564 Am J Psychiatry 148:5, May 1991 Comorbidity of Attention Deficit Hyperactivity Disorder With Conduct, Depressive, Anxiety, and Other Disorders Joseph Biederman, M.D., Jeffrey Newcorn, M.D., and Susan Sprich, B.A. Qbjective: Attention deficit hypethctivity disorder is a heterogeneous disorder of unknown etiology. Little is known about the comorbidity of this disorder with disorders other than conduct. Therefore, the authors made a systematic search of the psychiatric and psycholog- ical literature for empirical studies dealing with the comorbidity of attention deficit hyper- activity disorder with other disorders. Data Collection: The search terms included hyperac- tivity, hyperkinesis, attention deficit disorder, and attention deficit hyperactivity disorder, cross-referenced with antisocial disorder (aggression, conduct disorder, antisocial disorder), depression (depression, mania, depressive disorder, bipolar), anxiety (anxiety disorder, anx- iety), learning problems (learning, learning disability, academic achievement), substance abuse (alcoholism, drug abuse), mental retardation, and Tourette’s disorder. Findings: The literature supports considerable comorbidity of attention deficit hyperactivity disorder with conduct disorder, oppositional defiant disorder, mood disorders, anxiety disorders, learning disabilities, and other disorders, such as mental retardation, Tourette’s syndrome, and bor- derline personality disorder. Conclusions: Subgroups of children with attention deficit hy- peractivity disorder might be delineated on the basis ofthe disorder’s comorbidity with other disorders. These subgroups may have differing risk factors, clinical courses, and pharmaco- logical responses. Thus, their proper identification may lead to refinements in preventive and treatment strategies. Investigation of these issues should help to clarify the etiology, course, and outcome of attention deficit hyperactivity disorder. (AmJ Psychiatry 1991; 148:564-577) A ttention deficit hyperactivity disorder is a hetero- geneous disorder of unknown etiology. The prey- alence of the disorder has been estimated to range from 2% (1) in primary care pediatric samples to 6% (2) and 9% (3) in large-scale population studies of school- age children. Attention deficit hyperactivity disorder is one of the most common sources of referrals to family physicians, pediatricians, pediatric neurologists, and child psychiatrists. Its impact on society is enormous in terms of financial cost, stress to families, disruption in schools, and the potential for leading to criminality and substance abuse (4). In recent years, evidence has been accumulating re- garding high levels of comorbidity of attention deficit hyperactivity disorder with a number of disorders, in- cluding mood and anxiety disorders as well as conduct Received April 20, 1990; revision receivedjuly 30, 1990; accepted Aug. 29, 1990. From the Pediatric Psychopharmacology Unit, Child Psychiatry Service, Massachusetts General Hospital and Harvard Medical School, Boston, and the Department of Psychiatry, Mount Sinai School of Medicine, New York. Address reprint requests to Dr. Biederman, Pediatric Psychopharmacology Unit (ACC 725), Massa- chusetts General Hospital, Fruit St., Boston MA 02114. Copyright C 1991 American Psychiatric Association. disorder. This high level of comorbidity has been found in culturally and regionally diverse epidemio- logic samples (i.e., New Zealand and Puerto Rico) (2, 3, 5) as well as in clinical samples (6), indicating that attention deficit hyperactivity disorder is most likely a group of conditions with potentially different etiologic and modifying risk factors and different outcomes rather than a single homogeneous clinical entity. Comorbidity raises fundamental questions as to whether psychiatric disorders are discrete and inde- pendent disease entities (7). Comorbidity pervasively affects research and clinical practice as a result of its influence on diagnosis, prognosis, treatment, and health care delivery (8). From the research perspective, subgroups of patients with attention deficit hyperac- tivity disorder and comorbid disorders may represent more homogeneous subgroups of patients with atten- tion deficit hyperactivity disorder. From the clinical perspective, subgroups of patients with attention def- icit hyperactivity disorder and comorbid disorders may respond differentially to specific therapeutic ap- proaches. From the public health perspective, such subgroups may be at high risk for the development of severe psychopathology. Subgrouping children with

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

564 Am J Psychiatry 148:5, May 1991
Comorbidity of Attention Deficit Hyperactivity Disorder
With Conduct, Depressive, Anxiety, and Other Disorders
Joseph Biederman, M.D., Jeffrey Newcorn, M.D., and Susan Sprich, B.A.
Qbjective: Attention deficit hypethctivity disorder is a heterogeneous disorder of unknownetiology. Little is known about the comorbidity of this disorder with disorders other thanconduct. Therefore, the authors made a systematic search of the psychiatric and psycholog-ical literature for empirical studies dealing with the comorbidity of attention deficit hyper-activity disorder with other disorders. Data Collection: The search terms included hyperac-tivity, hyperkinesis, attention deficit disorder, and attention deficit hyperactivity disorder,cross-referenced with antisocial disorder (aggression, conduct disorder, antisocial disorder),depression (depression, mania, depressive disorder, bipolar), anxiety (anxiety disorder, anx-iety), learning problems (learning, learning disability, academic achievement), substanceabuse (alcoholism, drug abuse), mental retardation, and Tourette’s disorder. Findings: Theliterature supports considerable comorbidity of attention deficit hyperactivity disorder withconduct disorder, oppositional defiant disorder, mood disorders, anxiety disorders, learningdisabilities, and other disorders, such as mental retardation, Tourette’s syndrome, and bor-derline personality disorder. Conclusions: Subgroups of children with attention deficit hy-peractivity disorder might be delineated on the basis ofthe disorder’s comorbidity with otherdisorders. These subgroups may have differing risk factors, clinical courses, and pharmaco-logical responses. Thus, their proper identification may lead to refinements in preventive andtreatment strategies. Investigation of these issues should help to clarify the etiology, course,and outcome of attention deficit hyperactivity disorder.
(AmJ Psychiatry 1991; 148:564-577)
A ttention deficit hyperactivity disorder is a hetero-geneous disorder of unknown etiology. The prey-
alence of the disorder has been estimated to range from2% (1) in primary care pediatric samples to 6% (2)and 9% (3) in large-scale population studies of school-age children. Attention deficit hyperactivity disorder isone of the most common sources of referrals to familyphysicians, pediatricians, pediatric neurologists, andchild psychiatrists. Its impact on society is enormous interms of financial cost, stress to families, disruption inschools, and the potential for leading to criminalityand substance abuse (4).
In recent years, evidence has been accumulating re-garding high levels of comorbidity of attention deficithyperactivity disorder with a number of disorders, in-cluding mood and anxiety disorders as well as conduct
Received April 20, 1990; revision receivedjuly 30, 1990; acceptedAug. 29, 1990. From the Pediatric Psychopharmacology Unit, Child
Psychiatry Service, Massachusetts General Hospital and HarvardMedical School, Boston, and the Department of Psychiatry, MountSinai School of Medicine, New York. Address reprint requests to Dr.Biederman, Pediatric Psychopharmacology Unit (ACC 725), Massa-chusetts General Hospital, Fruit St., Boston MA 02114.
Copyright C 1991 American Psychiatric Association.
disorder. This high level of comorbidity has been
found in culturally and regionally diverse epidemio-logic samples (i.e., New Zealand and Puerto Rico) (2,
3, 5) as well as in clinical samples (6), indicating thatattention deficit hyperactivity disorder is most likely a
group of conditions with potentially different etiologicand modifying risk factors and different outcomesrather than a single homogeneous clinical entity.
Comorbidity raises fundamental questions as towhether psychiatric disorders are discrete and inde-
pendent disease entities (7). Comorbidity pervasivelyaffects research and clinical practice as a result of itsinfluence on diagnosis, prognosis, treatment, andhealth care delivery (8). From the research perspective,subgroups of patients with attention deficit hyperac-tivity disorder and comorbid disorders may representmore homogeneous subgroups of patients with atten-tion deficit hyperactivity disorder. From the clinicalperspective, subgroups of patients with attention def-icit hyperactivity disorder and comorbid disorders mayrespond differentially to specific therapeutic ap-proaches. From the public health perspective, suchsubgroups may be at high risk for the development ofsevere psychopathology. Subgrouping children with
BIEDERMAN, NEWCORN, AND SPRICH
Am J Psychiatry I 48:5, May 1991 565
attention deficit hyperactivity disorder may permit thedevelopment of early intervention strategies. This lat-ter aspect is particularly important in the light of long-term follow-up studies of children with attention def-icit hyperactivity disorder (9, 10), which indicate thata subgroup of subjects with attention deficit hyperac-tivity disorder and comorbid disorders have a pooreroutcome as evidenced by significantly greater social,emotional, and psychological difficulties. Although thecomorbidity of psychiatric disorders has been studiedin adult psychiatry as a topic of major practical andtheoretical significance (1 1), research data on attentiondeficit hyperactivity disorder have only recently beenanalyzed with comorbidity taken into account. There-fore, it remains to be determined whether researchfindings previously reported in children with attentiondeficit hyperactivity disorder are related to the atten-tion deficit hyperactivity disorder itself, the existenceof comorbid disorders, or the combination of both(12).
Several competing hypotheses have been proposedto account for patterns of comorbidity (12): 1) thecomorbid disorders do not represent distinct entitiesbut, rather, are the expression of phenotypic variabil-ity of the same disorder, 2) each of the comorbid dis-orders represents distinct and separate clinical entities,3) the comorbid disorders share common vulnerabili-ties (13), either genetic (genotype), psychosocial (ad-versity), or both, 4) the comorbid disorders represent adistinct subtype (genetic variant) within a heteroge-neous disorder (13) (i.e., attention deficit hyperactivitydisorder plus conduct disorder may be a subtype ofattention deficit hyperactivity disorder), 5) one syn-drome is an early manifestation of the comorbid dis-order (i.e., attention deficit hyperactivity disorder is anearly manifestation of a conduct or mood disorder),and 6) the development of one syndrome increases therisk for the comorbid disorder (i.e., attention deficithyperactivity disorder increases the risk for conduct ormood disorder). Investigation of these issues shouldhelp to clarify the etiology, course, and outcome ofattention deficit hyperactivity disorder.
The development of a conceptual model for under-standing the high rate of comorbidity of other disor-ders in attention deficit hyperactivity disorder is corn-plicated by controversy regarding the validity ofattention deficit hyperactivity disorder itself as a dis-tinct clinical entity. Disagreements remain as to whichof the multiple symptom domains represented in thecriteria for attention deficit hyperactivity disordershould be viewed as constituting the core deficit (i.e.,inattentiveness versus hyperactivity), the categorical ortypological nature of the medically dominated diag-nostic system versus a dimensional approach to classi-fication, and whether pervasive or situational symp-toms should be required for diagnosis. For example, anumber of authorities have argued that evidence forthe validity of attention deficit hyperactivity disorder islimited to a rather severe or pervasive type of the dis-order (14-17). Despite this controversy, however, an
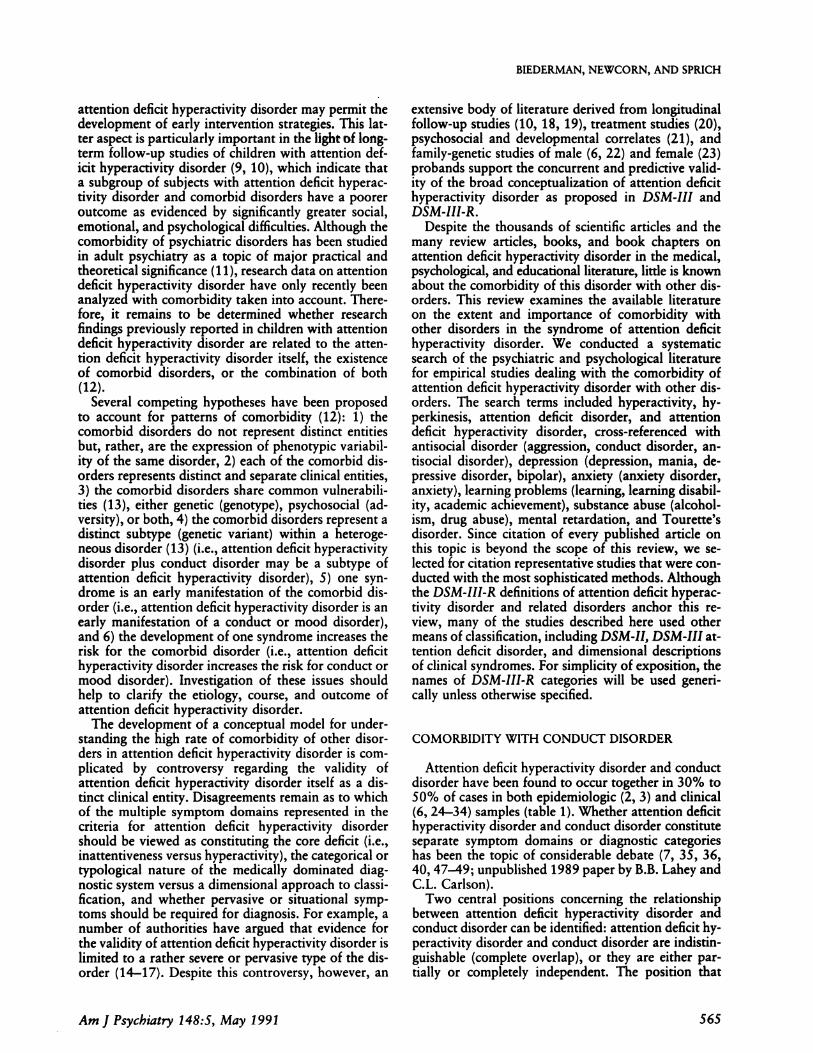
extensive body of literature derived from longitudinalfollow-up studies (10, 18, 19), treatment studies (20),psychosocial and developmental correlates (21), andfamily-genetic studies of male (6, 22) and female (23)probands support the concurrent and predictive valid-ity of the broad conceptualization of attention deficithyperactivity disorder as proposed in DSM-III andDSM-III-R.
Despite the thousands of scientific articles and themany review articles, books, and book chapters onattention deficit hyperactivity disorder in the medical,psychological, and educational literature, little is knownabout the comorbidity of this disorder with other dis-orders. This review examines the available literatureon the extent and importance of comorbidity withother disorders in the syndrome of attention deficithyperactivity disorder. We conducted a systematicsearch of the psychiatric and psychological literaturefor empirical studies dealing with the comorbidity ofattention deficit hyperactivity disorder with other dis-orders. The search terms included hyperactivity, hy-perkinesis, attention deficit disorder, and attentiondeficit hyperactivity disorder, cross-referenced withantisocial disorder (aggression, conduct disorder, an-tisocial disorder), depression (depression, mania, de-pressive disorder, bipolar), anxiety (anxiety disorder,anxiety), learning problems (learning, learning disabil-ity, academic achievement), substance abuse (alcohol-ism, drug abuse), mental retardation, and Tourette’sdisorder. Since citation of every published article onthis topic is beyond the scope of this review, we se-lected for citation representative studies that were con-ducted with the most sophisticated methods. Althoughthe DSM-III-R definitions of attention deficit hyperac-tivity disorder and related disorders anchor this re-view, many of the studies described here used othermeans of classification, including DSM-II, DSM-III at-tention deficit disorder, and dimensional descriptionsof clinical syndromes. For simplicity of exposition, thenames of DSM-III-R categories will be used generi-cally unless otherwise specified.
COMORBIDITY WITH CONDUCT DISORDER
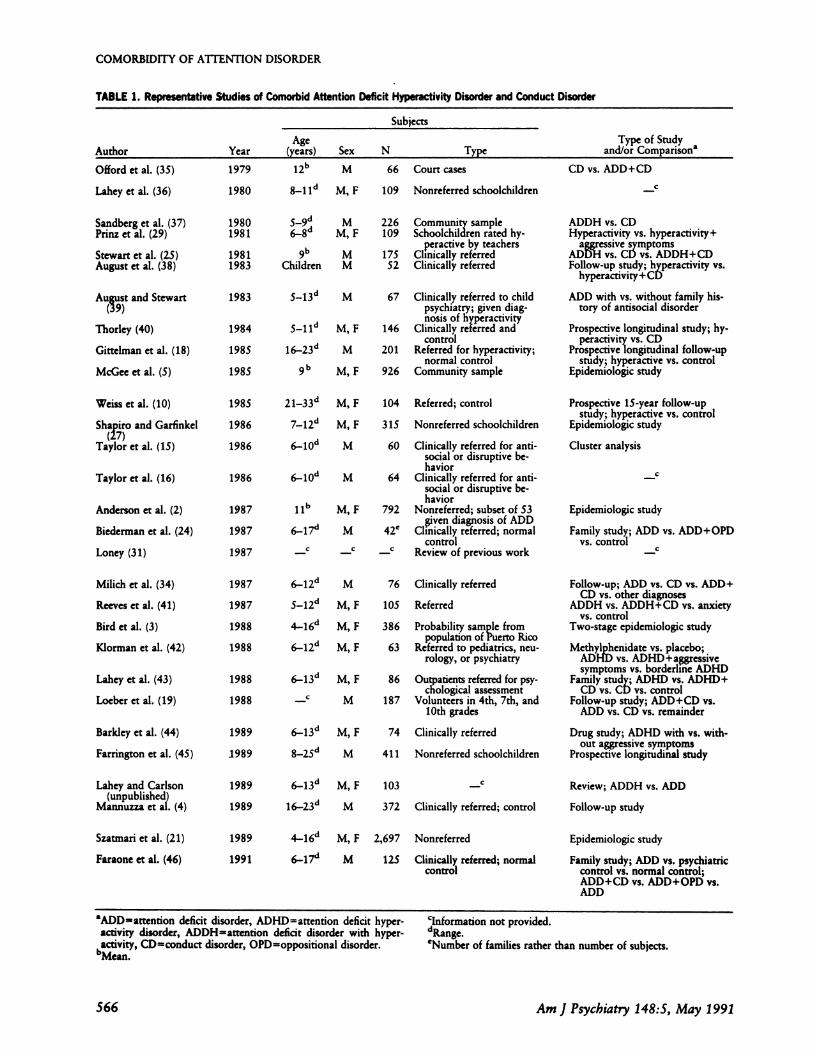
Attention deficit hyperactivity disorder and conductdisorder have been found to occur together in 30% to50% of cases in both epidemiologic (2, 3) and clinical(6, 24-34) samples (table 1). Whether attention deficithyperactivity disorder and conduct disorder constituteseparate symptom domains or diagnostic categorieshas been the topic of considerable debate (7, 35, 36,40, 47-49; unpublished 1989 paper by B.B. Lahey andC.L. Carison).
Two central positions concerning the relationshipbetween attention deficit hyperactivity disorder andconduct disorder can be identified: attention deficit hy-peractivity disorder and conduct disorder are indistin-guishable (complete overlap), or they are either par-tially or completely independent. The position that
Age
(years)
l2�’
8-1 1d
9b
Children
Sex
M
M, F
MM, F
MM
Type of Study
and/or Comparison
CD vs. ADD+CD
C
226 Community sample109 Schoolchildren rated hy-
peractive by teachers175 ClInically referred
52 Clinically referred
Year
1979
1980
19801981
19811983
1983
1984
1985
1985
1985
1986
1986
S_l3c� M 67 Clinically referred to childpsychiatry; given diag-nosis of hyperactivity
s-i 1d M, F 146 Clinically referred andcontrol
16�23�I M 201 Referred for hyperactivity;normal control
9 b M, F 926 Community sample
Author
Offord et at. (35)
Lahey et at. (36)
Sandberg et al. (37)Prinz et al. (29)
Stewart et al. (25)August et al. (38)
August and Stewart�39)
Thorley (40)
Gittelman et al. (18)
McGee et al. (5)
Weiss et al. (10)
Shapiro and Garfinkel(27)
Taylor et al. (15)
Taylor et al. (16)
Anderson Ct al. (2)
Biederman et al. (24)
Loney (31)
Milich et al. (34)
Reeves et al. (41)
Bird et al. (3)
Kiorman et al. (42)
Lahey et al. (43)
Loeber et al. (19)
Barkley et al. (44)
Farrington et al. (45)
2l_33c�
7�l2”
6-10d
M, F
M, F
M
1986 6-10d M
M, F
M
M
M, F
M, F
M, F
M, F
M
M, F
M
M, F
M
1987
1987
1987
1987
1987
1988
1988
1988
1988
1989
1989
1989
1989
1989
1991
I 1b
6-17”
6-12”
5-12”
4-16”
6-12”
6-13”
C
6-13”
8-25”
6-13”
16-23”
4-16”
6-17’�
76 Clinically referred
105 Referred
386 Probability sample frompopulation of Puerto Rico
63 Referred to pediatrics, neu-rology, or psychiatry
86 Outpatients referred for psy-chological assessment
187 Volunteers in 4th, 7th, and10th grades
74 Clinically referred
41 1 Nonreferred schoolchildren
103 C
372 Clinically referred; control
Szatmari et al. (21)
Faraone et al. (46)
Review; ADDH vs. ADD
Follow-up study
M, F 2,697 Nonreferred
M 125 Clinically referred; normalcontrol
COMORBIDITY OF ATfENTION DISORDER
566 Am J Psychiatry 148:5, May 1991
TABLE 1. Representative Studies of Comorbid Attention Deficit Hyperactivity Disorder and Conduct Disorder
Subjects
Lahey and Carlson(unpublished)
Mannuzza et at. (4)
N Type
66 Court cases
109 Nonreferred schoolchildren
104 Referred; control
315 Nonreferred schoolchildren
60 Clinically referred for anti-social or disruptive be-havior
64 Clinically referred for anti-social or disruptive be-havior
792 Nonreferred; subset of 53given diagnosis of ADD
42e Clinically referred; normalcontrol
_c Review of previous work
ADDH vs. CDHyperactivity vs. hyperactivity+
aggressive sjrmptomsADDH vs. CD vs. ADDH+CDFollow-up study; hyperactivity vs.
hyperactivity+CD
ADD with vs. without family his-tory of antisocial disorder
Prospective longitudinal study; hy-peractivity vs. CD
Prospective longitudinal follow-upstudy; hyperactive vs. control
Epidemiologic study
Prospective 15-year follow-upstudy; hyperactive vs. control
Epidemiologic study
Cluster analysis
C
Epidemiologic study
Family study; ADD vs. ADD+OPDvs. control
C
Follow-up; ADD vs. CD vs. ADD+CD vs. other diagnoses
ADDH vs. ADDH+CD vs. anxietyvs. control
Two-stage epidemiologic study
Methylp�hemdate vs. placebo;ADHD vs. ADHD+a�gressivesymptoms vs. borderline ADHD
Family study; ADHD vs. ADHD+CD vs. CD vs. control
Follow-up study; ADD+CD vs.ADD vs. CD vs. remainder
Drug study; ADHD with vs. with-out aggressive symptoms
Prospective longitudinal study
Epidemiologic study
Family study; ADD vs. psychiatriccontrol vs. normal control;ADD+CD vs. ADD+OPD vs.ADD
aADDatrention deficit disorder, ADHD=attention deficit hyper-
activity disorder, ADDH=attention deficit disorder with hyper-activity, CDconduct disorder, OPDoppositional disorder.bMun
%�formation not provided.d�nge.eNumber of families rather than number of subjects.

BIEDERMAN, NEWCORN, AND SPRICH
Am J Psychiatry 148:5, May I 991 567
TABLE 1 (continued)
Instruments Used
C
Behavior checklists, achievement tests, peerrating scales
C
Rating scales
Clinical assessment, rating scalesStructured interviews, behavior checklists,
achievement tests
Clinical assessments, clinical interviews,WISC-R
Clinical rating sheets (ICD-9), factor scales
Structured interviews
Teacher ratings
Structured interviews, self-rating scales, psy-chiatric histories (DSM-III)
Teacher ratings, structured interview, atten-tional battery, achievement tests
Behavior checklists, psychiatric interviews
Semistructured interviews, behavior check-
lists, psychological testing
Structured interviews, behavior checklists
Clinical interviews, structured interviews
C
Structured interviews, statistical analysis ofindividual ADD and CD symptoms
Structured interviews, cognitive tests, behav-ior questionnaires
Behavior checklists, structured interviews
Achievement test, rating scales
Structured interviews, rating scales
Behavior and health checklists, intelligencetests, psychosocial assessment, police re-ports
Parental interview, behavior rating scales,cognitive tests
Behavior checklist, cognitive assessments,criminal records
Structured interviews, rating scales
Structured interviews
Structured interviews, behavior checklists,clinical diagnoses
Structured interviews, morbidity risk
Findings5
More perinatal events in ADD+CD; no differences on other measures of psychosocialdisadvantage or cognitive skills
H�gh intercorrelations for hyperactivity and conduct problem scale factors, similar corre-lation patterns for criterion variables; similar multiple regressions for combined andseparate factors
No differencesPositive correlation between hyperactive and aggressive symptoms; hyperactivity and ag-
gressive symptoms intertwinedNo differences in age, IQ, and family size; more school problems in ADDHAt follow-up hyperactive children still inattentive and impulsive; those with
hyperactivity+CD still inattentive, impulsive, aggressive, noncompliant, antisocial, andabusing alcohol
ADD with family history of antisocial diagnosis significantly higher on aggression, non-compliance, antisocial behavior, egocentricity; significantly higher rate of CD in sib-lings
CD had greater frequency of aggressive, antisocial, emotional, and psychosocial disrur-bances; hyperactive had greater frequency of hyperactivity and inattention
Full ADDH in 31% of hyperactive vs. 3% of control; CD and substance use disorders�gnificantly higher in hyperactive
ADDH ratings correlated with cognitive skills no differences on psychosocial disadvan-tage; inattention correlated with cognitive skills; CD and hyperactivity correlated withpsychosocial disadvantage
66 /o of hyperactive continued to have one or more disabling symptoms; 23% of hyper-active vs. 2.4% of control had antisocial personality disorder
2.3% had ADD; 3.6% had CD; 3.0% had ADD+CD; interdependence between ADDand CD
25% had high scores on hyperactivity and inattention; good response to stimulants; clas-sification of pervasive hyperactivity with inattention robust
Independence of inattentive and antisocial, defiant, CD dimensions
47% of ADD had CD and/or OPD; 35% of CD and/or OPD had ADD
64% of ADD had CD and/or OPD; 46% of ADD+CD/OPD relatives vs. 13% of ADDrelatives vs. 7% of control relatives had antisocial disorders
Aggressive symptoms differentiated hyperactive/minimal brain dysfunction boys on sev-eral measures; differentiation between hyperactivity+aggressive symptoms and hyper-activity valuable
Conditional probability of ADD in CD was 0.67; conditional probability of CD in ADDwas 0.30; ADD and CD are partially independent
52% had two or more diagnoses; 85% of CD had ADD; ADDH and CD are partiallyindependent
57% of ADD had CD and/or OPD; 47% of CD and/or OPD had ADD
Similar responses to methylphenidate in all three groups
Higher rates of aggression arrest, and imprisonment in fathers of ADHD+CD; familial-ity of ADD not reported
Highest rates of police contacts and self.reported delinquency in ADD+CD; 30.8% ofADD+CD vs. 3.4% of ADD vs. 20.7% of CD vs. 1.7% of remainder were multipleoffenders
Aggressive and nonaggressive ADHD similar in drug responses; aggressive had more im-paired family situataons
Hyperactivity and CD independently predictive of juvenile convictions; 4S.8% ofhyperactive+CD vs. 35% of CD vs. 23.5% of hyperactive vs. 12.6% with neitherwere convicted as juveniles
41% of ADDH vs. 20% of ADD had CD
For cohort 1, 68% of ADD vs. 13% of control had ADD and 4S% of ADD vs. 16% ofcontrol had CD; for cohort 2, 70% of ADD vs. 10% of control had ADD and 59%of ADD vs. 18% of control had CD
ADD and CD occurred together significantly often; ADD+CD seemed true hybriddisorder
Higher familial risk for ADD, antisocial disorders, and substance use disorder inADD+CD; earlier age at onset of ADD and highest rates of school dysfunction inADD+CD; ADD+CD had more virulent form of ADD OPD was familial (validity ofOPD); ADD+OPD was intermediate between ADD and ADD+CD (OPD may be sub-syndromal manifestation of CD)

COMORBIDITY OF ATfENTION DISORDER
568 Am J Psychiatry 148:5, May 1991
attention deficit hyperactivity disorder and conductdisorder are indistinguishable suggests that, given themeasurement and/or diagnosis of either attention def-icit hyperactivity disorder or conduct disorder, theidentification of the other yields no additional infor-mation. Proponents of this position point to the simi-larities between children with attention deficit hyper-activity disorder and children with conduct disorderfrequently reported in studies of correlates, outcome,and treatment responses (44, 50). Similarly, they pointto intercorrelations between symptoms of attentiondeficit hyperactivity disorder and symptoms of con-duct disorder (aggressive, disruptive, and noncompli-ant behaviors) often reported in factor-analytic studiesof children with behavioral disorders (Si, 52). In ad-dition, they cite a lack of substantial differences in psy-chosocial, neurodevelopmental, and perinatal factorsbetween children with attention deficit hyperactivitydisorder and children with conduct disorder (37).
Proponents of the independent position view atten-tion deficit hyperactivity disorder and conduct disor-der as either completely or partially independent. Sup-port for this position can be derived from studies thatcompared patterns of familial aggregation, cognitiveperformance, and outcome of children with attentiondeficit hyperactivity disorder with those of childrenwith attention deficit hyperactivity disorder plus con-duct disorder. In the studies of Loney et al. (53), symp-toms of hyperactivity and aggression were not highlycorrelated and showed different patterns of concurrentand predictive validity, suggesting that they were sep-arate dimensions. In those studies, the presence of con-duct disorder in childhood, whether associated withattention deficit hyperactivity disorder or not, was sig-nificantly correlated with aggressive behavior and de-linquency in adolescence (53), but childhood attentiondeficit hyperactivity disorder without conduct disorderwas correlated with cognitive and academic deficits(21, 32, 54). Similar findings emerged from a fol-low-up study in a nonclinical sample (55, 56). Otherstudies (21, 34, 38, 41, 45, 57, 58) have demonstratedthat children with attention deficit hyperactivity dis-order with an associated childhood-onset conduct dis-order have more serious clinical courses and pooreroutcomes than children with attention deficit hyperac-tivity disorder without conduct disorder.
Family studies have shown that childhood conductdisorder, but not attention deficit hyperactivity disor-der, is associated with parental antisocial behaviorsand alcoholism (6, 25, 38, 46, S4). Investigators havefound that the familial risk for attention deficit hyper-activity disorder and antisocial disorders is highestamong relatives of children with attention deficit hy-peractivity disorder with concomitant conduct disor-der (24, 28, 46, 54, 59). Several reports have alsoshown that a current or past history of attention deficithyperactivity disorder is frequently reported amongpatients with alcohol dependence (60-62) and drugaddiction (63, 64). Since follow-up studies of childrenand adolescents with the diagnosis of conduct disorder
are in agreement regarding the strong predictive powerof conduct disorder for future psychiatric disorders,social adjustment problems, antisocial personality, al-coholism, and criminality (58), it has been suggestedthat the delinquent behaviors and substance abuse of-ten reported in follow-up studies of boys with atten-tion deficit hyperactivity disorder (18, 65) may belinked to childhood antisocial disorders rather than tothe syndrome of attention deficit hyperactivity disor-der per se (4, 39, 45).
Two studies examining the response to stimulants ofchildren with attention deficit hyperactivity disorderwith and without associated conduct disorder (42, 44)found that the two groups of children showed similarpatterns of improvement with regard to symptoms ofattention deficit hyperactivity disorder. Although thesetwo studies cannot help resolve the debate regardingthe independence of attention deficit hyperactivity dis-order and conduct disorder, they support the clinicalrelevance of diagnosing both attention deficit hyperac-tivity disorder and conduct disorder when the disor-ders occur together.
Although debate continues as to whether attentiondeficit hyperactivity disorder is distinct from conductdisorder, the bulk of the evidence appears to indicatethat attention deficit hyperactivity disorder and con-duct disorder are at least partially independent dimen-sions and/or categories. Attention deficit hyperactivitydisorder and conduct disorder differ not only in theirdefining clinical features but also in external variablessuch as outcome (cognitive dysfunction for attentiondeficit hyperactivity disorder versus aggression, antiso-cial behaviors, substance abuse, and delinquency forconduct disorder), etiologic factors (familial aggrega-tion), and psychosocial and developmental correlates.Thus far, data from treatment studies have not re-solved the debate. There is increasing evidence thatchildren with attention deficit hyperactivity disorderplus conduct disorder appear to have a particularlysevere form of attention deficit hyperactivity disorder.Thus, subgrouping based on comorbidity with conductdisorder may be of potential value in determiningwhich children with attention deficit hyperactivity dis-order have a more serious prognosis and different fam-ily-genetic risk factors and require specialized compre-hensive therapeutic interventions.
COMORBIDITY WITH OPPOSITIONAL DEFIANTDISORDER
The nosologic status of oppositional defiant disorderand consequently that of attention deficit hyperactivitydisorder plus oppositional defiant disorder remains un-clear (66, 67). To date, only a few studies have gener-ated data on oppositional defiant disorder. Some ofthese have grouped oppositional defiant disorder andconduct disorder together into a single antisocial be-havioral category, making it difficult to draw conclu-sions about oppositional defiant disorder itself. The
BIEDERMAN, NEWCORN, AND SPRICH
Am J Psychiatry 1 48:5, May 1991 569
few studies available report an overlap of at least 35%between attention deficit hyperactivity disorder andoppositional defiant disorder, either alone or ‘cOrn-bined with conduct disorder, in both epidemiologic (2,3) and clinical (6, 46) studies of children and adoles-cents. Faraone et al. (46) recently demonstrated thatDSM-III oppositional disorder itself is also familialand that the risk for oppositional disorder among rel-atives of probands with attention deficit disorder plusoppositional disorder is three times greater than therisk among relatives of probands with attention deficitdisorder without oppositional disorder and nearly tentimes greater than the risk among relatives of normalcontrol subjects. These data provide some evidence forthe validity of DSM-III oppositional disorder.
In terms of severity of the clinical picture, the avail-able data suggest that children with attention deficithyperactivity disorder plus oppositional defiant disor-der may form an intermediate subgroup between thosewho have attention deficit hyperactivity disorder aloneand those with attention deficit hyperactivity disorderplus conduct disorder. For example, Faraone et al. (46)showed that although probands with DSM-III atten-tion deficit disorder plus oppositional disorder had ahigher rate of school dysfunction than those with at-tention deficit disorder alone, this rate was lower thanthat of subjects with attention deficit disorder plusconduct disorder. A similar pattern was observed inthe risk for attention deficit disorder and antisocialdisorders among relatives of probands: family mem-bers of probands with attention deficit disorder plusoppositional disorder were at higher risk for antisocialdisorders and attention deficit disorder than relativesof probands with attention deficit disorder alone but atlower risk than relatives of probands with attentiondeficit disorder plus conduct disorder. These findingsare consistent with the hypothesis that oppositionaldefiant disorder may be a subsyndromal manifestationof conduct disorder (unpublished 1985 paper by J.Loney).
COMORBIDITY WITH MOOD DISORDERS
Attention deficit hyperactivity disorder and mooddisorders have been found to occur together in 15% to75% of cases in both epidemiologic (2, 3) and clinical(6, 68-71) samples of children and adolescents (table2). Some investigators, however, have not found high-er-than-expected rates of mood disorders in childrenwith attention deficit hyperactivity disorder (10, 18,43, 72). In clinical samples, the association betweenattention deficit hyperactivity disorder and mood dis-orders has been reported in studies of children withnonbipolar major depression and dysthymia (75),studies of adolescents with bipolar disorder (80), andstudies of children with attention deficit hyperactivitydisorder (6, 69, 73, 77). Studies of high-risk children ofparents with mood disorders have found high rates ofattention deficit hyperactivity disorder in these chil-
dren (78, 79; unpublished 1989 paper by H. Orva-schel), and family studies of children with attentiondeficit hyperactivity disorder have found a significantlyhigher rate of mood disorders in probands with atten-tion deficit hyperactivity disorder and in their first-degree relatives than in normal control children andtheir first-degree relatives (74, 76). Studies of adoptedchildren with the diagnosis of attention deficit hyper-activity disorder found higher rates of major depres-sive disorder in the biological relatives of these chil-dren than in their adoptive relatives and the biologicalrelatives of control subjects (82). Case reports havedescribed individuals with childhood histories of atten-tion deficit hyperactivity disorder who developed ma-jor affective disorders in later years (83). It is doubtfulthat the comorbidity of attention deficit hyperactivitydisorder and mood disorders can be explained by as-certainment bias because high levels of comorbidity ofthese disorders have also been found in culturally andregionally diverse population-based epidemiologic sam-ples (2, 3, 5).
Findings reported by Biederman et al. (84) supportthe hypothesis that DSM-III attention deficit disorderand major depressive disorder share common familialvulnerabilities. Familial risk analyses revealed the fol-lowing: 1) the risk for major depressive disorderamong the relatives of probands with attention deficitdisorder was significantly higher than the risk amongrelatives of normal comparison children, 2) the risk formajor depressive disorder was the same among therelatives of probands with and without major depres-sive disorder and significantly higher in both groupsthan among the relatives of normal control children,and 3) the two disorders did not cosegregate withinfamilies. These findings are consistent with the hypoth-esis that attention deficit disorder and major depressivedisorder represent different expressions of the sameetiologic factors responsible for the manifestation ofattention deficit disorder. The reasons why the sharedgenotype may have differing phenotypic expressionssuch as attention deficit disorder, major depressive dis-order, or attention deficit disorder plus major depres-sive disorder remain unknown.
Follow-up data for children with attention deficithyperactivity disorder as well as for children with ma-jor depressive disorder (85, 86) strongly suggest thatalthough these disorders are individually associatedwith substantial long-term psychiatric morbidity, theiroccurrence together may be associated with a particu-larly poor outcome. In a study that evaluated predic-tors of suicide in adolescents, Brent et al. (87) reportedthat adolescents who committed suicide had higherrates of bipolarity and attention deficit hyperactivitydisorder than did those who attempted suicide. Thus,the occurrence together of attention deficit hyperactiv-ity disorder and mood disorder is suggestive of a sub-group of children with attention deficit hyperactivitydisorder at higher risk for greater psychiatric morbid-ity and disability (81) and perhaps at higher risk forsuicide than other children with attention deficit hy-
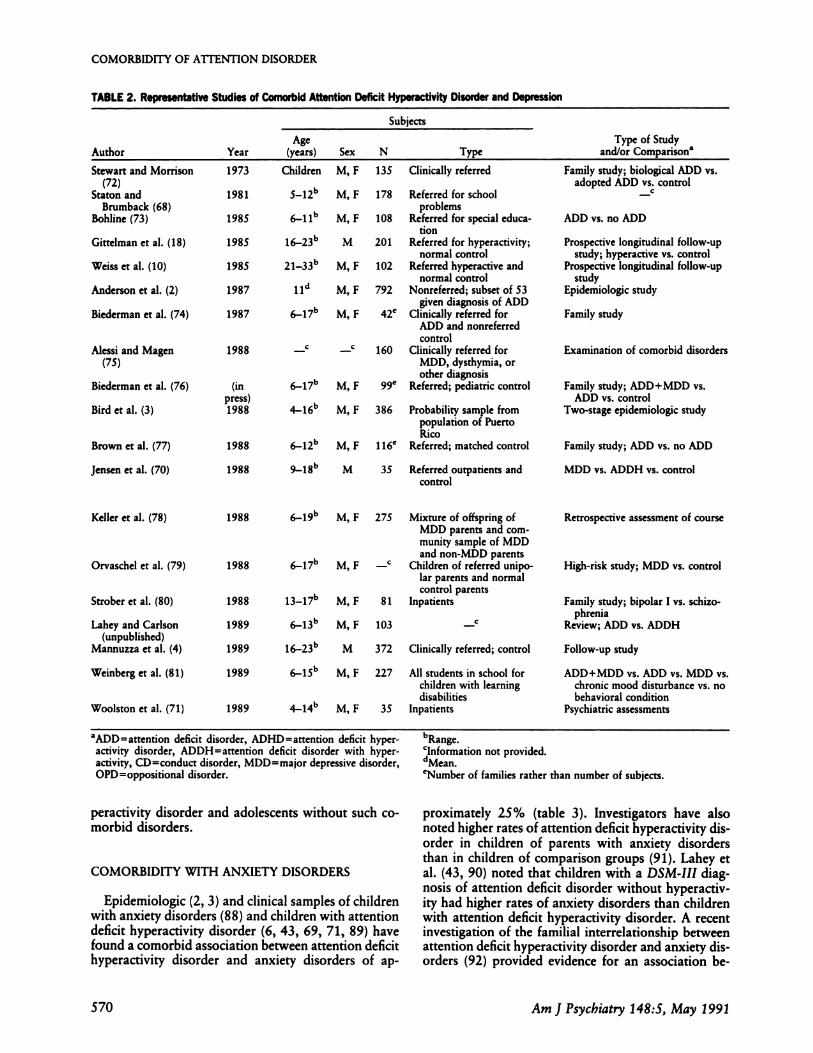
TABLE 2. Representative Studies of Comorbid Attention Deficft Hyperactivity Disorder and Depression
Subjects
AgeAuthor Year (years) Sex N
Type of StudyType and/or Comparisona
Stewart and Morrison(72)
Staton andBrumback (68)
Bohline (73)
Gittelman et al. (18)
Weiss et al.(10)
Anderson er al. (2)
Biederman et al. (74)
1973
1981
1985
1985
1985
1987
1987
Children M, F
5-12” M, F
6-11b M,F
16�23L� M
2l-33�’ M, F
11” M,F
6-17” M,F
6�l7L�
4-1&’
Alessi and Magen 1988(75)
Biederman et al. (76) (inpress)
Bird ct al. (3) 1988
Brown et al. (77) 1988
Jensen er al. (70) 1988
Keller et al. (78) 1988
1988 6-17b M, FOrvaschel et al. (79)
Strober et al. (80)
Lahey and Carlson(unpublished)
Mannuzza et al. (4)
Retrospective assessment of course
1988
1989 6-13b
Weinberg et al. (81) 1989
Woolston et al.(71) 1989
C
1989 16-23b M 372 Clinically referred; control
COMORBIDITY OF A1TENTION DISORDER
570 Am J Psychiatry 1 48:5, May 1991
135 Clinically referred
178 Referred for schoolproblems
108 Referred for special educa-tion
201 Referred for hyperactivity;normal control
102 Referred hyperactive andnormal control
792 Nonreferred; subset of 53given diagnosis of ADD
42C Clinically referred forADD and nonreferredcontrol
_C C 160 Clinically referred forMDD, dysthymia, orother diagnosis
Referred; pediatric controlM,F 99e
M,F 386 Probability sample frompopulation of PuertoRico
6-12” M, F 1 16e Referred; matched control
9-1&’ M 35 Referred outpatients andcontrol
6-19k’ M, F 275 Mixture of offspring ofMDD parents and com-munity sample of MDDand non-MDD parents
_C Children of referred unipo-lar parents and normalcontrol parents
M, F 81 lnpatients
M,F 103
6-15b M, F 227 All students in school for
children with learningdisabilities
4-14” M, F 35 Inpatients
Family study; biological ADD vs.adopted ADDv5. control
ADD vs. no ADD
Prospective longitudinal follow-upstudy; hyperactive vs. control
Prospective longitudinal follow-upstudy
Epidemiologic study
Family study
Examination of comorbid disorders
Family study; ADD+MDD vs.ADD vs. control
Two-stage epidemiologic study
Family study; ADD vs. no ADD
MDD vs. ADDH vs. control
High-risk study; MDD vs. control
Family study; bipolar I vs. schizo-phrenia
Review; ADD vs. ADDH
Follow-up study
ADD+MDD vs. ADD vs. MDD vs.chronic mood disturbance vs. nobehavioral condition
Psychiatric assessments
aADDattention deficit disorder, ADHD=attention deficit hyper-
activity disorder, ADDH=artention deficit disorder with hyper-activity, CD=conduct disorder, MDD=major depressive disorder,OPD=oppositional disorder.
peractivity disorder and adolescents without such co-morbid disorders.
COMORBIDITY WITH ANXIETY DISORDERS
Epidemiologic (2, 3) and clinical samples of childrenwith anxiety disorders (88) and children with attentiondeficit hyperactivity disorder (6, 43, 69, 71, 89) havefound a comorbid association between attention deficithyperactivity disorder and anxiety disorders of ap-
bRange.Clnformation not provided.dMeaneNumber of families rather than number of subjects.
proximately 25% (table 3). Investigators have alsonoted higher rates of attention deficit hyperactivity dis-order in children of parents with anxiety disordersthan in children of comparison groups (91). Lahey etal. (43, 90) noted that children with a DSM-III diag-nosis of attention deficit disorder without hyperactiv-
ity had higher rates of anxiety disorders than childrenwith attention deficit hyperactivity disorder. A recentinvestigation of the familial interrelationship betweenattention deficit hyperactivity disorder and anxiety dis-orders (92) provided evidence for an association be-

Clinical assessments
Questionnaires
Structured interviews
Structured interviews, self-rating scales, psy-chiatric histories (DSM-III)
Structured interviews, behavior checklists
Structured interviews
Structured interviews
Behavior checklists, structured interviews
Depression inventory
Rating scales, structured interviews
Structured interviews
_C High rates of MDD and ADD in children of MDD parents
C
No case of current major depression in ADD; lifetime (since age 13) prevalence of MDDnot significantly different between ADD and control
ADD+MDD had most behavioral problems
32% had ADHD with dysthymia
BIEDERMAN, NEWCORN, AND SPRICH
Am J Psychiatry 148:5, May 1991 S71
TABLE 2 (continued)
Instruments Used Findings5
Interviews No significant differences in rates of bipolar and unipolar affective disorder
60% met criteria for MDD; 44% met criteria for hyperactivity; 75% of hyperactive hadMDD; 55% of MDD had hyperactivity
ADD more depressed than no ADD
3% of hyperactive vs. 2% of control had current affective disorder; 6% of hyperactivevs. 10% of control had history of affective disorder
More suicide attempts by hyperactive than control in year before follow-up; no signifi-cant differences in depression scores on self-rating scale
15% of ADD met criteria for depression and/or dysthymia; 57% of MDD met criteriafor ADD
32% of ADD and 27% of ADD relatives met criteria for MDD vs. none of control and6% of control relatives
Interviews 25% of ADD, 25% of CD, and 25% of anxious had MDD; 22% of ADD, 33% of CD,and 89% of anxious had dysthymia
26% of ADD probands had MDD; morbidity risks for ADD and MDD in ADD andADD+MDD differed significantly from control
19% of ADD met criteria for MDD; 30% of MDD met criteria for ADD
ADD and ADD parents were significantly more depressed than no ADD and no ADDparents
Rates of specific disorders not reported; significant symptom (externalizing) overlapbetween ADD and MDD; few ADD symptoms in MDD boys but high rates of exter-nalizing behaviors and impulsivity and low frustration tolerance (question of OPD);depressive symptoms commonly noted in ADDH boys (question of dysthymia)
14% had MDD; 87% had at least one MDD parent; 53% had anxiety, ADD, CD, orsubstance use disorder; 29% had two or more comorbid diagnoses; 45% with two ormore diagnoses had ADD
Structured interviews, RDC 24% of adolescent bipolar I probands had childhood history of ADDH; rate of ADDHin relatives not reported
9% of ADDH vs. 8% of ADD had MDD (n.s.)
Structured interviews
Standardized psychometric intelligence andachievement tests, semistructured inter-views
Clinical diagnoses, behavior checklists, intel-ligence tests
tween the two disorders. This study found 1) that therisk for anxiety disorders among the relatives of pa-tients with attention deficit hyperactivity disorder wassignificantly higher than the risk among relatives ofnormal comparison children, 2) that the risk for anx-iety disorders was significantly higher in relatives ofprobands with attention deficit hyperactivity disorderand anxiety disorders than in relatives of children withattention deficit hyperactivity disorder without anxietydisorders, and 3) that nonindependent transmission ofattention deficit hyperactivity disorder and anxiety dis-
orders within families could not be established. Thesefindings suggest that attention deficit hyperactivity dis-order and anxiety disorders transmit independently infamilies.
COMORBIDITY WiTH LEARNING DISABIL�ES
An overlap between attention deficit hyperactivitydisorder and learning disabilities has been consistentlyreported in the literature. The reported degree of over-

Author Year
Subjects
Type of Studyand/or Comparisona
Age(years) Sex N Type
Gittelman et al. (18)
Anderson et al. (2)
Lahey et al. (90)
Last et al. (88)
Munir et al. (69)
Sylvester et al. (91)
Bird et al. (3)
Mannuzza et al. (4)
1985
1987
1987
1987
1987
1987
1988
1989
16-23b
1 1C
6-13b
5_18b
516b
7��17b
4-16b
16-23b
M
M, F
M, F
M, F
M
M, F
M, F
M
201
792
63
73
42
91
386
372
Referred hyperactive andnormal control
Nonreferred; subset of 53given diagnosis of ADD
Clinically referred; givendiagnosis of ADD
Outpatients at anxietyclinic
Clinically referred; pediat-nc control
High-risk children of anx-ious, depressed, or con-trol parents
Probability sample frompopulation of PuertoRico
Clinically referred; control
Prospective longitudinal follow-upstudy; hyperactive vs. control
Epidemiologic study
ADDH vs. ADD
Assessment of comorbidity
Family study
Comparison of three structuredinterviews
Two-stage epidemiologic study
Follow-up study
Pliszka (89) 1989 M, F 79 Clinically referred Drug study
Woolston er al. (71)Biederman er al. (92)
19891991
4-14b
6-17bM, FM, F
35125
InpatientsClinically referred; pediat-
nc control
Psychiatric assessmentsFamily study; ADD vs. psychiatric
control vs. normal control
COMORBIDITY OF AUENTION DISORDER
572 Am J Psychiatry 1 48:5, May 1991
TABLE 3. Representative Studies of Comorbid Attention Deficit Hyperactivity Disorder and Anxiety
aADDattention deficit disorder, ADHD=attention deficit hyper-
activity disorder, ADDH=attention deficit disorder with hyperac-
tivity, CD=conduct disorder.
lap ranges from as low as 10% (57, 93) to as high as92% (94). This variability is most likely due to differ-ences in selection criteria, sampling, and measurementinstruments, as well as inconsistencies in the criteriaused to define both attention deficit hyperactivity dis-order and learning disabilities in different studies(95, 96). In addition to these inconsistencies in thedefinitions of learning disabilities and attention deficithyperactivity disorder, the academic dysfunction corn-monly associated with both conditions and the hetero-geneity of the learning disabilities have led to wide-spread confusion about these disorders.
Studies have consistently shown that children withattention deficit hyperactivity disorder perform morepoorly in school than control subjects, as evidenced bymore grade repetitions, poorer grades in academic sub-jects, more placement in special classes, and more tu-toring (94, 97-99). Findings also indicate that childrenwith attention deficit hyperactivity disorder performmore poorly than control subjects on standard meas-ures of intelligence and achievement (Si). Follow-up
studies have found that the academic and learningproblems of children with attention deficit hyperactiv-
ity disorder persist into adolescence and are associatedwith chronic underachievement and school failure (10,18). It is still unknown whether school failure in chil-dren with attention deficit hyperactivity disorder isrelated to the psychiatric picture of inattention andimpulsivity (attention deficit hyperactivity disorder),cognitive deficits (learning disabilities), a combinationof both factors (attention deficit hyperactivity disorder
bRange.Clnformation not provided.dMean
plus learning disabilities), or perhaps other factors
such as social disadvantage or demoralization and con-sequent decline in motivation (51).
The finding in some studies that learning disabilitiesare almost universally found among children with at-tention deficit hyperactivity disorder (94) has led someauthors to suggest that attention deficit hyperactivitydisorder and learning disabilities may be indistinguish-able (100). However, important differences exist in thedefining characteristics of both disorders. Although at-tention deficit hyperactivity disorder is a behavioralsyndrome with characteristic symptoms of inattentive-ness, impulsivity, and hyperactivity, learning disabili-ties refer to a group of cognitive disorders thought toreflect perceptual handicaps in one or more basic cog-nitive processes manifested as disorders of language,reading, writing and spelling, or arithmetic. Moreover,many children with attention deficit hyperactivity dis-order are achieving adequately, and not all childrenwith learning disabilities have attention deficit hyper-activity disorder, suggesting that the two disordersmay be independent but can overlap in some individ-uals (101).
In an attempt to clarify the nature of the associationbetween attention deficit hyperactivity disorder andlearning disabilities, researchers have begun to corn-pare subgroups of children with learning disabilities,attention deficit hyperactivity disorder, and attentiondeficit hyperactivity disorder plus learning disabilities(93, 102). Although this approach holds promise, moststudies have found few differences among subgroups.

BIEDERMAN, NEWCORN, AND SPRICH
Am J Psychiatry 148:5, May 1991 573
TABLE 3 (continued)
Instruments Used Findings5
Structured interviews
Structured interviews, behavior checklists
None of hyperactive vs. 2% of control had current anxiety disorder; none of hyperactivevs. 3% of control had history of anxiety disorder
26% of ADD had anxiety; 24% of anxious had ADD
Structured interviews, behavior checklists 43% of ADD vs. 10% of ADDH had concurrent internalizing diagnosis
Semistructured interviews 16.7% of those with separation anxiety had ADD; 18.2% of overanxious had ADD
Structured interviews 27% of ADD vs. 15% of control had anxiety
Structured interviews, personalityinventories
Structured interviews, behavior checklists
33% with panic disorder parents vs. 6% with control parents had ADD according tochild report; 43% with panic disorder parents had panic disorder by parent report;40% with panic disorder parents had panic disorder by child report
8% of ADD had anxiety; 18% of anxious had ADD
Structured interviews
Clinical interviews, observational measures,memory tests
Behavior checklists, IQ testsStructured interviews
Current anxiety disorders rare in ADD; lifetime (since age 13) prevalence of anxiety dis-orders not significantly different between ADD and control
28% of ADHD had anxiety; ADHD+anxiety had significantly less CD than did ADHD;ADHD+anxiety had poorer response to methylphemdate than ADHD
61% had ADHD+anxiery30% of ADD vs. 15% of normal control had anxiety
For example, Halperin et al. (93) compared childrenwith attention deficit hyperactivity disorder plus learn-ing disabilities (reading disabilities) with children withonly attention deficit hyperactivity disorder to examinewhether children with both disorders constitute a dis-tinct subgroup. The authors interpreted their findingthat the two groups did not differ behaviorally or insociodemographic characteristics as giving minimalsupport to the usefulness of subgrouping attention def-icit hyperactivity disorder on the basis of the presenceof learning disabilities. In a study using a similar designand analytic approach, Ackerman et al. (102) alsofailed to find differences between children with comor-bid attention deficit hyperactivity disorder and learn-ing disabilities and children with attention deficit hy-peractivity disorder alone on measures of impulsivityand response to stimulants. It is important to stress,however, that although the children in these studies allshared the clinical features of attention deficit hyper-activity disorder, they may have differed in fundamen-tal ways determined by the presence of learning dis-abilities and its correlates. The identification of thesedifferences may have major clinical and educationalimportance because the two disorders require differentintervention approaches. Although more research isneeded to further evaluate the nature of the associationbetween attention deficit hyperactivity disorder andlearning disabilities, the subgroup of children withattention deficit hyperactivity disorder plus learningdisabilities deserves special clinical and educationalattention.
COMORBIDITY WITH OTHER DISORDERS
Attention deficit hyperactivity disorder is generallyconsidered to be three to four times more prevalent inmentally retarded children than in those with normalIQ scores (103-106). In a study that analyzed the typeof behavioral disturbance as a function of IQ (104),conduct disorder was found to be far more commonthan attention deficit hyperactivity disorder in boyswith IQs greater than SO, but attention deficit hyper-activity disorder and conduct disorder were equallyprevalent in children with IQs less than SO. In anotherstudy (103), attention deficit hyperactivity disorderwas found to be much more common in the educablementally retarded (IQ greater than SO) than in the gen-eral population. Russell (106) has noted that individ-uals with IQs less than SO may exhibit different typesof psychiatric disorders than those with milder mentalretardation. In addition, studies in which stimulanttreatment has been shown to be effective in childrenwith attention deficit hyperactivity disorder plus men-tal retardation have been conducted only in subjectswith mild mental retardation (107, 108). These dataare consistent with a definition of attention deficit hy-peractivity disorder that allows comorbidity with mildmental retardation but imposes an IQ cutoff belowwhich attention deficit hyperactivity disorder shouldnot be diagnosed. Since attention deficit hyperactivitydisorder appears to occur with increasing frequency inindividuals with mental retardation, more work needsto be done to evaluate whether attention and activity

COMORBIDITY OF A1TEN11ON DISORDER
574 Am J Psychiatry 148:5, May 1991
problems in the mentally retarded should be viewed asconstituting attention deficit hyperactivity disorder orwhether they are a consequence of having a low IQ.
Comorbidity of Tourette’s syndrome and attentiondeficit hyperactivity disorder has been well docu-mented. Approximately 60% of children and adoles-cents with Tourette’s syndrome have been shown tohave comorbid attention deficit hyperactivity disorder(13, 109-1 1 1). Because the prevalence of attentiondeficit hyperactivity disorder is much higher than thatof Tourette’s syndrome, only a small percentage ofchildren with attention deficit hyperactivity disorderwill have comorbid Tourette’s syndrome. Although thecomorbidity figures from these studies are in closeagreement, discrepant viewpoints have been proposedregarding their interpretation. Comings and Comings(109, 1 1 1) contended that there is a genetic relation-ship between Tourette’s syndrome and attention deficithyperactivity disorder and that a Tourette’s syndromegene (as yet unidentified) accounts for approximately10%-30% of attention deficit hyperactivity disorder.Conversely, Pauls et al. (13) disputed the conclusionthat attention deficit hyperactivity disorder andTourette’s syndrome are genetically related. Identi-fication of children at risk for the development ofTourette’s syndrome within the larger population ofindividuals with attention deficit hyperactivity disor-der has important practical implications because psy-chostimulant treatment has been associated with thedevelopment of Tourette’s syndrome in some studies(1 12) and may be contraindicated in children at highrisk for Tourette’s syndrome.
Comorbidity of attention deficit hyperactivity disor-der and borderline personality disorder has been de-scribed by Andrulonis et al. (1 13), who found that25% of a group of 106 borderline patients with IQsgreater than 80 had a current or past history of atten-tion deficit hyperactivity disorder and/or learning dis-abilities. Similarly, Bellak et al. (1 14-1 16) described agroup of subjects with impulsive behavior, learningproblems, mood lability, impaired judgment, disorga-nization, and intermittently poor reality testing whomthey referred to as having attention deficit hyperac-tivity disorder psychosis. Successful treatment of co-morbid attention deficit hyperactivity disorder andborderline personality with methyiphenidate (1 1 7) andimipramine (1 1 8) has been described in case reports.
CONCLUSIONS
There is increasing recognition that attention deficithyperactivity disorder is a heterogeneous disorder withconsiderable and varied comorbidity. The weight ofthe available literature indicates the frequent occur-rence together of conduct, mood, and anxiety disor-ders, as well as learning disabilities, with attention def-icit hyperactivity disorder in childhood, adolescence,and adulthood. The observed comorbidity does notappear to be either random or artifactual. Rather, spe-
cific patterns of symptoms and syndromes tend to oc-cur together in individuals and families. Current re-search findings have begun to suggest that subgroupsmight be delineated on the basis of patterns of comor-bidity. Recent family-genetic data suggest that atten-tion deficit hyperactivity disorder plus conduct disor-der may be a distinct subtype, that attention deficithyperactivity disorder and major depression may sharecommon familial vulnerabilities, and that attentiondeficit hyperactivity disorder and anxiety disordersmay be independently transmitted. Ongoing researchon attention deficit hyperactivity disorder and comor-bid learning disabilities as well as other comorbid dis-orders will determine the nature of their association.Subgroups of patients with attention deficit hyper-activity disorder may have different risk factors,clinical courses, neurobiology, and pharmacologicalresponses, so their proper identification may lead torefinements in prevention and treatment strategies. Al-though the high level of comorbidity within attentiondeficit hyperactivity disorder may lead to problems indifferential diagnosis, these difficulties do not invali-date the diagnosis of the disorder. Rather, further ex-amination of the patterns and structure of observedcomorbidity could help to revise and improve existingmethods of classification.
REFERENCES
1. Costello EJ, Costello AJ, Edelbrock C, et al: Psychiatric dis-orders in pediatric primary care. Arch Gen Psychiatry 1988;45:1107-1116
2. AndersonJC, Williams 5, McGee R, et al: DSM-III disorders inpreadolescent children: prevalence in a large sample from thegeneral population. Arch Gen Psychiatry 1987; 44:69-76
3. Bird HR, Canino G, Rubio-Stipec M, et al: Estimates of theprevalence of childhood maladjustment in a community surveyin Puerto Rico. Arch Gen Psychiatry 1988; 45:1120-1126
4. Mannuzza 5, Gittelman-Klein R, Horowitz-Konig P, et al: Hy-peractive boys almost grown up, IV: criminality and its rela-tionship to psychiatric status. Arch Gen Psychiatry 1989; 46:1073-1079
S. McGee R, Williams 5, Silva PH: Factor structure and corre-lates of ratings of inattention, hyperactivity, and antisocialbehavior in a large sample of 9-year-old children from thegeneral population. J Consult Clin Psychol 1985; 53:480-490
6. Biederman J, Faraone SV, Keenan K, et al: Family-genetic andpsychosocial risk factors in DSM-III attention deficit disorder.J Am Acad Child Adolesc Psychiatry 1990; 29:526-533
7. Hinshaw SP: On the distinction between attentional deficits/hyperactivity and conduct problems/aggression in child psy-chopathology. Psychol Bull 1987; 101:443-463
8. Maser JD, Cloninger CR: Comorbidity of anxiety and mooddisorders: introduction and overview, in Comorbidity ofMood and Anxiety Disorders. Edited by Maser JD, CloningerCR. Washington, DC, American Psychiatric Press, 1990
9. Gittelman R, Mannuzza 5: Hyperactive boys almost grownup, III: methylphenidate effects on ultimate height. Arch GenPsychiatry 1988; 45:1131-1134
10. Weiss G, Hechtman L, Milroy T, et at: Psychiatric status ofhyperactives as adults: a controlled prospective 15-year fol-low-up of63 hyperactive chuldren.J Am Acad Child Psychiatry1985; 24:211-220
11. Maser JD, Cloninger CR (eds): Comorbidiry of Mood andAnxiety Disorders. Washington, DC, American PsychiatricPress, 1990, p 867

BIEDERMAN, NEWCORN, AND SPRICH
Am J Psychiatry 148:5, May I 991 575
12. Rutter M: Isle of Wight revisited: twenty-five years of childpsychiatric epidemiology. J Am Acad Child Adolesc Psychiatry1989; 28:633-653 ‘. ..
13. Pauls DL, Hurst CR, Kruger SD, et al: Gilles de Ia burette’ssyndrome and attention deficit disorder with hyperactivity:evidence against a genetic relationship. Arch Gen Psychiatry1986; 43:1177-1179
14. Taylor EA: Childhood hyperactivity. Br J Psychiatry 1986;149:562-573
is. Taylor E, Everitt B, Thorley G, et al: Conduct disorder andhyperactivity, II: a cluster analytic approach to the identifica-tion of a behavioural syndrome. Br J Psychiatry 1986; 149:768-777
16. Taylor E, Schachar R, Thorley G, et al: Conduct disorder andhyperactivity, I: separation of hyperactivity and antisocial con-duct in British child psychiatric patients. Br J Psychiatry 1986;149:760-767
17. Rutter M: Syndromes attributed to “minimal brain dysfunc-tion” in childhood. Am J Psychiatry 1982; 139:21-33
18. Gittelman R, Mannuzza 5, Shenker R, er al: Hyperactive boysalmost grown up. Arch Gen Psychiatry 1985; 42:937-947
19. Loeber R, Brinthaupt VP, Green SM: Attention deficits, im-pulsivity, and hyperactivity with or without conduct prob-lems: relationships to delinquency and unique contextualfactors, in Behavior Disorders of Adolescence: Research, In-tervention, and Policy in Clinical and School Settings. Editedby McMahon RJ, Peters RD. New York, Plenum, 1988
20. Barkley RA: A review of stimulant drug research with hyper-active children. J Child Psychol Psychiatry 1977; 18:137-165
21. Szatmari P, Boyle M, Offord DR: ADDH and conduct disor-der: degree of diagnostic overlap and differences among cor-relates. J Am Acad Child Adolesc Psychiatry 1989; 28:865-872
22. Biederman J, Munir K, Knee D, et al: A controlled family studyof patients with attention deficit disorder and normal controls.J Psychiatr Res 1986; 20:263-274
23. Faraone SV, Biederman J, Keenan K, et al: A family-geneticstudy of girls with DSM-III attention deficit disorder. Am JPsychiatry 1991; 148:112-117
24. Biederman J, Munir K, Knee D: Conduct and oppositionaldisorder in clinically referred children with attention deficitdisorder: a controlled family study. J Am Acad Child AdolescPsychiatry 1987; 26:724-727
25. Stewart MA, Cummings C, Singer 5, er al: The overlap be-tween hyperactive and unsocialized aggressive children. JChild Psychol Psychiatry 1981; 22:35-45
26. Stewart MA, Behar D: Subtypes of aggressive conduct disor-der. Acta Psychiatr Scand 1983; 68:178-185
27. Shapiro 5K, Garfinkel HD: The occurrence of behavior disor-ders in children: the interdependence of attention deficit dis-order and conduct disorder.J Am Acad Child Psychiatry 1986;25:809-819
28. Sandberg Sb, Rutter M, Taylor E: Hyperkinetic disorder inpsychiatric clinic attenders. Dcv Med Child Neurol 1978; 20:279-299
29. Prinz RJ, Connor PA, Wilson CC: Hyperactive and aggressivebehaviors in childhood: intertwined dimensions. J AbnormChild Psychol 1981; 9:191-202
30. Loney J, Langhorne JEJ, Paternite CE: Empirical basis for sub-grouping the hyperkinetic/minimal brain dysfunction syn-drome. J Abnorm Psychol 1978; 87:431-441
31. Loney J: Hyperactivity and aggression in the diagnosis of at-tention deficit disorder, in Advances in Clinical Child Psychol-ogy. Edited by Lahey BB, Kazdin AE. New York, Plenum,1987
32. Milich R, Loney J: The role of hyperactive and aggressivesymptomatology in predicting adolescent outcome among hy-peractive children. J Pediatr Psychol 1979; 4:93-i 12
33. Milich R, Loney J, Landau 5: Independent dimensions of hy-peractivity and aggression: a validation with playroom obser-vation data. J Abnorm Psychol 1982; 91:183-198
34. Milich R, Widiger TA, Landau 5: Differential diagnosis ofattention deficit and conduct disorders using conditional prob-
abilities. J Consult Clin Psychol 1987; 55:762-76735. Offord DR, Sullivan K, Allen N, et al: Delinquency and hy-
peractivity. J Nerv Ment Dis 1979; 167:734-74136. Lahey BD, Green KD, Forehand R: On the independence of
rating hyperactivity, conduct problems, and attention deficitsin children: a multiple regression analysis. J Consult Clin Psy-chol 1980; 48:566-574
37. Sandberg Sb, Wieselberg M, Shaffer D: Hyperkinetic and con-duct problem children in a primary school population: someepidemiologic considerations. J Child Psychol Psychiatry1980; 21:293-311
38. August GJ, Stewart MA, Holmes CS: A four-year follow-up ofhyperactive boys with and without conduct disorder. Br J Psy-chiatry 1983; 143:192-198
39. August GJ, Stewart MA: Familial subtypes of childhood hy-peractivity. J Nerv Ment Dis 1983; 171:362-368
40. Thorley G: Hyperkinetic syndrome ofchildhood: clinical char-acteristics. Br J Psychiatry 1984; 144:16-24
41. Reeves JC, Werry JS, Elkind GS, et al: Attention deficit, con-duct, oppositional, and anxiety disorders in children, II: din-ical characteristics. J Am Acad Child Adolesc Psychiatry 1987;26: 144-155
42. Klorman R, Brumaghim JT, Salzman LF, et al: Effects of meth-ylphenidate on attention-deficit hyperactivity disorder withand without aggressive/noncompliant features. J Abnorm Psy-chol 1988; 97:413-422
43. Lahey BB, Peiham WE, Schaughency EA, er al: Dimensionsand types of attention deficit disorder. J Am Acad Child Ad-olesc Psychiatry 1988; 27:330-335
44. Barkley RA, McMurray MB, Edelbrock CS, et al: The re-sponse of aggressive and nonaggressive ADHD children to twodoses of methylphenidate. J Am Acad Child Adolesc Psychia-try 1989; 28:873-881
45. Farrington DP, Loeber R, Van Kammen WB: Long-term aim-inal outcomes of hyperactivity-impulsivity-attention deficitand conduct problems in childhood, in Straight and DeviousPathways to Adulthood. Edited by Robins LN, Rutter MR.New York, Cambridge University Press, 1989
46. Faraone SV, Biederman J, Keenan K, et al: Separation of DSM-III attention deficit disorder and conduct disorder: evidencefrom a family-genetic study of American child psychiatric pa-tients. Psychol Med (in press)
47. Rutter M: Questions and findings on the concept of a distinctsyndrome, in Developmental Neuropsychiatry. Edited by Rut-ter M. New York, Guilford Press, 1983
48. Quay HC: A critical analysis of DSM-III as a taxonomy ofpsychopathology in childhood and adolescence, in Contempo-rary Issues in Psychopathology. Edited by Millon T, KlermanG. New York, Guilford Press, 1986
49. Loney J, Milich R: Hyperactivity, inattention, and aggressionin clinical practice, in Advances in Developmental and Behav-ioral Pediatrics, vol 3. Edited by Wolraich M, Routh DK.Greenwich, Conn, JA! Press, 1982
so. Quay HC, Routh DK, Shapiro 5K: Psychopathology of child-hood: from description to validation. Annu Rev Psychol 1987;38:491-532
Si. Campbell SB, Werry JS: Attention deficit disorder (hyperactiv-ity), in Psychopathologic Disorders of Childhood. Edited byQuay HC, Werry JS. New York, John Wiley & Sons, 1986
52. Quay HC: Conduct disorder, in Psychopathologic Disordersof Childhood. Ibid
53. LoneyJ, KramerJ, Milich RS: The hyperactive child grows up:predictors of symptoms, delinquency and achievement at fol-low-up, in Psychosocial Aspects of Drug Treatment for Hy-peractivity. Edited by Gadow KD, Loney J. Boulder, CO,Westview Press, 1981
54. Stewart MA, DeBlois CS, Cummings C: Psychiatric disorder inthe parents of hyperactive boys and those with conduct disor-der. J Child Psychol Psychiatry 1980; 21:283-292
55. McGee R, Williams 5, Silva PA: Behavioral and developmentalcharacteristics of aggressive, hyperactive and aggressive-hyper-active boys. J Am Acad Child Psychiatry 1984; 23:270-279
56. McGee R, Williams 5, Silva PA: Background characteristics of

COMORBIDITY OF A1TENTION DISORDER
576 Am J Psychiatry 148:5, May 1991
aggressive, hyperactive and aggressive-hyperactive boys. J AmAcad Child Psychiatry 1984; 23:280-284
57. August GJ, Holmes CS: Behavior and academic achievementin hyperactive subgroups and learning-disabled boys. Am J DisChild 1984; 138:1025-1029
58. Robins L (ed): Deviant Children Grown Up. Baltimore, Wil-hams & Wilkins, 1966
59. Singer SM, Stewart MA, Pulaski L: Minimal brain dysfunc-tion: differences in cognitive organization in two groups ofindex cases and their relatives. J Learning Disord 1981; 14:470-473
60. Wood D, Wender PH, Reimherr FW: The prevalence of atten-tion deficit disorder, residual type, or minimal brain dysfunc-tion, in a population of male alcoholic patients. Am J Psychi-atry 1983; 140:95-98
61. Alterman Al, Petrarulo E, barter R, et al: Hyperactivity andalcoholism: familial and behavioral correlates. Addict Behav1982; 7:413-421
62. DeObaldia R, Pasons OA: Relationship of neuropsychologicalperformance to primary alcoholism and self-reported symp-toms of childhood minimal brain dysfunction. J Stud Alcohol1984; 45:386-391
63. Eyre SL, Rounsaville BJ, Kleber HD: History of childhoodhyperactivity in a clinical population of opiate addicts. J NervMent Dis 1982; 170:522-529
64. Cocores JA, Davies RK, Mueller PS, et al: Cocaine abuse andadult attention deficit disorder. J Clin Psychiatry 1987; 48:376-377
65. Weiss G: Follow-up studies on outcome of hyperactive chil-dren. Psychopharmacol Bull 1985; 21:169-177
66. Popper CW: Disorders usually first evident in infancy, child-hood, or adolescence, in The American Psychiatric Press Text-book of Psychiatry. Edited by TalbottJA, Hales RE, YudofskySC. Washington, DC, American Psychiatric Press, 1988
67. Werry JS, Reeves JC, Elkind GS: Attention deficit, conduct,oppositional, and anxiety disorders in children, I: a review ofresearch on differentiating characteristics. J Am Acad ChildAdolesc Psychiatry 1987; 26:133-143
68. Staton RD, Brumback RA: Non-specificity of motor hyperac-tivity as a diagnostic criterion. Percept Mot Skills 1981; 52:323-332
69. Munir K, Biederman J, Knee D: Psychiatric comorbidity inpatients with attention deficit disorder: a controlled study. JAm Acad Child Adolesc Psychiatry 1987; 26:844-848
70. Jensen JB, Burke N, Garfinkel BD: Depression and symptomsof attention deficit disorder with hyperactivity. J Am AcadChild Adolesc Psychiatry 1988; 27:742-747
71. Woolston JL, Rosenthal SL, Riddle MA, et al: Childhood co-morbidity of anxiety/affective disorders and behavior disor-ders. J Am Acad Child Adolesc Psychiatry 1989; 28:707-713
72. Stewart MA, Morrison JR: Affective disorders among the rd.atives of hyperactive children. J Child Psychol Psychiatry1973; 14:209-212
73. Bohline DS: Intellectual and affective characteristics of atten-tion deficit disordered children. J Learning Disord 1985; 18:604-608
74. Biederman J, Munir K, Knee D, er al: High rate of affectivedisorders in probands with attention deficit disorder and intheir relatives: a controlled family study. Am J Psychiatry1987; 144:330-333
75. Alessi NE, Magen J: Comorbidity of other psychiatric distur-bances in depressed, psychiatrically hospitalized children. AmJ Psychiatry 1988; 145:1582-1584
76. Biederman J, Faraone SV, Keenan K, et al: Evidence of familialassociation between attention deficit disorder and major affec-tive disorders. Arch Gen Psychiatry (in press)
77. Brown Rb, Borden KA, Clingerman SR, er al: Depression inattention deficit-disordered and normal children and their par-ents. Child Psychiatry Hum Dcv 1988; 18:119-132
78. Keller MB, Beardslee W, Lavori PW, et al: Course of majordepression in non-referred adolescents: a retrospective study. JAffective Disord 1988; 15:235-243
79. Orvaschel H, Walsh-Allis G, Ye W: Psychopathology in chit-
dren of parents with recurrent depression. J Abnorm ChildPsychol 1988; 16:17-28
80. Strober M, Morrell W, Burroughs J, et al: A family study ofbipolar I disorder in adolescence: early onset of symptomslinked to increased familial loading and lithium resistance. JAffective Disord 1988; 15:255-268
81. Weinberg WA, McLean A, Snider RL, et al: Depression, learn-ing disability and school behavior problems. Psychol Rep1989; 64:275-283
82. Deutsch CK, Swanson JM, Bruell JM, et al: Overrepresenta-non of adoptees in children with the attention deficit disorder.Behav Genet 1982; 12:231-238
83. Dvoredsky A, Stewart M: Hyperactivity followed by manicdepressive disorder: two case reports. J Clin Psychiatry 1981;42:212-214
84. Biederman J, Faraone 5, Keenan K, et al: Family genetic andpsychosocial risk factors in attention deficit disorder (ab-stract). Biol Psychiatry 1989; 25(7A, suppl): 145A
85. Kovacs M, Feinberg TL, Crouse N, et al: Depressive disordersin childhood, I: a longitudinal prospective study of character-istics and recovery. Arch Gen Psychiatry 1984; 41:229-237
86. Kovacs M, Paulauskas 5, Gatsonis C, et al: Depressive disor-ders in childhood, III: a longitudinal study ofcomorbidity withand risk for conduct disorders. J Affective Disord 1988; 15:205-217
87. Brent DA, Perper JA, Goldstein CE, et al: Risk factors foradolescent suicide: a comparison of adolescent suicide victimswith suicidal inpatients. Arch Gen Psychiatry 1988; 45:58 1-588
88. Last CG, Strauss CC, Francis G: Comorbidity among child-hood anxiety disorders. J Nerv Ment Dis 1987; 17S:726-730
89. Pliszka SR: Effect of anxiety on cognition, behavior, and stim-ulant response in ADHD.J Am Acad Child Adolesc Psychiatry1989; 28:882-887
90. Lahey BB, Schaughency EA, Hynd GW, et al: Attention deficitdisorder with and without hyperactivity: comparison of be-havioral characteristics of clinic-referred children. J Am AcadChild Adolesc Psychiatry 1987; 26:718-723
91. Sylvester CE, Hyde TS, Reichler RJ: The Diagnostic Interviewfor Children and Personality Inventory for Children in studiesof children at risk for anxiety disorders or depression. J AmAcad Child Adolesc Psychiatry 1987; 26:668-675
92. Biederman J, Faraone SV, Keenan K, et al: Familial associationbetween attention deficit disorder and anxiety disorders. Am JPsychiatry 1991; 148:251-256
93. Halperin JM, Gittelman R, Klein DF, et al: Reading-disabledhyperactive children: a distinct subgroup of attention deficitdisorder with hyperactivity. J Abnorm Child Psychol 1984;12:1-14
94. Silver LB: The relationship between learning disabilities, hy-peractivity, distractibility, and behavioral problems. J AmAcad Child Psychiatry 1981; 20:385-397
95. Halperin JM, Gittelman R: Do hyperactive children and theirsiblings differ in IQ and academic achievement? Psychiatry Res1982; 6:253-258
96. August GJ, Garfinkel BD: Behavioral and cognitive subtypesof ADHD. J Am Acad Child Adolesc Psychiatry 1989; 28:739-748
97. Weiss G, Hechtman L, Perlman b, et al: Hyperactives as youngadults: a controlled prospective ten-year follow-up of 75 cliii-dren. Arch Gen Psychiatry 1979; 36:675-681
98. Edelbrock C, Costello AJ, Kessler MD: Empirical corrobora-tion of attention deficit disorder. J Am Acad Child Psychiatry1984; 23:285-290
99. Lahey BB, Schaughency EA, Strauss CC, et al: Are attentiondeficit disorders with and without hyperactivity similar or dis-similar disorders? J Am Acad Child Psychiatry 1984; 23:302-309
100. Prior M, Sanson A: Attention deficit disorder with hyperactiv-ity: a critique. J Child Psychol Psychiatry 1986; 27:307-3 19
101. Interagency Committee on Learning Disabilities (eds): Learn-ing Disabilities: A Report to the US Congress. Washington,DC, US Government Printing Office, 1987

BIEDERMAN, NEWCORN, AND SPRICH
Am J Psychiatry 148:5, May 1991 S77
102. Ackerman Pb, Elardo PT, Dykman RA: A psychosocial studyof hyperactive and learning-disabled boys. J Abnorm ChildPsychol 1979; 7:91-99 .
103. Epstein MH, Cullinan D, Polloway ED: Patterns of maladjust-ment among mentally retarded children and youth. Am J MentDefic 1986; 91:127-134
104. Koller H, Richardson SA, Katz M: Behavior disturbance sincechildhood among a 5-year birth cohort of all mentally retardedyoung adults in a city. Am J Ment Defic 1983; 87:386-395
105. Hunt RD, Cohen DJ: Attentionat and neurochemical compo-nents of mental retardation: new methods for an old problem,in Mental Retardation and Mental Health: Classification, Di-agnosis, Treatment Services. Edited by Stark JA, MenolascinoFJ, Albaretli MM, et al. New York, Springer-Verlag, 1988
106. Russell AT: The association between mental retardation andpsychiatric disorder: epidemiological issues. Ibid
107. Chandler M, Guattieri CT, Fahs JJ: Other psychotropic drugs:stimulants, antidepressants, the anxiotytics, and lithium car-bonate, in Psychopharmacology of the Developmental Disabil-ities. Edited by Aman MG, Singh DN. New York, Springer-Verlag, 1988
108. Varley CK, brupin EW: Double-blind administration of meth-‘ ylphenidate to mentally retarded children with attention deficit
disorder: a preliminary study. AmJ Ment Defic 1982; 86:560-566
109. Comings DE, Comings BG: A controlled study of bourette
syndrome, 1: attention deficit disorder, learning disorders, andschool problems. Am J Hum Genet 1987; 41:701-741
110. Comings DE, Comings BG: bourette syndrome: clinical andpsychological aspects of 250 cases. Am J Hum Genet 1985;37:435-450
1 1 1 . Comings DE, Comings BG: Tourette syndrome and attentiondeficit disorder with hyperactivity: are they genetically related?J Am Acad Child Psychiatry 1984; 23:138-146
1 12. Lowe U, Cohen DJ, Detlor J: Stimulant medications precip-itate bourette’s syndrome. JAMA 1982; 247:1168-1169
1 13. Andrulonis PA, Glueck BC, Stroebel CF, er al: Borderline per-sonality subcategories. J Nerv Ment Dis 1982; 170:670-679
1 14. Bellak L: Schizophrenic syndrome related to minimal braindysfunction. Schizophr Bull 1979; 11:523-527
1 15. Bellak L: ADD psychosis as a separate entity. Schizophr Bull1985; 11:523-527
1 16. Bellak L, Kay SR, Opler LA: Attention deficit disorder psy-chosis as a diagnostic category. Psychiatr Dcv 1987; 3:239-263
1 1 7. Hooberman D, Stern TA: Treatment of attention deficit dis-order and borderline personality disorders with psychostimu-lants: case report. J Clin Psychiatry 1984; 45:441-442
1 18. Satel S, Southwick 5, Denton C: Use of imipramine for atten-tion deficit disorder in a borderline patient. J Nerv Ment Dis1988; 176:305-307
Related Documents