Comparison of Complete Versus Incomplete Stent Frame Expansion After Transcatheter Aortic Valve Implantation With Medtronic CoreValve Bioprosthesis Hasan Jilaihawi, MD a , Derek Chin, MD b , Tomasz Spyt, MD b , Mohamed Jeilan, MD b , Mariuca Vasa-Nicotera, MD b , Noor Mohamed, MD b , Johan Bence, MD b , Elaine Logtens, RN b , and Jan Kovac, MD b, * We sought to determine the significance of incomplete stent frame expansion after trans- catheter aortic valve implantation with the Medtronic-CoreValve device. Incomplete cor- onary stent expansion is a well-described phenomenon. Transcatheter valves are mounted on stents; however, the incidence of incomplete stent expansion after transcatheter aortic valve implantation, its sequelae and predictors are poorly elucidated. The 18Fr CoreValve revalving system was used to treat anatomically and clinically suitable patients with severe calcific aortic stenosis. The postdeployment stent dimensions were measured on fluoro- scopic images at multiple levels of the stent frame. Incomplete expansion at each was defined as <100% expected and complete expansion as >100%. These parameters were correlated to the hemodynamic and clinical end points. A total of 50 consecutive patients underwent transcatheter aortic valve implantation with the Medtronic-CoreValve at a single center from January 2007 to December 2008. For the inflow portion, incomplete expansion was seen in 54% of patients and was unrelated to the aortic valve area, peak or mean aortic valve gradients, or measures of aortic regurgitation, although it was paradox- ically associated with a lower incidence of prosthesis–patient mismatch. Incomplete ex- pansion of the constrained portion was seen in 62% of the patients and displayed a trend toward a greater incidence of aortic regurgitation grade 2 or greater, although this was rare. Incomplete expansion of the Medtronic CoreValve stent frame is common. For the most part, valvular hemodynamic function was satisfactory, regardless of the degree of expan- sion of the stent frame that carries it and a strategy of reluctant postdilation in the context of incomplete stent frame expansion was supported. © 2011 Elsevier Inc. All rights reserved. (Am J Cardiol 2011;107:1830 –1837) Incomplete coronary stent expansion is a well-described phenomenon, has a greater likelihood in calcified lesions and can result in dramatically adverse sequelae such as restenosis and stent thrombosis. 1 Transcatheter aortic valve implantation (TAVI) has shown great promise in the treat- ment of severe aortic stenosis in patients regarded at high risk from conventional surgery. 2–7 Transcatheter valves are mounted on stents. The Medtronic-CoreValve stented bio- prosthesis (Medtronic Inc., Minneapolis, Minnesota) has a relatively long self-expanding stent frame and has the po- tential for incomplete expansion, particularly in the setting of severe calcific aortic stenosis. Moreover, incomplete ex- pansion could theoretically have a bearing on the leaflet function of the valve it carries. We sought to describe this phenomenon and assess its hemodynamic and early clin- ical significance in patients undergoing TAVI with the CoreValve bioprosthesis. Methods The clinical and anatomic selection criteria were in ac- cordance with the published investigational study for the third-generation (18Fr) CoreValve device. 5 The patients were recruited from a single center and underwent TAVI with the CoreValve bioprosthesis by way of a transfemoral route. All patients had severe calcific aortic stenosis (aortic valve area [AVA] 1 cm 2 or body surface area-indexed AVA 0.6 cm 2 /m 2 ). They were symptomatic, considered at high risk of, or inoperable by, conventional surgery, and had annuli of 20 to 27 mm and suitable peripheral vasculature (iliofemoral diameter 6 mm). Patients with annuli of 20 to 23 mm received a 26-mm prosthesis; those with annuli of 23 to 27 mm received a 29-mm prosthesis. The device was implanted as previously described. 5 The postdeployment stent dimensions were assessed in the optimal angiographic plane for implantation, which dis- played the 3 aortic valve sinuses in line and, in turn, min- imized the possibility of foreshortening during measure- ments. The stent measurements were made at the inflow level (level A) and at the level of the most constrained portion (level B, close to the level of central coaptation of the bioprosthetic leaflets, approximately 20 to 22 mm from the inflow margin of the stent-frame; Figure 1). Measure- a Cedars-Sinai Heart Institute, Los Angeles, California; and b Glenfield Hospital, Leicester, United Kingdom. Manuscript received July 29, 2010; manuscript received and accepted February 6, 2011. *Corresponding author: Tel: (44) 11-6250-2780; fax: (44) 11- 6250-2405. E-mail address: [email protected] (J. Kovac). 0002-9149/11/$ – see front matter © 2011 Elsevier Inc. All rights reserved. www.ajconline.org doi:10.1016/j.amjcard.2011.02.317

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Hm
6
0d
Comparison of Complete Versus Incomplete Stent FrameExpansion After Transcatheter Aortic Valve Implantation With
Medtronic CoreValve Bioprosthesis
Hasan Jilaihawi, MDa, Derek Chin, MDb, Tomasz Spyt, MDb, Mohamed Jeilan, MDb,Mariuca Vasa-Nicotera, MDb, Noor Mohamed, MDb, Johan Bence, MDb, Elaine Logtens, RNb,
and Jan Kovac, MDb,*
We sought to determine the significance of incomplete stent frame expansion after trans-catheter aortic valve implantation with the Medtronic-CoreValve device. Incomplete cor-onary stent expansion is a well-described phenomenon. Transcatheter valves are mountedon stents; however, the incidence of incomplete stent expansion after transcatheter aorticvalve implantation, its sequelae and predictors are poorly elucidated. The 18Fr CoreValverevalving system was used to treat anatomically and clinically suitable patients with severecalcific aortic stenosis. The postdeployment stent dimensions were measured on fluoro-scopic images at multiple levels of the stent frame. Incomplete expansion at each wasdefined as <100% expected and complete expansion as >100%. These parameters werecorrelated to the hemodynamic and clinical end points. A total of 50 consecutive patientsunderwent transcatheter aortic valve implantation with the Medtronic-CoreValve at asingle center from January 2007 to December 2008. For the inflow portion, incompleteexpansion was seen in 54% of patients and was unrelated to the aortic valve area, peak ormean aortic valve gradients, or measures of aortic regurgitation, although it was paradox-ically associated with a lower incidence of prosthesis–patient mismatch. Incomplete ex-pansion of the constrained portion was seen in 62% of the patients and displayed a trendtoward a greater incidence of aortic regurgitation grade 2 or greater, although this was rare.Incomplete expansion of the Medtronic CoreValve stent frame is common. For the mostpart, valvular hemodynamic function was satisfactory, regardless of the degree of expan-sion of the stent frame that carries it and a strategy of reluctant postdilation in the contextof incomplete stent frame expansion was supported. © 2011 Elsevier Inc. All rights
reserved. (Am J Cardiol 2011;107:1830–1837)A
Incomplete coronary stent expansion is a well-describedphenomenon, has a greater likelihood in calcified lesionsand can result in dramatically adverse sequelae such asrestenosis and stent thrombosis.1 Transcatheter aortic valveimplantation (TAVI) has shown great promise in the treat-ment of severe aortic stenosis in patients regarded at highrisk from conventional surgery.2–7 Transcatheter valves aremounted on stents. The Medtronic-CoreValve stented bio-prosthesis (Medtronic Inc., Minneapolis, Minnesota) has arelatively long self-expanding stent frame and has the po-tential for incomplete expansion, particularly in the settingof severe calcific aortic stenosis. Moreover, incomplete ex-pansion could theoretically have a bearing on the leafletfunction of the valve it carries. We sought to describe thisphenomenon and assess its hemodynamic and early clin-ical significance in patients undergoing TAVI with theCoreValve bioprosthesis.
aCedars-Sinai Heart Institute, Los Angeles, California; and bGlenfieldospital, Leicester, United Kingdom. Manuscript received July 29, 2010;anuscript received and accepted February 6, 2011.
*Corresponding author: Tel: (�44) 11-6250-2780; fax: (�44) 11-250-2405.
E-mail address: [email protected] (J. Kovac).
002-9149/11/$ – see front matter © 2011 Elsevier Inc. All rights reserved.oi:10.1016/j.amjcard.2011.02.317
Methods
The clinical and anatomic selection criteria were in ac-cordance with the published investigational study for thethird-generation (18Fr) CoreValve device.5 The patientswere recruited from a single center and underwent TAVIwith the CoreValve bioprosthesis by way of a transfemoralroute. All patients had severe calcific aortic stenosis (aorticvalve area [AVA] �1 cm2 or body surface area-indexed
VA �0.6 cm2/m2). They were symptomatic, considered athigh risk of, or inoperable by, conventional surgery, and hadannuli of 20 to 27 mm and suitable peripheral vasculature(iliofemoral diameter �6 mm). Patients with annuli of 20 to23 mm received a 26-mm prosthesis; those with annuli of 23to 27 mm received a 29-mm prosthesis. The device wasimplanted as previously described.5
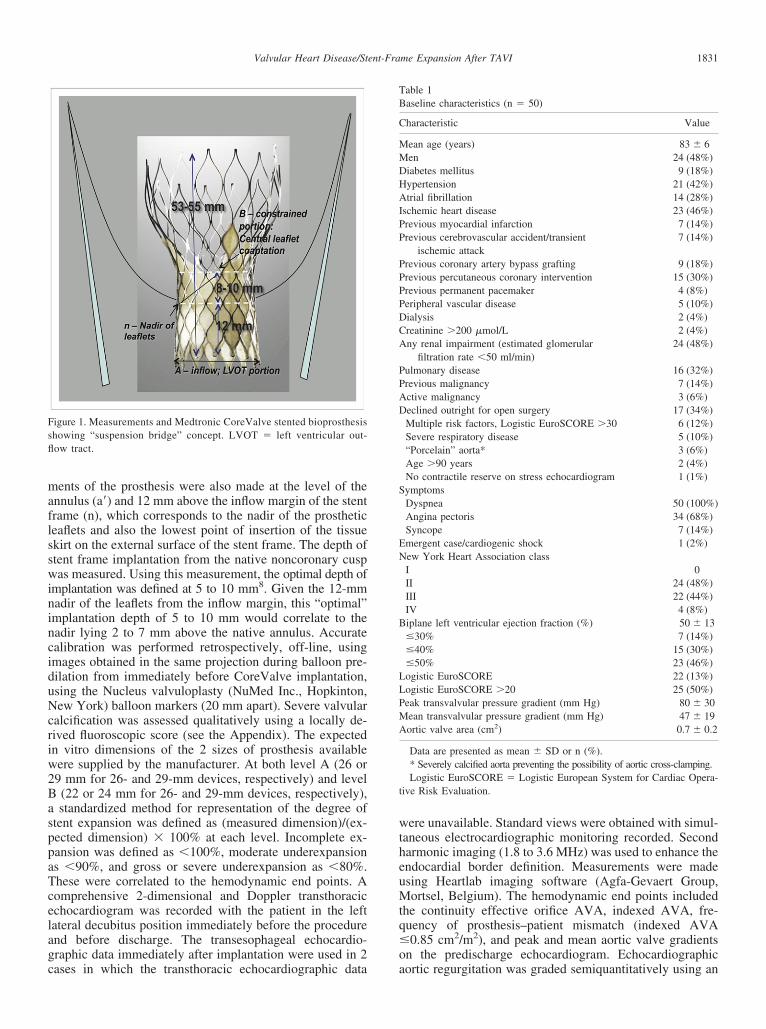
The postdeployment stent dimensions were assessed inthe optimal angiographic plane for implantation, which dis-played the 3 aortic valve sinuses in line and, in turn, min-imized the possibility of foreshortening during measure-ments. The stent measurements were made at the inflowlevel (level A) and at the level of the most constrainedportion (level B, close to the level of central coaptation ofthe bioprosthetic leaflets, approximately 20 to 22 mm from
the inflow margin of the stent-frame; Figure 1). Measure-www.ajconline.org
ninciduNcriw2BasppaTcelagc
wtheuMtq�
MM
A
PPAD
S
EN
B
LLPMA
1831Valvular Heart Disease/Stent-Frame Expansion After TAVI
ments of the prosthesis were also made at the level of theannulus (a=) and 12 mm above the inflow margin of the stentframe (n), which corresponds to the nadir of the prostheticleaflets and also the lowest point of insertion of the tissueskirt on the external surface of the stent frame. The depth ofstent frame implantation from the native noncoronary cuspwas measured. Using this measurement, the optimal depth ofimplantation was defined at 5 to 10 mm8. Given the 12-mmadir of the leaflets from the inflow margin, this “optimal”mplantation depth of 5 to 10 mm would correlate to theadir lying 2 to 7 mm above the native annulus. Accuratealibration was performed retrospectively, off-line, usingmages obtained in the same projection during balloon pre-ilation from immediately before CoreValve implantation,sing the Nucleus valvuloplasty (NuMed Inc., Hopkinton,ew York) balloon markers (20 mm apart). Severe valvular
alcification was assessed qualitatively using a locally de-ived fluoroscopic score (see the Appendix). The expectedn vitro dimensions of the 2 sizes of prosthesis availableere supplied by the manufacturer. At both level A (26 or9 mm for 26- and 29-mm devices, respectively) and level(22 or 24 mm for 26- and 29-mm devices, respectively),standardized method for representation of the degree of
tent expansion was defined as (measured dimension)/(ex-ected dimension) � 100% at each level. Incomplete ex-ansion was defined as �100%, moderate underexpansions �90%, and gross or severe underexpansion as �80%.hese were correlated to the hemodynamic end points. Aomprehensive 2-dimensional and Doppler transthoracicchocardiogram was recorded with the patient in the leftateral decubitus position immediately before the procedurend before discharge. The transesophageal echocardio-raphic data immediately after implantation were used in 2
Figure 1. Measurements and Medtronic CoreValve stented bioprosthesisshowing “suspension bridge” concept. LVOT � left ventricular out-flow tract.
ases in which the transthoracic echocardiographic data
ere unavailable. Standard views were obtained with simul-aneous electrocardiographic monitoring recorded. Secondarmonic imaging (1.8 to 3.6 MHz) was used to enhance thendocardial border definition. Measurements were madesing Heartlab imaging software (Agfa-Gevaert Group,ortsel, Belgium). The hemodynamic end points included
he continuity effective orifice AVA, indexed AVA, fre-uency of prosthesis–patient mismatch (indexed AVA0.85 cm2/m2), and peak and mean aortic valve gradients
on the predischarge echocardiogram. Echocardiographic
Table 1Baseline characteristics (n � 50)
Characteristic Value
ean age (years) 83 � 6en 24 (48%)
Diabetes mellitus 9 (18%)Hypertension 21 (42%)Atrial fibrillation 14 (28%)Ischemic heart disease 23 (46%)Previous myocardial infarction 7 (14%)Previous cerebrovascular accident/transient
ischemic attack7 (14%)
Previous coronary artery bypass grafting 9 (18%)Previous percutaneous coronary intervention 15 (30%)Previous permanent pacemaker 4 (8%)Peripheral vascular disease 5 (10%)Dialysis 2 (4%)Creatinine �200 �mol/L 2 (4%)
ny renal impairment (estimated glomerularfiltration rate �50 ml/min)
24 (48%)
ulmonary disease 16 (32%)revious malignancy 7 (14%)ctive malignancy 3 (6%)eclined outright for open surgery 17 (34%)Multiple risk factors, Logistic EuroSCORE �30 6 (12%)Severe respiratory disease 5 (10%)“Porcelain” aorta* 3 (6%)Age �90 years 2 (4%)No contractile reserve on stress echocardiogram 1 (1%)ymptomsDyspnea 50 (100%)Angina pectoris 34 (68%)Syncope 7 (14%)mergent case/cardiogenic shock 1 (2%)ew York Heart Association classI 0II 24 (48%)III 22 (44%)IV 4 (8%)iplane left ventricular ejection fraction (%) 50 � 13�30% 7 (14%)�40% 15 (30%)�50% 23 (46%)ogistic EuroSCORE 22 (13%)ogistic EuroSCORE �20 25 (50%)eak transvalvular pressure gradient (mm Hg) 80 � 30ean transvalvular pressure gradient (mm Hg) 47 � 19ortic valve area (cm2) 0.7 � 0.2
Data are presented as mean � SD or n (%).* Severely calcified aorta preventing the possibility of aortic cross-clamping.Logistic EuroSCORE � Logistic European System for Cardiac Opera-
tive Risk Evaluation.
aortic regurgitation was graded semiquantitatively using an
etciln(
ptctamM
P
1832 The American Journal of Cardiology (www.ajconline.org)
established integrative approach with parasternal long-axisview observations9: none (grade 0), trivial or mild (grade1�), moderate (grade 2�), moderate to severe (grade 3�),and severe (grade 4�). Paraprosthetic or transvalvular aor-tic regurgitation (AR) were determined qualitatively at eachpoint.
Statistical analysis was done using the Statistical Pack-age for Social Sciences software (SPSS, Chicago, Illinois).Differences were assessed using a paired sample t test fornormally distributed data or Wilcoxon signed rank 2-relatedsamples analyses for other distributions. For comparison ofindependent nonparametric variables, a chi-square statisticwas used and for independent normally distributed vari-ables, an independent samples t test. For correlations, Pear-son’s bivariate analysis with a 2-tailed test for significancewas used for parametric variables and Spearman’s rho cor-relation for nonparametric variables. Factors related uni-variately to incomplete stent expansion were studied in amultivariate binary logistic regression model, where appro-priate. We assessed the influence of the degree of stent-frame expansion on the echocardiographic, fluoroscopic,and cardiac catheter parameters described in the previousparagraphs.
Results
From January 2007 to December 2008, 50 patients un-
Table 2Hemodynamic and functional data
Variable Before After p Value
Peak aortic gradient (mm Hg) 81 � 30 16 � 6 �0.001Mean aortic gradient (mm Hg) 48 � 18 8 � 3 �0.001Aortic valve area (cm2) 0.7 � 0.2 1.7 � 0.5 �0.001Aortic valve area indexed to body
surface area (cm2/m2)0.4 � 0.1 1.0 � 0.3 �0.001
rosthetic aortic valve areaindexed to body surface area(cm2/m2)
�0.85 — 16 (32%) —�0.8 — 14 (28%) —�0.65 — 1 (2%) —
AR grade 0.1960 14 (28%) 8 (16%)1 32 (64%) 38 (76%)2 3 (6%) 2 (4%)3 1 (2%) 1 (2%)4 0 1 (2%)
Biplane left ventricular ejectionfraction (%)
50 � 13 56 � 9 0.001
�30% 7 (14%) 0 0.008�40% 15 (30%) 6 (12%) 0.005�50% 23 (46%) 12 (24%) 0.005
New York Heart Associationclass
�0.001
I 0 27 (54%)II 24 (48%) 16 (32%)III 22 (44%) 2 (4%)IV 4 (8%) 0
Data are presented as mean � SD or n (%).
derwent TAVI. The baseline demographics are listed in f
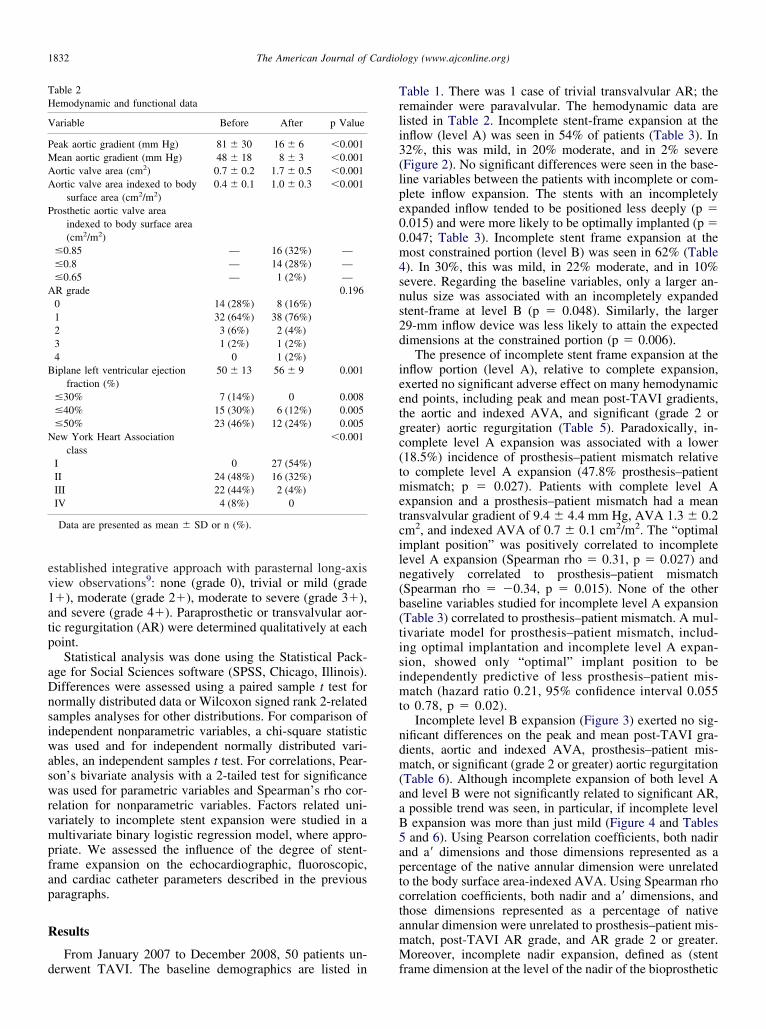
Table 1. There was 1 case of trivial transvalvular AR; theremainder were paravalvular. The hemodynamic data arelisted in Table 2. Incomplete stent-frame expansion at theinflow (level A) was seen in 54% of patients (Table 3). In32%, this was mild, in 20% moderate, and in 2% severe(Figure 2). No significant differences were seen in the base-line variables between the patients with incomplete or com-plete inflow expansion. The stents with an incompletelyexpanded inflow tended to be positioned less deeply (p �0.015) and were more likely to be optimally implanted (p �0.047; Table 3). Incomplete stent frame expansion at themost constrained portion (level B) was seen in 62% (Table4). In 30%, this was mild, in 22% moderate, and in 10%severe. Regarding the baseline variables, only a larger an-nulus size was associated with an incompletely expandedstent-frame at level B (p � 0.048). Similarly, the larger29-mm inflow device was less likely to attain the expecteddimensions at the constrained portion (p � 0.006).
The presence of incomplete stent frame expansion at theinflow portion (level A), relative to complete expansion,exerted no significant adverse effect on many hemodynamicend points, including peak and mean post-TAVI gradients,the aortic and indexed AVA, and significant (grade 2 orgreater) aortic regurgitation (Table 5). Paradoxically, in-complete level A expansion was associated with a lower(18.5%) incidence of prosthesis–patient mismatch relativeto complete level A expansion (47.8% prosthesis–patientmismatch; p � 0.027). Patients with complete level Axpansion and a prosthesis–patient mismatch had a meanransvalvular gradient of 9.4 � 4.4 mm Hg, AVA 1.3 � 0.2m2, and indexed AVA of 0.7 � 0.1 cm2/m2. The “optimalmplant position” was positively correlated to incompleteevel A expansion (Spearman rho � 0.31, p � 0.027) andegatively correlated to prosthesis–patient mismatchSpearman rho � �0.34, p � 0.015). None of the other
baseline variables studied for incomplete level A expansion(Table 3) correlated to prosthesis–patient mismatch. A mul-tivariate model for prosthesis–patient mismatch, includ-ing optimal implantation and incomplete level A expan-sion, showed only “optimal” implant position to beindependently predictive of less prosthesis–patient mis-match (hazard ratio 0.21, 95% confidence interval 0.055to 0.78, p � 0.02).
Incomplete level B expansion (Figure 3) exerted no sig-nificant differences on the peak and mean post-TAVI gra-dients, aortic and indexed AVA, prosthesis–patient mis-match, or significant (grade 2 or greater) aortic regurgitation(Table 6). Although incomplete expansion of both level Aand level B were not significantly related to significant AR,a possible trend was seen, in particular, if incomplete levelB expansion was more than just mild (Figure 4 and Tables5 and 6). Using Pearson correlation coefficients, both nadirand a= dimensions and those dimensions represented as aercentage of the native annular dimension were unrelatedo the body surface area-indexed AVA. Using Spearman rhoorrelation coefficients, both nadir and a= dimensions, andhose dimensions represented as a percentage of nativennular dimension were unrelated to prosthesis–patient mis-atch, post-TAVI AR grade, and AR grade 2 or greater.oreover, incomplete nadir expansion, defined as (stent
rame dimension at the level of the nadir of the bioprosthetic
n of ste
B
1833Valvular Heart Disease/Stent-Frame Expansion After TAVI
leaflets/native annular dimension) �1, did not correlatewith prosthesis–patient mismatch, post-TAVI AR grade, or
Figure 2. Range of expansio
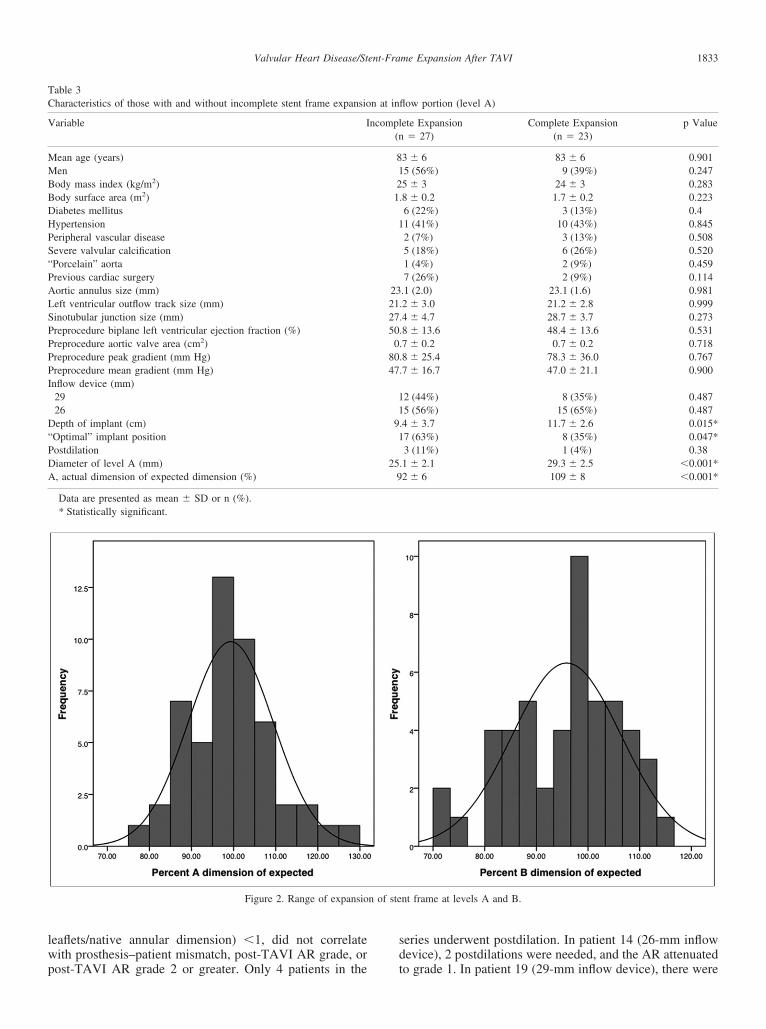
Table 3Characteristics of those with and without incomplete stent frame expansio
Variable I
Mean age (years)MenBody mass index (kg/m2)
ody surface area (m2)Diabetes mellitusHypertensionPeripheral vascular diseaseSevere valvular calcification“Porcelain” aortaPrevious cardiac surgeryAortic annulus size (mm)Left ventricular outflow track size (mm)Sinotubular junction size (mm)Preprocedure biplane left ventricular ejection fraction (%)Preprocedure aortic valve area (cm2)Preprocedure peak gradient (mm Hg)Preprocedure mean gradient (mm Hg)Inflow device (mm)
2926
Depth of implant (cm)“Optimal” implant positionPostdilationDiameter of level A (mm)A, actual dimension of expected dimension (%)
Data are presented as mean � SD or n (%).* Statistically significant.
post-TAVI AR grade 2 or greater. Only 4 patients in the
series underwent postdilation. In patient 14 (26-mm inflowdevice), 2 postdilations were needed, and the AR attenuated
nt frame at levels A and B.
flow portion (level A)
ete Expansion� 27)
Complete Expansion(n � 23)
p Value
3 � 6 83 � 6 0.9015 (56%) 9 (39%) 0.2475 � 3 24 � 3 0.283.8 � 0.2 1.7 � 0.2 0.2236 (22%) 3 (13%) 0.41 (41%) 10 (43%) 0.8452 (7%) 3 (13%) 0.5085 (18%) 6 (26%) 0.5201 (4%) 2 (9%) 0.4597 (26%) 2 (9%) 0.114.1 (2.0) 23.1 (1.6) 0.981.2 � 3.0 21.2 � 2.8 0.999.4 � 4.7 28.7 � 3.7 0.273.8 � 13.6 48.4 � 13.6 0.531.7 � 0.2 0.7 � 0.2 0.718.8 � 25.4 78.3 � 36.0 0.767.7 � 16.7 47.0 � 21.1 0.900
2 (44%) 8 (35%) 0.4875 (56%) 15 (65%) 0.487
.4 � 3.7 11.7 � 2.6 0.015*7 (63%) 8 (35%) 0.047*3 (11%) 1 (4%) 0.38
.1 � 2.1 29.3 � 2.5 �0.001*2 � 6 109 � 8 �0.001*
n at in
ncompl(n
8121
1
232127500
8047
11
91
259
to grade 1. In patient 19 (29-mm inflow device), there were
fwc
B
S“PALSPPPPI
D“PDB
TDi
P
PA
1834 The American Journal of Cardiology (www.ajconline.org)
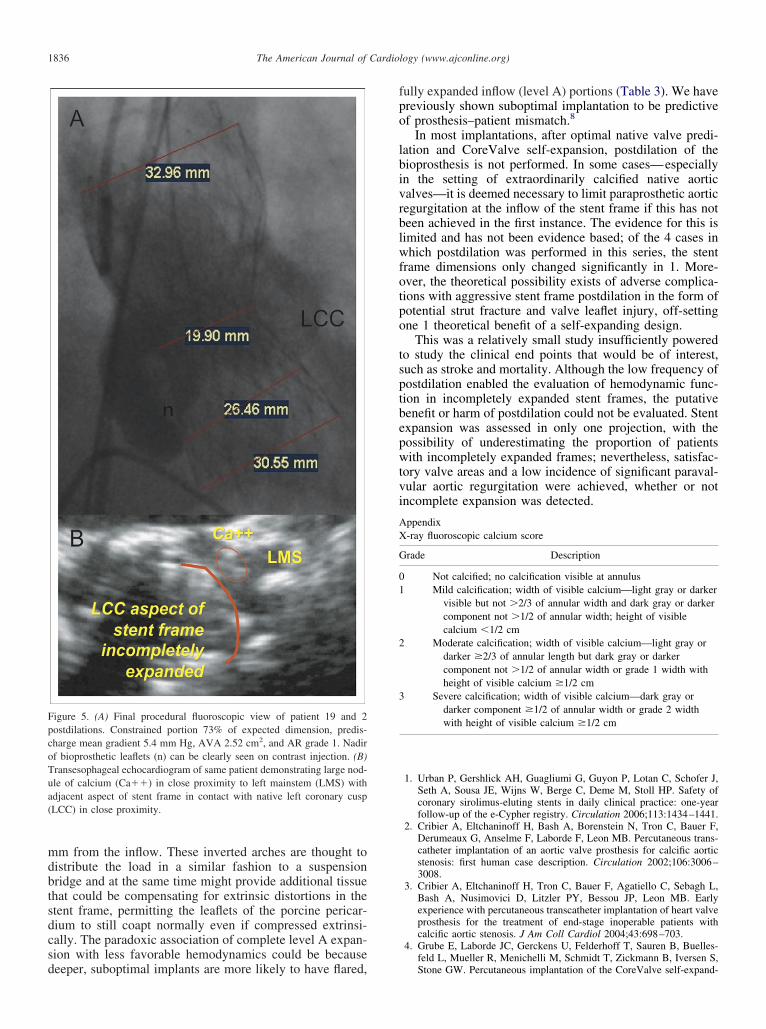
also 2 postdilations and the AR remained at grade 2 on thefinal aortogram but was seen to attenuate to grade 1 on thepredischarge echocardiogram. Additional postdilation wasnot performed, because a large nodule of calcium was ob-served close to the left mainstem (Figure 5). Patient 36underwent 1 postdilation, and the AR attenuated to grade 1.Patient 34 required a “bail-out” 29-mm inflow valve-in-valve after a very deep first implant with grade 4 AR; theAR attenuated to grade 1 after the second valve but the levelA and B dimensions were unchanged by 2 subsequent
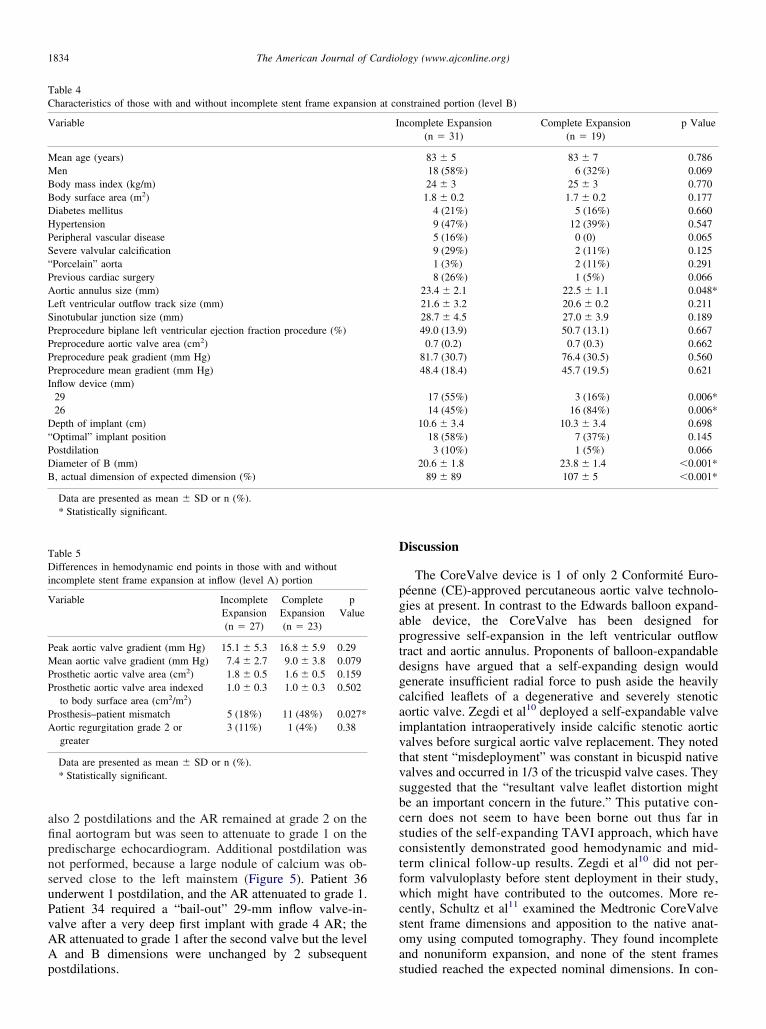
Table 4Characteristics of those with and without incomplete stent frame expansio
Variable
Mean age (years)MenBody mass index (kg/m)
ody surface area (m2)Diabetes mellitusHypertensionPeripheral vascular disease
evere valvular calcificationPorcelain” aortarevious cardiac surgeryortic annulus size (mm)eft ventricular outflow track size (mm)inotubular junction size (mm)reprocedure biplane left ventricular ejection fraction procedure (%)reprocedure aortic valve area (cm2)reprocedure peak gradient (mm Hg)reprocedure mean gradient (mm Hg)nflow device (mm)2926epth of implant (cm)
Optimal” implant positionostdilationiameter of B (mm), actual dimension of expected dimension (%)
Data are presented as mean � SD or n (%).* Statistically significant.
able 5ifferences in hemodynamic end points in those with and without
ncomplete stent frame expansion at inflow (level A) portion
Variable IncompleteExpansion(n � 27)
CompleteExpansion(n � 23)
pValue
Peak aortic valve gradient (mm Hg) 15.1 � 5.3 16.8 � 5.9 0.29Mean aortic valve gradient (mm Hg) 7.4 � 2.7 9.0 � 3.8 0.079Prosthetic aortic valve area (cm2) 1.8 � 0.5 1.6 � 0.5 0.159
rosthetic aortic valve area indexedto body surface area (cm2/m2)
1.0 � 0.3 1.0 � 0.3 0.502
rosthesis–patient mismatch 5 (18%) 11 (48%) 0.027*ortic regurgitation grade 2 orgreater
3 (11%) 1 (4%) 0.38
Data are presented as mean � SD or n (%).* Statistically significant.
postdilations.
Discussion
The CoreValve device is 1 of only 2 Conformité Euro-péenne (CE)-approved percutaneous aortic valve technolo-gies at present. In contrast to the Edwards balloon expand-able device, the CoreValve has been designed forprogressive self-expansion in the left ventricular outflowtract and aortic annulus. Proponents of balloon-expandabledesigns have argued that a self-expanding design wouldgenerate insufficient radial force to push aside the heavilycalcified leaflets of a degenerative and severely stenoticaortic valve. Zegdi et al10 deployed a self-expandable valveimplantation intraoperatively inside calcific stenotic aorticvalves before surgical aortic valve replacement. They notedthat stent “misdeployment” was constant in bicuspid nativevalves and occurred in 1/3 of the tricuspid valve cases. Theysuggested that the “resultant valve leaflet distortion mightbe an important concern in the future.” This putative con-cern does not seem to have been borne out thus far instudies of the self-expanding TAVI approach, which haveconsistently demonstrated good hemodynamic and mid-term clinical follow-up results. Zegdi et al10 did not per-orm valvuloplasty before stent deployment in their study,hich might have contributed to the outcomes. More re-
ently, Schultz et al11 examined the Medtronic CoreValvestent frame dimensions and apposition to the native anat-omy using computed tomography. They found incompleteand nonuniform expansion, and none of the stent frames
nstrained portion (level B)
ncomplete Expansion(n � 31)
Complete Expansion(n � 19)
p Value
83 � 5 83 � 7 0.78618 (58%) 6 (32%) 0.06924 � 3 25 � 3 0.7701.8 � 0.2 1.7 � 0.2 0.177
4 (21%) 5 (16%) 0.6609 (47%) 12 (39%) 0.5475 (16%) 0 (0) 0.0659 (29%) 2 (11%) 0.1251 (3%) 2 (11%) 0.2918 (26%) 1 (5%) 0.066
23.4 � 2.1 22.5 � 1.1 0.048*21.6 � 3.2 20.6 � 0.2 0.21128.7 � 4.5 27.0 � 3.9 0.18949.0 (13.9) 50.7 (13.1) 0.667
0.7 (0.2) 0.7 (0.3) 0.66281.7 (30.7) 76.4 (30.5) 0.56048.4 (18.4) 45.7 (19.5) 0.621
17 (55%) 3 (16%) 0.006*14 (45%) 16 (84%) 0.006*
10.6 � 3.4 10.3 � 3.4 0.69818 (58%) 7 (37%) 0.1453 (10%) 1 (5%) 0.066
20.6 � 1.8 23.8 � 1.4 �0.001*89 � 89 107 � 5 �0.001*
n at co
I
studied reached the expected nominal dimensions. In con-
a8
TDi
1835Valvular Heart Disease/Stent-Frame Expansion After TAVI
trast to our study, they found the functionally importantmidsegment was well expanded close to the portion ofleaflet coaptation.
Although incomplete stent frame expansion at the inflow(level A) was frequent in our study, it did not appear to occurto the extent to prevent a seal sufficient to limit paravalvularleak in most cases, perhaps owing to the high radial force thatthe inflow portion of the Medtronic-CoreValve stent frame isable to deliver and because a seal is not just the function ofinflow stent frame expansion, but also the collective inter-action between stent, excluded native leaflets, and the out-flow tract. Moreover, the incomplete expansion of the con-strained portion, close to the area of leaflet coaptation, didnot translate to bioprosthetic malfunction. Similarly, thestent frame dimension at the level of native annulus or thelevel of the nadir of the leaflets did not relate to the bodysurface area-indexed AVA or prosthesis–patient mismatch.This suggests an ability of the bioprosthetic leaflets to com-pensate for extrinsic compression. This compensation could
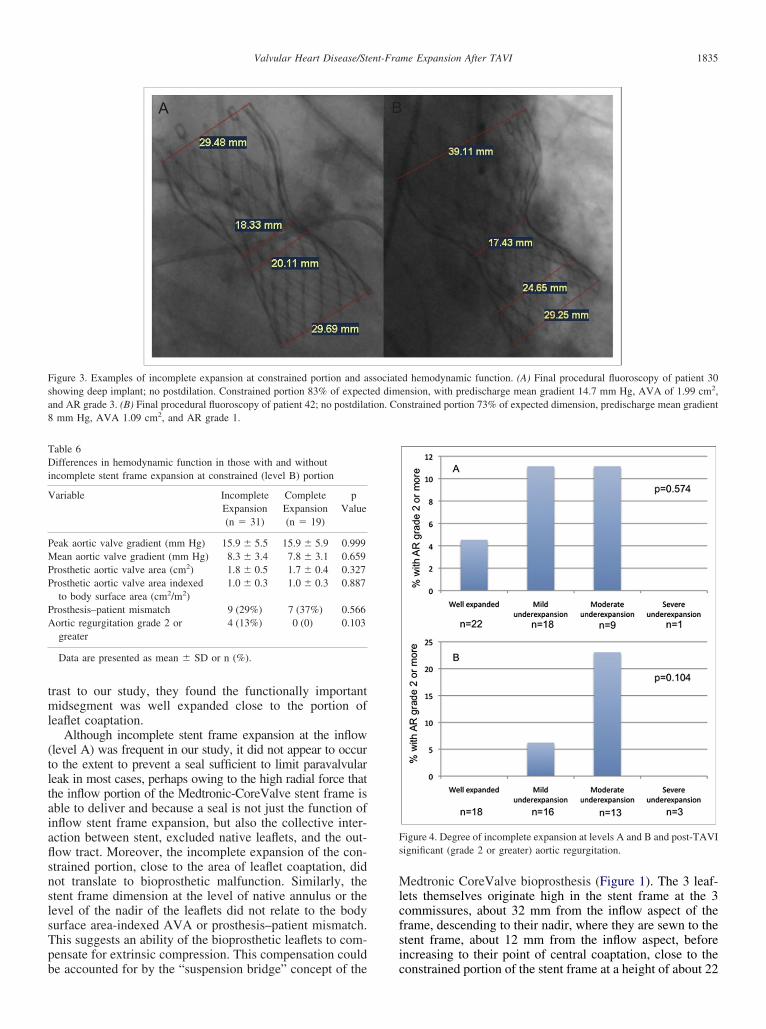
Figure 3. Examples of incomplete expansion at constrained portion and ashowing deep implant; no postdilation. Constrained portion 83% of expecnd AR grade 3. (B) Final procedural fluoroscopy of patient 42; no postdilamm Hg, AVA 1.09 cm2, and AR grade 1.
able 6ifferences in hemodynamic function in those with and without
ncomplete stent frame expansion at constrained (level B) portion
Variable IncompleteExpansion(n � 31)
CompleteExpansion(n � 19)
pValue
Peak aortic valve gradient (mm Hg) 15.9 � 5.5 15.9 � 5.9 0.999Mean aortic valve gradient (mm Hg) 8.3 � 3.4 7.8 � 3.1 0.659Prosthetic aortic valve area (cm2) 1.8 � 0.5 1.7 � 0.4 0.327Prosthetic aortic valve area indexed
to body surface area (cm2/m2)1.0 � 0.3 1.0 � 0.3 0.887
Prosthesis–patient mismatch 9 (29%) 7 (37%) 0.566Aortic regurgitation grade 2 or
greater4 (13%) 0 (0) 0.103
Data are presented as mean � SD or n (%).
be accounted for by the “suspension bridge” concept of the
Medtronic CoreValve bioprosthesis (Figure 1). The 3 leaf-lets themselves originate high in the stent frame at the 3commissures, about 32 mm from the inflow aspect of theframe, descending to their nadir, where they are sewn to thestent frame, about 12 mm from the inflow aspect, beforeincreasing to their point of central coaptation, close to the
d hemodynamic function. (A) Final procedural fluoroscopy of patient 30ension, with predischarge mean gradient 14.7 mm Hg, AVA of 1.99 cm2,nstrained portion 73% of expected dimension, predischarge mean gradient
Figure 4. Degree of incomplete expansion at levels A and B and post-TAVIsignificant (grade 2 or greater) aortic regurgitation.
ssociateted dimtion. Co
constrained portion of the stent frame at a height of about 22
oTua(
1836 The American Journal of Cardiology (www.ajconline.org)
mm from the inflow. These inverted arches are thought todistribute the load in a similar fashion to a suspensionbridge and at the same time might provide additional tissuethat could be compensating for extrinsic distortions in thestent frame, permitting the leaflets of the porcine pericar-dium to still coapt normally even if compressed extrinsi-cally. The paradoxic association of complete level A expan-sion with less favorable hemodynamics could be because
Figure 5. (A) Final procedural fluoroscopic view of patient 19 and 2postdilations. Constrained portion 73% of expected dimension, predis-charge mean gradient 5.4 mm Hg, AVA 2.52 cm2, and AR grade 1. Nadirf bioprosthetic leaflets (n) can be clearly seen on contrast injection. (B)ransesophageal echocardiogram of same patient demonstrating large nod-le of calcium (Ca��) in close proximity to left mainstem (LMS) withdjacent aspect of stent frame in contact with native left coronary cuspLCC) in close proximity.
deeper, suboptimal implants are more likely to have flared,
fully expanded inflow (level A) portions (Table 3). We havepreviously shown suboptimal implantation to be predictiveof prosthesis–patient mismatch.8
In most implantations, after optimal native valve predi-lation and CoreValve self-expansion, postdilation of thebioprosthesis is not performed. In some cases—especiallyin the setting of extraordinarily calcified native aorticvalves—it is deemed necessary to limit paraprosthetic aorticregurgitation at the inflow of the stent frame if this has notbeen achieved in the first instance. The evidence for this islimited and has not been evidence based; of the 4 cases inwhich postdilation was performed in this series, the stentframe dimensions only changed significantly in 1. More-over, the theoretical possibility exists of adverse complica-tions with aggressive stent frame postdilation in the form ofpotential strut fracture and valve leaflet injury, off-settingone 1 theoretical benefit of a self-expanding design.
This was a relatively small study insufficiently poweredto study the clinical end points that would be of interest,such as stroke and mortality. Although the low frequency ofpostdilation enabled the evaluation of hemodynamic func-tion in incompletely expanded stent frames, the putativebenefit or harm of postdilation could not be evaluated. Stentexpansion was assessed in only one projection, with thepossibility of underestimating the proportion of patientswith incompletely expanded frames; nevertheless, satisfac-tory valve areas and a low incidence of significant paraval-vular aortic regurgitation were achieved, whether or notincomplete expansion was detected.
AppendixX-ray fluoroscopic calcium score
Grade Description
0 Not calcified; no calcification visible at annulus1 Mild calcification; width of visible calcium—light gray or darker
visible but not �2/3 of annular width and dark gray or darkercomponent not �1/2 of annular width; height of visiblecalcium �1/2 cm
2 Moderate calcification; width of visible calcium—light gray ordarker �2/3 of annular length but dark gray or darkercomponent not �1/2 of annular width or grade 1 width withheight of visible calcium �1/2 cm
3 Severe calcification; width of visible calcium—dark gray ordarker component �1/2 of annular width or grade 2 widthwith height of visible calcium �1/2 cm
1. Urban P, Gershlick AH, Guagliumi G, Guyon P, Lotan C, Schofer J,Seth A, Sousa JE, Wijns W, Berge C, Deme M, Stoll HP. Safety ofcoronary sirolimus-eluting stents in daily clinical practice: one-yearfollow-up of the e-Cypher registry. Circulation 2006;113:1434–1441.
2. Cribier A, Eltchaninoff H, Bash A, Borenstein N, Tron C, Bauer F,Derumeaux G, Anselme F, Laborde F, Leon MB. Percutaneous trans-catheter implantation of an aortic valve prosthesis for calcific aorticstenosis: first human case description. Circulation 2002;106:3006–3008.
3. Cribier A, Eltchaninoff H, Tron C, Bauer F, Agatiello C, Sebagh L,Bash A, Nusimovici D, Litzler PY, Bessou JP, Leon MB. Earlyexperience with percutaneous transcatheter implantation of heart valveprosthesis for the treatment of end-stage inoperable patients withcalcific aortic stenosis. J Am Coll Cardiol 2004;43:698–703.
4. Grube E, Laborde JC, Gerckens U, Felderhoff T, Sauren B, Buelles-
feld L, Mueller R, Menichelli M, Schmidt T, Zickmann B, Iversen S,Stone GW. Percutaneous implantation of the CoreValve self-expand-
1837Valvular Heart Disease/Stent-Frame Expansion After TAVI
ing valve prosthesis in high-risk patients with aortic valve disease: theSiegburg first-in-man study. Circulation 2006;114:1616–1624.
5. Grube E, Schuler G, Buellesfeld L, Gerckens U, Linke A, WenaweserP, Sauren B, Mohr F-W, Walther T, Zickmann B, Iversen S, FelderhoffT, Cartier R, Bonan R. Percutaneous aortic valve replacement forsevere aortic stenosis in high-risk patients using the second- andcurrent third-generation self-expanding CoreValve prosthesis: devicesuccess and 30-day clinical outcome. J Am Coll Cardiol 2007;50:69–76.
6. Walther T, Simon P, Dewey T, Wimmer-Greinecker G, Falk V, Kasi-mir MT, Doss M, Borger MA, Schuler G, Glogar D, Fehske W,Wolner E, Mohr FW, Mack M. Transapical minimally invasive aorticvalve implantation: multicenter experience. Circulation 2007;116:I240–I245.
7. Webb J, Pasupati S, Humphries K, Thompson C, Altwegg L, Moss R,Sinhal A, Carere RG, Munt B, Ricci D, Ye J, Cheung A, LichtensteinSV. Percutaneous transarterial aortic valve replacement in selectedhigh-risk patients with aortic. Circulation 2007;116:755–763.
8. Jilaihawi H, Chin D, Spyt T, Jeilan M, Vasa-Nicotera M, Bence J,Logtens E, Kovac J. Prosthesis-patient mismatch after transcatheter
aortic valve implantation with the Medtronic CoreValve bioprosthesis.Eur Heart J 2009;31:857–864.9. Bonow RO, Carabello BA, Chatterjee K, de Leon AC Jr, Faxon DP,Freed MD, Gaasch WH, Lytle BW, Nishimura RA, O’Gara PT,O’Rourke RA, Otto CM, Shah PM, Shanewise JS, Smith SC Jr, JacobsAK, Adams CD, Anderson JL, Antman EM, Fuster V, Halperin JL,Hiratzka LF, Hunt SA, Nishimura R, Page RL, Riegel B. ACC/AHA2006 guidelines for the management of patients with valvular heartdisease: a report of the American College of Cardiology/AmericanHeart Association Task Force on Practice Guidelines (Writing Com-mittee to Revise the 1998 guidelines for the management of patientswith valvular heart disease) developed in collaboration with the Soci-ety of Cardiovascular Anesthesiologists endorsed by the Society forCardiovascular Angiography and Interventions and the Society ofThoracic Surgeons. J Am Coll Cardiol 2006;48:e1–148.
10. Zegdi R, Ciobotaru V, Noghin M, Sleilaty G, Lafont A, LatremouilleC, Deloche A, Fabiani JN. Is it reasonable to treat all calcified stenoticaortic valves with a valved stent? Results from a human anatomicstudy in adults. J Am Coll Cardiol 2008;51:579–584.
11. Schultz CJ, Weustink A, Piazza N, Otten A, Mollet N, Krestin G, vanGeuns RJ, de Feyter P, Serruys PWJ, de Jaegere P. Geometry anddegree of apposition of the CoreValve ReValving system with mul-
tislice computed tomography after implantation in patients with aorticstenosis. J Am Coll Cardiol 2009;54:911–918.
Related Documents











