Cultural Competence July 2008

Cultural Competence July 2008. The ACE Cultural Competence Committee Margaret M. Andrews, PhD, RN, CTN, FAAN Lauren Clark, PhD, RN, FAAN Katherine Foss,
Dec 25, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Cultural Competence
July 2008

The ACE Cultural Competence
Committee
Margaret M. Andrews, PhD, RN, CTN, FAAN
Lauren Clark, PhD, RN, FAAN
Katherine Foss, MS, RN
Sandie Kerlagon, MS, RN
Jo Keuhn, RN, BS(Original Date: 2004)

Cultural Competence in Clinical Settings: An
Introduction for New Nurses

What is Culture?
A definition: Leninger (1985) describes culture as: ‘the values, beliefs, norms, and practices
of a particular group that are learned and shared and that guide thinking, decisions and actions in a patterned way’
Or more simply: the luggage each of us carries around for our lifetime (Spector, 2003)

Culture determines….
Who is healthy & ill What people think causes health & illness What healers are sought to prevent and
treat disease What treatments are used Appropriate sick role behavior How long a person is sick & when he/she
has recovered

the ability of health care providers and health care organizations to understand and respond effectively to the cultural and linguistic needs brought by the patient to the health care encounter.
U.S. Department of Health & Human Services, 2003
Cultural and Linguistic Competence

Campinha-Bacote, 2008
1
2
3

Cultural Competence
Begins with understanding of own self
Includes knowledge of various cultural characteristics
Includes an understanding of cultural characteristics
Requires application of cultural knowledge and understanding in the healthcare setting

Non-ethnic CulturesSelected Examples
Socioeconomic status
Sexual Orientation
Handicap/Disability
Occupation
Age
Poverty The Homeless The Affluent/Wealthy
Gay, Lesbian, Bisexual, Transgender
Deaf/Hearing Impaired Blind/Visually Impaired
Nurses, Military
Adolescents, Elderly
The Culture of…..

We must not presume that all people of a certain culture adhere to all aspects of their culture. The healthcare provider must identify which aspects are appropriate for each patient during the admission process.

Cultural Assessment
is a “systematic appraisal or examination of individuals, groups, and communities as to their cultural beliefs, values & practices to determine explicit needs & intervention practices within the cultural context of the people being evaluated.”
Leininger & McFarland, 2006

Explanatory Models
Explain why we are sick to other people and to ourselves to make sense of our misfortune
Example: “You have a terrible cold!”
“You’re right—It is because I got run down and then went outside without a coat yesterday. That’s why I’m sick.”

Explanatory Model Questions What is the patient’s ethnic affiliation? Who are the patient’s major support persons
and where do they live? With whom should we speak about the
patient’s health or illness? What are the patient’s primary and secondary
languages, and speaking and reading abilities? What is the patient’s economic situation? Is
income adequate to meet the patient’s and family’s needs? (Lipson & Dibble, 2005)

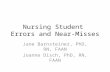
Spirituality & Religion

Spirituality refers to a subjective experience of the
sacred, whereas religion involves subscribing to a set
of beliefs or doctrines that are institutionalized.

33%
18%16%
16%
6%
4%4% 3%
Christianity
Islam
Hinduism
Nonreligious
Buddhism
ChineseTraditionalPrimal-indigenousOther
Major World Religions

U.S. Religions
354,194 Congregations
> 1,200 Denominations
Yearbook of American & Canadian Churches, 2002

Spiritual & Religious Healers
Priest
MonkShaman
Elder
BishopRabbi
Medicine Man
Medicine
Woman
Curandero/a

Religion & spirituality in healing….
Prayer, Chants Pilgrimages Fasting Amulets or talismans Healing rituals
Anointing with oil Sacraments Laying on of hands

Religion, Health & Culture
Research demonstrates positive health outcomes for people with strong spiritual and religious beliefs
Congruent with holistic philosophical beliefs about human nature
Dietary & lifestyle practices often promote health & prevent disease (e.g., lower incidence of heart disease among Mormons & Seventh-day Adventists)
Guides moral & ethical decision making

Symbols of Ethnoreligious Identity
Shrines with Buddha, candles, incense, and various artifacts (Buddhist)
Presence of prayer beads (Muslim) Amulets and talismans (charms) to ward off illness or
bring good health (Mexican, Puerto Rican, & many African groups)
Rosaries, religious medals, statues, votive candles (Catholics)
Presence of mezuzza (small case containing torah passages on parchment--usually hung in doorway)

Include Religious & Spiritual Factors in Cultural Assessment
Health-related beliefs & practices, e.g., diet, medications, medical & surgical procedures
Religious calendar & holy days Healing practices Religious network for providing spiritual &
emotional support for sick & dying members. Spiritual & religious healers

Religious, Cultural & Civic Holidays
Avoid scheduling medical appointments during holidays
Avoid disruption to holy days (such as fasting during Ramadan)

Promoting Effective Cross-Cultural Communication.....
Always ask, “By what name may I
call you?”

What do Limited-English Speakers Want?
Speaking one’s native language is….
• Easier when feeling ill• More comfortable• More accurate

What is unsafe practice with Limited-English speakers?
Using family members as interpreters Recruiting ad hoc (or untrained)
interpreters Writing instructions in English
Interpreter errors cause medical errors (Levine, JAMA, 2006)

Why not use a family member as an interpreter?
Office for Civil Rights (OCR) Policy Guidance (2000) states that untrained “interpreters”:
May not understand the concepts or official terminology they are asked to interpret or translate
Obstruct the flow of confidential information to the provider.
Fail to disclose intimate details of personal and family life; Clinicians, too, refrain from candid discussions with untrained interpreters present.

Requirements in Using a Translator
• Use approved Interpreter Services
OR
• Use the Interpreter Telephone

Using Appropriate Interpreter Services in Clinical Care
Speak with Charge Nurse for assistance
Call Operator to place call 1-800 number Client code/ID Request language

Directness in Clinical Encounters Americans value
directness: “Spit it out” “Say what’s on your mind”
Languages that depend on subtle contextual cues: Infer meaning Imply, but do not state,
the point
(Japanese, Arabic)

Directness and Subtlety
“Maybe” or “That would be difficult” is probably a polite “no”
Avoid yes/no questions Phrase your inquiry as a multiple choice
question

Nonverbal Communication
Facial expressions, body language, & tone of voice play a much greater role in cultures where people prefer indirect communication & talking around the issue.

Gestures and Facial Expressions
Another culturally influenced aspect of communication is the demonstration of emotion, such as joy, affection, anger, or upset.
Most Koreans, for instance, are taught that laughter & frequent smiling make a person appear unintelligent, so they prefer to wear a serious expression.
While Americans widen their eyes to show anger, Chinese people narrow theirs.
Vietnamese, conversely, consider anger a personal thing, not to be demonstrated publicly.

Smiling & laughter may be signs of embarrassment & confusion on the part of some Asians.
Talking with one’s hands is more common in southern Europe than in northern Europe.
A direct stare by an African American or Arab is not meant as a challenge to your authority, while dropped eyes may be a sign of respect from Latino or Asian patients & coworkers.

Gestures
Use gestures with care, as they can have negative meanings in other cultures.
Thumbs-up and the OK sign are obscene gestures in parts of South America & the Mediterranean.
Pointing with the index finger and beckoning with the hand as a “come here” sign are seen as rude in some cultures much as snapping one’s fingers at someone would be viewed in the United States.

American culture generally expects people to stand about an arm’s length apart when talking in a business situation.
Any closer is reserved for more intimate contact or seen as aggression.
In the Middle East, however, it is normal for people to stand close enough to feel each other’s breath on their faces.

Touch
Different rules about who can be touched & where.
A handshake is generally accepted as a standard greeting in business, yet the kind of handshake differs. North America = hearty grasp Mexico = softer hold Asia = soft handshake with the second
hand brought up under the first is a sign of friendship & warmth

Touch
Religious rules may apply to appropriate touch. Touching between men & women in public is not permitted by
some orthodox religions, so a handshake would not be appropriate.
Ideas about respect are conveyed through touch Touching the head, even tousling a child’s hair as an
affectionate gesture, would be considered offensive by many Asians.
If you need to touch someone for purposes of an examination, explain the purpose & procedure before you begin.

Topics Appropriate for Discussion
What is acceptable for nurse and patient to discuss? Many Asian groups regard feelings as too private to
be shared. Latinos generally appreciate inquiries about family
members, while most Arabs & Asians regard feelings as too personal to discuss in business situations.
In social conversations, Filipinos, Arabs, & Vietnamese might find it completely acceptable to ask the price you have paid for something or how much you earn, while most Americans would consider that behavior rude.

Inappropriate Conversation Topics
Even a seemingly innocuous comment on the weather is off limits in the Muslim world, where natural phenomena are viewed as Allah’s will, not to be judged by humans.
This points to another aspect that relates to privacy.
To many newcomers, Americans seem naively open. Discretion and purposeful communication help us judge when to converse and when to be silent.

Privacy
Discussing personal matters outside the family is seen as embarrassing by many cultures.
Thoughts, feelings, & problems are kept to oneself in most groups outside the dominant American culture.
Privacy boundaries may have implications when medical problems are exacerbated by personal or family problems.

Saving face…. In Asia, the Middle East, & to some extent Latin
America, one’s dignity must be preserved at all costs.
Death is preferred to loss of face in traditional Japanese culture, hence the suicide ritual, hara-kiri, as a final way to restore honor.
Any embarrassment can lead to loss of face, even in the dominant American culture.
To be criticized in front of others, publicly snubbed, or fired, would be humiliating in most any culture.
Seemingly harmless behaviors can be demeaning to some patients.

The Culturally Competent ClinicianAttitudes of the Culturally Competent Clinician
Understanding: Acknowledging that there can be differences between our Western and other cultures’ healthcare values and practices.
Empathy: Being sensitive to the feeling of being different.
Patience: Understanding the potential differences between our Western and other cultures’ concept of time and immediacy.
Ability: To laugh with oneself and others.
Trust: Investment in building a relationship with patients, which conveys a commitment to safeguard their well-being.

Non-Verbal Communication
All cultures have rules, often unspoken, about who touches
whom, when & where.

Nonverbal Communication(~65% of all communication)
Touch Facial expressions Eye movements Body posture

Modesty

Cultural Perspectives on Modesty
Patients may prefer clinicians of the same gender
May be taboo for males to examine or treat females (e.g., Middle Eastern groups)
In some Asian & Hispanic cultures, older adults may believe that hospital gowns cause disease by exposing them to cold drafts (related to yin/yang & hot/cold theories of disease)

Pain and Cultural Competence

Pain and Culture
Pain is an abstract concept which can be referred to as:
A personal private sensation
A stimulus that signals harm
A pattern of behavior to protect from harm

Pain Experience
Pain is a universal human experience, but pain reactions are unique to the individual and includes thoughts, feelings, reactions, expectations and past experiences associated with pain.
The experience of pain can also be described in physiologic, psychosocial, economic and spiritual contexts.

What is Included in a Pain Assessment Cross-Culturally?
Pain Expression: Verbal and non-verbal behaviors, including gestures and tone of voice.
Pain Language: Word(s) used to describe pain.
Language or other communication techniques such as pointing to site of pain.
Religious Beliefs: Meaning of pain or suffering.
Rituals and taboos associated with pain or pain treatment.

Pain Assessment and Cultural Factors Social Roles:Ethnic identity and degree of
acculturation: such as primary language used, identification of social support networks.
Family relationships, consider the role(s) the individual has within the family, extended family presence and role in community (such as employment).
Gender and Age Influences. Perception of the healthcare
system:Trust vs. suspicion. Use of traditional/layremedies.Past experience with the healthcare system.

Pain Treatment and Cultural Factors Attitudes and fears about pain
medications or other interventions may impact the patient and/or family compliance with a pain treatment plan.
Physiologic response to medications has race and age variations. For example, body composition of fat and serum protein in the elderly may alter distribution and absorption of medications.
Also elicit patient beliefs about: Meaning of pain or illness. Expectations of healthcare
providers. Therapeutic goals.

Barriers
Typical barriers to a cultural sensitive pain assessment and treatment by healthcare providers include: Stereotyping. Lack of empathy. Ethnocentrism. Language. Experience or expertise of practitioner and time
constraints.

National Institutes of Health
Facilitates research and evaluation of complementary and alternative practices
Provides information about a variety of methods

What is complementary and alternative medicine?
Includes a broad range of healing philosophies, approaches & therapies
A therapy is called complementary when it is used in addition to conventional biomedical/scientific treatments
An alternative therapy is used instead of conventional biomedical/scientific treatments.
Conventional refers to those widely accepted & practiced by the mainstream medical community

Complementary &
AlternativeTherapies
MassageTherapy
Aroma-therapy
Ayurveda
Chiropractic Therapeutic
Touch
Reflexology
Acupuncture
Shamanism
MusicTherapy
Hypno-therapy
ArtTherapy

Complementary Therapies: What is the Clinical Goal?
Gain the patient’s trust so he/she will tell you the truth about alternative and complementary practices used to treat pain or other symptoms.

What Does the Clinician do with a Patient Using Complementary Therapies?
Check for drug interactions with prescription or over-the-counter medications
Assess for harmful side effects Discourage over-reliance on traditional
healing if it delays necessary biomedical treatment (for example, conditions for which an antibiotic is needed)

Meta-Communicative Cultural Competence
Pay attention to body language, facial expressions & other behavioral cues; much information may be found in what is not said
Avoid yes/no questions; ask open ended questions or ones that give multiple choices; remember that a nod or yes may mean: “Yes, I heard” rather than “Yes, I understand” or “Yes, I agree”

Meta-Communicative Cultural Competence
Consider that smiles & laughter may indicate discomfort or embarrassment; investigate to identify what is causing the difficulty or confusion
Make formal introductions using titles (Mr., Mrs., Ms., Dr.) & surnames; let the individual take the lead in getting more familiar

Meta-Communicative Cultural Competence
Greet patients with “Good Morning” or “Good Afternoon” and when possible, in their language
If there is a language barrier, assume confusion; watch for tangible signs of understanding, such as taking out a driver’s license or social security card to get a required number

Meta-Communicative Cultural Competence
Take your cue from the other person regarding formality, distance, and touch
Question your assumptions about the other person’s behavior; expressions & gestures may not mean what you think; consider what a particular behavior may mean from the other person’s point of view
Explain the reasons for all information you request or directions you give.

Meta-Communicative Cultural Competence
Use a soft, gentle tone and maintain an even temperament
Spend time cultivating relationships by getting to know patients & coworkers
Be open to including patients’ family members in discussions & meetings with patients
Consider the best way to show respect, perhaps by addressing the ”head’ of the family or group first

Meta-Communicative Cultural Competence
Use pictures & diagrams where appropriate;
Pay attention to subtle cues that may tell you an individual’s dignity has been wounded
Recognize that differences in time consciousness may be cultural & not a sign of laziness or resistance

Main Points: Cultural Competence

• By being open-minded and respectful toward their beliefs, values, & practices, you can help patients feel more comfortable.
• Factors that may differ from patient to patient include ethnic, religious, and occupational factors.
• Some people belong to more than one ethnic group, as well as cultural groups, and other people have fewer group identities.

• Importance of religion can vary from person to person. For example, some people keep many daily traditions, such as eating certain foods.
• Others keep traditions only on special occasions, or not at all.
• For many different reasons, religious, ethnic, health, personal preference, etc., a person may eat or avoid certain foods at certain times, or not eat some foods at all.

• Different cultures have different ideas about how to express & respond to pain.
• Some cultures value bearing pain silently, while others expect expressiveness.
• Different cultures have different views about when to seek professional medical help, treat oneself, or be treated by a family member or traditional healer.

Thank you for your time!
Related Documents