DELIRIUM BY MOHAMED HAMDY

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
DELIRIUMBY
MOHAMED HAMDY
DELIRIUMBY
MOHAMED HAMDY
Definition and terminologyDefinition and terminologyDSM –IVDSM –IV
1.1. Disturbance of consciousness with reduced Disturbance of consciousness with reduced ability to focus, sustain, or shift attention.ability to focus, sustain, or shift attention.
2.2. not better accounted for by a preexisting, not better accounted for by a preexisting, established, or evolving dementia.established, or evolving dementia.
3.3. Over a short period of time (usually hours to Over a short period of time (usually hours to days), fluctuating during the course of the daydays), fluctuating during the course of the day
4.4. Evidence that it is caused by a medical Evidence that it is caused by a medical condition, substance intoxication, or condition, substance intoxication, or medication side effect.medication side effect.
DSM –IVDSM –IV
1.1. Disturbance of consciousness with reduced Disturbance of consciousness with reduced ability to focus, sustain, or shift attention.ability to focus, sustain, or shift attention.
2.2. not better accounted for by a preexisting, not better accounted for by a preexisting, established, or evolving dementia.established, or evolving dementia.
3.3. Over a short period of time (usually hours to Over a short period of time (usually hours to days), fluctuating during the course of the daydays), fluctuating during the course of the day
4.4. Evidence that it is caused by a medical Evidence that it is caused by a medical condition, substance intoxication, or condition, substance intoxication, or medication side effect.medication side effect.
Additional featuresAdditional features
Psychomotor behavioral Psychomotor behavioral disturbances such as hypoactivity, disturbances such as hypoactivity, hyperactivity w increased hyperactivity w increased sympathetic activity, impairment in sympathetic activity, impairment in sleep duration and architecturesleep duration and architecture
Variable emotional disturbances, Variable emotional disturbances, such as fear, depression, euphoria, such as fear, depression, euphoria, or perplexity.or perplexity.
Psychomotor behavioral Psychomotor behavioral disturbances such as hypoactivity, disturbances such as hypoactivity, hyperactivity w increased hyperactivity w increased sympathetic activity, impairment in sympathetic activity, impairment in sleep duration and architecturesleep duration and architecture
Variable emotional disturbances, Variable emotional disturbances, such as fear, depression, euphoria, such as fear, depression, euphoria, or perplexity.or perplexity.
Epidemiology of deliriumEpidemiology of delirium
30% - older medical patients30% - older medical patients
10-50% - older surgical patients10-50% - older surgical patients
70% - ICU70% - ICU
42% - Hospice units42% - Hospice units
16% - postacute care settings16% - postacute care settings
Delirium patients experience prolonged Delirium patients experience prolonged hospitalizations, functional decline, high hospitalizations, functional decline, high risk for institutionalization.risk for institutionalization.
30% - older medical patients30% - older medical patients
10-50% - older surgical patients10-50% - older surgical patients
70% - ICU70% - ICU
42% - Hospice units42% - Hospice units
16% - postacute care settings16% - postacute care settings
Delirium patients experience prolonged Delirium patients experience prolonged hospitalizations, functional decline, high hospitalizations, functional decline, high risk for institutionalization.risk for institutionalization.
DELIRIUM vs DEMENTIADELIRIUM vs DEMENTIA Delirium and dementia often occur together in Delirium and dementia often occur together in
older hospitalized patients; the distinguishing signs older hospitalized patients; the distinguishing signs of delirium are:of delirium are:
Acute onsetAcute onset
Cognitive fluctuations over hours or daysCognitive fluctuations over hours or days
Impaired consciousness and attentionImpaired consciousness and attention
Altered sleep cyclesAltered sleep cycles
Delirium and dementia often occur together in Delirium and dementia often occur together in older hospitalized patients; the distinguishing signs older hospitalized patients; the distinguishing signs of delirium are:of delirium are:
Acute onsetAcute onset
Cognitive fluctuations over hours or daysCognitive fluctuations over hours or days
Impaired consciousness and attentionImpaired consciousness and attention
Altered sleep cyclesAltered sleep cycles
DELIRIUM TAKES VARIOUS FORMSDELIRIUM TAKES VARIOUS FORMS
Hyperactive or agitated delirium Hyperactive or agitated delirium 25% of all cases25% of all cases
Hypoactive delirium Hypoactive delirium less recognized or appropriately treatedless recognized or appropriately treated
Mixed Mixed
Additional features include emotional Additional features include emotional symptoms, psychotic symptoms, “sundowning”symptoms, psychotic symptoms, “sundowning”
Hyperactive or agitated delirium Hyperactive or agitated delirium 25% of all cases25% of all cases
Hypoactive delirium Hypoactive delirium less recognized or appropriately treatedless recognized or appropriately treated
Mixed Mixed
Additional features include emotional Additional features include emotional symptoms, psychotic symptoms, “sundowning”symptoms, psychotic symptoms, “sundowning”
NEUROPATHOPHYSIOLOGYNEUROPATHOPHYSIOLOGY
Cholinergic deficiencyCholinergic deficiency
Delirium is associated with Delirium is associated with serum anticholinergic activity serum anticholinergic activity
Physostigmine and cholinesterase inhibitors are beneficialPhysostigmine and cholinesterase inhibitors are beneficial
Serotonin excess or deficiencySerotonin excess or deficiency
Dopamine excess (regulates release of acetylcholine)Dopamine excess (regulates release of acetylcholine)
Cytokines (interleukin-1,and 2, tumor necrosis factor)Cytokines (interleukin-1,and 2, tumor necrosis factor)
As seen in patients with cancer or infectionsAs seen in patients with cancer or infections
Increases permeability of the BBBIncreases permeability of the BBB Chronic stress and hypercorticolismChronic stress and hypercorticolism
Other neurotransmitters: GABA, glutamate, melatoninOther neurotransmitters: GABA, glutamate, melatonin
Cholinergic deficiencyCholinergic deficiency
Delirium is associated with Delirium is associated with serum anticholinergic activity serum anticholinergic activity
Physostigmine and cholinesterase inhibitors are beneficialPhysostigmine and cholinesterase inhibitors are beneficial
Serotonin excess or deficiencySerotonin excess or deficiency
Dopamine excess (regulates release of acetylcholine)Dopamine excess (regulates release of acetylcholine)
Cytokines (interleukin-1,and 2, tumor necrosis factor)Cytokines (interleukin-1,and 2, tumor necrosis factor)
As seen in patients with cancer or infectionsAs seen in patients with cancer or infections
Increases permeability of the BBBIncreases permeability of the BBB Chronic stress and hypercorticolismChronic stress and hypercorticolism
Other neurotransmitters: GABA, glutamate, melatoninOther neurotransmitters: GABA, glutamate, melatonin
Pathogenesis of deliriumPathogenesis of delirium
Poorly understoodPoorly understood
Difficult to study severely ill patients Difficult to study severely ill patients
Hard to separate from that of Hard to separate from that of underlying illness and drug underlying illness and drug treatmenttreatment
Poorly understoodPoorly understood
Difficult to study severely ill patients Difficult to study severely ill patients
Hard to separate from that of Hard to separate from that of underlying illness and drug underlying illness and drug treatmenttreatment
Pathogenesis: 1.Neurobiology of attention
Pathogenesis: 1.Neurobiology of attentionArousal and attention are governed by:Arousal and attention are governed by:
the ascending reticular activating the ascending reticular activating systemsystem
The “nondominant” parietal and The “nondominant” parietal and frontal lobesfrontal lobes
Intact higher order integrated cortical Intact higher order integrated cortical functionfunction
Arousal and attention are governed by:Arousal and attention are governed by:
the ascending reticular activating the ascending reticular activating systemsystem
The “nondominant” parietal and The “nondominant” parietal and frontal lobesfrontal lobes
Intact higher order integrated cortical Intact higher order integrated cortical functionfunction

Pathogenesis: 2. NeurotransmitterPathogenesis: 2. Neurotransmitter
1. Acetylcholine1. Acetylcholine
Cause delirium when given to Cause delirium when given to healthy personhealthy person
More likely to lead to confusion in More likely to lead to confusion in frailty elderlyfrailty elderly
Effects reversed with cholinesterase Effects reversed with cholinesterase inhibitors (physostigmine).inhibitors (physostigmine).
1. Acetylcholine1. Acetylcholine
Cause delirium when given to Cause delirium when given to healthy personhealthy person
More likely to lead to confusion in More likely to lead to confusion in frailty elderlyfrailty elderly
Effects reversed with cholinesterase Effects reversed with cholinesterase inhibitors (physostigmine).inhibitors (physostigmine).
Medical conditions precipitating Medical conditions precipitating delirium, such as hypoxia, delirium, such as hypoxia, hypoglycemia, thiamine deficiency, hypoglycemia, thiamine deficiency, decrease acetylcholine synthesis in decrease acetylcholine synthesis in CNSCNS
Alzheimer’s disease, characterized Alzheimer’s disease, characterized by a loss of cholinergic neurons, by a loss of cholinergic neurons, increases risk of delirium due to increases risk of delirium due to anticholinergic medications.anticholinergic medications.
Medical conditions precipitating Medical conditions precipitating delirium, such as hypoxia, delirium, such as hypoxia, hypoglycemia, thiamine deficiency, hypoglycemia, thiamine deficiency, decrease acetylcholine synthesis in decrease acetylcholine synthesis in CNSCNS
Alzheimer’s disease, characterized Alzheimer’s disease, characterized by a loss of cholinergic neurons, by a loss of cholinergic neurons, increases risk of delirium due to increases risk of delirium due to anticholinergic medications.anticholinergic medications.
neurotransmitters neurotransmitters
2. Alterations in neuropeptides (eg, 2. Alterations in neuropeptides (eg, somatostatin), endorphins, somatostatin), endorphins, serotonin, norepinephrine, and serotonin, norepinephrine, and GABAGABA
3. Cytokines, such as interleukins and 3. Cytokines, such as interleukins and interferonsinterferons
2. Alterations in neuropeptides (eg, 2. Alterations in neuropeptides (eg, somatostatin), endorphins, somatostatin), endorphins, serotonin, norepinephrine, and serotonin, norepinephrine, and GABAGABA
3. Cytokines, such as interleukins and 3. Cytokines, such as interleukins and interferonsinterferons
Pathogenesis: (3) risk factorsPathogenesis: (3) risk factors MultifactorialMultifactorial
Underlying brain diseases, such as Underlying brain diseases, such as dementia, stroke, Parkinson’s dementia, stroke, Parkinson’s diseasedisease
Advanced age and sensory Advanced age and sensory impairmentimpairment
MultifactorialMultifactorial
Underlying brain diseases, such as Underlying brain diseases, such as dementia, stroke, Parkinson’s dementia, stroke, Parkinson’s diseasedisease
Advanced age and sensory Advanced age and sensory impairmentimpairment

Pathogenesis: (4) precipitating factorsPathogenesis: (4) precipitating factors Polypharmacy (particularly Polypharmacy (particularly
psychoactive drugs)psychoactive drugs)
InfectionsInfections
DehydrationDehydration
Immobility (including restraint use)Immobility (including restraint use)
MalnutritionMalnutrition
The use of bladder cathetersThe use of bladder catheters
Polypharmacy (particularly Polypharmacy (particularly psychoactive drugs)psychoactive drugs)
InfectionsInfections
DehydrationDehydration
Immobility (including restraint use)Immobility (including restraint use)
MalnutritionMalnutrition
The use of bladder cathetersThe use of bladder catheters
Differential Diagnosis for Etiology of DeliriumDifferential Diagnosis for Etiology of Delirium I – InfectionI – Infection
W - WithdrawalW - Withdrawal
A – Acute metabolicA – Acute metabolic
T - TraumaT - Trauma
C – CNS pathologyC – CNS pathology
H - HypoxiaH - Hypoxia
D – DeficienciesD – Deficiencies
E - EndocrinopathiesE - Endocrinopathies
A – Acute vascularA – Acute vascular
T – Toxins and drugsT – Toxins and drugs
H – Heavy metalsH – Heavy metals
I – InfectionI – Infection
W - WithdrawalW - Withdrawal
A – Acute metabolicA – Acute metabolic
T - TraumaT - Trauma
C – CNS pathologyC – CNS pathology
H - HypoxiaH - Hypoxia
D – DeficienciesD – Deficiencies
E - EndocrinopathiesE - Endocrinopathies
A – Acute vascularA – Acute vascular
T – Toxins and drugsT – Toxins and drugs
H – Heavy metalsH – Heavy metals

Delirium in the ElderlyPredisposing FactorsDelirium in the ElderlyPredisposing Factors Visual impairment (< 20/70)Visual impairment (< 20/70)
Severe illness (APACHE > 16)Severe illness (APACHE > 16)
Cognitive impairment (MMSE < 24)Cognitive impairment (MMSE < 24)
SUN/Cr > 18SUN/Cr > 18
LOW RISK – 0 factorsLOW RISK – 0 factors
INTERMEDIATE RISK – 1 to 2 factorsINTERMEDIATE RISK – 1 to 2 factors
HIGH RISK – 3 to 4 factorsHIGH RISK – 3 to 4 factors
Visual impairment (< 20/70)Visual impairment (< 20/70)
Severe illness (APACHE > 16)Severe illness (APACHE > 16)
Cognitive impairment (MMSE < 24)Cognitive impairment (MMSE < 24)
SUN/Cr > 18SUN/Cr > 18
LOW RISK – 0 factorsLOW RISK – 0 factors
INTERMEDIATE RISK – 1 to 2 factorsINTERMEDIATE RISK – 1 to 2 factors
HIGH RISK – 3 to 4 factorsHIGH RISK – 3 to 4 factors

Delirium in the ElderlyPrecipitating FactorsDelirium in the ElderlyPrecipitating Factors Use of physical restraintUse of physical restraint
Malnutrition (loss of 5.6 kg)Malnutrition (loss of 5.6 kg)
> 3 medications added> 3 medications added
Use of bladder catheterUse of bladder catheter
Any iatrogenic eventAny iatrogenic event
Use of physical restraintUse of physical restraint
Malnutrition (loss of 5.6 kg)Malnutrition (loss of 5.6 kg)
> 3 medications added> 3 medications added
Use of bladder catheterUse of bladder catheter
Any iatrogenic eventAny iatrogenic event
LOW RISK – 0 factorsLOW RISK – 0 factorsINTERMEDIATE RISK – 1 to 2 factorsINTERMEDIATE RISK – 1 to 2 factorsHIGH RISK – 3 to 4 factorsHIGH RISK – 3 to 4 factors

Clinical presentation of deliriumClinical presentation of delirium1. 1. Disturbance of consciousnessDisturbance of consciousness
A change in the level of awareness and A change in the level of awareness and the ability to focus, sustain, or shift the ability to focus, sustain, or shift attention.attention.
Often subtle, may precede by one day or more.Often subtle, may precede by one day or more.
Patient “isn’t acting quite right”Patient “isn’t acting quite right”
Distractibility, often evident in Distractibility, often evident in conversation.conversation.
Appearing drowsy, lethargic, or even Appearing drowsy, lethargic, or even semi-comatose in advanced cases.semi-comatose in advanced cases.
1. 1. Disturbance of consciousnessDisturbance of consciousness
A change in the level of awareness and A change in the level of awareness and the ability to focus, sustain, or shift the ability to focus, sustain, or shift attention.attention.
Often subtle, may precede by one day or more.Often subtle, may precede by one day or more.
Patient “isn’t acting quite right”Patient “isn’t acting quite right”
Distractibility, often evident in Distractibility, often evident in conversation.conversation.
Appearing drowsy, lethargic, or even Appearing drowsy, lethargic, or even semi-comatose in advanced cases.semi-comatose in advanced cases.
2. Change in cognition2. Change in cognition
Cognitive problems: memory loss, Cognitive problems: memory loss, disorientation, difficulty with language disorientation, difficulty with language and speech.and speech.
Need to ascertain baseline.Need to ascertain baseline.
Perceptual problems: misidentify the Perceptual problems: misidentify the clinician, vague delusions of harm.clinician, vague delusions of harm.
Visual and tactile hallucinations are not Visual and tactile hallucinations are not uncommonuncommon
2. Change in cognition2. Change in cognition
Cognitive problems: memory loss, Cognitive problems: memory loss, disorientation, difficulty with language disorientation, difficulty with language and speech.and speech.
Need to ascertain baseline.Need to ascertain baseline.
Perceptual problems: misidentify the Perceptual problems: misidentify the clinician, vague delusions of harm.clinician, vague delusions of harm.
Visual and tactile hallucinations are not Visual and tactile hallucinations are not uncommonuncommon
3. Temporal course3. Temporal course
Develop over hours to days and Develop over hours to days and typically persist for days to monthstypically persist for days to months
Acuteness of presentation is the most Acuteness of presentation is the most helpful feature in differentiating from helpful feature in differentiating from dementia.dementia.
Fluctuating: typically most severe in Fluctuating: typically most severe in the evening and at night, and the evening and at night, and relatively lucid during morning.relatively lucid during morning.
3. Temporal course3. Temporal course
Develop over hours to days and Develop over hours to days and typically persist for days to monthstypically persist for days to months
Acuteness of presentation is the most Acuteness of presentation is the most helpful feature in differentiating from helpful feature in differentiating from dementia.dementia.
Fluctuating: typically most severe in Fluctuating: typically most severe in the evening and at night, and the evening and at night, and relatively lucid during morning.relatively lucid during morning.

4. Other features4. Other features
Not essential diagnostic but common, Not essential diagnostic but common, including psychomotor agitation, including psychomotor agitation, sleep-wake reversals, irritability, sleep-wake reversals, irritability, anxiety, emotional lability, and anxiety, emotional lability, and hypersensitivity to lights and sounds.hypersensitivity to lights and sounds.
Common among older patients Common among older patients includes relatively quiet, withdrawn includes relatively quiet, withdrawn state that frequently is mistaken for state that frequently is mistaken for depression.depression.
4. Other features4. Other features
Not essential diagnostic but common, Not essential diagnostic but common, including psychomotor agitation, including psychomotor agitation, sleep-wake reversals, irritability, sleep-wake reversals, irritability, anxiety, emotional lability, and anxiety, emotional lability, and hypersensitivity to lights and sounds.hypersensitivity to lights and sounds.
Common among older patients Common among older patients includes relatively quiet, withdrawn includes relatively quiet, withdrawn state that frequently is mistaken for state that frequently is mistaken for depression.depression.
Evaluation of delirium (1)Evaluation of delirium (1) Two important aspects to the diagnostic Two important aspects to the diagnostic
evaluation: recognizing that the disorder evaluation: recognizing that the disorder is present, and uncovering the underlying is present, and uncovering the underlying cause.cause.
In some reports, clinicians fail to In some reports, clinicians fail to recognize delirium in 70 percent of cases.recognize delirium in 70 percent of cases.
Wrongly attributed to the patient’s age, to Wrongly attributed to the patient’s age, to dementia, or to other mental disorders dementia, or to other mental disorders such as depression.such as depression.
Two important aspects to the diagnostic Two important aspects to the diagnostic evaluation: recognizing that the disorder evaluation: recognizing that the disorder is present, and uncovering the underlying is present, and uncovering the underlying cause.cause.
In some reports, clinicians fail to In some reports, clinicians fail to recognize delirium in 70 percent of cases.recognize delirium in 70 percent of cases.
Wrongly attributed to the patient’s age, to Wrongly attributed to the patient’s age, to dementia, or to other mental disorders dementia, or to other mental disorders such as depression.such as depression.
Must not “normalize” lethargy or Must not “normalize” lethargy or somnolence by assuming that somnolence by assuming that illness, sleep loss, fatigue, or anxiety illness, sleep loss, fatigue, or anxiety cause the change.cause the change.
Require knowledge of the patient’s Require knowledge of the patient’s baseline level of functioning.baseline level of functioning.
Must not “normalize” lethargy or Must not “normalize” lethargy or somnolence by assuming that somnolence by assuming that illness, sleep loss, fatigue, or anxiety illness, sleep loss, fatigue, or anxiety cause the change.cause the change.
Require knowledge of the patient’s Require knowledge of the patient’s baseline level of functioning.baseline level of functioning.
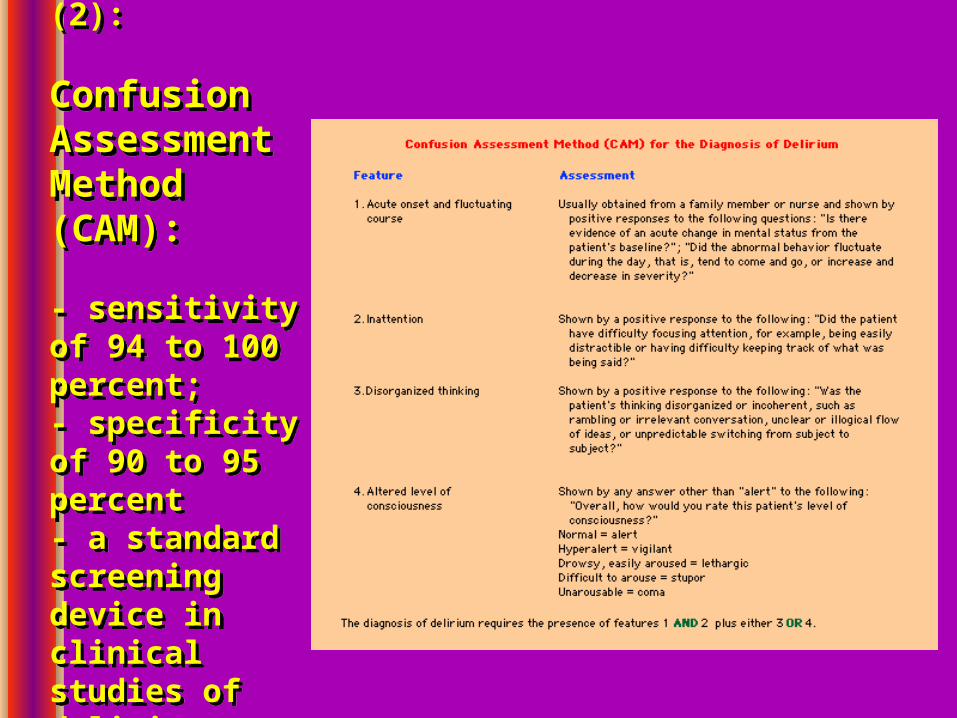
Evaluation (2):
Confusion Assessment Method (CAM):
- sensitivity of 94 to 100 percent;- specificity of 90 to 95 percent- a standard screening device in clinical studies of delirium
Evaluation (2):
Confusion Assessment Method (CAM):
- sensitivity of 94 to 100 percent;- specificity of 90 to 95 percent- a standard screening device in clinical studies of delirium

Evaluation (3)Evaluation (3) Investigating medical etiologies:Investigating medical etiologies:
Fluid and electrolyte disturbances Fluid and electrolyte disturbances (dehydration, hyponatremia and (dehydration, hyponatremia and hypernatremia)hypernatremia)
Infections (urinary, respiratory, skin and Infections (urinary, respiratory, skin and soft tissue)soft tissue)
Drug or alcohol toxicityDrug or alcohol toxicity
Withdrawal from alcoholWithdrawal from alcohol
Investigating medical etiologies:Investigating medical etiologies:
Fluid and electrolyte disturbances Fluid and electrolyte disturbances (dehydration, hyponatremia and (dehydration, hyponatremia and hypernatremia)hypernatremia)
Infections (urinary, respiratory, skin and Infections (urinary, respiratory, skin and soft tissue)soft tissue)
Drug or alcohol toxicityDrug or alcohol toxicity
Withdrawal from alcoholWithdrawal from alcohol

Withdrawal from barbiturates, Withdrawal from barbiturates, benzodiazepines, and SSRIbenzodiazepines, and SSRI
Metabolic disorders (hypoglycemia, Metabolic disorders (hypoglycemia, hypercalcemia, uremia, liver failure, hypercalcemia, uremia, liver failure, thyrotoxicosis)thyrotoxicosis)
Low perfusion states (shock, heart Low perfusion states (shock, heart failure)failure)
Postoperative states, especially in the Postoperative states, especially in the elderlyelderly
Withdrawal from barbiturates, Withdrawal from barbiturates, benzodiazepines, and SSRIbenzodiazepines, and SSRI
Metabolic disorders (hypoglycemia, Metabolic disorders (hypoglycemia, hypercalcemia, uremia, liver failure, hypercalcemia, uremia, liver failure, thyrotoxicosis)thyrotoxicosis)
Low perfusion states (shock, heart Low perfusion states (shock, heart failure)failure)
Postoperative states, especially in the Postoperative states, especially in the elderlyelderly

Evaluation (4): medication review
Evaluation (4): medication review
Differential DiagnosisDifferential Diagnosis
1.1. Sundowning: a frequently seen but Sundowning: a frequently seen but poorly understood; seen in evening poorly understood; seen in evening hours; typically in demented, hours; typically in demented, institutionalized patients.institutionalized patients.
2.2. Focal syndromesFocal syndromes
Temporal-parietal: patients w Temporal-parietal: patients w Wernicke’s aphasia – not comprehend, Wernicke’s aphasia – not comprehend, obey, seem confused; but restricted to obey, seem confused; but restricted to language.language.
1.1. Sundowning: a frequently seen but Sundowning: a frequently seen but poorly understood; seen in evening poorly understood; seen in evening hours; typically in demented, hours; typically in demented, institutionalized patients.institutionalized patients.
2.2. Focal syndromesFocal syndromes
Temporal-parietal: patients w Temporal-parietal: patients w Wernicke’s aphasia – not comprehend, Wernicke’s aphasia – not comprehend, obey, seem confused; but restricted to obey, seem confused; but restricted to language.language.

Occipital: Anton’s syndrome of cortical Occipital: Anton’s syndrome of cortical blindness and confabulationblindness and confabulation
Frontal: bifrontal lesions (eg, from tumor Frontal: bifrontal lesions (eg, from tumor or trauma) often show akinetic mutism, or trauma) often show akinetic mutism, lack of spontaneity, lack of judgment, lack of spontaneity, lack of judgment, problems w recent or working memory, problems w recent or working memory, blunted or labile emotional responses.blunted or labile emotional responses.
Occipital: Anton’s syndrome of cortical Occipital: Anton’s syndrome of cortical blindness and confabulationblindness and confabulation
Frontal: bifrontal lesions (eg, from tumor Frontal: bifrontal lesions (eg, from tumor or trauma) often show akinetic mutism, or trauma) often show akinetic mutism, lack of spontaneity, lack of judgment, lack of spontaneity, lack of judgment, problems w recent or working memory, problems w recent or working memory, blunted or labile emotional responses.blunted or labile emotional responses.

3. Nonconvulsive Status Epilepticus 3. Nonconvulsive Status Epilepticus (NCSE):(NCSE):
Requires EEG for detectionRequires EEG for detection
Show no classical ictal featuresShow no classical ictal features
Features: prominent bilateral facial Features: prominent bilateral facial twitching, unexplained nystagmoid eye twitching, unexplained nystagmoid eye movements during obtunded periods, movements during obtunded periods, spontaneous hippus, prolonged “ post-spontaneous hippus, prolonged “ post-ictal state”, automatisms (lip smacking, ictal state”, automatisms (lip smacking, chewing, swallowing movements).chewing, swallowing movements).
3. Nonconvulsive Status Epilepticus 3. Nonconvulsive Status Epilepticus (NCSE):(NCSE):
Requires EEG for detectionRequires EEG for detection
Show no classical ictal featuresShow no classical ictal features
Features: prominent bilateral facial Features: prominent bilateral facial twitching, unexplained nystagmoid eye twitching, unexplained nystagmoid eye movements during obtunded periods, movements during obtunded periods, spontaneous hippus, prolonged “ post-spontaneous hippus, prolonged “ post-ictal state”, automatisms (lip smacking, ictal state”, automatisms (lip smacking, chewing, swallowing movements).chewing, swallowing movements).
4. Dementia4. Dementia
Alzheimer’s – cognitive change is Alzheimer’s – cognitive change is insidious, progressive, without much insidious, progressive, without much fluctuation, over a much longer time fluctuation, over a much longer time (months to years).(months to years).
Lewy bodies – similar to Alzheimer’s, but Lewy bodies – similar to Alzheimer’s, but fluctuations and visual hallucinations fluctuations and visual hallucinations are more common and prominent.are more common and prominent.
5. Primary psychiatric illnesses: 5. Primary psychiatric illnesses:
Depression (poor sleep, difficulty w Depression (poor sleep, difficulty w attention or concentration)attention or concentration)
ManiaMania
4. Dementia4. Dementia
Alzheimer’s – cognitive change is Alzheimer’s – cognitive change is insidious, progressive, without much insidious, progressive, without much fluctuation, over a much longer time fluctuation, over a much longer time (months to years).(months to years).
Lewy bodies – similar to Alzheimer’s, but Lewy bodies – similar to Alzheimer’s, but fluctuations and visual hallucinations fluctuations and visual hallucinations are more common and prominent.are more common and prominent.
5. Primary psychiatric illnesses: 5. Primary psychiatric illnesses:
Depression (poor sleep, difficulty w Depression (poor sleep, difficulty w attention or concentration)attention or concentration)
ManiaMania
Laboratory testingLaboratory testing Serum electrolytes, creatinine, glucose, calcium, Serum electrolytes, creatinine, glucose, calcium,
CBC, and urinalysisCBC, and urinalysis
Drug levels, when appropriate. Drug levels, when appropriate. Delirium can occur even w “therapeutic” levels (digoxin, Delirium can occur even w “therapeutic” levels (digoxin,
lithium, or quinidine)lithium, or quinidine)
Toxic screen of blood and urineToxic screen of blood and urine
Blood gas: Respiratory alkalosis is due to early Blood gas: Respiratory alkalosis is due to early sepsis, hepatic failure, early salicylate sepsis, hepatic failure, early salicylate intoxication. Metabolic acidosis reflects uremia, intoxication. Metabolic acidosis reflects uremia, diabetic ketoacidosis, lactic acidosis, late phases diabetic ketoacidosis, lactic acidosis, late phases of sepsis or salicylate intoxication, methanol, of sepsis or salicylate intoxication, methanol, ethylene glycolethylene glycol
Serum electrolytes, creatinine, glucose, calcium, Serum electrolytes, creatinine, glucose, calcium, CBC, and urinalysisCBC, and urinalysis
Drug levels, when appropriate. Drug levels, when appropriate. Delirium can occur even w “therapeutic” levels (digoxin, Delirium can occur even w “therapeutic” levels (digoxin,
lithium, or quinidine)lithium, or quinidine)
Toxic screen of blood and urineToxic screen of blood and urine
Blood gas: Respiratory alkalosis is due to early Blood gas: Respiratory alkalosis is due to early sepsis, hepatic failure, early salicylate sepsis, hepatic failure, early salicylate intoxication. Metabolic acidosis reflects uremia, intoxication. Metabolic acidosis reflects uremia, diabetic ketoacidosis, lactic acidosis, late phases diabetic ketoacidosis, lactic acidosis, late phases of sepsis or salicylate intoxication, methanol, of sepsis or salicylate intoxication, methanol, ethylene glycolethylene glycol
NeuroimagingNeuroimaging Head CT may be used selectively rather Head CT may be used selectively rather
than routinely for evaluating delirium.than routinely for evaluating delirium.
May not be necessary if:May not be necessary if:
An obvious treatable medical illness or An obvious treatable medical illness or problemproblem
No evidence of traumaNo evidence of trauma
No new focal neurologic signs are presentNo new focal neurologic signs are present
Patient is arousable and able to follow simple Patient is arousable and able to follow simple commands.commands.
Head CT may be used selectively rather Head CT may be used selectively rather than routinely for evaluating delirium.than routinely for evaluating delirium.
May not be necessary if:May not be necessary if:
An obvious treatable medical illness or An obvious treatable medical illness or problemproblem
No evidence of traumaNo evidence of trauma
No new focal neurologic signs are presentNo new focal neurologic signs are present
Patient is arousable and able to follow simple Patient is arousable and able to follow simple commands.commands.
Head CT may be required if: Head CT may be required if:
Delirium does not improve despite Delirium does not improve despite appropriate treatment of underlying appropriate treatment of underlying medical conditionmedical condition
The neurologic examination is The neurologic examination is confounded by diminished patient confounded by diminished patient responsiveness or cooperation.responsiveness or cooperation.
Head CT may be required if: Head CT may be required if:
Delirium does not improve despite Delirium does not improve despite appropriate treatment of underlying appropriate treatment of underlying medical conditionmedical condition
The neurologic examination is The neurologic examination is confounded by diminished patient confounded by diminished patient responsiveness or cooperation.responsiveness or cooperation.
Lumbar punctureLumbar puncture
CSF analysis is the only diagnostic CSF analysis is the only diagnostic tool for the following mostly tool for the following mostly treatable conditions in delirium treatable conditions in delirium patients:patients:
Bacterial meningitisBacterial meningitis
EncephalitisEncephalitis
Nonbacterial CSF pleocytosis (eg, Nonbacterial CSF pleocytosis (eg, aseptic meningitis, carcinomatous aseptic meningitis, carcinomatous meningitis, encephalitis, seizures)meningitis, encephalitis, seizures)
CSF analysis is the only diagnostic CSF analysis is the only diagnostic tool for the following mostly tool for the following mostly treatable conditions in delirium treatable conditions in delirium patients:patients:
Bacterial meningitisBacterial meningitis
EncephalitisEncephalitis
Nonbacterial CSF pleocytosis (eg, Nonbacterial CSF pleocytosis (eg, aseptic meningitis, carcinomatous aseptic meningitis, carcinomatous meningitis, encephalitis, seizures)meningitis, encephalitis, seizures)
Elevated CSF glutamine concentration Elevated CSF glutamine concentration in hepatic encephalopathyin hepatic encephalopathy
Elevated opening pressure due to Elevated opening pressure due to increased ICPincreased ICP
LP is mandatory when the cause of LP is mandatory when the cause of delirium is not obvious.delirium is not obvious.
Elevated CSF glutamine concentration Elevated CSF glutamine concentration in hepatic encephalopathyin hepatic encephalopathy
Elevated opening pressure due to Elevated opening pressure due to increased ICPincreased ICP
LP is mandatory when the cause of LP is mandatory when the cause of delirium is not obvious.delirium is not obvious.
EEGEEG
Should be obtained for any patient Should be obtained for any patient with altered consciousness of with altered consciousness of unknown etiology.unknown etiology.
Useful to:Useful to:
Exclude seizures, esp. nonconvulsive or Exclude seizures, esp. nonconvulsive or subclinical seizuressubclinical seizures
Confirm the diagnosis of certain Confirm the diagnosis of certain metabolic encephalopathies or metabolic encephalopathies or infectious encephalopatidesinfectious encephalopatides
Should be obtained for any patient Should be obtained for any patient with altered consciousness of with altered consciousness of unknown etiology.unknown etiology.
Useful to:Useful to:
Exclude seizures, esp. nonconvulsive or Exclude seizures, esp. nonconvulsive or subclinical seizuressubclinical seizures
Confirm the diagnosis of certain Confirm the diagnosis of certain metabolic encephalopathies or metabolic encephalopathies or infectious encephalopatidesinfectious encephalopatides
Nonconvulsive seizuresNonconvulsive seizures lack motor lack motor manifestations or convulsions, but may manifestations or convulsions, but may impair consciousness.impair consciousness.
Nonconvulsive status epilepticusNonconvulsive status epilepticus may cause may cause continuous or fluctuating impairment of continuous or fluctuating impairment of consciousness.consciousness.
Metabolic encephalopathiesMetabolic encephalopathies may show may show diffuse bilateral slowing of background diffuse bilateral slowing of background rhythm and high wave amplitude.rhythm and high wave amplitude.
Viral encephalitisViral encephalitis may show diffuse may show diffuse background slowing and occasional background slowing and occasional epileptiform activity.epileptiform activity.
Nonconvulsive seizuresNonconvulsive seizures lack motor lack motor manifestations or convulsions, but may manifestations or convulsions, but may impair consciousness.impair consciousness.
Nonconvulsive status epilepticusNonconvulsive status epilepticus may cause may cause continuous or fluctuating impairment of continuous or fluctuating impairment of consciousness.consciousness.
Metabolic encephalopathiesMetabolic encephalopathies may show may show diffuse bilateral slowing of background diffuse bilateral slowing of background rhythm and high wave amplitude.rhythm and high wave amplitude.
Viral encephalitisViral encephalitis may show diffuse may show diffuse background slowing and occasional background slowing and occasional epileptiform activity.epileptiform activity.
TreatmentTreatment
1.1. Multicomponent interventionMulticomponent intervention
Standardized protocols to control six risk Standardized protocols to control six risk factors for delirium: cognitive impairment; factors for delirium: cognitive impairment; sleep deprivation; immobility; visual sleep deprivation; immobility; visual impairment; hearing impairment; and impairment; hearing impairment; and dehydration.dehydration.
Of 852 hospitalized pts aged 70 or older; Of 852 hospitalized pts aged 70 or older; resulted in significant reduction in the resulted in significant reduction in the number of delirium episodes vs usual care number of delirium episodes vs usual care ( 62 vs. 90) and in the total number of days w ( 62 vs. 90) and in the total number of days w delirium (105 vs 161)delirium (105 vs 161)
1.1. Multicomponent interventionMulticomponent intervention
Standardized protocols to control six risk Standardized protocols to control six risk factors for delirium: cognitive impairment; factors for delirium: cognitive impairment; sleep deprivation; immobility; visual sleep deprivation; immobility; visual impairment; hearing impairment; and impairment; hearing impairment; and dehydration.dehydration.
Of 852 hospitalized pts aged 70 or older; Of 852 hospitalized pts aged 70 or older; resulted in significant reduction in the resulted in significant reduction in the number of delirium episodes vs usual care number of delirium episodes vs usual care ( 62 vs. 90) and in the total number of days w ( 62 vs. 90) and in the total number of days w delirium (105 vs 161)delirium (105 vs 161)
Managing disruptive behaviorsManaging disruptive behaviors
Physical restraints should be used only as a Physical restraints should be used only as a last resort since they frequently increase last resort since they frequently increase agitation and create additional morbidity.agitation and create additional morbidity.
Hospital environment, characterized by high Hospital environment, characterized by high ambient noise, poor lighting, lack of ambient noise, poor lighting, lack of windows, frequent room changes, and windows, frequent room changes, and restraint use, often contribute to worsening restraint use, often contribute to worsening confusion.confusion.
Frequent reassurance, touch, and verbal Frequent reassurance, touch, and verbal orientation from familiar persons lessen orientation from familiar persons lessen disruptive behaviors.disruptive behaviors.
Physical restraints should be used only as a Physical restraints should be used only as a last resort since they frequently increase last resort since they frequently increase agitation and create additional morbidity.agitation and create additional morbidity.
Hospital environment, characterized by high Hospital environment, characterized by high ambient noise, poor lighting, lack of ambient noise, poor lighting, lack of windows, frequent room changes, and windows, frequent room changes, and restraint use, often contribute to worsening restraint use, often contribute to worsening confusion.confusion.
Frequent reassurance, touch, and verbal Frequent reassurance, touch, and verbal orientation from familiar persons lessen orientation from familiar persons lessen disruptive behaviors.disruptive behaviors.

Psychotropic medicationPsychotropic medication
A review by the Cochrane Collaborative A review by the Cochrane Collaborative found only one high-quality randomized trial, found only one high-quality randomized trial, which compared haloperidol, chlorpromazine, which compared haloperidol, chlorpromazine, and lorazepam in the treatment of deliriumand lorazepam in the treatment of delirium
Recommendation: low-dose haloperidol (0.5 Recommendation: low-dose haloperidol (0.5 to 1.0 mg PO, IV, or IM) be used to control to 1.0 mg PO, IV, or IM) be used to control agitation or psychotic symptoms.agitation or psychotic symptoms.
Jackson, Lipman. Drug therapy for delirium in terminally ill Jackson, Lipman. Drug therapy for delirium in terminally ill patients. The Cochrane Library, issue 2, 2004.patients. The Cochrane Library, issue 2, 2004.
A review by the Cochrane Collaborative A review by the Cochrane Collaborative found only one high-quality randomized trial, found only one high-quality randomized trial, which compared haloperidol, chlorpromazine, which compared haloperidol, chlorpromazine, and lorazepam in the treatment of deliriumand lorazepam in the treatment of delirium
Recommendation: low-dose haloperidol (0.5 Recommendation: low-dose haloperidol (0.5 to 1.0 mg PO, IV, or IM) be used to control to 1.0 mg PO, IV, or IM) be used to control agitation or psychotic symptoms.agitation or psychotic symptoms.
Jackson, Lipman. Drug therapy for delirium in terminally ill Jackson, Lipman. Drug therapy for delirium in terminally ill patients. The Cochrane Library, issue 2, 2004.patients. The Cochrane Library, issue 2, 2004.

Older patients are more likely to experience Older patients are more likely to experience severe extrapyramidal effects w haloperidol severe extrapyramidal effects w haloperidol (akathisia, potential fatal neuroleptic (akathisia, potential fatal neuroleptic malignant syndrome)malignant syndrome)
The newer antipsychotic agents The newer antipsychotic agents (risperidone, olanzapine) have fewer (risperidone, olanzapine) have fewer extrapyramidal side effects.extrapyramidal side effects.
Benzodiazepine (lorazepam 0.5 to 1.0 mg) Benzodiazepine (lorazepam 0.5 to 1.0 mg) have a more rapid onset of action (5 min have a more rapid onset of action (5 min after parenteral), but they commonly worsen after parenteral), but they commonly worsen confusion and sedation. Drug of choice only confusion and sedation. Drug of choice only in cases of sedative drug and alcohol in cases of sedative drug and alcohol withdrawal.withdrawal.
Older patients are more likely to experience Older patients are more likely to experience severe extrapyramidal effects w haloperidol severe extrapyramidal effects w haloperidol (akathisia, potential fatal neuroleptic (akathisia, potential fatal neuroleptic malignant syndrome)malignant syndrome)
The newer antipsychotic agents The newer antipsychotic agents (risperidone, olanzapine) have fewer (risperidone, olanzapine) have fewer extrapyramidal side effects.extrapyramidal side effects.
Benzodiazepine (lorazepam 0.5 to 1.0 mg) Benzodiazepine (lorazepam 0.5 to 1.0 mg) have a more rapid onset of action (5 min have a more rapid onset of action (5 min after parenteral), but they commonly worsen after parenteral), but they commonly worsen confusion and sedation. Drug of choice only confusion and sedation. Drug of choice only in cases of sedative drug and alcohol in cases of sedative drug and alcohol withdrawal.withdrawal.
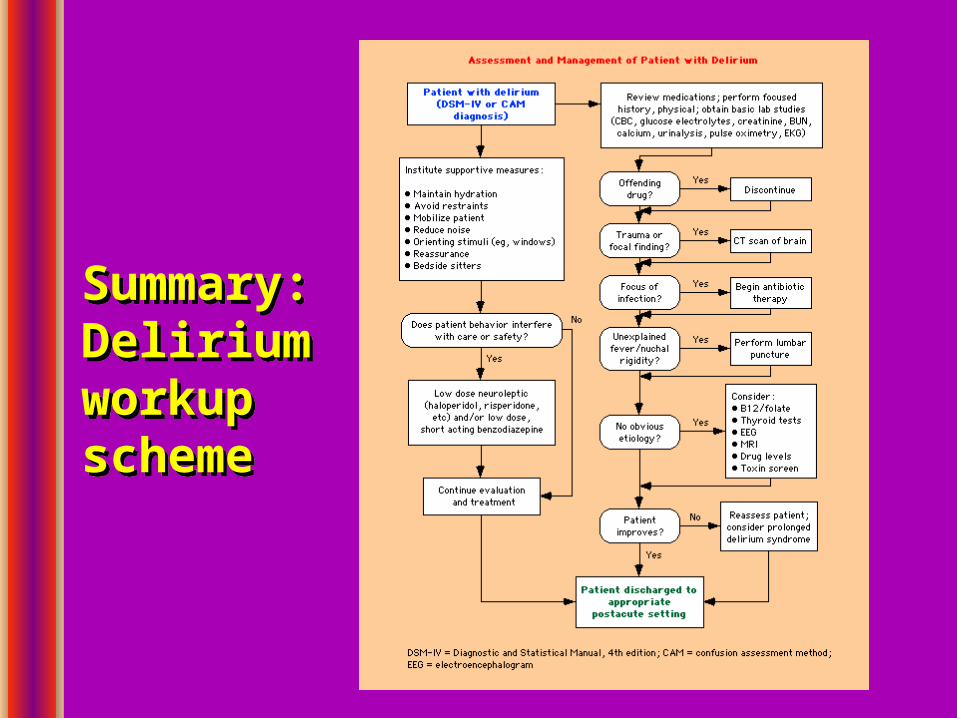
Summary:Delirium workup scheme
Summary:Delirium workup scheme

Summary: Common causes of Delirium
Summary: Common causes of Delirium
EEPPEECC
EEPPEECC
Thank YouThank You