9/13/2012 1 Comprehensive Stroke Systems: The Saint Luke’s Experience Debbie Summers MSN, ACNS-BC, CNRN, CCRN, FAHA Disclosures Comprehensive Stroke Systems: The Saint Luke’s Experience • Debbie Summers, MSN, APRN-BC – Speakers Bureau • Genentech, Inc

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

9/13/2012
1
Comprehensive Stroke Systems: The Saint Luke’s
Experience
Debbie Summers MSN, ACNS-BC, CNRN, CCRN, FAHA
Disclosures
Comprehensive Stroke Systems: The Saint Luke’s Experience
• Debbie Summers, MSN, APRN-BC– Speakers Bureau
• Genentech, Inc

9/13/2012
2
Kansas City
Saint Luke’s Hospital System Non Profit
• 10 Hospitals– 4 Metro
• SLH – 590 (PSC –CSC)
• SLH East – 174 (PSC)
• SLH South – 125 (PSC)
• SLH North – 150
– 2 Community – 2 Critical Access – 1 Free standing
rehabilitation – 1 Behavioral Health

9/13/2012
3
Objective
• At the conclusion of your presentation, participants should be able to understand the stroke systems of care framework.
1
St. Luke’s Neuroscience Institute
2004 – Joint Commission
Primary Stroke Certified
2011 Population• 678
Ischemic• 108 ICH• 80 SAH• 96 TIA
9/13/2012
4
St. Luke’s Neuroscience Institute
1992-03 Stroke program organize
2001 formally branded MABSI
2007 Re-branded as SLBSI
2012 Re-branded as SLNI
Organized around Centers of Excellence
Who We AreMission
To improve the health of the people of Kansas City and the surrounding region by advancing neuroscience research and education, pioneering emerging technology and therapy while sustaining cost effective clinical excellence in the treatment, prevention and rehabilitation of the nervous system and spine.
Vision
To be the regional leader in providing comprehensive integrated care and services for people with conditions of the nervous system and spine and to be nationally recognized as a “Best Place to Get and Give Neurological Care.”

9/13/2012
5
Media Recognition
The New York Times
48 Hours
Discovery Channel
Newsweek
Business Week
ABC World News
Progression from PSC - CSC
Clinical Trials
1994 IV tPANINDS Clinical
Trials
2002 IMS IV to IA
2002 MERCIMechanical
Process Structure
Flow of Patient care
Evaluation & management
Ease of Access
Capacity – No Diversion
Professional outreach
Clinical Tools
Science Based Evidence
Guidelines
Transport Protocols
Equipment
Point of Care
Radiology
Future -Institute
Data
Access Data Base
Tracking Treatment
90 day
Reporting Data
People
No Neurology or
Neurosurgery Residents
APN’s
CNN
9/13/2012
6
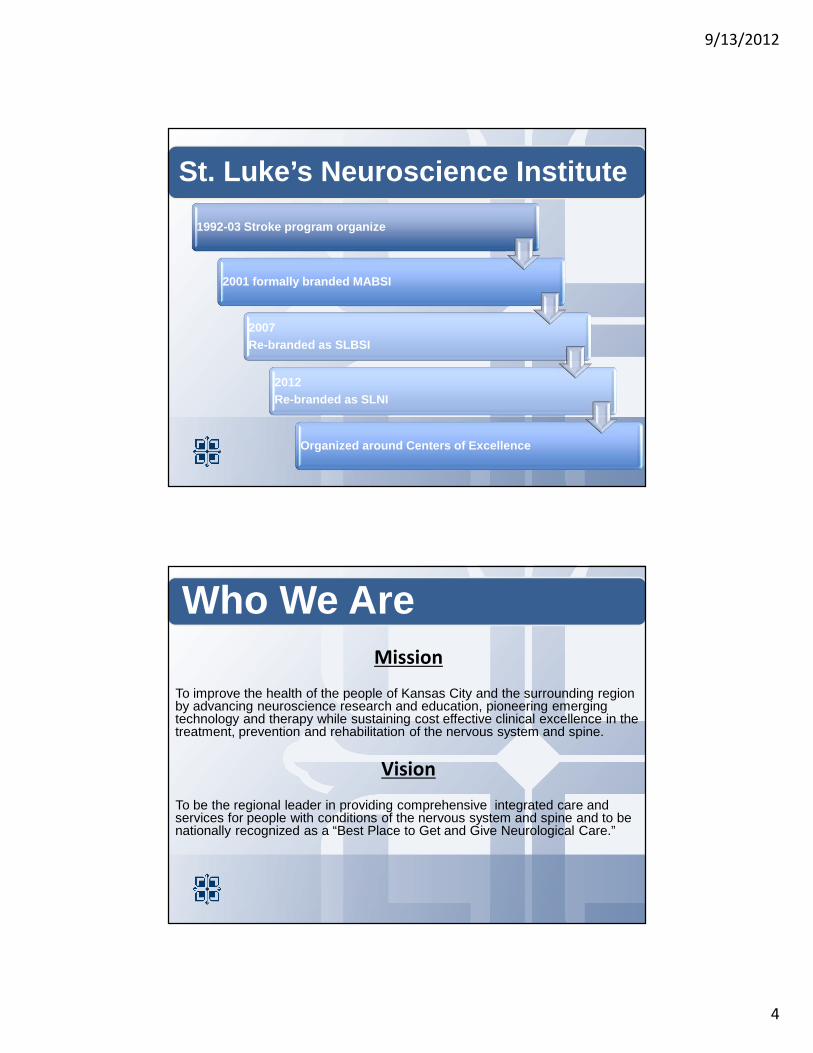
Progression to CSC • EMS and Regional Hospital OutreachSpoke and hub
networking
• Flow of Patient Care • Practice Changes Process Structure
• Clinical Orders• Severity Scoring
Evaluation and Management
• One Call Number (DOC One)Ease of Access to Stroke Program
• ED Initiatives • People - CNNNever on Diversion
• EMS Education• Shadowing Professional Outreach
Regional Networking 02-11

9/13/2012
7
Clinical Tools
• Neuro Evidenced Practice Team – System Orders
• Pre-Checked Orders -Guiding Care
• PSC/CSC Core Measure Integrated– NIH Stroke Scale
– CT time and results
– IV inclusion/Exclusions
– Hunt and Hess
– INR reversal
– mRS – 90 day
– TIA – ABCD Sco
• Transport Protocols
Clinical Tools • Ischemic
• ICH
• SAH
9/13/2012
8
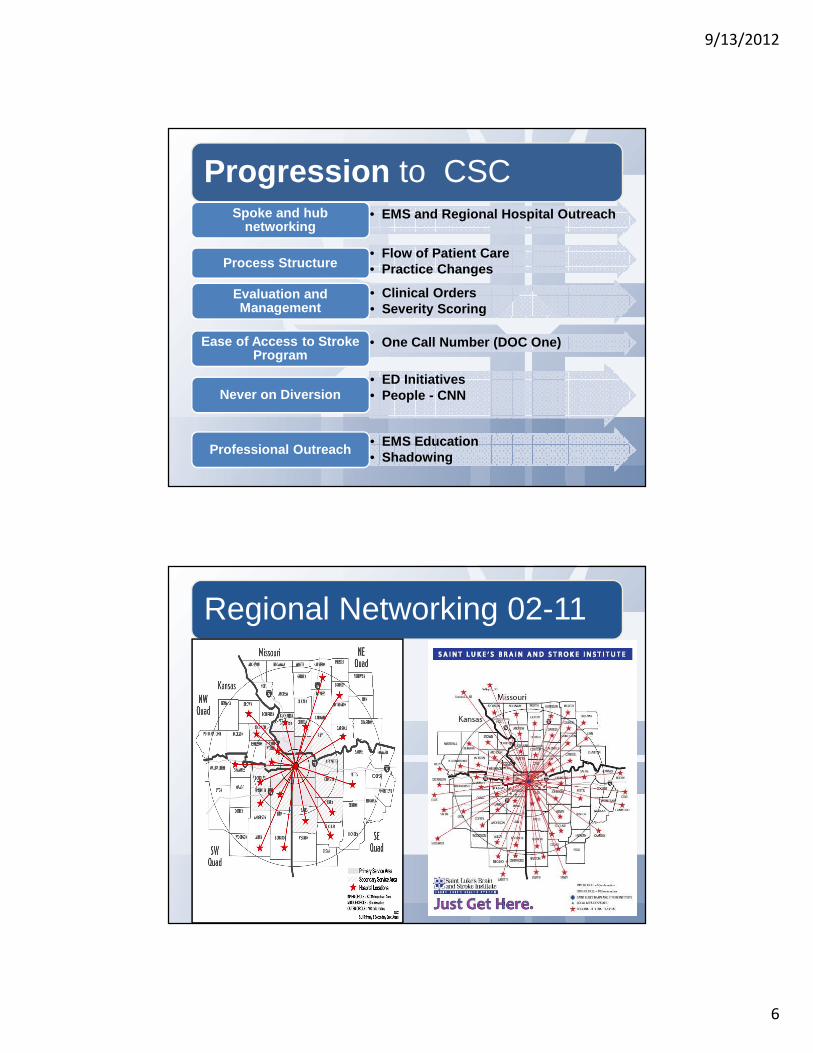
Example of Capturing Measures: Severity Scoring in ICH, SAH, TIA
1
Risk Factor Point Score
Age >60 years – 1 point 1BP Systolic BP > 140 or Diastolic > 90
1
Clinical FeaturesUnilateral weakness with or without speech impairment Speech impairment without unilateral weakness
21
Duration of TIA > 60 minutes 2Diabetes history 1
Total Score
1
Transport Protocols

9/13/2012
9
Additional Clinical Tools • Clinical Path
• Dysphagia Screening Tool
• Patient Education Book
• Discharge Tools
… an Extremely short amount of time to achieve the best outcome for stroke
Stroke
0 hour3 hours
National Stroke Reversal Treatment Rate = 2%
Clinton Mo.
Emergency Department
Doc One
Transfer
Team
9/13/2012
10
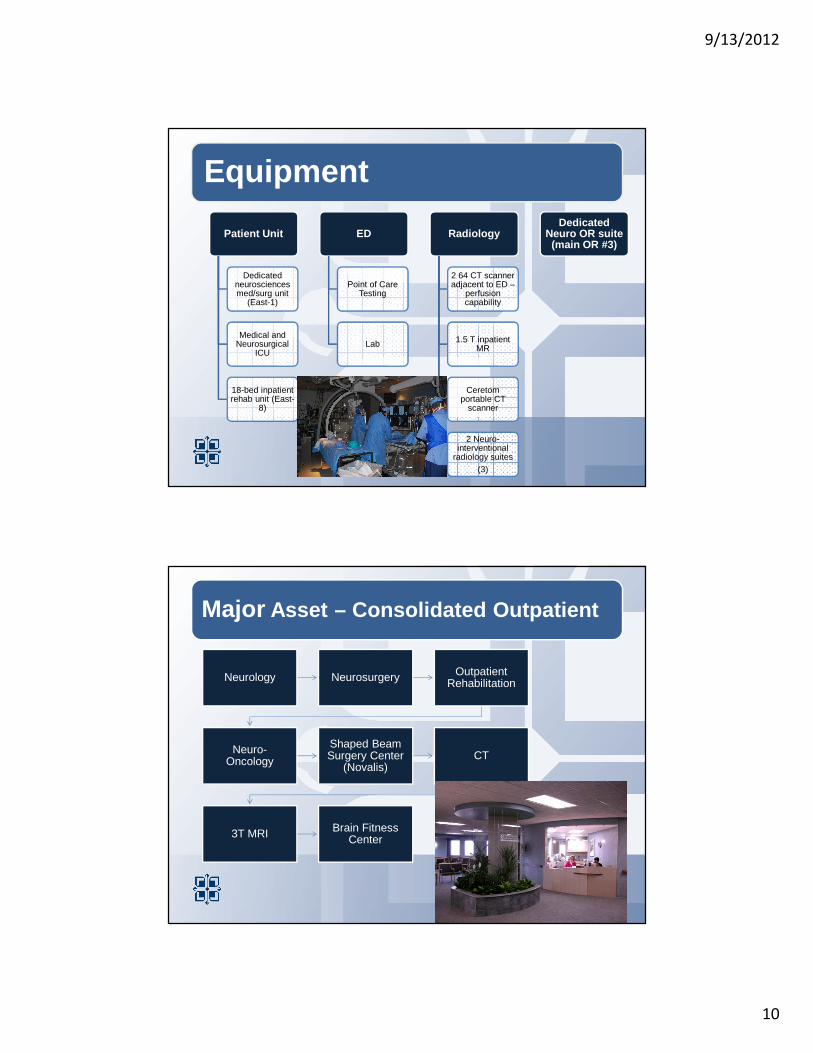
Equipment
Patient Unit
Dedicated neurosciences med/surg unit
(East-1)
Medical and Neurosurgical
ICU
18-bed inpatient rehab unit (East-
8)
ED
Point of Care Testing
Lab
Radiology
2 64 CT scanner adjacent to ED –
perfusion capability
1.5 T inpatient MR
Ceretomportable CT
scanner
2 Neuro-interventional
radiology suites(3)
Dedicated Neuro OR suite (main OR #3)
Major Asset – Consolidated Outpatient
Neurology Neurosurgery Outpatient Rehabilitation
Neuro-Oncology
Shaped Beam Surgery Center
(Novalis)CT
3T MRI Brain Fitness Center
9/13/2012
11
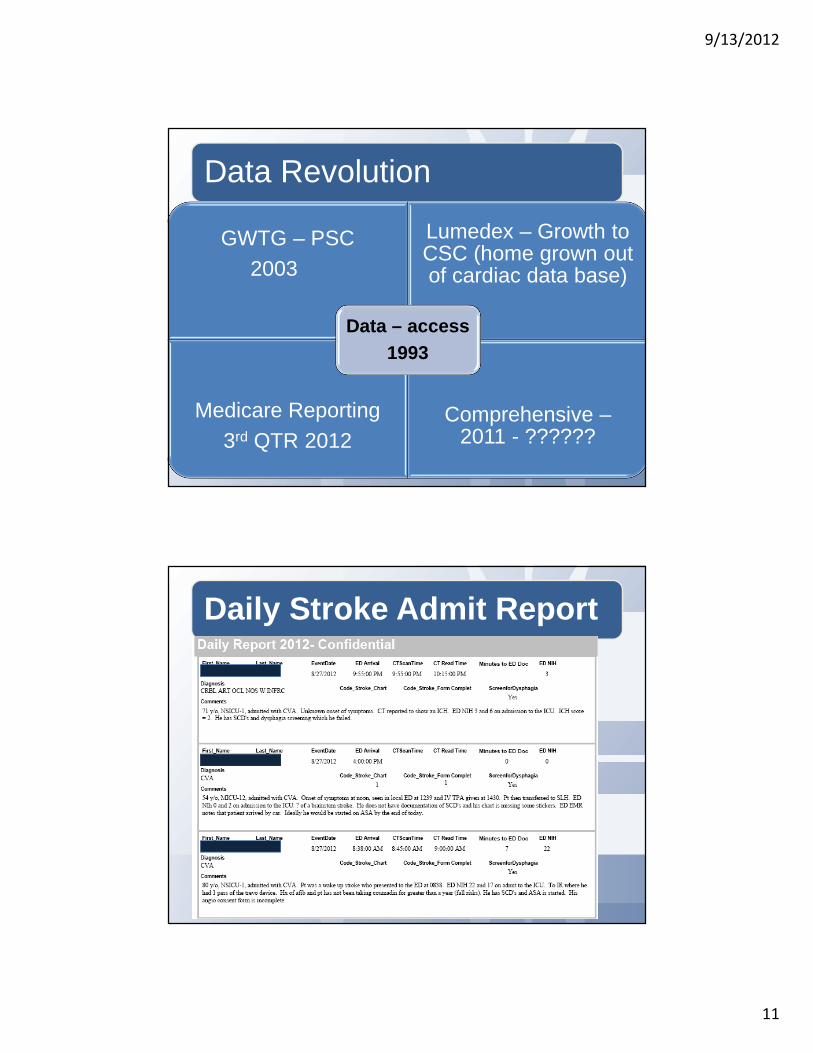
Data Revolution
GWTG – PSC2003
Lumedex – Growth to CSC (home grown out of cardiac data base)
Medicare Reporting3rd QTR 2012
Comprehensive –2011 - ??????
Data – access1993
Daily Stroke Admit Report
9/13/2012
12
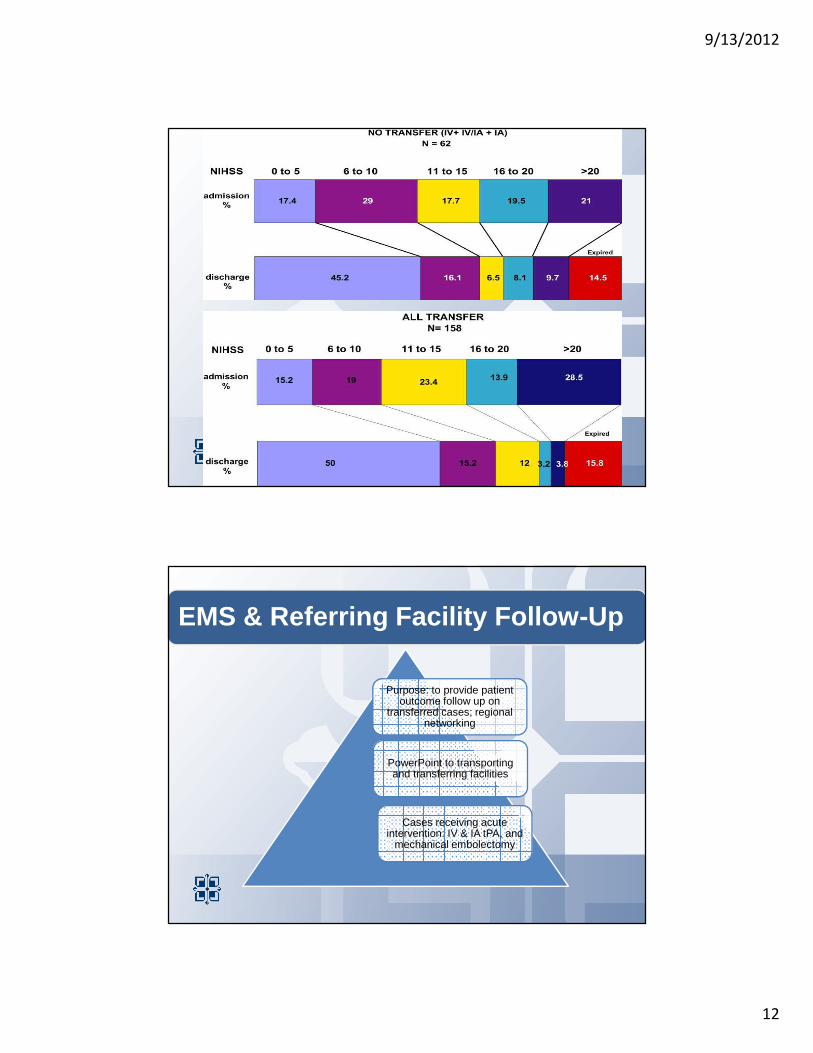
EMS & Referring Facility Follow-Up
Purpose: to provide patient outcome follow up on
transferred cases; regional networking
PowerPoint to transporting and transferring facilities
Cases receiving acute intervention: IV & IA tPA, and
mechanical embolectomy

9/13/2012
13
Expansions of Program Clinician Roles to CSC
Nurse Driven
1

9/13/2012
14
Primary Stroke Program Roles
Medical Director
Data Coordinator
Stroke Coordinator/
APN
ACNS-BC; Post Masters
Neurovascular Clinician
Training
Dr. Marilyn
Rymer
Comprehensive Program Growth
Increasing Volume
ED Capacity –
Core measure missing
Physician Burden
Physician Needs
• 1993 – 220 Ischemic• 2011 678 Ischemic
• IV tpa patients in ED• Lack of Intensive
Monitoring
• Primary • Comprehensive
• Intensive Call Schedule
• Recruitment
• Neurologist• INR’s• Neurosurgeon• Intensivist
1

9/13/2012
15
SLNI Clinician Roles
APN Stroke –Coordinator
(ED Workups, program process)
Code NeuroNurses – full
time 24/7
APN ‘s Center of Excellance
SLNI APN Role
– Staff education, oversight of patient care, acute patient care, community education, maintenance of paths and orders, quality improvement, involved in discharge planning
9/13/2012
16
Code Neuro Nurse Role
The CNN Scope of Practice
Key Functions:• Respond to all acute neurological admissions in ED• Assist transfer team as needed• Evaluate ED patients & provide critical info to other
required caregivers (physicians, nurses, technicians, etc.)• Preliminary screen for research studies; notify research
RNs of candidates as appropriate• Accompany patients to procedures or attend to patients in
ED if admit is delayed• Participates in Clinical practice changes - revision and
update of clinical tools (paths, orders, glucose management, and f/u to pre-hospital providers)

9/13/2012
17
Implementation of CNN
• High level of satisfaction from ED physicians, ED staff all members of the stroke team
• Improved the management of the acute neuro patient
• Provides “just in time” education to nursing staff
• Increased the immediate notification of the stroke team
SLNS Clinical Support Staff
Data - responsible for neurovascular
database and GWTG
Quality Informatics Specialist
RN
2 Research RN’s
Responsible for scope of clinical
trials
Administrative Assistant
Support to APN’s, research coordinator and Medical Director

9/13/2012
18
Neurologist – Stroke Team – 3 in 1993
2
Neuro Interventional Team - 1996

9/13/2012
19
Neurosurgeons – 3 in 1993
Dr. Lovick – Brain Tumor
Dr. Mollman -Spine
Dr. Milligan Skull base
Dr. Griffith – Tremor
Dr. Hiser – General
Outreach
As early as 1994 – clinical trial
Components…
•Education – EMS/hospitals,
community
•Pre-hospital care, NIHSS
•Follow-up inconsistent – 09 formal
•Team building and Collaboration
•Research
•Social media

9/13/2012
20
August 18, 2010
Time and Stroke
Just Get Here!
Code Neuro Nurses
Follow-up Reports – sporadic
•Life Flight Eagle
•Miami County, KS EMS
•MO State TCD Initiative
Outreach & Collaboration
9/13/2012
21
Formalized F/U Report
Follow-upsSporadic����formal
Outreach:Picture here of Template from before.
SLNI
Social Media
Outreach: Examples of blog
And fb site
9/13/2012
22
Leadership Structure
Medical Director
Stroke Coordinator
Data Coordinator
RN Abstractor
CNN-Clinical Leaders
VP Neuroscience
Institute
Clinical Director
Denise Mogg –SLNI Clinical Director
Kevin Thorpe VP SLNI
Nursing Experts and Leaders19 Certified CNRN’s 2011
9/13/2012
23
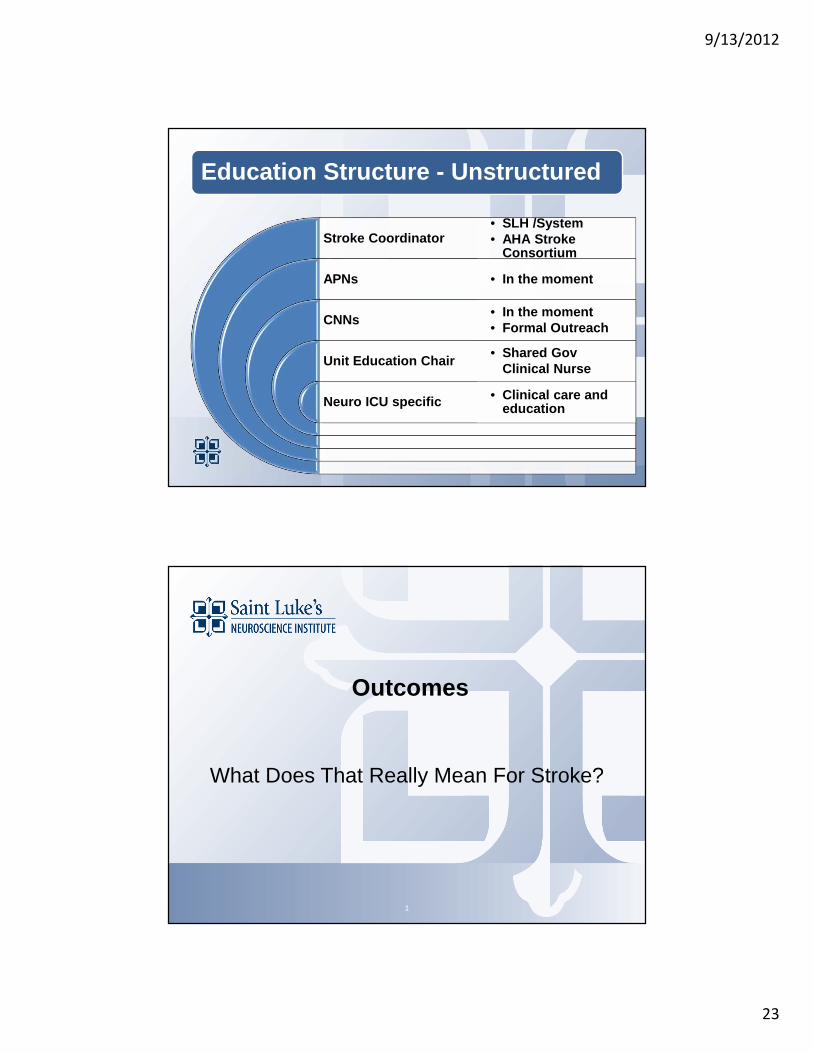
Education Structure - Unstructured
Stroke Coordinator
APNs
CNNs
Unit Education Chair
Neuro ICU specific
• SLH /System • AHA Stroke
Consortium
• In the moment
• In the moment• Formal Outreach
• Shared Gov Clinical Nurse
• Clinical care and education
Outcomes
What Does That Really Mean For Stroke?
1
9/13/2012
24
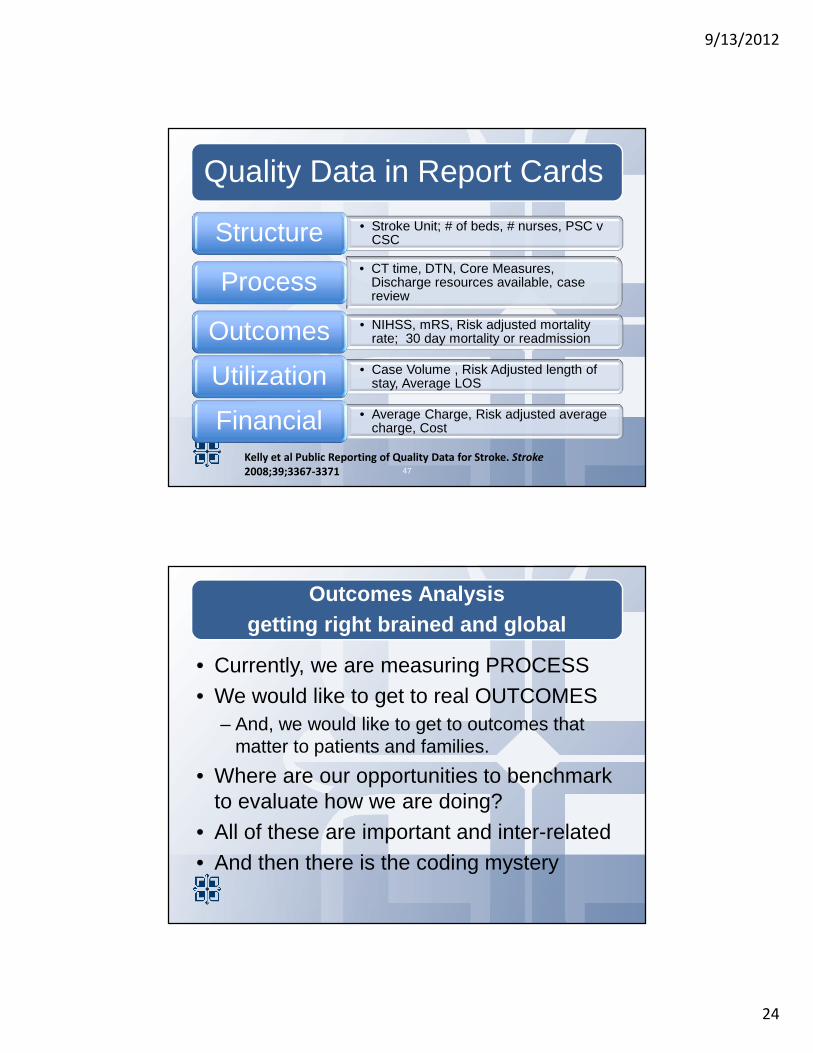
Quality Data in Report Cards
• Stroke Unit; # of beds, # nurses, PSC v CSCStructure
• CT time, DTN, Core Measures, Discharge resources available, case review
Process• NIHSS, mRS, Risk adjusted mortality
rate; 30 day mortality or readmissionOutcomes • Case Volume , Risk Adjusted length of
stay, Average LOSUtilization• Average Charge, Risk adjusted average
charge, Cost Financial
47
Kelly et al Public Reporting of Quality Data for Stroke. Stroke
2008;39;3367-3371
Outcomes Analysis getting right brained and global
• Currently, we are measuring PROCESS• We would like to get to real OUTCOMES
– And, we would like to get to outcomes that matter to patients and families.
• Where are our opportunities to benchmark to evaluate how we are doing?
• All of these are important and inter-related• And then there is the coding mystery

9/13/2012
25
Coding Struggles
1
STROKE MORTALITY IS A
BLACK BOX!!
All Patient Refined DX(APR DRG) key words
PROCESS

9/13/2012
26
National Hospital Inpatient Quality (“Core”) Measures for Stroke
• Acute Measures– Thrombolytic therapy – arrive in 2 hours and treated by 3 hours– Venous thrombo-embolism prophylaxis by end of day 2– Antithrombotic therapy by end of day 2 of admission
• Discharge Measures– Discharged on antithrombotic therapy– Discharged on statin medication if LDL>100– Anticoagulation therapy for atrial fibrillation/flutter
• Quality Measures– Door to CT time 25 minutes in patients presenting with stroke symptoms
3 hours’ duration (Door to CT 25 Minutes)– DTN Time < 60 minutes– Dysphagia screening– Stroke education– Assessed for rehabilitation
Quality Analysis IV t-PA DTN
1
STROKE MORTALITY IS A
BLACK BOX!!
APR DRG key words

9/13/2012
27
SLH Core Measures – Dash Board
SLH Secondary Core Measures
9/13/2012
28
Comprehensive Measures- TBA
• CSTK-01 National Institutes of Health Stroke Scale (NIHSS) Score on Arrival
• CSTK-02 Modified Rankin Score (mRS) at 90 Days
• CSTK-03 Severity Measurement on Arrival –NIHSS, ICH Score, Hunt and Hess
• CSTK-04 Median Time to Treatment with a Procoagulant Reversal Agent
• CSTK-04a Median Time to INR Reversal
Comprehensive Measures- TBA
• CSTK-05 Hemorrhagic Complication for Patients Treated with Intra-Venous (IV) Thrombolytic (t-PA) Therapy Without Catheter-Based Reperfusion
• CSTK-05a Hemorrhagic Complication for Patients Treated with Intra-Arterial (IA) Thrombolytic Therapy or Mechanical Endovascular Reperfusion Procedure With or Without Intra-Venous (IV)Thrombolytic (t-PA) Therapy

9/13/2012
29
Comprehensive Measures- TBA
• CSTK-06 Nimodipine Treatment Initiated• CSTK-07 Median Time to Recanalization
Therapy• CSTK-07a Thrombolysis in Cerebral Infarction
(TICI) Post- Treatment Reperfusion Grade
TICI - Thrombolysis in Cerebral Infarction
58
• 0 = No perfusion • 1 = Perfusion past the initial obstruction with little
or slow distal perfusion • 2A = Perfusion of < ½ of the occluded artery • 2B = Perfusion of ½ or >of the vascular
distribution of the occluded artery• 3 = Full perfusion with filling of all distal
branches

9/13/2012
30
Limitations - Documentation!
• The determination of whether a process of care was delivered to an individual patient was based on documentation in the medical record, and such data may be incomplete.
• EMR documentation is a challenge for neuro cases.
• Dawn M. Bravata. Processes of Care Associated With Acute Stroke Outcomes. Arch Intern Med. 2010;170(9):804-810
Standardized Order Sets Based on Current Evidence
The SLHS EPT Teams

9/13/2012
31
OUTCOMES(real ones- what are they?
The truth is-------------we don’t know yet)
Example of Measures
• Outcome measures include: mortality, readmissions, complications, and patient/caregiver satisfaction scores.
• Utilization measures include: data pertaining to the frequency of service use, including length of stay.
• Finance measures include economic data pertaining to the provision of stroke care.
9/13/2012
32
Mortality – What if you are a regional referral center and everything on Friday afternoon is “stroke like sx”
• All the bad cases are coming to you.• You need to know the code words for
documenting severity: brain edema, brain compression, encephalopathy, cognitive impairment, malnutrition, coma, etc.
• Case Study: Expected mortalility and observed mortality.
What Really Matters
• mRS at 90 days• NIHSS score on admission and discharge• How many days at home in 90 days after
stroke• FIM scores on admission and discharge
from rehab• Satisfaction and QOL scores

9/13/2012
33
Innovation and Research
•Clinical Research elevates practice–Participation in most major stroke treatment trials since
1994–Presentation/publications ISC–Collaboration with other top stroke centers: UCLA,
Pittsburgh, Massachusetts General, Stanford for reporting data
•Process Innovation improves outcomes–SWAT –Database –Code Neuro–Daily stroke report –Feedback reports to ED and EMS–Outcome measures – phone follow-up 2-3 day….. and at
90 day
Where are the Benchmarks?
• GWTG can provide comparative data for Primary Stroke Centers
• The MERCI Registry collected 1000 cases for analysis of interventional stroke center performance.
• There is no national ischemic stroke registry for benchmarking

9/13/2012
34
SLNI Acute Stroke Intervention2002 - 2011
Overview comparing St Luke’s patients to the “rest-of-world” (ROW)
Datacut Date: April 19, 2010

9/13/2012
35
Analysis Notes
• Datacut Date: April 19, 2010• Analysis cohort:
– All subjects with valid/complete 90d mRS
St Luke’s (N=84) All Others (N=702)
Age – Mean / Median (years) (N) 68.1 / 70 (84) 66.9 / 69 (702)
Baseline NIHSS – Mean / Median (N) 18.9 / 18.5 (84) 18 .0 / 18 (678)
Pre-Stroke mRS > 1 15.5% (13/84) 7.1% (49/690)
Merci Registry Procedural Data
St Luke’s (n=84) All Others (N=702)
% Receiving IV tPA 43% (36/84) 27% (192/702)
% Receiving IA lytic 50% (42/84) 47% (328/702)
% IIb/IIIa 0% (0/84) 7% (51/702)
Vasodilators 0% (0/84) 12% (82/702)
Time: Mean Onset to Groin Access (hrs)
5.4 7.3
Time: Mean Procedure Length (hrs)
1.5 3.1
Source: masterpatientlist_19APR2010.xls
9/13/2012
36
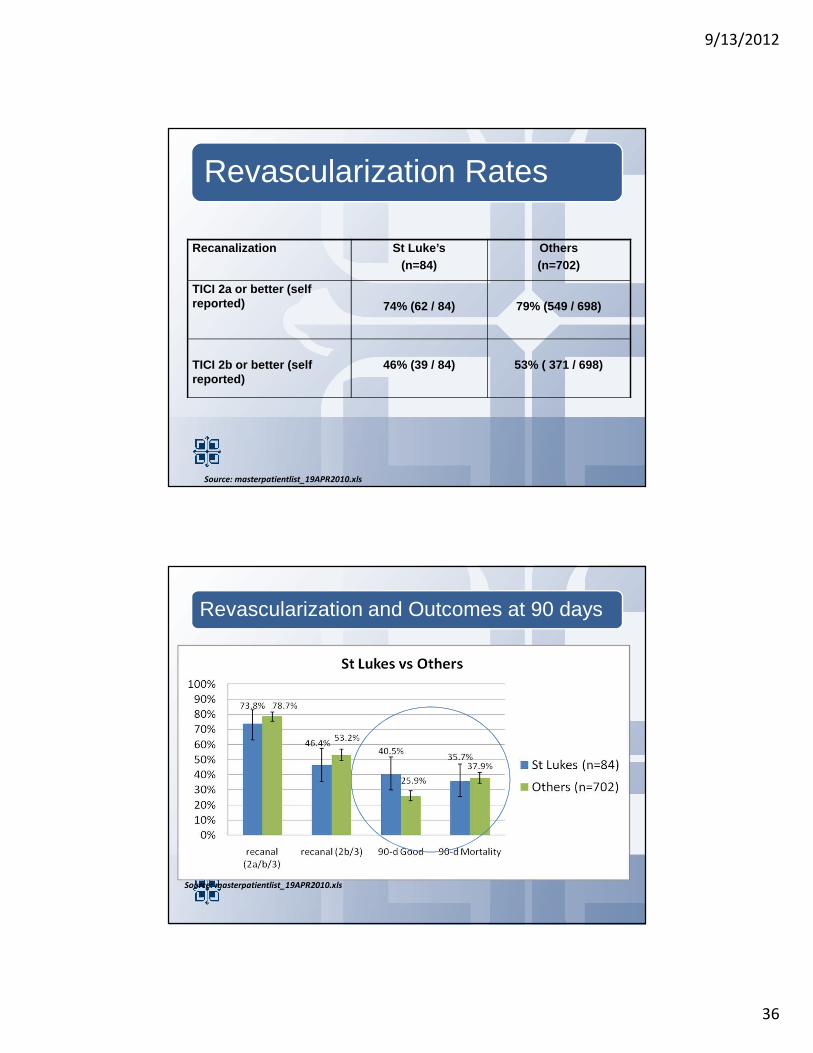
Revascularization Rates
Recanalization St Luke’s(n=84)
Others (n=702)
TICI 2a or better (self reported) 74% (62 / 84) 79% (549 / 698)
TICI 2b or better (self reported)
46% (39 / 84) 53% ( 371 / 698)
Source: masterpatientlist_19APR2010.xls
Revascularization and Outcomes at 90 days
Source: masterpatientlist_19APR2010.xls

9/13/2012
37
Stroke Mortality Rates
• Ischemic stroke mortality reported in Circulation 2010 18.4%
• SLBSI ischemic stroke mortality rate– Non intervention cases 10%– Intervention cases 16%– Overall 11.6%
SLH Rehabilitation Stroke OutcomesUDS Comparison of Regional and National Statistics
for Rehabilitation Programs
% of Cases SLH Region National
Discharged Home 80.8 65.5 67.3
CI 1.52 1.44 1.54
LOS 14.5 14.7 14.6
FIM Change 25.1 24.6 24.7
9/13/2012
38
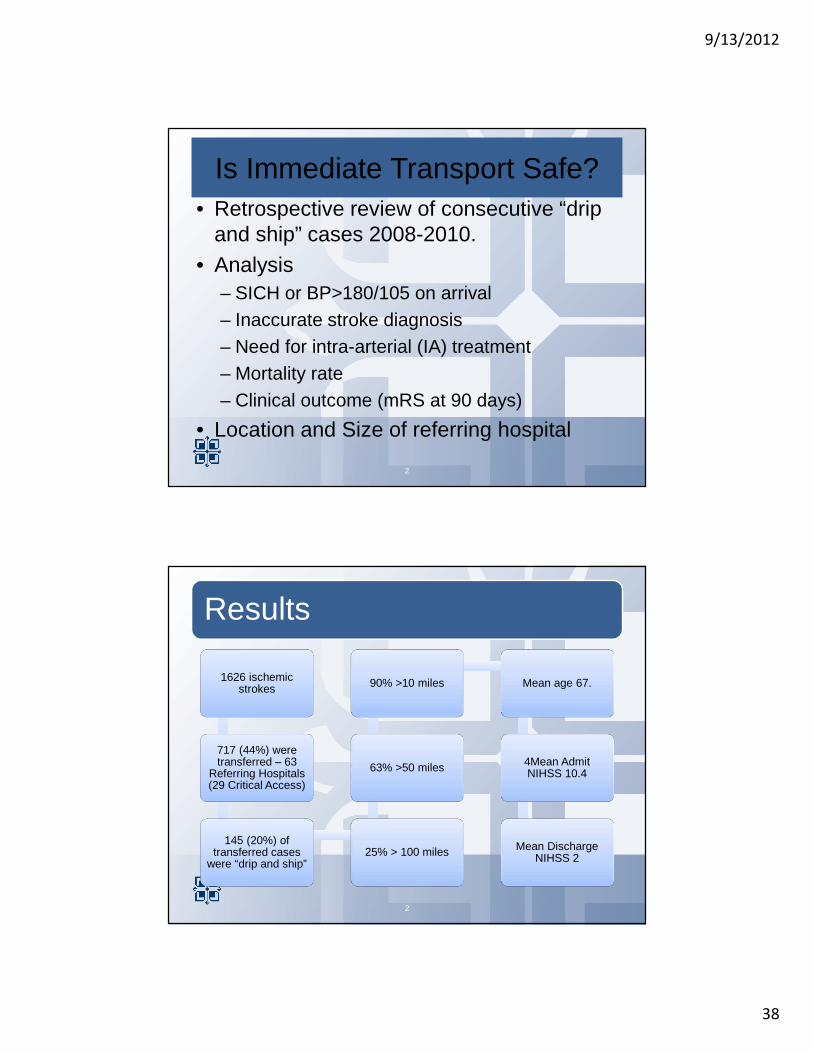
Is Immediate Transport Safe?• Retrospective review of consecutive “drip
and ship” cases 2008-2010.• Analysis
– SICH or BP>180/105 on arrival– Inaccurate stroke diagnosis– Need for intra-arterial (IA) treatment– Mortality rate– Clinical outcome (mRS at 90 days)
• Location and Size of referring hospital
2
Results
1626 ischemic strokes
717 (44%) were transferred – 63
Referring Hospitals (29 Critical Access)
145 (20%) of transferred cases
were “drip and ship”25% > 100 miles
63% >50 miles
90% >10 miles Mean age 67.
4Mean Admit NIHSS 10.4
Mean Discharge NIHSS 2
2

9/13/2012
39
Blood Pressure on Arrival
1 SICH
1 Mortality
10/14
2
• BP=183/77• Mortality
• BP=232/84• No Hemorrhage
• mRS 0-2 at 90 days
• mRS > 2
2
14/145 (9.6%) had BP >180/105
4 Cases with Hemorrhage on Arrival
4 SICH • 2.7 % (3 of these had BP <180/105)
2 Died
• 1 related to SICH• 1 BP>180/105
2 Lived
• Admit NIHSS 25; discharge NIHSS 4• Admit NIHSS 18; discharge NIHSS 10
2

9/13/2012
40
Outcomes
mRS 0-2 at 90 days = 72/114 (63%)Note: mRS scores not available for 2008
Mortality = 20/145 (13.7%) Further Endovascular therapy = 35/145 (24%)Inaccurate diagnosis at sending facility = 6/145 (4.1%) ; all had excellent clinical outcomes.
2
Conclusions
• Immediate transport of patients with IV tPA infusing is safe with a low incidence of SICH en route
• The 63% good outcomes may, in part, relate to early treatment with IV tPA in referring hospitals
• Hospitals of every size and location can safely treat stroke victims with IV tPA if they have access to consultation and transfer agreements with experienced stroke centers
2
9/13/2012
41
2
NEVER SETTLE
Changing Lives
THE EMS CREW WHO SAVED HER LIFE
Related Documents