Evaluation Complete mental health recovery: bridging mental illness with positive mental health Helene L. Provencher and Corey L.M. Keyes Abstract Purpose – The purpose of this paper is to propose that the study, and the promotion, of recovery can be augmented by adopting the model of mental health as a complete state. Design/methodology/approach – A literature review of the last two decades was undertaken and pathways to complete mental health in recovery are proposed. Findings – More work is needed to further develop interventions oriented towards the promotion of positive mental health in recovery, targeting the enhancement of positive emotions towards life and a sense of fulfillment in private and social life. Positive mental health also deserves more research attention to assess the full range of recovery outcomes related to the restoration and optimization processes. A better understanding of individual and environmental factors facilitating or hindering the achievement of complete mental health in recovery is warranted as well. Originality/value – Unlike previous conceptions, the model presented in the paper proposes to redefine recovery from the complete view of mental health and introduces positive mental health as an additional outcome of recovery. Keywords Mental illness, Quality of life Paper type General review Mental health, as more than the absence of mental illness and involving the presence of subjective well-being as well, is a view that has been represented in the scientific literature for more than half a century (Jahoda, 1958; The World Health Organization, 1948). However, this complete vision of mental health remained undefined, unmeasured and therefore largely ignored for several decades. Recently, a new approach has been developed for evaluating states of complete mental health, including criteria for combining indicators of mental illness and positive mental health (i.e. subjective well-being). This has been used to study the model of complete mental health, also called the two continua model (Keyes, 2005a, 2007). Overall, this line of research has demonstrated the independence of mental illness and positive mental health, representing two separate continua rather than the opposite ends of a single continuum. This implies that experiencing less mental illness does not necessarily equate with experiencing better positive mental health and also highlights the possibility of achieving a high level of positive mental health despite the presence of enduring psychiatric symptoms and deficits. Over the last two decades, recovery has become the overarching aim of mental health services systems in many countries, Australia, New Zealand, England, Scotland and the USA to name a few (Slade et al., 2008). An extensive body of literature on recovery has emerged from narrative studies (Silverstein and Bellack, 2008) and numerous published personal accounts (Ridgway, 2001; Spaniol and Koehler, 1994). This has provided a better understanding of personal and DOI 10.1108/17465721111134556 VOL. 10 NO. 1 2011, pp. 57-69, Q Emerald Group Publishing Limited, ISSN 1746-5729 j JOURNAL OF PUBLIC MENTAL HEALTH j PAGE 57 Helene L. Provencher is based in the Faculty of Nursing, Laval University, Quebec, Canada. Corey L.M. Keyes is based in the Department of Sociology, Emory University, Atlanta, Georgia, USA.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Evaluation
Complete mental health recovery: bridgingmental illness with positive mental health
Helene L. Provencher and Corey L.M. Keyes
Abstract
Purpose – The purpose of this paper is to propose that the study, and the promotion, of recovery can be
augmented by adopting the model of mental health as a complete state.
Design/methodology/approach – A literature review of the last two decades was undertaken and
pathways to complete mental health in recovery are proposed.
Findings – More work is needed to further develop interventions oriented towards the promotion of
positive mental health in recovery, targeting the enhancement of positive emotions towards life and a
sense of fulfillment in private and social life. Positive mental health also deserves more research attention
to assess the full range of recovery outcomes related to the restoration and optimization processes.
A better understanding of individual and environmental factors facilitating or hindering the achievement
of complete mental health in recovery is warranted as well.
Originality/value – Unlike previous conceptions, the model presented in the paper proposes to
redefine recovery from the complete view of mental health and introduces positive mental health as an
additional outcome of recovery.
Keywords Mental illness, Quality of life
Paper type General review
Mental health, as more than the absence of mental illness and involving the presence of
subjective well-being as well, is a view that has been represented in the scientific literature for
more than half a century (Jahoda, 1958; TheWorld Health Organization, 1948). However, this
complete vision of mental health remained undefined, unmeasured and therefore largely
ignored for several decades. Recently, a new approach has been developed for evaluating
states of complete mental health, including criteria for combining indicators of mental illness
and positivemental health (i.e. subjective well-being). This has been used to study themodel
of complete mental health, also called the two continua model (Keyes, 2005a, 2007). Overall,
this line of research has demonstrated the independence of mental illness and positive
mental health, representing two separate continua rather than the opposite ends of a single
continuum. This implies that experiencing less mental illness does not necessarily equate
with experiencing better positivemental health and also highlights the possibility of achieving
a high level of positive mental health despite the presence of enduring psychiatric symptoms
and deficits.
Over the last twodecades, recovery has become the overarchingaimofmental health services
systems inmany countries, Australia, New Zealand, England, Scotland and the USA to name a
few (Slade et al., 2008). An extensive body of literature on recovery has emerged fromnarrative
studies (Silverstein and Bellack, 2008) and numerous published personal accounts (Ridgway,
2001; Spaniol and Koehler, 1994). This has provided a better understanding of personal and
DOI 10.1108/17465721111134556 VOL. 10 NO. 1 2011, pp. 57-69, Q Emerald Group Publishing Limited, ISSN 1746-5729 j JOURNAL OF PUBLIC MENTAL HEALTH j PAGE 57
Helene L. Provencher is
based in the Faculty of
Nursing, Laval University,
Quebec, Canada.
Corey L.M. Keyes is based
in the Department of
Sociology, Emory
University, Atlanta,
Georgia, USA.
environmental factors hindering or facilitating this journey as well as valuable insight about its
key dimensions (e.g. hope, empowerment, positive identity) and phases (Onken et al., 2007).
Consumers’ views of recovery stress the importance of having a pleasant and fulfilling life
despite the presence of mental illness, drawing attention to aspirations that are similar to any
other citizen. As Deegan (1988, p. 15) put it, recovery implies ‘‘to live, work, and love in a
community in which one makes a significant contribution.’’ Consistent with this view, The
World Health Organization (2005, p. 2) has recently defined mental health as:
[. . .] a state of well-being in which the individual realizes his or her own abilities, can cope with the
normal stresses of life, canwork productively and fruitfully, and is able tomake a contribution to his
or her community.
This definition reflects a salutogenic approach of mental health focusing on the presence of
positive human capacities and functioning (Antonovsky, 1979), which has also been retained
to measure positive mental health within the model of complete mental health.
The consumer-oriented vision of recovery has been taken up by a large number of
researchers and clinicians and has challenged the traditional and clinical way of defining this
phenomenon. This second vision defines recovery through the lens of the disease and
improvements in psychiatric symptoms and impairments represent signs of recovery, which
may indicate partial or full remission from mental illness (Silverstein and Bellack, 2008).
Based on this vision, several long-term follow-up studies (Calabrese and Corrigan, 2005)
have reported that more than half of personswith schizophrenia had completely recovered or
had shown significant improvements in psychiatric symptoms and functional deficits over a
period of about 20 years.
In short, consumers’ viewpoints reflect a salutogenic approach of recovery which
emphasizes the achievement of positive mental health, indexed by a sense of pleasure
and accomplishment in life. On the other hand, scientifically oriented definitions reflect a
disease-oriented or pathogenic approach of recovery, focusing on psychiatric symptoms
and deficits. So far, theoretical guidelines for bridging together the pathogenic and
salutogenic views of recovery have been overlooked, and from these may emerge a more
integrated view of this phenomenon. We argue, in this paper, that the study and the
promotion of recovery, as a process and as an outcome, can be augmented by the model of
complete mental health (Keyes, 2005a, 2007).
Following a brief overview of Keyes’ model, current definitions of recovery are further
discussed based on their underlying conceptions ofmental health, including the relevance of
positive mental health to tackle this phenomenon. Third, recovery is redefined as a complete
mental health view, relying on two complementary experiences – restoration from mental
illness and optimization of positivemental health. An emphasis is placed on outcomes, which
are viewed as pathways in complete mental health over the recovery process. How the
proposed complete view of recovery coincides with and departs from previous conceptions
is discussed along with some suggestions for future interventions and research.
Mental health is a complete state
Positive mental health
Positive mental health corresponds to feelings, thoughts and behaviors that are required for
having a good life and those have been studied in the domain of subjective well-being for
more than four decades. Critical reviews of this literature (Keyes, 2006b; Ryan and Deci,
2001) has proposed that positive mental health relies on two distinct but complementary
perspectives: hedonic well-being (also called emotional well-being) refers to positive
emotions toward one’s life such as happiness and life satisfaction, whereas positive
functioning (also called eudaimonic well-being) consists of a sense of engagement and
fulfillment in one’s private and social life, which reflects psychological and social well-being
(Keyes, 1998; Ryff and Singer, 1996).
PAGE 58 j JOURNAL OF PUBLIC MENTAL HEALTHj VOL. 10 NO. 1 2011
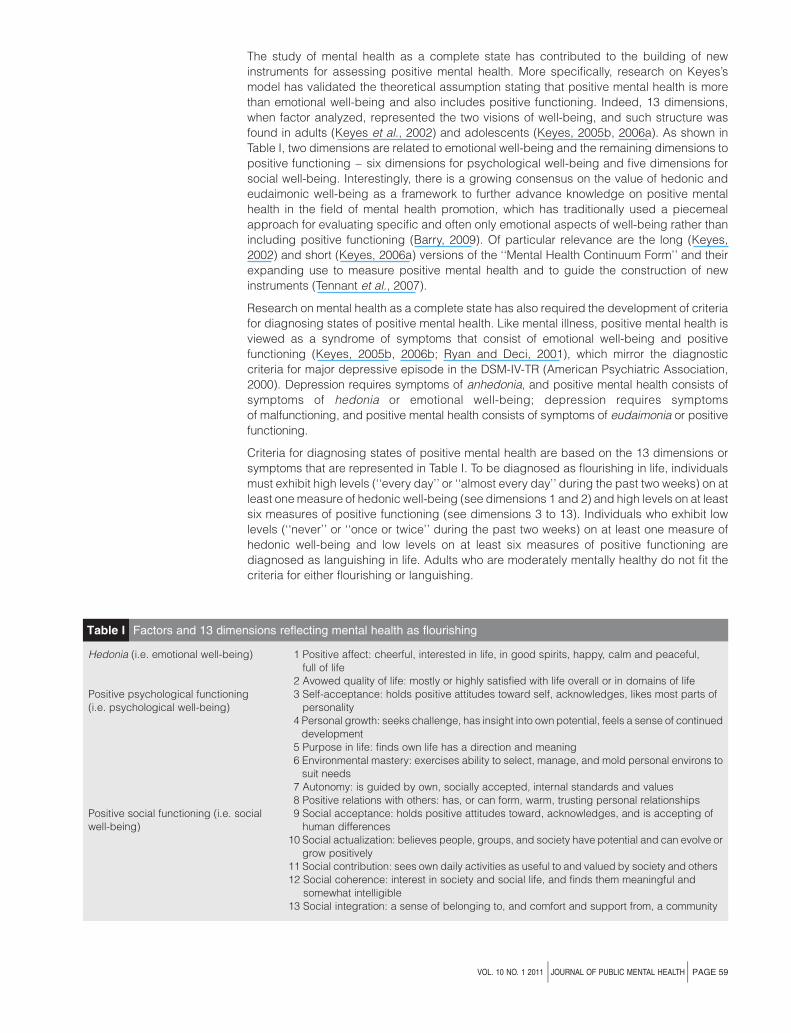
The study of mental health as a complete state has contributed to the building of new
instruments for assessing positive mental health. More specifically, research on Keyes’s
model has validated the theoretical assumption stating that positive mental health is more
than emotional well-being and also includes positive functioning. Indeed, 13 dimensions,
when factor analyzed, represented the two visions of well-being, and such structure was
found in adults (Keyes et al., 2002) and adolescents (Keyes, 2005b, 2006a). As shown in
Table I, two dimensions are related to emotional well-being and the remaining dimensions to
positive functioning – six dimensions for psychological well-being and five dimensions for
social well-being. Interestingly, there is a growing consensus on the value of hedonic and
eudaimonic well-being as a framework to further advance knowledge on positive mental
health in the field of mental health promotion, which has traditionally used a piecemeal
approach for evaluating specific and often only emotional aspects of well-being rather than
including positive functioning (Barry, 2009). Of particular relevance are the long (Keyes,
2002) and short (Keyes, 2006a) versions of the ‘‘Mental Health Continuum Form’’ and their
expanding use to measure positive mental health and to guide the construction of new
instruments (Tennant et al., 2007).
Research on mental health as a complete state has also required the development of criteria
for diagnosing states of positive mental health. Like mental illness, positive mental health is
viewed as a syndrome of symptoms that consist of emotional well-being and positive
functioning (Keyes, 2005b, 2006b; Ryan and Deci, 2001), which mirror the diagnostic
criteria for major depressive episode in the DSM-IV-TR (American Psychiatric Association,
2000). Depression requires symptoms of anhedonia, and positive mental health consists of
symptoms of hedonia or emotional well-being; depression requires symptoms
of malfunctioning, and positive mental health consists of symptoms of eudaimonia or positive
functioning.
Criteria for diagnosing states of positive mental health are based on the 13 dimensions or
symptoms that are represented in Table I. To be diagnosed as flourishing in life, individuals
must exhibit high levels (‘‘every day’’ or ‘‘almost every day’’ during the past two weeks) on at
least onemeasure of hedonic well-being (see dimensions 1 and 2) and high levels on at least
six measures of positive functioning (see dimensions 3 to 13). Individuals who exhibit low
levels (‘‘never’’ or ‘‘once or twice’’ during the past two weeks) on at least one measure of
hedonic well-being and low levels on at least six measures of positive functioning are
diagnosed as languishing in life. Adults who are moderately mentally healthy do not fit the
criteria for either flourishing or languishing.
Table I Factors and 13 dimensions reflecting mental health as flourishing
Hedonia (i.e. emotional well-being) 1 Positive affect: cheerful, interested in life, in good spirits, happy, calm and peaceful,full of life
2 Avowed quality of life: mostly or highly satisfied with life overall or in domains of lifePositive psychological functioning(i.e. psychological well-being)
3 Self-acceptance: holds positive attitudes toward self, acknowledges, likes most parts ofpersonality
4 Personal growth: seeks challenge, has insight into own potential, feels a sense of continueddevelopment
5 Purpose in life: finds own life has a direction and meaning6 Environmental mastery: exercises ability to select, manage, and mold personal environs tosuit needs
7 Autonomy: is guided by own, socially accepted, internal standards and values8 Positive relations with others: has, or can form, warm, trusting personal relationships
Positive social functioning (i.e. socialwell-being)
9 Social acceptance: holds positive attitudes toward, acknowledges, and is accepting ofhuman differences
10 Social actualization: believes people, groups, and society have potential and can evolve orgrow positively
11 Social contribution: sees own daily activities as useful to and valued by society and others12 Social coherence: interest in society and social life, and finds them meaningful and
somewhat intelligible13 Social integration: a sense of belonging to, and comfort and support from, a community
VOL. 10 NO. 1 2011 j JOURNAL OF PUBLIC MENTAL HEALTHj PAGE 59

Empirical support for mental health as a complete state
Findings summarized next come from papers using 1995 Midlife in the United States survey
(MIDUS), a random sample of 3,032 adults between the ages of 25-74 (Keyes, 2005a, 2007).
With regards to mental illness, the DSM-III-R (American Psychiatric Association, 1987)
criteria were used to diagnose four mental disorders – major depressive episode, panic,
generalized anxiety, and alcohol dependence – and the Composite International Diagnostic
Interview Short Form scales (Kessler et al., 1998) served to assess the number of symptoms
in those four psychiatric disorders over the past year. States of positive mental health were
evaluated through the above procedure.
The model of complete mental health is based on the assumption that mental illness and
positive mental health represent two distinct dimensions or continua. This suggests that the
absence of mental illness does not imply the presence of mental health (and, the absence of
mental health does not imply the presence of mental illness). Empirical findings have
supported this hypothesis, as confirmatory factor analysis revealed that the latent factor of
mental illness correlated 20.53 with the latent factor of mental health, providing support for
their relative independence. The two continua model has been validated in adults (Keyes,
2005a) and adolescents (Keyes, 2009b).
Languishing adults (e.g. low levels of positivemental health) reported the highest prevalence
of any of the four mental disorders as well as the highest prevalence of reporting two or more
mental disorders during the past year. In contrast, flourishing individuals reported the lowest
prevalence of any of the four 12-month mental disorders or their comorbidity. Compared with
languishing or flourishing, moderately mentally healthy adults were at intermediate risk of any
of the mental disorders or two or more mental disorders during the past year. Those findings
suggest that languishing may act as a risk factor of mental illness, and flourishing as a buffer
protective factor against mental illness.
Six states of complete mental health emerged from the combination of mental illness and
positive mental health and their prevalence rates were determined:
1. Mental illness and languishing (7%).
2. Mental illness and moderate mental health (15%).
3. Mental illness and flourishing (1%).
4. absence of mental illness and languishing (10%).
5. Absence of mental illness and moderate mental health (51%).
6. Absence of mental illness and flourishing (17%).
Of note, less of one-fifth of adults achieved a state of complete mental health, being free of
mental illness and flourishing.
Additional data revealed that any less than complete mental health resulted in increased
impairment and disability. Among adults who were free of mental illness, those who were
flourishing functioned better than those who were moderately mentally healthy, who in turn
functioned better than those who were languishing. Individuals free of mental illness and
flourishing reported the fewest workdays missed, fewest workdays cutback by one-half, the
lowest rate of cardiovascular disease, the lowest level of health limitations of activities of daily
living, the fewest chronic physical conditions at all ages, and the lowest healthcare use (e.g.
medical visits, hospitalizations, medications). Those individuals also reached the highest
levels of psychosocial functioning, showing the lowest level of perceived helplessness, the
highest level of knowing what they want from life, the highest level of self-reported resilience
(e.g. learning from adversities), and the highest level of close relationships and intimacy.
Finally, of adults who had at least one of the four mental disorders, those who were flourishing
functioned better than those with moderate mental health, who in turn functioned better than
those were languishing.
PAGE 60 j JOURNAL OF PUBLIC MENTAL HEALTHj VOL. 10 NO. 1 2011
Recovery
Current definitions of recovery
Two distinct but complementary definitions of recovery prevail in the literature. Reflecting the
disease-oriented or pathogenic approach, the first and traditional definition focuses on
psychiatric symptoms and impairments, which are used to evaluate the extent of remission
from mental illness (Silverstein and Bellack, 2008).
The second definition views recovery as a personal and social process (Noordsy et al., 2002;
Onken et al., 2007). The emphasis here is placed on personal transformations that emerge
throughout this journey, such as positive changes in views about oneself, purpose in life,
relationships with others, and ways of perceiving and managing the mental illness. These
personal changes interact with actions that are undertaken to make transformations at
the community level, involving the reduction of barriers to social exclusion (e.g. stigma,
discrimination) as well as the provision of opportunities and the creation of niches for
increasing social participation and civic engagement. Through their personal stories and
scientific work, consumers have particularly endorsed the view of recovery as a process,
insisting on the unique, non-linear, and subjective aspects of this experience. Such
conceptualization is represented in personal recovery (Slade, 2010) and the experience of
recovering ‘‘in’’ mental illness (Davidson and Roe, 2007).
Both the pathogenic and salutogenic views are represented in defining recovery as a
process. In line with the stress-vulnerability model of psychiatric disorders (Corrigan et al.,
2008), this vision of recovery highlights the importance of personal and environmental
changes that act as protective factors and contribute to the alleviation ofmental illness and its
negative social consequences, such as illness management strategies, restored functional
skills, or environmental support against social discrimination. Interestingly, other aspects of
recovery as a process concern the experience of moving beyond the mental illness and
growing from it (Onken et al., 2007). Rather overlooked, this underlies a salutogenic view in
which recovery is seen as the passage from a languishing to a flourishing life, which is
oriented towards the search for positive emotions (e.g. happiness, pleasure) and fulfilling
activities and roles (Table I). Therefore, recovery as a process is not only concerned with the
reduction of mental illness but the maximization of positive mental health as well.
Relevance of positive mental health to recovery
Although never recognized as such, the recovery literature has tapped on several
dimensions of subjective well-being that makeup the assessment and diagnosis of positive
mental health (Table I). First, qualitative research and personal accounts draw attention to
consumers’ experiences and aspiration that are aligned with positive mental health. Brown
and Kandirikirira (2007), for instance, found that persons in recovery require and strive for a
positive identity, which reflects ‘‘self acceptance.’’ Individuals also said they require and
seek to engage in meaningful activities and to develop positive relationships with other
people and with their environments, which reflect ‘‘purpose in life,’’ ‘‘positive relations with
others,’’ and ‘‘social acceptance.’’ Narratives of persons in recovery also reveal their need
and aspiration for living in communities where they are seen as more than their illness and
where their contributions are valued, which are signs of ‘‘social integration’’ and ‘‘social
contribution.’’ Persons in recovery also need and strive to manage their lives to stay healthy
and to be resilient to setback, which reflect ‘‘environmental mastery’’ and, to some extent,
‘‘autonomy’’ (i.e. confidence in own opinions and ideas).
Second, several aspects of positive mental health are promoted in recovery interventions.
As an example, supported socialization (Davidson et al., 2004) is an intervention program in
which positive emotions, such as pleasure, fun, and a sense of happiness, are enhanced
through involvement in leisure and social activities. The optimization of psychological
well-being (Table I) is also the target of a recent self-development program (Oades, 2008)
and other treatment programs, e.g. well-being therapy (WBT; Fava and Ruini, 2003) for
persons with depression, and functional cognitive behavioural therapy (Cather et al., 2005)
for those with schizophrenia.
VOL. 10 NO. 1 2011 j JOURNAL OF PUBLIC MENTAL HEALTHj PAGE 61
Measures of positive mental health – emotional, psychological, and social well-being – have
been underutilized in recovery. However, recovery instruments do include some dimensions
aligned with positive mental health. For instance, subjective quality of life, as indexed by life
satisfaction, reflects emotional well-being and has been widely used in clinical practice and
evaluation research. Another example is the Well-Being Scale (WBS; Campbell et al., 2004),
a self-report measure evaluating major subjective recovery outcomes, such as self-esteem,
self-worth, empowerment, self-efficacy, which reflect self-acceptance, environmental
mastery, and autonomy. The Recovery Assessment Scale (RAS; Corrigan et al., 2004) is
another questionnaire that is widely used and relies on five dimensions – personal
confidence and hope, willingness to ask for help, goal and success orientation, reliance on
others, and no domination by symptoms – and those somewhat overlap with purpose in life,
environmental mastery, autonomy, and positive relations with others. The WBS and RAS thus
reflect psychological well-being and, to a greater extent, post-traumatic growth, which
captures the process of thriving in recovery, or becoming better off than beforemental illness
(Onken et al., 2007). More specifically, post-traumatic growth refers to positive shifts in
personality schema and assumptive worlds (Tedeschi et al., 1998) and relies on three
dimensions that overlap with those of psychological well-being. Changes in philosophy
reflect the dimensions of purpose in life and autonomy; changes in perceptions of self are
aligned with environmental mastery, personal growth, and self-acceptance; and changes in
relationships mirror positive relationships with others (Table I). The assessment of
psychological well-being (Ryff and Singer, 1996) has been thus recommended for tracking
changes in growth in longitudinal studies (Joseph and Linley, 2008). However, flourishing
implies thriving but also directs attention to other meaningful experiences, such as positive
emotions and a sense of fulfillment in social life.
In short, recovery has been traditionally defined pathogenically, focusing on psychiatric
symptoms and impairments as outcomes. However, a salutogenic view of recovery has
emerged over the last two decades, as particularly expressed in narratives, focusing on
pleasant and fulfilling experiences despite the presence of mental illness.
Complete mental health recovery
The two continuamodel (Keyes, 2007) incorporates the pathogenic and salutogenic views into
a unitary, complete approach of recovery. From the perspective of complete mental health,
recovery is seen as restoration from mental illness and optimization of positive mental health,
which are viewed as two complementary processes and outcomes. Through restoration,
individuals seek to manage the limitations imposed by mental illness while working toward
symptom alleviation and reduction of impairments as well as healing from the negative social
consequences of the illness (e.g. stigma). Such personal efforts are supported by community
interventions aiming at the reduction of barriers to social exclusion (e.g. stigma, discrimination)
and the provision of accommodations and opportunities for restoring roles and regaining
human and civil rights (Noordsy et al., 2002; Onken et al., 2007). Through optimization,
individuals strive to reach a sense of accomplishment and to experience pleasure and
happiness in life while developing personal and social strengths (Davidson and Strauss, 1992;
Resnick and Rosenheck, 2006). This is supported by community interventions for reducing
poverty, increasing access to services (e.g. education, employment, affordable housing), and
promoting civic engagement andsocial participation (Ware et al., 2007), in linewith capabilities
approaches (Nussbaum, 2000; Sen, 1999). As an example, the Strengths Model (Rapp and
Goscha, 2006) targets the optimization process through the provision of support aimed at the
enhancement of personal and environmental strengths.
Restoration and optimization overlap with key features that underlie consumers-oriented
definitions of recovery (Silverstein and Bellack, 2008), personal recovery (Slade, 2009), and
the experience of recovering ‘‘in’’ mental illness (Davidson and Roe, 2007). What is here new
is that those processes are clearly distinguished, relying on the pathogenic and the
salutogenic views, respectively. The complete view of mental health also draws attention to
the combined use of restoration and optimization strategies, neither one being sufficient to
promote recovery. Although their detailed discussion is beyond the scope of this paper,
PAGE 62 j JOURNAL OF PUBLIC MENTAL HEALTHj VOL. 10 NO. 1 2011
several recovery-oriented programs provide restoration as well as optimization strategies,
such as supported approaches in the areas of employment, housing, and education
(Corrigan et al., 2008), peer support interventions and other specific interventions aligned
with the process of psychiatric rehabilitation (Farkas and Anthony, 2010). All these
interventions assist the person in the pursuit of meaningful goals in life, taking into account
individual preferences and aspirations and tailoring support for the restoration of skills
altered by the illness, the enhancement of personal strengths, and the provision of
opportunities for reducing social exclusion and promoting social inclusion.
Pathways to complete mental health in recovery
Recovery is a non-linear and highly individualized process that is punctuated by progress
and setbacks (Spaniol et al., 2002). Changes in mental health status occur throughout this
journey. As guided by Keyes’s model, a categorical approach here is used to illustrate
pathways in complete mental health over the recovery process. This implies the use of cut-off
points and other specific criteria to classify individuals into distinct and mutually exclusive
groups, as based on their ratings on outcomes of mental illness and positive mental health.
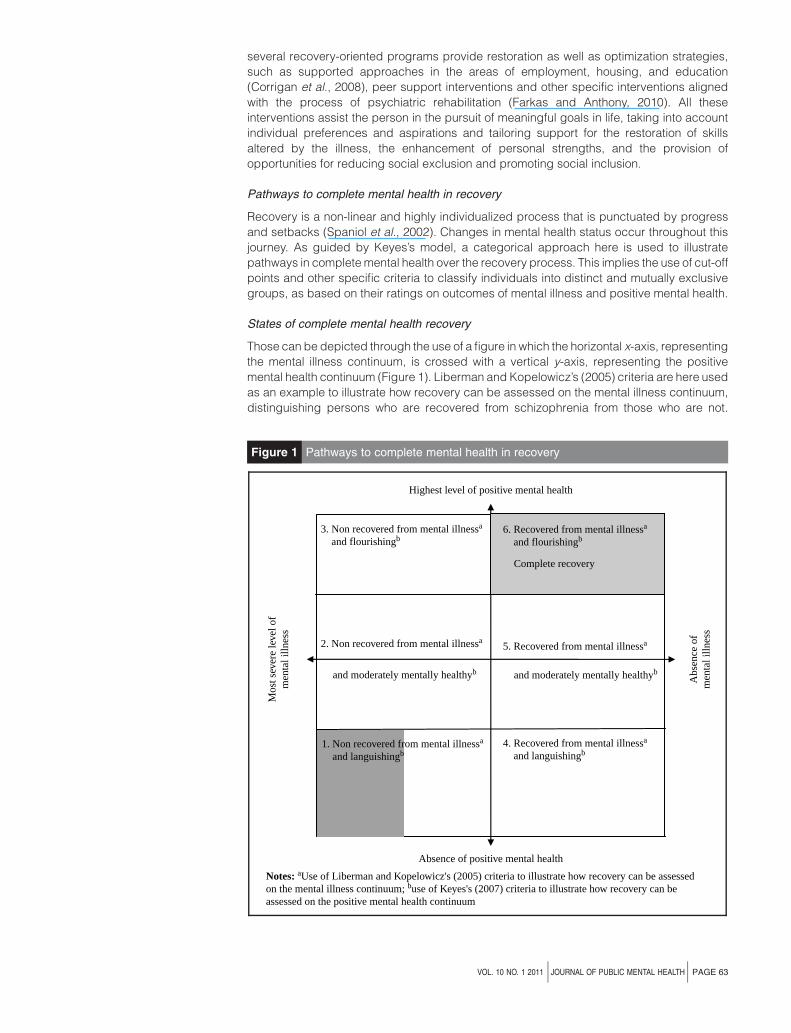
States of complete mental health recovery
Those can be depicted through the use of a figure in which the horizontal x-axis, representing
the mental illness continuum, is crossed with a vertical y-axis, representing the positive
mental health continuum (Figure 1). Liberman and Kopelowicz’s (2005) criteria are here used
as an example to illustrate how recovery can be assessed on the mental illness continuum,
distinguishing persons who are recovered from schizophrenia from those who are not.
Figure 1 Pathways to complete mental health in recovery
3. Non recovered from mental illnessa
and flourishingb
5. Recovered from mental illnessa
4. Recovered from mental illnessa
and languishingb
6. Recovered from mental illnessa
and flourishingb
Complete recovery
and moderately mentally healthyb
2. Non recovered from mental illnessa
and moderately mentally healthyb
1. Non recovered from mental illnessa
and languishingb
Mos
t sev
ere
leve
l of
men
tal i
llnes
s
Abs
ence
of
men
tal i
llnes
s
Absence of positive mental health
Notes: aUse of Liberman and Kopelowicz's (2005) criteria to illustrate how recovery can be assessedon the mental illness continuum; buse of Keyes's (2007) criteria to illustrate how recovery can beassessed on the positive mental health continuum
Highest level of positive mental health
VOL. 10 NO. 1 2011 j JOURNAL OF PUBLIC MENTAL HEALTHj PAGE 63
With regards to the positive mental health continuum, Keyes’s (2005a, 2007) criteria are used
to differentiate individuals who are flourishing, moderately mentally healthy, or languishing.
As shown in Figure 1, the midpoint of the horizontal axis corresponds to moderate levels of
symptoms (i.e. score of four or less on each of the positive and negative symptom items of the
brief psychiatry rating scale) and the restoration of roles in normative settings. Concerning
functional recovery, individuals who are located at the right side of the midpoint hold part- or
full-time competitive jobs whereas those who have other work status are located at the left
(e.g. unemployment, transitional jobs, prevocational training). In addition to work on the
regular market, recovered individuals have to live on their own (without supervision) and to be
involved weekly in social or recreational activities with persons without mental illness, and
those who do not meet these criteria are located at the left. The vertical axis is divided into
three parts corresponding to the states of languishing, moderate, and flourishing mental
health. Six states of complete mental health recovery emerge from the combination of mental
illness and positive mental health outcomes. What follows are plausible thumbnail sketches
of individuals from each of the six categories.
At the bottom left of Figure 1, the shaded area correspond to the initial phase of recovery, being
overwhelmed by the disability (Spaniol et al., 2002). These individuals use ineffective skills to
managemental illness and tend to feel disconnected from the self, others, and the community,
resulting in high levels of psychiatric symptoms and functional deficits. In addition, they are
languishing in life, as they sufferwith the lackof purposeandmeaning in lifeandhavedifficulties
to articulate clear and challenging goals that are anchored in reality. This state is thus
characterized by severe impairments in positive mental health and mental illness.
Among individuals who are not recovered from mental illness, perhaps the transition out of
languishing and movement toward flourishing (see states nos 1, 2, and 3 in Figure 1) comes
with the process of building on some talent or strength, and enabling them to transition from
placing importance on ‘‘who they want to be’’ rather than ‘‘who they are.’’ Activities such as
volunteering or prevocational training may start to bring joy and some realization they have
the potential for contributing to society. The learning of empowerment strategies over the
illness (e.g. coping skills for preventing relapses) also may help individuals to work towards
partial remission of mental illness – moving from the left side to the middle point of the
horizontal axis.
The complete recovery model highlights the need for continued work even after individuals
have recovered in the pathogenic sense, which here ranges from partial to full remission of
mental illness. Among individuals who have recovered from mental illness (see states nos 4,
5, and 6 in Figure 1), level of positive mental health may be implicated in the stability and the
quality of recovery from mental illness. Flourishing in life may reduce the vulnerability to
mental illness, acting as a buffer or a protective factor, whereas languishing may be a risk
factor for relapse and further deterioration in functioning.
Individuals who are recovered from mental illness and flourishing share characteristics with
those who are ‘‘living beyond the disability’’ (Spaniol et al., 2002). This profile corresponds to
the shaded area located at the top right of Figure 1. Individuals who belong to state no. 6 have
reached at least partial remission of mental illness as well as optimal levels of positive mental
health. They look for opportunities to challenge themselves and to reach a sense of serenity
and peace of mind. They hold competitive jobs, have intimate and reciprocal relationships
with others and may be involved in other roles, such as assuming parental responsibilities.
They see their futures as promising and perceive roles and activities as concrete means of
self-actualization as well as ways of contributing society. When deficits are still present,
individuals are well aware of them and know how to best use them while continuing to grow
and to optimize their own potential in the pursuit of challenging goals.
Finally, individuals who belong to state no. 3 are also flourishing even though they are not
engaged in normative activities and have not reached partial symptomatic remission. This
highlights the fact that consumers differ a great deal in their choice of meaningful and
challenging activities, some valuing normative activities while others do not. Several reasons
may account for preferences in non-normative activities (e.g. volunteering, transitional work)
PAGE 64 j JOURNAL OF PUBLIC MENTAL HEALTHj VOL. 10 NO. 1 2011
or occasional self-employment, such as having control over work hours, pacing the re-entry
to the regular market, or prioritizing creative or independent work over other types of jobs
(Brown and Kandirikirira, 2007). Individuals who are flourishing and performing
non-normative activities may see their impairments as parts of a positive identity, through
disability pride. In line with the social model of disability (Sayce, 2000), they may reject the
sick role, perceive social oppression as the main source of disability, advocate for their rights
and entitlements as disabled persons (e.g. housing and benefits services), and request
supportive and socially inclusive measures for living their lives as fully as possible (e.g.
vocational or educational opportunities, peer support, leisure activities). Some of them may
be involved in activism and join other disabled groups in the non-mental health sector for
struggling against social discrimination, which may enhance their sense of social
participation. On the other hand, other individuals belonging to state no. 3 may have built
a sense of positive identity apart from impairments, no longer viewing them as core aspects
of their selves. This may have emerged from the cultivation of personal strengths and positive
assets through volunteering or self-employment, providing a less structured working pattern
that allowed them to flourish alongside other preferential activities, such as leisure or artistic
work (e.g. painting, writing) (Brown and Kandirikirira, 2007).
Limitations
The proposed methodology for assessing pathways to complete mental health in recovery
should be seen as a first attempt to bridge mental illness and positive mental health, and in
need of refinement. Recovery from mental illness has been evaluated through the use of
Liberman and Kopelowicz’s (2005) criteria for three main reasons: both symptomatic and
functional recovery are assessed, clear guidelines are proposed for evaluating each
criterion, and previous research provides support for its discriminant and predictive validity.
However, consumers e.g., (Deegan, 1996) have disputed the re-entry into normal roles (even
on a partial basis) as a requirement for being considered as recovered from mental illness.
For them, roles and activities that bring a sense of satisfaction in life, pleasure and fulfillment
are the crucial issues, whatever the settings in which they are performed. There is also a lack
of consensus about criteria for evaluating partial or complete functional remission in the
scientific community. Beside the need to improve measures of functional recovery
(Mausbach et al., 2009), the debate needs to clarify issues that are related to both the level
(e.g. attempts, progress, and success in normative and non normative activities) and the
breadth of accomplishment in life domains (e.g. work, social activities) (Harvey and Bellack,
2009). For instance, there is considerable variation in the social life of healthy individuals,
which raises the question of the minimal requirement for recovery in this domain.
The three states of positive mental health have been mainly studied in persons with
depression and anxiety disorders. Additional research is required to further validate
the diagnostic criteria in persons with severe mental illness (e.g. schizophrenia, bipolar
disorders) and to specify how long a person has to meet the criteria for being considered as
flourishing, moderately mentally healthy, or languishing. Such refinement involves the
development of observer-rated measures for assessing positive mental health within this
population, making possible comparisons with self-report assessment and being more
suitable for persons with poor insight and severe cognitive deficits. Concerning the
subjective evaluation of positive mental health, new self-report measures are also needed
along with the further validation of available instruments, such as the mental health
continuum-short form (Keyes, 2009a) in which both emotional well-being and positive
functioning are assessed.
Discussion
Unlike previous conceptions, our model proposes to redefine recovery from the complete
view of mental health and introduces positive mental health as an additional outcome of
recovery. Complete mental health recovery relies on two independent but complementary
experiences – restoration from mental illness and optimization of positive mental health –
and each experience is defined as a process and as an outcome. The view of recovery
VOL. 10 NO. 1 2011 j JOURNAL OF PUBLIC MENTAL HEALTHj PAGE 65
‘‘as a process’’ (Davidson and Roe, 2007) is here revisited, making a distinction between
factors and strategies involved in the restoration (e.g. contributing to the alleviation of mental
illness) and optimization (e.g. contributing to the enhancement of positive mental health)
processes. Recovery ‘‘as an outcome’’ (Silverstein and Bellack, 2008) is also revisited,
‘‘having a good or flourishing life’’ being proposed as a sign of recovery and complementing
mental illness outcomes. Therefore, our model does not reject a pathogenic conception of
recovery but views it as insufficient to capture this phenomenon. A salutogenic approach is
also necessary to promote recovery, focusing on the optimal development of strengths and
other characteristics of positive mental health.
How restoration and optimization can contribute to each other deserves more research
attention. One hypothesis concerns resources developed during restoration (e.g.
empowerment over the illness) and the role they may play in promoting positive mental
health, as personal growth is associated with coping successfully with the illness (Onken
et al., 2007). Another hypothesis involves the possibility that a flourishing mental state may
counteract the reappearance of the illness (Keyes, 2007). For instance, acquired skills during
optimization, such as strategies for getting involved in fulfilling activities (Fava and Ruini,
2003), may not only enhance positive mental health but also act as a buffer against mental
illness, potentially decreasing the detrimental effects of stress or illness-related factors (e.g.
substance abuse, poor premorbid history) on mental illness outcomes.
At the practical level, helping people with mental illness to flourish in life requires scholars
and practitioners to better integrate psychiatric treatment and rehabilitation practices
(Corrigan et al., 2008) with those used in mental health promotion (Barry, 2009) and positive
psychology (Seligman and Csikszentmihalyi, 2000). Of note, the enhancement of positive
mental health in persons with mental illness has become an important target of interventions
in mental health promotion (Barry, 2009) and is also addressed in therapeutic approaches
that are directly borrowed or derived from positive psychology (Resnick and Rosenheck,
2006; Slade, 2010). Novel interventions are particularly needed for enhancing not only
emotional well-being and psychological well-being but social well-being as well – a
dimension of positive functioning that has been overlook – and for this purpose, WBT (Fava
and Ruini, 2003) may be used as a guide.
It is plausible that the six proposed states of complete recovery may represent specific
stepping stones, and longitudinal data thus are required to study the evolution of individuals
within each state and among the six states of recovery over time, including the process of
moving from one state to another one. Such line of research also needs to focus on process
variables that are potentially related to the six states, including subjective factors (e.g.
self-redefinition, hope, empowerment, social connectedness) that are here redefined within
the specific contexts of restoration and optimization. For instance, the building of a sense of
empowerment involves the learning of management strategies for preventing mental illness
(e.g. restoration) as well as for experiencing positive emotions and fulfilling activities (e.g.
optimization). However, their detailed discussion is beyond the scope of this paper as well as
how they may interact with other environmental factors, such as social discrimination,
accommodations, or access to affordable housing and other basic resources.
Finally, our model draws attention to individuals who are involved in non-normative activities
and are flourishing. This implies that not only normative but also non-normative activities may
provide opportunities for optimal experiences, which are characterized by full absorption
(awareness of time disappears), high involvement in the task regardless of external rewards
(e.g. paid work), enjoyment, sense of accomplishment, and perceived control over the task
although still viewed as challenging and maximizing competencies (Della Fave and
Massimini, 2004). In particular, more research is needed to further determine the profile of
individuals who perceived optimal experiences in doing non-normative activities (Frese et al.,
2009). A variety of factors may be explored, such as illness-related factors (e.g. premorbid
functioning, cognitive and functional deficits), personal factors (e.g. values, life goals,
meaning of recovery) and how they interact with environmental factors (e.g. support for the
person’s own choice and pursuit of activities).
PAGE 66 j JOURNAL OF PUBLIC MENTAL HEALTHj VOL. 10 NO. 1 2011
Conclusions
The purpose of this paper has been to elevate the place of complete mental health in
redefining the experience of recovery. Restoration from mental illness and optimization of
positive mental health represent the two distinct but complementary processes and
outcomes of recovery. Both the alleviation of mental illness and the promotion of positive
mental health are viewed as necessary to move towards recovery.
References
American Psychiatric Association (1987), Diagnostic and Statistical Manual of Mental Disorders:
DSM-III-R, American Psychiatric Association, Washington, DC.
American Psychiatric Association (2000), Diagnostic and Statistical Manual of Mental Disorders:
DSM-IV-TR, American Psychiatric Association, Washington, DC.
Antonovsky, A. (1979), Health, Stress, and Coping, Jossey-Bass, San Francisco, CA.
Barry, M. (2009), ‘‘Addressing the determinants of positive mental health: concepts, evidence and
practice’’, International Journal of Mental Health Promotion, Vol. 11 No. 3, pp. 4-17.
Brown, W. and Kandirikirira, N. (2007), Recovering Mental Health in Scotland: Report on Narrative
Investigation of Mental Health Recovery, Scottish Recovery Network, Glasgow.
Calabrese, J. and Corrigan, P. (2005), ‘‘Beyond dementia praecox: findings from long-term follow-up
studies of schizophrenia’’, in Ralph, R. and Corrigan, P. (Eds), Recovery in Mental Illness: Broadening
Our Understanding of Wellness, American Psychological Association, Washington, DC.
Campbell, J., Cook, J., Jonikas, J. and Einspahr, K. (2004), Peer Outcomes Protocol Questionnaire,
University of Illinois at Chicago, Chicago, IL.
Cather, C., Penn, D., Otto, M., Yovel, I., Mueser, K. and Goff, D. (2005), ‘‘A pilot study of functional
cognitive behavioral therapy (fCBT) for schizophrenia’’, Schizophrenia Research, Vol. 74 Nos 2-3,
pp. 201-9.
Corrigan, P., Salzer, M., Ralph, R., Sangster, Y. and Keck, L. (2004), ‘‘Examining the factor structure of
the recovery assessment scale’’, Schizophrenia Bulletin, Vol. 30 No. 4, pp. 1034-41.
Corrigan, P., Mueser, K., Bond, G., Drake, R. and Solomon, P. (2008), Principles and Practice of
Psychiatric Rehabilitation: An Empirical Approach, Guilford Press, New York, NY.
Davidson, L. and Roe, D. (2007), ‘‘Recovery from versus recovery in serious mental illness: one strategy
for lessening confusion plaguing recovery’’, Journal of Mental Health, Vol. 16 No. 4, pp. 459-70.
Davidson, L. and Strauss, J. (1992), ‘‘Sense of self in recovery from severe mental illness’’, British
Journal of Medical Psychology, Vol. 65 No. 2, pp. 131-45.
Davidson, L., Shahar, G., Stayner, D., Chinman, M., Rakfeldt, J. and Kraemer Tebes, J. (2004),
‘‘Supported socialization for people with psychiatric disabilities: lessons from a randomized controlled
trial’’, Journal of Community Psychology, Vol. 32 No. 4, pp. 453-77.
Deegan, P. (1988), ‘‘Recovery: the lived experience of rehabilitation’’, Psychosocial Rehabilitation
Journal, Vol. 11 No. 4, pp. 11-19.
Deegan,P. (1996), ‘‘Recoveryas journeyofheart’’,PsychiatricRehabilitationJournal, Vol. 19No.3,pp.91-7.
Della Fave, A. and Massimini, F. (2004), ‘‘Bringing subjectivey into focus: optimal experiences, life
themes, and person-centered rehabilitation’’, in Linley, P. and Joseph, S. (Eds), Positive Psychology in
Practive, Wiley, Hoboken, NJ.
Farkas, M. and Anthony, W. (2010), ‘‘Psychiatric rehabilitation interventions: a review’’, International
Review of Psychiatry, Vol. 22 No. 2, pp. 114-29.
Fava, G. and Ruini, C. (2003), ‘‘Development and characteristics of a well-being enhancing
psychotherapeutic strategy: well-being therapy’’, Journal of Behavior Therapy and Experimental
Psychiatry, Vol. 34 No. 1, pp. 45-63.
Frese, F., Knight, E. and Saks, E. (2009), ‘‘Recovery from schizophrenia: with views of psychiatrists,
psychologists, and others diagnosed with this disorder’’, Schizophrenia Bulletin, Vol. 35 No. 2,
pp. 370-80.
VOL. 10 NO. 1 2011 j JOURNAL OF PUBLIC MENTAL HEALTHj PAGE 67
Harvey, P. and Bellack, A. (2009), ‘‘Toward a terminology for functional recovery in schizophrenia: is
functional remission a viable concept?’’, Schizophrenia Bulletin, Vol. 35 No. 3, pp. 300-6.
Jahoda, M. (1958), Currents Concepts of Positive Mental Health, Basic Books, New York, NY.
Joseph, S. and Linley, P. (2008), Trauma, Recovery, and Growth: Positive Psychological Perspectives on
Post-taumatic Stress, Wiley, Hoboken, NJ.
Kessler, R., Andrews, G., Mroczek, D., Ustun, B. andWittchen, H. (1998), ‘‘The world health organization
composite international diagnostic interview short form (CIDIS-SF)’’, International Journal of Methods in
Psychiatry Research, Vol. 7 No. 4, pp. 171-85.
Keyes, C. (1998), ‘‘Social well-being’’, Social Psychology Quarterly, Vol. 61 No. 2, pp. 121-40.
Keyes, C. (2002), ‘‘The mental health continuum: from languishing to flourishing in life’’, Journal of Health
and Social Behavior, Vol. 43 No. 2, pp. 207-22.
Keyes, C. (2005a), ‘‘Mental illness and/or mental health? Investigating axioms of the complete state
model of health’’, Journal of Consulting and Clinical Psychology, Vol. 73 No. 3, pp. 539-48.
Keyes, C. (2005b), ‘‘The subjective well-being of America’s youth: toward a comprehensive
assessment’’, Adolescent and Family Health, Vol. 4 No. 1, pp. 3-11.
Keyes, C. (2006a), ‘‘Mental health in adolescence: is America’s youth flourishing?’’, American Journal of
Orthopsychiatry, Vol. 76 No. 3, pp. 395-402.
Keyes, C. (2006b), ‘‘Subjective well-being in mental health and human development research
worldwide: an introduction’’, Social Indicators Research, Vol. 77 No. 1, pp. 1-10.
Keyes, C. (2007), ‘‘Promoting and protecting mental health as flourishing’’, American Psychologist,
Vol. 62 No. 2, pp. 95-108.
Keyes, C. (2009a), ‘‘Brief description of the mental health continuum short form (MHC-SF)’’, available at:
www.sociology.emory.edu/ckeyes/ (accessed November 22, 2009).
Keyes, C. (2009b), ‘‘The nature and importance of positive mental health in America’s adolescents’’,
in Gilman, R., Huebner, E. and Furlong, M. (Eds), Handbook of Positive Psychology in Schools,
Routledge, New York, NY.
Keyes, C., Shmotkin, D. and Ryff, C. (2002), ‘‘Optimizing well-being: the empirical encounter of two
traditions’’, Journal of Personality and Social Psychology, Vol. 82 No. 6, pp. 1007-22.
Liberman, R. and Kopelowicz, A. (2005), ‘‘Recovery from schizophrenia: a criterion-based definition’’,
in Ralph, R. and Corrigan, P. (Eds), Recovery in Mental Illness: Broadening Our Understanding of
Wellness, American Psychological Association, Washington, DC.
Mausbach, B., Moore, R., Bowie, C., Cardenas, V. and Patterson, T. (2009), ‘‘A review of instruments for
measuring functional recovery in those diagnosedwith psychosis’’, Schizophrenia Bulletin, Vol. 35 No. 2,
pp. 307-18.
Noordsy, D., Torrey, W., Mueser, K., Mead, S., O’Keefe, C. and Fox, L. (2002), ‘‘Recovery from severe
mental illness: an intrapersonal and functional outcome definition’’, International Review of Psychiatry,
Vol. 14 No. 4, pp. 318-26.
Nussbaum, M. (2000), The Capabilities Approach, University of Cmabridge Press, Cambridge.
Oades, L. (2008), Helping People with Mental Illness Flourish Through Self-development Program,
Illawarra Institute for Mental Health, University of Wollongong, Wollongong, available at: http://media.
uow.edu.au/releases/UOW042499.html (accessed November 22, 2009).
Onken, S., Craig, C., Ridgway, P., Ralph, R. and Cook, J. (2007), ‘‘An analysis of the definitions and
elements of recovery: a review of the literature’’, Psychiatric Rehabilitation Journal, Vol. 31 No. 1,
pp. 9-22.
Rapp, C. and Goscha, R. (2006), The Strengths Model: Case Management with People with Psychiatric
Disabilities, Oxford University Press, New York, NY.
Resnick, S. and Rosenheck, R. (2006), ‘‘Recovery and positive psychology: parallel themes and
potential synergies’’, Psychiatric Services, Vol. 57 No. 1, pp. 120-2.
Ridgway, P. (2001), ‘‘Restorying psychiatric disability: learning from first person narratives’’, Psychiatric
Rehabilitation Journal, Vol. 24 No. 4, pp. 343-53.
PAGE 68 j JOURNAL OF PUBLIC MENTAL HEALTHj VOL. 10 NO. 1 2011
Ryan, R. and Deci, E. (2001), ‘‘On happiness and human potentials: a review of research on hedonic and
eudaimonic well-being’’, in Fishe, S. (Ed.), Annual Review of Psychopathology, Annuals Reviews, Palo
Alto, CA.
Ryff, C. and Singer, B. (1996), ‘‘Psychological well-being: meaning, measurement, and implications for
psychotherapy research’’, Psychotherapy and Psychosomatics, Vol. 65 No. 1, pp. 14-23.
Sayce, L. (2000), From Psychiatric Patient to Citizen: Overcoming Discrimination and Social Exclusion,
Macmillan, London.
Seligman, M. and Csikszentmihalyi, M. (2000), ‘‘Positive psychology: an introduction’’, American
Psychologist, Vol. 55 No. 1, pp. 5-14.
Sen, A. (1999), Development as Freedom, Anchor Books, New York, NY.
Silverstein, S. and Bellack, A. (2008), ‘‘A scientific agenda for the concept of recovery as it applies to
schizophrenia’’, Clinical Psychology Review, Vol. 28 No. 7, pp. 1108-24.
Slade, M. (2009), Personal Recovery and Mental Illness: A Guide for Mental Health Professionals,
Cambridge University Press, Cambridge.
Slade, M. (2010), ‘‘Mental illness and well-being: the central importance of positive psychology and
recovery approaches’’, BMC Health Services Research, Vol. 10, available at: www.biomedcentral/1472-
6963310/26
Slade, M., Amering, M. andOades, L. (2008), ‘‘Recovery: an international perspective’’, Epidemiologia e
Psichiatria Sociale, Vol. 17 No. 2, pp. 128-37.
Spaniol, L. and Koehler, M. (1994), The Experience of Recovery, Sargent College of Health and
Rehabilitation Sciences, Center for Psychiatric Rehabilitation, Boston University, Boston, MA.
Spaniol, L., Wewiorski, N., Gagne, C. and Anthony, W. (2002), ‘‘The process of recovery from
schizophrenia’’, International Review of Psychiatry, Vol. 14 No. 4, pp. 327-36.
Tedeschi, R., Park, C. and Calhoun, L. (1998), Posttraumatic Growth: Positive Changes in the Aftermath
of Crisis, Lawrence Erlbaum, Mahwah, NJ.
Tennant, R., Hiller, L., Fishwick, R., Platt, S., Joseph, S., Weich, S., Parkinson, J., Secker, J. and
Stewart-Brown, S. (2007), ‘‘The Warwick-Edinburg mental well-being scale (WEMWBS): development
and UK validation’’, Health and Quality of Life Outcomes, Vol. 63 No. 5, available at: www.hqlo.com/
content/5/1/63
Ware, N., Hopper, K., Tugenberg, T., Dickey, B. and Fisher, D. (2007), ‘‘Connectedness and citizenship:
redefining social integration’’, Psychiatric Services, Vol. 58 No. 4, pp. 469-74.
(The) World Health Organization (1948), World Health Organization Constitution: Basic Documents,
The World Health Organization, Geneva.
(The) World Health Organization (2005), Promoting Mental Health: Concepts, Emerging Evidence,
Practice, The World Health Organization, Geneva.
Corresponding author
Helene L. Provencher can be contacted at: [email protected]
To purchase reprints of this article please e-mail: [email protected]
Or visit our web site for further details: www.emeraldinsight.com/reprints
VOL. 10 NO. 1 2011 j JOURNAL OF PUBLIC MENTAL HEALTHj PAGE 69
Related Documents











