RESEARCH Open Access Cutis Aplasia as a clinical hallmark for the syndrome associated with 19q13.11 deletion: the possible role for UBA2 gene Joana B Melo 1,2,3* , Alexandra Estevinho 1,2 , Jorge Saraiva 4,5 , Lina Ramos 4 and Isabel M Carreira 1,2,3 Abstract Background: Wide genome screening through array comparative genomic hybridization made possible the recognition of the novel 19q13.11 deletion syndrome. There are very few cases reported with this deletion, but clinically this condition seems to be recognizable by pre and postnatal growth retardation, microcephaly, developmental delay/intellectual disabilities, speech disturbance, hypospadias (in males) and signs of ectodermal dysplasia and cutis aplasia over the posterior occiput. Results: Using oligoarray CGH, a 4.6 Mb deletion in 19q13.11q13.12 was detected in a 23 year old female patient that presented clinical features previously associated with 19q13.11 deletion. Conclusions: Our work reinforces the idea that a region encompassing four zinc finger genes is likely to be responsible for the syndrome, and that the difference in minor clinical manifestation depends on the genes present outside the minimal overlapping region proposed for this syndrome. We also review all cases described in the literature and discuss the correlation between haploinsufficiency of UBA2 gene and cutis aplasia present in the majority of the patients reported, and its importance as a clinical hallmark of 19q13.11 deletion syndrome, when associated with more common features like developmental delay, microcephaly, speech disturbance and hypospadias in males. Keywords: 19q13.11 deletion, UBA2 gene, Cutis aplasia Background The development of array comparative genomic hybri- dization technique (array CGH) greatly improved the de- tection of cryptic unbalanced rearrangements in mental retardation patients and made possible the identification of novel microdeletion and microduplication syndromes [1]. In 1998, Kulharya et al., reported a cytogenetically visible 19q12q13.1 deletion, in a fetus with intrauterine growth retardation and decreased fetal activity. At the age of 3 years the child presented mental retardation, developmental delay, absence of speech, multiple minor anomalies and cutis aplasia [2]. Eleven years later, Malan et al., identified by array CGH a 19q13.11 microdeletion in three patients who share common clinical features with Kulharya et al.’ s patient, and proposed the 19q13.11 microdeletion syndrome as a novel clinically recognizable syndrome [3]. In 2009, Schuurs-Hoeijmarkers et al. narrowed the critical region responsible for the new syndrome to a 750 kb segment within the 19q13.11 de- letion [4]. Recently Forzano et al. further refined the critical region and Gana et al. , proposed a minimal over- laping region (MOR) of 324 kb encompassing four zinc finger genes [5,6]. A total of 8 mental retardation patients and 1 aborted fetus, carrying the 19q13.11 deletion have been reported until now in addition to two more cases included in the Database of Chromosome Imbalance and Phenotype in Humans using Ensembl Resources (DECIPHER) [2-7]. Despite some phenotypic variability, all these patients pre- sented common features and the deletion of 19q13.11 is proposed as a new clinical recognizable syndrome [3]. * Correspondence: [email protected] 1 Cytogenetics and Genomics Laboratory, Faculty of Medicine, University of Coimbra, Coimbra, Portugal 2 CIMAGO - Center of Investigation on Environment Genetics and Oncobiology, Faculty of Medicine, University of Coimbra, Coimbra, Portugal Full list of author information is available at the end of the article © 2015 Melo et al.; licensee BioMed Central. This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly credited. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated. Melo et al. Molecular Cytogenetics (2015) 8:21 DOI 10.1186/s13039-015-0123-x

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Melo et al. Molecular Cytogenetics (2015) 8:21 DOI 10.1186/s13039-015-0123-x
RESEARCH Open Access
Cutis Aplasia as a clinical hallmark for thesyndrome associated with 19q13.11 deletion:the possible role for UBA2 geneJoana B Melo1,2,3*, Alexandra Estevinho1,2, Jorge Saraiva4,5, Lina Ramos4 and Isabel M Carreira1,2,3
Abstract
Background: Wide genome screening through array comparative genomic hybridization made possible therecognition of the novel 19q13.11 deletion syndrome. There are very few cases reported with this deletion, butclinically this condition seems to be recognizable by pre and postnatal growth retardation, microcephaly,developmental delay/intellectual disabilities, speech disturbance, hypospadias (in males) and signs of ectodermaldysplasia and cutis aplasia over the posterior occiput.
Results: Using oligoarray CGH, a 4.6 Mb deletion in 19q13.11q13.12 was detected in a 23 year old female patientthat presented clinical features previously associated with 19q13.11 deletion.
Conclusions: Our work reinforces the idea that a region encompassing four zinc finger genes is likely to beresponsible for the syndrome, and that the difference in minor clinical manifestation depends on the genespresent outside the minimal overlapping region proposed for this syndrome. We also review all cases describedin the literature and discuss the correlation between haploinsufficiency of UBA2 gene and cutis aplasia present inthe majority of the patients reported, and its importance as a clinical hallmark of 19q13.11 deletion syndrome,when associated with more common features like developmental delay, microcephaly, speech disturbance andhypospadias in males.
Keywords: 19q13.11 deletion, UBA2 gene, Cutis aplasia
BackgroundThe development of array comparative genomic hybri-dization technique (array CGH) greatly improved the de-tection of cryptic unbalanced rearrangements in mentalretardation patients and made possible the identification ofnovel microdeletion and microduplication syndromes [1].In 1998, Kulharya et al., reported a cytogenetically
visible 19q12q13.1 deletion, in a fetus with intrauterinegrowth retardation and decreased fetal activity. At theage of 3 years the child presented mental retardation,developmental delay, absence of speech, multiple minoranomalies and cutis aplasia [2]. Eleven years later, Malanet al., identified by array CGH a 19q13.11 microdeletion
* Correspondence: [email protected] and Genomics Laboratory, Faculty of Medicine, Universityof Coimbra, Coimbra, Portugal2CIMAGO - Center of Investigation on Environment Genetics andOncobiology, Faculty of Medicine, University of Coimbra, Coimbra, PortugalFull list of author information is available at the end of the article
© 2015 Melo et al.; licensee BioMed Central. TCommons Attribution License (http://creativecreproduction in any medium, provided the orDedication waiver (http://creativecommons.orunless otherwise stated.
in three patients who share common clinical features withKulharya et al.’s patient, and proposed the 19q13.11microdeletion syndrome as a novel clinically recognizablesyndrome [3]. In 2009, Schuurs-Hoeijmarkers et al.narrowed the critical region responsible for the newsyndrome to a 750 kb segment within the 19q13.11 de-letion [4]. Recently Forzano et al. further refined thecritical region and Gana et al., proposed a minimal over-laping region (MOR) of 324 kb encompassing four zincfinger genes [5,6].A total of 8 mental retardation patients and 1 aborted
fetus, carrying the 19q13.11 deletion have been reporteduntil now in addition to two more cases included in theDatabase of Chromosome Imbalance and Phenotype inHumans using Ensembl Resources (DECIPHER) [2-7].Despite some phenotypic variability, all these patients pre-sented common features and the deletion of 19q13.11 isproposed as a new clinical recognizable syndrome [3].
his is an Open Access article distributed under the terms of the Creativeommons.org/licenses/by/4.0), which permits unrestricted use, distribution, andiginal work is properly credited. The Creative Commons Public Domaing/publicdomain/zero/1.0/) applies to the data made available in this article,
Melo et al. Molecular Cytogenetics (2015) 8:21 Page 2 of 7
Patients with this deletion are characterized by intra-uterine and postnatal growth retardation, microcephaly,developmental delay/intellectual disabilities, speech dis-turbance, slender habitus, feeding difficulties, cutis aplasiaover the posterior occiput, signs of ectodermal dysplasia,and genital malformation in males (hypospadias). In thisstudy we report a case of a mentally retarded womancarrier of a 19q13.11 deletion and compare our findingswith the ones previously reported in the literature [2-7].
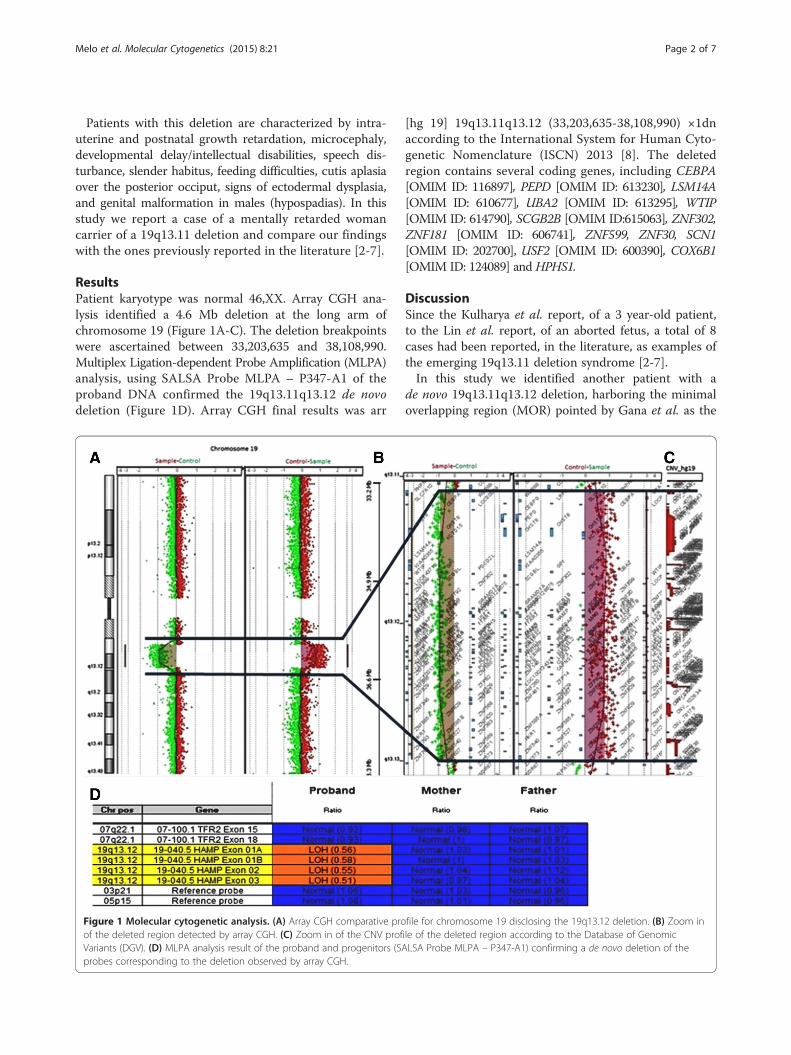
ResultsPatient karyotype was normal 46,XX. Array CGH ana-lysis identified a 4.6 Mb deletion at the long arm ofchromosome 19 (Figure 1A-C). The deletion breakpointswere ascertained between 33,203,635 and 38,108,990.Multiplex Ligation-dependent Probe Amplification (MLPA)analysis, using SALSA Probe MLPA – P347-A1 of theproband DNA confirmed the 19q13.11q13.12 de novodeletion (Figure 1D). Array CGH final results was arr
Figure 1 Molecular cytogenetic analysis. (A) Array CGH comparative proof the deleted region detected by array CGH. (C) Zoom in of the CNV profVariants (DGV). (D) MLPA analysis result of the proband and progenitors (SAprobes corresponding to the deletion observed by array CGH.
[hg 19] 19q13.11q13.12 (33,203,635-38,108,990) ×1dnaccording to the International System for Human Cyto-genetic Nomenclature (ISCN) 2013 [8]. The deletedregion contains several coding genes, including CEBPA[OMIM ID: 116897], PEPD [OMIM ID: 613230], LSM14A[OMIM ID: 610677], UBA2 [OMIM ID: 613295], WTIP[OMIM ID: 614790], SCGB2B [OMIM ID:615063], ZNF302,ZNF181 [OMIM ID: 606741], ZNF599, ZNF30, SCN1[OMIM ID: 202700], USF2 [OMIM ID: 600390], COX6B1[OMIM ID: 124089] and HPHS1.
DiscussionSince the Kulharya et al. report, of a 3 year-old patient,to the Lin et al. report, of an aborted fetus, a total of 8cases had been reported, in the literature, as examples ofthe emerging 19q13.11 deletion syndrome [2-7].In this study we identified another patient with a
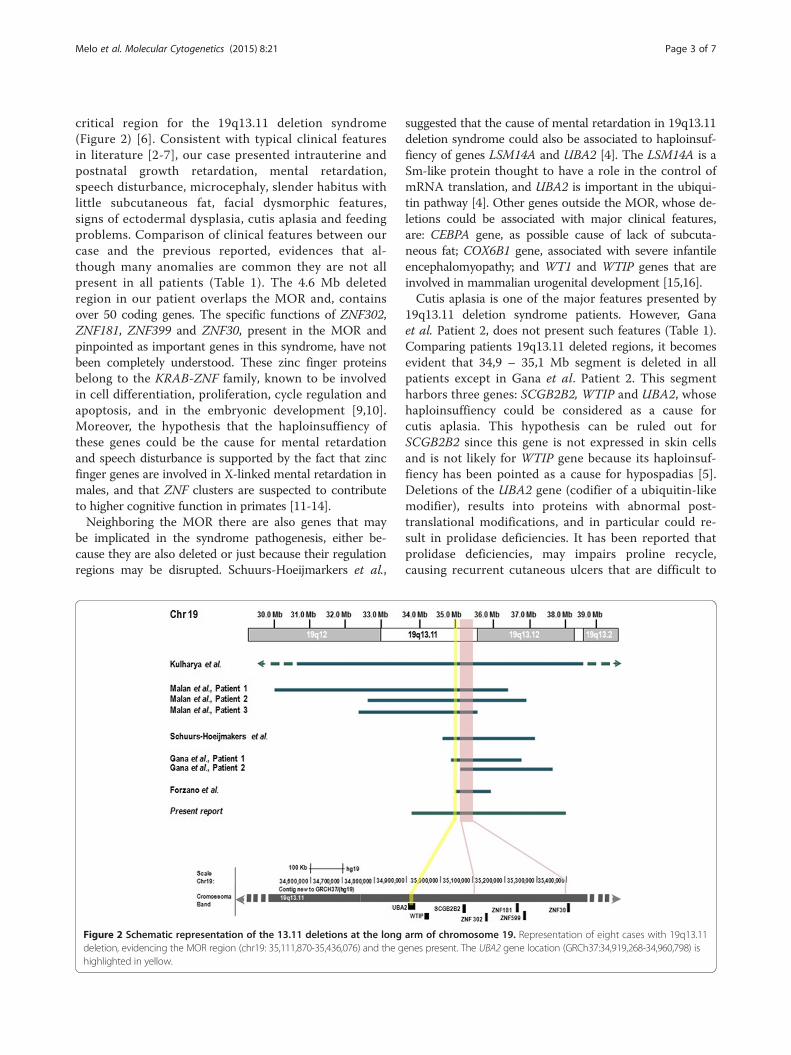
de novo 19q13.11q13.12 deletion, harboring the minimaloverlapping region (MOR) pointed by Gana et al. as the
file for chromosome 19 disclosing the 19q13.12 deletion. (B) Zoom inile of the deleted region according to the Database of GenomicLSA Probe MLPA – P347-A1) confirming a de novo deletion of the
Melo et al. Molecular Cytogenetics (2015) 8:21 Page 3 of 7
critical region for the 19q13.11 deletion syndrome(Figure 2) [6]. Consistent with typical clinical featuresin literature [2-7], our case presented intrauterine andpostnatal growth retardation, mental retardation,speech disturbance, microcephaly, slender habitus withlittle subcutaneous fat, facial dysmorphic features,signs of ectodermal dysplasia, cutis aplasia and feedingproblems. Comparison of clinical features between ourcase and the previous reported, evidences that al-though many anomalies are common they are not allpresent in all patients (Table 1). The 4.6 Mb deletedregion in our patient overlaps the MOR and, containsover 50 coding genes. The specific functions of ZNF302,ZNF181, ZNF399 and ZNF30, present in the MOR andpinpointed as important genes in this syndrome, have notbeen completely understood. These zinc finger proteinsbelong to the KRAB-ZNF family, known to be involvedin cell differentiation, proliferation, cycle regulation andapoptosis, and in the embryonic development [9,10].Moreover, the hypothesis that the haploinsuffiency ofthese genes could be the cause for mental retardationand speech disturbance is supported by the fact that zincfinger genes are involved in X-linked mental retardation inmales, and that ZNF clusters are suspected to contributeto higher cognitive function in primates [11-14].Neighboring the MOR there are also genes that may
be implicated in the syndrome pathogenesis, either be-cause they are also deleted or just because their regulationregions may be disrupted. Schuurs-Hoeijmarkers et al.,
Figure 2 Schematic representation of the 13.11 deletions at the longdeletion, evidencing the MOR region (chr19: 35,111,870-35,436,076) and the ghighlighted in yellow.
suggested that the cause of mental retardation in 19q13.11deletion syndrome could also be associated to haploinsuf-fiency of genes LSM14A and UBA2 [4]. The LSM14A is aSm-like protein thought to have a role in the control ofmRNA translation, and UBA2 is important in the ubiqui-tin pathway [4]. Other genes outside the MOR, whose de-letions could be associated with major clinical features,are: CEBPA gene, as possible cause of lack of subcuta-neous fat; COX6B1 gene, associated with severe infantileencephalomyopathy; and WT1 and WTIP genes that areinvolved in mammalian urogenital development [15,16].Cutis aplasia is one of the major features presented by
19q13.11 deletion syndrome patients. However, Ganaet al. Patient 2, does not present such features (Table 1).Comparing patients 19q13.11 deleted regions, it becomesevident that 34,9 – 35,1 Mb segment is deleted in allpatients except in Gana et al. Patient 2. This segmentharbors three genes: SCGB2B2, WTIP and UBA2, whosehaploinsuffiency could be considered as a cause forcutis aplasia. This hypothesis can be ruled out forSCGB2B2 since this gene is not expressed in skin cellsand is not likely for WTIP gene because its haploinsuf-fiency has been pointed as a cause for hypospadias [5].Deletions of the UBA2 gene (codifier of a ubiquitin-likemodifier), results into proteins with abnormal post-translational modifications, and in particular could re-sult in prolidase deficiencies. It has been reported thatprolidase deficiencies, may impairs proline recycle,causing recurrent cutaneous ulcers that are difficult to
arm of chromosome 19. Representation of eight cases with 19q13.11enes present. The UBA2 gene location (GRCh37:34,919,268-34,960,798) is
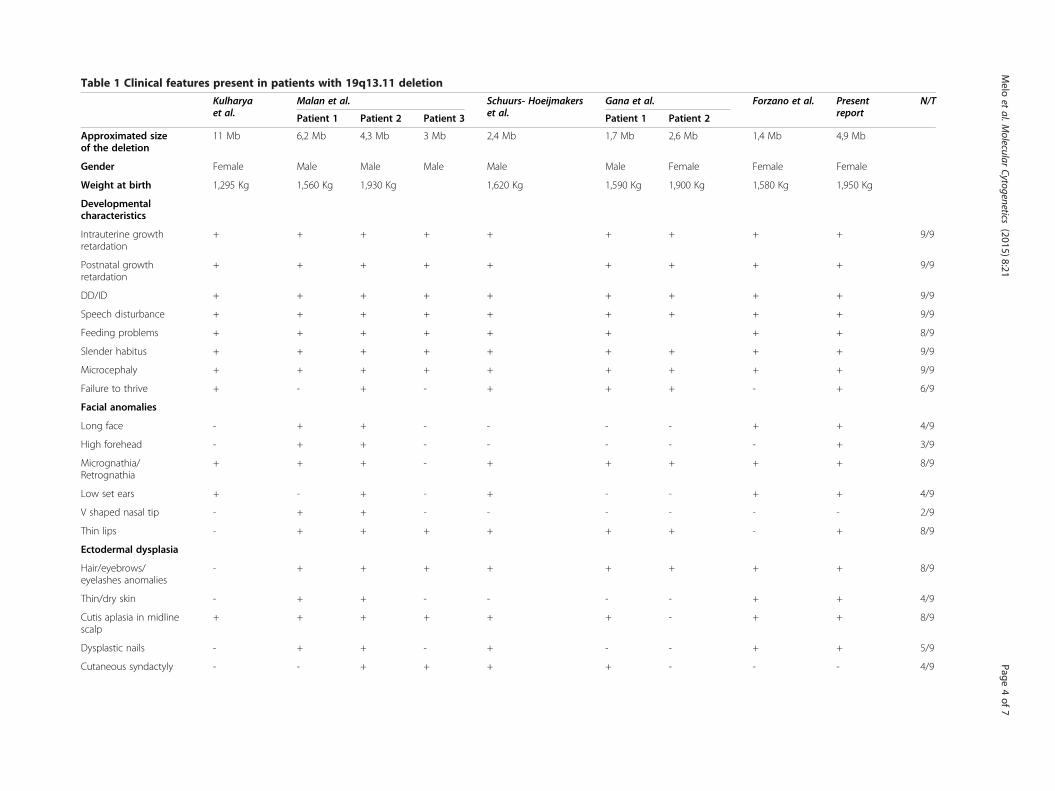
Table 1 Clinical features present in patients with 19q13.11 deletion
Kulharyaet al.
Malan et al. Schuurs- Hoeijmakerset al.
Gana et al. Forzano et al. Presentreport
N/T
Patient 1 Patient 2 Patient 3 Patient 1 Patient 2
Approximated sizeof the deletion
11 Mb 6,2 Mb 4,3 Mb 3 Mb 2,4 Mb 1,7 Mb 2,6 Mb 1,4 Mb 4,9 Mb
Gender Female Male Male Male Male Male Female Female Female
Weight at birth 1,295 Kg 1,560 Kg 1,930 Kg 1,620 Kg 1,590 Kg 1,900 Kg 1,580 Kg 1,950 Kg
Developmentalcharacteristics
Intrauterine growthretardation
+ + + + + + + + + 9/9
Postnatal growthretardation
+ + + + + + + + + 9/9
DD/ID + + + + + + + + + 9/9
Speech disturbance + + + + + + + + + 9/9
Feeding problems + + + + + + + + 8/9
Slender habitus + + + + + + + + + 9/9
Microcephaly + + + + + + + + + 9/9
Failure to thrive + - + - + + + - + 6/9
Facial anomalies
Long face - + + - - - - + + 4/9
High forehead - + + - - - - - + 3/9
Micrognathia/Retrognathia
+ + + - + + + + + 8/9
Low set ears + - + - + - - + + 4/9
V shaped nasal tip - + + - - - - - - 2/9
Thin lips - + + + + + + - + 8/9
Ectodermal dysplasia
Hair/eyebrows/eyelashes anomalies
- + + + + + + + + 8/9
Thin/dry skin - + + - - - - + + 4/9
Cutis aplasia in midlinescalp
+ + + + + + - + + 8/9
Dysplastic nails - + + - + - - + + 5/9
Cutaneous syndactyly - - + + + + - - - 4/9
Melo
etal.M
olecularCytogenetics
(2015) 8:21 Page
4of
7
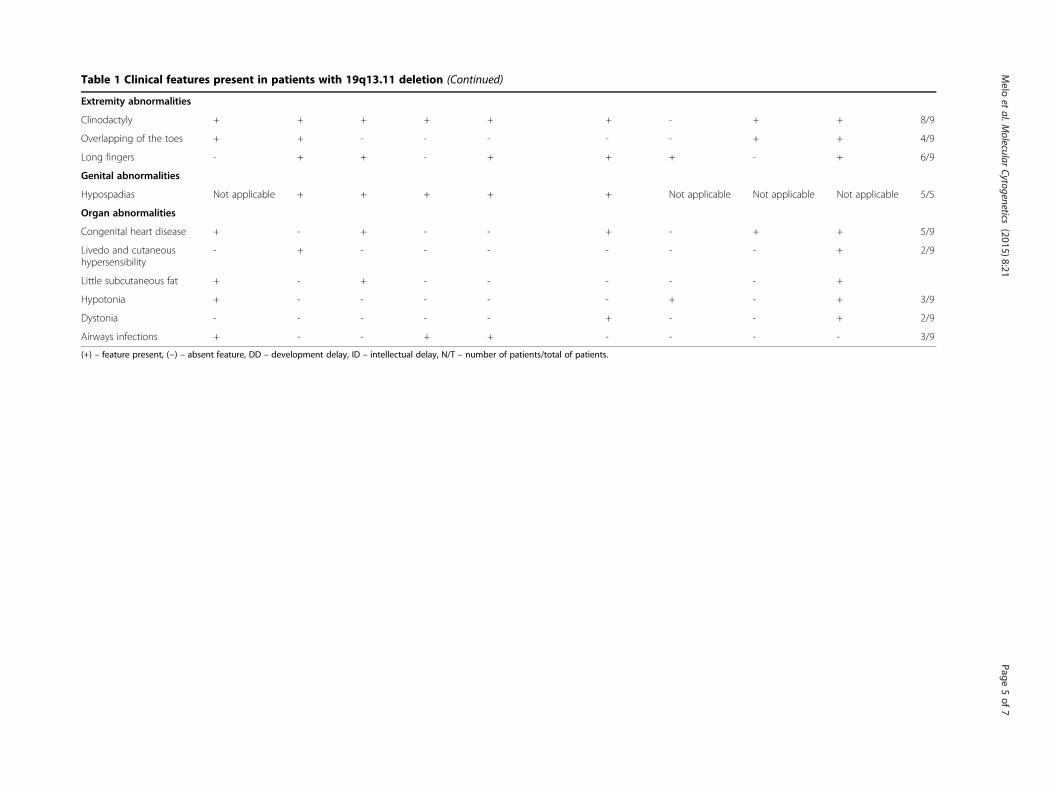
Table 1 Clinical features present in patients with 19q13.11 deletion (Continued)
Extremity abnormalities
Clinodactyly + + + + + + - + + 8/9
Overlapping of the toes + + - - - - - + + 4/9
Long fingers - + + - + + + - + 6/9
Genital abnormalities
Hypospadias Not applicable + + + + + Not applicable Not applicable Not applicable 5/5
Organ abnormalities
Congenital heart disease + - + - - + - + + 5/9
Livedo and cutaneoushypersensibility
- + - - - - - - + 2/9
Little subcutaneous fat + - + - - - - - +
Hypotonia + - - - - - + - + 3/9
Dystonia - - - - - + - - + 2/9
Airways infections + - - + + - - - - 3/9
(+) – feature present, (−) – absent feature, DD – development delay, ID – intellectual delay, N/T – number of patients/total of patients.
Melo
etal.M
olecularCytogenetics
(2015) 8:21 Page
5of
7

Melo et al. Molecular Cytogenetics (2015) 8:21 Page 6 of 7
heal resulting in cutis aplasia. This could also accountfor the thin skin, observed in some patients, reinforcingthe role for UBA2 gene in cutis aplasia [2].Apart from the core phenotype, other clinical features
seemed to be associated with genes outside the MOR:hypotonia has been reported and associated withUQCRFS1 and VIB genes; renal anomalies, associatedwith HPHS1 and USF2 genes; and cardiac defects associ-ated with SCN1B gene [2-5]. Although these genes aredeleted in several cases, patients do not present thesame phenotype, leading to suppose that they can actlike a predisposing factor that can be trigged under acertain genetic, epigenetic or environmental context.
ConclusionsIn conclusion, 19q13.11 deletion syndrome is a continu-ous genetic disease where a critical region is responsiblefor the major clinical features. Other genes outside thatregion contribute to clinical features observed less fre-quently. Reviewing all the reported cases and ours webelieved that cutis aplasia could be related to haploinsuf-fiency of UBA2 gene. The report of further patients withthis deletion would reinforce this evidence.
MethodsPatient reportOur patient was born from non-consanguineous healthyparents, after 39 weeks of gestation and a complicatedpregnancy due to intrauterine growth retardation. At birthshe weight 1950 g (<5th centile), measured 42 cm (<5thcentile) and her head circumference was 30 cm (<5thcentile). After birth, she presented feeding difficulties, andit was necessary the presence of a gastrostomy button.Some dysmorphic features were presented, like microceph-aly, long face, high forehead, low set ears, deep set eyes, Vshaped nasal tip, hipoplasic alae nasi, thin lips, retrognathiaand high arched palate. After teething, teeth abnormalities
Figure 3 Dysmorphic features presented by the 23 year old patient. (A)cutis aplasia over the posterior occiput. (C) Photograph evidencing dysplastic
were presented. Signs of ectodermal dysplasia includedsparse eyebrows and eyelashes, cutis aplasia in midlinescalp, thin and dry skin and dysplastic nails (Figure 3). Ex-tremity abnormalities were noticed, with clinodactyly, longfinger and overlapping toes. Other anomalies included con-genital heart disease, congenital dislocation of the hip,livedo and cutaneous hypersensibility. Her early years werecompromised by feeding difficulties and failure to thrive.From the first (7 month old) to her last examination(23 years old) she always presented slender habitus, shewas very thin with very little subcutaneous fat tissue.Throughout her growth dystonia, hiperlaxity of the joints,poor strength, walking disabilities, myopia, absence of ver-bal skills, and growth retardation were noticed.
Standard karyotypingChromosome analysis was performed on blood lympho-cytes, using GTG high resolution banding technique, ac-cording to standard procedures [17].
Array CGHDNA was extracted from the proband and parent’s periph-eral blood, using the QIAmp DNA Mini kit (Qiagen,Valencia, CA, USA) according to manufacturer’s ins-tructions. DNA concentration was determinate with Nano-Drop ND1000 spectrophotometer and software (NanoDropTechnologies, Berlin, Germany). Array CGH analysis wasperformed using the Agilent kit 4×180K (Human GenomeCGH Microarray, Agilent Technologies, Santa Clara, CA,USA), with a 17 Kb resolution, according to manufacturer’sprotocol [18]. Genomic positions are referred to theHuman Genome February 2009 assembly (hg19).
Multi ligation-dependent probe amplificationMulti ligation-dependent probe amplification was usedto confirm oligoarray-CGH results for chromosome 19in the proband and parents, with commercially available
Photograph of the patient with 23 years old. (B) Photograph evidencingnails.
Melo et al. Molecular Cytogenetics (2015) 8:21 Page 7 of 7
SALSA P347-A1 for microdeletions syndromes (MRC Hol-land, Amsterdam, Netherlands) and was performed accord-ing to manufacturer’s instructions. Amplification productswere electrophoresed on an ABI PRISM 3100 GeneticAnalyzer and the data obtained analyzed by excel spread-sheet (MRC Holland, Amsterdam, Netherlands) [19].Written informed consent was obtained for publication
and any accompanying images. A copy of the writtenconsent is available for review by the Editor-in-Chief ofthis journal.
AbbreviationsCGH: Comparative genomic hybridization; DECIPHER: Database ofChromosome Imbalance and Phenotype in Humans using EnsemblResources; ISCN: International System for Human Cytogenetic Nomenclature;MLPA: Multiplex Ligation-dependent Probe Amplification; MOR: Minimaloverlaping region; OMIM ID: Online Mendelian Inheritance in ManIdentification.
Competing interestsThe authors declare that they have no competing interests.
Authors’ contributionsJBM conceived the study, designed it, carried out the molecular andconventional cytogenetic analysis and helped to draft the manuscript. AEdrafted the manuscript. JS clinically evaluated the patient at her first’s yearsof life. LR clinically evaluated the patient at adult age. IMC participated in thestudy coordination and helped to draft the manuscript. All authors read andapproved the manuscript.
Author details1Cytogenetics and Genomics Laboratory, Faculty of Medicine, Universityof Coimbra, Coimbra, Portugal. 2CIMAGO - Center of Investigation onEnvironment Genetics and Oncobiology, Faculty of Medicine, University ofCoimbra, Coimbra, Portugal. 3CNC - IBILI - Center of Neurosciences - Institutefor Biomedical Imaging and Life Sciences, Coimbra, Portugal. 4Medical GeneticsUnit, Hospital Pediátrico, Centro Hospitalar e Universitário de Coimbra, Coimbra,Portugal. 5University Clinic of Pediatrics, Faculty of Medicine, University ofCoimbra, Coimbra, Portugal.
Received: 9 January 2015 Accepted: 25 February 2015
References1. Boone PM, Bacino CA, Shaw CA, Eng PA, Hixson PM, Pursley AN, et al.
Detection of clinically relevant exonic copy-number changes by array CGH.Hum Mut. 2010;31(12):1326–42.
2. Kulharya AS, Michaelis RC, Norris KS, Taylor HA, Garcia-Heras J. Constitutionaldel (19) (q12q13.1) in a three-year-old girl with severe phenotypic abnormalitiesaffecting multiple organ systems. Am J Med Genet. 1998;77:391–4.
3. Malan V, Raoul O, Firth HV, Royer G, Turleau C, Bernheim A, et al. 19q13.11deletion syndrome: a novel clinically recognizable genetic conditionidentified by array comparative genomic hybridisation. J Med Genet.2009;46:635–40.
4. Schuurs-Hoeijmakers JHM, Vermeer S, van Bon BWM, Plund R, Marcelis C, deBrouwer APM, et al. Refining the critical region of the novel 19q13.11microdeletion syndrome to 750 Kb. J Med Genet. 2009;46(6):421.
5. Gana S, Veggiotti P, Sciacca G, Fedeli C, Bersano A, Micieli G, et al. 19q13.11cryptic deletion: description of two new cases and indication for a role ofWTIP haploinsufficiency in hypospadias. Eur J Hum Genet. 2012;20:852–6.
6. Forzano F, Napoli F, Uliana V, Malacarne M, Viaggi C, Bloise R, et al. 19q13.11microdeletion syndrome: further refining the critical region. J Med Genet.2012;55:429–32.
7. Lin SY, Lee CN, Chen TC, Tu MP, Lin CY, Chang TY, et al. A fetus with19q13.11 microdeletion presenting with intrauterine growth restriction andmultiple cystic kidney. Case Rep Perinat Med. 2012;1(1–2):69–74.
8. Shaffer LG, McGowan-Jordan J, Schimid M. Annual international system forhuman cytogenetic nomenclature. ISCN: Karger. 2013.
9. Urritia R. KRAB-containing zinc-finger repressor proteins. Genome Biol.2003;4:231–7.
10. Kleefstra T, Yntema HG, Oudakker AR, Banning MJG, Kalscheuer VM, Chelly J,et al. Zinc finger 81 (ZNF81) mutations associated with X-linked mentalretardation. J Med Genet. 2004;41(5):394–9.
11. Lugtenberg D, Yntema HG, Banning MJG, Oudakker AR, Firth HV, Willatt L,et al. ZNF674: a new krüppel-associated box–containing zinc-finger geneinvolved in nonsyndromic X-linked mental retardation. Am J Hum Genet.2006;78(2):265–78.
12. Shoichet SA, Hoffmann K, Menzel C, Trautmann U, Moser B, Hoeltzenbein M,et al. Mutations in the ZNF41 gene are associated with cognitive deficits:identification of a new candidate for X-linked mental retardation. Am J HumGenet. 2003;73(6):1341–54.
13. Tadepally HD, Burger G, Aubry M. Evolution of C2H2-zinc finger genes andsubfamilies in mammals: species-specific duplication and loss of clusters,genes and effector domains. BMC Evol Biol. 2008;8:1471–2148.
14. Wang N-D, Finegold MJ, Bradley A, Ou CN, Abdelsayed SV, Wilde MD, et al.Impaired energy homeostasis in C/EBP-alpha knockout mice. Science.1995;269:1108–12.
15. Massa V, Fernandez-Vizzarra E, Alshahwan S, Bakhsh E, Goffrini P, Ferrero I,et al. Severe infantil encephalomyopathy caused by a mutation in COX6B1,a nucleus-encoded subunit of cytochrome c oxidase. Am J Hum Genet.2008;82:1281–9.
16. Regev M, Kirk R, Mashevich M, Bistritzer Z, Reish O. Vertical transmission of amutation in exon 1 of the WT1 gene: lessons for genetic counseling. Am JMed Genet Part A. 2008;146A:2332–6.
17. Rooney DE, Czepulkowski BH. Human cytogenetics: a practical approach.New York: Oxford University Press; 1992.
18. Matoso E, Melo JB, Ferreira SI, Jardim A, Castelo TM, Weise A, et al.Insertional translocation leading to a 4q13 duplication including the EPHA5gene in two siblings with attention-deficit hyperactivity disorder. Am J MedGenet A. 2013;161A(8):1923–8.
19. Ferreira SI, Matoso E, Venâncio M, Saraiva J, Melo JB, Carreira IM. Criticalregion in 2q31.2q32.3 deletion syndrome: reporto f two phenotypicallydistinct patients, one with an additional in alagille syndrome region. MolCytogenet. 2012;5:25–30.
Submit your next manuscript to BioMed Centraland take full advantage of:
• Convenient online submission
• Thorough peer review
• No space constraints or color figure charges
• Immediate publication on acceptance
• Inclusion in PubMed, CAS, Scopus and Google Scholar
• Research which is freely available for redistribution
Submit your manuscript at www.biomedcentral.com/submit
Related Documents











