“DREAM IS NOT WHAT YOU SEE DURING SLEEP, IT IS WHAT DON’T LET YOU SLEEP.”

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
“DREAM IS NOT WHAT YOU SEE
DURING SLEEP, IT IS WHAT DON’T
LET YOU SLEEP.”
CORTICOSTEROIDS
Presented by:
Dr. Ankit Patel
Contents History
Physiology
- Pituitary gland
- Adrenal gland
Regulation of Cortisol Release
Glucocorticoids and mineralocorticoids
- Pharmacological Actions
Classification of glucocorticoids and mineralocorticoids
Mechanism of Action
Pharmacokinetics
Therapeutic use
Use of corticosteroids in endodontics
Drug interaction
Adverse reactions
Contraindications
Conclusion
References
History
Addison (1849) first appreciated the clinical importance of the adrenal glands
and described fatal outcomes in patients with adrenal destruction during a
presentation to the South London Medical Society.
Brown sequard (1856) demonstrated that bilateral adrenalectomy was fatal in
laboratory animals. It was later shown that the adrenal cortex, rather than the
medulla, was essential for survival in these experiments. Subsequently, Tate
and colleagues isolated and characterized a distinct corticosteroid aldosterone,
that had potent effects on fluid and electrolyte balance (and therefore was
termed mineralocorticoid). During the decades following 1930, there was an
intensive search for the active principles that could account for the essential
role of the adrenal gland.
Reichstein and Von Euw (1937) prepared dexamethasone synthetically and
demonstrated its presence in adrenal glands.
Hench and Co-workers (1949) reported the effectiveness of cortisone and
corticotropin in the treatment of rheumatoid arthritis.
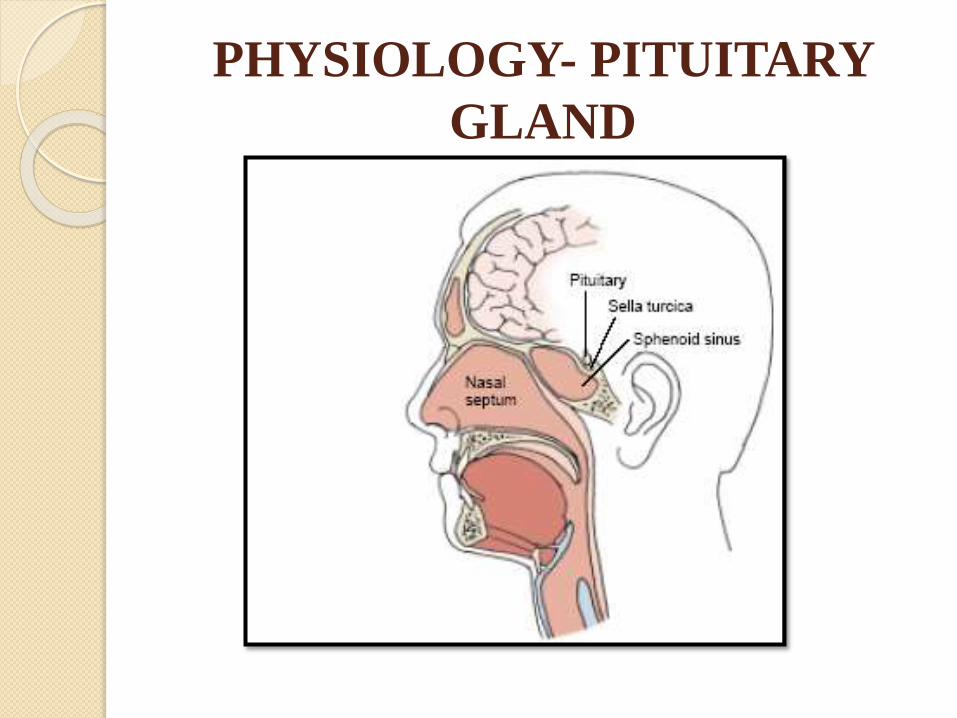
PHYSIOLOGY- PITUITARY
GLAND
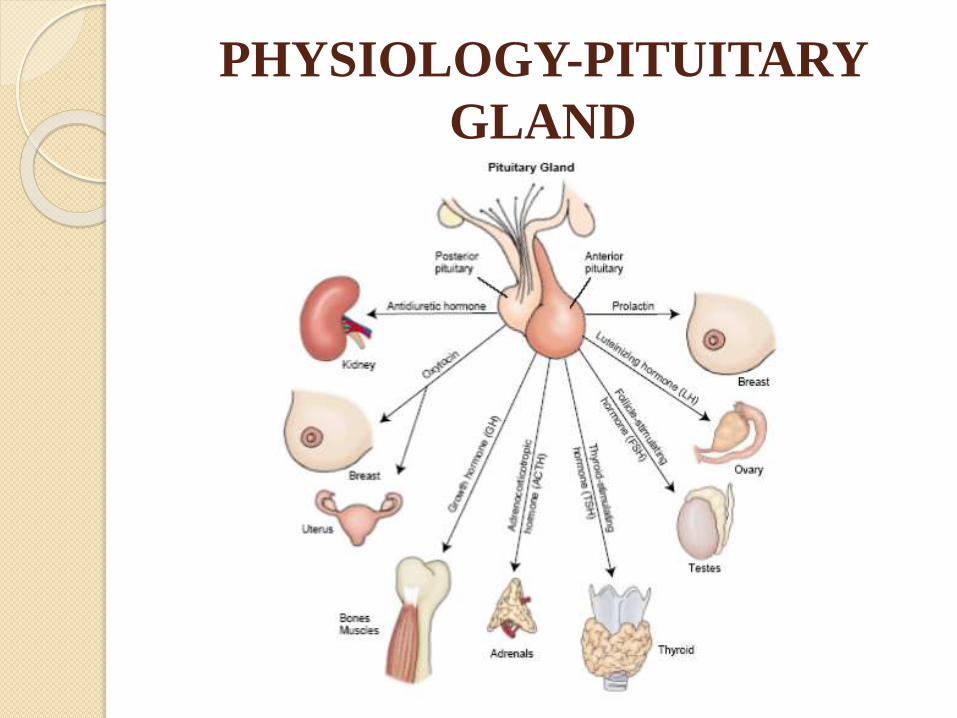
PHYSIOLOGY-PITUITARY
GLAND
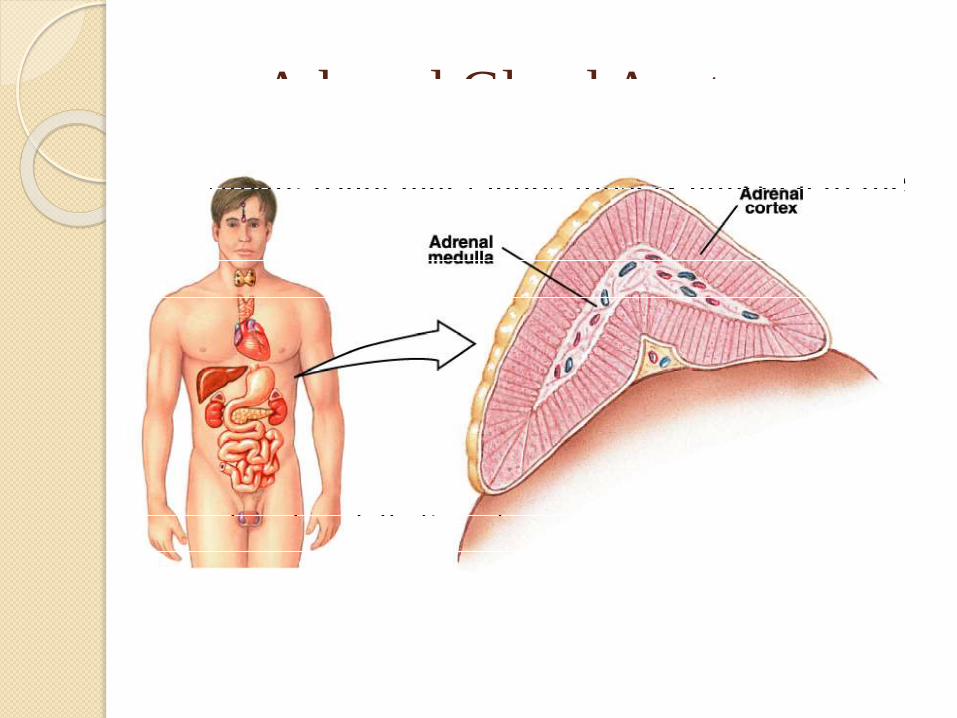
Adrenal Gland Anatomy
• Small, triangular glands loosely attached to the
superior aspects of the kidneys.
• Divided into two morphologically and distinct
regions
- adrenal cortex (outer)
- adrenal medulla (inner)
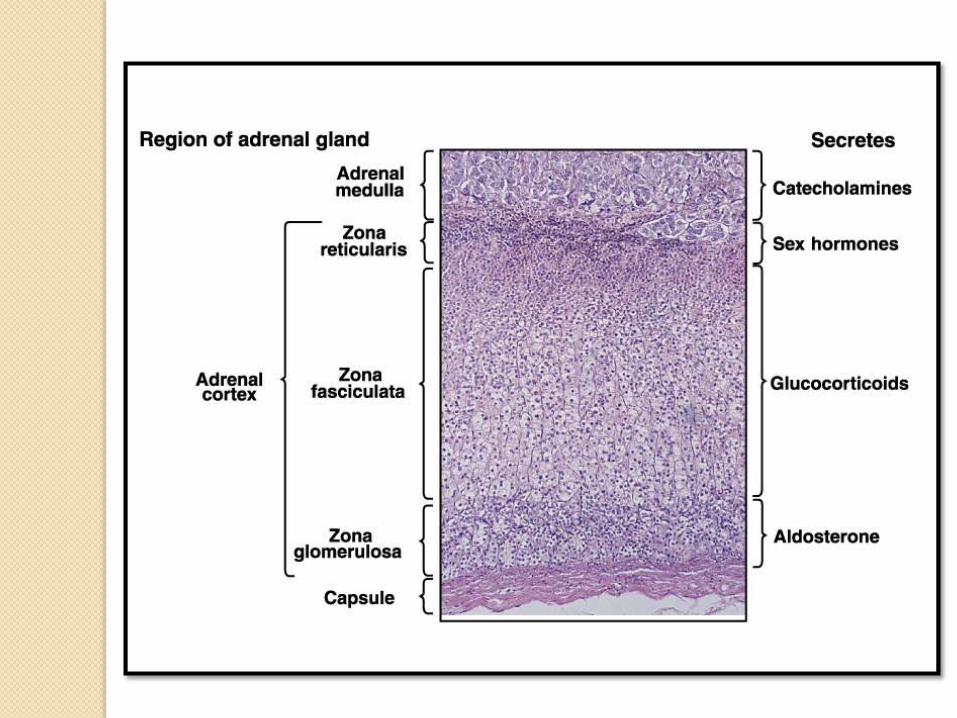
Adrenal Cortex
•Hormones produced by the adrenal cortex are referred to
as corticosteroids.
•These comprise mineralocorticoids, glucocorticoids and
androgens.
•The cortex is divided into three regions:
• zona glomerulosa
• zona fasciculata
• zona reticularis

Zona Glomerulosa
Outermost zone – just below the adrenal capsule
Secretes mineralocorticoids.
Mineralocorticoids are aptly termed as they are
involved in regulation of electrolytes in
extracellular fluid.
The naturally synthesized mineralocorticoid of
most importance is aldosterone.
Zona Fasciculata
Middle zone – between the glomerulosa and reticularis
Primary secretion is glucocorticoids.
Glucocorticoids, as the term implies, are involved the
increasing of blood glucose levels. However they have
additional effects in protein and fat metabolism.
The naturally synthesized glucocorticoid of most
importance is cortisol.
Zona Reticularis
Innermost zone – between the fasciculata and medulla
Primary secretion is androgens.
Androgenic hormones exhibit approximately the same effects as the male sex hormone –testosterone.
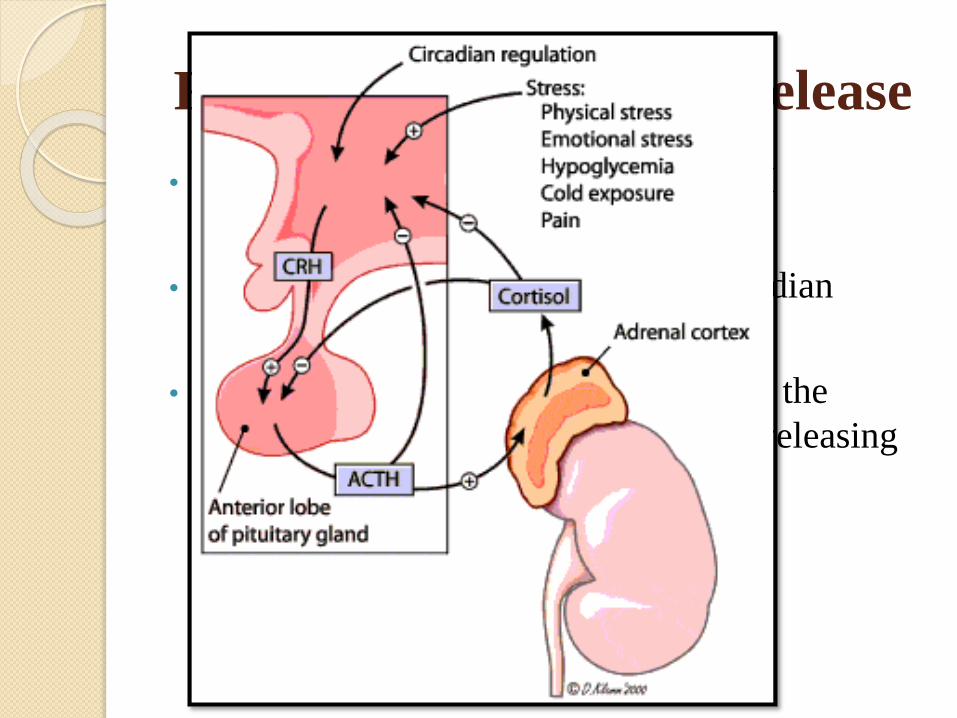
Regulation of Cortisol Release
• Cortisol release is regulated by ACTH
• Release follows a daily pattern - circadian
• Negative feedback by cortisol inhibits the
secretion of ACTH and Corticotropin releasing
hormone (CRH).
Regulation of Cortisol Release
The important glucocorticoid secreted in human
being is hydrocortisone (10 mg/ day)
Enhanced release can be caused by:
physical trauma
infection
extreme heat and cold
exercise to the point of exhaustion
extreme mental anxiety
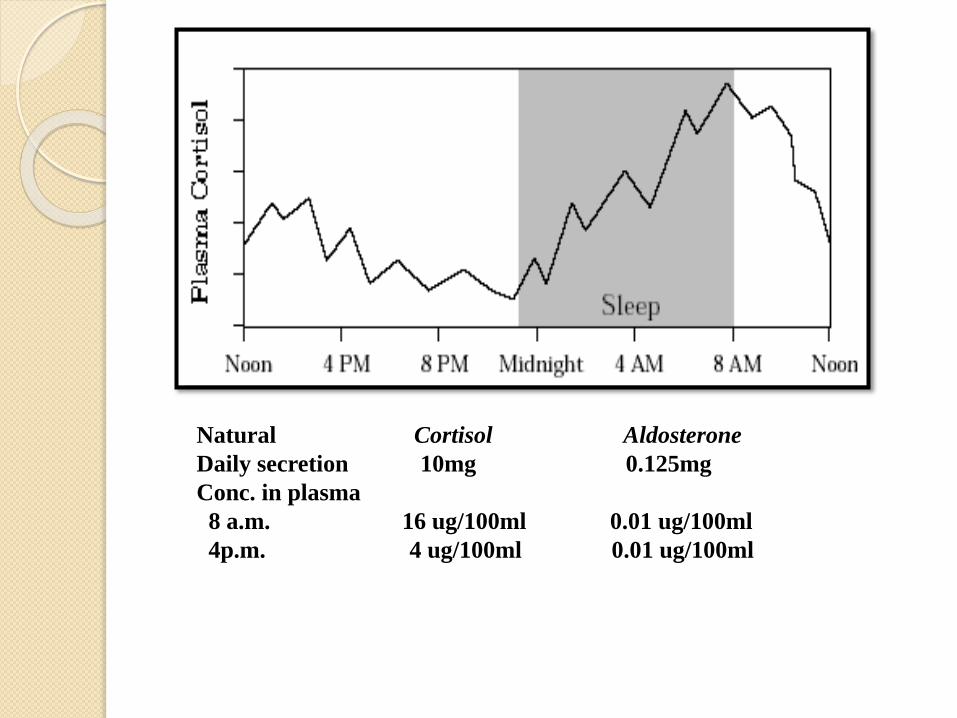
Natural Cortisol Aldosterone
Daily secretion 10mg 0.125mg
Conc. in plasma
8 a.m. 16 ug/100ml 0.01 ug/100ml
4p.m. 4 ug/100ml 0.01 ug/100ml
Regulation of Cortisol Release
• 95 % is bound to corticosteroid binding
globulin (CBG or transcortin).
• Free cortisol is only 1 µ gm per 100 ml.
Pharmacological Actions1. Carbohydrate
2. Protein
3. Lipid
4. Electrolyte & water(mineralocorticoid action)
5. CVS
6. Skeletal Muscle
7. CNS
8. Stomach
9. Blood
10. Anti-inflammatory
11. Immunosuppressant
12. Respiratory system
13. Growth & Cell Division
14. Calcium metabolism
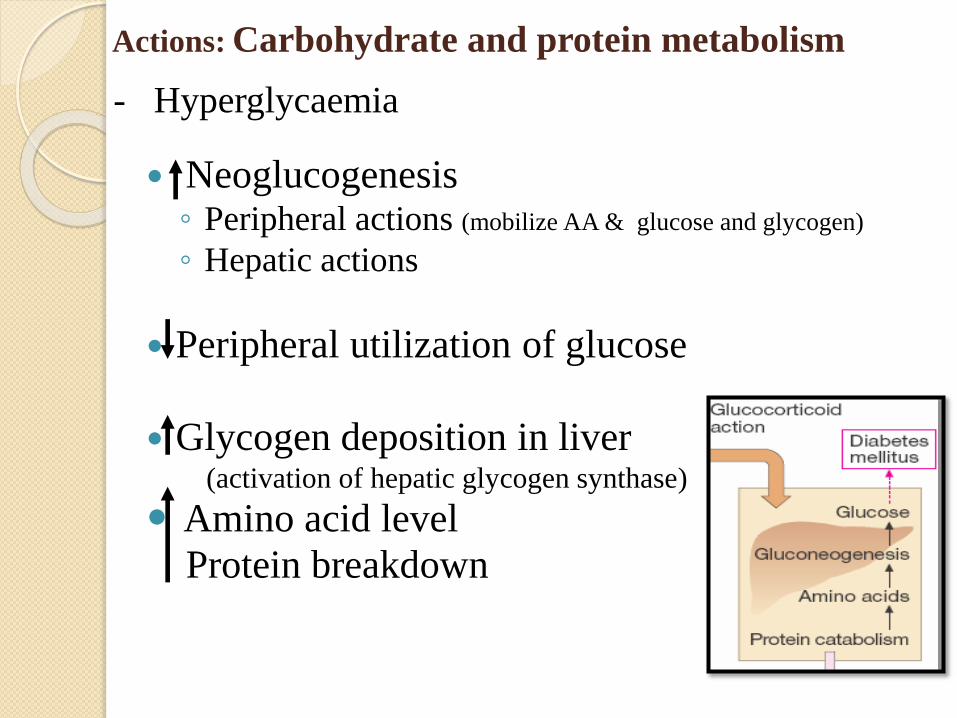
Actions: Carbohydrate and protein metabolism
Neoglucogenesis◦ Peripheral actions (mobilize AA & glucose and glycogen)
◦ Hepatic actions
Peripheral utilization of glucose
Glycogen deposition in liver(activation of hepatic glycogen synthase)
Amino acid level
Protein breakdown
- Hyperglycaemia
Permissive role in nature: promote lipolysis due
to glucagon, GH, Adr and throxine.
Redistribution of Fat over neck, face, and
shoulder-moon face, fish mouth, buffalo hump.
Increases sensitivity of adipocytes to insulin.
Actions: Lipid metabolism
Actions: Electrolyte and water balance
Aldosterone is more important
Act on D.T. & C.D. of kidney
◦ Na+ reabsorption
◦ Urinary excretion of K+ and H+
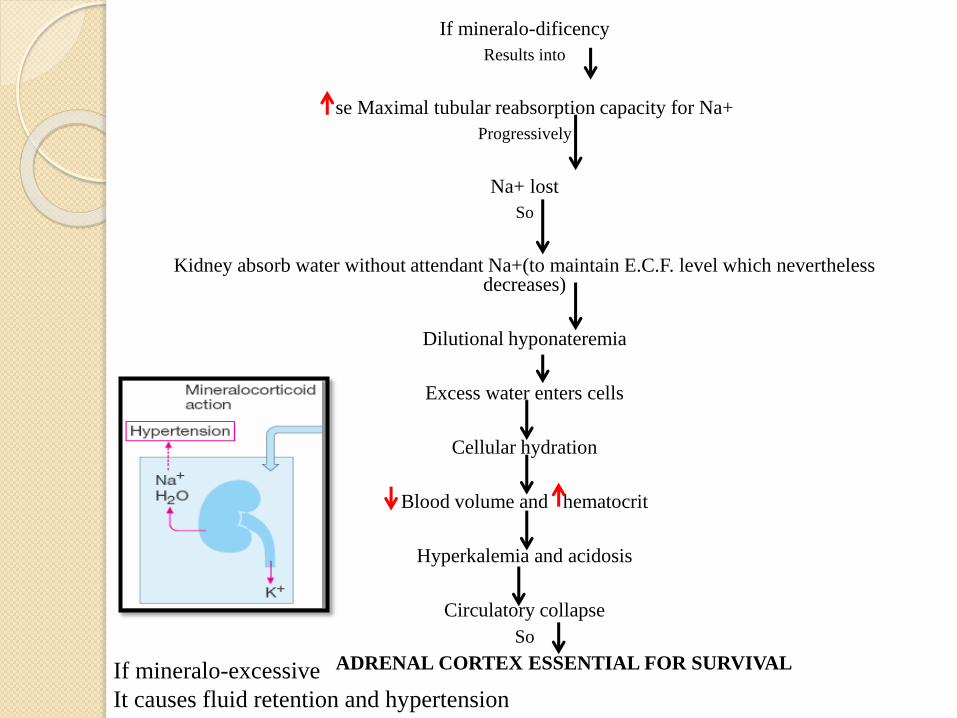
If mineralo-dificency
Results into
se Maximal tubular reabsorption capacity for Na+
Progressively
Na+ lost
So
Kidney absorb water without attendant Na+(to maintain E.C.F. level which nevertheless decreases)
Dilutional hyponateremia
Excess water enters cells
Cellular hydration
Blood volume and hematocrit
Hyperkalemia and acidosis
Circulatory collapse
So
ADRENAL CORTEX ESSENTIAL FOR SURVIVALIf mineralo-excessive
It causes fluid retention and hypertension
Restrict capillary permeability
Maintain tone of arterioles
Mineralocorticoid-induced Na+ retention
ECF
B.P.
Permissive action
α & βreceptors
Vascular reactivity
Actions: Cardiovascular system
Potentiates the pressor response of blood vessels to
the action of catecholamines
On Skeletal muscle has permissive action:
Weakness occur in both cases
Addison’s disease(hypocorticism)
Work capacity, weakness & fatigue
circulation
Addison's disease: weakness & fatigue is due to inadequacy of circulatory system to respond to stress of increased muscular activity.
Primary aldosteronism(hypercorticism)
Weakness
Hypokalemia
Excessive corticoids action causes muscle wasting and myopathy leads to weakness
Actions: Skeletal Muscles
Needed for maintaining the normal function of Skeletal muscle
Direct:
◦ Mood elevation
◦ Behavior –incresead Euphoria, nervousness, irritabilility
◦ Brain excitability
Indirect:
◦ maintain glucose, circulation and electrolyte balance
Actions: CNS ( Central nervous system)
Aggravate peptic ulcer. May be due to
Gastric acid & pepsin secretion
Actions: Stomach
RBC: Hb & RBC content
WBC: Lymphocytes, eosinophils,
monocytes, basophils
Actions: Blood
Recruitment of WBC and monocytes macrophage
into affected area & elaboration of chemotactic
substances
Lipocortin
TNF from phagocytic cells
IL1 from monocyte-macrophage
Formation of Plasminogen Activator
Expression of cyclo-oxygenase II
Actions: Anti-inflammatory
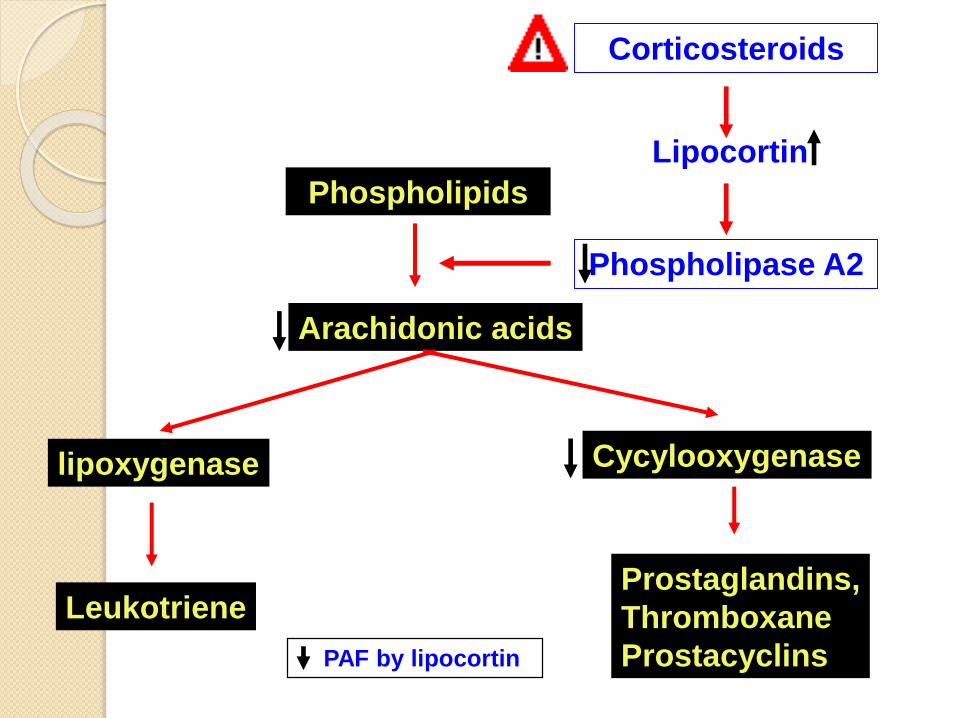
Phospholipids
Arachidonic acids
lipoxygenase Cycylooxygenase
LeukotrieneProstaglandins,
Thromboxane
Prostacyclins
Phospholipase A2
Lipocortin
Corticosteroids
PAF by lipocortin
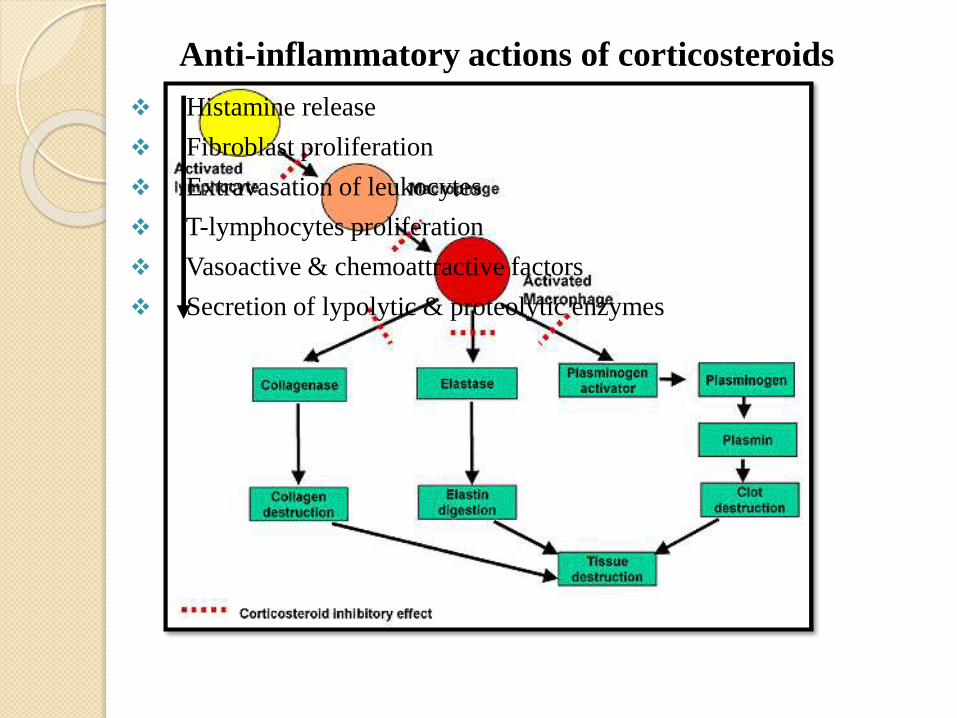
Anti-inflammatory actions of corticosteroids
Histamine release
Fibroblast proliferation
Extravasation of leukocytes
T-lymphocytes proliferation
Vasoactive & chemoattractive factors
Secretion of lypolytic & proteolytic enzymes
Immunosuppressive & anti-allergic actions
Suppresses all types of hypersensitivity & allergic
phenomenon
At High dose: Interfere with all steps of immunological
response
Causes greater suppression of CMI (graft rejection & delayed
hypersensitivity)
Transplant rejection: Antigen expression from grafted tissues, delay
revascularization, sensitization of T lymphocytes etc.
Inhibit cell division or synthesis of DNA
Delay the process of healing
Retard the growth of children
Actions: Growth & Cell division
Intestinal absorption
Renal excretion
Excessive loss of calcium from spongy bones (e.g.,
vertebrae, ribs etc)
Ca2+ absorption excretion
Total body calcium store
Actions: Calcium metabolism
Not bronchodilators
They reduce the bronchial hyper-reactivity and increase the peak
expiratory flow rate in asthmatic patients.
They are not effective during an acute attack or in status
asthmaticus.
Most potent and most effective anti-inflammatory
Effects not seen immediately (delay 6 or more hrs)
Inhaled corticosteroids are used for long term control
Before birth: Induce surfactant synthesis in fetal lung. Useful in
Respiratory Distress Syndrome
Actions: Respiratory system
Classification of glucocorticoids
and mineralocorticoids
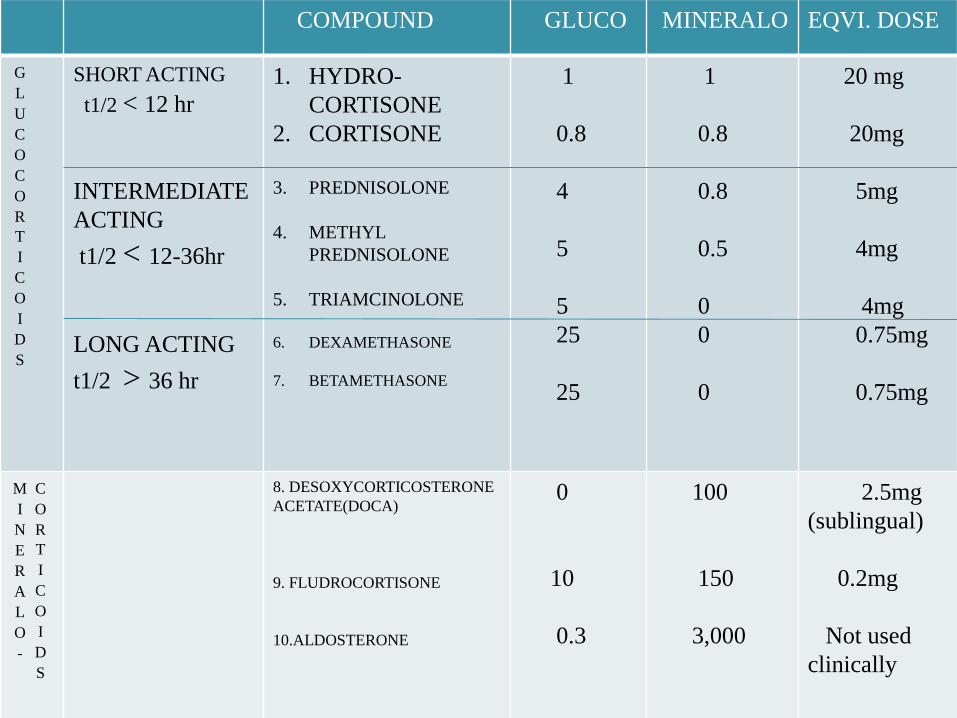
COMPOUND GLUCO MINERALO EQVI. DOSE
G
L
U
C
O
C
O
R
T
I
C
O
I
D
S
SHORT ACTING
t1/2 < 12 hr
INTERMEDIATE
ACTING
t1/2 < 12-36hr
LONG ACTING
t1/2 > 36 hr
1. HYDRO-
CORTISONE
2. CORTISONE
3. PREDNISOLONE
4. METHYL
PREDNISOLONE
5. TRIAMCINOLONE
6. DEXAMETHASONE
7. BETAMETHASONE
1
0.8
4
5
5
25
25
1
0.8
0.8
0.5
0
0
0
20 mg
20mg
5mg
4mg
4mg
0.75mg
0.75mg
M
I
N
E
R
A
L
O
-
C
O
R
T
I
C
O
I
D
S
8. DESOXYCORTICOSTERONE
ACETATE(DOCA)
9. FLUDROCORTISONE
10.ALDOSTERONE
0
10
0.3
100
150
3,000
2.5mg
(sublingual)
0.2mg
Not used
clinically
Mechanism of Action
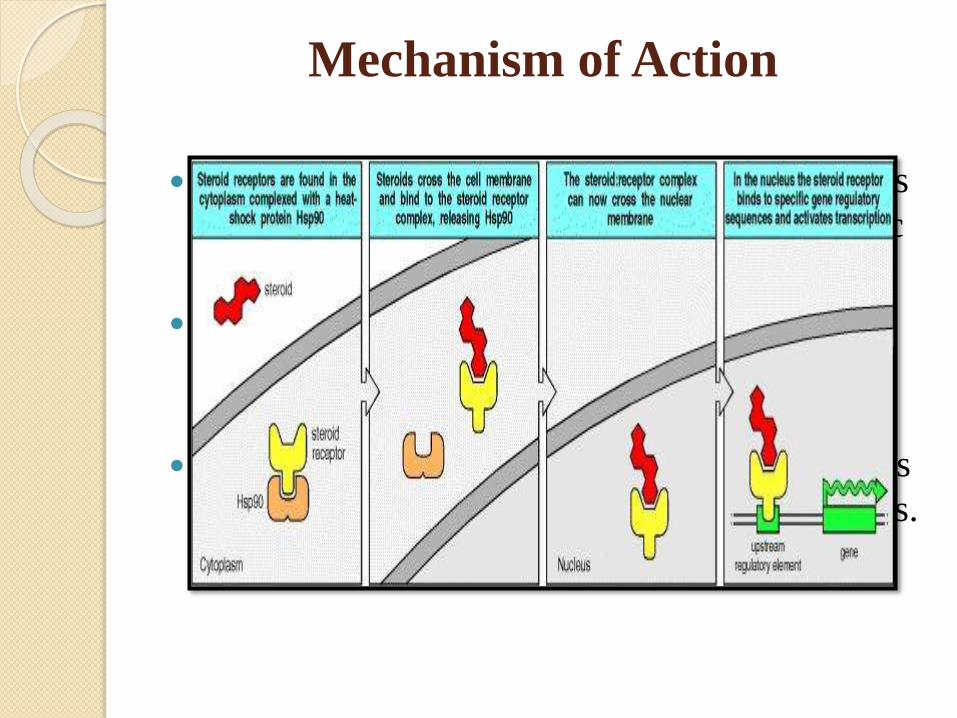
Mechanism of Action
Most of the established pharmacological effects
of glucocorticoids are mediated by cytoplasmic
glucocorticoid receptors.
After binding to the receptor, the steroid-
receptor complex binds to chromatin and
stimulate the formation of mRNA.
The mRNA stimulates the synthesis of enzymes
which produce various pharmacological actions.
Pharmacokinetics
ABSORPTION
Can be given by oral, parenteral and topical route.
Oral bioavailability of synthetic corticosteroids is high.
Hydrocortisone after oral administration undergoes extensive first pass metabolism in liver. So preferd route is parenteral.
Systemic absorption is by Topical/local e.g. Skin, synovial space, conjuctiva, intranasal, enema, inhalation.
DISTRIBUTION
90% bound to plasma protein, mostly to a specific corticosteroid binding globulin(globulinor Transcortin) and albumin.
METABOLISM: By reduction or conjugation
REDUCTION
4,5 bond,3ketone tetrahydrocortisol
( liver)
CONJUGATION
Sulfate or glucuronide (liver & kidney)
Excreted in urine
The synthetic derivatives are metabolised slowly and have longer duration of action.
Therapeutic uses:Endocrine Disorders• Replacement therapy
Acute adrenal insufficency: (emergency)
Hydrocortisone(100 mg IV q 6-8 h)/dexamethasone(4-10 mg IV q 6-8 h.)are given IV first as bolus injection and then infusion with NS and glucose solution. Inj.Hydrocortisone 100 mg every 4-6 hrs, Tab.Hydrocortisone 20mg in the morning, Tab.Hydrocortisone 10 mg in the evening, I.V. fluid.
Chronic adrenal insufficiency (addison’s disease)
Hydrocortisone given orally along with adequate salt and water allowance. Few pt. require mineralocorticoid: fludrocortisone/DOCA. Tab.Hydrocortisone 20mg in the morning, Tab.Hydrocortisone 10 mg in the evening, Fludrocortisone 0.05 to 0.2 mg/day oral.
Congenital adrenal hyperplasia (adrenogenital syndrome)
◦ Deficiency of steroidogenic enzymes mostly 21-hydroxylase. As a result synthesis of hydrocortisone and aldosterone suffers.
◦ Hydrocortisone 0.6mg/kg daily for suppression of pituitary.
◦ If salt wasting persists-fludrocortisone 10-20ug/kg daily.
Pharmacotherapy for nonendocrine diseases
General principles must be observed
1. Single dose (even excessive) is not harmful: can be used to
tide over mortal crisis even when benefits is not certain.
2. Short courses (even high doses) are not likely to be
harmful in the absence of contraindications: starting dose
can be high in severe illness.
3. Long term usesis potentially hazardous: keep the dose
minimum, which is found by trial and error; even partial
relief may have to be tolerated.
4. No abrupt withdrawal after a corticoids has been given >2-
3 weeks: may precipitate adrenal insufficiency.
5. Infection, severe trauma or any stress during corticoid
therapy-increase the dose.
Arthrides:
Rheumatic arthritis-Oral Prednisolone (5 to 10mg)/day, IA Triamcinolone acetonide 5-20mg
Osteoarthritis- IA Triamcinolone acetonide 5-20mg
Rheumatic fever
Gout
Collagen diseases: SLE, polyarthrits nodosa, dermatomyosotis, nephroticsyndrome, glomerulonephritis and related diseases need corticosteroids may be life saving. Prednisolone 1mg/Kg start; gradually reduce the dose
Severe allergic reactions
Autoimmune diseases: autoimmune hemolytic anaemia, thrombocytopenia, active hepatitis respond to corticoids. Its also in severe cases of myasthenia gravis along with neostigmine.
Bronchial asthma: used either for-status asthmaticus, severe chronic asthma. Nowadays corticoids are used for mid asthma and short couses of oral steroids may be used to tide over acute excerbations.
Other lung diseases: corticoids benefits aspiration pneumonia and
pulmonary oedema from drowning. Given during late pregnancy corticoids
accelerate lung maturation in the foetus and prevent respiratory distress
syndrome at birth. Such therapy may be undertaken if premature delivery
is contemplated.
Infective diseases: indicated in serious infection to tideover crisis to prevent
complications. They are indicated in conditions like severe forms of TB,
severe lepra reaction, certain forms of bacterial meningitis and
pneumocystis carinii pneumonia with hypoxia in AIDS
Eye diseases-diseases-Outer eye & anterior segment: local application,
Posterior segment: systemic use, Caution: bacterial, viral & fungal
conjunctivitis.
Skin diseases-Pemphigus: Life saving therapy is steroids. Eczema,
dermatitis & psoriasis: respond well
Intestinal diseases
Cerebral oedema-Questionable value in cerebral edema following trauma, cerebrovascular edema. Valuable in edema associated with neoplasm and parasites
Malignancies-Part of multi drug regimens for acute lymphatic leukaemia (children), chronic lymphatic leukaemia (adult).
Open transplantation and skin allograft
Shock: IV corticoids are given as a desperate measure in septicaemic shock.
To test adrenal-pituitary axis function: dexamethasone suppresses adrenal-pituitary axis at doses which do not contribute to steroid metabolites in urine-responsiveness of the axis can be tested by measuring daily urine steroid metabolite excretion.
Organ transplantation
Bell’s palsy
Thrombocytopenia
Myasthenia gravis
Spinal cord injury
Sarcoidosis
Non-endocrine diseases
- Miscellaneous
Use in endodontics
Corticosteroids in dentistry,are used primarily to decrease post-operative edema and manage oral inflammatory diseases.
Post treatment flare-ups after endodontic treatment can be attributed to the inflammation,infection or both in periradicular tissues.
Glucocorticosteroids are known to reduce the acute inflammatory response by suppressing vasodilatation,migration of PMN’s leukocytes,andphagocytosis.
Intracanal placement with 2.5% steroid and saline---study conducted—resulted in significant reduction of incidence of post-operative pain in teeth with vital pulp
Other study with Ledermix,Formocresol,or calcium hydroxide as intracanal medicament resulted in steroid showing significant effects in reducing post-operative pain.
Ledermix: Schroeder developed the material
Triamcinolone Acetonide and Demethylchlortetracycline
30% triamcinilone is released in first 24 hrs and remaining 70% over a period of 14 weeks
Available as 2 forms
1.Water soluble ‘cream’
2. Rapidly hardening ‘cement’
46
A. Open-cavity pulpitis
47
B: Closed-cavity pulpitis
48
Krasner P, Jackson E (1986)reported the use of orally
administered dexamethasone alone for the management
of pain following routine endodontic instrumentation.
Fachin EVF, Zaki AE (1991) conducted a study to
histologically investigate steroid effects on the dental
pulp. The results showed that topical application of
corticosteroids as an intracanal medicament reduced
inflammatory changes in the pulp as compared with
controls.
Erisen R, Yucel T, Kucukay S et al (1989) reported a
case of hypoesthesia caused by endomethasone
overflowing into the mandibular canal. Endomethasone
contains hydrocortisone, which can contribute to its
toxicity.
USES IN ORAL MEDICINE
Lichen planus
Oral submucous fibrosis
Aphthous stomatitis
Pemphigus
Bell’s palsy
Mucocele
Psoriasis
Erythema multiforme
Herpes virus infection
Central giant cell granuloma
Temporomandibular joint pain and dysfunction
Chronic ulcerative stomatitis
Pystomatitis vegetans
Giant haemangioma
Meischer’s granulomatous cheilitis
USES IN ORAL SURGERY :
Third molar surgery
Reconstructive oral surgery
Preprosthetic surgery
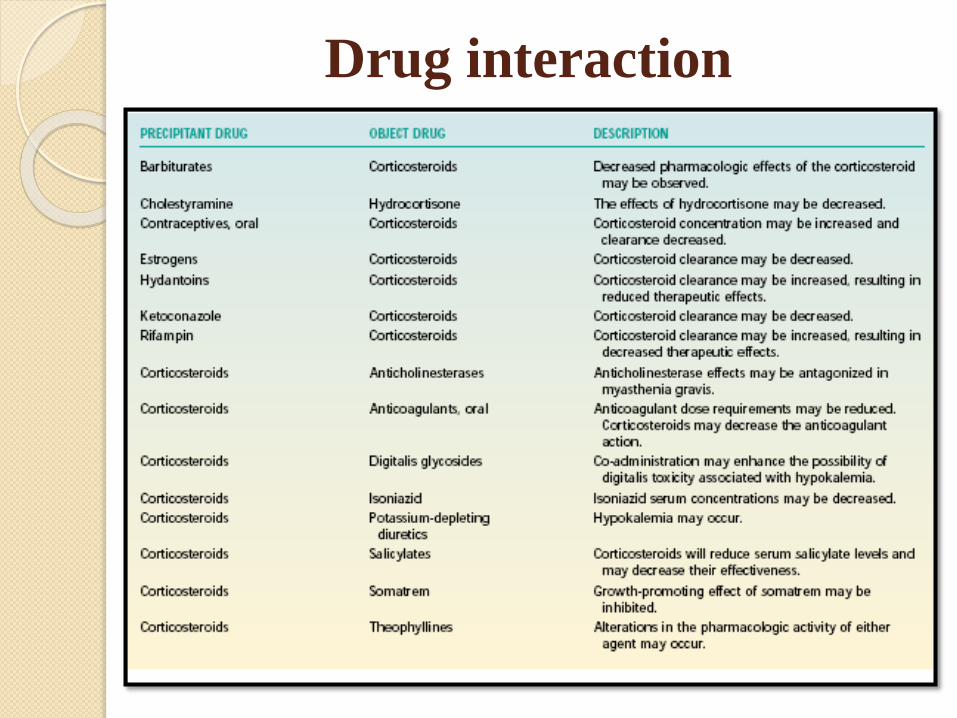
Drug interaction
Adverse reactions
Minerlocorticoid: sodium and water retention, edema, hypokalemia alkalosis
and a progrssive rise in BP(rarely).
Glucocorticoid
Cushing’s disease
Fragile skin, purple striae
Hyperglycaemia
Muscular weakness
Susceptibility to infection
Delayed wound healing
Peptic ulceration
Osteoporosis
Posterior subcapsular cataract
Glaucoma
Growth retardation
Fetal abnormalities
Psychiatric disturbances
Suppression of HPA axis
Contraindications
Infections
Hypertension with CCF
Psychosis
Peptic ulcer
Diabetes mellitus
Osteoporosis
Glaucoma
Pregnancy : (prednisolone preferred)
TB
Epilepsy
Renal failure
Precautions during therapy
Following examinations of the patient to be
done before, during and after steroid therapy
Body weight
X-ray of spine
Blood glucose
Examination of the eye
B.P.
TOPICAL CORTICOSTEROIDS
Examples of topical corticosteroids
include:Betamethasone dipropionate (diprosone),
Fluocinolone acetonide (flurosyn), Hydrocortisone (cort-
dome), Triamcinolone acetate (Aristocort).
ACTIONS AND USES
Topical corticosteroids exert localized anti-inflammatory
activity.
When applied to inflamed skin, they reduce itching,
redness, and swelling.
These drugs are useful in treating skin disorders, such as
psoriasis, dermatitis, rashes, eczema, insect bite
reactions, and first and second-degree burns, including
sunburns.
Adverse reactions
Localized reactions may include burning,
itching, irritation, redness, dryness of the
skin, and secondary infection.
CONTRAINDICATIONS, PRECAUTIONS,
AND INTERACTIONS
The topical corticosteroids are contraindicated
in patients with known hypersensitivity to the
drug and for ophthalmic use (may cause steroid-
induced glaucoma or cataracts).
The topical corticosteroids are used cautiously
during pregnancy and lactation.
There are no significant interactions when
administered as directed.
Conclusion
No doubt these are called as wonder drugs or
magic drugs which are used in life threatning
conditions can cost the life when not used
properly.
References
Pharmacology and Pharmacotherapeutics-
R.S. Satoskar
Textbook of pharmacology- K.D. Thripati.
Pharmacology for dentistry-Dr Surendra
Singh
Introductory Clinical Pharmacology- Roach
Related Documents











