Review Drug-induced hypersensitivity to artemisinin-based therapies for malaria Tamara Nordmann , 1,2 Steffen Borrmann , 3,4 and Michael Ramharter 1,2,4, * In the early 2000s, artemisinin-based combination therapy (ACT) was introduced as first-line treatment for uncomplicated Plasmodium falciparum malaria in virtually all endemic countries. However, despite the well-known excellent tolerability of ACTs, hypersensitivity to artemisinin derivatives remains a repeatedly documented adverse drug reaction of still unknown frequency. The clinical features of an artemisinin-induced hypersensitivity reaction range from mild to life- threatening severity, and a significant number of cases may pass unnoticed. In this review, we discuss the medical importance of hypersensitivity to artemisinin derivatives and we review data on the presumed frequency and its potential underlying mechanisms. Furthermore, we advocate to make alter- native non-artemisinin-based drugs available for patients who do not tolerate artemisinin derivatives and to continue investing in the development of novel non-artemisinin-based combination regimens. The era of ACT: a revolution in the treatment of malaria A third of the global population (36%) resides in malaria-endemic regions. The disease burden caused by malaria impedes economic and community development throughout these regions [1–3]. The discovery of artemisinin and its derivatives has been a major milestone for the treatment of malaria (Box 1). Today, artemisinin-based drugs constitute a central part of malaria control and first-line treatment for Plasmodium falciparum malaria in virtually all endemic countries (Figure 1), having contributed importantly to their remarkable success in reducing the global burden of malaria in addition to other control interventions, for example, insecticide-treated bednets [4–8]. Pharmacokinetic and pharmacodynamic properties of artemisinins are crucial factors for their success (Box 2). However, short treatment courses of artemisinin monotherapy are associated with recrudescence rates up to 25% [9,10]. Treatment success is signi ficantly improved by combining the artemisinin derivative with a long-lasting antimalarial drug. This concept of artemisinin-based combination therapy (ACT) was recommended by the World Health Organiza- tion (WHO) in 2006 [7] and consistently reaches more than 95% PCR-corrected efficacy in all en- demic regions outside the Greater Mekong Region [4,11,12]. To date, six different ACTs are recommended by WHO as first- or second-line treatment of uncomplicated P. falciparum malaria (see Glossary) or chloroquine-resistant Plasmodium vivax malaria: artesunate–amodiaquine, dihydroartemisinin–piperaquine, artesunate–mefloquine, artemether–lumefantrine, artesunate–sulfadoxine–pyrimethamine [13], and artesunate–pyronaridine [14]. Novel ACT regimens have recently been developed (arterolane–piperaquine [15], artemisinin– piperaquine base [16], and artemisinin–naphthoquinone [17]) and are in use in some countries. For severe P. falciparum malaria, intravenous and rectal artesunate (AS) monotherapy with sequential administration of slower-acting antimalarial drugs has proven to be highly efficacious, conferring a significant survival benefit compared with intravenous quinine therapy [18–20]. For non-falciparum Highlights Hypersensitivity reaction is one of the consistently occurring and clinically important side-effects of artemisinin- based combination therapy (ACT). Artemisinin-induced hypersensitivity re- action is presumed to be under-re- ported. Anaphylactic shock due to this type I IgE- mediated hypersensitivity reaction may require intensive care treatment. Hence, vigilant monitoring is mandatory after artemisinin administration, and ACT should be avoided in patients with previ- ous allergic reactions following artemisinin administration. Alternative antimalarial drugs are limited for patients with a known history of hypersensitivity to artemisinin, as a conse- quence of the predominance of ACTs, and thus treatment of these malaria patients is challenging. 1 Department of Tropical Medicine, Bernhard Nocht Institute for Tropical Medicine and I. Department of Medicine, University Medical Center Hamburg- Eppendorf, Hamburg, Germany 2 German Centre for Infection Research (DZIF), partner site Hamburg-Luebeck- Borstel, Hamburg, Germany 3 Institute for Tropical Medicine, Eberhard Karls University of Tübingen, Tübingen, Germany 4 Centre de Recherches Médicale de Lambaréné (CERMEL), Lambaréné, Gabon *Correspondence: [email protected] (M. Ramharter). 136 Trends in Parasitology, February 2022, Vol. 38, No. 2 https://doi.org/10.1016/j.pt.2021.08.011 © 2021 The Author(s). Published by Elsevier Ltd. This is an open access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/). Trends in Parasitology OPEN ACCESS

Drug-induced hypersensitivity to artemisinin-based therapies for malaria
Jan 12, 2023
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Drug-induced hypersensitivity to artemisinin-based therapies for malariaTamara Nordmann ,1,2 Steffen Borrmann ,3,4 and Michael Ramharter 1,2,4,*
Highlights Hypersensitivity reaction is one of the consistently occurring and clinically important side-effects of artemisinin- based combination therapy (ACT).
Artemisinin-induced hypersensitivity re- action is presumed to be under-re- ported.
Anaphylactic shockdue to this type I IgE- mediated hypersensitivity reaction may require intensive care treatment. Hence, vigilant monitoring is mandatory after artemisinin administration, and ACT should be avoided in patients with previ-
In the early 2000s, artemisinin-based combination therapy (ACT) was introduced as first-line treatment for uncomplicatedPlasmodium falciparummalaria in virtually all endemic countries. However, despite the well-known excellent tolerability of ACTs, hypersensitivity to artemisinin derivatives remains a repeatedly documented adverse drug reaction of still unknown frequency. The clinical features of an artemisinin-induced hypersensitivity reaction range from mild to life- threatening severity, and a significant number of cases may pass unnoticed. In this review, we discuss the medical importance of hypersensitivity to artemisinin derivatives and we review data on the presumed frequency and its potential underlying mechanisms. Furthermore, we advocate to make alter- native non-artemisinin-based drugs available for patients who do not tolerate artemisinin derivatives and to continue investing in the development of novel non-artemisinin-based combination regimens.
ous allergic reactions following artemisinin administration.
Alternative antimalarial drugs are limited for patients with a known history of hypersensitivity to artemisinin, as a conse- quence of the predominance of ACTs, and thus treatment of these malaria patients is challenging.
1Department of Tropical Medicine, Bernhard Nocht Institute for Tropical Medicine and I. Department of Medicine, University Medical Center Hamburg- Eppendorf, Hamburg, Germany 2German Centre for Infection Research (DZIF), partner site Hamburg-Luebeck- Borstel, Hamburg, Germany 3Institute for Tropical Medicine, Eberhard Karls University of Tübingen, Tübingen, Germany 4Centre de Recherches Médicale de Lambaréné (CERMEL), Lambaréné, Gabon
*Correspondence: [email protected] (M. Ramharter).
The era of ACT: a revolution in the treatment of malaria A third of the global population (36%) resides in malaria-endemic regions. The disease burden caused by malaria impedes economic and community development throughout these regions [1–3]. The discovery of artemisinin and its derivatives has been amajormilestone for the treatment of malaria (Box 1). Today, artemisinin-based drugs constitute a central part of malaria control and first-line treatment for Plasmodium falciparum malaria in virtually all endemic countries (Figure 1), having contributed importantly to their remarkable success in reducing the global burden of malaria in addition to other control interventions, for example, insecticide-treated bednets [4–8].
Pharmacokinetic and pharmacodynamic properties of artemisinins are crucial factors for their success (Box 2). However, short treatment courses of artemisinin monotherapy are associated with recrudescence rates up to 25% [9,10]. Treatment success is significantly improved by combining the artemisinin derivative with a long-lasting antimalarial drug. This concept of artemisinin-based combination therapy (ACT) was recommended by the World Health Organiza- tion (WHO) in 2006 [7] and consistently reaches more than 95% PCR-corrected efficacy in all en- demic regions outside the Greater Mekong Region [4,11,12].
To date, six different ACTs are recommended by WHO as first- or second-line treatment of uncomplicated P. falciparum malaria (see Glossary) or chloroquine-resistant Plasmodium vivax malaria: artesunate–amodiaquine, dihydroartemisinin–piperaquine, artesunate–mefloquine, artemether–lumefantrine, artesunate–sulfadoxine–pyrimethamine [13], and artesunate–pyronaridine [14]. Novel ACT regimens have recently been developed (arterolane–piperaquine [15], artemisinin– piperaquine base [16], and artemisinin–naphthoquinone [17]) and are in use in some countries. For severeP. falciparummalaria, intravenous and rectal artesunate (AS) monotherapy with sequential administration of slower-acting antimalarial drugs has proven to be highly efficacious, conferring a significant survival benefit compared with intravenous quinine therapy [18–20]. For non-falciparum
136 Trends in Parasitology, February 2022, Vol. 38, No. 2 https://doi.org/10.1016/j.pt.2021.08.011
© 2021 The Author(s). Published by Elsevier Ltd. This is an open access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/).
Numerous antimalarial drugs have been developed over the last century but their useful lifespan was repeatedly curtailed by the selection and spread of drug-resistance mutations. In 1957, chloroquine-resistant Plasmodium (P.) falciparum infections were first detected in Thailand. Widespread and unregulated use of chloroquine further intensified the spread of resistant P. falciparum lineages within South and Southeast Asia and later to the African continent. As a consequence of decreasing therapeutic effectiveness, malaria cases and malaria-related mortality surged [68]. Alternative antimalarial drugs, for example, mefloquine and sulfadoxine-pyrimethamine, were soon deployed [69], but in the late 1980s resistance against these novel antimalarial drugs was once again observed near the Thai–Cambodian border [70].
Despite the well-known antipyretic effects noted by Chinese physicians for centuries, the active constituent, artemisinin (qinghaosu), extracted from the plant Artemisia annua (qinghao), was discovered only in 1972 by a group of Chinese scientists lead by Tu Youyou [71]. Artemisinins were shown to be highly efficacious with an unparalleled tolerability profile [72] and were first deployed in China in 1979 followed by other malaria-endemic countries [73]. In order to prevent the de- velopment of resistance, theWorld Health Organization (WHO) advised replacement of artemisinin monotherapy with ACT in 2006 [74], in which the fast-acting artemisinin is administered together with a long-acting antimalarial drug of another therapeutic class to achieve radical cure with short 3-day regimens [75,76]. Based on these favorable features, the pro- duction of ACTs was rapidly scaled up with international financial support [77]. In 2010–2019 more than 3.1 billion treat- ment courses of ACTs were provided globally [58]. Among children aged under 5 years with malaria symptoms a median of 80% (interquartile range 31–94%) received ACTs as evaluated in a household survey in 2015–2019 [58].
Trends in Parasitology OPEN ACCESS
Glossary Anaphylaxis: an acute, potentially life- threatening, type I hypersensitivity reac- tion involving the sudden IgE-mediated release of histamine mediators with multisystemic effects. Symptoms include sudden onset of urticarial rash, angioedema, bronchospasm, dyspnea, circulatory failure, vomiting, and diar- rhea. Cinchonism: symptoms (tinnitus, high- tone deafness, visual disturbances, headache, dysphoria, vomiting, and postural hypotension) developed after the ingestion of quinoline derivatives. The term 'cinchonism' is derived from the cinchona tree out of which quinine is produced. Drug-induced: clinical presentation caused by a medical or recreational substance. Hypersensitivity reaction: over-reaction of the normally protective immune system with a potential harmful effect. Hypersensitivity can be classified into four types. Allergic and anaphylactic reactions (e.g., food allergy, insect venom allergy) are type I hypersensitivity reac- tions. Type I accounts for the activation of IgE antibodies coating immune cells which immediately release cytokines. Mass drug administration (MDA): a therapeutic dose of an effective (e.g., antimalarial drug) is provided to the entire target population, irrespective of infection status or symptoms. The aim is to eliminate the human reservoir of infec- tion. MDA is currently recommended by the WHO as a potential strategy for the elimination of P. falciparummalaria in some transmission settings. Severe malaria: malaria can be cate- gorized as uncomplicated or severe (complicated). WHO criteria define the presence of severe malaria when patients experience vital organ failure. Severe malaria can occur as a conse- quence of delayed treatment of uncom- plicated malaria. Nearly all deaths from severe malaria are caused by infections with P. falciparum. Severe malaria is defined as one or more of the following complications occurring and in the presence of P. falciparum parasitemia, if no alternative cause can be identified: impaired consciousness, acidosis, anemia, hypoglycemia, jaundice, renal failure, hyperparasitemia, pulmonary edema, significant bleeding, shock. Uncomplicated malaria: all symp- toms and signs of uncomplicated malaria are nonspecific. WHO criteria
malaria ACTs are recommended by the WHO as first-line treatments besides chloroquine. This be- comes increasingly important in areas where chloroquine-resistant P. vivax is prevalent or mixed in- fections are common.
Adverse events and tolerability of artemisinin Excellent tolerability of artemisinin and its derivatives was repeatedly observed in clinical trials, and the commonly reported adverse drug reactions (acute nausea, vomiting, anorexia, and dizziness) are usually mild. It might be worth mentioning that, in combination with mefloquine, these side- effects were observed more commonly than with artemisinin derivatives alone [21]. More serious adverse events, but much less frequently reported, are elevated liver enzymes and electrocardio- gram (ECG) abnormalities [6,22,23].
Furthermore, hematological changes (neutropenia, acute onset hemolysis) can be particularly worrying and their underlying pathological mechanisms are not yet fully understood. Delayed hemolysis after treatment with artemisinin derivatives was first described in returning travelers and subsequently also documented in patients residing in endemic regions [24]. This adverse drug reaction is consistently associated with high parasitemia and is thought to be associated with the rapid action of artemisinins on relatively young developmental stages [25]. By contrast, neutropenia seems to be a dose-dependent phenomenon that implicates a relatively narrow therapeutic range of artemisinin derivatives. An increase from the standard daily dose of 2 mg/kg body weight of artesunate to 6 mg/kg led to profound neutropenia in 20% of study participants after 7-day courses with artesunate monotherapy [26].
Hypersensitivity drug reactions (HDRs) are, in contrast to most other adverse drug reactions, me- diated by specific immunological pathways and are considered largely independent of the administered dose or pharmacological action [27]. Cases of allergic reaction following treatment with artemisinin derivatives have consistently been reported since the first clinical trials systematically evaluating artemisinins [5,19,28–35].
Hypersensitivity against artemisinin derivatives as a consistent adverse drug reaction The clinical presentation of drug-induced hypersensitivity reactions against artemisinins ranges from urticarial rashes to life-threatening anaphylactic shock. Data about severe allergic
Trends in Parasitology, February 2022, Vol. 38, No. 2 137
Trends in Parasitology OPEN ACCESS
define the presence of severe malaria when patients experience a sort of organ failure.
reactions, including breathing difficulties and hemodynamic insufficiency after artemisinin-based treatment, are scarce and mainly based on case reports from Asia (India, Thailand) [23,36,37] and Africa [Cameroon, Democratic Republic of Congo (DRC)] (see Table S1 in the supplemental information online) [38,39]. All of these severely compromised patients have initially been diag- nosed with P. falciparum and treated with artesunate or ACT according to local standard treatment recommendations. In two of these cases additional medication (paracetamol in one and vecuronium, fentanyl, and isoflurane in another) was given simultaneously. The causal relationship for artemisinin-induced hypersensitivity reaction was subsequently confirmed via skin test in four individuals, including one of the patients with concomitant medication.
Reports of milder episodes of HDR, such as pruritus, rash, or urticaria, are based on data from several larger clinical trials conducted in various Asian and African countries with study populations ranging from 40 to 8560 participants. The majority of clinical trials reporting artemisinin-induced allergic reactions investigated the efficacy and safety of orally administered ACT regimens (artesunate–amodiaquine, artemether–lumefantrine, artesunate–mefloquine, pyronaridine–artesunate), except for the AQUAMAT trial comparing intravenous artesunate with intravenous quinine therapy for severe falciparum malaria [19]. Evaluation of causal relationship of the exposure with artemisinins to allergic symptoms (e.g., skin test) can only be assumed based on the temporal association of signs and symptoms of HDRwith the intake of artemisinins. It can therefore not be fully excluded that some reactions were due to the partner drug instead of
TrendsTrends inin ParasitologyParasitology
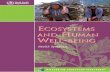
Figure 1. First-line treatment of uncomplicated Plasmodium falciparum malaria. The map shows data available to the World Health Organization by 2018 [87]. National guidelines may include more than one antimalarial regimen. Green. Artemisinin-based combination therapy (ACT) accounts for one or more of the recommended first-line antimalarial regimens. Yellow. No artemisinin-based drug among first-line antimalarial treatment regimens. Dark gray. First-line treatment of uncomplicated P. falciparum malaria not reported. Light gray. Not applicable, no endemic malaria cases.
138 Trends in Parasitology, February 2022, Vol. 38, No. 2
Box 2. The secret of artemisinin’s success is also its weakness: high efficacy and a short half-life
The mechanism of action of artemisinins is presumed to involve the production of oxygen radicals through the reduction of the artemisinin peroxide bridge in heme [78]. These radicals then cause oxidative damage in the parasite’s cell, and activated artemisinin endoperoxides interacting with iron–sulfur may lead to depolarization of mitochondrial membranes [79,80].
The alteration of membrane transport proteins, including Kelch13, adjacent to the parasite’s food vacuole, are expected to influence the parasite's susceptibility to artemisinin [81–83].
Artemisinin derivatives can be administered orally, intravenously, intramuscularly, and rectally. The bioavailability of the parent compound is low (30%) due to a high first-pass effect. The time to maximum concentration varies from minutes (intravenous artesunate) to 2–6 h (oral artemether). Through extensive metabolization, artemisinin converts quickly to dihydroartemisinin (half-life 1–2 h), which accounts for the main antimalarial activity [84,85]. Peak drug concentration (Cmax) has been identified as the main predictor associated with the rapid action of artemisinins in pharmacokinetic and pharma- codynamic (PK/PD) analyses [86]. Malaria patients benefit from the rapid antiparasitic activity of artemisinin against the blood stage of Plasmodium, including early gametocytes, with a consequential early clinical improvement and decrease in transmission. However, as a consequence of this short half-life, artemisinin monotherapy is associated with high recru- descence rates. A prolonged schedule to a 7-day treatment does not substantially decrease the rate of recrudescence [9]. Instead, artemisinin should be administered in combination with a long-acting antimalarial drug, as ACT.
Trends in Parasitology OPEN ACCESS
the artemisinin component. No severe HDR has been observed in any of these prospective clinical trials.
However, HDR is – besides rare cases of severe post-artemisinin delayed hemolysis – arguably the only other potentially fatal adverse drug reaction causatively associated with the appropriate clinical use of artemisinin derivatives, highlighting the potential importance of this clinical phenomenon. Interestingly, despite the large-scale use of artemisinins, systematic data about this clinically important phenomenon remain scarce.
Is the incidence of artemisinin-induced hypersensitivity low or simply under-reported? Despite the global use of ACT, the incidence of artemisinin-induced hypersensitivity is still largely unknown. A clear definition of artemisinin-induced hypersensitivity would be required to estimate its incidence but due to the broad clinical picture, HDRs are reported with varying frequencies.
According to Leonardi et al., six out of 17 000 malaria patients who have received artemisinin derivatives experienced allergic reactions. Consequently, the estimated risk for development of a hypersensitivity reaction was estimated to be one in 2833 (0.04%) (Table S1 in the supplemental information online) [40]. However, the authors considered only severe reactions with hemody- namic instability (hypotension, collapse, unconsciousness) or respiratory complications (dys- pnea, wheezing). Similarly, in a pilot study for the implementation of community-based case management of malaria in southern Katanga Province in the DRC, one severe reaction to artesunate–amodiaquine was observed in 1354 study participants (0.07%) [38].
The incidence of mostly mild reactions (nine participants) among 8572 treated malaria episodes was slightly higher (0.11%) in a more recent Phase IIIb/IV trial evaluating the safety of pyronaridine–artesunate (see Table S2 in the supplementary information online) [41]. Generally, signs and symptoms suggestive of HDR following ACT administration (artesunate/amodiaquine, artemether/lumefantrine, artesunate and mefloquine plus artesunate) were reported with varying frequency (0.00–20.33%) [5,19,21,28,30,31,41,42].
In a systematic review of drug-related anaphylactic reactions in India, artesunate was identified as the secondmost common antimicrobial agent (two cases) causing drug-related allergic reactions
Trends in Parasitology, February 2022, Vol. 38, No. 2 139
following β-lactam antibiotics (ten cases) [43]. In India, malaria is still endemic, and artesunate is frequently administered; however, as the denominator of administered courses of artemisinins and β-lactam antibiotics is unknown, and not all anaphylactic events necessarily published, the prevalence of hypersensitivity to artemisinins cannot be reliably quantified from this report.
Overall, the evidence for the true incidence of HDR to artemisinins remains largely unknown but seems to vary between 1:2000 for more severe reactions and about 1:1000 for milder forms of HDR. Given the fact that HDRs to artemisinins are reported consistently in large clinical trials, and given the high number of ACT treatments administered globally, HDR to artemisinins may account for a relevant number of adverse events.
The association of interindividual genetic factors that may be influencing the possibility and intensity of HDR has been demonstrated for other drugs (e.g., β-lactams) [44]. Similar associa- tions may be linked to artemisinin. It would therefore be particularly interesting to compare the frequency of artemisinin-induced hypersensitivity in various geographical regions. Interestingly, all studies and case reports about HDR after artemisinin administration (Tables S1 and S2 in the supplemental information online) were from malaria-endemic countries. Conversely, the vast majority of publications about general HDRs are from nonendemic countries where alterna- tive treatments are readily available and the overall number of malaria patients is limited. In order to obtain a more adequate estimate of the true incidence of artemisinin-induced HDR more data from population-based surveys in malaria-endemic countries are therefore needed. However, be- cause reliable population-based data from pharmacovigilance systems in many malaria-endemic countries are limited, most data about severe adverse events following artemisinin administration currently stem from clinical trials for antimalarial drug development. While anaphylaxis may be over-represented in individual case reports due to its clinical significance [23,36–40], most clinical trials may have insufficient sample size to provide accurate risk estimates, especially for extremely rare severe reactions, for example, anaphylactic shock. Milder clinical courses of HDR, including urticarial rash, pruritus, and cough, are more common but often remain unnoticed and unpub- lished. In addition, the relatedness to the administered drug may not be acknowledged by treating physicians or patients as a consequence of poor awareness of artemisinin-induced hy- persensitivity reactions, and the reporting of HDR may be challenged by well-known factors that generally hinder adverse event reporting during clinical trials, including barriers for reporting [45]. Therefore, a certain proportion of under-reporting must be assumed when estimating the true incidence of milder allergic reaction to artemisinin derivatives.
Pathophysiology of drug-induced hypersensitivity reaction to artemisinin-derived drugs HDRs can be divided into four categories by using the Gell and Coombs classification:
• Type I. Immediate reactions mediated by IgE antibodies; • Type II. Cytotoxic IgM- or IgG-mediated reactions; • Type III. Immune complex deposition reactions with activation of complement; • Type IV. Delayed T-lymphocyte-mediated reactions.
Some allergic reactions cannot be classified in any of the categories because the underlying mechanisms remain partly unknown or constitute a combination of more than one category.
The HDR to artemisinins has been described as a type I IgE-mediated hypersensitivity reaction. Characteristically, stimulated B cells produce IgE antibodies sensitizing mast cells and basophils. Re-exposure with the same allergen triggers mast cell degranulation, resulting in a release of
140 Trends in Parasitology, February 2022, Vol. 38, No. 2
histamine, leukotriene, and prostaglandin [37,46]. Hence, the symptoms of allergic reactions after oral or intravenous administration of artemisinins range from mild, self-limiting urticarial rash or angioedema to severe anaphylactic shock [23,36,37,40,43]. In published case reports the onset of symptoms was observed immediately after parental administration and up to 11 h after oral administration of the artemisinin derivative. After medical treatment and interruption of treatment with artemisinins the symptoms resolved, usually between 30 min and 2 h [23,36–40] (Table S1 in the supplemental information online).
The majority of severe artemisinin-induced hypersensitivity reactions were described for patients who received parental artesunate [23,36,37]. However, one allergic reaction following oral artesunate–amodiaquine [38], artesunate–mefloquine [40], and artemether–lumefantrine [39] treatment have been described, respectively. Despite the life-threatening potential of anaphylac- tic shock, no fatal case of an artemisinin-induced hypersensitivity reaction has been documented so far.
Proposal for the clinical management of hypersensitivity reactions Prior to administration of artemisinins, patients and health care personnel need to be informed about the risk of hypersensitivity to artemisinins. Importantly, patients need to be specifically asked for such symptoms associated to previous intake of artemisinins just as it is a standard of care prior to the administration of any β-lactam antibiotic. Clinicians should then observe the patient vigilantly for potential HDRs during and in the first hours after administration of artemisinin derivatives if logistically feasible [43].
In case of suspected HDR, an early clinical examination is particularly relevant. In the presence of a rash the localization, phenotype, and mucosal involvement may give important information about the potential nature of the reaction. Since the dermal reaction may resolve spontaneously, patients should be advised to obtain…
Highlights Hypersensitivity reaction is one of the consistently occurring and clinically important side-effects of artemisinin- based combination therapy (ACT).
Artemisinin-induced hypersensitivity re- action is presumed to be under-re- ported.
Anaphylactic shockdue to this type I IgE- mediated hypersensitivity reaction may require intensive care treatment. Hence, vigilant monitoring is mandatory after artemisinin administration, and ACT should be avoided in patients with previ-
In the early 2000s, artemisinin-based combination therapy (ACT) was introduced as first-line treatment for uncomplicatedPlasmodium falciparummalaria in virtually all endemic countries. However, despite the well-known excellent tolerability of ACTs, hypersensitivity to artemisinin derivatives remains a repeatedly documented adverse drug reaction of still unknown frequency. The clinical features of an artemisinin-induced hypersensitivity reaction range from mild to life- threatening severity, and a significant number of cases may pass unnoticed. In this review, we discuss the medical importance of hypersensitivity to artemisinin derivatives and we review data on the presumed frequency and its potential underlying mechanisms. Furthermore, we advocate to make alter- native non-artemisinin-based drugs available for patients who do not tolerate artemisinin derivatives and to continue investing in the development of novel non-artemisinin-based combination regimens.
ous allergic reactions following artemisinin administration.
Alternative antimalarial drugs are limited for patients with a known history of hypersensitivity to artemisinin, as a conse- quence of the predominance of ACTs, and thus treatment of these malaria patients is challenging.
1Department of Tropical Medicine, Bernhard Nocht Institute for Tropical Medicine and I. Department of Medicine, University Medical Center Hamburg- Eppendorf, Hamburg, Germany 2German Centre for Infection Research (DZIF), partner site Hamburg-Luebeck- Borstel, Hamburg, Germany 3Institute for Tropical Medicine, Eberhard Karls University of Tübingen, Tübingen, Germany 4Centre de Recherches Médicale de Lambaréné (CERMEL), Lambaréné, Gabon
*Correspondence: [email protected] (M. Ramharter).
The era of ACT: a revolution in the treatment of malaria A third of the global population (36%) resides in malaria-endemic regions. The disease burden caused by malaria impedes economic and community development throughout these regions [1–3]. The discovery of artemisinin and its derivatives has been amajormilestone for the treatment of malaria (Box 1). Today, artemisinin-based drugs constitute a central part of malaria control and first-line treatment for Plasmodium falciparum malaria in virtually all endemic countries (Figure 1), having contributed importantly to their remarkable success in reducing the global burden of malaria in addition to other control interventions, for example, insecticide-treated bednets [4–8].
Pharmacokinetic and pharmacodynamic properties of artemisinins are crucial factors for their success (Box 2). However, short treatment courses of artemisinin monotherapy are associated with recrudescence rates up to 25% [9,10]. Treatment success is significantly improved by combining the artemisinin derivative with a long-lasting antimalarial drug. This concept of artemisinin-based combination therapy (ACT) was recommended by the World Health Organiza- tion (WHO) in 2006 [7] and consistently reaches more than 95% PCR-corrected efficacy in all en- demic regions outside the Greater Mekong Region [4,11,12].
To date, six different ACTs are recommended by WHO as first- or second-line treatment of uncomplicated P. falciparum malaria (see Glossary) or chloroquine-resistant Plasmodium vivax malaria: artesunate–amodiaquine, dihydroartemisinin–piperaquine, artesunate–mefloquine, artemether–lumefantrine, artesunate–sulfadoxine–pyrimethamine [13], and artesunate–pyronaridine [14]. Novel ACT regimens have recently been developed (arterolane–piperaquine [15], artemisinin– piperaquine base [16], and artemisinin–naphthoquinone [17]) and are in use in some countries. For severeP. falciparummalaria, intravenous and rectal artesunate (AS) monotherapy with sequential administration of slower-acting antimalarial drugs has proven to be highly efficacious, conferring a significant survival benefit compared with intravenous quinine therapy [18–20]. For non-falciparum
136 Trends in Parasitology, February 2022, Vol. 38, No. 2 https://doi.org/10.1016/j.pt.2021.08.011
© 2021 The Author(s). Published by Elsevier Ltd. This is an open access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/).
Numerous antimalarial drugs have been developed over the last century but their useful lifespan was repeatedly curtailed by the selection and spread of drug-resistance mutations. In 1957, chloroquine-resistant Plasmodium (P.) falciparum infections were first detected in Thailand. Widespread and unregulated use of chloroquine further intensified the spread of resistant P. falciparum lineages within South and Southeast Asia and later to the African continent. As a consequence of decreasing therapeutic effectiveness, malaria cases and malaria-related mortality surged [68]. Alternative antimalarial drugs, for example, mefloquine and sulfadoxine-pyrimethamine, were soon deployed [69], but in the late 1980s resistance against these novel antimalarial drugs was once again observed near the Thai–Cambodian border [70].
Despite the well-known antipyretic effects noted by Chinese physicians for centuries, the active constituent, artemisinin (qinghaosu), extracted from the plant Artemisia annua (qinghao), was discovered only in 1972 by a group of Chinese scientists lead by Tu Youyou [71]. Artemisinins were shown to be highly efficacious with an unparalleled tolerability profile [72] and were first deployed in China in 1979 followed by other malaria-endemic countries [73]. In order to prevent the de- velopment of resistance, theWorld Health Organization (WHO) advised replacement of artemisinin monotherapy with ACT in 2006 [74], in which the fast-acting artemisinin is administered together with a long-acting antimalarial drug of another therapeutic class to achieve radical cure with short 3-day regimens [75,76]. Based on these favorable features, the pro- duction of ACTs was rapidly scaled up with international financial support [77]. In 2010–2019 more than 3.1 billion treat- ment courses of ACTs were provided globally [58]. Among children aged under 5 years with malaria symptoms a median of 80% (interquartile range 31–94%) received ACTs as evaluated in a household survey in 2015–2019 [58].
Trends in Parasitology OPEN ACCESS
Glossary Anaphylaxis: an acute, potentially life- threatening, type I hypersensitivity reac- tion involving the sudden IgE-mediated release of histamine mediators with multisystemic effects. Symptoms include sudden onset of urticarial rash, angioedema, bronchospasm, dyspnea, circulatory failure, vomiting, and diar- rhea. Cinchonism: symptoms (tinnitus, high- tone deafness, visual disturbances, headache, dysphoria, vomiting, and postural hypotension) developed after the ingestion of quinoline derivatives. The term 'cinchonism' is derived from the cinchona tree out of which quinine is produced. Drug-induced: clinical presentation caused by a medical or recreational substance. Hypersensitivity reaction: over-reaction of the normally protective immune system with a potential harmful effect. Hypersensitivity can be classified into four types. Allergic and anaphylactic reactions (e.g., food allergy, insect venom allergy) are type I hypersensitivity reac- tions. Type I accounts for the activation of IgE antibodies coating immune cells which immediately release cytokines. Mass drug administration (MDA): a therapeutic dose of an effective (e.g., antimalarial drug) is provided to the entire target population, irrespective of infection status or symptoms. The aim is to eliminate the human reservoir of infec- tion. MDA is currently recommended by the WHO as a potential strategy for the elimination of P. falciparummalaria in some transmission settings. Severe malaria: malaria can be cate- gorized as uncomplicated or severe (complicated). WHO criteria define the presence of severe malaria when patients experience vital organ failure. Severe malaria can occur as a conse- quence of delayed treatment of uncom- plicated malaria. Nearly all deaths from severe malaria are caused by infections with P. falciparum. Severe malaria is defined as one or more of the following complications occurring and in the presence of P. falciparum parasitemia, if no alternative cause can be identified: impaired consciousness, acidosis, anemia, hypoglycemia, jaundice, renal failure, hyperparasitemia, pulmonary edema, significant bleeding, shock. Uncomplicated malaria: all symp- toms and signs of uncomplicated malaria are nonspecific. WHO criteria
malaria ACTs are recommended by the WHO as first-line treatments besides chloroquine. This be- comes increasingly important in areas where chloroquine-resistant P. vivax is prevalent or mixed in- fections are common.
Adverse events and tolerability of artemisinin Excellent tolerability of artemisinin and its derivatives was repeatedly observed in clinical trials, and the commonly reported adverse drug reactions (acute nausea, vomiting, anorexia, and dizziness) are usually mild. It might be worth mentioning that, in combination with mefloquine, these side- effects were observed more commonly than with artemisinin derivatives alone [21]. More serious adverse events, but much less frequently reported, are elevated liver enzymes and electrocardio- gram (ECG) abnormalities [6,22,23].
Furthermore, hematological changes (neutropenia, acute onset hemolysis) can be particularly worrying and their underlying pathological mechanisms are not yet fully understood. Delayed hemolysis after treatment with artemisinin derivatives was first described in returning travelers and subsequently also documented in patients residing in endemic regions [24]. This adverse drug reaction is consistently associated with high parasitemia and is thought to be associated with the rapid action of artemisinins on relatively young developmental stages [25]. By contrast, neutropenia seems to be a dose-dependent phenomenon that implicates a relatively narrow therapeutic range of artemisinin derivatives. An increase from the standard daily dose of 2 mg/kg body weight of artesunate to 6 mg/kg led to profound neutropenia in 20% of study participants after 7-day courses with artesunate monotherapy [26].
Hypersensitivity drug reactions (HDRs) are, in contrast to most other adverse drug reactions, me- diated by specific immunological pathways and are considered largely independent of the administered dose or pharmacological action [27]. Cases of allergic reaction following treatment with artemisinin derivatives have consistently been reported since the first clinical trials systematically evaluating artemisinins [5,19,28–35].
Hypersensitivity against artemisinin derivatives as a consistent adverse drug reaction The clinical presentation of drug-induced hypersensitivity reactions against artemisinins ranges from urticarial rashes to life-threatening anaphylactic shock. Data about severe allergic
Trends in Parasitology, February 2022, Vol. 38, No. 2 137
Trends in Parasitology OPEN ACCESS
define the presence of severe malaria when patients experience a sort of organ failure.
reactions, including breathing difficulties and hemodynamic insufficiency after artemisinin-based treatment, are scarce and mainly based on case reports from Asia (India, Thailand) [23,36,37] and Africa [Cameroon, Democratic Republic of Congo (DRC)] (see Table S1 in the supplemental information online) [38,39]. All of these severely compromised patients have initially been diag- nosed with P. falciparum and treated with artesunate or ACT according to local standard treatment recommendations. In two of these cases additional medication (paracetamol in one and vecuronium, fentanyl, and isoflurane in another) was given simultaneously. The causal relationship for artemisinin-induced hypersensitivity reaction was subsequently confirmed via skin test in four individuals, including one of the patients with concomitant medication.
Reports of milder episodes of HDR, such as pruritus, rash, or urticaria, are based on data from several larger clinical trials conducted in various Asian and African countries with study populations ranging from 40 to 8560 participants. The majority of clinical trials reporting artemisinin-induced allergic reactions investigated the efficacy and safety of orally administered ACT regimens (artesunate–amodiaquine, artemether–lumefantrine, artesunate–mefloquine, pyronaridine–artesunate), except for the AQUAMAT trial comparing intravenous artesunate with intravenous quinine therapy for severe falciparum malaria [19]. Evaluation of causal relationship of the exposure with artemisinins to allergic symptoms (e.g., skin test) can only be assumed based on the temporal association of signs and symptoms of HDRwith the intake of artemisinins. It can therefore not be fully excluded that some reactions were due to the partner drug instead of
TrendsTrends inin ParasitologyParasitology
Figure 1. First-line treatment of uncomplicated Plasmodium falciparum malaria. The map shows data available to the World Health Organization by 2018 [87]. National guidelines may include more than one antimalarial regimen. Green. Artemisinin-based combination therapy (ACT) accounts for one or more of the recommended first-line antimalarial regimens. Yellow. No artemisinin-based drug among first-line antimalarial treatment regimens. Dark gray. First-line treatment of uncomplicated P. falciparum malaria not reported. Light gray. Not applicable, no endemic malaria cases.
138 Trends in Parasitology, February 2022, Vol. 38, No. 2
Box 2. The secret of artemisinin’s success is also its weakness: high efficacy and a short half-life
The mechanism of action of artemisinins is presumed to involve the production of oxygen radicals through the reduction of the artemisinin peroxide bridge in heme [78]. These radicals then cause oxidative damage in the parasite’s cell, and activated artemisinin endoperoxides interacting with iron–sulfur may lead to depolarization of mitochondrial membranes [79,80].
The alteration of membrane transport proteins, including Kelch13, adjacent to the parasite’s food vacuole, are expected to influence the parasite's susceptibility to artemisinin [81–83].
Artemisinin derivatives can be administered orally, intravenously, intramuscularly, and rectally. The bioavailability of the parent compound is low (30%) due to a high first-pass effect. The time to maximum concentration varies from minutes (intravenous artesunate) to 2–6 h (oral artemether). Through extensive metabolization, artemisinin converts quickly to dihydroartemisinin (half-life 1–2 h), which accounts for the main antimalarial activity [84,85]. Peak drug concentration (Cmax) has been identified as the main predictor associated with the rapid action of artemisinins in pharmacokinetic and pharma- codynamic (PK/PD) analyses [86]. Malaria patients benefit from the rapid antiparasitic activity of artemisinin against the blood stage of Plasmodium, including early gametocytes, with a consequential early clinical improvement and decrease in transmission. However, as a consequence of this short half-life, artemisinin monotherapy is associated with high recru- descence rates. A prolonged schedule to a 7-day treatment does not substantially decrease the rate of recrudescence [9]. Instead, artemisinin should be administered in combination with a long-acting antimalarial drug, as ACT.
Trends in Parasitology OPEN ACCESS
the artemisinin component. No severe HDR has been observed in any of these prospective clinical trials.
However, HDR is – besides rare cases of severe post-artemisinin delayed hemolysis – arguably the only other potentially fatal adverse drug reaction causatively associated with the appropriate clinical use of artemisinin derivatives, highlighting the potential importance of this clinical phenomenon. Interestingly, despite the large-scale use of artemisinins, systematic data about this clinically important phenomenon remain scarce.
Is the incidence of artemisinin-induced hypersensitivity low or simply under-reported? Despite the global use of ACT, the incidence of artemisinin-induced hypersensitivity is still largely unknown. A clear definition of artemisinin-induced hypersensitivity would be required to estimate its incidence but due to the broad clinical picture, HDRs are reported with varying frequencies.
According to Leonardi et al., six out of 17 000 malaria patients who have received artemisinin derivatives experienced allergic reactions. Consequently, the estimated risk for development of a hypersensitivity reaction was estimated to be one in 2833 (0.04%) (Table S1 in the supplemental information online) [40]. However, the authors considered only severe reactions with hemody- namic instability (hypotension, collapse, unconsciousness) or respiratory complications (dys- pnea, wheezing). Similarly, in a pilot study for the implementation of community-based case management of malaria in southern Katanga Province in the DRC, one severe reaction to artesunate–amodiaquine was observed in 1354 study participants (0.07%) [38].
The incidence of mostly mild reactions (nine participants) among 8572 treated malaria episodes was slightly higher (0.11%) in a more recent Phase IIIb/IV trial evaluating the safety of pyronaridine–artesunate (see Table S2 in the supplementary information online) [41]. Generally, signs and symptoms suggestive of HDR following ACT administration (artesunate/amodiaquine, artemether/lumefantrine, artesunate and mefloquine plus artesunate) were reported with varying frequency (0.00–20.33%) [5,19,21,28,30,31,41,42].
In a systematic review of drug-related anaphylactic reactions in India, artesunate was identified as the secondmost common antimicrobial agent (two cases) causing drug-related allergic reactions
Trends in Parasitology, February 2022, Vol. 38, No. 2 139
following β-lactam antibiotics (ten cases) [43]. In India, malaria is still endemic, and artesunate is frequently administered; however, as the denominator of administered courses of artemisinins and β-lactam antibiotics is unknown, and not all anaphylactic events necessarily published, the prevalence of hypersensitivity to artemisinins cannot be reliably quantified from this report.
Overall, the evidence for the true incidence of HDR to artemisinins remains largely unknown but seems to vary between 1:2000 for more severe reactions and about 1:1000 for milder forms of HDR. Given the fact that HDRs to artemisinins are reported consistently in large clinical trials, and given the high number of ACT treatments administered globally, HDR to artemisinins may account for a relevant number of adverse events.
The association of interindividual genetic factors that may be influencing the possibility and intensity of HDR has been demonstrated for other drugs (e.g., β-lactams) [44]. Similar associa- tions may be linked to artemisinin. It would therefore be particularly interesting to compare the frequency of artemisinin-induced hypersensitivity in various geographical regions. Interestingly, all studies and case reports about HDR after artemisinin administration (Tables S1 and S2 in the supplemental information online) were from malaria-endemic countries. Conversely, the vast majority of publications about general HDRs are from nonendemic countries where alterna- tive treatments are readily available and the overall number of malaria patients is limited. In order to obtain a more adequate estimate of the true incidence of artemisinin-induced HDR more data from population-based surveys in malaria-endemic countries are therefore needed. However, be- cause reliable population-based data from pharmacovigilance systems in many malaria-endemic countries are limited, most data about severe adverse events following artemisinin administration currently stem from clinical trials for antimalarial drug development. While anaphylaxis may be over-represented in individual case reports due to its clinical significance [23,36–40], most clinical trials may have insufficient sample size to provide accurate risk estimates, especially for extremely rare severe reactions, for example, anaphylactic shock. Milder clinical courses of HDR, including urticarial rash, pruritus, and cough, are more common but often remain unnoticed and unpub- lished. In addition, the relatedness to the administered drug may not be acknowledged by treating physicians or patients as a consequence of poor awareness of artemisinin-induced hy- persensitivity reactions, and the reporting of HDR may be challenged by well-known factors that generally hinder adverse event reporting during clinical trials, including barriers for reporting [45]. Therefore, a certain proportion of under-reporting must be assumed when estimating the true incidence of milder allergic reaction to artemisinin derivatives.
Pathophysiology of drug-induced hypersensitivity reaction to artemisinin-derived drugs HDRs can be divided into four categories by using the Gell and Coombs classification:
• Type I. Immediate reactions mediated by IgE antibodies; • Type II. Cytotoxic IgM- or IgG-mediated reactions; • Type III. Immune complex deposition reactions with activation of complement; • Type IV. Delayed T-lymphocyte-mediated reactions.
Some allergic reactions cannot be classified in any of the categories because the underlying mechanisms remain partly unknown or constitute a combination of more than one category.
The HDR to artemisinins has been described as a type I IgE-mediated hypersensitivity reaction. Characteristically, stimulated B cells produce IgE antibodies sensitizing mast cells and basophils. Re-exposure with the same allergen triggers mast cell degranulation, resulting in a release of
140 Trends in Parasitology, February 2022, Vol. 38, No. 2
histamine, leukotriene, and prostaglandin [37,46]. Hence, the symptoms of allergic reactions after oral or intravenous administration of artemisinins range from mild, self-limiting urticarial rash or angioedema to severe anaphylactic shock [23,36,37,40,43]. In published case reports the onset of symptoms was observed immediately after parental administration and up to 11 h after oral administration of the artemisinin derivative. After medical treatment and interruption of treatment with artemisinins the symptoms resolved, usually between 30 min and 2 h [23,36–40] (Table S1 in the supplemental information online).
The majority of severe artemisinin-induced hypersensitivity reactions were described for patients who received parental artesunate [23,36,37]. However, one allergic reaction following oral artesunate–amodiaquine [38], artesunate–mefloquine [40], and artemether–lumefantrine [39] treatment have been described, respectively. Despite the life-threatening potential of anaphylac- tic shock, no fatal case of an artemisinin-induced hypersensitivity reaction has been documented so far.
Proposal for the clinical management of hypersensitivity reactions Prior to administration of artemisinins, patients and health care personnel need to be informed about the risk of hypersensitivity to artemisinins. Importantly, patients need to be specifically asked for such symptoms associated to previous intake of artemisinins just as it is a standard of care prior to the administration of any β-lactam antibiotic. Clinicians should then observe the patient vigilantly for potential HDRs during and in the first hours after administration of artemisinin derivatives if logistically feasible [43].
In case of suspected HDR, an early clinical examination is particularly relevant. In the presence of a rash the localization, phenotype, and mucosal involvement may give important information about the potential nature of the reaction. Since the dermal reaction may resolve spontaneously, patients should be advised to obtain…
Related Documents