS, Sparkman CR, Cohen HG, GreenG, Stanislaw H. A comparison of intensivebehavior analytic and eclectic treatmentsfor young children with autism. Res DevDisabil. 2005;26(4):359–383
37. Drew A, Baird G, Baron-Cohen S, et al. Apilot randomised control trial of a par-ent training intervention for pre-schoolchildren with autism. Preliminary find-ings and methodological challenges. EurChild Adolesc Psychiatry. 2002;11(6):266–272
38. Smith T, Groen AD, Wynn JW. Randomizedtrial of intensive early intervention forchildren with pervasive developmentaldisorder. Am J Ment Retard. 2000;105(4):269–285
39. Green J, Wan MW, Guiraud J, et al; BASISTeam. Intervention for infants at riskof developing autism: a case series.J Autism Dev Disord. 2013;43(11):2502–2514
40. Leew SV, Stein NG, Gibbard WB. Weightedvests’ effect on social attention for toddlerswith autism spectrum disorders. Can JOccup Ther. 2010;77(2):113–124
41. Rocha ML, Schreibman L, Stahmer AC. Ef-fectiveness of training parents to teachjoint attention in children with autism.J Early Interv. 2007;29(2):154–172
42. Schertz HH, Odom SL. Promoting joint attentionin toddlers with autism: a parent-mediateddevelopmental model. J Autism Dev Dis-ord. 2007;37(8):1562–1575
43. Steiner AM, Gengoux GW, Klin A, ChawarskaK. Pivotal response treatment for infants at-risk for autism spectrum disorders: a pilotstudy. J Autism Dev Disord. 2013;43(1):91–102
44. Vismara LA, Colombi C, Rogers SJ. Can onehour per week of therapy lead to lastingchanges in young children with autism?Autism. 2009;13(1):93–115
45. Anderson DK, Oti RS, Lord C, Welch K. Pat-terns of growth in adaptive social abilitiesamong children with autism spectrumdisorders. J Abnorm Child Psychol. 2009;37(7):1019–1034
46. Hume K, Bellini S, Pratt C. The usage andperceived outcomes of early interventionand early childhood programs for youngchildren with autism spectrum disorder.Top Early Child Spec Educ. 2005;25(4):195–207
47. McGovern CW, Sigman M. Continuity andchange from early childhood to adoles-cence in autism. J Child Psychol Psychiatry.2005;46(4):401–408
48. Osborne LA, McHugh L, Saunders J, Reed P.Parenting stress reduces the effectivenessof early teaching interventions for autisticspectrum disorders. J Autism Dev Disord.2008;38(6):1092–1103
49. Paul R, Chawarska K, Cicchetti D, Volk-mar F. Language outcomes of toddlerswith autism spectrum disorders: a twoyear follow-up. Autism Res. 2008;1(2):97–107
50. Sallows GO, Graupner TD. Intensive behav-ioral treatment for children with autism:four-year outcome and predictors. Am JMent Retard. 2005;110(6):417–438
51. Eldevik S, Hastings RP, Hughes JC, Jahr E,Eikeseth S, Cross S. Meta-analysis of earlyintensive behavioral intervention for chil-dren with autism. J Clin Child AdolescPsychol. 2009;38(3):439–450
52. Virués-Ortega J. Applied behavior analyticintervention for autism in early childhood:meta-analysis, meta-regression and dose-response meta-analysis of multiple out-comes. Clin Psychol Rev. 2010;30(4):387–399
53. Warren Z, McPheeters ML, Sathe N, Foss-Feig JH, Glasser A, Veenstra-VanderweeleJ. A systematic review of early intensiveintervention for autism spectrum dis-orders. Pediatrics. 2011;127(5). Availableat: www.pediatrics.org/cgi/content/full/127/5/e1303
54. Reichow B, Wolery M. Comprehensive syn-thesis of early intensive behavioral inter-ventions for young children with autismbased on the UCLA young autism project
model. J Autism Dev Disord. 2009;39(1):23–41
55. Perry A, Cummings A, Dunn Geier J, et al.Effectiveness of intensive behavioral in-tervention in a large, community-basedprogram. Res Autism Spectr Disord. 2008;2(4):621–642
56. Rogers SJ, Vismara LA. Evidence-basedcomprehensive treatments for early au-tism. J Clin Child Adolesc Psychol. 2008;37(1):8–38
57. Myers SM, Johnson CP; American Academyof Pediatrics Council on Children With Dis-abilities. Management of children with au-tism spectrum disorders. Pediatrics. 2007;120(5):1162–1182
58. Harris SL, Handleman JS. Age and IQ atintake as predictors of placement foryoung children with autism: a four- to six-year follow-up. J Autism Dev Disord. 2000;30(2):137–142
59. Kasari C, Gulsrud A, Freeman S, Paparella T,Hellemann G. Longitudinal follow-up ofchildren with autism receiving targetedinterventions on joint attention and play.J Am Acad Child Adolesc Psychiatry. 2012;51(5):487–495
60. National Research Council. Committee onEducational Interventions for Children withAutism, Division of Behavioral and SocialSciences and Education. In: Lord C, McGeeJP, eds. Educating Children With Autism.Washington, DC: National Academy Press;2001
61. Garon N, Bryson SE, Zwaigenbaum L, et al.Temperament and its relationship to au-tistic symptoms in a high-risk infant sibcohort. J Abnorm Child Psychol. 2009;37(1):59–78
62. Posner MI, Rothbart MK. Research on at-tention networks as a model for the in-tegration of psychological science. AnnuRev Psychol. 2007;58:1–23
63. Woods JJ, Wetherby AM. Early identificationof and intervention for infants and toddlerswho are at risk for autism spectrum dis-order. Lang Speech Hear Serv Sch. 2003;34(3):180–193
64. Smith T, Scahill L, Dawson G, et al. De-signing research studies on psychosocialinterventions in autism. J Autism Dev Dis-ord. 2007;37(2):354–366
65. Coolican J, Smith IM, Bryson SE. Briefparent training in pivotal responsetreatment for preschoolers with autism.J Child Psychol Psychiatry. 2010;51(12):1321–1330
66. Campbell DB, Buie TM, Winter H, et al. Dis-tinct genetic risk based on association ofMET in families with co-occurring autism
S80 ZWAIGENBAUM et al by guest on March 4, 2020www.aappublications.org/newsDownloaded from

and gastrointestinal conditions. Pediatrics.2009;123(3):1018–1024
67. Warren Z, Veenstra-VanderWeele J, StoneW, et al. Therapies for children with au-tism spectrum disorders. Comparativeeffectiveness review no. 26. (Prepared bythe Vanderbilt Evidence-based PracticeCenter under Contract No. 290-2007-10065-I.) AHRQ publication no. 11-EHC029-
EF. Rockville, MD: Agency for HealthcareResearch and Quality; April 2011. Avail-able at: www.effectivehealthcare.ahrq.gov/reports/final.cfm. Accessed June 13,2011
68. Pavone P, Incorpora G, Fiumara A, Parano E,Trifiletti RR, Ruggieri M. Epilepsy is nota prominent feature of primary autism.Neuropediatrics. 2004;35(4):207–210
69. Tuchman RF, Rapin I, Shinnar S. Autistic anddysphasic children. II: epilepsy. Pediatrics.1991;88(6):1219–1225
70. Buie T, Campbell DB, Fuchs GJ III, et al.Evaluation, diagnosis, and treatmentof gastrointestinal disorders in indi-v iduals with ASDss : a consensusreport. Pediatrics . 2010;125(suppl 1):S1–S18
(Continued from first page)
Drs Zwaigenbaum and Bauman initiated a literature review, co-chaired the meeting that generated the consensus recommendations outlined in this article, anddrafted the initial manuscript; Drs Choueiri and Kasari co-chaired the working group that conducted the detailed literature review, generated initial recommen-dations that were discussed at the consensus meeting, and provided critical input to subsequent drafts of the manuscript; Drs Carter, Granpeesheh, Mailloux, SmithRoley, and Wagner were members of the working group that reviewed selected publications, contributed to initial recommendations that were reviewed at theconsensus meeting, and critically reviewed the manuscript; Drs Fein, Pierce, Buie, Davis, Newschaffer, Robins, Wetherby, Stone, Yirmiya, Estes, Hansen, McPartland,and Natowicz contributed to the consensus meeting that formed the basis for the manuscript and critically reviewed the manuscript; and all authors approved thefinal manuscript as submitted.
www.pediatrics.org/cgi/doi/10.1542/peds.2014-3667E
doi:10.1542/peds.2014-3667E
Accepted for publication Aug 3, 2015
Address correspondence to Lonnie Zwaigenbaum, MD, Autism Research Center, Glenrose Rehabilitation Hospital, Room E209, 10230 111 Ave, Edmonton, AB, CanadaT5G 0B7. E-mail: [email protected]
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright © 2015 by the American Academy of Pediatrics
FINANCIAL DISCLOSURE: Dr Zwaigenbaum was the site Principal Investigator of a study sponsored by SynapDx (he received operating funds but no honoraria).Drs Fein and Robins are co-owners of M-CHAT, LLC, which licenses use of the Modified Checklist for Autism in Toddlers in electronic products. Dr Stone is theauthor of the Screening Tool for Autism in Two-Year-Olds and receives a share of royalties from sales of this instrument. The authors received an honorariumas well as travel expenses from Autism Forum for contributing to the expert panels.
FUNDING: Sponsored by the Autism Forum under the guidance of the Northwest Autism Foundation and with the support of the Autism Research Institute.
POTENTIAL CONFLICT OF INTEREST: The authors have indicated they have no potential conflicts of interest to disclose.
SUPPLEMENT ARTICLE
PEDIATRICS Volume 136, Supplement 1, October 2015 S81 by guest on March 4, 2020www.aappublications.org/newsDownloaded from

DOI: 10.1542/peds.2014-3667E2015;136;S60Pediatrics
L. Hansen, James C. McPartland and Marvin R. NatowiczDiana Robins, Amy Wetherby, Wendy L. Stone, Nurit Yirmiya, Annette Estes, Robin
Deborah Fein, Karen Pierce, Timothy Buie, Patricia A. Davis, Craig Newschaffer,Carter, Doreen Granpeesheh, Zoe Mailloux, Susanne Smith Roley, Sheldon Wagner, Lonnie Zwaigenbaum, Margaret L. Bauman, Roula Choueiri, Connie Kasari, Alice
of Age: Recommendations for Practice and ResearchEarly Intervention for Children With Autism Spectrum Disorder Under 3 Years
ServicesUpdated Information &
http://pediatrics.aappublications.org/content/136/Supplement_1/S60including high resolution figures, can be found at:
References
BIBLhttp://pediatrics.aappublications.org/content/136/Supplement_1/S60#This article cites 66 articles, 8 of which you can access for free at:
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtmlin its entirety can be found online at: Information about reproducing this article in parts (figures, tables) or
Reprintshttp://www.aappublications.org/site/misc/reprints.xhtmlInformation about ordering reprints can be found online:
by guest on March 4, 2020www.aappublications.org/newsDownloaded from
DOI: 10.1542/peds.2014-3667E2015;136;S60Pediatrics
L. Hansen, James C. McPartland and Marvin R. NatowiczDiana Robins, Amy Wetherby, Wendy L. Stone, Nurit Yirmiya, Annette Estes, Robin
Deborah Fein, Karen Pierce, Timothy Buie, Patricia A. Davis, Craig Newschaffer,Carter, Doreen Granpeesheh, Zoe Mailloux, Susanne Smith Roley, Sheldon Wagner, Lonnie Zwaigenbaum, Margaret L. Bauman, Roula Choueiri, Connie Kasari, Alice
of Age: Recommendations for Practice and ResearchEarly Intervention for Children With Autism Spectrum Disorder Under 3 Years
http://pediatrics.aappublications.org/content/136/Supplement_1/S60located on the World Wide Web at:
The online version of this article, along with updated information and services, is
ISSN: 1073-0397. 60007. Copyright © 2015 by the American Academy of Pediatrics. All rights reserved. Print the American Academy of Pediatrics, 141 Northwest Point Boulevard, Elk Grove Village, Illinois,has been published continuously since 1948. Pediatrics is owned, published, and trademarked by Pediatrics is the official journal of the American Academy of Pediatrics. A monthly publication, it
by guest on March 4, 2020www.aappublications.org/newsDownloaded from
Related Documents











